Embed Size (px)
Citation preview
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al national survey of neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A
This information is current as of June 1 1996
httpwwwneurologyorgcontent4661534fullhtmlthe World Wide Web at
The online version of this article along with updated information and services is located on
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright Copyright 1996 by Advanstar Communications
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Antiepileptic medication and oral contraceptive interactions
A national survey of neurologists and obstetricians GL Krauss MD J Brandt PhD M Campbell RN C Plate BS and M Summerfield
Article abstract-Hepatic enzyme-inducing antiepileptic drugs (AEDs) lower oral contraceptive (OC) sex hormone levels approximately 40 and increase the risk of unplanned pregnancies in women with epilepsy AEDs also increase the risk of birth defects in offspring of women with epilepsy We performed a national survey to determine obstetriciansrsquo and neurologistsrsquo knowledge of OC and AED interactions and the risk of birth defects for women with epilepsy taking AEDs We received responses to a mailed questionnaire from 160 of 1000 neurologists (16) and 147 of 1000 obstetricians (15) from 47 states Practice demographics and ages of responders were typical for US neurologists and obstetricians Ninety-one percent of neurologists and 75 of obstetricians said they treat women with epilepsy of child-bearing age Only 4 of the neurologists and none of the obstetricians however knew the effects of the six most common AEDs on OCs even though 27 of neurologists and 21 of obstetricians reported OC failures in their patients taking AEDs Although increasing OC doses can compensate for insufficient OC sex hormone levels due to AEDs most physicians do not increase the doses Even though the risk of birth defects for the offspring of women with epilepsy is 4 to 6 up from the background level of 296 44 of neurologists thought the risk was lower (0 to 3) and some of the respondents guessed that it was as high as 50 Many neurologists and obstetricians do not have accurate information to counsel women with epilepsy properly about their contraceptive and pregnancy choices NEUROLOGY 199646 1534-1539
Antiepilepsy drugs (AEDs) are associated with two major reproductive risks for women with epilepsy of child-bearing age (1) an increased risk of unplanned pregnancies due to hepatic enzyme-inducing AEDs lowering sex hormone levels of oral contraceptives (OCs)rsquo (2) an increased risk of birth defect^^^ We conducted a national survey of obstetricians and neurologists to determine whether they were aware that enzyme-inducing AEDs decrease the effective- ness of OCs and whether their patients taking AEDs had become accidentally pregnant while taking OCs We also determined whether physicians accurately counsel women about their increased risk of birth defects due to AEDs
During the past 2 years we saw five women at Johns Hopkins Hospital with hormonal contracep- tive failures while taking AEDs These unexpected pregnancies caused major social and emotional dis- tress one woman also had a brain tumor one had mental retardation and epilepsy surgery was can- celed for a third We became concerned that neurolo- gists and obstetricians may not be aware of this drug interaction and that women with epilepsy taking AEDs are not being warned of their risk for acciden- tal pregnancies This is especially important because women with epilepsy are at an approximately 4 to 6 risk of birth defects (2-3X background) in their
offspring3 with even greater risks for high-risk group^^^ Physicians have been held legally responsi- ble for a ldquowrongful liferdquo when a woman was not in- formed of specific pregnancy risks associated with her AEDslsquoj
Over 80 women have been reported in the United States and United Kingdom with accidental preg- nancies due to enzyme-inducing AEDs interfering with O C S ~ gt ~ - ~ The enzyme-inducing AEDs associated with OC failures are carbamazepine phenytoin phe- nobarbital primidone and ethosuximide All reduce OC estradiol levels approximately 40 and may also decrease free progestin levels by increasing sex hor- mone-binding globulins12 Enzyme-inducing AEDs increase the expected OC failure ratelo of 01 to 3 by severalfold In one small study 7 of epilepsy patients taking OCs with AEDs had OC fai1ureslrsquo The nonhepatic enzyme-inducing AEDs -valproic acid and gabapentin- do not decrease OC levels and have not been associated with accidental pregnan- cies
Physicians can compensate for the influence of en- zyme-inducing AEDs on OC sex hormone levels by increasing OC estradiol doses from 20 to 35 pg to 50 kg especially if there is irregular or breakthrough menstrual bleeding on low-dose OCs27rsquo2-15 Because most reported OC failures have been with 50- to
From the Departments nf Neurology IDr Krauss Ms Campbell Ms Plate and Mr Summerfield and Psychiatry (Dr Brandt) Johns Hopkins University Baltimore MD Received July 11 1995 Accepted in final form October 2 1995 Address correspondence and reprint requests to Dr Gregory L Krauss Johns Hopkins Hospital Meyer 2-147 600 N Wolfe Street Baltimore MD 21287-7247
1534 Copyright S 1996 by the American Academy of Neurology
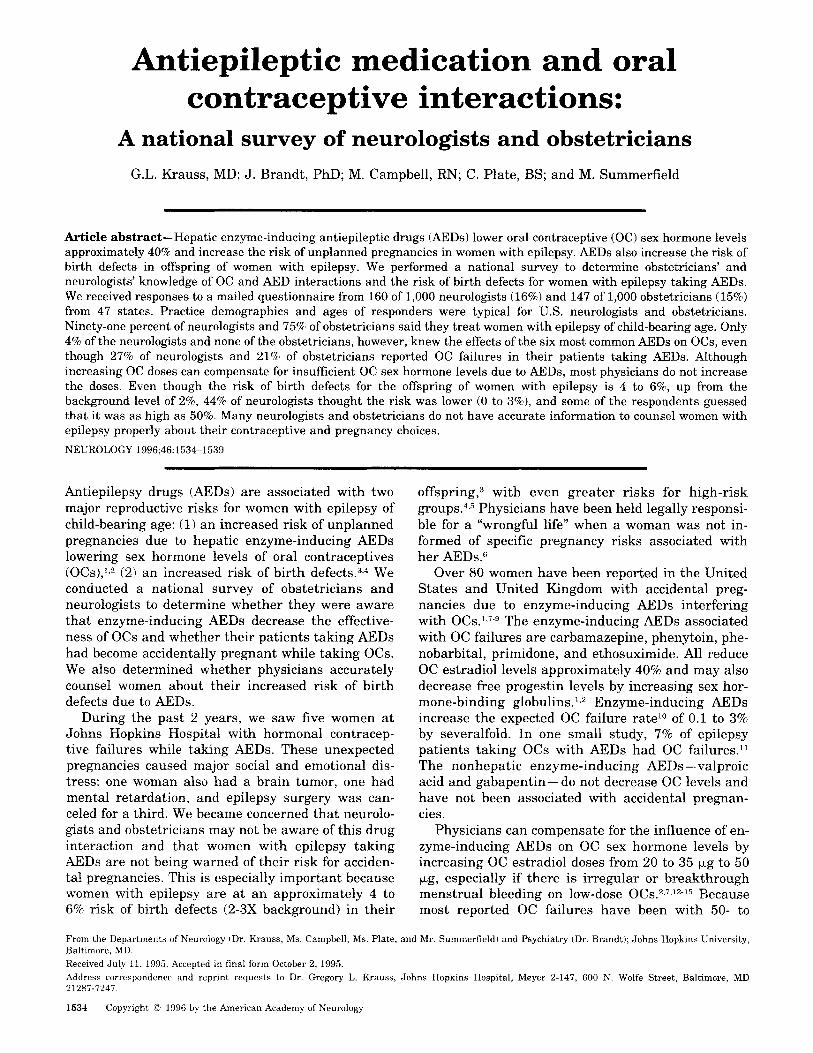
Table 1 Physician respondents
Survey neurologists National neurologists Survey obstetricians National obstetricians (1994) (1991-1992) (1994) (1992-1993)
-
Total responders
Mean age (range) (yr)
Work settings ()
Solo
Group Community Hospital
Med school
Research other
Board-Certified ()
Year of MD
160 (16)
453 (30-75) 445
316 232
513 373
33 154
112 203
26 38
925 776
1943-1990
80-kg doses these steps will not prevent all OC fail- ures but are likely to significantly reduce their fre- quency
Physicians caring for women with epilepsy may not be aware of these issues I t is particularly impor- tant to determine whether women with epilepsy are receiving accurate information about contraception because they are at increased risk for pregnancy complications and birth defects in their ~ffspr ing~
Methods Suruey We mailed surveys to a sample of 1000 neurologists and 1000 obstetriciadgynecologists randomly selected from a geographically stratified Ameri- can Medical Association ( M A ) master list of 10034 li- censed neurologists and 33208 licensed obstetricians in the United States This is a comprehensive list of nearly all active specialists The random selection of physicians was performed by sequentially selecting physicians from the AMA database listed by zip codes This resulted in a sample that included all states but also represented the relative population of physicians in various regions We asked the physicians to respond to a brief anonymous knowledge questionnaire without consulting texts or other sources Twenty questions probed physiciansrsquo practice de- mographics familiarity with AED and OC interactions knowledge of interactions between specific AEDs and OCs and whether physicians adjusted OC doses for patients taking AEDs To assess physiciansrsquo general awareness of reproductive health issues in women with epilepsy we also asked them to estimate the risk of birth defects in preg- nancies of women with epilepsy and whether they counsel women with epilepsy against pregnancy
The following questions were asked (1) Are you currently treating any women of child-bearing age with epilepsy (2) In counseling a pregnant woman with good seizure control on a single anticonvulsant what would you tell her the risk is of her having a baby with a birth defect (3) Do you generally recommend that women taking a single anticonvulsant not become pregnant be- cause of this risk (4) How familiar are you with the inter- actions between oral contraceptives and antiepileptic med- ications (5-12) To the best of your knowledge do the following antiepileptic medications interfere with levels of oral contraceptives phenytoin (Dilantin) carbamazepine (Tegretol) valproic acid (Depakote) phenobarbital primi-
Survey questions
147 (147)
424 (28-74) 420
341
507
58
58
876
66
12
36 33
925 71 1943-1992
done (Mysoline) ethosuximide (Zarontin) gabapentin (Neurontin) felbamate (Felbatol) (13) Do you have your patients adjust their oral contraceptive dose if they are taking antiepileptic medication (14) If ldquoYesrdquo what adjust- ment (15) Have any of your patients on antiepileptic med- ication accidentally become pregnant while taking oral contraceptives
Demographic questions were (16) age (17) year of MD (18) board certification and (19) primary work setting a general comments section (20) was provided
Questionnaires returned within 6 months of the mailing were included Responses were coded and analyzed using the SPSS for Windows statistical program Data for categorical responses were tabulated and continuous data are summarized by means ranges and variance One post-hoc response to the questionnaire was added Some neurologists did not adjust OC doses if their patients were taking antiepileptic medications (ldquonordquo to question 131 but they did refer patients to obstetricians for OC adjustments (comment under 14) Therefore ldquoyesrdquo ldquonordquo and ldquoreferrdquo were possible responses for neurologists to question 13
We tested six specific hypotheses separately for neurol- ogists and obstetricians using nonparametric (chi-square) and parametric analysis (independent t test and bivariate correlation) We did not correct for multiple comparisons to avoid type I1 statistical error The hypotheses were that obstetricians and neurologists are more likely to adjust OC doses for patients taking AEDs if (1) they knew that en- zyme-inducing AEDs interfere with OC levels (2) they were familiar with interactions between AEDs and OCs but did not necessarily recognize specific drug interactions (3) they had previously had patients on AEDs become acci- dentally pregnant while taking OCs (4) physicians with recent medical training would be most knowledgeable about OC-AED interactions (5) physiciansrsquo estimates of the risks of birth defects would influence whether they recommend against pregnancy and (6) physiciansrsquo knowl- edgeable about OC-AED interactions would provide more accurate estimates of the risks of birth defects than would physicians who were not aware of OC-AED interactions We also compared obstetriciansrsquo and neurologistsrsquo familiar- ity with and knowledge of OC-AED interactions and their estimates of the risk of malformations in offspring of women with epilepsy taking AEDs
Statisticat analysis
June 1996 NEUROLOGY 46 1535
Figure 1 Physiciansrsquo knowledge of OC interactions with six common AEDs (new AEDs excluded) AEDs carbamaz- epine phenytoin valproic acid phenobarbital primidone ethosuximide
Physicians were asked which of eight AEDs interfered with OCs Their knowledge of which AEDs interfere with OCs was estimated however using only six of eight AEDs (phenytoin carbamazepine valproic acid phenobarbital primidone and ethosuximide ) Gabapentin and felbamate were not included because they had been recently released at the time of the survey and were not recognized by many neurologists and most obstetricians Correct responses were tha t phenytoin carbamazepine phenobarbital primidone and ethosuximide interfere with OCs whereas valproic acid does notlsquo27-9
Results Characteristics of survey respondents A total of 160 neurologists (16) and 147 obstetricians (147) responded to the questionnaire (table 1) The ages work setting and geographic distribution for responders were representative of neurologists and obstetricians national- l ~ rsquo ~ rdquo The responders were from 47 states The largest numbers were in office-based practices with medical school graduation in the 1960s through 1980s
Most neurologists (91) and obstetricians (7596) said they treat women with epilepsy of child-bearing age Most neurolo- gists (75) and most obstetricians (59) believed they were moderately or very familiar with the interactions be- tween AEDs and OCs Physiciansrsquo actual knowledge of OC- AED interactions however was extremely poor When physicians were scored on their knowledge of whether six common AEDs interfered with OCs (phenytoin carbamaz- epine valproic acid phenobarbital primidone and etho- suximide) only 4 of the neurologists and none of the obstetricians were correct for all six AEDs (figure 1) The two new AEDs gabapentin and felbamate were excluded because they were not recognized by most physicians The average score for neurologistsrsquo knowledge of OC interac- tions with the six AEDs was 61 5 22 and for obstetri- cians was 378 f 19 Neurologists were both more famil- iar with ( t = 350 d f 297 p lt 0001) and more knowledgeable about ( t = 782 d f 292 p lt 0001) AED-OC interactions than obstetricians
Most neurologists (77 to 84) knew that phenytoin car- bamazepine and phenobarbital interfered with OCs but only 38 knew that valproic acid does not interfere with
Specialistsrsquo knowledge of OC-AED interactions
1536 NEUROLOGY 46 June 1996
Figure 2 Estimate of birth defect risk associated with AEDs
OCs Most obstetricians also knew that phenytoin inter- fered with OCs (77) but fewer knew that phenobarbital (54) carbamazepine (44) and primidone (17) lowered OC levels and only 29 know that valproic acid did not interfere with OCs Few neurologists and obstetricians knew whether ethosuximide or the two new AEDs gaba- pentin and felbamate interfere with OCs
Younger physicians were slightly more knowledgeable than older physicians about common AED-OC interactions although this was significant only for obstetricians (neurol- ogists r = 014 p = 009 obstetricians r = 030 p lt 0001)
Fewer than half of neurologists (41) and obstetricians (43) have patients adjust their OC doses if they are taking AEDs Moreover a number of physicians noted that they ldquoadjusted OC doses by lowering estrogen doses or using relatively low-dose 35-kg estrogen pills An additional 8 of neurologists refer their patients to obstetricians to have OC doses adjusted
There was a strong association between neurologistsrsquo and obstetriciansrsquo knowledge of which AEDs interfere with OCs and whether they adjust OC doses to compensate for AED effects (neurologists t = 277 d f 143 p = 0006 obstetricians t = 421 df 128 p lt 0001) Even physicians who were ldquofamiliarrdquo with this drug interaction but did not have accurate knowledge of which AEDs were involved usually adjusted their patientsrsquo OC doses for patients on AEDs 89 of neurologists and 76 of obstetricians famil- iar with OC-AED interactions adjust OC dosages for pa- tients on AEDs whereas only 19 of neurologists and 24 of obstetricians not familiar with OC-AED interactions ad- just OC dosages (neurologists chi-square 1043 p = 0001 obstetricians chi-square 1464 p = 00001)
Twenty-seven percent of neurologists and 21 of obste- tricians reported OC failure in their patients taking AEDs Neurologists whose patients had accidental pregnancies on OCs and AEDs were more likely to adjust OC doses (58 versus 35) than neurologists whose patients had not had such pregnancies (chi-square 633 p = 0011) Obstetri- cians whose patients had accidental pregnancies on OC and AEDs were more likely to adjust OCs than obstetri- cians who had not had patients with accidental pregnan- cies (57 versus 39) although this did not reach signifi- cance (chi-square 296 p = 0086)
Pregnancy risks and counseling Women with epilepsy have significant risks of approximately 4 to 6 for congen-
Factors influencing OC dosing
Table 2 Effects of AEDs on OC hormone levels
Enzyme-inducing AEDs
Phenobarbital
Phenytoin
Carbamazepine
Oxacarbamazepine Nonenzyme-inducing AEDs
Valproic acid
Gabapentin
-381
-490 -422
-470
110
60
Estradiol () -
~
Changes in 24-hour serum levels from baseline or control values No significant change References 1 2 7 20 23-25
ital malformations in their offspring compared with a background risk of approximately 23 This 2-3X in- creased risk is increased further for women with uncon- trolled seizures taking multiple AEDs5 or who belong to high-risk socioeconomic group^^ Despite this there was a wide variation in physiciansrsquo estimates of the risk of mal- formations with many physicians particularly neurolo- gists underestimating the risk (figure 2) When counseling a pregnant woman with good seizure control on a single antiepileptic medication obstetricians said they would es- timate a mean risk for birth defects of 689 (range 0 to 50) Most obstetricians (95) estimated a birth defect risk due to a single AED between 1 and 10 Over one- fifth (23) of obstetricians underestimated the risk as 0 to 3 In counseling a woman with epilepsy neurologists estimated a lower mean risk for birth defects than did obstetricians 475 (range 0 to 50) (neurologistsrsquo versus obstetriciansrsquo estimates t = 351 df 286 p = 001) Most neurologists (95) estimated a risk of birth defects be- tween 0 and 9 A large proportion of neurologists (44) underestimated the risk of birth defects as 0 to 3
Only 3 of neurologists and 5 of obstetricians recom- mend that their patients taking AEDs not become preg- nant Physiciansrsquo estimates of the risk of birth defects as- sociated with a single AED did not influence whether they would recommend that women taking single anticonvul- sants should avoid pregnancy (neurologists t = 139 df 147 p = 0165 obstetricians t = 078 df 132 p = 044) There was also no correlation between physiciansrsquo esti- mates of the risk of birth defects and their knowledge of OC-AED interactions (neurologists r = 005 p = 056 obstetricians r = 0 0 1 ~ = 081)
Table 3 Reported OC failures with AEDs
AED Accidental pregnancies
Phenobarbital
Phenytoin
Carbamazepine
Valproic acid
Ethosuximide
51
42
19
6 (0 monotherapy)
4
References 1 7 11 28
Norgestrel or norethindrone ()
- 187
-420
-397
-360
oo 30rsquo
Discussion Over one-fifth of neurologists and ob- stetricians reported accidental pregnancies in their patients taking AEDs with OCs Most physicians however did not know which common AEDs inter- fere with OCs do not adjust OC doses to overcome the effects of enzyme-inducing AEDs on sex hormone levels and did not know that valproic acid and gaba- pentin are nonenzyme-inducing alternatives to en- zyme-inducing AEDs Although physicians who were at least moderately familiar with OC-AED interac- tions tended to adjust OC doses for their patients it is unclear how they would do this without recogniz- ing specific AED-OC interactions These results oc- cur despite warnings of AED-OC interactions in pharmaceutical product inserts the Physiciansrsquo Desk Reference18 and in several medical reviews and edi- t o r i a l ~ ~ ~ ~ J ~ - ~ ~ Our survey suggests that a large num- ber of women in the United States with epilepsy are at risk for unplanned pregnancies while taking OCs
There are several limitations in our survey A re- sponse bias to the questionnaire is possible It is typical however for only a few mailed question- naires to be returned19 The geographic distribution practice types and ages of respondents were typical for American neurologists and obstetricians (see ta- ble l)16J7 Nonetheless the survey may have overes- timated physiciansrsquo lack of knowledge about AED complications for women with epilepsy particularly if nonrespondents were physicians who already knew about the reproductive risks of AEDs More likely however is that those who believed these issues are important would respond rather than those who do not recognize the reproductive complications associ- ated with AEDs This suggests in fact that any skew in the study would be toward overestimating physiciansrsquo knowledge of these issues Evidence that less-knowledgeable physicians were not over- represented in the survey is that a larger proportion of responders were board-certified specialists than the national average (see table 1) Another limitation is that several questions could not be asked directly without cuing other responses We could not ask for example questions to determine precisely how phy-
June 1996 NEUROLOGY 46 1537
Table 4 Suggestions for combining OCs and AEDs for women with epilepsy
1 Discuss contraceptive choices and the effects of enzyme- inducing AEDs (carbamazepine phenytoin phenobarbital primidone and ethosuximide) on OCs with all women of child-bearing years who have epilepsy This can be part of a general discussion of the risks of pregnancy and epilepsy
When treating women with epilepsy taking OCs continue to select AEDs according to recommended indications for epilepsy33
AED (valproic acid gabapentin vigabatrin) for women taking OCs
equivalent) for women taking enzyme-inducing AEDs who desire effective contraception Obstetricians and family physicians usually prescribe the OCs Counsel women that increased OC doses do not always protect from contraceptive failures due to AEDs but that OC failure rates are usually lower than with barrier methods alone
irregular menstrual bleeding while taking OCs Increase OC doses or switch contraceptives if irregular bleeding occurs
2
3 If AEDs are otherwise equivalent use a nonenzyme-inducing
4 Recommend OC doses of 50 pg estradiol (or mestranol
5 Have women with epilepsy monitor for breakthrough or
6 Advise women seeking very high levels of contraception protection that they may add spermicide or barrier contraception to their OCs
7 Alternative contraceptives that can be used for some women are medroxyprogesterone (Depo-Provera) and intrauterine devices Many pregnancies have occurred with levonorgestrol implant (ldquoNorplantrdquo) and enzyme-inducing AEDs
8 Oxcarbazepine lowers OC hormone levels whereas gabapentin and vigabatrin are nonenzyme-inducers that are unlikely to interfere with OCs The effects of lamotrigine and felbamate on OCs are unclear
Modified from references 7 13 15
sicians adjust OC doses whether physicians monitor patients for irregular menstrual bleeding as a sign of AED effects on OCs and how many total patients had accidental pregnancies due to AEDs
Enzyme-inducing AEDs including carbamaz- epine phenytoin phenobarbital primidone and ethosuximide decrease the effectiveness of OCs by lowering synthetic sex hormone levels Enzyme- inducing AEDs increase cytochrome P450 en- zymes12021 resulting in increased metabolism of syn- thetic estrogens (ethinyl estradiol and mestranol) and lowered serum levels of approximately 40 (ta- ble 2) 1 2 T Z2~25 Free progestin levels are also de- creased probably due to increased synthesis of sex hormone-binding globulins220 Valproic and two new AEDs- gabapentin and vigabatrin- do not induce hepatic P450 metabolism and are unlikely to interfere with OCs Gabapentin does not decrease estradiol levels24 and vigabatrin has not been stud- ied Oxcarbazepine lowers OC sex hormone levels2rdquo and is likely to interfere with OCs Effects of lam- otrigine and felbamate on OCs have not been stud- 1538 NEUROLOGY 46 June 1996
ied Lamotrigine is metabolized by hepatic glucu- ronidation however rather than by the microsomal P450 system and possibly may not stimulate sex hor- mone metabolism
Over 150 accidental pregnancies have been re- ported in patients taking enzyme-inducing AEDs primarily women from the United K i n g d ~ m ~ ~ ~ and including the minimum of 75 American patients reported in this survey17~s1126-28 Valproic acid a nonenzyme-inducing AED has not been associated with accidental pregnancies when used in mono- therapy (table 3)
There are recommendations that women taking enzyme-inducing mDs increase their OC dose from 20 to 35 pg estradiol to 50 pg particularly if break- through menstrual bleeding O C C U ~ S ~ ~ J ~ - ~ ~ OC failures may occasionally occur however at 50- to 80-pg es- tradiol doses and with no warning of irregular men- strual bleeding so women taking these doses of OCs with enzyme-inducing AEDs need counseling that they are not completely protected against pregnancy Most women who were previously reported with OC failures were taking 50- to 80-pg estradiol dose^^^^ Two of our four recent patients had OC failures de- spite taking OCs containing 50 pg estradiol (a fifth patient became pregnant while using levonorgestrol implant)
Physicians may use irregular or breakthrough menstrual bleeding as a clinical sign of low OC lev- els7J2 and the need to increase OC doses or add con- traceptives Enzyme-inducing AEDs produce break- through bleeding in 71 to 76 of women taking OCs whereas only 6 of those taking valproic acid had breakthrough bleeding7 Women taking 30 pg estra- diol had higher rates of bleeding than those taking 50 pg and when OC doses were increased from 50 to 75 pg estradiol breakthrough bleeding stopped in 10 of 12 women initially and in 8 of 12 chronically
This supports using ldquohigher doserdquo OCs with 50 pg estradiol for most women taking enzyme-inducing AEDs rather than the ldquolow doserdquo 20- to 35-pg estra- diol pills High-dose OCs with 80 pg estradiol are no longer available Women with breakthrough bleeding on 50 pg estradiol may supplement their dose by 25 pg estradiol using an extra half pill or use other contraceptive methods A small proportion of women do not have decreased OC levels with MDsZ0 and will be exposed to slightly increased steroid levels if OC doses are increased Those a t most risk for thromboembolic complications associated with high- dose OCs are smokers and women over 35 years
There are currently no routine clinical labora- tory measures to determine which women have suff- cient OC sex hormone levels to prevent conception
Despite the effects of AEDs on sex hormone levels OCs are still usually more effective than barrier con- traceptives The typical failure rate with barrier con- traceptives is 12 to 211deg Seven percent of women taking AEDs with OCs had accidental pregnancies in one small seriesll Women taking OCs who seek high levels of contraceptive protection can in addition to
increasing their OC dose add a spermicidal gel or foam or other barrier methods An effective alterna- tive hormonal therapy to OCs is the depo form of medroxyprogesterone (Depo Provera) a strong pro- gestin contraceptive that has not been associated with contraceptive failures due to AEDs~O Levonor- gestrol implant (ldquoNorplantrdquo) is not an effective alter- native for women with epilepsy Over 30 accidental pregnancies have occurred for women using levonorgestrol implant with AEDs31 this is probably due to increased sex hormone-binding globulin and decreased free norgestrol levels32 Certain women may also consider intrauterine devices instead of OCs for contraception
After our experience with accidental pregnancies in our patients we counsel women of child-bearing years with epilepsy about their contraceptive choices using guidelines based on previous recommenda- t i o n ~ ~ ~ rsquo rdquo ~ ~ and incorporating the new data about AEDs and contraceptives reviewed above (table 4) Women taking enzyme-inducing AEDs for other neu- rologic and psychiatric conditions will also benefit from contraceptive counseling
In addition to often not being aware of contracep- tive problems many physicians were not aware of the teratogenicity of AEDs Nearly one-half of neu- rologists (44) estimated the risk of birth defects in offspring of women treated for epilepsy as 0 to 3 This estimate is similar to the background rate of 2 for women not taking AEDs and underestimates the true risk of approximately 4 to 63 Obstetriciansrsquo estimates of the risk for malformations were more accurate than neurologists although 23 of them also underestimated the risk of birth defects
These results suggest that many neurologists and obstetricians do not have accurate knowledge to counsel women with epilepsy regarding their contra- ceptive and pregnancy choices Women with epilepsy might often benefit from discussing reproductive is- sues with both specialists because neurologists are generally more familiar with the effects of AEDs on OCs and obstetricians provide more accurate coun- seling about birth defect risks
References 1 Back DJ Orme ML Pharmacokinetic drug interactions with
oral contraceptives Clin Pharmacokinet 199018472-484 2 Crawford P Chadwick DJ Martin C Tjia J Back DJ Orme
M The interaction of phenytoin and carbamazepine with com- bined oral contraceptive steroids Br J Clin Pharmacol 1990
3 Yerby MS Treatment of epilepsy during pregnancy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993844-857
4 Waters CH Belai Y Gott PS Shen P De Giorgio CM Out- comes of pregnancy associated with antiepileptic drugs Arch Neurol 19945 1250 -253
5 Hauser WA HesdorfTer DC Pregnancy and teratogenesis In Epilepsy frequency causes and consequences New York Demos Publications 1990147-196
6 Beresford HR Legal issues roles of physicians in preventing fetal harm In Devinsky 0 Feldmann E Hainline B eds
30892-896
Neurological complications of pregnancy New York Raven Press 1994
7 Sonnen AE Sodium valproate and the contraceptive pill Br J Clin Prac Symp Suppl 19832731-36
8 Back DJ Evaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive drug interactions with anticonvulsants and antibiotics Br J Clin Pharmacol
9 Sparrow MF Pill method failures NZ Med J 1987100102- 103
10 Trussell J Kost K A guide to interpreting contraceptive effi- cacy studies Obstet Gynecol 199076558-567
11 Coulam CB Do anticonvulsants reduce the efficacy of oral contraceptives Epilepsia 197920519-525
12 Diamond MP Greene JW Thompson JM VanHooydonk JE Interactions of anticonvulsants and oral contraceptives in ep- ileptic adolescents Contraception 198531623-632
13 Mattson RH Cramer JA Darney PD Naftolin F Use of oral contraceptives by women with epilepsy JAMA 1986256238- 240
14 Cramer JA Mattson RH Hormones and epilepsy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993686-691
15 Editorial Drug interaction with oral contraceptive steroids
16 American Academy of Neurology Neurologists 1991-1992 Minneapolis AAN 1993
17 Roback G Randolph L Seldman B Pasko T Physician char- acteristics and distribution in the US Chicago AMA Depart- ment of Data Services 1994
18 Physiciansrsquo Desk Reference 48th ed Montvale Medical Eco- nomics Data Production Company 1994
19 Kerlinger F Foundations of behavioral research 2nd ed New York Holt Rinehart 1973414
20 Back DJ Breckenridge AM Crawford FE Orme ML Rowe PH Phenobarbitone interaction with oral contraceptive ste- roids in the rabbit and rat Br J Pharmacol 198069441-452
21 Levin W Welch RM Conney AH Effect of chronic phenobar- bital treatment on the liver microsomal metabolism and uterotropic action of 17s-estradiol Endocrinology 196780
22 Back DJ Bates M Bowden M Breckenridge AM Hall MJ The interaction of phenobarbital and other anticonvulsants with oral contraceptive steroid therapy Contraception 1980
23 Crawford P Chadwick D Cleland P e t al The lack of effect of sodium valproate on the pharmacokinetics of oral contracep- tive steroids Contraception 19853323-29
24 Eldon MA Underwood BA Randinitis EJ Posvar EL Sed- man AJ Lack of effect of gabapentin on the pharmacokinetics of a norethindrone acetateethinyl estradiol-containing oral contraceptive [abstract] Neurology 199343A307-A308
25 Jensen PK Saano V Haring P Svenstrup B Menge GP Possible interaction between oxcarbazepine and an oral con- traceptive Epilepsia 199233 1149 -1 152
26 Janz D Schmidt D Antiepileptic drugs and failure of oral contraceptives Lancet 197411113
27 Kenyon TW Unplanned pregnancy in an epileptic BMJ 1972
28 Krauss GL Brandt J Campbell M Plate C Summerfield M Anti-epileptic medicationioral contraceptive interactions a national survey of neurologists and obstetricians Neurology 1996461534-1539
29 Stadel BV Oral contraceptives and cardiovascular disease part 1 N Engl J Med 1981305612-618
30 Upjohn Laboratories Data on File 1995 31 Wyeth-Ayerst Laboratories Norplant System Data on file
1995 32 Haukkamaa M Contraception by Norplant subdermal cap-
sules is not reliable in epileptic patients on anticonvulsant treatment Contraception 198633559-565
33 Mattson RH Selection of antiepileptic drug therapy In Levy RH Mattson RH Meldrum BS eds Antiepileptic drugs 4th ed New York Raven Press 1995123-135
198825527-532
BMJ 198028193-94
135-140
22495-503
1686-687
June 1996 NEUROLOGY 46 1539
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Antiepileptic medication and oral contraceptive interactions
A national survey of neurologists and obstetricians GL Krauss MD J Brandt PhD M Campbell RN C Plate BS and M Summerfield
Article abstract-Hepatic enzyme-inducing antiepileptic drugs (AEDs) lower oral contraceptive (OC) sex hormone levels approximately 40 and increase the risk of unplanned pregnancies in women with epilepsy AEDs also increase the risk of birth defects in offspring of women with epilepsy We performed a national survey to determine obstetriciansrsquo and neurologistsrsquo knowledge of OC and AED interactions and the risk of birth defects for women with epilepsy taking AEDs We received responses to a mailed questionnaire from 160 of 1000 neurologists (16) and 147 of 1000 obstetricians (15) from 47 states Practice demographics and ages of responders were typical for US neurologists and obstetricians Ninety-one percent of neurologists and 75 of obstetricians said they treat women with epilepsy of child-bearing age Only 4 of the neurologists and none of the obstetricians however knew the effects of the six most common AEDs on OCs even though 27 of neurologists and 21 of obstetricians reported OC failures in their patients taking AEDs Although increasing OC doses can compensate for insufficient OC sex hormone levels due to AEDs most physicians do not increase the doses Even though the risk of birth defects for the offspring of women with epilepsy is 4 to 6 up from the background level of 296 44 of neurologists thought the risk was lower (0 to 3) and some of the respondents guessed that it was as high as 50 Many neurologists and obstetricians do not have accurate information to counsel women with epilepsy properly about their contraceptive and pregnancy choices NEUROLOGY 199646 1534-1539
Antiepilepsy drugs (AEDs) are associated with two major reproductive risks for women with epilepsy of child-bearing age (1) an increased risk of unplanned pregnancies due to hepatic enzyme-inducing AEDs lowering sex hormone levels of oral contraceptives (OCs)rsquo (2) an increased risk of birth defect^^^ We conducted a national survey of obstetricians and neurologists to determine whether they were aware that enzyme-inducing AEDs decrease the effective- ness of OCs and whether their patients taking AEDs had become accidentally pregnant while taking OCs We also determined whether physicians accurately counsel women about their increased risk of birth defects due to AEDs
During the past 2 years we saw five women at Johns Hopkins Hospital with hormonal contracep- tive failures while taking AEDs These unexpected pregnancies caused major social and emotional dis- tress one woman also had a brain tumor one had mental retardation and epilepsy surgery was can- celed for a third We became concerned that neurolo- gists and obstetricians may not be aware of this drug interaction and that women with epilepsy taking AEDs are not being warned of their risk for acciden- tal pregnancies This is especially important because women with epilepsy are at an approximately 4 to 6 risk of birth defects (2-3X background) in their
offspring3 with even greater risks for high-risk group^^^ Physicians have been held legally responsi- ble for a ldquowrongful liferdquo when a woman was not in- formed of specific pregnancy risks associated with her AEDslsquoj
Over 80 women have been reported in the United States and United Kingdom with accidental preg- nancies due to enzyme-inducing AEDs interfering with O C S ~ gt ~ - ~ The enzyme-inducing AEDs associated with OC failures are carbamazepine phenytoin phe- nobarbital primidone and ethosuximide All reduce OC estradiol levels approximately 40 and may also decrease free progestin levels by increasing sex hor- mone-binding globulins12 Enzyme-inducing AEDs increase the expected OC failure ratelo of 01 to 3 by severalfold In one small study 7 of epilepsy patients taking OCs with AEDs had OC fai1ureslrsquo The nonhepatic enzyme-inducing AEDs -valproic acid and gabapentin- do not decrease OC levels and have not been associated with accidental pregnan- cies
Physicians can compensate for the influence of en- zyme-inducing AEDs on OC sex hormone levels by increasing OC estradiol doses from 20 to 35 pg to 50 kg especially if there is irregular or breakthrough menstrual bleeding on low-dose OCs27rsquo2-15 Because most reported OC failures have been with 50- to
From the Departments nf Neurology IDr Krauss Ms Campbell Ms Plate and Mr Summerfield and Psychiatry (Dr Brandt) Johns Hopkins University Baltimore MD Received July 11 1995 Accepted in final form October 2 1995 Address correspondence and reprint requests to Dr Gregory L Krauss Johns Hopkins Hospital Meyer 2-147 600 N Wolfe Street Baltimore MD 21287-7247
1534 Copyright S 1996 by the American Academy of Neurology
Table 1 Physician respondents
Survey neurologists National neurologists Survey obstetricians National obstetricians (1994) (1991-1992) (1994) (1992-1993)
-
Total responders
Mean age (range) (yr)
Work settings ()
Solo
Group Community Hospital
Med school
Research other
Board-Certified ()
Year of MD
160 (16)
453 (30-75) 445
316 232
513 373
33 154
112 203
26 38
925 776
1943-1990
80-kg doses these steps will not prevent all OC fail- ures but are likely to significantly reduce their fre- quency
Physicians caring for women with epilepsy may not be aware of these issues I t is particularly impor- tant to determine whether women with epilepsy are receiving accurate information about contraception because they are at increased risk for pregnancy complications and birth defects in their ~ffspr ing~
Methods Suruey We mailed surveys to a sample of 1000 neurologists and 1000 obstetriciadgynecologists randomly selected from a geographically stratified Ameri- can Medical Association ( M A ) master list of 10034 li- censed neurologists and 33208 licensed obstetricians in the United States This is a comprehensive list of nearly all active specialists The random selection of physicians was performed by sequentially selecting physicians from the AMA database listed by zip codes This resulted in a sample that included all states but also represented the relative population of physicians in various regions We asked the physicians to respond to a brief anonymous knowledge questionnaire without consulting texts or other sources Twenty questions probed physiciansrsquo practice de- mographics familiarity with AED and OC interactions knowledge of interactions between specific AEDs and OCs and whether physicians adjusted OC doses for patients taking AEDs To assess physiciansrsquo general awareness of reproductive health issues in women with epilepsy we also asked them to estimate the risk of birth defects in preg- nancies of women with epilepsy and whether they counsel women with epilepsy against pregnancy
The following questions were asked (1) Are you currently treating any women of child-bearing age with epilepsy (2) In counseling a pregnant woman with good seizure control on a single anticonvulsant what would you tell her the risk is of her having a baby with a birth defect (3) Do you generally recommend that women taking a single anticonvulsant not become pregnant be- cause of this risk (4) How familiar are you with the inter- actions between oral contraceptives and antiepileptic med- ications (5-12) To the best of your knowledge do the following antiepileptic medications interfere with levels of oral contraceptives phenytoin (Dilantin) carbamazepine (Tegretol) valproic acid (Depakote) phenobarbital primi-
Survey questions
147 (147)
424 (28-74) 420
341
507
58
58
876
66
12
36 33
925 71 1943-1992
done (Mysoline) ethosuximide (Zarontin) gabapentin (Neurontin) felbamate (Felbatol) (13) Do you have your patients adjust their oral contraceptive dose if they are taking antiepileptic medication (14) If ldquoYesrdquo what adjust- ment (15) Have any of your patients on antiepileptic med- ication accidentally become pregnant while taking oral contraceptives
Demographic questions were (16) age (17) year of MD (18) board certification and (19) primary work setting a general comments section (20) was provided
Questionnaires returned within 6 months of the mailing were included Responses were coded and analyzed using the SPSS for Windows statistical program Data for categorical responses were tabulated and continuous data are summarized by means ranges and variance One post-hoc response to the questionnaire was added Some neurologists did not adjust OC doses if their patients were taking antiepileptic medications (ldquonordquo to question 131 but they did refer patients to obstetricians for OC adjustments (comment under 14) Therefore ldquoyesrdquo ldquonordquo and ldquoreferrdquo were possible responses for neurologists to question 13
We tested six specific hypotheses separately for neurol- ogists and obstetricians using nonparametric (chi-square) and parametric analysis (independent t test and bivariate correlation) We did not correct for multiple comparisons to avoid type I1 statistical error The hypotheses were that obstetricians and neurologists are more likely to adjust OC doses for patients taking AEDs if (1) they knew that en- zyme-inducing AEDs interfere with OC levels (2) they were familiar with interactions between AEDs and OCs but did not necessarily recognize specific drug interactions (3) they had previously had patients on AEDs become acci- dentally pregnant while taking OCs (4) physicians with recent medical training would be most knowledgeable about OC-AED interactions (5) physiciansrsquo estimates of the risks of birth defects would influence whether they recommend against pregnancy and (6) physiciansrsquo knowl- edgeable about OC-AED interactions would provide more accurate estimates of the risks of birth defects than would physicians who were not aware of OC-AED interactions We also compared obstetriciansrsquo and neurologistsrsquo familiar- ity with and knowledge of OC-AED interactions and their estimates of the risk of malformations in offspring of women with epilepsy taking AEDs
Statisticat analysis
June 1996 NEUROLOGY 46 1535
Figure 1 Physiciansrsquo knowledge of OC interactions with six common AEDs (new AEDs excluded) AEDs carbamaz- epine phenytoin valproic acid phenobarbital primidone ethosuximide
Physicians were asked which of eight AEDs interfered with OCs Their knowledge of which AEDs interfere with OCs was estimated however using only six of eight AEDs (phenytoin carbamazepine valproic acid phenobarbital primidone and ethosuximide ) Gabapentin and felbamate were not included because they had been recently released at the time of the survey and were not recognized by many neurologists and most obstetricians Correct responses were tha t phenytoin carbamazepine phenobarbital primidone and ethosuximide interfere with OCs whereas valproic acid does notlsquo27-9
Results Characteristics of survey respondents A total of 160 neurologists (16) and 147 obstetricians (147) responded to the questionnaire (table 1) The ages work setting and geographic distribution for responders were representative of neurologists and obstetricians national- l ~ rsquo ~ rdquo The responders were from 47 states The largest numbers were in office-based practices with medical school graduation in the 1960s through 1980s
Most neurologists (91) and obstetricians (7596) said they treat women with epilepsy of child-bearing age Most neurolo- gists (75) and most obstetricians (59) believed they were moderately or very familiar with the interactions be- tween AEDs and OCs Physiciansrsquo actual knowledge of OC- AED interactions however was extremely poor When physicians were scored on their knowledge of whether six common AEDs interfered with OCs (phenytoin carbamaz- epine valproic acid phenobarbital primidone and etho- suximide) only 4 of the neurologists and none of the obstetricians were correct for all six AEDs (figure 1) The two new AEDs gabapentin and felbamate were excluded because they were not recognized by most physicians The average score for neurologistsrsquo knowledge of OC interac- tions with the six AEDs was 61 5 22 and for obstetri- cians was 378 f 19 Neurologists were both more famil- iar with ( t = 350 d f 297 p lt 0001) and more knowledgeable about ( t = 782 d f 292 p lt 0001) AED-OC interactions than obstetricians
Most neurologists (77 to 84) knew that phenytoin car- bamazepine and phenobarbital interfered with OCs but only 38 knew that valproic acid does not interfere with
Specialistsrsquo knowledge of OC-AED interactions
1536 NEUROLOGY 46 June 1996
Figure 2 Estimate of birth defect risk associated with AEDs
OCs Most obstetricians also knew that phenytoin inter- fered with OCs (77) but fewer knew that phenobarbital (54) carbamazepine (44) and primidone (17) lowered OC levels and only 29 know that valproic acid did not interfere with OCs Few neurologists and obstetricians knew whether ethosuximide or the two new AEDs gaba- pentin and felbamate interfere with OCs
Younger physicians were slightly more knowledgeable than older physicians about common AED-OC interactions although this was significant only for obstetricians (neurol- ogists r = 014 p = 009 obstetricians r = 030 p lt 0001)
Fewer than half of neurologists (41) and obstetricians (43) have patients adjust their OC doses if they are taking AEDs Moreover a number of physicians noted that they ldquoadjusted OC doses by lowering estrogen doses or using relatively low-dose 35-kg estrogen pills An additional 8 of neurologists refer their patients to obstetricians to have OC doses adjusted
There was a strong association between neurologistsrsquo and obstetriciansrsquo knowledge of which AEDs interfere with OCs and whether they adjust OC doses to compensate for AED effects (neurologists t = 277 d f 143 p = 0006 obstetricians t = 421 df 128 p lt 0001) Even physicians who were ldquofamiliarrdquo with this drug interaction but did not have accurate knowledge of which AEDs were involved usually adjusted their patientsrsquo OC doses for patients on AEDs 89 of neurologists and 76 of obstetricians famil- iar with OC-AED interactions adjust OC dosages for pa- tients on AEDs whereas only 19 of neurologists and 24 of obstetricians not familiar with OC-AED interactions ad- just OC dosages (neurologists chi-square 1043 p = 0001 obstetricians chi-square 1464 p = 00001)
Twenty-seven percent of neurologists and 21 of obste- tricians reported OC failure in their patients taking AEDs Neurologists whose patients had accidental pregnancies on OCs and AEDs were more likely to adjust OC doses (58 versus 35) than neurologists whose patients had not had such pregnancies (chi-square 633 p = 0011) Obstetri- cians whose patients had accidental pregnancies on OC and AEDs were more likely to adjust OCs than obstetri- cians who had not had patients with accidental pregnan- cies (57 versus 39) although this did not reach signifi- cance (chi-square 296 p = 0086)
Pregnancy risks and counseling Women with epilepsy have significant risks of approximately 4 to 6 for congen-
Factors influencing OC dosing
Table 2 Effects of AEDs on OC hormone levels
Enzyme-inducing AEDs
Phenobarbital
Phenytoin
Carbamazepine
Oxacarbamazepine Nonenzyme-inducing AEDs
Valproic acid
Gabapentin
-381
-490 -422
-470
110
60
Estradiol () -
~
Changes in 24-hour serum levels from baseline or control values No significant change References 1 2 7 20 23-25
ital malformations in their offspring compared with a background risk of approximately 23 This 2-3X in- creased risk is increased further for women with uncon- trolled seizures taking multiple AEDs5 or who belong to high-risk socioeconomic group^^ Despite this there was a wide variation in physiciansrsquo estimates of the risk of mal- formations with many physicians particularly neurolo- gists underestimating the risk (figure 2) When counseling a pregnant woman with good seizure control on a single antiepileptic medication obstetricians said they would es- timate a mean risk for birth defects of 689 (range 0 to 50) Most obstetricians (95) estimated a birth defect risk due to a single AED between 1 and 10 Over one- fifth (23) of obstetricians underestimated the risk as 0 to 3 In counseling a woman with epilepsy neurologists estimated a lower mean risk for birth defects than did obstetricians 475 (range 0 to 50) (neurologistsrsquo versus obstetriciansrsquo estimates t = 351 df 286 p = 001) Most neurologists (95) estimated a risk of birth defects be- tween 0 and 9 A large proportion of neurologists (44) underestimated the risk of birth defects as 0 to 3
Only 3 of neurologists and 5 of obstetricians recom- mend that their patients taking AEDs not become preg- nant Physiciansrsquo estimates of the risk of birth defects as- sociated with a single AED did not influence whether they would recommend that women taking single anticonvul- sants should avoid pregnancy (neurologists t = 139 df 147 p = 0165 obstetricians t = 078 df 132 p = 044) There was also no correlation between physiciansrsquo esti- mates of the risk of birth defects and their knowledge of OC-AED interactions (neurologists r = 005 p = 056 obstetricians r = 0 0 1 ~ = 081)
Table 3 Reported OC failures with AEDs
AED Accidental pregnancies
Phenobarbital
Phenytoin
Carbamazepine
Valproic acid
Ethosuximide
51
42
19
6 (0 monotherapy)
4
References 1 7 11 28
Norgestrel or norethindrone ()
- 187
-420
-397
-360
oo 30rsquo
Discussion Over one-fifth of neurologists and ob- stetricians reported accidental pregnancies in their patients taking AEDs with OCs Most physicians however did not know which common AEDs inter- fere with OCs do not adjust OC doses to overcome the effects of enzyme-inducing AEDs on sex hormone levels and did not know that valproic acid and gaba- pentin are nonenzyme-inducing alternatives to en- zyme-inducing AEDs Although physicians who were at least moderately familiar with OC-AED interac- tions tended to adjust OC doses for their patients it is unclear how they would do this without recogniz- ing specific AED-OC interactions These results oc- cur despite warnings of AED-OC interactions in pharmaceutical product inserts the Physiciansrsquo Desk Reference18 and in several medical reviews and edi- t o r i a l ~ ~ ~ ~ J ~ - ~ ~ Our survey suggests that a large num- ber of women in the United States with epilepsy are at risk for unplanned pregnancies while taking OCs
There are several limitations in our survey A re- sponse bias to the questionnaire is possible It is typical however for only a few mailed question- naires to be returned19 The geographic distribution practice types and ages of respondents were typical for American neurologists and obstetricians (see ta- ble l)16J7 Nonetheless the survey may have overes- timated physiciansrsquo lack of knowledge about AED complications for women with epilepsy particularly if nonrespondents were physicians who already knew about the reproductive risks of AEDs More likely however is that those who believed these issues are important would respond rather than those who do not recognize the reproductive complications associ- ated with AEDs This suggests in fact that any skew in the study would be toward overestimating physiciansrsquo knowledge of these issues Evidence that less-knowledgeable physicians were not over- represented in the survey is that a larger proportion of responders were board-certified specialists than the national average (see table 1) Another limitation is that several questions could not be asked directly without cuing other responses We could not ask for example questions to determine precisely how phy-
June 1996 NEUROLOGY 46 1537
Table 4 Suggestions for combining OCs and AEDs for women with epilepsy
1 Discuss contraceptive choices and the effects of enzyme- inducing AEDs (carbamazepine phenytoin phenobarbital primidone and ethosuximide) on OCs with all women of child-bearing years who have epilepsy This can be part of a general discussion of the risks of pregnancy and epilepsy
When treating women with epilepsy taking OCs continue to select AEDs according to recommended indications for epilepsy33
AED (valproic acid gabapentin vigabatrin) for women taking OCs
equivalent) for women taking enzyme-inducing AEDs who desire effective contraception Obstetricians and family physicians usually prescribe the OCs Counsel women that increased OC doses do not always protect from contraceptive failures due to AEDs but that OC failure rates are usually lower than with barrier methods alone
irregular menstrual bleeding while taking OCs Increase OC doses or switch contraceptives if irregular bleeding occurs
2
3 If AEDs are otherwise equivalent use a nonenzyme-inducing
4 Recommend OC doses of 50 pg estradiol (or mestranol
5 Have women with epilepsy monitor for breakthrough or
6 Advise women seeking very high levels of contraception protection that they may add spermicide or barrier contraception to their OCs
7 Alternative contraceptives that can be used for some women are medroxyprogesterone (Depo-Provera) and intrauterine devices Many pregnancies have occurred with levonorgestrol implant (ldquoNorplantrdquo) and enzyme-inducing AEDs
8 Oxcarbazepine lowers OC hormone levels whereas gabapentin and vigabatrin are nonenzyme-inducers that are unlikely to interfere with OCs The effects of lamotrigine and felbamate on OCs are unclear
Modified from references 7 13 15
sicians adjust OC doses whether physicians monitor patients for irregular menstrual bleeding as a sign of AED effects on OCs and how many total patients had accidental pregnancies due to AEDs
Enzyme-inducing AEDs including carbamaz- epine phenytoin phenobarbital primidone and ethosuximide decrease the effectiveness of OCs by lowering synthetic sex hormone levels Enzyme- inducing AEDs increase cytochrome P450 en- zymes12021 resulting in increased metabolism of syn- thetic estrogens (ethinyl estradiol and mestranol) and lowered serum levels of approximately 40 (ta- ble 2) 1 2 T Z2~25 Free progestin levels are also de- creased probably due to increased synthesis of sex hormone-binding globulins220 Valproic and two new AEDs- gabapentin and vigabatrin- do not induce hepatic P450 metabolism and are unlikely to interfere with OCs Gabapentin does not decrease estradiol levels24 and vigabatrin has not been stud- ied Oxcarbazepine lowers OC sex hormone levels2rdquo and is likely to interfere with OCs Effects of lam- otrigine and felbamate on OCs have not been stud- 1538 NEUROLOGY 46 June 1996
ied Lamotrigine is metabolized by hepatic glucu- ronidation however rather than by the microsomal P450 system and possibly may not stimulate sex hor- mone metabolism
Over 150 accidental pregnancies have been re- ported in patients taking enzyme-inducing AEDs primarily women from the United K i n g d ~ m ~ ~ ~ and including the minimum of 75 American patients reported in this survey17~s1126-28 Valproic acid a nonenzyme-inducing AED has not been associated with accidental pregnancies when used in mono- therapy (table 3)
There are recommendations that women taking enzyme-inducing mDs increase their OC dose from 20 to 35 pg estradiol to 50 pg particularly if break- through menstrual bleeding O C C U ~ S ~ ~ J ~ - ~ ~ OC failures may occasionally occur however at 50- to 80-pg es- tradiol doses and with no warning of irregular men- strual bleeding so women taking these doses of OCs with enzyme-inducing AEDs need counseling that they are not completely protected against pregnancy Most women who were previously reported with OC failures were taking 50- to 80-pg estradiol dose^^^^ Two of our four recent patients had OC failures de- spite taking OCs containing 50 pg estradiol (a fifth patient became pregnant while using levonorgestrol implant)
Physicians may use irregular or breakthrough menstrual bleeding as a clinical sign of low OC lev- els7J2 and the need to increase OC doses or add con- traceptives Enzyme-inducing AEDs produce break- through bleeding in 71 to 76 of women taking OCs whereas only 6 of those taking valproic acid had breakthrough bleeding7 Women taking 30 pg estra- diol had higher rates of bleeding than those taking 50 pg and when OC doses were increased from 50 to 75 pg estradiol breakthrough bleeding stopped in 10 of 12 women initially and in 8 of 12 chronically
This supports using ldquohigher doserdquo OCs with 50 pg estradiol for most women taking enzyme-inducing AEDs rather than the ldquolow doserdquo 20- to 35-pg estra- diol pills High-dose OCs with 80 pg estradiol are no longer available Women with breakthrough bleeding on 50 pg estradiol may supplement their dose by 25 pg estradiol using an extra half pill or use other contraceptive methods A small proportion of women do not have decreased OC levels with MDsZ0 and will be exposed to slightly increased steroid levels if OC doses are increased Those a t most risk for thromboembolic complications associated with high- dose OCs are smokers and women over 35 years
There are currently no routine clinical labora- tory measures to determine which women have suff- cient OC sex hormone levels to prevent conception
Despite the effects of AEDs on sex hormone levels OCs are still usually more effective than barrier con- traceptives The typical failure rate with barrier con- traceptives is 12 to 211deg Seven percent of women taking AEDs with OCs had accidental pregnancies in one small seriesll Women taking OCs who seek high levels of contraceptive protection can in addition to
increasing their OC dose add a spermicidal gel or foam or other barrier methods An effective alterna- tive hormonal therapy to OCs is the depo form of medroxyprogesterone (Depo Provera) a strong pro- gestin contraceptive that has not been associated with contraceptive failures due to AEDs~O Levonor- gestrol implant (ldquoNorplantrdquo) is not an effective alter- native for women with epilepsy Over 30 accidental pregnancies have occurred for women using levonorgestrol implant with AEDs31 this is probably due to increased sex hormone-binding globulin and decreased free norgestrol levels32 Certain women may also consider intrauterine devices instead of OCs for contraception
After our experience with accidental pregnancies in our patients we counsel women of child-bearing years with epilepsy about their contraceptive choices using guidelines based on previous recommenda- t i o n ~ ~ ~ rsquo rdquo ~ ~ and incorporating the new data about AEDs and contraceptives reviewed above (table 4) Women taking enzyme-inducing AEDs for other neu- rologic and psychiatric conditions will also benefit from contraceptive counseling
In addition to often not being aware of contracep- tive problems many physicians were not aware of the teratogenicity of AEDs Nearly one-half of neu- rologists (44) estimated the risk of birth defects in offspring of women treated for epilepsy as 0 to 3 This estimate is similar to the background rate of 2 for women not taking AEDs and underestimates the true risk of approximately 4 to 63 Obstetriciansrsquo estimates of the risk for malformations were more accurate than neurologists although 23 of them also underestimated the risk of birth defects
These results suggest that many neurologists and obstetricians do not have accurate knowledge to counsel women with epilepsy regarding their contra- ceptive and pregnancy choices Women with epilepsy might often benefit from discussing reproductive is- sues with both specialists because neurologists are generally more familiar with the effects of AEDs on OCs and obstetricians provide more accurate coun- seling about birth defect risks
References 1 Back DJ Orme ML Pharmacokinetic drug interactions with
oral contraceptives Clin Pharmacokinet 199018472-484 2 Crawford P Chadwick DJ Martin C Tjia J Back DJ Orme
M The interaction of phenytoin and carbamazepine with com- bined oral contraceptive steroids Br J Clin Pharmacol 1990
3 Yerby MS Treatment of epilepsy during pregnancy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993844-857
4 Waters CH Belai Y Gott PS Shen P De Giorgio CM Out- comes of pregnancy associated with antiepileptic drugs Arch Neurol 19945 1250 -253
5 Hauser WA HesdorfTer DC Pregnancy and teratogenesis In Epilepsy frequency causes and consequences New York Demos Publications 1990147-196
6 Beresford HR Legal issues roles of physicians in preventing fetal harm In Devinsky 0 Feldmann E Hainline B eds
30892-896
Neurological complications of pregnancy New York Raven Press 1994
7 Sonnen AE Sodium valproate and the contraceptive pill Br J Clin Prac Symp Suppl 19832731-36
8 Back DJ Evaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive drug interactions with anticonvulsants and antibiotics Br J Clin Pharmacol
9 Sparrow MF Pill method failures NZ Med J 1987100102- 103
10 Trussell J Kost K A guide to interpreting contraceptive effi- cacy studies Obstet Gynecol 199076558-567
11 Coulam CB Do anticonvulsants reduce the efficacy of oral contraceptives Epilepsia 197920519-525
12 Diamond MP Greene JW Thompson JM VanHooydonk JE Interactions of anticonvulsants and oral contraceptives in ep- ileptic adolescents Contraception 198531623-632
13 Mattson RH Cramer JA Darney PD Naftolin F Use of oral contraceptives by women with epilepsy JAMA 1986256238- 240
14 Cramer JA Mattson RH Hormones and epilepsy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993686-691
15 Editorial Drug interaction with oral contraceptive steroids
16 American Academy of Neurology Neurologists 1991-1992 Minneapolis AAN 1993
17 Roback G Randolph L Seldman B Pasko T Physician char- acteristics and distribution in the US Chicago AMA Depart- ment of Data Services 1994
18 Physiciansrsquo Desk Reference 48th ed Montvale Medical Eco- nomics Data Production Company 1994
19 Kerlinger F Foundations of behavioral research 2nd ed New York Holt Rinehart 1973414
20 Back DJ Breckenridge AM Crawford FE Orme ML Rowe PH Phenobarbitone interaction with oral contraceptive ste- roids in the rabbit and rat Br J Pharmacol 198069441-452
21 Levin W Welch RM Conney AH Effect of chronic phenobar- bital treatment on the liver microsomal metabolism and uterotropic action of 17s-estradiol Endocrinology 196780
22 Back DJ Bates M Bowden M Breckenridge AM Hall MJ The interaction of phenobarbital and other anticonvulsants with oral contraceptive steroid therapy Contraception 1980
23 Crawford P Chadwick D Cleland P e t al The lack of effect of sodium valproate on the pharmacokinetics of oral contracep- tive steroids Contraception 19853323-29
24 Eldon MA Underwood BA Randinitis EJ Posvar EL Sed- man AJ Lack of effect of gabapentin on the pharmacokinetics of a norethindrone acetateethinyl estradiol-containing oral contraceptive [abstract] Neurology 199343A307-A308
25 Jensen PK Saano V Haring P Svenstrup B Menge GP Possible interaction between oxcarbazepine and an oral con- traceptive Epilepsia 199233 1149 -1 152
26 Janz D Schmidt D Antiepileptic drugs and failure of oral contraceptives Lancet 197411113
27 Kenyon TW Unplanned pregnancy in an epileptic BMJ 1972
28 Krauss GL Brandt J Campbell M Plate C Summerfield M Anti-epileptic medicationioral contraceptive interactions a national survey of neurologists and obstetricians Neurology 1996461534-1539
29 Stadel BV Oral contraceptives and cardiovascular disease part 1 N Engl J Med 1981305612-618
30 Upjohn Laboratories Data on File 1995 31 Wyeth-Ayerst Laboratories Norplant System Data on file
1995 32 Haukkamaa M Contraception by Norplant subdermal cap-
sules is not reliable in epileptic patients on anticonvulsant treatment Contraception 198633559-565
33 Mattson RH Selection of antiepileptic drug therapy In Levy RH Mattson RH Meldrum BS eds Antiepileptic drugs 4th ed New York Raven Press 1995123-135
198825527-532
BMJ 198028193-94
135-140
22495-503
1686-687
June 1996 NEUROLOGY 46 1539
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Table 1 Physician respondents
Survey neurologists National neurologists Survey obstetricians National obstetricians (1994) (1991-1992) (1994) (1992-1993)
-
Total responders
Mean age (range) (yr)
Work settings ()
Solo
Group Community Hospital
Med school
Research other
Board-Certified ()
Year of MD
160 (16)
453 (30-75) 445
316 232
513 373
33 154
112 203
26 38
925 776
1943-1990
80-kg doses these steps will not prevent all OC fail- ures but are likely to significantly reduce their fre- quency
Physicians caring for women with epilepsy may not be aware of these issues I t is particularly impor- tant to determine whether women with epilepsy are receiving accurate information about contraception because they are at increased risk for pregnancy complications and birth defects in their ~ffspr ing~
Methods Suruey We mailed surveys to a sample of 1000 neurologists and 1000 obstetriciadgynecologists randomly selected from a geographically stratified Ameri- can Medical Association ( M A ) master list of 10034 li- censed neurologists and 33208 licensed obstetricians in the United States This is a comprehensive list of nearly all active specialists The random selection of physicians was performed by sequentially selecting physicians from the AMA database listed by zip codes This resulted in a sample that included all states but also represented the relative population of physicians in various regions We asked the physicians to respond to a brief anonymous knowledge questionnaire without consulting texts or other sources Twenty questions probed physiciansrsquo practice de- mographics familiarity with AED and OC interactions knowledge of interactions between specific AEDs and OCs and whether physicians adjusted OC doses for patients taking AEDs To assess physiciansrsquo general awareness of reproductive health issues in women with epilepsy we also asked them to estimate the risk of birth defects in preg- nancies of women with epilepsy and whether they counsel women with epilepsy against pregnancy
The following questions were asked (1) Are you currently treating any women of child-bearing age with epilepsy (2) In counseling a pregnant woman with good seizure control on a single anticonvulsant what would you tell her the risk is of her having a baby with a birth defect (3) Do you generally recommend that women taking a single anticonvulsant not become pregnant be- cause of this risk (4) How familiar are you with the inter- actions between oral contraceptives and antiepileptic med- ications (5-12) To the best of your knowledge do the following antiepileptic medications interfere with levels of oral contraceptives phenytoin (Dilantin) carbamazepine (Tegretol) valproic acid (Depakote) phenobarbital primi-
Survey questions
147 (147)
424 (28-74) 420
341
507
58
58
876
66
12
36 33
925 71 1943-1992
done (Mysoline) ethosuximide (Zarontin) gabapentin (Neurontin) felbamate (Felbatol) (13) Do you have your patients adjust their oral contraceptive dose if they are taking antiepileptic medication (14) If ldquoYesrdquo what adjust- ment (15) Have any of your patients on antiepileptic med- ication accidentally become pregnant while taking oral contraceptives
Demographic questions were (16) age (17) year of MD (18) board certification and (19) primary work setting a general comments section (20) was provided
Questionnaires returned within 6 months of the mailing were included Responses were coded and analyzed using the SPSS for Windows statistical program Data for categorical responses were tabulated and continuous data are summarized by means ranges and variance One post-hoc response to the questionnaire was added Some neurologists did not adjust OC doses if their patients were taking antiepileptic medications (ldquonordquo to question 131 but they did refer patients to obstetricians for OC adjustments (comment under 14) Therefore ldquoyesrdquo ldquonordquo and ldquoreferrdquo were possible responses for neurologists to question 13
We tested six specific hypotheses separately for neurol- ogists and obstetricians using nonparametric (chi-square) and parametric analysis (independent t test and bivariate correlation) We did not correct for multiple comparisons to avoid type I1 statistical error The hypotheses were that obstetricians and neurologists are more likely to adjust OC doses for patients taking AEDs if (1) they knew that en- zyme-inducing AEDs interfere with OC levels (2) they were familiar with interactions between AEDs and OCs but did not necessarily recognize specific drug interactions (3) they had previously had patients on AEDs become acci- dentally pregnant while taking OCs (4) physicians with recent medical training would be most knowledgeable about OC-AED interactions (5) physiciansrsquo estimates of the risks of birth defects would influence whether they recommend against pregnancy and (6) physiciansrsquo knowl- edgeable about OC-AED interactions would provide more accurate estimates of the risks of birth defects than would physicians who were not aware of OC-AED interactions We also compared obstetriciansrsquo and neurologistsrsquo familiar- ity with and knowledge of OC-AED interactions and their estimates of the risk of malformations in offspring of women with epilepsy taking AEDs
Statisticat analysis
June 1996 NEUROLOGY 46 1535
Figure 1 Physiciansrsquo knowledge of OC interactions with six common AEDs (new AEDs excluded) AEDs carbamaz- epine phenytoin valproic acid phenobarbital primidone ethosuximide
Physicians were asked which of eight AEDs interfered with OCs Their knowledge of which AEDs interfere with OCs was estimated however using only six of eight AEDs (phenytoin carbamazepine valproic acid phenobarbital primidone and ethosuximide ) Gabapentin and felbamate were not included because they had been recently released at the time of the survey and were not recognized by many neurologists and most obstetricians Correct responses were tha t phenytoin carbamazepine phenobarbital primidone and ethosuximide interfere with OCs whereas valproic acid does notlsquo27-9
Results Characteristics of survey respondents A total of 160 neurologists (16) and 147 obstetricians (147) responded to the questionnaire (table 1) The ages work setting and geographic distribution for responders were representative of neurologists and obstetricians national- l ~ rsquo ~ rdquo The responders were from 47 states The largest numbers were in office-based practices with medical school graduation in the 1960s through 1980s
Most neurologists (91) and obstetricians (7596) said they treat women with epilepsy of child-bearing age Most neurolo- gists (75) and most obstetricians (59) believed they were moderately or very familiar with the interactions be- tween AEDs and OCs Physiciansrsquo actual knowledge of OC- AED interactions however was extremely poor When physicians were scored on their knowledge of whether six common AEDs interfered with OCs (phenytoin carbamaz- epine valproic acid phenobarbital primidone and etho- suximide) only 4 of the neurologists and none of the obstetricians were correct for all six AEDs (figure 1) The two new AEDs gabapentin and felbamate were excluded because they were not recognized by most physicians The average score for neurologistsrsquo knowledge of OC interac- tions with the six AEDs was 61 5 22 and for obstetri- cians was 378 f 19 Neurologists were both more famil- iar with ( t = 350 d f 297 p lt 0001) and more knowledgeable about ( t = 782 d f 292 p lt 0001) AED-OC interactions than obstetricians
Most neurologists (77 to 84) knew that phenytoin car- bamazepine and phenobarbital interfered with OCs but only 38 knew that valproic acid does not interfere with
Specialistsrsquo knowledge of OC-AED interactions
1536 NEUROLOGY 46 June 1996
Figure 2 Estimate of birth defect risk associated with AEDs
OCs Most obstetricians also knew that phenytoin inter- fered with OCs (77) but fewer knew that phenobarbital (54) carbamazepine (44) and primidone (17) lowered OC levels and only 29 know that valproic acid did not interfere with OCs Few neurologists and obstetricians knew whether ethosuximide or the two new AEDs gaba- pentin and felbamate interfere with OCs
Younger physicians were slightly more knowledgeable than older physicians about common AED-OC interactions although this was significant only for obstetricians (neurol- ogists r = 014 p = 009 obstetricians r = 030 p lt 0001)
Fewer than half of neurologists (41) and obstetricians (43) have patients adjust their OC doses if they are taking AEDs Moreover a number of physicians noted that they ldquoadjusted OC doses by lowering estrogen doses or using relatively low-dose 35-kg estrogen pills An additional 8 of neurologists refer their patients to obstetricians to have OC doses adjusted
There was a strong association between neurologistsrsquo and obstetriciansrsquo knowledge of which AEDs interfere with OCs and whether they adjust OC doses to compensate for AED effects (neurologists t = 277 d f 143 p = 0006 obstetricians t = 421 df 128 p lt 0001) Even physicians who were ldquofamiliarrdquo with this drug interaction but did not have accurate knowledge of which AEDs were involved usually adjusted their patientsrsquo OC doses for patients on AEDs 89 of neurologists and 76 of obstetricians famil- iar with OC-AED interactions adjust OC dosages for pa- tients on AEDs whereas only 19 of neurologists and 24 of obstetricians not familiar with OC-AED interactions ad- just OC dosages (neurologists chi-square 1043 p = 0001 obstetricians chi-square 1464 p = 00001)
Twenty-seven percent of neurologists and 21 of obste- tricians reported OC failure in their patients taking AEDs Neurologists whose patients had accidental pregnancies on OCs and AEDs were more likely to adjust OC doses (58 versus 35) than neurologists whose patients had not had such pregnancies (chi-square 633 p = 0011) Obstetri- cians whose patients had accidental pregnancies on OC and AEDs were more likely to adjust OCs than obstetri- cians who had not had patients with accidental pregnan- cies (57 versus 39) although this did not reach signifi- cance (chi-square 296 p = 0086)
Pregnancy risks and counseling Women with epilepsy have significant risks of approximately 4 to 6 for congen-
Factors influencing OC dosing
Table 2 Effects of AEDs on OC hormone levels
Enzyme-inducing AEDs
Phenobarbital
Phenytoin
Carbamazepine
Oxacarbamazepine Nonenzyme-inducing AEDs
Valproic acid
Gabapentin
-381
-490 -422
-470
110
60
Estradiol () -
~
Changes in 24-hour serum levels from baseline or control values No significant change References 1 2 7 20 23-25
ital malformations in their offspring compared with a background risk of approximately 23 This 2-3X in- creased risk is increased further for women with uncon- trolled seizures taking multiple AEDs5 or who belong to high-risk socioeconomic group^^ Despite this there was a wide variation in physiciansrsquo estimates of the risk of mal- formations with many physicians particularly neurolo- gists underestimating the risk (figure 2) When counseling a pregnant woman with good seizure control on a single antiepileptic medication obstetricians said they would es- timate a mean risk for birth defects of 689 (range 0 to 50) Most obstetricians (95) estimated a birth defect risk due to a single AED between 1 and 10 Over one- fifth (23) of obstetricians underestimated the risk as 0 to 3 In counseling a woman with epilepsy neurologists estimated a lower mean risk for birth defects than did obstetricians 475 (range 0 to 50) (neurologistsrsquo versus obstetriciansrsquo estimates t = 351 df 286 p = 001) Most neurologists (95) estimated a risk of birth defects be- tween 0 and 9 A large proportion of neurologists (44) underestimated the risk of birth defects as 0 to 3
Only 3 of neurologists and 5 of obstetricians recom- mend that their patients taking AEDs not become preg- nant Physiciansrsquo estimates of the risk of birth defects as- sociated with a single AED did not influence whether they would recommend that women taking single anticonvul- sants should avoid pregnancy (neurologists t = 139 df 147 p = 0165 obstetricians t = 078 df 132 p = 044) There was also no correlation between physiciansrsquo esti- mates of the risk of birth defects and their knowledge of OC-AED interactions (neurologists r = 005 p = 056 obstetricians r = 0 0 1 ~ = 081)
Table 3 Reported OC failures with AEDs
AED Accidental pregnancies
Phenobarbital
Phenytoin
Carbamazepine
Valproic acid
Ethosuximide
51
42
19
6 (0 monotherapy)
4
References 1 7 11 28
Norgestrel or norethindrone ()
- 187
-420
-397
-360
oo 30rsquo
Discussion Over one-fifth of neurologists and ob- stetricians reported accidental pregnancies in their patients taking AEDs with OCs Most physicians however did not know which common AEDs inter- fere with OCs do not adjust OC doses to overcome the effects of enzyme-inducing AEDs on sex hormone levels and did not know that valproic acid and gaba- pentin are nonenzyme-inducing alternatives to en- zyme-inducing AEDs Although physicians who were at least moderately familiar with OC-AED interac- tions tended to adjust OC doses for their patients it is unclear how they would do this without recogniz- ing specific AED-OC interactions These results oc- cur despite warnings of AED-OC interactions in pharmaceutical product inserts the Physiciansrsquo Desk Reference18 and in several medical reviews and edi- t o r i a l ~ ~ ~ ~ J ~ - ~ ~ Our survey suggests that a large num- ber of women in the United States with epilepsy are at risk for unplanned pregnancies while taking OCs
There are several limitations in our survey A re- sponse bias to the questionnaire is possible It is typical however for only a few mailed question- naires to be returned19 The geographic distribution practice types and ages of respondents were typical for American neurologists and obstetricians (see ta- ble l)16J7 Nonetheless the survey may have overes- timated physiciansrsquo lack of knowledge about AED complications for women with epilepsy particularly if nonrespondents were physicians who already knew about the reproductive risks of AEDs More likely however is that those who believed these issues are important would respond rather than those who do not recognize the reproductive complications associ- ated with AEDs This suggests in fact that any skew in the study would be toward overestimating physiciansrsquo knowledge of these issues Evidence that less-knowledgeable physicians were not over- represented in the survey is that a larger proportion of responders were board-certified specialists than the national average (see table 1) Another limitation is that several questions could not be asked directly without cuing other responses We could not ask for example questions to determine precisely how phy-
June 1996 NEUROLOGY 46 1537
Table 4 Suggestions for combining OCs and AEDs for women with epilepsy
1 Discuss contraceptive choices and the effects of enzyme- inducing AEDs (carbamazepine phenytoin phenobarbital primidone and ethosuximide) on OCs with all women of child-bearing years who have epilepsy This can be part of a general discussion of the risks of pregnancy and epilepsy
When treating women with epilepsy taking OCs continue to select AEDs according to recommended indications for epilepsy33
AED (valproic acid gabapentin vigabatrin) for women taking OCs
equivalent) for women taking enzyme-inducing AEDs who desire effective contraception Obstetricians and family physicians usually prescribe the OCs Counsel women that increased OC doses do not always protect from contraceptive failures due to AEDs but that OC failure rates are usually lower than with barrier methods alone
irregular menstrual bleeding while taking OCs Increase OC doses or switch contraceptives if irregular bleeding occurs
2
3 If AEDs are otherwise equivalent use a nonenzyme-inducing
4 Recommend OC doses of 50 pg estradiol (or mestranol
5 Have women with epilepsy monitor for breakthrough or
6 Advise women seeking very high levels of contraception protection that they may add spermicide or barrier contraception to their OCs
7 Alternative contraceptives that can be used for some women are medroxyprogesterone (Depo-Provera) and intrauterine devices Many pregnancies have occurred with levonorgestrol implant (ldquoNorplantrdquo) and enzyme-inducing AEDs
8 Oxcarbazepine lowers OC hormone levels whereas gabapentin and vigabatrin are nonenzyme-inducers that are unlikely to interfere with OCs The effects of lamotrigine and felbamate on OCs are unclear
Modified from references 7 13 15
sicians adjust OC doses whether physicians monitor patients for irregular menstrual bleeding as a sign of AED effects on OCs and how many total patients had accidental pregnancies due to AEDs
Enzyme-inducing AEDs including carbamaz- epine phenytoin phenobarbital primidone and ethosuximide decrease the effectiveness of OCs by lowering synthetic sex hormone levels Enzyme- inducing AEDs increase cytochrome P450 en- zymes12021 resulting in increased metabolism of syn- thetic estrogens (ethinyl estradiol and mestranol) and lowered serum levels of approximately 40 (ta- ble 2) 1 2 T Z2~25 Free progestin levels are also de- creased probably due to increased synthesis of sex hormone-binding globulins220 Valproic and two new AEDs- gabapentin and vigabatrin- do not induce hepatic P450 metabolism and are unlikely to interfere with OCs Gabapentin does not decrease estradiol levels24 and vigabatrin has not been stud- ied Oxcarbazepine lowers OC sex hormone levels2rdquo and is likely to interfere with OCs Effects of lam- otrigine and felbamate on OCs have not been stud- 1538 NEUROLOGY 46 June 1996
ied Lamotrigine is metabolized by hepatic glucu- ronidation however rather than by the microsomal P450 system and possibly may not stimulate sex hor- mone metabolism
Over 150 accidental pregnancies have been re- ported in patients taking enzyme-inducing AEDs primarily women from the United K i n g d ~ m ~ ~ ~ and including the minimum of 75 American patients reported in this survey17~s1126-28 Valproic acid a nonenzyme-inducing AED has not been associated with accidental pregnancies when used in mono- therapy (table 3)
There are recommendations that women taking enzyme-inducing mDs increase their OC dose from 20 to 35 pg estradiol to 50 pg particularly if break- through menstrual bleeding O C C U ~ S ~ ~ J ~ - ~ ~ OC failures may occasionally occur however at 50- to 80-pg es- tradiol doses and with no warning of irregular men- strual bleeding so women taking these doses of OCs with enzyme-inducing AEDs need counseling that they are not completely protected against pregnancy Most women who were previously reported with OC failures were taking 50- to 80-pg estradiol dose^^^^ Two of our four recent patients had OC failures de- spite taking OCs containing 50 pg estradiol (a fifth patient became pregnant while using levonorgestrol implant)
Physicians may use irregular or breakthrough menstrual bleeding as a clinical sign of low OC lev- els7J2 and the need to increase OC doses or add con- traceptives Enzyme-inducing AEDs produce break- through bleeding in 71 to 76 of women taking OCs whereas only 6 of those taking valproic acid had breakthrough bleeding7 Women taking 30 pg estra- diol had higher rates of bleeding than those taking 50 pg and when OC doses were increased from 50 to 75 pg estradiol breakthrough bleeding stopped in 10 of 12 women initially and in 8 of 12 chronically
This supports using ldquohigher doserdquo OCs with 50 pg estradiol for most women taking enzyme-inducing AEDs rather than the ldquolow doserdquo 20- to 35-pg estra- diol pills High-dose OCs with 80 pg estradiol are no longer available Women with breakthrough bleeding on 50 pg estradiol may supplement their dose by 25 pg estradiol using an extra half pill or use other contraceptive methods A small proportion of women do not have decreased OC levels with MDsZ0 and will be exposed to slightly increased steroid levels if OC doses are increased Those a t most risk for thromboembolic complications associated with high- dose OCs are smokers and women over 35 years
There are currently no routine clinical labora- tory measures to determine which women have suff- cient OC sex hormone levels to prevent conception
Despite the effects of AEDs on sex hormone levels OCs are still usually more effective than barrier con- traceptives The typical failure rate with barrier con- traceptives is 12 to 211deg Seven percent of women taking AEDs with OCs had accidental pregnancies in one small seriesll Women taking OCs who seek high levels of contraceptive protection can in addition to
increasing their OC dose add a spermicidal gel or foam or other barrier methods An effective alterna- tive hormonal therapy to OCs is the depo form of medroxyprogesterone (Depo Provera) a strong pro- gestin contraceptive that has not been associated with contraceptive failures due to AEDs~O Levonor- gestrol implant (ldquoNorplantrdquo) is not an effective alter- native for women with epilepsy Over 30 accidental pregnancies have occurred for women using levonorgestrol implant with AEDs31 this is probably due to increased sex hormone-binding globulin and decreased free norgestrol levels32 Certain women may also consider intrauterine devices instead of OCs for contraception
After our experience with accidental pregnancies in our patients we counsel women of child-bearing years with epilepsy about their contraceptive choices using guidelines based on previous recommenda- t i o n ~ ~ ~ rsquo rdquo ~ ~ and incorporating the new data about AEDs and contraceptives reviewed above (table 4) Women taking enzyme-inducing AEDs for other neu- rologic and psychiatric conditions will also benefit from contraceptive counseling
In addition to often not being aware of contracep- tive problems many physicians were not aware of the teratogenicity of AEDs Nearly one-half of neu- rologists (44) estimated the risk of birth defects in offspring of women treated for epilepsy as 0 to 3 This estimate is similar to the background rate of 2 for women not taking AEDs and underestimates the true risk of approximately 4 to 63 Obstetriciansrsquo estimates of the risk for malformations were more accurate than neurologists although 23 of them also underestimated the risk of birth defects
These results suggest that many neurologists and obstetricians do not have accurate knowledge to counsel women with epilepsy regarding their contra- ceptive and pregnancy choices Women with epilepsy might often benefit from discussing reproductive is- sues with both specialists because neurologists are generally more familiar with the effects of AEDs on OCs and obstetricians provide more accurate coun- seling about birth defect risks
References 1 Back DJ Orme ML Pharmacokinetic drug interactions with
oral contraceptives Clin Pharmacokinet 199018472-484 2 Crawford P Chadwick DJ Martin C Tjia J Back DJ Orme
M The interaction of phenytoin and carbamazepine with com- bined oral contraceptive steroids Br J Clin Pharmacol 1990
3 Yerby MS Treatment of epilepsy during pregnancy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993844-857
4 Waters CH Belai Y Gott PS Shen P De Giorgio CM Out- comes of pregnancy associated with antiepileptic drugs Arch Neurol 19945 1250 -253
5 Hauser WA HesdorfTer DC Pregnancy and teratogenesis In Epilepsy frequency causes and consequences New York Demos Publications 1990147-196
6 Beresford HR Legal issues roles of physicians in preventing fetal harm In Devinsky 0 Feldmann E Hainline B eds
30892-896
Neurological complications of pregnancy New York Raven Press 1994
7 Sonnen AE Sodium valproate and the contraceptive pill Br J Clin Prac Symp Suppl 19832731-36
8 Back DJ Evaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive drug interactions with anticonvulsants and antibiotics Br J Clin Pharmacol
9 Sparrow MF Pill method failures NZ Med J 1987100102- 103
10 Trussell J Kost K A guide to interpreting contraceptive effi- cacy studies Obstet Gynecol 199076558-567
11 Coulam CB Do anticonvulsants reduce the efficacy of oral contraceptives Epilepsia 197920519-525
12 Diamond MP Greene JW Thompson JM VanHooydonk JE Interactions of anticonvulsants and oral contraceptives in ep- ileptic adolescents Contraception 198531623-632
13 Mattson RH Cramer JA Darney PD Naftolin F Use of oral contraceptives by women with epilepsy JAMA 1986256238- 240
14 Cramer JA Mattson RH Hormones and epilepsy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993686-691
15 Editorial Drug interaction with oral contraceptive steroids
16 American Academy of Neurology Neurologists 1991-1992 Minneapolis AAN 1993
17 Roback G Randolph L Seldman B Pasko T Physician char- acteristics and distribution in the US Chicago AMA Depart- ment of Data Services 1994
18 Physiciansrsquo Desk Reference 48th ed Montvale Medical Eco- nomics Data Production Company 1994
19 Kerlinger F Foundations of behavioral research 2nd ed New York Holt Rinehart 1973414
20 Back DJ Breckenridge AM Crawford FE Orme ML Rowe PH Phenobarbitone interaction with oral contraceptive ste- roids in the rabbit and rat Br J Pharmacol 198069441-452
21 Levin W Welch RM Conney AH Effect of chronic phenobar- bital treatment on the liver microsomal metabolism and uterotropic action of 17s-estradiol Endocrinology 196780
22 Back DJ Bates M Bowden M Breckenridge AM Hall MJ The interaction of phenobarbital and other anticonvulsants with oral contraceptive steroid therapy Contraception 1980
23 Crawford P Chadwick D Cleland P e t al The lack of effect of sodium valproate on the pharmacokinetics of oral contracep- tive steroids Contraception 19853323-29
24 Eldon MA Underwood BA Randinitis EJ Posvar EL Sed- man AJ Lack of effect of gabapentin on the pharmacokinetics of a norethindrone acetateethinyl estradiol-containing oral contraceptive [abstract] Neurology 199343A307-A308
25 Jensen PK Saano V Haring P Svenstrup B Menge GP Possible interaction between oxcarbazepine and an oral con- traceptive Epilepsia 199233 1149 -1 152
26 Janz D Schmidt D Antiepileptic drugs and failure of oral contraceptives Lancet 197411113
27 Kenyon TW Unplanned pregnancy in an epileptic BMJ 1972
28 Krauss GL Brandt J Campbell M Plate C Summerfield M Anti-epileptic medicationioral contraceptive interactions a national survey of neurologists and obstetricians Neurology 1996461534-1539
29 Stadel BV Oral contraceptives and cardiovascular disease part 1 N Engl J Med 1981305612-618
30 Upjohn Laboratories Data on File 1995 31 Wyeth-Ayerst Laboratories Norplant System Data on file
1995 32 Haukkamaa M Contraception by Norplant subdermal cap-
sules is not reliable in epileptic patients on anticonvulsant treatment Contraception 198633559-565
33 Mattson RH Selection of antiepileptic drug therapy In Levy RH Mattson RH Meldrum BS eds Antiepileptic drugs 4th ed New York Raven Press 1995123-135
198825527-532
BMJ 198028193-94
135-140
22495-503
1686-687
June 1996 NEUROLOGY 46 1539
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

Figure 1 Physiciansrsquo knowledge of OC interactions with six common AEDs (new AEDs excluded) AEDs carbamaz- epine phenytoin valproic acid phenobarbital primidone ethosuximide
Physicians were asked which of eight AEDs interfered with OCs Their knowledge of which AEDs interfere with OCs was estimated however using only six of eight AEDs (phenytoin carbamazepine valproic acid phenobarbital primidone and ethosuximide ) Gabapentin and felbamate were not included because they had been recently released at the time of the survey and were not recognized by many neurologists and most obstetricians Correct responses were tha t phenytoin carbamazepine phenobarbital primidone and ethosuximide interfere with OCs whereas valproic acid does notlsquo27-9
Results Characteristics of survey respondents A total of 160 neurologists (16) and 147 obstetricians (147) responded to the questionnaire (table 1) The ages work setting and geographic distribution for responders were representative of neurologists and obstetricians national- l ~ rsquo ~ rdquo The responders were from 47 states The largest numbers were in office-based practices with medical school graduation in the 1960s through 1980s
Most neurologists (91) and obstetricians (7596) said they treat women with epilepsy of child-bearing age Most neurolo- gists (75) and most obstetricians (59) believed they were moderately or very familiar with the interactions be- tween AEDs and OCs Physiciansrsquo actual knowledge of OC- AED interactions however was extremely poor When physicians were scored on their knowledge of whether six common AEDs interfered with OCs (phenytoin carbamaz- epine valproic acid phenobarbital primidone and etho- suximide) only 4 of the neurologists and none of the obstetricians were correct for all six AEDs (figure 1) The two new AEDs gabapentin and felbamate were excluded because they were not recognized by most physicians The average score for neurologistsrsquo knowledge of OC interac- tions with the six AEDs was 61 5 22 and for obstetri- cians was 378 f 19 Neurologists were both more famil- iar with ( t = 350 d f 297 p lt 0001) and more knowledgeable about ( t = 782 d f 292 p lt 0001) AED-OC interactions than obstetricians
Most neurologists (77 to 84) knew that phenytoin car- bamazepine and phenobarbital interfered with OCs but only 38 knew that valproic acid does not interfere with
Specialistsrsquo knowledge of OC-AED interactions
1536 NEUROLOGY 46 June 1996
Figure 2 Estimate of birth defect risk associated with AEDs
OCs Most obstetricians also knew that phenytoin inter- fered with OCs (77) but fewer knew that phenobarbital (54) carbamazepine (44) and primidone (17) lowered OC levels and only 29 know that valproic acid did not interfere with OCs Few neurologists and obstetricians knew whether ethosuximide or the two new AEDs gaba- pentin and felbamate interfere with OCs
Younger physicians were slightly more knowledgeable than older physicians about common AED-OC interactions although this was significant only for obstetricians (neurol- ogists r = 014 p = 009 obstetricians r = 030 p lt 0001)
Fewer than half of neurologists (41) and obstetricians (43) have patients adjust their OC doses if they are taking AEDs Moreover a number of physicians noted that they ldquoadjusted OC doses by lowering estrogen doses or using relatively low-dose 35-kg estrogen pills An additional 8 of neurologists refer their patients to obstetricians to have OC doses adjusted
There was a strong association between neurologistsrsquo and obstetriciansrsquo knowledge of which AEDs interfere with OCs and whether they adjust OC doses to compensate for AED effects (neurologists t = 277 d f 143 p = 0006 obstetricians t = 421 df 128 p lt 0001) Even physicians who were ldquofamiliarrdquo with this drug interaction but did not have accurate knowledge of which AEDs were involved usually adjusted their patientsrsquo OC doses for patients on AEDs 89 of neurologists and 76 of obstetricians famil- iar with OC-AED interactions adjust OC dosages for pa- tients on AEDs whereas only 19 of neurologists and 24 of obstetricians not familiar with OC-AED interactions ad- just OC dosages (neurologists chi-square 1043 p = 0001 obstetricians chi-square 1464 p = 00001)
Twenty-seven percent of neurologists and 21 of obste- tricians reported OC failure in their patients taking AEDs Neurologists whose patients had accidental pregnancies on OCs and AEDs were more likely to adjust OC doses (58 versus 35) than neurologists whose patients had not had such pregnancies (chi-square 633 p = 0011) Obstetri- cians whose patients had accidental pregnancies on OC and AEDs were more likely to adjust OCs than obstetri- cians who had not had patients with accidental pregnan- cies (57 versus 39) although this did not reach signifi- cance (chi-square 296 p = 0086)
Pregnancy risks and counseling Women with epilepsy have significant risks of approximately 4 to 6 for congen-
Factors influencing OC dosing
Table 2 Effects of AEDs on OC hormone levels
Enzyme-inducing AEDs
Phenobarbital
Phenytoin
Carbamazepine
Oxacarbamazepine Nonenzyme-inducing AEDs
Valproic acid
Gabapentin
-381
-490 -422
-470
110
60
Estradiol () -
~
Changes in 24-hour serum levels from baseline or control values No significant change References 1 2 7 20 23-25
ital malformations in their offspring compared with a background risk of approximately 23 This 2-3X in- creased risk is increased further for women with uncon- trolled seizures taking multiple AEDs5 or who belong to high-risk socioeconomic group^^ Despite this there was a wide variation in physiciansrsquo estimates of the risk of mal- formations with many physicians particularly neurolo- gists underestimating the risk (figure 2) When counseling a pregnant woman with good seizure control on a single antiepileptic medication obstetricians said they would es- timate a mean risk for birth defects of 689 (range 0 to 50) Most obstetricians (95) estimated a birth defect risk due to a single AED between 1 and 10 Over one- fifth (23) of obstetricians underestimated the risk as 0 to 3 In counseling a woman with epilepsy neurologists estimated a lower mean risk for birth defects than did obstetricians 475 (range 0 to 50) (neurologistsrsquo versus obstetriciansrsquo estimates t = 351 df 286 p = 001) Most neurologists (95) estimated a risk of birth defects be- tween 0 and 9 A large proportion of neurologists (44) underestimated the risk of birth defects as 0 to 3
Only 3 of neurologists and 5 of obstetricians recom- mend that their patients taking AEDs not become preg- nant Physiciansrsquo estimates of the risk of birth defects as- sociated with a single AED did not influence whether they would recommend that women taking single anticonvul- sants should avoid pregnancy (neurologists t = 139 df 147 p = 0165 obstetricians t = 078 df 132 p = 044) There was also no correlation between physiciansrsquo esti- mates of the risk of birth defects and their knowledge of OC-AED interactions (neurologists r = 005 p = 056 obstetricians r = 0 0 1 ~ = 081)
Table 3 Reported OC failures with AEDs
AED Accidental pregnancies
Phenobarbital
Phenytoin
Carbamazepine
Valproic acid
Ethosuximide
51
42
19
6 (0 monotherapy)
4
References 1 7 11 28
Norgestrel or norethindrone ()
- 187
-420
-397
-360
oo 30rsquo
Discussion Over one-fifth of neurologists and ob- stetricians reported accidental pregnancies in their patients taking AEDs with OCs Most physicians however did not know which common AEDs inter- fere with OCs do not adjust OC doses to overcome the effects of enzyme-inducing AEDs on sex hormone levels and did not know that valproic acid and gaba- pentin are nonenzyme-inducing alternatives to en- zyme-inducing AEDs Although physicians who were at least moderately familiar with OC-AED interac- tions tended to adjust OC doses for their patients it is unclear how they would do this without recogniz- ing specific AED-OC interactions These results oc- cur despite warnings of AED-OC interactions in pharmaceutical product inserts the Physiciansrsquo Desk Reference18 and in several medical reviews and edi- t o r i a l ~ ~ ~ ~ J ~ - ~ ~ Our survey suggests that a large num- ber of women in the United States with epilepsy are at risk for unplanned pregnancies while taking OCs
There are several limitations in our survey A re- sponse bias to the questionnaire is possible It is typical however for only a few mailed question- naires to be returned19 The geographic distribution practice types and ages of respondents were typical for American neurologists and obstetricians (see ta- ble l)16J7 Nonetheless the survey may have overes- timated physiciansrsquo lack of knowledge about AED complications for women with epilepsy particularly if nonrespondents were physicians who already knew about the reproductive risks of AEDs More likely however is that those who believed these issues are important would respond rather than those who do not recognize the reproductive complications associ- ated with AEDs This suggests in fact that any skew in the study would be toward overestimating physiciansrsquo knowledge of these issues Evidence that less-knowledgeable physicians were not over- represented in the survey is that a larger proportion of responders were board-certified specialists than the national average (see table 1) Another limitation is that several questions could not be asked directly without cuing other responses We could not ask for example questions to determine precisely how phy-
June 1996 NEUROLOGY 46 1537
Table 4 Suggestions for combining OCs and AEDs for women with epilepsy
1 Discuss contraceptive choices and the effects of enzyme- inducing AEDs (carbamazepine phenytoin phenobarbital primidone and ethosuximide) on OCs with all women of child-bearing years who have epilepsy This can be part of a general discussion of the risks of pregnancy and epilepsy
When treating women with epilepsy taking OCs continue to select AEDs according to recommended indications for epilepsy33
AED (valproic acid gabapentin vigabatrin) for women taking OCs
equivalent) for women taking enzyme-inducing AEDs who desire effective contraception Obstetricians and family physicians usually prescribe the OCs Counsel women that increased OC doses do not always protect from contraceptive failures due to AEDs but that OC failure rates are usually lower than with barrier methods alone
irregular menstrual bleeding while taking OCs Increase OC doses or switch contraceptives if irregular bleeding occurs
2
3 If AEDs are otherwise equivalent use a nonenzyme-inducing
4 Recommend OC doses of 50 pg estradiol (or mestranol
5 Have women with epilepsy monitor for breakthrough or
6 Advise women seeking very high levels of contraception protection that they may add spermicide or barrier contraception to their OCs
7 Alternative contraceptives that can be used for some women are medroxyprogesterone (Depo-Provera) and intrauterine devices Many pregnancies have occurred with levonorgestrol implant (ldquoNorplantrdquo) and enzyme-inducing AEDs
8 Oxcarbazepine lowers OC hormone levels whereas gabapentin and vigabatrin are nonenzyme-inducers that are unlikely to interfere with OCs The effects of lamotrigine and felbamate on OCs are unclear
Modified from references 7 13 15
sicians adjust OC doses whether physicians monitor patients for irregular menstrual bleeding as a sign of AED effects on OCs and how many total patients had accidental pregnancies due to AEDs
Enzyme-inducing AEDs including carbamaz- epine phenytoin phenobarbital primidone and ethosuximide decrease the effectiveness of OCs by lowering synthetic sex hormone levels Enzyme- inducing AEDs increase cytochrome P450 en- zymes12021 resulting in increased metabolism of syn- thetic estrogens (ethinyl estradiol and mestranol) and lowered serum levels of approximately 40 (ta- ble 2) 1 2 T Z2~25 Free progestin levels are also de- creased probably due to increased synthesis of sex hormone-binding globulins220 Valproic and two new AEDs- gabapentin and vigabatrin- do not induce hepatic P450 metabolism and are unlikely to interfere with OCs Gabapentin does not decrease estradiol levels24 and vigabatrin has not been stud- ied Oxcarbazepine lowers OC sex hormone levels2rdquo and is likely to interfere with OCs Effects of lam- otrigine and felbamate on OCs have not been stud- 1538 NEUROLOGY 46 June 1996
ied Lamotrigine is metabolized by hepatic glucu- ronidation however rather than by the microsomal P450 system and possibly may not stimulate sex hor- mone metabolism
Over 150 accidental pregnancies have been re- ported in patients taking enzyme-inducing AEDs primarily women from the United K i n g d ~ m ~ ~ ~ and including the minimum of 75 American patients reported in this survey17~s1126-28 Valproic acid a nonenzyme-inducing AED has not been associated with accidental pregnancies when used in mono- therapy (table 3)
There are recommendations that women taking enzyme-inducing mDs increase their OC dose from 20 to 35 pg estradiol to 50 pg particularly if break- through menstrual bleeding O C C U ~ S ~ ~ J ~ - ~ ~ OC failures may occasionally occur however at 50- to 80-pg es- tradiol doses and with no warning of irregular men- strual bleeding so women taking these doses of OCs with enzyme-inducing AEDs need counseling that they are not completely protected against pregnancy Most women who were previously reported with OC failures were taking 50- to 80-pg estradiol dose^^^^ Two of our four recent patients had OC failures de- spite taking OCs containing 50 pg estradiol (a fifth patient became pregnant while using levonorgestrol implant)
Physicians may use irregular or breakthrough menstrual bleeding as a clinical sign of low OC lev- els7J2 and the need to increase OC doses or add con- traceptives Enzyme-inducing AEDs produce break- through bleeding in 71 to 76 of women taking OCs whereas only 6 of those taking valproic acid had breakthrough bleeding7 Women taking 30 pg estra- diol had higher rates of bleeding than those taking 50 pg and when OC doses were increased from 50 to 75 pg estradiol breakthrough bleeding stopped in 10 of 12 women initially and in 8 of 12 chronically
This supports using ldquohigher doserdquo OCs with 50 pg estradiol for most women taking enzyme-inducing AEDs rather than the ldquolow doserdquo 20- to 35-pg estra- diol pills High-dose OCs with 80 pg estradiol are no longer available Women with breakthrough bleeding on 50 pg estradiol may supplement their dose by 25 pg estradiol using an extra half pill or use other contraceptive methods A small proportion of women do not have decreased OC levels with MDsZ0 and will be exposed to slightly increased steroid levels if OC doses are increased Those a t most risk for thromboembolic complications associated with high- dose OCs are smokers and women over 35 years
There are currently no routine clinical labora- tory measures to determine which women have suff- cient OC sex hormone levels to prevent conception
Despite the effects of AEDs on sex hormone levels OCs are still usually more effective than barrier con- traceptives The typical failure rate with barrier con- traceptives is 12 to 211deg Seven percent of women taking AEDs with OCs had accidental pregnancies in one small seriesll Women taking OCs who seek high levels of contraceptive protection can in addition to
increasing their OC dose add a spermicidal gel or foam or other barrier methods An effective alterna- tive hormonal therapy to OCs is the depo form of medroxyprogesterone (Depo Provera) a strong pro- gestin contraceptive that has not been associated with contraceptive failures due to AEDs~O Levonor- gestrol implant (ldquoNorplantrdquo) is not an effective alter- native for women with epilepsy Over 30 accidental pregnancies have occurred for women using levonorgestrol implant with AEDs31 this is probably due to increased sex hormone-binding globulin and decreased free norgestrol levels32 Certain women may also consider intrauterine devices instead of OCs for contraception
After our experience with accidental pregnancies in our patients we counsel women of child-bearing years with epilepsy about their contraceptive choices using guidelines based on previous recommenda- t i o n ~ ~ ~ rsquo rdquo ~ ~ and incorporating the new data about AEDs and contraceptives reviewed above (table 4) Women taking enzyme-inducing AEDs for other neu- rologic and psychiatric conditions will also benefit from contraceptive counseling
In addition to often not being aware of contracep- tive problems many physicians were not aware of the teratogenicity of AEDs Nearly one-half of neu- rologists (44) estimated the risk of birth defects in offspring of women treated for epilepsy as 0 to 3 This estimate is similar to the background rate of 2 for women not taking AEDs and underestimates the true risk of approximately 4 to 63 Obstetriciansrsquo estimates of the risk for malformations were more accurate than neurologists although 23 of them also underestimated the risk of birth defects
These results suggest that many neurologists and obstetricians do not have accurate knowledge to counsel women with epilepsy regarding their contra- ceptive and pregnancy choices Women with epilepsy might often benefit from discussing reproductive is- sues with both specialists because neurologists are generally more familiar with the effects of AEDs on OCs and obstetricians provide more accurate coun- seling about birth defect risks
References 1 Back DJ Orme ML Pharmacokinetic drug interactions with
oral contraceptives Clin Pharmacokinet 199018472-484 2 Crawford P Chadwick DJ Martin C Tjia J Back DJ Orme
M The interaction of phenytoin and carbamazepine with com- bined oral contraceptive steroids Br J Clin Pharmacol 1990
3 Yerby MS Treatment of epilepsy during pregnancy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993844-857
4 Waters CH Belai Y Gott PS Shen P De Giorgio CM Out- comes of pregnancy associated with antiepileptic drugs Arch Neurol 19945 1250 -253
5 Hauser WA HesdorfTer DC Pregnancy and teratogenesis In Epilepsy frequency causes and consequences New York Demos Publications 1990147-196
6 Beresford HR Legal issues roles of physicians in preventing fetal harm In Devinsky 0 Feldmann E Hainline B eds
30892-896
Neurological complications of pregnancy New York Raven Press 1994
7 Sonnen AE Sodium valproate and the contraceptive pill Br J Clin Prac Symp Suppl 19832731-36
8 Back DJ Evaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive drug interactions with anticonvulsants and antibiotics Br J Clin Pharmacol
9 Sparrow MF Pill method failures NZ Med J 1987100102- 103
10 Trussell J Kost K A guide to interpreting contraceptive effi- cacy studies Obstet Gynecol 199076558-567
11 Coulam CB Do anticonvulsants reduce the efficacy of oral contraceptives Epilepsia 197920519-525
12 Diamond MP Greene JW Thompson JM VanHooydonk JE Interactions of anticonvulsants and oral contraceptives in ep- ileptic adolescents Contraception 198531623-632
13 Mattson RH Cramer JA Darney PD Naftolin F Use of oral contraceptives by women with epilepsy JAMA 1986256238- 240
14 Cramer JA Mattson RH Hormones and epilepsy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993686-691
15 Editorial Drug interaction with oral contraceptive steroids
16 American Academy of Neurology Neurologists 1991-1992 Minneapolis AAN 1993
17 Roback G Randolph L Seldman B Pasko T Physician char- acteristics and distribution in the US Chicago AMA Depart- ment of Data Services 1994
18 Physiciansrsquo Desk Reference 48th ed Montvale Medical Eco- nomics Data Production Company 1994
19 Kerlinger F Foundations of behavioral research 2nd ed New York Holt Rinehart 1973414
20 Back DJ Breckenridge AM Crawford FE Orme ML Rowe PH Phenobarbitone interaction with oral contraceptive ste- roids in the rabbit and rat Br J Pharmacol 198069441-452
21 Levin W Welch RM Conney AH Effect of chronic phenobar- bital treatment on the liver microsomal metabolism and uterotropic action of 17s-estradiol Endocrinology 196780
22 Back DJ Bates M Bowden M Breckenridge AM Hall MJ The interaction of phenobarbital and other anticonvulsants with oral contraceptive steroid therapy Contraception 1980
23 Crawford P Chadwick D Cleland P e t al The lack of effect of sodium valproate on the pharmacokinetics of oral contracep- tive steroids Contraception 19853323-29
24 Eldon MA Underwood BA Randinitis EJ Posvar EL Sed- man AJ Lack of effect of gabapentin on the pharmacokinetics of a norethindrone acetateethinyl estradiol-containing oral contraceptive [abstract] Neurology 199343A307-A308
25 Jensen PK Saano V Haring P Svenstrup B Menge GP Possible interaction between oxcarbazepine and an oral con- traceptive Epilepsia 199233 1149 -1 152
26 Janz D Schmidt D Antiepileptic drugs and failure of oral contraceptives Lancet 197411113
27 Kenyon TW Unplanned pregnancy in an epileptic BMJ 1972
28 Krauss GL Brandt J Campbell M Plate C Summerfield M Anti-epileptic medicationioral contraceptive interactions a national survey of neurologists and obstetricians Neurology 1996461534-1539
29 Stadel BV Oral contraceptives and cardiovascular disease part 1 N Engl J Med 1981305612-618
30 Upjohn Laboratories Data on File 1995 31 Wyeth-Ayerst Laboratories Norplant System Data on file
1995 32 Haukkamaa M Contraception by Norplant subdermal cap-
sules is not reliable in epileptic patients on anticonvulsant treatment Contraception 198633559-565
33 Mattson RH Selection of antiepileptic drug therapy In Levy RH Mattson RH Meldrum BS eds Antiepileptic drugs 4th ed New York Raven Press 1995123-135
198825527-532
BMJ 198028193-94
135-140
22495-503
1686-687
June 1996 NEUROLOGY 46 1539
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
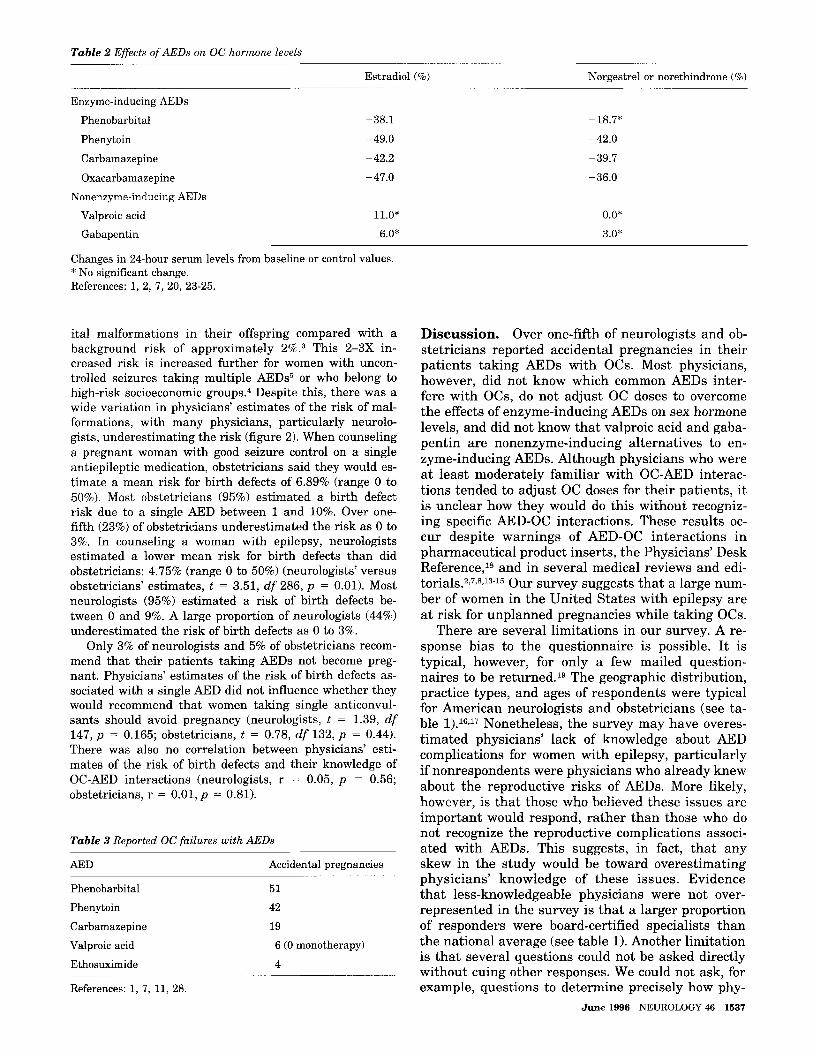
Table 2 Effects of AEDs on OC hormone levels
Enzyme-inducing AEDs
Phenobarbital
Phenytoin
Carbamazepine
Oxacarbamazepine Nonenzyme-inducing AEDs
Valproic acid
Gabapentin
-381
-490 -422
-470
110
60
Estradiol () -
~
Changes in 24-hour serum levels from baseline or control values No significant change References 1 2 7 20 23-25
ital malformations in their offspring compared with a background risk of approximately 23 This 2-3X in- creased risk is increased further for women with uncon- trolled seizures taking multiple AEDs5 or who belong to high-risk socioeconomic group^^ Despite this there was a wide variation in physiciansrsquo estimates of the risk of mal- formations with many physicians particularly neurolo- gists underestimating the risk (figure 2) When counseling a pregnant woman with good seizure control on a single antiepileptic medication obstetricians said they would es- timate a mean risk for birth defects of 689 (range 0 to 50) Most obstetricians (95) estimated a birth defect risk due to a single AED between 1 and 10 Over one- fifth (23) of obstetricians underestimated the risk as 0 to 3 In counseling a woman with epilepsy neurologists estimated a lower mean risk for birth defects than did obstetricians 475 (range 0 to 50) (neurologistsrsquo versus obstetriciansrsquo estimates t = 351 df 286 p = 001) Most neurologists (95) estimated a risk of birth defects be- tween 0 and 9 A large proportion of neurologists (44) underestimated the risk of birth defects as 0 to 3
Only 3 of neurologists and 5 of obstetricians recom- mend that their patients taking AEDs not become preg- nant Physiciansrsquo estimates of the risk of birth defects as- sociated with a single AED did not influence whether they would recommend that women taking single anticonvul- sants should avoid pregnancy (neurologists t = 139 df 147 p = 0165 obstetricians t = 078 df 132 p = 044) There was also no correlation between physiciansrsquo esti- mates of the risk of birth defects and their knowledge of OC-AED interactions (neurologists r = 005 p = 056 obstetricians r = 0 0 1 ~ = 081)
Table 3 Reported OC failures with AEDs
AED Accidental pregnancies
Phenobarbital
Phenytoin
Carbamazepine
Valproic acid
Ethosuximide
51
42
19
6 (0 monotherapy)
4
References 1 7 11 28
Norgestrel or norethindrone ()
- 187
-420
-397
-360
oo 30rsquo
Discussion Over one-fifth of neurologists and ob- stetricians reported accidental pregnancies in their patients taking AEDs with OCs Most physicians however did not know which common AEDs inter- fere with OCs do not adjust OC doses to overcome the effects of enzyme-inducing AEDs on sex hormone levels and did not know that valproic acid and gaba- pentin are nonenzyme-inducing alternatives to en- zyme-inducing AEDs Although physicians who were at least moderately familiar with OC-AED interac- tions tended to adjust OC doses for their patients it is unclear how they would do this without recogniz- ing specific AED-OC interactions These results oc- cur despite warnings of AED-OC interactions in pharmaceutical product inserts the Physiciansrsquo Desk Reference18 and in several medical reviews and edi- t o r i a l ~ ~ ~ ~ J ~ - ~ ~ Our survey suggests that a large num- ber of women in the United States with epilepsy are at risk for unplanned pregnancies while taking OCs
There are several limitations in our survey A re- sponse bias to the questionnaire is possible It is typical however for only a few mailed question- naires to be returned19 The geographic distribution practice types and ages of respondents were typical for American neurologists and obstetricians (see ta- ble l)16J7 Nonetheless the survey may have overes- timated physiciansrsquo lack of knowledge about AED complications for women with epilepsy particularly if nonrespondents were physicians who already knew about the reproductive risks of AEDs More likely however is that those who believed these issues are important would respond rather than those who do not recognize the reproductive complications associ- ated with AEDs This suggests in fact that any skew in the study would be toward overestimating physiciansrsquo knowledge of these issues Evidence that less-knowledgeable physicians were not over- represented in the survey is that a larger proportion of responders were board-certified specialists than the national average (see table 1) Another limitation is that several questions could not be asked directly without cuing other responses We could not ask for example questions to determine precisely how phy-
June 1996 NEUROLOGY 46 1537
Table 4 Suggestions for combining OCs and AEDs for women with epilepsy
1 Discuss contraceptive choices and the effects of enzyme- inducing AEDs (carbamazepine phenytoin phenobarbital primidone and ethosuximide) on OCs with all women of child-bearing years who have epilepsy This can be part of a general discussion of the risks of pregnancy and epilepsy
When treating women with epilepsy taking OCs continue to select AEDs according to recommended indications for epilepsy33
AED (valproic acid gabapentin vigabatrin) for women taking OCs
equivalent) for women taking enzyme-inducing AEDs who desire effective contraception Obstetricians and family physicians usually prescribe the OCs Counsel women that increased OC doses do not always protect from contraceptive failures due to AEDs but that OC failure rates are usually lower than with barrier methods alone
irregular menstrual bleeding while taking OCs Increase OC doses or switch contraceptives if irregular bleeding occurs
2
3 If AEDs are otherwise equivalent use a nonenzyme-inducing
4 Recommend OC doses of 50 pg estradiol (or mestranol
5 Have women with epilepsy monitor for breakthrough or
6 Advise women seeking very high levels of contraception protection that they may add spermicide or barrier contraception to their OCs
7 Alternative contraceptives that can be used for some women are medroxyprogesterone (Depo-Provera) and intrauterine devices Many pregnancies have occurred with levonorgestrol implant (ldquoNorplantrdquo) and enzyme-inducing AEDs
8 Oxcarbazepine lowers OC hormone levels whereas gabapentin and vigabatrin are nonenzyme-inducers that are unlikely to interfere with OCs The effects of lamotrigine and felbamate on OCs are unclear
Modified from references 7 13 15
sicians adjust OC doses whether physicians monitor patients for irregular menstrual bleeding as a sign of AED effects on OCs and how many total patients had accidental pregnancies due to AEDs
Enzyme-inducing AEDs including carbamaz- epine phenytoin phenobarbital primidone and ethosuximide decrease the effectiveness of OCs by lowering synthetic sex hormone levels Enzyme- inducing AEDs increase cytochrome P450 en- zymes12021 resulting in increased metabolism of syn- thetic estrogens (ethinyl estradiol and mestranol) and lowered serum levels of approximately 40 (ta- ble 2) 1 2 T Z2~25 Free progestin levels are also de- creased probably due to increased synthesis of sex hormone-binding globulins220 Valproic and two new AEDs- gabapentin and vigabatrin- do not induce hepatic P450 metabolism and are unlikely to interfere with OCs Gabapentin does not decrease estradiol levels24 and vigabatrin has not been stud- ied Oxcarbazepine lowers OC sex hormone levels2rdquo and is likely to interfere with OCs Effects of lam- otrigine and felbamate on OCs have not been stud- 1538 NEUROLOGY 46 June 1996
ied Lamotrigine is metabolized by hepatic glucu- ronidation however rather than by the microsomal P450 system and possibly may not stimulate sex hor- mone metabolism
Over 150 accidental pregnancies have been re- ported in patients taking enzyme-inducing AEDs primarily women from the United K i n g d ~ m ~ ~ ~ and including the minimum of 75 American patients reported in this survey17~s1126-28 Valproic acid a nonenzyme-inducing AED has not been associated with accidental pregnancies when used in mono- therapy (table 3)
There are recommendations that women taking enzyme-inducing mDs increase their OC dose from 20 to 35 pg estradiol to 50 pg particularly if break- through menstrual bleeding O C C U ~ S ~ ~ J ~ - ~ ~ OC failures may occasionally occur however at 50- to 80-pg es- tradiol doses and with no warning of irregular men- strual bleeding so women taking these doses of OCs with enzyme-inducing AEDs need counseling that they are not completely protected against pregnancy Most women who were previously reported with OC failures were taking 50- to 80-pg estradiol dose^^^^ Two of our four recent patients had OC failures de- spite taking OCs containing 50 pg estradiol (a fifth patient became pregnant while using levonorgestrol implant)
Physicians may use irregular or breakthrough menstrual bleeding as a clinical sign of low OC lev- els7J2 and the need to increase OC doses or add con- traceptives Enzyme-inducing AEDs produce break- through bleeding in 71 to 76 of women taking OCs whereas only 6 of those taking valproic acid had breakthrough bleeding7 Women taking 30 pg estra- diol had higher rates of bleeding than those taking 50 pg and when OC doses were increased from 50 to 75 pg estradiol breakthrough bleeding stopped in 10 of 12 women initially and in 8 of 12 chronically
This supports using ldquohigher doserdquo OCs with 50 pg estradiol for most women taking enzyme-inducing AEDs rather than the ldquolow doserdquo 20- to 35-pg estra- diol pills High-dose OCs with 80 pg estradiol are no longer available Women with breakthrough bleeding on 50 pg estradiol may supplement their dose by 25 pg estradiol using an extra half pill or use other contraceptive methods A small proportion of women do not have decreased OC levels with MDsZ0 and will be exposed to slightly increased steroid levels if OC doses are increased Those a t most risk for thromboembolic complications associated with high- dose OCs are smokers and women over 35 years
There are currently no routine clinical labora- tory measures to determine which women have suff- cient OC sex hormone levels to prevent conception
Despite the effects of AEDs on sex hormone levels OCs are still usually more effective than barrier con- traceptives The typical failure rate with barrier con- traceptives is 12 to 211deg Seven percent of women taking AEDs with OCs had accidental pregnancies in one small seriesll Women taking OCs who seek high levels of contraceptive protection can in addition to
increasing their OC dose add a spermicidal gel or foam or other barrier methods An effective alterna- tive hormonal therapy to OCs is the depo form of medroxyprogesterone (Depo Provera) a strong pro- gestin contraceptive that has not been associated with contraceptive failures due to AEDs~O Levonor- gestrol implant (ldquoNorplantrdquo) is not an effective alter- native for women with epilepsy Over 30 accidental pregnancies have occurred for women using levonorgestrol implant with AEDs31 this is probably due to increased sex hormone-binding globulin and decreased free norgestrol levels32 Certain women may also consider intrauterine devices instead of OCs for contraception
After our experience with accidental pregnancies in our patients we counsel women of child-bearing years with epilepsy about their contraceptive choices using guidelines based on previous recommenda- t i o n ~ ~ ~ rsquo rdquo ~ ~ and incorporating the new data about AEDs and contraceptives reviewed above (table 4) Women taking enzyme-inducing AEDs for other neu- rologic and psychiatric conditions will also benefit from contraceptive counseling
In addition to often not being aware of contracep- tive problems many physicians were not aware of the teratogenicity of AEDs Nearly one-half of neu- rologists (44) estimated the risk of birth defects in offspring of women treated for epilepsy as 0 to 3 This estimate is similar to the background rate of 2 for women not taking AEDs and underestimates the true risk of approximately 4 to 63 Obstetriciansrsquo estimates of the risk for malformations were more accurate than neurologists although 23 of them also underestimated the risk of birth defects
These results suggest that many neurologists and obstetricians do not have accurate knowledge to counsel women with epilepsy regarding their contra- ceptive and pregnancy choices Women with epilepsy might often benefit from discussing reproductive is- sues with both specialists because neurologists are generally more familiar with the effects of AEDs on OCs and obstetricians provide more accurate coun- seling about birth defect risks
References 1 Back DJ Orme ML Pharmacokinetic drug interactions with
oral contraceptives Clin Pharmacokinet 199018472-484 2 Crawford P Chadwick DJ Martin C Tjia J Back DJ Orme
M The interaction of phenytoin and carbamazepine with com- bined oral contraceptive steroids Br J Clin Pharmacol 1990
3 Yerby MS Treatment of epilepsy during pregnancy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993844-857
4 Waters CH Belai Y Gott PS Shen P De Giorgio CM Out- comes of pregnancy associated with antiepileptic drugs Arch Neurol 19945 1250 -253
5 Hauser WA HesdorfTer DC Pregnancy and teratogenesis In Epilepsy frequency causes and consequences New York Demos Publications 1990147-196
6 Beresford HR Legal issues roles of physicians in preventing fetal harm In Devinsky 0 Feldmann E Hainline B eds
30892-896
Neurological complications of pregnancy New York Raven Press 1994
7 Sonnen AE Sodium valproate and the contraceptive pill Br J Clin Prac Symp Suppl 19832731-36
8 Back DJ Evaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive drug interactions with anticonvulsants and antibiotics Br J Clin Pharmacol
9 Sparrow MF Pill method failures NZ Med J 1987100102- 103
10 Trussell J Kost K A guide to interpreting contraceptive effi- cacy studies Obstet Gynecol 199076558-567
11 Coulam CB Do anticonvulsants reduce the efficacy of oral contraceptives Epilepsia 197920519-525
12 Diamond MP Greene JW Thompson JM VanHooydonk JE Interactions of anticonvulsants and oral contraceptives in ep- ileptic adolescents Contraception 198531623-632
13 Mattson RH Cramer JA Darney PD Naftolin F Use of oral contraceptives by women with epilepsy JAMA 1986256238- 240
14 Cramer JA Mattson RH Hormones and epilepsy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993686-691
15 Editorial Drug interaction with oral contraceptive steroids
16 American Academy of Neurology Neurologists 1991-1992 Minneapolis AAN 1993
17 Roback G Randolph L Seldman B Pasko T Physician char- acteristics and distribution in the US Chicago AMA Depart- ment of Data Services 1994
18 Physiciansrsquo Desk Reference 48th ed Montvale Medical Eco- nomics Data Production Company 1994
19 Kerlinger F Foundations of behavioral research 2nd ed New York Holt Rinehart 1973414
20 Back DJ Breckenridge AM Crawford FE Orme ML Rowe PH Phenobarbitone interaction with oral contraceptive ste- roids in the rabbit and rat Br J Pharmacol 198069441-452
21 Levin W Welch RM Conney AH Effect of chronic phenobar- bital treatment on the liver microsomal metabolism and uterotropic action of 17s-estradiol Endocrinology 196780
22 Back DJ Bates M Bowden M Breckenridge AM Hall MJ The interaction of phenobarbital and other anticonvulsants with oral contraceptive steroid therapy Contraception 1980
23 Crawford P Chadwick D Cleland P e t al The lack of effect of sodium valproate on the pharmacokinetics of oral contracep- tive steroids Contraception 19853323-29
24 Eldon MA Underwood BA Randinitis EJ Posvar EL Sed- man AJ Lack of effect of gabapentin on the pharmacokinetics of a norethindrone acetateethinyl estradiol-containing oral contraceptive [abstract] Neurology 199343A307-A308
25 Jensen PK Saano V Haring P Svenstrup B Menge GP Possible interaction between oxcarbazepine and an oral con- traceptive Epilepsia 199233 1149 -1 152
26 Janz D Schmidt D Antiepileptic drugs and failure of oral contraceptives Lancet 197411113
27 Kenyon TW Unplanned pregnancy in an epileptic BMJ 1972
28 Krauss GL Brandt J Campbell M Plate C Summerfield M Anti-epileptic medicationioral contraceptive interactions a national survey of neurologists and obstetricians Neurology 1996461534-1539
29 Stadel BV Oral contraceptives and cardiovascular disease part 1 N Engl J Med 1981305612-618
30 Upjohn Laboratories Data on File 1995 31 Wyeth-Ayerst Laboratories Norplant System Data on file
1995 32 Haukkamaa M Contraception by Norplant subdermal cap-
sules is not reliable in epileptic patients on anticonvulsant treatment Contraception 198633559-565
33 Mattson RH Selection of antiepileptic drug therapy In Levy RH Mattson RH Meldrum BS eds Antiepileptic drugs 4th ed New York Raven Press 1995123-135
198825527-532
BMJ 198028193-94
135-140
22495-503
1686-687
June 1996 NEUROLOGY 46 1539
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
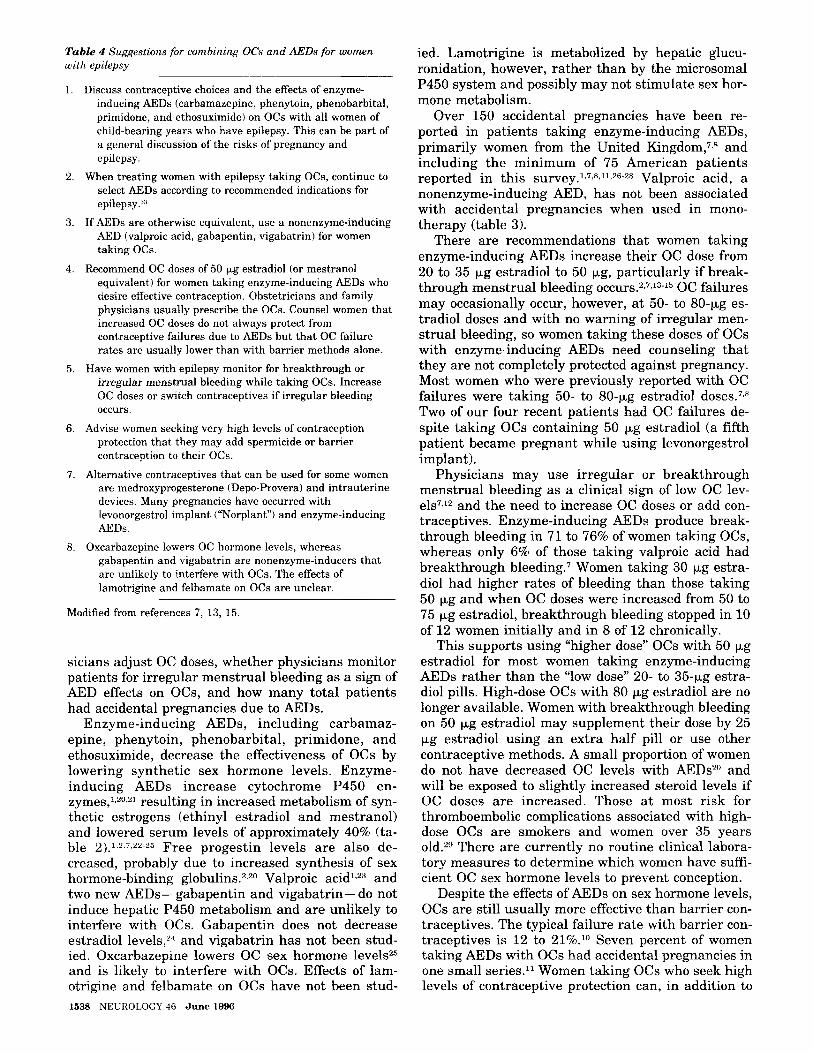
Table 4 Suggestions for combining OCs and AEDs for women with epilepsy
1 Discuss contraceptive choices and the effects of enzyme- inducing AEDs (carbamazepine phenytoin phenobarbital primidone and ethosuximide) on OCs with all women of child-bearing years who have epilepsy This can be part of a general discussion of the risks of pregnancy and epilepsy
When treating women with epilepsy taking OCs continue to select AEDs according to recommended indications for epilepsy33
AED (valproic acid gabapentin vigabatrin) for women taking OCs
equivalent) for women taking enzyme-inducing AEDs who desire effective contraception Obstetricians and family physicians usually prescribe the OCs Counsel women that increased OC doses do not always protect from contraceptive failures due to AEDs but that OC failure rates are usually lower than with barrier methods alone
irregular menstrual bleeding while taking OCs Increase OC doses or switch contraceptives if irregular bleeding occurs
2
3 If AEDs are otherwise equivalent use a nonenzyme-inducing
4 Recommend OC doses of 50 pg estradiol (or mestranol
5 Have women with epilepsy monitor for breakthrough or
6 Advise women seeking very high levels of contraception protection that they may add spermicide or barrier contraception to their OCs
7 Alternative contraceptives that can be used for some women are medroxyprogesterone (Depo-Provera) and intrauterine devices Many pregnancies have occurred with levonorgestrol implant (ldquoNorplantrdquo) and enzyme-inducing AEDs
8 Oxcarbazepine lowers OC hormone levels whereas gabapentin and vigabatrin are nonenzyme-inducers that are unlikely to interfere with OCs The effects of lamotrigine and felbamate on OCs are unclear
Modified from references 7 13 15
sicians adjust OC doses whether physicians monitor patients for irregular menstrual bleeding as a sign of AED effects on OCs and how many total patients had accidental pregnancies due to AEDs
Enzyme-inducing AEDs including carbamaz- epine phenytoin phenobarbital primidone and ethosuximide decrease the effectiveness of OCs by lowering synthetic sex hormone levels Enzyme- inducing AEDs increase cytochrome P450 en- zymes12021 resulting in increased metabolism of syn- thetic estrogens (ethinyl estradiol and mestranol) and lowered serum levels of approximately 40 (ta- ble 2) 1 2 T Z2~25 Free progestin levels are also de- creased probably due to increased synthesis of sex hormone-binding globulins220 Valproic and two new AEDs- gabapentin and vigabatrin- do not induce hepatic P450 metabolism and are unlikely to interfere with OCs Gabapentin does not decrease estradiol levels24 and vigabatrin has not been stud- ied Oxcarbazepine lowers OC sex hormone levels2rdquo and is likely to interfere with OCs Effects of lam- otrigine and felbamate on OCs have not been stud- 1538 NEUROLOGY 46 June 1996
ied Lamotrigine is metabolized by hepatic glucu- ronidation however rather than by the microsomal P450 system and possibly may not stimulate sex hor- mone metabolism
Over 150 accidental pregnancies have been re- ported in patients taking enzyme-inducing AEDs primarily women from the United K i n g d ~ m ~ ~ ~ and including the minimum of 75 American patients reported in this survey17~s1126-28 Valproic acid a nonenzyme-inducing AED has not been associated with accidental pregnancies when used in mono- therapy (table 3)
There are recommendations that women taking enzyme-inducing mDs increase their OC dose from 20 to 35 pg estradiol to 50 pg particularly if break- through menstrual bleeding O C C U ~ S ~ ~ J ~ - ~ ~ OC failures may occasionally occur however at 50- to 80-pg es- tradiol doses and with no warning of irregular men- strual bleeding so women taking these doses of OCs with enzyme-inducing AEDs need counseling that they are not completely protected against pregnancy Most women who were previously reported with OC failures were taking 50- to 80-pg estradiol dose^^^^ Two of our four recent patients had OC failures de- spite taking OCs containing 50 pg estradiol (a fifth patient became pregnant while using levonorgestrol implant)
Physicians may use irregular or breakthrough menstrual bleeding as a clinical sign of low OC lev- els7J2 and the need to increase OC doses or add con- traceptives Enzyme-inducing AEDs produce break- through bleeding in 71 to 76 of women taking OCs whereas only 6 of those taking valproic acid had breakthrough bleeding7 Women taking 30 pg estra- diol had higher rates of bleeding than those taking 50 pg and when OC doses were increased from 50 to 75 pg estradiol breakthrough bleeding stopped in 10 of 12 women initially and in 8 of 12 chronically
This supports using ldquohigher doserdquo OCs with 50 pg estradiol for most women taking enzyme-inducing AEDs rather than the ldquolow doserdquo 20- to 35-pg estra- diol pills High-dose OCs with 80 pg estradiol are no longer available Women with breakthrough bleeding on 50 pg estradiol may supplement their dose by 25 pg estradiol using an extra half pill or use other contraceptive methods A small proportion of women do not have decreased OC levels with MDsZ0 and will be exposed to slightly increased steroid levels if OC doses are increased Those a t most risk for thromboembolic complications associated with high- dose OCs are smokers and women over 35 years
There are currently no routine clinical labora- tory measures to determine which women have suff- cient OC sex hormone levels to prevent conception
Despite the effects of AEDs on sex hormone levels OCs are still usually more effective than barrier con- traceptives The typical failure rate with barrier con- traceptives is 12 to 211deg Seven percent of women taking AEDs with OCs had accidental pregnancies in one small seriesll Women taking OCs who seek high levels of contraceptive protection can in addition to
increasing their OC dose add a spermicidal gel or foam or other barrier methods An effective alterna- tive hormonal therapy to OCs is the depo form of medroxyprogesterone (Depo Provera) a strong pro- gestin contraceptive that has not been associated with contraceptive failures due to AEDs~O Levonor- gestrol implant (ldquoNorplantrdquo) is not an effective alter- native for women with epilepsy Over 30 accidental pregnancies have occurred for women using levonorgestrol implant with AEDs31 this is probably due to increased sex hormone-binding globulin and decreased free norgestrol levels32 Certain women may also consider intrauterine devices instead of OCs for contraception
After our experience with accidental pregnancies in our patients we counsel women of child-bearing years with epilepsy about their contraceptive choices using guidelines based on previous recommenda- t i o n ~ ~ ~ rsquo rdquo ~ ~ and incorporating the new data about AEDs and contraceptives reviewed above (table 4) Women taking enzyme-inducing AEDs for other neu- rologic and psychiatric conditions will also benefit from contraceptive counseling
In addition to often not being aware of contracep- tive problems many physicians were not aware of the teratogenicity of AEDs Nearly one-half of neu- rologists (44) estimated the risk of birth defects in offspring of women treated for epilepsy as 0 to 3 This estimate is similar to the background rate of 2 for women not taking AEDs and underestimates the true risk of approximately 4 to 63 Obstetriciansrsquo estimates of the risk for malformations were more accurate than neurologists although 23 of them also underestimated the risk of birth defects
These results suggest that many neurologists and obstetricians do not have accurate knowledge to counsel women with epilepsy regarding their contra- ceptive and pregnancy choices Women with epilepsy might often benefit from discussing reproductive is- sues with both specialists because neurologists are generally more familiar with the effects of AEDs on OCs and obstetricians provide more accurate coun- seling about birth defect risks
References 1 Back DJ Orme ML Pharmacokinetic drug interactions with
oral contraceptives Clin Pharmacokinet 199018472-484 2 Crawford P Chadwick DJ Martin C Tjia J Back DJ Orme
M The interaction of phenytoin and carbamazepine with com- bined oral contraceptive steroids Br J Clin Pharmacol 1990
3 Yerby MS Treatment of epilepsy during pregnancy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993844-857
4 Waters CH Belai Y Gott PS Shen P De Giorgio CM Out- comes of pregnancy associated with antiepileptic drugs Arch Neurol 19945 1250 -253
5 Hauser WA HesdorfTer DC Pregnancy and teratogenesis In Epilepsy frequency causes and consequences New York Demos Publications 1990147-196
6 Beresford HR Legal issues roles of physicians in preventing fetal harm In Devinsky 0 Feldmann E Hainline B eds
30892-896
Neurological complications of pregnancy New York Raven Press 1994
7 Sonnen AE Sodium valproate and the contraceptive pill Br J Clin Prac Symp Suppl 19832731-36
8 Back DJ Evaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive drug interactions with anticonvulsants and antibiotics Br J Clin Pharmacol
9 Sparrow MF Pill method failures NZ Med J 1987100102- 103
10 Trussell J Kost K A guide to interpreting contraceptive effi- cacy studies Obstet Gynecol 199076558-567
11 Coulam CB Do anticonvulsants reduce the efficacy of oral contraceptives Epilepsia 197920519-525
12 Diamond MP Greene JW Thompson JM VanHooydonk JE Interactions of anticonvulsants and oral contraceptives in ep- ileptic adolescents Contraception 198531623-632
13 Mattson RH Cramer JA Darney PD Naftolin F Use of oral contraceptives by women with epilepsy JAMA 1986256238- 240
14 Cramer JA Mattson RH Hormones and epilepsy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993686-691
15 Editorial Drug interaction with oral contraceptive steroids
16 American Academy of Neurology Neurologists 1991-1992 Minneapolis AAN 1993
17 Roback G Randolph L Seldman B Pasko T Physician char- acteristics and distribution in the US Chicago AMA Depart- ment of Data Services 1994
18 Physiciansrsquo Desk Reference 48th ed Montvale Medical Eco- nomics Data Production Company 1994
19 Kerlinger F Foundations of behavioral research 2nd ed New York Holt Rinehart 1973414
20 Back DJ Breckenridge AM Crawford FE Orme ML Rowe PH Phenobarbitone interaction with oral contraceptive ste- roids in the rabbit and rat Br J Pharmacol 198069441-452
21 Levin W Welch RM Conney AH Effect of chronic phenobar- bital treatment on the liver microsomal metabolism and uterotropic action of 17s-estradiol Endocrinology 196780
22 Back DJ Bates M Bowden M Breckenridge AM Hall MJ The interaction of phenobarbital and other anticonvulsants with oral contraceptive steroid therapy Contraception 1980
23 Crawford P Chadwick D Cleland P e t al The lack of effect of sodium valproate on the pharmacokinetics of oral contracep- tive steroids Contraception 19853323-29
24 Eldon MA Underwood BA Randinitis EJ Posvar EL Sed- man AJ Lack of effect of gabapentin on the pharmacokinetics of a norethindrone acetateethinyl estradiol-containing oral contraceptive [abstract] Neurology 199343A307-A308
25 Jensen PK Saano V Haring P Svenstrup B Menge GP Possible interaction between oxcarbazepine and an oral con- traceptive Epilepsia 199233 1149 -1 152
26 Janz D Schmidt D Antiepileptic drugs and failure of oral contraceptives Lancet 197411113
27 Kenyon TW Unplanned pregnancy in an epileptic BMJ 1972
28 Krauss GL Brandt J Campbell M Plate C Summerfield M Anti-epileptic medicationioral contraceptive interactions a national survey of neurologists and obstetricians Neurology 1996461534-1539
29 Stadel BV Oral contraceptives and cardiovascular disease part 1 N Engl J Med 1981305612-618
30 Upjohn Laboratories Data on File 1995 31 Wyeth-Ayerst Laboratories Norplant System Data on file
1995 32 Haukkamaa M Contraception by Norplant subdermal cap-
sules is not reliable in epileptic patients on anticonvulsant treatment Contraception 198633559-565
33 Mattson RH Selection of antiepileptic drug therapy In Levy RH Mattson RH Meldrum BS eds Antiepileptic drugs 4th ed New York Raven Press 1995123-135
198825527-532
BMJ 198028193-94
135-140
22495-503
1686-687
June 1996 NEUROLOGY 46 1539
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
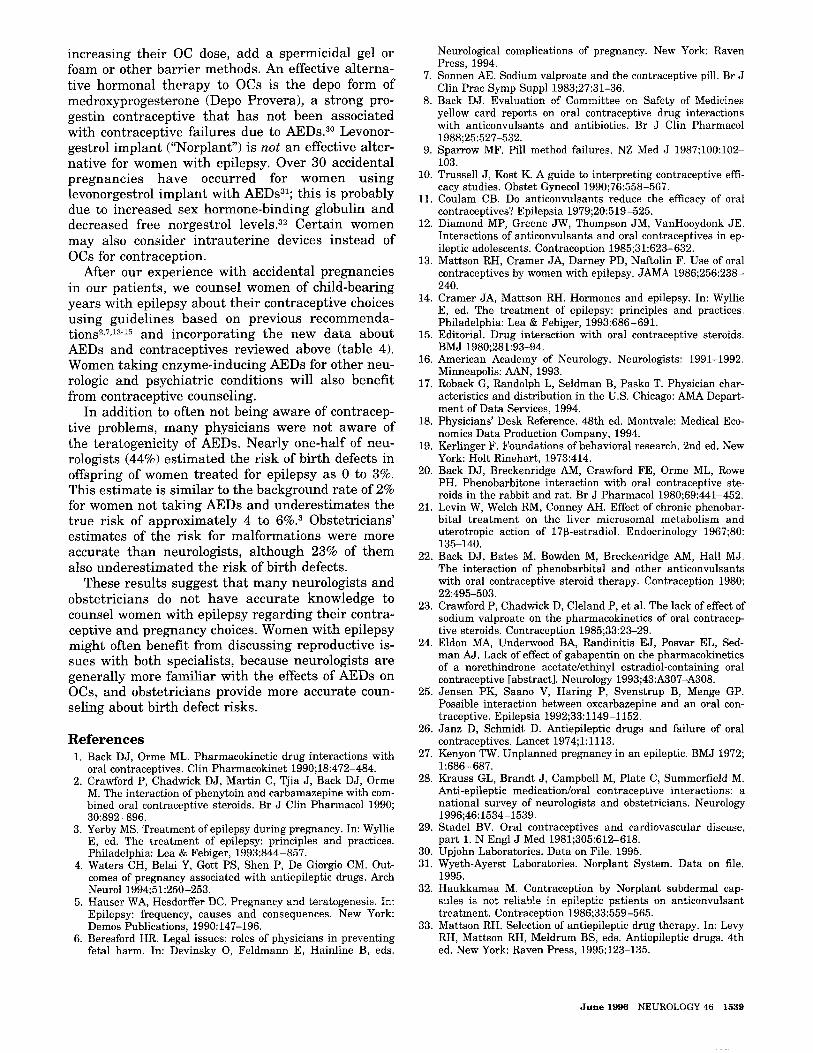
increasing their OC dose add a spermicidal gel or foam or other barrier methods An effective alterna- tive hormonal therapy to OCs is the depo form of medroxyprogesterone (Depo Provera) a strong pro- gestin contraceptive that has not been associated with contraceptive failures due to AEDs~O Levonor- gestrol implant (ldquoNorplantrdquo) is not an effective alter- native for women with epilepsy Over 30 accidental pregnancies have occurred for women using levonorgestrol implant with AEDs31 this is probably due to increased sex hormone-binding globulin and decreased free norgestrol levels32 Certain women may also consider intrauterine devices instead of OCs for contraception
After our experience with accidental pregnancies in our patients we counsel women of child-bearing years with epilepsy about their contraceptive choices using guidelines based on previous recommenda- t i o n ~ ~ ~ rsquo rdquo ~ ~ and incorporating the new data about AEDs and contraceptives reviewed above (table 4) Women taking enzyme-inducing AEDs for other neu- rologic and psychiatric conditions will also benefit from contraceptive counseling
In addition to often not being aware of contracep- tive problems many physicians were not aware of the teratogenicity of AEDs Nearly one-half of neu- rologists (44) estimated the risk of birth defects in offspring of women treated for epilepsy as 0 to 3 This estimate is similar to the background rate of 2 for women not taking AEDs and underestimates the true risk of approximately 4 to 63 Obstetriciansrsquo estimates of the risk for malformations were more accurate than neurologists although 23 of them also underestimated the risk of birth defects
These results suggest that many neurologists and obstetricians do not have accurate knowledge to counsel women with epilepsy regarding their contra- ceptive and pregnancy choices Women with epilepsy might often benefit from discussing reproductive is- sues with both specialists because neurologists are generally more familiar with the effects of AEDs on OCs and obstetricians provide more accurate coun- seling about birth defect risks
References 1 Back DJ Orme ML Pharmacokinetic drug interactions with
oral contraceptives Clin Pharmacokinet 199018472-484 2 Crawford P Chadwick DJ Martin C Tjia J Back DJ Orme
M The interaction of phenytoin and carbamazepine with com- bined oral contraceptive steroids Br J Clin Pharmacol 1990
3 Yerby MS Treatment of epilepsy during pregnancy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993844-857
4 Waters CH Belai Y Gott PS Shen P De Giorgio CM Out- comes of pregnancy associated with antiepileptic drugs Arch Neurol 19945 1250 -253
5 Hauser WA HesdorfTer DC Pregnancy and teratogenesis In Epilepsy frequency causes and consequences New York Demos Publications 1990147-196
6 Beresford HR Legal issues roles of physicians in preventing fetal harm In Devinsky 0 Feldmann E Hainline B eds
30892-896
Neurological complications of pregnancy New York Raven Press 1994
7 Sonnen AE Sodium valproate and the contraceptive pill Br J Clin Prac Symp Suppl 19832731-36
8 Back DJ Evaluation of Committee on Safety of Medicines yellow card reports on oral contraceptive drug interactions with anticonvulsants and antibiotics Br J Clin Pharmacol
9 Sparrow MF Pill method failures NZ Med J 1987100102- 103
10 Trussell J Kost K A guide to interpreting contraceptive effi- cacy studies Obstet Gynecol 199076558-567
11 Coulam CB Do anticonvulsants reduce the efficacy of oral contraceptives Epilepsia 197920519-525
12 Diamond MP Greene JW Thompson JM VanHooydonk JE Interactions of anticonvulsants and oral contraceptives in ep- ileptic adolescents Contraception 198531623-632
13 Mattson RH Cramer JA Darney PD Naftolin F Use of oral contraceptives by women with epilepsy JAMA 1986256238- 240
14 Cramer JA Mattson RH Hormones and epilepsy In Wyllie E ed The treatment of epilepsy principles and practices Philadelphia Lea amp Febiger 1993686-691
15 Editorial Drug interaction with oral contraceptive steroids
16 American Academy of Neurology Neurologists 1991-1992 Minneapolis AAN 1993
17 Roback G Randolph L Seldman B Pasko T Physician char- acteristics and distribution in the US Chicago AMA Depart- ment of Data Services 1994
18 Physiciansrsquo Desk Reference 48th ed Montvale Medical Eco- nomics Data Production Company 1994
19 Kerlinger F Foundations of behavioral research 2nd ed New York Holt Rinehart 1973414
20 Back DJ Breckenridge AM Crawford FE Orme ML Rowe PH Phenobarbitone interaction with oral contraceptive ste- roids in the rabbit and rat Br J Pharmacol 198069441-452
21 Levin W Welch RM Conney AH Effect of chronic phenobar- bital treatment on the liver microsomal metabolism and uterotropic action of 17s-estradiol Endocrinology 196780
22 Back DJ Bates M Bowden M Breckenridge AM Hall MJ The interaction of phenobarbital and other anticonvulsants with oral contraceptive steroid therapy Contraception 1980
23 Crawford P Chadwick D Cleland P e t al The lack of effect of sodium valproate on the pharmacokinetics of oral contracep- tive steroids Contraception 19853323-29
24 Eldon MA Underwood BA Randinitis EJ Posvar EL Sed- man AJ Lack of effect of gabapentin on the pharmacokinetics of a norethindrone acetateethinyl estradiol-containing oral contraceptive [abstract] Neurology 199343A307-A308
25 Jensen PK Saano V Haring P Svenstrup B Menge GP Possible interaction between oxcarbazepine and an oral con- traceptive Epilepsia 199233 1149 -1 152
26 Janz D Schmidt D Antiepileptic drugs and failure of oral contraceptives Lancet 197411113
27 Kenyon TW Unplanned pregnancy in an epileptic BMJ 1972
28 Krauss GL Brandt J Campbell M Plate C Summerfield M Anti-epileptic medicationioral contraceptive interactions a national survey of neurologists and obstetricians Neurology 1996461534-1539
29 Stadel BV Oral contraceptives and cardiovascular disease part 1 N Engl J Med 1981305612-618
30 Upjohn Laboratories Data on File 1995 31 Wyeth-Ayerst Laboratories Norplant System Data on file
1995 32 Haukkamaa M Contraception by Norplant subdermal cap-
sules is not reliable in epileptic patients on anticonvulsant treatment Contraception 198633559-565
33 Mattson RH Selection of antiepileptic drug therapy In Levy RH Mattson RH Meldrum BS eds Antiepileptic drugs 4th ed New York Raven Press 1995123-135
198825527-532
BMJ 198028193-94
135-140
22495-503
1686-687
June 1996 NEUROLOGY 46 1539
DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

DOI 101212WNL46615341996461534-1539 Neurology
G L Krauss J Brandt M Campbell et al neurologists and obstetricians
Antiepileptic medication and oral contraceptive interactions A national survey of
This information is current as of June 1 1996
ServicesUpdated Information amp
httpwwwneurologyorgcontent4661534fullhtmlincluding high resolution figures can be found at
References httpwwwneurologyorgcontent4661534fullhtmlref-list-1
This article cites 22 articles 2 of which you can access for free at
Citations httpwwwneurologyorgcontent4661534fullhtmlotherarticles
This article has been cited by 7 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsin its entirety can be found online atInformation about reproducing this article in parts (figurestables) or
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online