Embed Size (px)
Citation preview

Neuromodulation of perineally transposed antropylorus
with pudendal nerve anastomosis following total
anorectal reconstruction in humans
ABHIJIT CHANDRA,* HARDEEP S. MALHOTRA,† NOUSHIF M,* VISHAL GUPTA,* SUNIL K. SINGH,* NEERAJ KUMAR,†RAKESH S. LALLA,† AYUSH CHANDRA* & RAVINDRA K. GARG†
*Department of Surgical Gastroenterology, King George’s Medical University, Lucknow, India
†Department of Neurology, King George’s Medical University, Lucknow, India
Key Messages
Patients undergoing perineal antropylorus transposition with pudendal innervation for end stage fecal
incontinence have an intrinsic rhythm of 2–3 contractions per minute. Stimulated antropyloric electromyography
showed a latency of 2–5 seconds with a differential rise in amplitude according to the frequency of stimulation.
Perineally transposed antropylorus as a replacement for anal sphincter can be electrically modulated.
Abstract
Background We have reported perineal antropyloric
segment transposition with its pudendal innervation
as a replacement for anal sphincter. Our aim herein
was to neuromodulate this segment by electrical
stimulation. Methods Eight patients with a permanent
colostomy underwent perineal antropyloric segment
transposition followed by neural anastomosis of its
anterior vagus branch to pudendal nerve branch in
the perineum. Perineal antropyloric graft was assessed
for its functional integrity and electrophysiologi-
cal effects. Nerve stimulation was done by surface
stimulation technique, using a customized stimula-
tion protocol for smooth muscle. Antral pressures
were recorded on voluntary attempts and on nerve
stimulation with simultaneous concentric needle elec-
tromyography of the perineal antropylorus.KeyResults
The antral segment showed slow spontaneous contrac-
tions (2–3/min) on digital examination, endoscopy,
and electrophysiology. Stimulated antropyloric elec-
tromyography showed a latency of 2–5 s with a differ-
ential rise in amplitude (mean range 58.57–998.75 lV)according to the frequency of stimulation (range 10–
150 Hz). An average latency of 10 s in relation to rise in
the antral pressure was observed on pudendal nerve
stimulation. Triggering of the intrinsic rhythm was
observed in patients where it was initially absent.
Voluntary attempts at contraction also showed a rise in
perineally transposed antral pressure. Conclusions &
Inferences Spontaneous rhythm, its generation after
electrical stimulation, and response to voluntary con-
traction demonstrates the viability and functional
reinnervation of the perineally transposed antropyloric
segment. Rise in pressure on electrical stimulation
shows evidence for its neuromodulation.
Keywords anal sphincter, neuromodulation, puden-
dal nerve, pylorus, smooth muscle.
INTRODUCTION
Surgical options for total anorectal reconstruction or
contemporary alternatives for a permanent abdominal
stoma have suboptimal results. The prime reasons for
Address for Correspondence
Dr. Abhijit Chandra. MCh, Professor and Head, Departmentof Surgical Gastroenterology, King George’s MedicalUniversity, Lucknow 226003, India.Tel: +91-522-2256116; fax: 091-522-2256116;e-mail: [email protected] abstract of the paper was presented (P-28) at the AnnualScientific Meeting of The American Society of Colon andRectal Surgeons (ASCRS 2013) held at Phoenix, USA, fromApril 27–May 1, 2013.Received: 18 December 2013Accepted for publication: 16 June 2014
© 2014 John Wiley & Sons Ltd1342
Neurogastroenterol Motil (2014) 26, 1342–1348 doi: 10.1111/nmo.12398
Neurogastroenterology & Motility

the disappointing results achieved thus far after total
anorectal reconstruction are absence of adequate tonic
contractions, reflexmechanisms, and voluntary control
in the reconstructed neoanal sphincter.1,2 Skeletal
muscles have been earlier included in the tissue wraps
to increase urethral and anal resistance.3 In an attempt
to achieve voluntary control of neoanus, pudendal
nerve (PN) reinnervation of adjacent skeletal muscles
like gracilis and gluteus maximus has been performed
initially in the canine models.4,5 The human studies
which followed found gluteus maximus to be more
suitable for this purpose.2 Stem cells of skeletal muscle
origin have also been used to augment both anal and
urethral sphincters.6,7 In contrast to skeletal muscle,
smooth muscle is resistant to fibrosis and its natural
physiological properties provide a prolonged tonic
contraction with little fatigue, which may be function-
ally advantageous in neosphincter reconstruction.8–12
Another potential advantage of innervated smooth
muscle is its ability to maintain a continuous contrac-
tile state when its innervation is activated at a low
frequency – ‘the neurogenic tone’.11–14
We have shown the use of antropyloric valve (APV), a
smooth muscle segment, as a substitute for a perma-
nent colostomy for total anorectal reconstruction. The
antropylorus, when removed from the gastroduodenal
continuity, provides a continuous tone and functions as
an effective perineal sphincter.15 Our initial results
suggested less optimum results from the patients
undergoing this procedure following abdominoperineal
resection of anal sphincter (for malignancy) as com-
pared to those with intact sensate anorectum due to
lack of voluntary control and sensations.16 We subse-
quently innervated this perineally transposed APVwith
PN, by anastomosing the anterior vagus nerve (AVN)
branch of APV to the inferior rectal nerve (IRN) branch
in the perineum.17,18 This was aimed to circumvent the
problems of lack of voluntary control over the sphinc-
ter. We now describe the electrical effects of stimulat-
ing this perineally transposed APV segment.
METHODS
The study was approved by the Institutional Review Board andEthics committee of King George’s Medical University, India.Only those patients who expressed their willingness to participatewere recruited after a detailed discussion and careful consider-ation of the possible outcomes. The preliminary surgical resultsand evaluation of this cohort has been reported previously.18
Surgical technique
The APV together with its AVN branch based on left gastroepi-ploic arterial pedicle was harvested and perineally transposed by
the technique described previously.16,17 The antral end of APVwas anastomosed with the distal colonic segment after the nativediseased anorectum had been excised. Simultaneously, PN branch(IRN) was dissected in the perineum at 3 or 9 o’ clock positions inthe ischioanal fossa. The end of AVN was then anastomosed withIRN or its branches in a tension-free manner and a proximaldiverting colostomy made. Gastrointestinal continuity wasrestored by a posterior gastrojejunostomy. Sufficient time for6 months was allowed for the PN fibers to grow or regeneratethrough the AVN conduit and innervate the transposed APVsegment in the perineum, before closure of diverting colostomy inall the patients.
Evaluation
Functional evaluation of transposed APV segment (a) Digitalexamination: Two independent observers digitally examined thetransposed APV segment to assess its tone, rhythmicity, andspontaneous contractions.
(b) Colonoscopic examination: The APV segment was exam-ined by an endoscope (Olympus Optical Co. Ltd., Tokyo, Japan)once the neoanus healed in the perineum to assess the tone,rhythmicity, and spontaneous contractions.
(c) Neuromodulation and Pressure estimation: The evaluationof the patients was done using Duet Logic (version: 9.2.0.0;Mediwatch, Florida, USA) and Synergy (version: 14.0; ViasysHealthcare UK Limited, Old Woking, Surrey, UK) machines.High resolution ultrasound was performed with short focus linear15 and 12 MHz transducers (GE Voluson, E8 Tiefenbach, Austria)with direct contact scanning technique for localization of anas-tomosed IRN in the perineum, over the ischioanal region, asreported previously.18 Nerve stimulation was done using surfacestimulation technique after localization of the neural anastomo-sis by USG. The stimulation protocol was customized for thestudy of smooth muscles using a mixed set of frequencies(ranging from 10 to 150 Hz), current (depending upon thegeneration of impulse amplitude and tolerability), pulse width,and the duration of the stimulus. The customization was basedon the earlier data obtained from the stimulation studies of thelower esophageal sphincter, conducted in the canine model andthe human subjects.19,20 Unlike electrode implantation employedin these studies, surface stimulation was utilized by us. After aseries of applied permutations, a stimulation current range of 20–30 mA, to be assessed over a frequency range of 10–150 Hz,primarily at 20 Hz, delivered as square wave pulses with a widthof 200 ls, was finalized as the stimulation protocol. It wasrealized that the use of higher stimulation current range led tolesser sustenance of contractions, and being more painful. Toallow generation of adequate potentials and pressure, the stim-ulation was given for at least 30 s to counteract the associatedperiod of latency observed in the initial assessments. A minimumperiod of observation of 30 s, poststimulation, was allowed torecord the changes.
The antral pressures were measured using a Foley’s catheter(16F, filled with ≥20 mL saline), securely tucked at the antro-pyloric junction in the perineum, opposing the walls of thetransposed segment. The free end of the Foley’s catheter wasattached to the pressure recording gauze of the Duet Logicmachine, and calibrated to zero for all individual assessments tonullify the pressure effect caused by a different volumes ofsaline used for the retention balloon, and the possible effect ofabdominal pressure. Concentric needle electromyography (EMG)of the pyloric muscle was done to assess the response tostimulation at various frequencies; the voluntary neosphinctericcontrol was assessed by recording the generated pressure and
© 2014 John Wiley & Sons Ltd 1343
Volume 26, Number 9, September 2014 Neuromodulation of perineal antropylorus

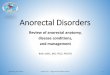
the summated myogenic potentials on the command to‘attempt to hold the urine’ primarily, or alternatively, to‘squeeze the anal canal’ if the sensory feedback was intact(Fig. 1).
RESULTS
Eight patients (mean age 35.5 years [range 15–55];
Male : female = 7 : 1) of Indian origin, who under-
went the surgery were evaluated (Table 1). All
patients were continent for solid stools, while three
patients experienced incontinence for liquid stools
initially. All patients used antimotility drugs ini-
tially. Pads were used by all patients for mucus
discharge from the duodenal mucosa of the perineal
graft. None of the patients had gastrojejunostomy
related complications.
Functional evaluation of transposed APVsegment
Digital examination The transposed antrum firmly
gripped the examining finger with a frequency of 2–3/
min in all patients, while the pyloric sphincter
remained tonically contracted throughout. This basic
rhythm of contraction was consistently observed in
the transposed antral segment of all patients.
Colonoscopic examination Endoscopy confirmed sim-
ilar rhythmic contractions of the transposed segment
with a spontaneous frequency of 2–3/min. Contrac-
tions were also observed on voluntary attempts to
squeeze the neoanum.
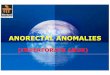
Neuromodulation and pressure estimation Stimu-
lated antral pressure recordings showed an average
latency of 10 s with a mean pressure generation of
37.2, 31.57, 26.57, 19.86, 28, and 35.85 cmH2O at 10,
20, 30, 50, 100, and 150 Hz stimulation, respectively
(range 8 cmH2O–90 cmH2O; Table 2, Fig. 2). The
results reiterated our preliminary assessment and
allowing us to choose 20 Hz as the preferred stimula-
tion frequency (Fig. 2, dashed line box). Rise in antral
pressures (ratio >1 from the maximally generated
pressure on stimulation) with simultaneous EMG
activity was observed on attempted voluntary contrac-
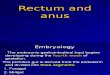
tion of the neosphincter. Stimulated antropyloric EMG
recording showed a latency of 2–5 s with a differential
rise in amplitude according to the frequency of stim-
ulation (Table 3, Figs 3 and 4). The mean generation of
amplitude of the myogenic potentials was 58.57, 77.38,
136.88, 243.13, 543.75, and 998.75 lV at 10, 20, 30, 50,
100, and 150 Hz, respectively (range 25–3400 lV); therise observed with stimulated EMG was linear and
directly related with the frequency of stimulation,
keeping the current constant. Triggering of the intrin-
sic rhythm, in patients who did not demonstrate this
initially, was observed in four patients (Patient 1, 3, 5,
and 8) on stimulation and was recorded at a mean of
1.75–2.25 contractions/min.
DISCUSSION
An intrinsic rhythm of 2–3 contractions/min on
digital and endoscopic examination, and 1.75–2.25
contractions/min on electrophysiological assessment
was observed in the transposed neurovascular antro-
pyloric segment. These findings reflect that the
intrinsic slow gastric rhythm is preserved in the
perineally transposed APV. The analysis of patients in
our study reveals certain important facts pertinent to
Figure 1 Schematic representation of the technique used for
neuromodulation and pressure estimation (A – antrum, B – pylorus,
C – Foleys catheter with inflated bulb tucked to antrum,
D – electromyography needle).
Table 1 Patient demographics
Patient no. Age/sex Indication
1 55/M APR for carcinoma anorectum
2 48/M APR for Carcinoma rectum
3 30/M Perineal injury with extensive
fibrosis
4 50/M APR for carcinoma anorectum
5 16/M Congenital high ARM with absent
anorectal sphincter
6 30/M APR for carcinoma anorectum
7 15/F APR for carcinoma anorectum
8 40/M APR for carcinoma anorectum
APR, abdominoperineal resection; ARM, anorectal malformation.
© 2014 John Wiley & Sons Ltd1344
A. Chandra et al. Neurogastroenterology and Motility

smooth muscle recording as the neosphincter was not
a conventional striated-muscle graft where standard
protocols for nerve conduction studies are used.19,20
The latencies observed in pressure and muscle
potential recordings point toward classical smooth
muscle stimulation characteristics perhaps consti-
tuted by a delay caused by an interplay of slow-
channels and summation potentials. The generation
of pressure in the antropyloric segment was observed
for all stimulation frequencies, but was best obtained
at 20 Hz. Our findings, as evident from Fig. 2, seem
to be in agreement with the stimulation protocol of
the lower esophageal sphincter which essentially is
the same upper gastrointestinal correlate of the
antropyloric graft used in our protocol.19 Although
the mean rise of pressure at 10 Hz was slightly
greater than that obtained at 20 Hz, its relevance is
marred by the lack of generation of any activity in
three of eight patients. Stimulation at frequencies
greater than 30 Hz did not show generation of extra-
pressure and was found to be associated with abnor-
mal sensations including pain.
It has also been observed that for sacral nerve
neurostimulation, the maximal rise in anal pressures
is achieved between frequencies of 10–25 Hz on sacral
root 3 nerve stimulation.21–23 Our observations are
similar to the stimulation protocols of these ear-
lier observations also where the use of striated
musculature was done. The current used for the
stimulation of PN in our study was on the higher side
(20–30 mA) because in contrast to electrode implanta-
tion,19 electrodes were placed superficially over the
neural anastomosis (after USG localization) adjacent to
the transposed APV segment which may account for
the dissipation of current in the intervening tissue.
Direct stimulation of the transposed antropylorus is
improbable in our protocol because the amount of
current used and the distance to be traversed are not
conducive to such a phenomenon. The stimulus,
therefore, follows the path of least resistance (IRN in
our study) in accordance with the properties of the
tissue, conductance as well as resistance, and dissipates
within millimeters of travel through alternate path-
ways (skin, subcutaneous tissue, bone). The simulta-
neous activity in the EMG during attempted voluntary
contraction points to at least some degree of intrinsic
voluntary control of the transposed segment; this
annuls the possibility of any significant contribution
Figure 2 Observed antral pressure
recordings at different rates of stimulation
(Dashed line box – 20 Hz).
Table 2 Antral pressure changes at different rates of stimulation
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8
Change in pressure (cmH2O)
Stimulation @ 10 Hz 80 No change No change 26 12 23 No change 45
Stimulation @ 20 Hz 90 22 – 18 20 26 15 30
Stimulation @ 30 Hz 65 20 – 13 16 21 26 25
Stimulation @ 50 Hz 45 8 – 11 10 26 17 22
Stimulation @ 100 Hz 70 17 – 25 18 21 25 20
Stimulation @ 150 Hz 70 29 – 25 32 40 40 15
Voluntary contraction 100 96 80 37 57 22 No change 80
Intrinsic
rhythm
@ 2–2.25/min
at stimulation
of 10 Hz
No
intrinsic
rhythm
Intrinsic
rhythm
@ 2–2.25/min
at stimulation
of 10 Hz
No
intrinsic
rhythm
Intrinsic
rhythm
@ 1.75–2/min
at stimulation
of 20 Hz
No
intrinsic
rhythm
No
intrinsic
rhythm
Intrinsic
rhythm
@ 2–2.25/min
spontaneously
present
© 2014 John Wiley & Sons Ltd 1345
Volume 26, Number 9, September 2014 Neuromodulation of perineal antropylorus

of abdominal pressure to the increase in the intrinsi-
cally generated antral pressures.
Neosphincter surgery, as an alternative for both anal
and urethral stomas, has been developed over many
years. Skeletal muscles like gracilis have been utilized
for anal neosphincter reconstruction because of the
nature of its physio-anatomic similarities, remarkably
consistent neurovascular supply, superficial location,
and minimal dysfunction to the donor site. The
introduction of electrostimulation rekindled the inter-
est in gracilis muscle neosphincter. However, prob-
lems of inadequate tonic contractions, reflex
mechanisms, and voluntary control do remain. To
circumvent this and to obtain voluntary control of the
neoanal sphincter, PN innervation of these skeletal
muscles has also been attempted.4,5 Smooth muscle
has advantages of a prolonged tonic contraction with-
out fatigue hence is better suited for neosphincter
Figure 3 Needle electromyography changes
observed at various stimulated frequencies.
Table 3 Needle electromyography changes at various stimulated frequencies
Stimulation
frequency Parameters Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8
10 Hz Wave Plateau No wave Plateau Plateau Plateau Plateau Plateau Plateau
Amplitude 40 lV 90 lV 60 lV 70 lV 30 lV 100 lV 20 lVDuration 30 s 30 s 30 s 30 s 180 s 180 s 180 s
Baseline Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
20 Hz Wave Plateau Spike Plateau Plateau Plateau Plateau Plateau Plateau
Amplitude 50 lV 44 lV 135 lV 80 lV 90 lV 50 lV 145 lV 25 lVDuration 40 s 1 s 40 s 40 s 40 s 180 s 180 s 180 s
Baseline Return
to base
No shift Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
30 Hz Wave Plateau Spike Plateau Plateau Plateau Plateau Plateau Plateau
Amplitude 50 lV 40 lV 370 lV 140 lV 210 lV 60 lV 190 lV 35 lVDuration 30 s 1 s 60 s 60 s 60 s 180 s 180 s 180 s
Baseline Return
to base
No shift Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
50 Hz Wave Plateau Plateau Plateau Plateau Plateau Plateau Plateau Plateau
Amplitude 90 lV 40 lV 530 lV 390 lV 340 lV 100 lV 330 lV 125 lVDuration 70 s 35 s 42 s 55 s 55 s 180 s 180 s 180 s
Baseline Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
100 Hz Wave Plateau Plateau Plateau Plateau Plateau Plateau Plateau Plateau
Amplitude 130 lV 40 lV 1350 lV 430 lV 470 lV 190 lV 1170 lV 570 lVDuration 40 s 50 s 60 s 50 s 50 s 180 s 180 s 180 s
Baseline Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
150 Hz Wave Plateau Plateau Plateau Plateau Plateau Plateau Plateau Plateau
Amplitude 280 lV 40 lV 3400 lV 580 lV 560 lV 480 lV 1600 lV 1050 lVDuration 40 s 50 s 45 s 60 s 60 s 60 s 60 s 120 s
Baseline Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
Return
to base
© 2014 John Wiley & Sons Ltd1346
A. Chandra et al. Neurogastroenterology and Motility

reconstruction as compared to a skeletal muscle.8–10
Besides, it can be transplanted as a free graft and can be
reinnervated by axons that grow in from nearby
adjacent tissues once implanted.11,12,24 The innervated
smooth muscle also has an intrinsic tone and can
maintain a continuous contractile state when acti-
vated at a low-frequency stimulation.11,13,14
The current technique has utilized a smooth muscle
segment (antropylorus) for anorectal reconstruction in
comparison to the previously reported alternatives
utilizing a skeletal muscle. The preliminary evaluation
of the non-stimulated pyloric valve in the current
cohort, reported previously,18 have shown a mean
resting and squeeze pressures of 26.25 mmHg (range
16–62 mmHg) and 50.25 mmHg (range 16–113 mmHg)
respectively on manometry. The electrophysiological
activity in the transposed segment demonstrates that it
can be manipulated by neurostimulation (functional
reinnervation). An analogous stimulation protocol has
shown promise in humans to maintain the tone at the
gastroesophageal junction (smooth muscle sphincter)
therapeutically.19 Although the initial results seem
encouraging at the gastroesophageal junction, long-
term functional outcomes and quality of life from a
larger series are still awaited. Direct stimulation
protocols, neural and muscular, also need to be eval-
uated to assess the comparative efficacy and therapeu-
tic benefit of smooth muscle as a sphincter.
The findings of the stimulated antropyloric EMG are
intriguing and demonstrate the excitability of the
antropyloric junction utilizing the surface stimulation
protocol. Besides demonstrating active nerve bundle
continuity, it indicates the feasibility of nerve stimu-
lators for improving the continence in this subset of
patients. The innervated APV segment in the perineum
can be controlled by electrical stimulation and it might
be appropriate to apply sacral nerve stimulation and
gastric pacing protocols for better fecal control in these
patients.
CONCLUSIONS
Perineally transposed and innervated antropylorus has
an intrinsic rhythm as in its native position in the gut.
This intrinsic rhythm could be generated where it was
not initially present following electrical stimulation.
The rise in antral pressures of this transposed segment
is best obtained at a stimulation frequency of 20 Hz
and show a corresponding rise in EMG amplitudes. The
innervated perineal antropyloric segment can thus be
electrically modulated on neurostimulation.
FUNDING
Grant number 2835/Lekha/09, Department of Surgical Gastroen-terology, King George Medical University, India.
DISCLOSURE
The authors have no competing interests.
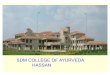
Figure 4 Antral pressure (Pabd) and
electromyography (EMG) tracing on
electrical stimulation (30 Hz, 20 mA,
200 ls).
© 2014 John Wiley & Sons Ltd 1347
Volume 26, Number 9, September 2014 Neuromodulation of perineal antropylorus

AUTHOR CONTRIBUTION
AC, HSM, VG, NM, NK, RSL planning and/or conducting thestudy, critical revision of the manuscript; AC, VG, SKS, NM
performed and/or assisted the surgical procedure; AC, HSM, VG,NM, NK, AC, RSL, RKG Drafting the manuscript, literaturereview.
REFERENCES
1 Mander BJ, Abercrombie JF, GeorgeBD, Williams NS. The electricallystimulated gracilis neosphincterincorporated as part of total anorectalreconstruction after abdominoperi-neal excision of the rectum. Ann Surg
1996; 224: 702–9.2 Sato T, Konishi F, Endoh N, Uda H,
Sugawara Y, Nagai H. Long-term out-comes of a neo-anus with a pudendalnerve anastomosis contemporane-ously reconstructed with an abdomi-noperineal excision of the rectum.Surgery 2005; 137: 8–15.
3 Mingin GC, Youngren K, Stock JA,Hanna MK. The rectus myofascialwrap in the management of urethralsphincter incompetence. BJU Int
2002; 90: 550–3.4 Congilosi SM, Johnson DR, Medot M,
Tretinyak A, McCormick SR, WongWD, Rothenberger DA, Madoff RD.Experimental model of pudendalnerve innervation of a skeletal muscleneosphincter for faecal incontinence.Br J Surg 1997; 84: 1269–73.
5 Pirro N, Sielezneff I, Malouf A,Oua€ıssi M, Di Marino V, Sastre B.Anal sphincter reconstruction using atransposed gracilis muscle with apudendal nerve anastomosis: a preli-minary anatomic study. Dis Colon
Rectum 2005; 48: 2085–9.6 Frudinger A, K€olle D, Schwaiger W,
Pfeifer J, Paede J, Halligan S. Muscle-derived cell injection to treat analincontinence due to obstetric trauma:pilot study with 1 year follow-up. Gut
2010; 59: 55–61.7 Furuta A, Jankowski RJ, Honda M,
Pruchnic R, Yoshimura N, Chancel-lor MB. State of the art of where weare at using stem cells for stressurinary incontinence. Neurourol Ur-
odyn 2007; 26: 966–71.8 Schmidt E, Bruch HP. Autotransplan-
tation of smooth muscle for treatingincontinence of sphincters. J Chir(Paris) 1981; 118: 315–20.
9 Lorenzi M, Vernillo R, Garzi A, Vin-digni C, D’Onofrio P, Angeloni GM,Stefanoni M, Picchianti D et al.
Experimental internal anal sphincterreplacement with demucosated colo-nic plication. Tech Coloproctol 2003;7: 9–16.
10 Ratani RS, Yazaki E, Scott M, PilotMA, Williams NS. Electrically stim-ulated smooth muscle neosphincter.Br J Surg 1997; 84: 1286–9.
11 Furness JB, Pontell L, Ferens D, Bra-mich N, McKeon B, O’Connell HE.Re-innervation of smooth musclethat is transplanted to provide ure-thral sphincter augmentation. AutonNeurosci 2011; 159: 71–6.
12 Furness JB, Shafton AD, HirstGD, O’Connell HE. Stimulatedsmooth muscle neosphincter inmale intrinsic sphincter deficiency:proof of principle studies in a rabbitmodel. Neurourol Urodyn 2010; 29:S24–8.
13 Canning BJ. Reflex regulation of air-way smooth muscle tone. J Appl
Physiol 2006; 101: 971–85.14 Guyenet PG. The sympathetic con-
trol of blood pressure. Nat Rev Neu-
rosci 2006; 7: 335–46.15 Chandra A, Ghoshal UC, Gupta V,
Jauhari R, Srivastava RN, Misra A,KumarA,KumarM. Physiological andfunctional evaluation of the trans-posed human pylorus as a distalsphincter. J Neurogastroenterol Motil
2012; 18: 269–77.16 Chandra A, Kumar A, Noushif M,
Gupta V, Singh D, Kumar M, Srivast-ava RN, Ghoshal UC. Perineal antro-pylorus transposition for end-stagefecal incontinence in humans: initialoutcomes. Dis Colon Rectum 2013;56: 360–6.
17 Chandra A, Kumar A, Noushif M,Gupta N, Kumar V, Chauhan NK,Gupta V. Feasibility of neurovascularantropylorus perineal transpositionwith pudendal nerve anastomosis fol-lowing anorectal excision: a cadaveric
study for neoanal reconstruction.Ann Coloproctol 2013; 29: 7–11.
18 Chandra A, Kumar A, Noushif M,Gupta V, Kumar V, Srivastav PK,Malhotra HS, Kumar M et al. Neuro-vascular antropylorus perinealtransposition using inferior rectalnerve anastomosis for total anorectalreconstruction: preliminary report inhumans. Tech Coloproctol 2014; 18:535–42.
19 Rodr�ıguez L, Rodr�ıguez P, Neto MG,Ayala JC, Saba J, Berel D, Conklin J,Soffer E. Short-term electrical stimu-lation of the lower esophageal sphinc-ter increases sphincter pressure inpatients with gastroesophageal refluxdisease. Neurogastroenterol Motil
2012; 24: 446–50.20 Sanmiguel CP, Hagiike M, Mintchev
MP, Cruz RD, Phillips EH, CunneenSA, Conklin JL, Soffer EE. Effect ofelectrical stimulation of the LES onLES pressure in a canine model. Am J
Physiol Gastrointest Liver Physiol
2008; 295: G389–94.21 Matzel KE, Schmidt RA, Tanagho EA.
Neuroanatomy of the striated mus-cular anal continence mechanism.Implications for the use of neurosti-mulation. Dis Colon Rectum 1990;33: 666–73.
22 Matzel KE, Stadelmaier U, Hohen-fellner M, Gall FP. Electrical stimu-lation of sacral spinal nerves fortreatment of faecal incontinence.Lancet 1995; 346: 1124–7.
23 Ganio E, Luc AR, Clerico G, Tromp-etto M. Sacral nerve stimulation fortreatment of fecal incontinence: anovel approach for intractable fecalincontinence. Dis Colon Rectum2001; 44: 619–31.
24 Malmfors T, Furness JB, CampbellGR, Burnstock G. Re-innervation ofsmooth muscle of the vas deferenstransplanted into the anterior cham-ber of the eye. J Neurobiol 1971; 2:193–207.
© 2014 John Wiley & Sons Ltd1348
A. Chandra et al. Neurogastroenterology and Motility