Embed Size (px)
Citation preview

58Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
© SIMTIPRO Srl
Background - In Italy, the National Register of Congenital Coagulopathies (NRCC) collects epidemiological and therapeutic data from patients affected by haemophilia A (HA), haemophilia B (HB), von Willebrand's disease (vWD) and other rare coagulation disorders. Here we present data from the 2016 annual survey.Materials and methods - Data are provided by the Italian Haemophilia Centres, on a voluntary basis. Information flows from every Centre to a web-based platform of the Italian Association of Haemophilia Centres, shared with the Italian National Institute of Health, in accordance with current privacy laws. Patients are classified by diagnosis, disease severity, age, gender and treatment-related complications.Results - In 2016, the total number of patients with congenital coagulopathies in the NRCC was 10,360: 39.8% of these patients had HA, 31.5% had vWD, 8.5% had HB, and 20.2% had less common factor deficiencies. The overall prevalence of HA and HB was 13.9/100,000 males and 3.0/100,000 males, respectively. The overall prevalence of vWD was 5.4/100,000 inhabitants. During 2016, 126 patients had current alloantibodies to factor VIII (FVIII) or factor IX (FIX) and were under treatment with bypassing agents and/or immune tolerance induction. Overall, 388 patients with a history of alloantibodies were recorded in the NRCC of whom 337 with severe HA and 12 with severe HB. Coagulation factor use, evaluated from treatment plans, was approximately 451,000,000 IU of FVIII for HA patients (7.5 IU/inhabitant), and approximately 53,000,000 IU of FIX for HB patients (0.9 IU/inhabitant).Discussion - The prevalences of HA and HB fall within the ranges reported in more developed countries; the consumption of FVIII and FIX was in line with that of other European countries (France, United Kingdom) and Canada. The NRCC, with its bleeding disorder dataset, is a helpful tool for shaping public health policies, as well as planning clinical and epidemiological research projects.
Keywords: registers, blood coagulation disorders, haemophilia A, haemophilia B, von Willebrand's disease.
New data from the Italian National Register of Congenital Coagulopathies, 2016 Annual SurveyFrancesca Abbonizio1, Hamisa J. Hassan1, Roberta Riccioni1, Elena Santagostino2*, Romano Arcieri3, Adele Giampaolo1, *on behalf of the Italian Association of Haemophilia Centres (see Appendix)
Original article
HAEMOSTASIS AND THROMBOSIS
Arrived: 30 October 2018 Revision accepted: 15 January 2019Correspondence: Adele Giampaolo e-mail: [email protected]
1Department of Oncology and Molecular Medicine, Italian National
Institute of Health, Rome; 2IRCCS Ca' Granda Foundation,
Maggiore Hospital, Milan; 3Grant Of fice and Technology Transfer,
Italian National Institute of Health, Rome, Italy
INTRODUCTIONCongenital bleeding disorders are a group of rare diseases caused by a deficiency of protein cofactors and enzymes implicated in blood coagulation1,2. The most frequent coagulopathies are von Willebrand's disease (vWD), an autosomal inherited bleeding
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

59Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
Italian National Register of Congenital Coagulopathies: 2016
severity of the pathology, complications and therapeutic regimens used. The NRCC represents a helpful tool for shaping health care and planning research projects.The aim of this article is to describe epidemiological, health and therapeutic aspects of Italian patients with congenital bleeding disorders in 2016, comparing data to those of patients from other European countries.
MATERIALS AND METHODS
Data collectionData on congenital bleeding disorders collected in the NRCC are provided by the Italian HTC on a voluntary basis. Information is secured by password, sent in a web-based f low from the HTC databases to AICE and then shared with the Italian National Institute of Health (ISS). The personal data of patients are collected in accordance with current privacy laws and standards and the quality of the information collected is verified through logical and formal controls. Haemophilic patients are classified by disease severity, which depends on the residual activity of coagulation FVIII or FIX1 and patients with vWD are classified by deficiency and/or defects of von Willebrand factor. The national usage of FVIII and FIX was calculated through an analysis of the therapeutic plans prescribed by HTC specialists for each patient for home therapy. The therapeutic plans, mandatory by law, indicate the diagnosis of the bleeding disorder, its severity, treatment regimen, treatment dosage, brand name of the product used, and the total number of International Units (IU) assigned. The reported data on consumption of coagulation factors are limited by the voluntary adhesion of each HTC to provide the therapeutic plans to the register database. We calculated the consumption for the haemophilic population for whom therapeutic plans were available. We compared the age of the patients (paediatric group: ≤18 years and adult group: >18 years) with and without therapeutic plans, by Fisher's test.Factors and bypassing agents administered to inpatients were not included in the study because the information is not available in the therapeutic plans.
RESULTS
Epidemiology 2016Epidemiological data were provided by 52/54 of the Italian HTC (coverage: 96.3%). A total number of 10,360 patients
disorder, caused by a deficiency or abnormality of von Willebrand factor, haemophilia A (HA) and haemophilia B (HB), both X-linked inherited disorders caused by deficiency of factor VIII (FVIII) and factor IX (FIX), respectively. The typical symptoms of haemophilia consist mainly of disabling and painful joint haemorrhages as well as bleeding in internal organs. Deficiencies of factor I (fibrinogen), factor II (prothrombin), factor V, factor VII (FVII), factor X, factor XI (FXI) and factor XIII are rarer and the bleeding episodes can range from muscle haematomas to major bleeds. Current therapy consists of replacing the deficient clotting factor through the intravenous administration of the specific factor concentrate, which can be derived from plasma or produced using recombinant technology; when the specific products are not available, human plasma or multi-factor concentrates can be used3.The main complication of replacement therapy in patients with haemophilia is the development of alloantibodies to FVIII or FIX1,2. These alloantibodies compromise the efficacy of therapy, increasing the risk of serious bleeding and disability, with important impacts on the quality of life of patients and health care costs4. Patients with a high inhibitor titre (>5 Bethesda Units/mL) are treated with bypassing agents (plasma-derived activated prothrombin-complex and recombinant activated FVII).People with congenital bleeding disorders need global and multidisciplinary care that, in Italy, is provided by Haemophilia Treatment Centres (HTC), which are part of the Italian Association of Haemophilia Centres (AICE), and form a network of care centres throughout the country. The importance of continuous epidemiological and pharmacovigilance monitoring, relative to patients affected by inherited bleeding disorders, has been confirmed by the World Federation of Hemophilia (WFH), which has long suggested the institution of specific registers dedicated to coagulation disorders, estimating that about 400,000 people have bleeding diseases worldwide5.In Italy, a National Register of Congenital Coagulopathies (NRCC) has been active, since 2005, on a voluntary basis. The aim of the NRCC is to collect epidemiological data on the prevalence of the different bleeding disorders, on the complications of their therapies and on the amount of drugs required to treat the patients, according to the
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

60
Abbonizio F et al
Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
with congenital coagulopathies were included in the NRCC (Table I). HA patients represented 39.8% of the total number of patients recorded in 2016. Patients with severe, moderate and mild HA accounted for 44.8%, 14.0% and 41.2%, respectively, of the overall number of patients with HA. Individuals with HB represented 8.5% of the total number of patients recorded, with 35.5% of these HB patients having a severe form of the disease, 21.0% a moderate form and 43.5% a mild form. Patients with vWD accounted for 31.5%: 3.7% of the patients had type 3 (the most severe form), 21.1% had type 2 and 75.2% had type 1. Female patients represented 57.8% of all the vWD patients recorded in the Register.Based on data relative to the Italian population, evaluated by the National Institute of Statistics, in 2016 the prevalence of HA was 13.9/100,000 males (95% confidence interval [CI]: 13.4-14.3) and that of HB was 3.0/100,000 males (95% CI: 2.8-3.2). The prevalence of vWD was 5.4/100,000 inhabitants (95% CI: 5.2-5.6). In Figure 1, the prevalences of HA and HB in Italy, distributed by severity, and the overall prevalence of vWD are compared with those of Canada, France and the United Kingdom (UK) - estimated on the basis of the 2016 Report of the WFH Annual Global Survey5.Details on age distribution of prevalence of the two forms of haemophilia and of vWD, distinguished by clinical group, are given in Figure 2. The other rare inherited bleeding disorders reported in the Register are deficiencies of factors I, II, V, VII, X, XI, XII, XIII and combined V+VIII (Table I). Patients with these disorders represented 20.2% of the total number of patients recorded in 2016. FVII was the most frequent factor deficiency, with about 900 recorded cases and a prevalence in the Italian population of 1.5/100,000 inhabitants. No differences in prevalences between females and males were observed for any of these disorders.Other individuals reported in the NRCC are carriers of HA (n=545) and HB (n=171).
InfectionsHuman immunodeficiency virus infectionIn the 2016 survey, 235 of the haemophilic patients recorded were infected with human immunodeficiency virus (HIV): most of them (n=207) were co-infected with hepatitis C virus (HCV) (Figure 3A). The haemophilic patients infected
with HIV represented 93.3% of all the HIV-infected patients recorded in the Register (n=252). Patients with severe HA and severe HB accounted for 68.1 and 17.0%, respectively, of the HIV-infected haemophilic population. Most of the patients were in the 41- to 60-year-old group. The prevalence of HIV in HA patients according to disease severity was 8.7% for severe HA, 2.2% for moderate HA and 0.5% for mild HA. In HB patients, the prevalence was 12.7%, 5.4% and 0.8% for severe, moderate and mild HB, respectively.The other individuals infected with HIV comprised ten with vWD, three with FVII deficiency, one HA carrier and one HB carrier. Four of the ten patients with vWD infected with HIV had HCV co-infection.Hepatitis C virus infectionIn 2016, a total of 1,382 haemophilic patients were infected with HCV: 1,175 with HCV alone and 207 co-
Table I - Total patients registered in the National Register of Congenital Coagulopathies - 2016
Patients PercentageHaemophilia A (HA)
Severe HA 1,846Moderate HA 578Mild HA 1,696Overall HA 4,120 39.8%
Haemophilia B (HB)Severe HB 314Moderate HB 186Mild HB 385Overall HB 885 8.5%
von Willebrand's disease (vWD)vWD type 3 120vWD type 2 687vWD type 1 2,455Overall vWD 3,262 31.5%
Other factor deficienciesFactor I 169Factor II 24Factor V 168Factor VII 894Factor X 113Factor XI 495Factor XII 132Factor XIII 58Factor V+VIII 37Fletcher factor 3Overall 2,093 20.2%
Total patients 10,360
HA and HB carriers 716
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

61Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
Italian National Register of Congenital Coagulopathies: 2016
infected with HIV (Figure 3A). These patients infected with HCV represented 87.9% of the total HCV-infected patients recorded in the Register (n=1,573).Patients with severe HA and severe HB accounted for 52.2% and 7.1%, respectively, of the HCV-infected haemophilic
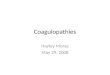
Figure 1 - Prevalences of haemophilia A and B/100,000 males, by severity, and overall prevalence of von Willebrand's disease/100,000 inhabitants in comparison with those of other countries.HA: haemophilia A; HB: haemophilia B; vWD: von Willebrand's disease.
Overall HA Severe HA Moderate HA Mild HA Overall HB Severe HB Moderate HB Mild HB
Overall vWD
Italian HA prevalence(N/100,000 males) by severity: comparison with other countries
20.418.7
17.6
13.9
5.95.95.16.3
2.72.61.62.0
11.810.2
11.0
5.7
UKFranceCanadaItaly
Italian HB prevalence(N/100,000 males) by severity: comparison with other countries
UKFranceCanadaItaly
4.64.3
3.9
3.0
1.1 1.11.0 1.20.6
1.2 1.2 1.1 1.3
2.4
1.72.0
UKFranceCanadaItaly
Italian vWD prevalence (N/100,000 inhabitants): comparison with other countries
16.3
3.2
12.2
5.4
2.8
3.6
1.5
1.00.7 0.6
1.41.2
3.6
5.8
0.1 0.20.8
1.2
2.7
4.3
5.95.94.3
1.92.2
7.7
14.313.8
Overall HB Severe HB Moderate HB Mild HBOverall HA Severe HA Moderate HA Mild HA Overall vWD Type 3 Type 2 Type 1
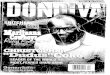
vWD prevalence (N/100,000 inhabitants) by age group
HB prevalence (N/100,000 males) by age groupHA prevalence (N/100,000 males) by age group
Paedriatric (≤18) Adult (>18)Paedriatric (≤18) Adult (>18)
Paedriatric (≤18) Adult (>18)
Figure 2 - Prevalences of haemophilia A and B/100,000 males and prevalence of von Willebrand's disease/100,000 inhabitants, by age group (paediatric and adults) and severity.HA: haemophilia A; HB: haemophilia B; vWD: von Willebrand's disease.
population. There were five HCV-positive haemophilic patients aged ≤18 years; these are foreign patients who were treated with plasma products in their countries of origin before starting replacement therapy at Italian HTC.The prevalence of HCV in HA patients, divided according
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

62
Abbonizio F et al
Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
to disease severity, was 39.1% in those with severe HA, 31.3% in those with moderate HA and 17.7% in those with mild HA. The corresponding prevalence in HB patients, again divided by disease severity, was 31.2%, 23.7% and 9.6%, respectively.Among the vWD patients recorded in the register in 2016, 115 were infected with HIV and/or HCV: six were infected with HIV, 105 with HCV and four with both infections (HIV+HCV).Another 57 patients with other factor deficiencies were infected with HCV: most of them with FVII deficiency (38.6%) and FXI deficiency (28.1%) (Figure 3B). Furthermore, 11 HA and two HB carriers were recorded with HCV infection.
Inhibitor developmentPatients with haemophilia who developed antibodies were recorded in the Register. During 2016, 126 patients had current inhibitors to FVIII and FIX and were under treatment with bypassing agents and/or immune tolerance induction (ITI). The diagnoses and age distribution of these patients are given in Table II: 42.9% were patients ≤18 years old and most of them (n=30) were children ≤10 years old.
Figure 3 - Patients positive for human immunodeficiency virus and hepatitis C virus in the National Register of Congenital Coagulopathies. (A) Italian haemophilic population, by age groups and disease severity. (B) Patients with other factor deficiencies. HA: haemophilia A; HB: haemophilia B; HIV: human immunodeficinecy virus; HIV: uman immunodeficiency virus; HCV: hepatitis C virus.
Overall, 388 patients with a history of alloantibodies to FVIII or FIX were recorded in the NRCC: 337 with severe HA and 12 with severe HB.
Home treatment The Register collected data on replacement therapy in patients with HA, HB and vWD. The evaluation of therapeutic regimen was based on an analysis of the therapeutic plans prescribed by clinicians for patients for home therapy. Therapeutic plans were provided to the Register database by the HTC for 71.3%
Table II - Patients with current inhibitors to factor VIII and factor IX during 2016
HA Severe HB
Total
Severe HA
Moderate HA
MildHA
Patients 114 3 3 6 126
≤18 years 47 1 2 4 54
19-40 years 19 1 1 2 23
41-60 years 37 - - - 37
>60 years 11 1 - - 12
HA: haemophilia A; HB: haemophilia B.
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

63Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
Italian National Register of Congenital Coagulopathies: 2016
of patients with severe HA, 60.5% of patients with severe HB and 36.7% of patients with vWD type 3. We compared the ages (paediatric and adult populations) of the patients with available therapeutic plans with those of the patients for whom therapeutic plans were not available, divided according to whether they had severe HA, severe HB or vWD type 3. Only for patients with severe HA there was a higher percentage of adults (>18 years old) in the group with missing therapeutic plans than in the group for whom therapeutic plans were available (p<0.01).Prophylaxis was the therapeutic regimen adopted in 85.9% of patients with severe HA, in 77.7% of patients with severe HB and in 47.7% of patients with vWD type 3.Details on age distribution of the therapeutic regimens adopted are given in Table III. Prophylaxis was the most widely used treatment regimen for patients with severe HA or HB, especially in the younger age groups except in the 0- to 3-year old age group in which the percentages of prophylactic and on-demand regimens were similar. In vWD type 3 patients, prophylaxis was the regimen of choice in the 4- to 18-year old age group.
On-demand therapy was the treatment of choice for moderate and mild HA and HB and vWD type 1 and 2 (data not shown). Among the 114 patients with severe HA with current inhibitors, ITI was used in 44 (38.6%) of whom 18 patients were also receiving bypassing agents. Of note, 40.9% of all patients on ITI were children ≤10 years old.In 2016, the amount of FVIII prescribed, obtained from the therapeutic plans provided to the Register, was ~451,000,000 IU (7.5 IU/per inhabitant), 80.0% of which was in the recombinant form. Analysed according to recipients' disease type and severity, 86.3% of the FVIII units were prescribed to patients with severe HA, 7.1% to patients with moderate HA, 3.0% to patients with mild HA, and the remaining 3.6% to patients with vWD. About 56,000,000 IU were used for ITI.The amount of FIX prescribed, again obtained from the therapeutic plans provided to the Register, was ~53,000,000 IU (0.9 IU/per inhabitant); most was in the form of recombinant products (80.3%). For patients with inhibitors treated with bypassing agents at home, the reported consumption of plasma-derived activated prothrombin-complex and recombinant activated FVII was ~13,000,000 IU and ~31,000 mg, respectively.
DISCUSSIONThe purpose of registers of nationally significant diseases is to ensure monitoring and benchmarking of quality of care and health outcomes. The importance of registers is underlined well in Italian Law 221/2012, in which they are defined as "an active system of systematic collection of personal, health and epidemiological data of a particular disease [...] established for the purposes of prevention, diagnosis, treatment and rehabilitation, health planning, verification of the quality of care, evaluation of health care and scientific research in the medical, biomedical and epidemiological fields, in order to ensure an active system of systematic collection of personal, health and epidemiological data to record and characterise all cases of risk for health, a particular disease or a relevant health condition in a defined population"6. In the field of haemophilia, monitoring patients by means of the establishment of a national disease register was clearly recommended by the WFH7. One of the first
Table III - Percentage of therapeutic regimens used for patients with severe haemophilia A, severe haemophilia B and von Willebrand's
disease - type 3, by age groups, during 2016
Age group Prophylaxis On demand
Severe HA
0-3 56.4% 43.6%
4-18 98.9% 1.1%
19-40 92.9% 7.1%
41-60 76.7% 23.3%
>60 63.6% 36.4%
Severe HB
0-3 57.1% 42.9%
4-18 89.6% 10.4%
19-40 78.5% 21.5%
41-60 59.5% 40.5%
>60 71.4% 28.6%
vWD - type 3
0-3 50.0% 50.0%
4-18 75.0% 25.0%
19-40 47.1% 52.9%
41-60 41.7% 58.3%
>60 44.4% 55.6%
HA: haemophilia A; HB: haemophilia B; vWD: von Willebrand's disease.
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

64
Abbonizio F et al
Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
haemophilia registers was set up in the UK in 1968, with the aim of determining how many patients with haemophilia there were in the UK and how much treatment they needed. Nowadays, the national haemophilia database collects and records larger amounts and more sophisticated types of data concerning epidemiological and clinical care, surveillance and safety, quality of care, and pharmacovigilance8.In Italy, surveillance of patients with bleeding disorders has been managed by the ISS in collaboration with AICE since 1988, with the purpose of surveying viral infections in the haemophilic population. Over the years, the aim of the Italian register has changed and the current NRCC supplies epidemiological data on the prevalence of the different congenital bleeding disorders, on therapy complications, and on drug requirements for haemophilia therapy. All HTC contribute on a voluntary basis to the NRCC, sending local epidemiological data, and details on disease severity and treatment regimens to the AICE database, shared with the ISS. Data are published on the website of the ISS (http://old.iss.it/binary/publ/cont/17_44_web.pdf) and through scientific publications9,10.In 2016, 10,360 patients with congenital coagulopathies were included in the NRCC. The percentage distribution of the different coagulopathies in Italy is in line with that determined by a survey conducted in the same year by the WFH in 113 countries, with a world population coverage of 90%. The 2016 WFH report described a total of about 296,000 people with coagulation disorders, of whom about 50.1% with HA, 10.0% with HB, 24.2% with vWD and 13.3% with other factor deficiencies. In Italy, of the total 10,360 patients registered, 39.8% are affected by HA (almost half with severe HA), 8.5% by HB, 31.5% by vWD and 20.2% by other coagulation factors deficiencies. The prevalence of HA (all degrees of severity) in Italy in 2016 was 13.9/100,000 males, compared to 17.6, 18.7 and 20.4 in Canada, France and the UK, respectively, while that of HB was 3.0 in Italy vs 3.9, 4.3 and 4.6, respectively. A more detailed comparison of the prevalences of HA and HB in Italy and other countries, by different degrees of disease severity, indicates that the lowest overall prevalence registered in NRCC was due mostly to an underreporting of patients with mild haemophilia. Nevertheless, the overall prevalences of HA and HB in
Italy fall within the ranges reported in more developed countries (HA=12.8±6.0 and HB=2.7±1.6)11,12.Based on the prevalence of bleeding disorders in Italy in different age groups, we can hypothesise an underestimation of the prevalence of mild HA in the paediatric population. Indeed, patients with mild haemophilia - who are usually "not bleeding patients" - may be recognised later in life, for example during surgery or dental procedures, or may be in the care of other doctors rather than HTC physicians and so not notified to the register.However, the overall prevalence of HA and HB in the paediatric population is slightly higher than that in the adult population, unlike the prevalence of vWD which is higher in the adult population because, as for mild HA, vWD is often recognised in adulthood. The increase in the life expectancy of patients with bleeding disorders, which has now become comparable to that of the general population13, is primarily the result of advances in factor replacement therapy and improvements of comprehensive health care provided by specialised haemophilia centres. Risk factors for viral infection are now similar to those to which the general population is exposed. However, there are 1,382 HCV-positive haemophilic patients registered in the NRCC, 207 of whom are also HIV-positive. The five HCV-positive subjects ≤18 years old are foreign patients treated with plasma products in their countries of origin before starting their replacement therapy in Italian HTC. The current major complication of haemophilia treatment is the development of inhibitory antibodies against FVIII or FIX. In 2016, 126 patients underwent inhibitor therapy (ITI and/or bypassing agents), of which about one quarter were children ≤10 years of age, as a consequence of the early appearance of this adverse event. The presence of high-titre responding inhibitors makes treatment with conventional replacement therapy ineffective, resulting in poorer control of haemorrhagic episodes and the need to use either bypassing therapies or, in order to eradicate the inhibitor, ITI which is successful in 60-80% of patients with HA14. The development of an inhibitor compromises the condition of a part of patients with haemophilia, but has a significant impact on treatment and management costs and patients' quality of life4.In general, although the coverage of treatment plans
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

65Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
Italian National Register of Congenital Coagulopathies: 2016
relating to severe HA (71.3%), severe HB (60.5%) and vWD type 3 (36.7%) increased in 2016, compared with that of previous years, it needs to be further improved. Indeed, comparing the ages of the group with and without therapeutic plans, no differences were found for severe HB and vWD type 3, whereas for severe HA there was a higher percentage of adults (>18 years old) in the group without therapeutic plans. This bias could inf luence the results on therapy (prophylaxis vs on-demand) of patients with severe HA. Prophylaxis was the therapeutic regimen adopted in 85.9% of patients with severe HA, in 77.7% with severe HB and in 47.7% with vWD type 3. The amount of FVIII used in 2016, evaluated from the treatment plans, was approximately 451,000,000 IU, corresponding to 7.5 IU/inhabitant, and was mainly in the form of recombinant products. The Italian National Blood Centre, through a comparative analysis of other Italian data sources15, estimated a total FVIII consumption in 2015 of 529,000,000 IU. The discrepancy with our findings is due to the incomplete data reporting in the Register by HTC because of the voluntary basis of the data collection and the lack of data on usage of coagulation factors during hospitalisation. The value of 7.5 IU/inhabitant is in line with values reported by other European countries (France 7.3 IU/inhabitant, UK 8.7 IU/inhabitant) and Canada (8.0 IU/inhabitant)5. The amount of FIX prescribed in therapeutic plans was about 53,000,000 IU, corresponding to 0.9 IU/inhabitant, in line with the amounts in France (1.2 IU/inhabitant), the UK (1.4 IU/inhabitant) and Canada (1.5 IU/inhabitant)5. The amount of FIX evaluated by the National Blood Centre was 60,000,000 IU15.The current profile of consumption and products used by the haemophilia population could undergo substantial changes as a result of the introduction of new concentrates, with long half-lives, which allow the intervals between infusions to be extended. Other treatments are currently being tested and/or studied: novel therapeutics have been developed with alternative modes of delivery, overcoming the limitations of current replacement therapy16.On May 12, 2017, the publication of the Decree of March 3, 2017 "Identification of surveillance systems and registers of mortality, cancer and other diseases", officially established a new "National Register of Congenital Coagulopathies" at the ISS17, which will be based on a data
f low from all Italian Regions. This f low will start when the law is implemented at a regional level.
CONCLUSIONThe availability of a national register on blood coagulation disorders improves the knowledge of the epidemiology, correlated diseases, and health care requirements of these disorders. However, the NRCC does have an important limitation due to the voluntary contribution of each HTC and the missing data on usage of coagulation factors during hospitalisation. The establishment of the NRCC by the Italian Decree of March 3, 2017, based on a mandatory data f low from all Italian Regions, will improve the monitoring of patients with coagulation disorders in the near future and will provide more reliable information to support decision-makers in adopting the most appropriate health policies.
ACKNOWLEDGEMENTS We are grateful to Giampiero Macioce and Gabriella Pietrangeli for data entry and participation in the maintenance of the NRCC.
AUTHORS' CONTRIBUTIONSFA and RR analysed and interpreted the data and prepared the draft manuscript. ES and RA edited and reviewed the manuscript. AG and HJH conceived the study design and critically revised the paper. All the authors read and approved the final version of the manuscript.
The Authors declare no conf licts of interest.
REFERENCES1. Mannucci PM, Tuddenham EG. The hemophilias - from royal genes to
gene therapy. N Engl J Med 2001; 344: 1773-9.
2. Hassan S, Cannavò A, Gouw SC, et al. Factor VIII products and inhibitor development in previously treated patients with severe or moderately severe haemophilia A: a systematic review. J Thromb Haemost 2018; 16: 1055-68.
3. Rocino A, Coppola A, Franchini M, et al. Working Party. Principles of treatment and update of recommendations for the management of haemophilia and congenital bleeding disorders in Italy. Blood Transfus 2014; 12: 575-98.
4. D’Angiolella LS, Cortesi PA, Rocino A, et al. The socioeconomic burden of patients affected by haemophilia with inhibitors. Eur J Haematol 2018; 101: 435-56.
5. World Federation of Hemophilia. Report on The Annual Global Survey 2016. Available at: http://www1.wfh.org/publications/files/pdf-1690.pdf. Accessed on 11/09/2018.
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission

66
Abbonizio F et al
Blood Transfus 2020; 18: 58-66 DOI 10.2450/2019.0211-18
APPENDIX
In alphabetical order, the Haemophilia Treatment Centres that participated in the survey and, in brackets, their directors and any other investigators directly involved:
Alessandria (Laura Contino), Arezzo (Arianna Accorsi, Alessandra Caremani), Bari (Pietro C. Ettorre, Paola Giordano, Giuseppe Lassandro), Bologna (Lelia Valdrè), Brescia (Lucia Notarangelo), Cagliari (Anna B. Aru), Castelfranco Veneto (Paolo Radossi, Giuseppe Tagariello), Catania (Dorina Cultrera), Catanzaro (Piergiorgio Iannaccaro, Rita Santoro), Cesena (Chiara Biasoli), Chieti (Patrizia Di Gregorio), Cosenza (Filomena Daniele), Cremona (Sophie Testa), Ferrara (Maria L. Serino), Florence (Giancarlo Castaman, Silvia Linari), Florence AICE (Massimo Morfini), Genoa (Angelo C. Molinari), Ivrea (Grazia Delios), Macerata (Isabella Cantori), Mantua (Massimo Franchini), Milan - Niguarda (Maria T. Caimi), Milan - Policlinico (M. Elisa Mancuso, Flora Peyvandi, Elena Santagostino), Modena (Marco Marietta), Monopoli (Angela Todisco, Vincenzo Speciale), Naples - Federico II (Anna M. Cerbone, Giovanni Di Minno), Naples - Pausilipon (Michele Schiavulli), Naples - S. Giovanni Bosco (Angiola Rocino, Maria M. Spiezia), Padua (Ezio Zanon), Palermo (Fabio Gagliano, Maria F. Mansueto, Sergio Siragusa), Parma (Antonio Coppola, Gabriele Quintavalle, Gianna F. Rivolta, Annarita Tagliaferri), Pavia (Chiara Ambaglio, Gabriella Gamba), Perugia (Emanuela Marchesini, Emily Oliovecchio), Pescara (Alfredo Dragani), Piacenza (Maria C. Arbasi), Ravenna (Silvia Macchi, Daniele Vincenzi), Reggio Calabria (Gianluca Sottilotta), Reggio Emilia (Attilia M. Pizzini), Rome - Bambino Gesù (Matteo Luciani), Rome - Gemelli (Raimondo De Cristofaro), Rome - La Sapienza (Erminia Baldacci, Maria G. Mazzucconi, Cristina Santoro), Sassari (Lucia A. Mameli), Scorrano (Antonella Coluccia), Termoli (Pasquale Marino), Turin - Le Molinette (Alessandra Borchiellini, Pier Carla Schinco), Turin - Children's Hospital (Maria Messina, Berardino Pollio, Irene Ricca), Trento (Paola Agostini, Attilio F. Cristallo), Udine (Giovanni Barillari, Vincenzo De Angelis, M. Elena Mosanghini), Vallo della Lucania (Giulio Feola), Verona - Polyclinic (Elisa Bonetti, Simone Cesaro), Verona - University (Giorgio Gandini, Annachiara Giuffrida), Vicenza (Alberto Tosetto).
6. Italian Law n. 221 of December 17, 2012. [Conversion into law, with amendments, of Legislative Decree n. 179 of October 18, 2012, containing further urgent measures for the growth of the country]. Italian Official Gazette - General Series n. 294, December 18, 2012 (Ordinary Supplement 208). [In Italian.]
7. Evatt BL. World Federation of Hemophilia guide to developing a national patient registry. World Federation of Hemophilia. Available at www1.wfh.org/publication/files/pdf-1288.pdf. Accessed on 18/06/2018.
8. Dolan G, Makris M, Bolton-Maggs PH, et al. Enhancing haemophilia care through registries. Haemophilia 2014; 20: 121-9.
9. Abbonizio F, Giampaolo A, Coppola A, et al. Therapeutic management and costs of severe haemophilia A patients with inhibitors in Italy. Haemophilia 2014; 20: 243-50.
10. Giampaolo A, Abbonizio F, Arcieri R, et al. Italian Registry of Congenital Bleeding Disorders. J Clin Med 2017; 6: 1-8.
11. Stonebraker JS, Bolton-Maggs PH, Soucie JM, et al. A study of variations in the reported haemophilia A prevalence around the world. Haemophilia 2010, 16: 20-32.
12. Stonebraker JS, Bolton-Maggs PH, Soucie JM, et al. A study of variations in the reported haemophilia B prevalence around the world. Haemophilia 2012; 18: e91-4.
13. Tagliaferri A, Rivolta GF, Iorio A, et al. Mortality and causes of death in Italian persons with haemophilia, 1990-2007. Haemophilia 2010; 16: 437-46.
14. Coppola A, Di Minno MN, Santagostino E. Optimizing management of immune tolerance induction in patients with severe haemophilia A and inhibitors: towards evidence-based approaches. Br J Haematol 2010; 150: 515-28.
15. Candura F, Calizzani G, Profili C, et al. [Demand for the main blood medicinal products in Italy. 2015]. Rapporti ISTISAN 17/20. [In Italian.]
16. Callaghan MU, Sidonio R and Pipe SW. Novel therapeutics for haemophilia and other bleeding disorders. Blood 2018; 132: 23-30.
17. Italian Decree of the President of the Council of Ministers March 3, 2017. [Identification of surveillance systems and registers of mortality, cancers and other diseases]. Italian Official Gazette - General Series n. 109, May 12, 2017. [In Italian.]
© SIMTIPRO Srl
All rights reserved - For personal use only No other use without premission