-
8/4/2019 Neuromuscular Coordination
1/66
1
NEUROMUSCULARCO-ORDINATION
-
8/4/2019 Neuromuscular Coordination
2/66
-
8/4/2019 Neuromuscular Coordination
3/66
3
INTRODUCTION
Motor control
Muscle tone
Postural response
Selective movement
CO-ORDINATION
-
8/4/2019 Neuromuscular Coordination
4/66
4
INTRODUCTION
Coordination is an ability to execute smooth,accurate,
controlled and purposeful motorresponse.
It is dependent on somatosensory, visual, andvestibular input as
well as a fully intactneuromuscular system.
Coordinated movts are characterized byappropriate speed,
distance, direction, timing,muscular tension,synergistic influence
(musclerecruitment), easy reversal between opposingmuscle groups
& proximal fixation to allow distalmotion or maintenance of
posture
-
8/4/2019 Neuromuscular Coordination
5/66
5
INTRODUCTION
DEXTERITY refers to the skillful use offingers during fine motor
tasks
AGILITY refers to the ability to rapidly andsmoothly initiate,
stop or modify movt whilemaintaining postural control
-
8/4/2019 Neuromuscular Coordination
6/66
6
INTRODUCTION
General types of coordination:- Intralimb coordination-movt
occurring with
single limb.
Interlimb coordination-integratedperformance of two or more limb
workingtogether.
Visual motor coordination-ability to integrateboth visual and
motor abilities
-
8/4/2019 Neuromuscular Coordination
7/66
7
INTRODUCTION
Several condition that typically demonstratecoordination
impairments include traumaticbrain injury, Parkinsons disease,
multiple
sclerosis, cerebral palsy, cerebellarpathology and vestibular
pathology
-
8/4/2019 Neuromuscular Coordination
8/66
8
1)INTRODUCTION
2) MOTOR SYSTEM
3) FEATURES OF CO-ORDINATIONIMPAIREMENT
4) CO-ORDINATION TESTING
5) TREATMENT
-
8/4/2019 Neuromuscular Coordination
9/66
9
MOTOR SYSTEM
Motor system
Peripheral element Central element
Muscles, joints,sensory & motor nerves
Association cortex, motor cortex,basal ganglia, cerebellum,brain
stem & spinal cord
-
8/4/2019 Neuromuscular Coordination
10/66
10
MOTOR SYSTEM
CENTRAL ELEMENT
-
8/4/2019 Neuromuscular Coordination
11/66
11
MOTOR CORTEX
-
8/4/2019 Neuromuscular Coordination
12/66
12
MOTOR CORTEX
AREA-4 primary motor cortex
-largest concentration ofcorticospinal neurons
-precentral gyrus
-controls contralateral
movements.
AREA-6 - anterior to area 4- superiorly placed SMA
- inferiorly placed PMA
-
8/4/2019 Neuromuscular Coordination
13/66
13
MOTOR CORTEX
SMA -initiation of movement
-simultaneous bil grasping movt.
-sequencential task
-orientation of eye & head
PMA -controls trunk & proximal limb movt.
-contribute to anticipatory postural
changes
-
8/4/2019 Neuromuscular Coordination
14/66
14
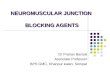
MOTOR HOMONUCULUS
Schematicallyillustrates theamount of cortical
area devoted tomotor control of agiven body part orregion
-
8/4/2019 Neuromuscular Coordination
15/66
15
MOTOR CORTEX
The motor cortex receives informationfrom three primary
sources:
1. The somatosensory cortex
2. The cerebellum
3. The basal ganglia
-
8/4/2019 Neuromuscular Coordination
16/66
16
CEREBELLUM
The primary function of cerebellum isregulation of movement,
postural control andmuscle tone.
It functions as comparator and errordetecting mechanism.
It compares information received from thecortex with that
obtained from peripheral
feedback mechanism
-
8/4/2019 Neuromuscular Coordination
17/66
17
CEREBELLUM
If the input from the feedback systems doesnot compare
appropriately, the cerebellumsupplies a corrective influence
This effect is achieved by corrective signalssent to the
cortex.
Cortex modifies or corrects the ongoingmovt via motor
pathways
-
8/4/2019 Neuromuscular Coordination
18/66
18
BASAL GANGLIA
Caudate nucleus,putamen, globuspallidus,
subthalamic nucleiand substantia nigraconstitute
basalganglia.
-
8/4/2019 Neuromuscular Coordination
19/66
19
BASAL GANGLIA
Basal ganglia play imp role in initiation andregulation of gross
intentional movts,planning and execution of complex motor
responses, facilitation of desired motorresponses while
selectively inhibiting others.
-
8/4/2019 Neuromuscular Coordination
20/66
20
DORSAL COLUMN TRACTS
They play imp rolein coordinated movtand posture.
They areresponsible formediatingproprioceptive input
from muscles andjoint receptors.
-
8/4/2019 Neuromuscular Coordination
21/66
21
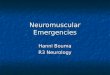
Basal ganglia Cerebellum
Cerebral cortex
Central pattern
generator
Receptors
Muscles
Feedback loops
Descendingmotor tracts
-
8/4/2019 Neuromuscular Coordination
22/66
22
1)INTRODUCTION
2) MOTOR SYSTEM
3) FEATURES OF CO-ORDINATIONIMPAIREMENT
4) CO-ORDINATION TESTING
5) TREATMENT
-
8/4/2019 Neuromuscular Coordination
23/66
23
C/F OF CEREBELLARDYSFUNCTION
ATAXIA is a general term used to describethe combined influence
of cerebellar andsensory dysfunction on gait, posture, and
patterns of movt. The c/f identified emphasis the crucial
influence of cerebellum on equilibrium,posture, muscle tone, and
force of movt.
-
8/4/2019 Neuromuscular Coordination
24/66
24
C/F OF CEREBELLARDYSFUNCTION
1. HYPOTONIAis decrease in muscle tone.
- diminished resistance to passive movt
- muscle may feel abnormally soft andflaccid
-diminished deep tendon reflexes.
2. DYSMETRIAis disturbance in the abilityto judge the distance
or range of movt
-manifested by hypermetria or hypometria
-
8/4/2019 Neuromuscular Coordination
25/66
25
C/F OF CEREBELLARDYSFUNCTION
3. DYSDIADOCHOKINESISis an impairedability to perform rapid
alternating movt.
-deficit observed in movts such as rapid
alteration between pronation and supinationof forearm
-movts are irregular with rapid loss ofrange, and rhythm
espescially as speed is
increased.
-
8/4/2019 Neuromuscular Coordination
26/66
26
C/F OF CEREBELLARDYSFUNCTION
4. TREMOR is an involuntary oscillatory movtresulting from
alternate contractions ofopposing muscle groups.
-two types of tremors associated withcerebellar lesion are
intention or kinetictremor and postural or static tremor.
-intention tremor occur during voluntary
motion of a limb and postural tremor maybe evident while the
patient maintains aposture
-
8/4/2019 Neuromuscular Coordination
27/66
27
C/F OF CEREBELLARDYSFUNCTION
5. MOVT DECOMPOSITION (DYSSYNERGIA ) describes a movtperformed
in a sequence of componentparts rather than as a single
smoothactivity. ASYNERGIA is the loss of abilityto associate
muscles together for complexmovements.
-
8/4/2019 Neuromuscular Coordination
28/66
28
C/F OF CEREBELLARDYSFUNCTION
6. DISORDERS OF GAITinvolve ambulatorypatterns that typically
demonstrate abroad base of support.
-the arms may be held away from the bodyto improve balance
-gait is unsteady, irregular and staggeringwith deviation from
an intended line of
progression
-
8/4/2019 Neuromuscular Coordination
29/66
29
C/F OF CEREBELLARDYSFUNCTION
7. DYSARTHRIA is referred to as scanningspeech
-speech is slow, slurred, hesitant with
inappropriate pauses.8. NYSTAGMUS is a rhythmic, oscillatory
movement of the eyes as the eyes moveaway from a midline resting
point to fix on
a peripheral object.
-
8/4/2019 Neuromuscular Coordination
30/66
30
C/F OF CEREBELLARDYSFUNCTION
9. ASTHENIA is generalized muscle weaknessassociated with
cerebellar lesions.
10. In addition to these c/f, difficulty may be
observed in stopping, or changing the force,speed, or direction
of movt.
-
8/4/2019 Neuromuscular Coordination
31/66
31
IMPAIREMENT OF BASALGANGLIA
1. BRADYKINESIA is slowed or decreasedmovt.
- e.g., slow shuffling gait, difficulty
initiating or changing direction of movt,lack of facial
expression, or difficultystopping a movt once begun.
2. RIGIDITY is an increase in muscle tone
causing greater resistance to passive movt.
-
8/4/2019 Neuromuscular Coordination
32/66
32
IMPAIREMENT OF BASALGANGLIA
3. Resting tremors typically disappear ordecrease with
purposeful movt, but mayincrease with emotional stress. E.g.,
pill
rolling tremors.4. Akinesia is the inability to initiate movt
and
is seen in late stages of parkisonism.
5. Chorea, athetosis, choreoathetosis,
hemibellismus and dystonia are involuntarymovts seen in basal
ganglia impairement.
-
8/4/2019 Neuromuscular Coordination
33/66
33
IMPAIREMENT OFDORSAL COLUMNS
Equilibrium and motor control disturbancesrelated to patients
lack of proprioception
Visioncompensates for the loss of
proprioception Problems will be exaggerated in poorly lit
areas or when patients eyes are closed.
Dysmetria is commonly seen in patient with
dorsal column impairement.
-
8/4/2019 Neuromuscular Coordination
34/66
34
IMPAIREMENT OFDORSAL COLUMNS
Noticeable slowing of voluntary movementsmay be observed
Gait pattern is wide-based, swaying with
uneven step length and excessive lateraldisplacement. Watching
the feet duringambulation is indicative of proprioceptiveloss
The leg may be lifted too high and thendropped abruptly.
-
8/4/2019 Neuromuscular Coordination
35/66
35
1)INTRODUCTION
2) MOTOR SYSTEM
3) FEATURES OF CO-ORDINATION
IMPAIREMENT
4) CO-ORDINATION TESTING
5) TREATMENT
-
8/4/2019 Neuromuscular Coordination
36/66
36
COORDINATIONTESTING
rigidity
Passive movts
hypotonia
absent
Deep tendon reflexes sluggish
exaggerated
at rest Tremors posture holding
intentional
-
8/4/2019 Neuromuscular Coordination
37/66
37
COORDINATIONTESTING
Postural holding
fixation or positionholding (upper and
lower extremity) Balance
displace balanceunexpectedly in
sitting or standing.in standing, alterbase of support
Observe gait
-
8/4/2019 Neuromuscular Coordination
38/66
38
COORDINATIONTESTING Romberg's sign
Standing: eyes open toeyes closed; inability tomaintain
uprightposture without visual
input is referred to aspositive rombergssign
Finger to nose test
The shoulder isabducted to 90 degrees
with the elbowextended. The patientis asked to bring the tipto
the nose. Look fortremors, dysmetria or
dyssynergia.
-
8/4/2019 Neuromuscular Coordination
39/66
39
COORDINATIONTESTING
Tandem walkingWalking, placing heelof one foot directly infront
of the toe ofthe opposite foot
Heel on shinFrom a supineposition, the heel ofone foot is slid
up and
down the shin of theopposite lowerextremity.
-
8/4/2019 Neuromuscular Coordination
40/66
40
COORDINATIONTESTING
Pronation/supination test
With elbows flexed to 90 degrees and heldclose to body the
patieht alternately turns
the palm up and down. Foot tapping
The patient is asked to tap the ball of thefoot on the floor
without raising the knee;
heel maintains the contact with the floor.
-
8/4/2019 Neuromuscular Coordination
41/66
41
COORDINATIONTESTING
Rebound test
The patient is positioned with elbows flexed.
The therapist applies sufficient manualresistance to produce the
isometriccontraction of the biceps. Resistance issuddenly
released.
-
8/4/2019 Neuromuscular Coordination
42/66
42
1)INTRODUCTION
2) MOTOR SYSTEM
3) FEATURES OF CO-ORDINATION
IMPAIREMENT
4) CO-ORDINATION TESTING
5) TREATMENT
-
8/4/2019 Neuromuscular Coordination
43/66
43
THERAPY IS DIRECTED ATPROMOTING POSTURAL
STABILITY, ACCURACY OF LIMBMOVTS, AND FUNCTIONAL
BALANCE AND GAIT
-
8/4/2019 Neuromuscular Coordination
44/66
44
TREATMENT(Postural stability)
Can be improved by focusing on holding innumber of different
weight bearing and anti-positions.
Progressed by gradually varying BOS, raisingthe COM, and
increasing the number of bodysegments that must be controlled.
PNF techniques:- joint approximation
- rhythmic stabilization- slow reversal hold and relax
-
8/4/2019 Neuromuscular Coordination
45/66
45
TREATMENT(Functional balance)
Static balance can be improved using forceplatform and
auditory/visual biofeedback.
Progression: standing eyes open to eyes
closed, standing on flat surface to foamsurface.
Dynamic balance can be challenged using selfinitiated movts.
A moveable surface like Swiss ball can alsobe used
TREATMENT
-
8/4/2019 Neuromuscular Coordination
46/66
46
TREATMENT(Limb movts)
Ataxic limb movts can be helped by lightweights to provide
additional proprioceptiveloading and stabilize movts. E.g.,
velcro
weight cuffs, weight belt, weighted jackets,weighted canes,
weighted walkers ortherabands.
The pool is an imp theraputic medium to
practice static and dynamic postural controlin sitting and
standing
-
8/4/2019 Neuromuscular Coordination
47/66
47
FRENKELS EXCERSICE
Dr H. S Frenkel was the medicalsuperintendent of the sanatorium
in theSwitzerland towards the end of last century.
He aimed at establishing voluntary control ofmovt by the use of
any part of the sensorymechanism which remained intact,
notablysight sound and touch to compensate for the
loss of kinesthetic sensation.
-
8/4/2019 Neuromuscular Coordination
48/66
48
FRENKELS EXCERSICE
The process of learning this techniquerequires:-
CONCENTRATION
PRECISIONREPETITION
-
8/4/2019 Neuromuscular Coordination
49/66
49
FRENKELS EXCERSICE(Technique)
1. The patient is suitably clothed andpositioned so that he can
see the limbsthroughout the exercise.
2. A concise explanation and demonstration ofthe exercise is
given before movt isattempted, to give the patient a clearmental
picture of it.
3. The patient must give his full attention tothe performance of
the movt to make themovt smooth and accurate.
-
8/4/2019 Neuromuscular Coordination
50/66
50
FRENKELS EXCERSICE(Technique)
4. The speedof the movt is dictated by thephysiotherapist by
means of rhythmiccounting, movt of her hand or the use of
suitable music.5. The range of movt is dictated by marking
the spot on which the foot or hand is to beplaced.
-
8/4/2019 Neuromuscular Coordination
51/66
51
FRENKELS EXCERSICE(Technique)
6. The exercise is to be repeated many timesuntil it is perfect
and easy. It is thendiscarded and the more difficult one is
substituted.7. As these exercise are very tiring at first,
frequent rest periods must be allowed. Thepatient retains little
or no ability to
recognize fatigue, but it is usually indicatedby the
deterioration in the quality of movt,or by a rise in the pulse
rate.
-
8/4/2019 Neuromuscular Coordination
52/66
52
FRENKELS EXCERSICE(Progression)
Progression is made by altering speed, rangeand complexity of
exercise.
Fairly quick movt require less control than
slow ones. Later, alteration in the speed of consecutive
movts, and interruptions which involvestarting and stopping to
command are
introduced.
F E E E E E
-
8/4/2019 Neuromuscular Coordination
53/66
53
FRENKELS EXCERSICE(Progression)
Wide range and primitive movts in whichlarge joints are used
gradually give way tothose involving the use of small joints,
limited range and frequent alteration ofdirection.
Finally simple movts are built up intosequences to form specific
actions which
require the use and control of a number ofjoints and more than
one limb, e.g., walking
F EN EL E E E
-
8/4/2019 Neuromuscular Coordination
54/66
54
FRENKELS EXCERSICE(Progression)
According the degree of disability,reeducation exs start in
lying with headpropped up and with the limbs fully
supported and progress is made to exs insitting and then in
standing.
FRENKEL EXCER CE
-
8/4/2019 Neuromuscular Coordination
55/66
55
FRENKELS EXCERSICE(Examples)
1. Half lying: hip and knee flexion andextension of each limb,
foot flat on theplinth.
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
56/66
56
FRENKELS EXCERSICE(Examples)
2. Half lying: Hip abduction and adductionwith leg fully
supported throughout on asmooth surface of a plinth or a
reeducation
board.3. Half lying: Hip abduction and adduction of
each limb with foot flat, with knee flexed
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
57/66
57
FRENKELS EXCERSICE(Examples)
4. Half lying: one leg raising to place the heelon a specified
mark.
Therapist
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
58/66
58
FRENKELS EXCERSICE(Examples)
5. Half lying: heel of one limb to opposite leg(toes ankle shin
and patella)
6. Half lying: reciprocal movt of both the
limbs7. Sitting: knee flexion and extension of each
limb.
8. Sitting: one leg stretching, to slide the heel
to a position indicated by the mark on thefloor.
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
59/66
59
FRENKELS EXCERSICE(Examples)
9. Sitting; alternate leg stretching and liftingto place heel or
toe on specified mark.
10. Stride sitting; change to standing and then
sit down again. The feet are drawn backand the trunk inclined
forwards from thehips to get the centre of gravity over thebase.
The patient then extends the legs
and draws himself up with the help of hishands grasping the wall
bars or othersuitable apparatus.
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
60/66
60
FRENKELS EXCERSICE(Examples)
11. Stride standing; transference of weightfrom foot to foot
12. Stride standing; walking sideways placing
feet on the marks on the floor.
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
61/66
61
FRENKELS EXCERSICE(Examples)
13. Standing; walking placing feet on the marks.
left
right
leftright
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
62/66
62
FRENKELS EXCERSICE(Examples)
14. Standing; turn around
1
2
3 4
5
6
8 7
2
1
3 4
5
6
8 7
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
63/66
63
FRENKELS EXCERSICE(Examples)
15. Standing; walking and changing direction toavoid
obstacles
Excercises for arm1. Sitting; one arm supported on a table or
on
a sling; shoulder flexion or extension toplace hand on a
specified mark
2. Sitting; one arm stretching to thread it
through a small loop or ring3. sitting; picking up objects and
putting them
down on a specified mark
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
64/66
64
FRENKELS EXCERSICE(Examples)
Exercise to promote movement andrhythm
1. Sitting; one hip flexion and adduction tocross one thigh over
the other, the movt isthen repeated and reversed.
2. Half lying; one leg abduction to bring kneeto side of plinth,
followed by one knee
bending to put foot on floor, the movt isthen reversed and
repeated
FRENKELS EXCERSICE
-
8/4/2019 Neuromuscular Coordination
65/66
65
FRENKELS EXCERSICE(Examples)
3. Sitting; lean forward and take weight onfeet (as if to
stand), then sit down again.
4. Standing; arm swing forwards and
backwards with partner, holding two sticks.5. Standing or
walking; bounce and catch, or
throw and catch a ball.
-
8/4/2019 Neuromuscular Coordination
66/66