Embed Size (px)
Citation preview

N E O N A T A L N E T W O R KV O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 © 2 0 1 1 S p r i n g e r P u b l i s h i n g C o m p a n y 3 8 1 h t t p : / / d x . d o i . o r g / 1 0 . 1 8 9 1 / 0 7 3 0 – 0 8 3 2 . 3 0 . 6 . 3 8 1
Accepted for publication May 2011.
Neutral Head Positioning in Premature Infants for Intraventricular
Hemorrhage Prevention: An Evidence-Based Review
Sheila Malusky, DNP, RN, NNP-BC Ann Donze, MSN, RN, NNP-BC
In the UnIted StAteS eAch yeAr, ApproxIMAtely 57,000 infants are born prematurely. With the advancement of
neonatal medicine during the past several decades, including improved methods of mechani-cal ventilation and the devel-opment of tota l parentera l nutrition (tpn) for neonates, even extremely low birth weight (elBW) infants are now living longer and surviving.1 of these infants, 20–25 percent of them will develop an intraventricular hemorrhage (IVh),2 with the incidence being inversely pro-portional to gestational age.3
the total financial cost that is estimated for these premature births is $26 billion or $51,600 for each individual prema-ture birth. these costs include medical care, delivery costs, early intervention services, educational services, and lost family income.4 Additionally, the average cost of an IVh adds another $53,600 to the cost of the initial hospi-talization.5 But the costs of IVh go far beyond the impact of the
injury in the individual and the financial burden to care for these babies. the impact can also be devastating to the family
who has the responsibility of caring for a disabled child. the lifelong commitments to care for these individuals tax the family structure, family resiliency, and bring about the additional need for community support.
there has been a multitude of research into the prevention of IVh in premature infants.6 Some of these studies examine prenatal factors such as antenatal steroid use.7 other studies have focused on antenatal factors such as delivery room resuscitation methods.8 Still other studies have focused on neonatal preven-tion methods such as pharmaco-logic interventions and neonatal care management methods.9
one neonatal care manage-ment activity that has been examined in association with IVh prevention is infant head positioning. First studied in adult patients, cerebral blood flow changes in response to head position were also examined in
neonates beginning in the 1980s.10–12
the purpose of this article is to review current evidence on midline head positioning in the prevention of IVh. the goal
AbstrAct
With the advancement of neonatal medicine during the past several decades, premature and critically ill infants are living past the neonatal period and surviving. the survival of these infants at smaller birth weights and younger gestational ages puts them at an increased risk for intraventricular hemorrhages (IVhs). Although shifts in cerebral perfusion have been linked to the development of these brain bleeds, many seemingly benign care activities have been linked to changes in cerebral blood flow patterns, possibly contributing to IVhs. the purpose of this article is to evaluate the current evidence to determine if the practice of midline positioning for infants born less than 32 weeks gestation for possible IVh prevention is supported by the literature. Many of the researchers involved in these studies attributed the consequential venule leakage of blood to occlusion of the jugular venous drainage system following a turn in the position of the head. Additionally, the articles that examined the connection between the effects of head tilting on brain hemodynamics attributed changes on the infants’ potential inability to autoregulate cerebral blood flow adequately. Both of these findings were linked to the development of IVhs. Based on physiologic data and expert opinion, the authors found support in the literature and recommend implementing a plan of care that includes midline head positioning for premature infants.
DisclosureThe author discloses no relevant financial interest or affiliations with any commercial interests.

3 8 2 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
of this review was to answer the clinical practice question: In infants born at ,32 weeks gestation, does midline head positioning along with head of bed tilted upward for the first 72 hours of life, when compared with standard posi-tioning, result in a lower incidence of IVH?
ETIOLOGY AND PATHOPHYSIOLOGY OF INTRAVENTRICULAR HEMORRHAGE
Although this potentially devastating medical condition can occur at any age, premature infants are at an increased risk because of their immature brain vasculature and also their inability to autoregulate shifts in cerebral perfusion, described as a pressure-passive circulatory state.13,14 Of the bleeds that occur, 90 percent will develop during the first 72 hours of life, a time when these infants are in their most critically ill state.3 Although extreme prematurity and illness have been associ-ated with shifts in brain perfusion, many seemingly benign care activities and environmental factors have also been shown to cause changes in cerebral blood flow patterns.2,13–16
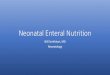
Although there are many risk factors associated with the development of an IVH, some of which are noted in Table 1, one of the most prominent risks is prematurity.3,17 This increased risk is caused by the presence of the germinal matrix, a network of delicate blood vessels within the pre-mature brain that usually involutes between 32 weeks and term gestation.3 Within this region, the capillary–venule juncture is the originating site of these hemorrhages.3 The fragile blood vessels within the germinal matrix are easily ruptured with any rapid changes in the levels of cerebral perfusion, which may lead to bleeding into the brain tissue or ventricles.18 The structure of the venous system in this area of the brain can also lead to IVH because the system has a U-shaped vessel pattern prone to venous congestion near the germinal matrix, again causing vessel damage and bleeding. A cranial ultrasound view of a neonate without IVH can be seen in Figure 1, whereas Figure 2 shows a drawing of the U-shaped vascular anatomy.
A factor unique to this population is the inability of premature infants to autoregulate cerebral perfusion in response to physi-ologic and positional changes.13 Autoregulation is the ability of the body to maintain a constant blood flow to the brain despite cerebral perfusion.19 Inconsistencies in cerebral blood flow pat-terns have been observed during routine critical care of the premature infant.16 Impaired autoregulation can be markedly pronounced in infants who are sick or extremely premature.14,20
The mechanism of action that has been postulated is that during head rotation to the side, an occlusion or obstruction of the jugular venous–venule drainage system could occur on the ipsilateral side of the head. This is followed by increased venous congestion in this area leading to vessel rupture.
Figure 1 n Cranial ultrasound of a neonate without IVH.
TABLe 1 n Associated Risk Factors for IVH
Antenatal Risk Factors
Prematurity
Maternal infection
Maternal inflammatory responses
Maternal hypertention
Maternal bleeding disorders
Absent maternal steroid administration maternal diabetes
Placental insertion disorders
Oligohydramnios
Maternal alcohol use
Maternal smoking
Poor prenatal care
Infertility treatments
Out-born delivery and neonatal transport
Initial resuscitation efforts
Asynchronous ventilatory support
High continuous airway pressure
Rapid fluid administration
Rapid alteration in blood pressure
Hypotension
Hypocarbia or hypercarbia
Pneumothorax
Asphyxia
Hypernatremia
Hypoglycemia
Thrombocytopenia
Patent ductus arteriosis
Seizure activity
Routine NICU care: Tracheal suctioning, excessive handling, noxious stimulation, painful procedures, stress
Any disease process or care activity associated with alteration in cerebral perfusion.

V O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 3 8 3N E O N A T A L N E T W O R K
By maintaining a neutral head position, it is theorized that venous obstruction could possibly be avoided, potentially preventing IVH caused by head position.
INTRAVENTRICULAR HEMORRHAGE SEVERITY AND OUTCOMES
Diagnosed by cranial ultrasound, an IVH can occur fol-lowing serious illness of the infant or after no apparent insult at all. During the first four to five days of life, a time when premature infants are in their most critical state, 95 percent of all cases of IVH will develop.21 Depending on the severity, some of these bleeds may be accompanied by an acute deteri-oration in clinical status, whereas some infants may show few symptoms until they reach school age.22 Overall, Paige and Carney found the associated sequelae of IVH to range from minimally distinguishable effects (50 percent), to abnormal neurologic outcomes (20–30 percent), to an increase in inci-dence of mortality (10–30 percent).22
Although the IVH has been broken down into classifica-tions by grade, Volpe later developed an IVH labeling system based on a description of the neurologic pathology.3,23,24 This was caused by some abnormalities that can occur that do not fit into the original classifications. Such cases could include isolated ventriculomegaly or instances of white matter injury that are not associated with IVH.25 Volpe also advocated for the cessation of labeling white matter brain tissue hemorrhages, or parenchymal hemorrhages, Grade IV IVH.3 This was caused by the origination of these bleeds, at times, occurring secondary to parenchymal infarction and not always being associated with bleeding within the ventricles.25
The Papile IVH grading system also does not describe the site of origin for the IVH.25 Most often, intracranial hemorrhages in premature infants originate in the germinal matrix, a highly vascular and fragile region in the premature infant’s brain. Alternately, the choroid plexus can also be
an origination site, although this is more common in term infants.25,26 Regardless of site of origination or description of pathology, many bleeds are now being associated with the level of neurodevelopmental outcomes risk.25 Low-grade risk bleeds are associated with Grade I and II hemorrhages. High-grade risk bleeds are associated with Grades III and IV hemorrhages. See Table 2 for a description of IVHs and statistics for very low birth weight (VLBW [,1,500 g]) infants.
Because an IVH can be such a devastating event, there is a critical need to identify strategies to reduce IVH in this pop-ulation. One proposed strategy is the use of midline position-ing during the first 72 hours of life, a time when 90 percent of all IVH occur.3
DEVELOPING THE CLINICAL PRACTICE QUESTION USING PICO FORMAT
When completing an evidence-based review of the liter-ature, developing a question that helps focus the literature search is the first step. PICO is a mnemonic term used to focus and describe each part of the clinical practice question: “P” is the population, “I” is the intervention, “C” is the comparison group, and “O” is the outcome.33
The PICO question focuses on an intervention that is compared to the current standard of care. If there is evi-dence that an intervention may provide benef it without harm, an intervention may be implemented into practice. The PICO or clinical practice question that prompted this search was:
“Do infants born at ,32 weeks gestation who are posi-tioned with head in midline position and head of bed tilted upward for the first 72 hours of life have a lower incidence of IVH than infants who receive standard positioning?” P 5 In infants born at ,32 weeks gestation I 5 does midline head positioning along with the head of
bed tilted upward for the first 72 hours of life C 5 compared with standard positioning O 5 result in a lower incidence of IVH
LITERATURE SEARCH STRATEGIESA literature search using the keywords intracranial hem-
orrhages, cerebral ventricles, infant, and newborn was per-formed using Medline, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Google Scholar. The search years were limited from 1980 to 2010. On the first search, 935 articles were found. The search was then limited to articles in English, human subjects, and infants from birth to 23 months of age. This search yielded 800 articles. The search was then altered to infant, premature, and cerebral ventricles and hemorrhage with the same limi-tations of English, human subjects, and infants from birth to 23 months of age. The reason that older research was admitted into this search is that this early time represents the initial study into IVH and premature infants. Many of the positioning studies were conducted during the 1980s
Figure 2 n U-shaped vascular anatomy.
Medullary veins
Choroidal vein
Thalamostriatevein
Vein of Golen
Terminalvein
Internalcerebral vein

3 8 4 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
and have not been repeated. The search then yielded 189 articles. When the term prevention was added to the search, 77 articles were found that most appropriately fit the clinical question.
Following this, a search of the Cochrane Systematic Review Database was completed. Although many reviews on IVH prevention were present, the reviews focused on the medical management of IVH, such as medication administration. There was one review regarding devel-opmental care and the prevention of morbidities, but no
systematic review of nursing care activities or positioning was found.34
Of the 77 articles reviewed, organization of the rest of the review consists of an evaluation of 11 articles. These articles most appropriately answered the review question regarding positioning the premature infant and IVH prevention. The other 66 articles that were discarded did not address research relating to positioning and IVH occurrence in the premature neonate. The following discussion synthesizes the evidence collected.
Table 2 n Intraventricular Hemorrhages
Papile’s Classification by Severity
Volpe’s Classification: Description by Pathology
Occurrence Rate
Morbidity and Neurologic Outcomes
Mortality Progression of Ventricular Dilatation
Grade I: least severe mild IVH
See Figure 3
Subependymal hemorrhage (SEH)—also called germinal matrix hemorrhage (GMH)
25%–30% for Grades I–II27
Ten percent motor disability. This rate is comparable to premature infants without documented hemorrhage.24
5%3 4%28
Grade II: considered mild-to-moderate IVH
See Figure 4
Intraventricular hemorrhage (IVH)—alternately called a SEH with progression into the lateral ventricles by ,50% without dilatation.
Most infants with Grade II IVH face the same neurologic outcomes associated with Grade I IVH, although the extent of bleed can lead to ventricular dilatation.18 Patra et al. found significantly poorer neurodevelopmental outcomes in extremely low birth weight (ELBW) infants (,1,000 g) with Grades I–II IVH at 20 months corrected age. This includes up to 15% of these ELBW infants with Grades I–II IVH who develop cerebral palsy (CP) and 9% who develop deafness.27
10%3 12%28
Grade III: considered moderate-to-severe IVH
IVH with ventricular dilatation—SEH with progression into the lateral ventricles by .50% and/or with dilatation of ventricles.
10%–12% for Grades III–IV29
Ventricular dilatation can result when blood blocks the cerebrospinal fluid pathway, leading to progressive ventricular dilatation and increased intracranial pressure. The morbidity related to posthemorrhagic hydrocephalus is significant, with up to 90% of these infants having some degree of neuromotor deficits and 25% with visual and auditory impairments.30 In total, 76% of these infants will have pronounced disability and 56% have multiple impairments.28 Fifty percent of these children will require some special education and enrichment programs.24
20%3 74%28
Grade IV: considered severe IVH
See Figure 5
Intraparenchymal hemorrhage (IPH)—hemorrhagic infarct into the white brain matter
Generally unilateral with the prognosis most often associated with poor motor deficits as well as significant cognitive impairments.24 Classified as the most severe IVH, many infants do not survive.
50%3 71%28
Periventricular leukomalacia (PVL)— parenchymal, or white brain matter, necrosis often occurring following Grade IV IVH or a parenchymal infarct.
Ten percent very low birth weight (VLBW) infants with PVL will develop CP with spastic diplegia and 50% will develop cognitive and behavioral deficits.31,32

V O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 3 8 5N E O N A T A L N E T W O R K
Figure 3 n Ultrasound of Grade I IVH.
Figure 4 n Ultrasound of Grade II IVH.
Figure 5 n Ultrasound of Grade IV IVH.

3 8 6 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
SYNTHESIS AND SUMMARYDetails of all appraised studies can be found in the Appendix.
The Five Strengths of Evidence35
Type 1: strong evidence from at least one systematic review of multiple, well-designed randomized, controlled trials.
Type 2: strong evidence from at least one properly designed randomized, controlled trial of appropriate size.
Type 3: evidence from well-designed trials without random-ization, single group pre–post, cohort, time series, or matched case-control studies.
Type 4: evidence from well-designed, nonexperimental studies from more than one center or research group.
Type 5: opinions of respected authorities (based on clinical evi-dence), descriptive studies, or reports of expert committees.
There was no meta-analysis or randomized controlled trials. The studies included nine predesigns and postdesigns, two repeated measures design, and one expert review panel report. One of the studies used both a premethodology and postmethodology as well as a repeated measure design, total-ing 11 reviewed articles.36
When synthesizing the evidence gathered regarding the positioning of premature infants and the potential effects of these positions on cerebral hemodynamics, the information gathered was analyzed following the PICO format. The purpose of this analysis was to determine whether the studies reviewed were homogenous. This is an important step in evaluating whether the study simi-larities lend to the pooling of evidence that may support a practice change.
First, did all of the studies ask the same question? Not all of them. Although the articles were included in the review because of similar subject matter, the focus of some of these articles was not exactly homogenous. Eight of the articles studied changes in cerebral hemodynamic and two studied changes in intracranial pressure (ICP) in response to position changes. The final article gave expert opinion about infant positioning after benchmarking hospitals with low IVH rates.
Next, the articles were examined to determine the homoge-neity of the “P,” or population. Of the articles reviewed, nine studies examined preterm infants. A tenth article that exam-ined full-term infants was also included because this study is often cited as a seminal article that examines changes in neo-natal cerebral hemodynamic in response to position change.11
Of the articles examined, there was a wide variation in ges-tational age, weight, postnatal age, and level of illness. These infants ranged from the most premature and critically ill infants to infants who were described by the authors as healthy pre-mature infants. Because of the profoundly wide variation in levels of health and gestational age of the subjects, comparing outcomes for infants in this review was difficult. Additionally, none of these studies strictly examined the neonates during their first 72 hours of life, a time when most IVHs occur.32
Next, the articles were examined to determine the homoge-neity of the “I,” or interventions. The interventions reported
for these studies centered on positioning or altering position of the newborn infant. Some of these articles focused on the effects of midline head positioning, whereas others looked at the effects of changes in the tilting position. Regardless of particular position change that each individual study exam-ined, they all evaluated changes in cerebral hemodynamics or ICP in response to position change.
Following the positioning interventions, an evaluation of cerebral blood flow or ICP was assessed. There were various instruments used to assess these measures. In the 10 articles with patient enrollment, 5 used near infrared spectroscopy (NIRS), 4 used ultrasound, and 2 used a transfontanel pres-sure transducer. The transfontanel pressure transducers were used in the first studies, followed by the use of ultrasound, and then NIRS methodology because technology has pro-gressed. A brief description of the instrumentation used for the evaluations is listed in Table 3.
The articles were then examined to determine the homoge-neity of the “O,” or outcomes. When evaluating the outcomes reported in these studies, the groups could be separated into two divisions: those that evaluated the effects of head or body position changes and those that evaluated the effects of tilting. In those that evaluated head and body changes, several outcome measures were used and not all assessed the incidence of IVH, making the evaluation of the intervention difficult.
In general, these articles demonstrated alterations in cere-bral blood flow following position changes. One study found a significant decrease in tissue hemoglobin index and tissue oxygen index during head rotation in infants ,26 weeks ges-tation.37 A second study found a significant increase in cerebral blood volume (CBV) during 90-degree head rotation, which was pronounced in infants ,1,200 g.38 The third study found cerebral blood flow velocities were significantly higher in the
TABLE 3 n Definition of Study Instruments
Ultrasonography A non-invasive radiological exam that uses a transducer to pass sound waves through soft tissue and fluid. A picture is produced when the returning echo bounces off internal structures and returns to the transducer. The resulting picture is formed when the data entered into the transducer is read by the ultrasound computer and is analyzed to produce real-time images.44
Trans-fontanel Pressure Transducer
A non-invasive device that measures intracranial pressure through a probe secured over the anterior fontanel.10
Near Infrared Spectroscopy (NIRS)
A non-invasive neuro-imaging device that uses near-infrared light to evaluate real-time tissue oxygen and blood volume to interpret blood hemodynamics of the brain.43

V O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 3 8 7N E O N A T A L N E T W O R K
supine position at one month of age during evaluation, and vertebral arterial flows in prone position were decreased.39 A fourth study found jugular blood flow was decreased during 90-degree head rotation.11 The three studies that evaluated ICP all found a significant decrease in ICP, with the head in midline position and the head of the bed elevated.10–12
The second group of studies examined the effects of tilting. These studies evaluated CBV and found a significant increase with the head lowered in a dependent position. These studies also found signif icant alterations in CBV in response to tilting, especially in preterm or brain-injured infants. Another study evaluated for biphasic responses in cerebral blood flow velocities, demonstrating autoregulatory responses in preterm infants, and found significantly more reliable responses were elicited as gestational age increased but IVH outcome was not evaluated.36 A complete description of the findings of these articles can be found in the Appendix.
Although the final article was not a research study, infor-mation from such an article can still be valuable. This article by Carteaux and colleagues detailed the work of a multidis-ciplinary focus group that was formed to complete an evi-dence-based literature review, benchmarking activities, and expert committee review. The purpose of this evaluation was to identify potentially better practices (PBPs) that could lead to the reduction of IVH and periventricular leukomalacia (PVL) in VLBW and premature infants.6
The group identified benchmark NICUs with the lowest incidence of IVH reported to the Vermont Oxford Network (VON). The VON, a consortium of more than 700 NICUs associated with the improvement of safety and quality of newborn care, formed a focus group to evaluate methods for reducing the incidence of IVHs in premature infants.40 It then developed an NICU practice questionnaire for VON sites. Four sites with low incidence of intracranial hemorrhage were iden-tified and used as a benchmark for clinical practice. Specific clinical practices at these sites were described through struc-tured questionnaires and site visits. The information obtained from these sites was analyzed and used to help identify NICU practices that might be related to IVH prevention. A complete literature review was then completed on each of these NICU practices. Following the benchmarking and literature review, the group identified a final list of ten recommended practices for NICUs that were PBPs, which could help with the reduc-tion of incidence of IVH. Use of midline positioning and bed elevation of 30 degrees was identified as PBPs.
DISCUSSIONThe decision to make a practice change should be based
on the grade, quality, and strength of the evidence after synthesizing all data. Of the 11 articles reviewed, 10 of them involved clinical trials. Of these, all were Type 3 evi-dence with a quasi-experimental, nonrandomized conve-nience sample design with five studies including a control group. All of the studies were small and no power analy-sis was commented upon. Many of the studies were older,
and technology and medical practices may have changed. Finally, all nine studies that examined preterm infants would be considered “stable” neonates and may not reflect the group of patients who are at greatest risk for IVH, those who are severely premature during their first 72 hours of life. The final article, based on expert opinion, benchmark-ing, and review of the literature, reviewed multiple practices and their recommendations varied between level, depending on the strength of the evidence.6 The level of evidence for the recommendations on head positioning by VON was IV and VI.6 According to the Muir Gray schema of evidence that was used to rate the evidence, IV is defined as a well-designed, nonexperimental study, and VI is defined as an evidence supported by casual theory of disease.35 Although there are limitations to these 11 studies, they may still, however, provide some benefit to our patient population. Many investigators included discussion about how their study results could be interpreted. The expert opinion of many of the researchers attribute changes in cerebral oxy-genation, increased CBV, and/or increased ICP to occlu-sion of the jugular venous drainage system following a turn in the position of the head. The proposed consequential backup of cerebral blood is an ongoing theme presented by many of the authors, although jugular blood flow was only analyzed in one study.6,11,12,37–39 These authors then specu-late that the risk of IVH was increased because of ruptures in the cerebral venous–venule drainage system following blood accumulation secondary to the occlusion. Although jugular obstruction studies during head rotation have been documented in the adult population, results in the neonatal population are limited and similar results in this population are theorized.11,38 The researchers concluded that venous obstruction caused by head position could be detrimental to these infants who are already at increased risk for IVH.
A second observation that was discussed by the investiga-tors was the connection between the effects of head tilting on brain hemodynamics. Of the four studies that examined tilting, the experts attributed the results, an increase in CBV and/or increased ICP, to the infants’ potential inability to autoregulate cerebral blood flow adequately. Because these findings were sig-nificantly increased in infants with PVL, brain injury, and those who were premature, the authors further speculated these find-ings may put these infants at a greater risk for developing IVH.
All of the methods of measurement used throughout the studies showed a difference in cerebral hemodynamics when positioning was changed. These findings were present in the head rotation studies as well as the tilting ones. These differences were most marked in the ELBW infant. Present studies, unfortunately, only include outcome measures that were short-term and any changes in practice should include long-term outcome measurement.
The investigators who completed the expert review6 did discuss the lack of high-level evidence when evaluating infant positioning.6 The decision to recommend the use of neutral head position was based on the potential benefits of this

3 8 8 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
practice and the lack of harm. Based on these recommenda-tions, many NICUs currently use these positioning practices.
IMPLEMENTATION OF NEUTRAL HEAD POSITIONING
The decision to implement midline/neutral head posi-tioning and a 30-degree elevation in the HB in infants less than 32 weeks gestation for the first 72 hours of life can be recommended, at this point, based on physiologic data and the views of experts in the field. Furthermore, there have not been any adverse consequences identified when implement-ing these positioning changes.
For units considering a change in neonatal positioning practices for potential IVH prevention such as the implemen-tation of neutral head positioning, there are several impor-tant steps to facilitate change. These steps should only occur following critical appraisal of the evidence.
Gather the StakeholdersThe stakeholders incorporated in this practice change
should include registered nurses who care for the infants and understand the fine nuances of caring for the infants. The physicians, advance practice nurses (APNs), and bedside staff nurses would be essential in identifying infants appropriate for this practice change and for ordering this care practice. Physical therapists would be needed to assist with positioning and obtaining positioning devices needed on an individual bases. Respiratory therapists would be important to help posi-tion infants in neutral head positioning while still receiving the necessary respiratory support. Specialized equipment may be needed to positioning these infants midline, especially if the infant is on an oscillating ventilator. Pharmacists input to maintain patient comfort may also be a necessity. Our unit has developed a multidisciplinary IVH prevention taskforce com-prised of representation from all the mentioned stakeholders to evaluate the evidence and provide recommendations.
Create a Detailed Action PlanThe first steps to creating an action plan would be to
use the stakeholders to discuss potential obstructions, plan nursing and medical team education, and plan parent educa-tion. An audit of current positioning practices can help the team assess the degree of change that is being proposed for the unit. This can help the team determine the amount of time this change may require and the amount of support needed to be successful with this change.
Planning to assess outcome measures (IVH rates) prior to the practice change is important in evaluating if the practice change of midline positioning has made a difference in this patient population. Our unit has done this step in the IVH prevention taskforce.
Assessing Environmental ReadinessThe stakeholders must evaluate and address the organi-
zation, environment, and whether it is supportive to this evidence-based practice (EBP) change at this time. The three
areas to assess are organizational culture, organizational infrastructure, and organizational resources.41 In assessing organizational culture, one would assess the values of the unit. Do the caregivers understand the importance of imple-menting evidence-based recommendations? Do the nurses and other caregivers understand the potential benefits and how to achieve neutral head positioning? Does the practice change support family-centered care, an important value to NICU caregivers? Does this practice change support devel-opmental care practices, another important care value in NICUs? Have the team given input in identifying potential barriers to this practice change, including nursing barriers to care and equipment needs?
In assessing organizational infrastructure, one would assess the organization’s willingness to support evidence-based care practice changes. Does the unit have goals that state support of practices based on the most current evidence?41 Has the organization made efforts to hire or train employees in the evidence-based process?
The organizational resource assessment evaluates whether an organization is willing to support the man-hours needed to evaluate the evidence and implement these changes. Can the organization financially support the EBP process, which includes the evaluation, implementation, and assessment phase of this process? Is the organization willing to supply equipment and training time? If the organization cannot give full financial support for the practice change, are they willing to support further planning to identify creative alter-nates that support the evidence?
Use Multiple Implementation StrategiesWhen implementing a practice change, multiple imple-
mentation strategies can help ensure success. Does the education plan include multiple methods to reach the care-giving team, such as demonstrations of midline positioning and posters with pictures? Does the education presentations included multiple levels of medical knowledge, with the dif-ference being parental education being easier to understand for the layperson and the medical education, including a more pathophysiologic approach to address the caregivers under-standing of the rationale for change? When implementing these changes, are there multiple approaches to support the bedside nurses such as the team members available to address technical questions and nursing champions to encourage practice change use through exemplifying the practice?
EVALUATING OUTCOMESProcess Outcomes
Once the practice change has occurred, a method to assess the practice change is essential. Is the practice implemented as designed? Can the caregiving team describe midline posi-tioning and demonstrate this practice change correctly? Is midline positioning being performed routinely? Have the caregiving team identified further barriers to midline posi-tioning as the practice occurs on a routine basis? A quality assurance plan to assess that the practice change is being

V O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 3 8 9N E O N A T A L N E T W O R K
executed regularly and correctly is essential. This is impor-tant because it assesses whether a practice change is truly being carried out as planned. A method to evaluate this could be the formation of “positioning super users” to audit patient positioning and evaluate the need for further educa-tion based on their findings. The identification of barriers and development of solutions to barriers is essential in the success of the implementation of this change.
Clinical OutcomesThe final step in this process is an evaluation of the clini-
cal outcomes. Has this change made an impact? How do the current IVH rates compare with the rates prior to the prac-tice change, as well as the rates of others such as NICUs? Can we follow long-term outcomes such as incidence of cognitive, behavioral, and physical disabilities?
Future DirectionAlthough the cause of IVH in premature infants may be
multifactorial and complicated, many investigators are cur-rently searching for prevention methods. Some neonatal units have adopted IVH prevention bundles or multiple care practice changes that can potentially reduce the incidence of IVH.42 Regardless of whether a unit is looking to make several practice changes or just one change at a time, there is little dispute that work toward a decrease in the incidence of IVH in premature infants should continue.
Additionally, further research into neonatal positioning for IVH prevention should continue. Although the strength of evidence to support this practice change could be stronger, the decision to adopt this practice change should be evalu-ated and discussed in individual neonatal units. The adoption of the practice of midline positioning could still be recom-mended based on its potential benefits.
With the increased survival of extremely premature infants, the incidence of IVH, a common neonatal morbidity, can be expected to rise proportionately. Although research into the prevention of this potentially devastating illness should continue, caregivers must continue to evaluate the litera-ture in evaluation of their current practices. Because IVH can be so devastating to the infant, caregivers must strive to provide evidence-based care that can potentially prevent these occurrences.
REFERENCES1. Committee on Hospital Care, American Academy of Pediatrics. (2003).
Family-centered care and the pediatrician’s role. Pediatrics, 112(3 Pt. 1), 691–697.
2. McCrea, H. J., & Ment, L. R. (2008). The diagnosis, management, and postnatal prevention of intraventricular hemorrhage in the preterm neonate. Clinics in Perinatology, 35(4), 777–792. http://dx.doi.org/10.1016/ j.clp.2008.07.014
3. Volpe, J. J. (2008). Intracranial hemorrhage: Germinal matrix-intraventricular hemorrhage of the premature infant. In Neurology of the newborn (5th ed., pp. 517–588). Philadelphia, PA: Saunders Elsevier.
4. March of Dimes. (2009). About prematurity: The economic costs. Retrieved from http://www.marchofdimes.com/prematurity/21198_10734.asp
5. Russell, R. B., Green, N. S., Steiner, C. A., Meikle, S., Howse, J. L., Poschman, K., . . . Petrini, J. R. (2007). Cost of hospitalization for preterm and low birth weight infants in the United States. Pediatrics, 120(1), e1–e9. http://dx.doi.org/10.1542/peds.2006-2386
6. Carteaux, P., Cohen, H., Check, J., George, J., McKinley, P., Lewis, W., . . . McConnell, C. (2003). Evaluation and development of potentially better practices for the prevention of brain hemorrhage and ischemic brain injury in very low birth weight infants. Pediatrics, 111(4 Pt. 2), e489–e496.
7. Crowley, P. (2000). Prophylactic corticosteroids for preterm births. Cochrane Database of Systematic Reviews, (2), CD000065.
8. Kattwinkel, J., Niermeyer, S., Nadkarni, V., Tibballs, J., Phillips, B., Zideman, D., . . . Osmond, M. (1999). Resuscitation of the newly born infant: An advisory statement from the Pediatric Working Group of the International Liaison Committee on Resuscitation. Resuscitation, 40(2), 71–88.
9. Vohr, B., & Ment, L. (1996). Intraventricular hemorrhage in the preterm infant. Early Human Development, 44(1), 1–16.
10. Emery, J. R., & Peabody, J. L. (1983). Head position affects intracranial pressure in newborn infants. The Journal of Pediatrics, 103(6), 950–953.
11. Cowan, F., & Thoresen, M. (1985). Changes in superior sagittal sinus blood velocities due to postural alterations and pressure on the head of the newborn infant. Pediatrics, 75(6), 1038–1047.
12. Goldberg, R. N., Joshi, A., Moscoso, P., & Castillo, T. (1983). The effect of head position on intracranial pressure in the neonate. Critical Care Medicine, 11(6), 428–430.
13. Owens, R. (2005). Intraventricular hemorrhage in the premature neonate. Neonatal Network, 24(3), 55–71.
14. Perlman, J. M. (2009). The relationship between systemic hemodynamic perturbations and periventricular-intraventricular hemorrhage—A historical perspective. Seminars in Pediatric Neurology, 16(4), 191–199. http://dx.doi.org/10.1016/j.spen.2009.09.006
15. Ballabh, P. (2010). Intraventricular hemorrhage in premature infants: Mechanism of disease. Pediatric Research, 67(1), 1–8.
16. Limperopoulos, C., Gauvreau, K. K., O’Leary, H., Moore, M., Bassan, H., Eichenwald, E. C., . . . du Plessis, A. J. (2008). Cerebral hemodynamic changes during intensive care of preterm infants. Pediatrics, 122(5), e1006–e1013. http://dx.doi.org/10.1542/peds.2008-0768
17. Vergani, P., Locatelli, A., Doria, V., Assi, F., Paterlini, G., Pezzullo, J. C., & Ghidini, A. (2004). Intraventricular hemorrhage and periventricular leukomalacia in preterm infants. Obstetrics and Gynecology, 104(2), 225–231.
18. Bloch, J. R. (2005). Antenatal events causing neonatal brain injury in premature infants. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 34(3), 358–366.
19. Kaiser, J. R., Gauss, C. H., & Williams, D. K. (2005). The effects of hypercapnia on cerebral autoregulation in ventilated very low birth weight infants. Pediatric Research, 58(5), 931–935.
20. Wong, F. Y., Leung, T. S., Austin, T., Wilkinson, M., Meek, J. H., Wyatt, J. S., & Walker, A. M. (2008). Impaired autoregulation in preterm infants identified by using spatially resolved spectroscopy. Pediatrics, 121(3), e604–e611. http://dx.doi.org/10.1542/peds.2007-1487
21. Linder, N., Haskin, O., Levit, O., Klinger, G., Prince, T., Naor, N., . . . Sirota, L. (2003). Risk factors for intraventricular hemorrhage in very low birth weight premature infants: A retrospective case-control study. Pediatrics, 111(5 Pt. 1), e590–e595.
22. Paige, P. L., & Carney, P. R. (2002). Neurological disorders. In G. B. Merenstein & S. L. Gardner (Eds.), Handbook of neonatal intensive care (5th ed., pp. 644–678). St. Louis, MO: Mosby.
23. Papile, L. A., Burstein, J., Burstein, R., & Koffler, H. (1978). Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1,500 gm. The Journal of Pediatrics, 92(4), 529–534.
24. Papile, L. A. (2002). Intracranial hemorrhage. In A. A. Fanaroff & R. J. Martin (Eds.), Neonatal-perinatal medicine: Diseases of the fetus and infant (7th ed., pp. 1001–1011). St. Louis, MO: Mosby.

3 9 0 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
25. Vasileiadis, G. T. (2004). Grading intraventricular hemorrhage with no grades. Pediatrics, 113(4), 930–931.
26. Annibale, D. J. (2010). Periventricular hemorrhage-intraventricular hemorrhage. Medscape. Retrieved from http://emedicine.medscape.com/ article/976654-overview
27. Patra, K., Wilson-Costello, D., Taylor, H. G., Mercuri-Minich, N., & Hack, M. (2006). Grade I-II intraventricular hemorrhage in extremely low birth weight infants: Effects on neurodevelopment. The Journal of Pediatrics, 149(2), 169–173.
28. Murphy, B. P., Inder, T. E., Rooks, V., Taylor, G. A., Anderson, N. J., Mogridge, N., . . . Volpe, J. J. (2002). Posthaemorrhagic ventricular dilatation in the premature infant: Natural history and predictors of outcome. Archives of Disease in Childhood. Fetal and Neonatal Edition, 87(1), F37–F41.
29. Ment, L. R., Allen, W. C., Makuch, R. W., & Vohr, B. (2005). Grade 3 to 4 intraventricular hemorrhage and Bayley scores predict outcome. Pediatrics, 116(6), 1597–1598. http://dx.doi.org/10.1542/peds.2005-2020
30. Chumas, P., Tyagi, A., & Livingston, J. (2001). Hydrocephalus—what’s new? Archives of Disease in Childhood. Fetal and Neonatal Edition, 85(3), F149–F154.
31. Perlman, J. M. (1998). White matter injury in the preterm infant: An important determination of abnormal neurodevelopment outcome. Early Human Development, 53(2), 99–120.
32. Volpe, J. J. (2003). Cerebral white matter injury of the premature infant-more common than you think. Pediatrics, 112(1 Pt. 1), 176–180.
33. Melnyk, B. M., & Fineout-Overholt, E. (2005). Evidence-based practice in nursing and healthcare: A guide to best practice. Philadelphia, PA: Lippincott, Williams & Wilkins.
34. Symington, A., & Pinelli, J. (2003). Developmental care for promoting development and preventing morbidity in preterm infants. The Cochrane Library, (4). Retrieved from http://www.nichd.nih.gov/COCHRANE/symington/symington.htm
35. Muir Gray, J. A. (1997). Evidence-based healthcare: How to make health policy and management decisions. London, United Kingdom: Churchill Livingstone.
36. Anthony, M. Y., Evans, D. H., & Levene, M. I. (1993). Neonatal cerebral blood flow velocity responses to changes in posture. Archives of Disease in Childhood, 69(3 Spec. No.), 304–308.
37. Ancora, G., Maranella, E., Aceti, A., Pierantoni, L., Grandi, S., Corvaglia, L., & Faldella, G. (2010). Effect of posture on brain hemodynamics in preterm newborns not mechanically ventilated. Neonatology, 97(3), 212–217. http://dx.doi.org/10.1159/000253149
38. Pellicer, A., Gayá, F., Madero, R., Quero, J., & Cabañas, F. (2002). Noninvasive continuous monitoring of the effects of head position on brain hemodynamics in ventilated infants. Pediatrics, 109(3), 434–440. http://dx.doi.org/10.1542/peds.109.3.434
39. Eichler, F., Ipsiroglu, O., Arif, T., Popow, C., Heinzl, H., Urschitz, M., & Pollak, A. (2001). Position dependent changes of cerebral blood flow velocities in premature infants. European Journal of Pediatrics, 160(10), 633–639. http://dx.doi.org/10.1007/s004310100806
40. Vermont Oxford Network. (2008). What is the Vermont Oxford Network? In About Us. Retrieved from http://www.vtoxford.org/home.aspx?p5about/index.htm
41. Smith, J. R., & Donze, A. (2010). Assessing environmental readiness: First steps in developing an evidence-based practice implementation culture. The Journal of Perinatal & Neonatal Nursing, 24(1), 61–71.
42. Bedwell, S. M., Sekar, K. C., & Bright, B. C. (2010, May). Decrease in the incidence of intraventricular hemorrhages after the introduction of an IVH prevention bundle in the NICU. Presented at the Pediatric Academic Society Conference, Neonatal Neurology Platform, Vancouver, British Columbia, Canada.
43. Bozkurt, A., Rosen, A., Rosen, H., & Onaral, B. (2005). A portable near infrared spectroscopy system for bedside monitoring of newborn brain. Biomedical Engineering OnLine, 4(1), 29. http://dx.doi.org/10.1186/1475-925X-4-29
44. U. S. Food and Drug Administration. (2008). Taking a close look at ultrasound. FDA Consumer Health Information. Retrieved from http://www.fda.gov/downloads/ForConsumers/ConsumerUpdates/UCM095487.pdf
45. Pichler, G., Urlesberger, B., Schmölzer, G., & Müller W. (2004). Effect of tilting on cerebral haemodynamics in preterm infants with periventricular leucencephalomalacia. Acta Paediatrica, 93(1), 70–75. http://dx.doi.org/10.1111/j.1651-2227.2004.tb00677.x
46. Pichler, G., van Boetzelar, M. C., Müller, W., & Urlesberger, B. (2001). Effect of tilting on cerebral hemodynamics in preterm and term infants. Biology of the Neonate, 80(3), 179–185.
47. Schrod, L., & Walter, J. (2002). Effect of head-up body tilt position on autonomic function and cerebral oxygenation in preterm infants. Biology of the Neonate, 81(4), 255–259.
About the AuthorsSheila Malusky is a neonatal nurse practitioner with over 19 years
of neonatal nursing care experience, currently working in the level III NICU at St. Louis Children’s Hospital. Her interests include neo-natal neurology and family-centered care. She would like to thank Dr. Lyla Lindholm at UMKC and St. Louis Children’s Hospital NICU IVH Prevention Taskforce. Ms Malusky would especially like to thank Ms. Donze for her continuing mentorship and caring guid-ance. Ms. Malusky received her undergraduate degree from Maryville University in St. Louis, her graduate degree from Barnes-Jewish College of Nursing and Allied Health, and her doctoral degree from the University of Missouri, Kansas City.
Ann Donze has over 34 years of experience in the NICU, with the past 15 years as a neonatal nurse practitioner. She has coordinated the neonatal nurse practitioner program at Barnes-Jewish College of Nursing and Allied Health. Ms. Donze currently cochairs the St. Louis Children’s NICU research committee. Ms. Donze received her nursing diploma from Barnes School of Nursing, her undergraduate degree from Maryville University, and her graduate degree from Southern Illinois University-Edwardsville.
For further information, please contact: Sheila Malusky, DNP, RN, NNP-BC E-mail: [email protected]

V O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 3 9 1N E O N A T A L N E T W O R K
ap
pen
dix�
n S
umm
ary
of
Evid
ence
6,10
–12
,36
–39,
45–4
7
Art
icle
Cit
atio
nEv
iden
ce T
ype
Rat
ing
St
ren
gth
/Q
ual
ity
PIC
O Q
uest
ion
Pop
ulat
ion
Inte
rven
tio
nO
utco
mes
Stud
y Li
mit
atio
ns
The
effe
cts
of
pos
ture
on
bra
in
hem
odyn
amic
s in
pre
term
ne
wb
orns
not
m
echa
nica
lly
vent
ilate
d
Anc
ora
et a
l., 2
010
Qua
si-e
xper
imen
tal,
non-
rand
omiz
ed,
conv
enie
nce
sam
ple
, with
in-
subj
ect
bef
ore-
and
-aft
er d
esig
n w
ith p
artic
ipan
ts
serv
ing
as t
heir
own
cont
rols
Leve
l 2A
re t
here
al
tera
tions
in
the
bra
in
hom
odyn
amic
s of
pre
term
ne
wb
orns
fo
llow
ing
head
and
b
ody
pos
ition
ch
ang
es?
The
influ
ence
of
ges
tatio
nal
age,
pos
tnat
al
age,
and
nas
al
CPA
P w
as a
lso
eval
uate
d.
infa
nts
: 24
sta
ble
p
rete
rm in
fant
s.
All
with
nor
mal
b
rain
stu
die
s.
Elev
en o
n na
sal
CPA
P.
Mea
n G
a:
27.5
wee
ks
Mea
n W
eig
ht:
92
5 gr
ams
Mea
n a
ge
: 10
.3 d
ays
Met
ho
d: I
nfan
ts w
ere
mea
sure
d af
ter
pla
cem
ent
in
6 di
ffer
ent
pos
ition
s.
Hea
d: m
idlin
e he
ad p
ositi
on o
r he
ad r
otat
ed 9
0 d
egre
es t
o th
e si
de.
Bo
dy:
pro
ne o
r su
pin
e.
HO
B: f
lat
or e
leva
ted.
Ges
tatio
nal a
ge,
CPA
P an
d p
ostn
atal
ag
e w
ere
anal
yzed
as
ind
epen
den
t va
riab
les.
Stu
dy
inst
rum
ent:
Nea
r-in
frar
ed s
pec
tros
copy
(N
IRS)
.
Bio
log
ical M
easu
res:
C
hang
es in
tis
sue
hem
oglo
bin
(hg
b)
ind
ex (
nTH
I) a
nd t
issu
e ox
ygen
atio
n in
dex
(TO
I)
afte
r p
ostu
re v
aria
tions
.
AN
OVA
was
per
form
ed
to e
valu
ate
tiss
ue
hem
oglo
bin
ind
ex (
nTH
I)
and
tiss
ue o
xyg
enat
ion
ind
ex (
TOI)
in a
ll p
osit
ions
. No
sig
nific
ant
chan
ges
in n
THIs
or
TOI
for
infa
nts
. 2
6 w
eeks
g
esta
tion
. nTH
I was
si
gni
fican
tly
red
uced
in
infa
nt ,
26
wee
ks d
urin
g he
ad r
otat
ion.
nTH
I w
as in
sup
ine
pos
itio
ns
(bot
h fla
t an
d at
30
deg
rees
ele
vate
d)
wer
e si
gni
fican
tly
hig
her
than
su
pin
e p
osit
ion
wit
h he
ad r
otat
ed t
o th
e si
de
(p ,
0.0
5). T
OIs
rem
aine
d st
able
in a
ll p
osit
ions
. C
PAP
and
pos
tnat
al a
ge
wer
e no
t si
gni
fican
tly
asso
ciat
ied
wit
h ch
ang
es
in n
THI a
nd T
OI.
Smal
l sam
ple
si
ze w
ith o
nly
8 p
atie
nts
in
the
, 2
6 an
d ,
27
wee
ks
GA
gro
ups.
Infa
nts
spen
t onl
y 10
min
utes
in e
ach
posi
tion,
whi
ch
mig
ht n
ot b
e lo
ng
enou
gh fo
r ful
l ev
alua
tion.
No
pow
er a
naly
sis
per
form
ed t
o d
eter
min
e nu
mb
er
of s
ubje
cts
need
ed
to r
each
sta
tistic
al
sign
ifica
nce.
Effe
cts
of t
iltin
g on
ce
reb
ral h
emo
-d
ynam
ics
in p
re-
term
infa
nts
with
p
eriv
entr
icul
ar
leuc
ence
pha
-lo
mal
acia
Pich
ler,
Url
esb
erg
er,
Schm
olze
r, &
M
ulle
r, 20
04
Qua
si-e
xper
imen
tal,
non-
rand
omiz
ed
conv
enie
nce
sam
ple
, with
co
ntro
l gro
up
desi
gn.
Leve
l 2Fo
llow
ing
tiltin
g b
ed u
p
20 d
egre
es,
are
ther
e an
y ef
fect
s in
th
e ce
reb
ral
hem
odyn
amic
s of
pre
term
in
fant
s w
ith o
r w
ithou
t PV
L id
enti
fied
?
infa
nts
: 35
stab
le
pret
erm
infa
nts:
C
ontr
ol g
roup
—25
infa
nts
with
nor
mal
br
ain
stud
ies.
Ex
perim
enta
l gr
oup
—10
in
fant
s w
ith P
VL.
Mea
n G
a:
30 w
eeks
Mea
n W
eig
ht:
12
25 g
ram
s
Mea
n a
ge
: 14
day
s
Met
ho
d: I
nfan
ts w
ere
mea
sure
d b
efor
e an
d af
ter
pos
ition
cha
nges
by
tiltin
g b
ed u
p 20
deg
rees
.
Hea
d a
nd
Bo
dy:
Rig
ht la
tera
l.
HO
B: F
rom
HO
B fla
t to
elev
ated
.
The
10 in
fant
s w
ith P
VL
had
24 e
pis
odes
of h
ead
tilte
d up
20
deg
rees
for
30 m
inut
es,
and
19 e
pis
odes
hor
izon
tal
for
30 m
inut
es.
The
25 in
fant
s w
ith P
VL
had
24 e
pis
odes
of h
ead
tilte
d up
20
deg
rees
for
30 m
inut
es,
and
23 e
pis
odes
hor
izon
tal
for
30 m
inut
es.
Stu
dy
inst
rum
ent:
NIR
S
Alth
ough
bot
h gr
oups
had
si
gnifi
cant
ly in
crea
sed
cere
bra
l blo
od v
olum
e fo
llow
ing
a til
ting
dow
nwar
d m
aneu
ver,
ce
reb
ral b
lood
vol
ume
and
cere
bra
l hem
oblo
bin
oxyg
en in
dex
was
si
gnifi
cant
ly in
crea
sed
in in
fant
s w
ith P
VL
com
par
ed t
o in
fant
s w
ithou
t PV
L p
ost
tiltin
g (p
, 0
.01)
. Pos
t til
ting
up, i
nfan
ts w
ith P
VL
had
a p
rono
unce
d d
ecre
ase
in C
BV a
nd p
ost
tiltin
g d
own
had
a p
rono
unce
d in
crea
se in
CBV
.
Smal
l sam
ple
siz
e.In
vest
igat
ors
note
d th
at it
w
as s
omet
imes
d
iffic
ult
to r
ule
out
arti
fact
s.
Infa
nts
in P
VL
grou
p
had
sign
ifica
ntly
lo
wer
ges
tatio
nal
age,
bir
thw
eigh
t,
and
wei
ght.
The
y ha
d si
gnifi
cant
ly
high
er P
CA
and
chro
nolo
gica
l age
.
Onl
y 30
min
utes
in
each
pos
ition
and
no
t al
l inf
ants
wer
e ab
le t
o co
mp
lete
th
e se
que
nce.
No
pow
er a
naly
sis.
(con
tinue
d)

3 9 2 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
Bio
log
ical M
easu
res:
M
easu
red
Cer
ebra
l blo
od
volu
me
(CBV
) an
d ce
reb
ral
hem
oglo
bin
oxy
gen
ind
ex
(cH
bD
).
Inve
stig
ator
s al
so r
ecor
ded
EKG
, pu
lse
oxim
etry
, cap
nogr
aphy
, an
d re
spira
tory
eff
ort.
The
anal
ysis
was
com
ple
ted
usin
g St
uden
t t-
test
for
pai
red
anal
ysis
and
Man
n-
Whi
tney
U-t
est
usin
g St
atvi
ew s
oftw
are.
Eval
uatio
n an
d d
evel
opm
ent
of
pot
entia
lly b
ette
r p
ract
ices
for
the
pre
vent
ion
of
bra
in h
emor
rhag
e an
d is
chem
ic
bra
in in
jury
in
very
low
bir
th
wei
ght
infa
nts.
Car
teau
x et
al.,
20
03
Evid
ence
-bas
ed
liter
atur
e re
view
, b
ench
mar
king
, an
d ex
per
t co
mm
itte
e re
view
des
ign
Leve
l 4
Exp
ert
Com
mitt
ee
Rep
ort.
D
o th
ey
have
a
leve
l for
cl
inic
al
pra
ctic
e g
uid
elin
e?
This
rea
lly
fits
that
d
efin
ition
.
Can
an
eval
uatio
n an
d d
evel
opm
ent
of p
oten
tially
b
ette
r p
ract
ices
for
the
pre
vent
ion
of b
rain
he
mor
rhag
e an
d is
chem
ic
bra
in in
jury
in
very
low
bir
th
wei
ght
infa
nts
be
iden
tifie
d?
Five
Ben
chm
ark
NIC
Us.
Fi
ve N
ICU
s w
ho w
ere
VON
m
emb
ers
par
tici
pat
ed in
a
QI p
roje
ct t
o ev
alua
te
pra
ctic
es in
ben
chm
arke
d ho
spit
al’s
IVH
pre
vent
ion
met
hod
s. T
hey
uti
lized
b
ench
mar
kin
g of
pra
ctic
es
in in
stit
utio
ns w
ith
low
in
cid
ence
of I
VH
an
d PV
L,
syst
emat
ic r
evie
w o
f th
e lit
erat
ure,
an
d ex
per
t co
nsut
atio
n, t
he
gro
up t
hen
m
ade
reco
mm
end
atio
ns.
Ten
pot
entia
lly b
ette
r p
ract
ices
wer
e id
enti
fied,
in
clud
ing
neut
ral h
ead
pos
ition
ing
and
the
use
of d
evel
opm
enta
l car
e st
rate
gies
.
Som
e of
the
PBP
s w
ere
bas
ed
on lo
wer
leve
l ev
iden
ce w
hen
no R
CTs
wer
e av
aila
ble
.
Non
inva
sive
co
ntin
uous
m
onito
ring
of t
he
effe
cts
of h
ead
pos
ition
on
bra
in
hem
odyn
amic
s in
ve
ntila
ted
infa
nts.
Pelli
cer,
Gay
a,
Mad
ero,
Que
ro,
& C
aban
as, 2
002
Qua
si-e
xper
imen
tal,
non-
rand
omiz
ed,
conv
enie
nce
sam
ple
, with
in-
subj
ect
bef
ore-
and
-aft
er d
esig
n w
ith p
artic
ipan
ts
serv
ing
as t
heir
own
cont
rols
.
Leve
l 2C
an t
he e
ffec
ts o
f he
ad p
ositi
on
on b
rain
he
mod
ynam
ics
or c
hang
es
in c
ereb
ral
veno
us b
lood
flo
w/
volu
me
in v
entil
ated
in
fant
s b
e id
enti
fied
?
Infa
nts
: 21
pre
term
in
fant
s. 1
3 on
co
nven
tiona
l ve
ntila
tors
, 8 o
n os
cilla
tors
Mea
n G
A:
30.9
4.9
wee
ks
Mea
n W
eig
ht:
15
75
80
3 gr
ams
Mea
n A
ge
: 5.
8 da
ys
Met
ho
d:
Infa
nts
mea
sure
d b
efor
e an
d af
ter
bei
ng p
lace
d in
mul
tiple
pos
ition
s.
Hea
d: m
idlin
e or
hea
d ro
tate
d 90
deg
rees
to
the
sid
e.
Bo
dy:
pro
ne o
r su
pin
e.
HO
B: F
lat o
r ele
vate
d 30
deg
rees
.
Infa
nts
mea
sure
d ev
ery
10 m
inut
es fo
r 30
min
utes
in
each
pos
ition
.
Stu
dy
Inst
rum
ent:
NIR
S H
US
was
obt
aine
d af
ter
stud
y to
d
etec
t ch
ang
es.
Bio
log
ical M
easu
res:
ch
ang
es in
cer
ebra
l blo
od
volu
me
(C
BV)
and
cere
bra
l b
lood
flow
(C
BF).
Cha
ng
e in
cer
ebra
l blo
od
volu
me
sig
nific
antl
y in
crea
sed
wit
h h
ead
turn
ed 9
0 d
egre
es.
(p 5
0.0
5). T
his
chan
ge
was
mos
t p
rono
unce
d in
infa
nts
, 1
200
gra
ms.
Th
ere
was
als
o a
sig
nific
ant
chan
ge
in c
ereb
ral b
lood
flo
w
rela
tive
to
tim
e sp
ent
in
sup
ine
wit
h h
ead
turn
ed
to s
ide
com
par
ed t
o h
ead
in m
idlin
e (p
5 0
.026
).
Ther
e w
as n
o si
gni
fican
t ch
ang
e in
cer
ebra
l b
lood
flo
w o
r an
y ot
her
p
hysi
olog
ic v
aria
ble
: BP
, ox
ygen
sat
urat
ion,
PC
O2.
Smal
l sam
ple
siz
e.
CBF
mea
sure
men
ts
wer
e un
succ
essf
ul
in 9
infa
nts.
Tri
ed
to m
inim
ize
bia
s by
ran
dom
ly
assi
gnin
g th
e st
artin
g p
ositi
on.
Als
o al
l HU
S an
d al
l NIR
wer
e re
ad
by t
he s
ame
inve
stig
ator
.
Ap
pen
dIx�
n S
umm
ary
of
Evid
ence
(co
ntin
ued)
Art
icle
Cit
atio
nEv
iden
ce T
ype
Rat
ing
St
ren
gth
/Q
ual
ity
PIC
O Q
uest
ion
Pop
ulat
ion
Inte
rven
tio
nO
utco
mes
Stud
y Li
mit
atio
ns
(con
tinue
d)

V O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 3 9 3N E O N A T A L N E T W O R K
ap
pen
dix�
n S
umm
ary
of
Evid
ence
(co
ntin
ued)
Art
icle
Cit
atio
nEv
iden
ce T
ype
Rat
ing
St
ren
gth
/Q
ual
ity
PIC
O Q
uest
ion
Pop
ulat
ion
Inte
rven
tio
nO
utco
mes
Stud
y Li
mit
atio
ns
Effe
ct o
f hea
d-u
p
bod
y til
t p
ositi
on
on a
uton
omic
fu
nctio
n an
d ce
reb
ral
oxyg
enat
ion
in
pre
term
infa
nts.
Schr
od &
Wal
ter,
2002
Qua
si-e
xper
imen
tal
Leve
l 2In
pre
term
in
fant
s, a
re
ther
e an
y ne
gati
ve
effe
cts
of h
ead
elev
ated
bod
y til
t p
ositi
on
(HET
P) o
n sy
stem
ic
and
cere
bra
l ox
ygen
atio
n,
circ
ulat
ion,
an
d sy
mp
athe
tic-
vaga
l bal
ance
?
infa
nts
: 36
pre
term
in
fant
s
Mea
n G
a: 2
5-3
6 w
eeks
. Med
ian
GA
32.
5 w
eeks
.
Mea
n W
eig
ht:
88
0-2
980
gram
s. M
edia
n w
eigh
t 14
60 g
ram
s.
Mea
n a
ge
: 2 t
o 12
day
s of
life
.
Met
ho
d: P
rete
rm in
fant
s w
ere
mea
sure
d af
ter
bei
ng
pla
ced
in m
ulti
ple
hea
d/b
ody
tilt
pos
itio
ns.
Hea
d a
nd
Bo
dy:
sup
ine
HO
B: h
oriz
onta
l the
n el
evat
ed
30 d
egre
es w
ith e
ach
pos
ition
last
ing
at le
ast
20 m
inut
es e
ach.
Infa
nts
wer
e ea
ch m
easu
red
4 tim
es in
the
var
ious
pos
ition
s d
urin
g st
udy.
Stu
dy
inst
rum
ent:
NIR
s
Bio
log
ical
Mea
sure
: Tot
al
cere
bral
hem
oglo
bin
cont
ent.
Inve
stig
ator
s al
so r
ecor
ded
EKG
, Pu
lse
oxim
etry
, mea
n ar
teria
l p
ress
ure,
and
res
pir
ator
y im
ped
ance
cur
ve.
Con
tinuo
us r
ecor
din
gs
reve
aled
initi
al m
axim
al
fluct
uatio
ns o
f tot
al
cere
bra
l hem
oglo
bin
co
nten
t (t
Hb)
up
to 4
2%
fo
llow
ing
HET
P. A
fter
st
abili
zatio
n w
ithin
sev
eral
m
inut
es, p
rolo
nged
tilt
ing
did
not
res
ult
in a
ny
furt
her
sign
ifica
nt c
hang
es
of t
Hb,
hea
rt r
ate,
m
ean
arte
rial p
ress
ure
and
oxyg
en s
atur
atio
n.
Onl
y p
rete
rm in
fant
s ,
or
51,
500
gram
s sh
owed
a
sign
ifica
nt d
ecre
ase
of
reg
iona
l cer
ebra
l oxy
gen
sa
tura
tion
(rSO
(2))
of
ab
out
2–5%
from
da
y 2
to 8
, mea
sure
d by
p
ulse
oxym
etry
.
The
stud
y an
alys
is w
as
com
ple
ted
usin
g SP
SS
stat
isti
c p
rog
ram
. Non
-p
aram
etri
c te
sts
wer
e ap
plie
d.
Smal
l sam
ple
siz
e.
The
inve
stig
ator
s d
id n
ot c
omm
ent
on d
irect
ion
of
head
(m
idlin
e or
ro
tate
d).
Pow
er a
naly
sis
not
com
ple
ted.
Posi
tion
dep
end
ent
chan
ges
of
cere
bra
l blo
od
flow
vel
ociti
es in
p
rem
atur
e in
fant
s.
Eich
ler
et a
l., 2
001
Qua
si-e
xper
imen
tal,
non-
rand
omiz
ed
conv
enie
nce
sam
ple,
non
-eq
uivo
cal c
ontr
ol
grou
p be
fore
-an
d-a
fter
des
ign,
an
d Re
peat
ed-
mea
sure
s de
sign
.
Leve
l 2
Can
pos
ition
d
epen
den
t ch
ang
es in
ce
reb
ral b
lood
flo
w v
eloc
ities
b
e id
enti
fied
in p
rem
atur
e in
fant
s?
infa
nts
: 23
stab
le
pre
term
infa
nts
all w
ith n
orm
al
bra
in s
tud
ies
and
none
m
echa
nica
lly
vent
ilate
d.
Mea
n G
a:
26.7
wee
ks
Mea
n W
eig
ht:
10
27 g
ram
s
Mea
n a
ge
: A
ll in
fant
s w
ere
stud
ies
pos
tnat
al
3-5
day
s.
Met
ho
d: I
nfan
ts w
ere
mea
sure
d b
efor
e an
d af
ter
4 p
osit
ion
chan
ges
on
3 s
epar
ate
occa
sion
s:
pos
tnat
al d
ay 3
-5, a
t on
e w
eek,
an
d at
on
e m
onth
.
Hea
d: C
ente
red
whe
n su
pin
e,
turn
ed t
o ei
ther
sid
e w
hen
sup
ine.
Bo
dy:
pro
ne o
r su
pin
e.
HO
B: N
ot d
iscu
ssed
.
Stu
dy
inst
rum
ent:
U
ltras
ound
Bio
log
ical M
easu
res:
C
ereb
ral b
lood
flow
vel
ociti
es
of in
tern
al c
arot
id a
rter
y,
vert
ebra
l art
ery,
and
bas
ilar
arte
ry.
Cer
ebra
l blo
od fl
ow
velo
citie
s w
ere
sign
ifica
ntly
hig
her
in t
he
sup
ine
pos
ition
at
the
one
mon
th o
f ag
e ev
alua
tion.
Th
e re
sear
cher
s fo
und
a d
ecre
ase
in v
erte
bra
l ar
teria
l flo
w in
pro
ne
pos
ition
, lik
ely
due
to
uni
late
ral v
esse
l co
mp
ress
ion.
Birt
hwei
ght
and
ges
tatio
nal
age
did
not
sign
fific
antly
in
fluen
ce c
ereb
ral b
lood
flo
w.
Smal
l sam
ple
siz
e.
6 in
fant
s lo
st t
o fo
llow
up
at 1
0 da
ys a
nd a
n ad
dito
nal i
nfan
t lo
st t
o fo
llow
up
at
1 m
onth
cor
rect
ed
age.
Att
empt
s to
elim
inat
e b
ias
incl
uded
the
us
e of
a s
econ
d in
vest
igat
or
blin
ded
to
infa
nt
pos
ition
s. (con
tinue
d)

3 9 4 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
Effe
cts
of t
iltin
g on
cer
ebra
l he
mod
ynam
ics
in
pre
term
and
ter
m
infa
nts
Pich
ler,
Boet
zela
r, M
ulle
r, &
U
rles
ber
ger
, 20
01
Qua
si-e
xper
imen
tal,
non
-ran
dom
ized
co
nven
ienc
e sa
mp
le, c
ontr
ol
grou
p b
efor
e-an
d-a
fter
des
ign.
Leve
l 2
Follo
win
g til
ting
bed
up
20
deg
rees
, ar
e th
ere
any
effe
cts
in
the
cere
bra
l he
mod
ynam
ics
of t
erm
and
p
rete
rm in
fant
s id
enti
fied
?
Thir
ty e
ight
in
fant
s: 2
5 p
rete
rm, m
ean
GA
33
wee
ks
and
mea
n w
eigh
t 18
99
gram
s. T
erm
: 13
infa
nts
with
m
ean
GA
39
wee
ks a
nd
mea
n w
eigh
t of
29
69 g
ram
s.
Met
ho
d: I
nfan
ts w
ere
mea
sure
d b
efor
e an
d af
ter
pos
ition
cha
nges
by
tiltin
g b
ed u
p 20
deg
rees
.
Hea
d a
nd
Bo
dy:
Rig
ht la
tera
l.
HO
B: F
rom
HO
B fla
t to
elev
ated
.
The
pre
term
infa
nts
had
24 e
pis
odes
of h
ead
tilte
d up
20
deg
rees
for
30 m
inut
es,
and
23 e
pis
odes
hor
izon
tal
for
30 m
inut
es.
The
term
infa
nts
had
12
ep
isod
es o
f hea
d ti
lted
up
20 d
egre
es fo
r 30
min
utes
, an
d 10
ep
isod
es h
oriz
onta
l fo
r 30
min
utes
.
Stu
dy
Inst
rum
ent:
NIR
S
Bio
log
ical
Mea
sure
s:
Mea
sure
d C
ereb
ral b
lood
vo
lum
e (C
BV) a
nd c
ereb
ral
hem
oglo
bin
oxyg
en in
dex
(cH
bD).
Inve
stig
ator
s al
so r
ecor
ded
EKG
, Pu
lse
oxim
etry
, cap
nogr
aphy
, an
d re
spir
ator
y ef
fort
.
Alth
ough
bot
h gr
oups
had
si
gnifi
cant
ly in
crea
sed
cere
bra
l blo
od v
olum
e fo
llow
ing
a til
ting
dow
nwar
d m
aneu
ver,
cere
bra
l blo
od v
olum
e (p
0
.01)
and
cer
ebra
l he
mob
lob
in o
xyg
en in
dex
(p
0
.001
) w
ere
bot
h si
gnifi
cant
ly a
ltere
d in
p
rete
rm in
fant
s in
bot
h til
ting
up a
nd t
iltin
g d
own
man
euve
rs. T
here
was
al
so a
cor
rela
tion
bet
wee
n p
ostc
once
ptio
nal a
ge
and
deg
ree
of c
hang
e in
ce
reb
ral b
lood
vol
ume
(p
0.0
5).
The
anal
ysis
was
com
ple
ted
usin
g St
uden
t t-
test
for
pai
red
anal
ysis
and
M
ann
-Whi
tney
U-t
est
usin
g St
atvi
ew s
oftw
are.
Smal
l sam
ple
siz
e.
Onl
y 30
min
utes
in
each
pos
ition
.
No
pow
er a
naly
sis.
Neo
nata
l cer
ebra
l b
lood
flow
ve
loci
ty r
esp
onse
s to
cha
nges
in
pos
ture
Ant
hony
, Eva
ns,
Leve
ne, 1
993
Qua
si-e
xper
imen
tal
non
rand
omiz
ed
conv
enie
nce
sam
ple
usi
ng
rep
eate
d m
easu
res
des
ign.
Leve
l 2
Cro
ss-
sect
iona
l st
udy
usin
g he
alth
y fu
ll te
rm
infa
nts
as
com
par
i-so
n gr
oup.
In n
eona
tes,
ca
n ce
reb
ral
blo
od fl
ow
chan
ges
, as
dem
onst
rate
d by
uni
pha
sic
or b
ipha
sic
resp
onse
s, b
e el
icite
d af
ter
chan
ges
in
pos
ture
?
Infa
nts
: 60
infa
nts
NIC
U In
fan
ts: 5
0,
all w
ith n
orm
al
brai
n st
udie
s.
Mea
n G
A:
28 w
eeks
Mea
n W
eig
ht:
11
50 g
ram
s
Mea
n A
ge
:
1 w
eek.
Met
ho
ds:
Infa
nts
mea
sure
d b
efor
e an
d af
ter
pos
ition
ch
ang
es b
y til
ting.
Hea
d, B
od
y, a
nd
HO
B:
In N
ICU
infa
nts,
mat
tres
s p
ositi
on w
as a
ltere
d fo
r ea
ch
test
ing
per
iod
20 d
egre
es u
p
and
20 d
egre
es d
own
from
ho
rizo
ntal
. Hea
lthy
infa
nts
wer
e p
lace
d in
a c
hair
with
a
tiliti
ng m
echa
nism
alte
rnat
ed
bet
wee
n up
righ
t an
d ly
ing
bac
k p
ositi
on.
Stu
dy
Inst
rum
ent:
U
ltras
ound
Dop
ple
r p
rob
e w
as a
ttac
hed
to e
ach
skin
ov
er t
emp
oral
bon
e.
Tota
l of 5
01 e
piso
des
in 6
0 ba
bies
wer
e m
onito
red.
In
crea
sing
per
cent
age
of b
ipha
sic
resp
onse
s in
cer
ebra
l blo
od fl
ow
velo
citie
s as
infa
nt g
ot
olde
r. Bi
phas
ic r
espo
nses
w
ere
cons
ider
ed s
econ
day
to a
utor
egul
ator
y re
spon
ses.
In t
he p
rete
rm
infa
nts,
nei
ther
a h
igh
Pco2
nor
a lo
w M
AP
(25
mm
HG
) in
fluen
ced
the
perc
enta
ge o
f bip
hasi
c re
spon
ses.
Unc
lear
if IC
U in
fant
s w
ere
sup
ine
or
pro
ne a
nd w
heth
er
head
was
in
mid
line.
Con
cent
rate
d on
ly o
n til
ting
tab
le.
Focu
s of
stu
dy
was
on
aut
oreg
ulat
ion.
Smal
l stu
dy.
Ap
peN
dIx�
n S
umm
ary
of
Evid
ence
(co
ntin
ued)
Art
icle
Cit
atio
nEv
iden
ce T
ype
Rat
ing
St
ren
gth
/Q
ual
ity
PIC
O Q
uest
ion
Po
pul
atio
nIn
terv
enti
on
Out
com
esSt
udy
Lim
itat
ion
s
(con
tinue
d)

V O L . 3 0 , N O . 6 , N O V E M B E R / D E C E M B E R 2 0 1 1 3 9 5N E O N A T A L N E T W O R K
Hea
lth
y Te
rm
Infa
nts
: 10
Mea
n G
A:
39 w
eeks
Mea
n W
eig
ht:
30
70 g
ram
s
Mea
n A
ge
:
1 w
eek
Bio
log
ical M
easu
res:
C
erb
ral p
erfu
sion
pre
ssur
e w
as m
easu
re a
t ea
ch
chan
ge
and
note
d to
be
equi
voca
l, no
res
pon
se,
unip
hasi
c (r
efle
ctin
g p
assi
ve
alte
ratio
n in
cer
ebra
l blo
od
flow
vel
ocit
y), o
r b
ipha
sic
(ref
lect
ing
initi
al p
assi
ve
alte
ratio
n, t
hen
acti
ve
resp
onse
to
chan
ge
in
cere
bra
l blo
od fl
ow v
eloc
ity)
.
Unc
lear
if
inve
stig
ator
s re
adin
g th
e C
BVV.
Cha
nges
in s
uper
ior
sag
itta
l sin
us
blo
od v
eloc
ities
d
ue t
o p
ostu
ral
alte
ratio
ns a
nd
pre
ssur
e on
th
e he
ad o
f the
ne
wb
orn
infa
nt.
Cow
en &
Tho
rese
n,
1985
Qua
si-e
xper
imen
tal,
non-
rand
omiz
ed
conv
enie
nce
sam
ple
, con
trol
gr
oup
bef
ore-
and
-aft
er d
esig
n.
Leve
l 2
Are
the
re
chan
ges
in
sup
erio
r sa
git
tal
sinu
s b
lood
ve
loci
ties
due
to
pos
tura
l ch
ang
es,
jug
ular
ven
ous
occl
usio
n,
and
incr
ease
d m
anua
l hea
d p
ress
ure
in t
he
new
bor
n?
Infa
nts
: 18
term
hea
lthy
new
bor
ns
Mea
n G
A:
39 w
eeks
Mea
n W
eig
ht:
36
83 g
ram
s
Mea
n A
ge
: 6
days
Met
ho
ds:
Infa
nts
wer
e m
easu
red
afte
r p
lace
men
t in
8 d
iffer
ent
pos
ition
s.
Infa
nts
wer
e al
so m
easu
red
whi
le a
pp
lyin
g ex
tern
al h
ead
pre
ssur
e an
d ju
gul
ar v
enou
s oc
clus
ion.
Hea
d:
mid
line
head
pos
ition
, he
ad r
otat
ed 9
0 d
egre
es t
o th
e si
de,
nec
k fle
xed
and
exte
nded
.
Bo
dy:
pro
ne, s
upin
e, o
r la
tera
l.
HO
B: f
lat
thro
ugho
ut t
he s
tud
y.
Stu
dy
Inst
rum
ent:
U
ltras
ound
Bio
log
ical M
easu
res:
C
ereb
ral b
lood
flow
vel
ociti
es
(CBF
V)
of t
he s
uper
ior
sag
itta
l sin
us.
Resu
lts r
evea
led
that
90˚
hea
d tu
rn o
cclu
des
the
jugu
lar
vein
on
the
ipsi
late
ral s
ide
and
occl
usio
n of
ven
ous
flow
on
the
cont
rala
tera
l si
de d
oes
not f
orce
blo
od
drai
nage
thr
ough
the
oc
clus
ion
with
sub
sequ
ent
incr
ease
d cr
ania
l pre
ssur
e ch
ange
s. E
xter
nal h
ead
pres
sure
als
o in
crea
ses
pres
sure
and
impe
des
veno
us d
rain
age.
Cer
ebra
l flo
od fl
ow
red
uctio
n:
Sup
ine
Bi
late
ral o
cclu
sion
of r
ight
an
d le
ft ju
gul
ar—
100
%
red
uctio
n in
flow
in a
ll su
bje
cts
Hea
d t
urn
ed 9
0 d
egre
es
to lef
t—O
cclu
sion
of
ipsi
late
ral j
ugul
ar r
esul
ted
in n
o ch
ang
e in
flow
in
25/2
6 su
bje
cts.
Occ
lusi
on o
f con
tral
ater
al
jugu
lar r
esul
ted
in 1
00%
oc
clus
ion
in 2
0/26
pat
ient
s
Incr
ease
in fo
ntan
el p
ress
ure
corr
elat
ed w
ith d
ecre
ased
ce
reb
ral b
lood
flow
ve
loci
ty. C
orre
latio
n co
effic
ient
of 0
.91.
Smal
l sam
ple
siz
e.U
ncle
ar r
egar
din
g re
liab
ility
of
font
anom
eter
us
ed t
o ac
cura
tely
m
easu
re
intr
acra
nial
p
ress
ure.
Inve
stig
ator
s st
ated
it
was
diff
icul
t to
ho
ld t
he h
and
held
Dop
ple
r tr
ansd
ucer
in p
lace
d
urin
g th
e st
udy.
In
vest
igat
ors
wer
e no
t b
lind
ed t
o in
fant
pos
ition
w
hen
inte
rpre
ting
resu
lts.
Old
er s
tud
y, b
ut c
ited
by m
any
othe
r st
udie
s.
Ap
pen
dIx�
n S
umm
ary
of
Evid
ence
(co
ntin
ued)
Art
icle
Cit
atio
nEv
iden
ce T
ype
Rat
ing
St
ren
gth
/Q
ual
ity
PIC
O Q
uest
ion
Po
pul
atio
nIn
terv
enti
on
Out
com
esSt
udy
Lim
itat
ion
s
(con
tinue
d)

3 9 6 N O V E M B E R / D E C E M B E R 2 0 1 1 , V O L . 3 0 , N O . 6N E O N A T A L N E T W O R K
Hea
d p
ress
ure
ante
rior
pos
-te
rior
, lat
eral
and
occ
ipita
l ar
eas
lead
to
varia
ble
re
sult
s. P
ress
ure
on p
oste
-ri
or fo
ntan
el a
lway
s re
sult-
ed in
dec
reas
ed c
ereb
ral
blo
od fl
ow v
eloc
ity
Hea
d p
ositi
on
affe
cts
intr
acra
nial
p
ress
ure
in
new
bor
n in
fant
s.
Emer
y &
Pea
bod
y,
1983
Qua
si-e
xper
imen
tal,
non-
rand
omiz
ed
conv
enie
nce
sam
ple
, con
trol
gr
oup
desi
gn.
Leve
l 2In
new
bor
n in
fant
s,
doe
s he
ad
pos
ition
aff
ect
intr
acra
nial
p
ress
ure?
Infa
nts
: 14
pre
term
in
fant
s— 6
with
a
hist
ory
of
asp
hyxi
a an
d 8
with
out.
Asp
hyx
iate
d
Infa
nts
: 6
Mea
n G
A:
35 w
eeks
Mea
n A
ge
: 54
hou
rs o
f life
.
No
n-
Asp
hyx
iate
d
Infa
nts
: 8
Mea
n G
A:
36 w
eeks
Mea
n A
ge
: 43
hou
rs o
f life
.
Met
ho
d: I
nfan
ts m
easu
red
bef
ore
and
afte
r 6
diff
eren
t p
ositi
on c
hang
es.
Hea
d: m
idlin
e or
90
deg
rees
he
ad t
urn
to r
ight
.
Bo
dy:
sup
ine
HO
B: F
lat,
ele
vate
d 30
deg
rees
or
dep
enda
nt 3
0 d
egre
es.
Stu
dy
Inst
rum
ent:
U
ltras
ound
and
tra
nsfo
ntan
el
pre
ssur
e tr
ansd
ucer
. M
easu
red
at le
ast
30 s
econ
ds
in e
ach
pos
ition
.
Bio
log
ical M
easu
res:
cer
ebra
l b
lood
flow
(C
Bf)
and
intr
acra
nial
pre
ssur
e (I
CP)
.
Stat
isti
cal A
naly
sis:
Stu
den
t p
aire
d t
test
usi
ng B
onfe
rron
i co
rrec
tion.
Sign
ifica
nt IC
P in
hor
izon
tal
and
dep
enda
nt p
ositi
on
whe
n he
ad t
urne
d to
the
ri
ght
(p
0.0
01)
for
bot
h gr
oups
.
Sign
ifica
nt in
crea
se in
ICP
with
hea
d m
idlin
e an
d tu
rned
whi
le in
dep
enda
nt
pos
ition
(p
0
.001
) fo
r b
oth
grou
ps.
Sign
ifica
nt d
ecre
ase
in IC
P w
hen
head
in m
idlin
e an
d el
evat
ed (
p
0.0
1) a
nd
even
mor
e d
ecre
ased
in
asp
hyxi
ated
infa
nts
(p
0
.02)
.
Smal
l sam
ple
siz
e
Old
er s
tud
y
The
effe
ct o
f he
ad p
ositi
on
on in
trac
rani
al
pre
ssur
e in
the
ne
onat
e w
as
stud
ied.
Gol
db
erg,
Josh
i, M
osco
so, &
C
astil
lo, 1
983
Qua
si-e
xper
imen
tal,
non-
rand
omiz
ed
conv
enie
nce
sam
ple
des
ign.
Leve
l 2
Are
the
re a
ny
iden
tifie
d ef
fect
s of
hea
d p
ositi
on o
n in
trac
rani
al
pre
ssur
e in
th
e ne
onat
e,
as is
foun
d in
the
ad
ult
liter
atur
e?
Infa
nts
: 26
pre
term
in
fant
s.
Mea
n G
A:
33 w
eeks
Mea
n W
eig
ht:
14
97 g
ram
s
Mea
n A
ge
: 3
days
, with
a
rang
e of
1-
10 d
ays.
Met
ho
d: I
CP
mea
sure
d ev
ery
1 m
inut
e fo
r 10
min
utes
in
each
of 4
pos
ition
s.
A 4
-min
ute
stab
iliza
tion
per
iod
was
giv
en a
fter
eve
ry
pos
ition
cha
nge.
Hea
d: m
idlin
e or
tur
ned
to t
he
righ
t.
Bo
dy:
sup
ine
HO
B: f
lat
or e
leva
ted
30
deg
rees
.
Stu
dy
Inst
rum
ent:
Lad
d m
onito
r to
stu
dy
intr
acra
nial
p
ress
ure.
The
resu
lts
sug
ges
t in
trac
rani
al p
ress
ure
was
sig
nific
antly
low
er
in m
idlin
e p
ositi
ons
com
par
ed t
o p
ositi
ons
with
the
hea
d tu
rned
.
The
intr
acra
nial
pre
ssur
e w
as a
lso
sign
ifica
ntly
lo
wer
in p
atie
nts
who
se
head
was
ele
vate
d to
30
deg
rees
.
The
pos
ition
with
the
low
est
mea
sure
d in
trac
rani
al
pre
ssur
e w
as h
ead
mid
line
with
hea
d of
bed
ele
vate
d 30
deg
rees
.
Smal
l sam
ple
siz
e.
Old
er s
tud
y.
Pow
er n
ot c
alcu
late
d.
10 m
inut
es is
a b
rief
tim
e p
erio
d fo
r st
udy.
To a
void
bia
s,
pos
ition
ord
er
was
ran
dom
ly
assi
gned
.
Ap
peN
dIx�
n S
umm
ary
of
Evid
ence
(co
ntin
ued)
Art
icle
Cit
atio
nEv
iden
ce T
ype
Rat
ing
St
ren
gth
/Q
ual
ity
PIC
O Q
uest
ion
Po
pul
atio
nIn
terv
enti
on
Out
com
esSt
udy
Lim
itat
ion
s