Embed Size (px)
Citation preview

http://nnr.sagepub.com/Repair
Neurorehabilitation and Neural
http://nnr.sagepub.com/content/27/3/208The online version of this article can be found at:
DOI: 10.1177/1545968312461715
2013 27: 208 originally published online 16 October 2012Neurorehabil Neural RepairMarousa Pavlou, Adolfo M. Bronstein and Rosalyn A. Davies
Vestibular DisordersRandomized Trial of Supervised Versus Unsupervised Optokinetic Exercise in Persons With Peripheral
Published by:
http://www.sagepublications.com
On behalf of:
American Society of Neurorehabilitation
can be found at:Neurorehabilitation and Neural RepairAdditional services and information for
http://nnr.sagepub.com/cgi/alertsEmail Alerts:
http://nnr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Oct 16, 2012OnlineFirst Version of Record
- Feb 20, 2013Version of Record >>
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

Neurorehabilitation and Neural Repair27(3) 208 –218© The Author(s) 2013Reprints and permission: http://www. sagepub.com/journalsPermissions.navDOI: 10.1177/1545968312461715http://nnr.sagepub.com
Clinical Research Articles
Introduction
Customized vestibular rehabilitation (VR) incorporating appropriate movements and sensory exposure is currently the standard of care for patients with peripheral vestibular disorders, with approximately 50% to 80% achieving sig-nificant subjective symptom, dynamic visual acuity, gait, and postural stability improvements.1-4 However, in per-sons with chronic peripheral vestibular disorders, visual vertigo (VV) symptoms do not always improve with cus-tomized exercises alone.5
Patients with a peripheral vestibular disorder may expe-rience dizziness, disorientation, and/or unsteadiness in situations involving visual-vestibular conflict (eg, walking down supermarket aisles) or intense visual motion (eg, watching wide-screen movies). Visual vertigo,6 space and motion dicomfort,7 and visually induced dizziness8 are terms used to describe these symptoms.
Patients with VV over-rely on visual cues for perception and postural responses (ie, visually dependent).9 It is believed that this factor contributes to poor vestibular com-pensation, especially in visual-vestibular conflict situations, where a mismatch exists between visual and vestibular input regarding movement and orientation.6,9
Customized VR promoting desensitization and increased tolerance to visual stimuli through optokinetic stimuli (OK) exposure provides greater benefit, improving dizziness,
461715 NNRXXX10.1177/1545968312461715Neurorehabilitation and Neural RepairPavlou et al2013© The Author(s) 2013
Reprints and permission: http://www.sagepub.com/journalsPermissions.nav
1King’s College London, London, UK2Imperial College London, London, UK3National Hospital for Neurology and Neurosurgery, London, UK
Corresponding Author:Rosalyn A. Davies, PhD, FRCP, Department of Neuro-Otology, National Hospital for Neurology and Neurosurgery, Queen Square, London WC1 3BG, UK Email: [email protected]
Randomized Trial of Supervised Versus Unsupervised Optokinetic Exercise in Persons With Peripheral Vestibular Disorders
Marousa Pavlou, PhD1, Adolfo M. Bronstein, MD, PhD, FRCP2, and Rosalyn A. Davies, MD, PhD, FRCP3
Abstract
Background. Visual vertigo (VV) symptoms improve only when customized vestibular rehabilitation (VR) integrates exposure to optokinetic stimuli (OK). However, equipment is expensive, biweekly sessions are not standard practice, and therapy is often unsupervised. Methods. A controlled, parallel-group comparison was made of patients’ responses to an 8-week customized program incorporating OK training via a full-field visual environment rotator (group OKF) or DVD (an optokinetic disc or drum rotating at 40° or 60° s−1), supervised (group OKS) or unsupervised (group OKU). A total of 60 participants with chronic peripheral vestibular symptoms were randomly allocated to 1 of 3 treatment groups: group OKF (n = 20) or OKS (n = 20), in which participants attended weekly sessions and were prescribed customized home exercises incorporating the DVD, or group OKU (n = 20) who practiced customized exercises and the DVD unsupervised. Treatment response was assessed at baseline and at 8 weeks with dynamic posturography, Functional Gait Assessment (FGA), and questionnaires for symptoms, symptom triggers, and psychological state. Results. No significant between-group differences were present at baseline or at post interventions. All groups showed significant within-group improvements for vestibular (ie, lightheadedness), VV, and autonomic symptoms (P < .05). Posturography and FGA improved significantly for groups OKF and OKS (P ≤ .01) as well as anxiety scores for group OKS (P < .05) and depression for group OKF (P < .05). Migraine significantly affected VV improvement (migraineurs improved more; P = .01). The drop-out rate was 55% for group OKU and 10% for each supervised group (P < .01). Conclusions. The DVD may be an effective and economical method of integrating OK into VR. However, rehabilitation should be supervised for greater compliance and improvements, particularly for postural stability and psychological state.
Keywords
vestibular rehabilitation, optokinetic stimulation, visual vertigo, migraine, supervision
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

Pavlou et al 209
postural instability, and particularly VV symptoms in patients with chronic vestibular symptoms.5 However, the semiweekly therapy sessions and equipment used (ie, in-house built, expensive) make transferring OK exposure into everyday clinical practice difficult. Many clinics lack access to high-tech OK equipment such as optokinetic discs or moving rooms.5 Wrisley and Pavlou10 reported that busy screen savers (eg, mazes), head-mounted displays, or a DVD that includes OK recorded from available clinical equipment could provide similar, although less intense, stimulation. However, the effectiveness of low-tech meth-ods has not been investigated.
A relationship between motion sickness and increased visual dependence also exists with a stronger influence of disorienting visual stimuli on verticality perception11 and an inability to accurately use available visual input to resolve conflicting sensory information.12 Approximately two-thirds of migraineurs are prone to motion sickness.13 Patients with peripheral vestibular dysfunction and migraine headache demonstrate significant physical performance and subjective symptom score improvements following VR.14 However, no studies in this patient cohort have investigated VV symptoms, tolerability of VR incorporating OK expo-sure, and its impact on outcome.
This study aims to compare treatment responses to a cus-tomized VR program incorporating OK exposure via a full-field visual environment rotator and/or limited-field-of-view DVD and assess the role of supervision and migraine head-ache on treatment outcome.
MethodsAllocation
Figure 1 summarizes the flow of participants through this randomized, controlled, parallel-group study. Participants were assigned to an 8-week customized exercise group incorporating OK training via (1) a full-field visual envi-ronment rotator (group OKF), (2) supervised DVD (group OKS), or (3) unsupervised DVD (group OKU). An inde-pendent person randomly allocated eligible patients to a treatment group via sequentially numbered opaque sealed envelopes. Each envelope contained an insert indicating the allocated treatment group (OKF, OKS, or OKU). The thera-pist and patient were informed of group allocation after completing the baseline assessment. Local ethics commit-tee approval was obtained.
ParticipantsBetween 2007 and 2009, 60 patients were recruited from neuro-otology clinics at the National Hospital for Neurology and Neurosurgery, Queen Square and Charing Cross Hospital, London, UK, after a complete neurological and
neuro-otological examination, including Hallpike posi-tional testing, pure tone audiogram, electronystagmogra-phy, and caloric testing. Inclusion criteria were (1) clinical diagnosis of a peripheral vestibular disorder, (2) chronic dizziness and/or unsteadiness, (3) 18 to 80 years old, and (4) previous VR program completed with partial/no improvement. Patients with (1) CNS involvement exclud-ing migraine; (2) fluctuating symptoms, for example, active Ménière disease; (3) orthopedic deficit affecting balance and gait; or (4) inability to attend sessions, were excluded. Patients with severe migraine (>3 migrainous headaches monthly) or untreated severe depression (Beck Depression Inventory score >29) were excluded. No significant between-group differences were noted for age, sex, or symptom duration (Table 1).
Patient diagnosis was based on clinical history and/or neuro-otological findings, according to published normal data and limits.16 All patients with benign paroxysmal posi-tional vertigo entered the study because of a persistent sense of imbalance and dizziness after the condition resolved. In patients with recurrent headaches, migraine was diagnosed if all 5 major International Headache Society criteria for migraine17 were met (Table 1); vestibular migraine was diagnosed if symptoms fit the Neuhauser criteria.18 Diagnoses, vestibular findings, and presence of migraine headache for each group are listed in Table 1. Similar to previous findings,19 50% of patients with chronic peripheral vestibular disorders had normal test results.
Sample CalculationSample size was calculated based on the anticipated aver-age score change for the Situational Characteristic Questionnaire (SCQ).5 Anticipating average outcome values (T
end − T
initial) of −1.2 (group OKF), −0.8 (group
OKS), and −0.4/4 (group OKU) with a common standard deviation of 0.6, 20 patients were required in each group. This was assuming 5% statistical significance, 80% power, a 20% drop-out rate, and adjustments for multiple comparisons.
Outcome MeasuresSubjective symptoms, balance, and gait were assessed at baseline and 8 weeks (end of treatment).
Balance and Gait MeasuresComputerized dynamic posturography. The Sensory Orga-
nization Test was performed according to a published protocol (Equitest; Neurocom International, Oregon). Composite scores range from 0% (no balance) to 100% (maximum stability); scores <70% are considered abnormal.20
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

210 Neurorehabilitation and Neural Repair 27(3)
Functional Gait Assessment (FGA21). This is a 10-item test based on the Dynamic Gait Index.22 The maximum score is 30; higher scores indicate better performance.
Self-report MeasuresAll participants completed validated questionnaires regard-ing symptoms, symptom triggers, and psychological state during the previous month, unless otherwise stated. The primary outcome measure is the SCQ; all other measures are secondary outcomes.
The SCQ7,9 measures frequency of symptom provoca-tion or exacerbation in environments with visual-vestibular
conflict or intense visual motion. Scores ≥0.7/4 indicate VV symptoms.23 The Vertigo Symptom Scale (VSS)24 assesses common vestibular (VSS-V; eg, lightheadedness, unsteadi-ness, and/or spinning) and autonomic/somatic anxiety (VSS-A; eg, heart pounding) symptoms. The Beck Depression Inventory25 assesses depressive symptoms experienced during the “past few days.” Composite scores ≤9 are normal; scores of 10 to 16 indicate mild to moderate depression, 17 to 29 moderate to severe depression, and 30 to 63 severe depression. The Beck Anxiety Inventory26 assesses anxiety level. Composite scores ≤7 indicate mini-mal anxiety, 8 to 15 mild anxiety, 16 to 25 moderate anxiety, and >26 severe anxiety.
♦♦
Drop-outs (n=11)Non-compliance (n=5)Unrelated lower back pain (n=1)Unknown reason (n=5)
Analysed:Baseline (n=20) Post-treatment (n=9; follow-up
data unavailable for drop-outs)
Assessed for eligibility (n=80)
Excluded (n=20) ♦ Not meeting inclusion criteria (n=9)
• >3 migraine headaches monthly (n=4)• Untreated severe depression (n=3)• Central vestibular disorder (n=2)
♦ Declined to participate (n=6)♦ Living too far away from clinic site (n=5)
Analysed:♦Baseline (n=20) ♦Post-treatment (n=18; follow-up data unavailable for drop-outs)
Drop-outs (n=2)♦ Non-compliance (n=1)♦ Chronic neck and shoulder painafter whiplash injury (n=1)
Group OKFAllocated to intervention (n=20)♦Received allocated intervention (n=20)
♦♦♦
Group OKUAllocated to intervention (n=20)
Received allocated intervention (n=20)♦
Analysis
Randomized (n=60)
Enrollment
Group OKSAllocated to intervention (n=20)♦ Received allocated intervention (n=20)
Drop-outs (n=2)♦ Non-compliance (n=1)♦ Chronic daily headache (n=1)
Allocation
Follow-up
Analysed:♦Baseline (n=20)♦Post-treatment (n=18; follow-up data unavailable for drop-outs)
Figure 1. Flow diagram of the study with regard to enrollment, allocation, follow-up, and analysis: All groups received customized vestibular rehabilitation incorporating optokinetic stimulation training via (1) a full-field visual environment rotator (group OKF), (2) supervised DVD (group OKS), or (3) unsupervised DVD (group OKU).
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

Pavlou et al 211
Treatment
Group OKF and OKS patients attended individual 45- minute weekly physical therapy sessions for 8 weeks and received customized exercises and DVDs with which to practice on days with no clinic attendance. Group OKU patients attended a physical therapy assessment and were provided with customized exercises and a DVD to practice unsupervised for 8 weeks. Treatment goals were (1) improvement of functional balance, gait, and ability to per-form daily activities; (2) decrease in symptom severity; and (3) patient education.
All patients in each group were given a diary to record frequency, duration, and symptom level for each custom-ized and DVD exercise practiced daily at home. The diary was reviewed at each session (groups OKF and OKS); group OKU patients were asked to bring it to the final assessment session.
Customized Exercise ProgramAll patients in every group received a customized home exercise program based on individual functional deficits (neuromuscular, musculoskeletal, and eye-head coordina-tion) and subjective symptoms. All patients practiced 3 to 5 exercises (examples Pavlou et al5) for 1 minute, twice daily, and the movement velocity progressively increased over
time. A structured program for gradually increasing daily activities and exposure to symptom-provoking environ-ments was provided.
At each supervised session for groups OKU and OKS, progress was assessed, any concerns discussed, exercises not yet included in the home program were practiced, and exercises were modified to gradually increase task diffi-culty. For Group OKU, the customized program included individual stages of increasing task difficulty where each exercise was to be stopped and replaced with one from the next stage, when practiced symptom free for three consecu-tive days to ensure it consistently failed to provoke symptoms.
Optokinetic TrainingOptokinetic DVD (all groups). The DVD comprises 13 ses-
sions, lasting 2 minutes each, in which an optokinetic disc (Figure 2A) or drum rotates (Figure 2B) at constant veloci-ties or sinusoidally, with peak velocities of 40° or 60° s−1. The drum’s stripes are positioned vertically or horizontally. Exercises were divided into progressive levels (beginner, intermediate, and advanced). Patients were instructed to look at the disc’s center, or “stare” ahead in the case of the optokinetic drum. At beginner and intermediate levels, patients practiced this sitting and standing 1 and 0.5 m from the screen but with alternating repetitions of 10 vertical and
Table 1. Participant Characteristics at Baseline
Variable OKF (n = 20) OKS (n = 20) OKU (n = 20)
Age, mean (range), y 47.5 (30-70) 49.3 (28-73) 46 (33-62)Sex, n (%) Female 16 (80) 15 (75) 15 (75) Male 4 (20) 5 (25) 5 (25)Symptom duration, mean (range), mo 75.5 (11-300) 84.9 (8-600) 113.6 (9-600)Presence of migraine, n (%) 10 (50) 10 (50) 13 (65)Diagnosis, n
VN 7 5 4VM 6 9 9BPPV (+VM) 1 2 (1) 1 (1)BVH (+M) 2 2 1 (1)Posttraumatic dizziness (+M) 0 (2) 0 0Acoustic neuroma (+M) 0 0 0 (1)MDS15 (+M) 0 (2) 1 1 (1)
Vestibular findings, nCP 5 6 6BPPV 1 3 2BVH 2 2 2No abnormal findings 12 9 10
Abbreviations: OKF, full-field visual environment rotator group; OKS, supervised DVD group; OKU, unsupervised DVD group; VN, idiopathic peripheral vestibular disorder, compatible with a history of past vestibular neuritis; VM, vestibular migraine according to Neuhauser criteria; M, meets IHS diagnos-tic criteria for migraine; BPPV, benign paroxysmal positional vertigo; BVH, idiopathic bilateral vestibular hypofunction; VV, visual vertigo; MDS, motorist disorientation syndrome15; CP, canal paresis.
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

212 Neurorehabilitation and Neural Repair 27(3)
horizontal head movements at the intermediate level. The advanced level involved watching the video while walking forward/backward without and then with vertical and hori-zontal head movements or in tandem. For home practice, all groups received the same instruction sheet. In week 1, patients watched 4 optokinetic disc and 2 drum (horizontal stripe) sequences; 2 further sequences were added weekly until all sequences were watched once daily.
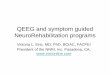
Optokinetic ball (group OKF). An externally illuminated rotating ball (Stimulopt, Framiral, Cannes, France; Figure 3A) covered with 1-cm reflective metal square pieces, induced a pattern of full-field, multiple rotating white squares (width 12 cm; Figure 3B). An external LED source, whose exact positioning could be adjusted to change pro-jection intensity and accuracy, illuminated the ball. Images
were projected by the ball positioned 2.33 m away from a white semicircular wall (area 3.26 m2, height 2.37 m). Exercises with head stationary or while performing various head (vertical and horizontal) movements in sitting or standing 1 and 0.5 m from the wall or while walking along-side or toward/away from it were practiced as the ball rotated clockwise, counterclockwise, or vertically at angu-lar velocities between 6° and 30° s−1, which were the equip-ment’s minimum and maximum velocities. Patients were instructed to constantly look ahead and try “to stare through the image avoiding following the images with your eyes.” These instructions were provided for two reasons: (1) optic flow desensitization and (2) because by following the images, an optokinetic nystagmus response with a gain of one, a nauseogenic stimulus26, would be generated. This additional stimulus combined with the effect of optic flow may provoke a severe level of symptoms preventing the patient from continuing the session.
Peak velocity discrepancies between the DVD and optoki-netic ball relate to each device’s specifications. The DVD was originally developed as an additional form of OK stimulation for home use on days with no clinic attendance in an earlier study5 and was recorded at the aforementioned velocities.
Exercise progression during supervised sessions (groups OKF and OKS). At the first session, a maximum of 4 optoki-netic ball (group OKF) or DVD (group OKS) sequences (2 horizontal clockwise and counterclockwise sequences at minimum and maximum velocities) were watched sitting 1 m from the wall/screen. Typically, 2 additional exercises were practiced at each session progressively increasing to 14 exercises. Each exercise lasted 2 minutes, followed by a minute’s break and was stopped if a participant felt unable to continue because of nausea/dizziness or symptoms verbally graded at 1 minute were reported as moderate or severe. No exercises were practiced until symptoms sub-sided to nil or mild. If no symptoms were induced, the exercise was progressed to the next level and/or OKS velocity increased in 5° increments (group OKF only). For group OKS, DVD exercises during supervised sessions were at a more advanced level than those practiced at home. All participants in both groups progressed.
AnalysisSPSS 17 (SPSS Inc, Chicago, Illinois) was used for statisti-cal analysis. Data are presented as mean ± SD. Between-group differences were determined using the Kruskal-Wallis test. Within-group differences pre intervention (baseline) and post intervention (week 8) were analyzed using Wilcoxon signed rank tests. Mann-Whitney U tests com-pared baseline data between migraineurs and nonmi-graineurs. The Pearson χ2 test compared the relationship between treatment group and completion rate. Preliminary screening with Spearman bivariate correlations enabled the
Figure 2. Still images from DVD optokinetic stimuli. A. Still image from an optokinetic drum sequence rotating clockwise at 40° s−1. B. Still image from an optokinetic disc sequence rotating counterclockwise at 60° s−1. Exercises while watching the DVD are divided into a progressive sequence where patients are asked to look at a particular area of the moving image while sitting or standing at varying distances from the screen or during walking toward and away from the screen with and without head movements.
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

Pavlou et al 213
selection of covariates (age, symptom duration, and migraine) and a fixed factor (sex) to be tested with analysis of covariance (ANCOVA) models of ranked data; only sig-nificant covariate and fixed-factor effects are reported. Spearman correlation assessed the relationship between pretreatment and post treatment changes for objective and self-report measures and for the relationship between psy-chological symptoms and drop-out rate.
ResultsBaseline data for all participants (60) showed no signifi-cant differences between treatment groups or study com-pleters (45) and noncompleters (15). At baseline, migraineurs experienced significantly greater autonomic/somatic anxiety symptoms compared with nonmigraineurs (U = 289; z = −2.327; P < .05; Figure 3B). No significant relationship was noted between sex, symptom duration, completion rate, baseline data, and treatment outcome.
Balance and Gait MeasuresPosturography. At baseline, 73.3% of scores were abnor-
mal (group OKF, n = 15; group OKS, n = 17; group OKU, n = 12). Within-group improvements (Table 1) were noted only for groups OKF (Z = −3.66; P < .01) and OKS (Z = −2.72; P = .01). In group OKF, 94% of patients improved and in group OKS, 78%. No significant between-group dif-ferences were noted (Table 2).
Patients with bilateral vestibular hypofunction (BVH) were unable to maintain balance in conditions 5 and 6 where vestibular cues play a major role; they did, however, show improvements of 19 and 11 points for group OKF, 17 and 7 points for group OKS, and 16 and 8 for group OKU. They
were included in the analysis because their removal did not significantly alter findings.
Functional Gait Assessment. A significant within-group improvement was noted for groups OKF (Z = −3.62; P < .01) and OKS (Z = −3.73; P < .01); group OKU showed a trend toward significance (Z = −1.90, P = .06; Table 2). No significant between-group differences were noted (Table 2). All group OKF and OKS patients and 89% of group OKU patients improved. Age had a significant effect on FGA baseline scores (poorer performance in older patients; F(1, 41) = 48.01, P < .01) and outcome (greater change for older patients; F
(1, 41) = 9.14, P < .01).
Questionnaires. No significant between-group differences were noted. All groups showed significant within-group improvements for VSS-S (group OKF: Z = −2.70, P < .01, 67% of patients improved; group OKS: Z = −2.94, P < .01, 78%; group OKU: Z = −2.38, P < .05, 78%), VSS-A (group OKF: Z = −2.42, P < .05, 72%; group OKS: Z = −2.86, P < .01, 78%; group OKU: Z = −1.97, P = .05, 78%), and SCQ (group OKF: Z = −3.16, P < .01, 89%; group OKS: Z = −3.59, P < .01, 89%; group OKU: Z = −2.49, P = .01, 89%). Only group OKF showed a significant within-group improvement for depression scores (Z = −2.59, P = .01, 61%), and group OKS showed a similar improvement for anxiety scores (Z = −2.62, P = .01, 78%). Descriptive data and statistics are displayed in Table 2.
At baseline, scores indicated mild depression for 5 patients in group OKF and 6 in group OKS and group OKU and mod-erate depression for 3, 4, and 6 patients in groups OKF, OKS, and OKU, respectively. No patient score indicated severe depression because this was an exclusion criterion. Individual baseline scores denoted (1) mild anxiety for 6, 7, and 3 patients; (2) moderate anxiety for 3, 6, and 5 patients; and (3) severe anxiety for 6, 4, and 7 patients in groups OKF, OKS,
Figure 3. Apparatus used for the “high-tech” full-field simulator-based intervention. A. A photo of the visual environment rotator apparatus (Stimulopt, Framiral, France). B. Participants are asked to stare ahead while the apparatus rotates in different directions and at differing speeds. Participants practice exercises while sitting, standing, and walking either toward and away from the stimulus or alongside it with or without sagittal or horizontal head movements.
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

214 Neurorehabilitation and Neural Repair 27(3)
and OKU, respectively. No correlation was noted between psychological symptoms at baseline and dropout.
When collapsing all patients’ scores independent of group, anxiety score improvements correlated with SCQ
improvement (r = 0.34; P < .05). VSS-A improvements sig-nificantly correlated with both SCQ (r = 0.34; P < .05) and VSS-S (r = 0.33; P < .05) improvement.
Migraine had a significant effect on pre-post treatment SCQ (F
(1, 41) = 7.50, P = .01; Figure 4A) and VSS-A (F
(1, 41)
= 7.39, P = .01; Figure 4B) change, whereby migraineurs showed greater improvement. Baseline scores indicated elevated SCQ scores for 100% and 89% of patients with and without migraine, respectively; 100% of migraineurs and 82% of nonmigraineurs improved.
Participation and dropout. A significant relationship was noted between treatment group and completion rate: χ²(2, n = 60) = 14.40; P < .01. The drop-out rate was 10% for groups OKF (noncompliance = 1; chronic neck and shoulder pain after whiplash injury = 1) and OKS (non-compliance = 1; chronic daily headache, present prior to participation in study = 1). The drop-out rate was 55% for group OKU (noncompliance = 5; unrelated lower back injury = 1; unknown reason [patients neither attended final assessment nor replied to e-mail/telephone messages or postal letters] = 5).
DiscussionThis study compared the effects of (1) a full-field rotating visual environment (group OKF) versus a DVD, (2) super-vised (groups OKF and OKS) versus unsupervised reha-bilitation (group OKU), and (3) treated migraine on treatment outcome. A major finding was the 55% drop-out rate for group OKU compared with only 10% for both supervised groups. Within-group analysis showed FGA, posturography, and psychological state significantly improved only for supervised treatment with a significant interaction noted between age and FGA results. Migraine had a significant effect on VV and autonomic symptoms, with migraineurs showing, surprisingly, greater improve-ment. The discussion is separated into (1) postural stability
Table 2. Mean (SD) of Outcome Measures
Measure
OKF OKS OKU
Baseline, n = 20
Posttreatment, n = 18
Baseline, n = 20
Posttreatment, n = 18
Baseline, n = 20
Posttreatment, n = 9
Posturography 58.7 (19.9) 71.5 (10.0)** 53.6 (18.8) 67.3 (11.6)** 52.6 (27.4) 56.4 (24.0)FGA 19.8 (6.1) 26.4 (2.8)** 19.5 (6.6) 26.0 (4.2)** 19.9 (6.3) 22.6 (8.9)SCQ 2.2 (1.1) 1.6 (1.0)** 2.4 (0.8) 1.6 (0.9)** 2.3 (0.9) 1.5 (1.1)**VSS-V 1.1 (0.8) 0.8 (0.9)** 1.4 (0.7) 0.7 (0.5)** 1.0 (0.8) 0.5 (0.5)*VSS-A 1.5 (0.8) 1.1 (0.7)* 1.4 (0.8) 1.0 (0.6)** 1.3 (0.5) 1.0 (0.7)*BDI 9.2 (7.8) 6.1 (5.1)** 10.5 (6.9) 8.4 (6.0) 11.9 (7.9) 9.2 (9.6)BAI 18.0 (11.9) 13.6 (10.9) 19.2 (12.1) 12.0 (6.7)** 19.0 (12.2) 16.1 (18.0)
Abbreviations: SD, standard deviation; OKF, full-field visual environment rotator group; OKS, supervised DVD group; OKU, unsupervised DVD group; FGA, Functional Gait Assessment; SCQ, Situational Characteristics Questionnaire; VSS-V, Vertigo Symptom Scale (global vertigo symptoms); VSS-A, Ver-tigo Symptom Scale (autonomic and somatic anxiety symptoms); BDI, Beck Depression Inventory; BAI, Beck Anxiety Inventory.a*P ≤ .05, ** P ≤ .01; indicate significant improvement compared with baseline.
A
B
0
1
2
3
4
SCQ
ave
rage
sco
re
†
Pre Post0
1
2
3
VSS
-A a
vera
ge s
core
Time
Figure 4. Mean and standard deviation of (A) Situational Characteristic Questionnaire (SCQ) scores for assessment of visual vertigo symptoms and (B) Vertigo Symptom Scale autonomic/somatic anxiety (VSS-A) scores pretreatment and posttreatment for patients with peripheral vestibular dysfunction without (black bars) and with (gray bars) history of migraine headache. “†” Indicates a significant difference between groups (P < .05).
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

Pavlou et al 215
and gait, (2) subjective symptoms, (3) psychological state, and (4) migraine and treatment outcome.
Postural Stability and GaitCurrent results resemble findings showing improved posturography scores following customized VR with or without OK exposure for patients with unilateral vestibu-lar hypofunction or BVH,1,2,5 although the latter remained unable to maintain balance in conditions relying on ves-tibular cues. As findings are similar to those reported following VR without OK stimulation,1,5 we hypothesize that posturography improvements are primarily a result of the former rather than the latter. As previously reported, approximately 30% of patients had normal posturography scores, and no correlation was noted with outcome measures related to symptom frequency, intensity, and/or triggers, or psychological state.5
Only groups receiving supervision achieved significant within-group posturography and FGA improvements. Outcome measures detecting a minimal clinically important difference (MCID) over time are necessary in determining an intervention’s efficacy.28 The MCID for posturography is 10 points in young adults with concussion29 and 7 points in patients with multiple sclerosis.30 Although this has not been established for the FGA, it has been reported as an average 6-point improvement based on clinical experi-ence.31 Both supervised groups achieved the MCID for both measures, regardless of whether they received full- or limited-field-of-view OK exposure, unlike group OKU, which did not. We believe lack of supervision contributed to the findings for group OKU. Frequent assessment allows the timely introduction of more challenging balancing tasks and ensures that exercises are correctly performed,2 a crucial element of supervised therapy, particularly when considering the implications of posttreatment FGA scores for group OKU.
Reduced gait speed is associated with reduced capacity in functional activities.32 The FGA includes timed walking at speeds required to safely cross a street (0.5 m/s)33 and many tasks necessary for functional mobility.34 Group OKU’s posttreatment FGA score indicates that gait speed and performance on tasks such as walking with head movements remains impaired. Furthermore, group OKU’s posttreatment score is just above the cutoff (22/30) for classifying fall risk and predicting unexplained falls in community-dwelling older adults,34 whereas scores for both supervised groups improve to normal ranges.
Age significantly influenced FGA results, with older patients showing poorer baseline performance, as previ-ously noted using the Dynamic Gait Index,35 as well as greater pre-post treatment change, because of a greater capacity for change resulting from poorer baseline scores. The findings emphasize the value of balance rehabilitation for older patients; however, final scores as noted in other
work36 remained significantly lower for older adults, indi-cating that they continue to perform worse on complex gait tasks.
Subjective SymptomsOur results agree with work showing that customized VR incorporating OK exposure significantly improves dizzi-ness, postural instability, psychological state, and particu-larly VV symptoms in patients with chronic vestibular symptoms.5 However, this is the first study comparing customized VR, incorporating full- or limited-field-of-view OK exposure, supervised and unsupervised.
It is hypothesized that improvements are based on neu-ral adaptability. Optokinetic stimulation induces adaptation of specific vestibular parameters, including postrotational vestibular sensation and vestibular ocular reflex gain in primates, chronic peripheral vestibular patients, and/or healthy individuals.37-40 Recently, short-term repeated exposure to visuovestibular exercises was found to induce adaptive changes, improving the magnitude of visual dependence in healthy controls.41 Although the current study did not directly measure this, we believe that VV improvements are the result of a decreased overreliance on visual input for perceptual and postural responses. In turn, the underlying mechanism is likely to relate to motion-induced changes in neuronal excitability in visual motion cortical areas (V5/MT).42
PET scans and functional MRI studies involving small- or large-field OK stimulation without additional vestibular stimulation note activation in cortical areas related to visual motion processing and eye movement control and deacti-vation of parietoinsular vestibular cortices, indicating a reciprocally inhibitory visual-vestibular interaction.43-45 Similarly, when multisensory vestibular cortex areas are stimulated, bilateral deactivation is noted in visual and somatosensory cortex areas.43 It is suggested that these interactions have a functional significance and indicate a sensory reweighting process with greater weight given to the more reliable input, thus suppressing the possible mis-match between contrasting sensory information.45 Recurring exposure to conflicting visual input, as in our study, is also believed to promote reduced visual reliance and foster a more effective use of vestibuloproprioceptive cues through sensory reweighting.46
Parameters that include frequency, velocity, texture, stimulus area, and position within the visual field influence postural response amplitudes and illusory perceptions of self-motion (ie, vection).47-49 Furthermore, small-field OK stimulation induces steady optokinetic nystagmus, whereas large-field stimulation induces vection, during which increased activity has been noted in, or close to, the cere-bellar nodulus.44 Despite these differences and varying OK parameters used in various studies,43-45,50 both small- and large-field OK stimulation show similar reciprocally
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

216 Neurorehabilitation and Neural Repair 27(3)
inhibitory visual-vestibular interactions, indicating that sensory reweighting occurs independent of visual field size and other aforementioned factors. This may explain why we noted significant VV improvements, both with full- and limited-field-of-view OK stimulation without significant between-group differences.
Because group OKF also viewed the DVD on days with no clinic attendance, it appears that there is no greater ben-efit to incorporating once weekly full-field OK exposure into VR programs. Earlier work5 included twice weekly full-field OK exposure incorporating various stimuli, and average VV improvements were greater compared with current results. Our inclusion of migraineurs cannot account for the difference because migraine had a positive effect on VV outcome. It may be that full-field OK expo-sure frequency or stimulus variety contributed to previous findings, but this cannot be confirmed, and further work is required.
Psychological StatePsychological symptoms are common in patients with peripheral vestibular disorders.51 It is unclear why within-group depression scores improved significantly only for group OKF and anxiety scores only for group OKS. However, the lack of psychological state change in group OKU is unambiguous and unsurprising. Supervision is believed to implicitly improve psychological status (eg, increasing confidence, providing reassurance, and emphasizing positive effects of VR).2 Our findings appear to indicate a direct relationship between supervision, motivation, and compliance, with an unacceptable 55% drop-out rate for the nonsupervised group.
Poor exercise compliance is a well-recognized problem across clinical populations, with reports of up to 70%.52 Reasons for noncompliance are multifactorial,52 including perceived barriers (ie, lack of time), lack of positive feed-back, support, and particularly motivation for unsupervised programs. In Ménière disease patients, the main reasons for noncompliance with an unsupervised VR program were symptom severity or aggravation by therapy with a similar, albeit higher rate than ours, at 62.5%.53
However, autonomic/somatic anxiety improvement significantly correlated with both VV and VSS-S improve-ments, whereas anxiety score improvements related only to VV improvements. Therefore, supervision, its associ-ated psychological effects, and subjective symptom improvements appear to influence improvement of psy-chological variables.5
Many similarities, including addressing distressing symptoms and functional impairments, promoting habitua-tion, gradual exposure to symptoms and provoking situa-tions, and challenging negative beliefs, exist between VR and cognitive-behavioral therapy (CBT).54 Studies compar-ing VR with explicit CBT with waiting-list controls or no
control group demonstrate improvements in patients’ cop-ing ability, function, symptoms, and care satisfaction.55 However, the clear additional effect of combining CBT with VR remains unknown.
All groups continue to indicate mild anxiety posttreat-ment, which may partly relate to the observation that anxi-ety and psychiatric problems often exist prior to vestibular disorder onset.51 Mild remaining VV symptoms posttreat-ment may have also influenced final anxiety scores.
Migraine and Treatment OutcomeCurrent results agree with findings reporting that patients with vestibular dysfunction and migraine history can adhere to and benefit from VR.14,56 The new finding is that patients with treated migraine also tolerate structured OK exposure, and migraine history does not influence the drop-out rate. Subjective vestibular symptoms and psychological state improvements were similar in migraineurs and nonmi-graineurs, and migraine history, as previously reported,56 did not influence postural and gait responses. However, migraine significantly affected VV and autonomic/somatic anxiety scores.
Migraineurs showed significantly elevated baseline autonomic/somatic anxiety scores. However, scores improved significantly with a greater pre-post treatment change compared with nonmigraineurs. Our work differs from studies demonstrating significant improvements in all Dizziness Handicap Inventory (DHI) scores apart from the emotional subscale in persons with migraine-associated dizziness14 and less improvement in the self-perception of dizziness in persons with peripheral vestibular dysfunction and migraine.56 We believe that the discrepancy with cur-rent findings is a result of the OK exposure and resulting VV improvements noted, which significantly correlated with VSS-A and anxiety score improvements. Participant numbers were insufficient to compare patients with vestibu-lar migraine with those with migraine headache and other etiologies in regard to their symptoms of unsteadiness and/or dizziness. The analysis included all patients with migraine because removing the latter did not alter findings.
Baseline VV symptoms were significantly elevated and similar for migraineurs and nonmigraineurs. Studies show-ing increased visual cortical excitability both in patients with BVH50 and migraineurs57 support these findings. In migraineurs, this response persists during the interictal state58 and is further enhanced in patients with chronic daily headache,59 which may explain why the patient with this diagnosis could not complete the study.
As OK exposure increases migraineurs’ symptoms,60 they would be expected to perform less well. However, a higher percentage of migraineurs reported VV improve-ments that were significantly greater compared with those for nonmigraineurs. Previous authors suggested that medication may help control VV symptoms in migraineurs
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

Pavlou et al 217
enabling better exercise tolerance.14 All participants with >3 migraines per month had been treated with prophylactic medication prior to commencing the study. Medication though was not controlled for, apart from no patients changing medication during the study, and therefore, its role in VV improvements cannot be clarified.
ConclusionThe visual motion DVD may be an economical, clinic friendly, and effective method of incorporating OK expo-sure into VR programs. Patients with migraine can tolerate and benefit from OK exposure. However, supervision promotes greater compliance and improvements in pos-tural stability and psychological state. Future research should investigate optimal treatment duration, stimulus, long-term benefit, and the role of medication, particularly for VV improvements in vestibular patients with migraine.
Acknowledgments
The authors would like to thank Dr Bernard Cohen for his guid-ance in using the optokinetic ball and Mr Peter Milligan for statis-tical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
1. Brown KE, Whitney SL, Wrisley DM, Furman JM. Physical therapy outcomes for persons with bilateral vestibular loss. Laryngoscope. 2001;111:1812-1817.
2. Black FO, Angel CR, Pesznecker SC, Gianna C. Outcome analysis of individualized vestibular rehabilitation protocols. Am J Otol. 2000;21:543-551.
3. McGibbon CA, Krebs DE, Parker SW, Scarborough DM, Wayne PM, Wolf SL. Tai Chi and vestibular rehabilitation improve vestibulopathic gait via different neuromuscular mechanisms: preliminary report. BMC Neurol. 2005;5:3.
4. Schubert MC, Migliaccio AA, Clendaniel RA, Allak A, Carey JP. Mechanism of dynamic visual acuity recovery with vestib-ular rehabilitation. Arch Phys Med Rehabil. 2008;89:500-507.
5. Pavlou M, Lingeswaran A, Davies RA, Gresty MA, Bronstein AM. Simulator based rehabilitation in refractory dizziness. J Neurol. 2004;251:983-995.
6. Bronstein AM. Visual vertigo syndrome: clinical and pos-turography findings. J Neurol Neurosurg Psychiatry. 1995;59: 472-476.
7. Jacob RG, Lilienfeld SO, Furman JMR, Durrant JD, Turner SM. Panic disorder with vestibular dysfunction: further
clinical observations and description of space and motion pho-bic stimuli. J Anxiety Disord. 1989;3:117-130.
8. Bisdorff A, Von Brevern M, Lempert T, Newman-Toker DE. Classification of vestibular symptoms: towards an interna-tional classification of vestibular disorders. J Vestib Res. 2009;19:1-13.
9. Guerraz M, Yardley L, Bertholon P, et al. Visual vertigo: symptom assessment, spatial orientation and postural control. Brain. 2001;124:646-656.
10. Wrisley DM, Pavlou M. Physical therapy for balance disor-ders. Neurol Clin. 2005;23:855-874, vii-viii.
11. Yardley L. Contribution of somatosensory information to per-ception of the visual vertical with body tilt and rotating visual field. Percept Psychophys. 1990;48:131-134.
12. Bijveld MM, Bronstein AM, Golding JF, Gresty MA. Nau-seogenicity of off-vertical axis rotation vs. equivalent visual motion. Aviat Space Environ Med. 2008;79:661-665.
13. Baloh RW. Neurotology of migraine. Headache. 1997;37:615-621. 14. Whitney SL, Wrisley DM, Brown KE, Furman JM. Physi-
cal therapy for migraine-related vestibulopathy and ves-tibular dysfunction with history of migraine. Laryngoscope. 2000;110:1528-1534.
15. Page NG, Gresty MA. Motorist’s vestibular disorientation syndrome. J Neurol Neurosurg Psychiatry. 1985;48:729-735.
16. Davies RA, Luxon LM. Dizziness following head injury: a neuro-otological study. J Neurol. 1995;242:222-230.
17. International Headache Society Classification Subcommittee. International classification of headache disorders, 2nd edition. Cephalalgia. 2004;24:1-160.
18. Neuhauser H, Leopold M, von Brevern M, Arnold G, Lempert T. The interrelations of migraine, vertigo, and migrainous ver-tigo. Neurology. 2001;56:436-441.
19. Herzog N, Allum JH, Probst R. Follow-up of caloric test response after acute peripheral vestibular dysfunction. HNO. 1997;45:123-127.
20. Equitest system Version 7.0. The sensory organization test. In: Data Interpretation Manual. Clackamas, OR: Neurocom International, Inc; 1999.
21. Wrisley DM, Marchetti GF, Kuharsky DK, Whitney SL. Reli-ability, internal consistency, and validity of data obtained with the functional gait assessment. Phys Ther. 2004;84:906-918.
22. Shumway-Cook A, Woollacott MH. Motor Control: Theory and Practical Applications. Baltimore, MD: Lippincott Wil-liams & Wilkins; 1995.
23. Pavlou M, Davies RA, Bronstein AM. The assessment of increased sensitivity to visual stimuli in patients with chronic dizziness. J Vestib Res. 2006;16:223-231.
24. Yardley L, Masson E, Verschuur C, Haacke N, Luxon L. Symptoms, anxiety and handicap in dizzy patients: development of the Vertigo Symptom Scale. J Psychosom Res. 1992; 36:731-741.
25. Beck AT, Steer RA. Manual for the Beck Depression Inven-tory. San Antonio, TX: Psychological Corporation; 1993.
26. Leyfer OT, Ruberg JL, Woodruff-Borden J. Examination of the utility of the Beck Anxiety Inventory and its factors as
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from

218 Neurorehabilitation and Neural Repair 27(3)
a screener for anxiety disorders. J Anxiety Disord. 2006;20: 444-458.
27. Stern RM, Hu S, Anderson RB, Leibowitz HW, Koch KL. The effects of fixation and restricted visual field on vec-tion-induced motion sickness. Aviat Space Environ Med. 1990;61:712-715.
28. Guyatt G, Walter S, Norman G. Measuring change over time: assessing the usefulness of evaluative instruments. J Chronic Dis. 1987;40:171-178.
29. Broglio SP, Ferrara MS, Sopiarz K, Kelly MS. Reliable change of the sensory organization test. Clin J Sport Med. 2008;18:148-154.
30. Hebert JR, Corboy JR, Manago MM, Schenkman M. Effects of vestibular rehabilitation on multiple sclerosis-related fatigue and upright postural control: a randomized controlled trial. Phys Ther. 2011;91:1166-1183.
31. Alsalaheen BA, Mucha A, Morris LO, et al. Vestibular reha-bilitation for dizziness and balance disorders after concussion. J Neurol Phys Ther. 2010;34:87-93.
32. Whitney SL, Wrisley DM, Brown KE, Furman JM. Is percep-tion of handicap related to functional performance in persons with vestibular dysfunction? Otol Neurotol. 2004;25:139-143.
33. Robinett CS, Vondran MA. Functional ambulation velocity and distance requirements in rural and urban communities: a clinical report. Phys Ther. 1988;68:1371-1373.
34. Wrisley DM, Kumar NA. Functional gait assessment: concur-rent, discriminative, and predictive validity in community-dwelling older adults. Phys Ther. 2010;90:761-773.
35. Marchetti GF, Whitney SL. Construction and validation of the 4-item dynamic gait index. Phys Ther. 2006;86:1651-1660.
36. Herdman SJ, Hall CD, Delaune W. Variables associated with outcome in patients with unilateral vestibular hypofunction. Neurorehabil Neural Repair. 2012;26:151-162.
37. Grunfeld EA, Okada T, Jáuregui-Renaud K, Bronstein AM. The effect of habituation and plane of rotation on vestibular perceptual responses. J Vestib Res. 2000;10:193-200.
38. Shelhammer M, Tiliket C, Roberts D, Kramer PD, Zee DS. Short-term vestibulo-ocular reflex adaptation in humans II: error signals. Exp Brain Res. 1994;100:328-336.
39. Szturm T, Ireland DJ, Lessing-Turner M. Comparison of different exercise programs in the rehabilitation of patients with chronic peripheral vestibular dysfunction. J Vestib Res. 1994;4:461-479.
40. Miles FA, Eighmy BB. Long-term adaptive changes in pri-mate vestibulo-ocular reflex: I. Behavioral observation. J Neurophysiol. 1980;43:1406-1425.
41. Pavlou M, Quinn C, Murray K, Spyridakou C, Faldon M, Bronstein AM. The effect of repeated visual motion stimuli on visual dependence and postural control in normal subjects. Gait Posture. 2011;33:113-118.
42. Guzman-Lopez J, Silvanto J, Seemungal BM. Visual motion adaptation increases the susceptibility of area V5/MT to phos-phene induction by transcranial magnetic stimulation. Clin Neurophysiol. 2011;122:1951-1955.
43. Dieterich M, Bense S, Stephan T, Yousry TA, Brandt T. fMRI signal increases and decreases in cortical areas during small-field optokinetic stimulation and central fixation. Exp Brain Res. 2003;148:117-127.
44. Kleinschmidt A, Thilo KV, Büchel C, Gresty MA, Bronstein AM, Frackowiak RS. Neural correlates of visual-motion perception as object- or self-motion. Neuroimage. 2002;16: 873-882.
45. Brandt T, Bartenstein P, Janek A, Dieterich M. Reciprocal inhibitory visual-vestibular interaction: visual motion stimu-lation deactivates the parieto-insular vestibular cortex. Brain. 1998;121:1749-1758.
46. Shumway-Cook A, Horak FB. Rehabilitation strategies for patients with vestibular deficits. Neurol Clin. 1990;8:441-455.
47. Post RB. Circular vection is independent of stimulus eccen-tricity. Perception. 1988;17:737-744.
48. Redfern MS, Furman JM. Postural sway of patient with vestibular disorders during optic flow. J Vestib Res. 1994;4: 221-230.
49. Stoffregen TA. Flow structure vs. retinal location in the opti-cal control of stance. J Exp Psychol Hum Percept Perform. 1985;11:554-565.
50. Dieterich M, Bauermann T, Best C, Stoeter P, Schlindwein P. Evidence for cortical visual substitution of chronic bilat-eral vestibular failure (an fMRI study). Brain. 2007;130: 2108-2116.
51. McKenna L, Hallam RS, Hinchcliffe R. The prevalence of psychological disturbance in neuro-otology outpatients. Clin Otolaryngol. 1991;16:452-456.
52. Sluijs EM, Kok GJ, van der Zee J. Correlates of exercise com-pliance in physical therapy. Phys Ther. 1993;73:771-782.
53. Yardley L, Kirby S. Evaluation of booklet-based self- management of symptoms in Ménière disease: a randomized controlled trial. Psychosom Med. 2006;68:762-769.
54. Biedel DC, Horak FB. Behavior therapy for vestibular rehabilitation. J Anxiety Disord. 2001;15:121-130.
55. Andersson G, Asmundson GJ, Denev J, Nilsson J, Larsen HC. A controlled trial of cognitive-behavior therapy combined with vestibular rehabilitation in the treatment of dizziness. Behav Res Ther. 2006;44:1265-1273.
56. Wrisley DM, Whitney SL, Furman JM. Vestibular rehabili-tation outcomes in patients with a history of migraine. Otol Neurotol. 2002;23:483-487.
57. Aurora SK, Wilkinson F. The brain is hyperexcitable in migraine. Cephalalgia. 2007;27:1442-1453.
58. Antal A, Polania R, Saller K, et al. Differential activation of the middle-temporal complex to visual stimulation in migraineurs. Cephalalgia. 2011;31:338-345.
59. Chen WT, Wang SJ, Fuh JL, Lin CP, Ko YC, Lin YY. Persis-tent ictal-like visual cortical excitability in chronic migraine. Pain. 2011;152:254-258.
60. Drummond PD. Motion sickness and migraine: optokinetic stimulation increases scalp tenderness, pain sensitivity in the fingers and photophobia. Cephalalgia. 2002;22:117-124.
at AZIENDA USL MODENA on February 22, 2013nnr.sagepub.comDownloaded from