Embed Size (px)
Citation preview

1482 THE JOURNAL OF BONE AND JOINT SURGERY
Neurological deficit after surgical enucleation of schwannomas of the upper limb
M. J. Park, K. N. Seo, H. J. Kang
From Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
M. J. Park, MD, PhD, Professor
H. J. Kang, MD, Clinical FellowDepartment of Orthopaedic SurgerySamsung Medical Center, Sungkyunkwan University School of Medicine, 50 Irwon-dong, Gangnam-gu, Seoul 135-710, Korea.
K. N. Seo, MD, Orthopaedic SurgeonIncheon Sarang Hospital, 144-2 Juan-dong, Nam-gu, Incheon 402-835, Korea.
Correspondence should be sent to Professor M. J. Park; e-mail: [email protected]
©2009 British Editorial Society of Bone and Joint Surgerydoi:10.1302/0301-620X.91B11.22519 $2.00
J Bone Joint Surg [Br] 2009;91-B:1482-6.Received 2 March 2009; Accepted after revision 9 June 2009
We evaluated 56 patients for neurological deficit after enucleation of a histopathologically confirmed schwannoma of the upper limb. Immediately after the operation, 41 patients (73.2%) had developed a new neurological deficit: ten of these had a major deficit such as severe motor or sensory loss, or intolerable neuropathic pain. The mean tumour size had been significantly larger in patients with a major neurological deficit than in those with a minor or no deficit. After a mean 25.4 months (12 to 85), 39 patients (70%) had no residual neurological deficit, and the other 17 (30%) had only hypoaesthesia, paraesthesiae or mild motor weakness.
This study suggests that a schwannoma in the upper limb can be removed with an acceptable risk of injury to the nerve, although a transient neurological deficit occurs regularly after the operation. Biopsy is not advised. Patients should be informed pre-operatively about the possibility of damage to the nerve: meticulous dissection is required to minimise this.
A schwannoma is a benign peripheral nervesheath tumour consisting of Schwann cells. It isusually solitary but multiple tumours in a limbhave been reported.1 Overall, 19% of schwan-nomas are found in the upper limb,2 wherethey comprise 5% of all soft-tissue tumours.3
They usually grow slowly and present as apainless swelling for several years withoutspecific symptoms. They are frequently mis-diagnosed as a benign solitary mass such as aganglion, fibroma or myxoma.4
A schwannoma is well encapsulated andeventually displaces the fascicles of the nerve,whereas a neurofibroma envelops them. Forthis reason, it is generally believed that aschwannoma can easily be enucleated from thenerve without producing a neurological deficit.However, even with meticulous dissection,removal of a tumour without damaging anyfascicles can be technically difficult, andincreases the risk of transient or permamentneurological damage. The threshold for iatro-genic injury during surgical dissection of aperipheral nerve tends to be lower in the upperlimb than in the trunk or lower limbs. Even aminor neurological deficit in the upper limb israpidly identified by the patient. The purposeof this study was to evaluate any temporary orpermanent neurological deficit after enucle-ation of a histopathologically confirmedschwannoma of the upper limb.
Patients and MethodsWe identified 56 patients who had undergoneenucleation of a schwannoma of the upper limbbetween June 1996 and December 2007. Therewere 30 males and 26 females, with a mean ageof 43.9 years (17 to 72). We included only histo-pathologically confirmed schwannomas of thebrachial plexus and peripheral nerves of theupper limb. Those that originated from cutane-ous nerves or unidentified branches wereexcluded, but we included schwannomas of thedigital nerve in the hand. Patients who hadundergone previous surgery or open biopsywere excluded. Multiple schwannomas presentin the brachial plexus or one peripheral nervewere included, but patients who had schwan-nomas in multiple nerve sites were not includedbecause of difficulty in interpreting the source ofthe neurological deficit. There was no case ofplexiform schwannoma.
There were 14 schwannomas of the brachialplexus, 13 of the ulnar nerve, 24 of the mediannerve, and five of the radial nerve. The loca-tions and distributions of these tumours aresummarised in Table I. The interval betweendetection and excision was a mean of 6.1 years(0.3 to 20). Spontaneous pain occurred in threepatients. Paraesthesiae or hypoaesthesia of theskin innervated by the affected nerve was pres-ent in 38 patients, and motor weakness inthree.

NEUROLOGICAL DEFICIT AFTER SURGICAL ENUCLEATION OF SCHWANNOMAS OF THE UPPER LIMB 1483
VOL. 91-B, No. 11, NOVEMBER 2009
At their initial presentation, each patient had a palpablemass with a positive Tinel’s sign. A peripheral nerve sheathtumour was diagnosed clinically when a mass in the line ofa nerve was accompanied by a positive Tinel’s sign andmotor or sensory loss in the distribution of that nerve. AnMRI was performed in 22 patients, and an ultrasound in20. Each MRI correctly diagnosed a peripheral nervesheath tumour, but ultrasound suggested a ganglion orgiant cell tumour of tendon sheath on four occasions.
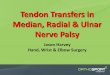
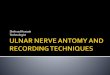
Although we did not perform a biopsy because of the riskof iatrogenic injury and its adverse effect on subsequentenucleation, 13 patients had undergone a fine needle aspi-ration biopsy in other departments of our hospital or inother hospitals. The diagnosis was confirmed in only sixpatients and was inconclusive in the rest.Surgical technique. Each operation was performed by ahand surgeon under loupe magnification using a microsurgi-cal technique. Skin incisions were longitudinal except fortumours of the brachial plexus, which were approachedthrough a transverse supraclavicular incision. First, weexposed the tumour and the nerve above and below it. Theusual finding was that of a tumour arising within the sub-stance of the nerve, with uninvolved fascicles splayed over itssurface (Fig. 1a). We carefully made a longitudinal incision inthe epineurium between the fascicles and dissected theonion-skin-like epineurial layers until the shiny surface of thetumour was exposed (Fig. 1b). Gentle dissection along theplane of the tumour capsule from the epineurial layers usu-ally allowed the tumour to be shelled out in one piece with-out disturbing the nerve fascicles (Fig. 1c). However, smallfascicles entering either the capsule or the substance of thetumour were sometimes found as we approached the proxi-mal and distal poles. We tried to isolate these fascicles tominimise the risk of damage to the nerve, but it was fre-quently impossible and on occasion we had to divide some ofthe fascicles, particularly when they entered the substance ofthe tumour. We did not carry out intra-operative nerve con-duction studies to identify non-functioning fascicles.
The mean maximum diameter of the tumours was 2.4 cm(0.7 to 7).Evaluation of neurological deficit. The ‘immediate’ post-operative neurological status of each patient was evaluatedwithin five days when they were discharged from hospitalor attended their first outpatient appointment. They wereasked if they had any neurological symptoms such as pain,paraesthesiae or weakness, and were examined.
Any new symptom was recorded and classified as amajor or minor neurological deficit. Major deficitsincluded anaesthesia or marked hypoaesthesia, motorweakness of grade 3 or less according to the MedicalResearch Council muscle strength grading system5 andneuropathic pain. Patients with neuropathic pain weretreated with nerve blocks as well analgesics, including opi-ates. Minor deficits indicated tolerable symptoms such asmild hypoaesthesia, paraesthesiae, and mild motor weak-ness (grade 4).
All patients who had major deficits after the operationwere subsequently re-examined to assess their final neuro-logical status. Those with minor subjective changes were usu-ally contacted by telephone and asked if they had anyremaining deficit. The mean follow-up was 25.4 months(12 to 85).
We used Student’s t-test to identify significant factorsrelated to the development of an ‘immediate’ major post-operative neurological deficit. The patient’s age, durationof symptoms and maximum diameter of the tumour werecompared between patients with major deficits and thosewho had minor or no deficits. The level of significance wasset at p < 0.05.
ResultsTen patients had a major neurological deficit immediatelyafter surgery. There were seven with a motor palsy or severeweakness, one with marked sensory loss, and two withsevere neuropathic pain. Three patients with a schwan-noma of the brachial plexus developed an incomplete nervepalsy, and one with a schwannoma of the deep branch ofthe ulnar nerve had increased weakness and definite claw-ing. Three patients developed a radial nerve palsy that lim-ited finger extension. One patient developed sensoryimpairment of the thumb, index and middle fingers afterexcision of a schwannoma of the median nerve in the fore-arm. Two patients developed neuropathic pain withhypoathesia and weakness after excision of a schwannomafrom the brachial plexus.
Of the seven patients with severe motor weakness, sixrecovered to some extent between three weeks and sixmonths post-operatively, with restoration of muscle powerto grade 4 or more at final follow-up. However, a 27-year-old woman with a schwannoma of the deep radial nerve inthe radial tunnel developed a complete palsy and showedno evidence of recovery one year later. A sural nerve graftwas performed, which resulted in motor recovery to grade4 at final follow-up. One patient with a sensory deficitrecovered gradually but had some persistent paraesthesiaeat final follow-up. Two patients who had neuropathic painrecovered after analgesics and a nerve block within fourweeks of their operation, but some tingling persisted.
Of those with minor defects, 31 patients, who had nosubjective symptoms or mild paraesthesiae pre-operatively,developed hypoaesthesia or paraesthesiae, post-operatively.Mild motor weakness with sensory impairment was noted
Table I. Location and distribution of 56 schwannomas of the upperlimb
Nerve Arm Forearm Hand Number
Brachial plexus 14Ulnar nerve 4 4 5 13Median nerve 6 4 14 24Radial nerve 4 1 5

GNAK.J.H ,OES.N.K ,KRAP.J.M4841
THE JOURNAL OF BONE AND JOINT SURGERY
in three patients with schwannomas of the ulnar nerve inthe forearm, the median nerve in the palm, and the mediannerve at the wrist, respectively. Although the sensory ormotor change was recognised immediately after surgery,their symptoms were tolerable and further treatment wasnot required. Of these, 24 recovered completely withinthree months, but seven had persistent paraesthesiae atfinal follow-up. Nine patients who had pain or paraesthe-siae pre-operatively improved after their operation.
Overall, 41 patients (73.2%) developed a new major orminor neurological deficit or an exacerbation of their pre-operative neurological symptoms immediately after the oper-ation. At the final follow-up, 39 patients (70.0%) showed noresidual neurological deficit, and the remaining 17, includingone who required a nerve graft, had hypoaesthesia, paraes-
thesiae, or mild motor weakness. None of these complica-tions limited the daily activities of these patients. Norecurrence of tumour was seen during the follow-up period.
When the age, duration of symptoms and maximumdiameter of the tumour were considered, the mean diameterof the tumour was significantly greater in those with amajor neurological defect than in those without (p = 0.01).Age and duration of symptoms did not appear to affect theoutcome significantly.
DiscussionSchwannomas are rare tumours. In contrast to a neuro-fibroma, in which intraneural dissection with maintenance ofnerve continuity is impossible because the fascicles are embed-ded in the tumour, the schwannoma is well encapsulated, with
Fig. 1c
Photographs showing the enucleation of a schwannoma from the median nerve at the elbow. a) A schwannoma is seen inside the epineurial layer.b) The onion-skin-like epineurial layers are gently dissected off until the shiny surface of the tumor is exposed. c) The entire tumour mass is shelledout in one piece, without damage to the nerve fascicles. The tumour is more vascular than it appears, because it was enucleated under tourniquet.
Fig. 1a Fig. 1b

NEUROLOGICAL DEFICIT AFTER SURGICAL ENUCLEATION OF SCHWANNOMAS OF THE UPPER LIMB 1485
VOL. 91-B, No. 11, NOVEMBER 2009
the fascicles of the nerve spread over its surface. This wouldsuggest that a schwannoma can be removed without damageto the underlying nerve fascicles. However, our study showsthat an immediate neurological deficit was seen in 75% ofpatients, which suggests a high incidence of iatrogenic nerveinjury during dissection. Although only ten patients devel-oped a major neurological deficit, even a minor sensory ormotor deficit was easily perceived by the patient.
It is essential to make the correct clinical diagnosis ofschwannoma pre-operatively. Although pre-operative neuro-logical impairment is rare, we found that Tinel’s sign hadbeen elicited in all patients, suggesting that it is the singlemost useful sign in making the correct diagnosis. Althoughthe diagnosis of a soft-tissue tumour is usually confirmed byopen biopsy, we do not recommend this when a peripheralnerve sheath tumour is suspected. It should be rememberedthat open biopsy risks iatrogenic nerve injury, sometimesresulting in a permament neurological deficit, and leaves ascar that may interfere with the meticulous dissectionrequired for enucleation. If necessary, instead of open biopsy,fine needle biopsy can be performed with a lesser risk ofnerve injury. Our study included 13 patients who had under-gone needle biopsy before operation. Only six of these con-firmed the diagnosis, which demonstrates its limitation as adiagnostic tool. After definitive enucleation of the schwan-noma in these 13 patients, four had a major deficit, sevenhad paraesthesiae and only two showed an improvement ontheir pre-operative symptoms. Although a needle biopsyseems less invasive, we are concerned that it might increasethe risk of nerve injury during surgical enucleation. Conse-quently, we no longer perform needle biopsy. MRI is mosthelpful in confirming the diagnosis pre-operatively, andultrasound may be of use.6
The technique of removal or enucleation of the schwan-noma has been described by several authors.7-10 Somerecommend extracapsular excision and have reported goodresults,11,12 but it would seem possible to damage the fasci-cles in the capsular layer during dissection. We advocateintra-capsular enucleation to minimise the risk of injury.We believe that gentle dissection of the epineurial layerdown to the shiny surface of the tumour is essential toallow the tumour mass to be shelled out safely while pre-serving the fascicles within the layers. Great attention mustbe paid when the dissection approaches the proximal anddistal poles of the tumour, because small fascicles that can-not be separated from the tumour are frequently present. Itis necessary to check whether there is a further layerbeneath the plane of dissection. If so, this should be peeledoff before shelling out the tumour. In some cases, despitemeticulous dissection, we found one or more fasciclesentering and leaving the substance of the tumour at its pole.We tried to isolate these small fascicles, but this was almostalways unsuccessful because the fascicles became attentu-ated as we traced them into the tumour. Donner et al12
stimulated the fascicles entering the tumour substance andreported that their division did not usually lead to an
increased neurological deficit because they were usuallynon-functional. However, the high incidence of immediateneurological deficit in this study suggests that their conclu-sion is incorrect. We believe that the transection of fasciclesthat run through the tumour is the cause of major post-operative neurological deficit. Oberle et al9 reported thatpost-operative neurological deficits occur mostly inpatients with large tumours or long-standing symptoms.We observed that larger tumours tended to have more fas-cicles entering the tumour substance and were at greaterrisk of major neurological deficit after surgery. On the basisthat a larger schwannoma is associated with a higher risk offascicular injury during dissection, we strongly recommendearly surgical enucleation when a schwannoma is found inthe upper limb. Sawada et al13 has suggested that a schwan-noma arising in the brachial plexus or in the proximal partof the upper arm may be at a higher risk of injury duringsurgery. We found no association between tumour locationand post-operative neurological deficit.
Despite the high incidence of immediate neurologicaldeficits, most tended to resolve with time. About one-thirdof the patients still had hypoaesthesia, paraesthesiae, ormild motor weakness, but most were not really trouble-some and did not affect activities of daily living. Our finalresults are comparable with those reported by otherauthors.10,12 Knight, Birch and Pringle14 reported that sig-nificant complications occurred in only five of 198 patientswith a schwannoma. Artico et al11 reported that motorstrength was reduced in five of 73 patients, including16 who needed a nerve graft, mainly due to damage fromprevious operations.
Our study shows that a schwannoma in the upper limbcan be removed with an acceptable risk of injury to thenerve, but with a high incidence of immediate neurologicaldeficit. The correct clinical diagnosis of a schwannomashould be made pre-operatively so that the patient may beinformed of potential neurological problems. Biopsy of thenerve should be avoided.
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.
References1. Phalen GS. Neurilemmomas of the forearm and hand. Clin Orthop 1976;114:219-22.
2. Das Gupta TK, Brasfield RD, Strong EW, Hajdu SI. Benign solitary schwannomas(neurilemomas). Cancer 1969;24:355-66.
3. Strickland JW, Steichen JB. Nerve tumours of the hand and forearm. J Hand Surg[Am] 1977;2:285-91.
4. Rockwell GM, Thoma A, Salama S. Schwannoma of the hand and wrist. PlastReconstr Surg 2003;111:1227-32.
5. James MA. Use of the Medical Research Council muscle strength grading system inthe upper extremity. J Hand Surg Am 2007;32:154-6.
6. Nawabi DH, Sinisi M. Schwannoma of the posterior tibial nerve: the problem ofdelay in diagnosis. J Bone Joint Surg [Br] 2007;89-B:814-16.
7. Kim DH, Murovic JA, Tiel RL, Moes G, Kline DG. A series of 397 peripheral neuralsheath tumors: 30-year experience at Louisiana State University Health SciencesCenter. J Neurosurg 2005;102:246-55.
8. Ozdemir O, Ozsoy MH, Kurt C, Coskunol E, Calli I. Schwannomas of the hand andwrist: long-term results and review of the literature. J Orthop Surg (Hong Kong)2005;13:267-72.

1486 M. J. PARK, K. N. SEO, H. J. KANG
THE JOURNAL OF BONE AND JOINT SURGERY
9. Oberle J, Kahamba J, Richter HP. Peripheral nerve schwannomas: an analysis of16 patients. Acta Neurochir 1997;139:949-53.
10. Kang HJ, Shin SJ, Kang ES. Schwannomas of the upper extremity. J Hand Surg [Br]2000;25:604-7.
11. Artico M, Cervoni L, Wierzbicki V, D’Andrea V, Nucci F. Benign neural sheathtumours of major nerves: characteristics in 119 surgical cases. Acta Neurochir1997;139:1108-16.
12. Donner TR, Voorhies RM, Kline DG. Neural sheath tumors of major nerves. J Neu-rosurg 1994;81:362-73.
13. Sawada T, Sano M, Ogihara H, et al. The relationship between pre-operativesymptoms, operative findings and postoperative complications in schwannomas. JHand Surg [Br] 2006;31:629-34.
14. Knight DM, Birch R, Pringle J. Benign solitary schwannomas: a review of 234cases. J Bone Joint Surg [Br] 2007;89-B:382-7.