-
Brain (1999), 122, 21832194
Neurological complications in Behcets syndromeD. Kidd,1 A
Steuer,2,3 A. M. Denman2,3 and P. Rudge1
1The National Hospital for Neurology and Neurosurgery,
Correspondence to: Dr Desmond Kidd, Department ofLondon and the
Departments of 2Immunology and Clinical Neurosciences, Royal Free
Hospital, Pond Street,3Rheumatology, Northwick Park Hospital,
Harrow, UK London NW3 2QG, UK
E-mail: [email protected]
SummaryThe neurological complications of Behcets syndrome have
good, and the majority of those followed-up over a median
of 3 years (range 119 years) had only single attacks.not been
characterized with clarity. We present the clinicalfeatures,
imaging characteristics and CSF findings of a One-third of patients
underwent further attacks, and four
underwent progressive deterioration leading to disability.series
of 50 patients seen at the National Hospital forNeurology and
Neurosurgery over the past 10 years. In Factors suggesting a poor
prognosis are repeated attacks,
incomplete recovery, progressive disease course and athis
series, vascular complications had a low prevalence,whereas
involvement of the brainstem was common; high level of CSF
leucocytosis during acute attack. These
data should be of help in the further definition of thespinal
cord lesions, hemisphere lesions and meningo-encephalitis also
occurred. Optic neuropathy, vestibulo- clinical characteristics of
this rare neurological disorder
and in the planning of treatment trials.cochlear and peripheral
nerve involvement occurred, butwere rare. The prognosis for
recovery was in general
Keywords: neurological diseases; Behcets syndrome; MRI; CSF
IntroductionBehcets syndrome is an episodic disorder of unknown
were sufficiently high have suggested a prevalence of 5.3%
in Istanbul (Serdaroglu et al., 1989), 16% in
Casablancaaetiology or pathogenesis, characterized by recurrent
oral andgenital ulceration and panuveitis. Constitutional
disturbance is (Benamour et al., 1990), 25% in Alexandria
(Assaad-Khalil
et al., 1993) and 3.3% in a nationwide survey in Irancommon, and
there is malaise, fatigue and loss of weight. Skininvolvement,
characterized by erythema nodosum, pustular (Davitchi et al.,
1997). In an autopsy series, 20% of 170
cases of patients with Behcets syndrome showed
pathologicaleruptions or pseudofolliculitis, is also common, and
there isan oligoarthropathy of large joints such as the knees,
ankles evidence for neurological involvement (Lakhanpal et al.,
1985).and shoulders. Involvement of the lungs, gastrointestinal
tractand kidneys has also been noted, but is rare (ODuffy,
1994).
DiagnosisThe diagnostic criteria are summarized in Table
1Epidemiology
Behcets syndrome is most common in the countries around
(International Study Group for Behcets Disease, 1990).These are
based on a cohort of 914 patients from severalthe eastern shores of
the Mediterranean, the Middle East and
Eastern Asia, particularly Japan, where the prevalence was
centres around the world. Clinical features were comparedwith those
of 308 patients with connective tissue diseases7/105 in 1974
(Yamamoto et al., 1974). In Turkey the
prevalence was found to be higher in rural than in urban who had
also had recurrent oral ulceration. Use of the newcriteria offered
an increase in diagnostic sensitivity andareas (37/105 versus
8/105) (Yurdakul et al., 1988). There
has been only one published survey of the disease in the UK
specificity compared with previously published diagnosticcriteria.
Although it was specified that recurrent oral(Chamberlain, 1977),
in which the prevalence was found to
be 0.4/105. There has been no epidemiological study of cases
ulceration was a prerequisite, it was acknowledged that
casesexisted in which there was pathologically proven Behcetsof
Behcets syndrome with neurological complications, other
than those that have reported the prevalence of such syndrome
without oral ulceration; it was stated that thecriteria would
exclude only 3% of patients in whom recurrentcomplications in
hospital populations attending specialist
Behcets syndrome clinics. Authors whose patient populations oral
ulceration was not a feature.
Oxford University Press 1999
-
2184 D. Kidd et al.
Table 1 International Study Group for Behcets disease describe a
response to corticosteroids, which Evans andcriteria colleagues
confirmed (Evans et al., 1957), although others
noted some cases in which no response was evident. All
hadRecurrent major or minor aphthous or herpetiform ulceration
ofnoted a propensity for relapse and remission. Further reviewsthe
mouthhave been published from time to time (Wolf et al., 1965;Plus
recurrent genital ulcerationODuffy and Goldstein, 1976; Al-Kawi,
1992; Serdaroglu,erythema nodosum
pseudofolliculitis 1998).papulopustular eruption Bienenstock and
Margulies (1961) described a case inacneiform nodules which
cerebral angiography revealed venous sinus thrombosispathergy test
positivity
as the cause of their patients syndrome. Vascular
complic-anterior or posterior uveitisations as a result of dural
venous sinus thrombosis occurretinal vasculitiscommonly in some
series (Bousser et al., 1980; el-Ramahiand Al-Kawi, 1991;
Serdaroglu, 1998). Others present with
Aetiology isolated intracranial hypertension (Pamir et al.,
1981; ShakirThe aetiology is unknown; an infective agent has long
et al., 1990; Akman-Demir et al., 1996a); dural venous sinusbeen
postulated but has never been identified. Neutrophil thrombosis is
found in association with this in most (but nothyperfunction and an
increase in the CD81/CD41 cell ratio all) cases, and the CSF is in
general inactive. Arterialoccur. There is an increase in
circulating T cells bearing thrombosis is rarer, and aneurysm
formation has been reportedreceptors; indeed, peptides derived from
the 65 kDa heat (Wechsler et al., 1989).shock proteins have been
shown to stimulate T cells Involvement of muscle (Arkin et al.,
1980; Lang et al.,specifically from patients with the disease
(Suzuki et al., 1990), causing a polymyositis, appears to be rare.
Peripheral1992; Lehner, 1997). Such cells have been shown to be
neuropathy has been reported (ODuffy and Carney, 1971;uveitogenic
to Lewis rats (Stanford et al., 1994). The Rougemont et al., 1982),
with nerve biopsy and electrophysio-association with HLA B51 is
well known and this is logical characteristics of a non-vasculitic
axonal neuropathy.particularly associated with uveitis, although
even in Japanese A predominately motor polyradiculopathy has also
beenseries the prevalence of HLA B51 is only 57% (Mizuki et
reported (Bakouche and Guillard, 1984).al., 1997). There is some
evidence that HLA B51, as wellas B12, DR7 and DR2, may bear a
relationship with thetissue location of the disease. Vascular
complications may Neuropathologybe related to abnormal procoagulant
activity, which may have The first paper to describe the
neuropathology of such casesa primary role, or they may be
secondary to endothelial cell was in 1944 (Berlin, 1944); in this
report the basal meningesactivation. were seen to be thickened and
multiple foci of cellular
infiltration within the meninges and parenchymal lesionswere
observed. Silfverskiold described findings in a patient
Clinical picture of neurological Behcets who had died within 5
days of the onset of a severe brainstemsyndrome and saw that there
was considerable swelling ofsyndrome
Neurological involvement in Behcets syndrome was first the
brainstem with multiple foci of cellular infiltration
andperivascular inflammatory cell cuffs (Silfverskiold,
1951).described in the early decades of this century. Pallis
and
Fudge (1956) and Wadia and Williams (1957) described the
McMenemey and Lawrence described these cases and twoothers; in
these, as in the others published previously, theclinical syndromes
and classified them into three types.
(i) Brainstem disturbance associated with systemic symptoms
brainstem was predominately involved, and areas of softeningwith
cellular infiltration and perivascular cuffing were seensuch as
fever, arthralgia and skin eruption; the brainstem
signs developed subacutely with evolving cranial neuro-
(McMenemey and Lawrence, 1957). Lesions also involvedthe cortex and
other grey matter structures, in which loss ofpathies, ocular motor
dysfunction, nystagmus and gaze
palsies, dysarthria and ataxia and, on occasions, bulbar muscle
neurons was seen. Rubinstein and Urich reported a furthercase in
which the patient died after a 6 year disease courseweakness.
Headache with meningism was commonly cited,
and in these cases CSF pleocytosis and high protein content
characterized initially by relapses and then
progressivedeterioration (Rubinstein and Urich, 1961). Their
findingswere observed. (ii) Meningomyelitis, comprising a
meningitis
with varying neurological signs, including spinal cord and were
typical of those previously described: there was a
chronicmeningoencephalitis with inflammatory cell infiltration
andhemisphere signs (Silfverskiold, 1951). (iii) A confusional
syndrome, in which meningoencephalitis without focal
circumscribed areas of necrosis with loss of all tissueelements,
accumulation of lipid-laden macrophages andneurological signs
arose, which was in some instances chronic
and progressive, resulting ultimately in the development of
gliosis. Although the white matter was more often involved,there
was clear evidence for lesion formation within the greydementia,
Parkinsonism, pseudobulbar palsy and quadri-
paresis. Pallis and Fudge (1956) also described a case with
structures, including the cortex, basal ganglia and
brainstemnuclei. A large series from Japan (Kawakita et al.,
1967)acute myelitis. Wadia and Williams (1957) were the first
to
-
Neurological complications in Behcets syndrome 2185
Table 2 Clinical presentation in the 50 patientssummarized the
findings in nine cases from that country andcompared them with the
13 published from Europe and North
Meningoencephalitis with brainstem involvement 25America. No
difference was noted. Miyakawa and colleagues Spinal cord
involvement 7and Yamamori and colleagues described cases in which
Hemisphere involvement 5
Meningitis 4marked cerebral atrophy was seen; in these cases
involvementIsolated intracranial hypertension 4of the cortex with
marked loss of neurons was observed inCerebral venous sinus
thrombosis* 2addition to the white matter findings noted in
previous reports Cranial neuropathy* II 1(Miyakawa et al., 1976;
Yamamori et al., 1994). Lueck and V 1 VII 2
co-authors, from this institution, published the post-mortem VII
2VIII 3findings of their case, who had presented with a relapsing
then
progressive meningoencephalitis without systemic features
in*Some patients shared different clinical subgroups.
which the neuropathology showed features characteristic
ofBehcets disease (Lueck et al., 1993). Hadfield and colleagueshave
shown that there is a marked infiltration by neutrophils
and/or uveitis. The median latency from onset of systemicand
eosinophils as well as by lymphocytes, and there is at
symptoms to neurological presentation was three (028)times
marked axonal degeneration within lesions (Hadfield years. Twelve
patients presented first with neurologicalet al., 1996). No
evidence for vasculitis has been found in
symptoms. In one case, published previously (Lueck et al.,this
or other pathological studies. 1993), the diagnosis was made only
at autopsy, following a
neurological illness without any evidence of a
systemicdisturbance at all.Current study
The purpose of this study was to define further the
variousclinical syndromes associated with this disorder,
tocharacterize the various immunological and imaging Neurological
presentation (Table 2)
Twenty-five patients presented with a
meningoencephalitisabnormalities seen and to attempt to identify
clinical andimmunological prognostic factors for subsequent disease
involving the brainstem, seven with spinal cord syndromes
and five with hemisphere signs. Four presented withactivity. We
also investigated possible differences in thesecharacteristics
between patients of European stock and those symptoms and signs of
meningitis and encephalopathy alone.
One patient had signs of an optic neuropathy for which noborn in
regions with higher disease prevalence.other cause has been found.
One presented with bilateralfacial weakness, two with acute
vestibular disturbance dueto an isolated vestibular lesion, and one
with isolated bilateralPatients and methods
The medical notes of all patients admitted to the National
sensorineural deafness. Vascular complications were rare inour
series; two presented with cortical venous thrombosis.Hospital for
neurological investigation and treatment with a
diagnosis of Behcets syndrome over the past 15 years were Four
patients presented with intracranial hypertension alone.In the
patients with isolated brainstem disturbance, thereviewed. Most had
been under the care of one of the authors
(P.R.). Many had been referred by another (A.M.D.), and in
disorder had a tendency to arise subacutely over days.
Twentypatients presented with ataxia and ocular motor
dysfunction,order to follow-up their cases the medical notes of
such
patients were scrutinized at Northwick Park Hospital. The one
having signs indicating a pontine disturbance and twohaving bulbar
symptoms, with dysarthria and dysphagia. Thediagnosis of Behcets
syndrome was accepted if the clinical
course and features fulfilled the International Study Group
severity of the accompanying long tract signs was variable.In two
cases the patient presented acutely with a severecriteria
(International Study Group for Behcets Disease,
1990). Statistical comparison of groups used the Mann brainstem
encephalitis requiring intensive and ventilatorycare. Isolated
cranial nerve lesions also occurred; in theseWhitney test.cases
lesion of nerve VII was the most prevalent (three cases,of which
two also had trigeminal involvement).
Seven patients presented with spinal cord disease; two
ofResultsFifty patients were studied; their mean age was 31 years
(SD these patients presented with a severe transverse myelitis
with paraplegia, two with a BrownSequard syndrome and6 years).
Thirty-one (62%) were male. Thirty-nine were ofEuropean stock,
three were born in Iran, three in Turkey, the others with sensory
disturbance with increased reflexes
and sphincter disturbance but without weakness.two in the Indian
subcontinent and three in North Africa. Allbut one had had mouth
ulcers, 41 had had orogenital ulceration Of the patients with
hemisphere disturbance, four presented
with hemiparesis and one with hemisensory disturbanceand 29 had
developed uveitis. Systemic symptoms, such asoligoarthritis (20
cases) and skin lesions (22 cases), were alone. Three had seizures,
including one patient who presented
de novo with hippocampal complex partial seizures.relatively
common, although in 30 cases the neurologicalsyndrome arose in
conjunction only with orogenital ulceration Symptoms of meningitis
that preceded or were an important
-
2186 D. Kidd et al.
of CSF and imaging abnormalities was also
non-significantlydifferent.
Imaging resultsImaging showed MRI abnormalities in the
clinically affectedarea in all but one case of those presenting
with a brainstemsyndrome (Table 3). The other was a normal CT scan.
Inthree cases in addition to the brainstem lesion,
multiplepredominantly periventricular white-matter lesions were
seenin the hemispheres bilaterally. Lesions correlated well withthe
clinical syndrome; 20 showed lesions within the midbrainor superior
cerebellar peduncle (Fig. 2), sometimes extendingto the
diencephalon, one showed a single lesion within thepons, and two
showed medullary lesions. Severe atrophy wasnoted in cases with
progressive disease (Fig. 2). In two cases,in whom the clinical
syndrome was of a severe acutebrainstem disturbance, the entire
brainstem was seen to beinvolved (Fig. 3) and considerable
brainstem swelling wasobserved in the acute phase (Fig. 4).
All those with hemisphere syndromes showed multiplewhite matter
lesions in both hemispheres, which tended not
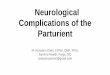
Fig. 1 FLAIR (fluid attenuated inversion recovery) sequence MRI
to be localized to the periventricular regions. Among patients[1.0
T; TR (repetition time) 7000 ms, TE (echo time) 150 ms] of with
cord syndromes, spinal cord imaging was undertakena patient who
presented with seizures and hemiparesis due to in three cases; the
image was abnormal in two cases, onecortical vein thrombosis with
infarction.
showing a high signal intensity lesion with and one
withoutadjacent cord swelling (Fig. 5). In two other cases the
brainalone was scanned, and this was normal in both cases.part of
the clinical syndrome in those with parenchymal
In the single patient with an isolated optic
neuropathy,involvement were common, arising in 16 out of the 39
cases.imaging showed no abnormality, including the optic nerves.Two
patients presented with an isolated vestibulopathy;In the two
patients with isolated vestibulopathy and the singleone of these
patients showed evidence for canal paresis andcase with bilateral
deafness, imaging of the brain was normal.a preponderance of
directional rotation on electronystagmo-
In patients presenting with meningitis alone or
isolatedgraphy.intracranial hypertension, imaging of the brain was
normalCortical vein thrombosis was seen in two cases, onein each
case.of whom showed evidence of concurrent meningitis. One
presented with a hemisphere lesion with seizures due tocortical
vein thrombosis (Fig. 1) and the other with intracranial CSF
resultshypertension. Isolated intracranial hypertension was seen
in
CSF examination was carried out in 18 of 25 patients withthree
other cases, in whom no evidence for meningitisbrainstem
disturbance; CSF was active in 17 cases, in whichwas
found.leucocytosis was seen. In 11 of the latter cases there was
anincrease in protein concentration (Table 3). Those withmeningitis
and encephalopathy had abnormal CSF in all fourcases, whilst half
of the samples examined were abnormalEthnic differences
Eleven (22%) patients were not born of Northern European in
patients with hemisphere and spinal cord disturbance.Among those
presenting with isolated intracranial hyper-stock. There was no
difference in the age of onset of the
disease [23 years (range 1052 years) versus 27 years (range
tension the CSF was abnormal in one case, and in the singlecases of
those with dural vein thrombosis, optic neuropathy1044 years), P 5
0.34], age at onset of neurological
complications [31 years (range 1452 years) versus 28 years and
isolated vestibulopathy, CSF was normal. Intrathecalsynthesis of
immunoglobulin was not observed in the cases(range 1844 years), P 5
0.54] (non-European and European
subjects, respectively), characteristics of the systemic disease
studied; matched serum/CSF bands were seen in seven cases(18%). In
one case a monoclonal band was seen which hadand the
characteristics of the neurological disorder. Similar
conclusions have been drawn in a series from France disappeared
6 months later when the CSF examination hadbeen repeated during a
reappraisal of the diagnosis.(Wechsler et al., 1988). Six patients
had had a brainstem
syndrome, two a cord lesion, two a hemisphere disturbance The
difference between median CSF protein concentrationin the brainstem
group and the meningoencephalitis groupand one isolated
intracranial hypertension. The prevalence
-
Neurological complications in Behcets syndrome 2187
Table 3 MRI and CSF results in patient subgroups, divided into
the clinical syndromes with which they presented
Patient Number MRI CSFsubgroup
No data Normal Local Local 1 No data Protein Total WCC % % % OB
OB OBperiventricular (mg/mm3) (cells/mm3) polymorphs lymphocytes
monocytes / 1/ 1/1
median median(range) (range)
Brainstem 25 2 1 19 3 7 0.51 40 9.5 80 0 14 0 4(0.17-3.70)
(1360) (080) (20100) (050)
Cord 7 2 3* 2 0 2 0.57 67 0 75 0 3 0 2(0.372.4) (10103) (050)
(0100) (0100)
Hemisphere 5 1 0 0 4 1 0.69 2 6.0 67 5 4 0 0(0.280.79) (122)
(553) (4090) (05)
Meningitis 4 0 2 n/a 2 0 1.01 15 82 10 0 4 0 0(0.622.5) (2368)
(090) (10100) (08)
ICH 4 0 4 0 0 0 0.53 2 4.0 95 0 3 0 1(0.30.66) (128) (020)
(80100) 0
OB x/x 5 oligoclonal immunoglobulin bands in CSF/serum; WCC 5
CSF white cell count; ICH 5 intercranial hypertension. *Twonormal
brain MRI, one normal cord MRI.
Fig. 2 T2-weighted MRI (1.5 T; TR 3000 ms, TE 91 ms) of a
patient with multiple brainstem attacksand a progressive disease
course, showing a lesion within the midbrain, and brainstem and
cerebellaratrophy.
-
2188 D. Kidd et al.
Fig. 3 T2-weighted MRI (0.5 T; TR 3800 ms, TE 92 ms) of a
patient who presented with an acutebrainstem syndrome with apnoea
requiring prolonged ventilatory support, showing very
pronouncedhigh signal intensity abnormalities throughout the
brainstem.
was significant (P 5 0.042); in all other cases CSF protein well
without residual disability. Three patients (one withtransverse
myelitis and two with a brainstem disturbance),and white cell count
were not significantly different between
groups (P . 0.05). however, made no improvement and are left
with severeneurological impairments. Further attacks occurred in
12patients, in whom a median of one relapse (range 16) hasarisen to
date. Relapse occurred frequently in patients withEvoked
potentials
The visual evoked potential was measured in 10 cases; it
brainstem involvement at onset (Table 4), and eight patientshad
further brainstem attacks. One patient with cordwas abnormal in one
case. Sensory evoked potentials were
measured in eight cases and were normal in each case.
involvement initially had a further cord syndrome, and oneeach with
cord involvement and hemisphere involvement hadBrainstem auditory
evoked potentials were measured in 12
cases and abnormalities were detected in two cases, in which a
brainstem attack at a later point. Four patients havesubsequently
undergone progressive deterioration leading tothere was a delay in
conduction at the level of the pons in
patients with brainstem dysfunction. severe impairment and
disability; all of these patients hadbrainstem disturbance
initially and all have had furtherattacks. There were two deaths,
both owing to aspirationpneumonia with severe brainstem
impairment.Clinical follow-up
Thirty-five (70%) patients have been followed-up for a In an
attempt to identify significant prognostic factorsduring the first
neurological attack, CSF protein and whitemedian of 3 years (range
119 years). All four cases of
intracranial hypertension underwent shunting procedures and cell
count were measured. There was no significant differencein CSF
protein or white cell count between patients followedhave remained
well. Recovery from attacks with parenchymal
lesions was in general good; the majority of patients recovered
up who had had a single attack and those whose attacks were
-
Neurological complications in Behcets syndrome 2189
Fig. 4 T1-weighted MRI (0.5 T; TR 420 ms, TE 15 ms) following
injection of gadoliniumDTPA ofthe same patient as in Fig.3, showing
swelling of the brainstem and enhancement of the lesion withinthe
pons.
recurrent. However, the median CSF white cell count was suggest.
This may also account for the lower incidence ofprogressive disease
than that noted in other studies, althoughhigher in patients who
subsequently became disabled or died
[103 (range 5368)] than in those who were not disabled at we did
take care to follow up patients who returned to therheumatology
clinics in order to minimize this potential bias.follow-up [12
(range 1180)] (P 5 0.02).
One patient presented with signs of optic neuropathy, forwhich
no alternative cause has been found; imaging wasnormal and CSF
immunoglobulin oligoclonal bands wereDiscussion
In this large clinical series of patients with neurological
absent. Optic neuropathy is rare in Behcets syndrome, onlya handful
of cases having been published (Colvard et al.,involvement in
Behcets syndrome the incidence of brainstem
involvement was high (52%) and that of vascular 1977; Kansu et
al., 1989). Pathological examination of onecase has shown gliosis
and demyelination within the nervecomplications low (4%).
Involvement of the hemisphere,
spinal cord and optic nerves was also seen. No difference
(Colvard et al., 1977).Of particular interest are the three
patients who presentedwas noted between the small number of
non-Northern
European-born patients and the others. Patients with active with
or developed vertigo or hearing loss. There has beenonly one report
of auditory findings, in a small series ofdisease showed a mixed
lymphocyte and neutrophil
pleocytosis and there was no evidence for intrathecal synthesis
patients with Behcets syndrome (Brama and Fainaru, 1980).In two of
our patients, initial asymmetrical hearing lossof immunoglobulin.
Imaging revealed lesions localized to
the clinically affected areas in most cases examined, with
progressed to involve both ears, but there were fluctuations,often
over a period of weeks, in the magnitude of the hearingevidence for
lesion dissemination in a further three cases.
The prognosis for recovery following acute relapse was in
deficit. Extensive tests of auditory function showed that
thehearing decline was due to hair cell loss; both patientsgeneral
good, the majority of patients becoming symptom-
free. However, of those who were followed-up 28% showed
recruitment on assessment of loudness discomfortlevel and the
stapedius reflex measurement; they had normalunderwent further
attacks and 14% became significantly
disabled as a consequence of either the absence of recovery
brainstem auditory evoked potentials and absent echoes.
Theintolerance of loud sounds reported by one patient is alsoor the
development of a progressive disease course. It should
be noted, however, that in this series the median follow-up
consistent with hair cell loss. Both had recurrent attacks ofsevere
vertigo that resolved over 14 weeks. Only one ofwas 3 years (range
119 years); a longer follow-up may
reveal a more frequently relapsing disease than these data the
patients had abnormal caloric responses, indicating loss
-
2190 D. Kidd et al.
Fig. 5 T2-weighted MRI (1.5 T; TR 5000 ms, TE 130 ms) of a
patient who presented with an acutedisturbance of sensation in the
upper and lower limbs, with urgency of micturition, showing a
cordlesion adjacent to C2.
of horizontal canal function on one side. Ultimately this
submitted that this may offer prognostic information. In ourseries,
disabled patients at follow-up had a higher medianpatient developed
complete vestibular failure. Both patients
had normal vestibulo-ocular reflex suppression on rotational CSF
white cell count during the acute attack than those whohad improved
and remained stable. More recent reportsand caloric testing,
indicating a peripheral origin of the
dysfunction. Thus the three patients with auditory vestibular
(Akman-Demir et al., 1996c; Bohlega, 1996; Siva et al.,1998), in
which larger patient groups have been studied,abnormalities or
symptoms all had a progressive peripheral
rather than a central nervous system disorder, which to some
have shown a frequency of relapse similar to that in our ownseries,
but a greater frequency of progressive disease courseextent
mimicked Menie`res syndrome.
Previous clinical series have been small with a variable
(3040%). They suggest that adverse prognostic factorsinclude young
age of onset, brainstem involvement, highfollow-up. In one of the
larger series (Serdaroglu et al., 1989;
Akman-Demir et al., 1996b), which followed-up 15 patients
frequency of relapse and the presence of CSF abnormalities.
Inaddition, one group has suggested that a primarily progressivewho
had had abnormal neurological signs out of a series of
45 who had had neurological symptoms, seven were stable
(progressive from symptom onset) disease course may
exist(Akman-Demir et al., 1996c). Our series and those of othersand
three had died (one during a relapse); of the remaining
five, one had had two further relapses and four had undergone
suggest that in general the prognosis for isolated
intracranialhypertension and dural venous sinus thrombosis is
goodprogressive deterioration without superimposed relapse. In
this group of patients the incidence of CSF abnormalities
following satisfactory treatment. For those with
parenchymalinvolvement it appears that prognosis is related to
thewas higher than in those who were stable, and the authors
-
Neurological complications in Behcets syndrome 2191
Table 4 Frequency of relapse and site of further attacks
Wechsler et al., 1993; Coban et al., 1996; Tali et al.,
1997).according to clinical subgroup at presentation In acute
lesions there may be oedema, and enhancement is
present in the majority of cases (Kazui et al., 1991;
TaliClinical subgroup No. of No. of cases Site ofet al., 1997).
T1-weighted hypointensity is seen in chroniccases with relapse
relapselesions. There is a close clinicalradiological
correlation
Brainstem 25 8 Brainstem (Morrissey et al., 1993; Wechsler et
al., 1993; Akman-DemirCord 7 1 Cord et al., 1998). A striking
feature noted by many (Kermode1 Brainstem
et al., 1989; Al-Kawi et al., 1991; Nussell et al.,
1991;Hemisphere 5 1 BrainstemGerber et al., 1996; Akman-Demir et
al., 1998) is that T2-Meningitis 4 1 Meningitis
1 Brainstem weighted white matter lesions reduce in size
markedly inIntracranial 4 0 conjunction with clinical recovery and
often become invisible,hypertension at least on low-strength
magnets (Kermode et al., 1989; TaliCranial neuropathy II 1 0
et al., 1997). Brainstem atrophy may be striking, as evidentVII
4 0in several of our cases (Fig. 2) and noted by others
(MorrisseyVIII 3 1 Progressive
vestibular failure et al., 1993; Wechsler et al., 1993; Coban et
al., 1996).The largest published study involved 15 patients
with
parenchymal involvement; atrophy was seen in three
cases,involvement of the brainstem and basal ganglia alone in
eightfrequency and number of further attacks and the
development
of a progressive disease course. The pathophysiology of this
cases, and in three further cases periventricular lesions wereseen
in addition to brainstem lesions. MRIs were normal inis not clear
but is likely to be linked to progressive axonal
degeneration leading to atrophy, as has been intimated in two
cases, scanned at least 11 months after resolution of theclinical
attack (Wechsler et al., 1993). In a further 10 patientsmultiple
sclerosis (Kidd et al., 1996, 1998; Trapp et al.,
1998). Further prospective studies are required in order to with
cerebral vein thrombosis, MRI of the brain was normaland the
imaging abnormality was restricted to the venousdefine further the
pathophysiology of the disease course and
the prognostic features. system. In a further five cases with
headache alone withoutintracranial hypertension, three of whom had
CSF pleocytosis,In our series no patient showed intrathecal
synthesis of
immunoglobulin. Other papers (Sharief et al., 1991; McLean MRI
was normal. More recently (Akman-Demir et al., 1998),a study of a
series of 59 patients with brainstem involvementet al., 1995;
Serdaroglu, 1998) have reported series in
which the majority showed evidence of bloodbrain barrier and 14
with intracranial hypertension has shown
similarfindings.dysfunction but few papers have shown intrathecal
synthesis
of IgG, and Gille and colleagues reported that oligoclonal
Magnetic resonance spectroscopy investigations have beenpublished
for only three cases (Nussel et al., 1991), inimmunoglobulin bands
disappeared from CSF following an
acute attack (Gille et al., 1990). This is in stark contrast to
which a reduced NAA/Cr (N-acetyl aspartate/creatine
1phosphocreatine) ratio was seen in the acute phase, whichmultiple
sclerosis, in which persistent oligoclonal bands are
present in the CSF of 97% of patients (McLean et al., 1990;
subsequently normalized following clinical recovery; in allthree
cases substantial radiological recovery had occurred.Zeman et al.,
1996). Sharief and colleagues found a greater
incidence of IgA and IgM bands (Sharief et al., 1991), which No
long-term or systematic studies have been published.Few
electrophysiological studies have been publishedmay suggest an
alternative antigenic stimulus, and Jongen
and colleagues in a single case found that IgM and IgA (Nakamura
et al., 1980; Besana et al., 1989; Rizzo et al.,1989; Stigsby et
al., 1994); abnormalities of brainstembands disappeared following
recovery from episodes of
meningoencephalitis (Jongen et al., 1992). In neurosarcoid-
auditory evoked potentials are most frequent, and are moreprevalent
in patients in acute attacks than in patients studiedosis,
oligoclonal bands are also infrequent (McLean et al.,
1995); indeed, there is recent evidence to suggest that they in
remission. Visual evoked potential abnormalities are alsocommon in
other series, although not in ours; this is interestingmay also be
absent, as in Behcets syndrome (V. Chamoun
and L. J. Thompson, personal communication). The mixed in view
of the fact that the optic nerve is involved clinicallyin a small
minority of cases (Colvard et al., 1977; Kansupleocytosis and high
frequency of neutrophils was noted in
early publications and was subsequently confirmed et al., 1989).
Characteristically, recordings show reducedamplitude with little or
no prolongation in latency. This is in(Nakamura et al., 1980).
These authors also noted that the CSF
cell count diminished in response to steroid administration,
contrast to that of demyelination, in which it is characteristicto
see prolonged latency with temporal dispersion but normalprompting
speculation that there is an anti-inflammatory role
for steroids rather than simply an anti-oedema mode of action.
amplitude (Halliday et al., 1972). Visual evoked
potentialabnormalities occurred in patients without uveitis withOur
series confirms the findings of previous MRI studies
that have shown that involvement of the clinically affected
frequency equal to that in patients who had had ocularinvolvement
(Stigsby et al., 1994). A study of central motorregion alone is
most common. Most prevalent is the lesion
of the midbrain extending to the basal ganglia or internal
conduction times in 20 patients, 13 of whom had
neurologicalsymptoms and signs, has shown that abnormalities
comprisingcapsules (Kermode et al., 1989; Morrissey et al.,
1993;
-
2192 D. Kidd et al.
Akman-Demir G, Baykan-Kurt B, Serdaroglu P, Gurvit H,
Yurdakulmild conduction slowing and reduction in amplitude wereS,
Yazici H, et al. Seven year follow-up of neurologic
involvementpresent in half of those with abnormal neurological
signs,in Behcet syndrome. Arch Neurol 1996b; 53: 6914.and also
arose in those without signs (Parisi et al., 1996). In
our series the prevalence of evoked potential abnormalities
Akman-Demir G, Serdaroglu P, Tasci B, Baykan-Kurt B, Gurvitwas low
(two out of 12 patients in whom data were available). IH, Bahar S,
et al. Neurological involvement in Behcets disease.
There has been no prospective placebo-controlled trial of Rev
Rheum Engl Ed 1996c; 63: 549.any form of treatment in Behcets
syndrome with neurological Akman-Demir G, Bahar S, Coban O, Tasci
B, Parman Y, Serdaroglucomplications. Anecdotal evidence has
pressed forward the P. Cranial MRI findings in Behcets disease: a
study of 134 MRIopinion that use of corticosteroids is mandatory in
acute of 98 cases [abstract]. J Neurol 1998; 245: 362.attacks and
possibly thereafter. Intravenous methylpred-
Al-Kawi MZ. Neuro-Behcet disease: a review. J Trop
Geographnisolone is often given in acute attacks. Other forms
ofNeurol 1992; 2: 4956.immunosuppressive treatment, such as
azathioprine, cyclo-
phosphamide, chlorambucil and cyclosporin A, have been Al-Kawi
MZ, Bohlega S, Banna M. MRI findings in neuro-Behcetsadvocated as
maintenance therapy (Serdaroglu, 1998). disease. Neurology 1991;
41: 4058.Colchicine is thought to act by inhibiting neutrophil
Alpsoy E, Yilmaz E, Basaran E. Interferon therapy for
Behcetschemotaxis (Matsumara and Mizushima, 1975). For adequate
disease. J Am Acad Dermatol 1994; 31: 6179.treatment trials one
must turn to the ophthalmologists, who
Arkin CR, Rothschild BM, Florendo NT, Popoff N. Behcet
syndromehave shown clearly that the use of cyclosporin A in
uveitiswith myositis: a case report with pathologic findings.
Arthritisresults in an alteration of the visual prognosis in
thisRheum 1980; 23: 6004.complication of the disease (Graham et
al., 1985; Masuda
et al., 1989). More recently, reports of beneficial effects on
Assaad-Khalil S, Abou-Seif M, Abou-Seif S, El-Sewy F,
El-Sewysystemic features of the disease with tacrolimus (Ishioka M.
Neurologic involvement in Behcets disease: clinical, genetic
and computed tomographic study. In: Wechsler B, Godeau P,et al.,
1994; Sakane et al., 1995) and interferon -2a (Alpsoyeditors.
Behcets disease. Amsterdam: Excerpta Medica Internationalet al.,
1994; Azizlerli et al., 1996) have been published.Congress Series
1037; 1993. p. 40914.Treatment for dural venous sinus thrombosis
involves
anticoagulation; Wechsler and colleagues advocate the Azizlerli
G, Sarica R, Kose A, Ovul C, Kavala M, Kayabali M, etconcurrent use
of corticosteroids (Wechsler et al., 1992), al. Interferon -2a in
the treatment of Behcets disease. Dermatologyalthough again this
has not been established by means of a 1996; 192: 23941.prospective
clinical trial.
Bakouche P, Guillard A. Polyradiculonevrite au cours dune
pousseeIn summary, this clinical series of patients with
Behcetsevolutive de maladie de Behcet. Rev Neurol (Paris) 1984;
140:
syndrome with neurological complications has shown and
5202.confirmed that, in general, patients develop subacute
episodes
Benamour S, Zeroual B, Bennis R, Amraoui A, Bettal S. Maladieof
neurological dysfunction predominantly situated withinde Behcet:
316 cas. Presse Med 1990; 19: 14859.the brainstem, but also the
hemisphere and the spinal cord.
Involvement of the optic nerve was seen, but is exceedingly
Berlin C. Behcets syndrome with involvement of the central
nervousrare; involvement of the spinal roots, peripheral nerves and
system. Arch Derm Syph 1944; 49: 22733.muscle is also rare and was
not seen in this series. MRI reveals Besana C, Comi G, Del Maschio
A, Praderio L, Vergani A,lesions that enhance and show close
clinicalradiological Medaglini S, et al. Electrophysiological and
MRI evaluation ofcorrelation. Evidence for lesion dissemination is
uncommon, neurological involvement in Behcets disease [see
comments]. Jin contrast to multiple sclerosis. The spinal fluid
shows a Neurol Neurosurg Psychiatry 1989; 52: 749754. Comment in:
Jmixed pleocytosis with predominance of lymphocytes but Neurol
Neurosurg Psychiatry 1989; 52: 1212, Comment in: J Neurolalso
neutrophils, and intrathecal synthesis of immunoglobulin Neurosurg
Psychiatry 1990; 53: 442.is not or very rarely seen. The majority
of patients do not Bienenstock H, Margulies ME. Behcets syndrome:
report of a caseundergo relapses, but those who do have a poor
prognosis
with extensive neurologic manifestations. N Engl J Med 1961;
264:for the development of fixed impairments and disability, and
13425.a proportion develop a progressive course with
accumulating
Bohlega S. Prognostic factors in neuro-Behcets disease. Rev
Rheumdisability. No formal trial of treatment in this disorder
hasEngl Ed 1996; 63: 550.been published, and there is now an urgent
need to do so
through multicentre clinical trials. Bousser MG, Bletry O,
Launay M, Portier E, Guillard A, CastaigneP. Thromboses veineuses
cerebrales au cours de la maladie deBehcet. Rev Neurol (Paris)
1980; 136: 75362.Brama I, Fainaru M. Inner ear involvement in
Behcets disease.
References Arch Otolaryngol 1980; 106: 2157.Akman-Demir G, Bahar
S, Baykan-Kurt B, Gurvit IH, SerdarogluP. Intracranial hypertension
in Behcets disease. Eur J Neurol 1996a; Chamberlain MA. Behcets
syndrome in 32 patients in Yorkshire.
Ann Rheum Dis 1977; 36: 4919.3: 6670.
-
Neurological complications in Behcets syndrome 2193
Coban O, Bahar S, Akman-Demir G, Serdaroglu P, Baykan-Kurt
Thompson AJ, et al. Central motor conduction time in
progressivemultiple sclerosis: correlations with MRI and disease
activity. BrainB, Tolun R, et al. A controlled study of reliability
and validity of
MRI findings in neuro-Behcets disease. Neuroradiology 1996; 38:
1998; 121: 110916.3126.
Lakhanpal S, Tani K, Lie JT, Katoh K, Ishigatsubo Y, Ohokubo
T.Colvard M, Robertson MA, ODuffy JD. The ocular manifestations
Pathologic features of Behcets syndrome: a review of Japaneseof
Behcets disease. Arch Ophthalmol 1977; 95: 18137. autopsy registry
data. Hum Pathol 1985; 16: 7905.Davitchi F, Shavran F, Akbarin M,
Gharbdoost F, Nadjii A, Chaim Lang BA, Laxer RM, Thorner P,
Greenberg M, Silverman ED.C, et al. Behcets disease: analysis of
3443 cases. APLAR J Pediatric onset of Behcets syndrome with
myositis: case reportRheumatol 1997; 1: 25. and literature review
illustrating unusual features [see comments].
[Review]. Arthritis Rheum 1990; 33: 418425. Comment in:el-Ramahi
KM, al-Kawi MZ. Papilloedema in Behcets disease;Arthritis Rheum
1990; 34: 791.value of MRI in diagnosis of dural sinus thrombosis.
J Neurol
Neurosurg Psychiatry 1991; 54: 8269. Lehner T. The role of heat
shock protein, microbial and autoimmuneagents with the aetiology of
Behcets disease. [Review]. Intern RevEvans AD, Pallis CA, Spillane
JD. Involvement of the nervousImmunol 1997; 14: 2132.system in
Behcets syndrome: report of three cases and isolation of
virus. Lancet 1957; 2: 34953. Lueck CJ, Pires M, McCartney AC,
Graham EM. Ocular andneurological Behcets disease without
orogenital ulceration? J NeurolGerber S, Biondi A, Dormont D,
Wechsler B, Marsault C. Long-Neurosurg Psychiatry 1993; 56:
5058.term MR follow-up of cerebral lesions in neuro-Behcets
disease.
Neuroradiology 1996; 38: 7618. McMenemey WH, Lawrence BJ.
Encephalomyelopathy in Behcetsdisease: report of necropsy findings
in two cases. Lancet 1957; 2:Gille M, Sindic CJ, Laterne PF, de
Hertoghe P, Hotermans JM,3538.Selak I, et al. Atteintes
neurologiques et la maladie de Behcet. Acta
Neurol Belg 1990; 90: 23447.Masuda K, Nakajima A, Urayama A,
Nakae K, Kogure M, Inaba
Graham EM, Sanders MD, James DG, Hamblin A, Kasp Grochowska G.
Double-masked trial of cyclosporin versus colchicine and long-E,
Dumonde D. Cyclosporin A in the treatment of posterior uveitis.
term open study of cyclosporin in Behcets disease. Lancet
1989;Trans Ophthalmol Soc UK. 1985; 104: 14651. 1: 10936.Hadfield
MG, Aydin F, Lippman HR, Kubal WS, Sanders KM. Matsumura N,
Mizushima Y. Leucocyte movement and colchicineNeuro-Behcets
disease. Clin Neuropathol 1996; 15: 24955. treatment in Behcets
disease. Lancet 1975; 2: 813.Halliday MA, McDonald WI, Mushin J.
Delayed visual evoked McLean BN, Luxton RW, Thompson EJ. A study of
immunoglobulinresponse in optic neuritis. Lancet 1972; 1: 9825. G
in the cerebrospinal fluid of 1007 patients with suspected
neurological disease using isoelectric focusing and the Log
IgG-International Study Group for Behcets Disease. Criteria
forIndex. Brain 1990; 113: 126989.diagnosis of Behcets disease.
[Review]. Lancet 1990; 335: 107880.McLean BN, Miller D, Thompson
EJ. Oligoclonal banding of IgGIshioka M, Ohno S, Nakamura S, Isobe
K, Watanabe N, Ishigatsuboin CSF, bloodbrain barrier function, and
MRI findings in patientsY, et al. FK506 treatment of non-infectious
uveitis. Am J Ophthalmolwith sarcoidosis, systemic lupus
erythematosus and Behcets disease1994; 118: 7239.involving the
nervous system. J Neurol Neurosurg Psychiatry 1995;
Jongen PJ, Daelmans HE, Bruneel B, den Hartog MR. Humoral 58:
54854.and cellular immunologic study of cerebrospinal fluid in a
patient
Miyakawa T, Murayama E, Deshimaru M, Shikai I, Kozuma S.with
Behcet encephalitis. Arch Neurol 1992; 49: 10758.Neuro-Behcets
disease showing severe atrophy of the cerebrum.Kansu T, Kirkali P,
Kansu E, Zileli T. Optic neuropathy in Behcets Acta Neuropathol
(Berl) 1976; 34: 95103.disease. J Clin Neuroophthalmol 1989; 9:
27780.Mizuki N, Inoko H, Ohno S. Pathogenic gene responsible for
theKawakita H, Nishimura M, Satoh Y, Shibata N. Neurological
aspectspredisposition to Behcets disease. [Review]. Int Rev
Immunol
of Behcets disease: a case report and clinico-pathological
review1997; 14: 3348.
of the literature in Japan. J Neurol Sci 1967; 5:
41739.Morrissey SP, Miller DH, Hermaszewski R, Rudge P,
MacManusKazui S, Naritomi H, Imakita S, Yamada N, Ogawa M, Sawada
T.DG, Kendall BE, et al. Magnetic resonance imaging of the
centralSequential gadoliniumDTPA enhanced MRI studies in
neuro-nervous system in Behcets disease. Eur Neurol 1993; 33:
28793.Behcets disease. Neuroradiology 1991; 33: 1369.Nakamura S,
Takase S, Itahara K. Cytological examination ofKermode AG, Plant
GT, MacManus DG, Kendall BE, Kingsley DP,cerebrospinal fluid in
eight patients with neuro-Behcets disease.Moseley IF. Behcets
disease with slowly enlarging midbrain massTohoku J Exp Med 1980;
132: 42130.on MRI: resolution following steroid therapy. Neurology
1989; 39:
12512. Nussel F, Wegmuller H, Laseyras F, Posse S, Herschowitz
N, HuberP. Neuro-Behcet: acute and sequential aspects by MRI and
MRS.Kidd D, Thorpe JW, Kendall BE, Barker GJ, Miller DH,
McDonaldEur Neurol 1991; 31: 399402.WI, et al. MRI dynamics of
brain and spinal cord in progressive
multiple sclerosis. J Neurol Neurosurg Psychiatry 1996; 60: 159.
ODuffy JD. Behcets disease. [Review]. Curr Opin Rheumatol1994; 6:
3943.Kidd D, Thompson PD, Day BL, Rothwell JC, Kendall BE,
-
2194 D. Kidd et al.
ODuffy JD, Goldstein NP. Neurologic involvement in seven
patients visual and somatosensory evoked potentials in 44
patients.Electroencephalogr Clin Neurophysiol 1994; 92: 27381.with
Behcets disease. Am J Med 1976; 61: 1708.
Suzuki Y, Hoshi K, Matsuda T, Mizushima Y. Increased
peripheralODuffy JD, Carney JA, Deodhar S. Behcets disease: report
of 10blood T cells and natural killer cells in Behcets disease.
Jcases, 3 with new manifestations. Ann Intern Med 1971; 75:
56170.Rheumatol 1992; 19: 58892.
Pallis CA, Fudge BJ. The neurological complications of
BehcetsTali ET, Atilla S, Keskin T, Simonson T, Isik S, Yuh WT. MRI
insyndrome. Arch Neurol Psychiatry 1956; 75: 114.neuro-Behcets
disease. Neuroradiology 1997; 39: 26.
Pamir MN, Kansu T, Erbengi A, Zileli T. Papilloedema in
BehcetsTrapp BD, Peterson J, Ransohoff RM, Rudick R, Mork S, Bo
L.syndrome. [Review]. Arch Neurol 1981; 38: 6435.Axonal transection
in the lesions of multiple sclerosis [see
Parisi L, Terracciano ME, Valente GO, Calendriello E, Accorinti
M, comments]. N Engl J Med 1998; 338: 27885. Comment in: N
EnglSpadaro M. Pre-symptomatic neurological involvement in Behcets
J Med 1998; 338: 3235.disease: the diagnostic role of magnetic
transcranial stimulation.
Wadia N, Williams E. Behcets syndrome with
neurologicalElectrencephalogr Clin Neurophysiol 1996; 101:
427.complications. Brain 1957; 80: 5971.
Rizzo PA, Valle E, Mollica MA, Sanarelli L, Pozzessere
G.Wechsler B, LeThi Huong Du, Massim I, Ziza JM, Piette JC,
BletryMultimodal evoked potentials in neuro-Behcet: a longitudinal
studyO, et al. Behcets disease in France: a propos of 60
autochthonousof two cases. Acta Neurol Scand 1989; 79:
1822.subjects. [Review]. Ann Med Interne (Paris) 1988; 139:
3159.
Rougemont D, Bousser MG, Wechsler B, Bletry O, Castaigne
P,Wechsler B, Huong LT, de Gennes LC, Bletry O, Pette JL,
MathieuGodeau P. Manifestations neurologiques de la maladie du
Behcet.A, et al. Arterial involvement in Behcets disease. Rev Med
InterneVingt-quatre observations. Rev Neurol (Paris) 1982; 138:
493505.1989; 10: 30311.
Rubinstein LJ, Urich H. Meningo-encephalitis of Behcets
disease:Wechsler B, Vidailhet M, Piette JC, Bousser MG, DellIsola
B,
case report with pathological findings. Brain 1963; 86:
15160.Bletry O, et al. Cerebral venous thrombosis in Behcets
disease:
Serdaroglu P. Behcets disease and the nervous system. [Review].
clinical study and long-term follow-up of 25 cases. Neurology
1992;J Neurol 1998; 245: 197205. 42: 6148.
Wechsler B, DellIsola B, Vidailhet M, Dormont D, Piette
JC,Serdaroglu P, Yazici H, Ozdemir C, Yurdakul S, Bahar S, Atkin
E.Bletry O, et al. MRI in 31 patients with Behcets disease
andNeurologic involvement in Behcets syndrome: a prospective
study.neurological involvement: prospective study with clinicalArch
Neurol 1989; 46: 2659.correlation. J Neurol Neurosurg Psychiatry
1993; 56: 7938.Shakir RA, Sulaiman K, Kahn RA, Rudwan M.
NeurologicalWolf SM, Schotland DL, Phillips LL. Involvement of
nervouspresentation of neuro-Behcets syndrome: clinical categories.
Eursystem in Behcets syndrome. Arch Neurol 1965; 12: 31525.Neurol
1990; 30: 24953.Yamamori C, Ishino H, Inagaki T, Seno H, Ijima M,
Torii I, et al.Sharief MK, Hentges R, Thomas E. Significance of
CSFNeuro-Behcet disease with demyelination and gliosis of the
frontalimmunoglobulins in monitoring neurologic disease activity
inwhite matter. Clin Neuropathol 1994; 13: 20815.Behcets disease.
Neurology 1991; 41: 1398401.Yamamoto SI, Toyokawa H, Matsubara J,
et al. A nationwide surveySilfverskiold BP. Recurrent uveitis
(Behcets syndrome) andof Behcets disease in Japan. I.
Epidemiological survey. Jpn Jencephalomyelomeningitis. Acta
Psychiatr Neurol Scand 1951; 26:Ophthalmol 1974; 18:
28290.44353.Yurdakul S, Gunaydin I, Tuzun Y, Tankurt N, Pazarli H,
OzyazganSiva A, Kantarcy O, Saip S, Hamuryudan V, Altyntas A,
YazycyY, et al. The prevalence of Behcets syndrome in a rural area
inH. Neuro-Behcet syndrome (NBS): prognostic factors and
survivalnorthern Turkey. J Rheumatol 1988; 15: 8202.[abstract]. J
Neurol 1998; 245: 362.Zeman AZ, Kidd D, McLean BN, Kelly MA,
Francis DA, MillerStanford MR, Kasp E, Whiston R, Hasan A, Todryk
S, Shinnick T,DH, et al. A study of oligoclonal band negative
multiple sclerosis.et al. Heat shock protein peptides reactive in
patients with BehcetsJ Neurol Neurosurg Psychiatry 1996; 60:
2730.disease are uveitogenic in Lewis rats. Clin Exp Immunol 1994;
97:
22631.
Stigsby B, Bohlega S, al-Kawi MZ, al-Dalaan A, el-Ramahi K.
Received February 8, 1999. Revised June 6, 1999.Accepted June 14,
1999Evoked potential findings in Behcets disease. Brain-stem
auditory,