Embed Size (px)
Citation preview
Susan E. Langmore, PhD, BCS-SBoston University School of MedicineBoston University, Sargent CollegeBoston University Medical Center
NeuroStimulationTechniques for Dysphagia
Boston UniversitySlideshow Title Goes Here
THREE STIMULATION TECHNIQUES TO BE COVERED… in 17 minutes or less!
§ Transcutaneous electrical stimulation
§ Pharyngeal stimulation
§ Transcortical brain stimulation
Boston UniversitySlideshow Title Goes Here
For each technique…...
§ 1. How it works and the desired effect§ 2. Evidence for actually attaining the desired effect

Boston UniversitySlideshow Title Goes Here
1. Transcutaneous Electrical Stimulation
§ Neuromuscular Electrical Stimulation - NMES§ “Vital Stim” – a brand of NMES
§ some key differences from common NMES devices§ Constant stimulation on;; § Multiple electrode placements above/below hyoid and larynx
Boston UniversitySlideshow Title Goes Here
Vital Stim
Boston UniversitySlideshow Title Goes Here
Example of traditional Estim device: BMR NeuroTech (NT) 2000
Boston UniversitySlideshow Title Goes Here
How it Works§ Electrodes placed on the skin overlying muscles of interest;; current at high level will trigger peripheral nerves in region to fire à muscles they innervate contract (= NMES)§ Used to augment contraction;; increase force of swallow;; increase speed of contraction
§ OR Can be set at lower level of current flow;; only the sensory nerves are stimulated, The patient feels TINGLING, VIBRATION.§ TENS is example;; to alleviate pain§ A few studies in dysphagia: Aim: to facilitate a brisker swallow
Boston UniversitySlideshow Title Goes Here
Have studies proven a positive effect?
§ Many studies …§ Most of them used VitalStim –§ Most done on stroke patients
§ Many uncontrolled studies…....
Boston UniversitySlideshow Title Goes Here
Controlled Treatment Studies with Estim -‐> mixed results
§ Stroke – (Ludlow 06)–estim helped some patients; worsened the swallow in others
§ Stroke – RCT no significant effect on patients (Bulow et al., 2008)
§ Stroke -‐ RCT (Lim et al, 2009) – estim group did signif better than pts w/ alternate tx
§ Stroke – RCT (reported by Carnaby-‐Mann – not yet published) Estim group did worse than alternate therapy group
Boston UniversitySlideshow Title Goes Here
Recent study
§ Terre 2015 (Spain) – 20 acute stroke or TBI (mean time post = 3 month). Randomized to NMES or sham
§ Results: some sig different measures at 1 month….. but at 3 months, no difference!
§ Their conclusion – NMES accelerated recovery
Boston UniversitySlideshow Title Goes Here
Chen 2015. Systematic Review & MetaAnalysis§ Identified 8 controlled studies of post stroke dysphagia : § 6 compared NMES plus Swallow tx to Swallow txalone;;
§ 3 compared NMES to Swallow Tx aloneConclusions:NMES plus Swallow Tx was signif better than Swallow Tx alone or NMES alone
Boston UniversitySlideshow Title Goes Here§ Ryu – 2008 § Lin – 2009 § Long -2015weaker designs
NMES for Head/Neck Cancer?
Boston UniversitySlideshow Title Goes Here
Our Study: Randomized Clinical Trial: The Efficacy of Electrical Stimulation for Dysphagia in Patients with Head and Neck Cancer
Susan Langmore - (PI) Co-Investigators: Tim McCulloch,CathyLazarus, Doug VanDaele, Jeri Logemann
Just published: 2015, Head & Neck
Boston UniversitySlideshow Title Goes Here
Patients
§ 179 Subjects enrolled:§ HNC treated with RT/CRT at least 3 months prior to enrolling (range 3 months to 15 years post RT)
§ Moderate to severe dysphagia
Boston UniversitySlideshow Title Goes Here
The Intervention
Subjects randomized to 2 intervention groups;; 1. Estim group - swallow exercises with e-stim, 2. “Sham Estim” group - swallow exercises w/ sham
estim device (no current)
Stretching and Swallow exercises = Mendelsohn maneuver, supra superglottic, and Effortful swallowsHome program;; exercises 2x/day, 6d/week, 3 months
Boston UniversitySlideshow Title Goes Here
§ Two electrodes placed submentally to activate the suprahyoid muscles
§ Patient swallowed each time thestimulation came on…..relaxedbetween cycles of stimulation
Estim device = NT2000 (BMR)
Boston UniversitySlideshow Title Goes Here
Outcome Measures
Swallow function – from MBS studies§ PAS (Rosenbek, 1996)§ OPSE (Rademaker, 1994)§ Hyoid superior, hyoid anterior movement§ Percent Pharyngeal residue (from OPSE)
§ Diet and quality of life§ PSS (Performance Status Scale, (List, 1990)§ HNCI (Head/Neck Cancer Inventory, Funk, 2003)
Boston UniversitySlideshow Title Goes Here
Question #1
§ Was there a significant difference in measures of swallowing, diet, or quality of life in the Estimgroup vs. the Sham Estim group at the end of the trial?
Boston UniversitySlideshow Title Goes Here
Results: Q#1
Only 1 significant difference: § Sham Estim group - significantly lower PAS scores than the Active Estim group
§ Effect size analysis = “moderate effect” (Cohen’s d = 0.472);; not impressive, clinically
No other significant differences between the 2 groups
Boston UniversitySlideshow Title Goes Here
Question #2
§ Did either or both groups show a significant improvement over time – from start to end of treatment (Week 12) -- in swallowing, diet or QOL measures?
Boston UniversitySlideshow Title Goes Here
Results: Change over Time
§ Sham group improved PAS score – small decrease
No other MBS measures improved over the trial
§ Both groups significantly improved diet and quality of life
Boston UniversitySlideshow Title Goes Here
Conclusions from our Study
§ E-stim did not add therapeutic benefit
§ Neither group improved significantly in any swallow outcome measure over the therapy - from the estim - or the swallow maneuver exercises
§ But quality of life and diet improved
Boston UniversitySlideshow Title Goes Here
Should you use NMES?
§ Promising studies with acute stroke – but mixed results – more research needed (what parameters are best? How long? etc)
§ Good evidence that it should be paired with swallowing to stimulate neuroplasticity
§ No support for NMES with other medical conditions, including chronic stroke - and negative evidence for HNC
Boston UniversitySlideshow Title Goes Here
ELECTRICAL PHARYNGEAL STIMULATION
Boston UniversitySlideshow Title Goes Here
Pharyngeal Stimulation
§ Catheter containing the electrodes - passed transnasally –electrical stimulators are positioned within the pharynx against the mucosa
§ Stimulus delivered at a given intensity –mostly at a sensory level but some motor effect
§ Stimulation induces swallowing§ Usually done 10-20 min/day for 3 days
Boston UniversitySlideshow Title Goes Here
Pharyngeal Stimulation§ How does it work?
§ Stimulate the pharyngeal mucosa at right frequency -> excites the motor cortex for an hour after stimulation ends
Phagenesis device (www.phagenesis.com)
Boston UniversitySlideshow Title Goes Here
Pharyngeal Electrical Pharyngeal Stimulation indluces cortical activity
In normals:§ Shaneen Hamdy’s lab (UK)
§ Fraser, (2002) – pharyngeal stim showed changes in cortical excitability with pharyngeal stimulation w/ normals – lasted 30-60 min post stimulation
§ Sundrup (2014) confirmed this;; added to knowledge of cortical processing w/ magnetoencephalography
§ (This has not been shown for NMES)
Boston UniversitySlideshow Title Goes Here
Good Evidence for Pharyngeal Stimwith Acute Stroke/Dysphagia§ Jayasekeran, et al (2010) – reported signifimprovements in swallowing-related outcomes in 28 patients (PharyStim vs Sham)
§ Suntrup 2015: (Germany) 30 stroke patients w/ trachsreceived pharyngeal stim or sham for 3 days. Decannulation signif sooner in pharyn stim group cf to sham group
Boston UniversitySlideshow Title Goes Here
More Research on Pharyngeal Stim§ Restivo 2013 (Italy): 20 MS patients: pharyngeal stimvs sham. Pharyn Stim pts signif better on all swallow measures
BUT§ Largest RCT (P Bath, PI, Nottingham) on stroke patients showed NO significant difference in pharynstim vs sham groups in any outcome (not published yet)
Boston UniversitySlideshow Title Goes Here
SHOULD YOU USE PHARYNGEAL STIMULATION?
Not yet approved in US by FDA Research pending in US to show efficacyBut promising! Good research will prove whether it is effective and for whomDifferent frequencies, other parameters reflect cortical activity differently – these must be established before used clinically
Boston UniversitySlideshow Title Goes Here
NON-INVASIVE CORTICAL STIMULATION FOR DYSPHAGIA
Boston UniversitySlideshow Title Goes Here
Transcranial Neurostimulation
§ Non-invasive brain stimulationused to enhance neuroplasticity
§ Two most common types:
(1) Transcranial Direct Current Stimulation (tDCS)
(2) Transcranial Magnetic Stimulation (TMS) repetitive Transcranial Magnetic Stimulation (rTMS)
This image cannot currently be displayed.
Boston UniversitySlideshow Title Goes HereTRANSCRANIAL DIRECT CURRENT STIMULATION
tDCS
Boston UniversitySlideshow Title Goes Here
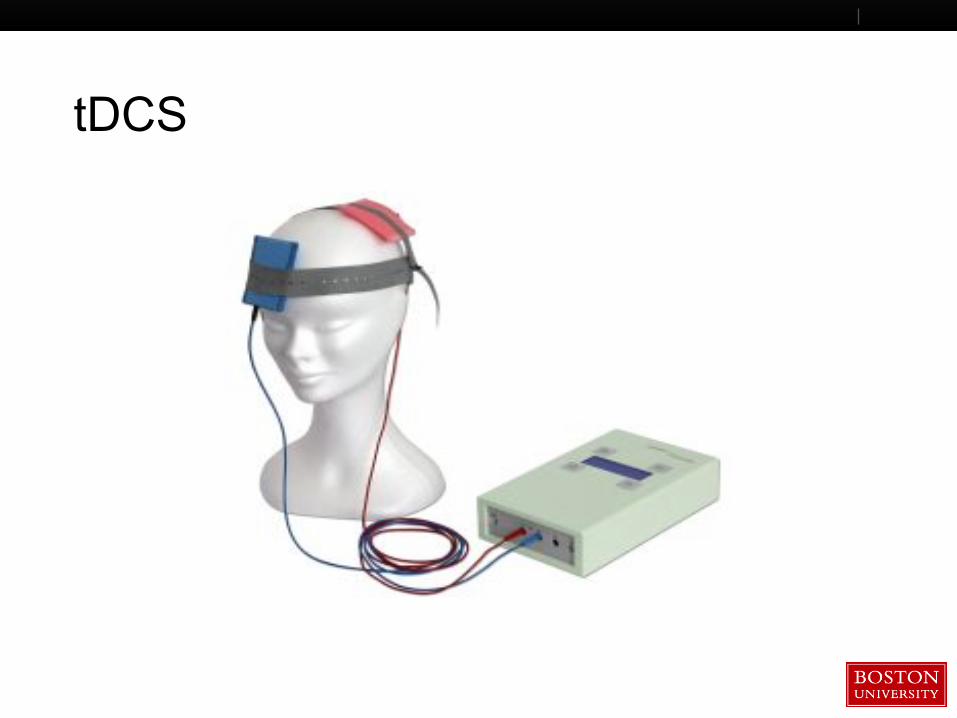
tDCS
Boston UniversitySlideshow Title Goes Here
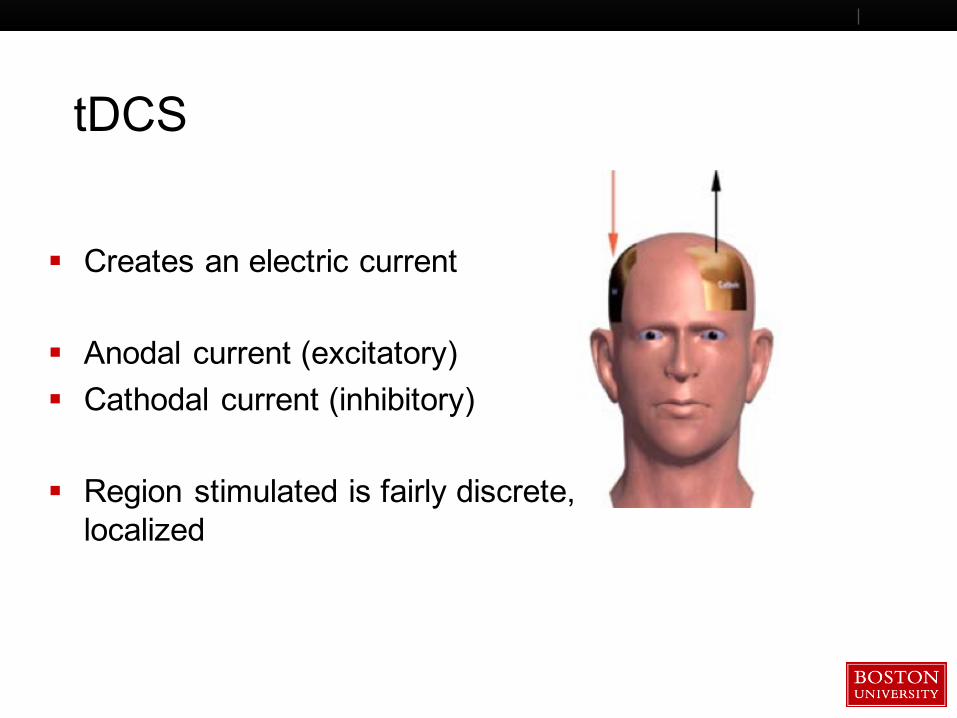
tDCS
§ Creates an electric current
§ Anodal current (excitatory)§ Cathodal current (inhibitory)
§ Region stimulated is fairly discrete, localized
Boston UniversitySlideshow Title Goes HereTRANSCRANIAL MAGNETIC STIMULATION
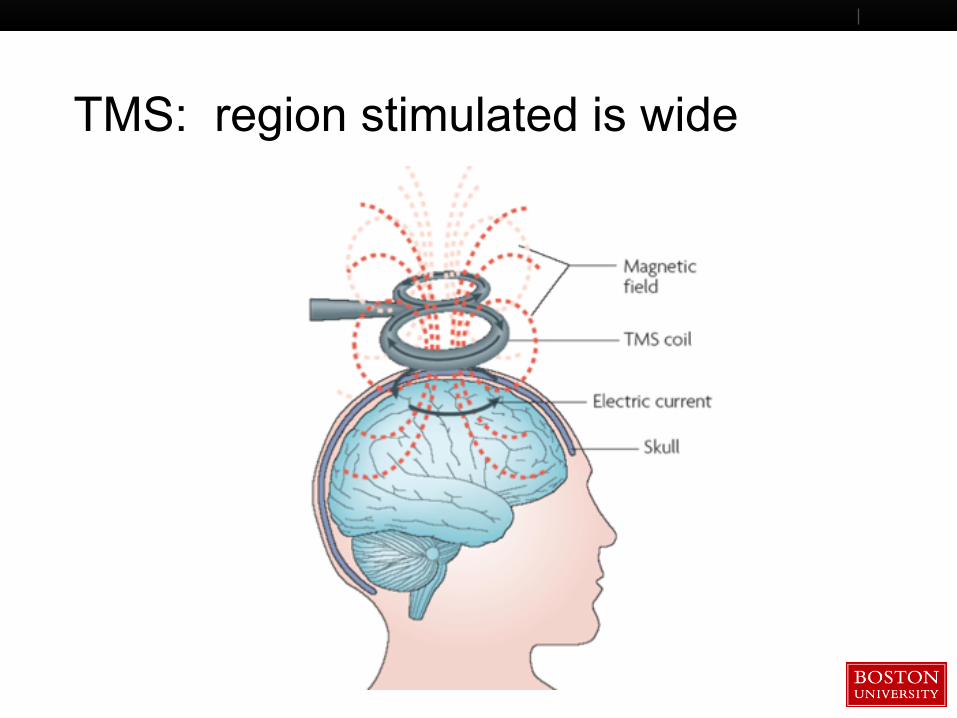
Electromagnetic induction produces magnetic fields inside the brain
Boston UniversitySlideshow Title Goes HereREPETITIVE TMS
High frequency stimulation causes brain excitationLow frequency stimulation causes neuronal inhibition
Boston UniversitySlideshow Title Goes Here
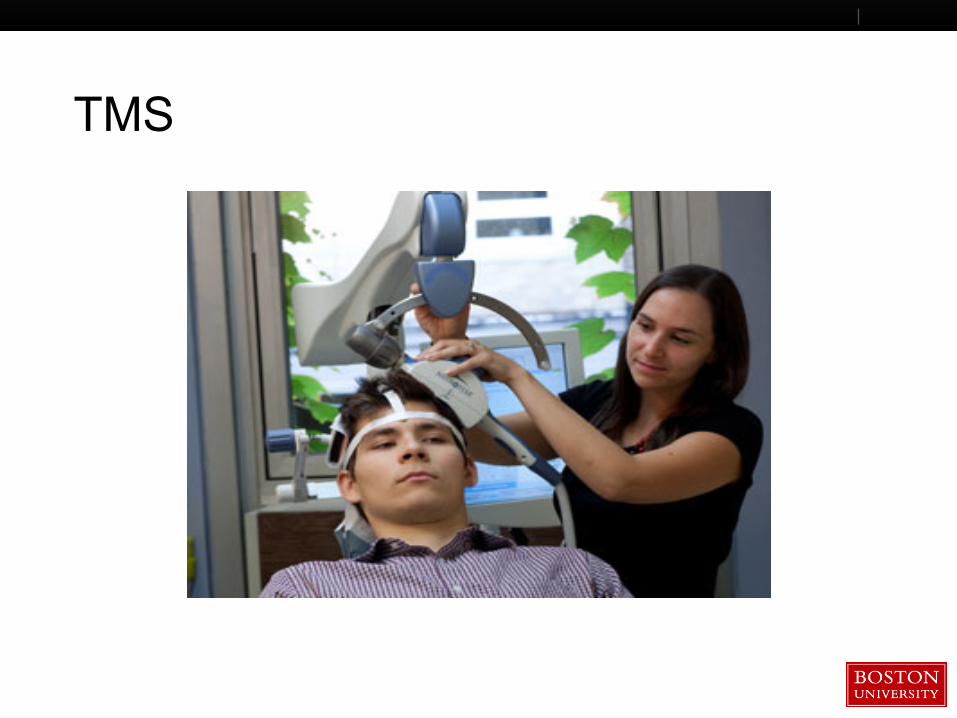
TMS
Boston UniversitySlideshow Title Goes Here
TMS: region stimulated is wide
Boston UniversitySlideshow Title Goes Here
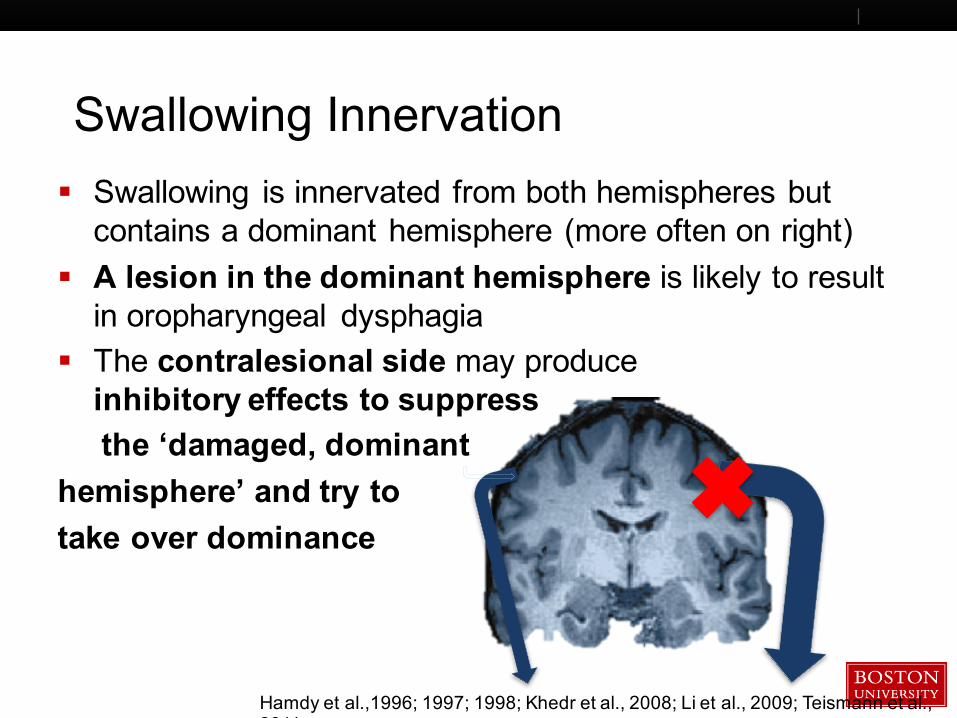
Swallowing Innervation§ Swallowing is innervated from both hemispheres but contains a dominant hemisphere (more often on right)
§ A lesion in the dominant hemisphere is likely to result in oropharyngeal dysphagia
§ The contralesional side may produceinhibitory effects to suppressthe ‘damaged, dominant
hemisphere’ and try totake over dominance
Hamdy et al.,1996;; 1997;; 1998;; Khedr et al., 2008;; Li et al., 2009;; Teismann et al., 2011
Boston UniversitySlideshow Title Goes Here
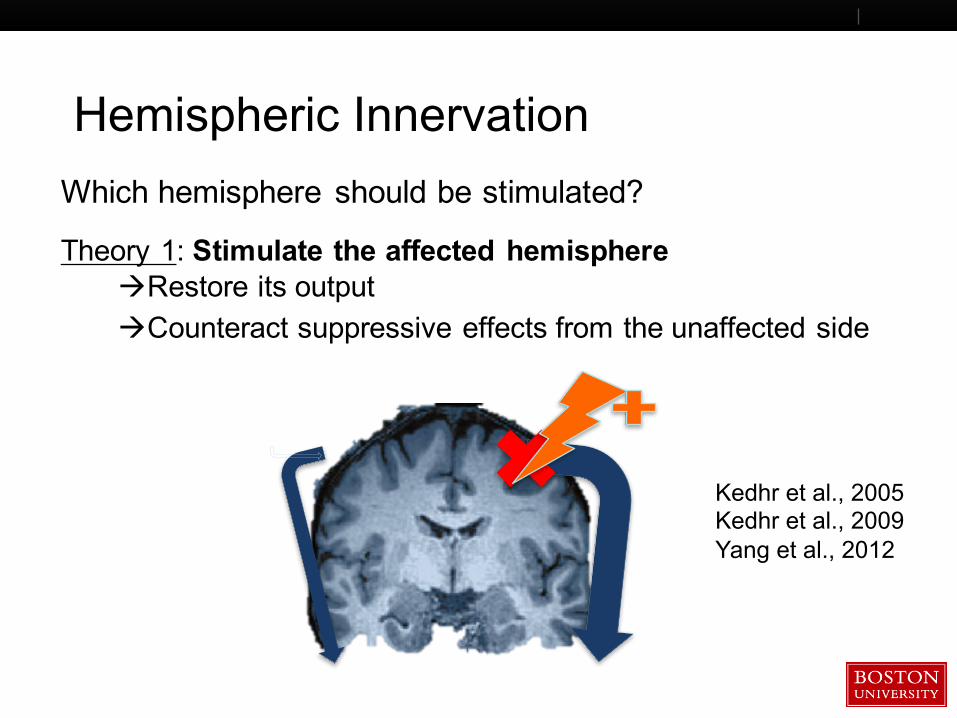
Hemispheric InnervationWhich hemisphere should be stimulated?
Kedhr et al., 2005Kedhr et al., 2009Yang et al., 2012
Theory 1: Stimulate the affected hemisphereàRestore its outputàCounteract suppressive effects from the unaffected side
Boston UniversitySlideshow Title Goes Here
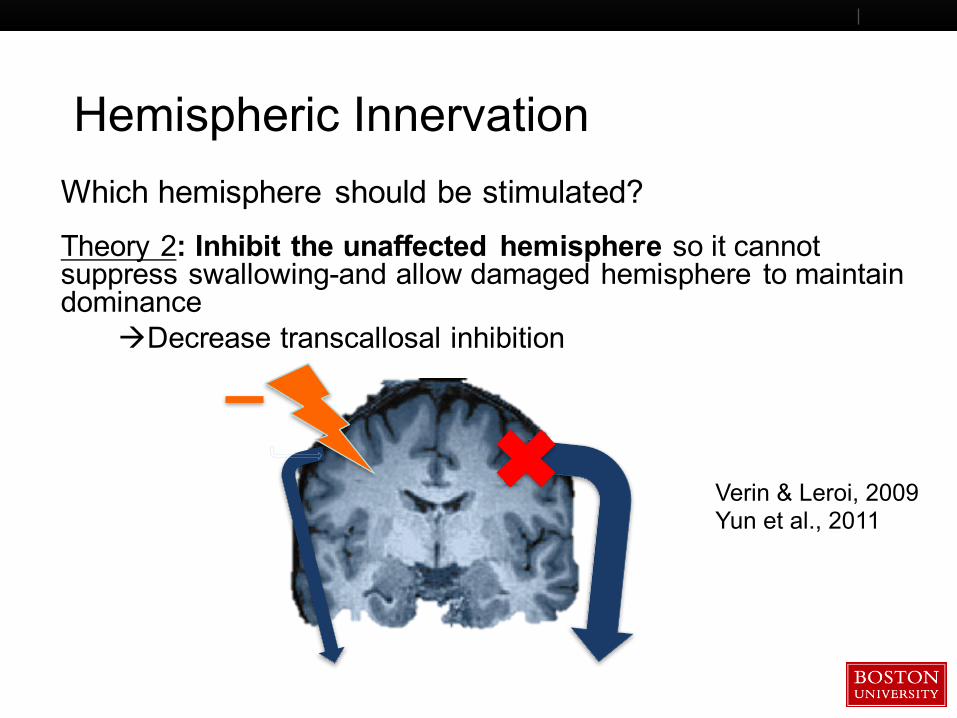
Hemispheric InnervationWhich hemisphere should be stimulated?
Verin & Leroi, 2009Yun et al., 2011
Theory 2: Inhibit the unaffected hemisphere so it cannot suppress swallowing-and allow damaged hemisphere to maintain dominance
àDecrease transcallosal inhibition
Boston UniversitySlideshow Title Goes Here
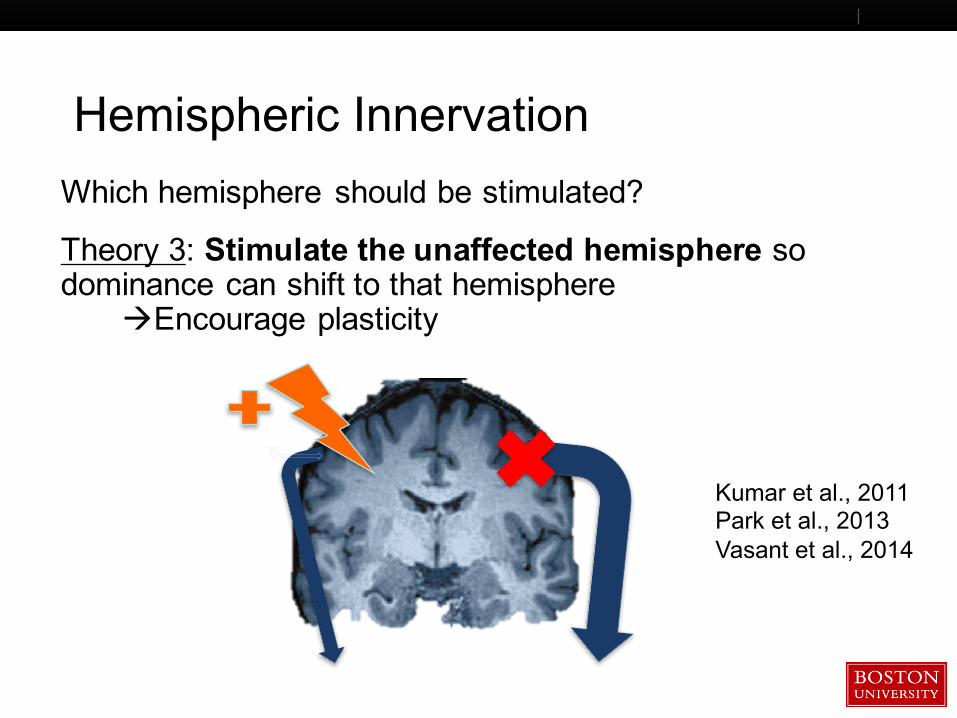
Hemispheric InnervationWhich hemisphere should be stimulated?
Kumar et al., 2011Park et al., 2013Vasant et al., 2014
Theory 3: Stimulate the unaffected hemisphere so dominance can shift to that hemisphere
àEncourage plasticity
Boston UniversitySlideshow Title Goes Here
Systematic Review and Meta-Analysis
Jessica Pisegna, 2015, Clinical Neurophysiology
Boston UniversitySlideshow Title Goes Here
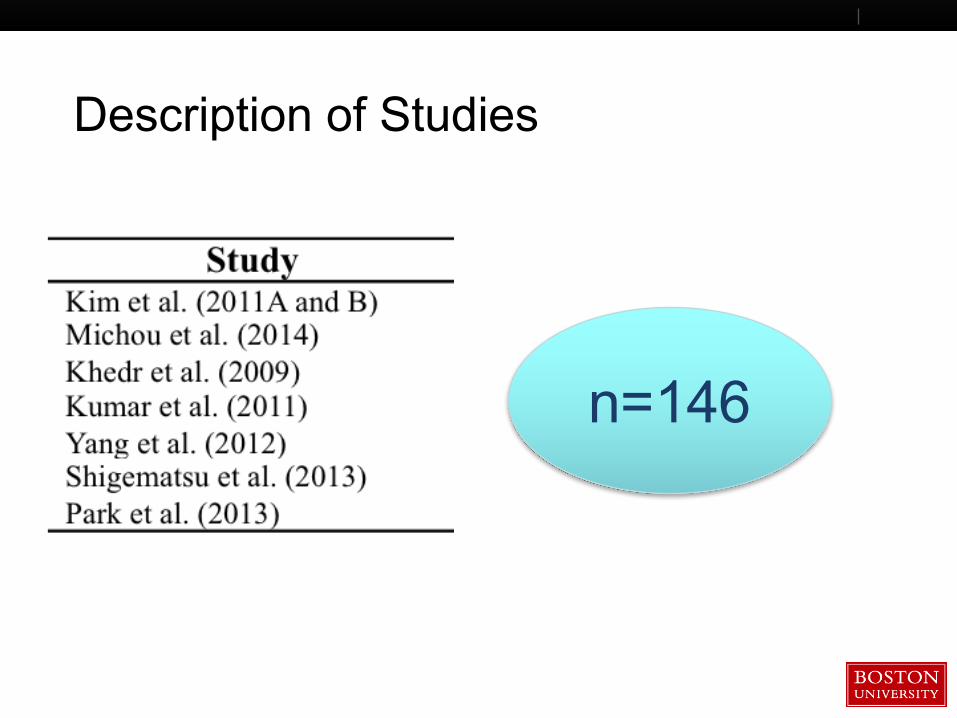
Description of Studies
n=146
Boston UniversitySlideshow Title Goes Here
Research Question
§ Does transcranial neurostimulation (tDCS, TMS, or rTMS) improve swallowing in patients with post-stroke dysphagia?
Boston UniversitySlideshow Title Goes Here
Overall, in these 8 trials,
transcranial neurostimulation improved dysphagia.
(Pooled ES=0.55;;
95% CI= 0.17, 0.93;; p=0.004)
Boston UniversitySlideshow Title Goes Here
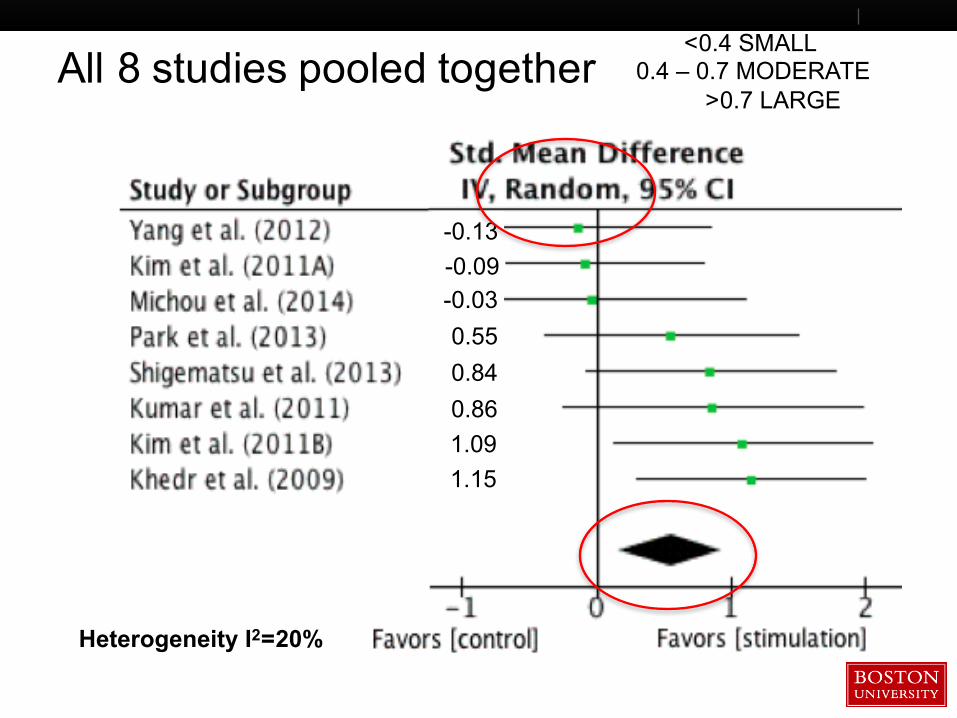
All 8 studies pooled together
-0.13-0.09-0.030.550.840.861.091.15
<0.4 SMALL 0.4 – 0.7 MODERATE
>0.7 LARGE
Heterogeneity I2=20%
Boston UniversitySlideshow Title Goes Here
tDCS vs. rTMS
§ Similar effect sizes (0.52, p=0.12 vs. 0.56, p=0.03)
§ Both were effective
Boston UniversitySlideshow Title Goes Here
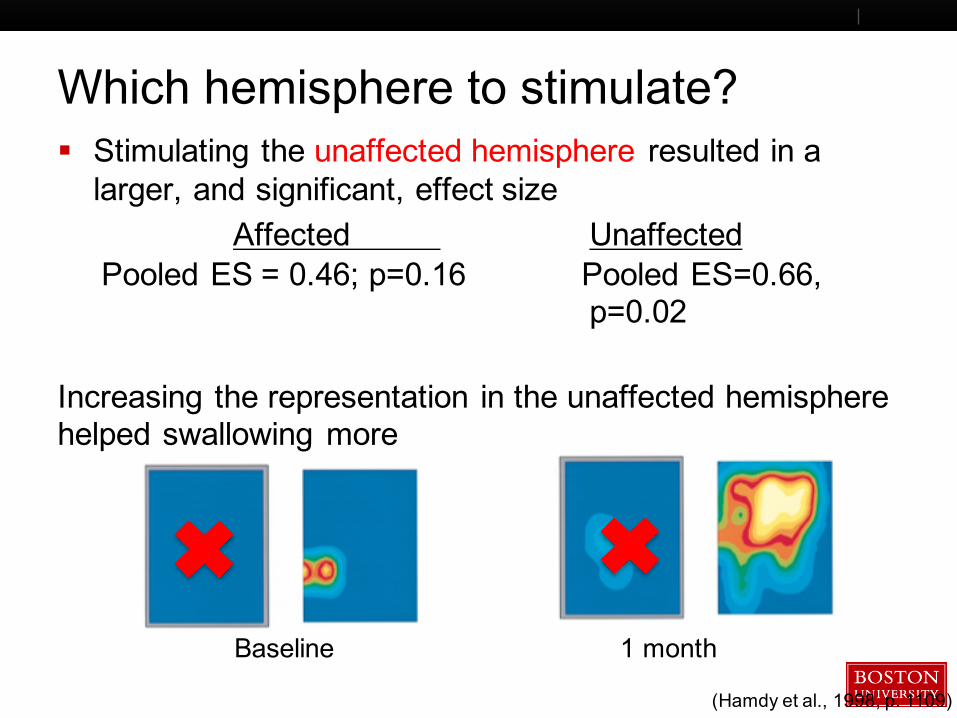
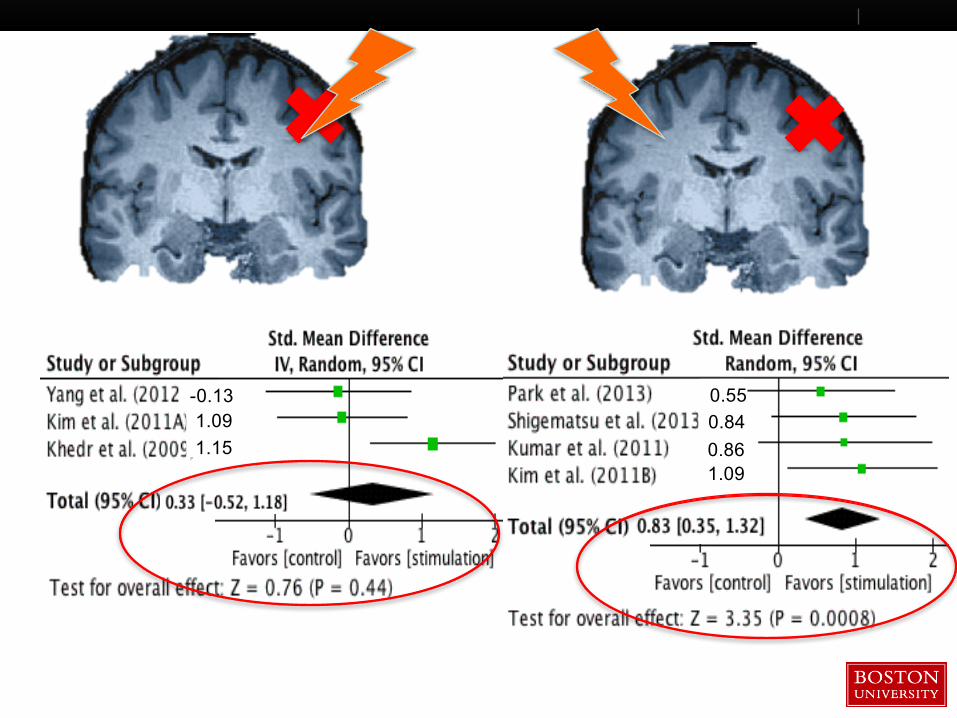
Which hemisphere to stimulate?§ Stimulating the unaffected hemisphere resulted in a larger, and significant, effect size
Affected Unaffected Pooled ES = 0.46;; p=0.16 Pooled ES=0.66,
p=0.02
Increasing the representation in the unaffected hemisphere helped swallowing more
(Hamdy et al., 1998, p. 1109)
Baseline 1 month
Boston UniversitySlideshow Title Goes Here
1.091.15
-0.13
1.09
0.55
0.860.84
Boston UniversitySlideshow Title Goes Here
Our Working Philosophy
Can a magnet, pair of wires and a battery can fix everything ?
Not really, more well designed studies are needed!!
Boston UniversitySlideshow Title Goes Here
Ongoing study in Boston: Fostering Eating After Stroke using tDCS (FEASt) Trial (Kumar, PI – Beth Israel)Aim: To determine safety and effect of 2 different doses of tDCS, compared to sham- in acute stroke patients with dysphagiaDesign: Randomized, sham-controlled clinical trial;;Stimulating the unaffected hemisphere
(NIH/NIDCD funded)
Boston UniversitySlideshow Title Goes Here
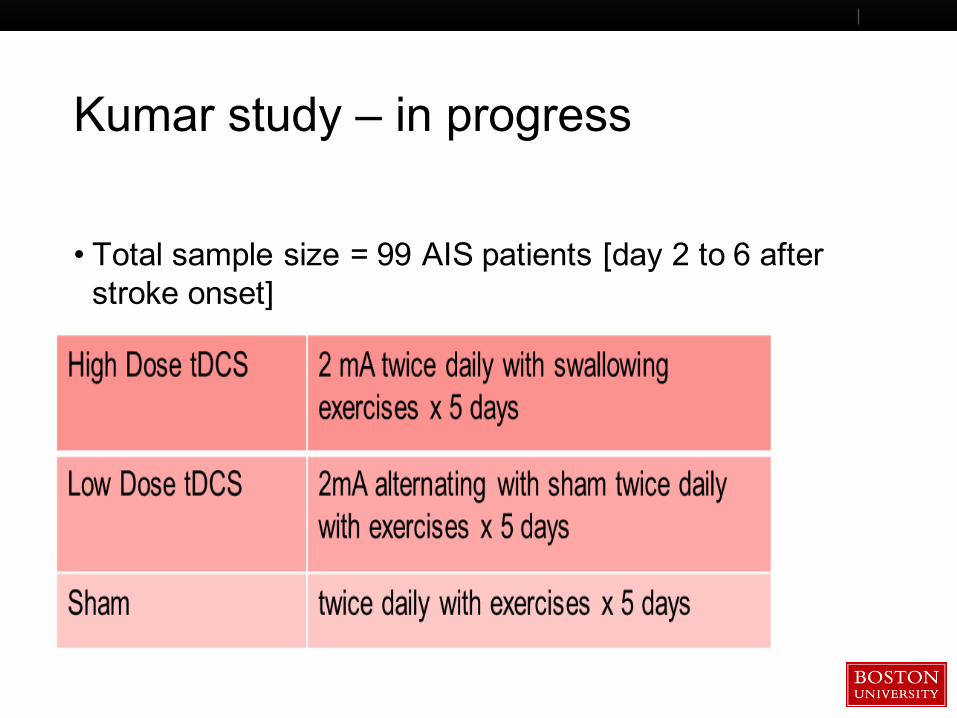
Kumar study – in progress
• Total sample size = 99 AIS patients [day 2 to 6 after stroke onset]
Boston UniversitySlideshow Title Goes Here
FEASt-Outcomes
• Primary efficacy outcome• change in PAS score
• Primary safety endpoints
Boston UniversitySlideshow Title Goes Here
Current Large RCT Clinical Trials
RCTRCT RCT
RCT
Boston UniversitySlideshow Title Goes HereSHOULD YOU USE BRAIN STIMULATION?
Not yetStill experimentalBUT Brain stimulation is very promising for stroke