Embed Size (px)
Citation preview

New Atrial Fibrillation/Flutter Pathway and GRASP Tool
Kay Elliott British Heart Foundation
Arrhythmia Nurse Specialist
Dorset County Hospital NHS Foundation Trust

AimAim
To Discuss:
• Primary/Secondary Care Pathway for new onset atrial fibrillation/Flutter
• GRASP* Tool – Identifying and risk stratifying chronic AF/Flutter in primary care
*Guidance on Risk Assessment for Stroke Prevention in Atrial Fibrillation in Patients in Primary Care

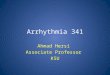
Admit to Hospital
Primary CareSTART WARFARIN AND RATE CONTROL (see box A)
Issue patient education leaflet:‘Atrial Fibrillation and Warfarin’. Attached, also available: www.patient.co.uk/showdoc/23068883
ParoxysmalRefer to cardiology team in the usual way.
Cardiologist
PersistentFax referral to Rapid Access Atrial Fibrillation/Flutter Clinic. (Form attached. Also available on Dorset County Hospital intranet or by contacting BHF Arrhythmia Nurse)
NEED FURTHER ADVICE? CONTACT:BHF ARRHTYHMIA NURSE: 01305 254920
Box A: Rate control First Line:1. 1. Beta-blocker (e.g. Bisoprolol)
or a rate limiting calcium antagonist (e.g. Diltiazem), if beta-blocker contraindicated
2. 2. Digoxin – additional to optimise rate control, where required. As monotherapy only in predominantly sedentary patients.
NICE (2006)
New Onset Atrial Fibrillation or FlutterIs the patient acutely unwell?
Yes No
Rapid Access Atrial
Fibrillation/Flutter Clinic

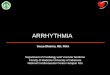
Rapid Access Atrial Fibrillation/Flutter Clinic
ONE STOP APPOINTMENT (WITHIN 4 WEEKS OF REFERRAL)
1. ECHO AND ECG2. BHF ARRHYTHMIA NURSE CLINIC:
Review history, symptoms, test and examination results
Patient education Agree treatment plan: DC Cardioversion or
Rate Control Arrange ongoing follow-up, where required
Cardiologist input into RAAF clinic. Also patients referred for DC Cardioversion from cardiology clinic or in-patient stay.
Cardiologist
Primary CareManage long-term warfarin and rate-control
BHF Arrhythmia Nurse Specialist:Arrange DC Cardioversion

Prepare for DC Cardioversion:Weekly INR (Target 2.5-3.0), must have INR >2.0 for four full weeks prior to DC Cardioversion (see next page)
DC Cardioversion – BHF ARRHYTHMIA NURSE/DAY SURGERY UNIT
Procedure Review of medications and treatment pre-discharge (Cardiology Specialist Registrar and BHF Arrhythmia Nurse) Review with BHF Arrhythmia Nurse at 4 weeks, ongoing treatment plan
N.B. Maintaining a therapeutic INR during the four weeks post successful DC Cardioversion is important in terms of stroke risk reduction.

4 Weeks post procedure Follow-Up (NICE, 2006) BHF Arrhythmia Nurse
Is the Patient in Sinus Rhythm?
Cardiology Review
Patient remains symptomatic despite adequate rhythm or rate control.
Other cardiac complications are revealed.
Depending on clinical indications and patient preference either:
1. Re-attempt DC Cardioversion with amiodarone cover
2. Refer for ablation therapy3. Rate control/Warfarin (primary Care)
YES NO
Refer to Electrophysiology centre for ablation therapy, if appropriate
Yes/No
6 months post procedure Follow-Up (NICE, 2006) BHF Arrhythmia Nurse
Is the Patient in Sinus Rhythm?

6 months post procedure Follow-Up (NICE, 2006) BHF Arrhythmia Nurse
Is the Patient in Sinus Rhythm?
Yes No
Depending on clinical indications and patient preference either:
1. Re-attempt DC Cardioversion with amiodarone cover
2. Referral for ablation therapy3. Rate control/Warfarin (primary
Care)
Discharged to primary care and advised to seek medical attention if symptoms recur

Guidance on Risk Assessment for Guidance on Risk Assessment for Stroke Prevention in Atrial Stroke Prevention in Atrial Fibrillation (GRASP – AF)Fibrillation (GRASP – AF)
• Prevalence of AF in primary care is 1.2% (England)
• 12,500 strokes per year are thought to be directly attributable to AF
• Estimated annual cost of maintaining one patient on warfarin: £383
• Estimated cost per stroke due to AF is £11,900 in the first year post stroke occurrence

Guidance on Risk Assessment for Guidance on Risk Assessment for Stroke Prevention in Atrial Stroke Prevention in Atrial Fibrillation (GRASP – AF)Fibrillation (GRASP – AF)
NICE estimate that 46% of patients that
should be on warfarin are not receiving it
Warfarin reduces risk of stroke by 64% in atrial fibrillation
Aspirin reduces the risk of stroke by 22% in atrial fibrillation

Guidance on Risk Assessment for Guidance on Risk Assessment for Stroke Prevention in Atrial Stroke Prevention in Atrial Fibrillation (GRASP – AF)Fibrillation (GRASP – AF)
The GRASP-AF Tool facilitates audit to identify high risk AF patients not on warfarin
It is a MIQUEST IT tool that can be freely downloaded from www.improvement.nhs.uk

Guidance on Risk Assessment for Guidance on Risk Assessment for Stroke Prevention in Atrial Stroke Prevention in Atrial Fibrillation (GRASP – AF)Fibrillation (GRASP – AF)
It can be used to identify patients in atrial fibrillation with a CHADS2 score of >1
The final report can exclude those with recorded contraindications to warfarin

SummarySummary
• Identify new atrial fibrillation/flutter – (include routine pulse checks at all appropriate consultations)
• Refer to RAAF clinic (persistent), consultant (paroxysmal) or admit if acutely unwell
• Rate Control and warfarin/aspirin in primary care• Patients will be reviewed with echocardiogram and • specialist clinic/consultant input• GRASP-AF Tool – opportunity to ensure practice
population on evidence based stroke prophylaxis in atrial fibrillation – Potential to reduce morbidity/mortality
and health costs

Over to You – Any Questions?Over to You – Any Questions?