Embed Size (px)
Citation preview

CONTENTSCOMMENTARY: Can microbiota research change our understanding of neurodegenerative diseases? Neurodegenerative Disease Management Vol. 6 Issue 2
REVIEW: Ischemic, traumatic and neurodegenerative brain inflammatory changes Future Neurology Vol. 11 Issue 1
REVIEW: tau protein, ischemic injury and vascular dementia Future Neurology Vol. 10 Issue 6
www.Neurology-Central.com
NeurologyTOP ARTICLE SUPPLEMENTS
Neurodegenerative diseasesTOP ARTICLE SUPPLEMENTS
Powered by

81ISSN 1758-2024Neurodegener. Dis. Manag. (2016) 6(2), 81–85
part of
10.2217/nmt-2015-0012 © 2016 Future Medicine Ltd
Commentary
Can microbiota research change our understanding of neurodegenerative diseases?
Filip Scheperjans*
*Department of Neurology, Helsinki University Hospital & Department of Clinical Neurosciences (Neurology), University
of Helsinki, Helsinki, Finland, Tel.: +358 9 4711; [email protected]
On the clinical and scientif ic level, most neurodegenerative diseases such as Alzheimer’s disease (AD), Parkinson’s dis-ease (PD) and amyotrophic lateral sclerosis (ALS) share common problems such as:
● Their etiology is unknown;
● Their pathogenesis is relatively poorly understood;
● As a consequence, no effective disease modifying treatments are available.
Nevertheless, our understanding of the underlying molecular processes has improved in recent years and, again, several shared features have emerged:
● The vast majority of cases is sporadic and the neurodegenerative process likely arises from an interaction of genetic and environmental factors;
● Misfolding and accumulation of certain neuronal proteins (amyloid-β [Aβ] and
tau in AD, α-synuclein [α-syn] in PD and TDP‐43 in ALS) is a pathological hallmark of the diseases;
● Disease-related pathology may spread across the nervous system in a self-propagative fashion;
● A neuroinf lammatory component is present;
● There can be clinical and pathological overlap between different neurodegenera-tive disorders.
However, after decades of intensive research we are not even close to answer the most elusive, and probably most important question of all, namely “What initiates the pathological cascade that leads to progres-sive neurodegeneration?” In the desperate battle against these devastating disorders we should be open for theories that are free of the legacy of previous approaches, but instead examine the problem from a new perspective.
“In the desperate battle against these devastating disorders we should be open for theories that are
free of the legacy of previous approaches, but instead examine the problem from a new
perspective.”
First draft submitted: 15 December 2015; Accepted for publication: 7 January 2016; Published online: 1 April 2016
“For gastroenterologists, microbiota-based treatment
approaches are already routine procedures, namely fecal
microbiota transplantation for the treatment of refractory
Clostridium difficile infection.”
Keywords • Alzheimer’s disease • amyloid • amyotrophic lateral sclerosis • biomarker • gut–brain-axis • microbiome • microbiota • neuroinflammation • Parkinson’s disease
For reprint orders, please contact: [email protected]

Neurodegener. Dis. Manag. (2016) 6(2)82
Commentary Scheperjans
future science group
“...it has become clear that invasive infection by a
pathogen is not the only mechanism by which microbes can cause
disease.”
an unknown organIt is nowadays an exceedingly rare event that a previously unknown organ of the human body is discovered and awaiting scientific exploration. The contemporary biomedical research com-munity can regard itself privileged for being granted such a unique opportunity. The newly discovered organ of interest, that progressively entered the spotlight of mainstream research during the last decade, has a weight of approxi-mately 1.5 kg, encompasses about 90% of the cells of the human body and has a genetic reper-toire exceeding that of the remaining organism by a factor of 100–200 [1]. This organ has been named ‘microbiota’ and is the ecological com-munity of commensal, symbiotic and pathogenic microorganisms that literally share our body space [2,3]. The term ‘microbiome’ refers to the collective genomes of these microorganisms, but both terms have been used largely synonymously.
In recent years, microbiota research has gained huge momentum through the development of next-generation sequencing approaches allowing rather unbiased assessment of all microbial taxa in a given sample with unprecedented detail and effi-cacy. The Human Microbiome Project found the diversity and abundance of signature microbes of different habitats (e.g., gut, skin, vagina) to vary widely even among healthy subjects, with strong niche specialization both within and among individuals [4]. The gut harbors by far the high-est concentrations of microbiota and is the best studied habitat. Initial studies have focused on the mere description of microbiota composition, for example, measuring the abundances of different microbial taxa in samples. From these studies we have learned that clear alterations of gut microbi-ome community structure are associated not only with gastrointestinal diseases such as inflamma-tory bowel disease or colonic cancer, but also with other disorders such as diabetes, obesity, arthritis, allergy and cardiovascular disease. More recently, using multiomics and experimental approaches, the scope of microbiota research has expanded toward functional aspects of our microbial eco-system. Together with integrative systems biology these studies are beginning to elucidate how gut microbiota interacts with the human host and may be related to health and disease.
microbiota, the brain & neurodegenerationPossible infectious etiologies of neurodegenera-tive diseases have been studied for a long time.
In AD, connections to for example, Herpes simplex virus 1, spirochetal and Chlamydophila pneumoniae infections have been reported [5,6]. Recently, one group found signs of fungal infec-tion in the brains of AD and ALS patients [7,8]. Helicobacter pylori has been suspected as a causal agent in PD [9]. Also bacterial toxins have been discussed as a possible cause of neurodegenera-tive diseases [10]. However, so far, no single infec-tious agent has emerged as being unequivocally associated with any of these disorders and it has been discussed that instead overall infectious burden and resulting systemic inflammation could predispose to neurodegeneration [11,12]. Furthermore, it has become clear that invasive infection by a pathogen is not the only mecha-nism by which microbes can cause disease. Possibly even more relevant are remote systemic influences of commensal microbiota mediated through numerous physiological pathways such as the immune system, autonomic nervous sys-tem (in particular the enteric nervous system and vagal nerve), metabolic routes as well as intercellular signaling locally and through the blood stream.
Importantly, there is a strong bidirectional interaction between the gut microbiota and the CNS, a connection recently termed the ‘micro-biota–gut–brain axis’. While the effects of the autonomic nervous system on gut physiology have been known for a long time, we are just beginning to understand that gut microbiota has strong effects on CNS physiology as well. For example, in animal models, changes in gut microbiota composition rapidly affect behav-ior, neurotransmitter balance and expression of neuronal growth factors which has sparked great interest in the possible connection between gut microbiota and mental disorders [13,14]. Microbiota alterations early in life may have per-manent structural and physiological neurodevel-opmental consequences fueling hope for better understanding of neurodevelopmental problems such as autism spectrum disorders.
In terms of adult neurology, we have recently seen first concrete examples supporting a role of microbiota in neurological disorders. In 2011, Berer et al. demonstrated that in the relapsing-remitting mouse model of spontaneously devel-oping experimental autoimmune encephalomy-elitis, an animal model of MS, commensal gut microbiota is essential for the development of CNS autoimmunity since germ-free mice were protected from encephalomyelitis [15]. Later,

83
Can microbiota research change our understanding of neurodegenerative diseases? Commentary
future science group www.futuremedicine.com
a Japanese study reported alterations of gut microbiota in MS patients [16]. Furthermore, gut microbiota changes have been recently associated with atherosclerosis and ischemic stroke and this association may be mediated through bacterial metabolization of ingested nutrients [17].
The vast number of ways through which gut microbiota affects the host shows intriguing overlaps with pathways previously implicated in neurodegeneration, for example, mitochon-drial function, neuroinflammation and micro-glial activation, growth factors. Microbiota research in neurodegenerative diseases is still in the earliest phases and so far mainly descrip-tive in nature. In PD, there is a strong and early involvement of the gastrointestinal tract. It has long been speculated that in PD an environ-mental factor could act via the gut and initiate the pathological process leading to neurode-generation, but no specific agent could so far be identified [18]. PD patients have a higher prevalence of small intestinal bacterial over-growth which has been linked to worse motor function and fluctuations, as has been H. pylori infection [19].
Recently, Forsyth et al. demonstrated that the colonic mucosa of PD patients shows signs of bacterial invasion, oxidative stress and an impaired barrier function leading to an increased systemic exposure to proinflammatory bacterial lipopolysaccharide [20]. The first comprehensive study of fecal microbiota composition in neuro-degenerative disease revealed clear differences between PD patients and control subjects even after adjustment for potential confounders such as medication and constipation [21]. The most striking finding was a 78% lower abundance of Prevotellaceae in the feces of PD subjects while several other bacterial families were more abundant than in controls. Furthermore, micro-biota was related to the motor phenotype of PD patients. This study suggested that gut micro-biota could be implicated in PD and might be a promising biomarker. Recently, two independ-ent studies confirmed microbiota differences between PD and control subjects [22,23]. Both studies found decreased Prevotellaceae abun-dance in PD, but not all differences reached sta-tistical significance which may at least in part be explained by differences in sample size, subject characteristics and methodology.
Not much is known about pathophysiologi-cal microbiota–host interactions in PD. An
interesting initial finding pointing to interac-tions between the host genome and microbiota is the reported association of common variants in peptidoglycan recognition protein genes with PD risk in two independent studies [24]. These proteins maintain healthy gut microbial flora by regulating the immune response to both com-mensal and harmful bacteria. Variants in these genes could thus influence microbiota compo-sition and the immunological reaction to it. According to one hypothesis, local inflamma-tion in the gut mucosa, which may be related to microbiota and barrier dysfunction, could promote prion-like behavior of α-syn as an ini-tial event in the neuropathological cascade that subsequentally progresses along the vagal and sacral autonomic nerves leading eventually to CNS neurodegeneration [25]. A comparable pro-cess has also been proposed for the nasal route through the olfactory bulb, referring to the early olfactory dysfunction and related neuropathol-ogy in PD subjects. Following a similar line of thought, it was hypothesized that, in diseases such as AD and PD, amyloid proteins produced by bacteria could induce misfolding of host proteins and thus initiate a prion-like cascade leading to progressive neurodegeneration, pos-sibly enhanced by amyloid-induced inflamma-tion and oxidative stress [26,27]. Finally, although not yet confirmed by specific studies, it has been speculated based on a literature review that gut microbiota could play a role in mediating the protective effects of coffee and tobacco use on PD risk [28].
With respect to AD, no detailed study of human microbiota composition or func-tion has been published yet. However, some studies have examined a possible connection between oral microbiota and AD. It has been reported that serum antibodies to oral bacte-ria have been associated with AD and risk for developing incident AD [29,30]. In one study, next-generation sequencing was used to com-pare subgingival plaque microbiota between elderly subjects with and without dementia, without specifying what type of dementia was present [31]. A higher level of Fusobacteriaceae and a lower level of Prevotellaceae was seen in subjects without dementia, although the dif-ference did not reach statistical significance, possibly because of the small sample size. While no state-of-the art assessment of microbiota in AD has been published, yet, interesting find-ings have been recently reported from an AD

Neurodegener. Dis. Manag. (2016) 6(2)84
Commentary Scheperjans
future science group
“...there is a great interest in the potential of microbiota research for reshaping our
understanding and treatment of enigmatic
diseases.”
animal model. According to a not yet peer-reviewed manuscript on arXiv, Harach et al. studied gut microbiota in APPPS1 mice that coexpress the KM670/671NL Swedish muta-tion of human amyloid precursor protein and the L166P mutation of human preseni-lin 1 under control of the Thy‐1 promoter and show age-dependent accumulation of cerebral Aβ plaques [32]. They found that, in comparison to wild-type mice, gut microbiota of APPPS1 mice showed reduced levels of Firmicutes, Verrucomicrobia, Proteobacteria and Actinobacteria with a concurrent increase in Bacteroidetes and Tenericutes. Furthermore, they generated a germ-free version of the APPPS1 mouse model and observed that these mice showed clearly less Aβ amyloid pathol-ogy in the brain than the conventionally raised APPPS1 mice. Colonization of germ-free APPPS1 mice with harvested microbiota from conventionally raised APPPS1 mice increased cerebral Aβ pathology. In contrast, coloniza-tion with microbiota from wild-type mice was ineffective in increasing cerebral Aβ levels. This important study suggests that, at least in this mouse model of AD, commensal gut micro-biota plays a causal role in promoting cerebral Aβ amyloid pathology and thus provides an important proof-of-concept warranting further studies of microbiota in AD.
With respect to ALS, no comprehensive assessment of microbiota has been published. One small study in transgenic a mouse model (G93A) expressing mutant superoxide dismutase reported alterations of intestinal tight junctions and increased intestinal permeability associated with microbiota alterations [33].
Conclusion & future perspectiveFor gastroenterologists, microbiota-based treatment approaches are already routine pro-cedures, namely fecal microbiota transplanta-tion for the treatment of refractory Clostridium difficile infection [34]. In endocrinology, trans-lational studies for microbiota-based inter-ventions targeting diabetes and obesity are underway. Also in many other specialties there is a great interest in the potential of micro-biota research for reshaping our understand-ing and treatment of enigmatic diseases. Such new treatments frequently aim at changing microbiota composition and thus shifting the equilibrium of microbiota–host interac-tions to a state that is beneficial for the host.
One way is to replace patients’ gut microbiota by that of a healthy donor (fecal microbiota transplantation). Alternatively, the abundance of beneficial microbes can be increased by sup-plementing such live organisms directly (pro-biotics) or instead by using compounds that promote their growth (dietary interventions or prebiotics). Another approach is to specifically identify molecules excreted by such beneficial microbes and to use them pharmacologically (postbiotics).
For neurologists, gut microbiota is still rather unknown territory and its connection to neuro-logical diseases may appear counterintuitive. It should not. As outlined above, recent develop-ments in sequencing techniques and molecular biology allow studies of microbiota in unprec-edented detail and the theoretical framework for relevance of the microbiota–gut–brain axis in neurological disorders is actually very strong. Although evidence for involvement of microbiota in neurodegenerative diseases is still very preliminary, initial findings are extremely promising. Future research will need to estab-lish how stable and specific these findings are and whether microbiota changes precede or follow neurodegeneration. Such associations per se could indicate a possible biomarker role of microbiota. More difficult to answer will be the question of causality and what mechanisms drive the interaction with the host and other environmental factors such as diet. Ahead is a long scientific journey that could fundamen-tally reshape our understanding of neurodegen-erative diseases. The time to embark is now. If this endeavor is successful, we may end up with completely new therapeutic approaches that could hopefully turn the ship around toward effective disease modification or even prevention.
Financial & competing interests disclosureThe author has received funding from the Michael J Fox foundation for Parkinson’s Research, the Finnish Parkinson Foundation, the Finnish Medical Foundation, Helsinki University Hospital (T1010NL101), and Hyvinkää Hospital (M6095PEV12). The author is listed as inventor on Finnish patent application 20145492. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript.
No writing assistance was utilized in the production of this manuscript.

85
Can microbiota research change our understanding of neurodegenerative diseases? Commentary
future science group www.futuremedicine.com
references1 Qin J, Li R, Raes J et al. A human gut
microbial gene catalogue established by metagenomic sequencing. Nature 464(7285), 59–65 (2010).
2 Baquero F, Nombela C. The microbiome as a human organ. Clin. Microbiol. Infect. 18(Suppl. 4), 2–4 (2012).
3 Lederberg J, McCray AT. ‘Ome SweetOmics – a genealogical treasury of words. Scientist 15(7), 8 (2001).
4 Human Microbiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature 486(7402), 207–214 (2012).
5 Maheshwari P, Eslick GD. Bacterial infection and Alzheimer’s disease: a meta-analysis. J. Alzheimers Dis. 43(3), 957–966 (2015).
6 Agostini S, Clerici M, Mancuso R. How plausible is a link between HSV‐1 infection and Alzheimer’s disease? Expert Rev. Anti Infect. Ther. 12(3), 275–278 (2014).
7 Alonso R, Pisa D, Marina AI, Morato E, Rabano A, Carrasco L. Fungal infection in patients with Alzheimer’s disease. J. Alzheimers Dis. 41(1), 301–311 (2014).
8 Alonso R, Pisa D, Marina AI et al. Evidence for fungal infection in cerebrospinal fluid and brain tissue from patients with amyotrophic lateral sclerosis. Int. J. Biol. Sci. 11(5), 546–558 (2015).
9 Dobbs SM, Dobbs RJ, Weller C, Charlett A. Link between Helicobacter pylori infection and idiopathic Parkinsonism. Med. Hypotheses 55(2), 93–98 (2000).
10 Banack SA, Caller TA, Stommel EW. The cyanobacteria derived toxin Beta-N-methylamino-l-alanine and amyotrophic lateral sclerosis. Toxins (Basel) 2(12), 2837–2850 (2010).
11 Lim SL, Rodriguez-Ortiz CJ, Kitazawa M. Infection, systemic inflammation, and Alzheimer’s disease. Microbes Infect. 17(8), 549–556 (2015).
12 Bu XL, Wang X, Xiang Y et al. The association between infectious burden and Parkinson’s disease: a case–control study. Parkinsonism Relat. Disord. 21(8), 877–881 (2015).
13 Bravo JA, Forsythe P, Chew MV et al. Ingestion of Lactobacillus strain regulates
emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc. Natl Acad. Sci. USA 108(38), 16050–16055 (2011).
14 Bercik P, Denou E, Collins J et al. The intestinal microbiota affect central levels of brain-derived neurotropic factor and behavior in mice. Gastroenterology 141(2), 599–609, 609.e1–3 (2011).
15 Berer K, Mues M, Koutrolos M et al. Commensal microbiota and myelin autoantigen cooperate to trigger autoimmune demyelination. Nature 479(7374), 538–541 (2011).
16 Miyake S, Kim S, Suda W et al. Dysbiosis in the gut microbiota of patients with multiple sclerosis, with a striking depletion of species belonging to Clostridia XIVa and IV clusters. PLoS ONE 10(9), e0137429 (2015).
17 Yin J, Liao SX, He Y et al. Dysbiosis of gut microbiota with reduced trimethylamine-N-oxide level in patients with large-artery atherosclerotic stroke or transient ischemic attack. J. Am. Heart Assoc. 4(11), e002699 (2015).
18 Hawkes CH, Del Tredici K, Braak H. Parkinson’s disease: a dual-hit hypothesis. Neuropathol. Appl. Neurobiol. 33(6), 599–614 (2007).
19 Fasano A, Bove F, Gabrielli M et al. The role of small intestinal bacterial overgrowth in Parkinson’s disease. Mov. Disord. 28(9), 1241–1249 (2013).
20 Forsyth CB, Shannon KM, Kordower JH et al. Increased intestinal permeability correlates with sigmoid mucosa alpha-synuclein staining and endotoxin exposure markers in early Parkinson’s disease. PLoS ONE 6(12), e28032 (2011).
21 Scheperjans F, Aho V, Pereira PA et al. Gut microbiota are related to Parkinson’s disease and clinical phenotype. Mov. Disord. 30(3), 350–358 (2015).
22 Keshavarzian A, Green SJ, Engen PA et al. Colonic bacterial composition in Parkinson’s disease. Mov. Disord. 30(10), 1351–1360 (2015).
23 Hasegawa S, Goto S, Tsuji H et al. Intestinal dysbiosis and lowered serum lipopolysaccharide-binding protein in Parkinson’s disease. PLoS ONE 10(11), e0142164 (2015).
24 Goldman SM, Kamel F, Ross GW et al. Peptidoglycan recognition protein genes and risk of Parkinson’s disease. Mov. Disord. 29(9), 1171–1180 (2014).
25 Lema Tome CM, Tyson T, Rey NL, Grathwohl S, Britschgi M, Brundin P. Inflammation and alpha-synuclein’s prion-like behavior in Parkinson’s disease-is there a link? Mol. Neurobiol. 47(2), 561–574 (2013).
26 Friedland RP. Mechanisms of molecular mimicry involving the microbiota in neurodegeneration. J. Alzheimers Dis. 45(2), 349–362 (2015).
27 Hill JM, Lukiw WJ. Microbial-generated amyloids and Alzheimer’s disease (AD). Front. Aging Neurosci. 7, 9 (2015).
28 Scheperjans F, Pekkonen E, Kaakkola S, Auvinen P. Linking smoking, coffee, urate, and Parkinson’s disease – a role for gut microbiota? J. Parkinsons Dis.5(2), 255–262 (2015).
29 Kamer AR, Craig RG, Pirraglia E et al. TNF-alpha and antibodies to periodontal bacteria discriminate between Alzheimer’s disease patients and normal subjects. J. Neuroimmunol. 216(1), 92–97 (2009).
30 Noble JM, Scarmeas N, Celenti RS et al. Serum IgG antibody levels to periodontal microbiota are associated with incident Alzheimer disease. PLoS ONE 9(12), e114959 (2014).
31 Cockburn AF, Dehlin JM, Ngan T et al. High throughput DNA sequencing to detect differences in the subgingival plaque microbiome in elderly subjects with and without dementia. Investig. Genet. 3(1), 19 (2012).
32 Harach T, Marungruang N, Dutilleul N et al. Reduction of Alzheimer’s disease beta-amyloid pathology in the absence of gut microbiota. arXiv:1509.02273v2 [q-bio.MN] (2015).
33 Wu S, Yi J, Zhang YG, Zhou J, Sun J. Leaky intestine and impaired microbiome in an amyotrophic lateral sclerosis mouse model. Physiol. Rep. 3(4), e12356 (2015).
34 van Nood E, Vrieze A, Nieuwdorp M et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N. Engl. J. Med. 368(5), 407–415 (2013).

77ISSN 1479-6708Future Neurol. (2016) 11(1), 77–96
part of
10.2217/fnl.16.5 © 2016 Future Medicine Ltd
REVIEW
Ischemic, traumatic and neurodegenerative brain inflammatory changes
Rachelle Dugue1 & Frank C Barone*,1
1Departments of Neurology & Physiology & Pharmacology, SUNY Downstate Medical Center, Brooklyn, NY 11203, USA
*Author for correspondence: Frank C Barone, [email protected]
This review serves to link the role of the immune system in the neuropathology of acute ischemic stroke, traumatic brain injury and neurodegenerative disease. The blood–brain barrier delineates the CNS from the peripheral immune system. However, the blood–cerebrospinal fluid barrier acts as a gate between the periphery and the brain, permitting immune activity crosstalk and modulation. In acute ischemic stroke, traumatic brain injury and other neurodegenerative diseases, the blood–brain barrier is compromised and an influx of inflammatory cells and plasma proteins occurs, resulting in edema, demyelination, cell dysfunction and death, and neurobehavioral changes. The role of the complement system, key cytokines, microglia and other neuroglia in brain degenerative pathology will be discussed.
First draft submitted: 7 December 2015; Accepted for publication: 19 January 2016; Published online: 22 February 2016
KEYWORDS • brain injury • complement • inflammasome • innate immunity • neurodegeneration • neurodegenerative disease • neuroimmunology • neuroinflammation • stroke • traumatic brain injury
The innate immune system in the periphery versus the CNS●● Innate immunity in the periphery
The innate immune system of the periphery acts as a first responder to pathogens. Also known as the nonspecific immune system, the components of innate immunity provide general, nonspecific defense mechanisms to control infection. In addition to anatomical barriers like the skin and GI tract to physically prevent pathogen invasion, innate immunity provides two important initial functions: it immediately recognizes pathogens, pathogenic by-products, pathogen-altered human cells and proteins, and tissue injury; and it rapidly recruits and initiates effector cells to eliminate/regulate these intruders/changes [1].
In order to recognize pathogens and other markers of bodily harm, the innate immune system utilizes an arsenal of receptor types (referred to as ‘pattern recognition receptors’ [PRRs]) that are expressed on cell membranes, within the cytoplasm of cells, or secreted in soluble forms by effector cells. Different PRRs and cell systems can detect self-MHC class I molecules, pathogen-associated molecular patterns (PAMPs) and/or damage-associated molecular patterns (DAMPs) [2]. PAMP detecting receptors include Toll-like receptors (TLRs), nucleotide oligomerization domain-like receptors (NLRs), RIG-like receptors, AIM2-like receptors, scavenger receptors and the soluble collagen-containing C-type lectins (i.e., collectin receptors) [3,4]. Many of these same receptors, including TLRs, NLRs, as well as the scavenger receptor, receptor for advanced glycation end prod-ucts, detect DAMPs as well [5]. DAMPs are produced when tissue is damaged or cells lyse during injury/inflammation [2–3,6]. DAMP receptors are of particular importance to neurodegenerative pathologies like acute ischemic stroke (AIS) and traumatic brain injury (TBI) where noninfectious
For reprint orders, please contact: [email protected]

Future Neurol. (2016) 11(1)78
REviEW Dugue & Barone
future science group
tissue injury occurs.In response to DAMPs and PAMPs detected
by their receptor complexes, effector cells of the peripheral innate immune system are activated. Thus, macrophages, dendritic cells, neutrophils, mast cells, eosinophils, natural killer cells and γδ T cells collectively contribute to host defense via phagocytosis of pathogens, the destruc-tion of compromised host cells, cell toxin and cytokine release, and the activation of the adap-tive immune response via antigen presentation to naive T cells [1,2].
Inflammatory cytokines are small cell sign-aling proteins such as interleukins, TNF-α, interferons and chemokines (e.g., chemoat-tractant cytokines such as MCP-1). Cytokines contribute both locally and systemically to pro-inf lammatory and anti-inf lammatory responses [7]. The imbalance of pro- versus anti-inflammatory cytokines contributes to vasodila-tion, edema, the development, activation and recruitment of immune cells, and apoptotic cell death [1,8–9]. In cooperation with the innate immune system’s cellular and molecular immune defense system, is the complement system (see ‘The complement system’ section). The com-plement system is comprised of plasma proteins and proteases that tag pathogens for destruction, initiate cell death, recruit inflammatory cells and induce inflammation [1,10].
In summary, the rapid, highly organized and interlocked system of innate immunity in the periphery showcases three main players: the effector cell bound and soluble PRRs; the effector cells (macrophages, dendritic cells, neutrophils, mast cells, eosinophils, natural killer cells and γδ T cells), which act in response to their PRRs, binding to PAMPs and/or DAMPs to produce both pro- and anti-inflammatory cytokines, acti-vate the adaptive immune response via antigen presentation, recruit cells and induce cell death via phagocytosis, toxin release and other mecha-nisms; and the complement system, which con-tains both PRRs to PAMPs and DAMPs and mechanisms to tag damaged cells, pathogens and induce cell death and other cellular (e.g., synaptic) changes following injury or infection.
●● Innate immunity in the CNSSimilar to the anatomical barriers of innate immunity in the periphery, the CNS blood–brain barrier (BBB) generally isolates the brain from the cells and molecules of the periphery. However, the blood–cerebrospinal fluid barrier
(BCSFB), formed by the choroid plexus, arach-noid and arachnoid villi, lines each ventricle and provides regulated communication between the brain and the periphery [11]. It filters out meta-bolic waste, excess neurotransmitter and foreign substances from the cerebrospinal fluid (CSF), in addition to conditionally permitting immune cell trafficking [12]. The choroid plexus of the BCSFB acts as a gate, allowing leukocytes to enter the CNS in specific physiological and path-ological conditions [13]. These mechanisms pro-vide immune cells that can contribute to injury as well as brain protection and repair [12]. The CNS also contains a meningeal lymphatic sys-tem, recently discovered along the dural sinuses, through which CSF contents can be transported to and activate immune responses in the deep cervical lymph nodes [14]. The pathways through which immune cells are transported may relate to their function [15].
Like the peripheral innate immune system, the CNS contains its own effector cell types, in addition to all complement components. Astrocytes, microglia, oligodendrocytes, mast cells, and NG2 chondroitin sulfate and PDGF-α receptor-positive oligodendrocyte precursor cells (NG2-OPCs), in addition to complement com-ponents produced locally within the brain itself, contribute to the brain’s immune response [16,17]. Microglia act as the brain’s phagocytes and patrol the brain tissue for any threats (see ‘The role of microglia in AIS, TBI & neurodegeneration’ section), while astrocytes regulate the concen-trations of ions, glutamate and water, store gly-cogen and offer metabolic support to neurons, in addition to regulating synaptogenesis, forming the BBB and defending against oxidative dam-age [1–4,18]. Astrocytes and microglia produce many pro- and anti-inflammatory cytokines following DAMP and/or PAMP detection. For example, microglia, astrocytes, neurons, mast cells and oligodendrocytes all express TLRs. TLRs 3, 7 and 8 are present on neurons and, when activated, can inhibit post-injury axonal growth and repair. The accumulation of TLR-activating DAMPs after neuronal injury may prevent axon regeneration and repair by induc-ing TLR3-mediated axonal growth cone col-lapse and/or TLR7- and 8-mediated neuronal death [4].
In the CNS and peripheral immune sys-tem (see Figure 1), while infection causes the release of PAMPs, injury causes the release of DAMPs, both of which can drive inflammasome

79
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
future science group www.futuremedicine.com
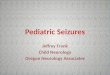
Figure 1. The innate immune response of the periphery versus the CNS. The innate immune response in the periphery, like the innate immune response of the CNS, is activated by PAMPs related to infection and DAMPs related to tissue injury. Pattern recognition receptors like TLRs, NLRs, RLRs and ALRs detect these signals and induce a cellular and molecular response from the effector cells containing these receptors. In the periphery, major effector cells are natural killer cells, macrophages, neutrophils and dendritic cells. Natural killer cells induce apoptosis of infected cells, while neutrophils use a respiratory burst response involving the release of ROS to destroy phagocytosed material. Effector cells like dendritic cells and macrophages detect PAMPs and act as antigen-presenting cells. These antigen-presenting cells travel to the nearest draining lymph node and trigger the maturation of naive T cells and the more effective, long-term adaptive immune response of the peripheral immune system. In contrast, the CNS innate immune response mainly utilizes microglia, astrocytes and neurons. These cells express PRRs like TLRs and NLRs to detect PAMPs and DAMPs. In response to these signals, astrocytes are activated leading to astrogliosis, glial scar formation, and the release of complement, cytokines and growth factors. Microglia become activated in response to these signals and via their interaction with neurons, phagocytose debris, and release cytokines, complement, growth factor, reactive oxygen species, glutamate, histamine and chemokines. Cytokines and chemokines recruit and activate glial and immune cells, increase vascular permeability, and participate in cell death and survival signaling. The interaction between PAMPs or DAMPs and PRRs leads to the formation of inflammasomes, multimolecular complexes that permit the release of active pro-inflammatory cytokines IL-1β and IL-18, as well as apoptosis; AIM-2 inflammasomes form in neurons in response to DNA released from dying and injured cells and contribute to pyroptotic neuronal death. A variety of NLR inflammasomes (NLRP1, NLRP2, NLRP3) are expressed in neurons, microglia and astrocytes. The formation of the NLR inflammasome involves an initial activation of the NF-κB pathway via pattern-recognition receptors like TLRs (signal 1). The NF-κB pathway transcribes pro-IL-1β and pro-IL-18, which are cleaved to their pro-inflammatory active form by caspase-1. NLRs are activated by ATP (signal 2) and form inflammasomes that recruit and activate caspase, thereby catalyzing this reaction [4]. Inflammasomes can form in both the periphery and the CNS. Furthermore, frequent communication occurs between the periphery and the CNS via the BCSFB and meningeal lymphatic system. ALR: AIM-like receptor; BBB: Blood–brain barrier; BCSFB: Blood–cerebral spinal fluid barrier; DAMP: Damage-associated molecular pattern; NLR: Nucleotide oligomerization domain-like receptor; PAMP: Pathogen-associated molecular pattern; ROS: Reactive oxygen species; RLR: RIG-like receptor; TLR: Toll-like receptor.
Periphery CNS
DAMPs
Tissue injuryInfection
PAMPs
Macrophage
Naive T-cell
Th1Th2cells
Th17
*Antigen presentation
Lymph node
BBB disruptionin brain injury
Dendritic cell Natural killer cell
NeutrophilRespiratory burst(ROS release)
Peripheral effector cell infiltration
DAMPs
Neuron
PAMPs
BB
B
*
– Edema– Recruitment of peripheral immune cells (macrophages,neutrophils, T cells)via chemokines
TLR
TLR
TLR
RLR
NLR
NLRMicroglia
AstrocyteALR
Cytokine and chemokine release
Signal 1
NF-κB pathway
pro-IL-1β IL-1βpro-IL-18 IL-18
Caspa
se-1
Inflammation
Pyroptosis
Activated cytosolic sensors
(NLRs, ALRs)
Inflammasome
Signal 2
Adaptive immune response
Meningeal lymphatics
BCSFB
Production of inflammatory markers

Future Neurol. (2016) 11(1)80
REviEW Dugue & Barone
future science group
formation. The inflammasome is a cytoplasmic complex that responds to DAMPs and PAMPs (e.g., changes in cytoplasmic pH, ion concen-trations, the presence of reactive oxygen species or microbial products) in the CNS and periph-ery. The NACHT domain-, LRR domain- and pyrin domain-containing protein (NALP) fam-ily of NLRs are common catalysts of inflamma-some formation, in which a PRR is connected to caspase-1, often via an ASC adaptor (apoptosis-associated speck-like protein containing a caspase recruitment domain) [6]. Various inflammas-omes are defined by their PRRs. Simultaneous to inflammasome formation, cell surface bound PRRs, for example, TLRs are activated, leading to the production of pro-IL-1β and pro-IL-18; pro-IL-1β and pro-IL-18 are then cleaved into their active pro-inflammatory forms by caspase-1, a protease activated in response to inflammasome formation [4,6]. Recent studies have elucidated caspase-1-induced extracellular release of ASC specks (ASC-NALP3 oligomers) after inflamma-some activation in the periphery. These specks could serve as additional DAMP signals and acti-vators of pro-caspase-1 and pro- IL-1β [19,20]. ASC, NALP-1 and caspase-1 have all been detected in CSF and are related to worse outcomes post-TBI [17]. Caspase-1-activated IL-1β and IL-18 lead to effector cell activation and recruitment, further cytokine synthesis and release, autophagy, enzy-matic inhibition, and programmed cell death (see ‘Neuroglia & BBB disruption in AIS, TBI & neurodegeneration’ section) [4,21]. Mechanisms like this constitute the immediate response of the innate immune system.
The complement system●● The complement system in the CNS
The complement system is heavily integrated in the CNS, contributing to neuronal development, synaptic remodeling and neuropathology. The complement system has three main activation pathways: the alternative pathway, the lectin pathway and the classical pathway (see Figure 2 for a pictorial summary of the complement cas-cade). The alternative pathway is spontaneously activated via hydrolysis of complement protein C3 and in response to pathogen-induced changes in the physiochemical environment. The lectin pathway is activated by mannose-binding lectin binding to mannose-containing glycoproteins and carbohydrates of pathogens and PAMPs. The classical pathway is activated when the ini-tiating complement protein, C1q, binds to any
of the following: antigen–antibody complexes, apoptotic cells, certain coagulation cascade fac-tors, serum pentraxin proteins like CRP, and serum amyloid P [22,23].
The central event within the complement cas-cade is the cleavage of complement protein C3 to C3a and C3b. C3b tags pathogens and deposits on membranes in a process called opsonization to encourage phagocytosis, while C3a is an ana-phylatoxin, an inflammatory modulator that recruits effector cells to complement-targeted sites and increases effector cell activity [22]. The formation of C3b and C3a from C3 permits the complement system to respond rapidly and robustly; this is the primary amplification step in the cascade.
All activation pathways lead to the formation of C3 convertases. The C3 convertases of the classical and lectin pathways form from cleav-age of C4 and C2, while the C3 convertase of the alternative pathway forms from C3b and Factor B’s cleavage product, Bb. C3 convertases bind and cleave C3, creating a positive feedback loop, in addition to contributing to the forma-tion of the terminal C5 convertase. C5 con-vertase is the substrate for the terminal comple-ment proteins C5b-9. All complement pathways converge to form the membrane attack complex (MAC) from terminal complement proteins for membrane lysis of pathogens and abnormal cells, in addition to the production of anaphylatoxin, C5a (see Figure 2) [10,24–25].
Complement proteins can also activate cytokines and intracellular signaling pathways. For example, C3 can trigger TNF-α release, which intensifies inflammation by leading to the release of IL-1, IL-6 and IL-18 [10]. To reg-ulate this cascade, inhibitory proteins such as Factor H, C1-inhibitor, decay-accelerating fac-tor, membrane cofactor protein (i.e., CD46) and MAC-inhibitory protein (i.e., CD59) oppose complement cascade promoting factors [1,26].
Complement factors and receptors are synthe-sized throughout the CNS by neurons, microglia, astrocytes, oligodendrocytes, as well as endothe-lial cells of the microvasculature. Most neurons express C1q, C5, the C5a receptor (i.e., CD88) and CD59, but have the potential to produce other complement proteins when stimulated to do so [3,27]. Astrocytes produce C1q, C1r, C1s and C2–4 of the classical pathway, C3, Factor B and Factor D of the alternative pathway, and C5–9 of the terminal part of the pathway. Astrocytes also express complement receptors

81
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
future science group www.futuremedicine.com
C1qr, CR2, C3aR and C5aR, while produc-ing regulatory proteins C1-inhibitor, Factor H, Factor I, clusterin, CD59, decay-accelerating fac-tor, membrane cofactor protein and CR1 [26]. Microglia express the same complement com-ponents of the classical pathways as astrocytes, but only produce C3 of the alternative pathway, while expressing the receptors C1qR, C3R, C3aR, CR4, C5aR and the regulatory proteins C1-inhibitor, CD59 and CR1 [16,26]. In contrast to microglia and astrocytes, oligodendrocytes
produce complement components C1q, C1s, C4, C2, C3, C5–9, but have no regulatory proteins; oligodendrocytes are therefore more susceptible to complement-mediated attack.
In addition to its immunoregulatory func-tions within the brain, the complement cascade is involved in neurogenesis, cell migration and survival, and synaptic development and elimi-nation [25,28]. For example, adult hippocampal neurogenesis was discovered to be regulated by CR2, a receptor that binds C3 fragments and
Figure 2. The complement cascade. The complement system is comprised of three pathways: the classical pathway, the lectin pathway and the alternative pathway. These pathways are activated by different signals, but all culminate in the production of C3 and later the formation of the MAC, which lyses abnormal cell membranes and pathogens. C3b deposits on pathogens and cell membranes to encourage phagocytosis via phagocytes containing CR3 in a process termed opsonization. Anaphylatoxins C5a and C3a, recruit and increase the activity of effector cells and are a by-product of C3 and C5 cleavage, respectively. Various proteins such as DAF, MCP and C1-inhibitor protein regulate the complement cascade. DAF: Decay-accelerating factor; MAC: Membrane attack complex; MASP: Mannose-binding lectin-associated serine protease; MBL: Mannose-binding lectin; MCP: Membrane cofactor protein, i.e., CD46 complement regulatory protein; PAMP: Pathogen-associated molecular pattern; SAP: Serum amyloid P.
C1-inhibitor
C1rC1s
C2 C4
C1q
C4b2b
C3bBb
C4b2b3b C3bBbC3b
C3 convertases:
C5 convertases:
DAFMCP
iC3b
CR3
MBL
MASPs
C3a
C3
C5a
C5
C5aR
C5b CD59 C5b-9 (MAC)
C3 (H2O)
C3b
Factor BFactor D
Active B
Bb Ba
iC3b
Classical pathway Lectin pathway Alternative pathway
Activation Pentraxins (SAP, CRP)Antigen–antibody complexes
Apoptotic cellsCoagulation factors
Mannose-containingPAMPs
Spontaneous hydrolysis of C3

Future Neurol. (2016) 11(1)82
REviEW Dugue & Barone
future science group
IFN-α, and is therefore sensitive to inflamma-tory changes [29]. Complement proteins are also utilized in the elimination of synapses in the developing brain. C1q, the initiating comple-ment protein in the classical pathway, is upreg-ulated in developing neurons during periods of pruning and is hypothesized to localize to synapses destined for elimination through com-munication with immature astrocytes [30,31]. The presence of C1q on such synapses triggers C3 activation and opsonization for phagocytosis by C3R bearing microglia, as well as the forma-tion of the terminal MAC [31]. The increased presence of activated microglia during periods of developmental pruning supports this idea [10].
These mechanisms of synaptic modifica-tion have also been implicated in TBI, AIS and neurodegenerative diseases such as Alzheimer’s disease (AD), Parkinson’s disease (PD), and multiple sclerosis (MS). The involvement of complement in neurodegenerative pathologies will be explored in the following section.
●● The complement system in AIS, TBI & neurodegenerationThe basic pathophysiology of TBI involves the initial traumatic insult followed by a complex cas-cade of events in response to the primary injury; the release of excessive amounts of excitatory neurotransmitters and increases in intracellular calcium, immune activation and dysfunction, free radical release, ion flux and metabolic imbal-ances, BBB disruption, and vasogenic edema, all contribute to disruptions in homeostasis lead-ing to cell death via necrosis and apoptosis [32,33]. Similarly, the basic pathophysiology of ischemic stroke involves an initial event – the interrup-tion of blood flow to the brain via embolism, hypoperfusion, or arterial or venous thrombosis, producing a severely hypoperfused area termed the core and a moderately perfused surround-ing area termed the penumbra; the core of the lesion undergoes widespread necrosis, while the penumbra is at risk of cell death via neurotoxic factors from the core [34]. The ischemic event leads to a cascade of responses: excitotoxicity, inf lammation, oxidative damage, apoptosis, angiogenesis and changes in ionic balance [35].
The expression of complement components in the brain is highly upregulated following ischemic stroke, TBI and other forms of brain injury. Reactive astrocytes and microglia pro-duce high levels of C3 and complement proteins, in addition to cytokines and other inflammatory
signals. For example, the anaphylatoxins C3a, C4a and C5a are produced by complement sys-tem activation in AIS and TBI. These anaphyla-toxins increase vascular permeability and recruit and activate inflammatory cells. Because the BBB is breached in these conditions, immune cells from the periphery quickly enter the brain in response to such signals; C5a induces chem-otaxis of basophils, neutrophils, macrophages and microglia to the site of injury. In ischemic stroke, C5a is increased in ischemic neurons, likely driving neuronal apoptosis, while C3a and C5a receptors, C1q and C3 are increased in the infarct core [27,36].
Complement depletion has been shown to improve neurological function in cerebral ischemia [37]. C3 is detrimental in ischemic stroke. For example, following AIS, C3-/- mice had smaller infarct volumes, less granu-locyte infiltration into the brain, decreased oxidant stress levels, and better neurological function than wild-type mice. Similar results were obtained in wild-type mice when a C3R antagonist was administered following ischemic stroke [38]. In patients with MS, C3 has also been shown to positively correlate with disease sever-ity, and neurofilament light levels, a biomarker of nerve injury [39].
C5-/- mice were also protected from brain injury [40]. In neurons, C5a receptor (i.e., CD88) expression and the production of C5a are increased in response to ischemic stress. CD88-/- mice and neuronal cultures treated with CD88 receptor blockers were significantly protected in models of AIS and TBI, suggesting that C5a and its receptor contribute significantly to neuronal death [27]. C5a, in addition to mediat-ing the release of pro-inflammatory cytokines, upregulates the expression of coagulation cascade-activating tissue factor in endothelial cells. Importantly, C3 and C5 can be proteolyti-cally activated by plasmin, thrombin and other coagulation cascade factors [22].
Regulators of the complement system, such as C1 inhibitor, have exhibited protection in AIS models. C1 inhibitor-treated mice had lower degrees of neuronal degeneration, improved neu-rological deficit scores, smaller infarct volumes and decreased leukocyte infiltration [41–43]. This could occur through the upregulation of the anti-inflammatory cytokines IL-10 and IL-6 [42]. A lack of mannose-binding lectin has also been associated with improved outcomes following stroke in mouse models and in patient cases [22].

83
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
future science group www.futuremedicine.com
Complement activation also acts as a mediator of injury in TBI. C1q, C3b, C3d and MAC levels are increased in TBI brains. In TBI brains, MAC levels have been observed to correlate with the level of BBB disruption [44]. In stroke patients, serum levels of MAC components C5b-9 have been positively correlated with ischemic stroke severity [45]. These levels rise and exacerbate injury in the absence of complement regulator, CD59 [3].
Unlike astrocytes and microglia, neurons and oligodendrocytes do not express as much CD59, the complement regulatory protein responsible for inhibiting the formation of the terminal MAC. They are therefore more sus-ceptible to complement-mediated damage and death. This is especially true of apoptotic neu-rons that lose complement regulatory proteins, permitting their progression toward cell lysis and phagocytosis [46]. The absence of protective CD59 in oligodendrocytes and some neurons could explain the selective white matter damage of diffuse axonal injury in some forms of TBI. Furthermore, mice overexpressing complement inhibitor Crry had fewer neurological deficits following TBI [3].
Although complement-mediated synaptic pruning is a normal aspect of neuronal devel-opment, the elimination of synapses is likely to contribute to neurodegeneration in AIS and TBI, as well as in other neurological diseases such as MS, AD and PD. Reactive astrocytes upregulated following injury are of a similar composition to immature astrocytes involved in signaling related to C1q upregulation at synapses during developmental synaptic prun-ing [34]. Following injury, C1q is upregulated in microglia and neurons, while reactive astro-cytes begin to appear and downstream compo-nents of the complement cascade are activated. Supporting the concept of complement-medi-ated synaptic elimination in neurodegenerative disease, is the recent observation of a combina-tion of hypoxia and the inflammatory stimulus lipopolysaccharide (LPS) inducing long-term depression (LTD) in the hippocampus. The LTD observed was triggered by microglial CR3 activation and involved NADPH oxi-dase production of the potent reactive oxygen species superoxide, leading to AMPA recep-tor internalization [47]. Long-lasting LTD at a synapse can result in the elimination of that synapse by microglia. Furthermore, CRP (i.e., a serum pentraxin that activates the classical
complement cascade via binding to C1q) lev-els positively correlate with infarct volume in AIS patients [48]. Thus, an excess of CRP could trigger C1q upregulation and contribute to synaptic elimination via mechanisms simi-lar to those occurring during developmental synaptic pruning.
In MS, synaptic loss was shown alongside increases in synaptic C1q and C3 deposition in MS hippocampi with and without lesions and demyelination. C1q deposition positively correlated with synaptophysin staining for syn-aptic density, as well as mtHSP70 density, a marker of neuronal stress, in the hippocampi of patients with progressive MS. These find-ings, in addition to observations of C1q and C3 deposition co-localized with CR3 in synapses within microglial processes, support comple-ment-mediated synapse elimination in MS [49]. In a study on age-related cognitive decline, C1q levels increased with age and were far higher in aged mice, as well as in aged human brains, especially in the dentate gyrus molecular layer; C1q-deficient aged mice had greater cognitive flexibility than wild-type aged mice [50]. In a transgenic mouse model of AD, the absence of C1q protected neuronal integrity and decreased astrocytic and microglial activity [51]. A model of PD showed increased C1q expression in activated microglia surrounding degenerating dopaminergic neurons in the substantia nigra. However, C1q-deficient PD mice had the same degree of nigrostriatal degeneration as wild-type mice [52]. Furthermore, in humans, genetic variants of C1q are not likely to influence cog-nitive decline in PD [53]. Therefore, C1q may not be detrimental in PD pathology.
Key cytokines & immune players in brain injury & neurodegeneration●● Neuroglia & BBB disruption in AIS, TBI
& neurodegenerationBrain injury puts extreme stress on the regulatory function of astrocytes and other brain cells. The destruction of neurons and glial cells causes the release of ATP and many DAMPs, thus activat-ing microglia, neurons, mast cells and glial cells to produce cytokines, chemokines and comple-ment [17,26]. Tissue injury-induced stress disturbs astrocyte-driven ion and glutamate homeosta-sis resulting in the substantial release of gluta-mate, K+ ions and reactive oxygen species, all of which contribute to neurotoxicity [54]; astrocytes downregulate their glutamate transporters, thus

Future Neurol. (2016) 11(1)84
REviEW Dugue & Barone
future science group
contributing to glutamate-induced excitotoxic-ity [55]. Astrocytes are activated very early in AIS and TBI, as well as in neurodegenerative diseases such as PD, AD and MS (i.e., reactive astrogliosis, an excessive proliferation and acti-vation of astrocytes, a necessary response to all CNS injury) [56–59]. Microglia also play a key role in neurodegenerative disease pathology. When stimulated in these conditions, microglia may switch to a state in which they phagocytose dead or dying cells and debris, while producing cytokines and neurotoxic substances that can exacerbate cell damage [23].
The common disruption of the BBB in AIS and TBI results in vasogenic edema, permits the influx of immune cells from the periphery and signals the immediate migration of microglia and NG2-OPCs to BBB leak sites and sites of tissue injury [60,61]. Chemokines and cytokines recruit immune and glial cells, in addition to increasing vascular permeability, while adhe-sion molecules drive neutrophils and other leukocytes to adhere to endothelial cell layers and infiltrate both injured and nearby brain tis-sue [62,63]. Activated neutrophils produce neuro-toxic free radicals, in addition to upregulating inflammatory cytokines and oxidative enzymes like NADPH oxidase and inducible nitric oxide synthase through their oxidative burst response [64]. Mast cells promote BBB changes and promote neuroinflammation in AIS and TBI via the release of substances (histamine, proteases, cytokines) that degrade matrix, recruit and communicate with other immune cells, and alter cerebral blood flow [17]. Infiltrating macrophages and resident microglia of the ‘M1 type’ are also thought to mediate injury, while macrophages/microglia of the ‘M2 type’ are hypothesized to be beneficial in ischemic injury (see ‘The role of microglia in AIS, TBI & neurodegeneration’ section). A decrease in the number of infiltrating macrophages via deletion of MCP-1 (i.e., CCL2) or its receptor results in smaller infarcts and fewer pro-inflammatory molecules (Figure 3) [65,66].
By binding to activated endothelium and entering the brain via BBB injury, CD4+ and CD8+ T cells contribute to damage in both TBI and AIS within the first 24 h post-injury. This implies that T cells are not exerting an adaptive immune response attack, which normally takes days to mobilize, but are contributing to neuro-inflammation immediately via cytotoxic mech-anisms of perforin-mediated apoptosis and the
secretion of IFN-γ [67]. CD4+/CD28- T cells are increased and associated with higher stroke reoccurrence risks and death [68]. Upregulation of MHC-I and MHC-II on neurons facilitates the destructive action of T cells. However, some T-cell types produce protective molecular mediators, assisting in defense and repair [69].
In accordance with the interaction between the peripheral and CNS immune responses in neurodegenerative pathologies, splenectomy has conferred protection in AIS when con-ducted prior to stroke, decreasing lesion vol-ume and reducing the number of T cells, neu-trophils, macrophages and pro-inflammatory cytokines [70]. Splenectomy has also reduced mortality and improved cognition in a rat model of severe TBI [71]. Brain injury itself also interacts with the spleen and other organs. For example, post-TBI, inflammatory cytokines are released in the gut and post-stroke, a reduction in the size of the spleen and thymus has been observed [72]. A recent study using CD74-deficient mice showed neuroprotection, further evidencing peripheral–CNS immune system interactions and a role for peripheral adaptive immunity in TBI pathology [73]. Neuroinflammatory responses observed periph-erally could potentially be used as noninvasive clinical biomarkers in AIS and other neuro-degenerative diseases, using gene-expression profiling obtained from blood samples [74,75].
In MS, demyelinating white matter lesions are invaded by many immune cells including T and B lymphocytes, macrophages, microglia, plasma cells and MHC class II-positive dendritic cells. It is hypothesized that peripheral autore-active T cells infiltrate the CNS and induce an inflammatory milieu that further recruits immune cells that destroy myelin and glial cells while exacerbating inflammation [76]. Therefore, treatments suppressing peripheral immunity help to control symptoms of MS. However, such immuno suppression is detrimental in other neu-rodegenerative diseases, such as AD, as immu-noregulatory cells from the periphery may aid the brain in such diseases [12].
Although a host of molecules facilitate neu-roinflammation, not all molecules produced in response to brain injury are bad. For exam-ple, although activated astrocytes form a glial scar that later inhibits axon regrowth, it ini-tially serves to wall off the site of injury from healthy tissue to protect healthy tissue from pro-inflammatory mediators and debris from

85
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
future science group www.futuremedicine.com
the injury site. Activated astrocytes also produce neuroprotective molecules such as NGF, TGFβ1 and BDNF to assist in repair/growth [5,41].
Additionally, some cytokines are also known to exert protective effects (see ‘Key cytokines in AIS, TBI, and neurodegeneration’ section).
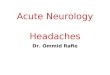
Figure 3. Microglial activation. Microglial activation occurs in response to infection or tissue injury leading to the production of PAMPs and DAMPs, respectively. This activation results in the production of activated microglial phenotypes like M1 and M2. The M1 phenotype is promoted by IFN-γ, while the M2 phenotype is promoted by IL-13 and IL-10 production. The M2 phenotype promotes neuroprotective factors like neurotrophins BDNF and NGF, and anti-inflammatory cytokines. The M1 phenotype promotes neurodegeneration via the release of pro-inflammatory cytokines, ROS, RNS, nitric oxide, excitotoxic factors like glutamate, and results in increased BBB permeability and immune cell recruitment and activation. However, microglial activation is not limited to these two activation types, but is broad, with a spectrum of activation states that continue to be characterized. Synaptic elimination (‘synaptic stripping’) is the removal of dysfunctional synapses by activated microglia. The occurrence of LTD in weaker synapses as well as the presence of molecular signals of cell damage, allow microglia to target such dysfunctional synapses for elimination via phagocytosis. It is possible that some of these interactions are mediated by complement receptor CR3 and the tagging of synapses via C1q, similar to synaptic pruning in early development. BBB: Blood–brain barrier; DAMP: Damage-associated molecular pattern; LTD: Long-term depression; PAMP: Pathogen-associated molecular pattern; RNS: Reactive nitrogen species; ROS: Reactive oxygen species.
Microglia
Activation via PAMPsand DAMPs
Amoeboid M1phenotype
Amoeboid M2phenotype
Neurotoxic factors
Synaptic eliminationvia interaction withcomplement
Excitotoxicity
Neurodegeneration
BBB permeabilityLeukocyte recruitment/activation
Cytotoxicity (via ROS, RNS)Apoptosis (via proteases)
IFN-γ
Pro-inflammatory cytokine release(IL-1, TNF-α, IL-6)
+IL-13IL-10
+
Neurotrophic factorsBDNFNGF
Anti-inflammatory cytokines IL-4IL-10
LTD

Future Neurol. (2016) 11(1)86
REviEW Dugue & Barone
future science group
●● The role of microglia in AIS, TBI & neurodegenerationMicroglia are activated within minutes of an insult to the brain. These cells are the main source of pro-inf lammatory cytokines and chemokines. Microglia express PRRs that sense molecular signals indicating harm (DAMPs and PAMPs), enabling them to initiate the appropri-ate inflammatory response. For example, ATP released from dying and dysregulated cells serves as a chemotactic signal to microglia. In response to neuronal damage in TBI and AIS, rami-fied microglia are activated to their amoeboid form, producing cytotoxic factors like reactive oxygen species, NO, glutamate [77] and hista-mine, pro-inflammatory cytokines like IL-1, TNF-α [78], IL-6 and IFN- γ [79], in addition to neurotrophic and anti-inflammatory cytokines like IL-4, IL-10, BDNF, neurotrophin-3,-4 and -5, and NGF, depending on the signals encoun-tered [80–82]. A protective microglial phenotype can be induced in response to IL-10 and IL-13 stimulation, while a pro-inf lammatory M1 microglial phenotype can be induced via IFN-γ exposure. Pro-inf lammatory cytokines drive apoptosis and cell death, excitotoxicity, increases in BBB permeability and leukocyte infiltration, to contribute to neurodegeneration (see Figure 3 for schematic of microglia activation) [83]. Anti-inflammatory M2 microglial phenotypes can help to remove obstructive myelin debris, deliver trophic factors and recruit oligodendrocyte pre-cursor cells to lesion sites in order to promote remyelination [17,84]. However, such micro-glia activation states operate on a continuum, expressing different degrees of pro- versus anti-inflammatory and immunoregulatory action [85]. For example, when microglia incubated with TGF-β, IFN-γ or IL-10 were added to organo-typic hippocampal slice cultures, there was a sig-nificant decrease in neuronal death implicating these cytokines in the induction of a protective microglia phenotype [67,86]. Similarly, IL-4- as well as low concentration IFN-γ-activated micro-glia primarily promoted oligodendrogenesis and neurogenesis from adult stem cells, respectively. The roles of these different phenotypes can be even more complex for neurodegeneration in AD, as reviewed very recently [87].
The DNA-binding protein HMGB1 is actively released from injured or dying cells and inflammatory cells, binds to the microglial receptor for advanced glycation end products, and thus promotes neurodegeneration via NO
and prostaglandin E2 release [88]. In a mouse model of AIS, the HMGB1 ligand was elevated in ischemic brain tissue, in addition to being elevated in the serum of stroke patients, thus evi-dencing the role of this ligand in the pathophysi-ology of stroke [5]. TLR2 and TLR4 on microglia sense damage in ischemic stroke and exacerbate the infarct via the production of pro-inflamma-tory cytokines. TLR2 activation mainly results in the production of IL-6 and IL-1β release from microglia. TLR4 detects the presence of amy-loid beta (Aβ; peptides significantly involved in Alzheimer’s disease plaques and aging), as well as HSP60 from dying cells in the CNS leading to the production of cytokines and reactive oxygen species that worsen injury [89].
Diffuse TBI injury leads to the presence of activated microglia and elevated cytokine and chemokine levels chronically, for at least 7 days. To induce the inflammatory response from acti-vated microglia, intracellular signaling path-ways are activated in response to injury signals. For example, a recent study examined the role of p38α MAPK, the inflammatory cytokine arm of MAPK signaling, in a model of diffuse TBI. In microglia, p38α MAPK is important in the production of IL-1β and TNF-α and in the phagocytosis of Aβ and axonal debris. In the study, TBI-injured p38α-deficient mice were protected from TBI-related motor defi-cits and synaptic protein loss, but exhibited less activated microglia morphology following injury, and had an increase in the early peak of cytokine and chemokine levels that decreased by day 7 post-TBI. The mixed actions of p38α in chronic microglia activation and the control of cytokine levels attest to the dynamic role of microglia in the immune response following injury [90].
Interestingly in TBI, a distinct rod-like microglial morphology is found throughout the cortex aligning and proliferating in a unique ‘train formation’ in response to injury. Rod microglia, microglia with narrow cell bodies and few polar processes, previously associated with infection, have recently been described in the sterile inflammatory condition of TBI. In a model of diffuse TBI, rod microglia appeared at 1 day post-injury and remained detectable for up to 28 days post-injury. These microglia become significantly elongated on day 1 post-injury and return to sham-injured lengths by day 2. The primary and secondary processes of rod microglia also retracted over the course of

87
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
future science group www.futuremedicine.com
7 days post-injury [91]. These dynamic morpho-logical changes in response to injury probably reflect the active involvement of this microglia type in brain injury. In another study examin-ing microvascular pathology and delayed white matter damage in TBI, activated microglia accu-mulated within the site of injury and migrated over time into neighboring and distal white matter outside of the lesion site. These acti-vated microglia were present as late as 3 months post-injury and found near focal microbleeds despite the fact that the initial injury was local-ized [92]. In TBI patients, activated microglia and neuroinflammation potentially associated with axonal degeneration and tissue atrophy has been observed in the corpus callosum up to 18 years post-injury. This chronic neuroinflam-mation may contribute to the higher incidence of Alzheimer’s disease and dementia in TBI survivors [93].
It has been suggested that with aging, micro-glia are ‘primed’ by previous infections and pathology to elicit a more intense inflammatory response to inflammatory stimuli encountered later in life [17]. Increases in microglial activa-tion have generally been observed in the aging brain and manifest as abnormal, often extreme responses to activating stimuli, thus contribut-ing to neuropathology in the elderly. Some stud-ies have observed increases in the expression of CR3 on microglia, but this is a variable result, perhaps due to region-specific increases in CR3 expression [94]. Increased synaptic loss in neuro-degenerative diseases of the aged could be related to an increase in the activation of microglia via CR3 and to the potential interaction of micro-glial CR3 with C1q complement to eliminate synapses [31].
●● Key cytokines in AIS, TBI & neurodegenerationCytokines are small cell signaling proteins encompassing a wide range of protein families including the tumor necrosis family (TNF-), lymphokines, interleukins (IL-) and interferons (IFN-). In AIS, IL-1β, IL-6, IL-10 and TNF-α are secreted in ischemic brain tissue within the first 24-h. Additional cytokines known to be involved in AIS are IFN- γ, IL-2, IL-4, IL-16, IL-17, granulocyte–macrophage colony stimu-lating factor, TGF-β (also considered to be a growth factor) and recently, IL-9 [2–3,6,35,48]. In TBI, IL-1β, IL-6, IL-10 and TNF-α are among the first cytokines upregulated. Other cytokines
involved in the pathophysiology of TBI include IL-8, granulocyte colony stimulating factor, FAS ligand and MCP-1 [1–2,95]. Many of these cytokines influence the production of other cytokines, alter the BBB and recruit inflamma-tory cells [6,7]. Furthermore, cytokine concen-trations have been associated with behavioral changes following brain injury, such as post-stroke depression and apathy, as well as post-traumatic stress disorder and anxiety [1,8,96–99]. For example, cytokines can affect neurotrans-mitter metabolism of monoamines, serotonin, dopamine and glutamate [100].
InterleukinsInterleukins, IL-1β and IL-18 play a prominent role in the pathology of TBI and AIS. Both IL-1β and IL-18 are activated by the protease caspase-1, activated by the formation of inflammasomes via a host of PRRs, including NLRP1, NLRP3, AIM-2 and RIG-I. The NLRP3 inflamma-some is most often associated with ‘sterile’ or DAMP-associated inflammation, as occurs in brain injury [101]. However, the inflammasomes NLRP1, AIM-2 and NLRC4 have also been implicated in brain injury pathology. A recent study elucidated important contributions of the inflammasomes NLRC4 and AIM-2, as well as the inflammsome component ASC, to ischemic brain injury through the use of knockout mice missing various inflammasome components. NLRC4-/- mice, AIM-2-/- mice and ASC-/- mice showed functional improvement and decreased microglia activation, leukocyte recruitment and infarct volume post-middle cerebral artery occlusion [101]. These observations highlight additional players in sterile injury and the result-ant inflammasome-activated interleukins and caspase.
IL-1β and IL-18 also initiate transcription through NF-κB via their respective receptors on microglia, astrocytes, neurons and other cells. IL-18 helps regulate IFN-γ signaling in T cells and natural killer cells; an IL-18 inhibi-tor administered 1 h after brain injury improved subsequent recovery [24,102]. IL-1β helps to acti-vate microglia and astrocytes, while also pro-moting the production of cytokines like IL-6 and TNF-α [1,10,103]. IL-1β has also been shown to inhibit long-term potentiation in the hip-pocampus, evidencing its ability to interfere with synaptic activity [104].
In AIS, IL-1β is released by activated micro-glia as early as 30 mins after injury. By contrast,

Future Neurol. (2016) 11(1)88
REviEW Dugue & Barone
future science group
mRNA and protein expression studies show a delayed rise and peak in IL-18 post-stroke, at 24–48 h and 6 days respectively [105]. Activated IL-1β stimulates the release of VEGF from locally reactive astrocytes and the release of MMP-9 from NG2-OPCs during the acute phase of injury. IL-1β-specific monoclonal antibodies and IL-1R antagonists (IL-1Ra) have shown protection against brain injury in ischemic stroke. Specifically, IL-1β concen-tration in relation to the concentration of its endogenous inhibitor, IL-1Ra, has been hypoth-esized to be an important factor in the degree of neuroinflammation. IL-1β levels positively cor-relate with increased severity in TBI, AIS and neurodegeneration, and IL-1Ra has exhibited significant brain protective effects [61,106–107]. For example, a small Phase II, double-blind, randomized controlled study indicated that IL-1Ra can cross the BBB to achieve CSF con-centrations in humans previously shown to be neuroprotective in rats, and reduce inflamma-tion following hemorrhagic stroke [108]. Phase II clinical studies using IL-1Ra in severe TBI also proved safety and BBB penetration, while characterizing treated versus control patient cytokine responses [109,110].
The interleukin IL-6 helps to regulate the inflammatory response and has been associated with both neuroprotection and neuroinflam-mation. IL-6 regulates transcription via the JAK/STAT pathway and is a known agonist of VEGF, which alters tight junction proteins to promote disruptions in the BBB and NO production [6,61,111]. The JAK/STAT pathway is integral to NMDA receptor-triggered long-term depression and may contribute to synapse elimination, while another cytokine-activated pathway, the PI3K/Akt pathway may contrib-ute to synapse survival via NMDA receptor-triggered long-term potentiation [54,112]. The balance between such pathways may contribute to synapse survival and improved outcome in TBI and AIS.
Injection of IL-6 in a model of ischemic stroke resulted in a reduction in ischemic damage. Clinical studies have demonstrated that lower IL-10 levels are associated with an increased risk of stroke [35,55]. IL-10 admin-istration reduces ischemic stroke injury and suppresses the expression of TNF-α and IFN-γ [23,113–114]. IL-33, an interleukin cleaved into its active form by inflammasome-induced caspase-1, also confers protection following AIS
by supporting a beneficial Th2 response and decreasing detrimental Th1 and Th17 upregu-lation; when IL-33 was administered to mice, pre-AIS, the neurological score, infarct volume, edema levels, as well as the balance between det-rimental and beneficial T-helper cells improved at 24 and 72 h post-stroke, but not at 6 h post-stroke [115,116]. IL-33 levels assayed in patients within 4.5 h post-stroke were extremely low, while the endogenous IL-33 receptor inhibitor ST2 was high and could be used as an out-come predictor, correlating with worse outcome at 3 months; there was a trend toward better recovery at 24 and 48 h in patients with lower ST2 levels [117].
IL-2, IL-4, IL-17, IFN-γ and TGF-βs have also distinguished themselves in the pathophys-iology of AIS. IL-2 activates immunomodula-tory regulatory T cells that may be potentially beneficial in AIS [60–61,118]. IL-4 also activates astrocytes to produce BDNF, decreases the levels of TNF-α produced by microglia, and increases TGF-β2, while promoting an anti-inflamma-tory microglial phenotype that may be reli-ant on TGF-β signaling (inhibition of TGF-β receptor I also reduced IL-4-induced microglia activation, while addition of TGF-β1 upregu-lated IL-4 receptor α on microglia) [69,119]. Excessive microglia activation was decreased via the TGF-β1:microglial TGF-β receptor I interaction in an in vitro model of PD, while another in vitro model demonstrated the abil-ity of TGF-β1 to reduce IFN-γ-induced neu-rodegeneration and IFN-γ signaling/microglia promotion [120,121].
In a study by Stoll et al., TGF-β1 rapidly rose post-ischemia (within 16 h and was sus-tained for at least 7 days) along with phago-cytic microglia, in contrast to TGF-β2, which did not increase until day 14 and 28 post-injury and appeared in active astrocytes along the infarct perimeter post-microglia and macrophage invasion; when TGF-β2 was applied to an assay for Wallerian degenera-tion in the CNS, the ability of local microglia to phagocytose myelin was reduced [122]. As with all cytokines involved in neurodegen-erative disease pathology, time course is an important factor in assessing whether a mol-ecule is contributing positively or negatively to recovery from injury and should be considered when determining appropriate inflammation-modifying treatments and their dosing. The time course of TGF-βs’ expression contribute

89
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
future science group www.futuremedicine.com
to the timing of microglia activation states as evidenced by these observations and may be important when determining when and how to employ treatment strategies that modulate TGF-βs, such as minocycline, a drug now in Phase I clinical trials for severe TBI [123].
IL-9, granulocyte colony stimulating fac-tor and granulocyte–macrophage colony stimulating factor may also potentially ben-efit AIS pathology via anti-apoptotic mecha-nisms [65,124–125]. In contrast, IL-17 is largely produced by γδ T cells in the ischemic brain, promotes the production of inf lammatory cytokines from macrophages and disrupts the BBB via upregulation of MMPs and ICAM-1. Preclinical studies have shown IL-17 to be detri-mental in AIS via calpain (a cysteine protease)-mediated proteolysis. IL-17 knockout mice and treatments blocking IL-17 in an animal model of AIS resulted in a decrease in infarct size and neurological improvements, in addition to a decrease in calpain activation [62,126]. Clinical evaluation of γδ T cells in stroke showed a large decrease (∼50%) in the number of circulating γδ T cells; decreases were also associated with hypertension (∼65%), coronary artery disease and advanced age. However, the γδ T cells present expressed more IL-17 [127].
TNF-αTNF-α is produced by microglia, astrocytes, endothelial cells and neurons. It binds to TNFR1, a TNF receptor expressed on all cell types that mediates cell death via activation of caspase-8, caspase-10 and pro-apoptotic proteins through the formation of com-plex II. Complex II formation is the TNF receptor-associated death domain adaptor protein ‘TRADD’ complexed with TNFR1 and Fas-associated death domain protein. In contrast, TNF-α can also mediate cell sur-vival via NF-κB-mediated transcription of anti-apoptotic proteins initiated by complex I formation (i.e., TRADD associated with TNFR1, TNF receptor-associated proteins 2/5, cellular inhibitor of apoptosis proteins 1/2, ubiquitin-conjugating enzyme 13 and receptor-interacting protein); TNF-α also binds to the less abundant TNFR2 which induces antiapop-totic signaling pathways via NF-κB-mediated transcription [128].
TNF-α has been implicated in the regula-tion of microglial activation, as well as gluta-matergic glial and synaptic transmission [129].
Even peripherally produced TNF-α can affect inflammation in the CNS; a recent study showed that peripheral TNF-α induced the microglial production of MCP-1/CCL2 to recruit mono-cytes into the CNS [130]. Peripheral TNF-α is also known to induce leukocyte rolling and adhesion in cerebral vasculature via E- and P-selectins [131]. When administered by intrac-erebroventricular injection in an experimental model of AIS, TNF-α exacerbated the infarct in a dose-related manner that was reversed by administration of TNF-α monoclonal anti-body. Administration of soluble TNFR1 alone, applied to the brain to sequester released TNF-α, also reduced AIS injury [4,6,132]. AIS-induced TNF-α in endothelial cells and leukocytes upregulates MMP-9, thus exacerbating BBB permeability, allowing leukocytes and serum proteins like proteases, immunoglobulins and thrombin to enter the CNS and contribute to extracellular matrix destruction and brain injury [133–137]. Normalization of TNF-α levels by treatment with an analog of thalidomide in a rat model of chronic neuroinflammation resulted in decreased TLR-mediated signal-ing associated with microglia activation and improved cognitive function as indicated by improved performance in the Morris water maze task and the novel object recognition task [4,138–139]. Experiments using a TNF-α decoy receptor resulted in reduced infarct volumes and neural deficits post-ischemia, evidencing the destructive role of TNF-α. Furthermore, improvements in post-stroke cog-nitive dysfunction and TBI have been reported from the recent off-label clinical use of etaner-cept, an anti-TNF-α monoclonal antibody, when administered perispinally [26,140].
The loss of neurons in AIS and TBI results in a loss of inhibitory signals that help to control the production of pro-inflammatory cytokines and neurotoxins [26]. Numerous cytokines are produced and can be detected clinically in cerebrospinal fluid and serum; clinical studies still seek to determine definitive cytokine and molecular biomarkers for injury severity [48]. A number of studies are now examining how single nucleotide polymorphisms (SNPs) in cytokines and other markers can affect the duration and severity of the neuroinflammatory response in addition to informing diagnoses and prognoses in TBI and AIS [141–144].
Associations between clinical outcomes as assessed by the Glasgow outcome scale 6 months

Future Neurol. (2016) 11(1)90
REviEW Dugue & Barone
future science group
following TBI and cytokine gene polymor-phisms found that TNF-α -308 SNP allele 2 carriers had a worse outcome at 6 months post-injury than noncarriers. This SNP is found in the promoter region of the gene and increases TNF-α transcription [144]. The investigation of cytokine actions, as well as variations in cytokine genes and concentrations, show the importance of these immunomodulatory mol-ecules in TBI and AIS. Further research on cytokines, genetic polymorphisms influencing inflammation, and mechanisms of neuroin-flammation will assist in our understanding of neurodegenerative disease, its pathologi-cal sequela, and individualized approaches to treatment.
●● Timing & location as factors in post-injury recoveryKey factors in facilitating recovery post-injury are the spatiotemporal nature and relative contributions of inflammatory cells and mol-ecules [145]. These factors should also be con-sidered in identifying effective treatments. For example, a study on the role of TNF-α in TBI using TNF-/- mice showed better motor function within the first 48 h post-injury than wild-type mice, but demonstrated larger amounts of cor-tical tissue loss and comparatively worse motor function at 2 and 4 weeks post-injury as com-pared with wild-type mice [146]. These results can inform how TNF-α inhibitors could be used post-injury.
The close evaluation of timing and location of inflammatory responses gives insight into the development of cell- or location-specific targeted treatments, in addition to the timing and dos-ing of drugs. Clinical evaluation of high-dose corticosteroids for the treatment of TBI in the CRASH study, proved that total inhibition of neuroinflammation could be harmful [147]. Drugs attempting to target inflammation must carefully consider timing, dosing and duration of drug administration, as well as the injury-dependent heterogeneity of the inflammatory response. These factors could have contributed to the fail-ure of drugs attempting to target inflammation, such as the PRoTECT III and SyNAPSe clinical trials assessing progesterone for TBI treatment and the Enlimomab Acute Stroke Trial.
ConclusionThis review has discussed the immune sys-tem in the periphery versus the CNS, and has
examined the role of complement, inflammas-omes and immune cells in AIS, TBI and neu-rodegenerative diseases. We hope that by pro-viding a focus on the roles/actions of immune mediators and cells, this review helps to provide a framework to identify opportunities for reduc-ing brain injury and neurodegeneration in the future. Some examples of approaches for use in the clinic have been included above and follow (see the ‘Future perspective’ section).
Future perspectiveIt will be important to address neuroinflam-matory cascades in the development of future therapeutics for brain protection, as well as in the determination of effective biomarkers of injury severity and post-injury dysfunction for early clinical monitoring. In order to elu-cidate the pathology of TBI and AIS, as well as other neurodegenerative diseases, the role of immune cells and mediators (both positive and negative) in the CNS and periphery must be considered. Clearly there are issues with early versus delayed interference with neuroinflam-mation. Furthermore, due to the complex role of inflammatory mediators like cytokines and chemokines in the evolution of brain injury, it is necessary to characterize the time course, concentrations, multiple receptor effects and interactions of such substances. Generally, blocking early inflammatory changes can pro-tect the brain, but later interventions might interfere with reparative processes that require inflammatory mediators. Post-injury changes in circulating immune cells might also pro-vide additional, novel opportunities for inter-vention. More research needs to be done to understand this.
The role of the complement cascade and its degree of activation in individual neuro-degenerative diseases warrants more detailed investigation. Research should also exam-ine targeting infiltrating macrophages and endogenous microglia to promote reduced inf lammatory/increased anti-inf lammatory phenotypes. Patient data attempting to iden-tify and correlate inflammatory biomarkers to brain injury and neurodegeneration should be based upon preclinical studies and interpreted alongside clinical data to maximize translation of results. Thus, inflammatory cells and their contents marking phenotypic changes could serve as prognostic/diagnostic markers in CNS disease. Additionally, the potential use of new

91
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
future science group www.futuremedicine.com
or existing clinically used monoclonal antibod-ies and biologics could be further explored to modulate cytokine levels in brain injury and neurodegenerative diseases, as inhibition of specif ic pro-inf lammatory cytokines may improve outcomes. Again, the timing of such interventions will be critical to their efficacious use. It will be important to identify combi-nation therapeutic targeted approaches that provide improved outcomes. In order to bet-ter develop questions and discover meaning-ful answers to the challenge of brain ischemia, trauma and neurodegeneration, we must con-tinue to integrate and translate findings from
diverse fields of medical research, while exam-ining diseases individually for appropriate new intervention opportunities.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
EXECUTivE SUMMARYThe innate immune system in the periphery versus the CNS
● Innate immunity involves the detection of pathogen-associated molecular patterns and damage-associated molecular patterns by soluble and effector cell bound pattern recognition receptors in both the periphery and the CNS.
● The blood–brain barrier (BBB), the blood–cerebrospinal fluid barrier and the meningeal lymphatic system regulate the degree to which the peripheral immune system and the CNS interact.
The complement system
● The complement system has three main activation pathways (the classical, alternative and lectin pathways) that culminate in the formation of a membrane attack complex to lyse pathogens and abnormal cells. This system is implicated in development and neurodegenerative disease since it tags synapses with complement factors for elimination (termed ‘synaptic pruning’ in development).
● Following brain injury, complement factors are upregulated by both neurons and neuroglia. Knockout mice have elucidated the contribution of complement to brain injury and neurodegenerative diseases; C3-/- mice had smaller ischemic stroke infarcts and better neurological function after stroke; C5-/- mice also exhibited protection from brain injury. Complement downregulatory proteins and inhibitors protect the brain from injury, while increases in C1q and C3 levels correlate with increased injury.
Key cytokines & immune players in brain injury & neurodegeneration
● Tissue injury and BBB disruption in neurodegenerative disease disrupts brain homeostasis, causing astrogliosis (excessive proliferation/activation of astrocytes), activation of microglia and an influx of immune cells, all of which produce both pro- and anti-inflammatory substances. The balance and timing of pro- versus anti-inflammatory substances and actions influence the severity of injury.
● Microglia have a spectrum of activation states in response to pathogen-associated molecular patterns and damage-associated molecular patterns detected by their pattern recognition receptors. Microglial activation phenotypes can range from helping to remove debris from tissue injury, producing trophic factors and promoting axonal remyelination, to producing pro-inflammatory cytokines that encourage apoptosis, increased BBB permeability and detrimental neuroinflammation. These phenotypes are induced by microvascular injury, leukocyte infiltration and exposure to various cytokines and signaling molecules.
● Major inflammatory cytokines involved in traumatic brain injury, acute ischemic stroke and neurodegeneration include interleukins IL-1β and IL-18 and TNF- α. IL-1β and IL-18 are released upon activation via inflammasome formation (a multi-molecular complex that releases pro-inflammatory cytokines and promotes cell death via apoptosis and pyroptosis) and are linked to increased injury severity, BBB permeability and decreased synaptic activity. TNF-α primarily promotes cell death via pro-apoptotic caspase activation upon binding to its receptor, TNFR1. Other key cytokines that can play an anti-inflammatory role in traumatic brain injury, acute ischemic stroke and neurodegeneration include IL-33, IL-6, IL-10 and IL-4.

Future Neurol. (2016) 11(1)92
REviEW Dugue & Barone
future science group
ReferencesPapers of special note have been highlighted as: • of interest; •• of considerable interest
1 Parham P. The Immune System Ch.1 Elements of the immune system and their roles in defense, Ch.2 Innate immunity (3rd Edition). Foltin J (Ed.). Garland Science, NY, USA (2000).
2 Turvey SE, Broide DH. Innate immunity. J. Allergy Clin. Immun. 125(2), S24–S32 (2010).
3 Shastri A, Bonifati DM, Kishore U. Innate immunity and neuroinflammation. Mediators Inflamm. 2013(6), 1–19 (2013).
4 Kigerl KA, de Rivero Vaccari JP, Dietrich WD, Popovich PG, Keane RW. Pattern recognition receptors and central nervous system repair. Exp. Neurol. 258, 5–16 (2014).
5 Muhammad S, Barakat W, Stoyanov S et al. The HMGB1 receptor RAGE mediates ischemic brain damage. J. Neurosci. 28(46), 12023–12031 (2008).
6 Ransohoff RM, Brown MA. Innate immunity in the central nervous system. J. Clin. Invest. 122(4), 1164–1171 (2012).
7 Ghirnikar RS, Lee YL, Eng LF. Inflammation in traumatic brain injury: role of cytokines and chemokines. Neurochem. Res. 23(3), 329–340 (1998).
8 Swardfager W, Winer DA, Herrmann N, Winer S, Lanctôt KL. Interleukin-17 in post-stroke neurodegeneration. Neurosci. Biobehav. Rev. 37(3), 436–447 (2013).
9 Barone FC, Feuerstein GZ. Inflammatory mediators and stroke: new opportunities for novel therapeutics. J. Cereb. Blood Flow Metab. 19(8), 819–834 (1999).
10 Alexander JJ, Anderson AJ, Barnum SR, Stevens B, Tenner AJ. The complement cascade: Yin-Yang in neuroinflammation – neuro-protection and -degeneration. J. Neurochem. 107(5), 1169–1187 (2008).
11 Liddelow SA. Development of the choroid plexus and blood–CSF barrier. Front. Neurosci. 9(154), 319–313 (2015).
12 Schwartz M, Baruch K. Breaking peripheral immune tolerance to CNS antigens in neurodegenerative diseases: boosting autoimmunity to fight-off chronic neuroinflammation. J. Autoimmun. 54, 8–14 (2014).
•• Anexplorationof‘protectiveautoimmunity’asatooltoattenuateacuteandchronicneuroinflammatoryconditions;studiesobservingtheperipheralautoimmuneresponseagainstCNSantigensasamediatorofneuroprotectionandtheadaptiveimmunesystem’stargetedrolein
normalbrainfunctionandplasticityarediscussed.
13 Baruch K, Schwartz M. CNS-specific T cells shape brain function via the choroid plexus. Brain Behav. Immun. 34, 11–16 (2013).
14 Louveau A, Smirnov I, Keyes TJ et al. Structural and functional features of central nervous system lymphatic vessels. Nature 523(7560), 337–341 (2015).
15 Shechter R, Miller O, Yovel G et al. Recruitment of beneficial M2 macrophages to injured spinal cord is orchestrated by remote brain choroid plexus. Immunity 38(3), 555–569 (2013).
16 Veerhuis R, Nielsen HM, Tenner AJ. Complement in the brain. Mol. Immunol. 48(14), 1592–1603 (2011)
17 Skaper SD, Facci L, Giusti P. Mast cells glia and neuroinflammation: partners in crime? Immunology 141(3), 314–327 (2014).
18 Wake H, Moorhouse AJ, Nabekura J. Functions of microglia in the central nervous system – beyond the immune response. Neuron Glia Biol. 7(1), 47–53 (2012).
19 Baroja-Mazo A, Martín-Sánches F, Gomez AI et al. The NLRP3 inflammasome is released as a particulate danger signal that amplifies the inflammatory response. Nat. Immunol. 15(8), 738–748 (2014).
20 Franklin BS, Bossaller L, De Nardo D et al. The adaptor ASC has extracellular and ‘prionoid’ activites that propagate inflammation. Nat. Immunol. 15(8), 727–737 (2014).
21 Adamczak S, Dale G, de Rivero Vaccari JP, Bullock MR, Dietrich WD, Keane RW. Inflammasome proteins in cerebrospinal fluid of brain-injured patients as biomarkers of functional outcome. J. Neurosurg. 117(6), 1119–1125 (2012).
22 Oikonomopoulou K, Ricklin D, Ward PA, Lambris JD. Interactions between coagulation and complement – their role in inflammation. Semin. Immunopathol. 34(1), 151–165 (2011).
23 Bonifati DM, Kishore U. Role of complement in neurodegeneration and neuroinflammation. Mol. Immunol. 44(5), 999–1010 (2007).
24 Rittirsch D, Redl H, Huber-Lang M. Role of complement in multiorgan failure. Clin. Dev. Immunol. 2012(7), 1–10 (2012)
25 Stephan AH, Barres BA, Stevens B. The complement system: an unexpected role in synaptic pruning during development and disease. Annu. Rev. Neurosci. 35(1), 369–389 (2012)
26 Amor S, Peferoen LAN, Vogel DYS et al.
Inflammation in neurodegenerative diseases – an update. Immunology 142(2), 151–166 (2014).
27 Pavlovski D, Thundyil J, Monk PN, Wetsel RA, Taylor SM, Woodruff TM. Generation of complement component C5a by ischemic neurons promotes neuronal apoptosis. FASEB J. 26(9), 3680–3690 (2012).
28 Mastellos DC. Complement emerges as a masterful regulator of CNS homeostasis, neural synaptic plasticity, and cognitive function. Exp. Neurol. 261, 469–474 (2014).
•• Reviewsrecentworkexaminingcomplement’sroleinsynaptogenesis,neuralplasticity,microgliarecruitment,synaptictaggingandneurogenesisinthehealthyandinjuredCNS.
29 Moriyama M, Fukuhara T, Britschgi M et al. Complement receptor 2 is expressed in neural progenitor cells and regulates adult hippocampal neurogenesis. J. Neurosci. 31(11), 3981–3989 (2011).
30 Stevens B, Allen NJ, Vazquez LE et al. The classical complement cascade mediates CNS synapse elimination. Cell 131(6), 1164–1178 (2007)
31 Schafer DP, Stevens B. Synapse elimination during development and disease: immune molecules take centre stage. Biochem. Soc. Trans. 38(2), 476 (2010)
32 Dietrich WD, Alonso O, Halley M. Early microvascular and neuronal consequences of traumatic brain injury: a light and electron microscopic study in rats. J. Neurotraum. 11(3), 289–301 (1994).
33 McConeghy KW, Hatton J, Hughes L, Cook AM. A review of neuroprotection pharmacology and therapies in patients with acute traumatic brain injury. CNS Drugs 26(7), 613–636 (2012)
34 Esiri M. The interplay between inflammation and neurodegeneration in CNS disease. J. Neuroimmunol. 184(1–2), 4–16 (2007).
35 Deb P, Sharma S, Hassan KM. Pathophysiologic mechanisms of acute ischemic stroke: An overview with emphasis on therapeutic significance beyond thrombolysis. Pathophysiology 17(3), 197–218 (2010).
36 Van Beek J, Bernaudin M, Petit E et al. Expression of receptors for complement anaphylatoxins C3a and C5a following permanent focal cerebral ischemia in the mouse. Exp. Neurol. 161(1), 373–382 (2000).
37 Vasthare US, Barone FC, Sarau HM et al. Complement depletion improves neurological function in cerebral ischemia. Brain Res. Bull. 45(4), 413–419 (1998).

93future science group www.futuremedicine.com
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
38 Mocco J, Mack WJ, Ducruet AF, Sosunov SA, Sughrue M, Hassid BG. Complement component C3 mediates inflammatory injury following focal cerebral ischemia. Circ. Res. 99(2), 209–217 (2006).
39 Aeinehband S, Lindblom RPF, Al Nimer F et al. Complement component C3 and butyrylcholinesterase activity are associated with neurodegeneration and clinical disability in multiple sclerosis. PLoS ONE 10(4), 1–13 (2015).
40 Arumugam TV, Tang S-C, Lathia JD et al. Intravenous immunoglobulin (IVIG) protects the brain against experimental stroke by preventing complement-mediated neuronal cell death. Proc. Natl Acad. Sci. USA 104(35), 14104–14109 (2007)
41 De Simoni MG, Storini C, Barba M et al. Neuroprotection by complement (C1) inhibitor in mouse transient brain ischemia. J. Cereb. Blood Flow Metab. 23(2), 232–239 (2003).
42 Arumugam TV, Magnus T, Woodruff TM, Proctor LM, Shiels IA, Taylor SM. Complement mediators in ischemia – reperfusion injury. Clin. Chim. Acta 374(1–2), 33–45 (2006).
43 Albert-Weißenberger C, Sirén A-L, Kleinschnitz C. Ischemic stroke and traumatic brain injury: the role of the kallikrein-kinin system. Prog. Neurobiol. 101–102, 65–82 (2013).
44 Stahel PF, Morganti-Kossmann C, Perez D et al. Intrathecal levels of complement-derived soluble membrane attack complex (sC5b-9) correlate with blood–brain barrier dysfunction in patients with traumatic brain injury. J. Neurotraum. 18(8), 773–781 (2001).
45 Széplaki G, Szegedi R, Hirschberg K et al. Strong complement activation after acute ischemic stroke is associated with unfavorable outcomes. Atherosclerosis 204(1), 315–320 (2009).
46 Pedersen ED, Aass HCD, Rootwelt T, Fung M, Lambris JD, Mollnes TE. CD59 efficiently protects human NT2-N neurons against complement-mediated damage. Scand. J. Immunol. 66(2–3), 345–351 (2007).
47 Zhang J, Malik A, Choi HB, Ko RWY, Dissing-Olesen L, MacVicar BA. Microglial CR3 activation triggers long-term synaptic depression in the hippocampus via NADPH oxidase. Neuron 82(1), 195–207 (2014).
48 Ormstad H, Aass HCD, Lund-SØrensen N, Amthor K-F, Sandvik L. Serum levels of cytokines and C-reactive protein in acute ischemic stroke patients, and their relationship to stroke lateralization, type, and infarct volume. J. Neurol. 258(4), 677–685 (2011).
49 Michailidou I, Willems JGP, Kooi E-J et al. Complement C1q–C3-associated synaptic changes in multiple sclerosis hippocampus. Ann. Neurol. 77(6), 1007–1026 (2015).
50 Stephan AH, Madison DV, Mateos JM et al. A dramatic increase of C1q protein in the CNS during normal aging. J. Neurosci. 33(33), 13460–13474 (2013).
51 Fonseca MI, Zhou J, Botto M, Tenner AJ. Absence of C1q leads to less neuropathology in transgenic mouse models of Alzheimer’s disease. J. Neurosci. 24(29), 6457–6465 (2004).
52 Depboylu C, Schorlemmer K, Klietz M et al. Upregulation of microglial C1q expression has no effects on nigrostriatal dopaminergic injury in the MPTP mouse model of Parkinson disease. J. Neuroimmunol. 236(1–2), 39–46 (2011).
53 Duff J, Yarnall A, Burn DJ, Hudson G, Hudson G. Variation in complement protein C1q is not a major contributor to cognitive impairment in Parkinson’s disease. Neurosci. Lett. 594(6), 66–69 (2015).
54 Heneka MT, Rodríguez JJ, Verkhratsky A. Neuroglia in neurodegeneration. Brain Res. Rev. 63(1–2), 189–211 (2010).
55 Allaman I, Bélanger M, Magistretti PJ. Astrocyte-neuron metabolic relationships: for better and for worse. Trends Neurosci. 34(2), 76–87 (2011).
56 Clark RK, Lee EV, Fish CJ et al. Development of tissue damage, inflammation and resolution following stroke: an immunohistochemical and quantitative planimetric study. Brain Res. Bull. 31(5), 565–572 (1993).
57 Sofroniew MV. Multiple roles for astrocytes as effectors of cytokines and inflammatory mediators. Neuroscientist 20(2), 160–172 (2014).
58 Barreto GE. Astrocytic modulation of blood brain barrier: perspectives on Parkinson’s disease. Front Cell Neurosci. 211(8), 1–11 (2014).
59 Cabezas R, Ávila M, Gonzalez J et al. Astrocytic modulation of blood brain barrier: perspectives on Parkinson’s disease. Front Cell Neurosci. 211(8), 1–11 (2014).
60 Hughes EG, Kang SH, Fukaya M, Bergles DE. Oligodendrocyte progenitors balance growth with self-repulsion to achieve homeostasis in the adult brain. Nat. Neurosci. 16(6), 668–676 (2013).
61 Helmy A, De Simoni M-G, Guilfoyle MR, Carpenter KLH, Hutchinson PJ. Cytokines and innate inflammation in the pathogenesis of human traumatic brain injury. Prog. Neurobiol. 95(3), 352–372 (2011).
62 Werner C, Engelhard K. Pathophysiology of traumatic brain injury. Br. J. Anaesth. 99(1), 4–9 (2007).
63 Iadecola C, Anrather J. The immunology of stroke: from mechanisms to translation. Nature 17(7), 796–808 (2011).
• Exploresthepathophysiologyofstrokewithafocusonthecontributionoftheadaptiveandinnateimmunesystem.
64 Liao Y, Liu P, Guo F, Zhang Z-Y, Zhang Z. Oxidative burst of circulating neutrophils following traumatic brain injury in human. PLoS ONE 8(7), e68963 (2013).
65 Xu X, Jiang Y. Review article: the yin and yang of innate immunity in stroke. Biomed Res. Int. 2014, 1–8 (2014).
66 Jha MK, Lee W-H, Suk K. Functional polarization of neuroglia: implications in neuroinflammation and neurological disorders. Biochem. Pharmacol. doi:10.1016/j.bcp.2015.11.003. (2015) (Epub ahead of print).
67 Yilmaz G, Arumugam TV, Stokes KY, Granger DN. Role of T lymphocytes and interferon-γ in ischemic stroke. Circ. Res. 113(17), 2105–2112 (2006).
68 Hallenbeck JM, Dambrosia J, Barker JL, Baird AE. Elevated pro-inflammatory CD4+ CD28- lymphocytes and stroke recurrence and death. Neurology 63(8), 1446–1451 (2004).
69 Butovsky O, Ziv Y, Schwartz A et al. Microglia activated by IL-4 or IFN-γ differentially induce neurogenesis and oligodendrogenesis from adult stem/progenitor cells. Mol. Cell Neurosci. 31(1), 149–160 (2006).
70 Zhang B-J, Men X-J, Lu Z-Q, Li H-Y, Qiu W, Hu X-Q. Splenectomy protects experimental rats from cerebral damage after stroke due to anti-inflammatory effects. Chin. Med. J. 126(12), 2354–2360 (2013).
71 Li M, Li F, Luo C et al. Immediate splenectomy decreases mortality and improves cognitive function of rats after severe traumatic brain injury. J. Trauma 71(1), 141–147 (2011).
72 Stein DG, Geddes RI, Sribnick EA. Recent developments in clinical trials for the treatment of traumatic brain injury. Handb. Clin. Neurol. 127, 433–451 (2015).
73 Tobin RP, Mukherjee S, Kain JM et al. Traumatic brain injury causes selective, CD74-dependent peripheral lymphocyte activation that exacerbates neurodegeneration. Acta Neuropathol. Commun. 143(2), 1–10 (2016).
74 Baird AE. Blood genomics in human stroke. Stroke 38(2 Suppl.), 694–698 (2007).

Future Neurol. (2016) 11(1)94
REviEW Dugue & Barone
future science group
75 Moore DF, Li H, Jeffries N et al. Using peripheral blood mononuclear cells to determine a gene expression profile of acute ischemic stroke: a pilot investigation. Circulation 111(2), 212–221 (2005).
76 Hemmer B, Kerschensteiner M, Korn T. Role of the innate and adaptive immune responses in the course of multiple sclerosis. Lancet Neurol. 14(4), 406–419 (2015).
•• Describesthepathophysiologyandroleoftheinnateandadaptiveimmunesystemintheearlyversusprogressivestagesofmultiplesclerosis.
77 Kingham PJ, Cuzner ML, Pocock JM. Apoptotic pathways mobilized in microglia and neurones as a consequence of chromogranin A‐induced microglial activation. J. Neurochem. 73(2), 538–547 (1999).
78 Combs CK, Karlo JC, Kao SC, Landreth GE. β-amyloid stimulation of microglia and monocytes results in TNFα-dependent expression of inducible nitric oxide synthase and neuronal apoptosis. J. Neurosci. 21(4), 1179–1188 (2001).
79 Suzuki Y, Claflin J, Wang X, Lengi A, Kikuchi T. Microglia and macrophages as innate producers of interferon-gamma in the brain following infection with Toxoplasma gondii. Int. J. Parasitol. 35(1), 83–90 (2005).
80 Kim OS, Lee CS, Kim HY, Joe E, Jou I. Characterization of new microglia-like cells obtained from neonatal rat brain. Biochem. Biophys. Res. Commun. 328(1), 281–287 (2005).
81 Ekdahl CT, Kokaia Z, Lindvall O. Review: brain inflammation and adult neurogenesis: the dual role of microglia. Neuroscience 158(3), 1021–1029 (2009).
82 Kettenmann H, Kirchhoff F, Verkhratsky A. Microglia: new roles for the synaptic stripper. Neuron 77(1), 10–18 (2013).
83 Liguz-Lecznar M, Kossut M. Influence of Inflammation on poststroke plasticity. Neural Plast. 2013(7), 1–9 (2013).
84 Hernandez-Ontiveros DG, Tajiri N, Acosta S, Giunta B, Tan J, Borlongan CV. Microglia activation as a biomarker for traumatic brain injury. Front Neurol. 4(30), 1–9 (2013).
• Explainstraumaticbraininjurypathophysiology,theroleofmicrogliaandtheinflammatorystatethatmaypersistyearspostinjury.Theprotectiveversusharmfulfunctionsofmicrogliaandbiomarkersbasedonmicrogliacellsareexplored.
85 Heppner FL, Ransohoff RM, Becher B. Immune attack: the role of inflammation in
Alzheimer disease. Nat. Rev. Neurosci. 16(6), 358–372 (2015). .
•• AdiscussionofneuroinflammationinAlzheimer’sdisease;theroleof‘CNS-residentimmunecells’,especiallymicrogliainthepathologyofAlzheimer’sdiseaseandneuroinflammatorytargetsfortherapeuticintervention,manyofwhichareproducedbyorinteractwithmicroglia,arereviewed
86 Kipnis J, Avidan H, Caspi RR, Schwartz M. Dual effect of CD4+CD25+ regulatory T cells in neurodegeneration: a dialogue with microglia. Proc. Natl Acad. Sci. USA 101(Suppl. 2), 14663–14669 (2004).
87 ElAli A, Rivest S. Microglia in Alzheimer’s disease: a multifaceted relationship. Brain Behav. Immun. doi:10.1016/j.bbi.2015.07.021 (2015) (Epub ahead of print).
88 Verkhratsky A, Butt AM. Glial Physiology and Pathophysiology. Wiley Blackwell, Oxford, UK (2013).
89 Harry GJ. Microglia during development and aging. Pharmacol. Ther. 139(3), 313–326 (2013).
90 Bachstetter AD, Rowe RK, Kaneko M, Goulding D, Lifshitz J, Van Eldik LJ. The p38 MAPK regulates microglial responsiveness to diffuse traumatic brain injury. J. Neurosci. 33(14), 6143–6153 (2013).
91 Taylor SE, Morganti-Kossmann C, Lifshitz J, Ziebell JM. Rod microglia: a morphological definition. PLoS ONE 9(5), e97096 (2014).
92 Glushakova OY, Johnson D, Hayes RL. Delayed increases in microvascular pathology after experimental traumatic brain injury are associated with prolonged inflammation, blood–brain barrier disruption, and progressive white matter damage. J. Neurotraum. 31(13), 1180–1193 (2014).
93 Johnson VE, Stewart JE, Begbie FD, Trojanowski JQ, Smith DH, Stewart W. Inflammation and white matter degeneration persist for years after a single traumatic brain injury. Brain 136(1), 28–42 (2013).
94 Conde JR, Streit WJ. Microglia in the aging brain. J. Neuropathol. Exp. Neurol. 65(3), 199–203 (2006).
95 Ziebell JM, Morganti-Kossmann MC. Involvement of pro- and anti-inflammatory cytokines and chemokines in the pathophysiology of traumatic brain injury. Neurotherapeutics 7(1), 22–30 (2010).
96 Pascoe MC, Crewther SG, Carey LM, Crewther DP. Inflammation and depression: why poststroke depression may be the norm and not the exception. Int. J. Stroke 6(2), 128–135 (2011).
97 Wohleb ES, Patterson JM, Sharma V, Quan N, Godbout JP, Sheridan JF. Knockdown of interleukin-1 receptor type-1 on endothelial cells attenuated stress-induced neuroinflammation and prevented anxiety-like behavior. J. Neurosci. 34(7), 2583–2591 (2014).
98 Swardfager W, Herrmann N, Andreazza AC et al. oststroke neuropsychiatric symptoms: relationships with IL-17 and oxidative stress. Biomed. Res. Int. 245210, 1–6 (2014).
99 Spalletta G, Cravello L, Imperiale F et al. Neuropsychiatric symptoms and interleukin-6 serum levels in acute stroke. J. Neuropsychiatry Clin. Neurosci. 25(4), 255–263 (2013).
100 Haroon E, Raison CL, Miller AH. Psychoneuroimmunology meets neuropsychopharmacology: translational implications of the impact of inflammation on behavior. Neuropsychopharmacology 37(1), 137–162 (2011).
101 Kinoshita T, Imamura R, Kushiyama H, Suda T. NLRP3 mediates NF-κB activation and cytokine induction in microbially induced and sterile inflammation. PLoS ONE 10(3), e0119179 (2015).
102 Denes A, Coutts G, Lénárt N et al. AIM2 and NLRC4 inflammasomes contribute with ASC to acute brain injury independently of NLRP3. Proc. Natl Acad. Sci. USA 112(13), 4050–4055 (2015).
103 Yatsiv I, Morganti-Kossmann MC, Perez D et al. Elevated intracranial IL-18 in humans and mice after traumatic brain injury and evidence of neuroprotective effects of IL-18-binding protein after experimental closed head injury. J. Cereb. Blood Flow Metab. 22(8), 971–978 (2002).
104 Walsh JG, Muruve DA, Power C. Inflammasomes in the CNS. Nat. Rev. Neurosci. 15(2), 84–97 (2014).
105 Cunningham AJ, Murray CA, O’Neill LA, Lynch MA, O’Connor JJ. Interleukin-1β (IL-1β) and tumour necrosis factor (TNF) inhibit long-term potentiation in the rat dentate gyrus in vitro. Neurosci. Lett. 203(1), 17–20 (1996).
106 Rothwell N, Allan S, Toulmond S. The role of interleukin 1 in acute neurodegeneration and stroke: pathophysiological and therapeutic implications. J. Clin. Invest. 100(11), 2648–2652 (1997).
107 Allan SM, Tyrrell PJ, Rothwell NJ. Interleukin-1 and neuronal injury. Nat. Rev. Immunol. 5(8), 629–640 (2005).
108 Singh N, Hopkins SJ, Hulme S et al. The effect of intravenous interleukin-1 receptor antagonist on inflammatory mediators in

95future science group www.futuremedicine.com
Ischemic, traumatic & neurodegenerative brain inflammatory changes REviEW
cerebrospinal fluid after subarachnoid haemorrhage: a Phase II randomised controlled trial. J. Neuroinflammation 11, 1 (2014).
109 Helmy A, Guilfoyle MR, Carpenter KL, Pickard JD, Menon DK, Hutchinson PJ. Recombinant human interleukin-1 receptor antagonist in severe traumatic brain injury: a Phase II randomized control trial. J. Cereb. Blood Flow Metab. 34(5), 845–851 (2014).
110 Helmy A, Guilfoyle MR, Carpenter KL, Pickard JD, Menon DK, Hutchinson PJ. Recombinant human interleukin-1 receptor antagonist promotes M1 microglia biased cytokines and chemokines following human traumatic brain injury. J. Cereb. Blood Flow Metab. pii:0271678X15620204 (2015) (Epub ahead of print).
111 Burda JE, Sofroniew MV. Reactive gliosis and the multicellular response to CNS damage and disease. Neuron 81(2), 229–248 (2014).
112 Collingridge GL, Peineau S. Strippers reveal their depressing secrets: removing AMPA receptors. Neuron 82(1), 3–6 (2014).
113 Shichita T, Ago T, Kamouchi M, Kitazono T, Yoshimura A, Ooboshi H. Novel therapeutic strategies targeting innate immune responses and early inflammation after stroke. J. Neurochem. 123(Suppl. 2), 29–38 (2012).
114 Spera PA, Ellison JA, Feuerstein GZ, Barone FC. IL-10 reduces rat brain injury following focal stroke. Neurosci. Lett. 251(3), 189–192 (1998).
115 Luo Y, Zhou Y, Xiao W et al. Interleukin-33 ameliorates ischemic brain injury in experimental stroke through promoting Th2 response and suppressing Th17 response. Brain Res. 1597(C), 86–94 (2015).
116 Singhal G, Jaehne E, Corrigan F, Toben C, Baune BT. Inflammasomes in neuroinflammation and changes in brain function: a focused review. Front Neurosci. 315(8), 1–13 (2014).
117 Korhonen P, Kanninen KM, Lehtonen Š et al. Immunomodulation by interleukin-33 is protective in stroke through modulation of inflammation. Brain Behav. Immun. 49, 322–336 (2015).
118 Chen S, Wu H, Klebe D, Hong Y, Zhang J, Tang J. Regulatory T cell in stroke: a new paradigm for immune regulation. Clin. Dev. Immunol. 2013(2), 1–9 (2013).
119 Zhou X, Spittau BR, Krieglstein K. TGFβ signalling plays an important role in IL4-induced alternative activation of microglia. J. Neuroinflamm. 9(1), 1–1 (2012).
120 Liu Z, Chen H-Q, Huang Y et al. Transforming growth factor-beta 1 acts via
TbetaR-I on microglia to protect against MPP+-induced dopaminergic neuronal loss. Brain Behav. Immun. 51, 131–143 (2016).
121 Zhou X, Zöller T, Krieglstein K, Spittau B. TGFβ1 inhibits IFNγ-mediated microglia activation and protects mDA neurons from IFNγ-driven neurotoxicity. J. Neurochem. 134(1), 125–134 (2015).
122 Stoll G, Schroeter M, Jander S et al. Lesion-associated expression of transforming growth factor-beta-2 in the rat nervous system: evidence for down-regulating the phagocytic activity of microglia and macrophages. Brain Pathol. 14(1), 51–58 (2004).
123 Yang Y, Salayandia VM, Thompson JF, Yang LY, Estrada EY, Yang Y. Attenuation of acute stroke injury in rat brain by minocycline promotes blood–brain barrier remodeling and alternative microglia/macrophage activation during recovery. J. Neuroinflammation 26(12) 1–15 (2015).
124 Fontaine RH, Cases O, Renauld JC et al. IL-9/IL-9 receptor signaling selectively protects cortical neurons against developmental apoptosis. Cell Death Differ. 15(10), 1542–1552 (2008).
125 Krüger C, Laage R, Pitzer C, Schäbitz WR, Schneide A. The hematopoietic factor GM-CSF (granulocyte–macrophage colony stimulating factor) promotes neuronal differentiation of adult neural stem cells in vitro. BMC Neurosci. 88(8), 1–7 (2007)
126 Zhang J, Mao X, Zhou T, Cheng X, Lin Y. IL-17A contributes to brain ischemia reperfusion injury through calpain-TRPC6 pathway in mice. Neuroscience 274(C), 419–428 (2014).
127 Adamski MG, Li Y, Wagner E et al. Pre-existing hypertension dominates γδT cell reduction in human ischemic stroke. PLoS ONE 9(5), e97755 (2014).
128 Smith JA, Das A, Ray SK, Banik NL. Role of pro-inflammatory cytokines released from microglia in neurodegenerative diseases. Brain Res. Bull. 87(1), 10–20 (2012).
129 Santello M, Bezzi P, Volterra A. TNFa controls glutamatergic gliotransmission in the hippocampal dentate gyrus. Neuron 69(5), 988–1001 (2011).
130 D’Mello C, Le T, Swain MG. Cerebral microglia recruit monocytes into the brain in response to tumor necrosis factor signaling during peripheral organ inflammation. J. Neurosci. 29(7), 2089–2102 (2009).
131 Carvalho-Tavares J, Hickey MJ, Hutchison J, Michaud J, Sutcliffe IT, Kubes P. A role for platelets and endothelial selectins in tumor
necrosis factor-alpha-induced leukocyte recruitment in the brain microvasculature. Circ. Res. 87(12), 1141–1148 (2000).
132 Barone FC, Arvin B, White RF et al. Tumor necrosis factor-alpha: a mediator of focal ischemic brain injury. Stroke 28(6), 1233–1244 (1997).
133 Seo JH, Miyamoto N, Hayakawa K et al. Oligodendrocyte precursors induce early blood–brain barrier opening after white matter injury. J. Clin. Invest. 123(2), 782–786 (2013).
134 Rosenberg GA, Navratil M, Barone F, Feuerstein G. Proteolytic cascade enzymes increase in focal cerebral ischemia in rat. J. Cereb. Blood Flow Metab. 16(3), 360–366 (1996).
135 Candelario-Jalil E, Taheri S, Yang Y et al. Cyclooxygenase inhibition limits blood–brain barrier disruption following intracerebral injection of tumor necrosis factor-alpha in the rat. J. Pharmacol. Exp. Ther. 323(2), 488–498 (2007).
136 Romanic AM, White RF, Arleth AJ, Ohlstein EH, Barone FC. Matrix metalloproteinase expression increases after cerebral focal ischemia in rats: inhibition of matrix metalloproteinase-9 reduces infarct size. Stroke 29(5), 1020–1030 (1998).
137 Gidday JM, Gasche YG, Copin J-C et al. Leukocyte-derived matrix metalloproteinase-9 mediates blood–brain barrier breakdown and is proinflammatory after transient focal cerebral ischemia. Am. J. Physiol. Heart Circ. Physiol. 289(2), H558–H568 (2005).
138 Czirr E, Wyss-Coray T. The immunology of neurodegeneration. J. Clin. Invest. 122(4), 1156–1163 (2012).
139 K Jopson T, Tweedie D et al. TNF-α protein synthesis inhibitor restoresneuronal function and reverses cognitive deficits induced by chronic neuroinflammation. J. Neuroinflamm. 9(1), 23 (2012).
140 Ignatowski TA, Spengler RN, Dhandapani KM, Folkersma H, Butterworth RF, Tobinick E. Perispinal etanercept for post-stroke neurological and cognitive dysfunction: scientific rationale and current evidence. CNS Drugs 28(8), 679–697 (2014).
141 Weinstein JR, Schulze J, Lee RV et al. Functional polymorphisms in Toll-like receptor 4 are associated with worse outcome in acute ischemic stroke patients. Neuroreport 25(8), 580–584 (2014).
142 Maiti TK, Konar S, Bir S, Kalakoti P, Bollam P, Nanda A. Role of apolipoprotein E polymorphism as a prognostic marker in traumatic brain injury and neurodegenerative

Future Neurol. (2016) 11(1)96
REviEW Dugue & Barone
future science group
disease: a critical review. Neurosurg. Focus 39(5), E3 (2015).
143 Muiño E, Krupinski J, Carrera C, Gallego-Fabrega C, Montaner J, Fernández-Monreal M. An inflammatory polymorphisms risk scoring system for the differentiation of ischemic stroke subtypes. Mediators Inflamm. doi:10.1155/2015/569714 (2015) (Epub ahead of print).
144 Waters RJ, Murray GD, Teasdale GM et al. Cytokine gene polymorphisms and outcome
after traumatic brain injury. J. Neurotraum. 30(20), 1710–1716 (2013).
145 Jander S, Schroeter M, Stoll G. Interleukin-18 expression after focal ischemia of the rat brain: association with the late-stage inflammatory response. J. Cereb. Blood Flow Metab. 22(1), 62–70 (2002).
146 Scherbel U, Raghupathi R, Nakamura M et al. Differential acute and chronic responses of tumor necrosis factor-deficient
mice to experimental brain injury. Proc. Natl Acad. Sci. USA 96(15), 8721–8726 (1999).
147 Roberts I, Yates D, Sandercock P et al. Effect of intravenous corticosteroids on death within 14 days in 10008 adults with clinically significant head injury (MRC CRASH trial): randomised placebo-controlled trial. Lancet 364(9442), 1321–1328 (2004).

559ISSN 1479-6708Future Neurol. (2015) 10(6), 559–575
part of
10.2217/fnl.15.46 © 2015 Future Medicine Ltd
REVIEW
tau protein, ischemic injury and vascular dementia
Elizabeta B Mukaetova-Ladinska*,1, Mosi Li2 & Raj N Kalaria1
1Institute of Neuroscience, Newcastle University, Campus for Ageing & Vitality, Newcastle upon Tyne, NE4 5PL, UK 2Centre for Neuroregeneration, University of Edinburgh, Edinburgh, EH16 4SB, UK
*Author for correspondence: Tel: +44 191 246 8777; [email protected]
Clinical, neuroimaging and neuropathological studies have confirmed overlap between Alzheimer’s disease (AD) and vascular dementia (VaD). Classical neuropathological changes of AD (plaques and tangles) can be present in VaD. We review neuroimaging, biochemical and animal studies to consider the role of tau protein in ischemic injury and VaD pathogenesis. The evidence comes largely from transgenic animal studies that confirm that tau transgenes influence cerebral vasculature. Clinicobiochemical studies in the cerebrospinal fluid (CSF) have, similarly, confirmed alterations in both total and phosphorylated tau protein in VaD. These data suggest that tau protein not only serves as a potential diagnostic tool for differential diagnosis of VaD from other types of dementia, but may also be a therapeutic target in ischemic stroke.
KEYWORDS: • Alzheimer’s disease • cerebrospinal fluid biomarkers • cerebral ischemia • tau protein • vascular dementia
Both Alzheimer’s disease (AD) and vascular dementia (VaD) contribute to the increased burden of dementia prevalence worldwide. Thus, the prevalence rates of VaD double every 5.3 years, ranging from 1.5% (70–75y) to 15% in >80y olds [1], and are very similar to those reported in older AD subjects [2]. More detailed epidemiological studies on dementia and its subtypes have confirmed regional differences in the prevalence estimates of VaD and AD from three continents, with the highest proportion of VaD in older Asian population, accounting for 38% of all dementia cases [3].
In contrast to AD, which has been extensively investigated at clinical and molecular levels, there is a paucity in advances in respect to treatments available for subjects with VaD. This is accompa-nied by enormous medical care costs VaD patients require worldwide. Remarkably, the longer life expectancy in developing countries, including China, has resulted in VaD, together with cerebral vascular diseases, to become leading challenges to their aging population. The epidemiological research on dementia in four major cities of China has provided informative results, indicating that China may have the largest population of people with VaD in the world [4], amounting to 14 million cases. The northern regions of China, in particular, are estimated to have higher prevalence of VaD (1.11 vs 0.97%) [5], which can be attributed to higher incidence of stroke, different lifestyle and diet in these northern areas.
Prevailing studies on AD have enriched our knowledge about the molecular substrates of dementia in general. The characteristic neuropathological changes in AD are the presence of amyloid plaques and neurofibrillary tangles with a predilection of the latter in the medial temporal lobe [6]. Amyloid (Aβ) deposition also occurs in the temporal lobe in VaD subjects [7] with greater age [8]. Some VaD subjects also bear neurofibrillary pathology, for example, tangles and neuritic plaques [9] over and above that in normally aging individuals without any overt neurological or psychiatric disease. Thus, the presence of some Aβ and neurofibrillary pathology in older VaD subjects indicates that both
For reprint orders, please contact: [email protected]

Future Neurol. (2015) 10(6)560
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group
AD and VaD share a certain level of vascular and neurodegenerative pathological features [8].
In correlative clinico-neuropathological and biochemical studies, the characteristic hall-marks of AD correlate with the clinical course of dementia [10]. Pathological advances have led to the development of novel diagnostic tools to visualize brain amyloid in vivo (e.g., PiB [11], flor-betapir F18 [12]) and treatments to regulate the cholinergic deficits (e.g., cholinesterase inhibi-tors) and glutamatergic (NMDA antagonists) changes in AD subjects [13].
What is the fate of tau protein in VaD?tau protein is a microtubule-associated protein (MAP) that stabilizes microtubules and is the major constituent of the paired helical filaments that give rise to neurofibrillary pathology in AD [14,15] tau protein regulates the microtubule (MT) assembly and provides the dynamic stabil-ity of tubulin to assemble into MT and regulates the MT spatial organization under physiological condition [13] Although most of the drug trails today focus on the Aβ peptide in AD, studies on tau protein and its neurobiological function in neurodegenerative disorders provide evidence for development of novel disease-modifying demen-tia treatments based on prevention of the tau truncation/aggregation, modifying tau hyper-phosphorylation and tau-clearance [16].
It is plausible that novel emerging thera-peutics find a place in the treatment of other types of dementia, including VaD. In support of this are the clinical trials that have used the currently available AD antidementia drugs in VaD subjects. For example, memantine [17] and acetylcholinesterase inhibitors (donepezil [18]; galantamine [19] and rivastigmine [20]) have been documented to improve both cognitive and behavioral symptoms in VaD [18]. A most recent study on an animal (rat) model of VaD similarly confirmed the beneficial effect donepezil has on the cognitive function, with the neurobiologi-cal substrate of this being the enhancement of immature, new-born neurons [21], although ace-tylcholinesterase inhibitor effects upon angio-genesis cannot be excluded [22]. These studies provide further support for altered cholinergic system in VaD. In addition, acetylcholine is a powerful dilatator of most vascular beds, and any changes in its expression and/or altered muscarinic receptors but not nicotinic recep-tors [23] result in loss of the ability to dilate spe-cifically cerebral arteries and arterioles [24]. Thus,
impaired cholinergic dilatation of blood vessels may play a role not only in the pathophysiol-ogy of AD, but also in focal cerebral ischemia. However, the etiological drivers for the altered cholinergic neurotransmission in VaD are poorly understood. We cannot exclude the possibility that they may well be similar to those described in AD, including dendritic, synaptic, and axonal degeneration, neurofibrillary pathology and neu-ronal cell loss [25]. This also suggests that tau protein may be similarly altered in VaD and also underlie both cognitive and behavioral symp-toms in this disease.
tau protein in dementiatau protein is a natively microtubule-associated protein that regulates the assembly and stabi-lization of microtubules under physiological conditions [26]. Within neurons, tau protein is concentrated in axons in a highly soluble fash-ion [27]. It plays a role in axonal transport of neuronal organelles and even has a dendritic function in postsynaptic targeting of NMDA receptor substrate [28,29]. There are six distinct isoforms of tau protein identified in the human brain, and they are generated through alterna-tive mRNA splicing from a single microtubule-associated protein tau (MAPT ) gene [30,31]. The interaction between tau protein and tubulin is regulated by the repeated tau protein domains encoded by exons 9–12 [32]. A variety of neu-rodegenerative disorders, including AD, fron-totemporal dementia, parkinsonism linked to chromosome 17, corticobasal degeneration and progressive supranuclear palsy (PSP), have char-acteristic tau pathology, and they are referred to as tauopathies.
In AD, tau protein is posttranslationally modi-fied (e.g., hyperphosphorylated) and forms intra-neuronal aggregates [33]. Hyperphosphorylation of tau protein is the most common posttransla-tional modification occurring in taupathies [33] and it results in detaching tau protein from microtubules, and destabilizing them, giving rise to reduction of axons, dendrites and syn-apses [34], degeneration of plasma membrane and subsequently apoptosis [35]. The tau protein hyperphosphorylation alone [36] or resulting in tau truncation [37] leads to the formation of insol-uble and filamentous intraneuronal structures, known as paired helical filaments (PHF) [38] (Figure 1). A number of evidence suggests that fibrillar tau inclusions have a key role in clinical symptoms and pathology in taupathies. More

561
Figure 1. Sketch of a neuron, amyloid plaques, neurofibrillary tangles and aggregated paired helical filaments (PHF).
Aβ42
Axonal tau
Aggregated PHF tauPhosphorylated andtruncated tau protein
Aβ metabolism and formation of senile plaques
tau protein, ischemic injury & vascular dementia REviEW
future science group www.futuremedicine.com
importantly, frontal-temporal dementia and Parkinsonism linked to chromosome 17 muta-tions within the MAPT gene (FTDP–17) pro-vide further support that tau dysfunction in the absence of amyloid pathology is sufficient to trig-ger clinical dementia, neurofibrillary pathology, neuronal loss [40] and collagen deposits within the blood vessel walls [41].
Linking vascular pathology to neuronal cytoskeletal changesA number of clinical, neuroimaging and neu-ropathological studies has confirmed overlap between clinical risk factors and pathological changes in VaD and AD. Vascular changes are involved in the pathogenesis of both AD and VaD, with nearly half of all older subjects having pronounced vascular pathology in their brain tis-sue [42]; similarly, large vessel abnormalities, such as carotid artery stenosis and bilateral carotid plaques are common in AD [43]. Furthermore, about 30% of AD cases have some degree of vascular pathology, and a similar proportion of VaD cases have AD pathology, with perivascular Aβ depositions being present in both VaD and AD [43,44]. Meanwhile, there is an increasing evidence supporting the role of Aβ peptide and apolipoproteins in VaD [8,45], and their links to tau protein. Thus, Aβ protein toxicity appears to be tau dependent [29], though the mechanism of this link still remains unclear. Interestingly, a most recent neuroepidemiological study, con-ducted on a total number of 6025 subjects with
a single neurodegenerative diseases, linked coin-cident cerebrovascular disease with lower neu-rofibrillary pathology (e.g., Braak stages I-IV), with subjects with sole tau pathology (e.g., fron-totemporal lobar dementia) exhibiting substan-tially lower rate of vascular pathology (<60%) than that seen in AD [46]. These findings bear resemblance to an earlier correlative cliniconeu-ropathological study that reported dementia dur-ing life to be linked to medial temporal lobe neurofibrillary pathology in those with a clinical diagnosis of AD, whereas vascular pathologies, especially microinfarcts, were more common in those with clinical diagnoses of vascular dementia [47]. These findings raise an interest-ing possibility that vascular pathology may halt the progression of neurofibrillary degeneration in the aging brain. However, the mechanisms behind this remain unknown. One possibility is that vascular pathology influences directly the expression of tau protein in the human brain [48] and thus the pathophysiological mechanisms underlying the development of neurofibrillary pathology, that of phosphorylation [49] and trun-cation [50] of the tau protein.
Imaging studies have reported that Aβ burden in VaD is related to white matter ischemia [51], the latter corresponding to axonal changes as demonstrated in postmortem studies [52]. The widespread axonal damage in VaD likely alters tau protein function or physical status. Furthermore, these changes not only appear to be confined to axons with microtubule structures

Future Neurol. (2015) 10(6)562
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group
but also involve glial cells. It has been previously shown that after focal cerebral ischemia, there is an increase in tau expression in glial cells within the neuropil and in oligodendrocytes [53]. This suggests that tau protein undergoes dephos-phorylation and degradation in axons and peri-karya as a result of cerebral ischemic injury [53]. Moreover, pathologically modified tau protein exists in microglial cells around the cerebral ischemic focus [54].
The above findings indicate that tau protein alterations may be an early pathological change in response to ischemic mechanisms in certain neurons [55]. Furthermore, the dephosphoryla-tion of tau protein may cause damage to the organelle transport between axons and neuro-some, and subsequently influence its susceptibil-ity to proteolysis [56]. Nonetheless, following a brain ischemia, accumulation of hyperphospho-rylated tau protein occurs in cortical neurons and accompanies apoptosis [57]. Furthermore, ischemic damage alone is associated with neu-rofibrillary tangle-like tauopathy [58]. Similarly, blood–brain barrier (BBB) dysfunction results in brain parenchymal accumulation of blood (plasma) derived neurotoxic and vasculotoxic molecules (e.g., fibrinogen, thrombin, hemosi-derin, plasmin), cerebral hypoxia and reduction in cerebral blood flow. All these vascular-derived insults can precede, initiate and/or contribute to neuronal degeneration, including altered tau processing [59–62]. Transgenic mice expressing human tau besides the well documented neurofi-brillary degeneration also show mild BBB dis-ruption [63]. Interestingly, most recent research supports that tau alone can both initiate BBB breakdown and reverse it [64]. The stabilization of the BBB disruption in this transgenic animal model was achieved via depletion of tau protein (Figure 2). All these studies provide a neuropatho-logical explanation for the role of tau protein in dementia after ischemic event.
Cerebrospinal fluid tau protein in VaDAnother piece of evidence for tau protein involvement in VaD comes from cerebrospinal fluid (CSF) biomarker studies in dementia [65] (Table 1; [66–84]). CSF-tau protein is considered as a peripheral biomarker of neurodegenerative changes [85] and dementia progression in several types of dementia [86]. A number of studies have shown a consistent increase in CSF total (t-) and phosphorylated (p-) tau protein levels in sub-jects with AD (Table 1). In most reports, in VaD,
CSF tau protein levels (both t- and p-tau) were somewhat lower than those in AD subjects (Table
1), thus suggestive of these differences to have a potential to discriminate VaD from AD, irre-spectively, of the clinical stage of the disease [69]. However, several studies also demonstrated con-flicting evidences [87]. Thus, the use of CSF tau protein in discrimination between AD and VaD remains still controversial in clinical practice.
●● t-tau in VaD CSFBoth studies on subjects with VaD, subcortical vascular disease and stroke indicate an increase in CSF t-tau levels, which are significantly higher than those in age-matched control subjects or those with mental health problems (e.g., depres-sion) but substantially lower than in AD (Table
1; [51]). Similarly, CSF samples obtained after stroke contain increased t-tau levels, with a peak after 1 week following the acute stroke, and normalization of the t-tau levels after 3–5 months [88]. Furthermore, the level of t-tau pro-tein appears to reflect the size of the stroke, but not the clinical measures of disability [89].
A recent meta-analysis of CSF tau measures in the Chinese population included 16 studies on VaD, which consisted of heterogeneous vascular dementia syndromes, in the context of ischemic and hemorrhagic strokes, cerebral hypoxic-ischemic events, and senile leukoencephalo-pathic lesions. Consistently higher CSF t-tau was reported in VaD subjects compared with con-trols, but still lower in relation to AD [65]. This analysis of CSF did not include phosphorylated tau. All these findings argue that the increase in CSF t-tau in VaD subjects may reflect a degree of neuronal damage following ischemia [88,89], that appears to be normalized in the follow-up period [89], suggesting that the transient upregu-lation of t-tau is an immediate response to an acute axonal injury, This would be consistent with the previously attributed increase in t-tau in AD as a result of axonal damage [90]. However, in some instances, normal CSF levels of t-tau have also been reported in VaD (Table 1; [39]), and they correspond to white matter changes, occurring in the absence of recent stroke and concomitant AD pathology [70].
●● p-tau in VaD CSFPhosphorylated tau (p-tau) has similarly been investigated in VaD, and attributed to the under-lying AD pathology [91]. Similarly to t-tau, the increase in CSF p-tau in VaD does not exceed

563
Figure 2. Brain ischemic damage and tau protein and Aβ. NFTs: Neurofibrillary tangles; p-tau: Hyperphosphorylated tau.
Brain ischemia Oxidative stress BBB breakdown
Aβ clearance ↓
Amyloid plaques
Vasculotoxic and neurotoxic proteins ↑
Major vascular risk factors
p-tau
NFTs
Aβ
?
Neuronal damage
Alzheimer’s disease
tau protein, ischemic injury & vascular dementia REviEW
future science group www.futuremedicine.com
that found in AD (Table 1). Interestingly, the apoptosis of neurons due to ischemia gives rise to hyperphosphorylated intraneuronal tau protein, which does not appear to be elevated immediately after the stroke, in contrast to CSF t-tau [91]. This finding argues that changes in t-tau happen quickly following a sudden damage to the neuronal and axonal integrity, whereas p-tau elevation legs behind.
Previous studies found increased CSF p-tau to be more characteristic for subjects with cognitive disturbances attributed to AD than other forms of dementia, including VaD, Dementia with Lewy Body, Parkinson’s Disease Dementia or cognitively intact population [68,78–80]. However, elevated CSF p-tau (phosphorylated at Thr181; p-tau181) is also present in VaD (Table 1; [78]).
One large-scale, multicenter study reported ele-vated CSF p-tau199 to discriminate AD from other forms of dementia, including VaD [92]. Moreover, p-tau181 has been most consistently reported to be similarly increased in both pure VaD and AD [69]. In the latter study, most of the VaD cases had also chronic leukoencepha-lopathy and multiple infarcts rather than sin-gle cortical infarct. Although CSF p-tau181 failed to discriminate between different types of dementia, it, however, predicted a more rapid cognitive decline, irrespective of the clinical dementia diagnosis [78]. The reported high CSF p-tau level, irrespective of the phosphorylation site, in both VaD and AD might be explained by the similar neurodegenerative and vascular pathological features in VaD and AD, which also

Future Neurol. (2015) 10(6)564
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group
Table 1. Summary of most relevant cerebrospinal fluid tau studies in vascular dementia.
Study tau-measures Technique No. of subjects
No. of controls
Results t-tau p-tau
VaD vs AD
Arai et al. 1998 [66] √ – ELISA 29 CVD (21 demented and 8 non-demented), 69 AD, 21 VaD
17 CSF t-tau was significantly decreased in VaD than AD (p < 0.0001). However, CSF t-tau in VaD was not significantly different from nondemented CVD and control subjects
de Jong et al. 2006 [67]
√ p-tau 181 ELISA 61 AD, 25 VaD, 30 t-tau was significantly increased in AD compared to VaD and control group (p < 0.001). However, VaD and control participants had similar levels of t-tau. p-tau 181 was significantly increased in AD compared to VaD and control participants (p < 0.001). No significant differences between VaD and control participants were reported
Schonknecht et al. 2003 [68]
√ – ELISA 88 AD, 23 VaD, 25 major depression
17 t-tau was significantly increased in VaD compared to controls and subjects with major depression, but significantly lower than in AD (p < 0.05)
Stefani et al. 2005 [69]
√ p-tau 181 ELISA 20 VaD, 66 AD (31 AD+WMC; 35 AD)
24 Increased t-tau in AD and VaD compared to controls (p < 0.001). However, VaD subjects had similar level t-tau with AD (p = 0.5). Increase in p-tau was similarly noted in both VaD and AD subjects (p < 0.005). VaD subjects had lower levels of p-tau than their AD counterparts (p < 0.05)
Wallin and Sjögren, 2001 [70]
√ – ELISA 25 subjects with SWD
17 Although CSF t-tau was increased in the SWD cases, this increase was not statistically significant. However, the CSF tau measures had specificity of 85% and 36% sensitivity for SWD
Hjalmarsson et al. 2014 [71]
√ p-tau 181 ELISA 20 patients studied after AIS onset
20 Patients with AIS had significantly higher levels of neurofilament (NFL), t-tau, myelin basic protein (MBP) and inflammatory markers such as YKL–40, and glial fibrillary acidic protein (GFAP) compared with controls. t-tau, MBP, GFAP, and YKL–40 correlated with clinical stroke severity, whereas NFL correlated with severity of white matter leasions
Roseels et al. 2014 [72]
√ - ELISA 20 AD and 20 VaD
20 Novel anti-tau protein antibody that recognizes tau protein oligomers shows similar distribution of tau protein as that of t-tau; the tau protein oligomers in the CSF are significantly increased in VaD subjects compared to that of controls (p < 0.05), and slightly, but not significantly, lower than those of AD subjects
Liquori et al. 2015 [73]
√ p-tau 181 ELISA 145 AD (mild 67 and moderate–severe 78) and 44 VaD
80 Significant increases of CSF lactate concentration were observed in AD group compared to control and VaD, which had a negative correlation with the CSF t-tau and p-tau levels in corresponding groups
Hermann et al. 2014 [74]
√ p-tau 181 ELISA 27 AD; 59 CSVD with cognitive impairment
33 with CSVD and intact cognition
After stratification of cognitive impaired patients (n = 59) two groups were identified: 32 patients with normal beta-amyloid 42/40 ratio (>0.975) who had impaired blood–brain barrier function (e.g., elevated albumin ratio), representing pure AD and AD+CSVD, and the other group (VaD) consisting of subjects with normal beta-amyloid ratio. The CSVD subjects, irrespectively of their cognitive functioning, had similar levels of both t-tau and p-tau Thr181, and substantially lower than that observed for participants with pure AD and AD+CSVD
p-tau alone is used when studies did not report the site of tau protein phosphorylation.AD: Alzheimer’s disease; AIS: Acute ischemic stroke; ALS: Amyotrophic lateral sclerosis; CJD: Creutzfeldt-Jakob disease; CSVD: Cerebral small vessel disease; CVD: Cerebrovascular disease; DLB: Dementia with Lewy bodies; FTLD: Frontotemporal lobar degeneration; HCONT: Healthy controls; NCONT: Neurological controls; SWD: Subcortical white matter dementia; VaD: Vascular dementia; WMC: White matter changes.

565
tau protein, ischemic injury & vascular dementia REviEW
future science group www.futuremedicine.com
Table 1. Summary of most relevant cerebrospinal fluid tau studies in vascular dementia (cont.).
Study tau-measures Technique No. of subjects
No. of controls
Results t-tau p-tau
Kester et al. 2014 [75]
√ p-tau 181 ELISA 547 AD; 30 VaD 337 Presence of microbleeds was linked to lower CSF Aβ42 (p = 0.003) in both AD and VaD subjects, whereas in control subjects there were higher levels of CSF t-tau (p = 0 .03). White matter hyperintensity was associated with lower Aβ42 in control and VaD participants (p = 0.002), whereas lacunes with higher Aβ42 in VaD (p = 07) and lower t-tau in AD participants (p = 0.05). None of the vascular pathology influenced the CSF levels of p-tau181. These effects were mostly attributable to APOEε4 allele
Krishnan and Rani, 2014 [76]
√ - ELISA 30 AD; 35 VaD 40 Plasma Aβ42 level were significantly elevated in both AD and VaD subjects compared to controls (p < 0.001). In contrast, CSF t-tau and tau-to-amyloid ratio were significantly lower in both AD and VaD subjects compared to controls (p < 0.001), with the VaD participants having significantly higher values in both measurements compared to the AD subjects. The receiver operating characteristic (ROC) curve-derived cut-off values of <3.5 for tau-to-Aβ42 ratio and <520 pg/ml for t- tau had 67–72% sensitivity and specificity for differentiating AD from VaD and 90 % for AD from controls
VaD vs mixed and cerebrovascular dementias
Paraskevas et al. 2009 [77]
√ p-tau 181 ELISA 92 AD, 23 VaD, 17 Mixed
68 CSF t-tau was slightly, but significantly (p < 0.05) increased in VaD compared to control; t-tau levels were highest in mixed group and followed by AD (p < 0.0001). p-tau 181 was significantly decreased in VaD compared to control, mixed and AD groups (Mixed>AD>control>VaD; p = 0.0021)
Ravaglia et al. 2008 [78]
– p-tau 181 ELISA 51 AD, 13 pure VaD, 6 possible VaD
36 CSF p-tau discriminated patients with dementia from control group (p=0.0001, 100% specificity), However, p-tau was not useful in differentiating distinct forms of dementia
VaD vs other forms of dementia
Blennow et al. 1995 [79]
√ p-tau ELISA 17 VaD, 44 AD, 11 FTLD, 15 PD, 10 Depression
31 CSF t-tau was significantly higher in AD (p < 0.0001), VaD (p < 0.0001) and FTLD (p < 0.05) compared to control subjects. However, AD and VaD subjects had similar levels of CSF t-tau. CSF p-tau was significantly higher in AD (p < 0.0001) VaD (p < 0.01) and FTLD (p < 0.01, than in controls. CSF p-tau in AD was significantly higher than VaD (p < 0.005), TFLD (p < 0.05), PD (p < 0001) and subjects with depression (p < 0001)
Andreasen et al. 1998 [80]
√ – ELISA 21 VaD, 43 AD 11 MIX(AD/VaD), 18 NCONT, 18 HCONT, 9 ALS
17 CSF t-tau was significantly increased in AD subjects compared to ALS (p < 0.002), NCONT (p < 0.0001) and HCONT (p < 0.0001), whereas there was no significant difference between AD and VaD. CSF t-tau was also significantly higher in VaD than NCONT (p < 0.005) and HCONT (p < 0.0001). Moreover, in MIX group CSF t-tau was significantly increased as compared with NCONT (p < 0.005) and HCONT (p < 0.0001)
Herbert et al. 2013 [81]
√ p-tau ELISA 14 DLB, 64 AD, 15 VaD, 26 FTLD
– CSF t -tau levels in AD were significantly increased compared to DLB and VaD (p < 0.01)CSF p-tau levels were also significantly increased in AD compared to other groups (p < 0.001), but no significant difference between VaD, DLB or FTD groups
p-tau alone is used when studies did not report the site of tau protein phosphorylation.AD: Alzheimer’s disease; AIS: Acute ischemic stroke; ALS: Amyotrophic lateral sclerosis; CJD: Creutzfeldt-Jakob disease; CSVD: Cerebral small vessel disease; CVD: Cerebrovascular disease; DLB: Dementia with Lewy bodies; FTLD: Frontotemporal lobar degeneration; HCONT: Healthy controls; NCONT: Neurological controls; SWD: Subcortical white matter dementia; VaD: Vascular dementia; WMC: White matter changes.

Future Neurol. (2015) 10(6)566
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group
share a number of genetic and pathophysiologi-cal similarities [93].
●● Does CSF tau differentiate VaD from other dementia subtypes?The potential value of CSF tau in differentiating VaD from AD and other dementia subtypes still remains controversial. The heterogeneity of VaD needs to be taken into account when interpreting the CSF findings. Although elevated CSF tau in VaD group may reflect a direct acute cerebral ischemic injury, this needs to be interpreted cau-tiously, taking into account the temporal rela-tionship between the onset of ischemic event(s) and the CSF examination. Thus, CSF t-tau levels in acute cerebral infarction are transiently upreg-ulated after 2–3 weeks following an ischemic event, and are normalized few months later [66]. Another study showed that the elevation of t-tau in the CSF happens within the first 1–2 days of an acute ischemic stroke and similarly falls back to baseline levels after 3–5 months of the stroke [89]. Although the role of p-tau in differentiating VaD from AD is disputable, a combination strategy measuring CSF biomark-ers including tau (both t- and p-tau), Aβ
1–42 and
inflammatory cytokines (e.g., IL–6 and TNF) may improve the sensitivity and specificity of these biomarkers to diagnose and differentiate VaD from other types of dementia [94], predict extent of cognitive deterioration [66], and even be used to monitor treatment outcomes.
tau protein in animal models with altered cerebral circulation●● Animal models with induced
neurovascular changesDespite the paucity of detailed neuropathological studies on tau protein changes in VaD, the strong-est evidence for vascular mechanisms influenc-ing tau protein in VaD pathogenesis comes from animal models with neurovascular pathology. Thus, rodents with permanent middle cerebral artery occlusion show a total neuronal loss in the center of the infarct lesion as well as in the border zone (penumbra) [95]. Although this study did not address specifically tau protein changes, it provides indirect evidence that tau protein may be significantly altered as a result of the observed neuronal cell death. This has been now confirmed in a study on transient ischemic cerebral ischemia in wild type rats and gerbils, that not only
Study tau-measures Technique No. of subjects
No. of controls
Results t-tau p-tau
Schoonenboomet al. 2012 [82])
√ p-tau 181 ELISA 52 DLB, 512 AD, 34 VaD, 16 CBD, 144 FTLD, 20 PSP, 6 CJD
135, 275 SMC
In VaD, CSF t-tau levels were similar to those seen in control subjects (p>0.05), but substantially lower than those in AD (p<0.05). In contrast the VaD subjects had the; lowest CSF p-tau levels, significantly lower than control and AD subjects (p < 0.05)
Herbert et al. 2014 [83]
√ p-tau 181 ELISA 14 DLB; 64 AD; 15 VaD;26 FTLD
- All groups had similar levels of CSF t-tau and p-tau Thr181. The combination of Aβ42, t-tau, and p-tau yielded a sensitivity of 61.9% and a specificity of 91.7% for the discrimination between DLB and AD, but could not discriminate between DLB and VaD or FTLD. The addition of 3-methoxy-4-hydrophenylethyleneglycol to the Aβ42, t-tau, and p-tau improves the discrimination of DLB from AD (65.1% sensitivity and 100% specificity), but did not distinguish DLB or VaD from other forms of dementia
Amadoro et al. 2014 [84]
√ p-tau 181 ELISA western blot
26 AD, 6 MIX, 9 VaD, and 22 other forms of dementia, (e.g., PDD, PSP, FTLD, MSA, CBD, ALS, CJD etc.)
14 t-tau and p- tau (Thr181) and N-terminal end tau measured. No specific reference for VaD or mixed dementia. However, t- and p-tau CSF measures in the other dementia forms were with intermediate values between control and AD subjects. Subjects with AD and other forms of dementia had similar elevated levels of amino-terminal end of tau protein in comparison to their control counterparts (p < 0.0001)
p-tau alone is used when studies did not report the site of tau protein phosphorylation.AD: Alzheimer’s disease; AIS: Acute ischemic stroke; ALS: Amyotrophic lateral sclerosis; CJD: Creutzfeldt-Jakob disease; CSVD: Cerebral small vessel disease; CVD: Cerebrovascular disease; DLB: Dementia with Lewy bodies; FTLD: Frontotemporal lobar degeneration; HCONT: Healthy controls; NCONT: Neurological controls; SWD: Subcortical white matter dementia; VaD: Vascular dementia; WMC: White matter changes.
Table 1. Summary of most relevant cerebrospinal fluid tau studies in vascular dementia (cont.).

567
tau protein, ischemic injury & vascular dementia REviEW
future science group www.futuremedicine.com
causes neuronal apoptosis, but also induces tau hyperphosphorylation at multiple sites, includ-ing Ser202/Thr205, Ser214, Ser396/Ser404 [81] and Ser199/Ser202 sites as early as 6 h postisch-emia [96], and results in PHF-like conformational changes [91]. However, the hyperphosphorylation of tau protein appears to be a secondary response following the initial rapid dephosphorylation of the protein that occurs within the first 5 min of the ischemic insult [96]. Accumulation of Aβ deposits within the brain microvasculature is similarly associated with increased level of hyper-sphosphorylated tau protein in a rodent model of a neurovascular injury (e.g., embolism; [97]. These findings provide support that changes in tau pro-tein due to ischemia may underlie the cognitive impairment in people with ischemic strokes.
●● Hyperglycemia & neurovascular changesChanges to the vascular endothelium are con-sistently found in the presence of hypergly-cemia [98], a characteristic feature of one of the major risk factors for dementia, diabetes. However, the neurophysiological mechanisms by which diabetes influences cognitive func-tioning are poorly understood. Rodents with streptozotocin-induced Type 1 diabetes exhibit various extent of cognitive deficits and this is accompanied by exacerbation of Aβ deposits, especially in a highly vascularized area of the hippocampus, where amyloid deposits are found surrounding but not within the blood vessels [99]. These Type 1 diabetic mice also have an increase in hyperphosphorylated tau at Ser396, whereas their total tau protein remains unaltered [99]. These findings confirm that diabetes can induce endogeneous amyloid and tau pathology that is also accompanied by changes in the cerebral vasculature. Furthermore, they provide further support between the link between diabetes, tau pathogenesis and amyloid deposits, although they fail to address the specific link in relation to the development of brain vascular pathology in diabetes-induced VaD.
●● Transgenic tau animal models & VaD disease mechanismsTransgenic (Tg) animal models similarly can aid the understanding of VaD disease mechanisms and provide a further research platform to inves-tigate the overlap of VaD with other forms of dementia, including AD. One such study indi-cates that overexpression of tau protein (TgP301L tau mice) may reduce the volume of ischemic
infarcts and reduce the neuronal apoptosis [100]. Furthermore, this study also reported that differ-ent tau phosphorylation sites may be altered dif-ferently in ischemia/hypoxia, and they can appear as early as 24 h posttrauma. Thus, phosphoryla-tion at Ser199/Ser202 and the phosphorylated independent tau sequence 210–230 of human tau protein remain unaltered, whereas Thr231 phos-phorylation is significantly decreased in the wild strain postischemia [100]. This study was done on young animals that did not harbor any neu-rofibrillary pathology at the time of the ischemic insult and were sacrificed 24 h post the insult. It, thus, remains undetermined how these biochemi-cal and neuropathological changes would have progressed long-term postinsult, and influence the neurofibrillary pathology p rogression poststroke.
Another way of addressing the tau protein in relation to vascularly mediated mechanisms in VaD is via the use of adeno-associated virus (AVV) vector-mediated expression of mutant P301L tau protein (AVV-tauP301L), injected in the left hip-pocampus. This novel model for tau-mediated hippocampal neurodegeneration results in early apical dendrites damage in CA1 pyramidal hip-pocampal neurons, and is accompanied by loss of dendritic spines, damage to the brain–blood barrier integrity, constriction of brain capillaries that are surrounded by swollen astrocytes with extensions contacting degenerated dendrites and axons [101]. These data provide further evidence to link tau neurodegeneration with inflammation and vascular changes in the brain tissue as a result of the initial neuronal injury due to tau protein overexpression.
●● Triple transgenic mouse model & vasculature changesThe triple transgenic mouse model of Alzheimer’s disease [3xTg-AD; harboring PS1 (M146V), APP (Swedish mutation; dou-ble mutation at codons 670 and 671 of APP 770 transcript in exon 16), and tau(P301L) transgenes] which is characterized by both Aβ and tau protein rapid brain accumulation, can be, particularly, useful to address the interphase between the neurodegenerative changes charac-teristic of both aging and AD and those of VaD. This 3xTg AD model has reduced cerebrovas-cular volume (27%; initially evident in the hip-pocampus and later on spreading to other brain areas, including cortex [102,103]. The reduced cerebrovascular volume precedes the onset of AD pathology by at least 6 months, and is not

Future Neurol. (2015) 10(6)568
Total tau protein
Phosphorylated tau protein (Ser262)
Synaptophysin
C VaD AD
* **
*
*
BA9
BA21
0
2
4
6
8
14
12
10
0
50
250
200
150
100
0
50
200
150
100
C VaD AD
C VaD AD
***
******
Figure 3. tau protein and synaptophysin in control, VaD and AD subjects. (Top) Total tau protein was measured with mAb 7/51, that recognizes a microtubule binding region of the tau protein molecule. (Middle) Phosphorylated tau protein measured with pAb Ser262 antibody that recognizes phosphorylation site at Ser262 of the tau protein molecule. (Bottom) Synaptophysin was measured with mAb EP10 (a gift from Professor W Honer, University of British Columbia, Canada). All values on y-axes represent percentage Relative Values (RV%). *p < 0.05. **p < 0.01. ***p < 0.0001. AD: Alzheimer’s disease; C: Control group; VaD: Vascular dementia. Figure based on data from [45].
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group

569
tau protein, ischemic injury & vascular dementia REviEW
future science group www.futuremedicine.com
associated with reduction in microvessel den-sity [103]. Since the microvessel lumen is reduced as a result of the thickening of the blood ves-sel wall [102], this 3xTg-AD animal model may also serve as a model of cerebral hypoperfusion. Interestingly, the reduction in cerebrovascular volume is not characteristic for the APP/PS1 transgene [103,104], thus suggesting an inter-esting role for tau protein in neurovascular pathology in AD. It is of interest to speculate that tau protein may similarly play such a role in non-taupathies, such as VaD. In support of the latter is a study by Head et al. [105] who described a negative correlation between hyper-phosphorylation of tau protein and decrease in cerebrovascular volume in Caveolin–1 knock-out mice. This proved further support for the role of tau protein in cerebrovascular integrity and function.
●● Acute & chronic hypoperfusion in transgenic animal models of ADAcute cerebral ischemic damage in 3xTg-AD model resulted in elevated total tau accompanied by enhanced phosphorylation of the amyloid pre-cursor protein (APP) but had not effect on the Aβ level at 3–months posthypoperfusion [106]. Similarly, transient reduction of blood volume (oligemic hypoperfusion), produces acute, sig-nificant and long lasting impact on APP and tau protein in this animal AD model, increas-ing Aβ levels via enhancing β-secretase protein expression. In addition it also leads to significant changes in tau protein expression: a decrease in total tau levels and an increase specifically in phosphorylated tau at Ser212 and Thr214 [106], tau epitopes associated with paired helical fila-ments in AD. Vasoconstriction on its own, used to mimic small lacunar infracts, similarly leads to an upregulation of tau protein and APP, even in very young animals (5 months old App23 mice [107]).
Chronic cerebral hypoperfusion induced by obstructing right common carotid artery in Tg 2576 APPs(swe) AD mice produces aggrava-tion of cognitive decline in this animal model of VaD, which is not related to neuronal and axonal loss, or amyloid deposits [108]. The meta-bolic deficit as documented on FDG-PET scans is suggestive of severe synaptic loss and MAP–2 depletion, as a result of accompanying dendritic loss. This per sé does not exclude the possibility that tau protein may also be affected, but this was not addressed in the study.
In another model of chronic cerebral hypop-erfusion exhibiting cerebral amyloid angiopa-thy (CAA) [Tg-SwDI mice, that express APP harboring tandem Dutch (E22Q) and Iowa (D23N) amyloid β mutations [109] bred onto a nitric oxide synthase 2 gene knockout back-ground], the cerebral Aβ deposition occurs along cerebral capillaries and is accompanied by perivascular neuroinflammation, accumula-tion of phosphorylated tau protein and neuronal loss [110,111]. The accumulation of phosphoryl-ated tau protein (Ser202/Thr205) appears to be restricted to perivascular cortical neurons and activated microglia in thalamus tightly associ-ated with capillary amyloid deposits [111]. This pattern of phosphorylated tau localization is highly reminiscence of that seen in the human CAA Type 1 brain.
Experimental studies, irrespectively whether conducted on disease models of AD, diabetes, or vascular diseases, link tau protein with the neurovascular changes. Furthermore, tau pro-tein undergoes posttranslational changes, for example, hyperphosphorylation similar to that seen in AD as a result of ischemia. However, the extent of phosphorylation of tau protein varies. Nevertheless, it is undoubtful that drugs that decrease the extent of tau protein phosphoryla-tion, as well as APP phosphorylation and pro-tein kinase C activation [e.g., potassium 2-(1–hydroxypentyl)-benzoate] also have an impact on improving spatial learning and memory deficits in both transgenic APP and PS1 [112] as well as in chronic cerebral hypoperfused animal models [113]. We need now further studies that would provide firmer evidence for the exact role of tau protein in relation to altered inflamma-tion, amyloid processing and vascular changes.
ConclusionsThe role of tau protein in ischemic injury and VaD is poorly understood. Except for the clini-cal biochemical studies on tau protein measure-ments in the CSF, the evidence for altered tau protein metabolism at a molecular level is still lacking. The negligible amount of neurofibrillary pathology that occurs in VaD in most instances is similar to that found in age-matched control subjects [8], thus, arguing that tau protein may not be contributing to the dementia syndrome in VaD subjects. This is in contrast to the neu-roradiological evidence of white matter ischemia in VaD [51] that corresponds to extensive axonal loss in postmortem studies [52]. Interestingly, the

Future Neurol. (2015) 10(6)570
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group
latter findings correspond well to the biochemi-cal evidence from CSF studies of consistently increased t-tau protein in subjects with clinical symptoms of dementia and various extent of vascular pathology. This provides further evi-dence for widespread axonal damage occurring in VaD [90]. Since tau protein is predominantly enriched in axons [13], it is not surprising that the focal white matter changes in VaD would also result in changes in tau protein, as it was recently confirmed in a CSF study on subcortical white mater changes [70].
Neurobiochemical and neuroimaging stud-ies argue that in VaD there is a widespread axonal damage. The latter may be a result of the ischemic changes triggering posttransla-tional modification to tau [106], or the white matter rarefication and microinfarction [114]. In this, the neurofibrillary pathology appears not to play a major role, unless there is a concomi-tant AD pathology documented [80]. However, the obvious link between vascular pathology and altered tau protein function is still miss-ing. Interestingly, novel rodent models in trans-genic mice genetically engineered to express AD pathology show that transient global ischemic injury significantly decreases both total and phosphorylated tau, with coincident activation of macroautophagy and ubiquitin-proteosome pathways [106]. In both these studies, there was a specific increase in tau protein phosphorylated at Ser212 and Thr214, tau epitopes associated with paired helical filaments in AD. The observed pattern of decreased total tau, altered phospho-rylated tau and increased Aβ persisted for sev-eral weeks after the transient period of cerebral hypoperfusive injury [106]. The findings from these studies display similarities with those in human subjects, where transient up-regulation of CSF t-tau occurs within days following an ischemic injury and is normalized in the follow-ing several months [66]. However, we have to bear in mind that although translational dementia research needs to be based on valid animal mod-els to help alleviate some of the unmet needs of dementia sufferers (e.g., diagnosis, disease pro-gression and treatment), none of the currently available models recapitulates all aspects of any of the known dementia syndromes, including VaD. Furthermore, the well-researched amyloid AD animal models proved not to be good in prediction of the drug efficacy in human subjects (reviewed in [115]), thus confirming that difficul-ties in extrapolating conclusions from animal
to human conditions. More neurobiochemi-cal studies on tau protein in VaD subjects are, therefore, needed to determine whether there is a role of this microtubule associated protein in generating cognitive impairment in VaD, and if so, to address the underlying neurobiological mechanisms leading to the altered tau protein processing. If indeed tau protein plays a role in vascular type dementia, this may trigger more vigorous development of much awaited novel therapeutics to combat VaD,
Future perspectiveRecently, we reported selective loss of both total tau loss and phosphorylated tau at Ser262 in the temporal lobe in VaD subjects (Figure 3A
& B; [48]). This loss occured in the absence of overt synaptic loss (Figure 3C) and was associated neither with the extent of underlying neurofi-brillary and amyloid pathology, nor the age at death. These findings argue that selective tau protein loss in the temporal lobe in VaD sub-jects may be a result of distal neuropathological changes, for example, deep micro- and macroin-farcts leading to white-matter tracts damage that have been described to be characteristic for the temporal lobe in VaD [116]. However, we cannot exclude the possibility that the temporal lobe per sé may be more susceptible to tau protein oli-gomerization, and more profound inhibition of the anterograde fast axonal transport [117], thus resulting in impaired movement of synaptic vesi-cles, axonemal precursors and mitochondria, all known to be altered in VaD [118]. It is interest-ing to note that in an animal model, multiple infarcts were shown to lead to a delayed neuronal death confined predominantly to the temporal lobe [119], suggesting that the vascular changes may result in an ongoing neuropathological pro-cess, and the extent of the tau protein loss may be associated also with the time-lapse between the cerebrovascular incident and the lethal outcome.
Similar loss of tau protein has been described in mutant knock-out MAPT gene mice. In this rodent tau model, the tau protein loss resulted in reduced brain volumes in the absence of overt histological changes to brain structure and organization, including cortical or hippocam-pal lamination [120]. This may correspond to the reduced temporal lobe and hippocampal forma-tion volumes in VaD or post-stroke dementia subjects [121,122]. In addition, there is a genetic link between the MAPT gene and VaD [123] that has not been investigated fully. Thus, MAPT

571
tau protein, ischemic injury & vascular dementia REviEW
future science group www.futuremedicine.com
single nucleotide polymorphism rs1467967 has been linked to VaD, with the G allele in particular, doubling the risk for developing VaD [124]. Interestingly, the G allele is also asso-ciated with lower CSF t-tau levels [124]. Since the G allele is common in both Caucasian and Chinese populations (57% and 84%, respec-tively) [123,124] it is intriguing to speculate that it may well be over-represented in VaD and thus linked to the down-regulation of temporal lobe tau protein in VaD. Further studies are now needed to explore the effect of vascular pathol-ogy upon the tau protein metabolism in both aging and dementia, and address in depth the mechanisms underlying the temporal lobe t-tau protein loss in VaD.
Moreover, the reviewed neurofibrillary tangle-like tauopathy after an ischemic cerebral damage has provided a potential neuropathological basis for the progression of dementia in postischemic brains [58]. Meanwhile, tau protein also dem-onstrates the potential as a therapeutic target in ischemic stroke [125] and a diagnostic tool
to differentiate distinct types of dementia [126]. However, more explorations are still needed to determine how specific vascular pathologi-cal changes influence tau protein metabolism in both aging and dementia and vice versa, and address in depth the mechanisms underlying the increase in CSF tau, the neuroradiological evi-dence of axonal changes and the neurobiochemi-cal loss and role of posttranslational modifica-tions (e.g., hyperphosphorylation) of tau protein in VaD.
Financial and competing interests disclosurePart of this review was included in a MSci thesis, submitted to Newcastle University (Mosi Li). Elizabeta B Mukaetova-Ladinska was supported by Alzheimer’s Society, London, UK. The authors have no other relevant affiliations or financial involvement with any other organizations or entity with financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from the disclosed.
No writing assistance was utilized in the production of the manuscript.
EXECUTivE SUMMARY
Vascular dementia
● Prevalence rates of vascular dementia double every 5 years, and range from 1.5% (70–75 years) to 15% in those over the age of 80 years.
● The highest proportion of VaD is in older Asian population, accounting for 38% of all dementia cases.
● There is a paucity of therapeutic advances available for subjects with VaD.
tau protein in ischemic injury & vascular dementia
● Animal studies indicate tau protein alterations may be an early pathological change in response to ischemic mechanisms in the cerebral neurons.
● CSF measures of total tau are consistently increased in VaD subjects, providing further evidence for the widespread axonal damage in VaD.
Conclusions
● tau protein role is poorly investigated in VaD.
● Further studies are needed to explore the effect of vascular pathology upon tau protein metabolism in both aging and dementia.
● The link between MAPT polymorphism rs1467967 and VaD needs further exploration.
● Since vascular incidents may halt the tau protein processing to neurofibrillary pathology, identifying the molecular mechanisms of tau protein changes in VaD has a potential for further development of novel anti-dementia treatments.

Future Neurol. (2015) 10(6)572
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group
ReferencesPapers of special note have been highlighted either as • of interest or •• of considerable interest
1 Roman GC. The Epidemiology of vascular dementia. Handb Clin Neurol. 89, 639–658 (2009).
2 Seshadri S, Beiser A, Kelly-Hayes M et al. The lifetime risk of stroke: estimates from the Framingham Study. Stroke 37(2), 345–350 (2006).
3 Fratiglioni L, De Ronchi D, Agüero-Torres H. Worldwide prevalence and incidence of dementia Drugs Aging 15(5), 365–375 (1999).
•• Reviewsprevalenceandincidencedatafordementiareportedintheinternationalliteratureover10yearsperiod.
4 Zhang ZX, Zahner GE, Roman GC et al. Dementia subtypes in China: prevalence in Beijing, Xian, Shanghai, and Chengdu’. Arch Neurol. 62(3), 447–453 (2005).
5 Liu J, Wan LN, Tan JP. Dementia in China: current status. Neurology 81(12), 1077–1078 (2013).
6 Blennow Kde Leon MJ, Zetterberg H. Alzheimer’s disease. Lancet 368(9533), 387–403 (2006).
7 Kalaria RN. Comparison between Alzheimer’s disease and vascular dementia: implications for treatment. Neurol. Res. 25(6), 661–664 (2003).
••ComparesriskfactorsandneuropathologybetweenAlzheimer’sdisease(AD)andvasculardementia(VaD).
8 Lewis H, Beher D, Cookson N et al. Quantification of Alzheimer pathology in ageing and dementia: age-related accumulation of amyloid-beta(42) peptide in vascular dementia. Neuropathol. Appl. Neurobiol. 32(2), 103–118 (2006).
• ReportsthatbrainAβaccumulatesincreasinglywithageinVaDsubjectsmoresothaninelderlywithoutcerebrovasculardisease.
9 Kalaria R. Similarities between Alzheimer’s disease and vascular dementia. J. Neurol. Sci. 203, 29–34 (2002).
•• ProvidesevidenceofacausalconnectionbetweenstrokeorCVDandAD.
10 Joachim CL, Morris JH, Selkoe DJ. Clinically diagnosed Alzheimer’s disease: autopsy results in 150 cases. Ann. Neurol. 24(1), 50–56 (1988).
11 Kemppainen NM, Scheinin NM, Koivunen J et al. Five-year follow-up of 11C-PIB uptake in Alzheimer’s disease and MCI. Eur. J. Nucl. Med. Mol. Imaging 41(2), 283–289 (2014).
12 Yang L, Rieves D, Ganley C. Brain amyloid imaging FDA approval of florbetapir F18 injection. N. Engl. J. Med. 367(10), 885–887 (2012).
13 Medina M, Avila J. New perspectives on the role of tau in Alzheimer’s disease. Implications for therapy. Biochem. Pharmacol. 88(4), 540–547 (2014).
•• ReviewsemergingtherapeuticstrategiesaimedattreatingtheunderlyingcausesoftaupathologyintauopathiesandAD.
14 Wischik CM, Novak M, Edwards PC, Klug A, Tichelaar W, Crowther RA. Structural characterization of the core of the paired helical filament of Alzheimer-Disease. Proc. Natl. Acad. Sci. USA 85(13), 4884–4888 (1988).
•• Demonstratesthatpairedhelicalfilaments(PHFs)consistoftwostructurallydistinctparts:anexternalfuzzyregionandapronase-resistantcorestructure,bothcontainingdistincttauproteinepitopes.
15 Wischik CM, Novak M, Thogersen HC et al. Isolation of a fragment of tau-derived from the core of the paired helical filament of Alzheimer-Disease. Proc. Natl. Acad. Sci. USA 85(12), 4506–4510 (1988).
•• DescribesisolationoftauproteinfragmenttightlyboundtothePHFcore.
16 Wischik CM, Harrington CR, Storey JM. tau-aggregation inhibitor therapy for Alzheimer’s disease Biochem. Pharmacol. 88(4), 529–539 (2014).
17 Peng D, Yuan X, Zhu R. Memantine hydrochloride in the treatment of dementia subtypes. J. Clin. Neurosci. 20(11), 1482–1485 (2013).
18 Rockwood K, Mitnitski A, Black SE et al. Cognitive change in donepezil treated patients with vascular or mixed dementia. Can. J. Neurol. Sci. 40(4), 564–571 (2013).
19 Birks J, Craig D. Galantamine for vascular cognitive impairment. Cochrane Database Syst. Rev. 4, CD004746 (2013).
20 Birks J, McGuinness B, Craig D. Rivastigmine for vascular cognitive impairment. Cochrane Database Syst. Rev. 5, CD004744 (2013).
21 Kwon KJ, Kim MK, Lee EJ et al. Effects of donepezil, an acetylcholinesterase inhibitor, on neurogenesis in a rat model of vascular dementia. J. Neurol. Sci. 347(1–2), 66–77 (2014).
22 Mortazavian SM, Parsaee H, Mousavi SH et al. Acetylcholinesterase inhibitors promote angiogenesis in chick chorioallantoic membrane and inhibit apoptosis of
endothelial cells. Int. J. Alzheimers Dis. 2013, 121068 (2013).
23 Elhusseiny A, Hamel E. Muscarinic but not nicotinic acetylcholine receptors mediate a nitric oxide-dependent dilation in brain cortical arterioles: a possible role for the M5 receptor subtype. J. Cereb. Blood. Flow Metab. 20(2), 298–305 (2000).
24 Yamada M, Lamping KG, Duttaroy A et al. Cholinergic dilation of cerebral blood vessels is abolished in M(5) muscarinic acetylcholine receptor knockout mice. Proc. Natl Acad. Sci. USA 98(24), 14096–14101 (2001).
25 Schliebs R, Arendt T. The cholinergic system in aging and neuronal degeneration. Behav Brain Res 221(2), 555–563 (2011).
26 Goedert M, Spillantini MG. A century of Alzheimer’s disease. Science 314(5800), 777–781 (2006).
27 Binder LI, Frankfurter A, Rebhun LI. The distribution of tau in the mammalian central nervous-system. J. Cell. Biol. 101(4),1371–1378 (1985).
•• Reportsthattauproteinisneuronspecificandrestrictedtoaxons.
28 Ebneth A, Godemann R, Stamer K, Illenberger S, Trinczek B, Mandelkow E. Overexpression of tau protein inhibits kinesin-dependent trafficking of vesicles, mitochondria, and endoplasmic reticulum: Implications for Alzheimer’s disease. J. Cell. Biol. 143(3),777–794 (1998).
29 Ittner LM, Ke YD, Delerue F et al. Dendritic function of tau mediates amyloid-beta toxicity in Alzheimer’s disease mouse models. Cell 142(3), 387–397 (2010).
30 Goedert M, Spillantini MG, Jakes R, Rutherford D, Crowther RA. Multiple isoforms of human microtubule-associated protein tau: Sequences and localization in neurofibrillary tangles of Alzheimer’s disease. Neuron 3(4), 519–526 (1989).
•• Reportsthesequencesofisoformsofhumantauproteinisoforms,withmultipletauproteinisoformsbeingincorporatedintoneurofibrillarytanglesinAD.
31 Andreadis A, Brown WM, Kosik KS. Structure and novel exons of the human tau gene. Biochemistry 31(43), 10626–10633 (1992).
32 Lee G, Neve RL, Kosik KS. The microtubule binding domain of tau protein. Neuron 2(6), 1615–1624 (1989).
•• Describesthemicrotubulebindingdomainoftauprotein,containingthree18aminoacidrepeatedsequences,whiletheamino-terminalhalfoftheproteindoesnotbind.

573future science group www.futuremedicine.com
tau protein, ischemic injury & vascular dementia REviEW
33 Kovacech B, Novak M. tau truncation is a productive posttranslational modification of neurofibrillary degeneration in Alzheimer’s disease. Curr. Alz. Res. 7(8), 708–716 (2010).
34 Mukaetova-Ladinska EB, Garcia-Siera F, Hurt J et al. Staging of cytoskeletal and beta-amyloid changes in human isocortex reveals biphasic synaptic protein response during progression of Alzheimer’s disease. Am. J. Pathol. 157(2), 623–636 (2000).
35 Iqbal K, Liu F, Gong CX, Alonso AD, Grundke-Iqbal I. Mechanisms of tau-induced neurodegeneration. Acta Neuropathologica (Berl) 118(1), 53–69 (2009).
36 Iqbal K, Gong CX, Liu F. Microtubule-associated protein tau as a therapeutic target in Alzheimer’s disease. Expert Opin. Ther. Targets 18(3), 307–318 (2014).
37 Wischik CM, Edwards PC, Lai RY et al. Quantitative analysis of tau protein in paired helical filament preparations: Implications for the role of tau protein phosphorylation in PHF assembly in Alzheimer’s disease. Neurobiol. Aging 16(3), 409–417 (1995).
38 Grundke-Iqbal I, Iqbal K, Quinlan M, Tung YC, Zaidi MS, Wisniewski HM. Microtubule-associated protein tau. a component of Alzheimer paired helical filaments. J. Biol. Chem.261(13), 6084–6089 (1986).
39 Andreasen N, Sjogren M, Blennow K. CSF markers for Alzheimer’s disease: total tau, phospho-tau and Abeta42. World J. Biol. Psychiatry 4(4),147–155 (2003).
40 Goedert M, Jakes R. Mutations causing neurodegenerative tauopathies Biochim. Biophys. Acta 1739(2–3), 240–250 (2005).
41 Wierzba-Bobrowicz T, Lewandowska E, Zaremba J et al. Frontotemporal lobar degeneration with MAPT mutation in an Italian-Polish family. A case report. Folia Neuropathol. 52(4), 457–466 (2014).
42 Kovacs GG, Milenkovic I, Wöhrer A et al. Non-Alzheimer neurodegenerative pathologies and their combinations are more frequent than commonly believed in the elderly brain: a community-based autopsy series. Acta Neuropathol. (Berl) 126(3), 365–384 (2013).
43 Kaerst L, Kuhlmann A, Wedekind D, Stoeck K, Lange P, Zerr I. Cerebrospinal fluid biomarkers in Alzheimer’s disease, vascular dementia and ischemic stroke patients: a critical analysis. J. Neurol. 260(11), 2722–2727 (2013).
•• ReportschangesintheCSFprofilebetweenAD,VaDandacuteischemia,withtotaltauCSFlevelsbeingusefulindifferentiating
VaDfromstrokesubjects.
44 Sadowski M, Pankiewicz J, Scholtzova H et al. Links between the pathology of Alzheimer’s disease and vascular dementia. Neurochem. Res. 29(6), 1257–1266 (2004).
45 Borenstein AR, Wu Y, Bowen JD et al. Incidence rates of dementia, Alzheimer disease, and vascular dementia in the Japanese American oopulation in Seattle, WA: the Kame project. Alzheimer Dis. Assoc. Disord. 28(1), 23–29 (2014).
46 Toledo JB, Arnold SE, Raible K et al. Contribution of cerebrovascular disease in autopsy confirmed neurodegenerative disease cases in the National Alzheimer’s Coordinating Centre. Brain 136(Pt 9), 2697–2706 (2013).
•• Aneuropathologialstudyexploringrelevanceofcerebrovasculardisease,vascularpathologyandvascularriskfactorsindementa–reportsthatwhencerebrovasculardiseasepresent,patientswithADhaverelativelylowerburdensofNFTs.
47 Brayne C, Richardson K, Matthews FE et al. Neuropathological correlates of dementia in over–80–year-old brain donors from the population-based camrbidge city over 75s cohort (CC75C) study. J. Alzheimers Dis. 18(3), 645–658 (2009).
•• Correlativeclinico-neuropathologicalstudyreportingthatvascularpathologies,especiallymicroinfarcts,aremorecommoninthosewithclinicaldiagnosesofVaD,butnototherdementiasubtypes.
48 Mukaetova-Ladinska EB, Abdel-All Z, Mugica ES et al. tau proteins in the temporal and frontal cortices in patients with vascular dementia. J. Neuropathol. Exp. Neurol. 74(2), 148–157 (2015).
•• Reportsthatchangesinmicrovascularormicrostructuraltissueintegrityduetoischemicinjuryinolderagemaymodifytauproteinmetabolismorphosphorylation,andthushaveeffectsontheburdenofneurofibrillarypathology.
49 Lee VM, Balin BJ, Otvos L Jr, Trojanowski JQ. A68:A major subunit of paired helical filaments and derivatized forms of normal tau. Science 251(4994), 675–678 (1991).
• ProvidestheaminoacidsequenceandimmunologicaldatathatA68,althoughindistinguishablefromtauprotein,isphosphorylated.
50 *Novak M, Kabat J, Wischik CM. Molecular characterization of the minimal protease resistant tau unit of the Alzheimer’s disease paired helical filament. EMBO J. 12(1),
365–370 (1993).
• IdentifiestheminimalproteaseresistanttauunitofthecorePHFs.
51 Lee MJ, Seo SW, Na DL et al. Synergistic effects of ischemia and beta-amyloid burden on cognitive decline in patients with subcortical vascular mild cognitive impairment. JAMA Psychiatry 71(4), 412–422 (2014).
52 Gouw AA, Seewann A, Vrenken H et al. Heterogeneity of white matter hyperintensities in Alzheimer’s disease: Post-mortem quantitative MRI and neuropathology. Brain 131(Pt 12), 3286–3298 (2008).
53 Dewar D, Dawson D. tau-protein is altered by focal cerebral-ischemia in the rat – an immunohistochemical and immunoblotting study. Brain Res 684(1), 70–78 (1995).
•• tauproteinisdephosphorylatedand/ordegradedinaxonsandsomeneuronalperikaryainresponsetofocalcerebralischaemia.
54 Uchihara T, Nakamura A, Arai T, Ikeda K, Tsuchiya K. Microglial tau undergoes phosphorylation-independent modification after ischemia. Glia 45(2), 180–187 (2004).
55 Irving EA, Yatsushiro K, McCulloch J, Dewar D. Rapid alteration of tau in oligodendrocytes after focal ischemic injury in the rat: Involvement of free radicals. J. Cereb. Blood Flow Metab. 17(6), 612–622 (1997).
56 Shackelford DA, Yeh RY. Dephosphorylation of tau during transient forebrain ischemia in the rat. Mol. Chem. Neuropathol. 34(2–3), 103–120 (1998).
57 Pluta R, Ulamek M, Jablonski M. Alzheimer’s mechanisms in ischemic brain degeneration. Anat. Rec. (Hoboken) 292(12), 1863–1881 (2009).
58 Wen Y, Yang SH, Liu R, Brun-Zinkernagel AM, Koulen P, Simpkins JW. Transient cerebral ischemia induces aberrant neuronal cell cycle re-entry and Alzheimer’s disease-like tauopathy in female rats. J. Biol. Chem. 279(21), 22684–22692 (2004).
59 Zlokovic B. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat. Rev. Neurosci. 12(12), 723–738 (2011).
•• Examinesmechanismsofblood–brainbarrierdysfunctionasaresultofvascularchangesandhighlightstherapeuticopportunitiesrelatingtoneurovasculardeficits.
60 Bell RD, Winkler EA, Singh I et al. Apolipoprotein E controls cerebrovascular

Future Neurol. (2015) 10(6)574
REviEW Mukaetova-Ladinska, Li & Kalaria
future science group
integrity via cyclophilin A. Nature 485(7399), 512–516 (2012).
61 Sagare AP, Bell RD, Zhao Z et al. Pericyte loss influences Alzheimer-like neurodegeneration in mice. Nat. Commun. 4, 2932 (2013).
62 Winkler EA, Sagare AP, Zlokovic BV. The pericyte: a forgotten cell type with important implications for Alzheimer’s disease? Brain Pathol 24(4), 371–386 (2014).
63 Forman MS, Lal D, Zhang B et al. Transgenic mouse model of tau pathology in astrocytes leading to nervous system degeneration. J. Neurosci. 25(14), 3539–3550 (2005).
64 Blair LJ, Frauen HD, Zhang B et al. tau depletion prevents progressive blood-brain barrier damage in a mouse model of tauopathy. Acta Neuropathol. Commun. 8 (2015).
65 Liu B, Tang Y, Shen Y, Cen L, Han M. Cerebrospinal fluid tau protein in differential diagnosis of Alzheimer’s disease and vascular dementia in Chinese population: A Meta-Analysis. Am. J. Alzheimers Dis. Other Demen. 29(2), 116–122 (2014).
66 Arai H, Satoh-Nakagawa T, Higuchi M et al. No increase in cerebrospinal fluid tau protein levels in patients with vascular dementia. Neurosci. Lett. 256(3), 174–176 (1998).
67 de Jong D, Jansen RW, Kremer BP, Verbeek MM. Cerebrospinal fluid amyloid beta(42)/phosphorylated tau ratio discriminates between Alzheimer’s disease and vascular dementia. J. Gerontol. A Biol. Sci. Med. Sci. 61(7), 755–758 (2006).
68 Schonknecht P, Pantel J, Hartmann T et al. Cerebrospinal fluid tau levels in Alzheimer’s disease are elevated when compared with vascular dementia but do not correlate with measures of cerebral atrophy. Psychiatry Res. 120(3), 231–238 (2003).
69 Stefani A, Bernardini S, Panella M. AD with subcortical white matter lesions and vascular dementia: CSF markers for differential diagnosis. J. Neurol. Sci. 237(1–2), 83–88 (2005).
70 Wallin A, Sjögren M. Cerebrospinal fluid cytoskeleton proteins in patients with subcortical white-matter dementia. Mech. Ageing. Dev. 22(16), 1937–1949 (2001).
71 Hjalmarsson C, Bjerke M, Andersson B et al. Neuronal and glia-related biomarkers in cerebrospinal fluid of patients with acute ischemic stroke. J. Cent. Nerv. Syst. Dis. 6, 51–58 (2014).
72 Rosseels J, Van den Brande J, Violet M et al. tau monoclonal antibody generation based on humanized yeast models: impact on tau
oligomerization and diagnostics’. J. Biol. Chem. 290(7), 4059–4074 (2015).
73 Liguori C, Stefani A, Sancesario G, Sancesario GM, Marciani MG, Pierantozzi M. CSF lactate levels, tau proteins, cognitive decline: a dynamic relationship in Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 86(6). 655–659 (2015).
74 Hermann P, Romero C, Schmidt C, Reis C, Zerr I. CSF biomarkers and neuropsychological profiles in patients with cerebral small-vessel disease. PLoS One 9(8), e105000 (2014).
75 Kester MI, Goos JD, Teunissen CE et al. Associations between cerebral small-vessel disease and Alzheimer disease pathology as measured by cerebrospinal fluid biomarkers’. JAMA Neurol 71(7), 855–862 (2014).
• Cross-sectionalstudyover10yearsperiod,reportingthatCSFAβaappearsaggravatedinpatientswithcerebralsmall-vesseldisease,especiallyinapolipoproteinEε4carriers.
76 Krishnan S, Rani P. Evaluation of selenium, redox status and their association with plasma amyloid/tau in Alzheimer’s disease. Biol Trace Elem Res 158(2), 158–165 (2014).
77 Paraskevas GP, Kapaki E, Papageorgiou SG et al. CSF biomarker profile and diagnostic value in vascular dementia. Eur. J. Neurol. 16(2), 205–211 (2009).
78 Ravaglia S, Bini P, Sinforiani E et al. Cerebrospinal fluid levels of tau phosphorylated at threonine 181 in patients with Alzheimer’s disease and vascular dementia. Neurol. Sci. 29(6), 417–423 (2008).
79 Blennow K, Wallin A, Agren H, Spenger C, Siegfried J, Vanmechelen E. tau protein in cerebrospinal fluid – a biochemical marker for axonal degeneration in Alzheimer disease? Mol. Chem. Neuropathol. 26(3), 231–245 (1995).
80 Andreasen N, Vanmechelen E, Van de Voorde A et al. Cerebrospinal fluid tau protein as a biochemical marker for Alzheimer’s disease: A community based follow up study. J. Neurol. Neurosurg. Psychiatry 64(3), 298–305 (1998).
81 Herbert MK, Aerts MB, Kuiperij HB et al. Addition of MHPG to Alzheimer’s disease biomarkers improves differentiation of dementia with Lewy bodies from Alzheimer’s disease but not other dementias. Alzheimers Dement. 10(4), 448–455 (2013).
82 Schoonenboom NSM, Reesink FE, Verwey NA et al. Cerebrospinal fluid markers for differential dementia diagnosis in a large memory clinic cohort. Neurology 78(1), 47–54 (2012).
83 Herbert MK, Aerts MB, Kuiperij HB et al. Addition of MHPG to Alzheimer’s disease biomarkers improves differentiation of dementia with Lewy bodies from Alzheimer’s disease but not other dementias. Alzheimers Dement. 10(4), 448–455 (2014).
84 Amadoro G, Corsetti V, Sancesario GM et al. Cerebrospinal fluid levels of a 20–22 kDa NH2 fragment of human tau provide a novel neuronal injury biomarker in Alzheimer’s disease and other dementias. J. Alzheimers Dis. 42(1), 211–226 (2014).
85 Leszek J, Malyszczak K, Janicka B, Kiejna A, Wiak A. Total tau in cerebrospinal fluid differentiates Alzheimer’s disease from vascular dementia. Med. Sci. Monit. 9(11), CR484–488 (2003).
86 Skogseth RE, Fladby T, Mulugeta E, Aarsland D. [Biomarkers in spinal fluid of patients with dementia]. Tidsskr Nor Laegeforen 131(22), 2235–2238 (2011).
87 Bibl M, Mollenhauer B, Esselmann H et al. Cerebrospinal fluid neurochemical phenotypes in vascular dementias: original data and mini-review. Dement. Geriatr. Cogn. Disord. 25(3), 256–265 (2008).
88 Hesse C, Rosengren L, Vanmechelen E et al. Cerebrospinal fluid markers for Alzheimer’s disease evaluated after acute ischemic stroke. J. Alzheimers Dis. 2(3–4), 199–206 (2000).
89 Hesse C, Rosengren L, Andreasen N et al. Transient increase in total tau but not phospho-tau in human cerebrospinal fluid after acute stroke. Neurosci. Lett. 297(3), 187–190 (2001).
90 Kowall NW, Kosik KS. Axonal disruption and aberrant localization of tau-Protein characterize the neuropil pathology of Alzheimer’s disease. Ann. Neurol. 22(5), 639–643 (1987).
91 Wen Y, Yang SH, Liu R, Simpkins JW. Transient cerebral ischemia induces site-specific hyperphosphorylation of tau protein. Brain Res. 1022(1–2), 30–38 (2004).
92 Itoh N, Arai H, Urakami K et al. Large-scale, multicenter study of cerebrospinal fluid tau protein phosphorylated at serine 199 for the antemortem diagnosis of Alzheimer’s disease. Ann. Neurol. 50(2), 150–156 (2001).
93 Kalaria RN, Ballard C. Overlap between pathology of Alzheimer disease and vascular dementia Alzheimer Dis. Assoc. Disorders 13, S115–S123 (1999).
94 Jia JP, Meng R, Sun YX, Sun WJ, Ji XM, Jia LF. Cerebrospinal fluid tau, A beta(1–42) and inflammatory cytokines in patients with Alzheimer’s disease and vascular dementia. Neurosci. Lett. 383(1–2), 12–16 (2005).

575future science group www.futuremedicine.com
tau protein, ischemic injury & vascular dementia REviEW
95 Hartig W, Reichenbach A, Voigt C et al. Triple fluorescence labelling of neuronal, glial and vascular markers revealing pathological alterations in various animal models. J. Chem. Neuroanat. 37(2), 128–138 (2009).
96 Morioka M, Kawano T, Yano S et al. Hyperphosphorylation at serine 199/202 of tau factor in the gerbil hippocampus after transient forebrain ischemia. Biochem. Biophys. Res. Commun. 347(1), 273–278 (2006).
97 Han F, Ali Raie A, Shioda N, Qin ZH, Fukunaga K. Accumulation of beta-amyloid in the brain microvessels accompanies increased hyperphosphorylated tau proteins following microsphere embolism in aged rats. Neuroscience 153(2), 414–427 (2008).
•• MicrosphereembolisminbrainmicrovesselsleadstostromgAβaccumulationinbrainparenchyma,withhyperphosphorylatedtauproteinsincreasedinneuronssurroundingregionsofAβaccumulation.
98 Mazzone T, Chait A, Plutzky J. Cardiovascular disease risk in type 2 diabetes mellitus: Insights from mechanistic studies. Lancet 371(9626), 1800–1809 (2008).
99 Currais A, Prior M, Lo D, Jolivalt C, Schubert D, Maher P. Diabetes exacerbates amyloid and neurovascular pathology in aging-accelerated mice. Aging Cell 11(6), 1017–1026 (2012).
100 Liao GH, Zhou M, Cheung S et al. Reduced early hypoxic/ischemic brain damage is associated with increased GLT–1 levels in mice expressing mutant (P301L) human tau. Brain Res 1247, 159–170 (2009).
101 Jaworski T, Lechat B, Demedts D. Dendritic degeneration neurovascular defects, and inflammation precede neuronal loss in a mouse model for tau-mediated neurodegeneration. Am J Pathol 179(4), 2001–2015 (2011).
102 Bourasset F, Ouellet M, Tremblay C. Reduction of the cerebrovascular volume in a transgenic mouse model of Alzheimer’s disease. Neuropharmacology 56(4), 808–813 (2009).
103 Do TM, Alata W, Dodacki A. Altered cerebral vascular volumes and solute transport at the blood-brain barriers of two transgenic mouse models of Alzheimer’s disease. Neuropharmacology 81, 311–317 (2014).
104 Poduslo JF, Curran GL, Wengenack TM, Malester B, Duff K. Permeability of proteins at the blood-brain barrier in the normal adult mouse and double transgenic mouse model of Alzheimer’s disease. Neurobiol Dis 8(4), 555–567 (2001).
105 Head BP, Peart JN, Panneerselvam M et al. Loss of Caveolin–1 accelerates neurodegeneration and aging. Plos One 5(12), e15697 (2010).
106 Koike MA, Garcia FG, Kitazawa M, Green KN, LaFerla FM. Long term changes in phospho-APP and tau aggregation in the 3xTg-AD mice following cerebral ischemia. Neurosci. Lett. 495(1), 55–59 (2011).
•• Transientglobalischemicinsultinaged3xTg-ADmicedoesnotincreasethelevelsofAβ,butresultsinincreaseininsolubletotaltauprotein3-monthspost-injury.
107 Whitehead SN, Massoni E, Cheng G. Triflusal reduces cerebral ischemia induced inflammation in a combined mouse model of Alzheimer’s disease and stroke. Brain Res. 1366, 246–256 (2010).
108 Lee JS, Im DS, An YS, Hong JM, Gwag BJ, Joo IS. Chronic cerebral hypoperfusion in a mouse model of Alzheimer’s disease: an additional contributing factor of cognitive impairment. Neurosci. Lett. 489(2), 84–88 (2011).
109 Davis J, Xu F, Deane R et al. Early-onset and robust cerebral microvascular accumulation of amyloid beta-protein in transgenic mice expressing low levels of a vasculotropic Dutch/Iowa mutant form of amyloid beta-protein precursor. J. Biol. Chem. 279(19), 20296–20306 (2004).
110 Wilcock DM, Lewis MR, Van Nostrand WE et al. Progression of amyloid pathology to Alzheimer’s disease pathology in an amyloid precursor protein transgenic mouse model by removal of nitric oxide synthase 2. J. Neurosci. 28(7), 1537–1545 (2008).
111 Van Nostrand WE, Xu F, Rozemuller AJ, Colton CA. Enhanced capillary amyloid angiopathy-associated pathology in Tg-SwDI mice with deleted nitric oxide synthase 2. Stroke 41(10 Suppl), S135–138 (2010).
112 Peng Y, Hu Y, Xu S et al. Potassium 2-(1–hydroxypentyl)-benzoate improves memory deficits and attenuates amyloid and tau pathologies in a mouse model of Alzheimer’s disease. J. Pharmacol. Exp. Ther. 350(2), 361–374 (2014).
113 Zhao W, Xu S, Peng Y et al. Potassium 2–(1–hydroxypentyl)-benzoate improves learning and memory deficits in chronic cerebral hypoperfused rats. Neurosci. Lett. 541, 155–160 (2013).
114 Kalaria RN, Kenny RA, Ballard CG, Perry R, Ince P, Polvikoski T. Towards defining the neuropathological substrates of vascular dementia. J. Neurol. Sci. 226(1–2), 75–80 (2004).
115 Li C, Ebrahimi A, Schluesener H. Drug pipeline in neurodegeneration based on transgenic mice models of Alzheimer’s disease. Ageing Res. Rev. 12(1), 116–140 (2013).
116 Tatemichi TK, Desmond DW, Prohovnik I. Strategic infarcts in vascular dementia. A clinical and brain imaging experience. Arzneimittelforschung 45(3A), 371–385 (1995).
117 Ward SM, Himmelstein DS, Lancia JK, Binder LI. tau oligomers and and tau toxicity in neurodegenerative disease. Biochem. Soc. Trans. 40(4), 667–671 (2012).
118 Baloyannis SJ. Pathological alterations of the climbing fibres of the cerebellum in vascular dementia: a Golgi and electron microscope study. J. Neurol. Sci. 257(1–2), 56–61 (2007).
119 Wang M, Iliff JJ, Liao Y et al. Cognitive deficits and delayed neuronal loss in a mouse model of multiple microinfarcts. J. Neurosci. 32(50), 17948–17960 (2012).
120 Holth JK, Bomben VC, Reed JG et al. tau loss attenuates neuronal network hyperexcitability in mouse and Drosophila genetic models of epilepsy. J. Neurosci. 33(4), 1651–1659 (2013).
121 Allan LM, Rowan EN, Firbank MJ. Long term incidence of dementia, predictors of mortality and pathological diagnosis in older stroke survivors. Brain 134(Pt 12), 3716–3727 (2011).
122 Firbank MJ, He J, Blamire AM. Cerebral blood flow by arterial spin labeling in poststroke dementia. Neurology 76(17), 478–484 (2011).
123 Ning M, Zhang Z, Chen Z. Genetic evidence that vascular dementia is related to Alzheimer’s disease: genetic association between tau polymorphism and vascular dementia in the Chinese population. Age Ageing 40(1), 12512–12518 (2011).
124 Elias-Sonnenschein LS, Helisalmi S, Natunen T et al. Genetic loci associated with Alzheimer’s disease and cerebrospinal fluid biomarkers in a Finnish case-control cohort. PLoS One 8(4), e59676 (2013).
125 Zheng GQ, Wang XM, Wang Y, Wang XT. tau as a potential novel therapeutic target in ischemics stroke. J. Cell. Biochem. 109(1), 26–29 (2010).
• Addressesdevelopmentofnoveltherapeutictargetsinischaemicstroke,addressingregulationofphosphorylationoftauproteinasapotentialnewtherapeutictarget.
126 Boban M, Sarac H, Mimica N et al. CSF tau proteins in differential diagnosis of dementia. Trans. Neurosci. 1(1), 43–48 (2010).



![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://img.pdfslide.us/doc/110x75/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)