Embed Size (px)
Citation preview
AANEM MONOGRAPH ABSTRACT: The bladder has only two essential functions. It stores andperiodically empties liquid waste. Yet it is unique as a visceral organ,allowing integrated volitional and autonomous control of continence andvoiding. Normal function tests the integrity of the nervous system at alllevels, extending from the neuroepithelium of the bladder wall to the frontalcortex of the brain. Thus, dysfunction is common with impairment of eitherthe central or peripheral nervous system. This monograph presents anoverview of the neural control of the bladder as it is currently understood. Adescription of pertinent peripheral anatomy and neuroanatomy is provided,followed by an explanation of common neurophysiological tests of the lowerurinary tract and associated structures, including both urodynamic andelectrodiagnostic approaches. Clinical applications are included to illustratethe impact of nervous system dysfunction on the bladder and to provideindications for testing.
Muscle Nerve 38: 815–836, 2008
NEUROPHYSIOLOGY IN NEUROUROLOGY
MARGARET M. ROBERTS, MD, PhD
AANEM, Illinois Urogynecology, LTD, Oak Lawn, Illinois, USA
Accepted 29 January 2008
The bladder has two essential functions: the storageand periodic elimination of liquid waste. It has acapacity in the range of 400–500 ml1,2,44,56 in anaverage adult but is typically emptied 5–7 times aday,3,24 often at much smaller volumes. With an av-erage urine flow time of less than 30 s,91 the bladderis actively emptying less than 1% of the time. Thus,the predominant role of the bladder is that of areservoir, storing urine at low pressures even duringfilling to capacity. When necessary, the bladder isalso dynamic, responding to increased filling, infec-tion, or even emotional stimuli with elimination atessentially any volume, any time, as many times asnecessary.
The significance of normal bladder function maybe more readily apparent if one considers the impactof dysfunction. Urinary incontinence is readily ap-preciated as a prevalent and costly problem, affect-ing 17 million Americans at an annual cost of more
than 26 billion dollars.1,63,154 This is similar to theprevalence of diabetes in the United States6,140 andthe total cost of health care for the entire country ofSwitzerland.86 Urinary retention, though less preva-lent in the general population, is a common condi-tion in patients with neurologic disorders. It hasbeen identified in more than 27% of patients admit-ted for rehabilitation, with 20% of cases both asymp-tomatic and unsuspected at presentation.160 Reten-tion may be equally burdensome to the individual,and untreated; it may result in devastating complica-tions including renal failure and death. Until the1970s, upper urinary tract disease was the leadingcause of death in patients with spinal cord injury(SCI) and myelomeningocele.57,75,128
While impressive for the sheer size of the num-bers, statistics tend to be sterile and dry, failing tocapture the human aspect of disease and impair-ment. Consider the stigmatization, isolation, loss ofself esteem, depression, and risk of institutionaliza-tion that occurs in those with bladder dysfunc-tion.1,43 Failure to maintain continence is a majorfactor for institutionalization,141 with more than halfof those in nursing homes suffering from urinaryincontinence.1,3,43 Following hemispheric stroke,urinary continence is the main determinant of dis-charge home within 6 months, independent of se-verity of hemiparesis.9
The causes of storage and voiding dysfunctionare myriad, diverse, and often multifactorial rangingfrom a simple and reversible urinary tract infection
Abbreviations: ASIA, American Spinal Injury Association; BC, bulbocavern-osus; CAR, clitoroanal reflex; DLPP, detrusor leak point pressure; DSD, de-trusor sphincter dyssynergia; EAS, external anal sphincter; EDX, electro-diagnostic; EMG, electromyographic; EUS, external urethral sphincter; IC,ischiocavernosus; MUAP, motor unit action potential; NCS, nerve conductionstudy; PAG, periaqueductal gray; PAR, peniloanal reflex; PMC, pontine mic-turition center; SCI, spinal cord injury; SEP, somatosensory evoked potential;VLPP, Valsalva leak point pressureKey words: needle electromyography; nerve conduction study; urinary in-continence; urodynamic study; voiding dysfunctionCorrespondence to: M. Roberts; e-mail: [email protected].
© 2008 Wiley Periodicals, Inc.Published online 14 June 2008 inWiley InterScience (www.interscience.wiley.com). DOI 10.1002/mus.21001
AANEM Monograph MUSCLE & NERVE July 2008 815

to prostatic hypertrophy or cancer, urethral hyper-mobility with or without associated pelvic organ pro-lapse, pharmacologic effects, and neurologic dys-function, anywhere along the neuraxis from thebrain to the spinal cord, or in the peripheral nervesor ganglia.36
Fortunately, neurourology, the study of the func-tion of the bladder, is a rapidly expanding field.Since this monograph was originally written in1977,35 more than 60,000 publications have ap-peared on human bladder function/dysfunction inthe English language. The explosion of interest andresearch with the concomitant emergence of tech-nology has provided new information on bladderfunction from the molecular level of the neuroepi-thelium of the bladder wall to the cellular interac-tion in the frontal cortex of the brain. It is the role ofneurophysiologists to elicit symptoms and clinicalfindings which are sometimes nonspecific or silent;identify those patients in which neurological diseaseis potentially altering bladder function; and exam-ine, diagnose, and ultimately ensure implementa-tion of optimal treatment.
BLADDER DYSFUNCTION
Urinary incontinence is defined by the InternationalContinence Society as “the complaint of any invol-untary leakage of urine.”4 It may be a symptom, asign, or a condition,1 but it is a nonspecific diagnosisand fails to identify the underlying pathophysiologicprocess. It is sometimes categorized by the clinicalpresentation as stress incontinence (occurring with
cough, laugh, sneeze, or other exertion which ele-vates the intraabdominal pressure); urge inconti-nence (which is accompanied by or immediatelypreceded by urgency); or continuous leakage. Mixedurinary incontinence has features of both stress andurge incontinence. While more descriptive, thesecategories still fail to define the underlying causeand any combination of these conditions may coex-ist. In addition, leakage may be insensible and pa-tients may not be able to characterize their urineloss. Common conditions associated with these pre-sentations are indicated in Table 1. Voiding dysfunc-tion may result from impaired bladder contractility(due to sensory or motor defects), elevated outletresistance, or a combination of the two. It is oftenidentified after a patient presents with urinary reten-tion and complaints of recurrent urinary tract infec-tion, urinary frequency, nocturia, or even inconti-nence, but patients with chronic urinary retentionmay be asymptomatic in spite of large volume reten-tion (1,000 ml) and associated upper urinary tractinjury.53,160 Some causes of urinary retention arelisted in Table 2.
OVERVIEW OF NEURAL CONTROL
Normal bladder function requires the integrity ofextensive neurologic circuitry of the central and pe-ripheral nervous systems supplied by the somatic andautonomic nervous systems under both voluntaryand involuntary control.30 While many of the detailshave not yet been elucidated, a sophisticated modelhas been developed over the past eight decades with
Table 1. Urinary incontinence. Symptoms and associatedconditions1
StressInadequate pelvic support with urethral hypermobilityInadequate sphincter closure due to anatomic defect or
functional impairmentLower motor neuron injuryRetention (See text)Low compliancePharmacologic agents (adrenergic antagonists, e.g.)
UrgeDetrusor overactivityIdiopathicNeurogenic (upper motor neuron involvement)Continuous
FistulaEctopic ureterSevere stress incontinenceUnrecognized detrusor overactivityRetention (See below)Low compliance
Table 2. Causes of urinary retention.1,53
Decreased contractilityLower motor neuron injury (cauda equina, radiculopathyincluding herpes zoster or simplex, neuropathy)
Rapid overdistention such as with diuresis.Pharmacologic agents (e.g., anticholinergic)
Decreased afferent functionLower motor neuron injury (cauda equina, radiculopathyincluding herpes zoster or simplex, neuropathy)
Analgesics (including alcohol)Outlet obstructionProstatic hypertrophy (benign or malignant)Pelvic organ prolapseStricture, stenosis, post-operative changesStonesDetrusor sphincter dyssynergia (upper motor neurondysfunction)
Non-neurogenic neurogenic bladder (Hinman syndrome) orpseudodyssynergia
Pharmacologic agents (e.g., adrenergic agonists)Combined factors (e.g., diuresis and analgesia such as alcohol)
816 AANEM Monograph MUSCLE & NERVE July 2008

supporting evidence drawn from experimentation inanimals, monitoring of normal human function, andevidence drawn from clinical observation of patientswith neurologic lesions.7
It is generally accepted that afferent informationregarding bladder filling is conveyed via the visceralafferent fibers of the sympathetic and parasympa-thetic systems to neurons in the lumbar and sacralspinal cord, and then to the periaqueductal gray(PAG).7,23,90 During urine storage the PAG main-tains input to an area of the ventral pons known asthe L (lateral) region,7,23 which results in contrac-tion of the urethral sphincter and related muscula-ture to increase urethral closure pressure and main-tain continence.23,44 In contrast, at the appropriatelevel of filling and/or in the appropriate situation,the PAG activates a region of the dorsomedial pon-tine tegmentum known as the M (medial) region,analogous to the pontine micturition center (PMC)or Barrington’s nucleus.7,23,90 This activates descend-ing pathways to excite parasympathetic neurons inthe sacral spinal cord,90 resulting in increased intra-vesical pressure while concomitantly stimulating in-hibitory interneurons which relax the urethralsphincter and facilitate flow.7,23,44 It is not clear whatregulates the PAG.23,90
While the forebrain is not essential for the mic-turition reflex, multiple forebrain structures are in-volved in the initiation of micturition. In particular,the hypothalamus appears to have a role in activat-ing the PMC when the situation is deemed “safe” tovoid. In addition, the cingulate gyrus and the pre-frontal cortex are thought to be involved in attentionand response selection.23,25
ANATOMY
While the following discussion focuses on the lowerurinary tract, information regarding related systemsis sometimes included due to common innervationand interrelated symptoms, function, and examina-tion.
Peripheral Innervation. The bladder, the urethra,and the associated striated musculature of the ure-thra and pelvic floor are innervated by three sets ofperipheral nerves, each with efferent and afferentcomponents.
Autonomic. The sympathetic system supplies bothsomatic and visceral structures.118 In general, so-matic structures are innervated in a segmental fash-ion, along with the somatic spinal nerves to the area,whereas visceral structures are innervated in con-
junction with the vascular supply of the area. Perti-nent effects of sympathetic stimulation include con-traction of sphincter muscles, relaxation of smoothmuscle in the wall of hollow viscera, and constrictionof blood vessels. The parasympathetic system has amore limited distribution, with no innervation ofsomatic structures and no supply to blood vessels ingeneral.118 Parasympathetic stimulation results in re-laxation of sphincter muscles and contraction ofsmooth muscle in the wall of hollow viscera. In thesingle instance of parasympathetic innervation ofblood vessels, stimulation results in vasodilation ofvessels in the erectile tissue of the genitals and,hence, the pelvic splanchnic nerves may be referredto as nervi erigentes.
Visceral afferent fibers supply the visceral perito-neum, the pelvic organs, and the blood vessels. Ingeneral, sympathetic afferent fibers mediate dull,aching, poorly localized pain sensation, whereasparasympathetic afferent fibers convey visceral sen-sations including bladder distention, rectal fullness,urge to urinate or defecate, and sexual sensations.28However, parasympathetic fibers have been impli-cated in mediating pain from all of the organs of thepelvis except the uterus.83,118 Both sympathetic andparasympathetic afferent fibers participate in vis-ceral reflex activity.
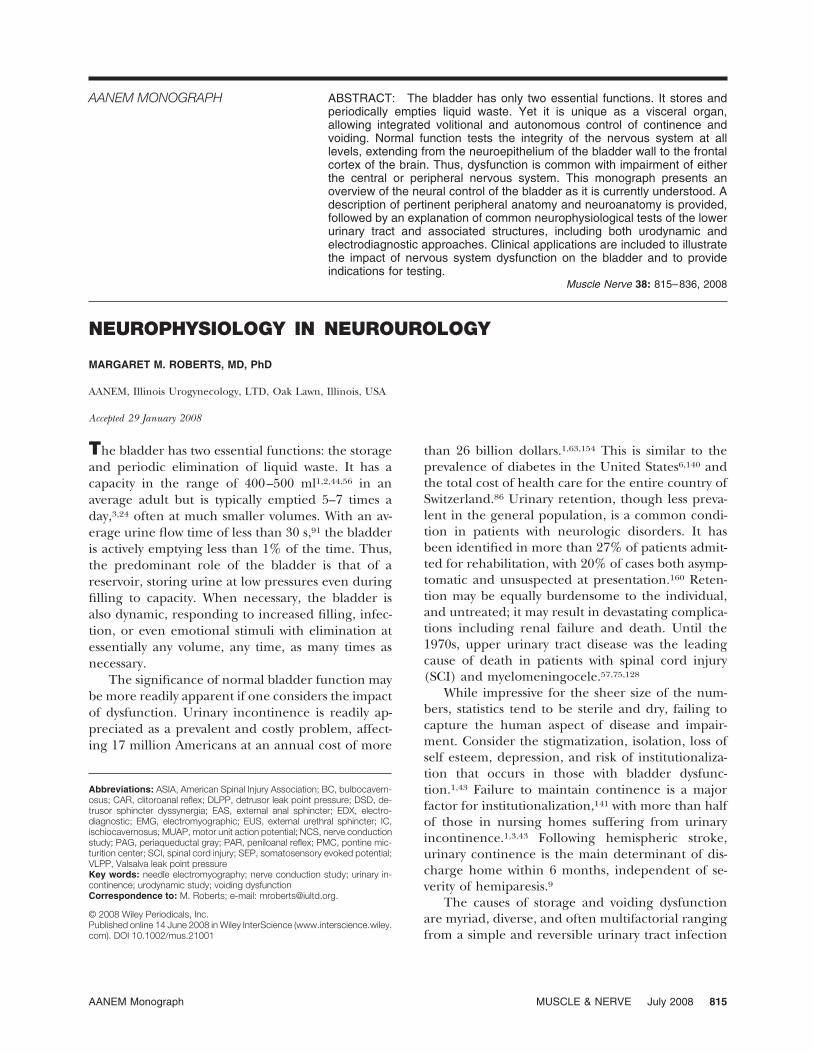
Sympathetic. The sympathetic efferent fibers to thelower urinary tract originate in the intermediolateralcell column of the spinal cord at T10 to L2.1,2 Theyexit the spinal cord through the anterior root, inter-mingled with somatic efferent fibers forming thespinal nerve and synapse in one of the nearby para-vertebral ganglia of the sympathetic chain which jointhe anterior rami and continue peripherally withassociated somatic segmental fibers to reach the pel-vic floor. Alternatively, those fibers destined for thebladder and urethra may pass directly through theparavertebral ganglia and exit as preganglionic vis-ceral or splanchnic nerves. These fibers may synapseon one of the prevertebral or collateral ganglia onthe anterior aspect of the aorta or internal iliacvessels such as the inferior mesenteric ganglia,2,118before continuing inferiorly as the right and lefthypogastric nerves which contribute to the pelvicplexus. Other fibers pass through both the paraver-tebral and prevertebral ganglia before reaching thepelvic plexus, resulting in a dense complex of pre-and postganglionic sympathetic and parasympa-thetic fibers and ganglia. The pelvic plexus gives riseto multiple named and unnamed subsidiary plexiand nerves including the vesical plexus to the blad-der and the urethra38,118 and the cavernous nerves to
AANEM Monograph MUSCLE & NERVE July 2008 817
the urethral sphincter complex1,165 (Fig. 1). Thepostganglionic fibers of the sympathetic nervous sys-tem produce excitation of the bladder base andurethra via �1-adrenoceptors or inhibition of detru-sor muscle via �-adrenoreceptors. Further, these fi-bers may inhibit bladder parasympathetic ganglia via�2-adrenoreceptors, or facilitate bladder parasympa-thetic ganglia via �1-adrenoreceptors.30,52 Based onfindings in animal studies, it appears that inhibitionand facilitation occur at different firing frequencies,thus allowing the same mechanism to facilitate stor-age and emptying as appropriate.30
Parasympathetic. The parasympathetic efferentfibers to the lower urinary tract originate as pregan-glionic neurons in the intermediolateral cell columnof the spinal cord at S2, S3, and S4. As with thesympathetic fibers, they exit the spinal cord throughthe anterior roots, intermingled with somatic effer-ent fibers forming the spinal nerves, continue in theanterior spinal rami, and finally travel via the pelvicsplanchnic nerves to ganglion cells in the pelvicplexus, the subsidiary vesical plexus, cavernousnerves, and the wall of the bladder and ure-thra38,52,118 (Fig. 1). Preganglionic synapses are nic-otinic cholinergic, but they may be modulated bymuscarinic, adrenergic, purinergic, and peptidergicinput.30 The postganglionic fibers of the parasympa-
thetic system are typically microscopic and are lo-cated intramurally in the detrusor. Cholinergic exci-tatory transmission in the bladder is mediated viamuscarinic, primarily subtype M3, receptors. In ad-dition, noncholinergic excitatory transmission is me-diated by adenosine triphosphate acting on puriner-gic receptors.30 Postganglionic neurons innervatingthe bladder also contain neuropeptides, such as va-soactive intestinal polypeptide and neuropeptide Yand may modulate neurotransmission. Parasympa-thetic nerve fibers release nitric oxide which is in-hibitory to urethral smooth muscle.30,31
Sympathetic and parasympathetic afferent fibersare found in the hypogastric and pelvic nerves, re-spectively, as well as the many autonomic plexi of thepelvis, after originating in the proximal urethra andbladder2,15,38 As with all peripheral sensory nerves,the cell bodies are located in the spinal ganglia. Thesympathetic fibers enter the spinal cord at T11 to L2and the parasympathetic fibers enter at S2 to S4.38Sensation from the bladder is carried predominantlyin the parasympathetic system2,118 but there aresome afferent fibers that travel in the hypogastricnerves to the spinal cord. Sensation from the prox-imal urethra is also thought to be carried by bothsympathetic and parasympathetic pathways.15
Somatic. The somatic efferent fibers to the pel-vis originate from motor neurons in the anterior cellcolumn of the spinal cord at the lumbar, sacral, andcoccygeal levels, with the sole purpose of innervatingskeletal muscle.114,118 These fibers exit the spinalcord as the anterior root, form the spinal nerve withthe posterior root, and contribute fibers through theanterior (or ventral) ramus to the lumbar and sacralplexuses. Anococcygeal nerves are formed fromlower sacral and coccygeal anterior rami and spinalnerves. Somatic afferent fibers supply sensation tothe parietal layer of the peritoneum, as well as theskin, muscles, tendons, and joints of the entire pelvisand perineum, including the outer urethra, vagina,anus, and genitalia. These fibers travel proximallyalong the same pathway to the posterior root and thespinal ganglion containing the cell body before en-tering the spinal cord through the lumbar, sacral, orcoccygeal roots. These fibers convey pain, tempera-ture, touch, vibration, and proprioception.
Onuf’s Nucleus. A subgroup of closely packed,atypical alpha motor neurons, collectively known asOnuf’s nucleus (after the original description byOnufrowicz) is located ventrolaterally within the an-terior horns at S1 to S3 and provides innervation tothe urethral and anal sphincters and the levatorani.2,143 The unique properties of these cells includeanatomic features such as their uniformly smaller
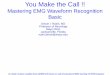
FIGURE 1. The sympathetic, parasympathetic, and somatic path-ways of the pelvis. SPLN, splanchnic nerves; GR, gray rami; WR,white rami; BC, bulbocavernosus muscle; IC, ischiocavernosusmuscle; SPH, sphincter. Adapted from de Groat and Steers32 inRoberts116 with permission from Lippincott Williams & Wilkinsand Elsevier.
818 AANEM Monograph MUSCLE & NERVE July 2008

size and dense dendritic bundling with extensiveinterconnections, as well as high numbers of norad-renergic and serotonin terminals not seen in adja-cent cells. Their distinctive character is further sub-stantiated by their relative resistance to polio andamyotrophic lateral sclerosis, both of which affectother anterior horn cells, and their selective involve-ment in multiple system atrophy.15,88
Pudendal Nerve. After forming on the posterioraspect of the pelvis as part of the sacral plexus, thepudendal nerve exits the pelvic cavity below thepiriformis via the greater sciatic foramen. It reentersthe pelvic cavity by curving around the sacrospinousligament just medial to the ischial spine and passingthrough the lesser sciatic foramen. Finally, it runsforward along the lateral wall of the ischiorectal fossain the pudendal (or Alcock’s) canal.2,118 There arethree major branches of the pudendal nerve: thedorsal nerve of the penis/clitoris that arises proxi-mally and travels with the major trunk of the puden-dal nerve in the pudendal canal, continuing forwardalong the ischiopubic ramus to provide cutaneoussupply to the clitoris/penis; the inferior rectal nervewhich leaves the main trunk of the pudendal nervewithin the canal and crosses the ischiorectal fossa tosupply the lining of the lower anal canal, the exter-nal anal sphincter, and the skin around the anus;and the perineal nerve which divides into cutaneousbranches to the posterior labia and lower vagina/scrotum and ventral penis144 and distal urethra,2,15and muscular branches to the superficial and deepperineal muscles, including the external urethralsphincter2 and parts of the levator ani.2,67,118
Bladder. The bladder is a muscular organ whichresides in the pelvis when empty but expands intothe abdominal cavity as it fills.1,2,118 It is composed ofan outer adventitial layer of connective tissue, aninner mucosal layer consisting of transitional epithe-lium (or urothelium) and submucosal lamina pro-pria, and a middle muscular layer, the detrusor mus-cle.1,2,42 The muscle layer consists of circular smoothmuscle situated between inner and outer layers oflongitudinal muscle, but large interlacing bundles ofsmooth muscle cells may travel between layers form-ing a meshwork.1,2,38 The trigone is a specialized areaof the bladder base extending from the two uretericorifices to the internal urethral meatus. It is charac-terized by the presence of a superficial muscle layer,which is morphologically distinct from the deepertrigonal detrusor, consisting of small diameter mus-cle bundles which are continuous with those of theintramural ureters above and the smooth muscle ofthe proximal urethra below.1,2,38,52
The detrusor muscle of the bladder is richly in-nervated by parasympathetic cholinergic nerve fiberswith ganglion cells in the anterior portion of thepelvic plexus (vesical plexus) as well as the bladderwall itself. There are also sympathetic noradrenergicfibers to the detrusor but they are few in number andgenerally, though not exclusively, innervate the vas-cular supply.1,2,38,52 In contrast, the superficial tri-gone muscle has relatively few parasympathetic cho-linergic nerves while sympathetic noradrenergicfibers are prevalent. Sensory fibers have been iden-tified as a suburothelial plexus beneath the epithe-lial lining of the bladder.2 It is somewhat sparsethroughout the dome of the bladder, but becomesprogressively denser approaching the trigone andbladder neck and extends into the urethra.38
The bladder neck, i.e., the internal urethral ori-fice, is 3–4 cm behind the lower symphysis pubis. Inmales the bladder neck rests on the prostate.2 At thislevel, smooth muscle forms a complete collar ofcircular fibers surrounding the preprostatic urethrato serve as an internal sphincter, with a well-definedadrenergic innervation which prevents retrogradeejaculation,1,2 but has an uncertain role in conti-nence.2,38,52 In females the bladder neck is associatedwith the endopelvic fascia and supporting pubovesi-cal ligaments with smooth muscle extending fromthe trigone and continuing obliquely or longitudi-nally into the urethral wall. The circular smoothmuscle sphincter seen in the male is poorly devel-oped or absent1 and few adrenergic fibers are iden-tified.38 In contrast to the male, the bladder neck ofthe female receives an abundant supply of cholin-ergic fibers.1,38,50
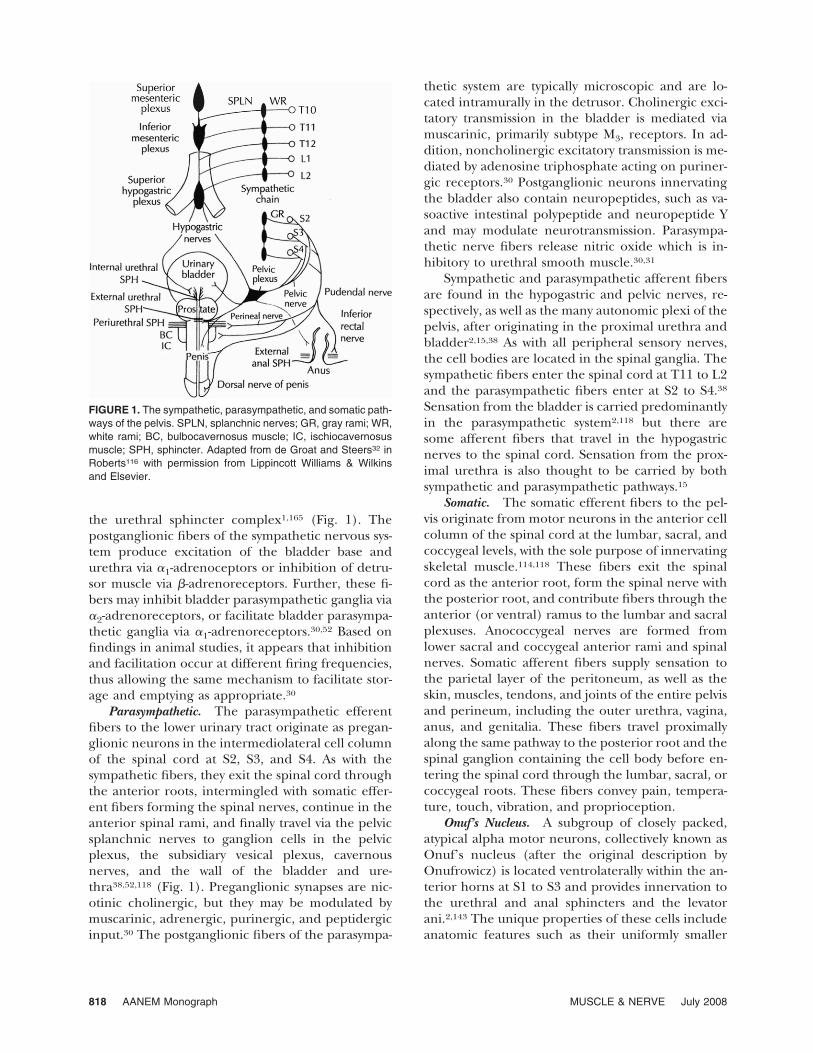
Pelvic Floor. The pelvic floor can be thought of inlayers34 with the pelvic viscera and supporting en-dopelvic fascia forming the first layer. The next layeris the muscular diaphragm (Fig. 2) consisting of thelevator ani and two muscles of the lower limb (piri-formis and obturator internus). The piriformis arisesfrom the sacrum and the ilium and forms the pos-terolateral wall of the pelvis. The obturator internusarises from the inner surface of the obturator fora-men, forming the anterolateral wall. Both attach tothe greater trochanter.116,118 The levator ani is acomplex sheet of muscle arising from the posterioraspect of the pubic bone, the inner surface of theobturator fascia extending along the arcuate line tothe ischial spine, and from the ischial spine it-self.115,118 Collectively, the fibers run down and backwith varying degrees of obliquity to form a funnelwhich inserts into the anococcygeal ligament andthe coccyx posteriorly, while narrowing to encircle
AANEM Monograph MUSCLE & NERVE July 2008 819
and fuse with the urethra, the vagina (in females),and the anal canal inferiorly.118 Although not well-defined, several named regions are described, some-times with variations in terminology between au-thors. The pubococcygeus runs almost horizontallyfrom the pubis to insert into the anococcygeal liga-ment and the coccyx posteriorly. The most medialfibers bordering the urogenital hiatus are often re-ferred to as the pubovaginalis in the female and thepubourethralis/levator prostate in the male. Posteri-orly, the muscle fibers encircle the anal canal, some-times blending with the longitudinal fibers of therectal muscle. Inferiorly, muscle fibers from eachside unite with the contralateral fibers behind therectum to form a “sling” at the level of the anorectalangle. This region of muscle, referred to as thepuborectalis portion of the pubococcygeus muscle,maintains the anorectal angle which is critical foranal continence.2,101 The iliococcygeus arises fromthe arcuate line and the ischial spine and runs pos-teriorly to join with fibers from the opposite side andform a raphe just superior to (and sometimes con-tinuous with) the anococcygeal ligament and thecoccyx inferior to the attachment of the pubococcy-geus.2,118 The ischiococcygeus (sometimes referredto as a separate muscle, the coccygeus)118 is the mostposterior and superior portion of the levator ani,arising from the ischial spine and running posteri-orly to insert on the lateral margins of the lower
sacrum and coccyx. In some cases it may be tendi-nous rather than muscular.2
Just below the muscular diaphragm, the perinealmembrane, sometimes referred to as the urogenitaldiaphragm, spans the anterior portion of the pelvicoutlet. It consists of striated muscles including thedeep transverse perineal muscles as well as the com-pressor urethrae and the urethrovaginal sphincter inthe female.1,34,85 The urethral sphincter muscle inthe male is vertically oriented and does not contrib-ute to the urogenital diaphragm.92
The most superficial layer of the pelvic floor isthe external genital muscles consisting of the bulbo-cavernosus (BC) also referred to as the bulbospon-giosus, the ischiocavernosus (IC) and superficialtransverse perineal muscles anteriorly, with the ex-ternal anal sphincter located posteriorly.34,118 In themale the BC lies at midline anterior to the perinealbody and runs forward with the contralateral sidesunited by a median raphe. Its fibers encircle the bulbof the penis and adjacent corpus spongiosum ex-tending anteriorly to spread over the corpora caver-nosa. In the female the BC attaches to the perinealbody and runs anteriorly on each side of the vagina,covering the vestibular bulbs.2,118
The levator ani is innervated on its pelvic surfaceby small twigs arising directly from the S3, S4,101,118and sometimes S5 nerve roots.8 The anterior portionof the levator ani, particularly the puborectalis, may
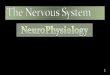
FIGURE 2. Female pelvic diaphragm from above. Adapted from Mattingly and Thompson82 in Stenchever et al135 with permission fromLippincott Williams & Wilkins and Elsevier.
820 AANEM Monograph MUSCLE & NERVE July 2008
also receive some innervation from the pudendalnerve,118 but the primary source of innervation forthe puborectalis is direct branches of S3 and S4.8,101The posterior portion of the levator, especially theischiococcygeus, is thought to receive innervationfrom S5.115 The most superficial layer of pelvic floormuscles (BC, IC, and transverse perineal) is inner-vated on its inferior aspect by distal (perineal)branches of the pudendal nerve.2,8,67,118
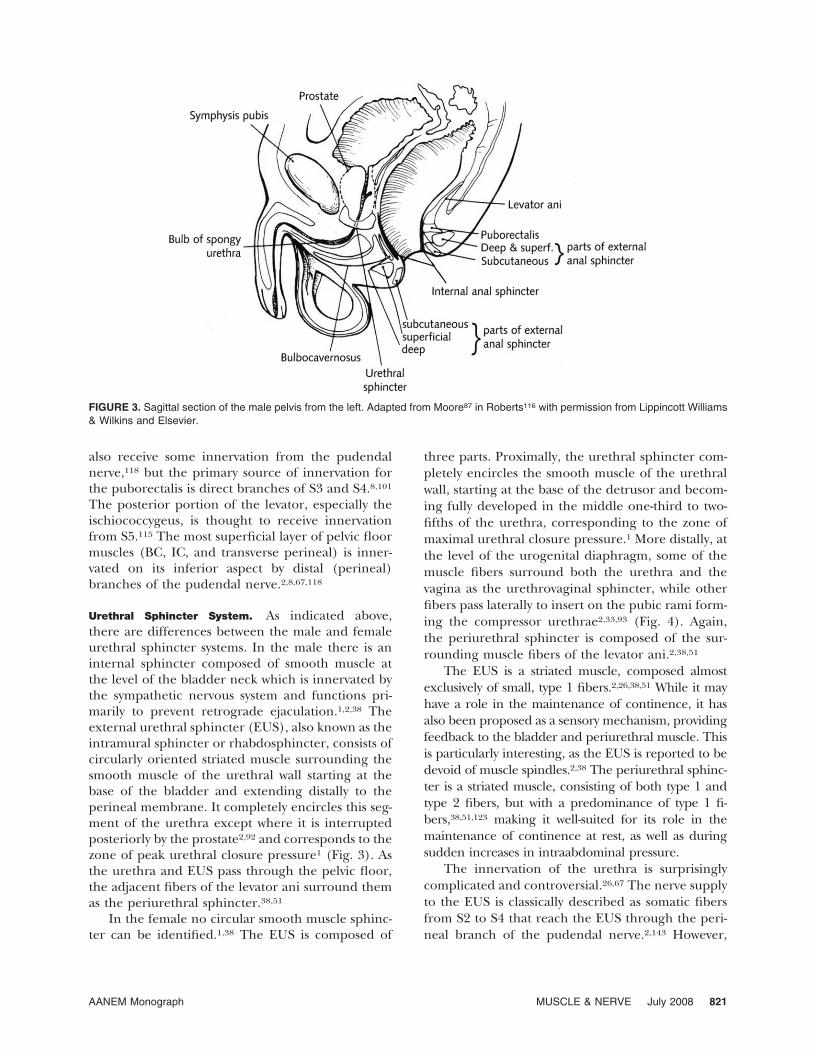
Urethral Sphincter System. As indicated above,there are differences between the male and femaleurethral sphincter systems. In the male there is aninternal sphincter composed of smooth muscle atthe level of the bladder neck which is innervated bythe sympathetic nervous system and functions pri-marily to prevent retrograde ejaculation.1,2,38 Theexternal urethral sphincter (EUS), also known as theintramural sphincter or rhabdosphincter, consists ofcircularly oriented striated muscle surrounding thesmooth muscle of the urethral wall starting at thebase of the bladder and extending distally to theperineal membrane. It completely encircles this seg-ment of the urethra except where it is interruptedposteriorly by the prostate2,92 and corresponds to thezone of peak urethral closure pressure1 (Fig. 3). Asthe urethra and EUS pass through the pelvic floor,the adjacent fibers of the levator ani surround themas the periurethral sphincter.38,51
In the female no circular smooth muscle sphinc-ter can be identified.1,38 The EUS is composed of
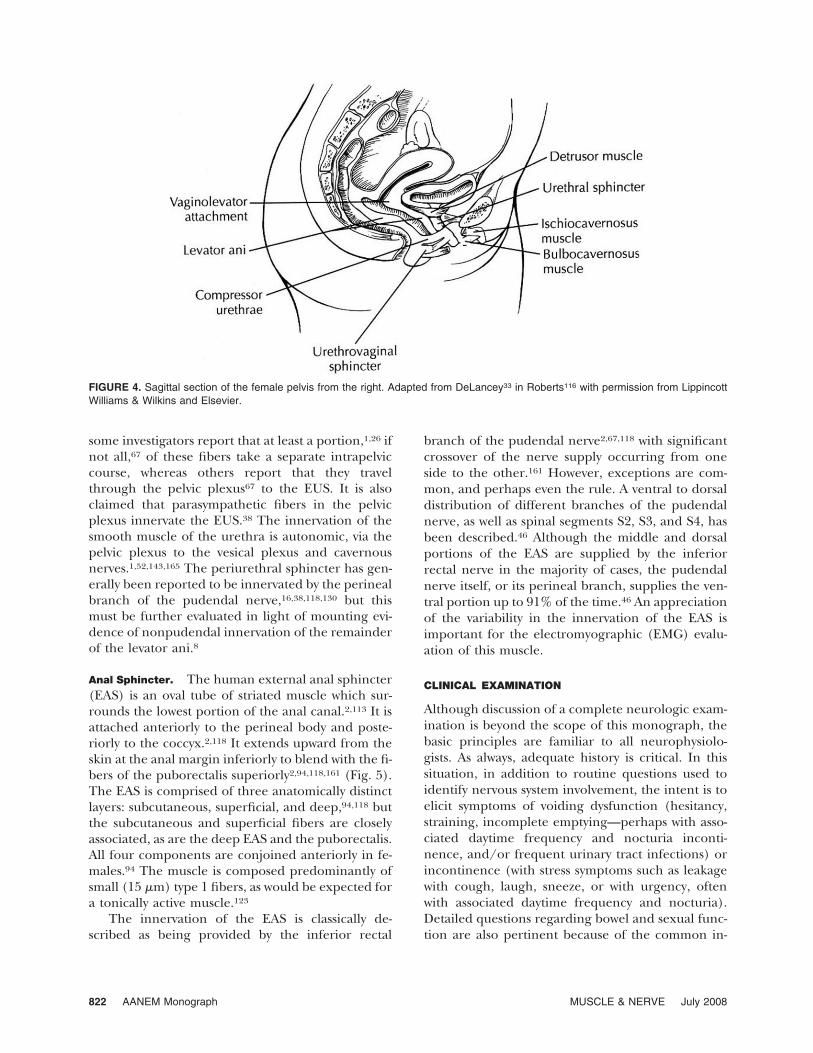
three parts. Proximally, the urethral sphincter com-pletely encircles the smooth muscle of the urethralwall, starting at the base of the detrusor and becom-ing fully developed in the middle one-third to two-fifths of the urethra, corresponding to the zone ofmaximal urethral closure pressure.1 More distally, atthe level of the urogenital diaphragm, some of themuscle fibers surround both the urethra and thevagina as the urethrovaginal sphincter, while otherfibers pass laterally to insert on the pubic rami form-ing the compressor urethrae2,33,93 (Fig. 4). Again,the periurethral sphincter is composed of the sur-rounding muscle fibers of the levator ani.2,38,51
The EUS is a striated muscle, composed almostexclusively of small, type 1 fibers.2,26,38,51 While it mayhave a role in the maintenance of continence, it hasalso been proposed as a sensory mechanism, providingfeedback to the bladder and periurethral muscle. Thisis particularly interesting, as the EUS is reported to bedevoid of muscle spindles.2,38 The periurethral sphinc-ter is a striated muscle, consisting of both type 1 andtype 2 fibers, but with a predominance of type 1 fi-bers,38,51,123 making it well-suited for its role in themaintenance of continence at rest, as well as duringsudden increases in intraabdominal pressure.
The innervation of the urethra is surprisinglycomplicated and controversial.26,67 The nerve supplyto the EUS is classically described as somatic fibersfrom S2 to S4 that reach the EUS through the peri-neal branch of the pudendal nerve.2,143 However,
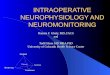
FIGURE 3. Sagittal section of the male pelvis from the left. Adapted from Moore87 in Roberts116 with permission from Lippincott Williams& Wilkins and Elsevier.
AANEM Monograph MUSCLE & NERVE July 2008 821
some investigators report that at least a portion,1,26 ifnot all,67 of these fibers take a separate intrapelviccourse, whereas others report that they travelthrough the pelvic plexus67 to the EUS. It is alsoclaimed that parasympathetic fibers in the pelvicplexus innervate the EUS.38 The innervation of thesmooth muscle of the urethra is autonomic, via thepelvic plexus to the vesical plexus and cavernousnerves.1,52,143,165 The periurethral sphincter has gen-erally been reported to be innervated by the perinealbranch of the pudendal nerve,16,38,118,130 but thismust be further evaluated in light of mounting evi-dence of nonpudendal innervation of the remainderof the levator ani.8
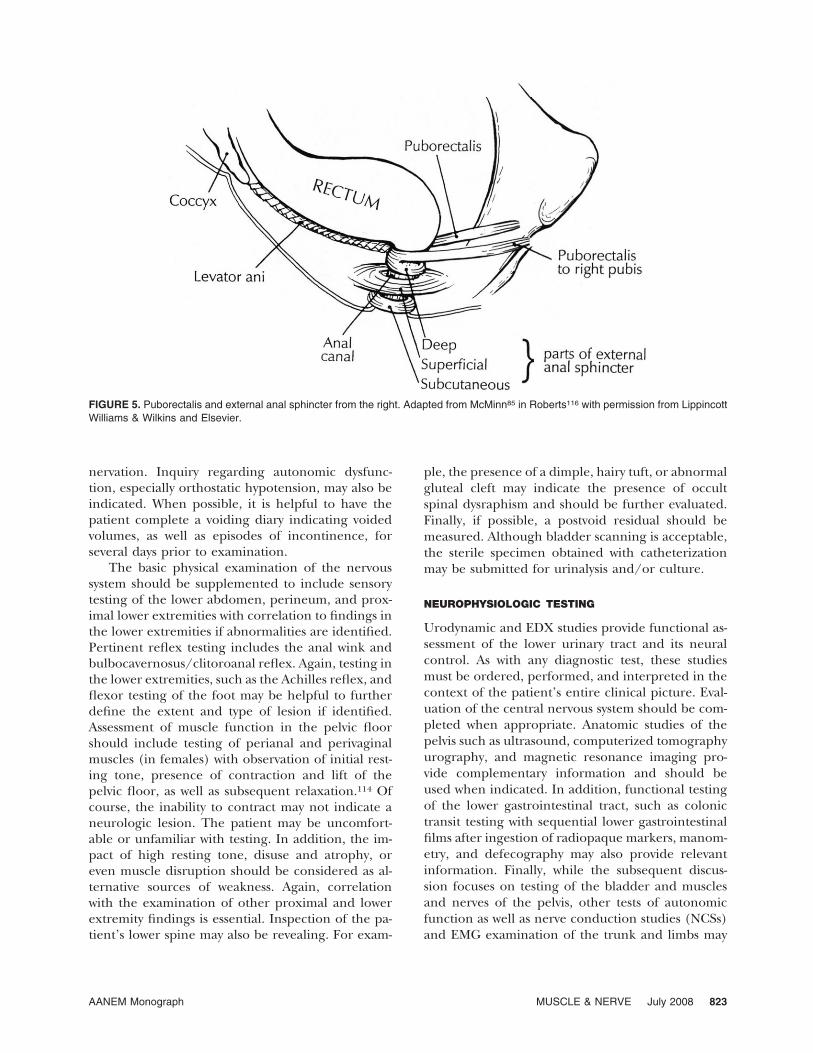
Anal Sphincter. The human external anal sphincter(EAS) is an oval tube of striated muscle which sur-rounds the lowest portion of the anal canal.2,113 It isattached anteriorly to the perineal body and poste-riorly to the coccyx.2,118 It extends upward from theskin at the anal margin inferiorly to blend with the fi-bers of the puborectalis superiorly2,94,118,161 (Fig. 5).The EAS is comprised of three anatomically distinctlayers: subcutaneous, superficial, and deep,94,118 butthe subcutaneous and superficial fibers are closelyassociated, as are the deep EAS and the puborectalis.All four components are conjoined anteriorly in fe-males.94 The muscle is composed predominantly ofsmall (15 �m) type 1 fibers, as would be expected fora tonically active muscle.123
The innervation of the EAS is classically de-scribed as being provided by the inferior rectal
branch of the pudendal nerve2,67,118 with significantcrossover of the nerve supply occurring from oneside to the other.161 However, exceptions are com-mon, and perhaps even the rule. A ventral to dorsaldistribution of different branches of the pudendalnerve, as well as spinal segments S2, S3, and S4, hasbeen described.46 Although the middle and dorsalportions of the EAS are supplied by the inferiorrectal nerve in the majority of cases, the pudendalnerve itself, or its perineal branch, supplies the ven-tral portion up to 91% of the time.46 An appreciationof the variability in the innervation of the EAS isimportant for the electromyographic (EMG) evalu-ation of this muscle.
CLINICAL EXAMINATION
Although discussion of a complete neurologic exam-ination is beyond the scope of this monograph, thebasic principles are familiar to all neurophysiolo-gists. As always, adequate history is critical. In thissituation, in addition to routine questions used toidentify nervous system involvement, the intent is toelicit symptoms of voiding dysfunction (hesitancy,straining, incomplete emptying—perhaps with asso-ciated daytime frequency and nocturia inconti-nence, and/or frequent urinary tract infections) orincontinence (with stress symptoms such as leakagewith cough, laugh, sneeze, or with urgency, oftenwith associated daytime frequency and nocturia).Detailed questions regarding bowel and sexual func-tion are also pertinent because of the common in-
FIGURE 4. Sagittal section of the female pelvis from the right. Adapted from DeLancey33 in Roberts116 with permission from LippincottWilliams & Wilkins and Elsevier.
822 AANEM Monograph MUSCLE & NERVE July 2008
nervation. Inquiry regarding autonomic dysfunc-tion, especially orthostatic hypotension, may also beindicated. When possible, it is helpful to have thepatient complete a voiding diary indicating voidedvolumes, as well as episodes of incontinence, forseveral days prior to examination.
The basic physical examination of the nervoussystem should be supplemented to include sensorytesting of the lower abdomen, perineum, and prox-imal lower extremities with correlation to findings inthe lower extremities if abnormalities are identified.Pertinent reflex testing includes the anal wink andbulbocavernosus/clitoroanal reflex. Again, testing inthe lower extremities, such as the Achilles reflex, andflexor testing of the foot may be helpful to furtherdefine the extent and type of lesion if identified.Assessment of muscle function in the pelvic floorshould include testing of perianal and perivaginalmuscles (in females) with observation of initial rest-ing tone, presence of contraction and lift of thepelvic floor, as well as subsequent relaxation.114 Ofcourse, the inability to contract may not indicate aneurologic lesion. The patient may be uncomfort-able or unfamiliar with testing. In addition, the im-pact of high resting tone, disuse and atrophy, oreven muscle disruption should be considered as al-ternative sources of weakness. Again, correlationwith the examination of other proximal and lowerextremity findings is essential. Inspection of the pa-tient’s lower spine may also be revealing. For exam-
ple, the presence of a dimple, hairy tuft, or abnormalgluteal cleft may indicate the presence of occultspinal dysraphism and should be further evaluated.Finally, if possible, a postvoid residual should bemeasured. Although bladder scanning is acceptable,the sterile specimen obtained with catheterizationmay be submitted for urinalysis and/or culture.
NEUROPHYSIOLOGIC TESTING
Urodynamic and EDX studies provide functional as-sessment of the lower urinary tract and its neuralcontrol. As with any diagnostic test, these studiesmust be ordered, performed, and interpreted in thecontext of the patient’s entire clinical picture. Eval-uation of the central nervous system should be com-pleted when appropriate. Anatomic studies of thepelvis such as ultrasound, computerized tomographyurography, and magnetic resonance imaging pro-vide complementary information and should beused when indicated. In addition, functional testingof the lower gastrointestinal tract, such as colonictransit testing with sequential lower gastrointestinalfilms after ingestion of radiopaque markers, manom-etry, and defecography may also provide relevantinformation. Finally, while the subsequent discus-sion focuses on testing of the bladder and musclesand nerves of the pelvis, other tests of autonomicfunction as well as nerve conduction studies (NCSs)and EMG examination of the trunk and limbs may
FIGURE 5. Puborectalis and external anal sphincter from the right. Adapted from McMinn85 in Roberts116 with permission from LippincottWilliams & Wilkins and Elsevier.
AANEM Monograph MUSCLE & NERVE July 2008 823

be necessary to define the extent of abnormalitiesshould they be identified.
Prior to testing, these procedures should be fullyexplained to the patient.109,116 If voiding is to bemonitored the patient should be asked to avoid uri-nating prior to arrival in the clinic. Otherwise, thepatient should be given the opportunity to use aprivate toilet immediately prior to testing. After re-moving the undergarments, the patient should bedraped appropriately in a warm, secure room. Aurodynamics chair may accommodate both urody-namic and EDX testing. Alternatively, the patientmay be positioned on his or her side or supine withthe legs gently spread apart or placed in stirrups forEDX testing. If needle or wire EMG is planned,anesthetic cream containing 2.5% lidocaine and2.5% prilocaine (EMLA cream by Astra, Westbor-ough, Minnesota) may be applied periurethrallyand/or perianally 20 min prior to needle insertion.The ground electrode may be placed on the proxi-mal thigh. If a reference electrode is required, it maybe placed on the mons pubis or on the ipsilateralproximal thigh.
URODYNAMIC TESTING
Urodynamic testing generally refers to any/all of aseries of functional tests used to assess lower urinarytract storage and/or emptying.1,56,62,113,137 Methodsrange from simple noninvasive procedures such asuroflowmetry to highly sophisticated and invasivetechniques such as videocystometrography. Testingis tailored to the individual patient depending onthe nature of the clinical picture, much as variousEDX tests are performed to investigate a patient’snervous system. While urodynamic testing is indi-rect, it documents various aspects of bladder andsphincter function, allowing inferences to be maderegarding peripheral somatic and autonomic, as wellas central nervous system function in the context ofthe patient’s clinical picture. It is the best tool avail-able for the investigation of sacral parasympatheticactivity.18
The goal of urodynamic testing is to reproducethe patient’s symptoms while monitoring the lowerurinary tract to provide an objective description of itsfunction and/or dysfunction. Abnormalities are notspecific for a particular diagnosis, but facilitate iden-tification of pathophysiology and contribute to diag-nosis, prognosis, and ultimately, implementation ofoptimum management.1,56,122,137 Unfortunately, thenature of the study makes it prone to artifact and thismust always be considered in the interpretation ofresults.62
Most patients with neurologic impairment andlower urinary tract signs or symptoms should un-dergo urodynamic testing to characterize the func-tion of the bladder, the urethra, the pelvic floor, andtheir coordination.1,43,56,91,113 Indications includecentral nervous system lesions such as stroke,119,120spinal cord injury,68,157 and multiple sclerosis,20,79and peripheral nervous system disorders such ascauda equina syndrome108 and diabetic neuropathywith cystopathy,27,64 as well as combined disorderssuch as myelodysplasia (e.g., in which testing is indi-cated within the first months of life to direct appro-priate management and prevent upper urinary tractinjury).14,126 Exceptions are the few diseases in whichempirical, conservative therapy can be safely imple-mented56 (e.g., incontinence following corticalstroke without associated urinary retention) withsubsequent urodynamic testing if management isunsuccessful. Of course, testing may also be helpfulin identifying neurologic involvement.
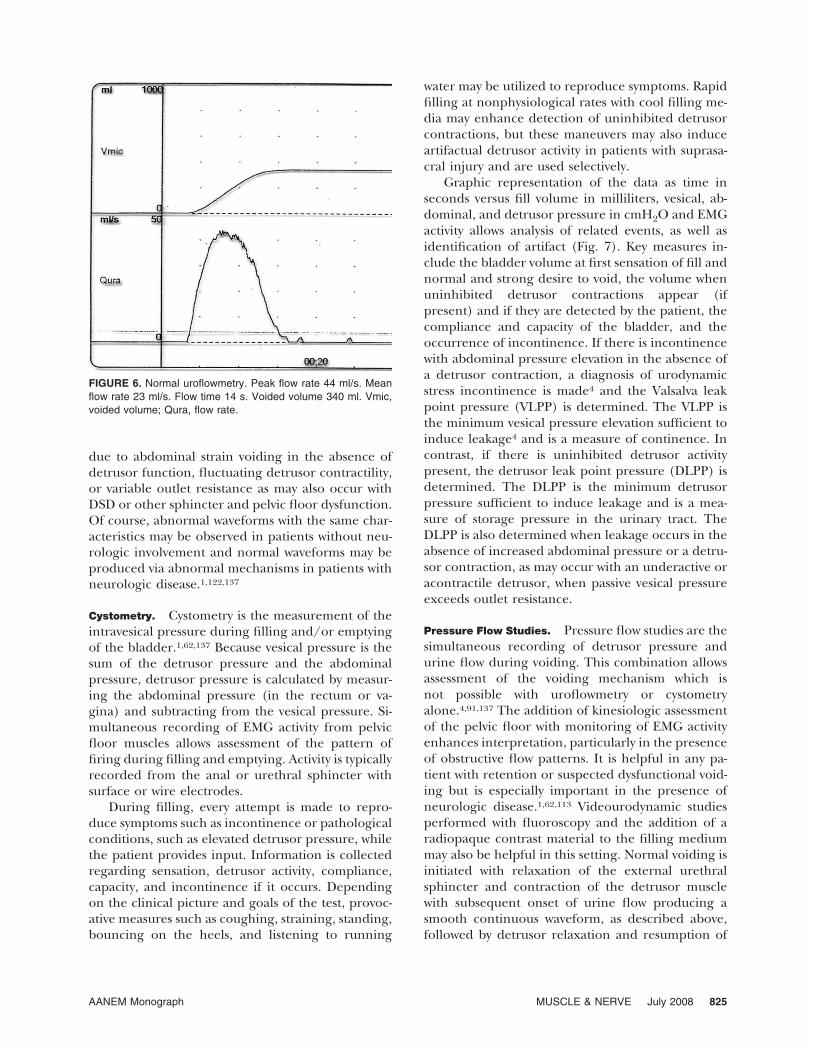
Uroflowmetry. Uroflowmetry is a simple, noninva-sive study of bladder emptying performed by mea-suring urine flow during voiding.1,91,122,137 Ideally,this study is done after a patient arrives with a com-fortably full bladder (with a minimum of 150–200ml) because flow is influenced by the voided volume.However, it is often impossible for patients to complywith this request due to urgency, frequency, and/orincontinence, and artificial filling may be required.After uroflowmetry, the postvoid residual is deter-mined with ultrasound or catheterization to deter-mine adequacy of emptying and to allow calculationof the total volume in the bladder. The data areusually displayed as a graph of urine flow in millili-ters versus time in seconds. The normal shape of thecurve is a smooth, continuous, slightly asymmetricbell curve which reaches its peak in the first third offlow (Fig. 6). Key measures include maximum andmean flow rates, voided volume, and flow time. Re-sults are nonspecific because flow is determined by acombination of abdominal pressure, detrusor pres-sure, and outflow resistance, but they provide a rea-sonable screen of voiding function when normal. Inaddition, this approach is most likely to documentthe patient’s typical flow pattern because the studycan be performed before examination or instrumen-tation of any kind. It can then be compared with datacollected subsequently with catheters and othermonitors in place.
Patients with neurologic impairment may havereduced flow, due to impaired detrusor contractilityor because of outlet obstruction such as detrusorsphincter dyssynergia (DSD). Flow may be irregular
824 AANEM Monograph MUSCLE & NERVE July 2008
due to abdominal strain voiding in the absence ofdetrusor function, fluctuating detrusor contractility,or variable outlet resistance as may also occur withDSD or other sphincter and pelvic floor dysfunction.Of course, abnormal waveforms with the same char-acteristics may be observed in patients without neu-rologic involvement and normal waveforms may beproduced via abnormal mechanisms in patients withneurologic disease.1,122,137
Cystometry. Cystometry is the measurement of theintravesical pressure during filling and/or emptyingof the bladder.1,62,137 Because vesical pressure is thesum of the detrusor pressure and the abdominalpressure, detrusor pressure is calculated by measur-ing the abdominal pressure (in the rectum or va-gina) and subtracting from the vesical pressure. Si-multaneous recording of EMG activity from pelvicfloor muscles allows assessment of the pattern offiring during filling and emptying. Activity is typicallyrecorded from the anal or urethral sphincter withsurface or wire electrodes.
During filling, every attempt is made to repro-duce symptoms such as incontinence or pathologicalconditions, such as elevated detrusor pressure, whilethe patient provides input. Information is collectedregarding sensation, detrusor activity, compliance,capacity, and incontinence if it occurs. Dependingon the clinical picture and goals of the test, provoc-ative measures such as coughing, straining, standing,bouncing on the heels, and listening to running
water may be utilized to reproduce symptoms. Rapidfilling at nonphysiological rates with cool filling me-dia may enhance detection of uninhibited detrusorcontractions, but these maneuvers may also induceartifactual detrusor activity in patients with suprasa-cral injury and are used selectively.
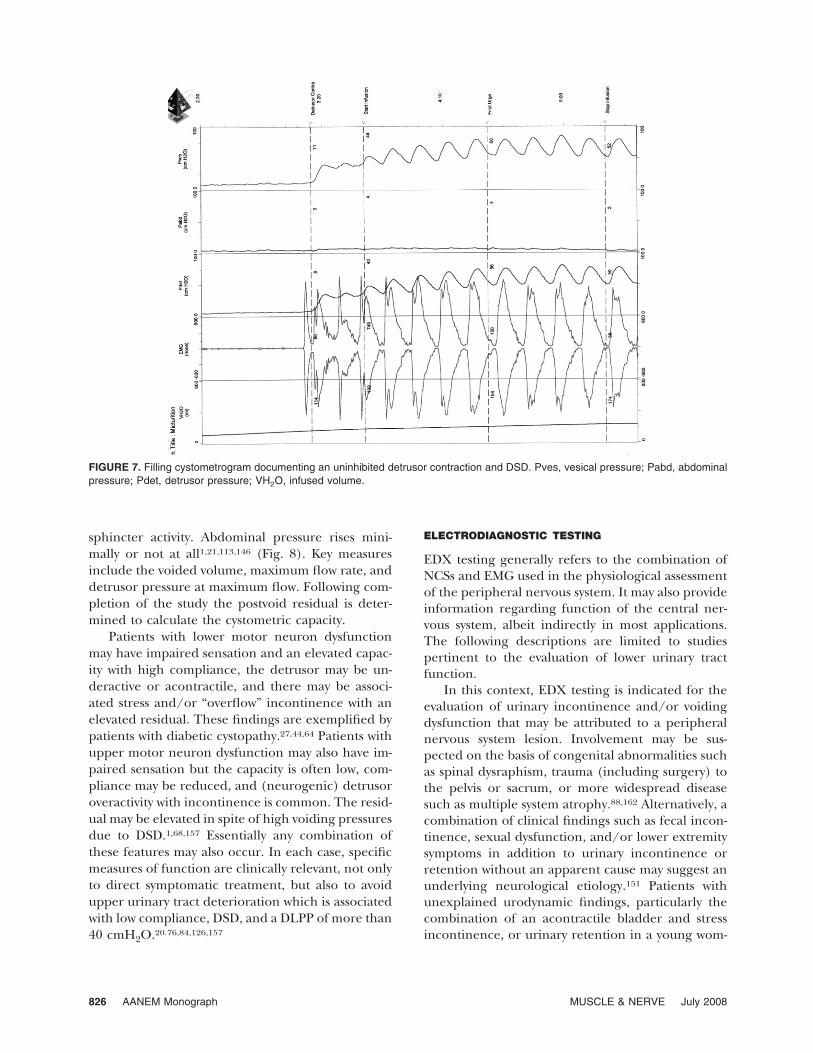
Graphic representation of the data as time inseconds versus fill volume in milliliters, vesical, ab-dominal, and detrusor pressure in cmH2O and EMGactivity allows analysis of related events, as well asidentification of artifact (Fig. 7). Key measures in-clude the bladder volume at first sensation of fill andnormal and strong desire to void, the volume whenuninhibited detrusor contractions appear (ifpresent) and if they are detected by the patient, thecompliance and capacity of the bladder, and theoccurrence of incontinence. If there is incontinencewith abdominal pressure elevation in the absence ofa detrusor contraction, a diagnosis of urodynamicstress incontinence is made4 and the Valsalva leakpoint pressure (VLPP) is determined. The VLPP isthe minimum vesical pressure elevation sufficient toinduce leakage4 and is a measure of continence. Incontrast, if there is uninhibited detrusor activitypresent, the detrusor leak point pressure (DLPP) isdetermined. The DLPP is the minimum detrusorpressure sufficient to induce leakage and is a mea-sure of storage pressure in the urinary tract. TheDLPP is also determined when leakage occurs in theabsence of increased abdominal pressure or a detru-sor contraction, as may occur with an underactive oracontractile detrusor, when passive vesical pressureexceeds outlet resistance.
Pressure Flow Studies. Pressure flow studies are thesimultaneous recording of detrusor pressure andurine flow during voiding. This combination allowsassessment of the voiding mechanism which isnot possible with uroflowmetry or cystometryalone.4,91,137 The addition of kinesiologic assessmentof the pelvic floor with monitoring of EMG activityenhances interpretation, particularly in the presenceof obstructive flow patterns. It is helpful in any pa-tient with retention or suspected dysfunctional void-ing but is especially important in the presence ofneurologic disease.1,62,113 Videourodynamic studiesperformed with fluoroscopy and the addition of aradiopaque contrast material to the filling mediummay also be helpful in this setting. Normal voiding isinitiated with relaxation of the external urethralsphincter and contraction of the detrusor musclewith subsequent onset of urine flow producing asmooth continuous waveform, as described above,followed by detrusor relaxation and resumption of
FIGURE 6. Normal uroflowmetry. Peak flow rate 44 ml/s. Meanflow rate 23 ml/s. Flow time 14 s. Voided volume 340 ml. Vmic,voided volume; Qura, flow rate.
AANEM Monograph MUSCLE & NERVE July 2008 825
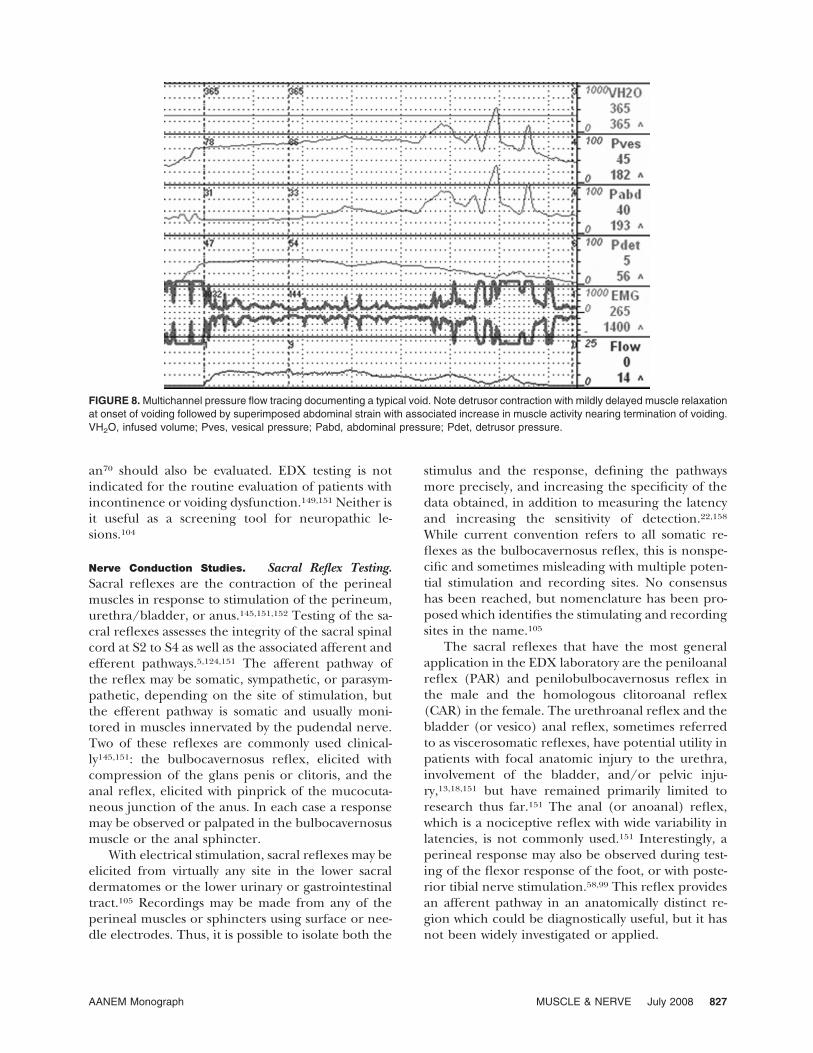
sphincter activity. Abdominal pressure rises mini-mally or not at all1,21,113,146 (Fig. 8). Key measuresinclude the voided volume, maximum flow rate, anddetrusor pressure at maximum flow. Following com-pletion of the study the postvoid residual is deter-mined to calculate the cystometric capacity.
Patients with lower motor neuron dysfunctionmay have impaired sensation and an elevated capac-ity with high compliance, the detrusor may be un-deractive or acontractile, and there may be associ-ated stress and/or “overflow” incontinence with anelevated residual. These findings are exemplified bypatients with diabetic cystopathy.27,44,64 Patients withupper motor neuron dysfunction may also have im-paired sensation but the capacity is often low, com-pliance may be reduced, and (neurogenic) detrusoroveractivity with incontinence is common. The resid-ual may be elevated in spite of high voiding pressuresdue to DSD.1,68,157 Essentially any combination ofthese features may also occur. In each case, specificmeasures of function are clinically relevant, not onlyto direct symptomatic treatment, but also to avoidupper urinary tract deterioration which is associatedwith low compliance, DSD, and a DLPP of more than40 cmH2O.20.76,84,126,157
ELECTRODIAGNOSTIC TESTING
EDX testing generally refers to the combination ofNCSs and EMG used in the physiological assessmentof the peripheral nervous system. It may also provideinformation regarding function of the central ner-vous system, albeit indirectly in most applications.The following descriptions are limited to studiespertinent to the evaluation of lower urinary tractfunction.
In this context, EDX testing is indicated for theevaluation of urinary incontinence and/or voidingdysfunction that may be attributed to a peripheralnervous system lesion. Involvement may be sus-pected on the basis of congenital abnormalities suchas spinal dysraphism, trauma (including surgery) tothe pelvis or sacrum, or more widespread diseasesuch as multiple system atrophy.88,162 Alternatively, acombination of clinical findings such as fecal incon-tinence, sexual dysfunction, and/or lower extremitysymptoms in addition to urinary incontinence orretention without an apparent cause may suggest anunderlying neurological etiology.151 Patients withunexplained urodynamic findings, particularly thecombination of an acontractile bladder and stressincontinence, or urinary retention in a young wom-
FIGURE 7. Filling cystometrogram documenting an uninhibited detrusor contraction and DSD. Pves, vesical pressure; Pabd, abdominalpressure; Pdet, detrusor pressure; VH2O, infused volume.
826 AANEM Monograph MUSCLE & NERVE July 2008
an70 should also be evaluated. EDX testing is notindicated for the routine evaluation of patients withincontinence or voiding dysfunction.149,151 Neither isit useful as a screening tool for neuropathic le-sions.104
Nerve Conduction Studies. Sacral Reflex Testing.Sacral reflexes are the contraction of the perinealmuscles in response to stimulation of the perineum,urethra/bladder, or anus.145,151,152 Testing of the sa-cral reflexes assesses the integrity of the sacral spinalcord at S2 to S4 as well as the associated afferent andefferent pathways.5,124,151 The afferent pathway ofthe reflex may be somatic, sympathetic, or parasym-pathetic, depending on the site of stimulation, butthe efferent pathway is somatic and usually moni-tored in muscles innervated by the pudendal nerve.Two of these reflexes are commonly used clinical-ly145,151: the bulbocavernosus reflex, elicited withcompression of the glans penis or clitoris, and theanal reflex, elicited with pinprick of the mucocuta-neous junction of the anus. In each case a responsemay be observed or palpated in the bulbocavernosusmuscle or the anal sphincter.
With electrical stimulation, sacral reflexes may beelicited from virtually any site in the lower sacraldermatomes or the lower urinary or gastrointestinaltract.105 Recordings may be made from any of theperineal muscles or sphincters using surface or nee-dle electrodes. Thus, it is possible to isolate both the
stimulus and the response, defining the pathwaysmore precisely, and increasing the specificity of thedata obtained, in addition to measuring the latencyand increasing the sensitivity of detection.22,158While current convention refers to all somatic re-flexes as the bulbocavernosus reflex, this is nonspe-cific and sometimes misleading with multiple poten-tial stimulation and recording sites. No consensushas been reached, but nomenclature has been pro-posed which identifies the stimulating and recordingsites in the name.105
The sacral reflexes that have the most generalapplication in the EDX laboratory are the peniloanalreflex (PAR) and penilobulbocavernosus reflex inthe male and the homologous clitoroanal reflex(CAR) in the female. The urethroanal reflex and thebladder (or vesico) anal reflex, sometimes referredto as viscerosomatic reflexes, have potential utility inpatients with focal anatomic injury to the urethra,involvement of the bladder, and/or pelvic inju-ry,13,18,151 but have remained primarily limited toresearch thus far.151 The anal (or anoanal) reflex,which is a nociceptive reflex with wide variability inlatencies, is not commonly used.151 Interestingly, aperineal response may also be observed during test-ing of the flexor response of the foot, or with poste-rior tibial nerve stimulation.58,99 This reflex providesan afferent pathway in an anatomically distinct re-gion which could be diagnostically useful, but it hasnot been widely investigated or applied.
FIGURE 8.Multichannel pressure flow tracing documenting a typical void. Note detrusor contraction with mildly delayed muscle relaxationat onset of voiding followed by superimposed abdominal strain with associated increase in muscle activity nearing termination of voiding.VH2O, infused volume; Pves, vesical pressure; Pabd, abdominal pressure; Pdet, detrusor pressure.
AANEM Monograph MUSCLE & NERVE July 2008 827
Peniloanal/Clitoroanal Reflex. The PAR/CAR uti-lizes pudendal nerve afferent and efferent pathways,as well as the sacral roots and sacral spinal cord withsuprasacral modulation during voiding.124 In themale the reflex is elicited by stimulating the dorsalnerve of the penis with either ring electrodes on theglans and shaft of the penis or with a standard bipo-lar stimulator at the base of the penis with the cath-ode proximal. The response is recorded from theEAS with a surface or needle electrode.19,145,152 It isalso convenient to record with a surface electrode onan anal plug inserted into the anus to record fromthe anal sphincter.48 However, this electrode doesnot allow for unilateral recording. The reflex mayalso be recorded from the BC muscle5,47,74,106,163 orthe EUS.22,58,124,145,152 In the female the reflex iselicited with transcutaneous stimulation of the dor-sal nerve of the clitoris on either side of the base ofthe clitoris.155 The response is recorded from theEAS with either needle or surface electrodes as indi-cated above.
Adequate stimulation intensity is important toelicit the response and most laboratories report theuse of 3–4 times the sensory threshold,47,112,158 butresponses are sometimes elicited at higher intensi-ties.5,111,148 Paired stimuli (2–5 ms apart) may also benecessary to facilitate the response even in normalindividuals and the response should not be consid-ered absent with single stimuli.18,58,109,147,151 An ini-tial, oligosynaptic response is recorded which is sta-ble and does not habituate. A second componentwith a longer latency has also been described, but itis less consistently identified as a discreet responseand may require higher stimulation intensity to elic-
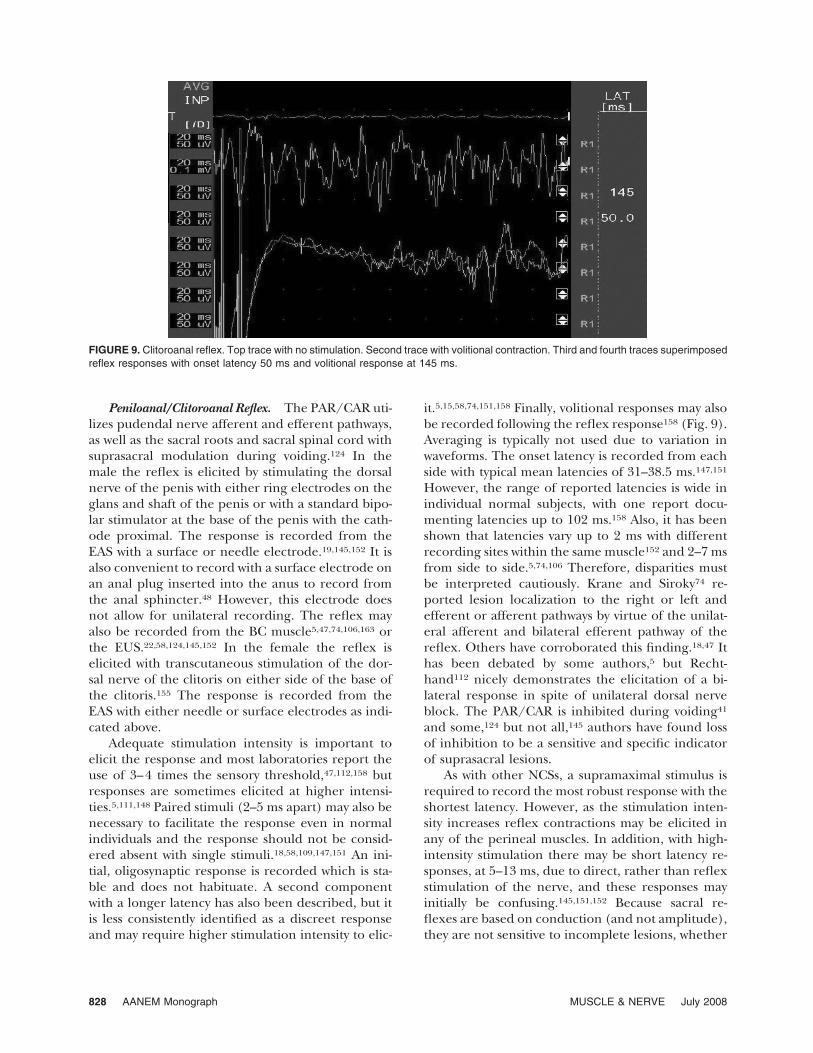
it.5,15,58,74,151,158 Finally, volitional responses may alsobe recorded following the reflex response158 (Fig. 9).Averaging is typically not used due to variation inwaveforms. The onset latency is recorded from eachside with typical mean latencies of 31–38.5 ms.147,151However, the range of reported latencies is wide inindividual normal subjects, with one report docu-menting latencies up to 102 ms.158 Also, it has beenshown that latencies vary up to 2 ms with differentrecording sites within the same muscle152 and 2–7 msfrom side to side.5,74,106 Therefore, disparities mustbe interpreted cautiously. Krane and Siroky74 re-ported lesion localization to the right or left andefferent or afferent pathways by virtue of the unilat-eral afferent and bilateral efferent pathway of thereflex. Others have corroborated this finding.18,47 Ithas been debated by some authors,5 but Recht-hand112 nicely demonstrates the elicitation of a bi-lateral response in spite of unilateral dorsal nerveblock. The PAR/CAR is inhibited during voiding41and some,124 but not all,145 authors have found lossof inhibition to be a sensitive and specific indicatorof suprasacral lesions.
As with other NCSs, a supramaximal stimulus isrequired to record the most robust response with theshortest latency. However, as the stimulation inten-sity increases reflex contractions may be elicited inany of the perineal muscles. In addition, with high-intensity stimulation there may be short latency re-sponses, at 5–13 ms, due to direct, rather than reflexstimulation of the nerve, and these responses mayinitially be confusing.145,151,152 Because sacral re-flexes are based on conduction (and not amplitude),they are not sensitive to incomplete lesions, whether
FIGURE 9. Clitoroanal reflex. Top trace with no stimulation. Second trace with volitional contraction. Third and fourth traces superimposedreflex responses with onset latency 50 ms and volitional response at 145 ms.
828 AANEM Monograph MUSCLE & NERVE July 2008

demyelinating or axonal. Thus, a normal responsedoes not exclude a lesion.150,151 Finally, most authorsreport difficulty eliciting the sacral reflexes in somenormal patients.15,145,148
Sacral reflex testing may be helpful in evaluatinglower motor neuron/peripheral nervous system le-sions of the conus, sacral roots, plexus, or branchesof the pudendal nerve.15,22,74,150,151,158 With a com-plete lesion, the reflex is absent. An incompletelesion may be associated with a prolonged latencyand a diminished or absent response. However, toreiterate, a normal response does not exclude alesion. It is also important to note that even mark-edly prolonged latencies may be associated with nor-mal bladder and sphincter function, as has beendocumented in patients with hereditary motor andsensory demyelinating neuropathy.153 Finally, an un-usually short latency has been documented in casesof tethered cord syndrome and should not be disre-garded.60 Thus far, sensitivity and specificity of sacralreflexes have not been determined and clinical rel-evance has not been clearly demonstrated.147
Somatosensory Evoked Potentials. Somatosensoryevoked potentials (SEPs) are waveforms recordedfrom the peripheral and central nervous system afteractivation of afferent nerve fibers.18,40,151 Large-di-ameter myelinated afferent fibers from the urogen-ital region and lower extremities generate impulseswhich enter the spinal cord and travel rostrally in theipsilateral dorsal columns, synapse in the nucleusgracilis, and cross to the contralateral brainstem tocontinue rostrally as the medial lemniscus and ter-minate in the ventral posterolateral thalamic nucleus(VPL). Neurons in the VPL project to the somato-sensory cortex. An additional pathway in the spi-nomedullothalamic tract may also participate intransmission of these impulses.40 The somatosensoryregion representing the urogenital region and lowerextremity is located along the medial aspect of thecerebral hemisphere.
SEPs may be used clinically to investigate conduc-tion in neural pathways extending from the periph-eral site of stimulation to the parietal sensory cortex.The tibial SEP is a routine study with well-establishedtechniques and normal values for evaluation of L4 toS2(S3)2 pathways from the lower extremity and willnot be discussed here. The pudendal SEP with S2 toS4 pathways from the pelvis is sometimes used in anattempt to evaluate urologic function more specifi-cally. It is elicited with stimulation of the dorsalnerve of the penis or the dorsal nerve of the clitorisusing ring or bar electrodes, as indicated above forthe sacral reflexes.40,47,97 Stimulation intensity is set
at 2–4 times the sensory threshold and cortical po-tentials are recorded from Cz� with reference to Fzor Fpz. One hundred to five hundred responses areaveraged and then repeated to document reproduc-ibility. The potential is readily elicited and consists ofa positive peak, with amplitudes of 0.5–12�V,138,147,148 designated as P1 or P40 (with a normalrange of 30–49 ms)40,47,59,148,164 followed by a seriesof additional waveforms which are more variable andof uncertain significance.15,40,138,147,148,151 Ampli-tudes have not been found to discriminate betweennormal and pathologic responses.35,47,138 It shouldalso be noted that even experienced authors reportsome difficulty recording bilateral responses in allwomen.40,164 A spinal potential may be recorded inmen from T12 to L1 with reference to the iliac crestor spine, but it is difficult to record in women, likelydue to activation of small numbers of afferent fibers.It is also difficult to record in obese male subjectsand it is not routinely performed.40,151 The some-what slower conduction in the pudendal response,compared to that in the tibial response, has beenattributed to slower conducting spinal pathways.15
Although this technique is technically feasible,and theoretically appealing, its utility in the evalua-tion of urologic function is limited.109,151 For exam-ple, peripheral neuropathies which may affect thebladder, particularly if there is small fiber involve-ment44 that could be expected to involve the puden-dal sensory fibers. In general, EDX studies are moreappropriately performed in the limbs to make thediagnosis of a neuropathy and urodynamic testingprovides more useful information regarding bladderfunction. Further, in patients with diabetic neurop-athy, abnormal tibial SEPs were correlated with boththe presence of lower urinary tract symptoms andurodynamic abnormalities, while abnormal puden-dal SEPs were not.111 Central nervous system lesionsin these pathways are also more likely to be identi-fied with tibial SEPs. Even in patients with multiplesclerosis and bladder symptoms, the tibial SEP ismore likely to be abnormal than the pudendalSEP.117 In patients with urologic complaints but noother neurologic symptoms and a normal neuro-logic examination, pudendal SEPs are unlikely to beabnormal.35
In patients with acute, traumatic tetraplegic SCI,recovery of both bladder and urethral sphincterfunction correlate better with the American SpinalInjury Association (ASIA) score and tibial SEPs thanwith pudendal SEPs. However, if a pudendal SEP canbe elicited, at least some recovery of bladder func-tion can be predicted. In patients with acute para-plegic SCI, ASIA scores, tibial and pudendal SEPs are
AANEM Monograph MUSCLE & NERVE July 2008 829

all predictive of recovery of urethral sphincter func-tion but not of bladder function. The pudendalSSEP appears more sensitive than the tibial SSEP inthis regard.29 SEPs have also been elicited from theurethra and bladder in an attempt to assess transmis-sion along small unmyelinated autonomic afferentfibers.59 The proximal urethra or bladder is stimu-lated with a bipolar surface electrode mounted on aFoley catheter. (Use of monopolar stimulation withthe anode on the skin has been demonstrated tostimulate somatic afferent nerves and the bipolartechnique is used to minimize their activation.)59Cortical responses are recorded from Cz� referencedto Fz. The most prominent and reproducible poten-tial is a negative peak with a latency of �100 ms,though earlier components may be identified. Am-plitudes are low, typically less than 1 �V, and config-uration is variable, making it difficult to identify evenin some normal subjects.15,59,147,151 These factors, aswell as the requirement for placement of the ure-thral ring electrode, which is somewhat uncomfort-able, particularly in men, have limited its use. How-ever, if the response is present it may help exclude asubpontine lesion in patients with bladder dysfunc-tion.15
Pudendal Nerve Conduction Studies. In 1984 Kiffand Swash72,133 described a method for the transrec-tal stimulation of the pudendal nerve. The initialreports were enthusiastically received. The tech-nique was refined, commercially available electrodeswere produced, and studies were performed to de-velop normative data based on age, gender, andparity.72,77,96 Prolonged pudendal nerve latencieswere reported in obstetrical lesions, constipation,perineal descent, and fecal and urinary inconti-nence.67,71,72,127,129,131,132,134,136 Unfortunately, anumber of issues related to this approach are nowapparent and the utility of the test has been ques-tioned and found lacking.11,45,55,61,78,98,149,151 To per-form the study, the St. Mark’s electrode (Dantec,Skovlunde, Denmark) is affixed to the examiner’sgloved hand with a bipolar stimulating electrode atthe tip of the index finger and recording electrodesat the base of the finger. The finger is insertedvaginally or rectally and the pudendal nerve is stim-ulated as it reenters the pelvis near the ischial spine.The response of the inferior rectal nerve is recordedfrom the anal sphincter with the electrodes at thebase of the index finger (or with surface electrodesover the anal sphincter) as the pudendal nerve ter-minal motor latency (PNTML).72 Because the pu-dendal nerve branches distal to the stimulation site,the response from the perineal nerve (perineal
nerve terminal motor latency [PeNTML]) may alsobe recorded from the urethral sphincter with a bi-polar surface electrode mounted on a Foley cathe-ter.133 Typical latencies of 1.9 ms and 2.4 ms wereinitially reported to the anal sphincter and urethralsphincter, respectively,133 but the range reported innormal subjects is quite variable, from 1.4 to 5.6ms77,96 to the anal sphincter and 1.7 to 3.8 ms to theurethral sphincter.96 As with all NCSs, the terminalmotor latency is determined by the fastest responsewith axonal integrity. In this case, the stimulation siteis fixed (at the ischial spine) without measurementof the nerve pathway in spite of differences due topatient size or position of the perineum. Further, thedistance between the stimulation site and pickupchanges as the examiner positions the electrode toobtain an optimal waveform. Latencies are not onlyvariable, but curiously short when compared to an-tidromic sensory responses recorded with this tech-nique5 or to other motor conduction techniquesusing transperineal stimulation.100,152 In addition,the response may be absent or uninterpretable in upto 30% of studies even in experienced laborato-ries.55,159 Due to local anatomy, it is not possible tostimulate a second site; thus, a nerve conductionvelocity cannot be obtained. Neither is it possible tolocalize focal changes in myelination if they arepresent.
Anatomical factors which may be confoundingthe technique include the proximity of the sacralnerve branches to the levator muscle near the ischialspine where stimulation occurs.8 In addition, therecording site is over multiple components of thesphincter mechanism, including the puborectalisand all the layers of the EAS. Studies using sacralmagnetic stimulation with needle recording elec-trodes in each muscle of the sphincter mechanismhave documented the shortest latency to the pubo-rectalis, with increasing latencies to the deep, super-ficial, and subcutaneous EAS with differences of 5.0ms or more from deepest to most superficial.121 Si-multaneous recordings of latencies with surface elec-trodes and needle electrodes may be similar, havedifferent responses, or even be present in one andabsent in the other.45
The amplitude of the response, which would pro-vide information regarding axonal integrity, has notbeen reliable. This may be due to anatomic factors asabove, but it is also likely influenced by positioningof both the active and the reference electrodes overthe sphincter muscle. While the contribution of thereference electrode has not been systematically stud-ied, this configuration likely reduces the amplitudeand may have other unrecognized consequences as
830 AANEM Monograph MUSCLE & NERVE July 2008

well.10 Finally, correlation with function has notbeen demonstrated.45,98,142,159
Theoretically, in spite of these limitations, pu-dendal nerve stimulation could be useful in distin-guishing an upper motor neuron lesion from a lowermotor neuron lesion if a response is obtained. It alsohas potential utility in differentiating axonotmesisfrom neurotmesis but clinical queries of this type areuncommon. It has been used to optimize stimulatorplacement during neuromodulation17 and it mayhave a role in monitoring acute change, particularlyfor research purposes. However, routine use of thistechnique cannot be recommended.11,45,151
Electromyography. As with muscles in other areas ofthe body, EMG of the pelvic floor may be performedwith various surface electrodes, fine wire electrodes,or needle electrodes. Selection is determined pri-marily by the type of information required and theease and comfort of application, but other factorssuch as cost and examiner familiarity may also beconsidered. Surface electrodes are noninvasive andeasy to apply but not all muscles are accessible andspecificity is limited by volume conduction. They areuseful for monitoring the presence or absence ofactivity, and may provide kinesiologic data duringurodynamic testing.1,116,151 Fine wire electrodes havethe additional advantages of precise and stable place-ment, even during provocative testing for inconti-nence and voiding, with less susceptibility to volumeconduction, but they are more invasive. In addition,after placement, wires may not be relocated. Investi-gation of specific muscle fiber and motor unit activ-ity, such as insertional and spontaneous activity, mo-tor unit action potential (MUAP) morphology, andrecruitment requires needle EMG. This approachalso allows accurate localization, with the option ofrepositioning as needed. The application of quanti-tative analysis to needle EMG provides automaticmeasurement of amplitude, duration, area, numberof phases and turns, rise time and duration of neg-ative peak, and mean frequency of firing with calcu-lation of thickness and size index.54,89,110,156 Single-fiber EMG has also been used extensively72,130,136 todetermine fiber density as an index of reinnervation,but is primarily limited to research applications.151
All findings on needle EMG are nonspecific andmust be interpreted based on the electrophysiologyof muscle, in the context of the patient’s clinicalpicture, to establish the most likely underlying pro-cess.39,69 Previous urethral or anal procedures,sphincter defects, or obstetric trauma and repairsshould be noted. Interpretation of needle EMG find-ings in the sphincters is further complicated by sev-
eral unique features of which the EDX physicianmust be aware. Normal MUAPs may have low ampli-tudes (with mean values of 300–600 �V but individ-ual units of 50–200 �V)18,21,37,54 and short duration(with mean values of 5–7 ms but individual units of3 ms)18,37,54,110 with complexity in as many as 15%–30% of units examined with concentric needleEMG.49,147,156 Thus, it may be difficult to identifyand/or differentiate changes reflective of myogenic(and/or neurogenic) involvement.115,139,149,151 Also,normal sphincter muscles are tonically active15,21,37and most patients are unable to completely relaxthem, except during normal reflex inhibition of thepelvic floor during voiding.15,21,144 The combinationof these factors may make it difficult to distinguishfibrillation potentials from MUAPs.88
The selection of muscles for examination followsthe principles common to all needle EMG studiesand is determined with thoughtful consideration ofboth the ease of examination and the amount ofdiscomfort to the patient, as well as the diagnosticinformation to be gained. As all relevant pelvic floormuscles are innervated by several sacral nerve roots,any normal muscle may suffice to exclude a diagno-sis of cauda equina syndrome if deemed a sufficientsample based on the clinical setting. However, oncean abnormality is identified, additional studies arerequired with evaluation of both pudendal- and non-pudendal-innervated muscles to determine the ex-tent of involvement. If only pudendal-innervatedmuscle is involved, consideration should be given toevaluation of muscles innervated by the perineal andthe inferior rectal branches to further localize thesite of the environment. Disparate findings havebeen well documented between the EUS and EAS aswell as other muscles of the pelvic floor.21,37,62,145,146Alternative strategies may be appropriate for theselection of muscles in other clinical settings. Forexample, the EAS is often selected for the assessmentof sphincter involvement in atypical parkinsonism.In contrast, the EUS must be included in the evalu-ation of urinary retention in a woman with possibleFowler’s syndrome.70 A protocol for the examinationof the pelvic floor has been proposed by Podnar andVodusek109 and may serve as a guide.
Even with thorough investigation, it is not alwayspossible to clearly define the site of injury, particu-larly in proximal lesions, such as the cauda equina,because paraspinal abnormalities are not presentdue to the lack of sacral innervation. The picturemay be further complicated if multiple lesions existand/or confounding issues such as previous surgeryor obstetric trauma coexist. In spite of these limita-tions, needle EMG is the most informative tool in the
AANEM Monograph MUSCLE & NERVE July 2008 831

evaluation of focal lesions in this group of patients,documenting the integrity or involvement of theperipheral nervous system, defining the severity,and contributing to the diagnosis and progno-sis.109,147,149,151
External Urethral Sphincter. The EUS has a fun-damental role in maintenance of urinary continenceand in voiding. Assessment is critical in the diagnosisof Fowler’s syndrome.70 Examination provides infor-mation about the integrity of the sacral roots andplexus, the pudendal nerve, and the perineal nervebranch.
In the female the EUS may be approachedtransvaginally or periurethrally. The transvaginalapproach is theoretically less painful, as the vagi-nal wall has a relative absence of pain fibers andspecialized sensory nerve endings.80 However,while comparison of the two approaches docu-mented higher pain scores with periurethral ex-amination, patients reported mild to moderatepain with both methods and the difference was notsignificant.95 Furthermore, twice as many MUAPswere identified using the periurethral technique.In this approach, 20 min after the application ofanesthetic cream, a 25-mm needle electrode isinserted �5 mm anterior or lateral to the urethralmeatus and advanced 10–20 mm while listeningfor EMG activity21,37,80,95,115,116 (Fig. 4).
In the male the EUS is usually examined with atransperineal approach. A 75-mm needle is insertedin the midline, �4 cm anterior to the anus at thebase of the penis and advanced toward the apex ofthe prostate. Localization may be facilitated by pal-pation of the apex of the prostate in the rectum, butthe finger should be withdrawn as the needle elec-trode is inserted21,37,115 (Fig. 3).
Bulbocavernosus. The BC muscle is easily acces-sible in the male and provides information about theintegrity of the sacral roots and plexus, the pudendalnerve, and the perineal nerve branch. Thus, it mayserve as an alternative to the EUS in the appropriatesetting. It may facilitate identification of musclemembrane irritability, as it is not tonically active atrest.109 The muscle lies superficially behind the scro-tum on either side of midline in the perineal region,where it surrounds the bulb of the penis (Fig. 3).The needle electrode is inserted through the peri-neal skin about 1 cm lateral to the bulb of the penisand advanced toward midline until EMG activity isseen and heard. If the needle is inserted too farlaterally, the superficial transverse perineal musclemay be entered. Localization may be confirmed byhaving the patient cough or mimic terminal voiding.Alternatively, the muscle may be activated by elicit-
ing the BC reflex.5,115,116 Examination of the BCmuscle is not routinely performed in women.
External Anal Sphincter. The EAS is easily acces-sible and provides information about the integrity ofthe sacral roots and plexus, the pudendal nerve, andthe inferior rectal nerve branch (except anteriorly).While examination of the subcutaneous fibers is the-oretically adequate to evaluate the integrity of theconus medullaris and cauda equina,103,107 it provideslimited sampling, and the sensitivity increases 18%with the additional examination of the “deeper” su-perficial and deep EAS muscle.103 In addition, thesuperficial and deep EAS muscles participate insphincter function while the subcutaneous fibers donot. Thus, their examination is particularly relevantin patients with anal incontinence. Examination isperformed with a 37- or 50-mm needle electrodedirected perpendicular to the skin 1 cm inside themucocutaneous junction.107 The subcutaneous por-tion of the muscle is encountered within the first 2–5mm. The needle is then directed medially, towardthe anal canal, and advanced until the superficialand deep muscles are entered at a depth of 1–5cm19,107,115 (Fig. 5).
Levator Ani. The levator ani provides informa-tion about the integrity of the sacral roots and hasthe distinction of nonpudendal innervation whichmay be helpful diagnostically. As this muscle is acontinuum of ill-defined regions which generallyfunction as a unit, isolating separate portions may bedifficult, and in many instances unnecessary. Thelevator is examined by inserting a 75-mm needleelectrode 1–2 cm outside the anal mucocutaneousjunction at the 3 to 4 o’clock or 8 to 9 o’clockposition (in dorsal lithotomy position) for the leftand right sides, respectively. The needle is advanceduntil EMG activity is identified 2–5 cm from the skinsurface102,125 (Fig. 2). In females the pubococcygeusis accessible just inside the vaginal introitus. Theneedle is inserted obliquely through the vaginal mu-cosa, while palpating the muscle with a digit of thecontralateral hand. Localization is facilitated if thepatient activates the muscle by squeezing as if todelay urination.73,81 Alternatively, the ischial spinemay serve as a landmark with needle placement me-dial and caudal to the ischial spine through thevaginal epithelium into the pubococcygeus/iliococ-cygeus.65,155,156 The puborectalis portion of thepubococcygeus is particularly useful in the evalua-tion of patients who have fecal incontinence becauseof the key role it plays in the maintenance of theanorectal angle. A 50- to 75-mm needle electrode isinserted 1 cm inside the mucocutaneous junctionbetween the 3 and 6 o’clock position on the left and
832 AANEM Monograph MUSCLE & NERVE July 2008

the 6 and 9 o’clock position on the right (in lithot-omy position). The electrode is directed mediallyand cephalad, paralleling the long axis of the rec-tum. The needle is advanced through the EAS toenter the puborectalis at a depth of 4–5 cm. In somecases, there is a subtle decrease in the EMG activitybetween the two muscles which is helpful in confirm-ing location. Localization may also be facilitated bypalpating the puborectalis sling posteriorly in therectum to estimate the depth required12,72,115,116(Fig. 5).
CONCLUSION
In conclusion, urodynamic and EDX studies arecomplementary tests of the neural pathways involvedin continence and voiding. While urodynamic test-ing is an indirect measure of neurologic function, itallows inferences to be made regarding peripheralsomatic and autonomic, as well as central nervoussystem integrity. Findings contribute to the diagnosisof bladder and pelvic floor dysfunction and are usedto direct clinical management. Urodynamic testing isindicated in most patients with known or suspectedneurologic disorders and lower urinary tract signs orsymptoms. EDX testing is a more direct measure ofneural integrity which assesses primarily somaticfunction and is recommended in a subset of patientswith incontinence or voiding dysfunction in whomthere is suspicion of a focal lesion in the peripheralnervous system or the conus. In this setting, sacralreflexes and needle EMG are most likely to be help-ful, with needle EMG the most informative investi-gation. EDX testing is not recommended for theroutine evaluation of patients with incontinence orvoiding dysfunction.
REFERENCES
1. Campbell’s urology. Philadelphia: Saunders; 2002.2. Gray’s anatomy. Edinburgh: Elsevier; 2005.3. Incontinence, 3rd International Consultation on Inconti-nence, June 26-29, 2004, Monaco. Health Publications; 2005.
4. Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, UlmstenU, et al. The standardisation of terminology of lower urinarytract function: report from the Standardisation Sub-commit-tee of the International Continence Society. Neurourol Uro-dyn 2002;21:167–178.
5. Amarenco G, Kerdraon J. Clinical value of ipsi- and con-tralateral sacral reflex latency measurement: a normativedata study in man. Neurourol Urodyn 2000;19:565–576.
6. American Diabetes Association. Study shows sharp rise incost of diabetes nationwide. American Diabetes Association.2-27-2003. Accessed: 7-19-2006.
7. Athwal BS, Berkley KJ, Hussain I, Brennan A, Craggs M,Sakakibara R, et al. Brain responses to changes in bladdervolume and urge to void in healthy men. Brain 2001;124:369–377.
8. Barber MD, Bremer RE, Thor KB, Dolber PC, Kuehl TJ,Coates KW. Innervation of the female levator ani muscles.Am J Obstet Gynecol 2002;187:64–71.
9. Barer DH, Mitchell JR. Predicting the outcome of acutestroke: do multivariate models help? Q J Med 1989;70:27–39.
10. Barkhaus PE, Nandedkar SD. Tibial motor conductionstudy: reference electrode contribution to the CMAP. Mus-cle Nerve 2005;32:396.
11. Barnett JL, Hasler WL, Camilleri M. American Gastroenter-ological Association medical position statement on anorectaltesting techniques. American Gastroenterological Associa-tion. Gastroenterology 1999;116:732–760.
12. Bartolo DC, Jarratt JA, Read MG, Donnelly TC, Read NW.The role of partial denervation of the puborectalis in idio-pathic faecal incontinence. Br J Surg 1983;70:664–667.
13. Basinski C, Fuller E, Brizendine EJ, Benson JT. Bladder-analreflex. Neurourol Urodyn 2003;22:683–686.
14. Bauer SB, Hallett M, Khoshbin S, Lebowitz RL, Winston KR,Gibson S, et al. Predictive value of urodynamic evaluation innewborns with myelodysplasia. JAMA 1984;252:650–652.
15. Beck R, Fowler CJ. Clinical neurophysiology in the investi-gation of genitourinary tract dysfunction. In: Rushton DN,editor. Handbook of neuro-urology. New York: MarcelDekkar; 1994. p 151–180.
16. Benson JT. Neurophysiologic control of lower urinary tract.Obstet Gynecol Clin North Am 1989;16:733–752.
17. Benson JT. Sacral nerve stimulation results may be improvedby electrodiagnostic techniques. Int Urogynecol J PelvicFloor Dysfunct 2000;11:352–357.
18. Benson JT. Clinical neurophysiologic techniques in urinaryand fecal incontinence. In: Bent AE, Ostergard DR, CundiffGW, Swift SE, editors. Ostergard’s urogynecology and pelvicfloor dysfunction. Philadelphia: Lippincott Williams &Wilkins; 2003. p 155–184.
19. Bilkey WJ, Awad EA, Smith AD. Clinical application of sacralreflex latency. J Urol 1983;129:1187–1189.
20. Blaivas JG, Barbalias GA. Detrusor-external sphincter dyssyn-ergia in men with multiple sclerosis: an ominous urologiccondition. J Urol 1984;131:91–94.
21. Blaivas JG, Labib KL, Bauer SB, Retik AB. A new approach toelectromyography of the external urethral sphincter. J Urol1977;117:773–777.
22. Blaivas JG, Zayed AA, Labib KB. The bulbocavernosus reflexin urology: a prospective study of 299 patients. J Urol 1981;126:197–199.
23. Blok BF. Brain control of the lower urinary tract. ScandJ Urol Nephrol Suppl 2002;11–15.
24. Blok BF. Central pathways controlling micturition and uri-nary continence. Urology 2002;59:13–17.
25. Blok BF, Willemsen AT, Holstege G. A PET study on braincontrol of micturition in humans. Brain 1997;120:111–121.
26. Borirakchanyavat S, Aboseif SR, Carroll PR, Tanagho EA,Lue TF. Continence mechanism of the isolated female ure-thra: an anatomical study of the intrapelvic somatic nerves.J Urol 1997;158:822–826.
27. Buck AC, Reed PI, Siddiq YK, Chisholm GD, Fraser TR.Bladder dysfunction and neuropathy in diabetes. Diabetolo-gia 1976;12:251–258.
28. Cervero F, Tattersall JE. Somatic and visceral sensory inte-gration in the thoracic spinal cord. Prog Brain Res 1986;67:189–205.
29. Curt A, Rodic B, Schurch B, Dietz V. Recovery of bladderfunction in patients with acute spinal cord injury: signifi-cance of ASIA scores and somatosensory evoked potentials.Spinal Cord 1997;35:368–373.
30. de Groat WC. Integrative control of the lower urinary tract:preclinical perspective. Br J Pharmacol 2006;147(Suppl 2):S25–S40.
31. de Groat WC, Fraser MO, Yoshiyama M, Smerin S, Tai C,Chancellor MB, et al. Neural control of the urethra. ScandJ Urol Nephrol Suppl 2001;35–43.
AANEM Monograph MUSCLE & NERVE July 2008 833
32. DeGroat W, Steers WD. Neuroanatomy and neurophysiologyof penile erection. In: Tanagho EA, Lue TF, McClure RD,editors. Contemporary Management of Impotence and In-fertility. Baltimore: Williams & Wilkins: 1988. p 3.
33. DeLancey JO. Correlative study of paraurethral anatomy.Obstet Gynecol 1986;68:91–97.
34. DeLancey JO, Richardson AC. Anatomy of genital support.In: Benson JT, editor. Female pelvic floor disorders. Investi-gation and management. New York: WW Norton; 1992.
35. Delodovici ML, Fowler CJ. Clinical value of the pudendalsomatosensory evoked potential. Electroencephalogr ClinNeurophysiol 1995;96:509–515.
36. Di Benedetto M. AAEE Minimonograph #4: Electromyogra-phy and nerve conduction in neuro-urology. Rochester, MN:American Association of Electromyography and Electrodiag-nosis; 1977.
37. DiBenedetto M, Yalla SV. Electrodiagnosis of striated ure-thral sphincter dysfunction. J Urol 1979;122:361–365.
38. Dixon J, Gosling J. Structure and innervation in the human.In: Torrens M, Morrison JFB, editors. The physiology of thelower urinary tract. London: Springer; 1987. p 3–22.
39. Dumitru D, Amato AA, Zwarts MJ. Electrodiagnostic medi-cine, 2nd ed. Philadelphia: Hanley & Belfus; 2002.
40. Dumitru D, Robinson LR, Zwarts MJ. Somatosensory evokedpotentials. In: Dumitru D, Amato AA, Zwarts MJ, editors.Electrodiagnostic medicine, 2nd ed. Philadelphia: Hanley &Belfus; 2002. p 357–413.
41. Dyro FM, Yalla SV. Refractoriness of urethral striated sphinc-ter during voiding: studies with afferent pudendal reflex arcstimulation in male subjects. J Urol 1986;135:732–736.
42. Epstein JI, The lower urinary tract and male genital system.In: Kumar V, Abbott R, Fausto N, editors. Pathologic basis ofdisease, 7th ed. Philadelphia: Elsevier Saunders; 2005.
43. Fantl JA, Newman DK, Colling J. Urinary incontinence inadults: acute and chronic management. AHCPR PublicationNo 96-0686 1996; Clinical Practice Guidelines, 1996 Update.
44. Fowler CJ. Neurological disorders of micturition and theirtreatment. Brain 1999;122:1213–1231.
45. Fowler CJ, Benson JT, Craggs MD, Vodusek DB, Yang CC,Podnar S. Clinical Neurophysiology. In: Abrams P, CardozoL, Khoury S, Wein A, editors. Incontinence. 2nd Interna-tional Consultation on Incontinence, 2001 July 1-3, Paris.Plymouth, UK: Health Publications; 2002. p 389–424.
46. Gagnard C, Godlewski G, Prat D, Lan O, Cousineau J, Mak-louf Y. The nerve branches to the external anal sphincter:the macroscopic supply and microscopic structure. Surg Ra-diol Anat 1986;8:115–119.
47. Galimberti V, Premoselli S, Passerini D, Cerri C. Sacral re-flexes normal values with monopolar short needle elec-trodes recording. Electromyogr Clin Neurophysiol 2001;41:457–462.
48. Galloway NT, Chisholm GD, McInnes A. Patterns and signif-icance of the sacral evoked response (the urologist’s kneejerk). Br J Urol 1985;57:145–147.
49. Gilad R, Giladi N, Korczyn AD, Gurevich T, Sadeh M. Quan-titative anal sphincter EMG in multisystem atrophy and 100controls. J Neurol Neurosurg Psychiatry 2001;71:596–599.
50. Gosling J. The structure of the bladder and urethra inrelation to function. Urol Clin North Am 1979;6:31–38.
51. Gosling JA, Dixon JS, Critchley HO, Thompson SA. A com-parative study of the human external sphincter and periure-thral levator ani muscles. Br J Urol 1981;53:35–41.
52. Gosling JA, Dixon JS, Jen PY. The distribution of noradren-ergic nerves in the human lower urinary tract. A review. EurUrol 1999;36(Suppl 1):23–30.
53. Gray M. Urinary retention: management in the acute caresetting. Part 1. Am J Nurs 2000;100:40–47.
54. Gregory WT, Clark AL, Johnson J, Willis K, Stuyvesant A, LouJS. Anal sphincter electromyography: editing of sampledmotor unit action potentials. Muscle Nerve 2005;31:256–259.
55. Gregory WT, Lou JS, Stuyvesant A, Clark AL. Quantitativeelectromyography of the anal sphincter after uncomplicatedvaginal delivery. Obstet Gynecol 2004;104:327–335.
56. Griffiths D, Kondo A, Bauer S, Diamant N, Liao L, Lose G, etal. Dynamic testing. In: Abrams P, Cardozo L, Khoury S,Wein A, editors. Incontinence. 3rd International Consulta-tion on Incontinence, 2004 June 26-29, Monaco. Plymouth,UK: Health Publications; 2005. Vol. 1, p 585–673.
57. Hackler RH. A 25-year prospective mortality study in thespinal cord injured patient: comparison with the long-termliving paraplegic. J Urol 1977;117:486–488.
58. Hallett M, Bauer S, Khoshbin S, Dyro F. Reflexes of theexternal urethral sphincter in children. Arch Neurol 1984;41:942–945.
59. Hansen MV, Ertekin C, Larsson LE. Cerebral evoked poten-tials after stimulation of the posterior urethra in man. Elec-troencephalogr Clin Neurophysiol 1990;77:52–58.
60. Hanson P, Rigaux P, Gilliard C, Biset E. Sacral reflex laten-cies in tethered cord syndrome. Am J Phys Med Rehabil1993;72:39–43.
61. Hill J, Hosker G, Kiff ES. Pudendal nerve terminal motorlatency measurements: what they do and do not tell us. Br JSurg 2002;89:1268–1269.
62. Homma Y, Batista J, Bauer S, Griffiths D, Hilton P, KramerG, et al. Urodynamics. In: Abrams P, Cardozo L, Khoury S,Wein A, editors. Incontinence. 2nd International Consulta-tion on Incontinence, 2001 July 1-3, Paris. Plymouth, UK:Health Publications; 2002.
63. Hu TW, Wagner TH, Bentkover JD, Leblanc K, Zhou SZ,Hunt T. Costs of urinary incontinence and overactive blad-der in the United States: a comparative study. Urology 2004;63:461–465.
64. Ioanid CP, Noica N, Pop T. Incidence and diagnostic aspectsof the bladder disorders in diabetics. Eur Urol 1981;7:211–214.
65. Jarvis SK, Abbott JA, Lenart MB, Steensma A, Vancaillie TG.Pilot study of botulinum toxin type A in the treatment ofchronic pelvic pain associated with spasm of the levator animuscles. Aust N Z J Obstet Gynaecol 2004;44:46–50.
66. Jones PN, Lubowski DZ, Swash M, Henry MM. Relationbetween perineal descent and pudendal nerve damage inidiopathic faecal incontinence. Int J Colorect Dis 1987;2:93–95.
67. Juenemann KP, Lue TF, Schmidt RA, Tanagho EA. Clinicalsignificance of sacral and pudendal nerve anatomy. J Urol1988;139:74–80.
68. Kaplan SA, Chancellor MB, Blaivas JG. Bladder and sphinc-ter behavior in patients with spinal cord lesions. J Urol1991;146:113–117.
69. Katirji B, Kaminski HJ, Preston DC, Ruff RL, Shapiro BE.Neuromuscular disorders in clinical practice. Boston: But-terworth-Heinemann; 2002.
70. Kavia RB, Datta SN, DasGupta R, Elneil S, Fowler CJ. Urinaryretention in women: its causes and management. BJU Int2006;97:281–287.
71. Kiff ES, Barnes PR, Swash M. Evidence of pudendal neurop-athy in patients with perineal descent and chronic strainingat stool. Gut 1984;25:1279–1282.
72. Kiff ES, Swash M. Slowed conduction in the pudendal nervesin idiopathic (neurogenic) faecal incontinence. Br J Surg1984;71:614–616.
73. Kjolhede P, Lindehammar H. Pelvic floor neuropathy inrelation to the outcome of Burch colposuspension. Int Uro-gynecol J Pelvic Floor Dysfunct 1997;8:61–65.
74. Krane RJ, Siroky MB. Studies on sacral-evoked potentials.J Urol 1980;124:872–876.
75. Kuhlemeier KV, Stover SL, Lloyd LK. Prophylactic antibac-terial therapy for preventing urinary tract infections in spinalcord injury patients. J Urol 1985;134:514–517.
76. Kurzrock EA, Polse S. Renal deterioration in myelodysplasticchildren: urodynamic evaluation and clinical correlates.J Urol 1998;159:1657–1661.
834 AANEM Monograph MUSCLE & NERVE July 2008
77. Lefaucheur J, Yiou R, Thomas C. Pudendal nerve terminalmotor latency: age effects and technical considerations. ClinNeurophysiol 2001;112:472–476.
78. Lefaucheur JP. Neurophysiological testing in anorectal dis-orders. Muscle Nerve 2006;33:324–333.
79. Lemack GE, Hawker K, Frohman E. Incidence of upper tractabnormalities in patients with neurovesical dysfunction sec-ondary to multiple sclerosis: analysis of risk factors at initialurologic evaluation. Urology 2005;65:854–857.
80. Lowe EM, Fowler CJ, Osborne JL, DeLancey JO. Improvedmethod for needle electromyography of the urethral sphinc-ter in women. Neurourol Urodyn 1994;13:29–33.
81. Lubowski DZ, King DW, Finlay IG. Electromyography of thepubococcygeus muscles in patients with obstructed defaeca-tion. Int J Colorectal Dis 1992;7:184–187.
82. Mattingly RF, Thompson JD. Anatomy of the Female Pelvis.Te Linde’s Operative Gynecology. Philadelphia: Lippincott;1985. p 41.
83. McDonald JS. Pain of childbirth. In: Loeser JD, editor. Boni-ca’s management of pain, vol. 2. Philadelphia: LippincottWilliams & Wilkins; 2001. p 1388–1414.
84. McGuire EJ, Woodside JR, Borden TA, Weiss RM. Prognosticvalue of urodynamic testing in myelodysplastic patients.J Urol 1981;126:205–209.
85. McMinn RMH. Last’s anatomy. Regional and applied. Lon-don: Churchill Livingstone; 1994.
86. Ministry of Health, Labour and Welfare. The level of stan-dard that Japan’s social security system has achieved. AnnualReports on Health and Welfare, 1998–1999 Social Securityand National Life. 1999.
87. Moore KL, Dalley AF. Clinically Oriented Anatomy. Balti-more: Williams & Wilkins; 1985. p 307.
88. Nahm F, Freeman R. Sphincter electromyography and mul-tiple system atrophy. Muscle Nerve 2003;28:18–26.
89. Nandedkar SD, Barkhaus PE. Quantitative electromyo-graphic analysis. In: Katirji B, Kaminski HJ, Preston DC, RuffRL, Shapiro BE, editors. Neuromuscular disorders in clinicalpractice. Boston: Butterworth-Heinemann; 2002. p 151–182.
90. Nour S, Svarer C, Kristensen JK, Paulson OB, Law I. Cerebralactivation during micturition in normal men. Brain 2000;123:781–789.
91. O’Donnell PD. Urinary Incontinence. St Louis: Mosby; 1997.92. Oelrich T. The urethral sphincter muscle in the male. Am J
Anat 1980;158:229–246.93. Oelrich TM. The striated urogenital sphincter muscle in the
female. Anat Rec 1983;205:223–232.94. Oh C, Kark AE. Anatomy of the external anal sphincter. Br J
Surg 1972;59:717–723.95. Olsen AL, Benson JT, McClellan E. Urethral sphincter nee-
dle electromyography in women: comparison of periurethraland transvaginal approaches. Neurourol Urodyn 1998;17:531–535.
96. Olsen AL, Ross M, Stansfield RB, Kreiter C. Pelvic floornerve conduction studies: establishing clinically relevantnormative data. Am J Obstet Gynecol 2003;189:1114–1119.
97. Opsomer RJ, Guerit JM, Wese FX, Van Cangh PJ. Pudendalcortical somatosensory evoked potentials. J Urol 1986;135:1216–1218.
98. Osterberg A, Graf W, Edebol Eeg-Olofsson K, Hynninen P,Pahlman L. Results of neurophysiologic evaluation in fecalincontinence. Dis Colon Rectum 2000;43:1256–1261.
99. Pedersen E, Harving H, Klemar B, Torring J. Human analreflexes. J Neurol Neurosurg Psychiatry 1978;41:813–818.
100. Pedersen E, Klemar B, Schroder HD, Torring J. Anal sphinc-ter responses after perianal electrical stimulation. J NeurolNeurosurg Psychiatry 1982;45:770–773.
101. Percy JP, Neill ME, Swash M, Parks AG. Electrophysiologicalstudy of motor nerve supply of pelvic floor. Lancet 1981;1:16–17.
102. Petersen I, Stener I. An electromyographical study of thestriated urethreal sphincter, the striated anal sphincter, and
the levator ani muscle during ejaculation. Electromyography1970;10:23–44.
103. Podnar S. Electromyography of the anal sphincter: whichmuscle to examine? Muscle Nerve 2003;28:377–379.
104. Podnar S. Critical reappraisal of referrals to electromyogra-phy and nerve conduction studies. Eur J Neurol 2005;12:150–155.
105. Podnar S. Nomenclature of the electrophysiologically testedsacral reflexes. Neurourol Urodyn 2006;25:95–97.
106. Podnar S. Neurophysiologic studies of the penilo-cavernosusreflex: normative data. Neurourol Urodyn 2007;26:864–869.
107. Podnar S, Rodi Z, Lukanovic A, Trsinar B, Vodusek DB.Standardization of anal sphincter EMG: technique of needleexamination. Muscle Nerve 1999;22:400–403.
108. Podnar S, Trsinar B, Vodusek DB. Bladder dysfunction inpatients with cauda equina lesions. Neurourol Urodyn 2006;25:23–31.
109. Podnar S, Vodusek DB. Protocol for clinical neurophysio-logic examination of the pelvic floor. Neurourol Urodyn2001;20:669–682.
110. Podnar S, Vodusek DB, Stalberg E. Comparison of quanti-tative techniques in anal sphincter electromyography. Mus-cle Nerve 2002;25:83–92.
111. Rapidi CA, Karandreas N, Katsifotis C, Benroubi M, Petro-poulou K, Theodorou C. A combined urodynamic and elec-trophysiological study of diabetic cystopathy. NeurourolUrodyn 2006;25:32–38.
112. Rechthand E. Bilateral bulbocavernosus reflexes: crossing ofnerve pathways or artifact? Muscle Nerve 1997;20:616–618.
113. Rivas DA, Chancellor MB. Neurogenic vesical dysfunction.Urol Clin North Am 1995;22:579–591.
114. Roberts M. Clinical neuroanatomy of the abdomen andpelvis: implications for surgical treatment of prolapse. ClinObstet Gynecol 2005;48:627–638.
115. Roberts MM, Barkhaus PE. Pelvic floor and related muscles.In: Nandedkar SD, editor. EMG on DVD: Electronic myo-anatomic atlas for clinical electromyography. CASA Engi-neering; 2005. p 103–116.
116. Roberts MM, Park TA. Pelvic floor function/dysfunction andelectrodiagnostic evaluation. Phys Med Rehabil Clin N Am1998;9:831–851.
117. Rodi Z, Vodusek DB, Denislic M. Pudendal nerve versustibial nerve somatosensory evoked potentials in patients withmultiple sclerosis and voiding dysfunction. Neurol Urodyn1994;13:362–363.
118. Rosse C, Gaddum-Rosse P. Hollinshead’s textbook of anat-omy. Philadelphia: Lippincott-Raven; 1997.
119. Sakakibara R, Hattori T, Yasuda K, Yamanishi T. Micturi-tional disturbance after acute hemispheric stroke: analysis ofthe lesion site by CT and MRI. J Neurol Sci 1996;137:47–56.
120. Sakakibara R, Hattori T, Yasuda K, Yamanishi T. Micturi-tional disturbance and the pontine tegmental lesion: urody-namic and MRI analyses of vascular cases. J Neurol Sci1996;141:105–110.
121. Sato T, Konishi F, Kanazawa K. Variations in motor evokedpotential latencies in the anal sphincter system with sacralmagnetic stimulation. Dis Colon Rectum 2000;43:966–970.
122. Schafer W, Abrams P, Liao L, Mattiasson A, Pesce F, Span-gberg A, et al. Good urodynamic practices: uroflowmetry,filling cystometry, and pressure-flow studies. Neurourol Uro-dyn 2002;21:261–274.
123. Schroder HD, Reske-Nielsen E. Fiber types in the striatedurethral and anal sphincters. Acta Neuropathol (Berl) 1983;60:278–282.
124. Sethi RK, Bauer SB, Dyro FM, Krarup C. Modulation of thebulbocavernosus reflex during voiding: loss of inhibition inupper motor neuron lesions. Muscle Nerve 1989;12:892–897.
125. Shafik A. Vesicolevator reflex. Description of a new reflexand its clinical significance. Urology 1993;41:96–100.
AANEM Monograph MUSCLE & NERVE July 2008 835
126. Sidi AA, Dykstra DD, Gonzalez R. The value of urodynamictesting in the management of neonates with myelodysplasia:a prospective study. J Urol 1986;135:90–93.
127. Smith AR, Hosker GL, Warrell DW. The role of pudendalnerve damage in the aetiology of genuine stress inconti-nence in women. Br J Obstet Gynaecol 1989;96:29–32.
128. Smith ED. Urinary prognosis in spina bifida. J Urol 1972;108:815–817.
129. Snooks SJ, Badenoch DF, Tiptaft RC, Swash M. Perinealnerve damage in genuine stress urinary incontinence. Anelectrophysiological study. Br J Urol 1985;57:422–426.
130. Snooks SJ, Barnes PR, Swash M. Damage to the innervationof the voluntary anal and periurethral sphincter muscula-ture in incontinence: an electrophysiological study. J NeurolNeurosurg Psychiatry 1984;47:1269–1273.
131. Snooks SJ, Barnes PR, Swash M, Henry MM. Damage to theinnervation of the pelvic floor musculature in chronic con-stipation. Gastroenterology 1985;89:977–981.
132. Snooks SJ, Henry MM, Swash M. Anorectal incontinence andrectal prolapse: differential assessment of the innervation topuborectalis and external anal sphincter muscles. Gut 1985;26:470–476.
133. Snooks SJ, Swash M. Perineal nerve and transcutaneousspinal stimulation: new methods for investigation of theurethral striated sphincter musculature. Br J Urol 1984;56:406–409.
134. Snooks SJ, Swash M, Mathers SE, Henry MM. Effect ofvaginal delivery on the pelvic floor: a 5-year follow-up. Br JSurg 1990;77:1358–1360.
135. Stenchever MA, Droegemueller W, Herbst AL, Mishell DR.Comprehensive Gynecology. St. Louis: Mosby; 2001. p 59.
136. Swash M, Snooks SJ, Henry MM. Unifying concept of pelvicfloor disorders and incontinence. J R Soc Med 1985;78:906–911.
137. Swinn MJ. Urodynamics. In: Fowler CJ, editor. Neurology ofbladder, bowel and sexual dysfunction, vol. 23. Boston: But-terworth-Heinemann; 1999. p 97–107.
138. Tackmann W, Vogel P, Porst H. Somatosensory evoked po-tentials after stimulation of the dorsal penile nerve: norma-tive data and results from 145 patients with erectile dysfunc-tion. Eur Neurol 1987;27:245–250.
139. Takahashi S, Homma Y, Fujishiro T, Hosaka Y, Kitamura T,Kawabe K. Electromyographic study of the striated urethralsphincter in type 3 stress incontinence: evidence of myogen-ic-dominant damages. Urology 2000;56:946–950.
140. The Endocrine Society. Diabetes/insulin. The EndocrineSociety. 2006. 7-19-2006.
141. Thom DH, Haan MN, Van Den Eeden SK. Medically recog-nized urinary incontinence and risks of hospitalization, nurs-ing home admission and mortality. Age Ageing 1997;26:367–374.
142. Thomas C, Lefaucheur JP, Galula G, de Parades V, Bour-guignon J, Atienza P. Respective value of pudendal nerveterminal motor latency and anal sphincter electromyogra-phy in neurogenic fecal incontinence. Neurophysiol Clin2002;32:85–90.
143. Thor KB. Serotonin and norepinephrine involvement inefferent pathways to the urethral rhabdosphincter: implica-tions for treating stress urinary incontinence. Urology 2003;62:3–9.
144. Uchio EM, Yang CC, Kromm BG, Bradley WE. Corticalevoked responses from the perineal nerve. J Urol 1999;162:1983–1986.
145. Vereecken RL, De Meirsman J, Puers B, Van Mulders J.Electrophysiological exploration of the sacral conus. J Neu-rol 1982;227:135–144.
146. Vereecken RL, Verduyn H. The electrical activity of theparaurethral and perineal muscles in normal and patholog-ical conditions. Br J Urol 1970;42:457–463.
147. Vodusek D, Fowler CJ. Clinical neurophysiology. In: FowlerCJ, editor. Neurology of bladder, bowel and sexual dysfunc-tion, vol. 23. Boston: Butterworth Heinemann; 1999. p 109–143.
148. Vodusek DB. Pudendal SEP and bulbocavernosus reflex inwomen. Electroencephalogr Clin Neurophysiol 1990;77:134–136.
149. Vodusek DB. The role of electrophysiology in the evaluationof incontinence and prolapse. Curr Opin Obstet Gynecol2002;14:509–514.
150. Vodusek DB. Bulbocavernous reflex revisited. NeurourolUrodyn 2003;22:681–682.
151. Vodusek DB, Amarenco G, Batra A, Benson T, Bharucha AE,Podnar S, et al. Clinical neurophysiology. In: Abrams P,Cardozo L, Khoury S, Wein A, editors. Incontinence, 3rdInternational Consultation on Incontinence, June 26-29,2004, Monaco. Plymouth, UK: Health Publications; 2005.Vol. 1, p 675–706.
152. Vodusek DB, Janko M, Lokar J. Direct and reflex responsesin perineal muscles on electrical stimulation. J Neurol Neu-rosurg Psychiatry 1983;46:67–71.
153. Vodusek DB, Zidar J. Pudendal nerve involvement in pa-tients with hereditary motor and sensory neuropathy. ActaNeurol Scand 1987;76:457–460.
154. Wagner TH, Hu TW. Economic costs of urinary inconti-nence in 1995. Urology 1998;51:355–361.
155. Weidner AC, Jamison MG, Branham V, South MM, BorawskiKM, Romero AA. Neuropathic injury to the levator ani oc-curs in 1 in 4 primiparous women. Am J Obstet Gynecol2006;195:1851–1856.
156. Weidner AC, Sanders DB, Nandedkar SD, Bump RC. Quan-titative electromyographic analysis of levator ani and exter-nal anal sphincter muscles of nulliparous women. Am JObstet Gynecol 2000;183:1249–1256.
157. Weld KJ, Graney MJ, Dmochowski RR. Clinical significanceof detrusor sphincter dyssynergia type in patients with post-traumatic spinal cord injury. Urology 2000;56:565–568.
158. Wester C, FitzGerald MP, Brubaker L, Welgoss J, Benson JT.Validation of the clinical bulbocavernosus reflex. NeurourolUrodyn 2003;22:589–592.
159. Williams AB, Malouf AJ, Bartram CI, Halligan S, Kamm MA,Kmiot WA. Assessment of external anal sphincter morphol-ogy in idiopathic fecal incontinence with endocoil magneticresonance imaging. Dig Dis Sci 2001;46:1466–1471.
160. Wu J, Baguley IJ. Urinary retention in a general rehabilita-tion unit: prevalence, clinical outcome, and the role ofscreening. Arch Phys Med Rehabil 2005;86:1772–1777.
161. Wunderlich M, Swash M. The overlapping innervation of thetwo sides of the external anal sphincter by the pudendalnerves. J Neurol Sci 1983;59:97–109.
162. Yamamoto T, Sakakibara R, Uchiyama T, Liu Z, Ito T, Awa Y,Yamamoto K, Kinou M, Yamanishi T, Hattori T. When isOnuf’s nucleus involved in multiple system atrophy? Asphincter electromyography study. J Neurol Neurosurg Psy-chiatry 2005;76:1645–1648.
163. Yang CC, Bradley WE. Reflex innervation of the bulbocav-ernosus muscle. BJU Int 2000;85:857–863.
164. Yang CC, Kromm BG. New techniques in female pudendalsomatosensory evoked potential testing. Somatosens MotRes 2004;21:9–14.
165. Yucel S, de Souza A Jr, Baskin LS. Neuroanatomy of thehuman female lower urogenital tract. J Urol 2004;172:191–195.
836 AANEM Monograph MUSCLE & NERVE July 2008