Embed Size (px)
Citation preview

New Diabetes Drugs: Where do they fit?Kathleen Dungan, MD 3/10/2012

2
Case 1
49 YO male with a 3 year history of T2DMPMH: osteoarthritis—unable to exercise PE: weight 120 kg, 5’10’’, BP 152/90, acanthosis nigricansMetformin 1gm BID, Glimepiride 8 mg. A1C is 7.7%.

Which of the following will likely get his A1c to goal?
a) b) c) d)
0% 0%0%0%
a) Begin an exercise program
b) Increase Glimepiride to 8 mg BID
c) Add Repaglinide 1 mg with meals
d) Add long-acting GLP-1

4
1950 1960 1970 1980 1990 2000 2010
1946: Sulfonylureas
1957: Biguanide
1995: α‐glucosidase Inhibitors
1997: M
egitinides
Thiazolidinediones
2005: GLP‐1 mimetics
Amylin analogue
2006: DPP‐IV Inhibitors
2008: Colesevalem
Tahrani et al. Lancet. 2011;378(9786):182‐97
2009: Bromocriptine
Colesevalem 2008Bromocriptine 2009Saxagliptin 2009Liraglutide 2010Linagliptin 2011
Exenatide QW 2012

5
Plasmaglucose
↓Insulinsecretion
↑Hepaticglucoseoutput
↓Peripheralglucose uptake
α‐Glucosidase inhibitorsIncretins
Pramlintide
Metformin
Cycloset
(glitazones)
Glitazones(metformin)Cycloset (adipose only)
Insulin SFU
Glinides
Incretins
Glucose influx↑ Glucagon secretion
Incretins
Pramlintide
Matching Pharmacology to Physiology
Renal glucose excretion
SGLT2 Inhibitor

Cycloset (Rapid-Release Bromocriptine)
Ventromedial hypothalamus (VMH)Circadian and seasonal changes in metabolismT2DM: Early AM dip in dopaminergic tone in T2DM→↑SNS activity
Energy Insulin VMH ActivityDopa Serotonin/NE
Summer Expending Sensitive ↑ ↓Winter Conserving Resistant ↓ ↑
Defronzo Diabetes Care 2011;34:789‐94

Efficacy
Given within 2 hr of awakening
Peak plasma conc. 60 min0.8 mg, titrate QW to max 4.8 mg/day
Shift workers excluded from trials
Defronzo Diabetes Care 2011;34:789‐94

Safety & Tolerability
Contra-indicationsOrthostasisSyncopal migrainesPsychotic disorders Other dopaminergic agonist therapy
TolerabilityN/VDizziness, fatigueHArhinitis

9
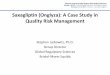
Kaplan‐Meier plot of time to first cardiovascular event T2DM treated with Cycloset or placebo for 52 weeks, N=3070.
DeFronzo R A Dia Care 2011;34:789‐794
Copyright © 2011 American Diabetes Association, Inc.
MACE: MI, stroke, death
CVE: MI, stroke, hospitalization for angina or CHF, coronary revascularization, death

10
Bile Acid Sequestrant
Agent in Class: ColesevalamOther BASs less selective for BA
May have glucose-lowering propertiesMore likely to bind to other meds
Mechanism of action uncertainEfficacy:
A1C -0.5-8% added to MTF, SFU or insulinLDL-C reductions of 12.3-16.1%
Bays HE, et al. Arch Intern Med. In press.Fonseca VA, et al. Diabetes Care. 2008; 31: 1479‐1484.Goldberg RB, et al. Arch Intern Med. 2008; 168: 1531‐1540.
Handelsman; Diabetes Care May 2011;34 :S244‐S250

Efficacy of Colesevalem
Reference N Background Baseline A1c
A1c Reduction*
LDL-c Reduction* (%)
TG Increase* (%)
1 216 MTF 7.65 0.30 16.3 18.62 286 MTF 8.15 0.54 15.9 4.73 316 SFU 8.25 0.55 16.7 17.74 287 Insulin 8.25 0.50 12.8 21.55 169 MTF 8.1 0.30 -11.6
*placebo adjusted except for reference 5, in which the comparator was rosiglitazone or sitagliptin and the A1c reduction was relative to baseline
1. Bays HE, et al. Arch Intern Med. 2008;168:1975‐1983.2. Rosenstock et al. Endocrine Practice. 2010;16(4):629‐640.3. Fonseca et al. Diabetes Care. 2008;31(8):1479‐14844. Goldberg et al. Arch Intern Med. 2008;168(14):1531‐1540.5. Rigby et al. Endocr Pract 2010;16:53–63
Brunetti & Campbell; Journal of Pharmacy Practice 24(4) 417‐425

12
Colesevelam
3.75 gm/dayTake with meals: 6 tablets QDAY or 3 tablets BIDNot systemically absorbed: no dose adjustments with hepatic or renal diseaseTake 4 hours after Glyburide, levothyroxine, and oral contraceptives containing ethinyl estradiol and norethindrone, phenytoin, warfarin, ?vitamins
Welchol® (colesevelam HCl) prescribing information. Daiichi Sankyo, Inc., Parsippany, NJ. January 2008.

Colesevalem
Adverse effects: constipationContraindications:
History of bowel obstruction Serum triglycerides >500 mg/dL (those with TG >300 were excluded from trials)?Fat soluble vitamins
Welchol® (colesevelam HCl) prescribing information. Daiichi Sankyo, Inc., Parsippany, NJ. January 2008.

14
GLP-1 Analog/mimetic and DPP-4 inhibitors:major differences
Properties/effect GLP-1 Analog/mimetic
DPP-4 inhibitors
Stimulation of insulin secretion exclusively through GLP-1
Yes Unknown
Hypoglycaemia No No
Inhibition of gastric emptying Yes Marginal
Effect on body weight Weight loss Weight neutral
Side effects Nausea None observed
Administration Subcutaneous Oral
Gallwitz. Eur Endocr Dis. 2006

GLP-1 Based TherapiesGeneric Name
Brand Name Dose forms Weight Contra-indications Renal dosing Interactions
DPP-IV inhibitors
Sitagliptin Januvia 25, 50, 100 mg Neutral Pancreatitis CrCl <30: 25 mg CrCl 30-50: 50 mg
NA
Linagliptin Tradjenta 5 mg Neutral Pancreatitis NA Avoid use with CYP3A4 or P-gp inducers
Saxagliptin Onglyza 2.5, 5 mg Neutral Pancreatitis 2.5 mg for CrCl<50
2.5 mg with strong CYP3A4/5 inhibitor
GLP-1 Analogues/Agonists
Exenatide Byetta 5, 10 mcg twice daily
Loss Pancreatitis, gastroparesis
contra-indicated if CCl<30
NA
Liraglutide Victoza 1.6, 1.2, 1.8 mg once daily
Loss Pancreatitis, gastroparesis, MEN2, medulary thyroid CA
NA NA
Exenatide QW (pending FDA)
Bydureon 2 mg Once weekly Loss Pancreatitis, gastroparesis, MEN2A, medullary thyroid CA
? NA

DPP-4 Inhibitors: Pharmacologic Comparisons
Sitagliptin Saxagliptin Linagliptin
DPP‐4 selectivity
Vs. DPP‐8 or 9 >2600 <100 >10,000
Vs. DPP‐2 >5550 >50,000 >100,000
Effect on active GLP‐1 levels
2x 1.5‐3x 4x
Renal excretion Predominant Predominant Minor
Plasma DPP‐4 Inhibition
>80% >80% >80%
Baetta & Corsini; Drugs 2011; 71 (11): 1441‐1467

17
Linagliptin
N Duration Back-ground
Comparator
Baseline A1c
A1c Reduction
Taskinen 688 24 wk MTF PBO 8.0 0.65Gomis 389 24 wk PIO PBO 8.6 0.5Owens 1040 24 wk MTF +
SFUPBO 8.1 0.62
Del Prato 469 24 wk None PBO 8.0 0.69
1. Taskinen et al. Diabetes Obes Metab. 2011;13:65–74.2. Gomis et al. Diabetes Obes Metab. 2011;13:653–661.3. Owens et al. Diabet Med. 2011 ;28(11):1352‐614. Del Prato et al. Diabetes Obes Metab. 2011;13:258–267.

18
Saxagliptin
N Duration Back-ground
Comparator
Baseline A1c
A1c Reduction
Rosenstock* 201 24 wk None PBO 8.0 0.7DeFronzo* 370 24 wk MTF PBO 8.1 0.8Chacra* 520 24 wk Glyburide Glyburide
uptitration8.5 0.7
Hollander* 370 24 wk TZD PBO 8.3 0.6Jadzinsky 648 24 wk MTF PBO 9.4 0.5
*Sustained A1c reduction over 76 weeks1.Rosenstock et al. Curr Med Res Opin. 2009;25:2401–11.2.DeFronzo et al. Diabetes Care. 2009;32:1649–55.3.Chacra et al. Int J Clin Pract. 2009;64.. Hollander P, et al. J Clin Endocrinol Metab. 2009;94:4810–9.5. Jadzinsky et al. Diabetes Obes Metab. 2009;11:611–22.

Safety of DPP-4
Meta-analysis of 53 trials at least 24 wk duration20,312 DPP-4, 13,569 comparators176 malignancies: MH-OR 1.02 [0.74-1.402]; p=0.90 257 MACE: MH-OR 0.69 [0.53-0.90], p = 0.00622 pancreatitis: 0.79 [0.36-1.73], p = 0.55
Monami et al. Curr Med Res Opin 2011;27:57-64

20
Liraglutide: A1c reduction
Blonde & Russell‐Jones. Diab Obes & Metab 2009;11:26‐34

21
Liraglutide: weight loss
Garber et al. Lancet. 2009;373(9662):473‐81

Liraglutide vs. Exenatide
Victoza associated with larger A1c reduction (0.33%, p<0.0001)Larger FBG reduction (18 mg/dl, p=0.0001)Less PPG reduction (24 mg/dl, p=0.0005)Similar weight loss 3.2 vs. 2.9 kg (p=0.22)Shorter duration of nausea (Treatment rate ratio 0.45, p<0.001), similar initial incidenceBetter treatment satisfaction (DTSQ, p=0.0004)
Buse et al. Lancet. 2009 Jul 4;374(9683):39-47.

23
Least squares mean CT concentration over 104 wk for liraglutide 0.6 mg (n = 242), 1.2 mg (n = 492), and 1.8 mg (n = 489); active comparator (n = 492); and placebo (n = 122).
Hegedüs L et al. JCEM 2011;96:853‐860
©2011 by Endocrine Society

24
2 mg once weekly, no dose titration

25

26
Adverse Event (AE) Related Withdrawals, and Selected AEs
DURATION StudiesExQW1,2
(n = 1379)ExBID1
(n = 147)Sita1
(n = 329)Pio1
(n = 328)IG1
(n = 223) MET1
(n = 246)Lira2
(n = 450)AE-Related Withdrawals (%) 4.5 4.9 1.8 3.4 0.9 1.6 5.3
Selected AE Incidences (%)*Nausea 14.5 34.3 6.7 4.6 1.3 6.9 20.4Vomiting 5.7 14.2 2.1 3.0 1.3 3.3 10.7Diarrhea 10.5 8.6 7.6 5.5 4.0 12.6 13.1Injection-Site Nodules 7.0 0.0 4.0 2.1 0.0 10.2 1.1
*The only AEs not included in this table that occurred at an incidence of ≥10% in the DURATION program were nasopharyngitis in 18.4% of IG patients, upper respiratory infection in 11.2% of ExBID patients and headache in 12.2% of MET patients; AE indicates adverse event; 1. Data on file, Amylin Pharmaceuticals; 2. Buse JB, et al. EASD 2011; 75-Oral
• The relative incidence of mild-to-moderate intensity nausea was reported to decrease over time with both exenatide formulations
• In DURATION-2 injection-site reactions with ExQW (10%) were comparable to injection-site reactions with placebo microsphere injections (7%)

Long-Acting GLP-1s
17 RCT, 6899 pts included Liraglutide and Exenatide QWTypically 26 weeks durationA1c reduction about 1%.
0.2% greater reduction than glargineGreater reduction than exenatide BID, sitagliptin and TZDSimilar reduction to SFU (Liraglutide)
Greater weight loss than most active comparators, including patients without nausea.
Shyangdan et al. Cochrane Database Syst Rev. 2011 Oct 5;(10):CD006423

AACE Guidelines
Endocrine Practice 2010

Approach to TherapyBest Next best No
Weight loss GLP‐1 SFU, Insulin, TZD
Weight‐sparing DPP‐4, MTF Bromocriptine, Colesevalem
SFU, Insulin, TZD
Cheap MTF, SFU Insulin, AGI All others
Renal disease DPP‐4 (may require dose‐adjust)
Liraglutide, Meglitinide, AGI
MTF, TZD
A1c lowering Insulin LA‐GLP‐1, MTF, TZD, SFU
No hypoglycemia MTF, GLP‐1, DPP‐4, TZD, AGI
Bromocriptine, Colesevalem
Insulin, SFU
Postprandial control
SA‐GLP‐1 DPP‐4, Meglitinide, LA‐GLP‐1, Prandial Insulin
Hyperlipidemia Colesevalem (except for high TG)
Rosiglitazone
Durability GLP‐1, TZD MTF? SFU

Case 2
58 YOF with a 5-year h/o T2DM PMH: HTN, dyslipidemia, CKDGlipizide 10 mg BID monotherapyPE: BP 110/70, BMI 29, 2+ pitting edemaLabwork:
HbA1c 7.5%Creatinine 1.6 mg/dlLipids: TC 198, LDLc 110 mg/dl, TG 401, HDLc 32MCR: 1200 mg/gm

Which of the following is appropriate next therapy?
1 2 3 4
0% 0%0%0%
1. Pioglitazone2. Colesevalem3. RA Bromocriptine4. Metformin