Embed Size (px)
Citation preview

Neuroimaging findings in pediatric cerebral sinovenous thrombosis
Matthias W. Wagner ¹, Thangamadhan Bosemani ¹, Alexander Oshmyansky 1,2, Andrea Poretti ¹, Thierry A.G.M. Huisman ¹
¹Section of Pediatric Neuroradiology, Division of Pediatric Radiology, Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins University School of Medicine, Baltimore, MD, USA; ²School of Mathematical Sciences, Faculty of Science and
Engineering, Queensland University of Technology, Brisbane, QLD, Australia
EP-120
ASNR 53rd Annual Meeting, Chicago, April 25-30, 2015

Disclosure
We have nothing to disclose No relevant financial relations interfering
with the presentation

Cerebral sinovenous thrombosis (CSVT)
Thrombosis in:Superficial (cortical veins, superior sagittal sinus,
transverse sinus, sigmoid sinus, and jugular vein) or Deep (inferior sagittal sinus, internal cerebral veins,
vein of Galen, straight sinus) venous system Incidence: 1 of 100,000 children Accounts for 1 in 4 cases of pediatric stroke Mortality rate = 8-19% Severe long-term neurological sequelae in 38-48%
of patients

CSVT and neuroimaging
Role of neuroimaging in the diagnosis of CSVT:1. To visualize and characterize the thrombus
2. To identify the degree of impaired flow within affected venous system
3. To rule out secondary complications (venous ischemia / hemorrhage)
Techniques CT ± venography (CTV) MRI ± venography (MRV) Conventional angiography Trans-fontanel Doppler ultrasonography
MRI = modality of choice in pediatric CSVT Conventional sequences (T1, T2, FLAIR) Advanced sequences (DWI/DTI, SWI)

Purpose
1. Analysis of MRI signal changes of the thrombus over time in pediatric CSVT
2. Evaluation of the role of DWI/DTI in the diagnosis of pediatric CSVT

Inclusion criteria
A. Age at MRI < 18 years
B. Neuroimaging diagnosis of CSVT

Methods 1
Clinical histories reviewed for:1. Age and gender of children 2. Risk factors for CSVT3. Neurologic manifestation related to CSVT4. Time point of 1) onset of symptoms and 2)
neuroimaging diagnosis
Definition of thrombus age: Interval: onset of symptoms/findings
neuroimaging diagnosis of CSVT

Methods 2
Retrospective evaluation of thrombi for:1. Location2. Number3. Signal characteristics
Assessment of intraparenchymal edema and/or hemorrhagic infarction secondary to CSVT

Methods 3
MRI sequences used:1. T1w/T2w/FLAIR: iso-, hypo-, hyperintense
signal compared to adjacent gray matter2. CE-MRV and TOF-MRV: presence or absence
of flow3. DTI: normal or restricted diffusion4. SWI: hypointense signal

Methods 4
Statistical analysis:Evaluation of relation between age of
thrombus and appearance of thrombus on T1w, T2w, FLAIR, and DWI/DTI images z-test
p-value <0.05 = statistically significant

Results 1: Patients
33 children with CSVT 18 male (55%) Median age at time of brain MRI: 5.59 years
(range: 4 days to 17.75 years) 5 patients (15%) = neonates 10 patients (30%) = < 1 year

Results 2: Risk factors
Risk factors found in 28 children (85%):1. Traumatic head injury (12 patients, 37%) 2. Head and neck infections (6 patients, 18%)
• Bacterial meningitis (Strep. pneumoniae / anginosus, MRSA), 4 children
• Viral encephalitis (presumed Herpes simplex virus), 1 child • Lemierre syndrome, 1 child • Otitis media complicated by mastoiditis due to Strep. pneumoniae, 1
child
3. Prothrombotic disorders (5 patients, 15%) • Acute lymphatic leukemia, Antiphospholipid syndrome, Prothrombin
G20210A mutation, Antithrombin III deficiency, Elevated homocysteine level, each 1 child
4. Other (5 patients, 15%)

Results 3: Neurologic manifestation
Seizures = 11 children (37%) Diffuse neurologic signs:
Decreased level of consciousness = 15 children (50%) Headache = 11 children (37%) Papilledema = 1 child (3%)
Focal neurologic signs: Hemiparesis = 2 children (7%) Acute visual, speech or hearing impairment = 4 children (13%) Paraplegia = 1 child (3%)
None = 3 children (9%)

Results 4: Thrombus age/location
Data for thrombus age calculation available in 26/33 children: <1 day = 15 patients (45%); <8 days = 10 children (31%); >8 days =
1 child (3%)
33 children total of 77 thrombi Multiple thrombi found in 24 patients (73%):
5 thrombi = 1 child; 4 thrombi = 3 children; 3 thrombi = 9 children; 2 thrombi = 11 children; 1 thrombus = 9 patients
Location: 89% in superficial venous system transverse (34%) / sigmoid
(24%) sinuses most common locations

Results 5: MRI characteristics
Intraparenchymal changes in 11/33 children (33%) cytotoxic edema + hemorrhagic infarction in 7, cytotoxic edema in 2, hemorrhagic infarction in 2 patients
Number of thrombi
Hypo Iso HyperReduced/absent
flowRestricted diffusion
T1w 77 (100%) 14 (19%) 21 (28%) 39 (53%) - -
T2w 77 (100%) 16 (22%) 20 (27%) 38 (51%) - -
FLAIR 77 (100%) 14 (21%) 6 (8%) 48 (71%) - -
TOF-MRV 47 (61%) - - - 40 (85%) -
CE-MRV 14 (18%) - - - 14 (100%) -
DTI 72 (94%) - - - - 29 (40%)
SWI 33 (43%) 11 (33%) 9 (27%) - - -

Results 6: MRI pattern of 77 thrombi
Pattern T1w T2w FLAIR DTI n (%)
1 iso hyper variable normal/restricted 14 (18%)
2 hyper iso variable normal/restricted 14 (18%)
3 hyper hyper variable normal/restricted 13 (17%)
4 hyper hypo variable normal/restricted 10 (13%)
5 hypo hyper variable normal/restricted 9 (12%)
6 iso hypo variable normal/restricted 4 (5%)
7 iso iso variable normal/restricted 3 (4%)
8 hypo iso variable normal/restricted 2 (3%)
9 hypo hypo variable normal/restricted 2 (3%)
For 6 thrombi (7%) no pattern could be defined; hyper, hyperintense; hypo, hypointense; iso, isointense

Results 7: Statistics
Age of thrombus hyperintense signal on T1w: p=0.002 for thrombus age <1 day vs. 1-8 days p=0.036 for thrombus age <1 day vs. >8 days
No statistically significant correlation age of thrombus signal on T2w, FLAIR, and DTI

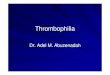
Example 111-year-old male with early subacute thrombosis (7 days to diagnosis) of the superior sagittal sinus
A: Isointense clot on sagittal T1w (arrow)B: Hyperintense clot on axial T2w (arrow)
C: Isointense clot onaxial FLAIR image D: Trace of diffusion and E: matching ADC map: restricted diffusion (bright on D, dark on E) within clot in the superior sagittal sinus (arrows)

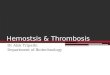
Example 26-year-old female with hyperacute thrombosis (hours to diagnosis) of the right jugular vein
A: Hyperintense clot on sagittal T1w (arrow)B: Hyperintense clot on axial T2w (arrow)
C: Hyperintense clot on axial FLAIR (arrow) D: Trace of diffusion and E: matching ADC map: normal diffusion in right jugular vein (arrows)

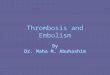
Example 37-month-old female with hyperacute thrombosis (hours to diagnosis) of the right sigmoid sinus A: Hyperintense clot on axial T2w (arrow) B: Matching axial minimum intensity projection (minIP)-SWI image: isointense signal in same location (arrow)
6-year-old female with hyperacute thrombosis (hours to diagnosis) of the right transverse sinus C: Isointense clot on axial T2w (arrow) D: Matching axial minIP-SWI image shows hypointense signal at corresponding level (arrow)

Conclusions
1. Diagnosis of CSVT in children = CHALLENGING
2. MR sequences individually not sensitive enough for an accurate diagnosis of pediatric CSVT
3. DTI + SWI = no complementary value
4. Correlation between thrombus age and signal intensity on different MR sequences: Only age <1 day hyperintense signal on T1w