Embed Size (px)
DESCRIPTION
A publication of the Georgia Regents University Departments Volume 10 | Issue 2
Citation preview

News aNd research from the departmeNts of Neurology aNd Neurosurgery at georgia regeNts NeuroscieNce center
NEUROSCIENCE OUTLOOK
STROKE: EXPLORING NOVEL THERAPIESBone marrow-derived stem cells promote recovery after stroke
VOL. 10 | ISSUE 2

2 NEUROSCIENCE OUTLOOK Volume 10 | Issue 2
Welcome to another expanded issue of Neuroscience Outlook from both the Neurosurgery and the Neurology departments. Our publication schedule has changed from twice a year to three times a year, i.e., every four months.
In this issue we feature news items from our departments, including the recent awards to the Neurology department for teaching, and to individual members of both departments for teaching, patient care, and research, respectively. Also newsworthy was a recent $66 million gift to the institution from one of the graduates of the Medical College of Georgia at Georgia Regents University. Additionally, William E. Mayher III, M.D., a 1970 graduate of the Neurosurgery department and board member of the MCG Foundation, was honored with a boardroom dedication and portrait unveiling.
In the research spotlight, we describe a variety of important clinical trials in acute stroke being conducted by our clinical faculty. In the clinical spotlight, we focus on minimally invasive surgery for lumbar disc disease and a minimally invasive approach to the clivus. The academic output of our departments is also chronicled.
Cargill H. Alleyne Jr., M.D.Professor and Marshall Allen Distinguished Chair of [email protected]/neurosurgery
David C. Hess, M.D.Professor and Presidential Distinguished Chair of [email protected]/neurology
A publication of the Georgia Regents University Departments of Neurology and Neurosurgery
Editor-in-chief: Cargill H. Alleyne Jr., M.D.Editor: Phil MalkinsonIllustrations: Colby Polonsky, M.S.Contributors: David C. Hess, M.D., Askiel Bruno, M.D., Jeffrey A. Switzer, D.O., Jonathan Tuttle, M.D., Arturo Solares, M.D., John Vender, M.D.
NEUROSCIENCE OUTLOOK
Cargill H. Alleyne Jr., M.D., and David
C. Hess, M.D.
FROM THE CHAIRMEN
DEPARTMENT NEWS
Unprecedented GiftMCG at Georgia Regents University receives $66 million gift The Medical College of Georgia at Georgia Regents University was fortunate to receive a $66 million gift from the late J. Harold Harrison, M.D. Dr. Harrison was a 1948 graduate of the Medical College of Georgia and a vascular surgeon from Kite, Ga. This gift, one of the largest ever received by a U.S. medical school, is directed to fund student scholarships and endowed chairs for faculty. Dr. Harrison and his wife have already contributed $10 million to the construction of a new Education Commons named in his honor.
award cornerThe Department of Neurology was awarded the Outstand-ing Clinical Science Teaching Department from the Class of 2013.
Three faculty members from the Neurosurgery and Neurology depart-ments (Drs. S. Dion Macomson, Elizabeth Sekul, and Jeffrey Switzer) won awards from the MCG faculty senate for teaching, patient care, and research, respectively.
Drug WarningStudy co-authored by faculty leads to FDA warningMorris Cohen, M.D., (Department of Neurology) was a co-author of a prospective NIH study of cognitive outcomes after fetal exposure to antiepi-leptic drugs [Fetal antiepileptic drug exposure and cognitive outcomes at age 6 years (NEAD Study): A Prospective Observational Study. Lancet Neurology, March 12 (3):244–252, 2013; the NEAD, now MONEAD, group]. Based upon this study, the FDA has placed a warning on Valproic acid use in the treatment of migraines in women who are pregnant.
Honored AlumnusNeurosurgery alumnus honored with Boardroom dedicationWilliam E. Mayher III, M.D., a retired neurosurgeon and 1964 graduate of MCG and 1970 graduate of the Department of Neurosurgery, was honored in April by the Medical College of Georgia Foundation with the dedication of an Executive Boardroom and a portrait unveiling. Dr. Mayher is a board member of MCG Foundation and was its former Chairman. He has provided many years of dedicated service to the institution and has been a great friend and contributor to the Department of Neurosurgery. His portrait was painted by Georgia Regents University Emeritus Associate Professor of Medical Illustration David Mascaro.
Phot
os b
y L.B
. Sch
nuck

3Volume 10 | Issue 2 gru.edu/neuro
The Neurosurgery department has always had strong international connections. Beginning in 2006, our faculty members have served as mentors for several visitors at varying levels of training (medical students, pre-residency fellows, practicing physicians, etc.) from a variety of countries around the world, including Haiti, El Salvador, Greece, India, Egypt, Saudi Arabia, Kuwait, and Pakistan. Within the last three years, Dr. Haroon Choudhri has performed complex spinal procedures on several international patients from the latter four countries as well as patients from Canada, Puerto Rico, Algeria, United Arab
Emirates, and Afghanistan. We expect the variety of international cases to expand in the future.
In addition, Georgia Regents University has recently collaborated with Jiangsu Province Department of Health in China for the purpose of enhancing collaboration in medicine, education, health science, and research. Specifically, an observership program will be established to facilitate the education of medical doctors and other health care professionals in this Chinese province. The department of Neurosurgery is one of a handful of departments that will participate in this program beginning in summer 2013.
International ConnectionsGRU Neurosurgery fosters collaboration with health care providers and patients from other countries
The map below shows the variety of nations from which GRU Neurosurgery faculty members have mentored health care providers and treated patients.

4 NEUROSCIENCE OUTLOOK Volume 10 | Issue 2
Minimally invasive spinal surgery provides the surgeon an alternative to open procedures for spinal disorders. The benefits ascribed to minimally invasive surgery include lower surgical blood loss, decreased length of stay, and lower risk of infection. A recent meta-analysis compared randomized controlled trials to determine the efficacy of open versus minimally invasive discectomies.1 The study results will be discussed after a short case.
A 36-year-old man presented with a four-month history of low back pain radiating down his left lower extremity to the heel and lateral aspect of his foot. He had been previously treated with NSAIDs, muscle relaxants, and ultimately epidural steroid injections, but they produced no relief. He underwent
a CT myelogram as he would not agree to an MRI of the lumbar spine. He also underwent EMG/NCV studies. His physical exam was significant for a left-sided straight leg raise and left ankle DTR ¼. The electrodiagnostic studies revealed a left S1 radiculopathy. His CT myelogram (figure 2) showed a left-sided disc herniation at L5-S1. A minimally invasive discectomy was planned after a discussion of the treatment options with the patient.
CLINICAL SPOTLIGHT
The surgery was done through an incision about 2.5 centimeters long and about 2.5 centimeters to the left of midline. Fluoroscopy was used to place the initial dilator tube and dilate up to the working channel. A K-wire was not used, because some believe its use increases the chance of a durotomy. The operating microscope was utilized (figures 3–6).
Minimally invasive spinal surgery
Evaluating the efficacy of minimally invasive discectomies versus open discectomies
by Jonathan Tuttle, M.D.
Figure 1. Muscle sparing approach showing the lamina that will be removed with a high speed drill.
Figure 2. CT myelogram of the lumbar spine showing a left-sided L5–S1 disc herniation with S1 nerve root compression.
Figure 3. Enhanced view of the lamina after removal of interlaminar paraspinal muscle.
Figure 5. The traversing root is identified.
Figure 4. Laminectomy being performed using a cylindrical coarse diamond drill bit.
Figure 6. The traversing root is retracted and the extruded disc is removed.

5Volume 10 | Issue 2 gru.edu/neuro
The surgery went well and the patient was discharged home later the same day. Immediately after surgery and at the initial follow-up visit six weeks later, he had complete resolution of his radicular pain. There was no durotomy and there was no evidence of a wound infection.
Dasenbrock et al. discussed the efficacy of minimally invasive discectomy (MID) compared to open discectomy (OD).1 They included six trials with a total of 837 patients (388 randomized to MID and 449 randomized to OD). The MID trials included one full endoscopy, and two trials with tubular retractor systems with a microscope. In the OD group, two trials did not use the microscope and the third trial randomized the patients to MID or OD. The OD in the third trial allowed a microscope or no microscope, based upon randomization.
The results showed a few statistically insignificant differences. Operative time in the OD trials was an average of five minutes shorter. Estimated blood loss was less in one OD trial whereas four MID trials reported less blood loss. Although rare, surgical site infections were noted to be higher in the three studies that recorded the data, all with an OD approach. Subsequent reoperation for recurrent disc herniation, also insignificant, was more common in the MID group.
Dasenbrock et al. reported one significant com-plication difference in their meta-analysis. The incidental durotomy rate was statistically higher in the MID group. They listed possible causes, including limited visualization, poor depth per-ception, and a steep learning curve; however, they noted “many of the incidental durotomies” came from the double- blinded study. In the double-blinded study, patients had a midline incision for either MID or OD, which the authors hypothesized could have limited visualiza-tion. With regards to the sequelae, persistent CSF leakage with subsequent reoperation was performed on two MID patients compared with three OD patients.
In regards to short- and long-term outcomes, Dasenbrock et al. reported the VAS scores were not significantly different between the MID and OD approaches. Likewise, the total complications were not significantly different between the two groups, MID versus OD. Ultimately, the results seem somewhat equivalent.
Figure 7. Sagittal illustration depicting a single incision for a two level bilateral hemilaminectomy.
Figure 8. Axial illustration depicting lumbar stenosis and a herniated disc as well as the decompression pathway visualized through the tube.
Figure 9. Axial view of a well decompressed
spinal canal after bilateral
laminectomies or discectomy through a unilateral approach.
1. Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A: The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized con-trolled trials. J Neurosurgery Spine. 16:452–62, 2012.

6 NEUROSCIENCE OUTLOOK Volume 10 | Issue 2
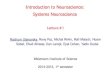
The clivus is composed of the posterior/inferior portion of the sphenoid bone and basilar portion of the occipital bone. This anatomic region separates the nasopharynx from the posterior cranial fossa. Clival lesions are of varied pathology and clinical behaviors. Their location and proximity to critical structures make operative management challenging.
At our institution, the endoscopic endonasal approach has been adopted for selected pathologies. The standard approach involves
a posterior septectomy, some degree of ethmoidectomy, and wide sphenoidotomies extending laterally to the level of the medial pterygoid plates. The sphenoid septations are then removed with the understanding that these may lead to the carotid canal. Finally, the sphenoid floor is removed to the level of the clival recess.
With this exposure completed, vital landmarks are now readily identifiable, including the medial and lateral opticocarotid recesses (OCR), the carotid protuberance within the parasellar space,
Minimally invasive approach to the clivus
CLINICAL SPOTLIGHT
Figure 1. Upper and middle clivus drilled-out. Pituitary remains in situ. AICA—Anterior inferior cerebellar artery; BA—Basilar artery; CN II—Optic nerve; CN III—oculomotor nerve; CN VI Abducens nerve; GC—Gasserian ganglion; ICA—Internal carotid artery; V1—Ophthalmic, V2—Maxillary, and V3—Mandibular branches of the trigeminal nerve
by Arturo Solares, M.D., John Vender, M.D., and Cargill H. Alleyne Jr., M.D.
Navigating the clivus with an endonasal transclival approach

7Volume 10 | Issue 2 gru.edu/neuro
the sellar face, clival recess, and strut of tuberculum bone overlying the superior intercavernous sinus (SIS). The clival dura is then exposed by drilling the posterior wall of the sphenoid sinus starting at the sella and working inferiorly. Adequate carotid exposure is paramount when the tumor extends laterally into the cavernous sinus. Following dural exposure and removal, the following structures are visualized (figures 1 and 2). This technique provides unparalleled visualization to lesions in the central skull base.
Figure 2. Upper and middle clivus drilled-out. Pituitary has been transposed to expose the interpeduncular fossa. BA—Basilar artery; CN III—oculomotor nerve; CN VI Abducens nerve; ICA—Internal carotid artery; PCA—Posterior cerebellar artery; SCA—Superior cerebellar artery
Cargill H. Alleyne Jr., M.D., (Department of Neurosurgery) gave an invited lecture (“Hereditary Hemorrhagic Telangiectasia: The Georgia Health Sciences
University Experience”) at the Southern Neurosurgical Society meeting in Sarasota, Fla., in February. He was also a panel member of a breakfast seminar (“The safe operating room environment: How do we make it safe for the patient?”) at the American Association of Neurological Surgeons meeting in New Orleans in April.
Darrell W. Brann, Ph.D., (Department of Neurology) was awarded a VA Merit review grant (Principal Investigator, with Krishnan Dhandapani, Ph.D.,
as co-investigator) entitled “Role of NADPH Oxidase in TBI” ( June 1, 2013–May 30, 2017).
Krishnan Dhandapani, Ph.D., (Department of Neurosurgery) was awarded an NIH/NINDS R03 grant (as co-investigator with John Vender, M.D.) entitled
“NLRP3 inflammasome and TBI” (July 1, 2013–June 30, 2015). He was also co-investigator on the grant awarded to Darrell Brann, Ph.D.
David C. Hess, M.D., (Department of Neurology) was an invited speaker at the Second International Conference on Regenerative
Medicine at the Vatican in April. His presentation was “Cell therapy of stroke and traumatic brain injury.”
Sergei A. Kirov, Ph.D., (Department of Neurosurgery) gave two invited lectures. The first (“Evolution of astroglial and neuronal disruption in stroke and TBI revealed
by in vivo two-photon imaging”) was at the Satellite Caribe Glia Symposium on Molecular Mechanisms of Neuron-Glia Interactions at Universidad Central del Caribe in San Juan, Puerto Rico in January. The second (“Neurons, astrocytes and microglia in early stroke and brain trauma”) was at the University of Virginia, Center for Brain Immunology & Glia (BIG) Seminar Series in Charlottesville, Va., in April.
S. Dion Macomson, M.D., (Department of Neurosurgery) was awarded an Exemplary Teacher Award by the MCG Faculty Senate.
Elizabeth Sekul, M.D., (Department of Neurology) was awarded a Patient Care Award by the MCG Faculty Senate.
Jeffrey Switzer, D.O., (Department of Neurology) was awarded a Distinguished Faculty Award for Clinical Science Research by the MCG Faculty Senate.
John Vender, M.D., (Department of Neurosurgery) was awarded an NIH/ NINDS R03 grant (as co-investigator with Krishnan Dhandapani,
Ph.D.) entitled “NLRP3 inflammasome and TBI” ( July 1, 2013–June 30, 2015).
FACULTY & STAFF UPDATES
NEUROSURGERYGeorgia Neurological
Surgery (in honor of William Ford, M.D.)
Mr. & Mrs. Lint Eberhardt
Mr. Kenneth DrakeRoyston Diagnostic
Center
THANKS TO OUR DONORS
Carol BachusSusan R. KayCargill H. Alleyne Jr., M.D.
NEUROLOGYMrs. Eileen V. BrandonNicholas Schlageter, M.D.Ms. Rachel ArnettALS Association of
GeorgiaMrs. Mary Ruth HaworthKapil Sethi, M.D.Georgia Power

8 NEUROSCIENCE OUTLOOK Volume 10 | Issue 2
trials, initiated by our local stroke experts.The MultiStem trial is a phase 2, randomized,
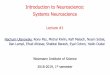
double-blind, placebo-controlled, dose-escalation trial of MultiStem®, intravenously-delivered allogeneic multipotent bone marrow stem cells for acute ischemic stroke. David Hess, M.D., Chairman of the Department of Neurology at GRU, is the principal investigator of MultiStem. This trial builds upon a substantial body of preclinical work at GRU and other institutions supporting the utility of cell-based therapies hours to days after stroke. Although the neurorestorative mechanisms of cell therapies are incompletely elucidated, MultiStem appears to work through an immunomodulatory effect, reducing the exodus of monocytes from the spleen to the site of brain injury that appear to aggravate the damage (figure 1). Further, it is encouraging that previous studies of multipotent bone marrow cells in myocardial infarction and graft-versus-host disease have demonstrated safety.
MultiStem is the first intravenously delivered allogeneic cell therapy to be tested in stroke, and it has several features that suggest potential generalizability to a substantial number of stroke patients. Targeting the “neurorestorative window,” patients are enrolled between 24 and 36 hours after stroke onset, and the inclusion criteria include recipients of tPA who have not had substantial improvement. In addition, since the cell source is allogeneic, as opposed to autologous, it can be prepared as an “off the shelf ” product, allowing for potential storage at most community hospitals.
A total of 136 subjects will be randomized. If MultiStem® is safe and there is a signal of efficacy, a late-stage phase 2b–3 trial is planned.
SHINE (Stroke Hyperglyecemia Network Effort) is a phase 3, randomized, blinded, multicenter trial that will determine the safety and efficacy of standard versus intensive glucose control with insulin in hyperglycemic acute ischemic stroke patients.
RESEARCH SPOTLIGHT
Stroke: Exploring novel therapiesInvestigator-initiated clinical trials in acute stroke seek to develop treatment strategies to promote recoveryby David C. Hess, M.D., Askiel Bruno, M.D., and Jeffrey Switzer, D.O.
Figure 1. These bone marrow-derived stem cells migrate to the spleen, where they prevent activation of splenocytes. They also reduce activation of other white blood cells, including lymphocytes.
A primary goal of the Georgia Regents Comprehensive Stroke Center is to develop novel therapies and treatment strategies to lessen the long-term disability from stroke. Toward this end, we are currently conducting three novel clinical

9Volume 10 | Issue 2 gru.edu/neuro
The trial is sponsored by the NIH (NINDS) and represents the collaboration of co-investigators from GRU (Askiel Bruno, M.D.), University of Virginia, and University of Texas Southwestern.
While hyperglycemia occurs commonly in acute ischemic stroke (~40 percent) and is associated with worse clinical outcomes, whether or not intensive glucose control with IV insulin improves clinical outcome is not established. Preclinical and clinical data have suggested potential benefit from tight glucose control in the setting of brain ischemia. However, these benefits must be balanced against the risks of hypoglycemia. In SHINE, 1,400 hyperglycemic acute ischemic stroke patients presenting within 12 hours of symptom onset will be randomly assigned to continuous IV infusion of insulin or standard therapy (sliding scale subcutaneous insulin) for three days (figure 2). This trial will provide important novel information about preferred management of acute ischemic stroke patients with hyperglycemia. It will determine the potential benefits and risks of intensive glucose control during acute stroke.
MACH (Minocycline in Acute Cerebral Hemorrhage) is an American Heart Association, SE Affiliate-sponsored pilot trial of minocycline for the treatment of intracerebral hemorrhage. Jeffrey Switzer, D.O., is the principal investigator. Unfortunately, there are currently no established effective treatments for intracerebral hemorrhage, a disease with a mortality of 40 percent and with few survivors who achieve long-term independence.
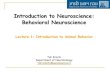
Following hemorrhage, blood constituents and their degradation products cause direct toxic injury to neurons and supporting tissue, and trigger a secondary inflammatory response. These pathways result in acute cell death, blood-brain barrier disruption, and edema, followed long-term by tissue loss and permanent neurologic deficits. Several key mediators, including matrix metalloproteinases (MMP-9), iron, and activated microglia/macrophages, have been identified. Minocycline, a so-called “dirty drug,” has been proposed as a putative therapy for hemorrhage patients. With a long track record as an antibiotic and several promising trials of neuroprotection in ischemic stroke, a short course of treatment should be safe and tolerable in intracerebral hemorrhage. Importantly, minocycline is a potent inhibitor of matrix metalloproteinases, an iron chelator, and suppresses the inflammatory response post-stroke (figure 3).
In this pilot study, we will determine whether minocycline reduces MMP-9, serum iron, and inflammation (IL-6) in ICH patients, and we will evaluate hemorrhage growth, perihematomal edema, and clinical outcome. Finally, an important additional rationale for studying minocycline in intracerebral hemorrhage is that if shown to be safe, it could be initiated in the pre-hospital setting (prior to neuroimaging and the differentiation of ischemic stroke from ICH), permitting ultra-early treatment and possibly increasing the likelihood of benefit for both ICH and ischemic stroke patients.
Figure 2 . When there is hyperglycemia, insulin is given either subcutaneously or intravenously during acute ischemic stroke for up to three days. These two treatment options will be compared according to functional outcomes.
Figure 3. Proposed pathophysiologic targets of minocycline in intracerebral hemorrhage

10 NEUROSCIENCE OUTLOOK Volume 10 | Issue 2
PUBLICATIONS & PRESENTATIONS
Vender JR, Youssef PPLateral skull base epidermoids, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:1448–1454
Rivner MHNerve excitability test, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:1840–1842
Rivner MHEvoked EMG, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:841–846
Strelzik J, Carroll JENeonatal intraventricular hemorrhage. MedLink Neurology Jan 29, 2013
Hess DC, Hoda MN, Bhatia KRemote limb preconditioning and postconditioning: Will it translate into a promising treatment for acute stroke? PMID: 2333996, Stroke 44:1191-7, 2013
Smitherman AD, Woodall MN, Alleyne CH, Rahimi SYOpen surgical management of a ruptured intracranial aneurysm in Klippel-Trenaunay-Weber syndrome. BMJ Case Reports, Jan 2013 [doi:10.1136/bcr-2012-0006857]
Samuel TA, Parikh, J, Sharma S, Giller CA, Sterling K, Kapoor S, Pirkle C, Jillella ARecurrent adult choroid plexus carcinoma treated with high-dose chemotherapy and syngeneic stem cell (bone marrow) transplant. J Neurol Surg A Cent Eur Neurosurg 1–6, 2013
Sword J, Masuda T, Croom D, Kirov SAEvolution of neuronal and astroglial disruption in the peri-contusional cortex of mice revealed by in vivo two-photon imaging.
Brain 136: 1446-1461, [Epub ahead of print; (2013) Mar 6], 2013
Meador KJ, Baker GA, Browning N, Cohen MJ, Bromley RL, Clayton-Smith J, Kalayjian LA, Kanner A, Liporace JD, Pennell PB, Privitera M, Loring DWFetal antiepileptic drug exposure and cognitive outcomes at age 6 years (NEAD Study): A Prospective Observational Study. Lancet Neurology 12:244-252, 2013
Switzer JA, Demaerschalk BM, Xie J, Liangyi F, Villa KF, Wu EQCost-effectiveness of hub-and-spoke telestroke networks for the management of acute ischemic stroke from the hospitals’ perspectives. Circ Cardiovasc Qual Outcomes 6:18-26, 2013
Howard G, Cushman M, Howard VJ, Kissela BM, Kleindorfer DO, Moy CS, Switzer J, Woo DRisk factors for intracerebral hemorrhage: The Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Stroke 44:1282-1287, 2013
Alleyne CHAngiography, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:167–172
Rivner MHTranscranial magnetic stimulation of facial nerve, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:2845–2847
Rivner MHMaximum stimulation test, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:1590–1592
Alleyne CHArteriovenous malformations, ed: Kountakis SE Encyclopedia of Otolaryngology, Head and Neck, Springer, 2013:186–191
Hartmann JEThe blink reflex, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:337–341
Hartmann JEElectromyography, ed: Kountakis SEEncyclopedia of Otolaryngology, Head and Neck, Springer, 2013:738–743
January–April 2013
Names in blue indicate faculty members in the Georgia Regents University Neurosurgery or Neurology department.
PUBLICATIONS
Afferent signals (blue) travel along the Trigeminal nerve (V1) to brainstem structures where it splits into direct (red) and indirect pathways (green) that exit via the facial nerve (CN VII) to the Orbicularis Oculi. Each pathway generates separate waveforms that can be recorded by specialized nerve stimulation techniques. (Hartmann JE, The blink reflex)

11Volume 10 | Issue 2 gru.edu/neuro
Kirov SAEvolution of astroglial and neuronal disruption in stroke and TBI revealed by in vivo two-photon imaging. Satellite Caribe Glia Symposium on Molecular Mechanisms of Neuron-Glia Interactions In Vivo and In Vitro.Universidad Central del Caribe, San Juan, Puerto Rico, January 2013
Alleyne CHHereditary Hemorrhagic Telangiectasia.The Georgia Health Sciences University Experience. Southern Neurosurgical Society Meeting, Sarasota, Fla., February 2013
Alleyne CHUpdate on subarachnoid hemorrhage and intracranial aneurysms.Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Bruno ATIA and Stroke: Clinical diagnosis and misdiagnosis. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Bruno ADecisions in the management of carotid artery disease. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Bruno AStroke in the young.
Management Update, Hilton Head, S.C., April 2013
Nichols FTEndovascular revascularization therapy update.Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Nichols FTPFOs: To close or not to close? and other evolving issues in cardioembolic stroke. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Ramesh S Contemporary management of
Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Hess DCThe borderlands of intravenous thrombolysis. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Hess DCThe challenge of psychogenic stroke. Comprehensive Stroke Management Update. Hilton Head, S.C., April 2013
Hess DCThe de-Alzheimerization of dementia: The role of ischemia in dementia.Comprehensive Stroke
intracerebral hemorrhage. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Switzer JAStroke Centers and Telestroke: An Evolving Landscape. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Switzer JAPFOs: Statin Controversy?: Separating the wheat from the chaff. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Switzer JA Special issues in atrial fibrillation and stroke. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Vender JRMalignant cerebral edema: from ventriculostomy to hemicraniectomy. Comprehensive Stroke Management Update, Hilton Head, S.C., April 2013
Alleyne CHSubarachnoid hemorrhage and unruptured intracranial aneurysms: Emphasis on diagnosis and early treatment plan. Primary Care and Family Practice Symposium, Augusta, Ga., April 2013
Alleyne CHThe safe operating room
environment: How do we make it safe for the patient? American Association of Neurological Surgeons Meeting, New Orleans, La., April 2013
Alleyne CH, Shields J, Kimbler DE, Dhandapani KMLipopolysaccharide upregulates aquaporin-4 expression in mouse cortical astrocytes via PI3K gamma-dependent mechanisms. American Association of Neurological Surgeons Meeting, New Orleans, La., April 2013 (poster)
Hess DCCell therapy of stroke and traumatic brain injury. Second International Conference on Regenerative Medicine, Vatican City, April 2013
Kirov SANeurons, astrocytes and microglia in early stroke and brain trauma. University of Virginia, Center for Brain Immunology & Glia (BIG) Seminar Series, Charlottesville, Va., April 2013
Viers A, Allen M, Alleyne CHHistorical vignette: George W. Smith, M.D. (1916–1964). American Association of Neurological Surgeons Meeting, New Orleans, La., April 2013 (poster)
PRESENTATIONS
Genealogical chart of a family with HHT treated at GRU. (Alleyne CH, Hereditary Hemorrhagic Telangiectasia)

CONFERENCE SCHEDULES
NON-PROFITUS POSTAGE
PAIDGEORGIA REGENTS
UNIVERSITY
GRU-003
Georgia Regents University1120 15th St., AD 1114Augusta, GA 30912
As a regional referral center for the Southeastern U.S., the Georgia Regents Neuroscience Center of Excellence includes the
area’s largest, most diverse team of adult and pediatric neurologists and neurosurgeons, including renowned experts in Parkinson’s disease, stroke, ALS, MS, functional and cerebrovascular neurosurgery, and complex spine surgery. To make an online referral, visit gru.edu/referral.
Neurosurgery Neurology
Upcoming Meetings
May–August 2013
Georgia Neurosurgical Society May 24–26, Sea Island, Ga.
Society of Neurological SurgeonsJune 8–11, Boston, Mass.
National Medical Association July 27–31, Toronto, Canada
Society of Neuro-Interventional Surgery July 29–Aug. 1, Miami, Fla.
May 2
All conferences are held from
8–9 am.
Karl Kieburtz, M.D. Assessing Progression in PD
May 9 Tom Swift, M.D. Case Presentation
May 16 Michael Rivner, M.D.
May 23 Christa Butler/ Jill Trumble PowerNote Training
May 30 Subhashini Ramesh, M.D.
June 6 Dagmara Pychynski, M.D.
June 13 Kent Posey, M.D.
June 20 Samer Kassar, M.D.
June 27 Tom Swift, M.D. Case Presentation
July 4 Independence Day Holiday No Grand Rounds
July 11 Kiawah Conference No Grand Rounds
July 18 J. Ned Pruitt II, M.D. Education Update
July 25 James Carroll
August 1 Ed Hartmann
August 8 Tom Swift Case Presentation
August 15 Anthony Murro
August 22 Elizabeth Sekul
August 29 Askiel Bruno
June 7
10–11 am Anatomy
11 am–noon Business Giller
noon–1 pm Case Conference
June 14
10–11 am Oral Board Review
11 am–noon Neuro 101 Doug Hughes
noon–1 pm Case Conference
June 21
10–11 am Radiology
11 am–noon Functional Giller
noon–1 pm Case Conference
June 28
10–11 am Resident Meeting
11 am–noon Journal Club
noon–1 pm M&M
July 12
10–11 am Oral Board Review
11 am–noon Neuro 101 Angela Viers
noon–1 pm Case Conference
July 19
10–11 am Radiology
11 am–noon Functional Giller
noon–1 pm Case Conference
July 26
10–11 am Resident Meeting
11 am–noon Journal Club
noon–1 pm M&M
August 211 am–noon Anatomy
noon–1 pm Case Conference
August 9
10–11 am Oral Board Review
11 am–noon Neuro 101 M. Woodall
noon–1 pm Case Conference
August 16
10–11 am Radiology
11 am–noon Functional Giller
noon–1 pm Case Conference
August 23
10–11 am Resident Meeting
11 am–noon Journal Club
noon–1 pm M&M