Embed Size (px)
Citation preview

Research report
New alterations at potentially regulated regions of the Glial DerivedNeurotrophic Factor gene in bipolar disorder
Roghaiyeh Safari a,n, Zeliha Tunca b, Aysegul Ozerdemb,c, Deniz Ceylan b,Cigdem Eresen Yazicioglu d, Meral Sakizli d
a Department of Molecular Medicine, Dokuz Eylul University, Faculty of Medicine and Institute of Health Sciences, Inciralti, Izmir, Turkeyb Department of Psychiatry, Dokuz Eylul University, Faculty of Medicine, Izmir, Turkeyc Department of Neuroscience, Dokuz Eylul University, Faculty of Medicine, Izmir, Turkeyd Department of Medical Biology and Genetics, Dokuz Eylul University, Faculty of Medicine, Izmir, Turkey
a r t i c l e i n f o
Article history:Received 11 February 2014Received in revised form2 May 2014Accepted 4 June 2014Available online 12 June 2014
Keywords:GDNFBipolar disorderSNP
a b s t r a c t
Introduction: Glial Derived Neurotrophic Factor (GDNF) plays an important role in the survival anddifferentiation of neurons. We examined 50upstream and 30 untranslated region of the GDNF gene by PCRamplification and direct sequencing to explore the effect of alteration in the potentially regulated part ofGDNF in bipolar disorder.Materials and methods: Sixty-six patients with bipolar disorder, 27 first degree relatives of these patientsand 56 healthy volunteers were screened for mutations and polymorphisms in GDNF gene.Results: Seven previously reported polymorphisms and additional three novel allele variants of GDNFwere detected. Association test of rs2075680 C4A SNP showed significant difference between patientsand healthy subjects with higher allele frequency in healthy subjects performing Chi-square test.However, there was no significant difference after multiple test corrections between groups. There wereno significant differences in association test of rs2075680 C4A SNP between first degree relatives andhealthy volunteers/patients. rs142426358 T4C SNP was seen only in one patient with an early age ofillness onset. New T4A alterations were found in chromosome locations 5:37812784 and 5:37812782 intwo male bipolar disorder patients with age of illness onset 12 and 24 years.Limitations: The sample size was relatively small.Discussion: Our study proposes the suggestive association between polymorphisms in the potentialregulatory sites of GDNF and bipolar disorder.
& 2014 Elsevier B.V. All rights reserved.
1. Introduction
Bipolar disorder (BD) is one of the most debilitating psychiatricdisorders which frequently presents with treatment resistance(Aziz et al., 2006). It is a chronic illness characterized by depressiveand manic/hypomanic episodes and well states in between(Barnett and Smoller, 2009). The life time prevalence of BD isbetween 1% and 4% (Barnett and Smoller, 2009; Hirschfeld andVornik, 2005; Kessler et al., 2005; Merikangas et al., 2007). BDdisrupts overall functioning and reduces quality of life of thesuffering individual. It causes 30% decrease in life expectancy ofthe patient. Comorbid medical conditions are frequent, long timehospitalization is common and suicide risk is high (20%) in bipolardisorder. Overall, the illness is an important socio-economicburden on the individual, family members and society (Fagiolini
and Goracci, 2009; Fiedorowicz et al., 2008; Goldberg and Harrow,2004; Kemp et al., 2014; McIntyre et al., 2008; Young and Grunze,2013). BD is a highly heritable disease. Family, twins and adapta-tion studies reveal a 60–85% genetic influence (Barnett andSmoller, 2009). Various molecular methods demonstrate that thegenetic etiology of BD is polygenic and multifactorial with avariable penetrance (Barnett and Smoller, 2009; Craddock andSklar, 2013).
Glial cell line Derived Neurotrophic Factor (GDNF) is a neuro-trophic factor that is widely distributed in the central nervoussystem. It has many important roles in the nervous system such assynapse formation, plasticity, survival, neurogenesis, neuronalgrowth, neuritis outgrowth and differentiation of distinct popula-tions of central and peripheral neurons, especially the midbraindopaminergic neurons and spinal motor neurons (Airaksinen andSaarma, 2002; Ledda et al., 2007; Wang et al., 2008). As a whole,GDNF is a survival factor for midbrain neurons during develop-ment (Lin et al., 1993). Also it is important for the maintenance ofmature neurons in the adult brain, as well as for their protection/
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jad
Journal of Affective Disorders
http://dx.doi.org/10.1016/j.jad.2014.06.0020165-0327/& 2014 Elsevier B.V. All rights reserved.
n Corresponding author. Tel.: þ90 5548846886.E-mail address: [email protected] (R. Safari).
Journal of Affective Disorders 167 (2014) 244–250
repair upon injury (Benn and Woolf, 2004; Sariola and Saarma,2003). There is a growing body of evidence demonstrating thatGDNF and other neurotrophic factors have crucial roles in thepathophysiology of mood disorders (Nibuya et al., 1999; Otsuki etal., 2008). Recent studies showed alteration in the expression ofGDNF in bipolar disorder patients (Barbosa et al., 2011; Rosa et al.,2006; Zhang et al., 2010).
50 upstream and 30UTRs of the genes contain elements arran-ging mRNA and protein expression. Regulatory elements in 50
upstream control the gene expression by mRNA transcription(Maston et al., 2006). The regulatory elements in 30UTR organizethe expression by multiple aspects of mRNA metabolism, includingnuclear export, cytoplasmic localization, translational efficiencyand mRNA stability (Andreassi and Riccio, 2009).
The aim of the study was to investigate the effect of 50upstreamand 30UTRs of GDNF alterations in association with bipolar dis-order. We examined these potential regulatory parts of GDNF geneby PCR amplification and direct sequencing.
2. Materials and methods
2.1. Subjects
The study was conducted at Dokuz Eylul University Hospital inIzmir in Caucasian Turkish population. The diagnosis of bipolardisorder was confirmed by two psychiatrists through structuredinterview for axis I disorders for the Diagnostic and StatisticalManual of Mental Disorders (DSM-IV) (SCID-I) (First et al., 2002).Fifty-six healthy volunteers among the residents, faculty or staff ofthe university hospital, who consented to participate, wereincluded in the study. They were not on any medication and hadno history of any psychiatric disorders as assessed by the SCID-Inon-patient version. First degree relatives of the patients (parents,siblings or offspring) without a history of physical and/or mentalillness (as assessed by the SCID-I non-patient version) and psy-chotropic medication use were included in the study.
The study was approved by Dokuz Eylul University HospitalEthics Committee. Written informed consent was obtained fromall participants. The demographic characteristics of 66 patients, 27first degree relatives and 56 healthy individuals are given inTable 1. Thirty-three of patients were euthymic; 15 were indepression and 18 were in manic episode at the time of the study.The majority of patients (s¼64) had bipolar disorder type I. Age ofonset of bipolar disorder was defined as the age at first affectiveepisode (Daban et al., 2006; Roy-Byrne et al., 1985). This informa-tion was obtained during interviews with patient and family and/or medical records. The age of illness onset younger than 19 yearswas considered as “early onset bipolar disorder” (Baldessariniet al., 2012; Sachs et al., 2000).
2.2. Genetic analysis
DNA was isolated from 2 cc peripheral blood sample using theRTA Blood Genomic DNA Isolation Kit following the manufac-turer's recommended protocol. The quality and quantity of DNAsamples were measured with Pico drop (Pico100) using 2 ml DNA.PCR primers were designed by primer 3.4 software (Rozen andSkaletsky, 2000) and manufactured by DNAlab. Primer sequences,amplification conditions and PCR components are shown inTable 2. We used recombinant taq polymerase (Fermantes), Taqbuffer þKCL–MgCl2 (Fermantes), MgCl2 (Fermantes) and dNTPmix (Fermantes) for PCR amplifications. The PCR reactions wereperformed on a 48 well Techne thermal Cycler in PCR tubes. 5 mlof each post-PCR reaction products was analyzed by agarosegel electrophoresis to determine the presence or absence of
nonspecific products. Those post-PCR reaction products withoutnonspecific products were selected for purification and cleaningfrom any primer, primer-dimer or dNTPs. Purification and sequen-cing of PCR products were performed by Macrogen sequencingservice.
Reference sequences for GDNF and SNP information were achievedfrom the Ensemble Human Genome Browser (ENSG00000168621).Sequences analyzed by using DNADynamo (BlueTractorSoftware Ltd.,North Wales, UK) and Chromas softwares. PROMO online softwareusing version 8.3 of TRANSFAC was used to predict transcriptionregulatory elements binding sites upstream of the GDNF before exon 1(Farre et al., 2003; Messeguer et al., 2002). To determine miRNA targetsite in 30UTR of GDNF we used miRBase (Griffiths-Jones, 2004;Griffiths-Jones et al., 2006; Griffiths-Jones et al., 2008; Kozomaraand Griffiths-Jones, 2011) DIANA LAB (Maragkakis et al., 2009) onlinesoftwares.
2.3. Data analysis
Hardy–Weinberg equilibrium was evaluated by using SHEsissoftware online (Shi and He, 2005). Odds ratio (OR) and itscorresponding 95% confidence interval (CI) were computed toquantify the association of genotype frequency and allele fre-quency with bipolar disorder risk. Chi-square test was used to testassociation of SNPs with bipolar disorder. Unpaired t-test was usedto compare age of onset of illness between groups with SNPs andwithout SNPs. Statistical significance was set at po0.05 for Chi-square test and t-test. The level of significance was corrected fortesting of the multiple SNPs (n¼10) and the p-value was set atpo0.005.
3. Results
3.1. New T4A alteration in chromosome locations 5:37812784 and5:37812782 in bipolar disorder patients
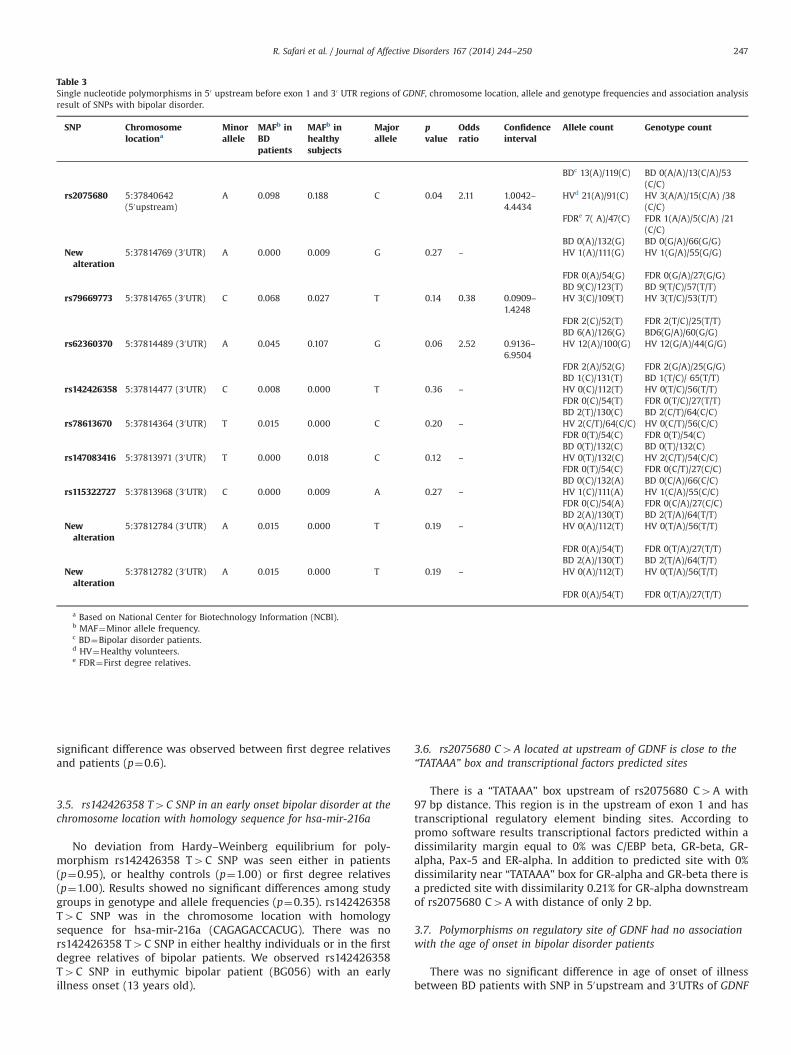
Single nucleotide polymorphisms in 50 upstream of exon 1 and30 UTR region of GDNF, chromosome locations, allele and genotypefrequencies and association analysis of SNPs with bipolar disorderare shown in Table 3. We found 10 single locus alterations in thisstudy. The alterations of rs2075680 C4A, rs79669773 T4C,rs62360370 G4A, rs142426358 T4C, rs786136670 C4T,rs147083416 C4T, rs115322727 A4C SNPs were previouslyreported. We have seen three new alterations in the entire group.rs2075680 C4A was located at 50 upstream of exon 1 and theother demonstrated SNPs were located at 30 UTR region of GDNF.There were new T4A alterations in chromosome locations5:37812784 and 5:37812782 in two male bipolar disorder patients(case code: BG518 and BG554) with age of illness onset 12 and 24years. We also found a new G4A alteration in chromosomelocation 5:37814769 in one male healthy participant (case code:BG310).
Table 1Demographic characteristics of the subjects showed no significant differences inage (p¼0.80) and gender (p¼0.90) among study groups.
Study group Number Female/male
Age (years)Mean7SD
Age of illness onsetMean7SD
BD patients 66 37/29 37.0710.42 26.60710.10Healthyvolunteers
56 32/24 37.49711.52 n.a.
First degreerelatives
27 19/8 42.19713.92 n.a.
R. Safari et al. / Journal of Affective Disorders 167 (2014) 244–250 245

rs142426358 T4C SNP was seen in a female euthymic patient(case code: BG056). There was no rs142426358 T4C SNP either inhealthy volunteers or in the first degree relatives. There was nosignificant difference between patients, relatives or healthy volun-teers (χ2¼0.85, p¼0.356). rs147083416 C4T SNP was observedonly in two healthy volunteers (case code: BG331 and BG283), butneither in patients nor in their first degree relatives. No significantdifference in allele and genotype frequencies was observed amonggroups (χ2¼2.39, p¼0.121). rs115322727 A4C SNP was found inone healthy volunteer (case code: BG624), but not in patients orrelatives. No significant difference was seen in allele and genotypefrequencies among groups (χ2¼1.18, p¼0.276). The two bipolardisorder type II patients in this study (BG012 and BG418) showedno SNP.
3.2. GDNF rs2075680 C4A SNP over-represented in healthyvolunteers compared to bipolar disorder patients
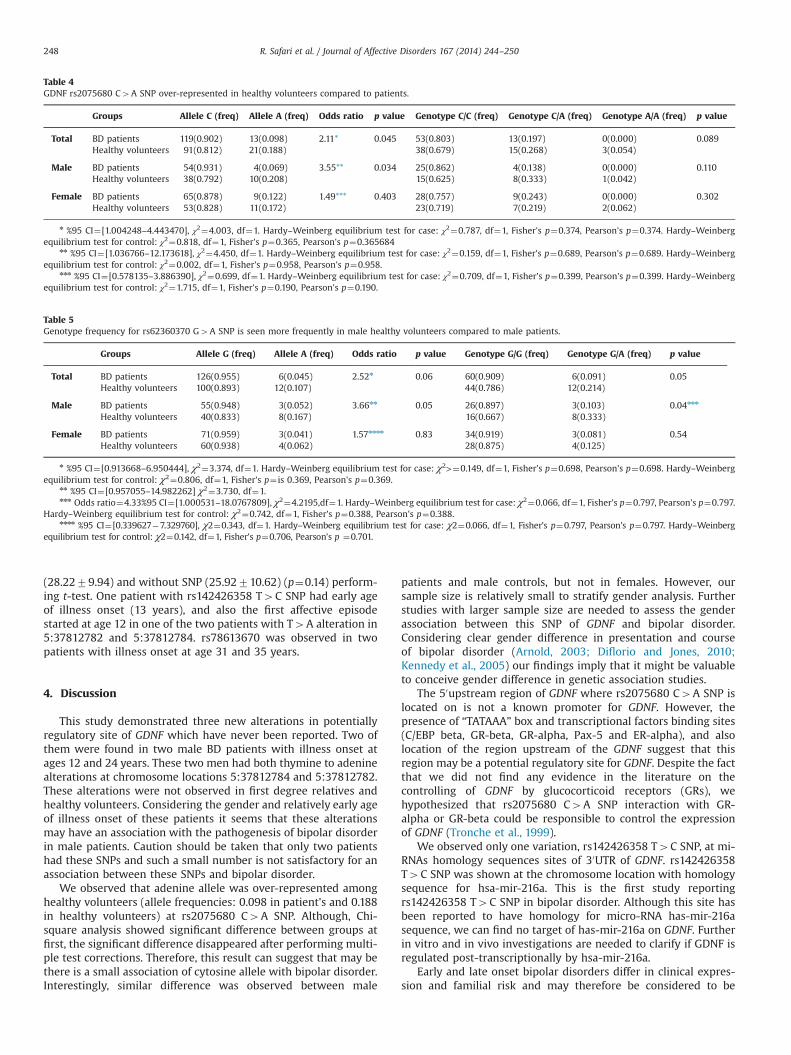
Genotype distributions, allele frequencies of rs2075680 C4ASNP and its risk prediction are presented in Table 4. No deviationfrom Hardy–Weinberg equilibrium for polymorphism rs2075680C4A was seen either in patients (p¼0.37), or in their first degreerelatives (p¼0.35) or in healthy volunteers (p¼0.36). rs2075680C4A over-represented in healthy volunteers (21/91) than patients(13/119) also in male healthy volunteers (10/38) than malepatients (4/54). Performing Chi-square test and considering pvalue threshold at 0.05 there were significant differences in theallele frequency for rs2075680 C4A SNP between BD patients andhealthy volunteers (p¼0.04; OR¼2.11, 95% CI¼[1.0042–4.4434])also between male patients and male volunteers (p¼0.03;OR¼3.55, 95% CI¼[1.0367–12.17]). However, after multiple testcorrections with the p value of 0.005 the significance disappeared.
rs2075680 C4A SNP was seen in six first degree relatives(BG007, BG060, BG069, BG 088, BG146, BG225) and the probondsof BG007, BG060, BG069 and BG225 had this SNP. No significantdifference in allele and genotype analysis was observed betweenfirst degree relatives and patients/healthy volunteers. No signifi-cant difference was observed in the genotype frequencies forrs2075680 C4A between BD patients and healthy volunteers(p¼0.09) or first degree relatives (p¼0.53). There was no sig-nificant difference in the genotype frequencies for rs2075680
C4A SNP between male patients and male healthy subjects.Moreover, no significant differences in either allele frequenciesor genotype frequencies of rs2075680 C4A was observedbetween female BD patients and female healthy subjects (p¼0.4;OR¼1.49, 95% CI¼[0.57–3.88]).
3.3. rs79669773 T4C SNP had no association with bipolar disorder
No deviation from Hardy–Weinberg equilibrium for poly-morphism rs79669773 T4C was seen in either patients(p¼0.55) or healthy subjects (p¼0.83) or first degree relatives(p¼0.84). There were no significant differences in either allelefrequencies or genotype frequencies among BD patients comparedwith healthy subjects (p¼0.13) and first degree relatives (p¼0.41).This SNP was seen in two first degree relatives (BG024 andBG204). The probond of BG024 also had this SNP.
3.4. Genotype frequency for rs62360370 G4A SNP was seen morefrequently in male healthy volunteers compared to male patients
Hardy–Weinberg equilibrium test showed no deviation in thepatients group (p¼0.69) or healthy volunteers group (p¼0.36) orfirst degree relatives group (p¼0.84) Table 5. There were nosignificant differences between patients group and healthy parti-cipants group in allele (p¼0.06; OR¼2.52, 95% CI¼[0.91–6.95])and genotype frequencies (p¼0.05; OR¼2.72, 95% CI¼[0.64–5.18]) for rs62360370 G4A SNP. Similarly, no significantly differ-ences were seen in female patients compared with female healthyparticipants in either allele (p¼0.83; OR¼1.57, 95% CI¼[0.33–7.32]) or genotype (p¼0.54; OR¼1.61, 95% CI¼[0.33–7.84]) fre-quencies. There was significant difference in the genotype fre-quency between male patients and healthy subjects (p¼0.04;OR¼4.33, 95% CI¼[1.00–18.076]) performing Chi-square and con-sidering the p value threshold at 0.05. However, after correctionfor multiple testing there was no significant difference betweenmale groups in genotype frequency. Statistical analysis showed nosignificant difference in the allele frequency between patients andhealthy subjects in males (p¼0.05; OR¼3.66, 95% CI¼[0.95–14.69]). This SNP was seen in two first degree relatives (BG060and BG225) that has not been seen in their probonds. However, no
Table 2PCR primers, amplification conditions and PCR components.
Primers PCR condition PCR components
Forward5′–TGGAGCCTAGGACTGAGGAG–3′Reverse5′–AAGGGGCAATCCGAACTT–3′
30 s at 95 1C, 45 s at 58.1 1C and30 s at 72 1C(35 cycles)
0.11 pM of the primers, 20 ng DNA template, 0.3 mM dNTP mix, 30 mM KCl taqbuffer, 0.3 mM MgCl2, 1 unit taq polymerase and 40 ml dH2O
5 min at 72 1C; 5 min at 94 1C(One cycle)
Forward5′–CCGCTAAAAGGTGTGGATGT–3′Reverse5′–CACACACCGTGATGGAAATC–3′
30 s at 951C, 30 s at 58.5 1C and30 s at 72 1C(35 cycles)
0.11 pM of the primers, 20 ng DNA template, 0.4 mM dNTP mix, 40 mM KCl taqbuffer, 0.5 mM MgCl2, 1 unit taq polymerase and 21.4 ml dH2O
5 min at 721C; 5 min at 941C(One cycle)
Forward5′–CAACCAAAAAGGCTGTGCTC–3′Reverse5′–CAGCATTAAATCCAGGACTACC–3′
30 s at 95 1C, 30 s at 58.5 1C and30 s at 72 1C(35 cycles)
0.11 pM of the primers, 20 ng DNA template, 0.4 mM dNTP mix, 40 mM KCl taqbuffer, 0.5 mM MgCl2, 1 unit taq polymerase and 21.4 ml dH2O
5 min at 721C; 5 min at 941C(One cycle)
Forward5′–ACCCAAACACCTGACAGCTC–3′Reverse5′–TGATGGAGGCCAGTATTTCA–3′
30 s at 95 1C, 30 s at 55.8 1C and30 s at 72 1C(35 cycles)
0.08 pM of the primers, 20 ng DNA template, 0.5 mM dNTP mix, 40 mM KCl taqbuffer, 1.5 mM MgCl2, 1 unit taq polymerase and 23.4 ml dH2O
5 min at 72 1C; 5 min at 94 1C(One cycle)
Forward5′–AAGGCCTTCCCTCTCACACT–3′Reverse5′–GTGATTGGTTGCTGGGAGTT–3′
30 s at 95 1C, 30 s at 62 1C and30 s at 72 1C(35 cycles)
0.11 pM of the primers, 20 ng DNA template, 0.4 mM dNTP mix, 40 mM KCl taqbuffer, 0.5 mM MgCl2, 1 unit taq polymerase and 29.5 ml dH2O
5 min at 72 1C; 5 min at 94 1C(One cycle)
R. Safari et al. / Journal of Affective Disorders 167 (2014) 244–250246
significant difference was observed between first degree relativesand patients (p¼0.6).
3.5. rs142426358 T4C SNP in an early onset bipolar disorder at thechromosome location with homology sequence for hsa-mir-216a
No deviation from Hardy–Weinberg equilibrium for poly-morphism rs142426358 T4C SNP was seen either in patients(p¼0.95), or healthy controls (p¼1.00) or first degree relatives(p¼1.00). Results showed no significant differences among studygroups in genotype and allele frequencies (p¼0.35). rs142426358T4C SNP was in the chromosome location with homologysequence for hsa-mir-216a (CAGAGACCACUG). There was nors142426358 T4C SNP in either healthy individuals or in the firstdegree relatives of bipolar patients. We observed rs142426358T4C SNP in euthymic bipolar patient (BG056) with an earlyillness onset (13 years old).
3.6. rs2075680 C4A located at upstream of GDNF is close to the“TATAAA” box and transcriptional factors predicted sites
There is a “TATAAA” box upstream of rs2075680 C4A with97 bp distance. This region is in the upstream of exon 1 and hastranscriptional regulatory element binding sites. According topromo software results transcriptional factors predicted within adissimilarity margin equal to 0% was C/EBP beta, GR-beta, GR-alpha, Pax-5 and ER-alpha. In addition to predicted site with 0%dissimilarity near “TATAAA” box for GR-alpha and GR-beta there isa predicted site with dissimilarity 0.21% for GR-alpha downstreamof rs2075680 C4A with distance of only 2 bp.
3.7. Polymorphisms on regulatory site of GDNF had no associationwith the age of onset in bipolar disorder patients
There was no significant difference in age of onset of illnessbetween BD patients with SNP in 50upstream and 30UTRs of GDNF
Table 3Single nucleotide polymorphisms in 50 upstream before exon 1 and 30 UTR regions of GDNF, chromosome location, allele and genotype frequencies and association analysisresult of SNPs with bipolar disorder.
SNP Chromosomelocationa
Minorallele
MAFb inBDpatients
MAFb inhealthysubjects
Majorallele
pvalue
Oddsratio
Confidenceinterval
Allele count Genotype count
BDc 13(A)/119(C) BD 0(A/A)/13(C/A)/53(C/C)
rs2075680 5:37840642(50upstream)
A 0.098 0.188 C 0.04 2.11 1.0042–4.4434
HVd 21(A)/91(C) HV 3(A/A)/15(C/A) /38(C/C)
FDRe 7( A)/47(C) FDR 1(A/A)/5(C/A) /21(C/C)
BD 0(A)/132(G) BD 0(G/A)/66(G/G)Newalteration
5:37814769 (30UTR) A 0.000 0.009 G 0.27 – HV 1(A)/111(G) HV 1(G/A)/55(G/G)
FDR 0(A)/54(G) FDR 0(G/A)/27(G/G)BD 9(C)/123(T) BD 9(T/C)/57(T/T)
rs79669773 5:37814765 (30UTR) C 0.068 0.027 T 0.14 0.38 0.0909–1.4248
HV 3(C)/109(T) HV 3(T/C)/53(T/T)
FDR 2(C)/52(T) FDR 2(T/C)/25(T/T)BD 6(A)/126(G) BD6(G/A)/60(G/G)
rs62360370 5:37814489 (30UTR) A 0.045 0.107 G 0.06 2.52 0.9136–6.9504
HV 12(A)/100(G) HV 12(G/A)/44(G/G)
FDR 2(A)/52(G) FDR 2(G/A)/25(G/G)BD 1(C)/131(T) BD 1(T/C)/ 65(T/T)
rs142426358 5:37814477 (30UTR) C 0.008 0.000 T 0.36 – HV 0(C)/112(T) HV 0(T/C)/56(T/T)FDR 0(C)/54(T) FDR 0(T/C)/27(T/T)BD 2(T)/130(C) BD 2(C/T)/64(C/C)
rs78613670 5:37814364 (30UTR) T 0.015 0.000 C 0.20 – HV 2(C/T)/64(C/C) HV 0(C/T)/56(C/C)FDR 0(T)/54(C) FDR 0(T)/54(C)BD 0(T)/132(C) BD 0(T)/132(C)
rs147083416 5:37813971 (30UTR) T 0.000 0.018 C 0.12 – HV 0(T)/132(C) HV 2(C/T)/54(C/C)FDR 0(T)/54(C) FDR 0(C/T)/27(C/C)BD 0(C)/132(A) BD 0(C/A)/66(C/C)
rs115322727 5:37813968 (30UTR) C 0.000 0.009 A 0.27 – HV 1(C)/111(A) HV 1(C/A)/55(C/C)FDR 0(C)/54(A) FDR 0(C/A)/27(C/C)BD 2(A)/130(T) BD 2(T/A)/64(T/T)
Newalteration
5:37812784 (30UTR) A 0.015 0.000 T 0.19 – HV 0(A)/112(T) HV 0(T/A)/56(T/T)
FDR 0(A)/54(T) FDR 0(T/A)/27(T/T)BD 2(A)/130(T) BD 2(T/A)/64(T/T)
Newalteration
5:37812782 (30UTR) A 0.015 0.000 T 0.19 – HV 0(A)/112(T) HV 0(T/A)/56(T/T)
FDR 0(A)/54(T) FDR 0(T/A)/27(T/T)
a Based on National Center for Biotechnology Information (NCBI).b MAF¼Minor allele frequency.c BD¼Bipolar disorder patients.d HV¼Healthy volunteers.e FDR¼First degree relatives.
R. Safari et al. / Journal of Affective Disorders 167 (2014) 244–250 247
(28.2279.94) and without SNP (25.92710.62) (p¼0.14) perform-ing t-test. One patient with rs142426358 T4C SNP had early ageof illness onset (13 years), and also the first affective episodestarted at age 12 in one of the two patients with T4A alteration in5:37812782 and 5:37812784. rs78613670 was observed in twopatients with illness onset at age 31 and 35 years.
4. Discussion
This study demonstrated three new alterations in potentiallyregulatory site of GDNF which have never been reported. Two ofthem were found in two male BD patients with illness onset atages 12 and 24 years. These two men had both thymine to adeninealterations at chromosome locations 5:37812784 and 5:37812782.These alterations were not observed in first degree relatives andhealthy volunteers. Considering the gender and relatively early ageof illness onset of these patients it seems that these alterationsmay have an association with the pathogenesis of bipolar disorderin male patients. Caution should be taken that only two patientshad these SNPs and such a small number is not satisfactory for anassociation between these SNPs and bipolar disorder.
We observed that adenine allele was over-represented amonghealthy volunteers (allele frequencies: 0.098 in patient's and 0.188in healthy volunteers) at rs2075680 C4A SNP. Although, Chi-square analysis showed significant difference between groups atfirst, the significant difference disappeared after performing multi-ple test corrections. Therefore, this result can suggest that may bethere is a small association of cytosine allele with bipolar disorder.Interestingly, similar difference was observed between male
patients and male controls, but not in females. However, oursample size is relatively small to stratify gender analysis. Furtherstudies with larger sample size are needed to assess the genderassociation between this SNP of GDNF and bipolar disorder.Considering clear gender difference in presentation and courseof bipolar disorder (Arnold, 2003; Diflorio and Jones, 2010;Kennedy et al., 2005) our findings imply that it might be valuableto conceive gender difference in genetic association studies.
The 50upstream region of GDNF where rs2075680 C4A SNP islocated on is not a known promoter for GDNF. However, thepresence of “TATAAA” box and transcriptional factors binding sites(C/EBP beta, GR-beta, GR-alpha, Pax-5 and ER-alpha), and alsolocation of the region upstream of the GDNF suggest that thisregion may be a potential regulatory site for GDNF. Despite the factthat we did not find any evidence in the literature on thecontrolling of GDNF by glucocorticoid receptors (GRs), wehypothesized that rs2075680 C4A SNP interaction with GR-alpha or GR-beta could be responsible to control the expressionof GDNF (Tronche et al., 1999).
We observed only one variation, rs142426358 T4C SNP, at mi-RNAs homology sequences sites of 30UTR of GDNF. rs142426358T4C SNP was shown at the chromosome location with homologysequence for hsa-mir-216a. This is the first study reportingrs142426358 T4C SNP in bipolar disorder. Although this site hasbeen reported to have homology for micro-RNA has-mir-216asequence, we can find no target of has-mir-216a on GDNF. Furtherin vitro and in vivo investigations are needed to clarify if GDNF isregulated post-transcriptionally by hsa-mir-216a.
Early and late onset bipolar disorders differ in clinical expres-sion and familial risk and may therefore be considered to be
Table 4GDNF rs2075680 C4A SNP over-represented in healthy volunteers compared to patients.
Groups Allele C (freq) Allele A (freq) Odds ratio p value Genotype C/C (freq) Genotype C/A (freq) Genotype A/A (freq) p value
Total BD patients 119(0.902) 13(0.098) 2.11* 0.045 53(0.803) 13(0.197) 0(0.000) 0.089Healthy volunteers 91(0.812) 21(0.188) 38(0.679) 15(0.268) 3(0.054)
Male BD patients 54(0.931) 4(0.069) 3.55** 0.034 25(0.862) 4(0.138) 0(0.000) 0.110Healthy volunteers 38(0.792) 10(0.208) 15(0.625) 8(0.333) 1(0.042)
Female BD patients 65(0.878) 9(0.122) 1.49*** 0.403 28(0.757) 9(0.243) 0(0.000) 0.302Healthy volunteers 53(0.828) 11(0.172) 23(0.719) 7(0.219) 2(0.062)
n %95 CI¼[1.004248–4.443470], χ2¼4.003, df¼1. Hardy–Weinberg equilibrium test for case: χ2¼0.787, df¼1, Fisher's p¼0.374, Pearson's p¼0.374. Hardy–Weinbergequilibrium test for control: χ2¼0.818, df¼1, Fisher's p¼0.365, Pearson's p¼0.365684
nn %95 CI¼[1.036766–12.173618], χ2¼4.450, df¼1. Hardy–Weinberg equilibrium test for case: χ2¼0.159, df¼1, Fisher's p¼0.689, Pearson's p¼0.689. Hardy–Weinbergequilibrium test for control: χ2¼0.002, df¼1, Fisher's p¼0.958, Pearson's p¼0.958.
nnn %95 CI¼[0.578135–3.886390], χ2¼0.699, df¼1. Hardy–Weinberg equilibrium test for case: χ2¼0.709, df¼1, Fisher's p¼0.399, Pearson's p¼0.399. Hardy–Weinbergequilibrium test for control: χ2¼1.715, df¼1, Fisher's p¼0.190, Pearson's p¼0.190.
Table 5Genotype frequency for rs62360370 G4A SNP is seen more frequently in male healthy volunteers compared to male patients.
Groups Allele G (freq) Allele A (freq) Odds ratio p value Genotype G/G (freq) Genotype G/A (freq) p value
Total BD patients 126(0.955) 6(0.045) 2.52n 0.06 60(0.909) 6(0.091) 0.05Healthy volunteers 100(0.893) 12(0.107) 44(0.786) 12(0.214)
Male BD patients 55(0.948) 3(0.052) 3.66nn 0.05 26(0.897) 3(0.103) 0.04nnn
Healthy volunteers 40(0.833) 8(0.167) 16(0.667) 8(0.333)
Female BD patients 71(0.959) 3(0.041) 1.57nnnn 0.83 34(0.919) 3(0.081) 0.54Healthy volunteers 60(0.938) 4(0.062) 28(0.875) 4(0.125)
n %95 CI¼[0.913668–6.950444], χ2¼3.374, df¼1. Hardy–Weinberg equilibrium test for case: χ2>¼0.149, df¼1, Fisher's p¼0.698, Pearson's p¼0.698. Hardy–Weinbergequilibrium test for control: χ2¼0.806, df¼1, Fisher's p¼ is 0.369, Pearson's p¼0.369.
nn %95 CI¼[0.957055–14.982262] χ2¼3.730, df¼1.nnn Odds ratio¼4.33%95 CI¼[1.000531–18.0767809], χ2¼4.2195,df¼1. Hardy–Weinberg equilibrium test for case: χ2¼0.066, df¼1, Fisher's p¼0.797, Pearson's p¼0.797.
Hardy–Weinberg equilibrium test for control: χ2¼0.742, df¼1, Fisher's p¼0.388, Pearson's p¼0.388.nnnn %95 CI¼[0.339627�7.329760], χ2¼0.343, df¼1. Hardy–Weinberg equilibrium test for case: χ2¼0.066, df¼1, Fisher's p¼0.797, Pearson's p¼0.797. Hardy–Weinberg
equilibrium test for control: χ2¼0.142, df¼1, Fisher's p¼0.706, Pearson's p ¼0.701.
R. Safari et al. / Journal of Affective Disorders 167 (2014) 244–250248

different sub-forms of bipolar disorder (Geoffroy et al., 2013;Schurhoff et al., 2000). Significantly decreased GDNF blood levelsin older, but not younger depressive patients were reported in arecent study (Tseng et al., 2013). This study also showed that GDNFlevels are not statistically associated with age of illness onset. Wefound rs142426358 T4C SNP in only one bipolar patient with anearly illness onset. Reversely rs78613670 was observed in twopatients with late age at of illness onset. There is evidencedemonstrating genetic association of ADRB2 (beta-2adrenorecep-tor) gene region and COMT rs4680 G/A polymorphism with theearly onset form of psychiatric disorders (Dizier et al., 2012;Massat et al., 2011). However, this is the first study reporting onrs142426358 T4C SNP in early onset bipolar disorder patients.
Recent studies showed alteration in the expression of GDNF inbipolar disorder patients (Barbosa et al., 2011; Rosa et al., 2006;Zhang et al., 2010). However there is no supporting report to showany SNPs in GDNF gene to control this alteration in bipolardisorder. One case control designed study that examined twointronic SNPs in GDNF showed no significant differences in thegenotype distribution of BD or MDD versus control patients(Kotyuk et al., 2013). Our result also does not show any strongassociation between SNPs in potentially regulated part of GDNFand bipolar disorder. Considering multifactorial and polygeniccharacter of bipolar disorder the findings point at a need forstudying epigenetic alterations together with genetic alterations toclarify the effect of environmental factors and stress as well asgene–gene interactions in the pathogenesis of bipolar disorder.
Despite absence of statistical significance, over-representationof rs2075680 C4A and rs62360370 G4A SNPs in healthy volun-teers compared to bipolar disorder patients, may point at apossible protective role of these SNPs for bipolar disorder.The significant association between rs2075680 C4A SNP andbipolar disorder that we find in Chi-square test was lost aftermultiple test corrections. In this study we performed sequenceanalysis in 30UTR and 50upstream of the GDNF and found 10 SNPs.Then we set the p-value less than 0.005. It may be argued that thenumber of SNPs tested should be corrected. Also, this findingneeds replication in larger group of patients to assess the associa-tion of GDNF SNPs with bipolar disorder.
Having a relatively small sample size is a limitation of thepresent study. However, the study has several strengths such ashaving no deviations from the Hardy–Weinberg equilibrium for allexamined alterations, inclusion of all Caucasian and clinically wellcharacterized participants.
Our results provide suggestive evidence of a possible associa-tion between bipolar disorder and potentially regulating sites ofGDNF. Further studies are needed to assess whether particularSNPs of this gene are protective and related with gender or age ofonset of bipolar disorder.
Role of funding sourceResearch supported by fund of Dokuz Eylul University with Project number of
2011.KB.SAG.022.
Conflict of interestThere is no conflict of interest.
AcknowledgmentsThe authors would like to thank all patients, patient's family and healthy
volunteers for their participation in this research and all medical staff membersinvolved in diagnosis and sample-collecting.
References
Airaksinen, M.S., Saarma, M., 2002. The GDNF family: signalling, biological func-tions and therapeutic value. Nat. Rev. Neurosci. 3, 383–394.
Andreassi, C., Riccio, A., 2009. To localize or not to localize: mRNA fate is in 30UTRends. Trends Cell Biol. 19, 465–474.
Arnold, L.M., 2003. Gender differences in bipolar disorder. Psychiatr. Clin. NorthAm. 26, 595–620.
Aziz, R., Lorberg, B., Tampi, R.R., 2006. Treatments for late-life bipolar disorder. Am.J. Geriatr. Pharmacother. 4, 347–364.
Baldessarini, R.J., Tondo, L., Vazquez, G.H., Undurraga, J., Bolzani, L., Yildiz, A.,Khalsa, H.M., Lai, M., Lepri, B., Lolich, M., Maffei, P.M., Salvatore, P., Faedda, G.L.,Vieta, E., Tohen, M., 2012. Age at onset versus family history and clinicaloutcomes in 1665 international bipolar-I disorder patients. World Psychiatry11, 40–46.
Barbosa, I.G., Huguet, R.B., Sousa, L.P., Abreu, M.N., Rocha, N.P., Bauer, M.E., Carvalho,L.A., Teixeira, A.L., 2011. Circulating levels of GDNF in bipolar disorder. Neurosci.Lett. 502, 103–106.
Barnett, J.H., Smoller, J.W., 2009. The genetics of bipolar disorder. Neuroscience 164,331–343.
Benn, S.C., Woolf, C.J., 2004. Adult neuron survival strategies – slamming on thebrakes. Nat. Rev. Neurosci. 5, 686–700.
Craddock, N., Sklar, P., 2013. Genetics of bipolar disorder. Lancet 381, 1654–1662.Daban, C., Colom, F., Sanchez-Moreno, J., Garcia-Amador, M., Vieta, E., 2006. Clinical
correlates of first-episode polarity in bipolar disorder. Compr. Psychiatry 47,433–437.
Diflorio, A., Jones, I., 2010. Is sex important? Gender differences in bipolar disorder.Int. Rev. Psychiatry 22, 437–452.
Dizier, M.H., Etain, B., Lajnef, M., Lathrop, M., Grozeva, D., Craddock, N., Henry, C.,Gard, S., Jamain, S., Leboyer, M., Bellivier, F., Mathieu, F., 2012. Geneticheterogeneity according to age at onset in bipolar disorder: a combinedpositional cloning and candidate gene approach. Am. J. Med. Genet. B:Neuropsychiatr. Genet. 159B, 653–659.
Fagiolini, A., Goracci, A., 2009. The effects of undertreated chronic medical illnessesin patients with severe mental disorders. J. Clin .Psychiatry 70 (Suppl 3),S22–S29.
Farre, D., Roset, R., Huerta, M., Adsuara, J.E., Rosello, L., Alba, M.M., Messeguer, X.,2003. Identification of patterns in biological sequences at the ALGGEN server:PROMO and MALGEN. Nucleic Acids Res. 31, 3651–3653.
Fiedorowicz, J.G., Palagummi, N.M., Forman-Hoffman, V.L., Miller, D.D., Haynes, W.G., 2008. Elevated prevalence of obesity, metabolic syndrome, and cardiovas-cular risk factors in bipolar disorder. Ann. Clin. Psychiatry 20, 131–137.
First, M.B., Spitzer, R.L., Gibbon, M., 2002. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version. Biometrics Research, New York StatePsychiatric Institute, New York.
Geoffroy, P.A., Etain, B., Scott, J., Henry, C., Jamain, S., Leboyer, M., Bellivier, F., 2013.Reconsideration of bipolar disorder as a developmental disorder: importance ofthe time of onset. J. Physiol. (Paris) 107, 278–285.
Goldberg, J.F., Harrow, M., 2004. Consistency of remission and outcome in bipolarand unipolar mood disorders: a 10-year prospective follow-up. J. Affect. Disord.81, 123–131.
Griffiths-Jones, S., 2004. The microRNA registry. Nucleic Acids Res. 32, D109–111.Griffiths-Jones, S., Grocock, R.J., van Dongen, S., Bateman, A., Enright, A.J., 2006.
miRBase: microRNA sequences, targets and gene nomenclature. Nucleic AcidsRes. 34, D140–144.
Griffiths-Jones, S., Saini, H.K., van Dongen, S., Enright, A.J., 2008. miRBase: tools formicroRNA genomics. Nucleic Acids Res. 36, D154–158.
Hirschfeld, R.M., Vornik, L.A., 2005. Bipolar disorder – costs and comorbidity. Am. J.Manag. Care 11, S85–90.
Kemp, D.E., Sylvia, L.G., Calabrese, J.R., Nierenberg, A.A., Thase, M.E., Reilly-Harrington, N.A., Ostacher, M.J., Leon, A.C., Ketter, T.A., Friedman, E.S., Bowden,C.L., Rabideau, D.J., Pencina, M., Iosifescu, D.V., 2014. General medical burden inbipolar disorder: findings from the LiTMUS comparative effectiveness trial. ActaPsychiatr. Scand. 129, 24–34.
Kennedy, N., Boydell, J., Kalidindi, S., Fearon, P., Jones, P.B., van Os, J., Murray, R.M.,2005. Gender differences in incidence and age at onset of mania and bipolardisorder over a 35-year period in Camberwell, England. Am. J. Psychiatry 162,257–262.
Kessler, R.C., Berglund, P., Demler, O., Jin, R., Merikangas, K.R., Walters, E.E., 2005.Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in theNational Comorbidity Survey Replication. Arch. Gen. Psychiatry 62, 593–602.
Kotyuk, E., Nemeth, N., Halmai, Z., Faludi, G., Sasvari-Szekely, M., Szekely, A., 2013.Association between mood characteristics and polymorphisms of glial cell line-derived neurotrophic factor (GNDF) in patients with depression. Neuropsycho-pharmacol. Hung. 15, 63–72.
Kozomara, A., Griffiths-Jones, S., 2011. miRBase: integrating microRNA annotationand deep-sequencing data. Nucleic Acids Res. 39, D152–157.
Ledda, F., Paratcha, G., Sandoval-Guzman, T., Ibanez, C.F., 2007. GDNF and GFRal-pha1 promote formation of neuronal synapses by ligand-induced cell adhesion.Nat. Neurosci. 10, 293–300.
Lin, L.F., Doherty, D.H., Lile, J.D., Bektesh, S., Collins, F., 1993. GDNF: a glial cell line-derived neurotrophic factor for midbrain dopaminergic neurons. Science 260,1130–1132.
Maragkakis, M., Alexiou, P., Papadopoulos, G.L., Reczko, M., Dalamagas, T., Gianno-poulos, G., Goumas, G., Koukis, E., Kourtis, K., Simossis, V.A., Sethupathy, P.,
R. Safari et al. / Journal of Affective Disorders 167 (2014) 244–250 249
Vergoulis, X., Koziris, N., Sellis, T., Tsanakas, P., Hatzigeorgiou, A.G., 2009.Accurate microRNA target prediction correlates with protein repression levels.BMC Bioinf. 10, 295.
Massat, I., Kocabas, N.A., Crisafulli, C., Chiesa, A., Calati, R., Linotte, S., Kasper, S.,Fink, M., Antonijevic, I., Forray, C., Snyder, L., Bollen, J., Zohar, J., De Ronchi, D.,Souery, D., Serretti, A., Mendlewicz, J., 2011. COMT and age at onset in mooddisorders: a replication and extension study. Neurosci. Lett. 498, 218–221.
Maston, G.A., Evans, S.K., Green, M.R., 2006. Transcriptional regulatory elements inthe human genome. Annu. Rev. Genomics Hum. Genet. 7, 29–59.
McIntyre, R.S., Nguyen, H.T., Soczynska, J.K., Lourenco, M.T., Woldeyohannes, H.O.,Konarski, J.Z., 2008. Medical and substance-related comorbidity in bipolardisorder: translational research and treatment opportunities. Dialogues Clin.Neurosci. 10, 203–213.
Merikangas, K.R., Akiskal, H.S., Angst, J., Greenberg, P.E., Hirschfeld, R.M., Petukhova,M., Kessler, R.C., 2007. Lifetime and 12-month prevalence of bipolar spectrumdisorder in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry64, 543–552.
Messeguer, X., Escudero, R., Farre, D., Nunez, O., Martinez, J., Alba, M.M., 2002.PROMO: detection of known transcription regulatory elements using species-tailored searches. Bioinformatics 18, 333–334.
Nibuya, M., Takahashi, M., Russell, D.S., Duman, R.S., 1999. Repeated stress increasescatalytic TrkB mRNA in rat hippocampus. Neurosci. Lett. 267, 81–84.
Otsuki, K., Uchida, S., Watanuki, T., Wakabayashi, Y., Fujimoto, M., Matsubara, T.,Funato, H., Watanabe, Y., 2008. Altered expression of neurotrophic factors inpatients with major depression. J. Psychiatr. Res. 42, 1145–1153.
Rosa, A.R., Frey, B.N., Andreazza, A.C., Cereser, K.M., Cunha, A.B., Quevedo, J., Santin, A.,Gottfried, C., Goncalves, C.A., Vieta, E., Kapczinski, F., 2006. Increased serum glialcell line-derived neurotrophic factor immunocontent duringmanic and depressiveepisodes in individuals with bipolar disorder. Neurosci. Lett. 407, 146–150.
Roy-Byrne, P., Post, R.M., Uhde, T.W., Porcu, T., Davis, D., 1985. The longitudinalcourse of recurrent affective illness: life chart data from research patients at theNIMH. Acta Psychiatr. Scand. 317, 1–34 (Suppl).
Rozen, S., Skaletsky, H., 2000. Primer3 on the WWW for general users and forbiologist programmers. Methods Mol. Biol. 132, 365–386.
Sachs, G.S., Baldassano, C.F., Truman, C.J., Guille, C., 2000. Comorbidity of attentiondeficit hyperactivity disorder with early- and late-onset bipolar disorder. Am. J.Psychiatry 157, 466–468.
Sariola, H., Saarma, M., 2003. Novel functions and signalling pathways for GDNF. J.Cell Sci. 116, 3855–3862.
Schurhoff, F., Bellivier, F., Jouvent, R., Mouren-Simeoni, M.C., Bouvard, M., Allilaire, J.F., Leboyer, M., 2000. Early and late onset bipolar disorders: two different formsof manic-depressive illness? J. Affect. Disord. 58, 215–221.
Shi, Y.Y., He, L., 2005. SHEsis, a powerful software platform for analyses of linkagedisequilibrium, haplotype construction, and genetic association at polymorph-ism loci. Cell Res. 15, 97–98.
Tronche, F., Kellendonk, C., Kretz, O., Gass, P., Anlag, K., Orban, P.C., Bock, R., Klein, R.,Schutz, G., 1999. Disruption of the glucocorticoid receptor gene in the nervoussystem results in reduced anxiety. Nat. Genet. 23, 99–103.
Tseng, P.T., Lee, Y., Lin, P.Y., 2013. Age-associated decrease in serum glial cell line-derived neurotrophic factor levels in patients with major depressive disorder.Prog. Neuropsychopharmacol. Biol. Psychiatry 40, 334–339.
Wang, H.J., Cao, J.P., Yu, J.K., Zhang, L.C., Jiang, Z.J., Gao, D.S., 2008. Calbindin-D28Kexpression induced by glial cell line-derived neurotrophic factor in substantianigra neurons dependent on PI3K/Akt/NF-kappaB signaling pathway. Eur. J.Pharmacol. 595, 7–12.
Young, A.H., Grunze, H., 2013. Physical health of patients with bipolar disorder. ActaPsychiatr. Scand. 442, 3–10 (Suppl).
Zhang, X., Zhang, Z., Sha, W., Xie, C., Xi, G., Zhou, H., Zhang, Y., 2010. Effect oftreatment on serum glial cell line-derived neurotrophic factor in bipolarpatients. J. Affect. Disord. 126, 326–329.
R. Safari et al. / Journal of Affective Disorders 167 (2014) 244–250250