Embed Size (px)
Citation preview
www.elsevier.com/locate/schres
Schizophrenia Research 71 (2004) 323–330
Neuropsychological correlates of symptom
profiles in first episode schizophrenia
Sara Lucasa, Dianne Fitzgeralda, M. Antoinette Redoblado-Hodgea,*,Josephine Andersona, Mark Sanbrookb, Anthony Harrisc,d, John Brennana
aDepartment of Child and Adolescent and Family Psychiatry, Westmead Hospital, Institute Road, Westmead NSW 2145, AustraliabDepartment of Psychological Medicine, Nepean Hospital, Australia
cDiscipline of Psychological Medicine, University of Sydney, AustraliadPrevention Early Intervention and Recovery Service, Western Sydney Area Health Service, Australia
Received 10 February 2004; received in revised form 19 March 2004; accepted 19 March 2004
Available online 30 April 2004
Abstract
This paper aimed to examine the relationship between the trichotomous symptom structure of psychopathology and
neuropsychological functioning in young people with first episode schizophrenia (FES), most of whom were receiving atypical
antipsychotic medication. This was with a view to providing insight into the underlying pathophysiology of the clinical
symptoms of schizophrenia. Fifty-three young people (aged 13–25 years) with FES participated in the study. Subjects
completed a comprehensive clinical and neuropsychological examination. Cognitive domain scores were correlated with
composite scores relating to Disorganisation, Psychomotor Poverty and Reality Distortion. A significant association was
identified between Disorganisation and Verbal Acquisition, Verbal Recall and Cognitive Flexibility. There were no significant
associations between cognitive domains and either Reality Distortion or Psychomotor Poverty, nor with measures of depressive
symptomatology. The present study provides preliminary evidence that symptoms associated with the Disorganisation factor are
significantly associated with cognitive deficits suggesting impaired frontal– temporal functioning. Differences between the
current findings and those of similar research may reflect the effects of different medication regimes, as well as the absence of
illness chronicity.
D 2004 Elsevier B.V. All rights reserved.
Keywords: First episode schizophrenia; Reality Distortion; Disorganisation; Psychomotor Poverty
1. Introduction the severity and pattern of cognitive deficits (Adding-
Neuropsychological studies of individuals with
schizophrenia have found considerable variability in
0920-9964/$ - see front matter D 2004 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2004.03.006
* Corresponding author. Tel.: +61-2-9845-6577; fax: +61-2-
9891-5690.
E-mail address: [email protected]
(M.A. Redoblado-Hodge).
ton et al., 2003; Bilder et al., 2000; Hoff et al. 1992;
Mohamed et al., 1999), reflecting in part the clinical
heterogeneity of the disorder. Attempts to reduce the
clinical complexity of schizophrenia have focused on
grouping symptoms into domains of psychopatholo-
gy, which are thought to reflect separate underlying
pathophysiological processes (Buchanan and Carpen-
ter, 1994). Of these, Liddle’s (Liddle, 1987a, 1989)

S. Lucas et al. / Schizophrenia Research 71 (2004) 323–330324
three -syndrome model of Reality Distortion (delu-
sions and hallucinations), Disorganisation (thought
disorder, inappropriate affect.) and Psychomotor Pov-
erty (poverty of speech, flat affect, decreased sponta-
neous movement) has found consistent support from
subsequent factor analytic studies (Bilder et al., 1985;
Peralta et al., 1992; Thompson and Meltzer, 1993;
Norman et al., 1997). Liddle postulated that the three
syndromes reflected discrete patterns of cerebral mal-
function, with Psychomotor Poverty associated with
left prefrontal dysfunction, Disorganisation with right
prefrontal dysfunction and Reality Distortion with
temporal lobe abnormalities. Further, examination of
this relationship in 47 patients with chronic schizo-
phrenia confirmed an association between Psychomo-
tor Poverty and decreased abstract reasoning, and
between Disorganisation and impaired attention and
new learning. However, Reality Distortion failed to
reveal significant associations with neuropsychologi-
cal impairment (Liddle, 1987b). Subsequent attempts
to replicate these findings in chronic schizophrenia
populations have provided mixed results, with some
studies corroborating Liddle’s findings (Baxter and
Liddle, 1998; Niewenstein et al., 2001), whereas
others have yielded contrary results (Williams, 1996;
Norman et al., 1997; O’Leary et al., 2000; Malla et al.,
2001).
This disparity in findings may reflect methodo-
logical variability between studies, and also raises
the question of whether findings from chronic
schizophrenia populations reflect primary effects re-
lated to the illness itself, or secondary effects of
long-term conventional antipsychotic treatment
(which has been shown to have detrimental effects
on cognition) (Sharma, 1999; Harvey and Keefe,
2001).
As a consequence, recent studies have focused on
the neuropsychological correlates of symptoms in first
episode psychosis (FEP). However, findings remain
mixed due to differences in sample selection, phase of
illness (acute or stabilised) and range of cognitive
functions assessed. For instance, Verdoux et al. (1999)
employed a positive–negative symptom dichotomy,
and found a significant association between positive
symptoms and poor verbal fluency, but no correlation
between negative symptoms and cognition in a sam-
ple of 34 FEP patients with a broad range of diagno-
ses. In contrast, a recent study of 94 FES subjects in
remission from acute symptoms and prescribed atyp-
ical antipsychotics, revealed several significant corre-
lations between Psychomotor Poverty and deficits in
speed of information processing, memory, visuospa-
tial abilities and executive functions. No associations
were found between Disorganisation or Reality Dis-
tortion syndromes and cognitive functioning (Bilder et
al., 2000). An earlier attempt to examine relationships
between cognitive function and positive, negative and
Disorganisation symptoms in 60 recent-onset adoles-
cent patients found that only symptoms of Disorgani-
sation and depression significantly correlated with
executive functioning (Van der Does et al., 1993),
whereas more recently, Joyce et al. (2002) failed to
identify any significant results between the three-
syndrome model and tests of executive functioning
in a sample of FES patients.
In summary, previous research into the neuropsy-
chological correlates of symptoms provides a con-
fusing picture which has been confounded by the
effects of medication (typical versus. atypical anti-
psychotics), chronicity of illness, depressive symp-
toms, population sample bias and phase of illness
(acute Vvs. stabilised). To address these problems,
the present study aimed to examine the relationships
between the trichotomous symptom structure and a
wide selection of neuropsychological domains in an
ecologically valid sample of young individuals with
FES, either unmedicated or receiving atypical anti-
psychotic medication.
2. Method
2.1. Participants
Participants were recruited as part of the Western
Sydney First Episode Psychosis Project. Inclusion
criteria for entry into the project were: (1). age from
13 to 25 years inclusive; (2). first contact with mental
health services with psychotic symptoms (prior contact
for non-psychotic problems was acceptable); (3). pres-
ence of psychotic symptoms as defined by hallucina-
tions, delusions, formal thought disorder or prominent
negative symptoms present for a minimum of 3three
days. Exclusion criteria included: (1). treatment with
electroconvulsive therapy in the six 6 months prior to
referral;, (2). gross neurological disease;, (3). devel-
S. Lucas et al. / Schizophrenia Research 71 (2004) 323–330 325
opmental delay (IQ < 75); or a (4). history of head
injury causing unconsciousness for at least one1 hour.
The 53 participants included in the present study
consisted of those diagnosed with either schizophre-
nia (n = 41), schizophreniform disorder (n = 11) or
schizoaffective disorder (n = 1) according to the Di-
agnostic and Statistical Manual of Mental Disor-
ders—Fourth Edition (APA, 1994), by consensus of
at least three fully qualified psychiatrists. At the time
of assessment, 47 (89%) individuals were prescribed
atypical antipsychotics with a mean chlorpromazine-
equivalent dose of 269 mg/day (S.D. = 192 mg/day),
and 6 were not prescribed any antipsychotic medica-
tion. Chlorpromazine -equivalents were calculated
using Lambert, (1999) methodology. Of those pre-
scribed antipsychotic medication, 4 (9%) participants
were also prescribed a mood stabiliser [(Llithium
[(n = 2) and Ssodium Vvalproate ([n = 2)]). In addi-
tion, 7 (13%) participants were receiving an antide-
pressant (5 SSRI, 2 tricyclic), 1 (2%) was prescribed
benzodiazepines and 3 (6%) were taking low dose
anticholinergics (benztropine) in conjunction with
antipsychotic medication. Table 1 presents the demo-
graphic details of the patient group.
Normative data from31 healthy control subjectswas
obtained during the same period that clinical patients
were assessed, and collected under the same conditions.
Control subjects within the age and educational level
range of the clinical group were recruited from local
high schools, vocational education centres and a first-
year undergraduate psychology course. In addition to
the exclusion criteria applicable to FEP subjects, con-
Table 1
Demographic and clinical characteristics for the first episode
schizophrenia (FES) group
FES
Mean S.D.
Age (years) 19.1 3.3
Education (years) 10.8 2.0
Estimated premorbid IQa 96.9 11.5
PANSS scores
Positive scale 17.6 5.8
Negative scale 19.0 5.5
General scale 39.4 8.5
Calgary depression scale 4.8 3.8
Young mania rating scale 9.3 6.3
a Wide Range Achievement Test, 3rd Edition—Standard Score.
trol subjects were excluded if they reported any per-
sonal or family history of mental illness. The healthy
control group’s cognitive performance on neuropsy-
chological assessment was used as an ecologically and
culturally valid normative data set, against which to
calculate z-scores for the clinical group.
2.2. Measures
The presence and severity of psychotic symptoms
was evaluated by interview, using the Positive and
Negative Syndrome Scale (PANSS; Kay et al., 1986).
Symptom clusters for Psychomotor Poverty, Disorga-
nisation and Reality Distortion were calculated by
summing the appropriate PANSS item scores, accord-
ing to the method derived by Harris et al. (1999). The
following items were combined for each symptom
cluster:
Psychomotor Poverty: blunted affect, emotional
withdrawal, social withdrawal, poor rapport, lack
of spontaneity.
Disorganisation: conceptual disorganisation, gran-
diosity, excitement, lack of abstract thinking.
Reality Distortion: suspiciousness, delusions, hos-
tility, hallucinatory behaviour.
The Calgary Depression Scale (Addington et al.,
1990) was also administered to provide information
on depressive symptomatology.
Comprehensive neuropsychological evaluation
was also undertaken. Selected measures from individ-
ual tests included in the battery were grouped into 10
cognitive domains based on findings from previous
meta-analytic research (Heinrichs and Zakzanis,
1998) and a priori assessment of content validity.
Table 2 displays the neurocognitive tests administered
and the individual measures included in each cogni-
tive domain. Due to the age range of participants in
the study, child ( < 16 years 11 months) and adult (>16
years 11 months) versions of individual tests within
the neuropsychological battery were administered as
appropriate.
To limit the confounding effects of acute symp-
tomatology and conceptual disorganisation on test
performance, assessments were commenced when
FES patients had achieved stabilisation of acute
symptoms, as indicated by a score of less than < 5

Table 2
Neuropsychological domains
Domain Tests
Current
intellectual
ability
Full scale IQ score [Wechsler Adult
Intelligence Scale, 3rd edition (WAIS-III)
(Wechsler, 1997a) or Wechsler Intelligence
Scale for Children (WISC-III) (Wechsler, 1991)]
Attention/
vigilance
Hits [Conners’ Continuous Performance Test
(CPT) Conners, 1995]
d’ (CPT)
Digits forward (span) (WAIS-III/WISC-III)
Failure to maintain set [Wisconsin Card
Sorting Test (WCST) (Heaton et al., 1993)]
Working
memory
Working memory index score [Wechsler
Memory Scale, 3rd edition (WMS-III)
(Wechsler, 1997b)] or freedom from
distractibility index score (WISC-III)
Verbal
acquisition
Logical memory I (WMS-III; Wechsler,
1997b) or stories I (Children’s memory
scale (CMS); Cohen, 1997)
Trials 1–5 total score [Rey Auditory
Verbal Learning Test (RAVLT) (Spreen and
Strauss, 1998)]
Verbal recall Logical memory II (WMS-III) or stories
II (CMS)
Trial 7 (RAVLT)
Visual recall 30 min delayed recall [Rey Complex Figure
Test (RCFT) (Spreen and Strauss, 1998)]
Faces II (WMS-III or CMS)
Visuospatial Block design (WAIS-III or WISC-III)
ability RCFT copy score
Cognitive Preservative errors (WCST)
flexibility Number of categories achieved (WCST)
Trail making test—Part B (Spreen and Strauss,
1998)
Verbal fluency FAS total score [Controlled oral word
association test (Spreen and Strauss, 1998)]
Animal fluency (Spreen and Strauss, 1998)
Speeded
visuomotor
Trail-making test—Part A (Spreen and Strauss,
1998)
processing Processing speed index (WAIS-III or WISC-III)
S. Lucas et al. / Schizophrenia Research 71 (2004) 323–330326
on the ‘conceptual disorganisation’ item of the
PANSS’ positive subscale. In the case of voluntary
inpatients, assessments were conducted as close to
discharge as possible. In order to ensure reliability of
associations between levels of symptomatology and
cognitive functioning, the neuropsychological battery
was generally administered within 1–2 days of symp-
tom ratings, with a maximum time interval of 14 days.
Tests were administered by Master’s level neuropsy-
chologists and psychologists, and given in the same
order to all subjects. The battery of tests was typically
completed in one session of 3–4 hours duration, with
rest breaks given as needed. All tests were adminis-
tered and scored according to published standardised
instructions.
2.3. Statistical analyses
In order to calculate composite scores for each
cognitive domain, the healthy control group data was
divided into two age brackets ( < 16:11 and >16:11
years) and mean raw scores for individual tests were
calculated for both age groups. On tests where higher
scores indicated impairment, scores were transformed
(reverse-scored) so that high scores always indicated
better functioning. Composite scores for each cogni-
tive domain were calculated for FES participants by
converting individual raw scores to standardised z-
scores based on the age-appropriate control group
mean scores. zZ-scores were then summed and aver-
aged across tests in each domain, to provide a single
score.
The syndrome scores for the three-factor model
were correlated with scores from the cognitive
domains using Pearson’s two-tailed correlations. Cor-
rections for multiple comparisons were applied using
the Bonferroni method [(critical p ([0.05/33)] =
< 0.002]). Fisher’s z-tests were used to compare syn-
dromes and their respective correlations with specific
cognitive domains.
In order to examine the contribution of depressive
symptoms to neuropsychological test performance,
scores for the PANSS depression item and Calgary
Depression Scale were also correlated with the cog-
nitive domains.
All analyses were carried out using Statistical
Package for Social Sciences, version 10.0 (SPSS,
2001).
3. Results
Results of the correlational analyses are shown in
Table 3 for the three-factor model. Psychomotor
Poverty and Reality Distortion produced no signif-
icant relationships with cognitive functioning after
Bonferroni corrections for multiple comparisons
( p < 0.002). However, Disorganisation was signifi-
cantly associated with poorer performance on verbal
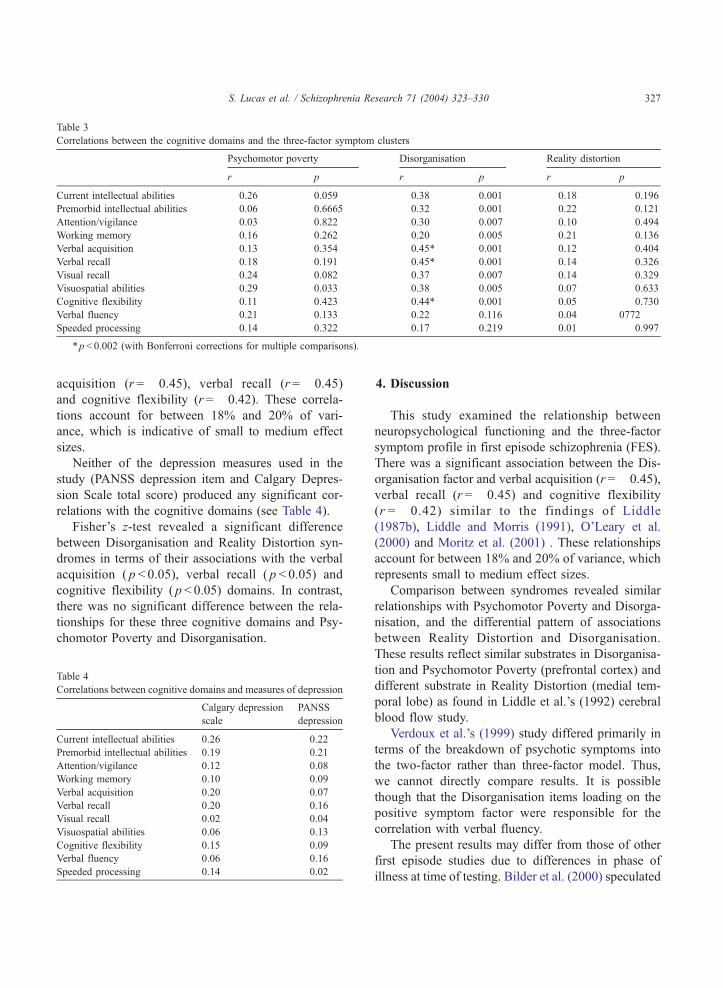
Table 3
Correlations between the cognitive domains and the three-factor symptom clusters
Psychomotor poverty Disorganisation Reality distortion
r p r p r p
Current intellectual abilities � 0.26 0.059 � 0.38 0.001 0.18 0.196
Premorbid intellectual abilities � 0.06 0.6665 � 0.32 0.001 0.22 0.121
Attention/vigilance 0.03 0.822 � 0.30 0.007 0.10 0.494
Working memory � 0.16 0.262 � 0.20 0.005 0.21 0.136
Verbal acquisition � 0.13 0.354 � 0.45* 0.001 0.12 0.404
Verbal recall � 0.18 0.191 � 0.45* 0.001 0.14 0.326
Visual recall � 0.24 0.082 � 0.37 0.007 0.14 0.329
Visuospatial abilities � 0.29 0.033 � 0.38 0.005 0.07 0.633
Cognitive flexibility � 0.11 0.423 � 0.44* 0.001 0.05 0.730
Verbal fluency � 0.21 0.133 � 0.22 0.116 0.04 0772
Speeded processing � 0.14 0.322 � 0.17 0.219 � 0.01 0.997
*p< 0.002 (with Bonferroni corrections for multiple comparisons).
S. Lucas et al. / Schizophrenia Research 71 (2004) 323–330 327
acquisition (r =� 0.45), verbal recall (r =� 0.45)
and cognitive flexibility (r =� 0.42). These correla-
tions account for between 18% and 20% of vari-
ance, which is indicative of small to medium effect
sizes.
Neither of the depression measures used in the
study (PANSS depression item and Calgary Depres-
sion Scale total score) produced any significant cor-
relations with the cognitive domains (see Table 4).
Fisher’s z-test revealed a significant difference
between Disorganisation and Reality Distortion syn-
dromes in terms of their associations with the verbal
acquisition ( p < 0.05), verbal recall ( p < 0.05) and
cognitive flexibility ( p < 0.05) domains. In contrast,
there was no significant difference between the rela-
tionships for these three cognitive domains and Psy-
chomotor Poverty and Disorganisation.
Table 4
Correlations between cognitive domains and measures of depression
Calgary depression
scale
PANSS
depression
Current intellectual abilities 0.26 0.22
Premorbid intellectual abilities 0.19 0.21
Attention/vigilance 0.12 0.08
Working memory 0.10 0.09
Verbal acquisition 0.20 0.07
Verbal recall 0.20 0.16
Visual recall 0.02 0.04
Visuospatial abilities 0.06 0.13
Cognitive flexibility 0.15 0.09
Verbal fluency 0.06 � 0.16
Speeded processing 0.14 � 0.02
4. Discussion
This study examined the relationship between
neuropsychological functioning and the three-factor
symptom profile in first episode schizophrenia (FES).
There was a significant association between the Dis-
organisation factor and verbal acquisition (r =� 0.45),
verbal recall (r =� 0.45) and cognitive flexibility
(r =� 0.42) similar to the findings of Liddle
(1987b), Liddle and Morris (1991), O’Leary et al.
(2000) and Moritz et al. (2001) . These relationships
account for between 18% and 20% of variance, which
represents small to medium effect sizes.
Comparison between syndromes revealed similar
relationships with Psychomotor Poverty and Disorga-
nisation, and the differential pattern of associations
between Reality Distortion and Disorganisation.
These results reflect similar substrates in Disorganisa-
tion and Psychomotor Poverty (prefrontal cortex) and
different substrate in Reality Distortion (medial tem-
poral lobe) as found in Liddle et al.’s (1992) cerebral
blood flow study.
Verdoux et al.’s (1999) study differed primarily in
terms of the breakdown of psychotic symptoms into
the two-factor rather than three-factor model. Thus,
we cannot directly compare results. It is possible
though that the Disorganisation items loading on the
positive symptom factor were responsible for the
correlation with verbal fluency.
The present results may differ from those of other
first episode studies due to differences in phase of
illness at time of testing. Bilder et al. (2000) speculated

S. Lucas et al. / Schizophrenia Research 71 (2004) 323–330328
that testing subjects in the acute phase of illness may
confound state and trait neuropsychological effects.
Research into the longitudinal course of the symptom-
atology of schizophrenia emphasises that symptom
domains enter a stable pattern of regular fluctuation
that may taper in acuity after 2–5 years (Birchwood et
al., 1998). This raises the possibility that the relation-
ships found between cognitive functioning and symp-
toms may represent more transient effects (given that
participants in both studies were assessed within 6
months of their first episode). The issue of when to test
is difficult to resolve. Delaying testing for too long
means the relationship of symptomatology to neuro-
psychological performance does not reflect the early
stages of illness, and fluctuation of symptoms means
not all patients are in remission at 6 months. Disorga-
nisation has been recognised as a stable, longitudinal
symptom domain and characterised as one of the
traditional subtypes of the disorder—hebephrenia.
Nonetheless, assessment during severe cognitive dis-
organisation will be affected by the acuity of symp-
toms. Thus, using a threshold level of symptoms rather
than an arbitrary period of time was seen as preferable
in this study. Further examination of the stability of the
relationship between symptoms and cognitive func-
tioning in the early stages of illness is important, and
will be explored as part of our longitudinal follow up
of the present cohort.
Another possible explanation for the inconsistent
results across studies is the difference in both medica-
tion type and dosage (Sharma, 1999; Harvey and
Keefe, 2001). For instance, there is a large discrepancy
between the chlorpromazine-equivalent dosage levels
in the current study (269 mg/day) and those reported by
Bilder et al. (2000; 712 mg/day). The significantly
higher dose of typical antipsychotics in the latter study
may have produced associations that were influenced
by medication interactions with symptoms.
In other studies including those of Bilder et al.
(2000), Verdoux et al. (1999) and Van der Does et al.
(1993), many subjects were either taking conventional
antipsychotic or anticholinergic medication which
have known adverse effects on cognition. This may
have influenced the association between symptoms
and cognition.
In contrast, no participants in the present study
were taking conventional antipsychotics, and only
three were prescribed anticholinergic medication.
Reality Distortion results were comparable to pre-
vious research findings which have failed to identify
relationships between hallucinations and delusions,
and neuropsychological deficits (Liddle, 1987b; Lid-
dle and Morris, 1991; Bilder et al., 2000). Contrary to
previous studies of chronic schizophrenia, there was
no association between Psychomotor Poverty and
cognitive functioning in the present study. This was
not due to low levels of negative symptoms as the
current sample demonstrated higher mean negative
subscale scores on the PANSS relative to the positive
subscale. As indicated earlier, this may be due to the
medication regime of atypical antipsychotic medica-
tion used (including some individuals on no antipsy-
chotic medication), given the results of Moritz et al.
(2001) discussed earlier.
The possibility that depressive symptoms may
have confounded the results was considered, given
that depression has consistently been found to affect
cognitive functioning (Cassens et al., 1990; Veiel,
1997). However, two separate measures of depres-
sion (PANSS depression item and Calgary Depres-
sion Scale score) failed to produce any significant
relationships with any of the cognitive domains
used in the present study. This may be due to
low levels of depressive symptomatology in the
present sample, given that only 22% of subjects
(n = 21) scored above the clinical cut off score of
8 for significant depressive symptomatology on the
Calgary Depression Scale (Addington et al., 1990).
Nevertheless, it suggests that depressive symptoms
may not relate to the cognitive dysfunction ob-
served, and that psychotic symptoms are the main
factor associated with such dysfunction in young
people with FES.
Some authors have suggested that the trichotomous
division of symptoms in schizophrenia is flawed
because of its simplicity and the limited range of
symptomatology that it encompasses (Stuart et al.,
1999). Certainly, the structure of symptomatology in
schizophrenia is varied, being determined as much by
the symptoms placed into the analysis, the number of
subjects and the mode of analysis, at a minimum.
These studies emphasise that the Reality Distortion
factor is the least stable, frequently breaking down
into two or more factors. This inherent instability may
reflect an inadequate model of psychopathology.
However, the validity of such criticism can only be

S. Lucas et al. / Schizophrenia Research 71 (2004) 323–330 329
tested via studies such as these that examine the fit of
the data with external factors and eventually with
underlying pathological mechanisms. Given the bur-
geoning research into the structure of psychotic symp-
tomatology (White et al., 1997), a contrasting and
more robust model may become apparent in the
future.
Despite these unresolved theoretical issues, the
current study has provided several methodological
improvements on previous research such as the use
of an ecologically valid sample of young FES
patients; the employment of a threshold level of
symptomatology (conceptual disorganisation) to stan-
dardise the assessment procedure; the inclusion of
only participants who were either unmedicated or
prescribed atypical antipsychotics; and specific exam-
ination of the effects of depression.
Although further research is warranted to clarify
the nature of the cognitive correlates of symptom
profiles in FES and their stability in the early
stages of this illness, the present study provides
preliminary evidence that symptoms loading on the
Disorganisation factor are significantly associated
with impaired frontal– temporal functioning, both
of which may represent core features of schizophre-
nia that are present at the earliest manifestations of
the illness. Concurrent validity from studies exam-
ining brain functioning by electrophysiological and
neuroanatomical means also needs to be established.
Clinically, these findings suggest that young people
with FES who appear to have a significant degree
of disorganised symptoms may be at greater risk of
cognitive dysfunction, and ultimately poorer out-
come (Green, 1996; Green et al., 2000). This
remains to be seen by researching the longitudinal
relationships between these factors.
Acknowledgements
The authors thank Dr. Wayne Reid and Ms.
Susanne Meares for their substantial contributions to
the development and implementation of this study,
and Dr. Anne Taylor, Dr. Mark Kneebone, Dr. Martyn
Patfield, Dr. Megan Chambers and Ms. Susan Cole-
man for their assistance and cooperation.
This research was supported by a grant from the
Centre for Mental Health (NSW Health, Australia).
References
Addington, D., Addington, J., Schissel, B., 1990. A depression
rating scale for schizophrenics. Schizophrenia Research 3,
247–251.
Addington, J., Brooks, B.L., Addington, D., 2003. Cognitive func-
tioning in first episode psychosis: initial presentation. Schizo-
phrenia Research 62 (1–2), 59–64 (Jul.).
American Psychiatric Association, 1994. Diagnostic and Sta-
tistical Manual of Mental Disorders, Fourth edition. Amer-
ican Psychological Association, Washington, DC.
Baxter, R.D., Liddle, P.F., 1998. Neuropsychological deficits asso-
ciated with schizophrenic syndromes. Schizophrenia Research
30, 239–249.
Bilder, R.M., Mukherjee, S., Rieder, R.O., et al., 1985. Symptom-
atic and neurological components of deficit states. Schizophre-
nia Bulletin 11, 409–419.
Bilder, R.M., Goldman, R.S., Robinson, D., Reiter, G., Bell, L.,
Bates, J.A., Pappadopoulos, E., Willson, D.F., Alvir, J.M.J.,
Woerner, M.G., Geisler, S., Kane, J.M., Lieberman, J.A.,
2000. Neuropsychology of first-episode schizophrenia: initial
characterization and clinical correlates. American Journal of
Psychiatry 157, 549–559.
Birchwood, M., Todd, P., Jackson, C., 1998. Early intervention in
psychosis. The critical period hypothesis. British Journal of
Psychiatry 172 (Suppl. 33), 53–59.
Buchanan, R.W., Carpenter, W.T., 1994. Domains of psychopa-
thology: an approach to the reduction of heterogeneity in
schizophrenia. Journal of Nervous and Mental Disease 182,
193–204.
Cassens, G., Wolfe, L., Zola, M., 1990. The neuropsychology of
depressions. Journal of Neuropsychiatry and Clinical Neuro-
sciences 2, 202–213.
Cohen, D., 1997. Children’s Memory Scale. The Psychological,
San Antonio.
Conners, C.K., 1995. Conner’s Continuous Performance Test.
Multi-Health Systems, North Tonawanda, NY.
Green, M.F., 1996. What are the functional consequences of neuro-
cognitive deficits in schizophrenia? American Journal of Psy-
chiatry 153, 321–330.
Green, M.F., Kern, R.S., Braff, D.L., Mintz, J., 2000. Neuro-
cognitive deficits and functional outcome in schizophrenia:
are we measuring the ‘‘right stuff’’? Schizophrenia Bulletin
26, 119–136.
Harris, A.W.F., Williams, L., Gordon, E., Bahramali, H., Slewa-
Younan, S., 1999. Different psychopathological models and
quantified EEG in schizophrenia. Psychological Medicine 29,
1175–1181.
Harvey, P.D., Keefe, R.S.E., 2001. Studies of cognitive change in
patients with schizophrenia following novel antipsychotic treat-
ment. American Journal of Psychiatry 158, 176–184.
Heaton, R.K., Chelune, G.J., Talley, J.L., Kay, G.G., Curtiss, G.,
1993. Wisconsin Card Sorting Test Manual—Revised and Ex-
panded. Psychological Assessment Resources, USA.
Heinrichs, R.W., Zakzanis, K.K., 1998. Neurocognitive deficit in
schizophrenia: a quantitative review of the evidence. Neuropsy-
chology 3, 426–445.
S. Lucas et al. / Schizophrenia Research 71 (2004) 323–330330
Hoff, A.L., Riordan, H., O’Donnell, D.W., Morris, L., DeLisi,
D.E., 1992. Neuropsychological functioning of first-episode
schizophreniform patients. American Journal of Psychiatry
149, 898–903.
Joyce, E., Hutton, S., Mutsatsa, S., et al., Executive dysfunction in
first-episode schizophrenia and relationship to duration of un-
treated psychosis: the West London Study. British Journal of
Psychiatry 181, s38–s44.
Kay, S.R., Opler, L.A., Fiszbein, A., 1986. Positive and Negative
Syndrome Scale (PANSS). Multi-Health Systems, NY.
Lambert, T., 1999. Switching to Risperdal. The Multimedia in Psy-
chiatry Unit, University of Melbourne, Parkville, Australia.
Liddle, P.F., 1987a. The symptoms of chronic schizophrenia: a re-
examination of the positive–negative dichotomy. British Jour-
nal of Psychiatry 151, 145–151.
Liddle, P.F., 1987b. Schizophrenic syndromes, cognitive perfor-
mance and neurological dysfunction. Psychological Medicine
17, 49–57.
Liddle, P.F., Friston, K.J., Frith, C.D., Hirsch, S.R., Jones, T.,
Frackowiak, R.S., 1992. Patterns of cerebral blood flow in
schizophrenia. British Journal of Psychiatry 160, 179–186.
Liddle, P.F., Morris, D.L., 1991. Schizophrenic syndromes and
frontal lobe performance. British Journal of Psychiatry 158,
340–345.
Liddle, P.F., Barnes, T.R.E., Morris, D., Haque, S., 1989. Three
syndromes in chronic schizophrenia. British Journal of Psychi-
atry 155, 119–122.
Malla, A.K., Norman, R.M.G., Morrison-Stewart, S., Williamson,
P.C., Helmes, E., Cortese, L., 2001. Does sex influence the
relation between symptoms and neurocognitive functions in
schizophrenia? Journal of Psychiatry and Neuroscience 26,
49–54.
Mohamed, S., Paulsen, J.S., O’Leary, D., Arndt, S., Andreasen, N.,
1999. Generalized cognitive deficits in schizophrenia: a study
of first-episode patients. Archives of General Psychiatry 56,
749–757.
Moritz, S., Andresen, B., Jacobsen, K., et al., 2001. Neuropsy-
chological correlates of schizophrenic syndromes in patients
treated with atypical neuroleptics. European Psychiatry 16,
354–361.
Niewenstein, M.R., Aleman, A., de Hann, E.H.F., 2001. Relation-
ship between symptom dimensions and neurocognitive func-
tioning in schizophrenia: a meta-analysis of WCST and CPT
studies. Journal of Psychiatric Research 35, 119–125.
Norman, R.M.G., Malla, A.K., Morrison-Stewart, S.L., Helmes, E.,
Williamson, P.C., Thomas, J., Cortese, L., 1997. Neuropsycho-
logical correlates of syndromes in schizophrenia. British Journal
of Psychiatry 170, 134–139.
O’Leary, D.S., Flaum, M., Kesler, M.L., Flashman, L.A., Arndt, S.,
Andreasen, N.C., 2000. Cognitive correlates of the negative,
disorganised and psychotic symptom dimensions of schizophre-
nia. Journal of Neuropsychiatry and Clinical Neurosciences 12,
4–15.
Peralta, V., de Leon, J., Cuesta, M.J., 1992. Are there more
than two syndromes in schizophrenia? A critique of the
positive negative dichotomy. British Journal of Psychiatry
161, 335–343.
Sharma, T., 1999. Cognitive effects of conventional and atypical
antipsychotics in schizophrenia. British Journal of Psychiatry
174, 44–51.
Spreen, O., Strauss, E., 1998. A Compendium of Neuropsycholog-
ical Tests. Administration, Norms and Commentary. Oxford
Univ. Press, NY.
SPSS Inc., 2001. Statistical Package for Social Sciences. SPSS Inc.,
Chicago, US.
Stuart, G.W., Pantelis, C., Klimidis, S., Minas, I.H., 1999. The
three-syndrome model of schizophrenia: meta analysis of an
artifact. Schizophrenia Research 39, 233–242.
Thompson, R.A., Meltzer, H.Y., 1993. Positive negative and disor-
ganisation factors from the schedule for affective disorders and
schizophrenia the present state examination. British Journal of
Psychiatry 163, 344–351.
Van der Does, A.J.W., Dingemans, P.M.A.J., Linszen, D.H.,
Nugter, M.A., Scholte, W.F., 1993. Symptom dimensions and
cognitive and social functioning in recent-onset schizophrenia.
Psychological Medicine 23, 745–753.
Veiel, H.O.F., 1997. A preliminary profile of neuropsychological
deficits associated with major depression. Journal of Clinical
and Experimental Neuropsychology 19, 587–603.
Verdoux, H., Lirand, F., Bourgeois, M.L., Gonzales, B.,
Assens, F., et al., 1999. The association of neuropsycho-
logical deficits to clinical symptoms in first-admission sub-
jects with psychotic disorders. Schizophrenia Research 37,
197–203.
Wechsler, D., 1991. Wechsler Intelligence Scale for Children, Third
edition. The Psychological, San Antonio.
Wechsler, D., 1997a. Wechsler Adult Intelligence Scale, Third edi-
tion. The Psychological, San Antonio.
Wechsler, D., 1997b. Wechsler Memory Scale Manual –Third
Edition Manual. The Psychological, San Antonio.
White, L., Harvey, P.D., Opler, L., Lindenmayer, J.P., The
PANSS Study Group, 1997. Empirical assessment of the fac-
torial structure of clinical symptoms in schizophrenia. Psycho-
pathology 30, 263–274.
Williams, L.M., 1996. Cognitive inhibition and schizophrenic
symptom subgroups. Schizophrenia Bulletin 22, 139–151.





























