Embed Size (px)
Citation preview

Neuroimage
AbstractThe pathogenesis and neuropathology of reversible posterior leukoencephalopathy (RPLE;a clinical and radiographical syndrome linked to malignant hypertension, eclampsia,immunosuppressive drugs, and chemotherapy) remain poorly understood. Autopsies onpatients with hypertensive encephalopathy have demonstrated arteriolar fibrinoid necro-sis with micro-infarcts and failed to show brain edema; nonetheless, magnetic resonanceimagings (MRIs) of patients with RPLE generally show findings most consistent with vaso-genic edema. This article reports a patient with RPLE in whom brain biopsy revealed ede-matous white matter with no evidence of vessel wall damage or infarction. This supportsthe concept that the imaging changes on MRI represent vasogenic edema and suggests thatthe changes observed on autopsy in malignant hypertension may be an epiphenomenon.
Key Words: Reversible posterior leukoencephalopathy; hypertensive encephalopathy;brain edema; renal dialysis.
(Neurocrit. Care 2005;2:303–305)
303
Neuropathological Correlates of Reversible PosteriorLeukoencephalopathyDavid Schiff1,* and Maria-Beatriz Lopes2
1Divisions of Neuro-Oncology and 2Neuropathology University of Virginia Health Sciences Center,Charlottesville,VA
*For correspondence andreprints:
David SchiffDivision of Neuro-Oncology,University of VirginiaHealth Sciences Center,Box 800432, Charlottesville,VA 22908-0432.E-mail: [email protected]
Neurocritical CareCopyright © 2005 Humana Press Inc. All rights of any nature whatsoever are reserved.ISSN 1541-6933/05/2:303–305DOI: 10.1385/Neurocrit. Care 2005;2:303–305
Humana Press
Case ReportThis 60-year-old man presented with
abrupt onset of headache, seizures, restless-ness, and confusion. Blood pressure waselevated to as high as 220/120 mmHg, andhe had several focal left hemibody focalmotor seizures with secondary generaliza-tion on the night of admission prior to laps-ing into stupor. Medical history was notablefor sequential removal of both kidneys forrenal cell carcinoma; he had been on hemodi-alysis for 8 months. The patient had beendialyzed 1 day earlier and had driven him-self home afterward. BUN 1 week earlier was17, and postdialysis on the day of ictuswas 16. Magnetic resonance imaging (MRI;Figure 1) demonstrated multifocal, subcor-tical T2 hyperintensities most prominent inthe parieto-occipital regions bilaterally.Some of the lesions showed faint contrast
enhancement. Diffusion-weighted imageswere not obtained. Cerebrospinal fluid examrevealed acellular fluid with 240 mg/dL ofprotein. The differential diagnosis wasbelieved to include infection, demyelina-tion, gliomatosis, and metastases. Thepatient was placed on dexamethasone andphenytoin and underwent stereotactic rightparietal lobe brain biopsy 5 days after presentation. He made a slow, but full, neu-rological recovery over several weeks.Follow-up MRI revealed complete resolutionof his lesions.
The biopsy (Figure 2) revealed white matterwith mild, diffuse vacuolation with mildinflammatory reaction characterized by scat-tered macrophages and rare lymphocytes.Abundant reactive astrocytes were present.Toluidine-stained sections showed no evidenceof myelinopathy, and in situ hybridization for
04-50_schiff.qxd 12/07/2005 02:00 pm Page 303

304 _____________________________________________________________________________________________Schiff and Lopes
Neurocritical Care ♦ Volume 2, 2005
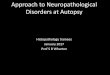
Fig. 1. (A) T2-weighted and (B) postgadolinium T1 MR scans demonstrate white matter T2 hyperintensities and small multifocal areas of con-trast enhancement most prominent in the parieto-occipital regions.
Fig. 2. Hematoxylin and eosin stains of right parietal brain biopsy. (A) White matter with mild vacuolation of the neuropil. (B) Higher magnifi-cation demonstrates intact myelinated fibers.
04-50_schiff.qxd 12/07/2005 02:00 pm Page 304

JC virus was negative. The findings were consistent with a non-specific process characterized by edematous white matter with-out evidence of demyelination, inflammatory process, orneoplasm.
DiscussionThis case report describes a patient with the clinical and
radiographical syndrome of reversible posterior leukoen-cephalopathy (RPLE), a constellation of findings that may beobserved with hypertensive encephalopathy, cyclosporinor tacrolimus toxicity, and eclampsia (1). The recent initiationof dialysis in this patient raises the possibility that thisrepresented a case of “dialysis dysequilibrium.” Although thepathophysiology of dialysis dysequilibrium may be distinct,a recent report suggests it may be part of the spectrum of RPLE(2). There has been a long debate regarding the pathogenesisof RPLE and hypertensive encephalopathy. Many have arguedthat sudden elevations in blood pressure exceed the autoreg-ulatory capacity of cerebral vessels, resulting in regions ofvasodilatation, focal breakdown of blood–brain barrier, andtransudation of fluid into brain parenchyma (3). Others haveproposed that overregulation leads to vasospasm and focalareas of cerebral ischemia. An autopsy study of neuropathol-ogy of patients who had experienced hypertensiveencephalopathy did not reveal cerebral edema, insteadreporting arteriolar fibrinoid necrosis and associated miliaryinfarctions. The authors concluded that the notion of cerebral
Reversible Posterior Leukoencephalopathy ________________________________________________________________________305
Neurocritical Care ♦ Volume 2, 2005
edema in hypertensive encephalopathy was unsupported bypathological evidence. More recently, however, diffusion-weighted MRI scans have suggested that the edema in RPLEis initially and primarily vasogenic (3).
To our knowledge, this is the first reported case of brainbiopsy in RPLE. The demonstration of white matter edemawithout evidence of fibrinoid necrosis or micro-infarction isconsistent with MRI findings of vasogenic edema withoutinfarction and suggests that RPLE or the dialysis dysequilib-rium syndrome may have distinct pathophysiology from thatof malignant hypertension (4).
AcknowledgmentWe appreciate the assistance of Julie Haught, RN, and
Jennifer Mabold, NP, in preparation of this manuscript.
References1. Hinchey J, Chaves C, Appignani B, et al. A reversible posterior
leukoencephalopathy syndrome. N Engl J Med 1996;334:494–500.2. Sheth KN, Wu GF, Messe SR, Wolf RL, Kasner SE. Dialysis dise-
quilibrium: another reversible posterior leukoencephalopathysyndrome? Clin Neurol Neurosurg 2003;105:249–252.
3. Schwartz RB, Feske SK, Polak JF, et al. Preeclampsia-eclampsia:clinical and neuroradiographic correlates and insights into thepathogenesis of hypertensive encephalopathy. Radiology2000;217:371–376.
4. Chester EM, Agamanolis DP, Banker BQ, Victor M. Hypertensiveencephalopathy: a clinicopathologic study of 20 cases. Neurology1978;28:928–939.
04-50_schiff.qxd 12/07/2005 02:00 pm Page 305