Embed Size (px)
Citation preview
New Data on Ultra Low-Dose Estradiol New Data on Ultra Low-Dose Estradiol Therapy in Osteoporosis PreventionTherapy in Osteoporosis Prevention
Marie Foegh, MD, DScMarie Foegh, MD, DScVP, Medical AffairsVP, Medical Affairs
Berlex LaboratoriesBerlex Laboratories
OutlineOutline
• BackgroundBackground
• StudyStudy– DesignDesign– EfficacyEfficacy– SafetySafety
• ConclusionConclusion
Loss of Estrogen has Profound Effects Loss of Estrogen has Profound Effects on Boneon Bone
• Increased resorptionIncreased resorption
• Rapid bone lossRapid bone loss
• Apoptosis of osteocytesApoptosis of osteocytes
• Increased risk of hip & spine Increased risk of hip & spine fracturefracture
Lowest effective doseLowest effective dose““for the individual patientfor the individual patient””
• Risk / Benefit Risk / Benefit
• Quality of Life Quality of Life
Ultra Low Dose TransdermalUltra Low Dose TransdermalEstrogen Replacement Assessment (ULTRA)Estrogen Replacement Assessment (ULTRA)
• UCSF Coordinating CenterUCSF Coordinating Center– Deborah Grady, Steven Cummings, Eric Vittinghoff, Deborah Grady, Steven Cummings, Eric Vittinghoff,
Judy Macer, Judy Quan, Lorie DentonJudy Macer, Judy Quan, Lorie Denton
• InvestigatorsInvestigators– B. Ettinger (Kaiser Permanente), K. Ensrud (University of Minnesota), B. Ettinger (Kaiser Permanente), K. Ensrud (University of Minnesota),
B. Wallace (University of Iowa), K. Johnson (University of Tennessee), B. Wallace (University of Iowa), K. Johnson (University of Tennessee),
P. Marx (Chicago Center for Clinical Research), S. Barbier (Seattle P. Marx (Chicago Center for Clinical Research), S. Barbier (Seattle
Women’s Clinical Research Center), J. Pinkerton (University of Women’s Clinical Research Center), J. Pinkerton (University of
Virginia), M. Farmer (Meridien Research) and D. Rowe (Palm Beach Virginia), M. Farmer (Meridien Research) and D. Rowe (Palm Beach
Research Center)Research Center)
DesignDesign
• Randomized, placebo-controlled, blinded trialRandomized, placebo-controlled, blinded trial
• 417 women (E2 n=208, placebo n=209)417 women (E2 n=208, placebo n=209)– 60 to 80 years old with an intact uterus60 to 80 years old with an intact uterus– More than 5 years post-menopausalMore than 5 years post-menopausal
– BMD z-score BMD z-score - 2.0 - 2.0
• Weekly transdermal E2 (0.014 mg/d) vs. placeboWeekly transdermal E2 (0.014 mg/d) vs. placebo– Goal to increase serum E2 to 10–15 pg/mLGoal to increase serum E2 to 10–15 pg/mL
• Daily calcium (800mg/d) and vitamin D (400 IU/d)Daily calcium (800mg/d) and vitamin D (400 IU/d)
• Duration of Study: 2 yearsDuration of Study: 2 years– Follow-up visits every 4 monthsFollow-up visits every 4 months
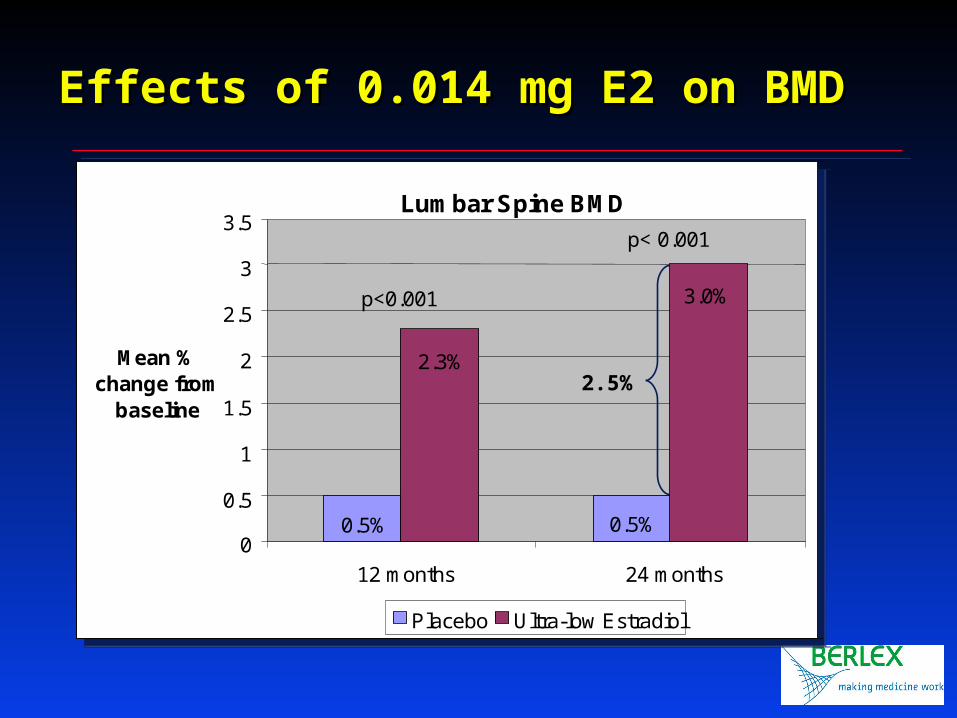
Lumbar Spine BMD
0.5% 0.5%
2.3%
3.0%
0
0.5
1
1.5
2
2.5
3
3.5
12 months 24 months
Mean % change from
baseline
Placebo Ultra-low Estradiol
p<0.001
p< 0.001
Lumbar Spine BMD
0.5% 0.5%
2.3%
3.0%
0
0.5
1
1.5
2
2.5
3
3.5
12 months 24 months
Mean % change from
baseline
Placebo Ultra-low Estradiol
p<0.001
p< 0.001
Effects of 0.014 mg E2 on BMDEffects of 0.014 mg E2 on BMD
2.5%
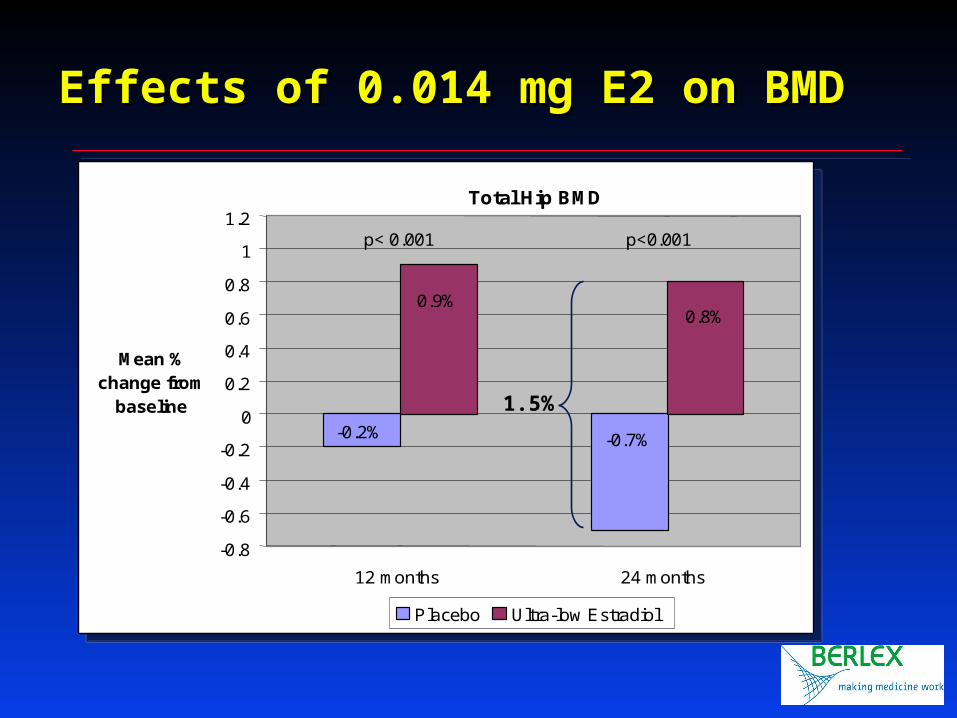
Total Hip BMD
-0.2% -0.7%
0.9% 0.8%
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
Mean % change from
baseline
Placebo Ultra-low Estradiol
12 months 24 months
p< 0.001 p<0.001
Total Hip BMD
-0.2% -0.7%
0.9% 0.8%
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
Mean % change from
baseline
Placebo Ultra-low Estradiol
12 months 24 months
p< 0.001 p<0.001
Effects of 0.014 mg E2 on BMDEffects of 0.014 mg E2 on BMD
1.5%
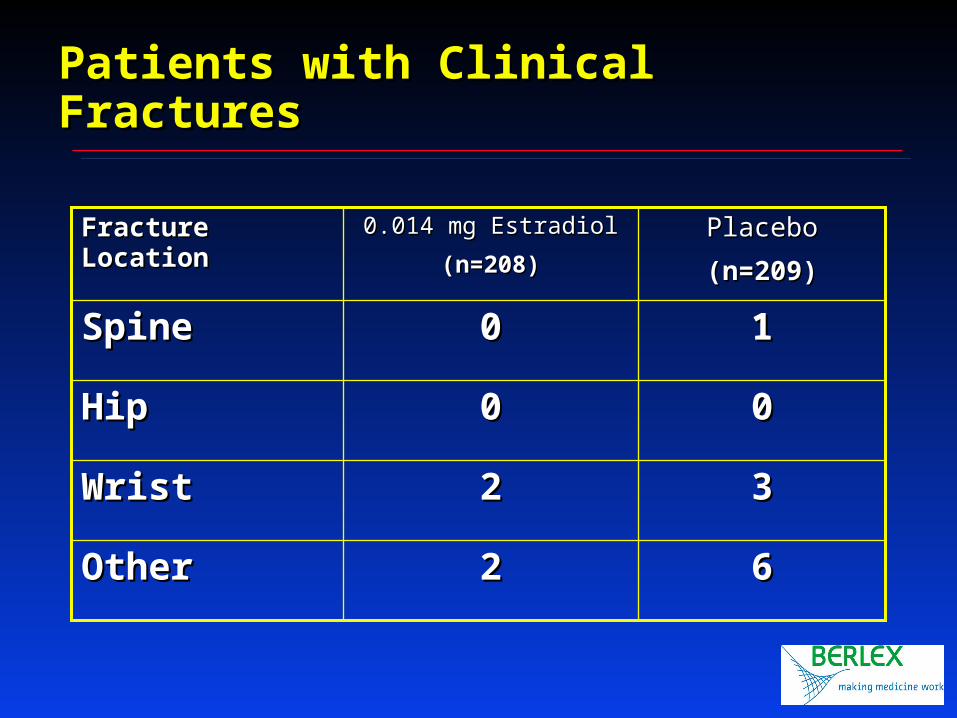
Patients with Clinical FracturesPatients with Clinical Fractures
6622OtherOther
3322WristWrist
0000HipHip
1100SpineSpine
PlaceboPlacebo
(n=209)(n=209)
0.014 mg Estradiol0.014 mg Estradiol
(n=208)(n=208)
Fracture LocationFracture Location
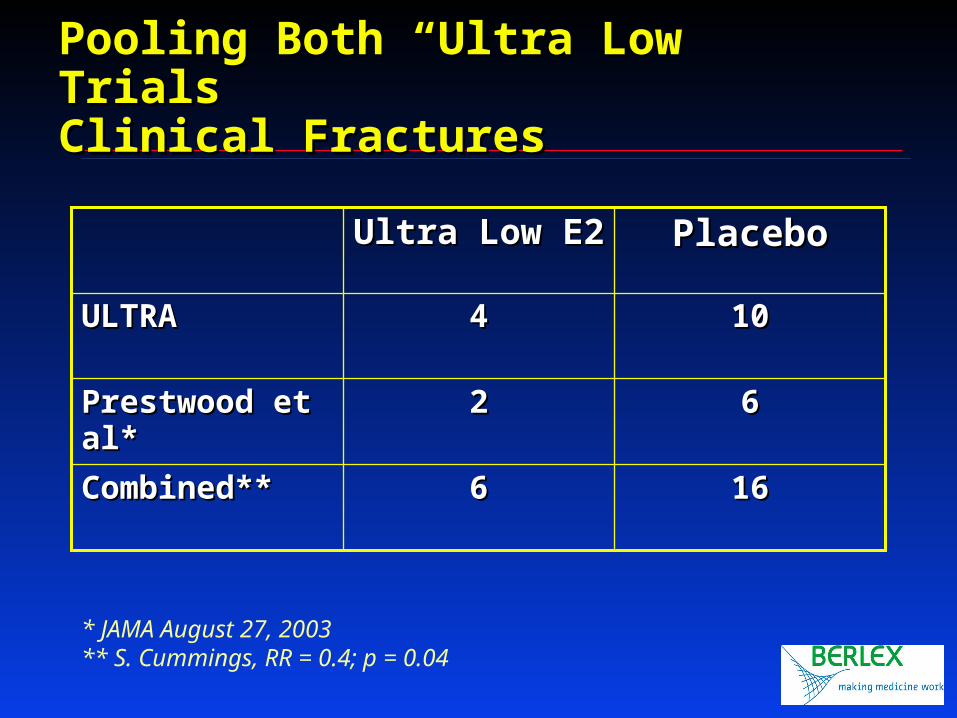
Pooling Both “Ultra Low” TrialsPooling Both “Ultra Low” TrialsClinical FracturesClinical Fractures
161666Combined**Combined**
6622Prestwood et al*Prestwood et al*
101044ULTRAULTRA
PlaceboPlaceboUltra Low E2Ultra Low E2
* JAMA August 27, 2003** S. Cummings, RR = 0.4; p = 0.04
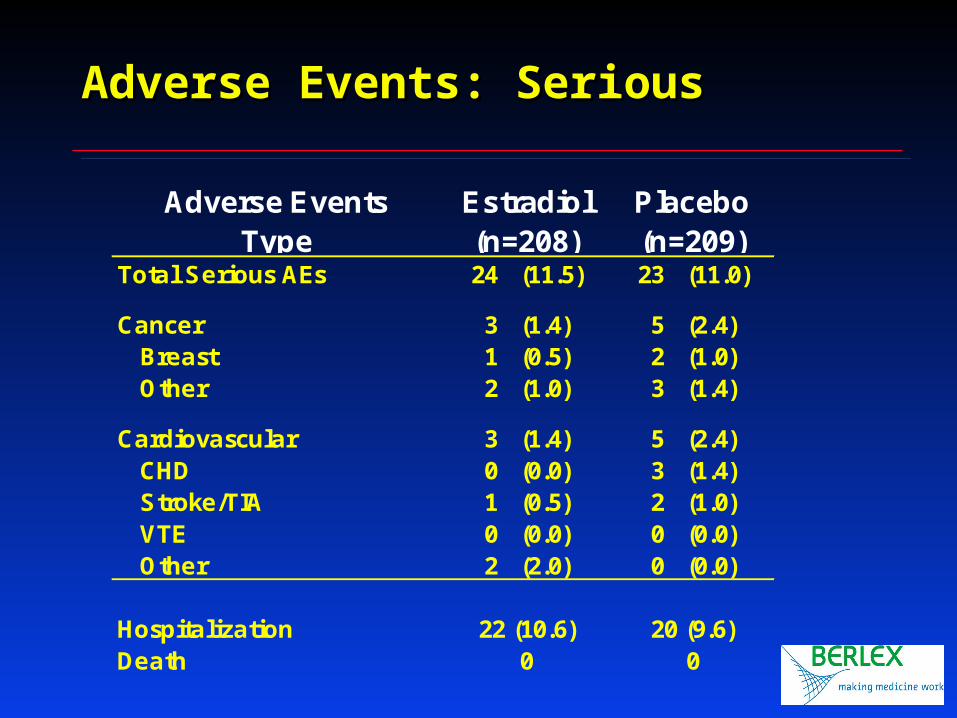
Adverse Events: SeriousAdverse Events: Serious
Adverse EventsType
Estradiol(n=208)
Placebo(n=209)
Total Serious AEs 24 (11.5) 23 (11.0)
Cancer 3 (1.4) 5 (2.4)Breast 1 (0.5) 2 (1.0)Other 2 (1.0) 3 (1.4)
Cardiovascular 3 (1.4) 5 (2.4)CHD 0 (0.0) 3 (1.4)Stroke/TIA 1 (0.5) 2 (1.0)VTE 0 (0.0) 0 (0.0)Other 2 (2.0) 0 (0.0)
Hospitalization 22 (10.6) 20 (9.6)Death 0 0
Ultra Trial ConclusionUltra Trial Conclusion
• Two years of unopposed ultra low dose Two years of unopposed ultra low dose transdermal estradioltransdermal estradiol–Prevents bone loss in older post-menopausal Prevents bone loss in older post-menopausal
womenwomen–Safe for the endometriumSafe for the endometrium–Decrease in markers of bone turnoverDecrease in markers of bone turnover–No increase in breast tenderness, headache and No increase in breast tenderness, headache and
other common estrogen-related adverse eventsother common estrogen-related adverse events–No effect on C-RP, SHBG, LipidsNo effect on C-RP, SHBG, Lipids
Paradigm Shift:Paradigm Shift:Changing the Risk/Benefit ProfileChanging the Risk/Benefit Profile
Ultra low dose estradiol:Ultra low dose estradiol:
• Fracture reduction in osteopenic patientsFracture reduction in osteopenic patients
• Ultra low dose Ultra low dose unopposedunopposed safe for the safe for the endometrium for up to two yearsendometrium for up to two years
• Adverse event profile similar to placeboAdverse event profile similar to placebo– No negative GI or vasomotor effectsNo negative GI or vasomotor effects

Markers of Bone TurnoverMarkers of Bone Turnover
* Change in median* Change in median
12 months* P-value
sCTX -20% <0.001Osteocalcin -16% <0.001BsAP -15% <0.001
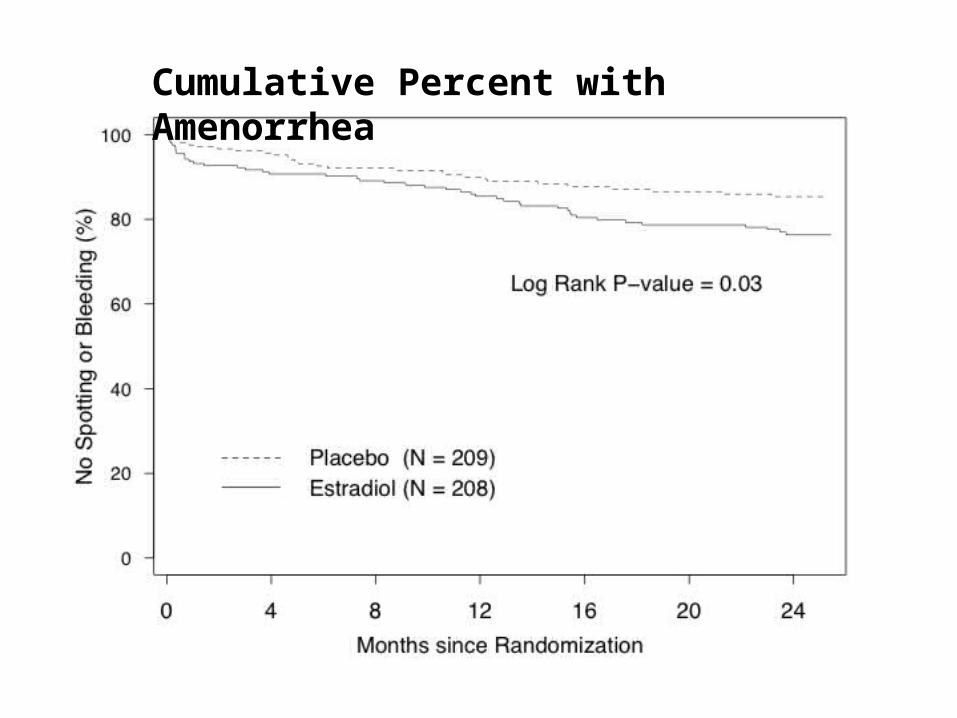
Cumulative Percent with Amenorrhea
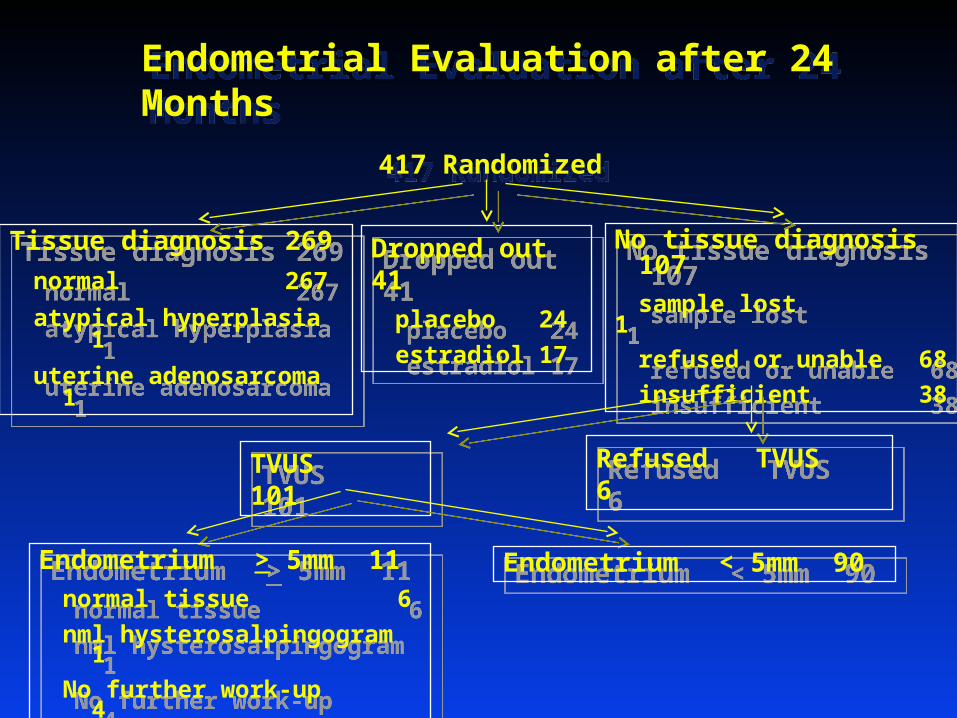
Endometrial Evaluation after 24 MonthsEndometrial Evaluation after 24 Months
417 Randomized417 Randomized
Tissue diagnosis 269
normal 267
atypical hyperplasia 1
uterine adenosarcoma 1
Tissue diagnosis 269
normal 267
atypical hyperplasia 1
uterine adenosarcoma 1
Dropped out 41
placebo 24
estradiol 17
Dropped out 41
placebo 24
estradiol 17
No tissue diagnosis 107
sample lost 1
refused or unable 68
insufficient 38
No tissue diagnosis 107
sample lost 1
refused or unable 68
insufficient 38
Refused TVUS 6Refused TVUS 6TVUS 101TVUS 101
Endometrium > 5mm 11
normal tissue 6
nml hysterosalpingogram 1
No further work-up 4
Endometrium > 5mm 11
normal tissue 6
nml hysterosalpingogram 1
No further work-up 4
Endometrium < 5mm 90Endometrium < 5mm 90
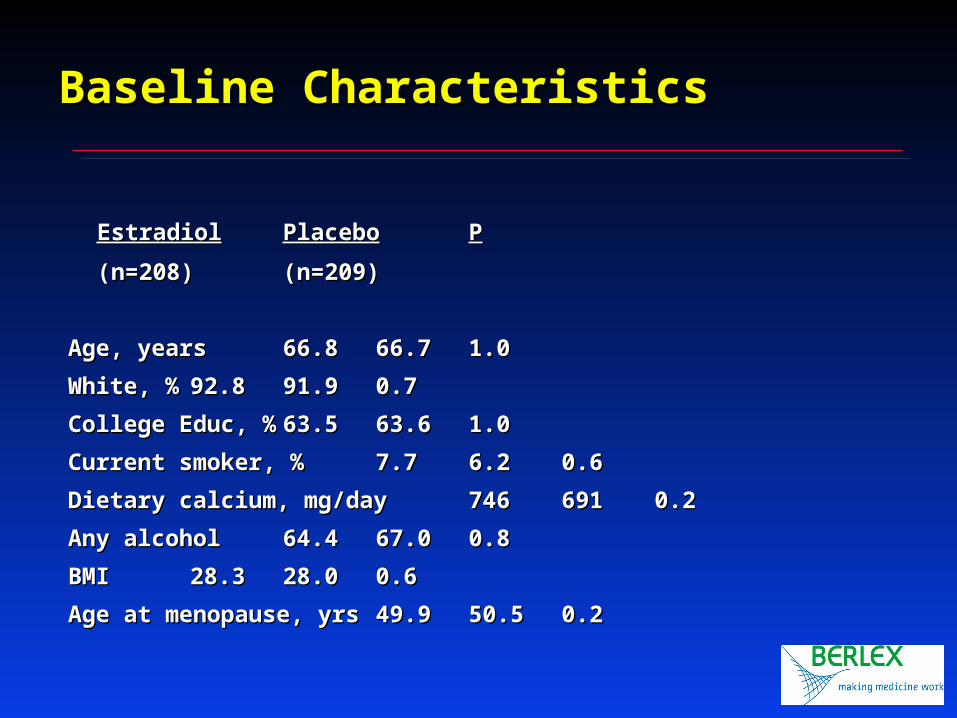
Baseline CharacteristicsBaseline Characteristics
EstradiolEstradiol PlaceboPlacebo PP
(n=208)(n=208) (n=209)(n=209)
Age, yearsAge, years 66.866.8 66.766.7 1.01.0
White, %White, % 92.892.8 91.991.9 0.70.7
College Educ, %College Educ, % 63.563.5 63.663.6 1.01.0
Current smoker, %Current smoker, % 7.77.7 6.26.2 0.60.6
Dietary calcium, mg/dayDietary calcium, mg/day 746746 691691 0.20.2
Any alcoholAny alcohol 64.464.4 67.067.0 0.80.8
BMIBMI 28.328.3 28.028.0 0.60.6
Age at menopause, yrsAge at menopause, yrs 49.949.9 50.550.5 0.20.2
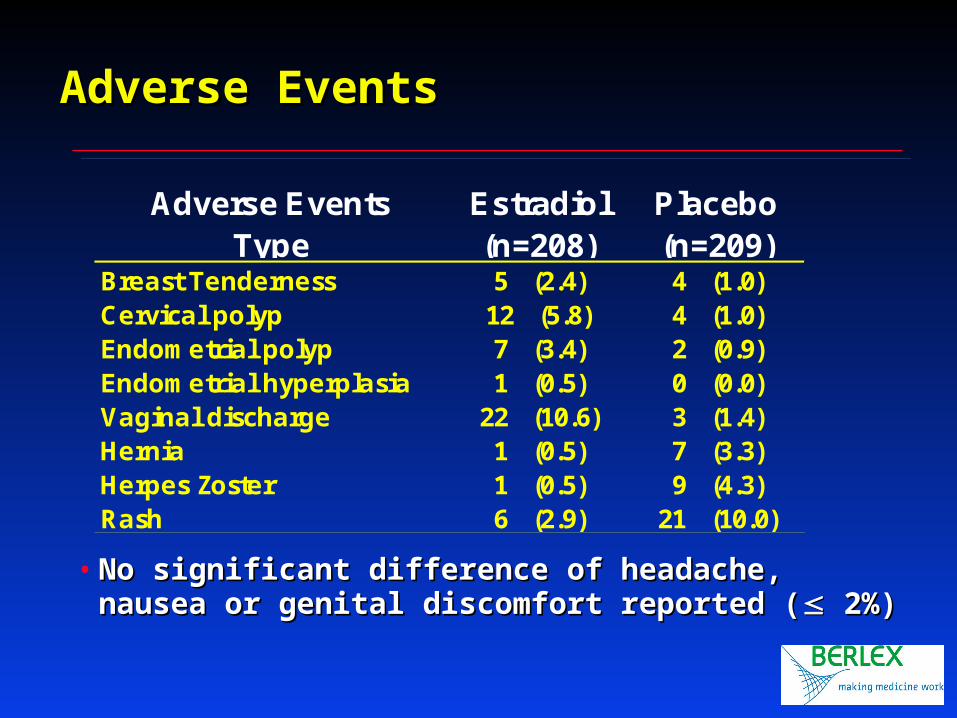
Adverse EventsAdverse Events
• No significant difference of headache, nausea or No significant difference of headache, nausea or genital discomfort reported (genital discomfort reported ( 2%) 2%)
Adverse EventsType
Estradiol(n=208)
Placebo(n=209)
Breast Tenderness 5 (2.4) 4 (1.0)Cervical polyp 12 (5.8) 4 (1.0)Endometrial polyp 7 (3.4) 2 (0.9)Endometrial hyperplasia 1 (0.5) 0 (0.0)Vaginal discharge 22 (10.6) 3 (1.4)Hernia 1 (0.5) 7 (3.3)Herpes Zoster 1 (0.5) 9 (4.3)Rash 6 (2.9) 21 (10.0)
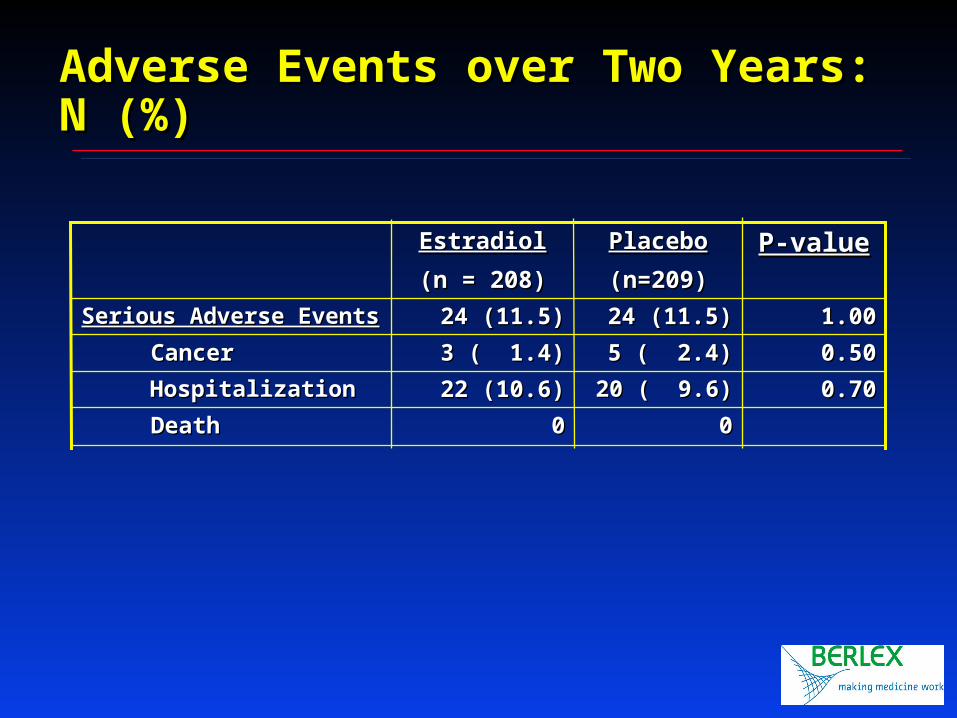
Adverse Events over Two Years: N (%)Adverse Events over Two Years: N (%)
0000 DeathDeath
0.700.7020 ( 9.6)20 ( 9.6)22 (10.6)22 (10.6) HospitalizationHospitalization
0.500.505 ( 2.4)5 ( 2.4)3 ( 1.4)3 ( 1.4) CancerCancer
1.001.0024 (11.5)24 (11.5)24 (11.5)24 (11.5)Serious Adverse EventsSerious Adverse Events
P-valueP-valuePlaceboPlacebo
(n=209)(n=209)
EstradiolEstradiol
(n = 208)(n = 208)
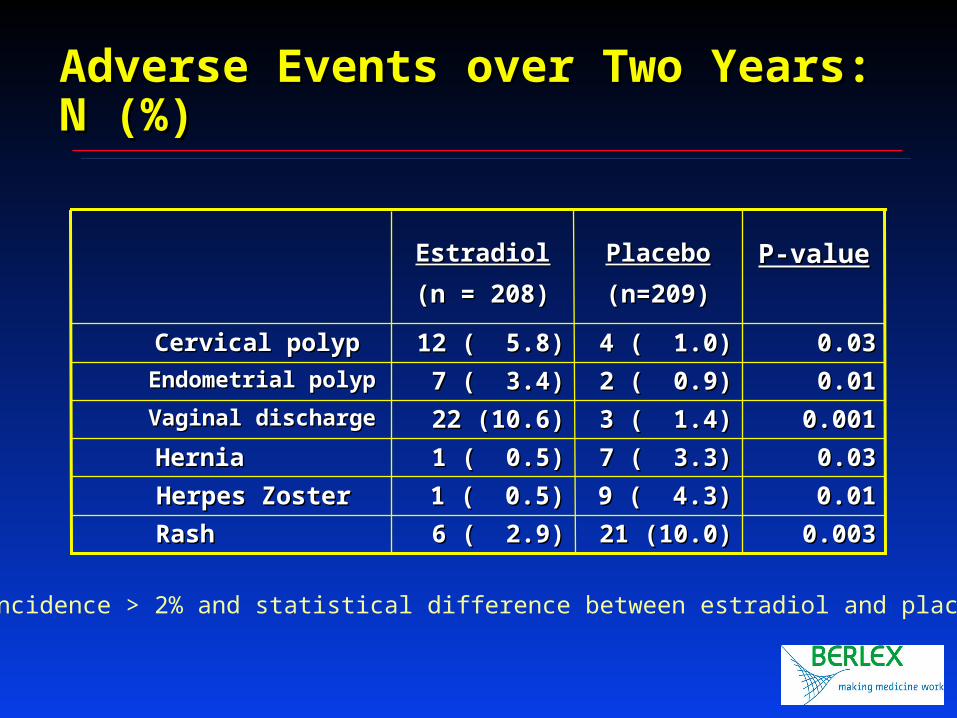
0.0030.00321 (10.0)21 (10.0)6 ( 2.9)6 ( 2.9) RashRash
0.010.019 ( 4.3)9 ( 4.3)1 ( 0.5)1 ( 0.5) Herpes ZosterHerpes Zoster
0.030.037 ( 3.3)7 ( 3.3)1 ( 0.5)1 ( 0.5) HerniaHernia
0.0010.0013 ( 1.4)3 ( 1.4)22 (10.6)22 (10.6) Vaginal dischargeVaginal discharge
0.010.012 ( 0.9)2 ( 0.9)7 ( 3.4)7 ( 3.4) Endometrial polypEndometrial polyp
0.030.034 ( 1.0)4 ( 1.0)12 ( 5.8)12 ( 5.8) Cervical polypCervical polyp
P-valueP-valuePlaceboPlacebo
(n=209)(n=209)
EstradiolEstradiol
(n = 208)(n = 208)
* incidence > 2% and statistical difference between estradiol and placebo
Adverse Events over Two Years: N (%)Adverse Events over Two Years: N (%)
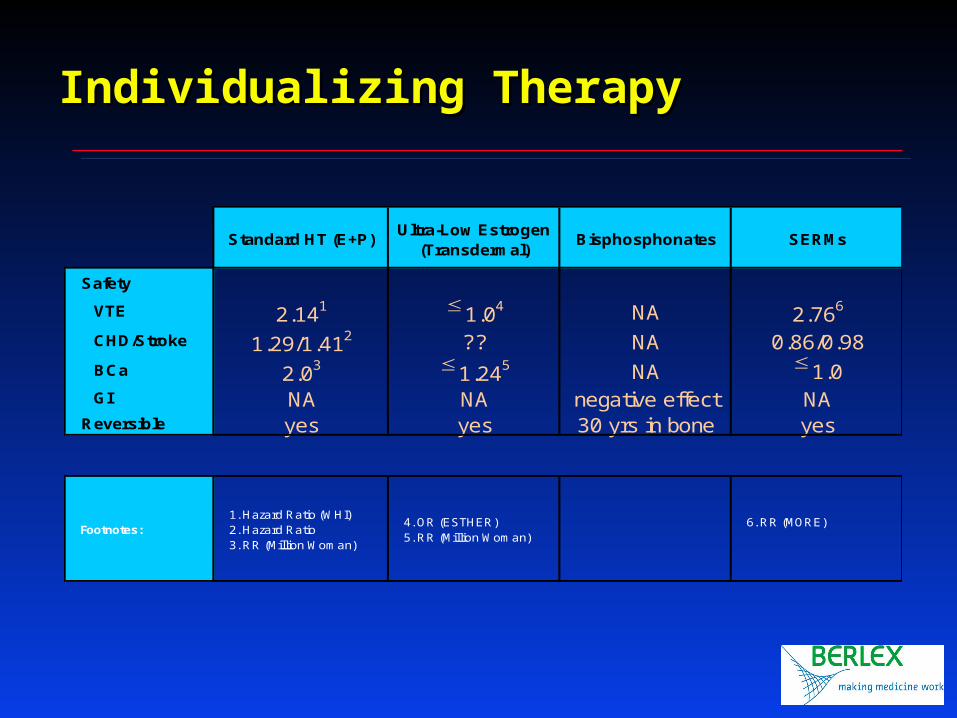
Standard HT (E+P)Ultra-Low Estrogen
(Transdermal)Bisphosphonates SERMs
Safety
VTE 2.141 1.04 NA 2.766
CHD/Stroke 1.29/1.412 ?? NA 0.86/0.98BCa 2.03 1.245 NA 1.0GI NA NA negative effect NA
Reversible yes yes 30 yrs in bone yes
Footnotes:1. Hazard Ratio (WHI)2. Hazard Ratio3. RR (Million Woman)
4. OR (ESTHER)5. RR (Million Woman)
6. RR (MORE)
Individualizing TherapyIndividualizing Therapy





























