Embed Size (px)
Citation preview
Neuromuscular Re-education of the Submandibular Muscles to Increase Laryngeal Elevation
Using any Class II NMES Device
1
Understand the anatomy and physiology of swallowing
Review principles of electrophysiology Discuss rationale for using NMES to the
submandibular region for improving laryngeal elevation
Documentation and billing specifics
2
Dysphagia affects: 15 million people in the USA 45%-87% of residents in long-
term care One out of 17 people will eventually
develop dysphagia Aspiration pneumonia is the 5th leading
cause of death in the elderly and the most common cause of death in persons with severe dementia.
3
Traditional indirect or direct treatments for dysphagia include:
Oral motor exercises Hyolaryngeal exercises/Shaker
exercises Mendelsohn maneuver Thermal stimulation
4

Traditional indirect or direct treatments for dysphagia
Often difficult to perform with geriatric patients due to co-morbidities such as Alzheimer’s Disease, various severities of CVAs, and Parkinson’s Disease
5
Electrical Stimulation Has been used for decades in PT/OT Little is known on how it affects
swallowing physiology It has been proven that Estim can
assist in hyolaryngeal elevation Hypothesized that increase sensory
input to the CNS enhances swallow
6

Neuromuscular Electrical Stimulation (NMES) Low current levels activate
superficial sensory nerve endings providing feedback to the peripheral and central nervous systems
Increased current levels (intensity or pulse width) penetrate deeper depolarizing nerve endings to produce a muscular contraction when the peripheral nervous system is intact
7

NMES Using NMES to treat dysphagia, due
in part to decreased laryngeal elevation, provides the SLP with another safe and effective treatment option to help patients improve their swallow
8
A&P is the key to diagnosing and treating muscles and cranial nerves
What muscles raise the larynx and what muscles depress the larynx?
Where are they located? Where is the hyoid bone? Where is the trachea? Is it a muscle? Where are the carotid arteries?
9
10

11

12

3 separate phases of the swallow Oral - Preparatory/Transport Pharyngeal Esophageal
Three phases of the swallow work together to produce a functional swallow.
13

Phases of Swallow Any breakdown in a phase can
cause dysphagia From initiation to its end, the
swallow takes 8-20 seconds. This time significantly increases with age.
14

Oral Phase Begins at the lips and ends at the base
of the tongue behind the velum Bolus is formed and positioned in the
middle of the tongue Tongue is elevated and retracted to
create a lingual velar seal to avoid posterior bolus leakage
Can be subdivided into:▪ Oral Preparatory phase▪ Oral Transport phase
15
Oral Preparatory Phase A voluntary act that precedes the
swallow Converts food from solid to bolus
state Affected by dentition and salivary
gland function Must be in place before the
pharyngeal phase is initiated16

FACT
Aspiration most often occurs during the
pharyngeal phase but can occur due to
oral stage dysfunction
17

Oral Preparatory Phase Lips, tongue, mandible, palate, and
cheeks act in concert with salivary flow to grind and manipulate food into a consistency and position for subsequent phases of swallow to take place
18

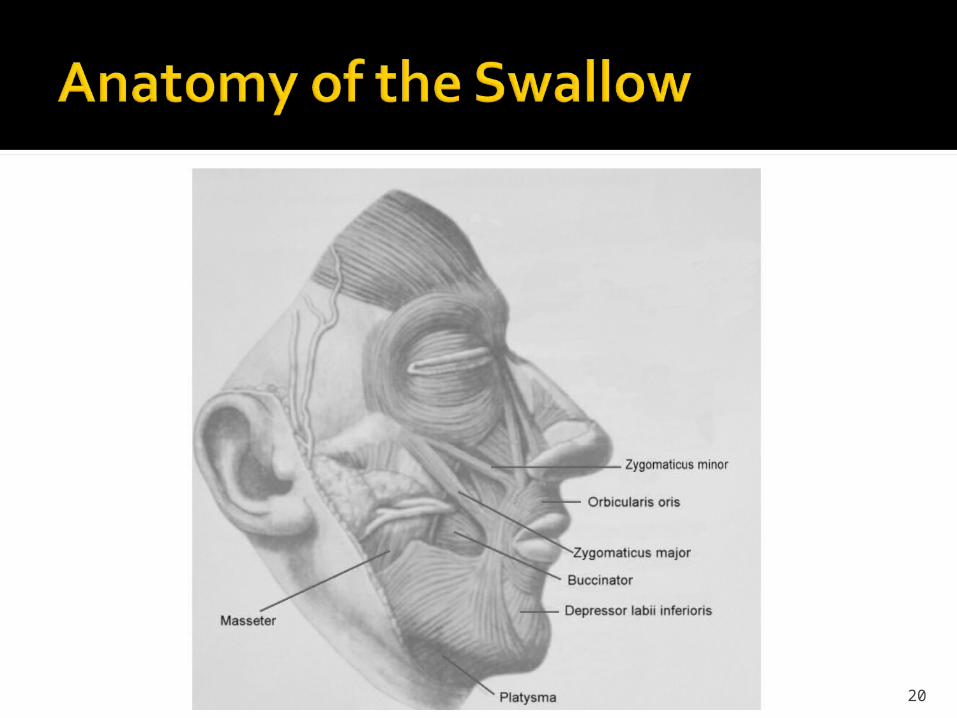
Zygomaticus major and minor move outer part of lips
Buccinator maintains food between teeth
Masseter assists in chewing Obicularis oris is in motion when
pursing lips to accept liquid bolus from a straw
Soft palate elevates as tensor veli palatini, levator veli palatini and musculus uvulae muscles contract
19
20

Oral Transport Phase Begins when the tongue contracts
against the hard palate Normal movement of the anterior
2/3 of the tongue is essential for carrying out the tasks of the oral stage of swallow
21

Oral Transport Phase Tongue Muscles - Intrinsic vs.
Extrinsic Intrinsic Tongue Muscles
Primary action is to produce changes in the shape of the tongue during articulation and deglutition (cradling the bolus)
Superior/Inferior Longitudinal Transversus Verticalis
22

Oral Transport Phase Extrinsic Tongue Muscles:
Genioglossus – protracts and depresses tongue
Hyoglossus – depresses tongue Styloglossus – retracts and elevates
tongue Palatoglossus – elevates tongue
23

24

Oral Transport Phase Musculature
Originates along the mental spine, hyoid bone, styloid process, and soft palate respectively; insert into other extrinsic or intrinsic tongue muscles
25
FACT
The tongue provides a supplemental role as it provides
anchoring during hyoid bone elevation and upper esophageal
sphincter (UES) opening. It is connected to the hyoid bone,
pharynx, and epiglottis26
27
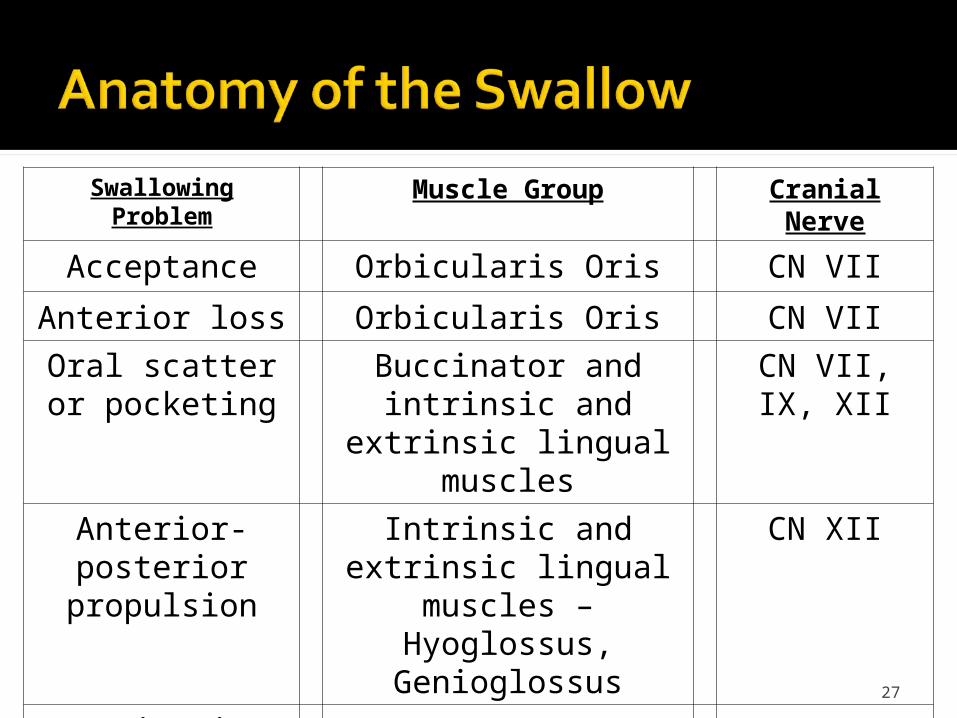
Swallowing Problem Muscle Group Cranial Nerve
Acceptance Orbicularis Oris CN VII
Anterior loss Orbicularis Oris CN VII
Oral scatter or pocketing
Buccinator and intrinsic and extrinsic lingual
muscles
CN VII, IX, XII
Anterior-posterior propulsion
Intrinsic and extrinsic lingual muscles –
Hyoglossus, Genioglossus
CN XII
Mastication Masseter, Pterygoids, and Temporalis
CN V
Cranial Nerves (see booklet on how to test) V : Trigeminal VII : Facial IX : Glossopharyngeal X : Vagus XI : Accessory XII : Hypoglossus
28
Pharyngeal Phase Shortest but most complex phase Requires 1-2 seconds to complete –
does not vary with consistency of food, age, or gender
29

Pharyngeal Phase Involves highly cortical centers as
well as brainstem centers including CN V, IX, X, XI, and XII
Involuntary, with 90% occurring during expiration
30
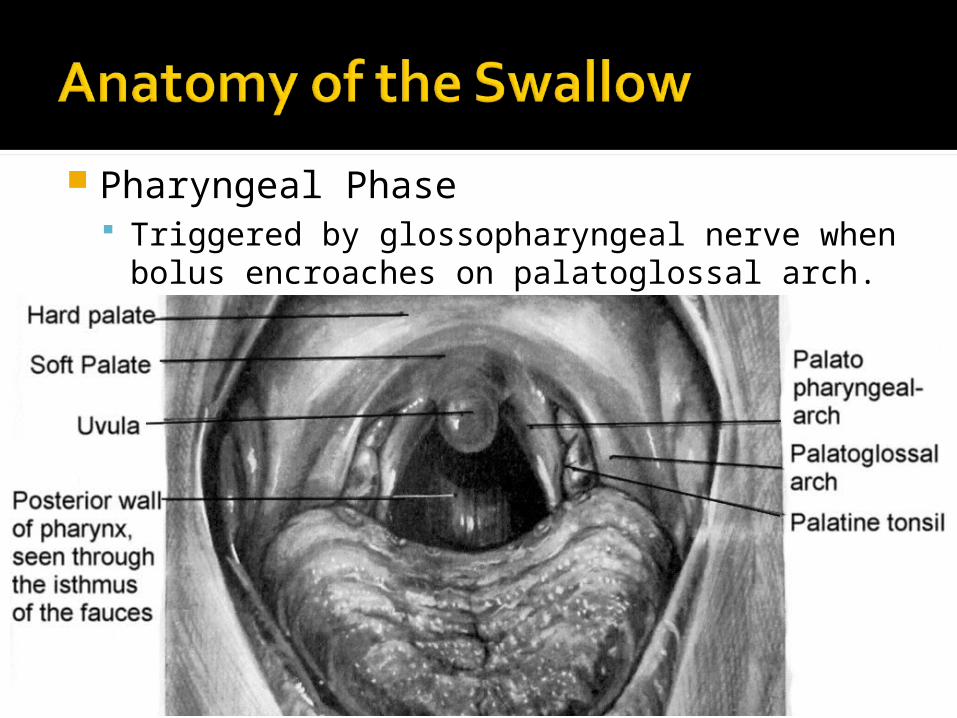
Pharyngeal Phase Triggered by glossopharyngeal nerve when
bolus encroaches on palatoglossal arch.
31
Pharyngeal Phase Additional factors may be
responsible for initiation of swallow:▪ May also be triggered late by superior
laryngeal nerve – “delayed swallow reflex” when this occurs
▪ Posterior tongue movement▪ Stimulation of the pharynx
32
Pharyngeal Phase Afferent impulses from cranial
nerves reach the brainstem completing a reflex arc affecting the following automatic events:
33
Pharyngeal Phase1) Velopharyngeal closure to prevent
reflux2) Specific sequential closure of the
larynx to prevent aspiration; vocal and aryepiglottic fold adduction; retroversion of the epiglottis
34

Pharyngeal Phase3) Pharyngeal constrictor contraction
superiorly to inferiorly while the tongue drives the bolus posteriorly
4) Elevation and anterior pull of the larynx and hyoid bone toward base of tongue
35
Pharyngeal Phase5) Relaxation of tonically contracted
cricopharyngeus and inferior pharyngeal constrictor muscles allowing passage of bolus into esophagus
36
Pharyngeal Phase As the true vocal folds adduct a
finite period of apnea occurs during swallow lasting approximately 0.3 – 2.5 sec
Deglutition occurs most often during expiration
Can lead to fatigue during the meal and consequent risks of laryngeal penetration and aspiration
37

Pharyngeal Phase Following closure of larynx, pharyngeal
peristalsis by contraction of superior, middle and inferior pharyngeal constrictor muscles, then laryngeal elevation takes place.
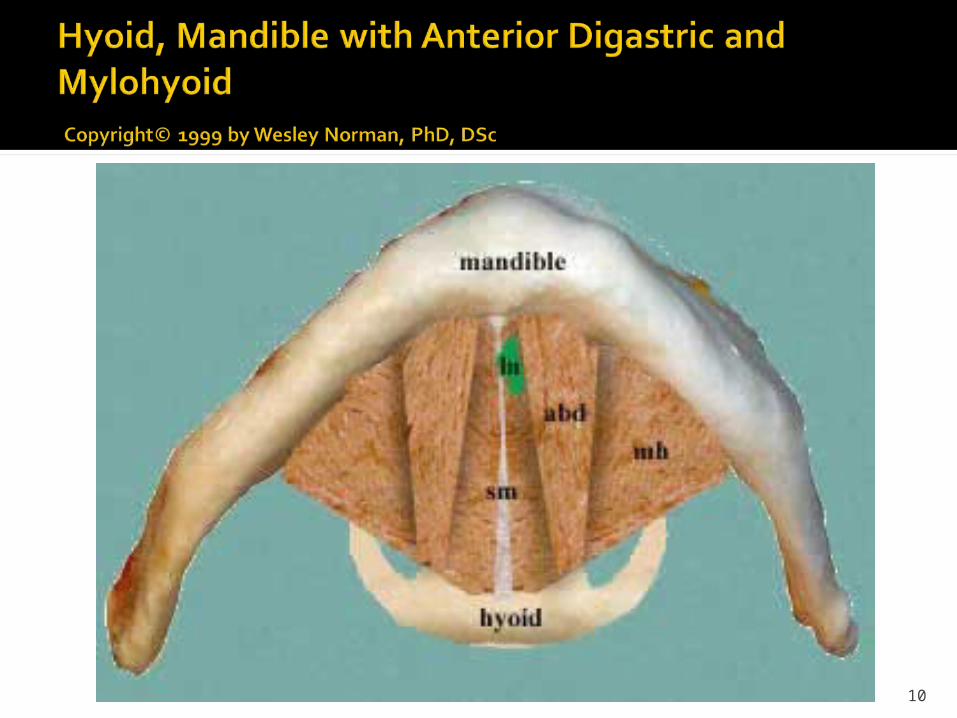
Laryngeal elevation takes places because the hyoid bone and tongue base move anteriorly and superiorly secondary to contraction of the anterior digastric, mylohyoid, geniohyoid, and stylohyoid muscles.
38

Suprahyoids (sling muscles)LARYNGEAL ELEVATORS Digastrics – anterior – elevates/protracts
hyoid, assists with jaw depression Mylohyoid – elevates/protracts hyoid Geniohyoid – depresses jaw,
elevates/protracts hyoid Stylohyoid – elevates/retracts hyoid
Located in the submental area of the submandibular triangle.
39

40

Pharyngeal Phase The first movement of the epiglottis
occurs synchronously with the elevation of the larynx.
Epiglottis acts to anatomically direct food bolus laterally toward the UES, as well as assisting in airway protection
41

Pharyngeal Phase The anterior and superior
movement of the larynx combined with the contraction of the middle and inferior constrictor muscles strips the bolus inferiorly ushering in the final portion of the pharyngeal phase – entry of the bolus into the cervical esophagus
42
Pharyngeal Phase Studies have shown that PES
relaxation takes place during elevation of the hyoid and larynx and reaches its most complete relaxation at their apex of elevation
The following table shows common swallowing problems in the pharyngeal phase along with associated muscle groups and cranial nerves:
43

44
Swallowing Problem Muscle Group Cranial Nerve
Poor velopharyngeal seal
Decreased closure of the larynx
Weak contraction -pharyngeal constrictors
Tensor Veli Palatini, Levator Veli Palatini, Musculus Uvulae
Post. and Lat. Cricoarytenoids, Transverse Arytenoid
Superior, Middle, and Inferior Pharyngeal Constrictors
CN V, XI
CN IX, X
CN IX, X
Decreased ant/superior elevation - hyolaryngeal complex
Anterior Digastric, Mylohyoid, Geniohyoid
CN V, XII
Difficulty relaxing the cricopharyngeus
Inferior Pharyngeal Constrictor, Cricopharyngeus, Upper Esophageal Musculature
CN IX , X

Esophageal Phase Involuntary action, involves
rhythmic contractions Transit time can increase
significantly with age Transit time range is from 6 – 18
seconds to clear solids
45

Esophageal Phase Cricopharyngeal and inferior
pharyngeal constrictor muscles relax allowing the bolus to pass into the upper esophagus.
The bolus passage triggers relaxation of the UES/PES to allow passage via peristaltic contractions
46
UES/PES Function: Protects pharynx by preventing
reflux Prevents air entering the
gastrointestinal tract during normal respirations
Relaxes completely to allow gas to exit or when vomiting occurs
47
UES/PES Dysfunction may occur secondary to: Reduced laryngeal elevation Abnormal cricopharyngeal
contraction And/or inflammation as a result of
GERD
48
Esophageal Phase The upper and lower esophageal
sphincters elongate/relax as much as needed. The LES allows the bolus to enter the stomach.
The following table shows common swallowing problems in the esophageal phase along with associated muscles and cranial nerves:
49
50
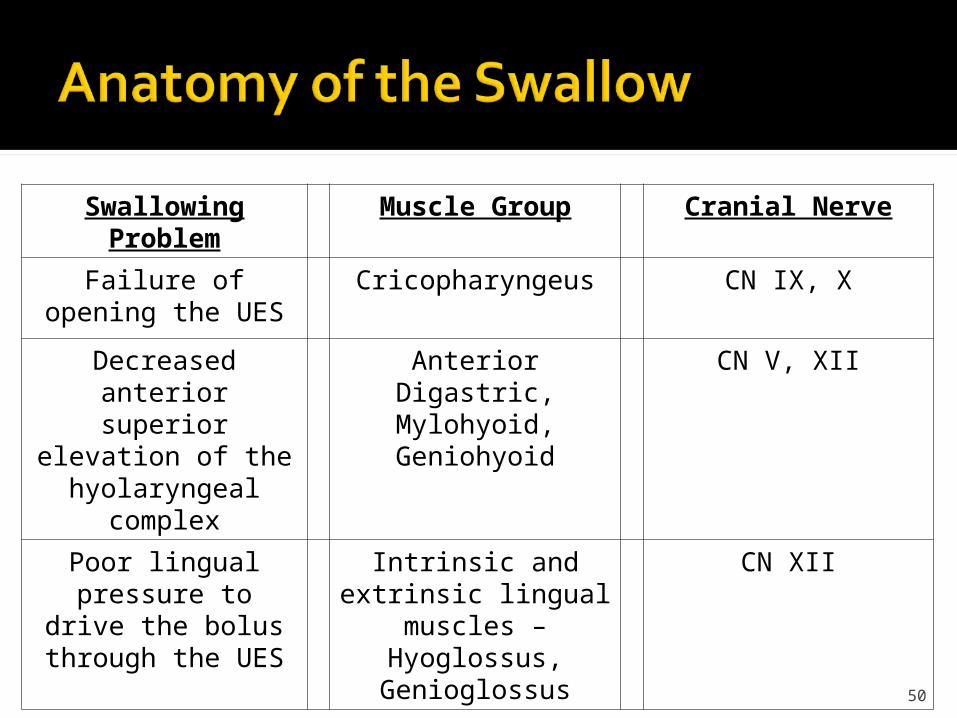
Swallowing Problem Muscle Group Cranial Nerve
Failure of opening the UES
Cricopharyngeus CN IX, X
Decreased anterior superior elevation of
the hyolaryngeal complex
Anterior Digastric, Mylohyoid,Geniohyoid
CN V, XII
Poor lingual pressure to drive the bolus through the UES
Intrinsic and extrinsic lingual muscles –
Hyoglossus, Genioglossus
CN XII
Swallow Reflex Term is deceptive in that the swallow is an elicited response requiring both sensory and motor information to initiate the swallow reflex.
One muscle and/or one nerve with impairment can affect the normal swallow function.
51

The swallow reflex is NOT a “no brainer”. The brain stem is involved. A typical reflex arc is a “no brainer”.
Information travels to the spinal cord and returns to the limbs.
Normal swallow is a dynamic activity that is dependent on both conscious, volitional cortical action, and reflexive subcortical neuromuscular patterns.
Two reasons we swallow▪ Maintenance – to manage own secretions▪ Swallow food or liquid
52

Swallow reflex arc affects: Velopharyngeal closure Laryngeal closure (specific
sequence); vocal and aryepiglottic fold adduction and epiglottis retroversion
Pharyngeal constrictor contraction Laryngeal/hyoid bone elevation and
anterior pull Cricopharyngeus/inferior pharyngeal
constrictor muscles53
54
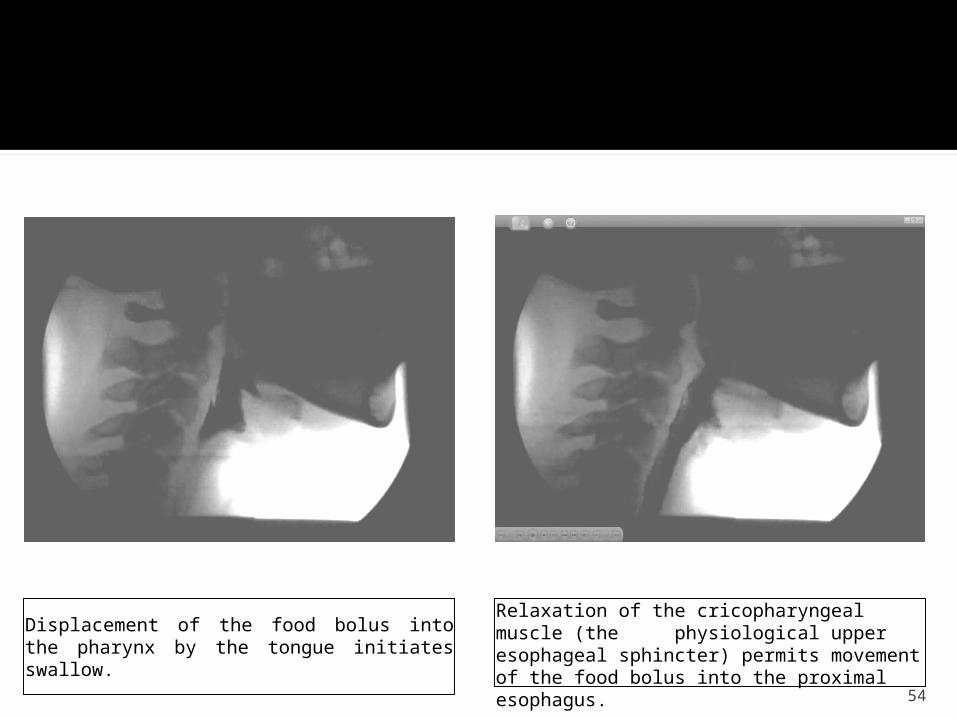
Displacement of the food bolus into the pharynx by the tongue initiates swallow.
Relaxation of the cricopharyngeal muscle (the physiological upper esophageal sphincter) permits movement of the food bolus into the proximal esophagus.
Assessment forms the basis of developing management strategies
Rarely does one form of assessment provide complete diagnostic information
55
Bedside Swallowing Evaluation (BSE) 1st step in a clinical assessment Head and neck examination Cranial nerve examination Oral phase – observe chewing Clinical signs of pharyngeal dysphagia Determines need for instrumental evaluation,
and specific diagnostic questions to be answered by instrumental evaluation
56

Fiberoptic Endoscopic Evaluation of Swallowing (FEES) Evaluates pharyngeal stage of swallow;
oral phases only evaluated indirectly; no esophageal phase evaluation
Mildly invasive Limited to events immediately before
swallow and after the swallow event
57

Modified Barium Swallow Study (MBSS) Assesses oral, pharyngeal,
esophageal phases Aspiration cannot be confirmed or
ruled out without MBSS Approximately 40% of patients
aspirating on MBSS were not identified as aspirators during BSE
58

MBSS Allows visualization of pharyngeal
phase while compensatory strategies are tested
59

There is a 3.7 times greater likelihood that aspiration is occurring with dysphagia if hyoid movement is reduced during swallow.
Reduced elevation of the larynx and pharynx is usually due to reduced hyoid bone elevation.
60
The muscles of the floor, specifically the paired Mylohyoid, Geniohyoid, and Anterior Belly of the Digastric are responsible for the anterior and superior movement of the Hyoid.
This motion plays a crucial part in moving the larynx forward reducing risk of aspiration.
61
Suprahyoids - Laryngeal Elevators (sling muscles) Ant. Digastric – elevates/protracts hyoid Post. Digastric – elevates/retracts hyoid
together assist with mandible depression Mylohyoid – elevates/protracts the hyoid Geniohyoid – elevates/protracts hyoid,
depresses mandible Stylohyoid – elevates/retracts hyoid
62

Infrahyoids - Laryngeal Depressors (strap muscles) Omohyoid – depresses hyoid Sternohyoid – depresses hyoid Sternothyroid – depresses thyroid Thyrohyoid – shortens the distance
between the thyroid and hyoid bone
63

Hyoid bone moves an average of 9-12 mm anteriorly and 11-12 mm superiorly
Duration of hyoid movement is influenced by bolus size, however extent of displacement is not
64
Reduced laryngeal elevation is strongly associated with aspiration
Superior movement of the larynx helps to bring the airway safely away from the path of the bolus
65

Manually lifting the larynxProlong laryngeal elevationLimited benefit with those with
severe cognitive deficits. NMES with proper submandibular
placement can produce a involuntary pseudo Mendelsohn Maneuver
66

Patients with reduced epiglottic function are 4.4 times more likely to aspirate
Epiglottis is cartilage, not muscle Does not have independent movement Moves passively by force of muscles
attached to it – pulls tip posteriorly, giving epiglottis a horizontal tilt, bending from the top down
67

Primary attachments at top/sides is hyoid bone
Primary attachments at bottom is thyroid cartilage ligament
68

The first epiglottis movement occurs synchronously with laryngeal elevation – thickening the base of the epiglottis and assisting with closure of the laryngeal vestibule
Due to anterior movement of hyoid and approximation of thyroid cartilage to the hyoid bone
69

4 types of impaired epiglottic function: Rigid/absent –
calcification/osteophytes Incomplete inversion or lowering –
nasogastric tubes Prolonged inversion or lowering –
exaggerated curvature of epiglottis Base of tongue approximation of
epiglottis – rests against tongue base, eliminates vallecular space
70
Compensatory Strategies Designed to redirect or improve
food flow, eliminate symptoms such as aspiration
71
Therapy Procedures Designed to change swallow
physiology (in contrast to compensatory strategies)
Improve range of motion of oropharyngeal structures
Improve sensory integration Take voluntary control of timing/
coordination of orophargyngeal movements
72
Indirect Therapy Exercise Programs or swallow
saliva, but no food/liquid givenDirect Therapy
Practice swallow techniques with small amount of food/liquid
73

Postural Techniques NO single posture improves
swallowing in all patients. Correct physiologic/anatomic
disorder must be identified in order to implement the correct compensatory posture(s).
Changing the head or body posture can be effective in eliminating aspiration 50% of the time.
74

Postural Techniques Some patients can’t use postural
strategies because of head stabilization devices or other physical/cognitive constraints.
Use of postural techniques is generally temporary.
Patients use them until swallow recovers or other treatment procedures which improve oropharyngeal motor function take effect
75
Muscle tissue – highly specialized fibers that generate a force for contraction
Nerves connect the spinal cord to the muscle
Neuromuscular junction – spot where nerve meets muscle
76
Electrical signal (nerve impulse) crosses neuromuscular junction – transmitted deep inside muscle fibers
Signal stimulates flow of calcium – causes thick and thin myofilaments to slide across each other – causing muscle to shorten, generating a force
77

Global view of a neuromuscular junction:
1. Nerve2. Neuromuscular junction3. Muscle fiber4. Myofibril with myofilaments inside
78

Billions of myofilaments in muscle shorten all at once to cause contraction of entire muscle fiber
79
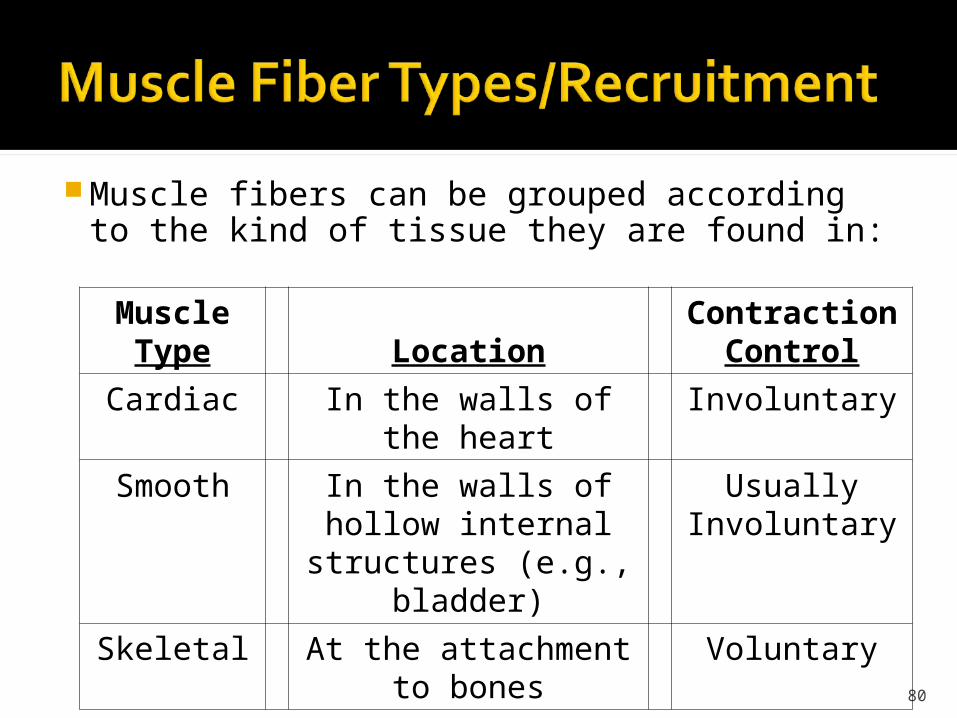
Muscle fibers can be grouped according to the kind of tissue they are found in:
80
Muscle Type Location
Contraction Control
Cardiac In the walls of the heart Involuntary
Smooth In the walls of hollow internal structures (e.g.,
bladder)
Usually Involuntary
Skeletal At the attachment to bones
Voluntary

Skeletal muscle – further divided into 2 basic types: Type I (slow-twitch fibers) –
primarily use cellular respiration, relatively high endurance – contain high levels of mitochondria (powerhouse of the cell) and myoglobin (oxygen storage) – responsible for red color of tissue
81

Type II (fast-twitch fibers) – relatively low endurance – typically used for short bursts of strength – cannot not sustain contractions for significant lengths of time▪ Further divided into: Types IIa and IIb
82
Type II (fast-twitch) Type IIa – appear red due to high
content of myoglobin and mitochondria
Type IIb – fastest firing, most powerful, but tire the fastest – appear white due to low oxygen demand
83
84
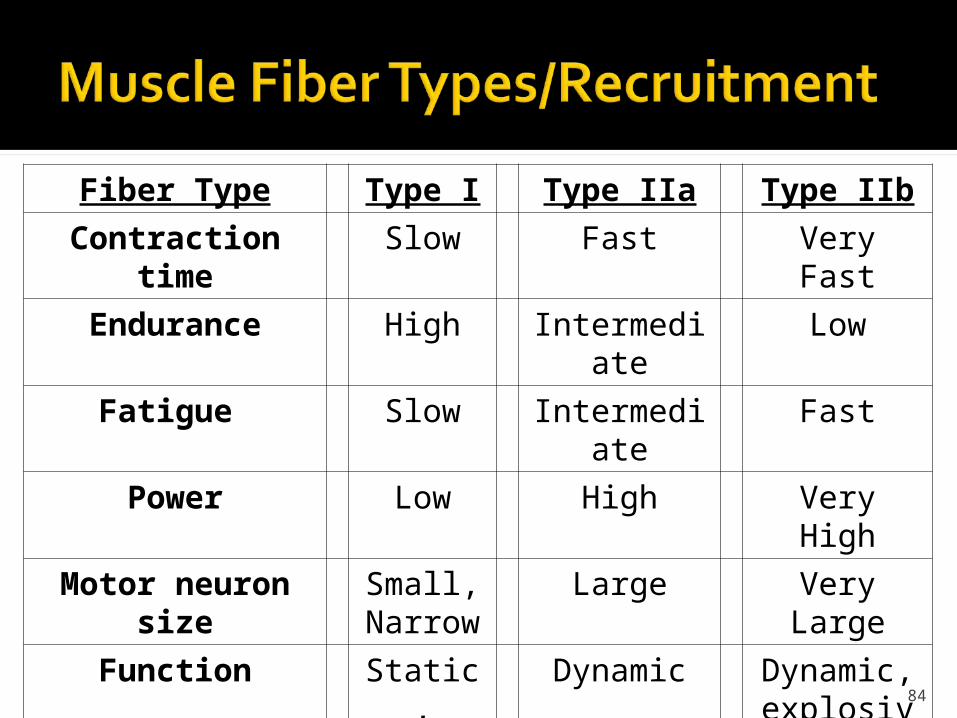
Fiber Type Type I Type IIa Type IIb
Contraction time Slow Fast Very Fast
Endurance High Intermediate Low
Fatigue Slow Intermediate Fast
Power Low High Very High
Motor neuron size Small, Narrow
Large Very Large
Function Static, Postural
Dynamic Dynamic, explosive
Energy Source Oxygen Oxygen, Glycogen
Glycogen
Color Red Red White
Most skeletal muscles contain a mixture of all 3 types of fibers – proportion depends on “usual” action of the muscle Posterior neck/back – postural
muscles – higher proportion of type I Anterior/lateral neck – rotating,
flexing, nodding – higher proportion of type II
85

Several swallowing muscles have: higher proportion of type II fibers -
▪ Anterior digastric▪ Mylohyoid▪ Upper pharyngeal constrictors
higher proportion of type I fibers – ▪ Cricopharyngeus
86

During contraction muscle fibers relay message to each other If a weak contraction is needed,
only type I fibers are activated If a maximal contraction is needed,
then type II fibers are activated as well
87
Consequently type I fibers receive the primary benefit from low intensity exercises found early in rehabilitation
The larger, type II fibers can only be exercised when dynamic activity calls on their recruitment – missed early on in rehab, this quickly leads to disuse atrophy of these fibers/muscles
88
Recruitment pattern with estim is reverse of that through exercise Type IIb fibers are first to contract as
the motor neuron for these fibers is larger and has a lower depolarization threshold
Type IIb fibers therefore respond sooner to electrical current when exposed
89
Estim and active exercise together - ideal way to treat swallowing musculature, due to high overall percentage of type II fibers present in muscles
90
91
Process by which electrical stimulation works has been well documented and studies
Extrinsic muscles of the swallowing mechanism bear no histological difference to any other skeletal muscles typically treated by PT and OT.
92

46 AD Torpedo fish were used to treat pain Late 1700’s Galvani stimulates frog muscle
with electrical charge of metal First identified research of motor points
was in the 1800’s Electrical Stimulation potentials
documented in articles as early as 1951 to prevent disuse atrophy Orborne, SL, 1951 on The Retardation of
Atrophy in Man by E-Stim of Muscles.
Current practices?93
Brief history of Neuromuscular Electrical Stimulation (NMES) or “E-Stim.” Currently an FDA approved modality used
primarily by Physical/Occupational Therapists and now entering the field of Speech Pathology
Stimulation requires an intact peripheral nerve
Treatment goals: strengthening and recovery of motor control
Use requires extended education in the area of electrotherapy
94

Prevent disuse atrophyIncrease range of motionRe-educating of muscle functionTemporarily decrease spasticityServe as an electrical orthosisIncrease local blood circulation
95
Neuromuscular Electrical Stimulation (NMES) is the use of electricity to stimulate the nerves that correspond to a targeted muscle or group of muscles and cause it to contract. This occurs when negatively charged subatomic particles, called electrons, flow from the negative to the positive pole in tissue, via transcutaneous electrodes for therapeutic benefit. It requires an intact peripheral nerve. This includes the health and integrity of the cell body, axon, myelin sheath, nerve and muscle.
96

97

Patients with any implanted electronic device e.g. cardiac pacemakers, spinal cord stimulators
Over neoplasm or infectionPlaces where active motion is contra-indicated
(i.e., fractures, anastomosis or fusions)Use during pregnancyCarotid Sinus Reflex Sensitivity
Do Not Stim Over Carotid Sinuses. Particularly in patients with a known sensitivity to carotid sinus reflux, due to blood pressure changes.
98

Patients with suspected or diagnosed epilepsy or seizure disorder
Stimulation on the anterior neck Skin with absent or diminished sensation History of Laryngeal Spasm
Stimulation should not be applied over the anterior neck. Severe spasm of the laryngeal and pharyngeal muscles may occur, causing difficulty breathing.
99

What are you doing? DYSPHAGIA TREATMENT – 92526 CMS stipulates SLP should bill this for
treatment of swallowing dysfunction and/or oral function of feeding.
Denials for 97110 and 97112▪ G0283 - Electrical Stim (unattended), 97032 (face to
face) Payor denial prompted CMS to review coding
issues. CMS does not support the use of physical
medicine codes.
100
Not a timed code, it is a service codeTreatment of swallowing dysfunction
and/or oral function for feeding.Must provide treatment exercises to
make it substantial and avoid denials if reviewed.
No modality should be used in isolation
101

You are doing a speech treatment to improve swallowing.
Goals are the same as tx with the Mendelsohn maneuver, hyolaryngeal exercises etc. (see example of goals in booklet)
You are achieving laryngeal elevation, improved timing of the swallow, increasing PO etc.
102

Always indicate your proof of disorder (i.e. decreased laryngeal elevation) which includes evaluation of the pharyngeal phase, which would include an MBSS.
Techniques utilized (Mendelsohn, Supraglottic swallow, etc.) must be considered appropriate based on patients documented condition.
103

Ethics Individuals should only practice in areas
which they are competent based on their education, training, and expertise. (Principles of Ethics II Rule B, ASHA Code of Ethics)
Rule A insists that clinicians provide all service “competently and admonishes against misrepresenting one’s competence.
Rule G states individuals shall evaluate effectiveness of services rendered.
104
Electrical Stimulation for Swallowing:In early 2004, speech-language pathologists, the California Physical Therapy Association, and manufacturers of electrical, stimulating devices asked about the licensing authority for speech-language pathologists to use electrical stimulation applied to the surface of the anterior neck to treat swallowing disorders. The Board discussed the issue at its public meetings during which device manufactures provided background on the specific devices cleared by the Federal Drug Administration. Licensees also discussed their therapy successes in applying electrical stimulation to the skin of a patient with swallowing disorders. Further, the Board consulted with otolaryngologists about the research and application of this new therapy, and sought the advice of legal counsel whether existing scope of practice laws and regulations permit licensed practitioners to use an electrical instrument as a therapeutic intervention to treat swallowing disorders.
Although legal counsel concluded that the law does provide the authority for speech-language pathology licensees to use electrical stimulation to treat swallowing disorders, counsel concluded that such authority does not imply that all licensed practitioners are competent to provide it. Concurrent provisions relating to the professional conduct of a licensees enforces that "incompetence in the practice of speech-language pathology which has endangered or is likely to endanger the health, welfare, or safety of the public" constitutes unprofessional conduct and is grounds for formal discipline. As such, licensed professionals should not engage in providing electrical stimulation therapy for swallowing unless they are adequately trained and competent in its application, are aware of the potential risks, and are able to respond to any adverse reaction that may occur.
Finally, the Board also expressed concern regarding the deficiency of peer-reviewed research to support the efficacy of using electrical stimulation to treat swallowing disorders. Even though electrical stimulation may be within the scope of practice of a speech-language pathologist, the Board is unclear whether it is a beneficial therapy that provides significant, sustained relief to affected members of the public.
105
Permission to reproduce the illustrations from Dr. Wesley Norman was granted to AMPCARE, LLC.
Copyright© 1999 by Wesley Norman, PhD, DSc
http://www.wesnorman.com
106

Permission for AMPCARE, LLC to reproduce these illustrations from Grays Anatomy, Vol. 36, 1980, Williams et al granted by Elsevier Ltd, The Netherlands.
107