Embed Size (px)
Citation preview

David C. Metz, MD
Neuroendocrine Tumors: The GI PerspectiveGI Perspective
David C. Metz, MDProfessor of Medicine
Perelman School of Medicine at the University of Pennsylvania
Neuroendocrine Tumors
• Second most prevalent cancer of the GI tract b hi d l t l 1behind colorectal cancer1
• Over 100,000 patients are living with NETs in the United States
• Principles of care are different/uniquePrinciples of care are different/unique compared to other solid tumors
JC et al. One hundred years after "Carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008;26 ::3063–72.
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
1

David C. Metz, MD
Neuroendocrine Terminology
• Neuroendocrine tumors include carcinoid tumors and pancreatic neuroendocrine tumors (PNETs)and pancreatic neuroendocrine tumors (PNETs)
• Carcinoid tumors are in the alimentary tract or elsewhere (lung, thymus, testis ovary, etc); PNETs are in the pancreas
• Carcinoid tumors may be functional (carcinoid syndrome) or non-functional
• PNETs may be functional (various types) or non-functional
• Functional syndromes require production of biologically active amines
Incidence of Neuroendocrine TumorsOver Time is IncreasingAnalysis of SEER database (1973–2004)1
Yao JC et al. One hundred years after "Carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008;26(18):3063–72.
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
2

David C. Metz, MD
Classic vs NET Tumor Size Paradigm
Lymph Nodes
Metastases
Primary
Classic solid tumor Neuroendocrine tumor
Grade and Differentiation• GRADE refers to pathologic features of growth rate
– Mitoses or Ki 67 staining (biologic aggressiveness)• DIFFERENTIATION refers to pathologic features ofDIFFERENTIATION refers to pathologic features of
malignancy – Histologic appearance (degree of resemblance to normal)
• Grade and differentiation are related but not equal• Biological behavior of low or Intermediate grade• Biological behavior of low or Intermediate grade
well differentiated tumors can only be determined clinically during follow up
Kulke, MH. Pancreas 2010;39:735-52. Klimstra, DS. Pancreas 2010;39:707-12
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
3

David C. Metz, MD
Pathologic Classification of NETs
Differentiation Grade Frequency Comments
Well Low Common <2 mitoses/10hpf Low Ki 67
Variable prognosis
Intermediate Less common Intermediate prognosis
Poor High Rare Poor prognosis
Klimstra, DS. Pancreas 2010;39:707-12
Hereditary vs. Sporadic
• Multiple Endocrine Neoplasia syndrome type 1
• Three of the five phacomatoses– Von Hippel-Lindau (VHL)
• PETs (non-functional >>insulinoma/vipoma) in 12-17%– Von Recklinghausen’s disease (NF-1)
• Occasional duodenal somatostatinomas (often non-functional) >>insulinoma/gastrinomas) g
– Tuberous sclerosis • Rare PETs (non-functional, insulinomas/gastrinomas)
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
4

David C. Metz, MD
MEN-1 Syndrome
• Multiple Endocrine Neoplasia syndrome type 1A t l d i t (K d ’ t hit• Autosomal dominant (Knudsen’s two hit hypothesis; retinoblastoma)
• Gene cloned (11q13), product Menin• 3 P’s: Parathyroid hyperplasia (early)
Pituitary adenomas (Prolactinoma, Cushings)
Entero-Pancreatic tumorsOthers: Lipomas, adrenal hyperplasia, etc
Biochemical Products• Functional products
– Carcinoid syndrome• Serotonin, 5HIAA, 5HTP, substance P, kallikrein, etc
P ti d i t– Pancreatic endocrine tumors• Gastrin• Insulin• VIP• Others (glucagon, somatostatin, etc)
– Utility• Syndrome diagnosis and to monitor hormonal therapy
N d i k• Neuroendocrine markers– Chromogranin A– Others (pancreatic polypeptide, bHCG, etc)– Utility
• Tumor diagnosis and to monitor growth or anti-tumor therapy
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
5

David C. Metz, MD
Functional NET Syndromes• Carcinoid syndrome
– Flushing, diarrhea, wheezing, pellagra, cardiac disease• Zollinger-Ellison syndrome (Gastrinoma)
– Gastric acid hypersecretion (pain ulcers diarrhea)Gastric acid hypersecretion (pain, ulcers, diarrhea)• Insulinoma Syndrome
– Neuroglycopenia, sympathetic overdrive, obesity• Glucagonoma
– hyperglycemia, rash (MNE), anemia, hypoaminoacidemia, weight loss, thromoboembolism, glossitis
• VIPoma – watery diarrhea hypokalemia achlorhydria and others (hyperglycemiawatery diarrhea, hypokalemia, achlorhydria and others (hyperglycemia,
hypercalcemia, flushing)• Others:
– ACTHoma – Cushing’s syndrome– GRFoma - acromegaly– Somatostatinoma – hyperglycemia, steatorrhea, gallstones– Rare syndromes (calcium, erythropoeitin, etc)
Octreotide for Functional NETs• Drug of choice for syndrome management
(FDA-approved for carcinoid, VIPoma and acromegaly)acromegaly)
• Role in tumor stabilization established for alimentary tract tumors (Promid)
• Correlate with hormonal measurements in nadir– Functional (24 hr urine)– Structural (CgA)
• Correlate with functional and structural imaging
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
6

David C. Metz, MD
Anatomic Classification of NETs1,2
1. Vinik AI, Renar IP. Neuroendocrine Tumors of Carcinoid Variety. In: De Grool L, ed. Endocrinology. 3rd ed. Philadelphia, PA: WB Saunders; 1995:2803–14.2. NCCN Clinical Practice Guidelines in Oncology: Neuroendocrine Tumors.
13
Gastric Carcinoids and Hypergastrinemia
Carcinoid % total Assoc. Gastrin Acid Sec. Mets
Type I 75 PA/atrophy Inc. Low V. rare
Type II 5-10 ZES/MEN-1 Inc. High Rare
Type III 15 25 None Normal Normal CommonType III 15-25 None Normal Normal Common
Adapted from Metz and Jensen. Chap. 48. In: Gastrointestinal Cancers. 2nd edition. Rustgi AK and Crawford JM, editors. WB Saunders, Philadelphia, PA. 2001; pp681
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
7

David C. Metz, MD
Midgut Carcinoids
Location Multiplicity Functional Surgically curable
Ileal Yes Yes (mets) Rarely (mets)
Appendiceal No Rarely Yes (esp <1-2 cm)pp y ( p )
Isac. Acta Oncol 2003;42:672. and Yantiss. Am J Surg Pathol 2003;27:811
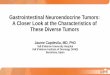
Extent of Disease at Diagnosis Diagnosis is often delayed 5–7 years on average, and the
probability of metastatic disease at diagnosis is increased1
5%4% 28% 30%
92%
49%
23%
29%
41%
The median age of diagnosis for NETs of the rectum is 56 years, for NETs of the lung is 64 years, and for NETs of the jejunum/ileum is 66 years2
1. Modlin IM et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol 2008;9:61–72.2. Yao JC et al. One hundred years after “Carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in
the United States. J Clin Oncol 2008;26:3063–72.
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
8

David C. Metz, MD
Staging of Disease
• Imaging– Cross sectional studies (CT/MRI)– Functional Imaging (Octeoscan/MIBG scan)
• Endoscopy– Optical (EGD/Colonoscopy)
Capsule Endoscopy– Capsule Endoscopy– Deep Enteroscopy (Spiral/Single-/double Balloon)– Endosonography (EUS-PNETs)
EGD
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
9

David C. Metz, MD
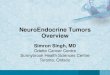
Colonoscopy
Photographs courtesy David Jaffe, MD
Capsule Endoscopy
Liang PS et al. Radiol Case Rep. 2007;2:90.
Two endoscopic images that may show the location of the patient’s primary tumor in the submucosa
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
10

David C. Metz, MD
Fluoroscopic Results
AnterogradeAnterograde routeroute Retrograde routeRetrograde routeImages courtesy David Jaffe, MD
Primary Tumor IdentificationMRI EUS Octreoscan
Metz DC. Gastroenterology 2008;135:1469-1492Kwekkeboom DJ. Neuroendocrinology 2009;90:184-189
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
11

David C. Metz, MD
Liver MetastasesCT MRI Octreoscan
SensitivitySensitivity 80-90% 80-95% >90%
Sundin A. Neuroendocrinology 2009;90:167-183Schillaci O. J Nucl Med 2003;44:359-368
68 Ga Octreotide PET Imaging with CT fusion: Imaging of the future
Photographs Courtesy Kjell Oberg, MD
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
12

David C. Metz, MD
Management Principles
• Confirm the diagnosisC t l th h l d (if t)• Control the hormonal syndrome (if present)
• Determine extent of disease• Consider surgery
– For cure (if possible) – For debulking (if not)
• Long term management– Hormonal syndrome (if present)– Growth
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
13

David C. Metz, MD
Management Principles (Cont.)• Management is multidisciplinary
– Medicine (GI, endocrine, oncology)ed c e (G , e doc e, o co ogy)– Surgery– Radiology (XRT, IR)
• Non-surgical therapy should not be squandered– Wait for symptoms or evidence of rapid growth
Therapy for Metastatic Disease: Limited Options
• Watch (especially if asymptomatic)Octreotide (? retards growth)• Octreotide (? retards growth)
• Chemotherapy (temporizing, PNETs>> GI NETs)– Streptozotocin, capecitabine/temozolomide
• Small molecules– Everolimus, sunitinib
• PRRT (experimental)• PRRT (experimental)– Yttrium or lutetium octreotide/tate
• Regional therapy (XRT to bone, chemoembocryotherapy, yttrium beads, etc)
• Transplantation (difficult to qualify)
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
14

David C. Metz, MD
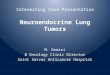
PROMID: Time to Progression
Rinke A, et al. J Clin Oncol 2009;27:4656-63
Other Methods of Debulking
Interventional RadiologyCh /bl d b li i• Chemo/bland embolization
• Radioactive beads• Radiofrequency ablation
SurgerySurgery• Transplantation (controversial)
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
15

David C. Metz, MD
Systemic Therapies• Radioactive
– MIBG– MIBG– PRRT
• Chemotherapy• Small molecules
(PNETs)Sunitinib– Sunitinib
– Everolimus– Many more to
come
Managing the Effects of Therapy
• Pancreatic resections (Distal or Whipple’s)
• OctreotideGallstones(Distal or Whipple s)
– Pancreatic insufficiency– Dumping syndrome– Diabetes– Immunity (spleen)
– Gallstones– Steatorrhea
• Others– Adhesions
• Terminal ileal resection– B12 deficiency– Bile Salt Diarrhea– Overgrowth
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
16

David C. Metz, MD
Multidisciplinary Care is Ideal• Many options and no standard algorithm
exists (therapy should be individualized)• Tumor Board is ESSENTIAL component• Tumor Board is ESSENTIAL component• Flexibility is KEY
Conclusions
• NETS come in many different flavors but h l t f f t ihave lots of features in common
• They differ in many important ways from other more typical solid malignancies
• Management requires consideration of both functionality and tumor growthboth functionality and tumor growth
• Multidisciplinary care is the norm
ACG Board of Governors/ASGE Best Practices Course - Las Vegas, NV Copyright 2014 American College of Gastroenterology
17