Embed Size (px)
Citation preview
Neurology of the Upper limb
Donald Sammut Hand Surgeon Kings Upper Limb Anatomy plus lecture notes
The$Neck$

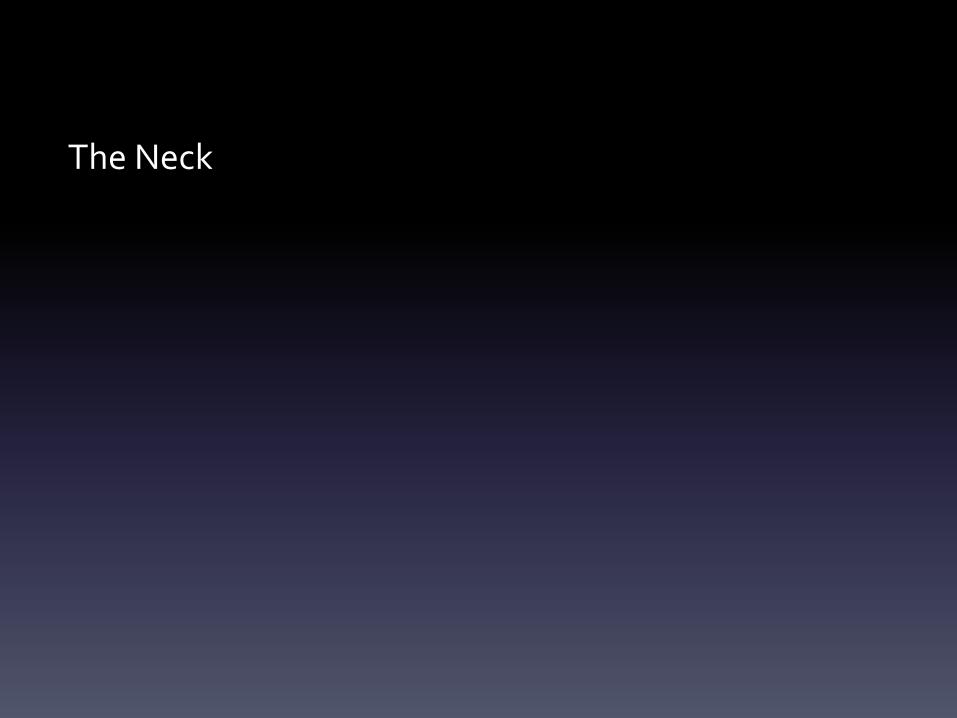
The$Nerve$roots$which$supply$the$Upper$Limb$are$C5$to$T1$Pre<fixed$(C4$to$C8)$and$Post<fixed$(C6$to$T2)$plexus$not$uncommon.$Also$common$contributions$from$C4$and$from$T2$in$a$normally$rooted$plexus.$$The$anterior$nerve$roots$emerge$between$the$vertebrae$and$immediately$pass$$through$the$first$area$of$possible$compression:$The$root$nerve$canal$is$bounded$$Anteriorly$by$the$posterior$margin$of$the$intervertebral$disc$and$$Posteriorly,$by$the$facet$joint$between$vertebrae.$$Pathology$of$the$disc,$or$joint,$or$both,$can$narrow$this$channel$and$compress$$the$nerve$root$

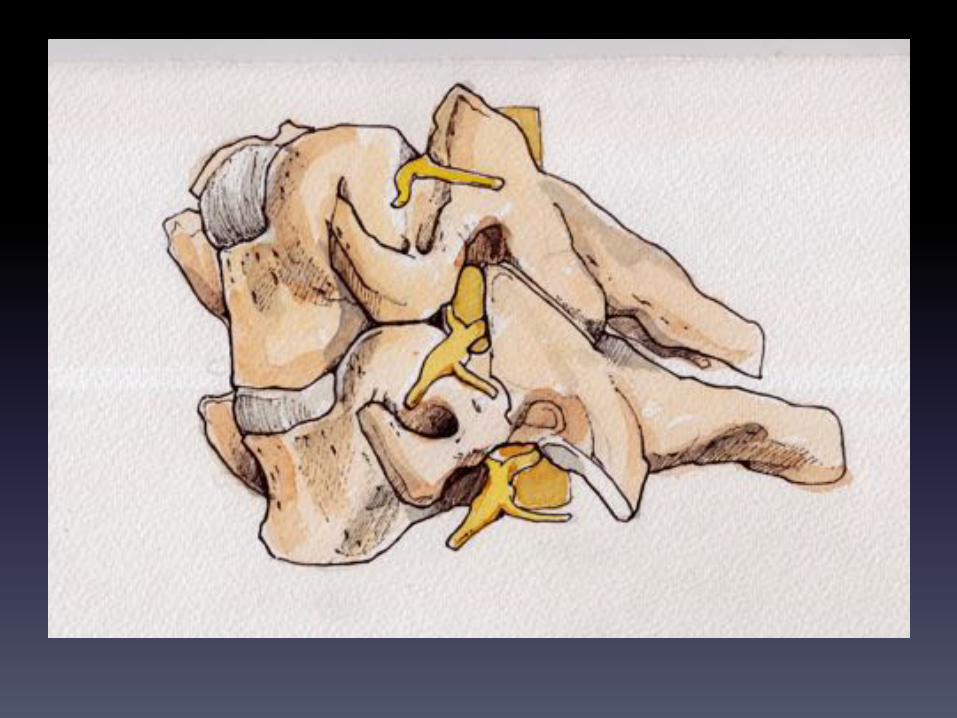

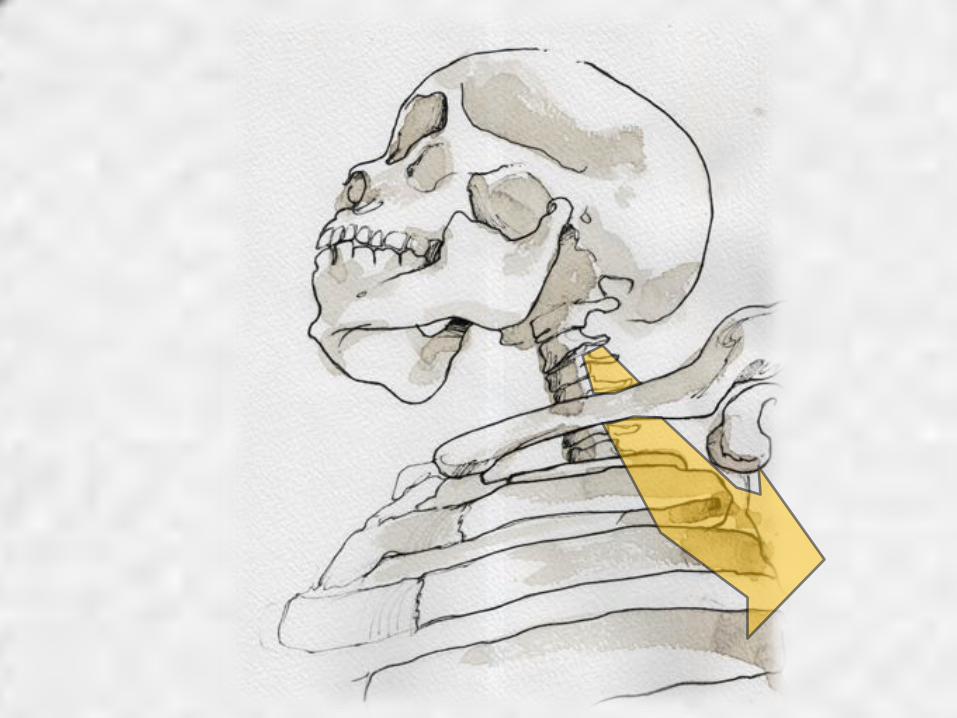
The$roots$emerge$from$the$cervical$spine$into$the$plane$between$$Scalenius$Anterior$and$Scalenius$Medius.$$$Scalenius*Anterior:**Origin:$Anterior$tubercles$of$Cervical$vertebae$C3$to$6$(C6$tubercle$is$the$Carotid$tubercle)$Insertion:$The$scalene$tubercle$on$inner$border/upper$surface$1st$rib$$Scalenius*Medius:*Origin:$Posterior$tubercles$of$all$cervical$vertebrae$Insertion:$Quadrangular$area$between$the$neck$and$subclavian$groove$1st$rib$$Exiting$from$the$Scalenes,$the$trunks$lie$in$the$posterior$triangle$of$the$neck.$The$posterior$triangle$is$bounded$anteriorly$by$SternoCleidoMastoid$and$$posteriorly$by$the$Trapezius.$The$inferior$border$is$the$clavicle$.$The$apex$of$the$triangle$superiorly$is$at$the$back$of$the$skull$on$the$superior$nuchal$line$$$
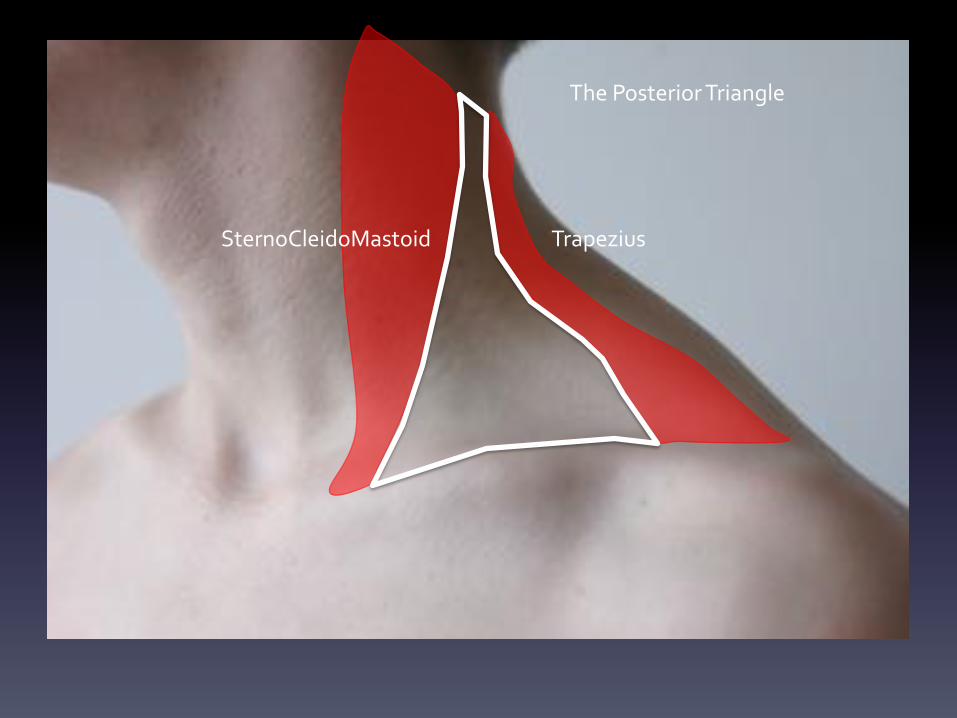
The$Posterior$Triangle$
SternoCleidoMastoid$ Trapezius$
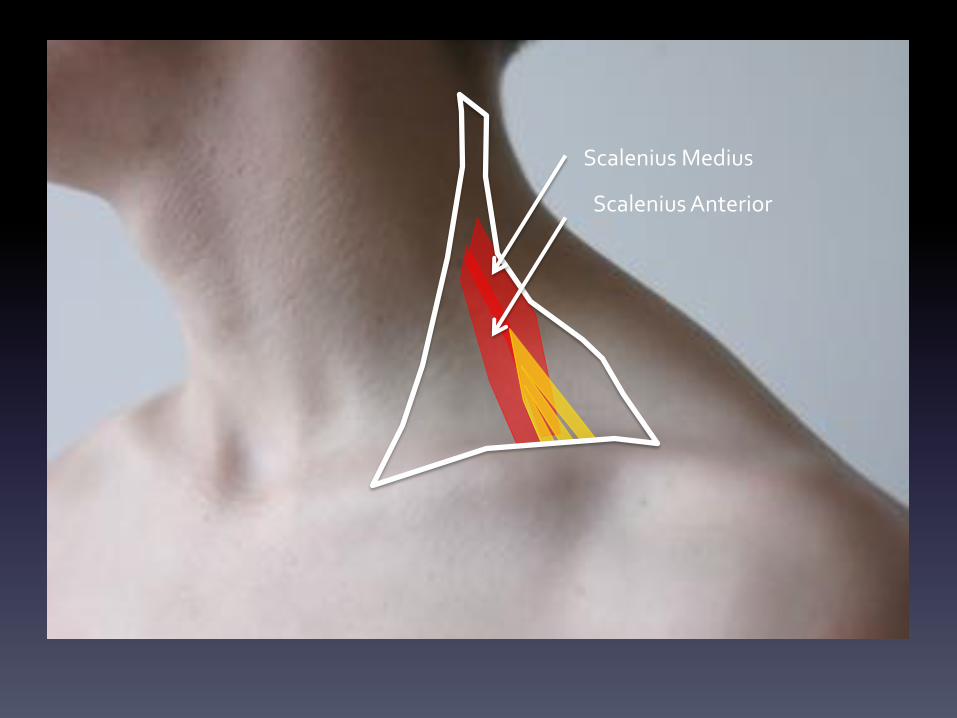
Scalenius$Medius$
Scalenius$Anterior$
The$general$route$of$travel$of$the$Brachial$$Plexus$:$$
$Exit$from$the$root$canals$$$–$travel$through$plane$between$Scalenius$Anterior$and$Scalenius$Medius$$–$In$posterior$triangle$covered$by$investing$layer$of$deep$Cervical$fascia$$$–$over$first$rib$in$company$of$Subclavian$artery$$–$enclosed$in$axillary$sheath$
$ $–$into$apex$of$axilla$$$–through$axilla$and$ending$in$5$main$terminal$branches$

The$Brachial$Plexus$is$formed$from$the$anterior$rami$of$C5,6,7,8,T1$after$they$$have$supplied$prevertebral$and$scalene$muscles$.$$The$various$parts$of$the$Brachial$Plexus$$and$their$location:$$ROOTS:$ $ $ $Between$the$scalenes$TRUNKS:$ $ $In$the$Posterior$Triangle$DIVISIONS: $ $Behind$the$clavicle$CORDS: $ $ $In$the$axilla$$(Thus$the$roots$and$Trunks$are$Supra<clavicular$while$the$Divisions$and$cords$are$Infra<Clavicular).$$The$Plexus$exists$as$a$system$of$delivering$fibres$from$more$than$one$root$into$a$$specific$end$nerve.$$$$

Dorsal$Scapular$Nerve$(nerve$to$Rhomboids)$
N.$To$$Subclavius$
Long$Thoracic$Nerve$(Nerve$to$Serratus$Anterior)$
Upper$Sub
scapular$N
erve$
Thoracod
orsal$Nerv
e$
Lower$Sub
scapular$N
erve$
Suprascapular$Nerve$
Lateral$Pectoral$Nerve$
MUSCULOCUTANEOUS$
MEDIAN$
ULNAR$
RADIAL$
AXILLARY$
THE$BRACHIAL$PLEXUS$
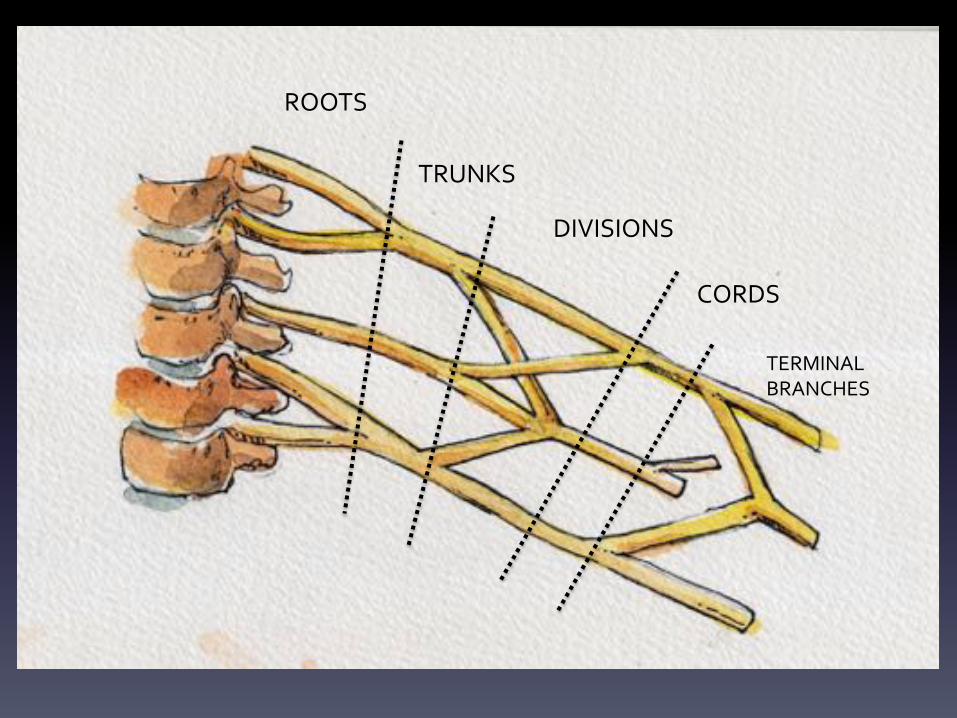
ROOTS$
TRUNKS$
DIVISIONS$
CORDS$
TERMINAL$$BRANCHES$
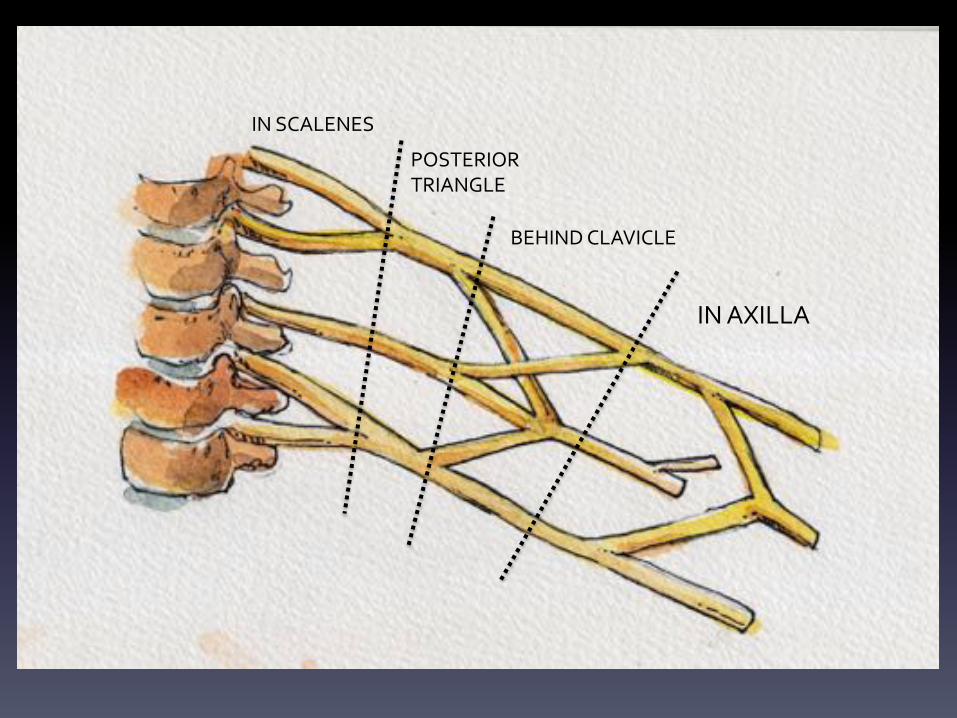
IN$SCALENES$
POSTERIOR$$TRIANGLE$
BEHIND$CLAVICLE$
IN$AXILLA$
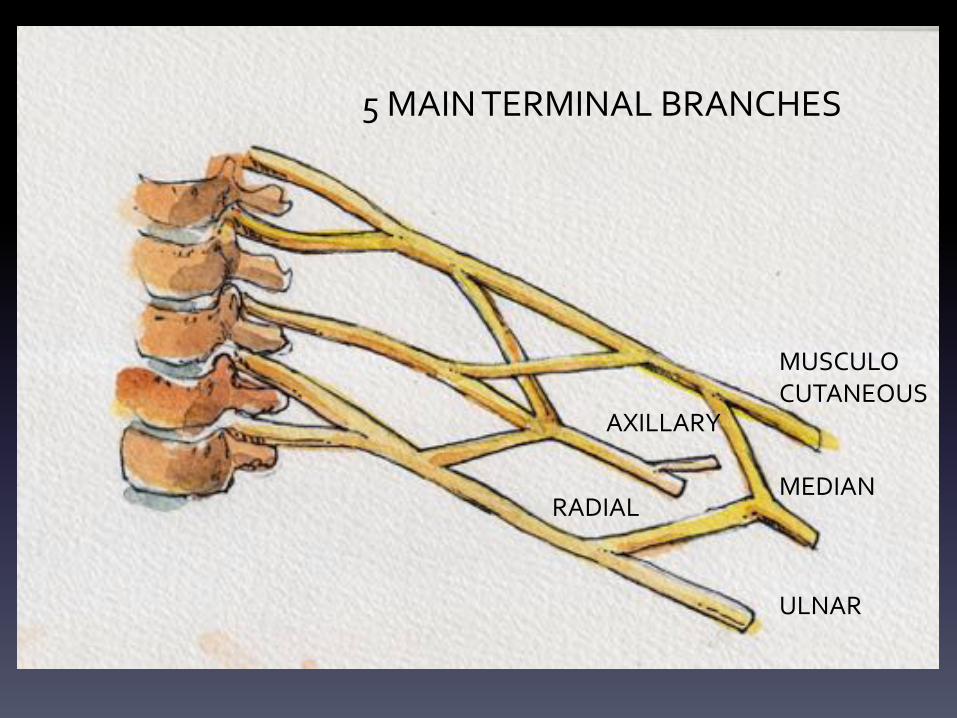
There$are$5$main$Terminal$Branches$of$the$Brachial$Plexus:$$FROM$THE$POSTERIOR$CORD:$ $ $THE$RADIAL$NERVE$
$ $ $ $ $THE$AXILLARY$NERVE$$FROM$THE$LATERAL$AND$MEDIAL$CORDS: $THE$MUSCULOCUTANEOUS$NERVE$
$ $ $ $ $THE$MEDIAN$NERVE$$ $ $ $ $THE$ULNAR$NERVE$
$$$$$
AXILLARY$
RADIAL$
ULNAR$
MEDIAN$
MUSCULO$CUTANEOUS$
5$MAIN$TERMINAL$BRANCHES$

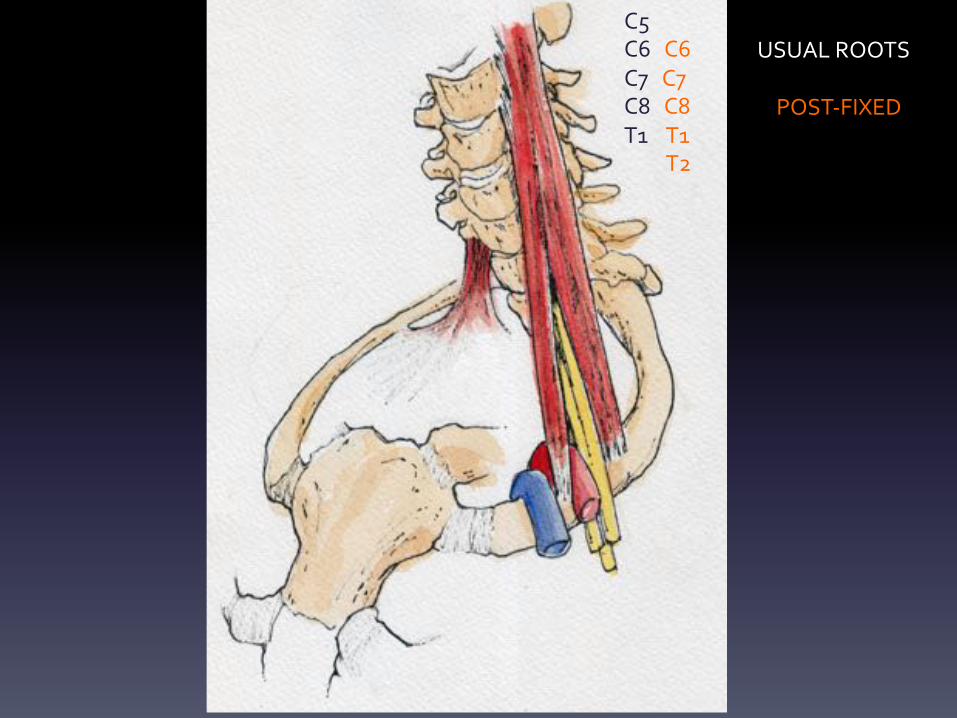
C5$C6$$$C6$C7$$$C7$C8$$$C8$T1$$$$T1$$$$$$$$$$T2$
USUAL$ROOTS$$$$$$POST<FIXED$
$$$$The$scalenes$are$Prevertebral$muscles$which$have$migrated$anteriorly$along$the$1st$rib.$Like$other$prevertebral$muscles$they$are$invested$in$Pre<Vertebral$fascia.$$$This$fascia$is$prolonged$over$the$Brachial$plexus$as$it$exits$between$the$two$scalenes$and$forms$$the$Axillary$sheath.$$Since$the$Subclavian$artery$passes$posterior$to$the$Scalenius$anterior,$it$comes$to$lie$within$the$$sheath$along$with$the$nerve.$$The$axillary$sheath$thus$contains$the$subclavian$artery$and$the$tightly$bunched$up$terminal$$branches$$of$the$plexus$–$an$important$anatomical$feature$relevant$t$o$the$administration$of$axillary$nerve$blocks.$$$$

BACHIAL$PLEXUS$BLOCKS$$Nerve$blocks$involve$the$infiltration$of$the$space$around$a$nerve$with$local$anaesthetic.$The$axillary$sheath$forms$a$convenient$discrete$compartment$which$retains$anaesthetic$$around$the$nerves.$The$subclavian$artery$pulsations$are$palpable$and$present$a$convenient$means$of$locating,$$by$palpation,$the$nerves.$$Blocking$of$the$Brachial$plexus$can$be$performed$at$many$levels:$Inter$Scalene$Supra$Clavicular$Infra$Clavicular$Axillary$$The$commonest,$and$safest,$method$of$locating$the$Brachial$plexus$is$by$the$use$of$an$$Ultrasound$Probe.$This$demonstrates$the$nerve$and$artery$and$also$the$needle$tip$as$it$is$$advanced.$$$Accurate$Placement$is$crucial:$The$infiltration$must$NOT$be$into$the$nerve$substance$–$this$causes$direct$nerve$damage.$The$anaesthetic$must$NOT$be$inserted$intravascularly$–$The$agent$works$by$blocking$electrical$conduction.$$It$will$do$so$equally$effectively$with$nerve$conduction$and$with$the$conduction$of$Cardiac$Muscle$$fibres.$Major$Intravascular$injection$of$local$anaesthetic$agent$will$cause$a$bradycaria$(slowing$of$heart$rhythm)$and$may$even$cause$total$block$i.e.$it$will$stop$the$heart.$$$$

THE$AXILLARY$$SHEATH$

Interscalene$Block$
Supraclavicular$Block$
Infraclavicular$Block$
Axillary$Block$
The$exit$of$the$nerve$roots$and$the$course$of$the$Brachial$plexus$through$the$neck$$make$it$vulnerable$to$various$points$of$compression$$1. Common,$high,$$insertion$of$Scalenius$Anterior$and$Scalenius$Medius.$$This$causes$the$lower$parts$of$the$Brachial$plexus$to$kink$over$the$(usually$sharp)$common$$Muscle.$Compression$at$this$point$will$mainly$affect$C8/T1.$
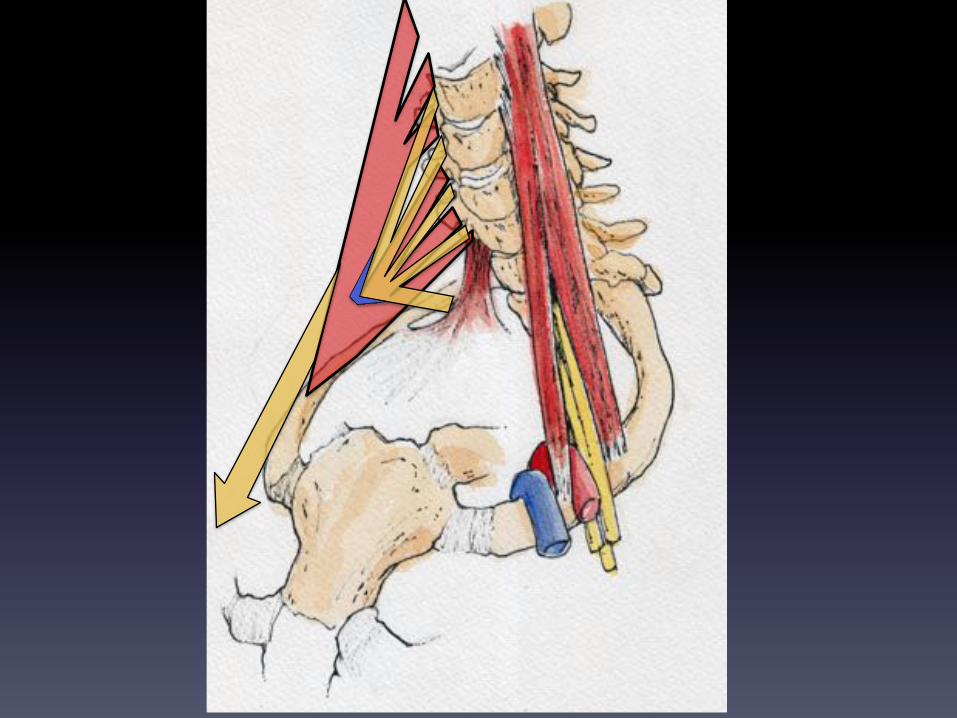
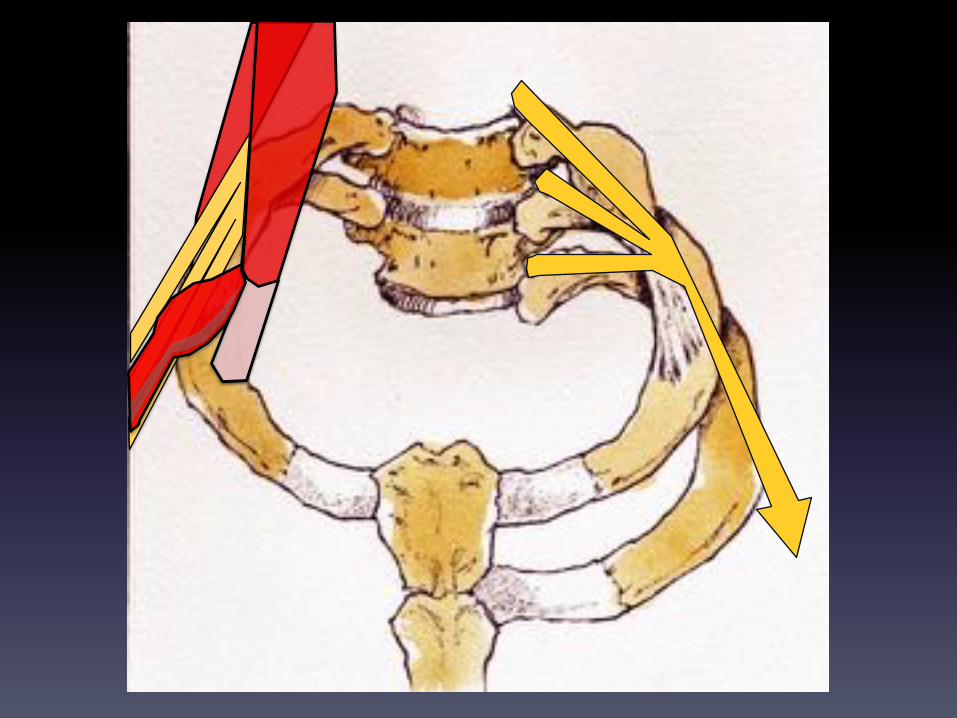
$2.$The$presence$of$an$anomalous$Cervical$Rib$or$Cervical$band,$will$also$cause$the$$lower$reaches$of$the$brachial$Plexus$to$kink$over$the$raised$exit$point$from$the$neck.$$The$presence$of$a$cervical$rib$is$associated$with$a$post<fixed$Brachial$plexus$$(i.e.$a$Plexus$formed$from$the$roots$of$C6$–$T2)$$

C6$C7$C8$T1$T2$
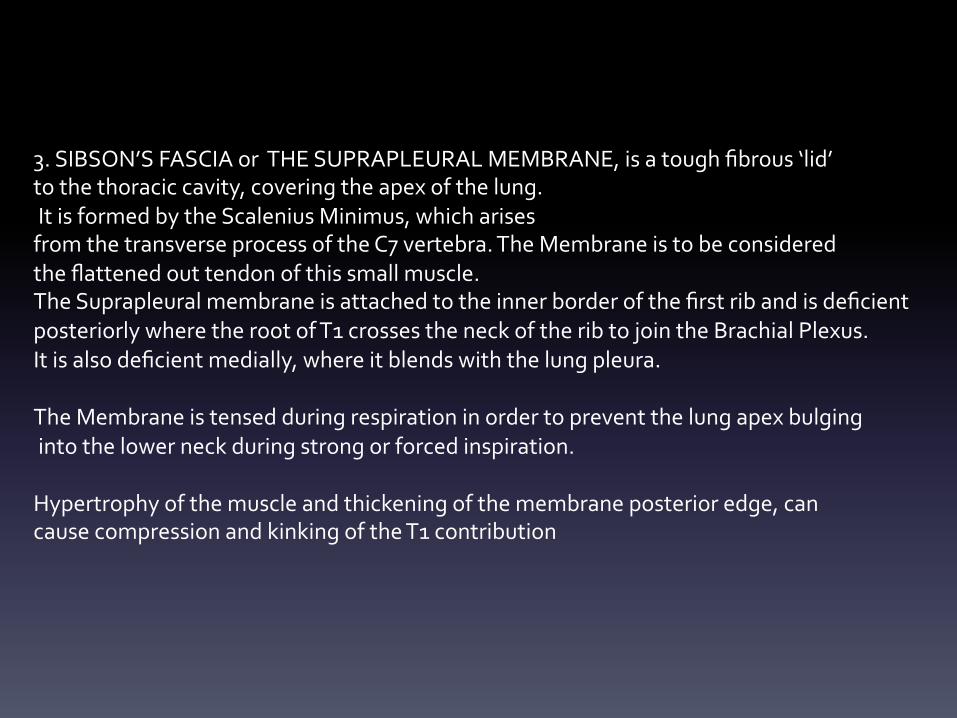
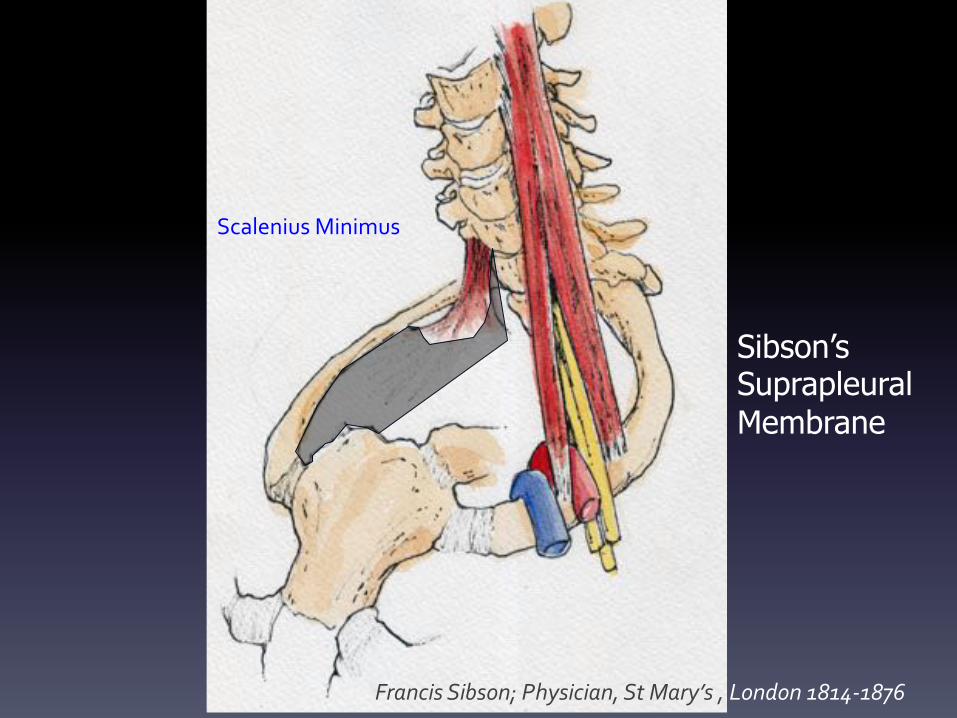
3.$SIBSON’S$FASCIA$or$$THE$SUPRAPLEURAL$MEMBRANE,$is$a$tough$fibrous$‘lid’$$to$the$thoracic$cavity,$covering$the$apex$of$the$lung.$$It$is$formed$by$the$Scalenius$Minimus,$which$arises$$from$the$transverse$process$of$the$C7$vertebra.$The$Membrane$is$to$be$considered$$the$flattened$out$tendon$of$this$small$muscle.$The$Suprapleural$membrane$is$attached$to$the$inner$border$of$the$first$rib$and$is$deficient$$posteriorly$where$the$root$of$T1$crosses$the$neck$of$the$rib$to$join$the$Brachial$Plexus.$$It$is$also$deficient$medially,$where$it$blends$with$the$lung$pleura.$$The$Membrane$is$tensed$during$respiration$in$order$to$prevent$the$lung$apex$bulging$$into$the$lower$neck$during$strong$or$forced$inspiration.$$Hypertrophy$of$the$muscle$and$thickening$of$the$membrane$posterior$edge,$can$$cause$compression$and$kinking$of$the$T1$contribution$$
Sibson’s Suprapleural Membrane
Francis(Sibson;(Physician,(St(Mary’s(,(London(181491876(
Scalenius$Minimus$
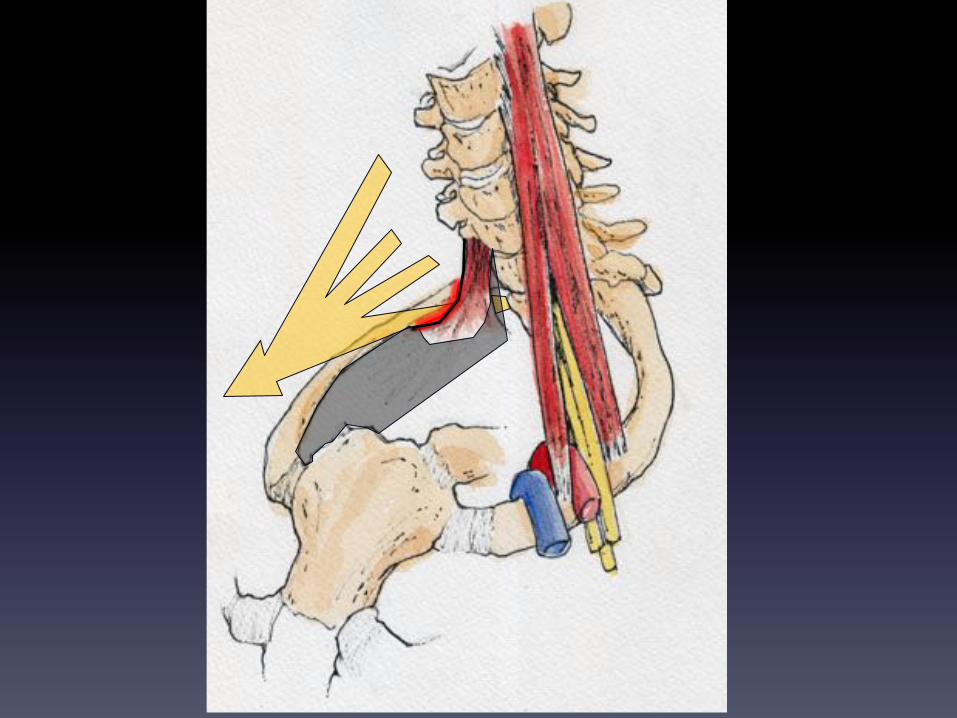
4.$A$tumour$in$the$apex$of$the$lung$can$infiltrate$all$structures$here$and$cause$compression$$or$direct$infiltration$of$the$lower$parts$of$the$Brachial$Plexus$($Thoracic$Outlet$Syndrome).$$$Typically,$an$early$sign$is$Horner’s$Syndrome$(compression$of$the$sympathetic$ganglion$$at$this$level)$and$can$present$with$Superior$Vena$Cava$obstruction$$
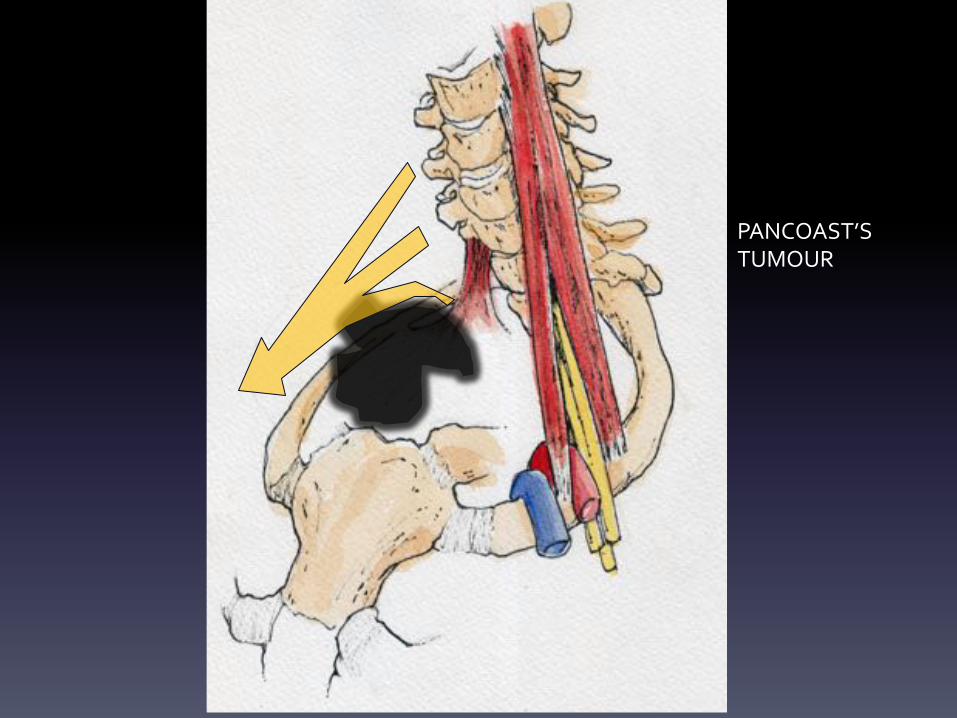
PANCOAST’S$$TUMOUR$
A$DERMATOME$is$an$area$of$skin$supplied$by$a$single$spinal$nerve.$$It$is$useful$to$know$the$general$distribution$of$dermatomes$(and$segmental$levels)$of$the$Upper$limb.$$The$general$pattern$is$that$of$the$‘apex’$of$the$limb,$the$hand,$being$supplied$by$C6,7,8$$Above$this,$along$the$pre<axial$border$of$the$limb,$are$the$upper$parts$of$the$Plexus:$C5,6,7$Below$this,$along$the$post$axial$border$of$the$limb,$are$the$lower$parts$of$the$Plexus:$C7$to$T2$$$This$general$pattern$is$consistent$and$reliable,$but$the$specific$areas$supplied$are$very$variable$$(i.e.$there$are$no$reliable$and$consistent$boundaries)$

C3,4$
C5,6$
T2$ C5,6$
C5,6$
C7,8$
C6,7,8$
C8,T1$
C8,T1$
DERMATOMES$$$$$$$FOREARM$$RADIAL:$$ $$$$$$$$C5,6$MEDIAL$CUTANEOUS:$C8,TI$$$$$$HAND$$MEDIAN:$$ $$$$$C6,7,8$ULNAR:$ $ $$$$$C8,$T1$

MYOTOMES$$The$same$segmental$innervation$applies$to$the$muscles.$$A$MYOTOME$is$a$group$of$muscles$innervated$by$a$single$spinal$nerve.$In$clinical$practice,$it$is$best$to$remember$actions$and$their$innervation,$rather$than$$single$groups$and$these$may$involve$more$than$one$root$$$SHOULDER:$ $ $Abduct$and$laterally$Rotate:$ $C5$
$ $ $Adduct$and$medially$Rotate:$ $C6,7,8$$$ELBOW: $ $ $Flex:$ $ $ $C5,6$
$ $ $Extend:$ $ $ $C7,8$$$FOREARM: $ $ $Pronate: $ $ $C7,8$
$ $ $Supinate $ $ $:C6$$$WRIST: $ $ $Flex: $ $ $C6,7$
$ $ $Extend: $ $ $C6,7$ $$
$$LONG$TENDONS $ $Flex: $ $ $C7,8$Fingers$and$Thumb $ $Extend: $ $ $C7,8
$ $ $$$
$ $ $$HAND$INTRINSICS $ $All $ $ $T1$$$$

It$is$useful$to$remember$the$main$nerve$to$each$functional$compartment:$Thus:$$In$the$arm:$Flexor$Compartment:$MUSCULOCUTANEOUS$NERVE$Extensor$Compartment:$RADIAL$NERVE$$In$the$forearm:$
Flexor$compartment:$MEDIAN$(and(some(by(Ulnar*)(
Extensor$Compartment:$POSTERIOR$INTEROSSEOUS$NERVE$$
In$the$hand: $$$$$$$$ULNAR$(and(some(by(Median*)(
(
*(See(below $$$$$

FLEX.$ARM:$MUSCULOCUTANEOUS$
EXT.$ARM:$RADIAL$
FLEX.$FOREARM:$MEDIAN$(+(Ulnar)(
EXT.$FOREARM$POST.$INTEROSS$
HAND:$ULNAR$(+Median)(

The$Musculo$cutaneous$Nerve$$
Nerve$of$the$Flexor$Compartment$of$the$arm$
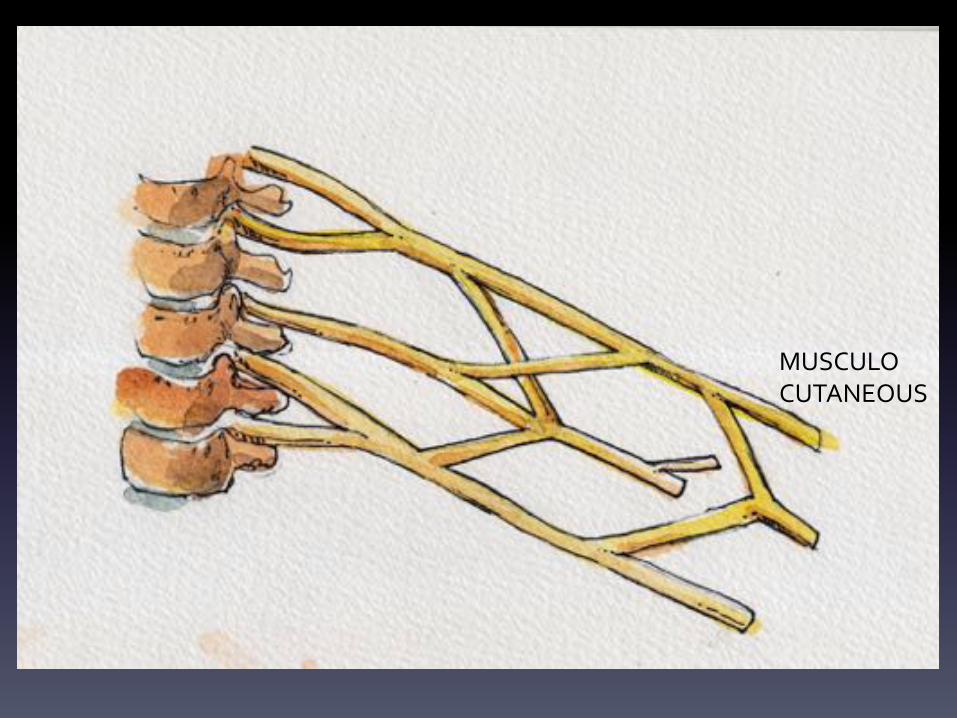
MUSCULO$CUTANEOUS$
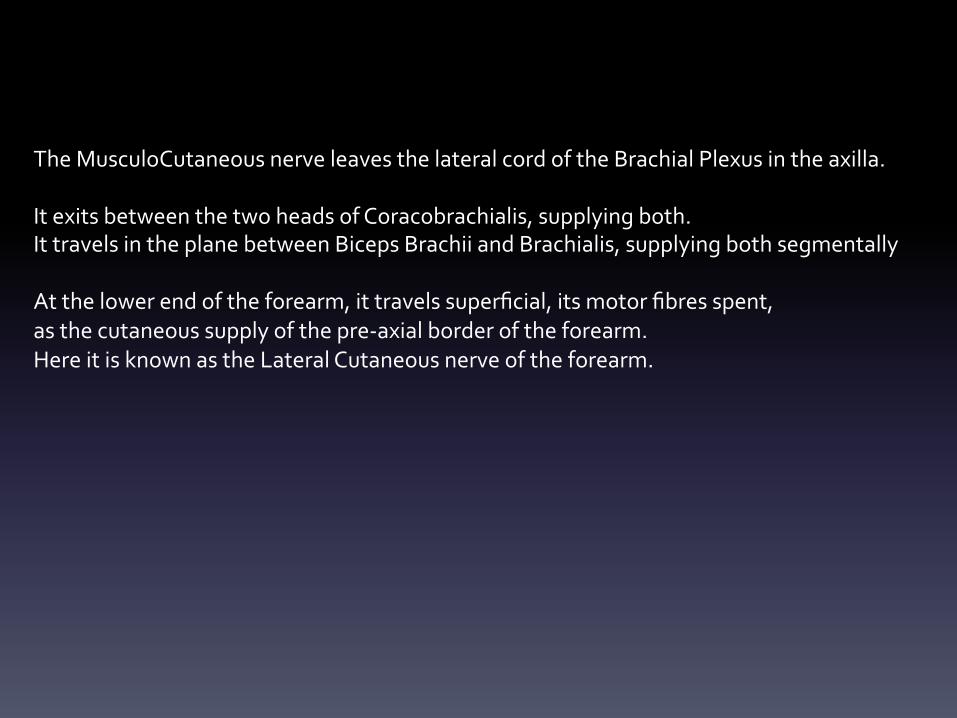
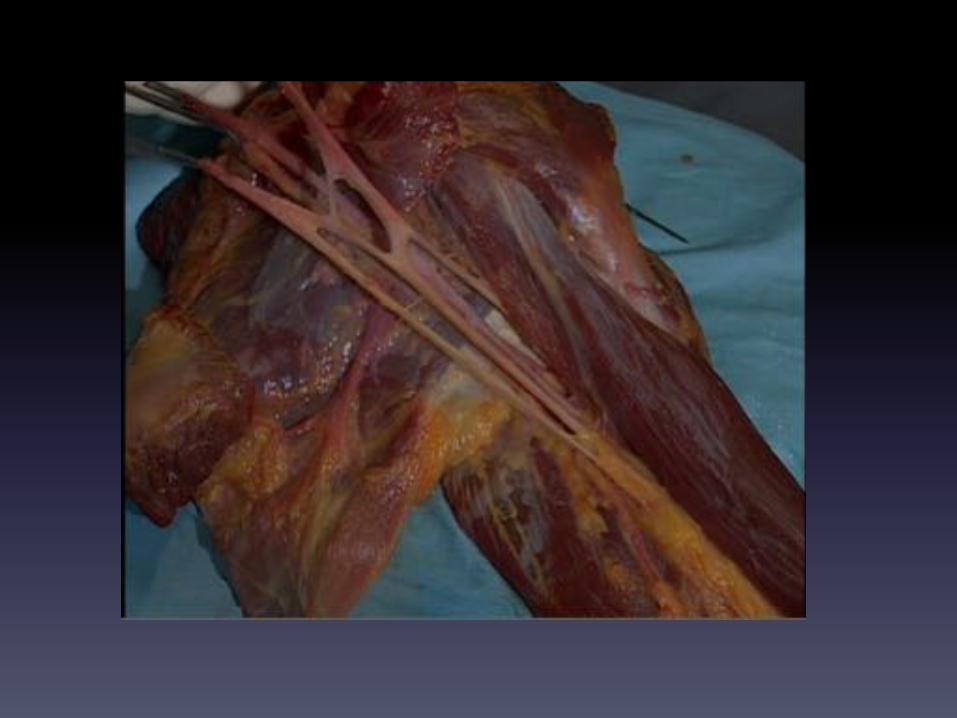
The$MusculoCutaneous$nerve$leaves$the$lateral$cord$of$the$Brachial$Plexus$in$the$axilla.$$It$exits$between$the$two$heads$of$Coracobrachialis,$supplying$both.$It$travels$in$the$plane$between$Biceps$Brachii$and$Brachialis,$supplying$both$segmentally$$At$the$lower$end$of$the$forearm,$it$travels$superficial,$its$motor$fibres$spent,$$as$the$cutaneous$supply$of$the$pre<axial$border$of$the$forearm.$$Here$it$is$known$as$the$Lateral$Cutaneous$nerve$of$the$forearm.$$
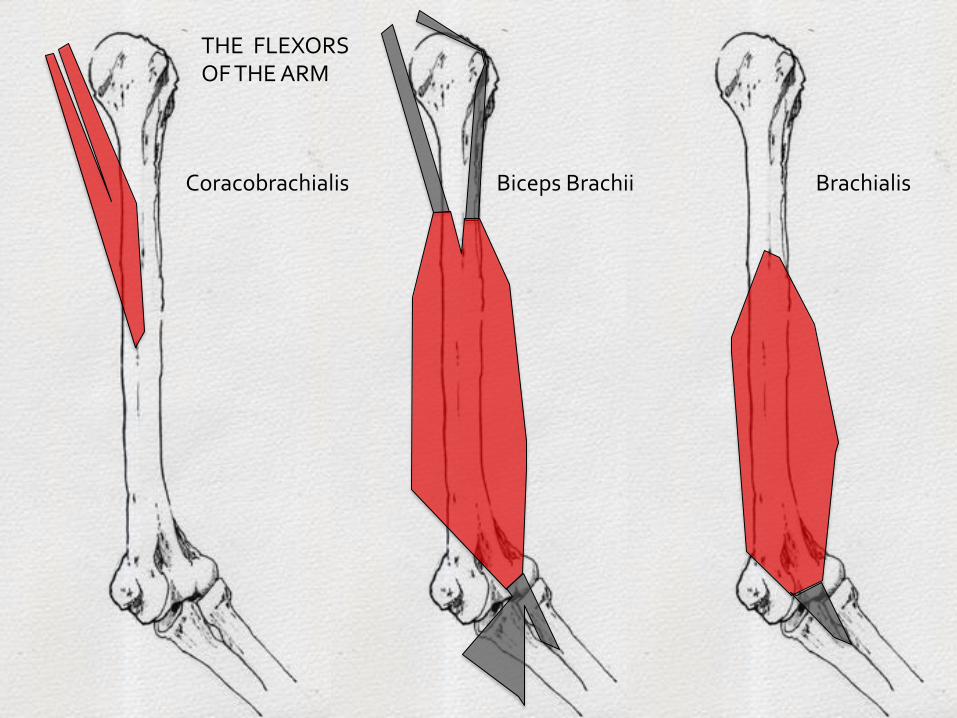
Coracobrachialis$ Brachialis$Biceps$Brachii$
THE$$FLEXORS$$OF$THE$ARM$
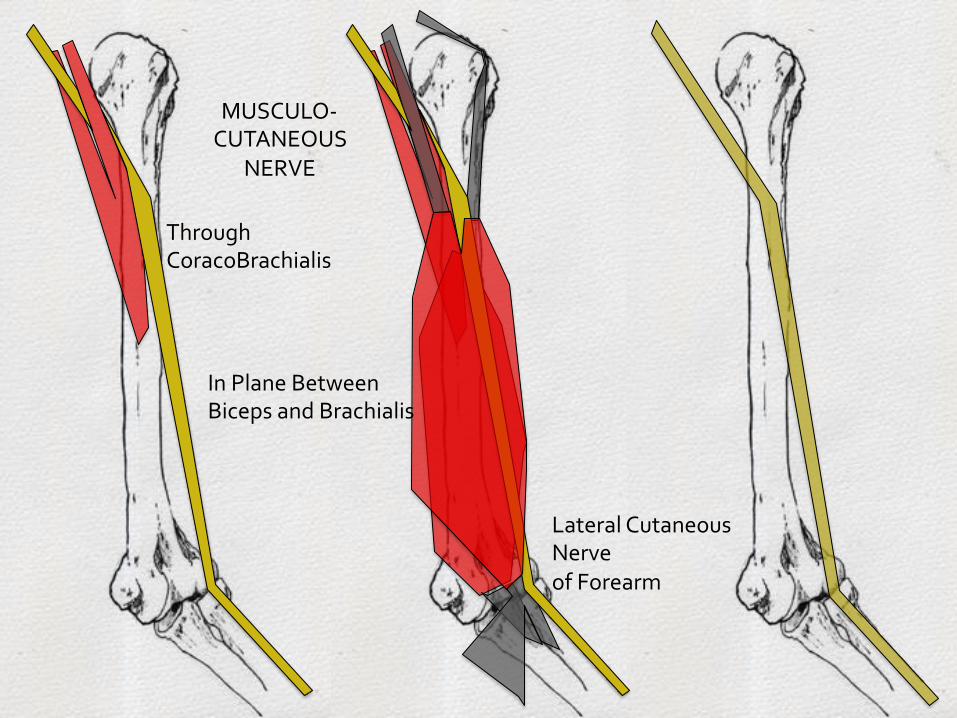
MUSCULO<$CUTANEOUS$
NERVE$
Through$$CoracoBrachialis$
In$Plane$Between$$Biceps$and$Brachialis$
Lateral$Cutaneous$$Nerve$of$Forearm$

The$Radial$Nerve$$
Nerve$of$the$Extensor$Compartment$of$the$arm$
The$Radial$nerve$is$the$nerve$of$the$extensor$compartment$of$the$arm.$$It$is$a$terminal$branch$of$the$posterior$cord$of$the$Brachial$Plexus,$exiting$the$axilla$$at$the$lower$border$(over$the$Latissimus$Dorsi$tendon),$by$passing$posterior$to$the$shaft$of$the$humerus.$It$runs$along$the$spiral$groove$of$the$humerus,$in$company$of$the$Profunda$Brachii$artery.$$Here$it$lies$virtually$directly$on$bone,$separated$from$the$bone$surface$by$fibres$of$the$medial$$head$of$triceps.$It$is$vulnerable$to$injury,$with$fracture$of$the$mid<shaft$of$the$humerus,$or$$the$surgery$and$dissection$to$fix$this.$$It$supplies$Triceps.$$It$pierces$the$lateral$intermuscular$septum$after$supplying$triceps$and$comes$to$lie,$briefly,$in$the$flexor$compartment$of$the$arm,$in$the$plane$between$Biceps/Brachialis$and$$Brachioradialis$
The$Axillary$Nerve,$leaves$the$Posterior$Cord$of$the$Brachial$Plexus$and$exits$the$axilla$$through$the$quadrangular$space,$between$subscapularis$and$Teres$Major.$$It$lies$directly$on$bone$at$this$level,$the$surgical$neck$of$the$humerus,$and$is$$vulnerable$to$injury$in$dislocation$of$the$shoulder$or$humeral$fractures.$$It$divides$into$anterior$and$posterior$branches$both$of$which$run$posterior$to$the$humerus:$$The$anterior$branch$supplies$Deltoid$including$the$overlying$skin$.$The$posterior$branch$supplies$Teres$Minor$and$then,$purely$cutaneous,$it$supplies$the$patch$$of$skin$over$the$prominence$of$Deltoid.$Here$it$is$called$the$Upper$lateral$Cutaneous$$nerve$$of$the$arm$$
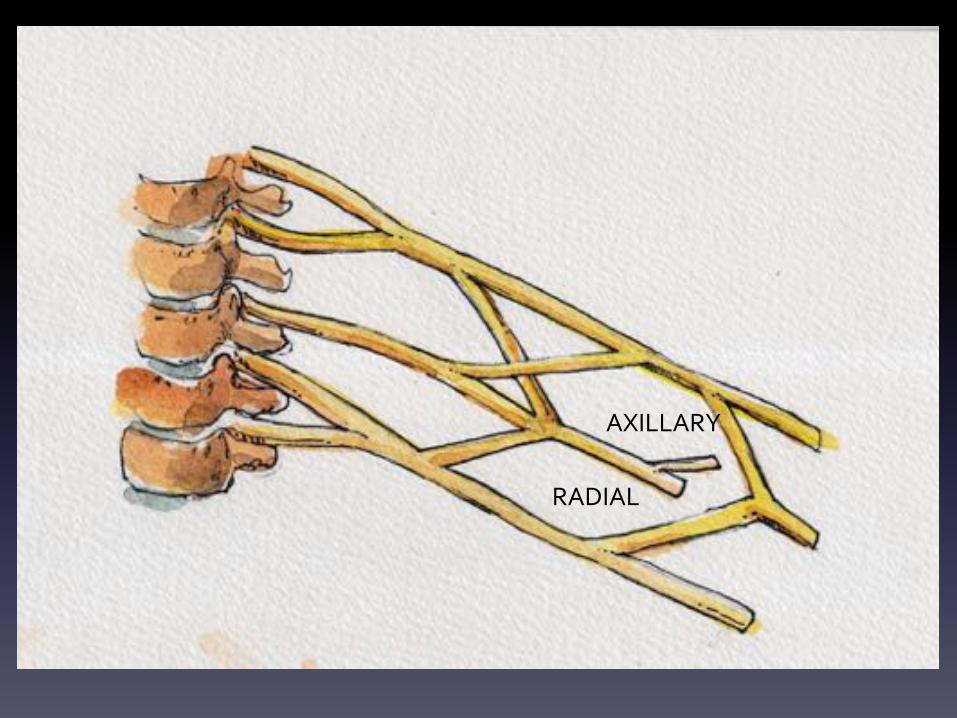
AXILLARY$
RADIAL$
$$
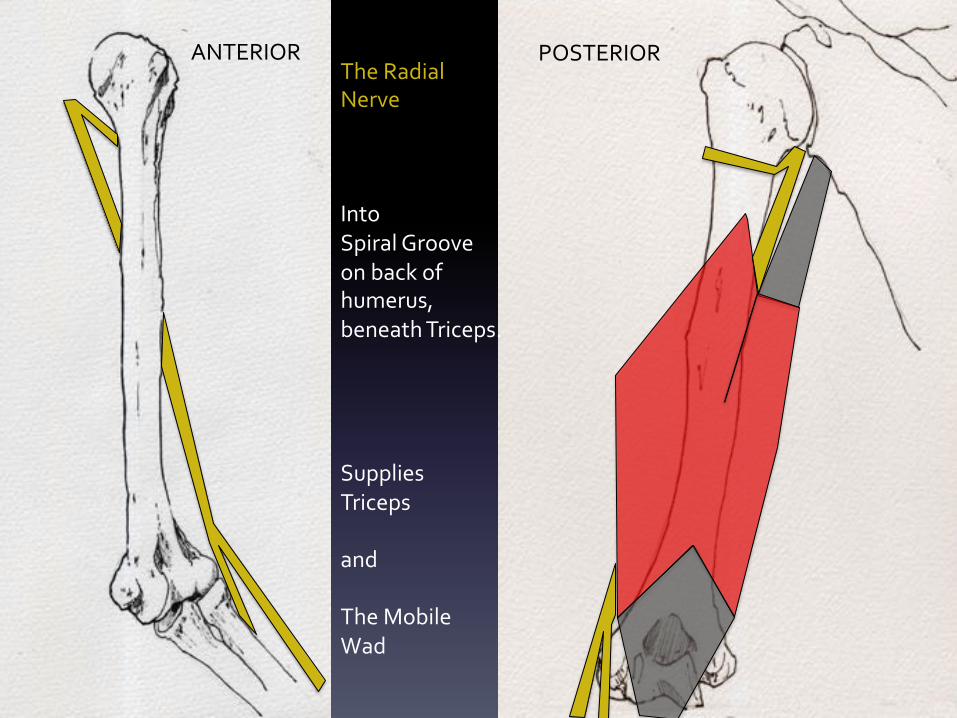
The$Radial$$Nerve$$$$Into$$Spiral$Groove$on$back$of$$humerus,$$beneath$Triceps.$$$$$Supplies$$Triceps$$and$$The$Mobile$$Wad$
ANTERIOR$ POSTERIOR$
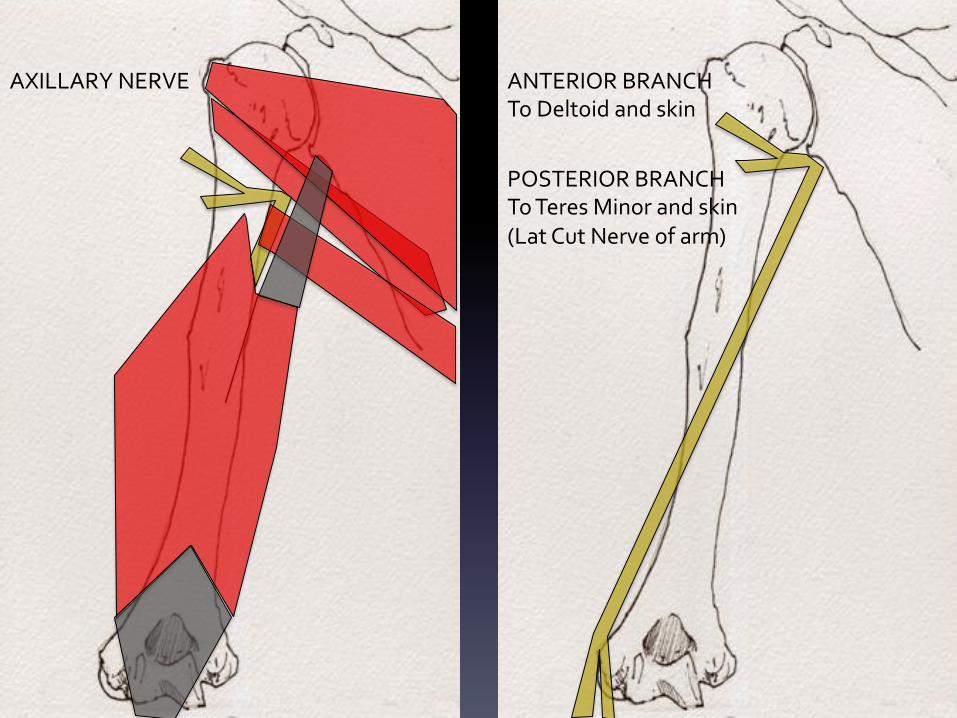
AXILLARY$NERVE$ ANTERIOR$BRANCH$To$Deltoid$and$skin$
POSTERIOR$BRANCH$To$Teres$Minor$and$skin$(Lat$Cut$Nerve$of$arm)$

The$Radial$Nerve$pierces$$the$Lateral$Intermuscular$septum$$From$Extensor$into$$Flexor$Compartment$
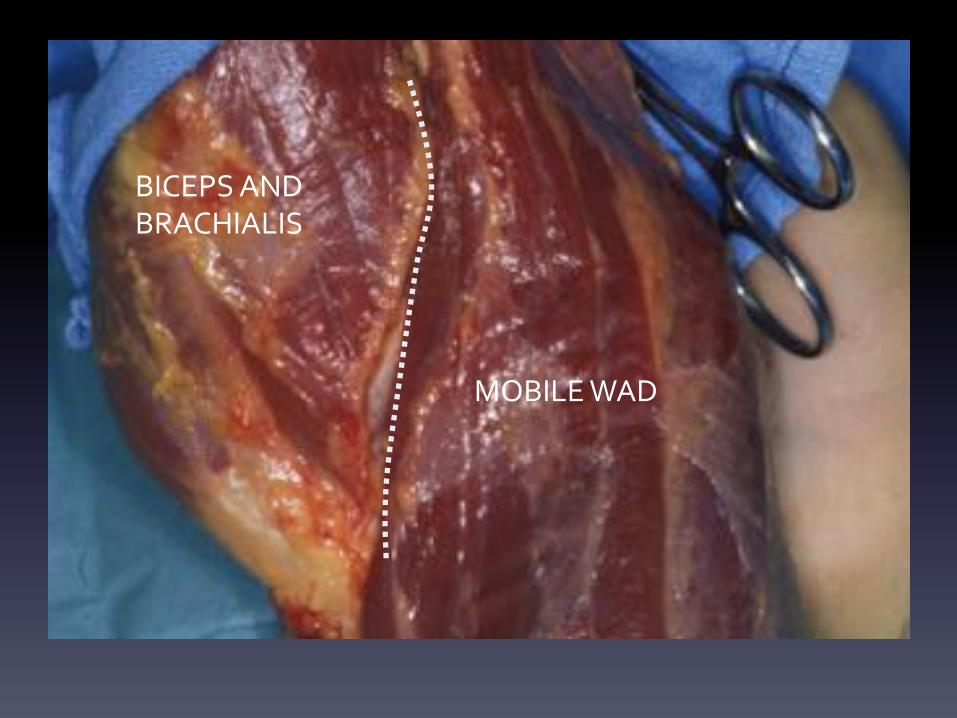
BICEPS$AND$$BRACHIALIS$
MOBILE$WAD$

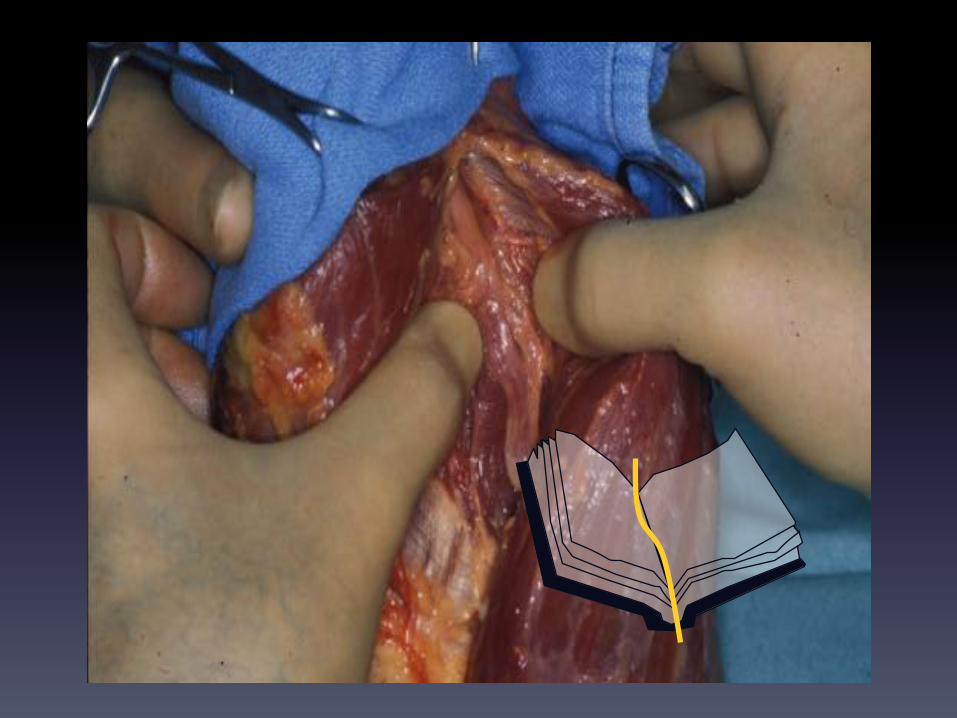
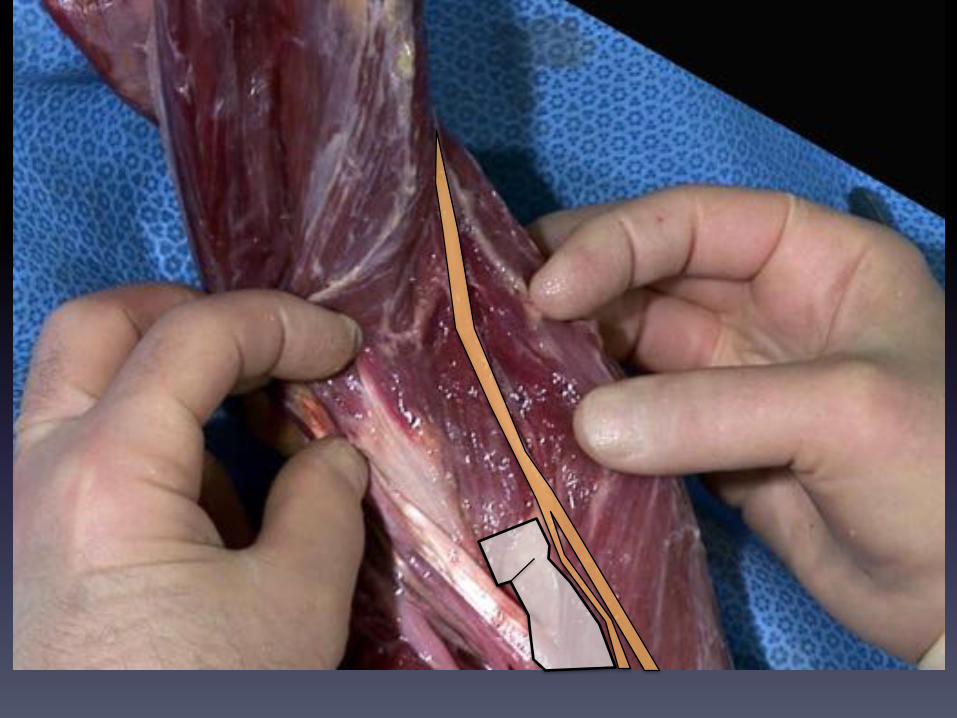
In$the$distal$arm,$the$radial$nerve$can$be$located$by$separation$of$the$muscle$masses$of$$$Biceps/brachialis$on$one$side$and$Brachioradialis$on$the$other.$$In$this$position,$the$Radial$Nerve$divides$into$its$two$terminal$branches$$1. The$Posterior$interosseous$nerve:$Motor$nerve$to$the$Extensor$compartment$of$the$
$$forearm.$$$This$leaves$the$main$trunk$and$reaches$the$extensor$compartment$by$curling$$$around$the$neck$of$the$radius,$between$the$two$heads$of$Supinator$
$



THE$CUBITAL$FOSSA$
2.$The$terminal$cutaneous$branch$which$lies$beneath$Brachioradialis.$It$reaches$the$skin$by$passing$between$Brachioradialis$and$Extensor$Carpi$Radialis$longus.$This$sharp$V$formation$of$tendons$can$cause$compression$of$the$nerve$(Wartenburg’s$syndrome).$$The$cutaneous$radial$nerve$ramifies$over$the$radial$half$of$the$back$of$the$hand.$$It$is$notoriously$vulnerable$t0$injury$on$the$back$of$the$wrist$and$hand$–$Blunt$trauma,$$heavy$bracelets$or$watches,$surgery$in$this$region$can$cause$injury$and$lead$to$a$painful$neuroma.$$$

BR$
ECRL$
The$Cutaneous$Terminal$Branch$of$the$$Radial$Nerve$


The$cutaneous$supply$of$the$back$of$the$hand$is$shared$between:$$The$terminal$cutaneous$radial$nerve$and$$The$dorsal$cutaneous$branch$of$the$ulnar$nerve$
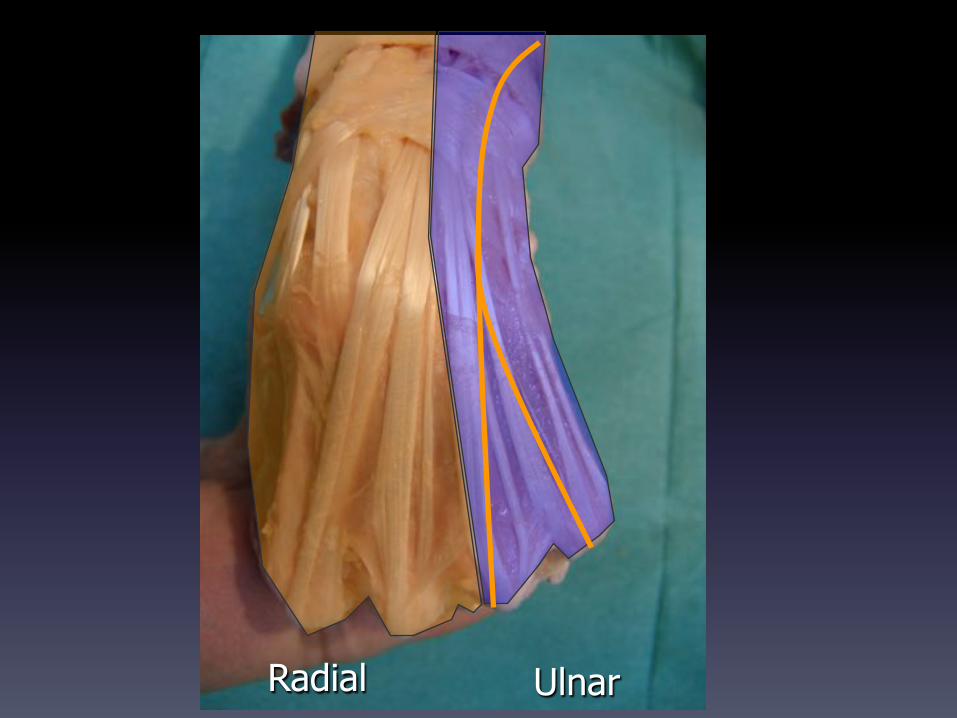
Radial Ulnar

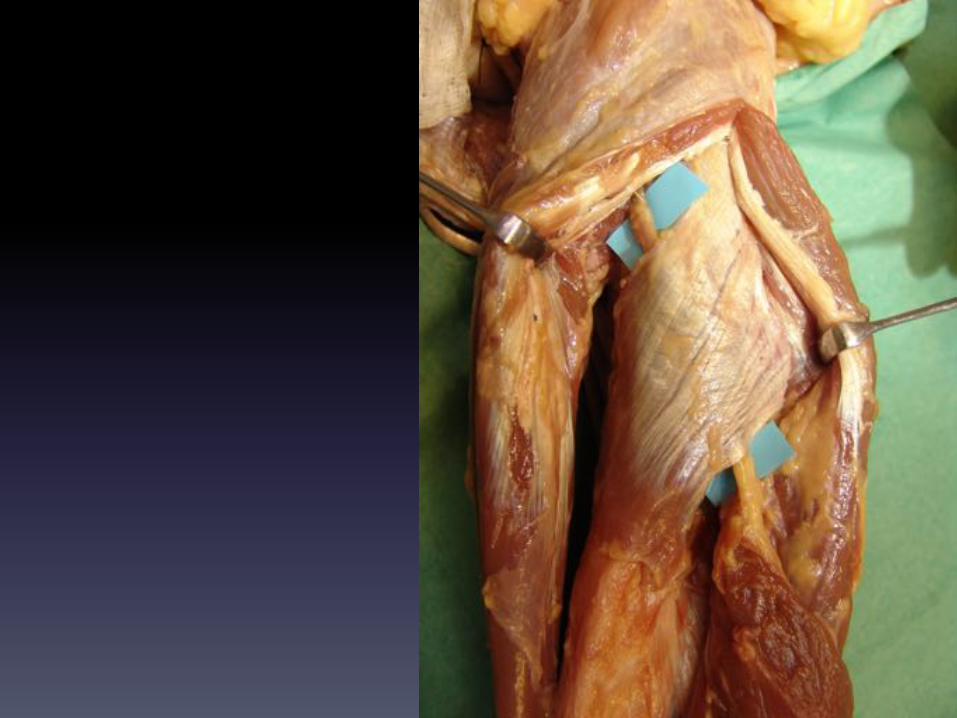
The$Posterior$Interosseous$Nerve$(PIN)$is$the$nerve$of$the$extensor$compartment$of$the$forearm$$It$passes$into$the$compartment$around$the$neck$of$the$radius$between$the$two$heads$of$$supinator,$where$it$is$vulnerable$to$compression$(Supinator$Tunnel)$
Reaching$the$deepest$plane$of$the$extensor$compartment,$on$the$posterior$surface$of$the$$interosseous$membrane,$the$PIN$runs$in$the$valley$between$muscle$groups,$supplying$all$muscles$in$$this$compartment.$$The$terminal$fibres,$now$purely$sensory,$run$in$the$floor$of$Compartment$4$on$the$$back$of$the$wrist$and$supply$the$wrist$joint$and$carpus,$with$proprioception.$


The Arcade of Frohse also The Supinator arch
Fritz$Frohse:$Anatomist$1871$<$1916$
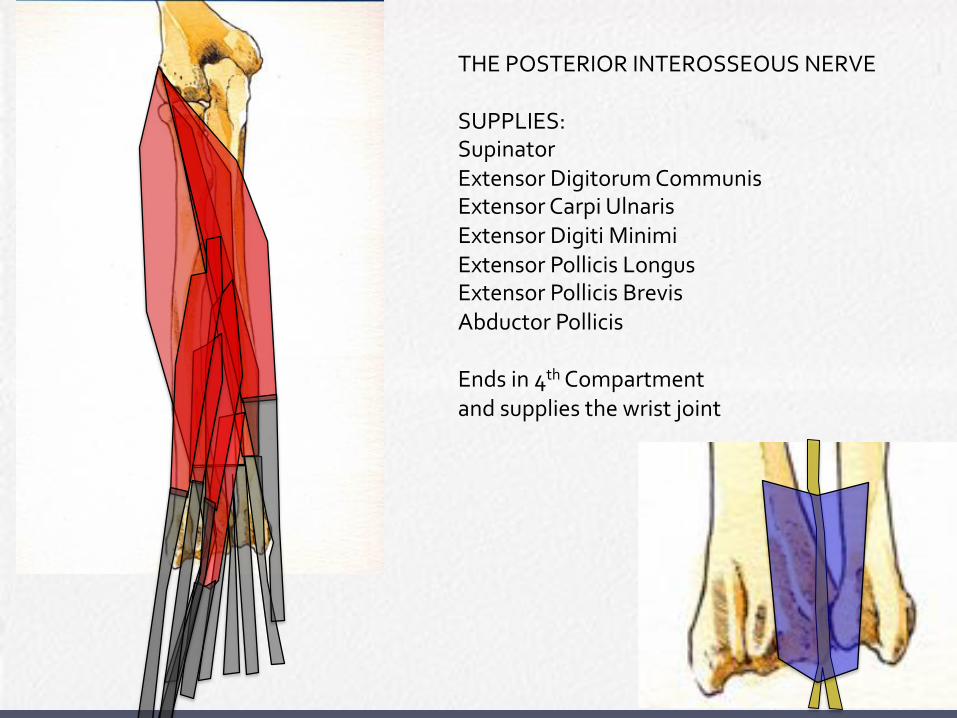
THE$POSTERIOR$INTEROSSEOUS$NERVE$$SUPPLIES:$Supinator$Extensor$Digitorum$Communis$Extensor$Carpi$Ulnaris$Extensor$Digiti$Minimi$Extensor$Pollicis$Longus$Extensor$Pollicis$Brevis$Abductor$Pollicis$$Ends$in$4th$Compartment$$and$supplies$the$wrist$joint$

The$Median$Nerve$$

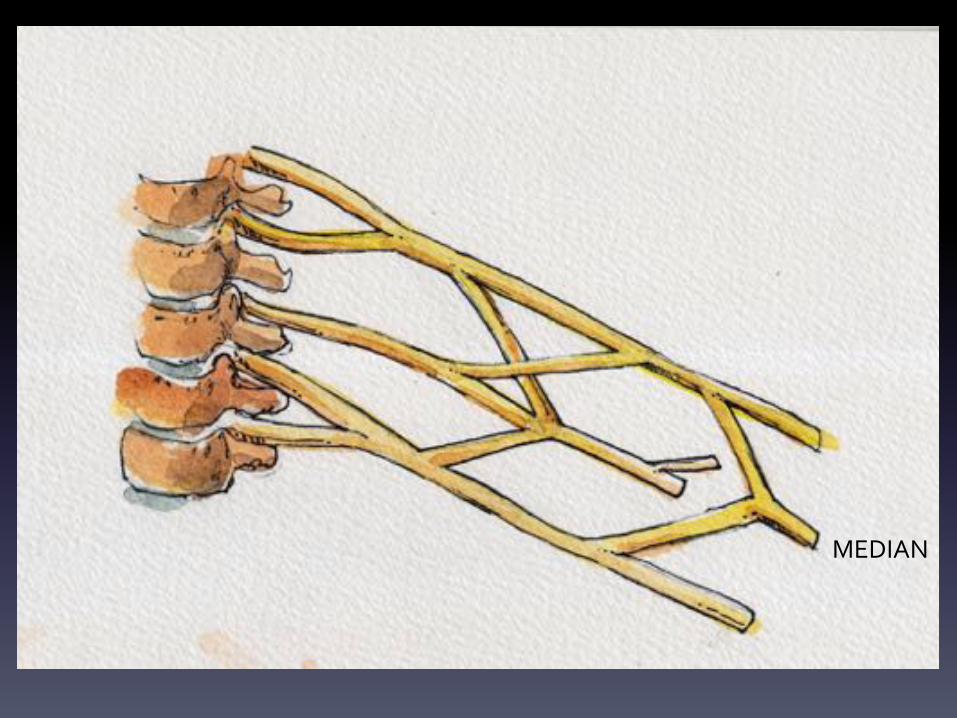
The$Median$Nerve$is$the$main$nerve$of$the$flexor$compartment$of$the$forearm.$$$It$supplies$virtually$all$muscles$in$this$compartment$$(The$Ulnar$nerve$supplies$FCU$and$half$of$FDP)$$It$is$formed$by$contribution$of$Lateral$and$Medial$cords$in$the$Brachial$Plexus.$$It$leaves$the$axilla$over$the$tendon$of$Latissimus$dorsi$and$runs$on$the$medial$aspect$of$the$arm,$along$biceps$brachii$and$brachialis.$It$gives$no$branches$in$the$arm.$$$
MEDIAN$
$$
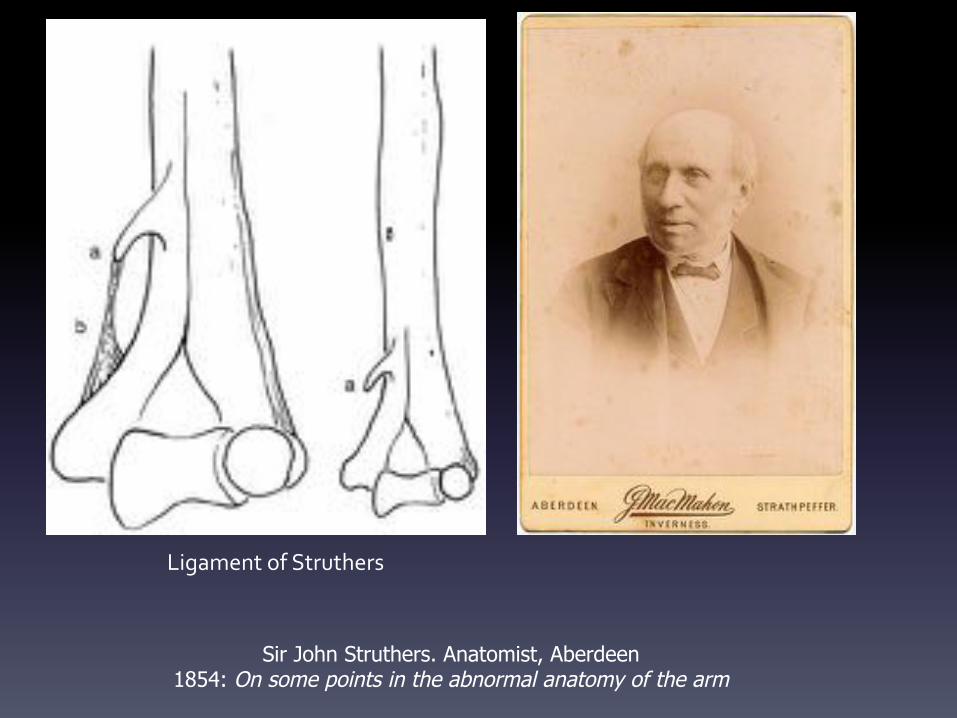
Sir John Struthers. Anatomist, Aberdeen 1854: On some points in the abnormal anatomy of the arm
Ligament$of$Struthers$
Struthers$(1854)$described$a$supracondylar$spur$and$ligament$(Ligament$of$Struthers)$$on$the$medial$border$of$the$distal$humerus.$When$this$is$present,$the$median$nerve$and$the$brachial$artery$pass$beneath$it$and$may$$be$compressed.$$This$vestigial$structure$is$consistently$present$in$some$Mammals,$such$as$the$cat$which$has$$a$constant$Endepitrochlear$foramen$through$which$passes$the$nerve.$It$is$not$to$be$$confused$with$the$supratrochlear$forearmen$which$is$an$inconsequential$perforation$of$$bone$above$the$humeral$trochlea.$$Darwin$cited$the$presence$of$the$ligament$of$Struthers$as$further$proof$of$the$evolution$of$$Man$from$lower$mammals.$


Other Mammals/ Marsupials Endepitrochlear foramen Supratrochlear foramen
Darwin$
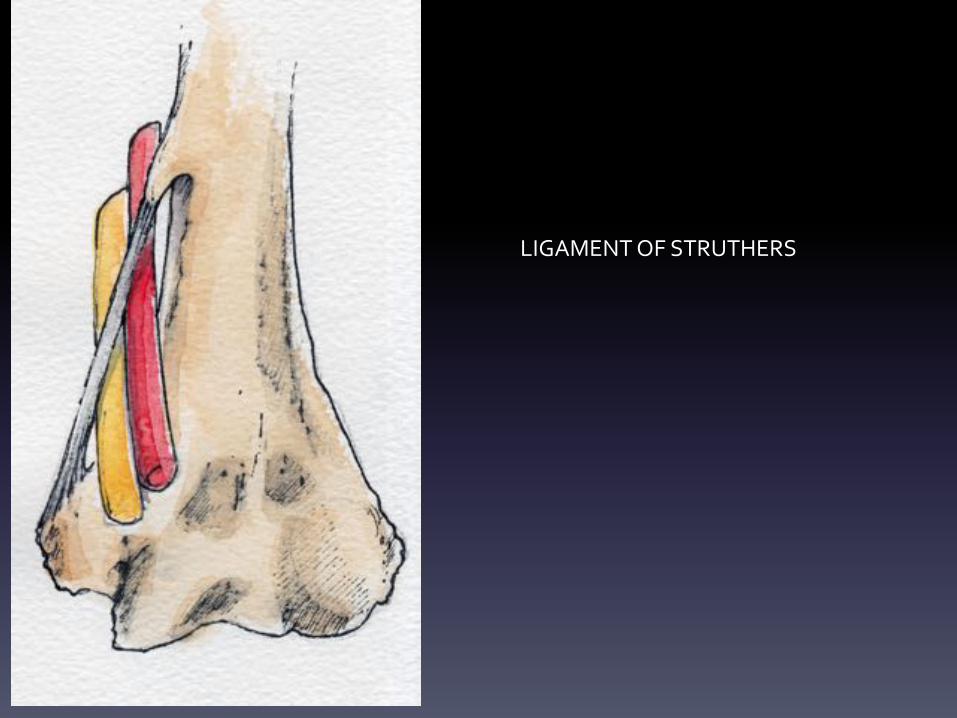
LIGAMENT$OF$STRUTHERS$
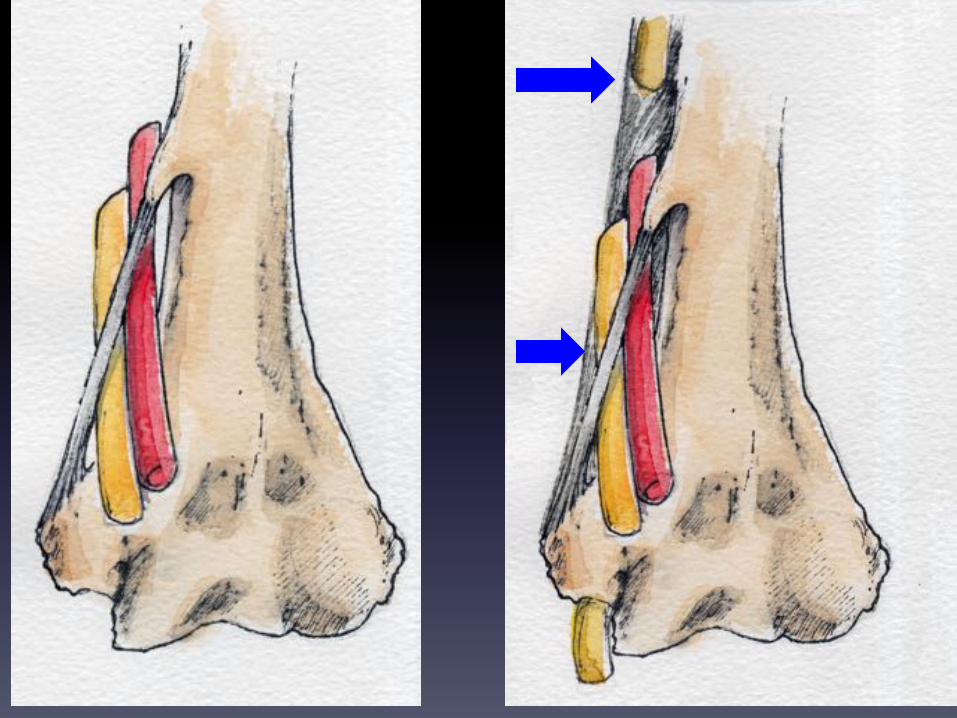
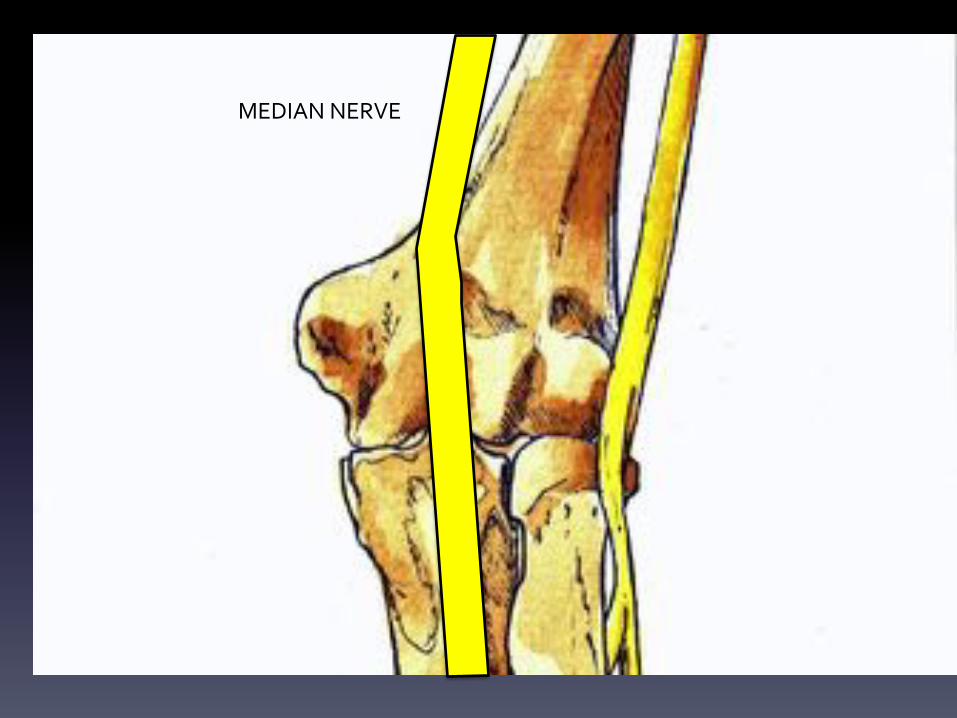
MEDIAN$NERVE$

The$median$nerve$runs$down$the$centre$of$the$cubital$fossa$lying$medial$to$$the$Brachial$artery$
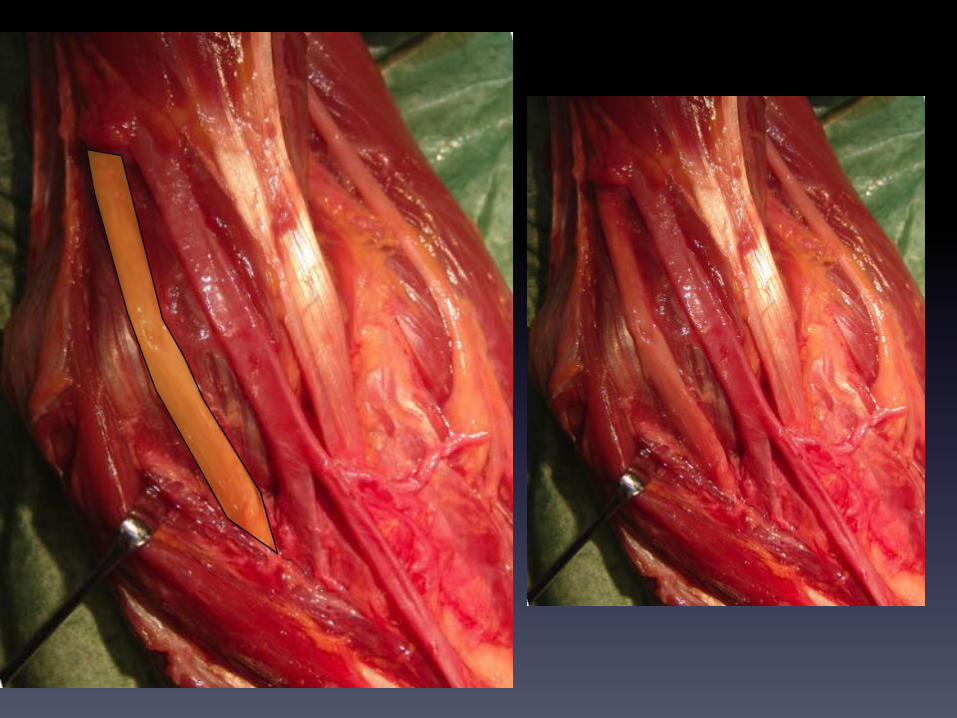
It$passes$deep$to$the$bicipital$aponeurosis,$which$is$another$point$of$possible$compression$

L

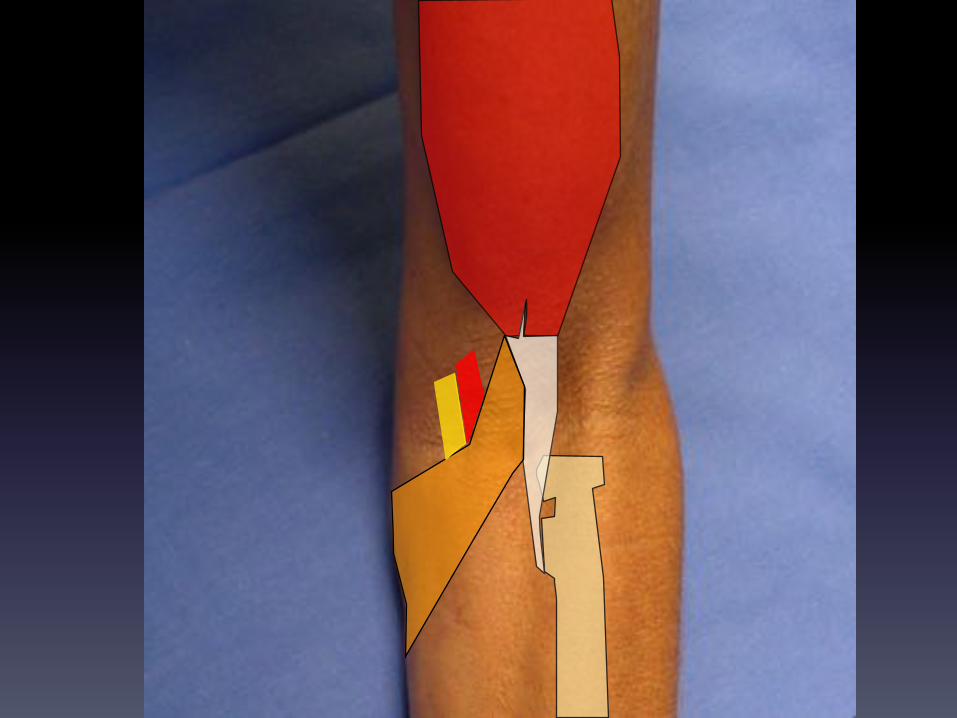
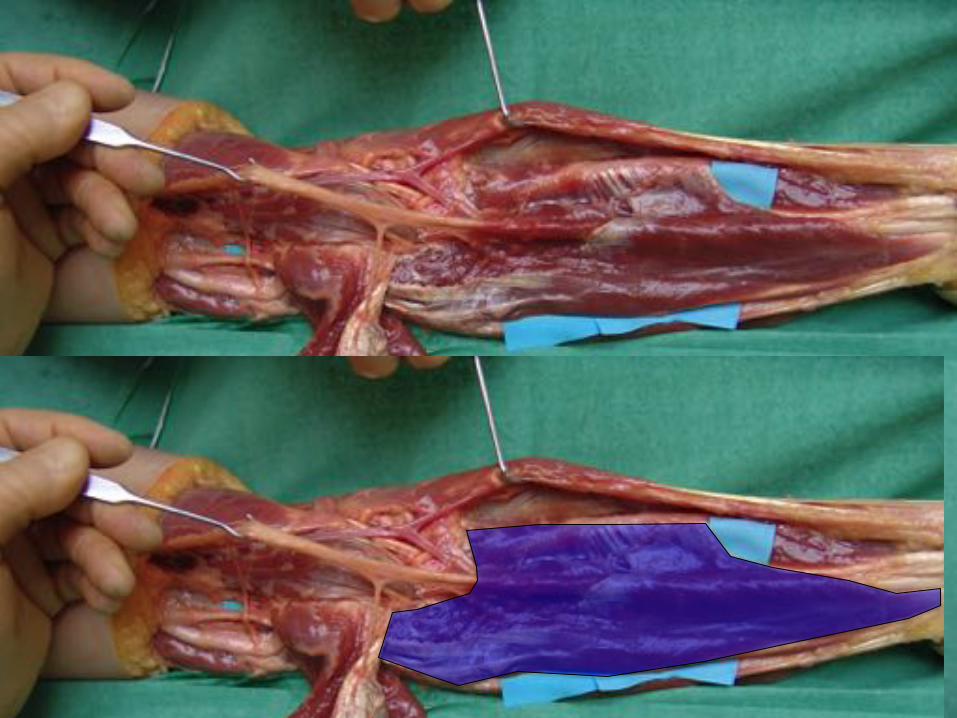
The$median$nerve$enters$the$forearm$by$passing$between$the$two$heads$of$the$$Pronator$Teres,$supplying$it$before$it$pierces$the$muscle.$

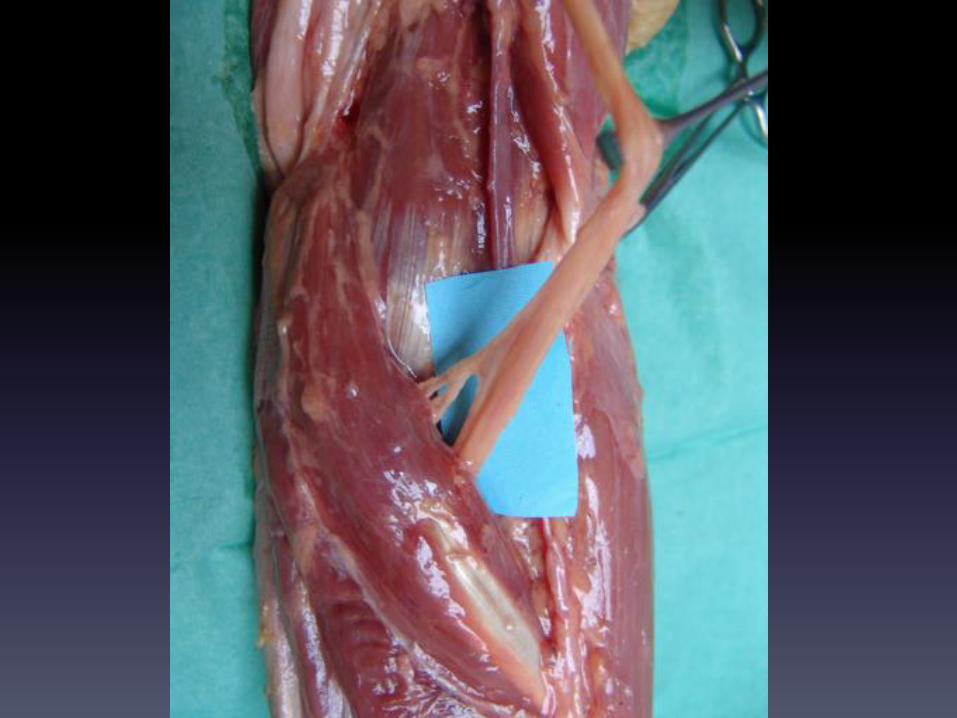
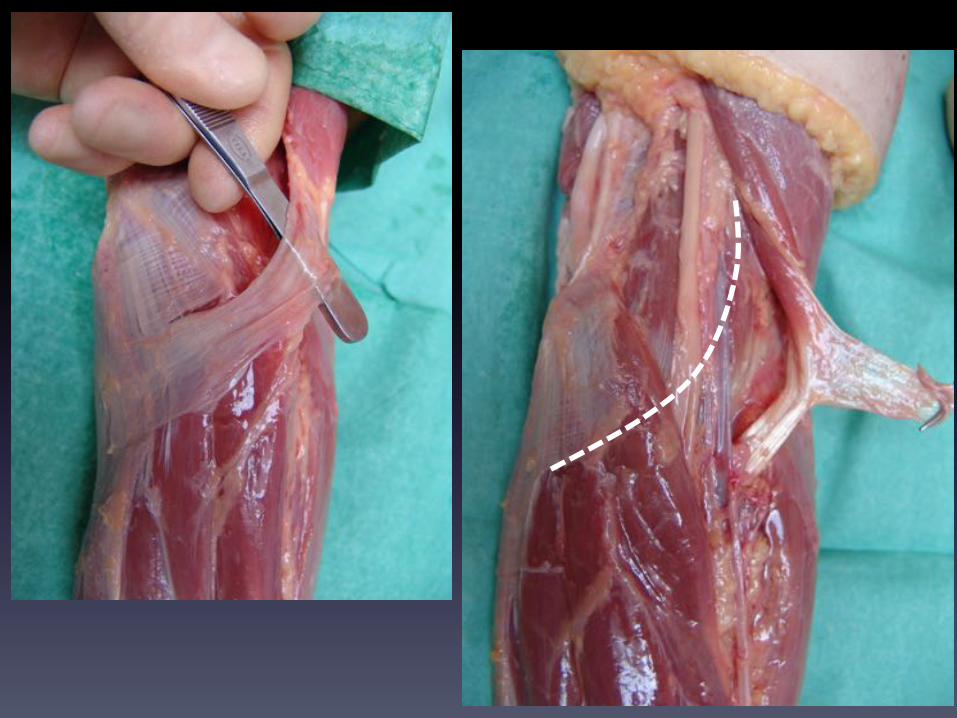
It$passes$deep,$beneath$the$arch$of$the$two$origins$of$Flexor$Digitorum$superficialis.$$At$this$point,$before,$or$after$the$arch,$it$gives$off$its$deep$branch,$$the$Anterior$Interosseous$Nerve.$$$The$main$trunk$of$the$nerve$courses$distally,$closely$attached$to$the$deep$surface$of$the$$FDS,$to$emerge$in$the$distal$forearm$between$the$tendons$of$Flexor$Carpi$Radialis$and$the$Palmaris$Longus.$$$It$leaves$the$forearm$by$passing$through$the$carpal$tunnel$$into$the$hand.$$



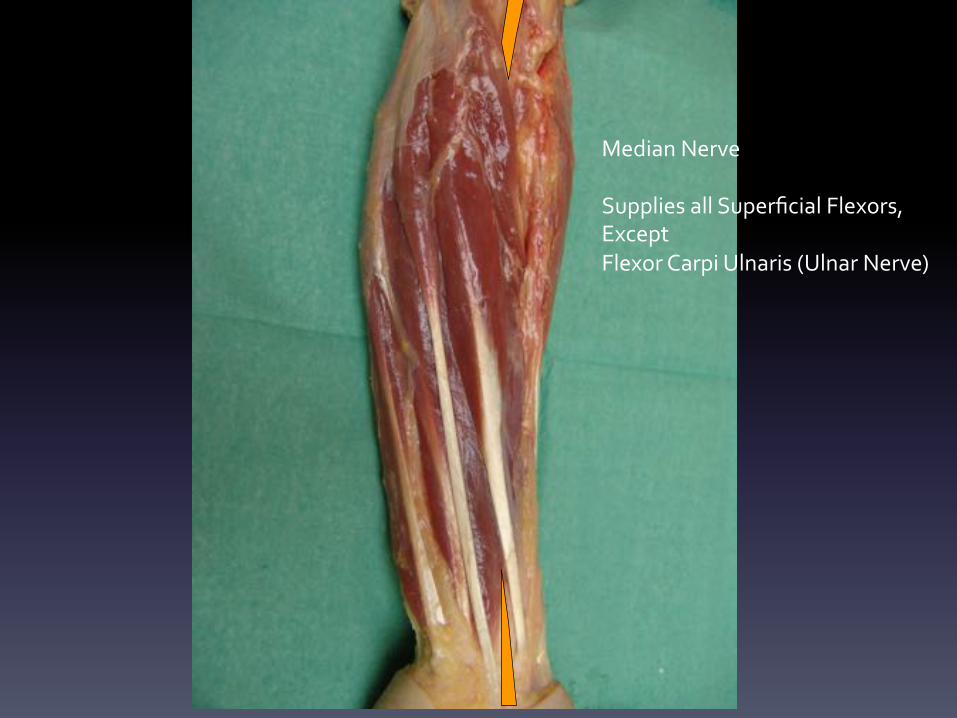
Median$Nerve$$Supplies$all$Superficial$Flexors,$$Except$Flexor$Carpi$Ulnaris$(Ulnar$Nerve)$

The$main$trunk$of$the$median$nerve$supplies$the$superficial$flexors,$except$for$FCU.$$The$Anterior$interosseous$nerve$runs$deep$in$the$forearm,$in$the$valley$between$$Flexor$Digitorum$Profundus$and$Flexor$Pollicis$longus$,$directly$on$the$$Interosseous$membrane.$It$supplies$FPL$and$Half$of$FDP$(see$below)$and$ends$by$supplying$$Pronator$Quadratus$$The$Median$nerve,$directly$or$through$the$Anterior$Interosseous,$supplies$all$the$$flexor$muscles$except:$$1. The$Flexor$Carpi$Ulnaris$(Ulnar$Nerve)$2. The$Ulnar$half$of$Flexor$Digitorum$Profundus$(Ulnar$Nerve)$$$

Anterior*Interosseous*Nerve*$Supplies $ $Flexor$Pollicis$Longus$
$ $Flexor$Digitorum$Profundus$(shared$with$Ulnar)$$ $Pronator$Quadratus$
The$median$nerve$can$be$compressed:$$In$the$arm$:$by$the$ligament$of$Struthers$$In$the$forearm$at$various$points:$
$The$bicipital$aponeurosis$$The$pronator$teres$$Vascular$leashes$recurrent$around$the$elbow$$The$arch$of$dual$origin$of$FDS$
$$Tenderness$over$the$area$of$Pronator$Teres$and$pain$0n$resisted$pronation$are$$corroborative$signs.$Involvement$of$the$Anterior$interosseous$(e.g.$beneath$the$arch$of$FDS)$may$lead$to$$weakness$of$Flexor$Pollicis$Longus,$tested$by$resisted$flexion$of$the$Thumb$IP$Joint$or$by$$inviting$the$patient$to$make$a$strong$‘O’$sign$with$thumb$and$index$finger.$$Weakness$of$either$causes$collapse$of$this$‘O’$



TESTING$FOR$FPL$
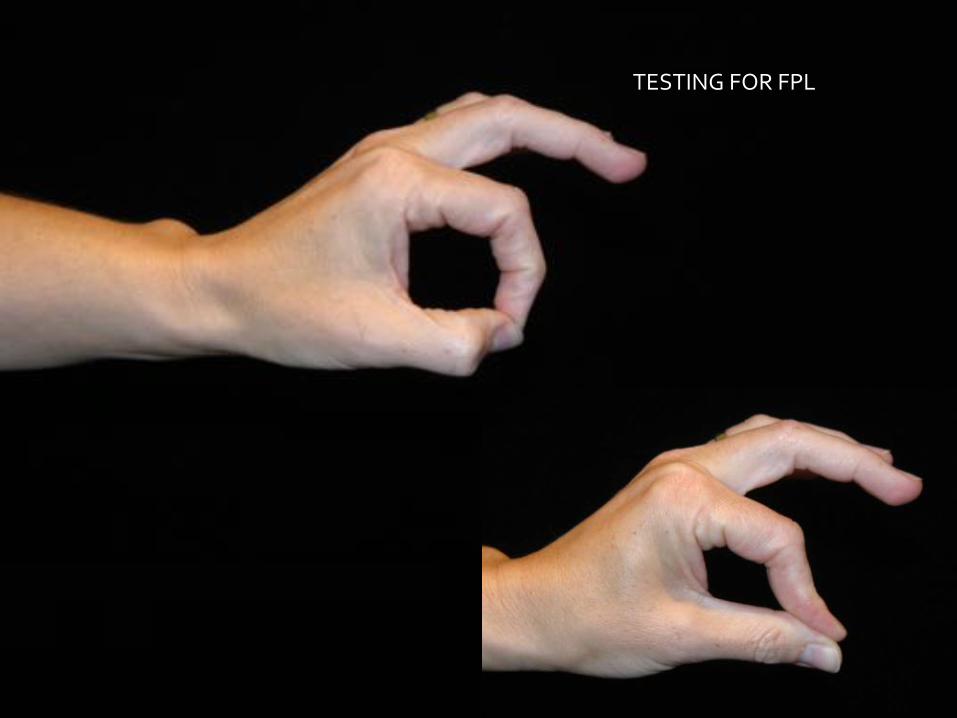
TESTING$FOR$FPL$
Carpal Tunnel syndrome

Carpal$tunnel$syndrome$includes$a$group$of$clinical$signs$secondary$to$compression$of$the$$median$nerve$in$the$carpal$tunnel.$$These$include:$$Paraesthesiae$(pins$and$needles)$in$the$median$$nerve$cutaneous$distribution$in$the$hand,$$Loss$of$sensation$in$$the$median$nerve$distribution$in$the$hand$Weakness$in$the$thenar$muscles$both$actual$(muscle$wasting)$and$perceived$$(altered$proprioception)$Loss$of$muscle$bulk$in$the$Thenar$muscles$especially$$Abductor$Pollicis$Brevis,$$supplied$exclusively$by$the$median$nerve$Pain$All$symptoms$increased$by$flexion$of$the$wrist$and$hence$worse$at$night$


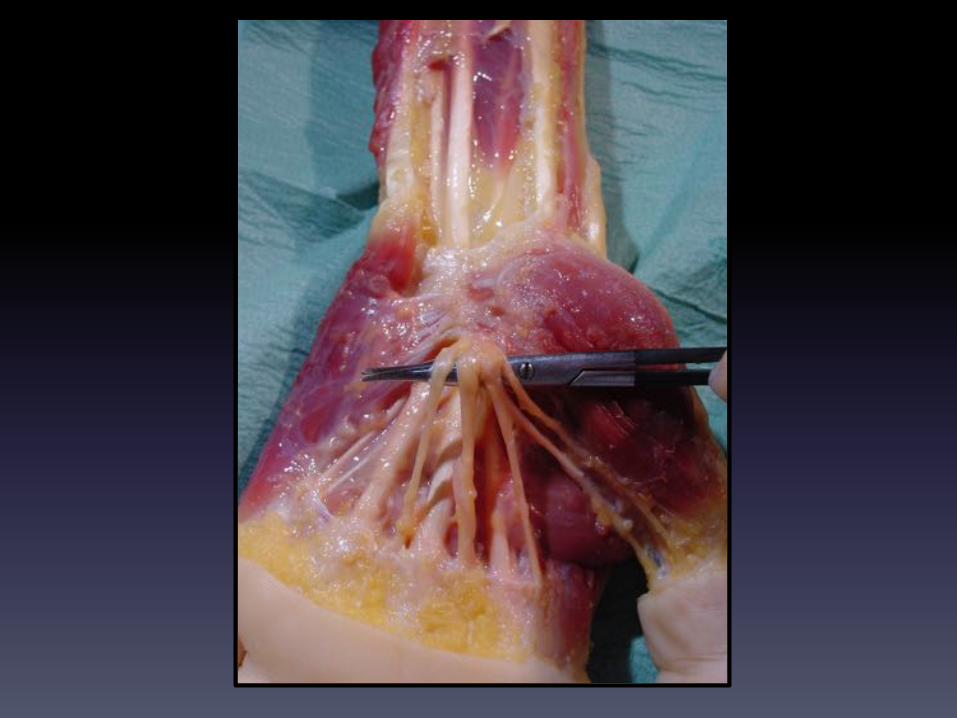

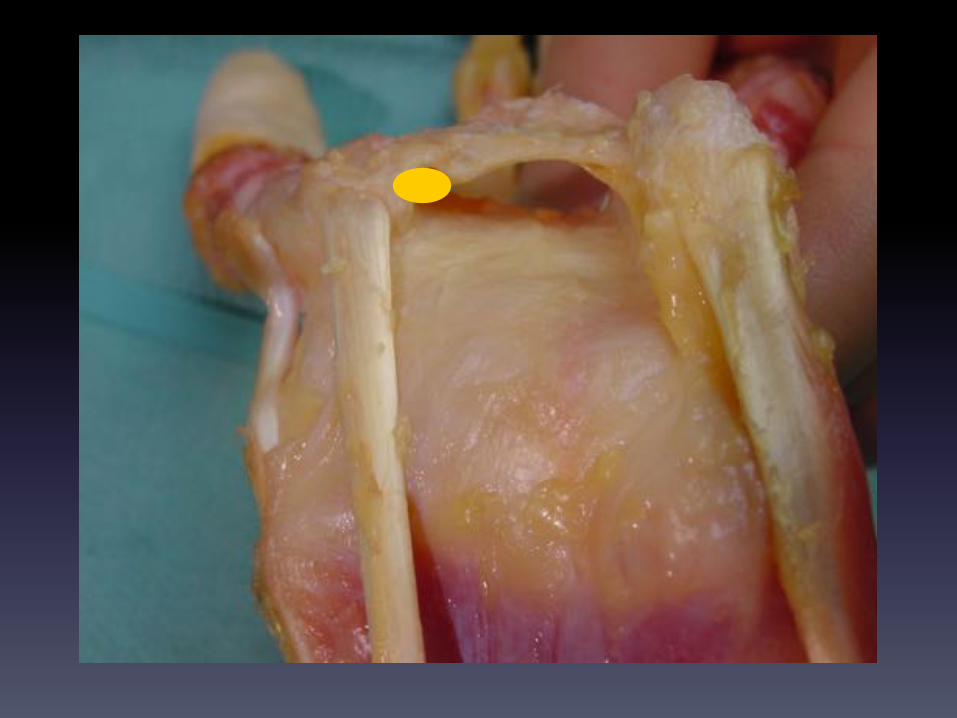

Thickening$of$the$synovium$surrounding$the$flexor$tendons$is$a$consistent$finding$$in$surgery$for$Carpal$tunnel$release,$but$the$cause$of$compression$is$usually$unknown.$$Synovial$thickening$may$be$a$consequence$rather$than$a$cause.$$
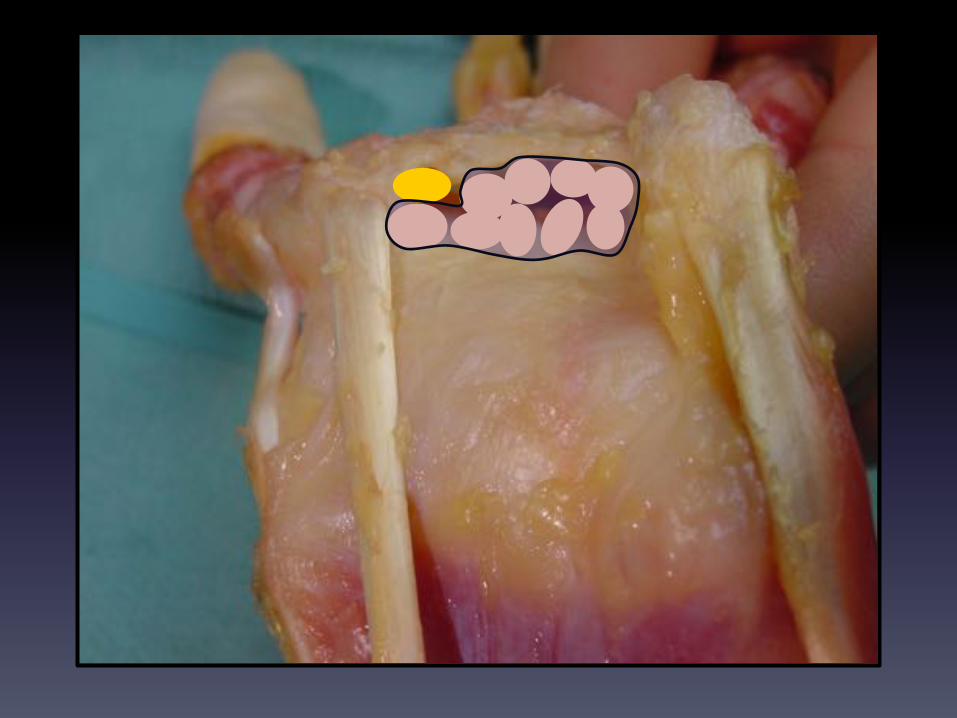

M
U
R
U

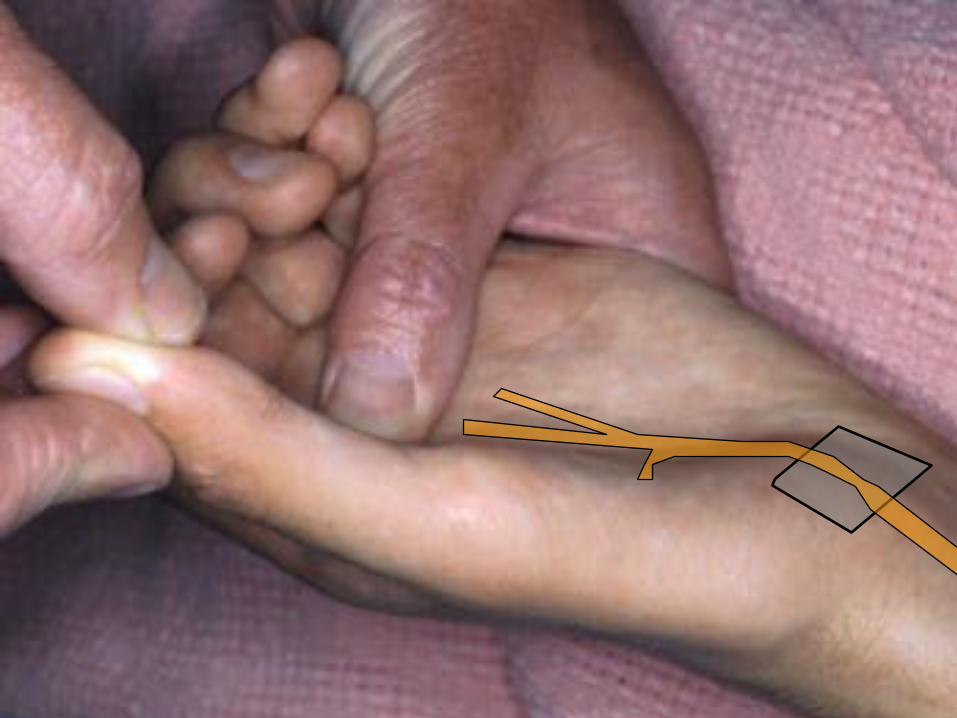
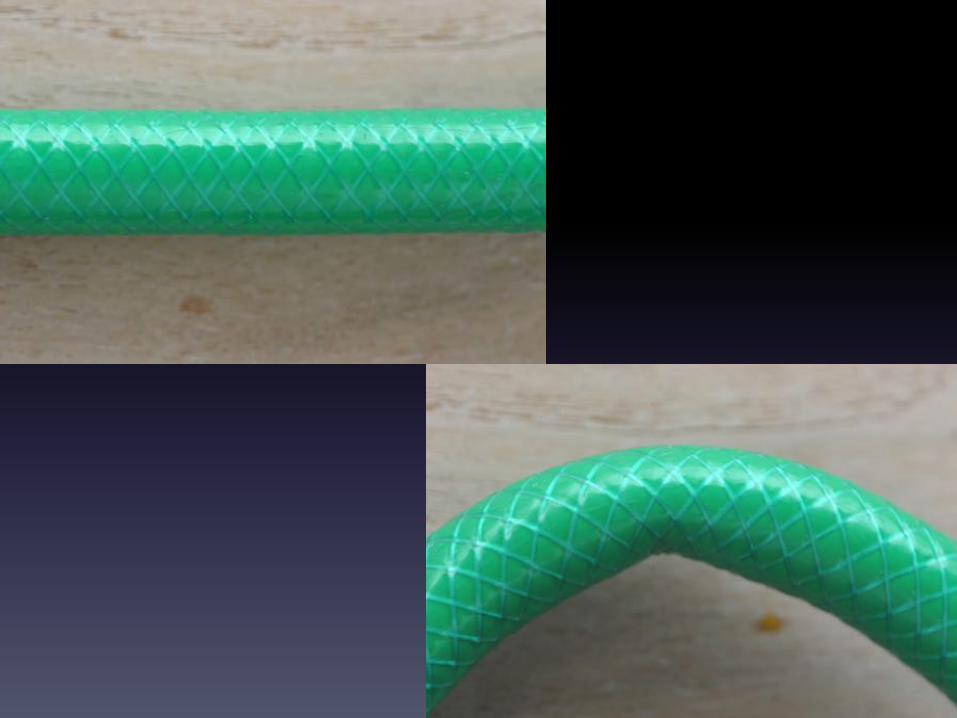
Diagnosis$depends$on$testing$all$modalities$of$the$median$nerve$beyond$the$wrist$–$$sensation,$sweating,$power$of$APB.$$The$Phalen$test$involves$allowing$the$wrist$to$fall$freely$into$flexion.$This$tends$to$kink$and$$compress$the$carpal$tunnel$and$provoke$symptoms$within$one$minute.$$
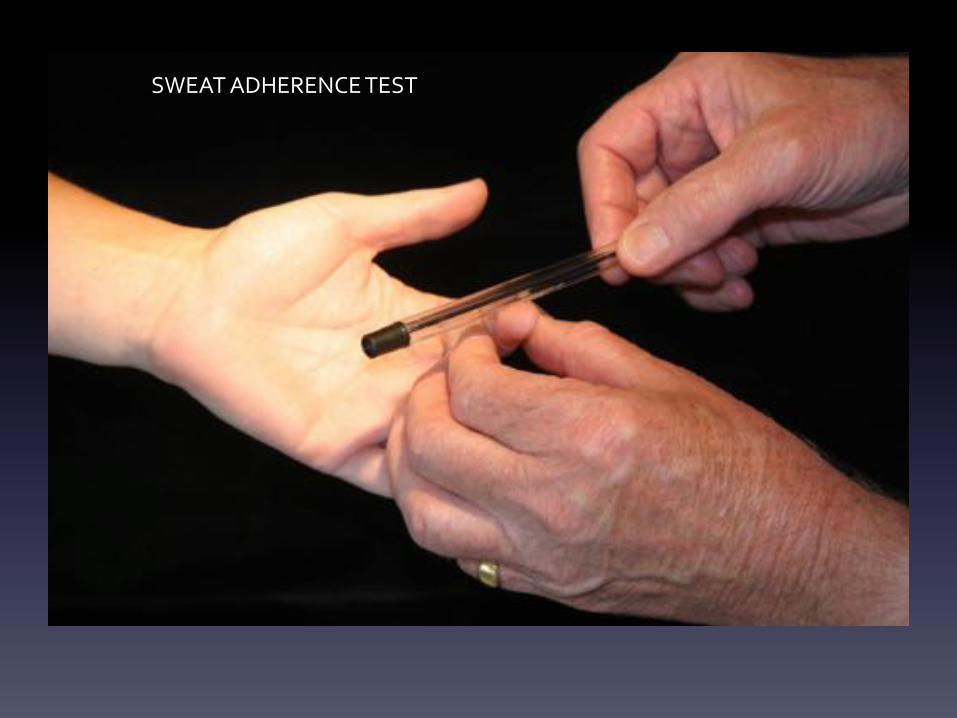
SWEAT$ADHERENCE$TEST$

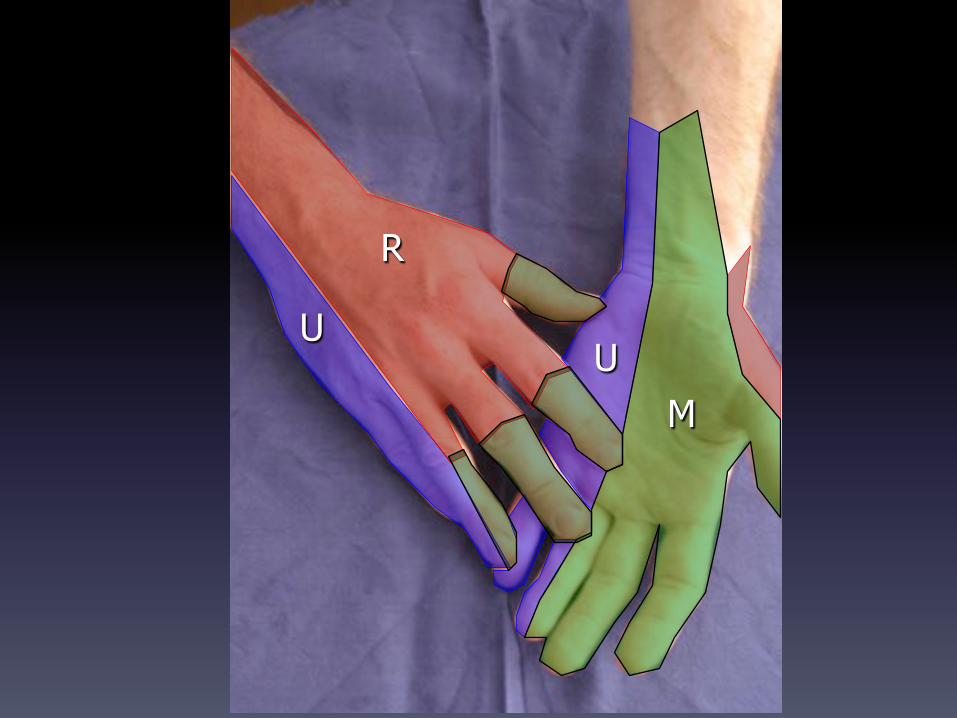
M
U
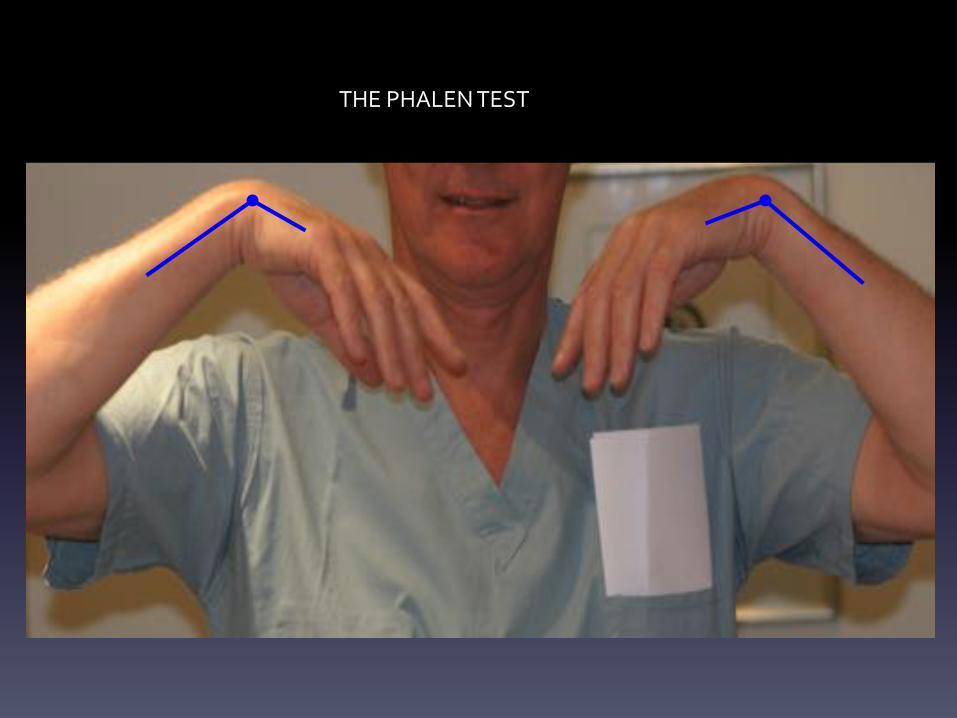
THE$PHALEN$TEST$
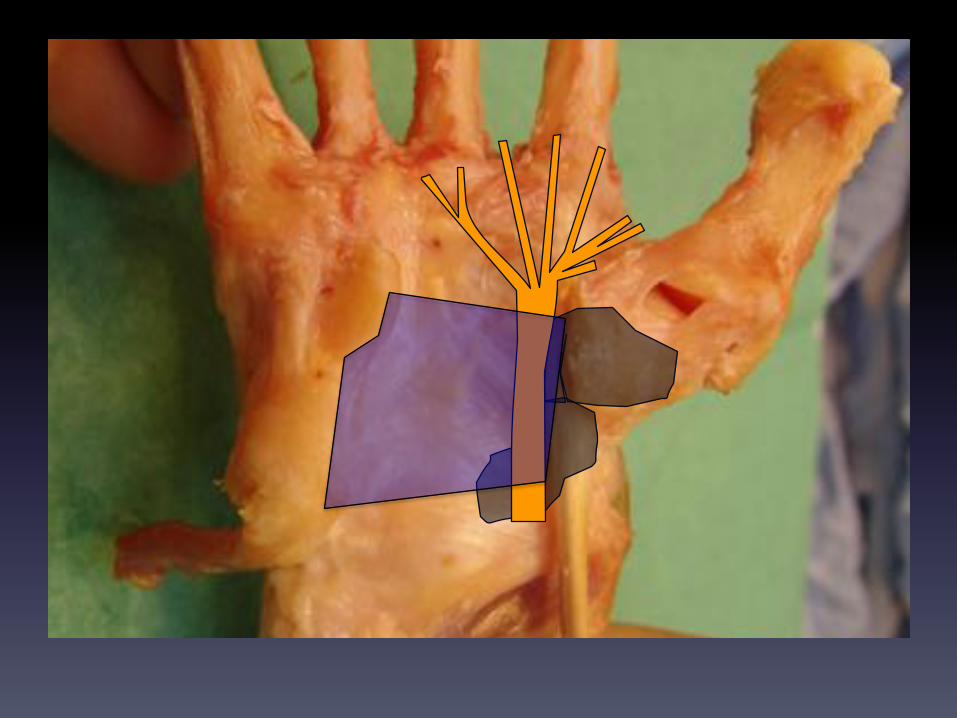
The$carpal$tunnel$can$also$be$compressed$by$(common)$osteoarthritis$of$the$basal$joint$of$the$thumb,$$since$the$Trapezium$also$forms$one$of$the$walls$of$the$carpal$tunnel$$
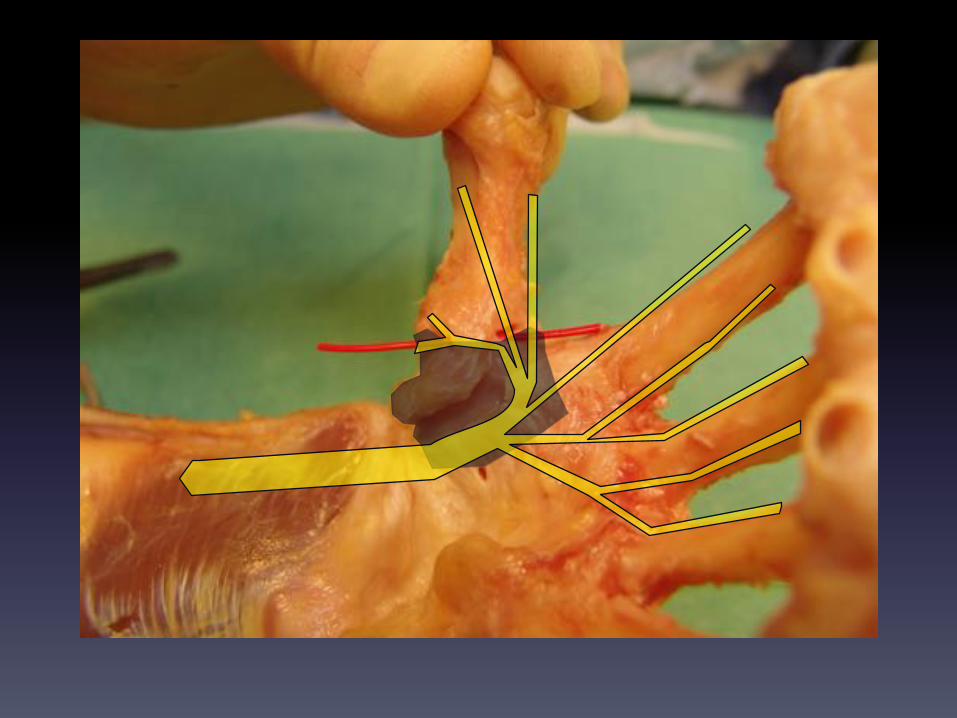

In$the$hand,$The$median$Nerve$usually$divides$into$its$terminal$branches$at$the$distal$end$$of$the$flexor$retinaculum$(there$are$uncommon$variations*).$$These$are:$$1. The$recurrent$motor$branch$to$the$thenar$muscles:$This$curls$back$and$sinks$into$the$thenar$muscles$supplying$Abductor$Pollicis$brevis$(exclusively)$and$sharing$supply$of$$Flexor$Pollicis$Brevis$and$Opponens$pollicis$with$the$ulnar$nerve.$$2.$The$Motor$branches$to$the$radial$lumbrical$i.e.$those$to$the$index$and$middle$$3.$Cutaneous$sensory$supply$to$the$radial$3$½$digits$i.e.$thumb,$index,$middle$and$half$the$ring$$$*Uncommon(variations(include(high(division(of(the(median(nerve,(a(bifid(median(nerve,(
high(branching(of(the(recurrent(motor(branch,(course(of(the(motor(branch(through(the((flexor(retinaculum,(bifid/double(motor(branch.(
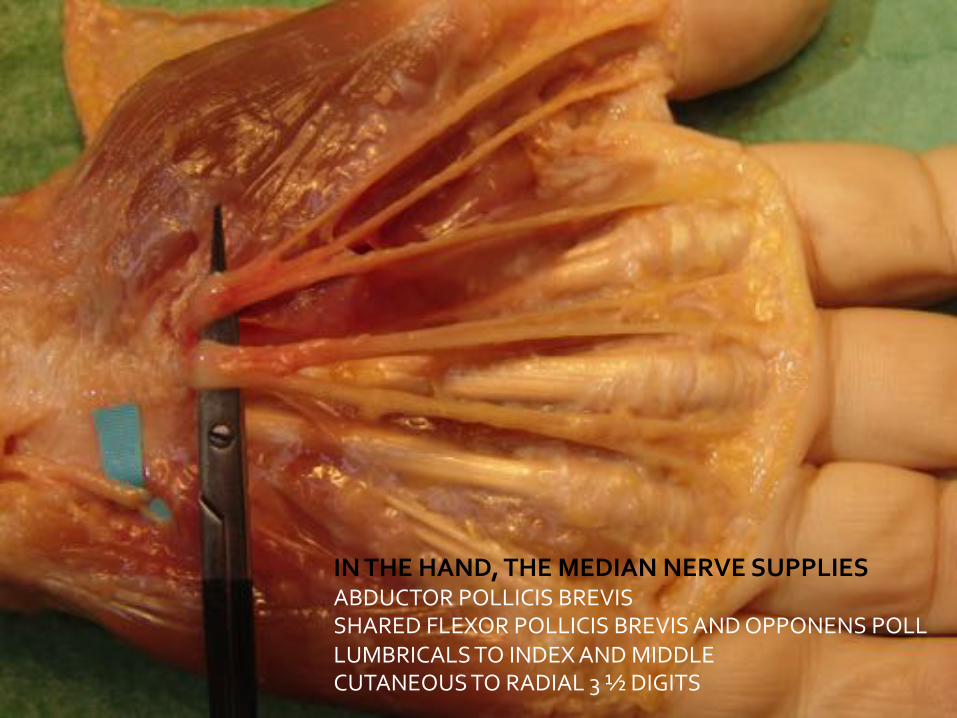
IN*THE*HAND,*THE*MEDIAN*NERVE*SUPPLIES*ABDUCTOR$POLLICIS$BREVIS$SHARED$FLEXOR$POLLICIS$BREVIS$AND$OPPONENS$POLL$LUMBRICALS$TO$INDEX$AND$MIDDLE$CUTANEOUS$TO$RADIAL$3$½$DIGITS$
The$Ulnar$Nerve$

The$ulnar$nerve$is$primarily$the$nerve$of$the$Intrinsic$muscles$in$the$hand.$$It$leaves$the$brachial$plexus$as$a$terminal$branch$of$the$medial$cord$of$the$Brachial$Plexus.$$It$gives$no$branches$in$the$arm.$$Halfway$down$the$medial$aspect$of$the$arm,$it$pierces$the$medial$intermuscular$septum$$from$flexor$into$extensor$compartment.$$It$runs$in$the$extensor$compartment$down$to$the$elbow,$lying$on$the$posterior$aspect$$of$the$medial$intermuscular$septum.$$

ULNAR$
$$

The$Ulnar$Nerve$Pierces$The$Medial$Intermuscular$Septum$$From$Flexor$into$$Extensor$Compartment$

2cm$proximal$to$medial$epicondyle$of$humerus$
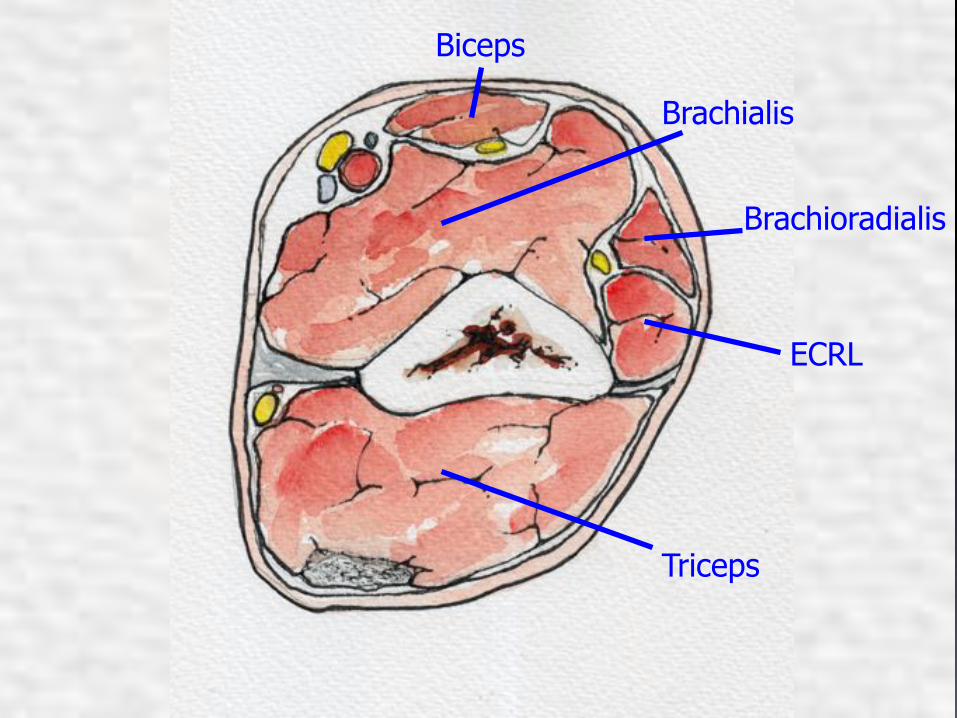
Biceps
Brachialis
Brachioradialis
ECRL
Triceps
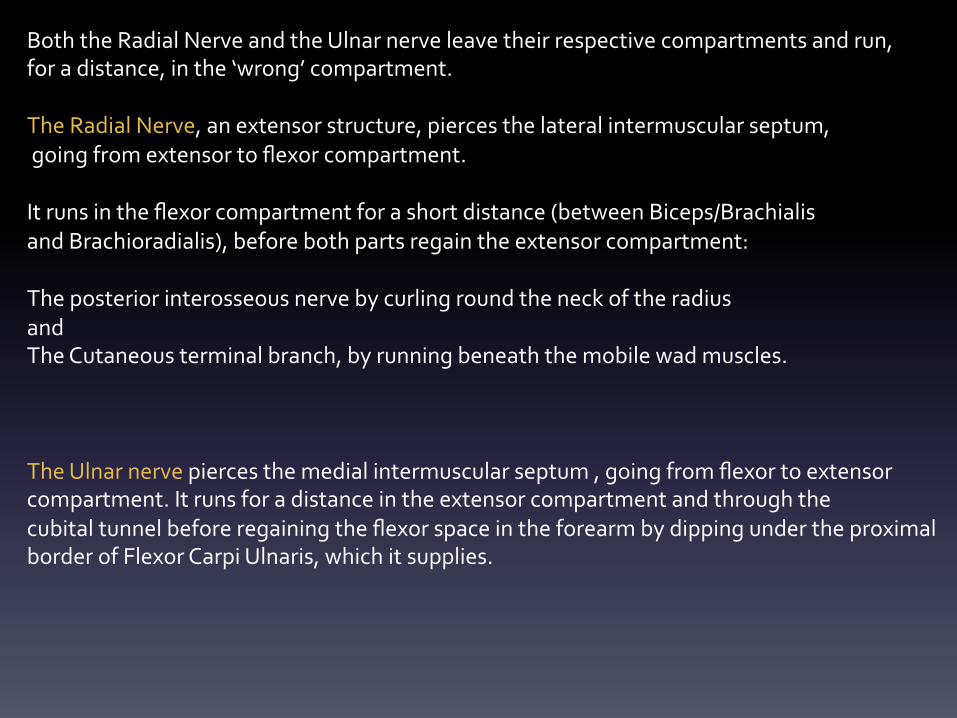
Both$the$Radial$Nerve$and$the$Ulnar$nerve$leave$their$respective$compartments$and$run,$$for$a$distance,$in$the$‘wrong’$compartment.$$The$Radial$Nerve,$an$extensor$structure,$pierces$the$lateral$intermuscular$septum,$$going$from$extensor$to$flexor$compartment.$$It$runs$in$the$flexor$compartment$for$a$short$distance$(between$Biceps/Brachialis$$and$Brachioradialis),$before$both$parts$regain$the$extensor$compartment:$$The$posterior$interosseous$nerve$by$curling$round$the$neck$of$the$radius$and$$The$Cutaneous$terminal$branch,$by$running$beneath$the$mobile$wad$muscles.$$$$The$Ulnar$nerve$pierces$the$medial$intermuscular$septum$,$going$from$flexor$to$extensor$$compartment.$It$runs$for$a$distance$in$the$extensor$compartment$and$through$the$$cubital$tunnel$before$regaining$the$flexor$space$in$the$forearm$by$dipping$under$the$proximal$border$of$Flexor$Carpi$Ulnaris,$which$it$supplies.$$$
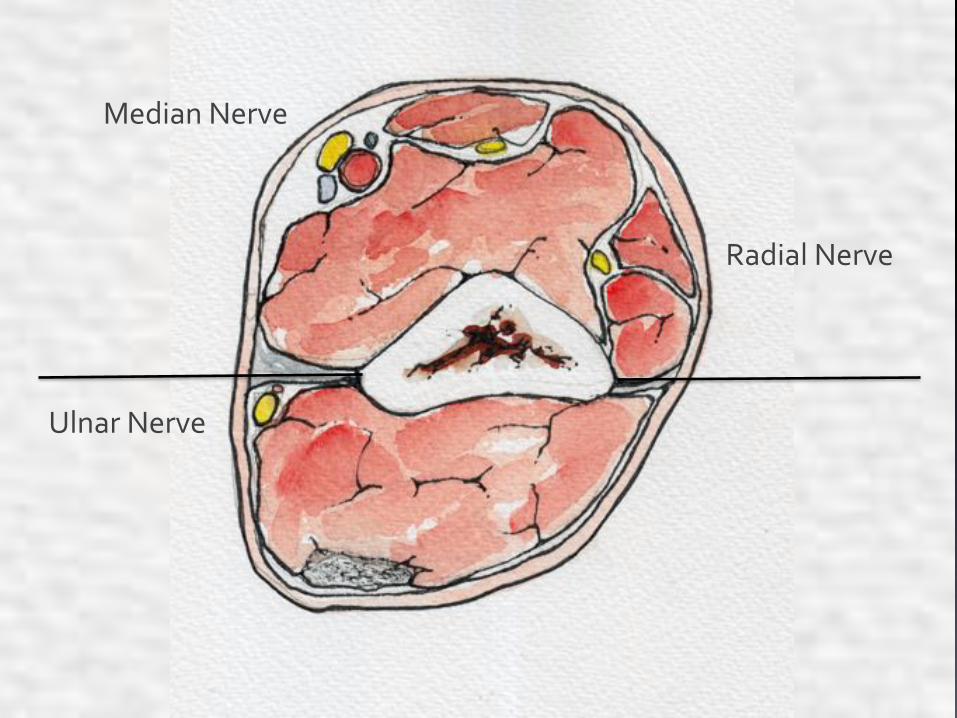
Ulnar$Nerve$
Radial$Nerve$
Median$Nerve$
$$$The$explanation$for$this$peculiar$brief$sojourn$in$the$‘wrong’$compartment$by$radial$and$ulnar$$lies$in$the$migration$of$the$foetal$intermuscular$septum.$$In$the$foetus,$the$radial$nerve$and$the$mobile$wad$lie,$throughout$their$course,$$in$the$extensor$compartment,$while$the$ulnar$nerve$runs,$throughout$its$course,$in$the$flexor$$compartment.$$The$migration$of$the$septum,$imprisons$either$nerve,$for$a$short$distance,$$$in$the$compartment$which$either$is$not$destined$to$supply.$$
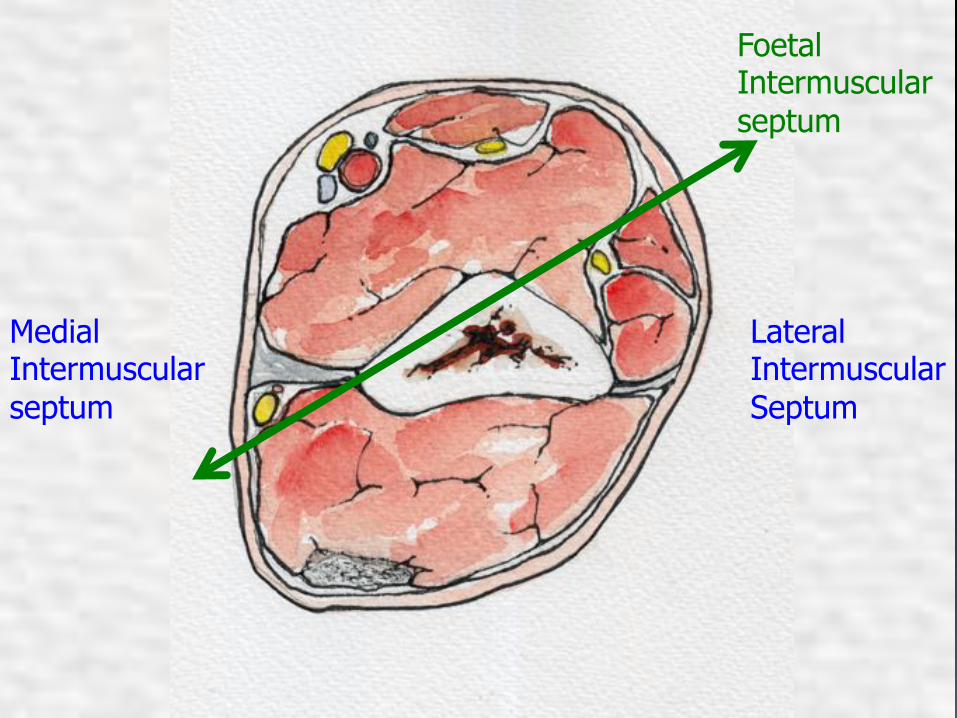
Medial Intermuscular septum
Lateral Intermuscular Septum
Foetal Intermuscular septum

U

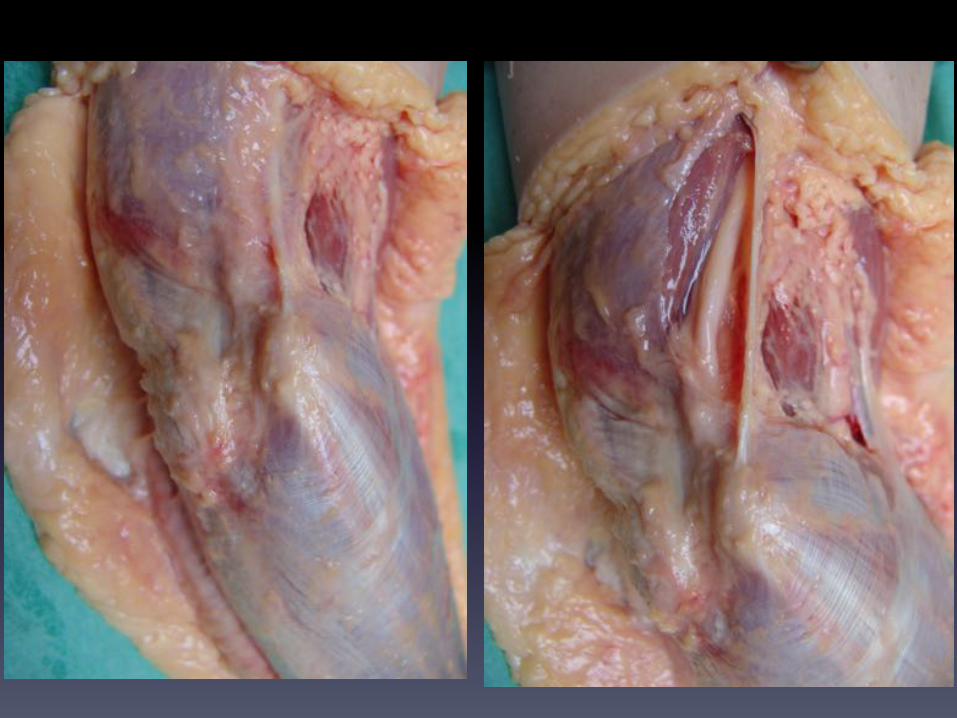
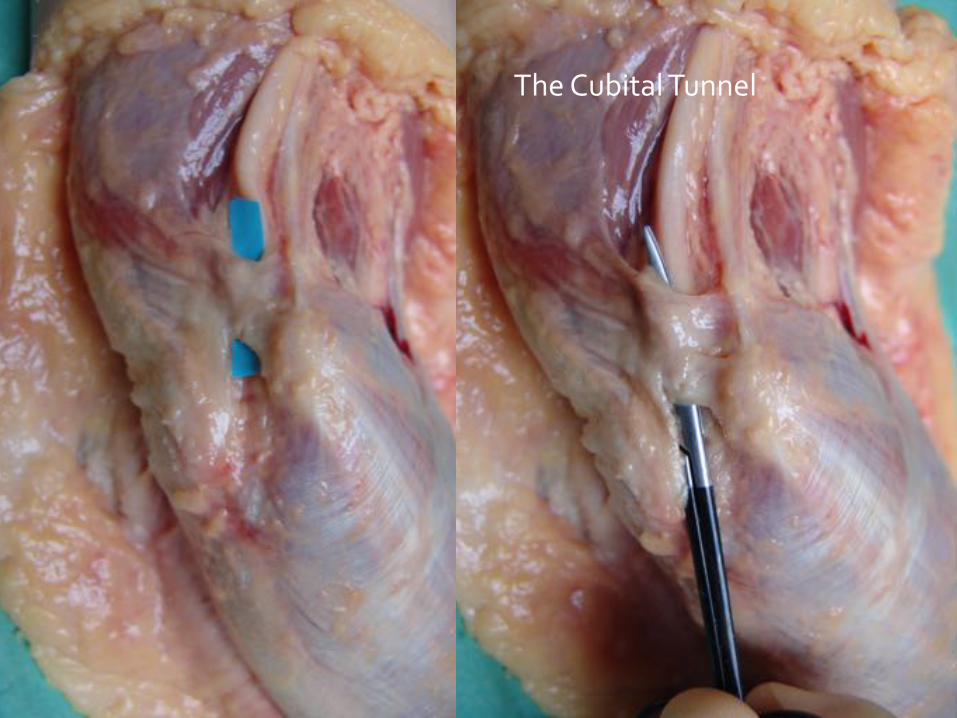
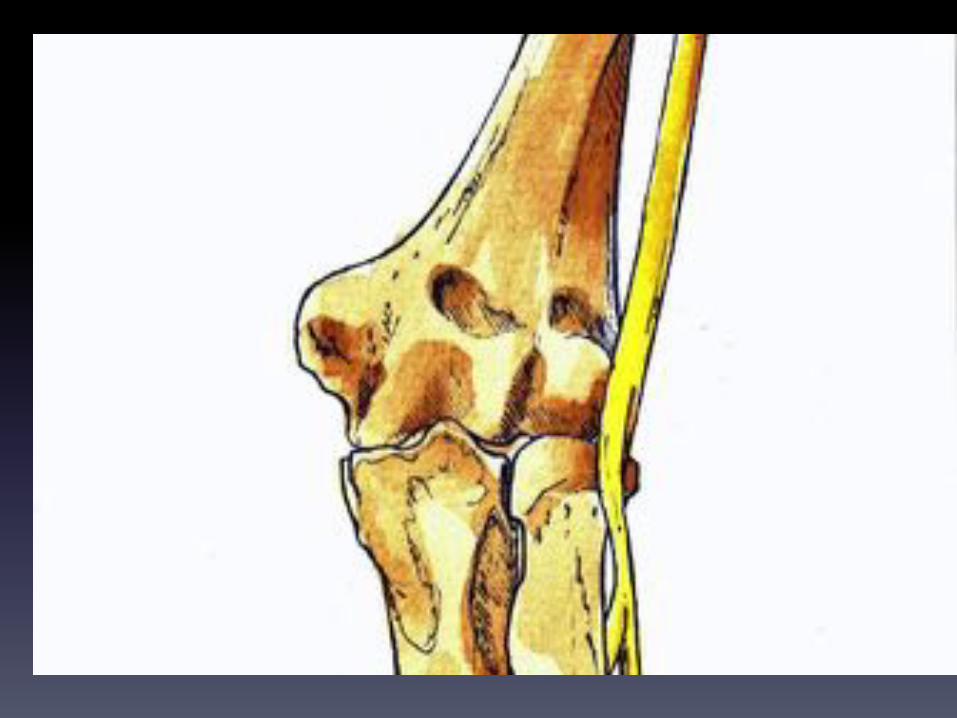
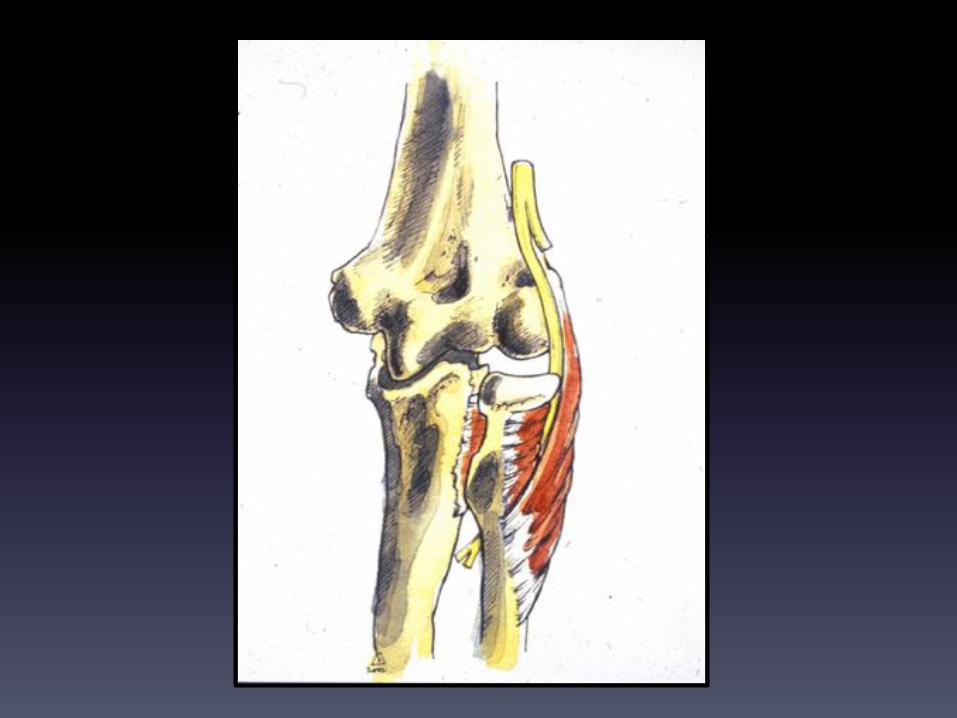
The$Cubital$Tunnel$
Behind$the$medial$epicondyle$it$runs$in$a$fibrous$tunnel$called$the$CUBITAL$TUNNEL$$(‘Cubital’(=(pertaining(to(elbow(or(ulna)$where$it$is$commonly$pathologically$compressed.$$$In$flexion,$the$nerve$describes$a$very$acute$bend$around$the$medial$epicondyle,$which$$causes$minor$trauma$particularly$in$the$presence$of$any$elbow$arthritis.$In$addition,$$the$nerve$is$very$superficial$at$this$point$and$is$vulnerable$to$blunt$trauma.$Tapping$at$this$site$easily$causes$tingling$and$paraesthesiae$$<$the$site$is$commonly$known,$for$this$reason,$as$‘the$funny$bone’.$In$fact$blunt$force$at$this$site$causes$trauma$to$the$nerve.$$The$nerve$then$passes$into$the$forearm$(leaving$the$extensor$compartment)$$by$dipping$beneath$the$two$heads$of$Flexor$Carpi$Ulnaris,$which$it$supplies.$
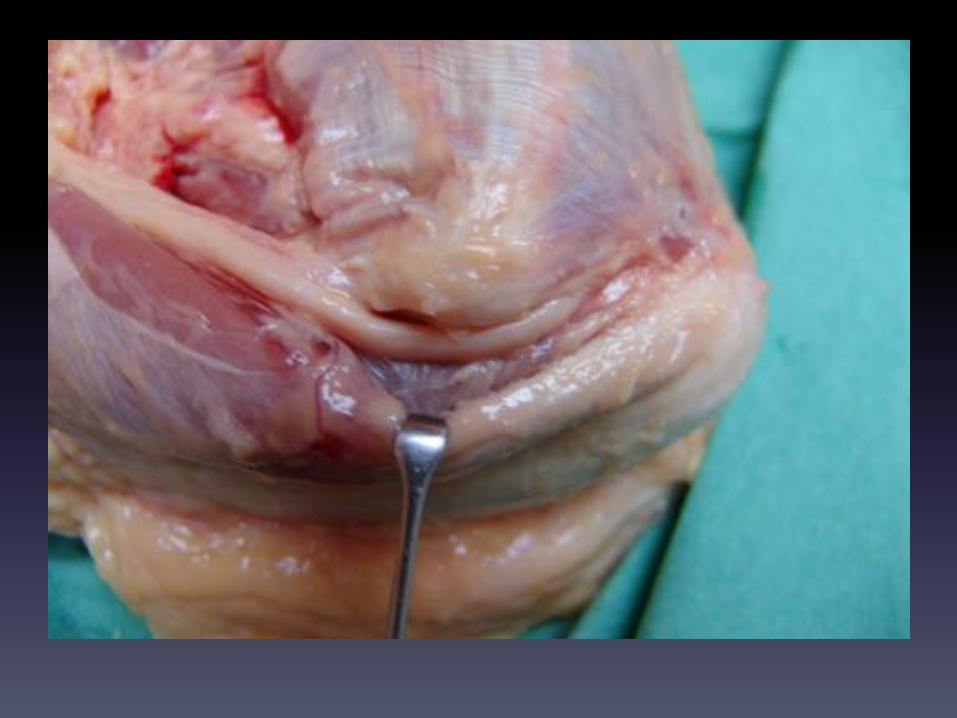
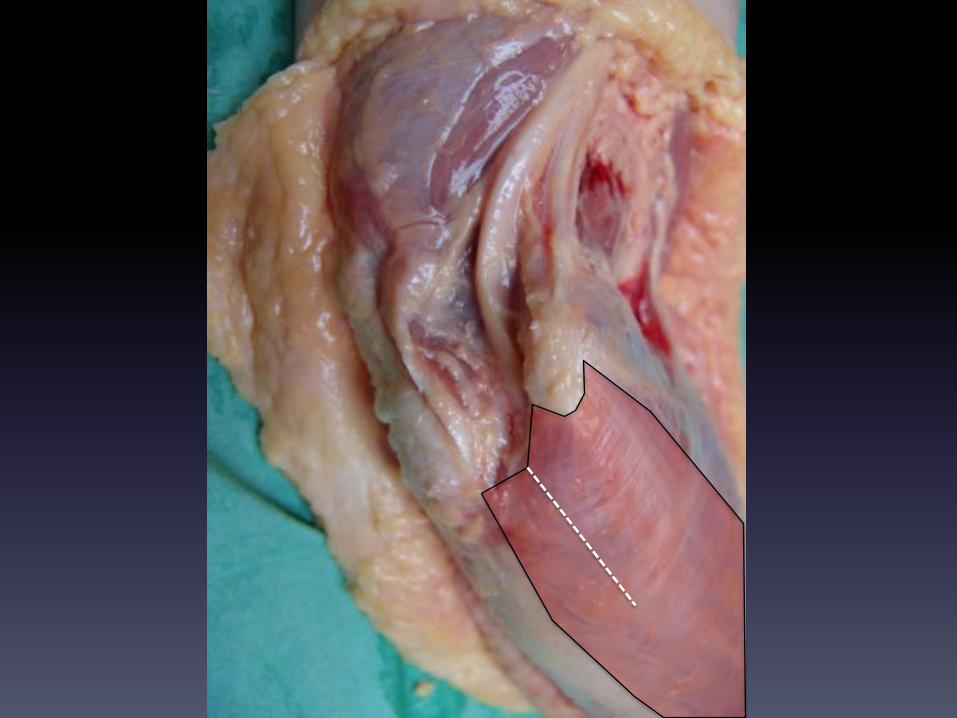


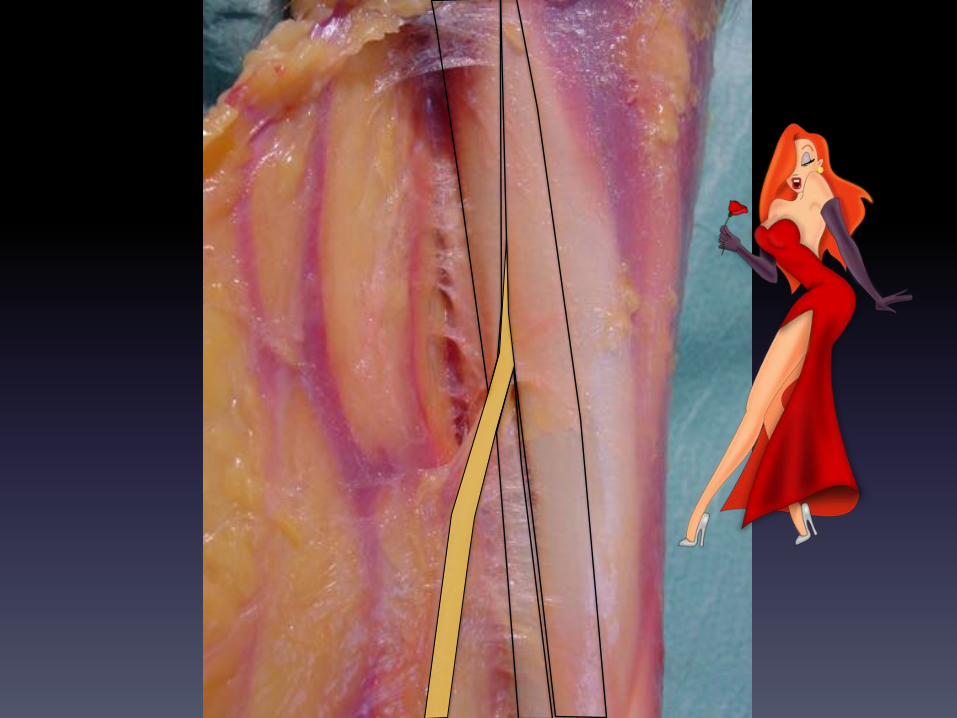
In$the$forearm,$the$ulnar$nerve$runs,$throughout,$under$cover$of$the$Flexor$Carpi$Ulnaris.$$A$handsbreadth$below$the$elbow$it$is$joined,$in$this$plane,$by$the$ulnar$artery$$which$runs$$Radial$to$the$nerve,$never$crossing$it.$$A$handsbreadth$proximal$to$the$wrist,$the$ulnar$nerve$gives$off$the$dorsal$cutaneous$branch$$which$courses$around$the$ulna$and$$supplies$cutaneous$sensation$to$the$ulnar$half$of$the$back$$of$the$hand$(sharing$the$back$of$the$hand$with$the$cutaneous$Radial$nerve).$$Nerve$and$artery$then$become$more$superficial$and$enter$the$hand$through$Guyon’s$canal,$$which$is$floored$by$the$flexor$retinaculum.$Both$nerve$and$artery$are$superficial$at$this$point,$$protected$only$by$skin$and$fat$pad.$$

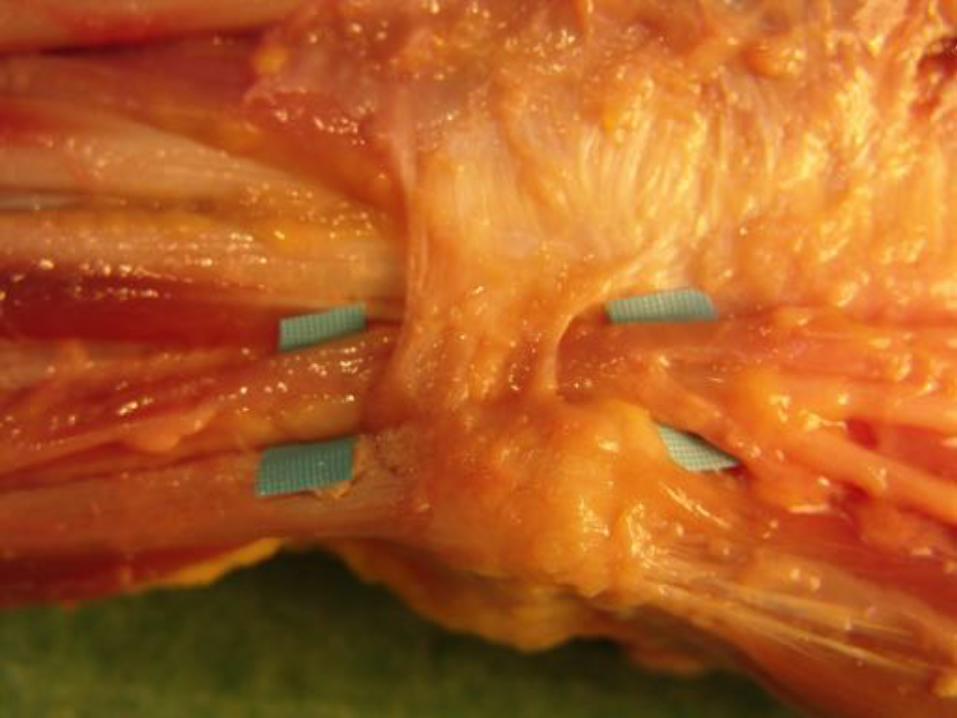
Ulnar$Nerve$$Ulnar$Artery$

GUYON’S$CANAL$

$In,$or$just$distal$to,$Guyon’s$canal,$the$ulnar$nerve$divides$into$its$terminal$branches:$$1. Motor$branch$to$the$hypothenar$muscles$2. Cutaneous$palmar$supply$to$the$little$and$half$the$ring$fingers$3. The$deep$motor$branch$which$supplies$ALL$intrinsics$except:$
1. The$Abductor$pollicis$brevis$(median)$2. The$lumbricals$to$the$index$and$middle$3. Parts$of$Flexor$pollicis$brevis$and$Opponens$pollicis$
(shared$with$median)$

Terminal*Branches*of*Ulnar*Nerve*$To$Hypothenar$Muscles$To$skin$Ulnar$1½$digits$Motor$Branch$to$Intrinsics.$
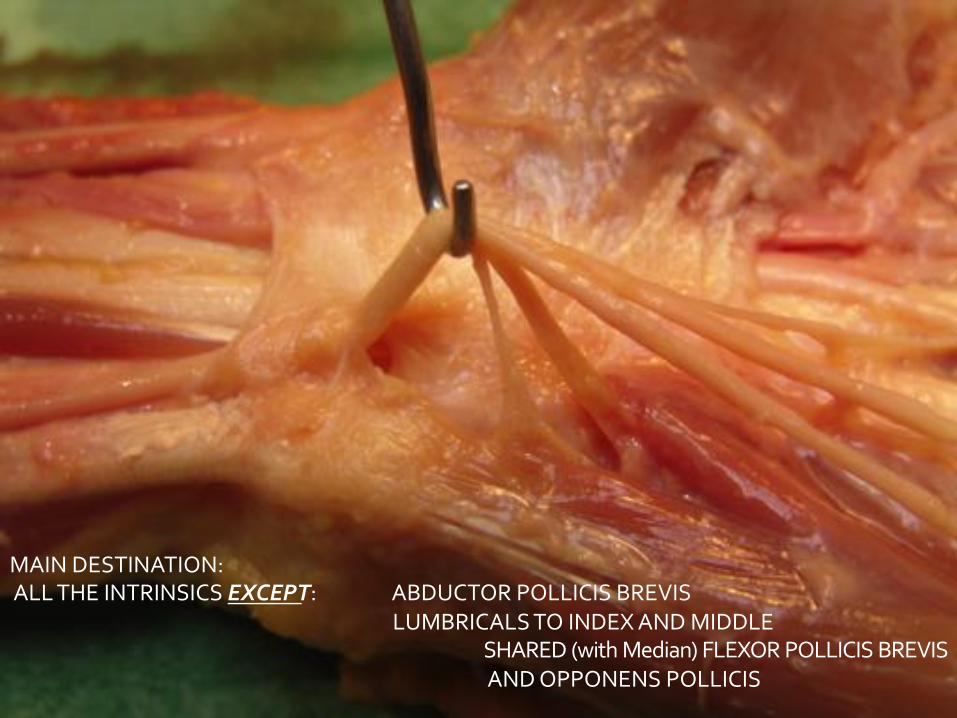
MAIN$DESTINATION:$$ALL$THE$INTRINSICS$EXCEP%T:$ $ABDUCTOR$POLLICIS$BREVIS$
$ $ $ $LUMBRICALS$TO$INDEX$AND$MIDDLE$$ $ $ $ $SHARED$(with$Median)$FLEXOR$POLLICIS$BREVIS$$$ $ $ $ $AND$OPPONENS$POLLICIS $ $$ $ $$
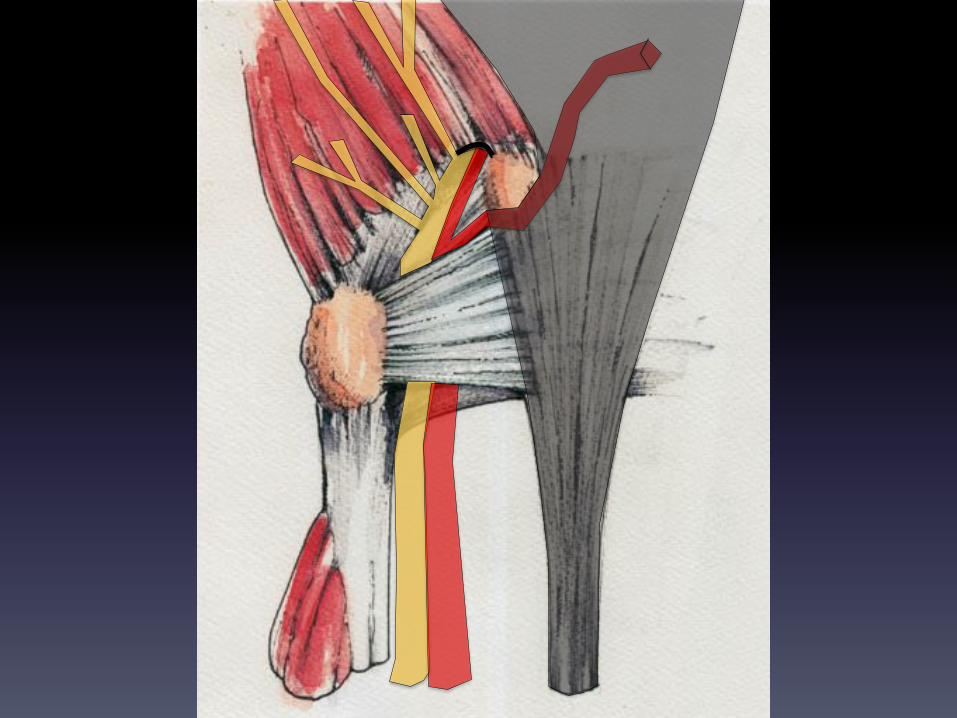
The$deep$motor$branch$of$the$Ulnar$nerve$reaches$the$deepest$level$of$the$palm$$(it$runs$on$the$bases$of$the$metacarpals)$by$$passing$beneath$the$two$heads$of$origin$of$$Opponens$digiti$Minimi.$$It$can$be$compressed$at$this$site,$producing$paralysis/weakness$of$the$intrinsics$but$not$of$the$$Hypothenar$muscles,$nor$any$cutaneous$sensory$loss,$both$supplied$before$the$course$$Through$Opponens$digiti$minimi$$
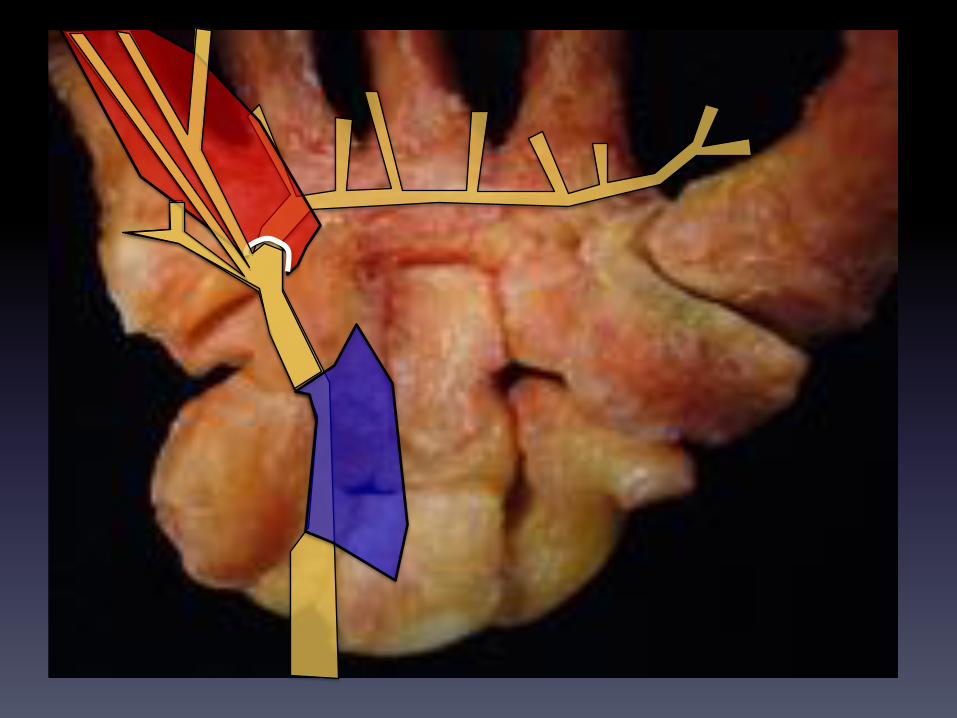
Testing$for$Ulnar$nerve$compromise$involves$testing$for$the$function$of$the$intrinsics,$Particularly$the$interossei.$$For$instance,$asking$the$patient$to$cross$his/her$fingers$tests$for$digit$abduction$and$adduction$$
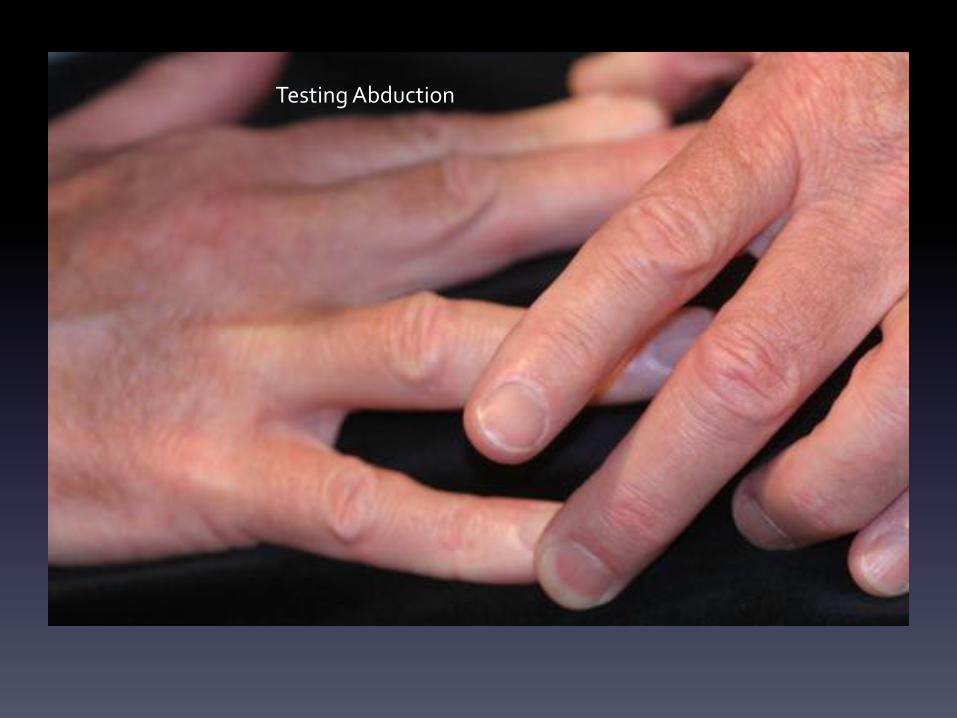
Testing$Abduction$
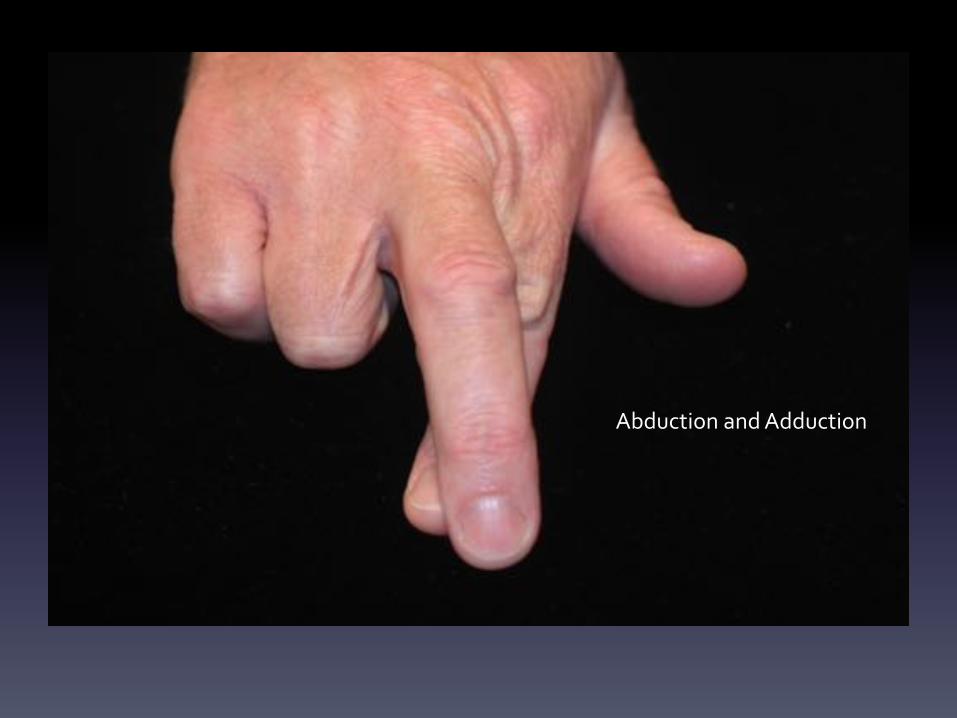
Abduction$and$Adduction$

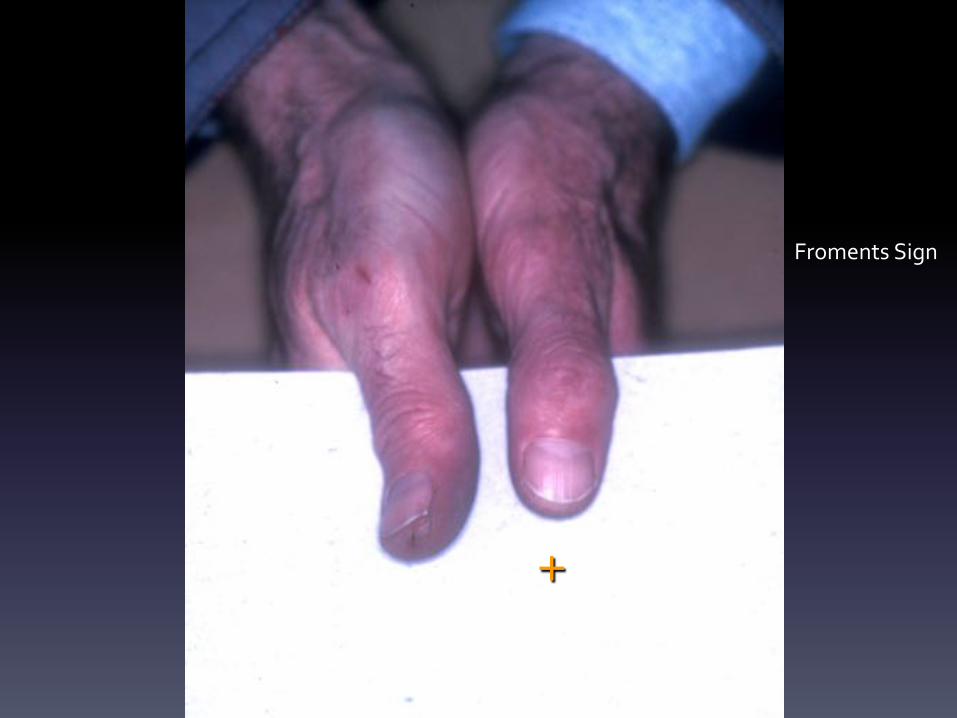
Froments’s$sign$$The$patient$is$asked$to$grasp$a$card$by$adducting$both$thumbs$to$the$index.$$On$the$paralysed$side,$the$Adductor$Pllicis$and$the$1st$Dorsal$interosseous$are$weak,$$or$inactive.$$Strong$Adduction$is$impossible$and$the$patient$compensates$by$holding$on$to$the$card$by$$flexing$the$Flexor$Pollicis$longus.$$A$flexed$thumb$in$performance$of$Froment’s$test,$is$a$positive$result.$$In$the$illustrated$case$the$patient$has$a$positive$Froment’s$sign$on$the$left$hand$$
+
Froments$Sign$
Froment’s$sign$is$also$visible$when$a$patient$is$invited$to$show$strong$key$pinch.$$The$weaker$thumb$flexes$at$the$Interphalangeal$joint.$$

Paralysis$of$Interossei$and$Lumbricals$produces$hyperextension$instability$of$the$MP$joints.$Attempted$extension$of$the$digit$causes$the$MP$joints$to$buckle$into$extension,$$while$the$Interphalangeal$joints$flex.$$Although$the$striking$feature$is$the$‘Claw’$or$flexion$of$the$digit,$$the$essential$defect$is$the$inability$to$stabilise$the$MP$joint.$$Loss$of$power$of$the$Interossei$and$lumbricals$produces$the$INTRINSIC$MINUS$hand$$Note$that$the$claw$deformity$is$less$marked$in$the$index$and$middle$where$the$$median<innervated$lumbricals$are$able$to$maintain$some$stability$(though$this$is$weak)$$

Intrinsic$Minus$(the$Claw$Hand)$