Embed Size (px)
Citation preview
Neurogenic speech
disorders
Dr. Szabó Edina
University of Debrecen, Medical and
Health Scienc Center Faculty of
Medicine, Dep. of Phisycal Medicine
and Rehabilitation
Animal difference
Soul (church model)
Toolmaking ability
Thinking skills/Ability
of thinking
Modeling capabilities
2
Darwin's theory of language origin
Darwin about animal intelligence
Ancient human cognitive function
Vocalization: rudimentary song
Articulated language
3
Cerebral lateralization
Evolutionary background
Speech and hemispheres
Left: verbal-logical
Right: visual-synthetic
Right: primitive forms of
knowledge is kept
Research of Gazzaniga (1983)
Testing split-brain patients
Phineas Gage (1848)
4
The brain without language
How can the human mind
function without a functioning
language system? (Lecours és
Joanette, 1980)
The case of Brother John
Different stages of aphasia
Abilities remained intact even under
attack: thinking, music, sound, face
detection, use of objects, spatial
orientation, mechanical intelligence,
working memory, episodic memory,
self-presentation
Changed skills: cognitive operations
that require symbolic representation
He could behave as a human being ! 5
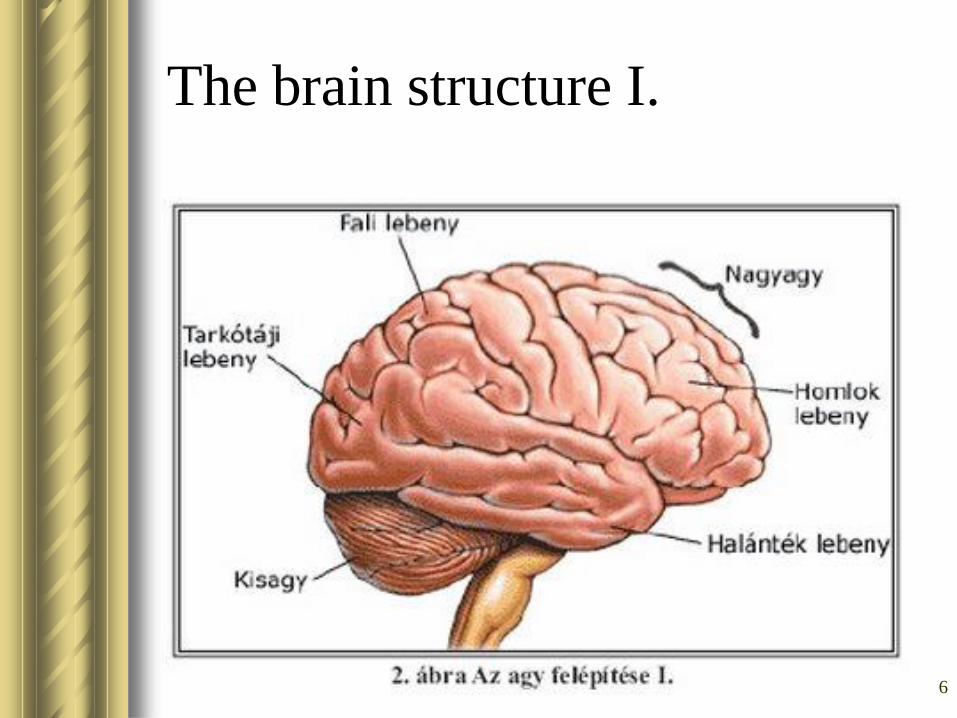
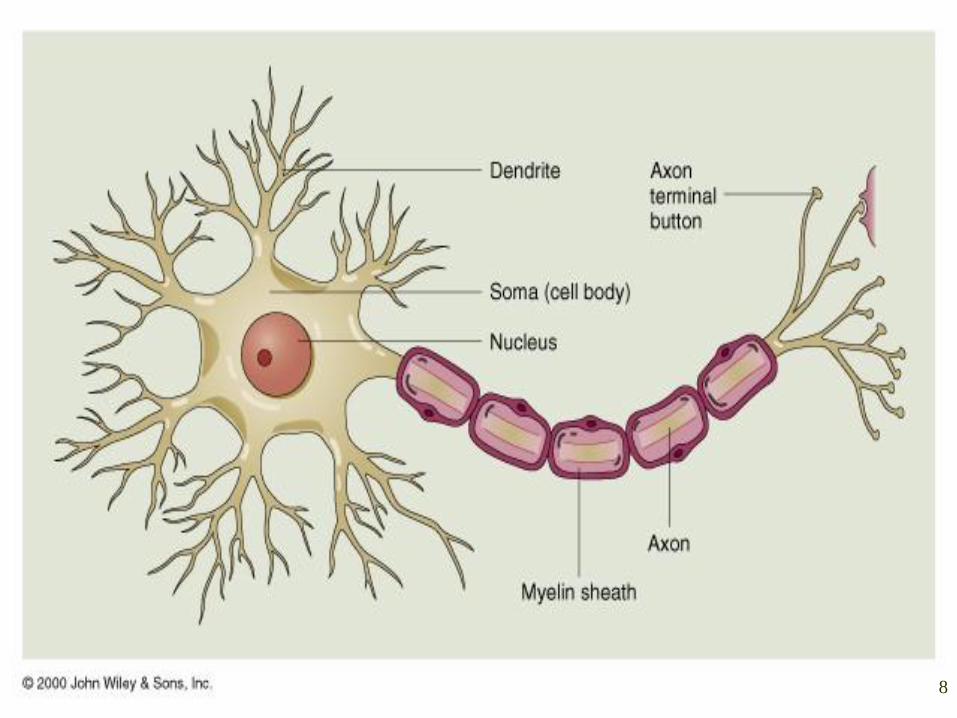
The communication of the brain
The basic structural and functional unit of
the nervous system is: the neuron
Parts: cell body, nucleus, extensions
(dendrites), axon (endings), myelin sheath
7
8
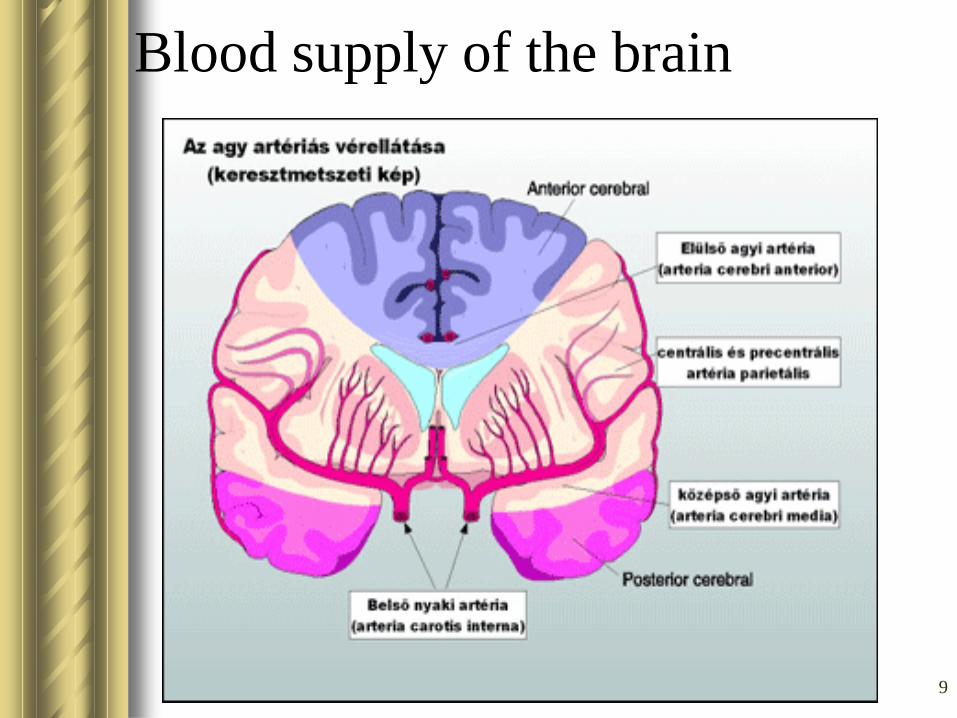
Blood supply of the brain
9
Introduction to the
clinical aphasiology
11
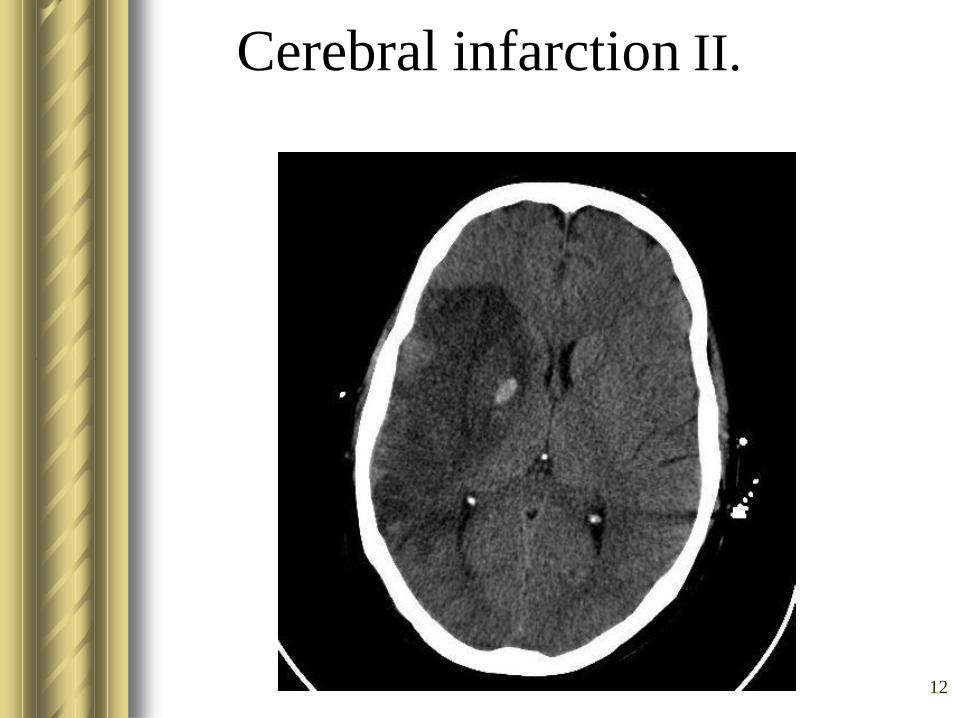
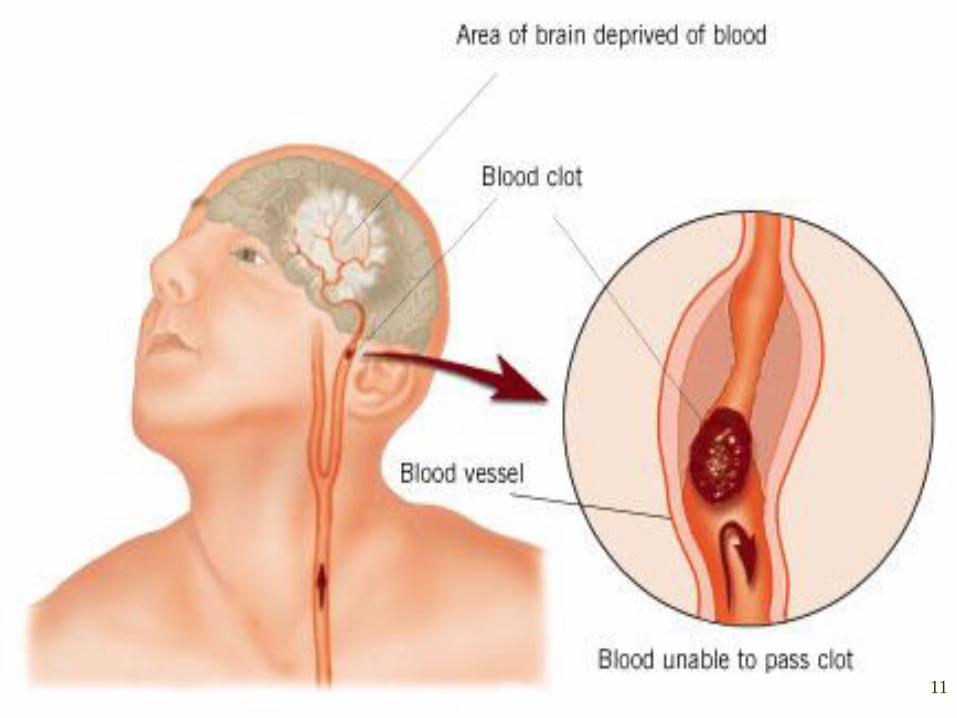
Cerebral infarction II.
12
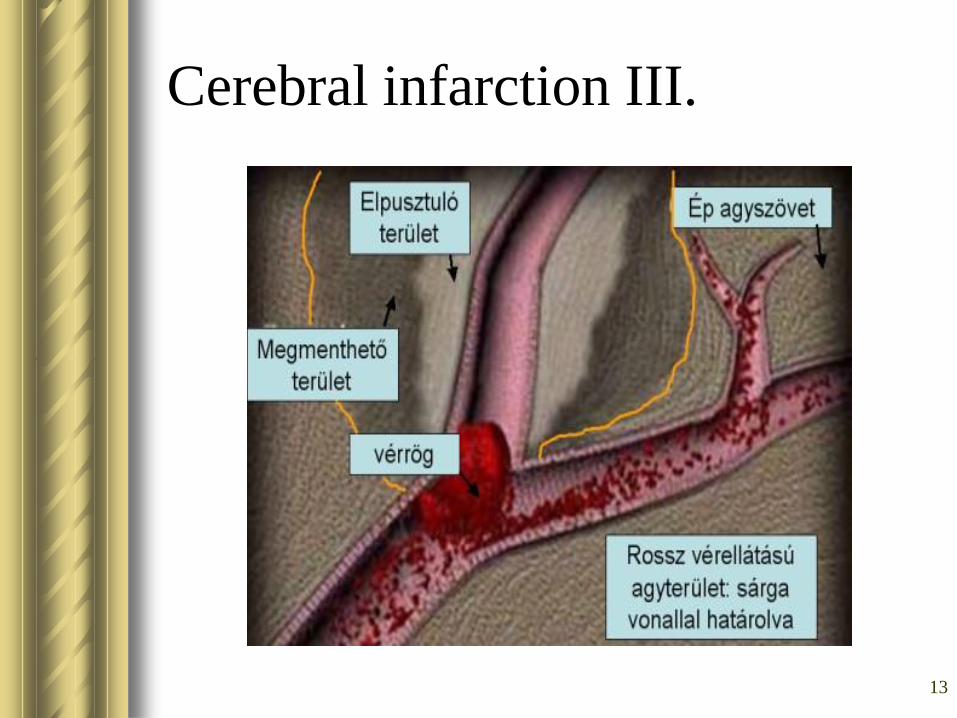
Cerebral infarction III.
13
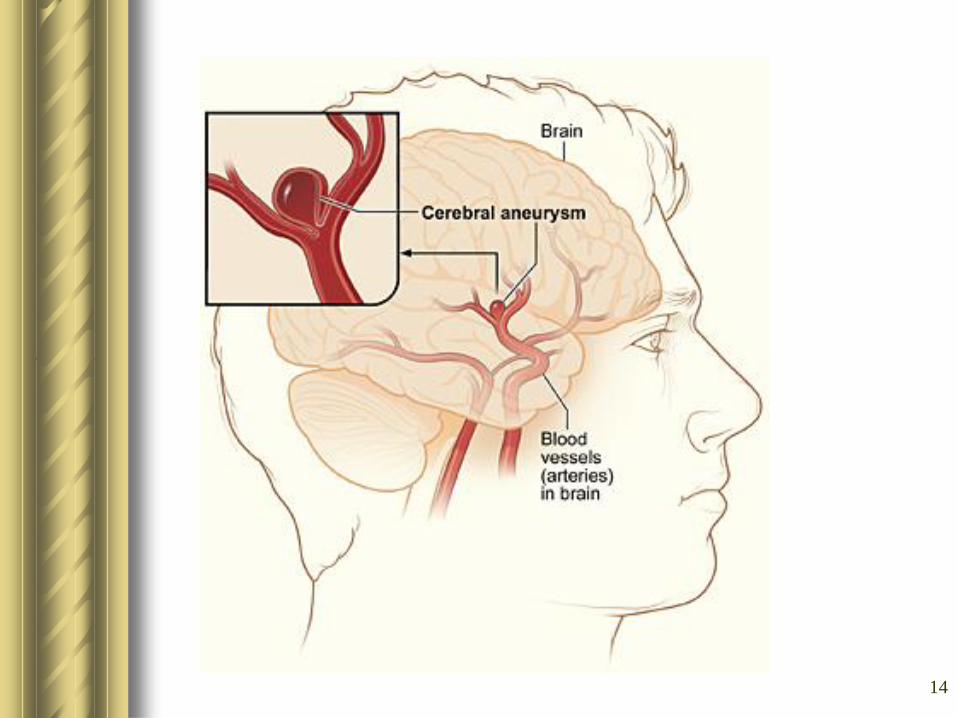
14
15
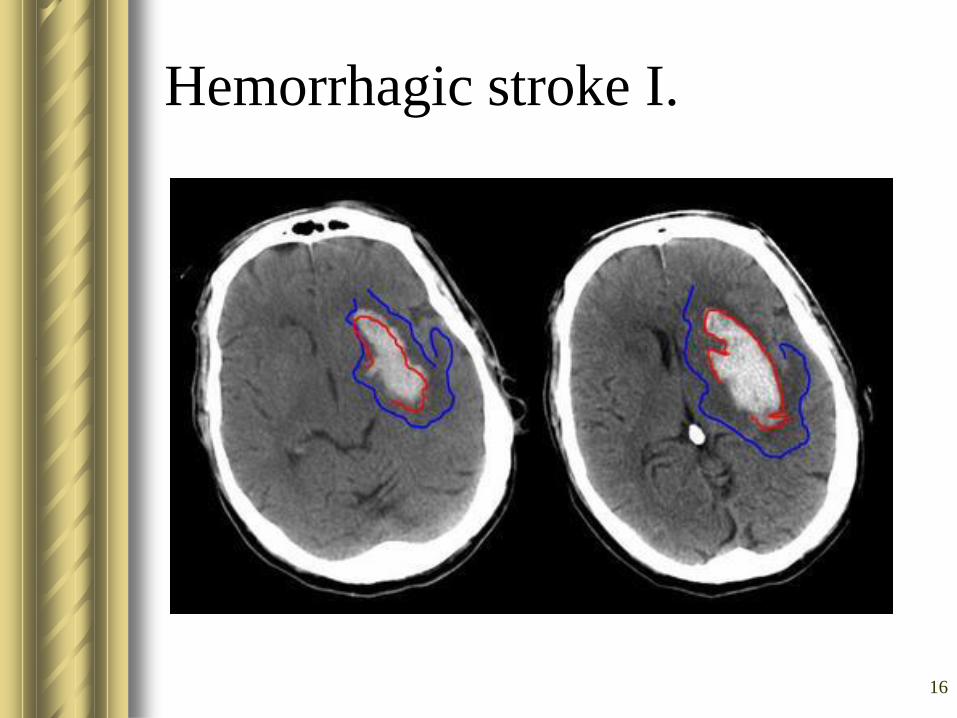
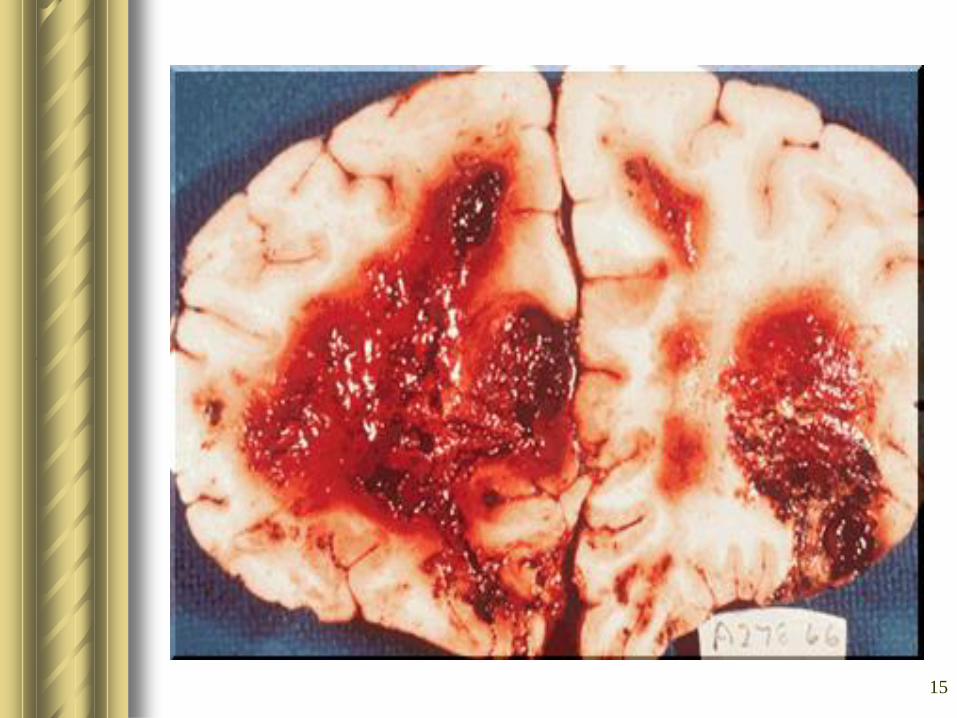
Hemorrhagic stroke I.
16
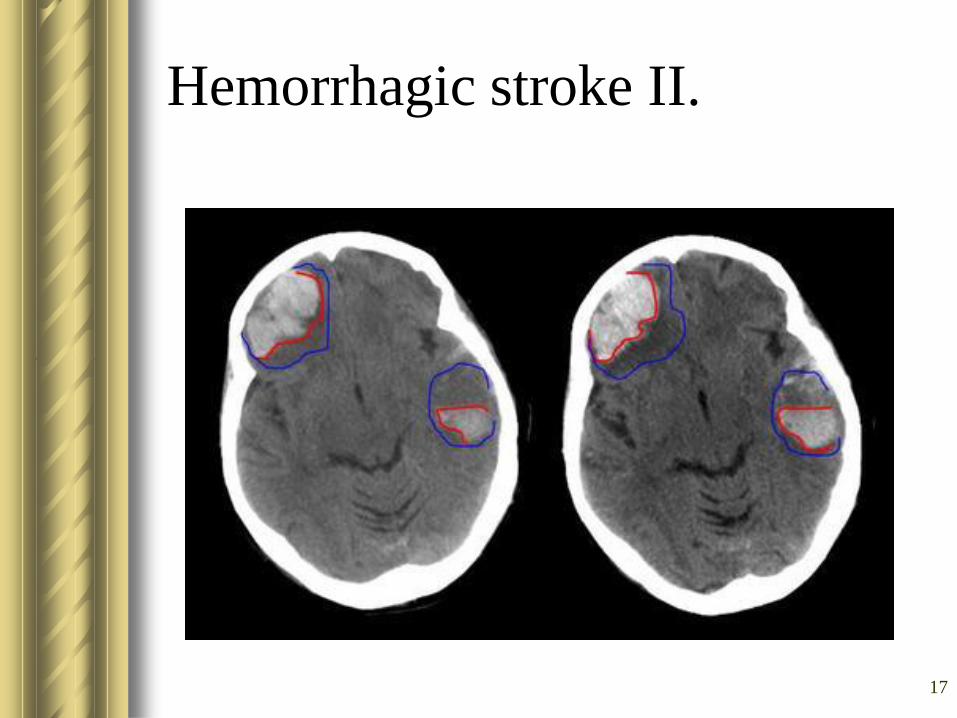
Hemorrhagic stroke II.
17
The communication-centered
definition of aphasia
The aphasia is
neurogenic
communication
disorder, which hides
the competence of
the person, which is
manifested in
conversations.
(Aura Kagan, Aphasia
Institute)
18
Etiology of aphasia
Hemorrhagic stroke
Cerebral infarction
Primary brain tumors or metastases
Trauma (concussion, skull fracture)
19
Symptoms of aphasia
Fluency disorder: nonfluent vs.
fluent aphasia
Understanding disorder
Agrammatism/paragrammatism
Perseveration
Paraphase: semantic, phonemic
Neologism
Verbal automatism
20
Syndroms of aphasia (Boston school)
Classical classification (BDAE, WAB)
Evaluation of the spontaneous
speech, speech repetition,naming and
the understanding
Localization principle: which language
areas of the brain are responsible for
different functions (FTP lobes parts of
perisylvian)
21
Global aphasia
Nonfluent speech
Verbal automatism
Perseverations
Severe understanding disorder
22
Paul Broca and the Broca lesion
23
Broca aphasia
Nonfluent speech
Agrammatism (missing suffixes, parts of sentences, suffixes)
Phonemic paraphases
Word finding difficulties
Faulty speech repetition
Mild, or moderate understanding disorder
Monotonous intonation
24
Carl Wernicke and the Wernicke lesion
25
Wernicke aphasia
Fluent, but empty speech
Meaningless, jargon words
Phonemic and semantic
paraphases
Severe understanding disorder
26
Conduction aphasia
Spontaneous speech: Fluent, but
with a lot of phonemic paraphase
The faulty repetition of words and
phrases
A striking difference between
spontaneous speech and speech
repetition
27
Anomic aphasia
Fluent spontaneous speech
Word finding disorder
Circumscription
Mild understanding disorder
Adequate speech repetition
28
Transcortical aphasias
TMA: nonfluent speech, adequate speech repetition
TSA: disorder of understanding words and sentences, speech repetition is good
Mixed TA: severe impairments in all language functions, repetition is slightly better
29
Atypical aphasias
Crossed aphasia
Subcortical aphasia
Bilingual aphasia
30
They do not understand him, but
he knows what he wants to say
World is narrowing or completely
closing up around him
Becomes shipwrecked among
people
He needs help, he needs to
learn to express himself again!
31
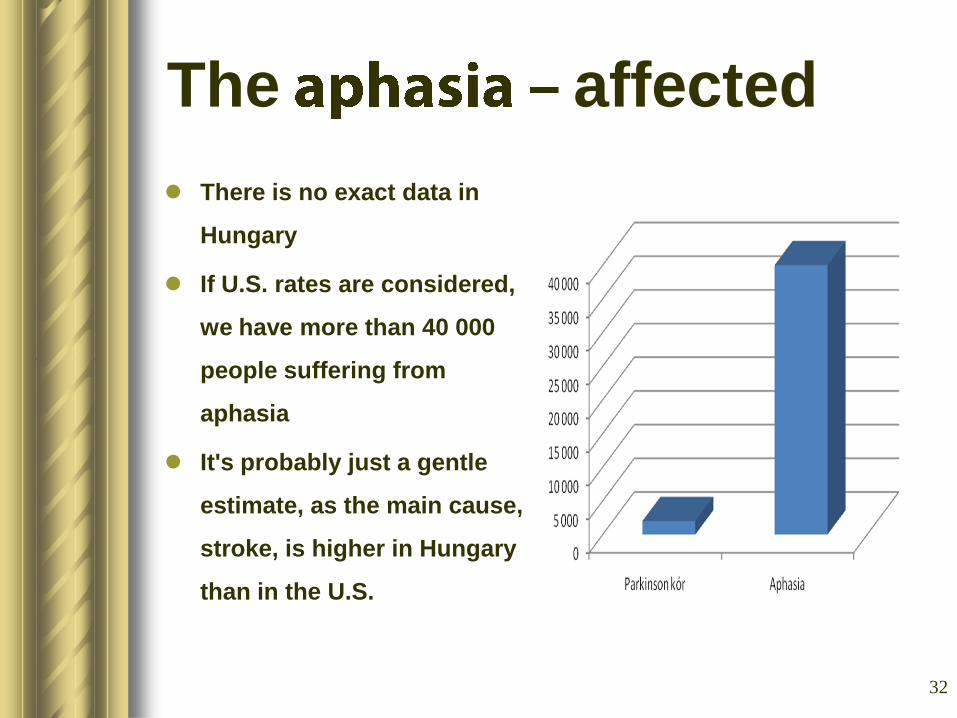
The affected
There is no exact data in
Hungary
If U.S. rates are considered,
we have more than 40 000
people suffering from
aphasia
It's probably just a gentle
estimate, as the main cause,
stroke, is higher in Hungary
than in the U.S.
32
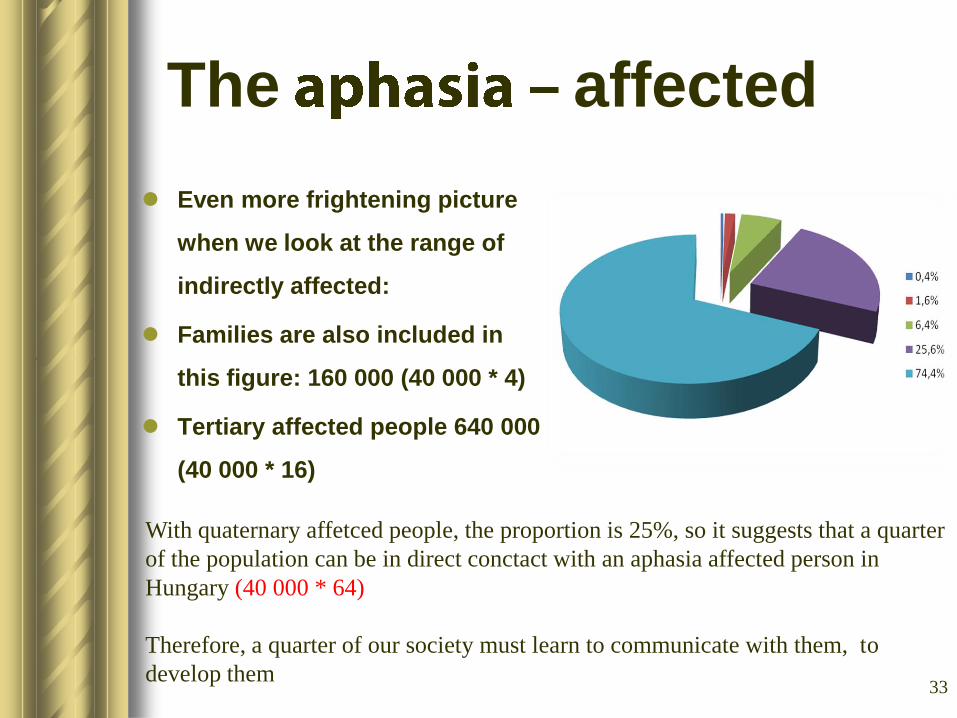
The affected
Even more frightening picture
when we look at the range of
indirectly affected:
Families are also included in
this figure: 160 000 (40 000 * 4)
Tertiary affected people 640 000
(40 000 * 16)
With quaternary affetced people, the proportion is 25%, so it suggests that a quarter
of the population can be in direct conctact with an aphasia affected person in
Hungary (40 000 * 64)
Therefore, a quarter of our society must learn to communicate with them, to
develop them 33
Motor speech
disorders
The speech is one of the most impressive motor activity
The control of speech movements in childhood is possible
The adults are forced to pay attention to their speech movements as a result of a cerebral accident
Two large groups: the apraxia and dysarthria
34
What is considered as motor
speech disorder?
The speech production deficit which develops
as a consequence of neuromuscular and /
or motor control system impairment
Sometimes occurs collectively with other
language impairments (eg aphasia)
Other oral movements can be damaged
besides speech, for example the smiling,
chewing, etc..
35
Determination of speech motor
system
Four Subsystems of Speech
Production:
Respiratory system
Phonatory system
Resonatory system
Articulatory system
36
Frequency of motor speech
disorders
Reliable estimates are rare, but ...
51% of adult speech disorders are
motor aphasia, dysarthria with 46%,
5% apraxia.
Among children 5 % of
developmental communication
disorders are due to motor
dysfunction
37
What about nonfluent aphasias?
Why not discuss the motor speech
disorder?
Nonfluent speech in aphasia is just
one component of a more complex
communication disorder
Differential diagnosis of motor
speech disturbances: always
understanding difference
38
What about stuttering?
Dysfluentia
Subcortical laesio, injury of basal
ganglions
Neurogen dysfluentia/neurogenic
stuttering
39
The common definition of motor
speech disorders according to their
characteristics
We talking about motor planning /
programming deficit when we
experience inability to select
appropriate muscle groups,
difficulty to sychronize them:
Apraxia
Muscles suffers physiological or
motor function injuries: Dysarthria
40
How can we classify motor
speech disorders?
After etiology: Acquired:
– Can be caused by cerebrovascular accident (stroke), degenerative diseases, traumatic brain injury or brain tumor
Developmental:
– Can be caused by congenital disease or injury caused to the developing nervous system
41
Apraxia
The failure of articulatory gestures in normal conversion, wrong linguistic representation (even in imitation tasks!)
Features: slow speech (rarely entire speech), sound distortions,
prolonged vowels (extended release), reduced prosody,
inconsistent defects, speech starting problems, searching
articulatory gestures
Speech disorder is a result of neurological damage: left frontal
cortex, stroke near Broca’area then it is called kinetic /
ideomotor apraxia and when the left parietal cortex is damaged
it’s kinesthetic / ideativ apraxia
Can appear due to cerebral injuries, illnesses, after infections.
42
Dysarthria
Neuromuscular disorder which affetcs execution of speech movements, regulation of muscle tone, reflexes,
movement kinematic aspects
It is characterized by a slow, erratic sounds harsh, raspy or whispering voice, consistent mistakes,or other features depending on the type of dysarthria
Three primal features (depending on model) spasticity, dyskinesia, ataxia.
Its common causes are progressive
neurological disease and stroke. 43
Etiology, symptoms,
and classification of
dysarthria
Definition of dysarthria
Darley, Aronson, Brown (1975):
Muscular control weakness, complex muscle (neurogenic) dysfunction.
Consequence of organic injury in the central or peripheral nervous system
Cséfalvay Zsolt, 2007
45
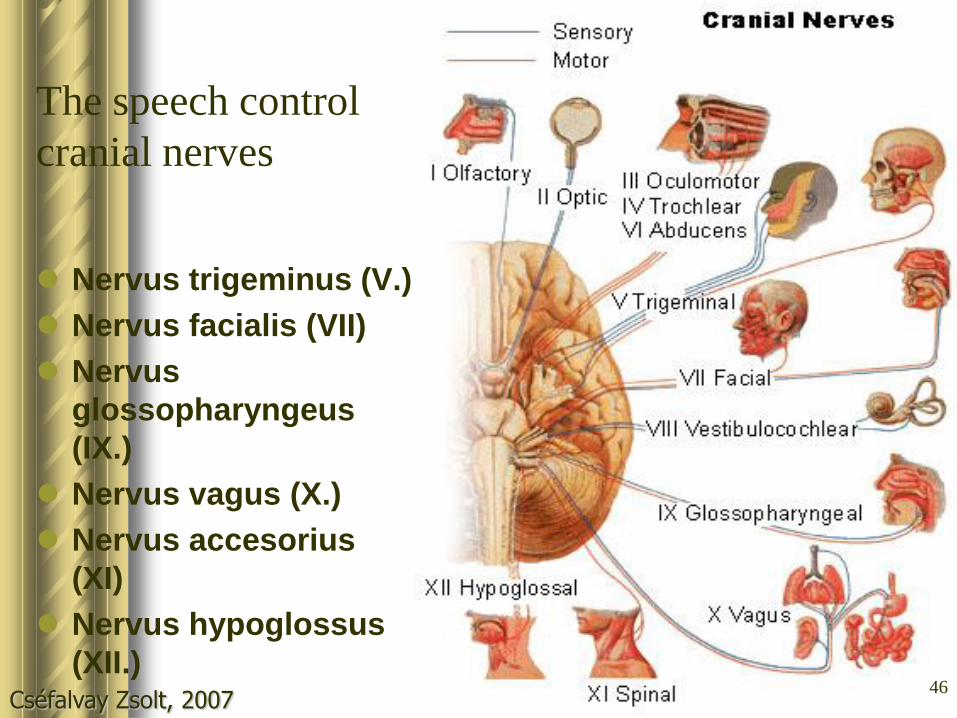
The speech control
cranial nerves
Nervus trigeminus (V.)
Nervus facialis (VII)
Nervus
glossopharyngeus
(IX.)
Nervus vagus (X.)
Nervus accesorius
(XI)
Nervus hypoglossus
(XII.) Cséfalvay Zsolt, 2007
46
Bulbar (or flaccid) dysarthria
(a) lesion in the peripheral motor neuron (involement of cranial nerves)
(b) muscle weakness (flaccid muscles)
Cséfalvay Zsolt, 2007
47
Etiology of bulbar (flaccid) dysarthria
Injury to the nuclei of 5, 7, 9, 10, 11,
12 th. cranial nerves or the bulbar
nuclei
Monopathia: affects only one nerve
Polypathia: more nerves are
concerned
Cséfalvay Zsolt, 2007 48
Etiology of bulbar (flaccid)
dysarthria
Physical injury: surgery, cranial
injury and neck injuries
Brainstem stroke (brainstem
vascular involvement)
Myasthenia gravis
Cséfalvay Zsolt, 2007 49
Etiology of bulbar (flaccid) dysarthria
Guillain Barré syndroma (progressive
inflammatory disease,
demyelinization)
Tumor (near the brain stem)
Muscular dystrophy (progressive
degeneration of muscle tissue)
Progressive bulbar paralyses.
Cséfalvay Zsolt, 2007
50
Symptoms of bulbar dysarthria
Resonance disorder : hypernasality
Artikulation disorder: slow
artikulation
51
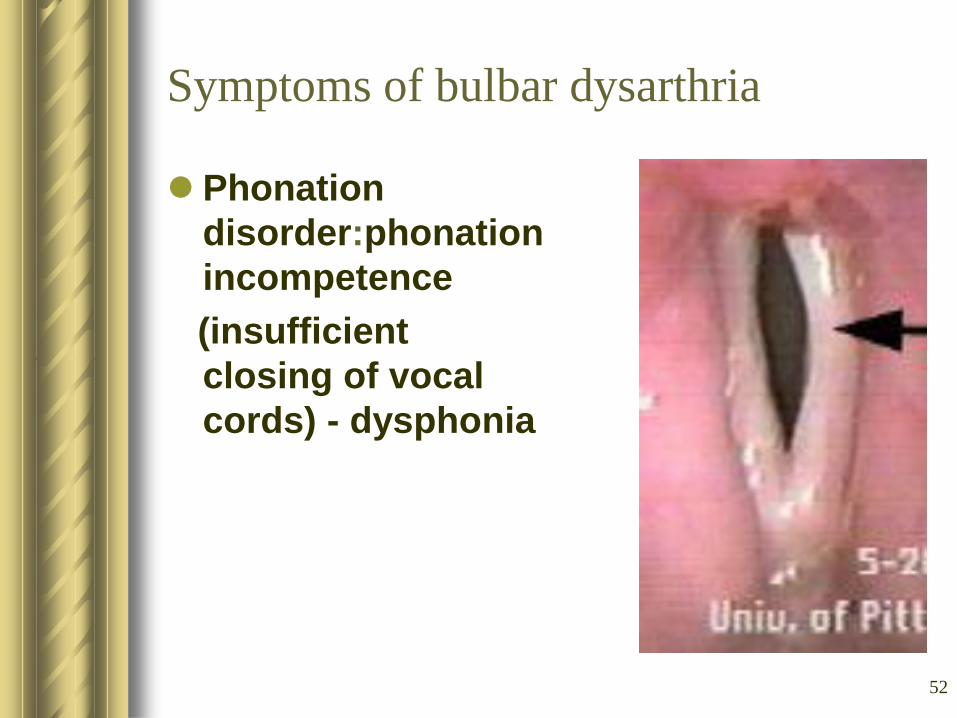
Symptoms of bulbar dysarthria
Phonation
disorder:phonation
incompetence
(insufficient
closing of vocal
cords) - dysphonia
52
Symptoms of bulbar dysarthria
Respiratory Disorder: C., Th nerve
problems only (diaphragm, damage
to intercostal muscle movement,
lack/insufficient subglottic
pressure, poor sound intensity
Prosodic disorder
Cséfalvay Zsolt, 2007
53
Symptoms of bulbar dysarthria
(Summary)
n. trigeminus laesio: artikulation disorder,
resonance disorder
n. facialis laesio: artikulation disorder
n. vagus laesio: resonance disorder,
phonation disorder
n. hypoglossus laesio: artikulation
disorder
Unilateral injury: milder symptoms
Bilateral injury – severe symptoms
Cséfalvay Zsolt, 2007
54
Spastic dysarthria
Bilateral central motor neuron
involvement
Cséfalvay Zsolt, 2007 55
Etiology of Spastic dysarthria
Stroke
Cerebrocranial trauma
Sclerosis multiplex (when central
motoneuron is affected)
Tumor
Cséfalvay Zsolt, 2007 56
Symptoms of spastic dysarthria
Spastic slow articulation (especially
consonants)
Spastic dysphonia (due to hyperadduction
of vocal cords)
Hypernasality – the spasticity slows down
and limits the movement of soft palate
muscles
Dysprosodia: limited range of voice and
volume, short phrases, slow speech rate
Rarely: respiratory problems Cséfalvay Zsolt, 2007
57
Accompanying symptoms of spastic
dysarthria
(1) spastic laughter, crying (which is
difficult to control voluntarily)
(2) hypersalivation (which may be the
control of salivary dysfunction, or as
a result of less frequent swallowing)
Cséfalvay Zsolt, 2007 58
Ataxic (cerebellar)
dysarthria
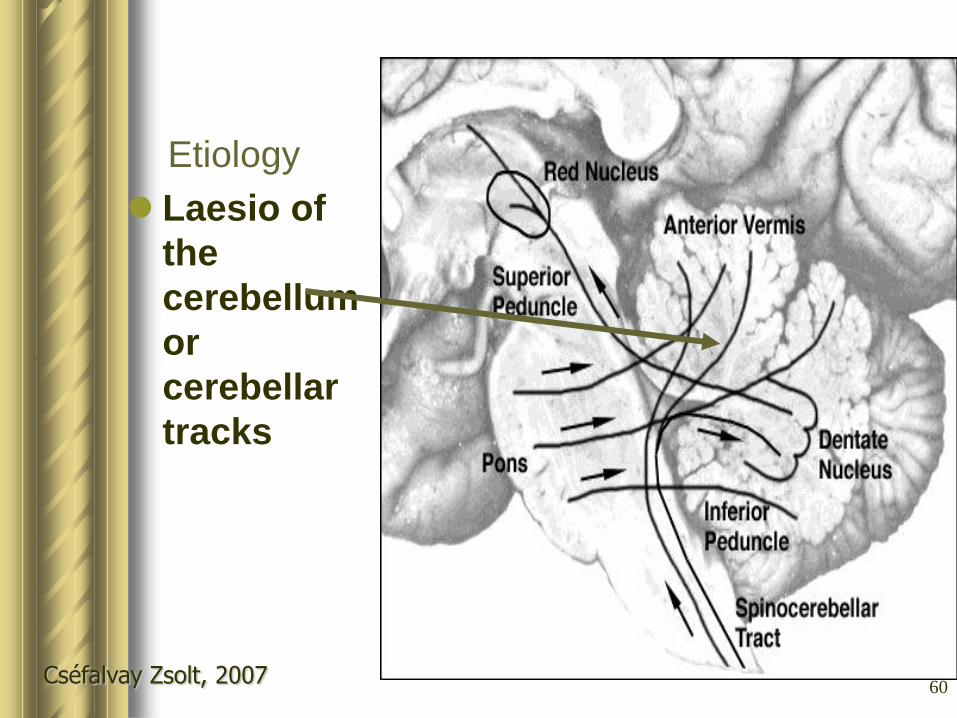
Etiology
Laesio of
the
cerebellum
or
cerebellar
tracks
Cséfalvay Zsolt, 2007 60
Etology of ataxic dysarthria
Degenerative disease: Cerebellar ataxia,
Friedreich ataxia (hereditary spinocerebellar disease),
Olivopontocerebellar degeneration
Stroke – blood supply dysfunction in the areas of the cerebellar
Toxic injury (chemical substances, alcohol, drugs)
Cranial trauma - cerebellar
Tumor ( eg. astrocytoma)
Cséfalvay Zsolt, 2007 61
Symptoms of ataxic dysarthria
Disorder of speech cordination
(artikulation, prosody)
Vague, indistinct articulation: "Boozer"
articulation, irregular intervals (more
syllable words)
Mild hyponasality
Mild dysphonia
Cséfalvay Zsolt, 2007
62
Hyperkinetic dysarthria
Hyperkinetic dysarthria
Hyperkinetic disorder: excessive involuntary movement (chorea, myoclonus, dystonia, essential tremor)
Etiology: Basal ganglia injury and areas around the BG (eg Huntington's disease).
Cséfalvay Zsolt, 2007 64
Symptoms of hyperkinetic dysarthria
Involuntary movements of (resp.,
phon., artik., reson.) muscles
Choreatic hyperkinesia –due to
simultaneous or successive
involvement of muscles (lip muscles
and phonation muscles are involved)
Cséfalvay Zsolt, 2007 65
Symptoms of Hyperkinetic dysarthria
CHOREA:
Long intervals between syllables and
words
Variable speech rate
Inadequate breaks (silence)
Variable volume
Prolonged vowels
Fast, and short inhalation, exhalation and phonation intervals
Cséfalvay Zsolt, 2007 66
Hypokinetic dysarthria
Occur due to pathological changes in
BG, their connection with other areas
of CNS
Cséfalvay Zsolt, 2007 67
Etiology of Hypokinetic dysarthria
Parkinson‘s disease
Postencephalopatic parkinsonism
Craniocerebral trauma (BG, substantia nigra)
Cséfalvay Zsolt, 2007 68
Symptoms of hypokinetic
dysarthria
Dysprosodia: monotone speech
(limited vocal range and volume)
Long pauses (due to akinesia)
Fast speech rate.
Cséfalvay Zsolt, 2007
69
Symptoms of hypokinetic dysarthria
Articulation disorder:
"blurry" articulation ,
atypic dysfluency: repetition
(initial phonemes)
palilalia (very fast repetition of
words)
Cséfalvay Zsolt, 2007 70
Symptoms of hypokinetic dysarthria
Dysphonia: Due to incomplete
closure of the vocal cords (breathy
voice quality, rough, raspy voice)
Mikrophonia: low sound level
Respiratory disorder: rapid, shallow
breathing
Resonance abnormalities: mild
symptoms (hypernasality)
Cséfalvay Zsolt, 2007 71
Mixed dysarthria
Etiology:
Sclerosis multiplex/multiple scerosis
Multisystemic atrophy (Shy-Drager sy, progressive supranuklear paralysis, olivopontocerebellar atrophy
ALS
Wilson's disease
Cséfalvay Zsolt, 2007 72
Symptoms of mixed dysarthria
SM: ataxic-spastic form (phonatio-
articulation disorder)
Wilson‘s disease (BG involvement)
hypokinetic form, later spastic-
ataxic form
ALS: initial stage
Cséfalvay Zsolt, 2007 73
How we can identify motor
speech disorders? Tests Frenchay Dysarthria Test
Apraxia Battery for Adults-2nd edition
Assessment of Intelligibility in Dysarthric Speakers (AIDS) (computerized version called CAIDS)
Sentence Intelligibility Test
TOCS+ for children by Megan Hodge is this website:
http://www.tocs.plus.ualberta.ca/videodemo.htm
These testing procedures are not adapted in Hungary for motor speech disorders
74
Diagnostic
A comprehensive assessment of communication disorder following a detailed diagnostic protocol
At present, the differential diagnosis is based on the professional perceptual, acoustic monitoring, psychological testing as there are no objective acoustic and physiological indicators available
The diagnosis itself should include the damage rate, the rate of mistakes, the rate of "false positive" responses and the rate of corrections
75
Diagnostic process
Assessment of the oral motorium
Testing of phonatio and prolong phonatio
The examination shall include, detailed diagnostics of the individual subsystems: respiration, phonation, resonance, articulation and prosody
Cognitive / Communication Skills Mapping
observe compensatory strategies used by patients
76
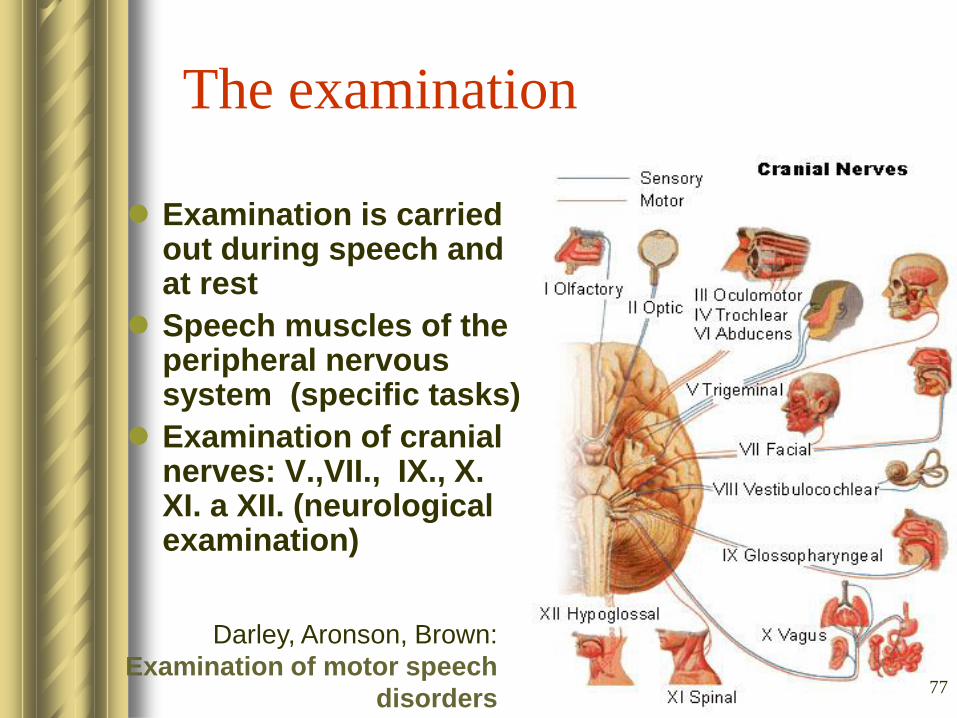
The examination
Examination is carried out during speech and at rest
Speech muscles of the peripheral nervous system (specific tasks)
Examination of cranial nerves: V.,VII., IX., X. XI. a XII. (neurological examination)
Darley, Aronson, Brown:
Examination of motor speech
disorders 77
Examination of the facial muscles at
rest (VII. n. facialis)
Is the face symmetrical?
Can you move your lips?
Can you show your teeth?
Eyes:open,or partially shut?
The face rigid, mask-like?
Are forehead muscles symmetrical
when raising
eyebrows/wrinkling/frowning?
Is the nose symmetrical?
78
Examination the facial muscles in
motion (VII. n. facialis)
Is the smile symmetrical?
Looking for the right position when smiling (apraxia?)
Pouching of lips
Close lips
Puffing up cheeks
Muscle strength
79
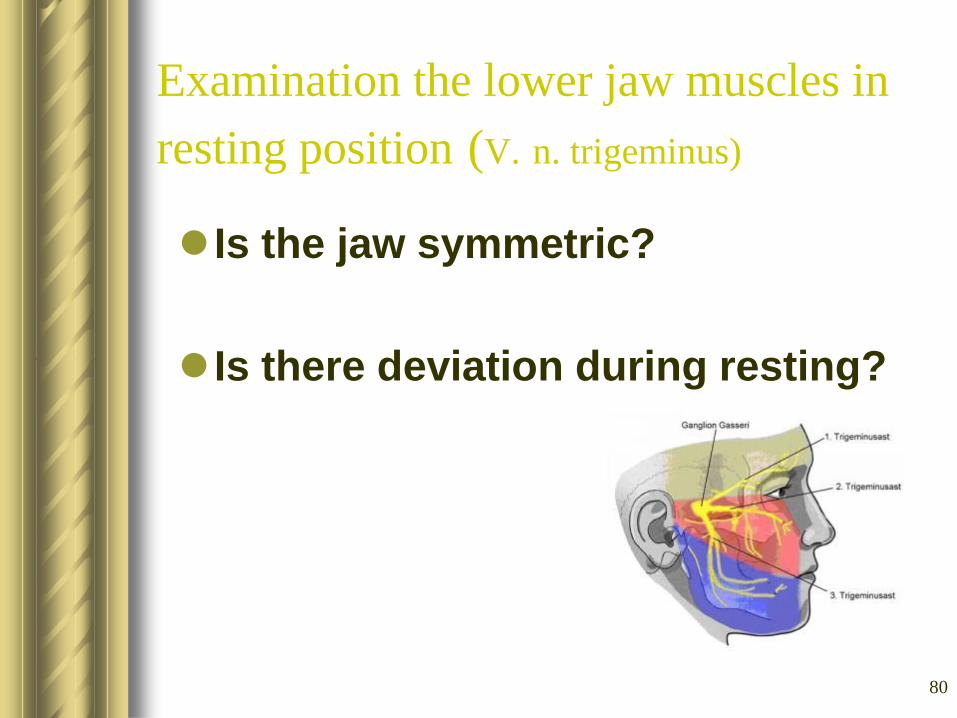
Examination the lower jaw muscles in
resting position (V. n. trigeminus)
Is the jaw symmetric?
Is there deviation during resting?
80
Examination of the lower jaw muscles
during spontaneous movements
There is a deviation jaw when the
mouth is open?
Looking for the right position whilst
opening (apraxia)?
Is there possible side movement?
Is there strong resistance against
pressure?
81
Examination of the tongue muscles at
rest (XII. n. hypoglossus)
Is the size and shape of the tongue normal?
In the located in the middle of the mouth?
Is the shape of the tongue symmetrical?
Is there fasciculation muscle of the tongue?
Can it remain inactive?
82
The examination of the tongue muscle
movements (XII. n. hypoglossus)
Can the tongue move out?
Can the patient stick his tongue out?
Can he resist lateral pressure to the tongue?
Can patient produce lateral movements?
83
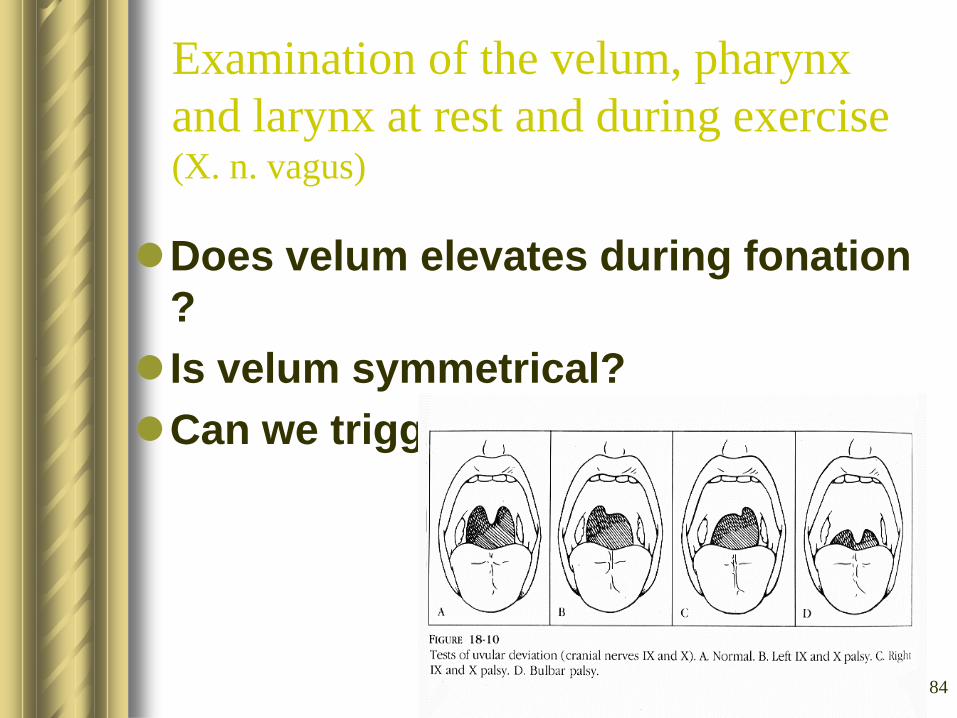
Examination of the velum, pharynx
and larynx at rest and during exercise (X. n. vagus)
Does velum elevates during fonation
?
Is velum symmetrical?
Can we trigger gag reflex?
84
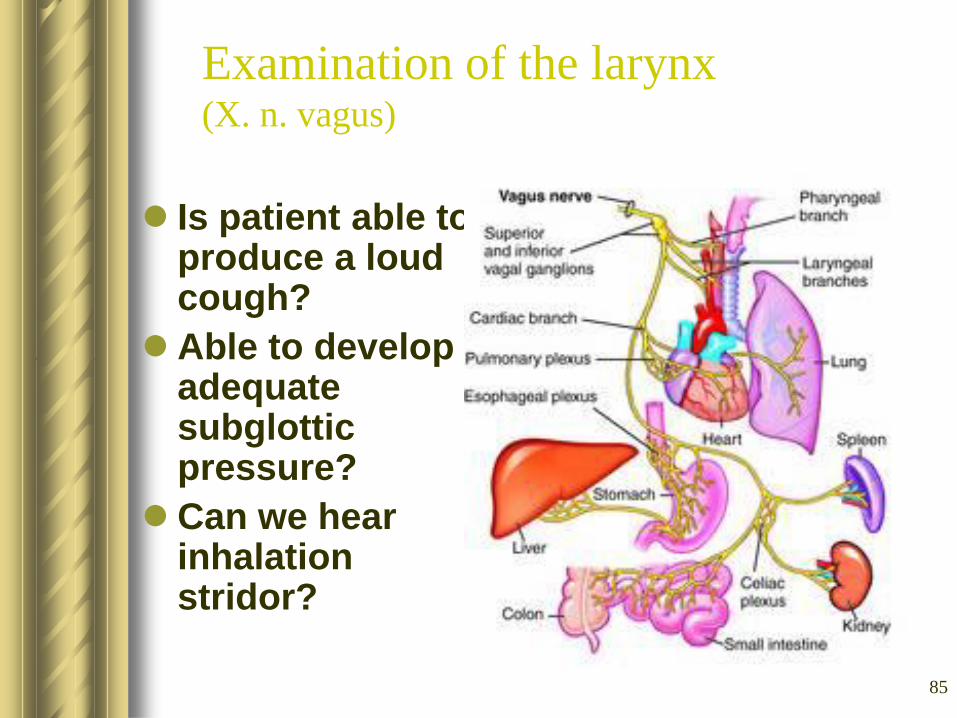
Examination of the larynx (X. n. vagus)
Is patient able to produce a loud cough?
Able to develop adequate subglottic pressure?
Can we hear inhalation stridor?
85
Summary
Must be able to distinguish between disorder of motor planning (apraxia) and disorder of motor execution (dysarthria)
Dysarthria: we must be able to determine the type of dysarthria
Be able to determine how damage to the motor subsystems affect intelligibility of speech
We have to know if the disease is acquired or developmental
Disorder emerged suddenly or gradually
Set up the treatment plan accordingly
86
From diagnosis to therapy
A detailed diagnostic protocol is an opportunity for better trauma-specific treatment plan
87
Vocalization and swallowing
Lungs provides air flow
Glottis: vocal phonation and
positioning
Resonator areas: synchronized
orientation
Swallow: Preoral, oral, pharyngeal
and oesophageal stages
Swallowing apnea, opening the top
of the esophagus 88
Dysphonias
Organic dysphonia
Functional dysphonia
89
Functional dysphonia
Change in the tone (usually hoarseness),
overuse of voice, larynx is less strainable
without primary structural difference in
the larynx itself. All complaints are
usually accompanied by paresthesia
Phonoponozis
Phononeurosis
Mészáros Krisztina 90
Phonoponozis I.
Definition:
Improper use of sounds, vocal
dysfunction due to overuse of the
phonatory apparatus
Mészáros Krisztina 91
Phonoponozis II.
Complaints:
Gradually formed, altered, hoarse
voice, becomes asymptomatic after
relaxing, urged to croak and
swallowing, globus sensation,
foreign body sensation, pain
sensation in the neck, sore throat,
and cough.
Mészáros Krisztina 92
Phonoponozis III. Symptoms: Changed, usually hoarse voice, but not
aphonic. Hard start-up sound, almost normal range of voice, prolonged sound shorter, limited volume.
Decreased, tight vocal movements, irregular, tight thoracic breathing. Face, tongue, jaw, neck under tension, neck veins visible during speech.
Larynx: false vocal cords distend due to straining, congestion in free margins of the vocal cords.
vocal knots, margin oedema appear, and failure of glottic closure at the back of the larynx
Mészáros Krisztina 93
Phonoponozis IV.
Treatment:
Voice Therapy and in cases of
existing tough vocal cord knots ,
surgical removal is recommended.
Mészáros Krisztina 94
Juvenilis dysphonia I.
Definition:
Formed in childhood, improper voice
use, excessive use of the phonation
apparatus due to vocal dysfunction.
Mészáros Krisztina 95
Juvenilis dysphonia II.
Complaints:
Hoarseness, deepening of the voice,
croaking
Mészáros Krisztina 96
Juvenilis dysphonia III.
Symptoms:
A sharp, deep-pitched, hoarse voice. Urge to croak, hard starting volume. Fast speech, rhythm, inaccurate articulation, irregular, tight thoracic breathing. Face, tongue, jaw, neck are tense, neck veins distended during speech.
Larynx: loose watery vocal cords, vocal bunch knots, failure of glottic closure.
Mészáros Krisztina 97
Juvenilis dysphonia IV.
Treatment:
Voice therapy and in cases of
existing tough vocal cord knots,
surgical removal is recommended.
Mészáros Krisztina 98
Phononeurosis
Voice production disorder of psychogenic origin, sudden and severe voice symptoms.
Psychogenic aphonia: inability to produce sounds, immediate psychiatric treatment and voice therapy.
Mészáros Krisztina 99
Dysodia
The functional voice disorders.
Respiratory defects
Incorrect setting of the articulation area
4-6 hours of overstraining
Caffeine, drugs
Early singing lessons
Ignoring vocal hygene recommendations
Mészáros Krisztina 100
Gastro-oesophageal reflux
disease in phoniatry
implications
101
The most common aspects in phoniatry
of the GERD
Dysphonia
Pharyngitis
Dysphagia
excess flow of mucus in the back of throat
Stimulated cough
Chronic Bronch.
Asthma bronch.
Mészáros Krisztina 102
Top phoniatric result
Hoarseness
Etiology:
The acid-induced vagal reflex
triggered recurrent coughing reflex.
There is direct acid effect on the
pharynx, larynx.
Mészáros Krisztina 103
Diagnostic, anamnesis
Substernal burning
sensation, pain
Nocturnal
regurgitation
Coughing, wheezing
Aspiration
Morning hoarseness
Croaking
Feeling of mucus
flow in the throat
Frequent throat
pains
Jugular
discomfort
Heartburn (rarely)
Mészáros Krisztina 104
Diagnostic, examination
oto-nasal laryngological
examination
laryngial video-stroboscopy
Auditory Sound Scan
examination of sound retention
time and vocal range
Analysis of sound dynamics 105
Stroboscop evidence
The congestion of inter-ary region of the
vocal cords, false vocal cords slight
oedema of the vocal cords.
Pronounced hyperplasia of the inter-ary
region, contact granuloma.
In general, the glottis level of
vasoconstriction, decreased vocal cord
vibration parameters, harsh sound start.
In addition to harsh sound start,
hypotonic vibration in front of the vocal
cords
Mészáros Krisztina 106
GERD and the phoniatry
Varying degrees of hoarseness
Vocal holding time shortens
Sound stage renal
Decreased ability of raising volume
20% of phoniatric patients affected
by clinical symptoms, 14% was
proven in during gastroenterologic
examination
Mészáros Krisztina
107
Treatment
Gastroenterology areas: Medication
and lifestyle counseling.
Phoniatric Therapy: Sound Therapy
treatment to the added functional
components.
Mészáros Krisztina
108
Thank you
for your
attention!
109