Embed Size (px)
Citation preview
Neurological Risk at Younger Ages
2015 AAIM Triennial
Paul J. Nittoli, MD

Presentation Objectives
• Discuss risk stratification of seizure disorders for both disability and life underwriting: clinical, diagnostic, treatment, and lifestyle factors
• Discuss mortality assessment in Multiple Sclerosis: risk implications of clinical features, diagnostic findings, and disease-modifying medication use
Brief History of Epilepsy
• 4500-1500 BC: described in Ayurvedic literature (‘apasmara’ = loss of consciousness)
• 1000 BC: described in a Babylonian tablet as supernatural
• 400 BC: Hippocrates’ monograph disputes supernatural cause
• 130-200 AD: Galen theorized it a brain disorder with manifestations governed by the moon (‘luna-tics’)
• 1494: Malleus Maleficarum links seizures with witchcraft• 1800s: John Harvey Kellogg (of corn flake fame)
attributed epilepsy to masturbationTemkin. The Falling Sickness: A history of Epilepsy from the Greeks to the
Beginnings of Modern Neurology. 2nd ed. 1971. The Johns Hopkins University Press

Seizure Disorders: Defining Terms
• “an excessive and disorderly discharge of central nervous system tissue on muscle” – John Hughlings Jackson MD, 1870
• Motor (convulsive)
• Sensory
• Autonomic
• Psychic
• Epilepsy: A) 2 unprovoked seizures 24 hrs apart; B) 1 seizure within the context of a predisposing cause
Seizure Disorders: Defining Terms
• Partial (focal) seizures – focal onset• Simple – no alteration of consciousness
• Complex – impaired consciousness
• Generalized seizures – bilateral onset, presumption of impaired consciousness
• Secondary generalization of partial seizures
• Absence (petit mal)
• Tonic +/- clonic (grand mal)
• Juvenile seizure disorders
• Pseudoseizures
Seizure Disorders: Defining Terms
• Idiopathic• No demonstrable neuropathology
• Often genetic, early life onset
• Symptomatic• Anatomy or pathology abnormal
• Often adult onset, focal seizures
• Cryptogenic• Unidentified etiology, presumed symptomatic
• Decreasing with improved imaging
• (Provoked)

Electroencephalogram
• “excessive and disorderly discharge” of cortical neurons
• Anticonvulsants have one (phenytoin, carbamazepine) or more (lamotrigine, valproate) mechanisms of action
• Asymptomatic interictal spikes may be present
• Absence of epileptiform discharges does not rule out a seizure disorder

Alternative AED Uses
• Valproic acid: psychiatric, analgesic
• Carbamazepine: psychiatric, analgesic
• Gabapentin: psychiatric, analgesic, menopausal sx
• Lamotrigine: psychiatric, analgesic
• Topiramate: psychiatric, analgesic, substance abuse, obesity
• Levetiracetam: psychiatric, autism, Tourette syndrome
• Primidone: essential tremor, LQTS
• Phenobarbital/ethosuximide/phenytoin: AED only
Nonpharmacologic Seizure
Management• Surgery
• Usually done for intractable epilepsy• Generalization improvement• Focal seizures may not be ameliorated and may worsen• Residual neurological deficits possible• Best outcomes: unilateral temporal or hippocampal loci
• Vagal nerve stimulation• Palliative not curative• Focal seizures
• Dietary modification• Ketogenic diet
» Mimics starvation – little or no carbs (Crisco)
» Best if NPO using G-tube
Epilepsy Treatment with Cannabinoid
• Mesopotamia 1800 BC
• In vivo and in vitro anti-seizure activity
• Lack of prospective or RCTs
• Dueling anecdotal & case reports
• Large placebo effect (CO peds cases)
Friedman D et al. NEJM 2015;373:1048
Occupational and Lifestyle
Precautions
• Motor vehicle operation
• Water• Swimming
• Bathing
• Boating
• Heights
• Fire (esp. cooking-related burns)
• Power tools
• Sports
Seizure Recurrence after AED
Withdrawal• Poor prognostic factors
• Abnormal (sleep-deprived) EEG
• Abnormal brain MRI
• Poor control with monotherapy (medically refractory = failure of 2 drugs alone or in combo)
• Genetic etiology
• FHx of seizure disorder» 70% of pre-adolescents (≤12yo) & 60% of adults who are seizure-
free x several years (2-5 yrs, mean 3 yrs) and w/o negative indicators will remain seizure-free off AEDs)
Neurology 1996;47:600
• Risk windows for relapse after AED withdrawal• 75% recur in the first year after withdrawal
• 50% who have a recurrence do so in the first 3 mos
Epileptic Syndromes - Infancy
• Seizures within 24-48 HOL are often indicative of severe cerebral insult
• Benign familial & idiopathic neonatal convulsions• Begin 48-72 HOL and remit by 2-6 mos
• West Syndrome/Infantile Spasm• May be symptomatic (75%), cryptogenic, or idiopathic
• 90% before 12mos, peak 4-6 mos
• Recurrent trunk/limb flexion “salaam seizures”
• Hypsarrhythmia (severely disordered EEG)
• Intellectual impairment, seizure disorder, autism spectrum disorder
Epileptic Syndromes – Infancy
• Febrile Seizures• 5% of kids ages 6mos – 5 yrs
• Simple: <15 min, single occurrence per febrile episode, 75%
• Complex: >15min or multiple times within a febrile episode, 25%
• 2x risk for future epilepsy if complex or symptomatic (about 2-3/100)
• Genetic etiology

Epileptic Syndromes - Childhood
• Lennox-Gastaut syndrome• Poor prognosis
• West syndrome development
• Rolandic epilepsy• Benign childhood epilepsy w/ centrotemporal spikes
• Auto dominant, onset 5-9yo, disappears during adolescence
• Majority occur while asleep or upon awakening
• Control w/monotherapy, if any
• Absence (petit mal) seizures• Onset 4-8yo
• 3Hz spike-and-wave pattern diagnostic
• Good AED response
• Seizures may remit or change character (GTCS, JME)
• Long-term neurobehavioral deficits in 30%
Epileptic Syndromes - Adolescence
• Most common neurological disorder
• Trauma
• Substance abuse
• Juvenile myoclonic epilepsy• Autosomal dominant, incomplete penetrance
• Peak incidence 12-18 yrs
• Complex seizure disorder in most
• Control w/low dose monotherapy
• Lifelong seizure risk

Epileptic Syndromes - Adulthood
• Cryptogenic
• Trauma
• Intracranial mass lesions
• Intracranial vascular lesions (blood is epileptogenic)
• Infections
• Metabolic encephalopathies
• Substance abuse

Pseudoseizures
• Psychogenic nonepileptic seizures
• 20-50% of referrals to tertiary epilepsy centers
• Conversion disorder, rarely factitious
• Typically begin in adolescence but incidence in all ages; 70% female
• Dx by video-EEG monitoring (gold std), provocative techniques, and CPK & prolactin measurement

Status Epilepticus
• Continuous seizures for >1 hour
• Neuronal death: combination of systemic and
CNS- specific factors (intraneuronal calcium)
• Mortality increases with age
• Frequently the initial presentation in children
• Mortality risk is defined by age, etiology, and
ability to achieve control

Sudden Unexpected Death in
Epilepsy (SUDEP)• Defined as SUD with or without evidence of a seizure in
a person without identified status epilepticus or toxicological, traumatic, anatomical cause
• Cardiopulmonary etiologies postulated
• Low incidence in community-based cohort: 0.35-2.7/1000 p-yrsLhatoo SD, et al. Epilepsia 2005;46 s11:36
• Risk factors• Males, age 20-40
• GTC seizures, polytherapy
• Treatment noncompliance
• Alcohol
Hesdorffer DC, et al. Epilepsia 2011;52:1150

Epilepsy-related Mortality
• Japanese population of an epilepsy center (1765); 43 deaths over an 8-year period– Accidents 30% (drowning & head injury)
– SUDEP 23%
– Status epilepticus 16%
– Suicide 14% (all temporal lobe epilepsy)
– Other 16%Fukuchi T, et al. Epilepsy Res 2002;51:233.
• Other community-based studies in Western countries show most of the mortality in accidents and “other” (CNS tumors, vascular disease, pneumonia)Lhatoo SD, et al. Epilepsia 2005;46 s11:36
Mohanraj R, et al. Lancet Neurol
2006;5:481
• 890 newly dx 8/91 => 5/01; f/up until 10/03
• Age-gender match to general population
(Scotland) ; avg age 31
• Overall SMR 1.42 (n=890;d=93)• Tx non-responders SMR 2.54 (n=318; d=42)
• Tx responders SMR 0.95 (n=462;d=41)
• Tx unknown response (n=110;d=10)
• Chronic epilepsy data not shown• Unsuccessful tx w/1-9 meds (median 3)
• Treatment response not recorded
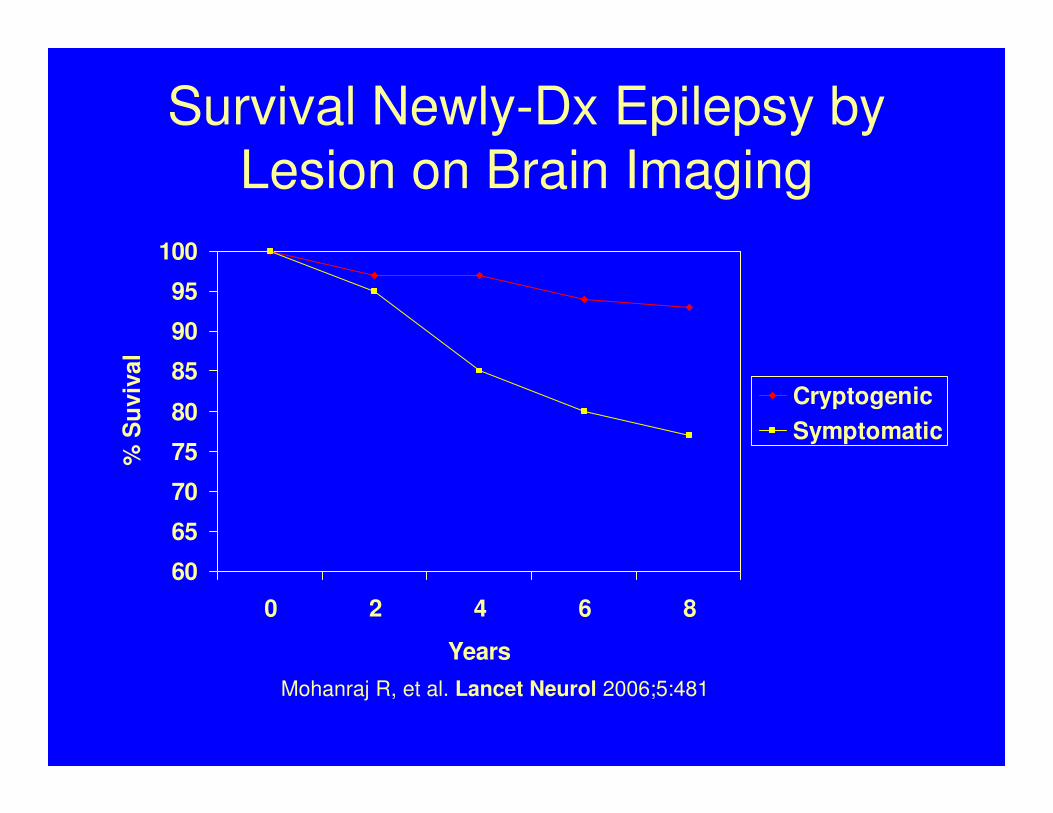
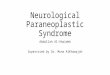
Survival Newly-Dx Epilepsy by
Lesion on Brain Imaging
60
65
70
75
80
85
90
95
100
0 2 4 6 8
Years
% S
uviv
al
Cryptogenic
Symptomatic
Mohanraj R, et al. Lancet Neurol 2006;5:481
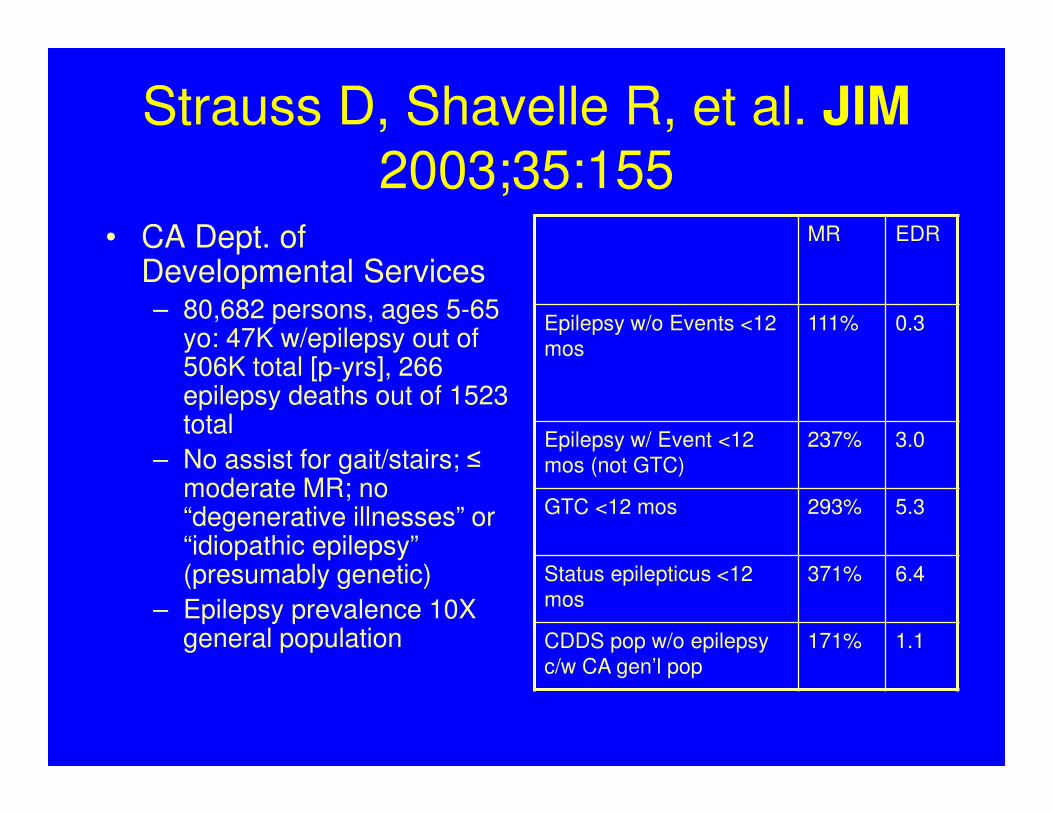
Strauss D, Shavelle R, et al. JIM
2003;35:155• CA Dept. of
Developmental Services– 80,682 persons, ages 5-65
yo: 47K w/epilepsy out of 506K total [p-yrs], 266 epilepsy deaths out of 1523 total
– No assist for gait/stairs; ≤ moderate MR; no “degenerative illnesses” or “idiopathic epilepsy” (presumably genetic)
– Epilepsy prevalence 10X general population
MR EDR
Epilepsy w/o Events <12
mos
111% 0.3
Epilepsy w/ Event <12
mos (not GTC)
237% 3.0
GTC <12 mos 293% 5.3
Status epilepticus <12
mos
371% 6.4
CDDS pop w/o epilepsy
c/w CA gen’l pop
171% 1.1

Approach to Epilepsy Risk
Assessment• Age
• Occupation/Avocation/MVR
• Seizure type• Focal vs. generalized
• Simple vs. complex
• Seizure Control• Frequency
• Number of AEDs in use
• Altered neuroanatomy• Brain injury/depressed skull fx
• Encephalitis
• SDH/AVM
• CVA
Approach to Epilepsy Risk Assessment - Mortality
• Etiology best predictor• Symptomatic > cryptogenic > idiopathic
• Highest risk first 2 years after dx
• Seizure-free status > 12 mos begins the approach to baseline mortality for the studied cohort
Additional resources:
Trinka E et al. Epilepsia 2013;54:495
Nevalainen O et al. Neurology 2014;83:1968
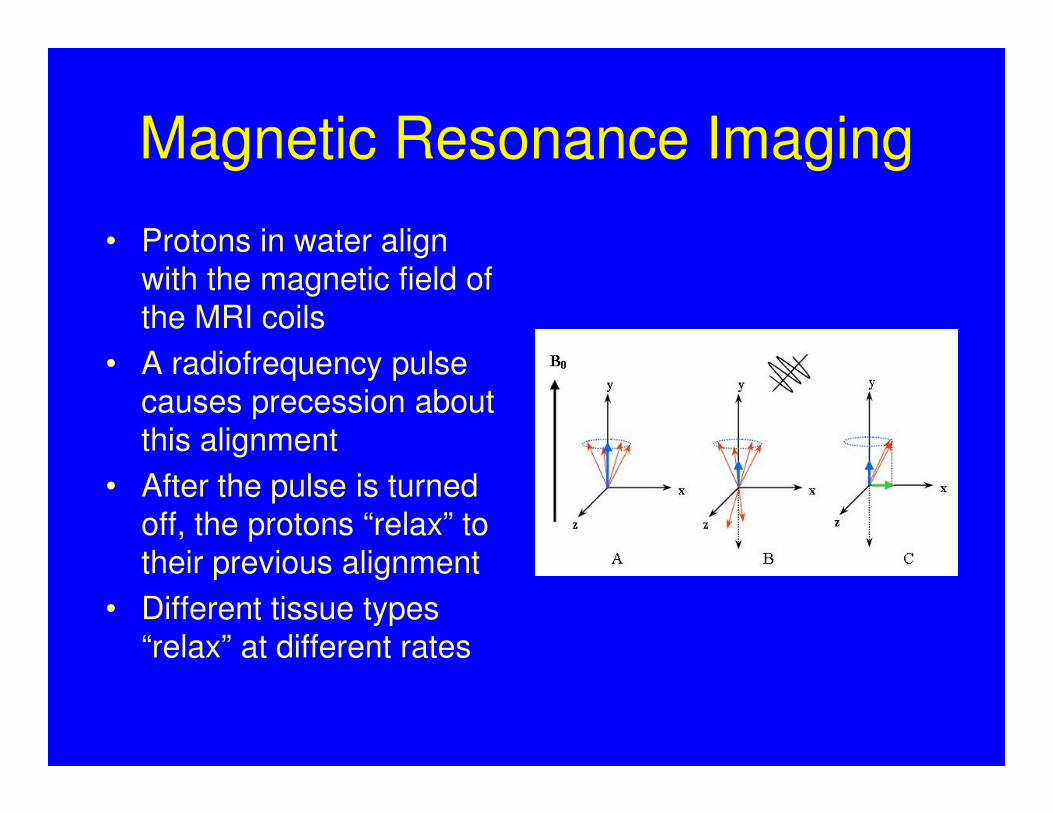
Magnetic Resonance Imaging
• Protons in water align with the magnetic field of the MRI coils
• A radiofrequency pulse causes precession about this alignment
• After the pulse is turned off, the protons “relax” to their previous alignment
• Different tissue types “relax” at different rates

MRI Terminology
• T1 – fat light, H2O dark (blackholes-MS/lacune; white-WMH); used with Gd contrast (active MS plaque)
• T2 – H2O light, fat dark (top right); white-MS plaque, lacune, WMH
• T2 FLAIR – free H2O dark, edema fluid light (bottom right)
• DWI – diffusion-weighted imaging (+) from minutes up to 2 weeks after acute ischemia

What can cause T2 Lesions on MRI?
• Demyelinating Disease
• Infectious illness
• Migraines
• Ischemic disease
• Neurofibromatosis
• Small vascular anomalies
• Unidentified Bright Objects
Multiple Sclerosis
• Lesions separated by space & time– Clinical exam – attack = neuro disturbance ≥
24hrs
– MRI – Gd/T1 or T2
– Lumbar puncture/CSF – oligoclonal IgG bands in CSF
• If suspicion of MS without meeting full criteria → clinically isolated syndrome (CIS)

MS – Signs & Symptoms
• Sensorimotor deficits (many CNS areas)
• Ataxia (parietal lobe/cerebellum/brainstem)
• Neurogenic bladder (multiple CNS areas)
• Internuclear ophthalmoplegia (abbrev. INO; brainstem)
• Facial pain/tic douloureux/trigeminal neuralgia (brainstem; trigeminal nerve)
• Lhermitte sign (cervical spinal cord)
• Cognitive impairment (50% eventually; diffuse cerebral disease)
• Optic neuritis (20% initial sx; optic nerve)

MS – Clinical Subtypes

MS Treatment
• Steroids• Interferon (IFN)– beta-1a (2 preps, A & R), beta-1b
(B)• Other Immune Modulator – glatiramer acetate (C)• Lymphocyte effects
– fingolimod (G)– teriflunomide (A)– Alemtuzumab (L)
• ?mechanism – BG-12• Monoclonal Antibody – natalizumab (T)• Immunosuppressive Agent – mitoxantrone
What Is the Impact of MS on Mortality?
• Uncommon disease(s) + variable clinical course + expect decades of life after onset = need for large cohort followed for many years to estimate and categorize risk
• Danish study Onset 1948-86 122,373 p-yr
MS + CIS gen’l pop controls
– SMR from onset = 3.25
– EDR from onset = 13.0/1000 p-yr
– Median survival time from onset = 30 yrs
– Median survival time from diagnosis = 25 yrs(Brønnum-Hansen. Neurology. 1994;44:1901)
(Pokorski RJ. JIM. 1997;29:100)
Underwriting MS – Forks in the Road
• Diagnosis
Indefinite Definite
CIS/ON Early Stage Late Stage

MS – Unfavorable Prognosis =
High Risk
• Immobility- think paralysis or quadriplegia
• Primary or secondary progression
• Brain atrophy & cognitive decline
• Multiple black holes on MRI
• Renal function
• Suicide/MDD/substance abuse
• “novel therapy”• Bee stings, cobra venom, pregnant cow milk
• Chronic cerebrospinal venous insufficiency (CCSVI)

MS – Favorable Prognosis = Better Risk
• ♀ (higher prevalence; better outcomes)
• Younger age @ onset (pivot = 40yo)*
• Low relapse rate in early disease (first 2 years)*
• Complete recovery after relapse*
• Sensory/CN/ON as initial sx (motor/cerebellar worse px as initial sx)*
• Lower lesion burden & accretion by MRI*
• EDSS = 0-3, 5 yrs after dx
• Response to disease-modifying MS drugs
(*early stage prognostic factors > Scott. Neurology2000;55:689.)

Kurtzke Expanded Disability Status Scale
• 10 point scale ranging from no disability (0.0) to death (10.0)
• “Functional systems” used for scores < 4.0
• “Cerebral” = cognition & mood
• Emphasizes ambulation
• Key breakpoints
– 3.0 moderate disability, fully ambulatory
– 6.0 at least unilateral ambulatory assist
– 7.0 wheelchair-dept; indept transfers
Generally, disability correlates with risk(Kurtzke. Neurology. 1983;33:1444.)
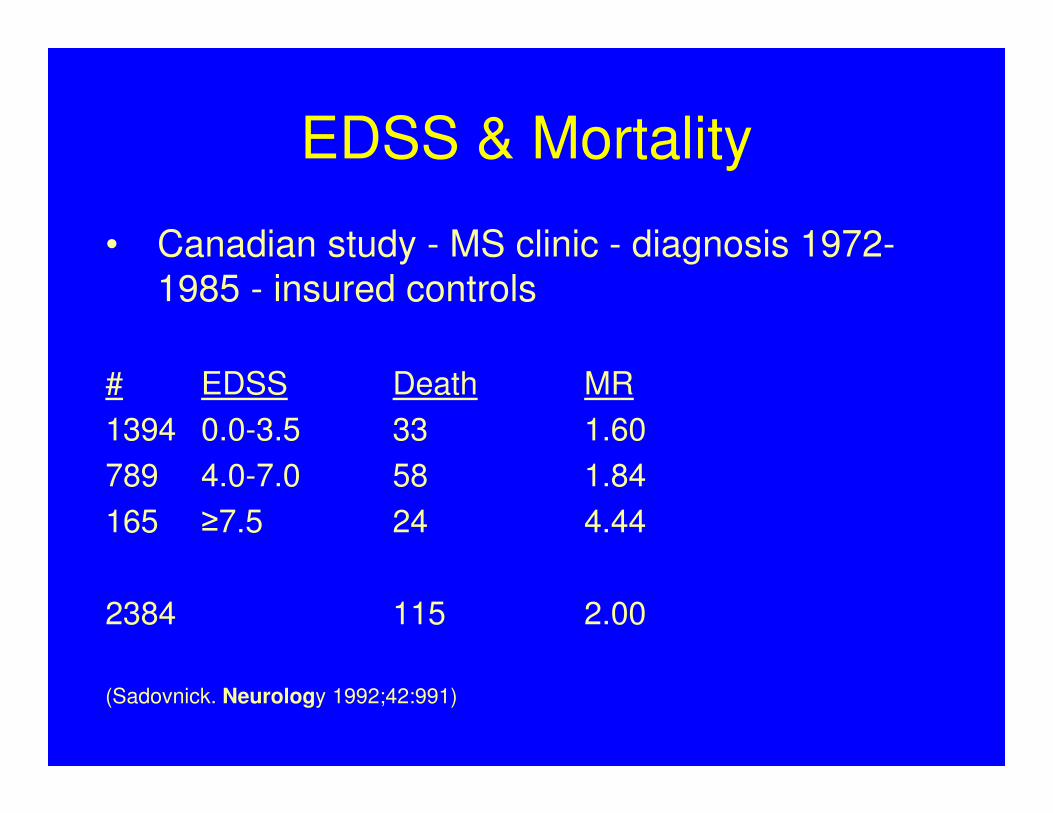
EDSS & Mortality
• Canadian study - MS clinic - diagnosis 1972-
1985 - insured controls
# EDSS Death MR
1394 0.0-3.5 33 1.60
789 4.0-7.0 58 1.84
165 ≥7.5 24 4.44
2384 115 2.00
(Sadovnick. Neurology 1992;42:991)
ABCR Drugs – Positive Factors
• In the short-term, they have been shown to reduce relapse-related EDSS progression; frequency of relapses; and MRI characteristics of inflammation
• IFNβ1a vs. placebo in delaying CDMS after CIS w/+MRI: CHAMPS trial RR=0.56 p=0.002 (Jacobs. NEJM 2000;343:898)
• IFNβ1b also delays CDMS after CIS: BENEFIT trial 8-yr extension RR 0.68 p=0.003 (Edan G. J Neurol Neurosurg Psychiatry
2014;85:1183)
• For risk assessment purposes, ABCR drugs are equivalent
Loredana LM. J Neurol Neurosurg Psychiatry 2015;86:1016.
(IFN 1b vs. glatiramer)

IFN Reduces RRMS => SPMS Progression
Trojano M. Ann Neurol 2007;61:300.
• Observational, non-randomized study, median f/u 5.7 yrs (up to 7 yrs)
• 1103 treated
• 401 untreated (refused; contraindicated; early drug d/c; no relapses in 2yrs & EDSS<3)
• Various ABR drugs
• End points: Secondary progressive dz; stable EDSS 4 or 6
SP EDSS 4 EDSS 6
HR-progression from first visit to end point
0.38
p<0.0001
0.70
p=0.0174
0.60
p=0.0304

Shirani A, et al. JAMA 2012;308(3):247Derfuss T, et al. JAMA 2012;308(3):290
• Well designed observational study failed to show IFN reduced disability progression over a long term (>5yrs)– IFN-treatment group– 2 untreated groups
• Contemporary untreated• Historical untreated
• Caveats– Bias against tx of benign disease– Underpowered
• IFN reduction in long-term disability, “although plausible, remains unproven”

Kerbat A. Eur J Neurol 2014;22:507
• Prospective, population-based cohort CIS dx 2000 – 2001 followed 10yrs
• End pts DSS 3 & 6
• @10yrs, 244 pts: 70% to RRMS; 80% txDMDs
• EDSS 3 16%; EDSS 6 6%; EDSS<3 78%
studies in in the pre-DMD era: 50% range for progression to EDSS 3

ABCR Caveats
• Need 6-12 months to determine efficacy• Barriers to Use
– Injection-site reactions– Depression– Flu-symptoms– Fatigue– Headache
• Adherence to therapy– Adherence = acceptance + persistence + compliance– 60-75% adhere for 2-5 yr (IFN)– Adherence rates similar to insulin for type 2 diabetes– Majority who discontinue do so in the first 2 yrs (ABCR)– Other studies show first 6 mos indicative of persistence
(Costello. Medscape J Med. 2008;10:225)
(Tremlett HL. Neurology. 2003;61:551)
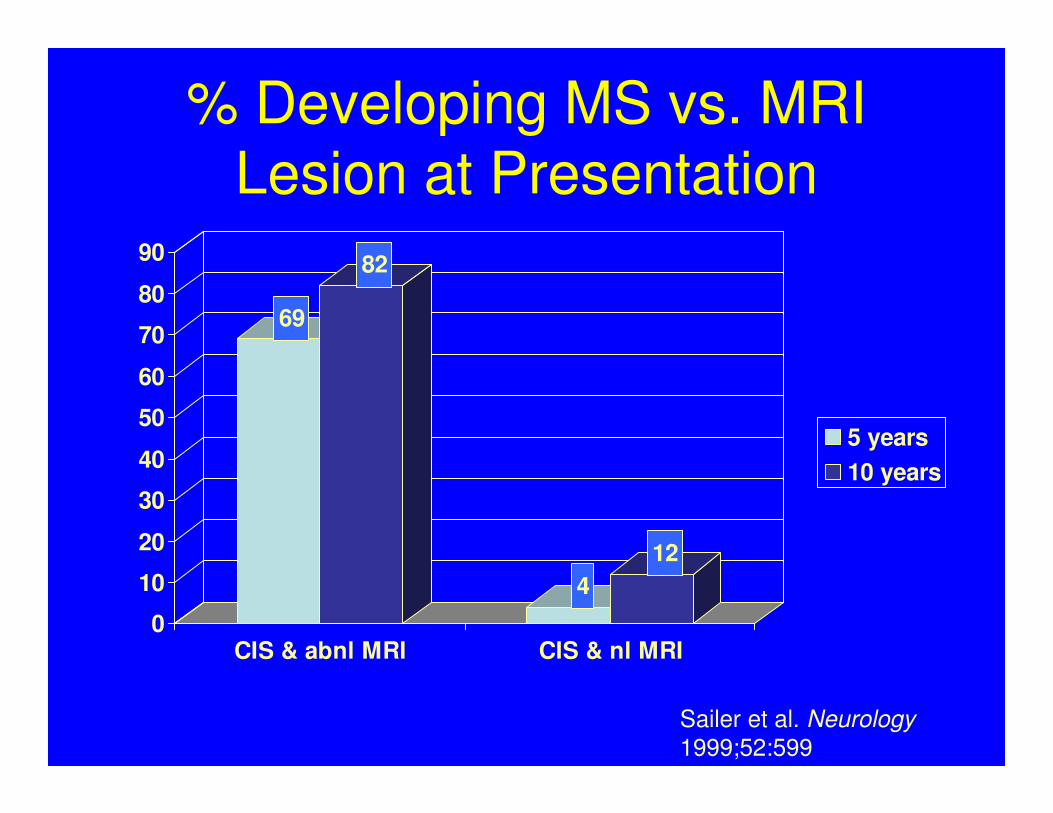
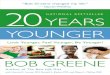
% Developing MS vs. MRI Lesion at Presentation
69
82
4
12
0
10
20
30
40
50
60
70
80
90
CIS & abnl MRI CIS & nl MRI
5 years
10 years
Sailer et al. Neurology
1999;52:599
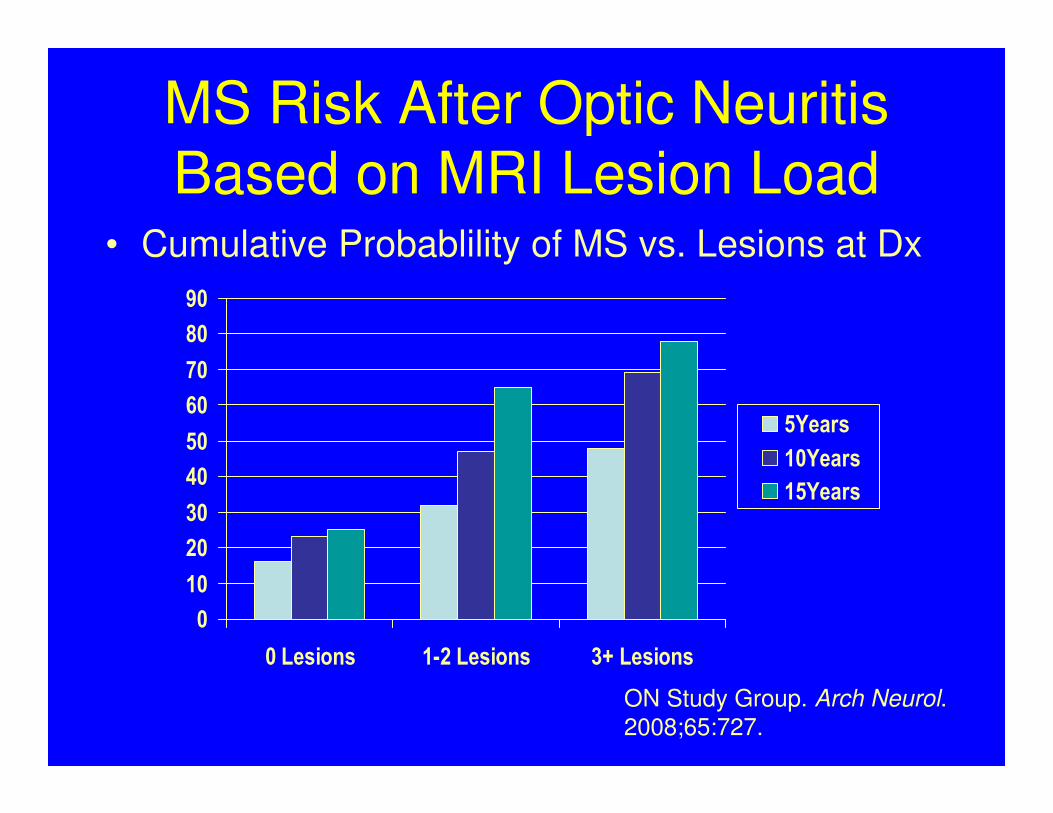
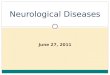
MS Risk After Optic Neuritis Based on MRI Lesion Load
• Cumulative Probablility of MS vs. Lesions at Dx
0
10
20
30
40
50
60
70
80
90
0 Lesions 1-2 Lesions 3+ Lesions
5Years
10Years
15Years
ON Study Group. Arch Neurol. 2008;65:727.

MS Risk After Optic Neuritis Based on MRI Lesion Load
• Conditional Probablility of MS vs. Lesions at Dx
0
5
10
15
20
25
30
35
40
45
0 lesions 1+ lesions
0-5Years
6-10Years
11-15Years
ON Study Group. Arch Neurol. 2008;65:727.
Approach to MS Risk Assessment
• MRI
• Lesion burden & accretion
• Black holes
• Relapse rate
• Frequency
• Proximity to pre-lapse baseline
• Clinical subtype
• EDSS – 3 & 6 are important scores
• Disease-modifying therapy
• Response to treatment
• Medication choice
• Markers of high risk

Case Presentation
Epilepsy

Case #1
• 34 yo male applies for coverage with a clean-sheeted Part 2.
As part of your age/amount requirements, a prescription
database check shows ongoing carbamazepine scrips. The
underwriting file documents that he was born in El Salvador.
• The underwriting file contains a PCP APS. Only “seizure
disorder” is listed as a diagnosis. The PCP prescribes the
client’s AED and follows the levels.
• The APS contains an MRI +/- Gd dated 6 years prior to the
date on the Part 2. It shows a single, non-enhancing T2
hyperintensity at the parieto-occipital grey-white junction;
ventricle size is nl
• Given what you know, what is a likely cause of his seizure
disorder?

Case #1Neurocystercercosis
• Ingestion of eggs of Taenia solium
• Epilepsy most common of a variety of neurological signs & symptoms
• Calcification = epileptogenic focus
• Seizures improved with anti-parasitic tx and usually controlled with monotherapy
• No guidelines on duration of AED tx

Case #2
• 34yo male applicant seeks life coverage with waiver of
premium. On the Part 2, he mentions TBI with hospitalization
3 yrs PTA. No other medical hx is noted. He is on no meds.
• You obtain an APS in which you learn he was the sole
occupant of a car which collided with a tree on an icy road.
Tox screen neg & BAL 0. ED intake notes parameds found
him slumped over the now deflated airbag, unresponsive and
“twitching”. He was loaded with phenytoin and intubated.
• Imaging showed few scattered punctate hemorrhages but no
SDHs, cerebral contusions or skull fractures. He completed
his acute hospitalization and post-acute rehab within 3mos
after injury and was transitioned back to full-time work.

History is as stated and…..
• …..there are no documented seizures after those observed in
the field. EEG done during rehab showed no irritable foci. You
note that the phenytoin was discontinued after the first week
of acute hospitalization.
– How do you view the seizure risk now? • Life?
• DI?
– What if you learn his occupation is self-employed “house painter”; does
that change your risk assessment re: seizures?• Life?
• DI?

History is as stated and…..
• …..since the accident, although independent for all
compulsory & instrumental ADLs, he has been unable to fully
transition back to work. He is under the care of a psychiatrist
and a neurologist, the latter continues to prescribe an AED.
The client is seizure-free on the AED though video-EEG
monitoring off AED demonstrates dissociation between brain
and spontaneous motor activities. What is the nature of the
risk now?

Case Presentation
Multiple Sclerosis
Case
• 29yo female applicant, lifelong North Dakota resident, seeks
life coverage. No medical hx is provided on the app but an
APS is an age/amount requirement. Per Part 1 she is an oil
futures trader.
• The APS notes a visit to her PCP for headaches and ill-
defined visual changes beginning about 4 yrs ago. A cursory
neuro exam is “nonfocal” and she is sent for an MRI. The
latter is done without contrast and shows several T2 lesions.
The APS notes absences from work for undefined periods but
she remains employed full-time to the best of your knowledge.

History is as stated and…..
• …..you have no neurology evaluation but multiple PCP evals
up to the last several weeks. Subsequent notes have a dx of
migraine with aura. Her visual sx are scintillating lights. Her
work absences were a day here and there when her
migraines got bad but since starting a triptan she has not
missed any more time. Her complaints and neuro exam raise
no red flags.
• How would you classify the risk?• Life?
• DI?
History is as stated and…..
• …..she has indeed been seen by a neurologist with ongoing
follow-up. The headaches are infrequent and do not have a
vascular quality. Her visual sx are actually spotty loss in OS
vision. Ophthalmic exam showed inflammation of her left optic
disc. A subsequent MRI with contrast showed no other lesions
apart from the left optic nerve. The remainder of her neuro
exams are unremarkable. She has had no further recurrence
but continues to experience the OS defect.
• How would you classify the risk of developing MS in the
future?

History is as stated and…..
• ….. she is seeing a neurologist and has ongoing follow-up. The headaches are infrequent and do not have a vascular quality. She currently demonstrates mild spasticity in the form of hyperreflexia; an upgoing left toe; nl sensory and cerebellar exam; intact CNs except for her left ON; and gait with subtle slowing of swing phase on the left as c/w the right.
• How would you classify the EDSS?
• What factors influence or modify the risk?

14 October 2015©
CRN000000-000000
Massachusetts Mutual Life Insurance Company, Springfield, MA 01111-0001. All rights reserved.
www.massmutual.com. MassMutual Financial Group is a marketing name for Massachusetts Mutual Life Insurance
Company (MassMutual) and its affiliated companies and sales representatives.
X000 000