Embed Size (px)
Citation preview

New Clinical Studies in Diabetic Kidney Disease
Sang Youb Han, MD, PhD
Division of Nephrology,
Inje University Ilsan-Paik Hospital

Contents
• Recent clinical data
• New therapeutic targets
• Remaining issues
Recent Clinical Data
• New issues: Normoalbuminuric DKD, eGFR • Target blood glucose level • Optimal BP • Nocturnal BP • Normoalbuminura to microalbuminuira • Remission of microalbuminuira • Optimal dose of RAS blockade • ACE inhibitor vs. ARB • Combination of ACE inhibitor and ARB • ARB + renin inhibitor • MR blockade

Recent Clinical Data
• Normoalbuminuric DKD • Target blood glucose level • Optimal BP • Nocturnal BP • Normoalbuminura to microalbuminuira • Remission of microalbuminuira • Optimal dose of RAS blockade • ACE inhibitor vs. ARB • Combination of ACE inhibitor and ARB • ARB + renin inhibitor • MR blockade

Normo Micro
• BENEDICT (N Engl J Med 2004)
: T2D, HTN, >3 yrs
: trandolapril (6.0%) vs. verapamil (11.9%) vs. combination(5.7%) vs. placebo(10%)
• ROADMAP (N Engl J Med 2011)
: T2DM, HTN, 3.2yrs
: olmesartan(8.2%) vs. control (9.8%)
: fatal cardiovascular events (0.7% vs. 0.1%, P=0.01)
• T1DM, normotensive for 5 yrs (Mauer, N Engl J Med 2009)
: renal biopsy & albuminuria
: losartan or enelapril - not effective
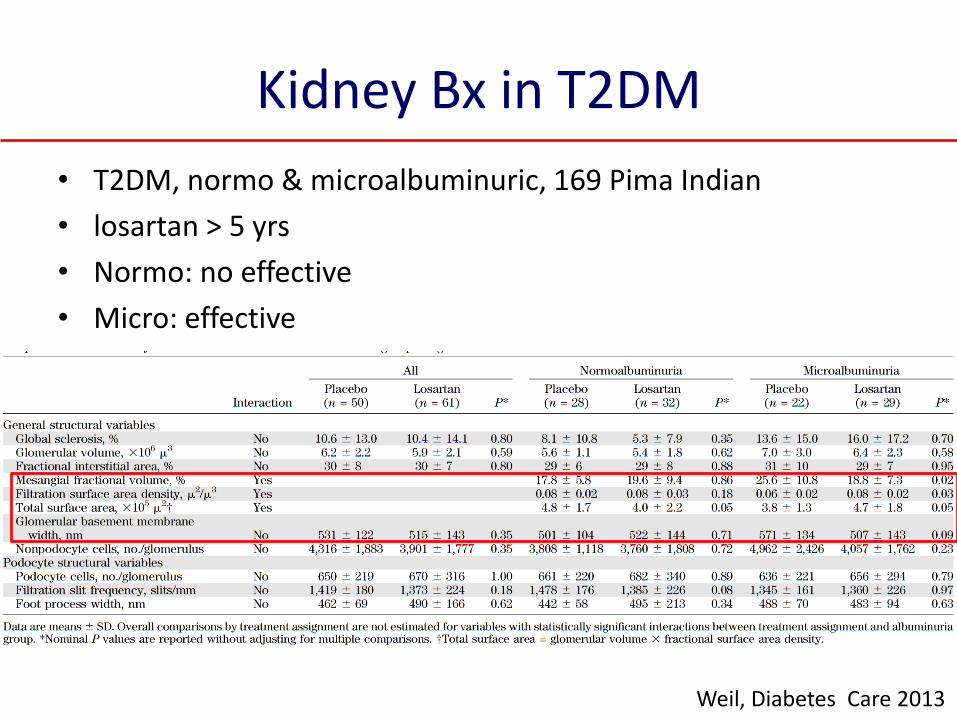
Kidney Bx in T2DM
• T2DM, normo & microalbuminuric, 169 Pima Indian
• losartan > 5 yrs
• Normo: no effective
• Micro: effective
Weil, Diabetes Care 2013

Combination of ACE Inhibitor and ARB
• CALM II: candesartan + lisinopril Andersen, Diabetes Care 2005
• ONTARGET: telmisartan + ramipril
• Lisinopril + irbesartan
• VA-NEPHRON: losartan + lisinopril – early termination
• Ongoing study: VALID: benazapril + valsartan
Mann, Lancet, 2008
Juarez, Am J Kidney Dis 2013
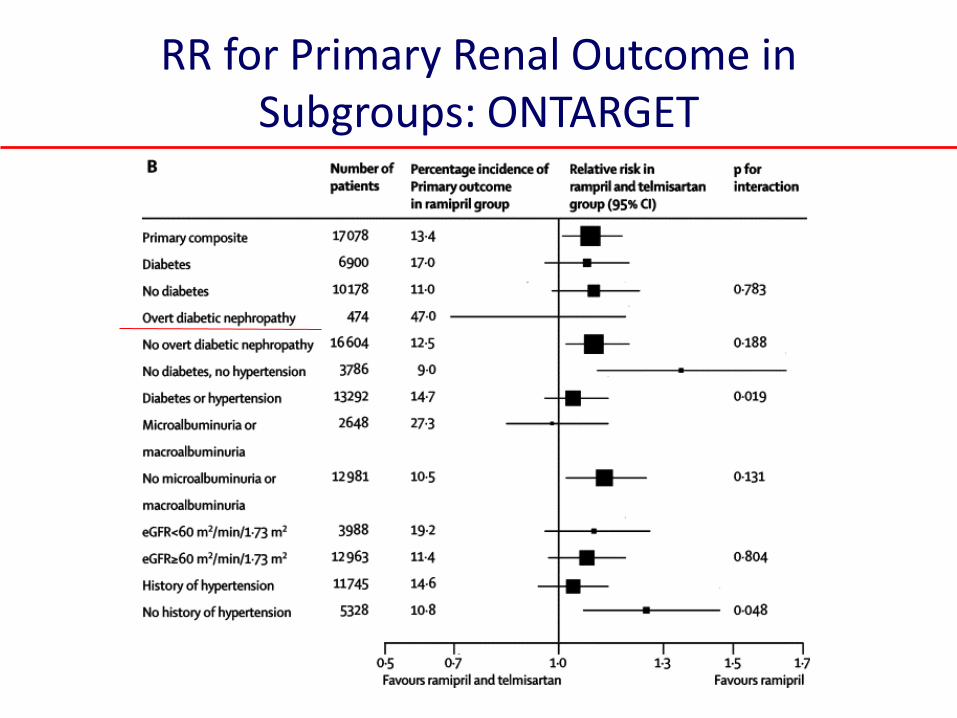
RR for Primary Renal Outcome in Subgroups: ONTARGET

• 132 T2 DKD, CKD 2-3
• UPCR>300mg/gCr
• Lisinopril vs. irbesartan
• equipotent half dose
• eGFR: 49±21
• PCR: 1.32
• F/U 3.2 yrs
• No benefit
• Similar adverse effects
Juarez, Am J Kidney Dis 2013
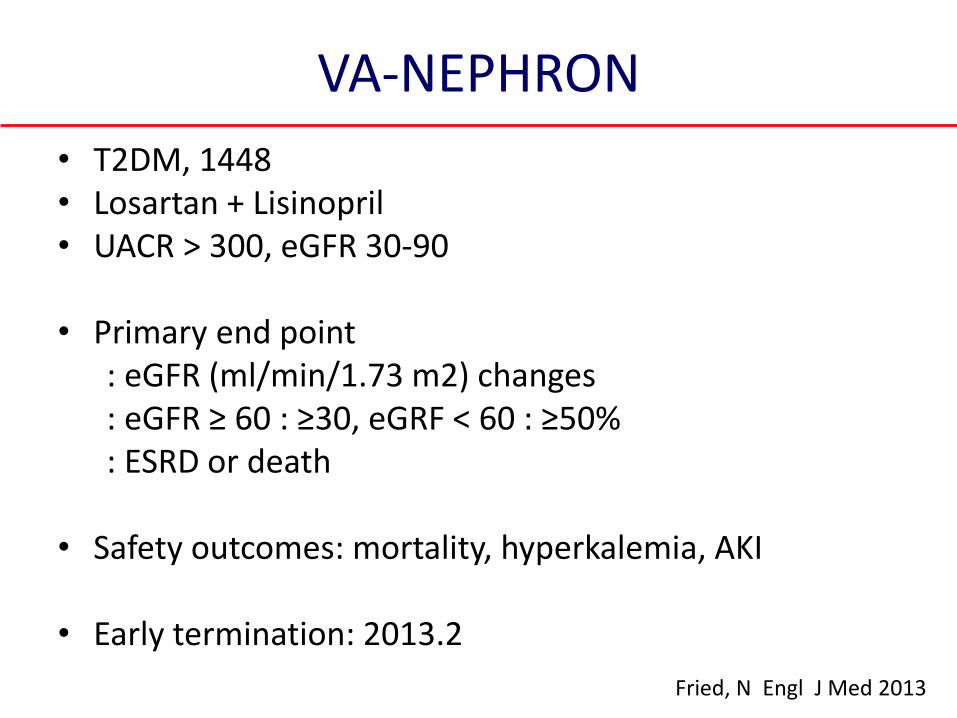
VA-NEPHRON
• T2DM, 1448 • Losartan + Lisinopril • UACR > 300, eGFR 30-90
• Primary end point : eGFR (ml/min/1.73 m2) changes : eGFR ≥ 60 : ≥30, eGRF < 60 : ≥50% : ESRD or death
• Safety outcomes: mortality, hyperkalemia, AKI
• Early termination: 2013.2
Fried, N Engl J Med 2013


Direct Renin inhibitor: Aliskiren
• Aliskiren (Persson, Kidney Int 2008)
: reduction of BP and albuminuria
• Aliskiren + ARB
1) AVOID, Parving, N Engl J Med 2008
2) Persson, Diabetes Care 2009
3) Persson, Clin J Am Soc Nephrol 2011
4) ALTITUDE: early termination
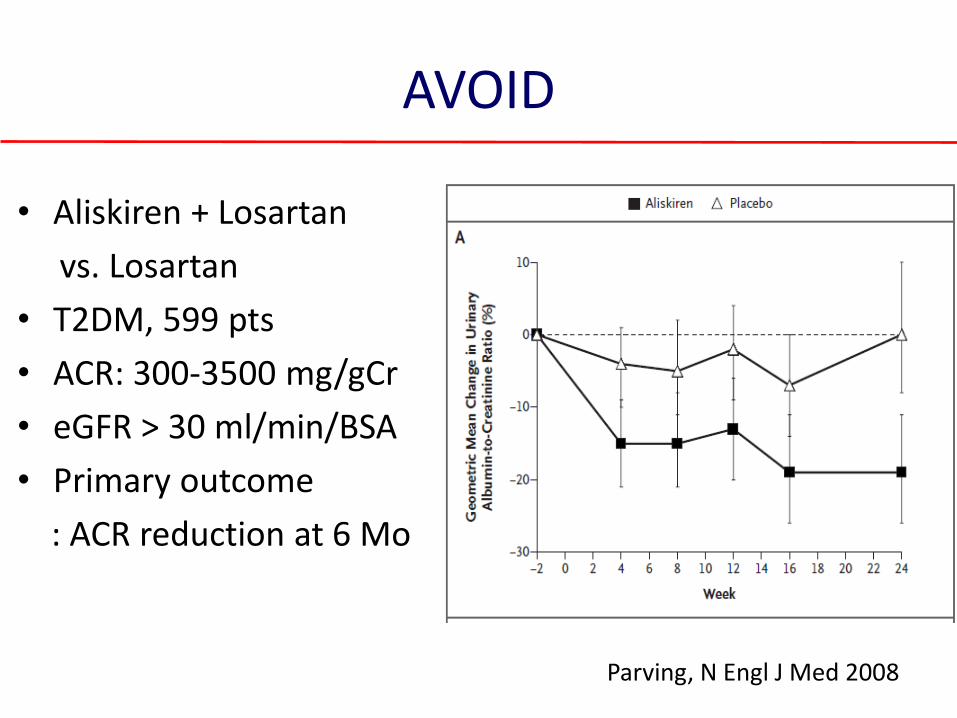
AVOID
• Aliskiren + Losartan
vs. Losartan
• T2DM, 599 pts
• ACR: 300-3500 mg/gCr
• eGFR > 30 ml/min/BSA
• Primary outcome
: ACR reduction at 6 Mo
Parving, N Engl J Med 2008
ALTITUDE (Aliskiren Trial in Type 2 Diabetes Using Cardio-
Renal Endpoints )
• Double-blind study, 8561 T2DM with RAAS blockade
• Aliskiren 300 mg once daily vs. or placebo
• Doubling of s-Cr or ESRD: similar
• 14% reduction in albuminuria
• Early termination d/t safety issue
: hyperK ≥6 mmol/L (8.8% vs. 5.6%)
: reported hypotension (12.1% vs. 8.0%)
: ischemic stroke
Parving, N Engl J Med 2012
MR blockade
• SPR vs. placebo(Schjoedt, Kidney Int 2005) : DM 1, RAS blockade : 30% (CI, 17-41) reduction in albuminuria
• SPR vs. placebo(Schjoedt, Diabetes Care 2005)
: DM 2, RAS blockade : 33%(CI, 25-41) reduction in albuminuria
• SPR vs. losartan(Mehdi, J Am Soc Nephrol 2009)
: 81 DM 2, lisinopril : reduction of ACR: SPR(34.0%) vs. losartan(16.8%) : hyperK
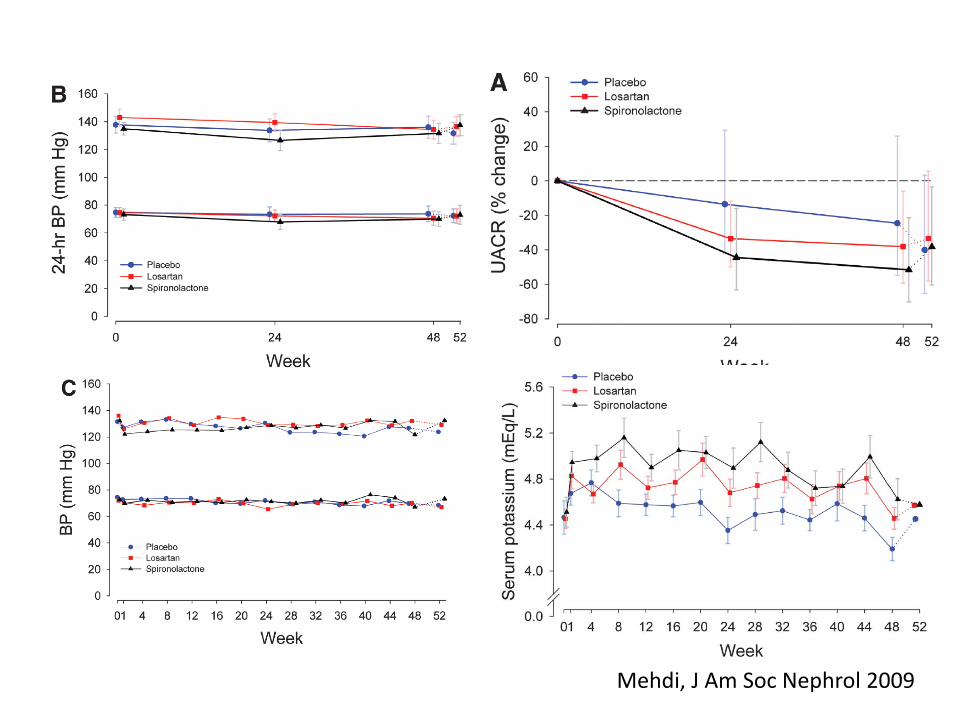
Mehdi, J Am Soc Nephrol 2009

New Therapeutic Targets
• Rho kinase inhibition • AGE inhibitor: thiamine, pyridoxamine • Inhibitor of fibrosis: TGF-β, CTGF, PDGF-pirfenidione, tranilast • PKC inhibitor: ruboxistaurin • JAK 1/2 inhibitor: CKD 3-4, macroalubminuria • Anti-oxidant, anti-inflammatory drugs: pentoxifyllin • Nitric oxide: NADPH oxidase inhibitor • Glycosaminoglycan: sulodoxide • Endothelin antagonist: atrasentan, avosentan • PPAR-α, γ • Vitamin D analgue

Alicic, Am J Kidney Dis 2014

Prevalence of vit D deficiency & 2’ hyperparathyroidism by GFR intervals
Levin, Kidney Int 2007
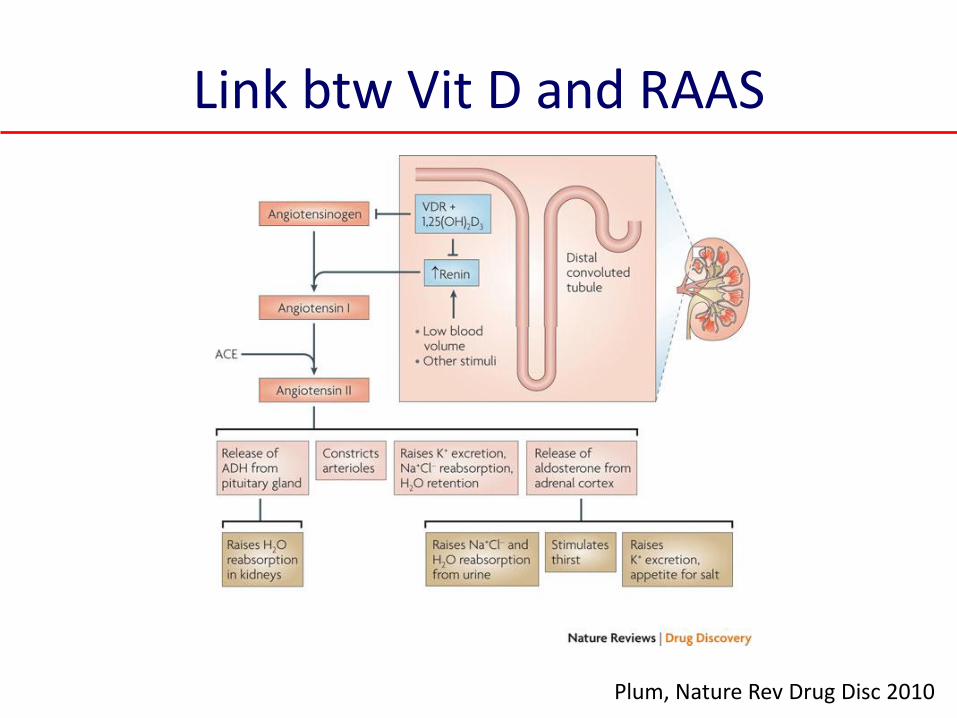
Link btw Vit D and RAAS
Plum, Nature Rev Drug Disc 2010

Vit D analogue: VITAL
• 281 DM(2) with RAS blockade
• 11–339 mg/mmol
• eGFR : 15–90 mL/min/BSA
• 1 μg & 2 μg paricalcitol
• Primary end points
: UACR at 24 wks
• Adverse events: similar
De Zeeuw, Lancet 2010
Glycosaminoglycans: Sulodexide
• DiNAS: 223 T2DM, ACR 20-300mg/g, CKD 2
• 50, 100, 200 mg
• 74% reduction after 4 Mo
• SUN-micro: 1056 T2DM, ACR 35-200mg/g, Cr<1.5mg/dL
• 200 mg + maximal dose of RAS blockade for 4 Mo
• SUN-macro: 2240 T2DM, proteinuria >900mg/d
• 200 mg + With maximal dose of RAS blockade for 24 Mo
• Early termination
Gamabaro, J Am Soc Nephrol 2002 Lewis, Am J Kidney Dis 2011 Packham, J Am Soc Nephrol 2012

Phosphodiesterase inhibitor: Pentoxifyllin
McCormick, Am J Kidney Dis 2008

Anti-Oxidant: Bardoxolone • Phase IIb
• 227 DM(2), eGFR 20 - 45 ml/min/BSA
• Bardoxolone methyl
• Primary outcome: change in eGFR at 24 weeks
• Secondary outcome change in eGFR at 52 wks
Pergola, N Engl J Med 2011
BEACON Bardoxolone Methyl in Patients With CKD and T2DM
• 2185 T2DM, CKD 4 • bardoxolone methyl 20 mg • Primary composite outcome : ESRD or death from CV causes
• 2012.10 : early termination • side effect : muscle spasm, hypomagnesaemia, nausea • Poor adherence : 81%-42%-25%(25-75-150 mg) at 52 wk
Zeewu, N Engl J Med 2013

Zeewu, N Engl J Med 2013

AGE inhibitor : Vitamin B derivatives
• Alkhalaf, Diabetes Care 2010 – DM(2), UAE : 15-300 mg/24 h(+ RAS blockade), 12 wks
– benfotiamine (900 mg/day) (n = 39) vs. placebo (n = 43)
– no difference
• House, JAMA 2010 – type 1 or 2 diabetes, 36 Mo
– radionuclide GFR: vit-B, 16.5 vs. Cont 10.7 , p= .02
– composite outcome: B-vitamin (HR, 2.0; 1.0-4.0)
– P-total homocysteine(umol/L) : 2.2 vs. 2.6, P < .001
Endotheline Receptor Antagonist
• Mann, J Am Soc Nephrol 2010
– 1392 DM(2), 4 Mo, RAS blokade + avosentan 25 & 50 mg/d
– significantly reduction of ACR: 44.3, 49.3, 9.7%(placebo)
– adverse events: fluid overload and CHF
– Early termination
• Kohan, J Am Soc Nephrol 2011
– 89 DM(2), eGFR > 20 ml/min/BSA, UACR 100-3000 mg/gCr
– significant reduction of ACR
– Peripheral edema
– 9% (placebo) vs. 14, 18, 46%(0.25, 0.5, 1.75 mg atrasentan)
ETRA: atresentan
• 211 T2DM • UACR 300-3500, eGFR 30-75 ml/min per 1.73 m2 • multinational, double-blind studies • placebo (n=50) vs. 0.75 (n=78) vs. 1.25 mg (n=83)
+ max. dose of RAS blockade • 12 weeks
• Reduced albuminuria • improved BP and lipid • Increase in weight, decrease in Hb
Zeeuw, J Am Soc Nephrol 2014
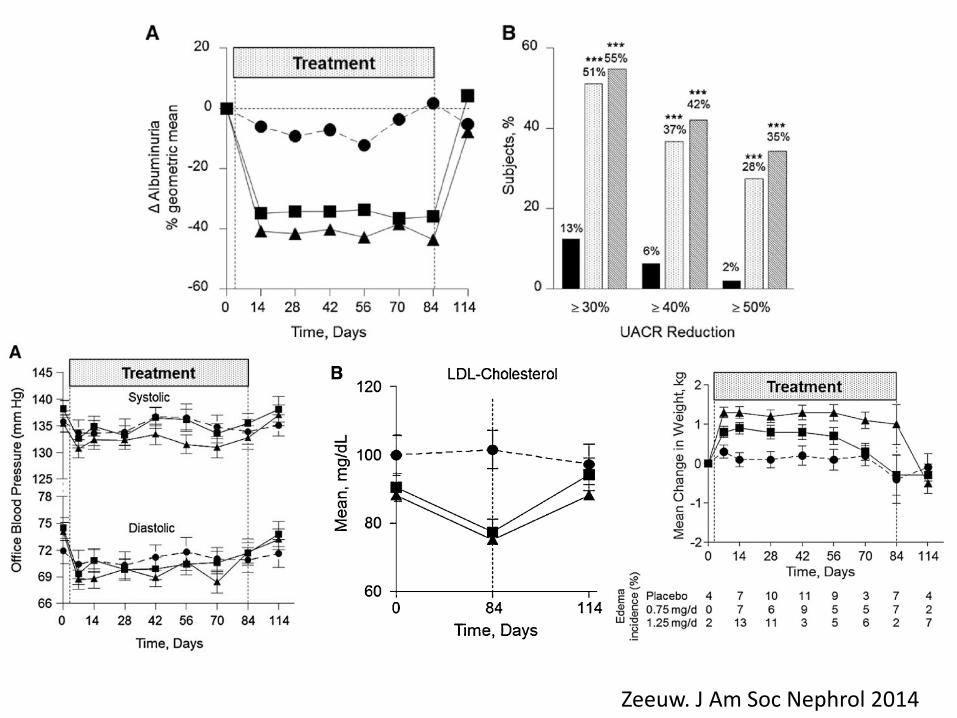
Albuminuria & BP
Zeeuw. J Am Soc Nephrol 2014
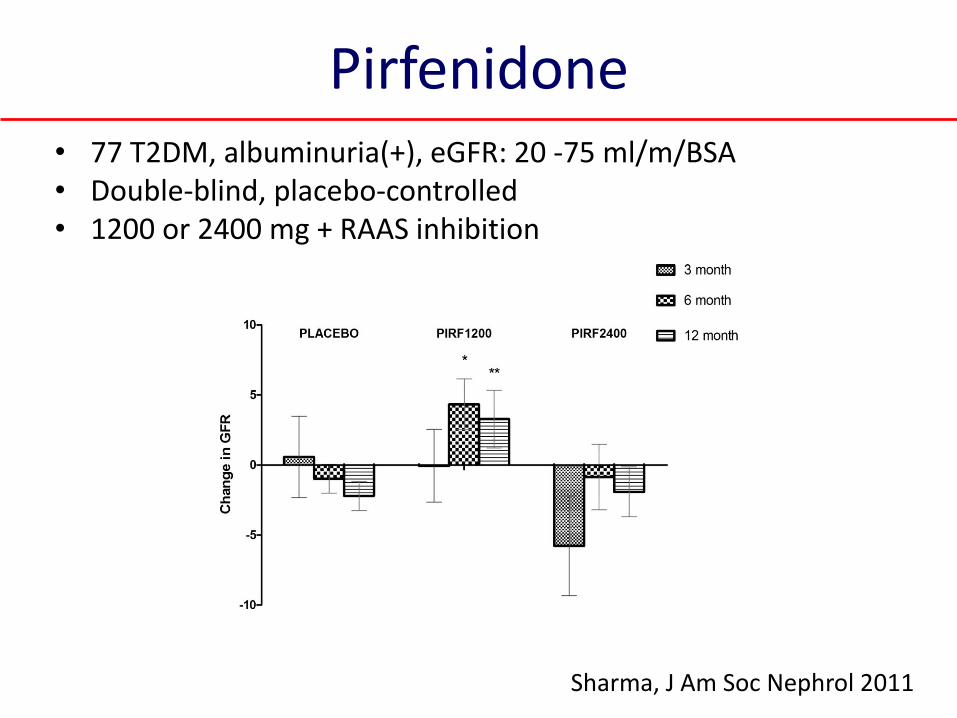
Pirfenidone • 77 T2DM, albuminuria(+), eGFR: 20 -75 ml/m/BSA • Double-blind, placebo-controlled • 1200 or 2400 mg + RAAS inhibition
Sharma, J Am Soc Nephrol 2011
Viable Candidates
• PKC inhibitor: ruboxistaurin, phase III (stop)
• Anti-CTGF Ab: phase II (stop)
• JAK ½ inhibitor: phase II
Remaining but Important Issues
• Acute kidney injury
: contrast, NSAIDs, heart failure, hypoglycemia,
DM foot, hospitalizations , surgical interventions,
UTI, Postinfectious glomerulonephritis
• Ischemic nephropathy, peripheral artery dz
• Smoking
• Diet: low salt, low protein
• Exercise, weight control

Kelly, Am J Nephrol 2010
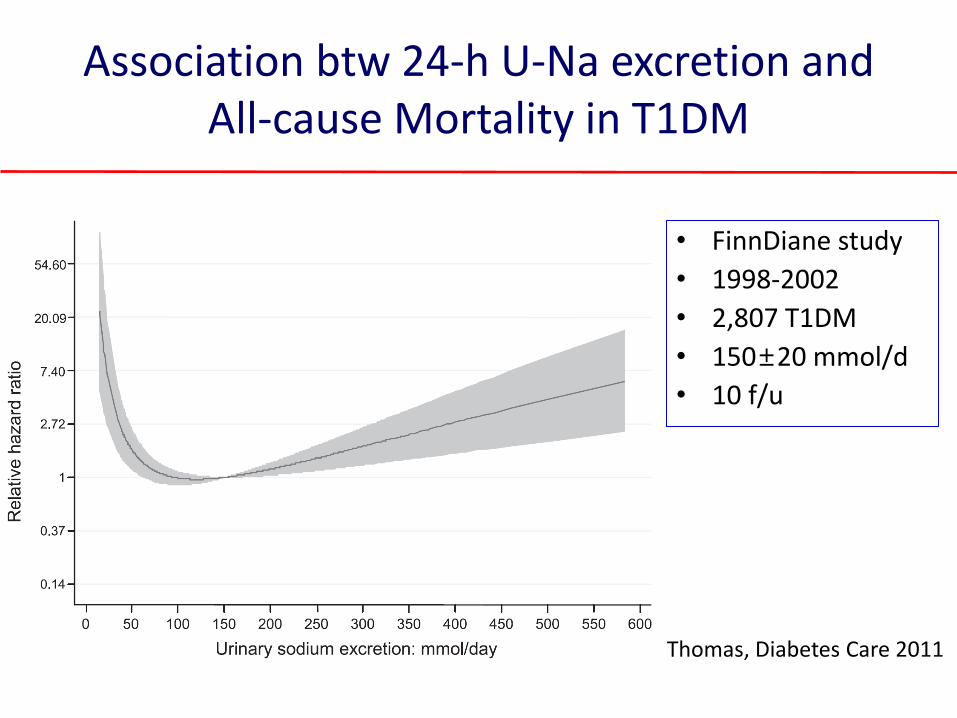
Association btw 24-h U-Na excretion and All-cause Mortality in T1DM
• FinnDiane study
• 1998-2002
• 2,807 T1DM
• 150±20 mmol/d
• 10 f/u
Thomas, Diabetes Care 2011
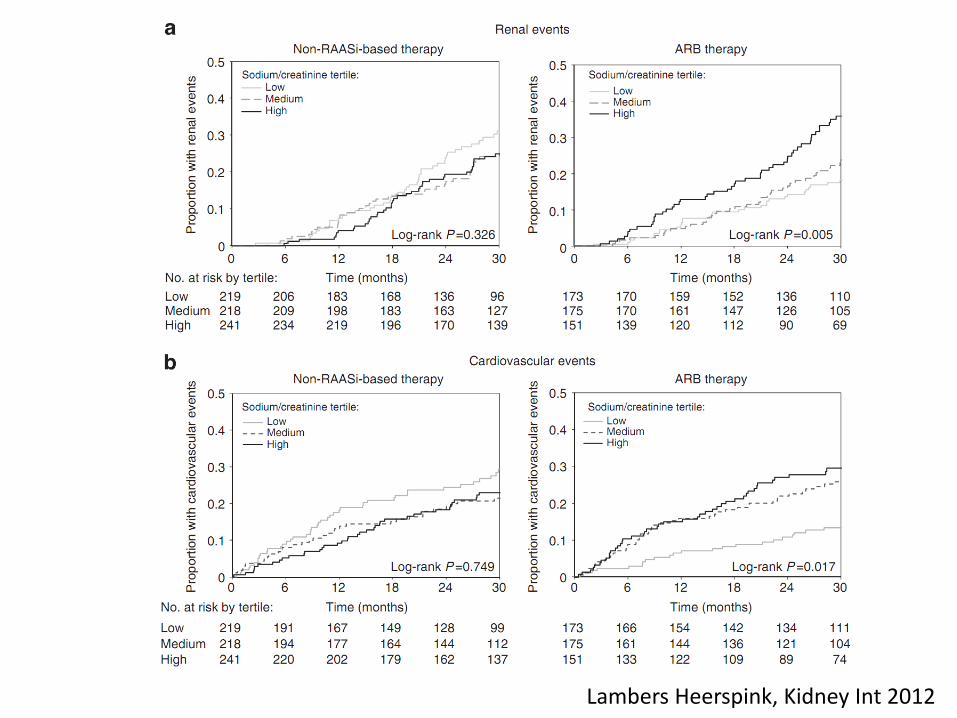
Lambers Heerspink, Kidney Int 2012

eGFR decline

Summary & Conclusion
• Primary prevention with RAS blockade : NO
• Combination of RAS blockade: NO
• Mineralocorticoid blocker: Yes
• New drugs: vit D analogue, pentoxifyllin, ETRA
• Individualized therapeutic strategy
• Multifactorial & non-pharmacological intervention





























