Embed Size (px)
Citation preview

APMIS 103: 54-58, 1995 Printed in Denmark . All rights reserved
Copvright 0 A P M l S 1995
Neuronal degeneration in subacute necrotizing encephalomyelopathy (Leigh’s disease)
Case report
C. E LINDBOE,’ A. K. LIE,’, S. T. AASE,’ 0. B. SCHJETNE’ and I. HAAVE’
IDepartment of Pathology, ’Department of Pediatrics, and 3MR-Center, Trondheim University Hospital, Trondheim, Norway
Lindboe, C. E, Lie, A. K., Aase, S. T., Schjetne, 0. B. & Haave, I . Neuronal degeneration in subacute necrotizing encephalomyelopathy (Leigh’s disease). Case report. APMIS 103: 5458, 1995.
We report clinical, radiological and pathological findings in a 5-year-old girl who died of subacute necrotizing encephalomyelopathy (SNE) after 4 weeks of illness. Autopsy revealed endothelial swelling and vacuolar degeneration of the neuropil in the brain, brain stem and cerebellum. In addition, the affected areas showed degeneration of the neurons which was different from anoxic nerve cell damage both with regard to morphological picture and topographical distribution. This neuronal degeneration was probably due to the underlying metabolic defect in SNE per se and resembled in several aspects the nerve cell changes seen in the thalami and inferior olives in active Wernicke’s encephalopathy. It is our opinion that more attention should be paid to the nerve cell degeneration in SNE rather than focusing on the relative preservation of these cells.
Key words: Degeneration; Leigh’s disease; nerve cells; subacute necrotizing encephalomyelopathy.
C. E Lindboe, Department of Pathology, Trondheim University Hospital, N-7006 Trondheim, Norway.
Subacute necrotizing encephalomyelopathy (SNE) or Leigh’s disease is an uncommon dis- ease mainly affecting infants and young children (14, 22). The clinical course may be stormy leading to death within a few weeks or it may progress insidiously for many years (9, 12, 14). Most cases are sporadic, but familial forms also occur (3, 8, 13). No consistent underlying metabolic defect has been deter- mined in SNE, but deficiency of cytochrome oxidase (1, 12, 13), pyruvate dehydrogenase complex (3, 17), pyruvate decarboxylase (6) and thiaminetriphosphate (2) have all been found. These deficiencies are similar to those seen in Wernicke’s encephalopathy, but treatment with thiamine has been without effect in SNE ( 3 , 7). The histopathological changes are widely dis-
Received October 19, 1994. Accepted November 14, 1994.
54
tributed throughout the brain, brain stem and spinal cord (14). Although of a different distri- bution, the lesions are similar to those seen in the mammillary bodies and periventricular locations in active Wernicke’s encephalopathy showing disintegration of the neuropil and en- dothelial swelling, but with a relative sparing of the neurons (5, 14, 16).
In this paper we report clinical, radiological and histopathological findings in a 5-year-old girl who died of SNE after 4 weeks of illness. The affected CNS areas revealed extensive neur- onal degeneration which was different from that seen in anoxia and which probably represents a reaction to the underlying metabolic disorder of SNE per se.
CASE REPORT
The patient was a 5-year-old previously healthy girl with a negative family history regarding neurological

NEURONAL DEGENERATION IN LEIGH’S DISEASE
diseases and early child deaths. There is one healthy younger brother. During a febrile episode the patient started to vomit. The fever disappeared after a few days, but vomiting several times a day persisted. After one week her parents noticed that she had periods with slurred speech and dysphasia, difficulty in recognizing people, and short periods with blurred consciousness. A weight loss of 5 kg was registered. On admission 10 days after the appearance of symp- toms, the patient was oriented and cooperated nor- mally. There were normal physical findings over the chest and abdomen. She was moderately dehydrated and intravenous rehydration was started. Metoclo- pramide was given against vomiting. Radiological examinations of chest and abdomen were normal as were abdominal ultrasound investigation and cer- ebral CT. EEG revealed slight unspecific abnormali- ties over both hemispheres. Blood samples revealed CRP 11 mg/l (normal <5) , haptoglobin 3.2 gil (nor- mal 0.2-2.2), ammonium 56 pmoM (normal <35) and lactate 1.4 mmol/l (normal 0.3-1.5). The CSF was physiologic. The patient’s clinical condition was stable during the next 10 days and she was able to play with other children, though she became easily tired. She was still vomiting now and then.
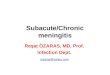
Eleven days after admission there was a dramatic worsening of the situation with acute onset of truncal ataxia, dysdiadochokinesia, dysarthria, dysphasia, nystagmus and diplopia. There were also involuntary movements of the eyes, the tongue and the extremi- ties. The patient responded only periodically to ver- bal contact and then answered with single words. At ophthalmoscopy there were blurred papillary mar- gins with hemorrhages on both sides. A cerebral MRI disclosed symmetrically increased signal inten- sity in the mammillary bodies, hypothalamus, medial parts of the thalami, and periventricular regions of the mesencephalon, pons and medulla oblongata (Fig. 1). Viral encephalitis with atypical distribution was suspected. EEG showed an unspecific slow activ- ity on both sides and SEP a lack of cortical re- sponses, indicating a transmission block in the brain stem and more centrally. The CSF was still normal.
All investigations with regard to infective agents were negative. The patient was treated with dexamethason 2 mgX4 and acyclovir sodium 400 mgx3. In spite of the treatment there was a gradual loss of conscious- ness. A SIADH syndrome was treated with diuretic drugs, fluid restriction and hypertonic saline solu- tions. On the 18th day there were episodes of apnoea which necessitated assisted ventilation. Cerebral CT revealed marked cerebral edema which was treated with large doses of dexamethason and mannitol. However, on the following day there was no intra- cranial blood flow at four-vessel cerebral angiogra- phy and the respirator was turned off.
Autopsy jindings Five-year-old girl, height 1 18 cm and weight 13 kg.
Macroscopic and microscopic examination of the thoracic and abdominal viscera revealed no signifi- cant pathological findings.
The brain was edematous and weighed 1450 g (nor- mal range 1050-1250 g), but there were no signs of herniation. Coronal sections showed symmetrical compression of the ventricles. Throughout both sides of the cerebral cortex there were small areas with punctate hemorrhages which in some places also affected the underlying white matter. There was a livid discoloration of the hypothalamic area, medial thalamus, periaqueductal gray matter, substantia nig- ra, floor of the 4th ventricle and inferior olives (Fig. 2). The spinal cord was not examined.
Histological examination revealed widespread
Fig. 1. Mesencephalon. T2-weighted MR image. In- creased signal intensity of periaqueductal region and substantia nigra bilaterally.
Fig. 2. Mesencephalon and medulla oblongata. Discoloration of the periventricular region, the sub- stantia nigra and the ventral medulla.
55

LINDBOE et al.
lesions in the brain, brain stem and cerebellum. The changes will be described according to their topo- graphical distribution.
Bruin. In multiple cortical locations on both sides of all four lobes there were areas with prominent en- dothelial swelling, perivascular hemorrhages and vacuolar degeneration of the neuropil with a slight macrophage reaction (Fig. 3a). In the affected areas the neurons were shrunken and angular with a pale pink or more strongly stained orange-red granular cytoplasm. The nuclei were pyknotic, but with intact nuclear membranes and distinct nucleoli (Fig. 3b). The adjacent white matter showed slight endothelial swelling and edema. In the hippocampi there were no neuronal changes in Sommer’s sector. Basal ganglia, thalamus and hypothalamus revealed focal lesions similar to those described on both sides of the cer- ebral cortex. The mammillary bodies were moder- ately affected.
Bruin stem. In the mesencephalon the changes were restricted to the substantia nigra and the raphe nu- clei, which revealed slight endothelial swelling, vacuo-
lar degeneration and groups of eosinophilic shrunken neurons. In the pons and medulla oblongata there were endothelial swelling, perivascular hemorrhages and vacuolar degeneration subependymally. The in- ferior olives on both sides revealed extensive loss of neurons and the remaining neurons showed various stages of eosinophilic degeneration.
Cerebellum. There was extensive involvement of the dentate nuclei which revealed vacuolar degeneration of the neuropil with infiltration of a few macro- phages. There was moderate swelling of the capillary endothelium. Unaffected neurons coexisted with others at various stages of degeneration. The latter had intense orange-red granular cytoplasm with blurred outlines and the nuceli showed different stages of pyknosis and karyolysis (Fig. 3c). The cere- bellar cortex was completely unaffected in all parts, including areas close to the severely affected dentate nuclei (Fig. 3d).
Electron microscopic examination of formalin- fixed specimens from brain, liver, kidney and heart was performed. The tissues were, however, badly pre-
Fig. 3. A: Cerebral cortex. Swelling of capillary endothelium, perivascular hemorrhages and slight vacuolar degeneration of the neuropil, HEX90. B: Cerebral cortex. Neurons showing shrunken cytoplasm and pyknotic nuclei, HEX 530. C: Dentate nucleus. Degenerated neurons (arrows) next to unaffected neurons, HEx220. D: Cerebellar cortex. Normal appearance of Purkinje cells and granular cells, HEX 220.
56

NEURONAL DEGENERATION IN LEIGH’S DISEASE
served and the findings must be regarded as incon- clusive.
DISCUSSION
The clinical course and the autopsy findings in the reported case are typical for subacute nec- rotizing encephalomyelopathy (SNE). SNE was not, however, suspected by the clinicians and a tentative diagnosis of encephalitis was made al- though no infective agent was found despite an intensive search. Postmortem examination of the CNS revealed widespread affection of cer- ebral cortex and adjacent white matter, basal ganglia, hypothalamus, brain stem and cerebel- lum. In addition to the characteristic disinte- gration of the neuropil and endothelial swelling, there was extensive degeneration of neurons in the affected areas. This neuronal degeneration was different from that seen in anoxic nerve cell damage both with regard to topographical dis- tribution and morphology. Thus, in our case the neuronal changes were restricted to areas of otherwise typical lesions of SNE whereas predi- lection sites for anoxic damage, i.e. hippocam- pal pyramidal cells of Sommer’s sector and Pur- kinje cells, were spared. Furthermore, anoxia damages all neurons simultaneously and the affected cells will consequently reveal the same stage of degeneration. In our case, however, the neurons were at different stages of degeneration. This was best seen in the brain stem nuclei and the dentate nuclei which showed a continuum from unaffected neurons to those which had completely disappeared.
Many cases of active Wernicke’s encephalopa- thy show a peculiar degeneration of neurons in the thalami and inferior olives without dis- playing the otherwise typical histological changes seen in the mammillary bodies and periventricular locations (19, 20). This de- generation is characterized by shrinkage and eosinophilia of the perikaryal cytoplasm and a relatively long-term preservation of the nuclear membranes and nucleoli. Furthermore, these neurons show various stages of disintegration indicating a gradual affection. Thus, the neur- onal degeneration found in our case has many morphological aspects in common with those seen in Wernicke’s encephalopathy. This could be indicative of certain common pathogenetic
mechanisms in Wernicke’s encephalopathy and SNE.
It should be recalled that Leigh in his first report of SNE in 1951 (10) wrote that “the nerve cells were often severely damaged, show- ing a variety of degenerative changes. These in- cluded swelling of the cell body with central chromatolysis and nuclear swelling, general cell shrinkage, neuronophagia and satellitosis. Nor- mal neurons were also present, however, and the nerve cell changes were by no means as promi- nent as the vascular proliferation.” Generally, subsequent authors have either emphasized the relative sparing of the neurons (4, 16, 18, 21) or they have considered the neuronal changes to be due to anoxia or “terminal events” ( 1 1, 18). An exception is Reye (1 5 ) who found that “the close proximity of undamaged neurones to tot- ally destroyed neurones is a very striking fea- ture” in the inferior olives.
In conclusion, we have found widespread neuronal degeneration in a 5-year-old girl who died of SNE after 4 weeks of illness. This de- generation is in histological appearance and topographical distribution different from that seen in anoxia and probably represents a reac- tion to the underlying metabolic defect of SNE per se. We think that more attention should be paid to the degenerative changes in the neurons in SNE rather than emphasizing the “relative preservation” of these cells. This may be one way to gain more knowledge concerning the pathogenetic mechanisms in SNE, especially if these changes can be correlated with certain en- zyme deficiencies or other metabolic par- ameters.
The authors wish to thank Ingt.borg Tonning for tech- nical assistance and Sigrun 0rn.sju for typing the manuscript.
REFERENCES
1. Arts, W. F. M . , Schlote, H. R., Loonen, M . C. B., Przyrembrl, H., Frrnundes, J . , Trijbels, J . M . F. & Luyt-Houwen, I . E. M . : Cytochrome c oxi- dase deficiency in subacute necrotizing encephalo- myelopathy. J. Neurol. Sci. 77: 103-1 15, 1987.
2. Cooper, J . R., Itokuwa, Y. & Pincus, J . H.: Thia- mine triphosphate deficiency in subacute necrot- izing encephalomyelopathy. Science 164: 74-75, 1969.
57

LINDBOE et al.
3. DeVivo, D. C., Haymond, M. W., Obert, K. A, , Nelson, J. S. & Pagliara, A. S.: Defective acti- vation of the pyruvate dehydrogenase complex in subacute necrotizing encephalomyelopathy (Leigh disease). Ann. Neurol. 6: 483494, 1979.
4. Egger, J., Wynne- Williams, C. J. E. & Erdohazi, M.: Mitochondrial cytopathy or Leigh’s syn- drome? Mitochondrial abnormalities in spongi- form encephalopathies. Neuropediatrics 13: 219-224, 1982.
5. Egger, J . , Pincott, J . R . , Wilson, J. & Erdohazi, M.: Cortical subacute necrotizing encephalomye- lopathy. A study of two patients with mitochon- drial dysfunction. Neuropediatrics 15: 150-1 58, 1984.
6. Farmer, T. W., Veath, L., Miller, A. L., O’Brien, J. S. & Rosenberg, R. N.: Pyruvate decarboxylase deficiency in a patient with subacute necrotizing encephalomyelopathy. Neurology 23: 429, 1973.
7. Grover, W. D., Auerbach, V. H. & Patel, M. S.: Biochemical studies and therapy in subacute nec- rotizing encephalomyelopathy (Leigh’s syn- drome). J. Pediatr. 81: 39-44, 1972.
8. Hommes, F. A, , Polman, H. A. & Reerink, J. D.: Leigh’s encephalomyelopathy: an inborn error of gluconeogenesis. Arch. Dis. Child. 43: 423426, 1968.
9. Kamoshita, S. , Aguilur, M. J. & Landing, B. H.: Infantile subacute necrotizing encephalomyelo- pathy. Am. J. Dis. Child. 116: 120-129, 1968.
10. Leigh, D. : Subacute necrotizing encephalomyelo- pathy in an infant. J. Neurol. Neurosurg. Psychi- at. 14: 216-221, 1951.
11. Lewis, A. J . ; Infantile subacute necrotizing en- cephalopathy. Can. Med. Ass. J. 93: 878-881, 1965.
12. Lombes, A , , Nakase, H., Tritschler, H. J . , Kaden- bach, B., Bonilla, E., DeVivo, D. C., Schon, E. A. & DiMauro, S.: Biochemical and molecular analysis of cytochrome c oxidase deficiency in Leigh’s syndrome. Neurology 41: 491498, 1991.
13. Miyabayashi, S., Narisawa, K., Iinuma, K., Tada, K., Sakai, K., Kobayashi, K., Kobayashi, Y. & Morinaga, S. : Cytochrome c oxidase deficiency in two siblings with Leigh encephalomyelopathy. Brain Dev. 6: 362-372, 1984.
14. Montpetit, V. J. A . , Anderrnann, F., Carpenter, S., Fawcett, J. S., Zborowska-Sluis, D. & Giber- son, H. R.: Subacute necrotizing encephalomyelo- pathy. A review and a study of two families. Brain 94: 1-30, 1971.
15. Reye, R. D. K.: Subacute necrotizing encephalo- myelopathy. J. Path. Bact. 79: 165-173, 1960.
16. Richter, R. B.: Infantile subacute necrotizing en- cephalopathy with predilection for the brain stem. J. Neuropathol. Exp. Neurol. 16: 281-307, 1957.
17. Siemes, H . , Goebel, H. H . , Sengers, R. C. A , , Rui- tenbeek, W. & Trijbels, J. M. F.: Subakute nekro- tisierende Encephalomyelopathie Leigh infolge verminderter Aktivitat des Pyruvat-Dehydrogen- ase-Komplexes. Monatsschr. Kinderheilkd. 135:
18. Tom, M . I. & Rewcastle, N. B.: Infantile subacu- te necrotizing encephalopathy. Neurology 12: 624628, 1962.
19. Torvik, A,: Two types of brain lesions in Wer- nicke’s encephalopathy. Neuropathol. Appl. Neu- robiol. 11: 179-190, 1985.
20. Vortmeyer, A. 0. & Colmant, H. J.: Differen- tiation between brain lesions in experimental thiamine deficiency. Virchows Arch. A Pathol. Anat. Histopathol. 414: 61-67, 1988.
21. Vuia, 0.; The cortical form of subacute necrotiz- ing encephalopathy of the Leigh type. A light- and electron-microscopic study. J. Neurol. Sci. 26: 295-304, 1975.
22. Walter, G. F., Brucher, J. M., Martin, J. J . , Cen- terick, C., Pilz, P. & Freund, M.: Leigh’s dis- ease - several nosological entities with an ident- ical histopathological complex? Neuropathol. Appl. Neurobiol. 12: 95-107, 1986.
821-826, 1987.
58