Embed Size (px)
Citation preview

International Journal of Cognitive Therapy, 4(1), 34–50, 2011© 2011 International Association for Cognitive Psychotherapy
34
Address correspondence to Marc E. Lavoie, Ph.D Associate research professor of Psychiatry. Université de Montréal. Centre de Recherche Fernand Seguin, Louis-H Lafontaine Hospital. 7331 Hochelaga Street , Montréal, QC. Canada, H1N 3V2. E–mail: [email protected] work was supported by a Canadian Institutes of Health Research (CIHR) operating grant (MOP57936) and a Fonds pour la Recherche en Santé du Québec (FRSQ) clinical research grant (5271) awarded to MEL, KPO, and ES. We wish to express our gratitude to Marie-Claude Pélissier, Frederic Aardema, Anick Laverdure, Ariane Fontaine, and Valérie Poulin for research coordination and clinical screening to Martine Germain for electrophysiological recordings, and Geneviéve Thibault, Sophie Lecourse, Maria-Teresa Her-nandez, Cathy Léveillé, and Anne-Marie Daost for neuropsychometric testings. At last but not the least, we thank all participants for their precious contribution in this study.
LAVOIE ET AL.CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME
Neurocognitive Changes Following Cognitive-Behavioral Treatment in Tourette Syndrome and Chronic Tic DisorderMarc E. Lavoie, Tina V. Imbriglio, and Emmanuel StipUniversité de Montréal, Canada
Centre de Recherche Fernand-Seguin de l’Hôpital Louis-H Lafontaine
Kieron P. O’ConnorUniversité de Montréal, Canada
Université du Québec en Outaouais, Canada
Centre de Recherche Fernand-Seguin de l’Hôpital Louis-H Lafontaine
Gilles de la Tourette Syndrome (GTS) is a neuropsychiatric disorder characterized by multiple fluctuating motor tics and one or more phonic tics. Various treat-ments have been administered with limited success to patients with GTS. For more than 40 years, the medication of choice has generally been neuroleptic medication. However, unwanted side effects often occur. For those patients, Cognitive-Behav-ioral Therapies (CBT) have shown some success. CBT is considered an effective adjunct to medication, but the cognitive and cerebral effect of CBT has not so far been explored within a GTS population. The current research focuses on the hypothesis that significant symptom improvements in GTS, following CBT, will relate to cerebral activity changes. The aim of our research program was to compare motor Event-Related Potentials (ERP) recorded pre- and post-CBT in a popula-tion of GTS. We recorded the electroencephalogram (EEG) and derived the ERPs of 10 GTS patients, matched with 14 controls on the basis of laterality, age and in-telligence. A traffic light task was administered to extract ERPs related to response processing. Results revealed that GTS had reduced cortical activation related to the inhibition of responses, which normalized following CBT. The treatment may induce cerebral changes that significantly improve both motor performances and brain activity.

CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 35
definition and ePideMiology of gts
Gilles de la Tourette Syndrome (GTS) is named after the French neurologist Georges Gilles de la Tourette, who, in 1885, described the condition in an 86-year-old French noblewoman, whom showed abrupt movements and sounds also known as tics (Gilles de la Tourette, 1885). The same year, Tourette also described nine patients with motor and vocal tics, some of who had echo phenomena (a tendency to repeat things said to them) and coprolalia (utterances of obscene phrases). The essential features of GTS are the presence of simple or complex multiple motor tics and one or more vocal tics. GTS is classified with disorders first diagnosed in infancy, childhood, or adolescence (Amer-ican Psychiatric Association, 2000). Simple tics are defined as repetitive non-voluntary contractions of functionally related groups of skeletal muscles in one or more parts of the body including blinking, cheek twitches, head or knee jerks, and shoulder shrugs (Leckman et al., 1997; Shapiro & Shapiro, 1986). Complex tics or habit disorders may take the form of self-inflicted repetitive actions such as nail biting, hair pulling, head slapping, face scratching, teeth grinding, tense-release hand gripping cycles, or finger twiddling. The tics appear many times a day with onset longer than a year and prior to 18 years of age. The Diagnostic and Statistical Manual of Psychiatric Disorders Text-Revised version (American Psychiatric Association, 2000), distinguishes between chronic tic disorder with one principal motor or phonic tic and GTS, with multiple tics and at least one phonic tic. There has been controversy about current criteria for GTS (Tourette Syndrome Study Group, 1993), but the diagnosis is currently dichotomous, not dimensional, and depends crucially on the existence of a phonic tic. However, cli-nician consensus suggests a continuum of severity, in particular between chronic mo-tor tic disorder and GTS (O’Connor, Brisebois, Brault, Robillard, & Loiselle, 2002; O’Connor, Brault, Robillard, Loiselle, Borgeat, & Stip, 2001)
The onset of symptoms starts early in childhood and GTS appears more frequent-ly in boys. Kadesjo & Gillberg (2000) found that, depending on the sample charac-teristics between 0.15% and 1.1% of all children had GTS and boys outnumbered girls by 4:1 through 6:1. The tic symptoms have a tendency to decrease with age. In a longitudinal cohort of 36 patients with GTS, it was found that the most severe period of tic severity occurred at 10 years of age (Leckman et al., 1998). In almost every case, this period was followed by a steady decline in tic severity. At adulthood, nearly half of the cohort was tic-free. Nevertheless, 11% of adults with tics, remain with moderate or marked level of tic severity (Bloch et al., 2006; Leckman et al., 1998) and follow-up studies revealed that adults with GTS are more severely impaired in daily life (Walkup et al., 1988). The expression of tics is part of a larger portrait of comorbid symptoms. Freeman et al. (2000) showed that anger control problems, sleep difficulties, coprola-lia, and self-injurious behavior, attain high levels in individuals with GTS, particularly those with comorbidity. The most commonly reported comorbidity, in GTS, is atten-tion deficit hyperactivity disorder (ADHD), which is also associated with reduced inhibition at multiple levels in the motor system (Hallett, 2001).
36 LAVOIE ET AL.
neuRocognitive etiology and behavioRal exPRession of gts
Understanding of this syndrome requires a multidimensional approach, ranging from clinical psychology to cognitive neuroscience. For instance, in addition to the nu-merous behavioral problems cited above, several neuropsychological studies have un-covered cognitive specificities in GTS such as deficits in learning for mathematics and written language (Brookshire et al., 1994; Como, 2001), verbal fluency (Born-stein, 1991; Brookshire, et al., 1994), fine motor coordination (Bornstein, Baker, Bazylewich, & Douglass, 1991; Bornstein, King, & Carroll, 1983; Brookshire, et al., 1994; Como, 2001; O’Connor, Lavoie, Stip, Borgeat, & Laverdure, 2008) and a nonverbal memory deficit associated with a visuoperceptual integration difficulty, in groups of children (Harris et al., 1995; Schuerholz, Baumgardner, Singer, Reiss, & Denckla, 1996) and adults (Lavoie, Thibault, Stip, & O’Connor, 2007). Moreover, earlier studies have reported that children with GTS achieved normal performances on tasks evaluating abstract concepts (Bornstein, 1990; Bornstein & Baker, 1991; Braun et al., 1993; Harris et al., 1995; Schuerholz et al., 1996), planning and response inhibition (Ozonoff & Jensen, 1999) as well as verbal fluency (Braun, et al., 1993; Mahone, Koth, Cutting, Singer, & Denckla, 2001), while other studies have proposed a plethora of other executive function impairments (Baron-Cohen, Cross, Crowson, & Robertson, 1994; Bornstein, et al., 1983; Brookshire, et al., 1994; Schuerholz, et al., 1996; Sutherland, Kolb, Schoel, Whishaw, & Davies, 1982). The lack of consis-tency or specificity in the neuropsychological results could be due to methodological problems considering that, in some cases, studies did not include a control group or did not control for the presence of comorbid disorders, such as attention deficit hyper-activity disorders (ADHD) or obsessive-compulsive disorders (OCD). The presence of ADHD or OCD symptoms in children often leads to poorer performance on execu-tive tasks (Bornstein, 1990; Harris, et al., 1995).
Despite this, there is relative consistency in the reports of a fine motor dexterity and a visuo-motor integration deficit in both children and adults with chronic GTS. Neurobiological hypotheses have centered on basal ganglia dysfunction similar to other movement disorders; in particular the orbital-frontal-basal ganglia loop (Casey, Tottenham, & Fossella, 2002). Another hypothesis is that GTSs show abnormally high levels of sensorimotor activation. This could cause problems with visuo-motor coordination, chronic muscle tension, and overgeneralized responding (O’Connor, Brisebois, Brault, Robillard, & Loiselle, 2002; O’Connor, 2002). This hypothesis also partially accounts for the success of relaxation and habit reversal techniques in tic man-agement (Peterson & Azrin, 1992).
Despite recent advances in the understanding of GTS etiology, neurobiologi-cal and cognitive factors have mostly been addressed independently. For this reason, brain Event-Related Potentials (ERPs) recording techniques constitute a useful tool for monitoring cerebral activity recorded in synchrony with cognitive events. Earlier investigations have found anomalies in motor ERPs with patients suffering from GTS and chronic tics. For instance, the Bereitschaftpotential (BP), or readiness potential, was consistently larger over frontal and smaller over central areas in the GTS group (Rothenberger & Kemmerling, 1982; Rothenberger, Schenk, Zerbin, & Voss, 1986). In a more recent ERP study, chronic tic disorder patients failed to demonstrate a normal relationship between motor responses and preparation of cortical activation
CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 37
(i.e., BP) during a foreperiod reaction time task (O’Connor, Lavoie, Robert, Stip, & Borgeat, 2005), supporting the hypothesis that people with tic disorders may not be able to modulate cortical activation optimally when planning and executing motor responses.
tReatMent issues in gts
Various treatments have been administered with limited success to patients with GTS. Since the discovery of Seignot (1961), the medication of choice is generally small doses of neuroleptic medication such as Haloperidol or Risperidone (Dion, Annable, Sandor, & Chouinard, 2002). This approach stems from a tentative neurobiological model of dopamine dysregulation (Ernst et al., 1999; Singer, Hahn, & Moran, 1991; Singer et al., 2002). Pharmacological agents that increase dopamine functioning such as L-dopa, stimulant medication (Golden, 1977), or neuroleptic withdrawal (Riddle, Hardin, Towbin, Leckman, & Cohen, 1987) exacerbate GTS symptoms. Conversely, drugs that lower or block the action of dopamine including typical (Shapiro et al., 1989) and atypical (Lombroso et al., 1995) neuroleptics tend to improve GTS symp-toms. Double-blind controlled designs have found tic frequencies reduction of about 50% using typical neuroleptics such as Haloperidol or Pimozide (Sallee, Nesbitt, Jack-son, Sine, & Sethuraman, 1997).
However, unwanted side effect occur in about 80% of individuals and Peterson, Campise, and Azrin (1994) estimate that only about 20-30% of clients continue their medication for an extended period of time. Alternative treatments have shown some mixed success with tic management, including hypnotism, relaxation, muscle feed-back, awareness training, negative reinforcement, response prevention, and massed practice (Bergin, Waranch, Brown, Carson, & Singer, 1998; 1992). Therapeutic in-terventions target not only tic symptoms, but also coping strategies that can modify the unique impact that GTS symptoms may have on an individual’s well-being (Peter-son & Cohen, 1998). The most compelling treatment medium for managing the tics themselves seems to be behavioral treatment, in particular “habit reversal” (HR; Azrin & Peterson, 1988; Himle & Woods, 2005). This package involves multiple stages, including relaxation, awareness, contingency training, and positive reinforcement of not ticcing and the crucial element of practice of a competitive antagonistic response. This latter technique involves tensing the muscle antithetical and incompatible with the tic-implicated muscle. Awareness training and competing response training seem the most crucial elements of the program (Miltenberger & Veltum, 1988), which can be applied to tic disorders. Azrin and Peterson (1988) report an improvement of between 64-100% in several studies using this method in populations with both simple tics and/or GTS. Peterson and Azrin (1992) compared the efficacy of aware-ness, relaxation, and HR in 6 participants using a within participants design. HR produced the largest overall reduction in tics (55%) and led to the largest reduction in total tics (95%) for any individual, but there was no significant difference between treatments. In a sample of four children with GTS, Woods, Miltenberger, and Lumley (1996) also demonstrated that the combined use of awareness training, social support, and competing response training was effective in eliminating motor tics. In a wait-list controlled treatment trial with adults, a cognitive-behavioral package partly based on HR showed significant posttreatment clinical improvement for 52% of the patients (O’Connor, Brault, Robillard, Loiselle, Borgeat, & Stip, 2001). Despite its utility,

38 LAVOIE ET AL.
HR is a multimodal treatment applying distinct components and the psychological processes involved are unclear. Notwithstanding an interesting effort to use neuropsy-chological predictors of HR and tic suppression (Woods et al., 2008), there has been no direct attempts to measure whether CBT could modulate GTS patients’ informa-tion processing and furthermore, how clinical and cognitive improvement could affect cerebral activity following CBT.
tReatMent issues and neuRoPlasticity in PsychiatRy
Several studies in the neuroimaging literature support the thesis that with appropri-ate training, people can alter cerebral activity associated with a variety of pathological mental states (see Cozolino, 2002). Such studies have already demonstrated a relation-ship between successful psychotherapy and neuroplasticity also termed “self-directed neuroplasticity” (Schwartz & Begley, 2002).
For instance, earlier works on patients with OCD demonstrated significant changes in caudate nucleus metabolism and the functional relationships of the orbito-frontal cortex–striatum–thalamus loop in patients who responded to a psychological treatment. Using PET imaging, Baxter et al. (1992) found a decrease in the glu-cose metabolic rate in the right head of the caudate nucleus, when people with OCD were treated successfully with Fluoxetine or CBT. Another investigation (Brody et al., 1998) suggested that participants with differing patterns of metabolism preferentially respond to CBT versus medication. Left orbital-frontal cortex metabolism alone pre-dicted treatment response in the CBT treated group. A strong relationship has also been found between symptom reduction following CBT and brain glucose metabo-lism normalization in OCD. A recent PET study by Saxena et al. (2008) revealed that compared with controls, people with OCD showed significant bilateral decreases in thalamic metabolism following intensive CBT, but had a significant increase in right dorsal anterior cingulate cortex activity which correlated strongly with the degree of improvement in OCD symptoms.
In other anxiety disorders, significant changes occurred in the dorsolateral pre-frontal cortex and parahippocampal gyrus after CBT for arachnophobia (i.e., phobia of spiders), with brain metabolic changes significantly related to both objective mea-surements and subjective reports of fear and aversion (Paquette et al., 2003). Another series of investigations with Posttraumatic Stress Disorder (PTSD) individuals also showed that better response to CBT was associated with larger right anterior cingulate cortex (ACC) volume (Felmingham et al., 2007). Whereas treatment responders were characterized by right ACC volume that was comparable to that of control subjects without PTSD, future nonresponders were distinguished by smaller right ACC vol-ume (Bryant, Felmingham, Kemp, et al., 2008; Bryant, Felmingham, Whitford, et al., 2008).
Despite these encouraging results with various anxiety and mood disorders, no studies of CBT and neuroplasticity have so far looked at GTS. Our own results have shown that CBT significantly affects response processing, particularly fine motor dex-terity (O’Connor et al., 2008). These results revealed that motor performance differed significantly on the Purdue pegboard tests in GTS as compared to the control group at baseline. CBT selectively improved motor dexterity compared to a wait-list control, and this improvement was related to clinical outcome measures.

CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 39
In summary, pharmacotherapy and CBT focusing on motor regulation can lead to significant clinical improvement. Brain imaging results after CBT and/or pharma-cotherapy, with OCD patients, also suggest strong relationships between altered brain activity and symptom reduction. This type of association has not been examined with a GTS population, but OCD shares several clinical features in common with GTS. In the current study, we investigated the relationships between symptom expression, complex motor processing, and brain activity in GTS before and after CBT in order to examine the impact of CBT on these parameters and how any changes in brain processes relates to a corresponding change in GTS symptomatology.
Method
Participants
All participants (n = 24) were recruited through local newspapers (Tourette group) or from staff members of the L-H Lafontaine hospital (control group). Fourteen control participants were matched for age, education, and gender (Table 1) to a sample of 10 GTS participants. They all had normal visual acuity (Snellen notation system: 11). The pre-CBT diagnosis was made by a certified psychiatrist (E.S.) and a clinical psycholo-gist (supervised by K.O.). The GTS group primarily fulfilled the diagnostic criteria for GTS (307.23: DSM-IV-TR; American Psychiatric Association, 2000). Exclusion criteria for all participants was the presence of diagnoses other than GTS as primary disorders on Axis I of the DSM IV-TR (APA, 2000) or any other diagnosed prob-lems on Axis II. Control participants were screened by questionnaire for psychiatric or neurological disease. Participants currently receiving any other form of behavioral or cognitive treatment were excluded. However, if participants were already receiving medications, for their tic or obsessive-compulsive symptoms, they were admitted on condition that they had been stabilized for at least 3 months. Two participants with GTS received Risperidal to treat their tics, while one was currently receiving Effexor. For these three patients, the medication had been stabilized pre- and post-therapy. The study was approved by the local ethics committee and all participants gave their writ-ten informed consent.
TABLE 1. Demographic Variables for Each Group
Tourette Syndrome (n = 10) Control (σ = 14) Comparisons
Demographic variables Mean σ Mean σ t-test p
Age (years) 40 13 36 11 -0,76 ns
Age at tic onset (years) 8 4 - — — —
Age at worst tic severity 21 16 — — — —
Schooling (years) 15 2,6 15 2,5 -0,58 ns
Raven (percentiles) 75 19 70 21 -0,65 ns
Laterality (right %) 100 — 100 — — ns
Gender (M/F ratio) 7/3 — 9/5 — — ns
Visual acuity (Snellen) 1,3 0,4 1,3 0,4 0,13 ns
Color perception (Ishihara) 10 2,5 11 0,5 0,79 ns
40 LAVOIE ET AL.
clinical assessment
GTS symptoms severity was assessed with the Tourette Syndrome Global Scale (TSGS; Harcherik, Leckman, Detlor, & Cohen, 1984) and the Yale Global Tourette Syndrome Scale (YGTSS; Leckman et al., 1989). Both questionnaires were admin-istered by the clinician via a structured interview. The first TSGS factor rates the na-ture of the tic (i.e., motor or phonic), while the second scale rates the tic complexity. A third scale assesses functional impairment, including behavioral, learning, motor restlessness and occupational problems. According to past research (Leckman, et al., 1989), the inter-rater reliability of the TSGS global score was found to be very good (k = 0.77, p < .001). The YGTSS (Leckman et al., 1989) was administered to assess symptoms demonstrated within the past 7 days, including a report of the history of the tic severity as well as the medication administered during that period if applicable. The YGTSS provides a comprehensive assessment of motor and phonic tics within five dimensions of tic severity: number, frequency, intensity, complexity, and interfer-ence. A separate rating of impairment assesses such issues as academic or occupational impairment, interpersonal difficulties, and negative self-evaluation that may be related to tic behaviors. For our purpose, a composite score (max = 20) specifically related to time without tics and the severity of tics (motor + vocal) was extracted from the YGTSS. Convergent validity of the motor and phonic tic factors is shown by strong correlations between the TSGS and the YGTSS, ranging from r = 0.86 to r = 0.91 (Leckman, et al., 1989). The OC symptoms severity was evaluated with the self-rated Yale-Brown Obsessive-Compulsive Scale (Y-BOCS; Goodman et al., 1989) for the clinical group. Other studies confirm the validity and reliability of the scales (internal consistency = 0.91-0.94, r = 0.90; Y-BOCS; Goodman, et al., 1989; Steketee, 1994; Taylor, 1995). Concomitantly, the self-rated Padua inventory (Sanavio, 1988) was also administered to all groups and constitutes a 60-item inventory of obsessions and compulsions. The total scale (α = 0.95) and the subscales (α = 0.75-0.91) are also reliable. The Beck Anxiety Inventory (BAI: Beck, Epstein, Brown, & Steer, 1988), which consists of 21-items relative to anxiety symptom intensity for the last week on a 0–3 scale (α = 0.91). The Beck Depression Inventory (BDI; Beck, Ward, Mendel-son, Mock, & Erbaugh, 1961), which consists of 21-item checklist relative to depres-sion (α = 0.91), was assessed. The Personality Diagnostic Questionnaire-4th Edition (PDQ-4) screened for personality disorders (α = 0.50-0.71) and is consistent with the DSM-IV (Hyler, 1994; Rodgers, Callahan, & Chabrol, 2004; Wilberg, Dammen, & Friis, 2000). Finally, the Anxiety Disorders structured Interview Schedule for DSM-IV (ADIS-IV; Brown, DiNardo, & Barlow, 1994) was administered by the clinician to assess comorbid anxiety disorders.
Cognitive-Behavioral Management Program. The cognitive-behavioral interven-tion followed general principles of habit reversal with the addition of cognitive and behavioral restructuring of approach and style of planning in situations at high risk for ticcing (see handbook of O’Connor, 2005 for more details).
Procedure: the traffic light task
The traffic light paradigm has already been applied to GTS and is described elsewhere (O’Connor et al., 2005). The paradigm allowed us to compare cortical events during
CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 41
the time to initiate an automated and controlled response. It consists of a fixed 4-sec-ond foreperiod reaction time task. The 4-second warning period permitted adequate preparation for controlled and automated responses. The interstimulus interval (ISI) was constant at 4 seconds, and the intertrial interval (ITI) varied randomly between 5 and 15 seconds. After a period of acclimatization of 20 trials, all subjects received two replications of 52 trials, with a short rest period between replications.
Two sets of three lights appeared side by side on a computer screen in the form of traffic lights. One set signaled an automated and the other a controlled response sequence. Each trial began with one of the two yellow READY lights signaling that in 4 seconds, the green GO light would appear and the participant would have to make either a controlled or an automated response. Subsequent to response initiation, on one-half of the trials, a red STOP sign would appear, indicating that the response should be terminated. The automated response was three taps on a lever with the two fingers of the dominant hand (– – –) while the controlled response was three taps of Morse code ‘‘dash-dot-dash’’ (––_––) on another lever, but using the same two fingers of the dominant hand. The controlled response differed solely in motor complexity and was equivalent to the automated response in terms of all other biomechanical and movement parameters. The controlled and automated conditions were presented in random order across trials.
electrophysiological Recordings
All electrophysiological signals were acquired through an analog amplifier (SA In-strumentation Inc., San Diego). Electroencephalogram (EEG) was recorded from 26 tin electrodes, referenced to linked mastoids with impedance kept below 5 KΩ. Elec-trodes, mounted in a nylon cap (ElectroCap International, Eaton, Ohio), were placed according to the guidelines for standard electrode position nomenclature (American EEG Society, 1994). EEG recordings were continuously sampled at 250 Hz and am-plified with a calibrated gain of ±10,000 with high-low pass filter settings at 0.01 and 30 Hz respectively. Electro-oculogram (EOG) was recorded from four bipolar electrodes placed horizontally at the outer canthus of each eye and vertically at infra- and supraorbital position on the right eye, in line with the pupil when looking straight ahead. Stimuli presentation and data acquisition were both controlled by a data acqui-sition program (InstEP Systems, Montréal, Canada) running on two Pentium PCs.
eeg and eRP signal extraction
EOG artifacts contaminating the EEG signal were corrected offline using dynamic re-gression in the frequency domain (Woestenburg method: InstEP-TALO). Remaining epochs exceeding 100 µV and clippings due to amplifiers saturation were eliminated during the averaging procedure. Raw signals were automatically averaged offline, time-locked to the response onset, in a time window from 1000 milliseconds before until 1000 milliseconds after response onset, for each stimulus category (Go-auto-mated | Go-complex | Stop-inhibit). A minimum amount of 20 trials were included in each category to ensure representative averaging. The Movement Associated Po-tentials (MAP) component was scored baseline-to-peak and was defined as the most

42 LAVOIE ET AL.
positive peak comprised between 100 and 400 ms post-response onset (see O’Connor et al., 2005).
Results
demographic and clinical characteristics at baseline
There were no group differences regarding age, education level, gender, and nonverbal intelligence (Table 1). Color perception and visual acuity was also comparable across groups. Group differences were observed on clinical questionnaires and interviews (Table 2). Depression (BDI), anxiety (BAI), and obsession-compulsion (Padua inven-tory) were all significantly higher in GTS than in the control group before CBT. The PDQ-4 also revealed significantly greater personality problems in GTS. However, no participant with GTS met the diagnostic criteria for personality disorders. The ADIS-IV also revealed anxiety disorders as the principle comorbidity in the GTS group, including specific phobia (n = 1), generalized anxiety disorders (n = 1) and obsessive-compulsive disorders (n = 2).
Clinical Changes Post-Therapy. The GTS group showed significant reduction in tic frequency as measured by TSGS global score and the YGTSS tic subscales. In addi-tion, improvement of tic symptoms was accompanied by significant changes in elec-trophysiological measures. There were no significant changes in measures of obses-sions, depression or anxiety, but their scores were not in the clinical range at baseline (see table 2).
Clinical Change in Neuropsychological Results. There was a significant difference in performance between the TS group and the control subjects, for the Purdue pegboard, in the number of pegs placed by dominant, non-dominant, and both hands simultane-ously (dominant F[2,139] = 5.52, p < 0.005; non-dominant F[2,139] = 3.56, p < 0.03; both hands F[2, 139] = 8.46, p < 0.001; total F[2, 139] = 8.90, p < 0.001). The controls performed better than the clinical group and placed a greater number of
TABLE 2. Clinical Comparison Pre-Post CBT and Comparison with the Control Group at Pre-CBT
Tourette Syndrome (n = 10) Group Comparisons
Pre-CBT Post-CBTPre-post
comparisonsControl (n = 14) Control vs pre-CBT
Mean σ Mean σPaired t-test p Mean σ
Indepen-dent t-test p
TSGS global score 28 16 12 8 4.39 ** — — — -
YGTSS (tic score) 15 2 12 4 3.35 * — — — -
PDQ-4 (Global personality) 27 16 12 4 2.50 * — — — -
Y-BOCS (Global OCD) 16 7 8 10 2.04 ns — — — -
Padua (Global- OCD) 32 22 37 32 -1,05 ns 12 8 -2,78 **
Beck depression (BDI) 6 5 5 4 1.08 ns 2 2 -3,30 **
Beck anxiety (BAI) 9 5 7 7 0.93 ns 3 3 -3,25 **
Note. Y-BOCS: Yale-Brown Obsessive-Compulsive Scale; PDQ: personality Diagnostic Questionnaire; BDI = Beck Depression Inventory; BAI : Beck Anxiety Inventory; YGTSS: Yale Global Tic Severity Scale; TSGS: Tourette Syndrome Global Scale. *p < .05; ** p < .01.

CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 43
pegs. The Purdue pegboard showed a significant improvement posttreatment for all conditions, F[1,9] = 6.33, p < 0.05.
electrophysiological Results
Group Effects at Baseline. Analysis of the MAP amplitude at pretherapy showed a significant effect of inhibition, F(3, 51) = 6.45; p < 0.001 and an inhibition by re-sponse complexity interaction, F(1, 22) = 3.97; p = 0.05 revealing a larger amplitude to the inhibition of the automated response trials. There was also a group by inhibi-tion interaction, F(3, 51) = 4.88; p < 0.01) and a three-way group by inhibition by hemisphere interaction, F(6,45) = 6, 45; p < 0.02. This interaction revealed a smaller go-stop amplitude difference in the GTS group compared to the control group in the automated response condition, mainly over the left hemisphere. Table 3 reveal that in the automated condition, the MAP amplitude to response inhibition (stop) was significantly correlated with the TSGS global score (left hemisphere electrode r = .81; p < 0.005 / right hemisphere electrode r = .75; p < 0.01). In the complex condition, the correlations were smaller, but remain significant. The MAP amplitude to response inhibition (stop) was correlated with the TSGS global score at both hemisphere (left hemisphere electrode r = .71; p < 0.05/right hemisphere electrode r = .63; p < 0.01).
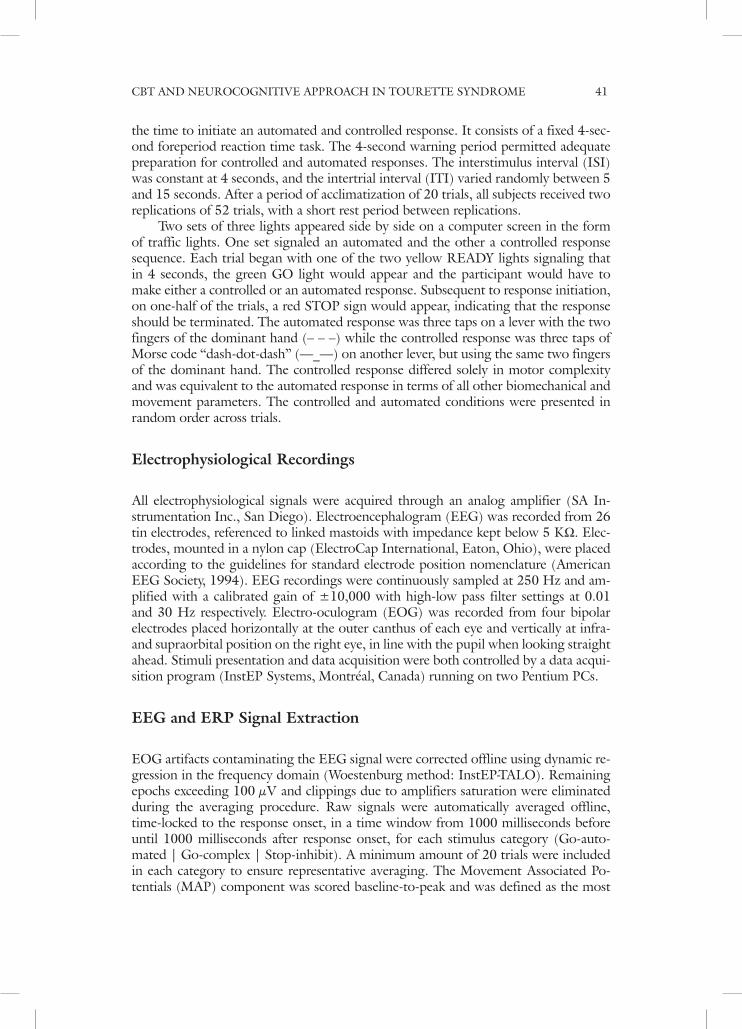
Treatment Effects (see Figure 1). Analysis of the response-locked MAP amplitude comparing pre- and post-CBT results in the GTS group revealed a significant effect of inhibition, F(1, 9) = 31.99; p < 0.001) and a therapy by inhibition interaction, F(1, 9]) = 5.91; p < 0.05). This interaction revealed a significant amplitude enhancement, after CBT, in response to the stop condition, F(1, 9) = 4.31; p < 0.05, while CBT didn’t impact on the MAP amplitude, in response to Go condition, F(1, 9) = 0.18; p = 0.68). Due to the significant diminution of symptoms following CBT, all correla-tions between tic symptoms and MAP amplitude, significant at pretherapy, became nonsignificant at post-CBT (Table 3).
discussion
Our findings confirmed that tic symptoms significantly improved post-CBT, which is consistent with a recent randomized controlled trials with GTS (Piacentini et al., 2010). Other symptoms, such as depression, anxiety, and obsession-compulsion were only marginally influenced. Generally speaking, this shows that our specialized CBT primarily target is restricted to tic symptoms. Even if the OCD and anxio-depressive symptoms didn’t reach a pathological level, a complementary CBT focusing on anxi-ety and obsessive-compulsive symptoms could also be administered to address these dimensions more specifically (O’Connor et al., 2001). In addition to improvement in fine motor dexterity, GTS showed a reduced cerebral activation post-CBT over central regions at the inhibition of automatic motor responses at the traffic light task. Impor-tantly, CBT may selectively impact on this atypical brain response in GTS, as shown by post-CBT normalization of motor cortical activation.
The impact of CBT on brain activity was also demonstrated with OCD patients using PET imaging. Brody et al. (1998) suggested that subjects with differing patterns of metabolism preferentially respond to CBT versus medication. Left orbitofrontal
44 LAVOIE ET AL.
cortex metabolism alone was selected as predicting treatment response in the CBT treated group. A strong relationship has also been found between symptom reduc-tion following CBT and brain glucose metabolism normalization in these patients with OCD. A recent PET scan study by Saxena et al. (2008) showed that compared with controls, OCD patients showed significant bilateral decreases in thalamic me-tabolism with intensive CBT, but had a significant increase in right dorsal anterior cingulate cortex activity that correlated strongly with the degree of improvement in OCD symptoms. These results, applied to OCD, showed that successful CBT has the potential to modify brain metabolism as well as cognitive and behavioral processing. In our results a successful CBT for a population of GTS explicitly addressed motor responses in terms of restructuring antagonist or competing responses to the tic situ-ation. Additionally, the overall style of action was addressed to deal with the tendency to complete everyday tasks in an over-effortful, over active, and tension-producing mode. Neurobiological hypotheses have centered on basal ganglia dysfunction simi-lar to other movement disorders; in particular the orbital-frontal-basal ganglia loop (Casey, et al., 2002). Earlier studies using magnetic resonance imaging (MRI), have identified minor reduction in the putamen and the caudate nuclei when confounding variables such as sex, age, OCD, attention-deficit hyperactivity disorders (ADHD), and strep infection were taken into account (Peterson et al., 2000). Other MRI and positron emission tomography (PET) studies have consistently reported volumetric and metabolic reductions in lentiform (Braun et al., 1995; Eidelberg et al., 1997) and caudate nuclei (Bloch, Leckman, Zhu, & Peterson, 2005; Hyde et al., 1995; Stoet-ter et al., 1992). The basal ganglia are not the sole cerebral structures involved in the pathogenesis of GTS. In addition to these networks, motor and sensorimotor cortices
FIGURE 1. Illustration depicting the event-Related Potentials (ERP) difference sig-nal (subtraction of the STOP minus GO) as a function of time following response generation in the automated and complex response condition recorded from C1 (left hemisphere) and C2 (right hemisphere) electrodes. The zero timescale on the x-axis represents the onset of the motor response (e.g. response-locked) whereas the y-axis the amplitude in microvolts.

CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 45
have showed metabolic increases associated with heightened activation in premotor cortex and supplementary motor area (SMA) with PET imaging (Braun, et al., 1993; Eidelberg, et al., 1997; Stoetter, et al., 1992). Cortical thinning in sensorimotor areas was also correlated with tic severity and was most prominent in ventral portions of the homunculi that control the facial, orolingual, and laryngeal muscles commonly involved in tic (Sowell et al., 2008). Another hypothesis is that people with GTS show abnormally high levels of sensorimotor activation, causing problem with visuomo-tor coordination, chronic muscle tension, frustration threshold, and overgeneralized responding (O’Connor et al., 2002; O’Connor, 2002). This hypothesis also partially accounts for the success of relaxation and habit reversal techniques in tic management (Peterson & Azrin, 1992).
But exactly, how do the findings of ERP differences fit within current neurobio-logical theories of GTS? Our results demonstrated consistency with earlier findings by showing that initiation of movement and the inhibition of the motor response itself produces the MAP, a potential maximal over the vertex, that is particularly af-fected in the GTS (O’Connor et al., 2005). The MAP represents a composite index of precentral cortex motor activation (Naito & Matsumura, 1996), while generating the pyramidal tract volley following response and may also be a function of reafferent and proprioceptive feedback to cortical areas from subcortical structures related to sensorimotor cortices and basal ganglia respectively (Brunia, 1983; Brunia, Scheirs, & Haagh, 1982; Rektor et al., 2003), two important regions of interest for GTS (Swain, Scahill, Lombroso, King, & Leckman, 2007). In clinical practice, GTS pa-tients frequently show motor restlessness and an overpreparation in their style of plan-ning action, often attempting too much at once and creating frustration and tension (O’Connor et al., 2003). The current differences in our cortical indices of inhibition support the hypothesis that difficulties in optimal planning actions are an inherent characteristic of GTS.
In the present case, the localization of deficit to particular problems in planning of action and inhibition, permits integration of style of planning as part of behavior modification. Cognitive behavior therapy, although increasingly specialized, still relies on standard procedures derived from learning principles, which may not be optimal for all types of disorders. Cognitive remediation therapy—a close neighbor of cog-nitive therapy—does attempt specifically to improve functions such as memory and
TABLE 3. Pearson Correlations at Pre- and Post-CBT Between Tic Frequency and ERP Amplitude Over Left (C1 Electrodes) and Right Hemisphere (C2 Electrodes).
Responses types Inhibition Electrodes Tic Frequency Symptoms
Pre-therapy Post-therapy
Automatic Stop C1 left hemisphere -.81** -.49
C2 right hemisphere -.75* -.50
Go C1 left hemisphere .20 .13
C2 right hemisphere .15 .10
Complex Stop C1 left hemisphere -.71* -.47
C2 right hemisphere -.63* -.52
Go C1 left hemisphere -.55 -.24
C2 right hemisphere -.43 -.03
Note. *p < .05; **p < .01.

46 LAVOIE ET AL.
visuospatial ability or attention if there is clear deficit. Behavioral therapy may, in future, need to be grounded not just on standard behavioral principles, but on specific behavioral and psychophysiological understanding of the cortical processes behind ab-normal behavior. The reciprocity of this brain behavior management means also that behavioral observation and modification informs understanding of brain mechanisms. Dynamic measurement of brain physiology can offer feedback to refine sensory or motor strategies for behavioral intervention. Therefore, a posttreatment improvement may reflect the acquisition of improved strategies of motor control. Our findings sug-gest a new and exciting way to bridge neuroscience and cognitive behavior therapy. Historically, these two disciplines have developed independently with an often hit and miss relationship between the content of therapy and the relationship with brain function. However, cognitive psychophysiology offers a methodology for quantifying cognitive operations neurometrically. Operationalizing behavioral constructs such as “preparation” by connecting specific components of action to specific electrophysi-ological waves, permits cross-talk between stages of processing and type of cognitive intervention (O’Connor, 2002; Thibault et al., 2008; Thibault, O’Connor, Stip, & Lavoie, 2009).
Obviously, the current research constitutes a first step in the comprehension of physiological changes following CBT. One of the main limitations of the current study is our small sample. We made the choice to investigate a well-selected and relatively homogeneous group, but the next step would certainly be to examine the impact of CBT on a wider range of GTS, with and without other comorbidity such as OCD or ADHD. Another limitation is the use of a control group only at baseline without a retest. In our past research, we reassessed motor dexterity in controls and also GTS after a natural wait-list period to ascertain that there is no learning or habituation ef-fect and that the test-retest effect didn’t significantly affect measures of motor dexterity (O’Connor et al., 2008). Similarly, we already know that the electrocortical activity is not affected, by test-retest, in the same traffic light task (O’Connor et al., 2005). Nonetheless, optimally, future research could benefit from a retest with the control group after 6 months and also the addition of a matched clinical group such as habit disorders, retested after a natural wait-list and then, a third time following CBT.
RefeRences
American EEG Society. (1994). Guideline thirteen: Guidelines for standard electrode position nomenclature. Journal of Clinical Neurophysi-ology, 11, 111-113.
American Psychiatric Association. (2000). Diagnos-tic and statistical manual of mental disorders (4th edition-Text revision). Washington DC: American Psychiatric Association.
Azrin, N. H., & Peterson, A. L. (1988). Habit reversal for the treatment of Tourette syn-drome. Behav Res Ther, 26(4), 347-351.
Baron-Cohen, S., Cross, P., Crowson, M., & Rob-ertson, M. (1994). Can children with Gilles de la Tourette syndrome edit their inten-tions? Psychol.Med., 24(1), 29-40.
Baxter, L. R., Schwartz, J. M., Bergman, K. S., Szuba, M. P., Guze, B. H., Maziotta, J. C.,
et al. (1992). Caudate glucose metabolic rate changes with both drug and behavior therapy for obsessive-compulsive disorder. Archives of General Psychiatry, 49, 681-689.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring clini-cal anxiety: psychometric properties. Journal of Consulting and Clinical Psychology, 56(6), 893-897.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for measuring depression. Archives of General Psychiatry, 4, 561-571.
Bergin, A., Waranch, H. R., Brown, J., Carson, K., & Singer, H. S. (1998). Relaxation therapy in Tourette syndrome: A pilot study. Pediatr Neurol, 18(2), 136-142.
CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 47
Bloch, M. H., Leckman, J. F., Zhu, H., & Peter-son, B. S. (2005). Caudate volumes in child-hood predict symptom severity in adults with Tourette syndrome. Neurology, 65(8), 1253-1258.
Bloch, M. H., Peterson, B. S., Scahill, L., Otka, J., Katsovich, L., Zhang, H., et al. (2006). Adulthood outcome of tic and obsessive-compulsive symptom severity in children with Tourette syndrome. Arch Pediatr Adolesc Med, 160(1), 65-69.
Bornstein, R. A. (1990). Neuropsychological per-formance in children with Tourette’s syn-drome. Psychiatry Research, 33(1), 73-81.
Bornstein, R. A. (1991). Neuropsychological per-formance in adults with Tourette’s syndrome. Psychiatry Research, 37(3), 229-236.
Bornstein, R. A., & Baker, G. B. (1991). Neuropsy-chological performance and urinary phenyl-ethylamine in Tourette’s syndrome. J Neu-ropsychiatry Clin Neurosci, 3(4), 417-421.
Bornstein, R. A., Baker, G. B., Bazylewich, T., & Douglass, A. B. (1991). Tourette syndrome and neuropsychological performance. Acta Psychiatr Scand, 84(3), 212-216.
Bornstein, R. A., King, G., & Carroll, A. (1983). Neuropsychological abnormalities in Gilles de la Tourette’s syndrome. J.Nerv.Ment.Dis., 171(8), 497-502.
Braun, A. R., Randolph, C., Stoetter, B., Mohr, E., Cox, C., Vladar, K., et al. (1995). The functional neuroanatomy of Tourette’s syn-drome: An FDG-PET Study. II: Relation-ships between regional cerebral metabolism and associated behavioral and cognitive fea-tures of the illness. Neuropsychopharmacology, 13(2), 151-168.
Braun, A. R., Stoetter, B., Randolph, C., Hsiao, J. K., Vladar, K., Gernert, J., et al. (1993). The functional neuroanatomy of Tourette’s syndrome: An FDG-PET study. I. Regional changes in cerebral glucose metabolism dif-ferentiating patients and controls. Neuropsy-chopharmacology, 9(4), 277-291.
Brody, A. L., Saxena, S., Schwartz, J. M., Stoessel, P. W., Maidment, K., Phelps, M. E., et al. (1998). FDG-PET predictors of response to behavioral therapy and pharmacotherapy in obsessive compulsive disorder. Psychiatry Re-search, 84(1), 1-6.
Brookshire, B. L., Butler, I. J., Ewing-Cobbs, L., & Fletcher, J. M. (1994). Neuropsychological characteristics of children with Tourette syn-drome : Evidence for a nonverbal learning disability? Journal of Clinical and Experimen-tal Neuropsychology (16), 289-302.
Brown, T. A., DiNardo, P. A., & Barlow, D. H. (1994). Anxiety disorders interview schedule for DSM-IV. Boulder, CO: Graywind Pub-lications.
Brunia, C. H. (1983). Motor preparation: Changes in amplitude of Achilles tendon reflexes dur-ing a fixed foreperiod of one second. Psy-chophysiology, 20(6), 658-664.
Brunia, C. H., Scheirs, J. G., & Haagh, S. A. (1982). Changes of Achilles tendon reflex amplitudes during a fixed foreperiod of four seconds. Psychophysiology, 19(1), 63-70.
Bryant, R. A., Felmingham, K., Kemp, A., Das, P., Hughes, G., Peduto, A., et al. (2008). Amygdala and ventral anterior cingulate ac-tivation predicts treatment response to cog-nitive behaviour therapy for posttraumatic stress disorder. Psychol Med, 38(4), 555-561.
Bryant, R. A., Felmingham, K., Whitford, T. J., Kemp, A., Hughes, G., Peduto, A., et al. (2008). Rostral anterior cingulate volume predicts treatment response to cognitive-behavioural therapy for posttraumatic stress disorder. J Psychiatry Neurosci, 33(2), 142-146.
Casey, B. J., Tottenham, N., & Fossella, J. (2002). Clinical, imaging, lesion, and genetic ap-proaches toward a model of cognitive con-trol. Dev Psychobiol, 40(3), 237-254.
Channon, S., Crawford,S., Vakili,K., & Robertson, M. M. (2003). Real-life-type problem solv-ing in Tourette syndrome. Cogn Behav Neu-rol, 16(1), 3-15.
Como, P. G. (2001). Neuropsychological func-tion in Tourette syndrome. Adv Neurol, 85, 103-111.
Cozolino, L. J. (2002). The neuroscience of psycho-therapy: Building and rebuilding the human brain. New York: Norton.
Dion, Y., Annable, L., Sandor, P., & Chouinard, G. (2002). Risperidone in the treatment of Tourette syndrome: A double-blind, place-bo-controlled trial. Journal of Clinical Psy-chopharmacology, 22(1), 31-39.
Eidelberg, D., Moeller, J. R., Antonini, A., Kazu-mata, K., Dhawan, V., Budman, C., et al. (1997). The metabolic anatomy of Tourette’s syndrome. Neurology, 48(4), 927-934.
Ernst, M., Zametkin, A. J., Jons, P. H., Matochik, J. A., Pascualvaca, D., & Cohen, R. (1999). High presynaptic dopaminergic activity in children with Tourette’s disorder. Journal of the American Academy of Child and Adolescent Psychiatry (38) 86-94.
Felmingham, K., Kemp, A., Williams, L., Das, P., Hughes, G., Peduto, A., et al. (2007). Changes in anterior cingulate and amygdala after cognitive behavior therapy of post-traumatic stress disorder. Psychol Sci, 18(2), 127-129.
Freeman, R. D., Fast, D. K., Burd, L., Kerbeshian, J., Robertson, M. M., & Sandor, P. (2000). An international perspective on Tourette syndrome: selected findings from 3,500
48 LAVOIE ET AL.
individuals in 22 countries. Dev Med Child Neurol, 42(7), 436-447.
Gilles de la Tourette, G. (1885). Étude sur une affection nerveuse caractérisée par de l’incoordination motrice accompagnée d’écholalie et de coprolalie. Archives de Neu-rologie, 9, 19-42; 158-200.
Goetz, C. G. T., C.M.,Stebbins, G.T., Leipzig, G., & Carr, W.C. (1992). Adult tics in Gilles de la Tourette syndrome: Description and risk factors. Neurology, 42, 784-788.
Golden, G. S. (1977). The effect of central nervous system stimulants on Tourette syndrome. Ann.Neurol., 2(1), 69-70.
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Delgado, P., Heninger, G. R., et al. (1989). The Yale-Brown Obsessive Com-pulsive Scale (Y-BOCS). II. Validity. Archives of General Psychiatry, 46(11), 1012-1016.
Hallett, M. (2001). Neurophysiology of tics. Adv Neurol, 85, 237-244.
Harcherik, D. F., Leckman, J. F., Detlor, J., & Co-hen, D. J. (1984). A new instrument for clinical studies of Tourette’s syndrome. Jour-nal of the American Academy of Child Psychia-try, 23(2), 153-160.
Harris, E. L., Schuerholz, L. J., Singer, H. S., Read-er, M. J., Brown, J. E., Cox, C., et al. (1995). Executive function in children with Tourette syndrome and/or attention deficit hyperac-tivity disorder. J.Int.Neuropsychol.Soc., 1(6), 511-516.
Himle, M. B., & Woods, D. W. (2005). An experi-mental evaluation of tic suppression and the tic rebound effect. Behav Res Ther, 43(11), 1443-1451.
Hyde, T. M., Stacey, M. E., Coppola, R., Handel, S. F., Rickler, K. C., & Weinberger, D. R. (1995). Cerebral morphometric abnormali-ties in Tourette’s syndrome: A quantitative MRI study of monozygotic twins. Neurology, 45(6), 1176-1182.
Hyler, S. E. (1994). Personality Questionnaire PDQ-41. New York: New York State Psychi-atric Institute.
Kadesjo, B., & Gillberg, C. (2000). Tourette’s dis-order: Epidemiology and comorbidity in pri-mary school children. Journal of the American Academy of Child and Adolescent Psychiatry, 39(5), 548-555.
Lavoie, M. E., Thibault, G., Stip, E., & O’Connor, K. P. (2007). Memory and executive func-tions in adults with Gilles de la Tourette syndrome and chronic tic disorder. Cognitive Neuropsychiatry, 12(2), 165-181.
Leckman, J. F., Peterson, B. S., Pauls, D. L., & Co-hen, D. J. (1997). Tic disorders. Psychiatric Clinics of North America, 20(4), 839-861.
Leckman, J. F., Riddle, M. A., Hardin, M. T., Ort, S. I., Swartz, K. L., Stevenson, J., et al. (1989). The Yale Global Tic Severity Scale:
Initial testing of a clinician-rated scale of tic severity (YGTSS). Journal of the American Academy of Child and Adolescent Psychiatry, 28(4), 566-573.
Leckman, J. F., Zhang, H., Vitale, A., Lahnin, F., Lynch, K., Bondi, C., et al. (1998). Course of tic severity in Tourette syndrome:The first two decades. Pediatrics, 102, pp. 14-19.
Lombroso, P. J., Scahill, L., King, R. A., Lynch, K. A., Chappell, P. B., Peterson, B. S., et al. (1995). Risperidone treatment of children and adolescents with chronic tic disorders: A preliminary report. Journal of the American Academy of Child and Adolescent Psychiatry, 34(9), 1147-1152.
Mahone, E. M., Koth, C. W., Cutting, L., Singer, H. S., & Denckla, M. B. (2001). Executive func-tion in fluency and recall measures among children with Tourette syndrome or ADHD. J.Int.Neuropsychol.Soc., 7(1), 102-111.
Miltenberger, R. G., & Veltum, L. G. (1988). Evaluation of an instructions and modeling procedure for training behavioral assessment interviewing. J Behav Ther Exp Psychiatry, 19(1), 31-41.
Naito, E., & Matsumura, M. (1996). Movement-related potentials associated with motor in-hibition under different preparatory states during performance of two visual stop sig-nal paradigms in humans. Neuropsychologia, 34(6), 565-573.
O’Connor, K. P. (2002). A cognitive-behavioral/psychophysiological model of tic disor-ders. Behaviour Research and Therapy, 40, 1113-1142.
O’Connor, K. P. (2005). Testing the cognitive-psy-chophysiological model: validation of a style of planning action (STOP) as a discriminator between tic disorder, obsessive-compulsive disorder and generalized anxiety. Cognitive-Behavioral Management of tic disorders (pp. 65-73.). Chichester: John-Wiley and Sons.
O’Connor, K. P., Brault, M., Robillard, S., Loiselle, J., Borgeat, F., & Stip, E. (2001). Evaluation of a cognitive-behavioural program for the management of chronic tic and habit disor-ders. Behaviour Research and Therapy, 39(6), 667-681.
O’Connor, K., Brisebois, H., Brault, M., Robillard, S., & Loiselle, J. (2003). Behavioral activity associated with onset in chronic tic and habit disorder. Behavior Research and Therapy, 41, 241-249.
O’Connor, K. P., Lavoie, M. E., Robert, M., Stip, E., & Borgeat, F. (2005). Brain-behavior re-lations during motor processing in chronic tic and habit disorder. Cognitive and Behav-ioral Neurology 18(2), 79-88.
O’Connor, K. P., Lavoie, M. E., Stip, E., Borgeat, F., & Laverdure, A. (2008). Cognitive-be-haviour therapy and skilled motor perfor-
CBT AND NEUROCOGNITIVE APPROACH IN TOURETTE SYNDROME 49
mance in adults with chronic tic disorder. Neuropsychol Rehabil, 18(1), 45-64.
Ozonoff, S., & Jensen, J. (1999). Brief report: Specific executive function profiles in three neurodevelopmental disorders. J.Autism Dev.Disord., 29(2), 171-177.
Paquette, V., Levesque, J., Mensour, B., Leroux, J. M., Beaudoin, G., Bourgouin, P., et al. (2003). “Change the mind and you change the brain”: Effects of cognitive-behavioral therapy on the neural correlates of spider phobia. Neuroimage, 18(2), 401-409.
Peterson, A. L., & Azrin, N. H. (1992). An evalu-ation of behavioral treatments for Tourette syndrome. Behavior Research and Therapy, 30(2), 167-174.
Peterson, A. L., Campise, R. L., & Azrin, N. H. (1994). Behavioral and pharmacological treatments for tic and habit disorders: A re-view. J Dev Behav Pediatr, 15(6), 430-441.
Peterson, B., Riddle, M. A., Cohen, D. J., Katz, L. D., Smith, J. C., Hardin, M. T., et al. (1993). Reduced basal ganglia volumes in Tourette’s syndrome using three-dimensional recon-struction techniques from magnetic reso-nance images. Neurology, 43(5), 941-949.
Peterson, B. S., & Cohen, D. J. (1998). The treat-ment of Tourette’s syndrome: multimodal, developmental intervention. Journal of Clini-cal Psychiatry, (59 Suppl 1), 62-72; discussion 73-64.
Peterson, B. S., Leckman, J. F., Tucker, D., Scahill, L., Staib, L., Zhang, H., et al. (2000). Pre-liminary findings of antistreptococcal anti-body titers and basal ganglia volumes in tic, obsessive-compulsive, and attention deficit/hyperactivity disorders. Archives of General Psychiatry, 57(4), 364-372.
Piacentini, J., Woods, D. W., Scahill, L., Wilhelm, S., Peterson, A. L., Chang, S., et al. (2010). Behavior therapy for children with Tourette disorder: a randomized controlled trial. Jama, 303(19), 1929-1937.
Rektor, I., Kaiiovsky, P., Bares, M., Brazdil, M., Streitova, H., Klajblova, H., et al. (2003). A SEEG study of ERP in motor and premo-tor cortices and in the basal ganglia. Clinical Neurophysiology, 114(3), 463-471.
Riddle, M. A., Hardin, M. T., Towbin, K. E., Leck-man, J. F., & Cohen, D. J. (1987). Tardive dyskinesia following haloperidol treatment in Tourette’s syndrome. Archives of General Psychiatry, 44(1), 98-99.
Rodgers, R., Callahan, S., & Chabrol, H. (2004). [Revision of the translation of certain items in the French version of PDQ-4 (Personality Diagnostic Questionnaire; Hyler, 1994)]. Encephale, 30(4), 408-409.
Rothenberger, A. K., & Kemmerling, S. (1982). Bereitschaftspotential in children with mul-tiple tics and Gilles de la Tourette syndrome.
In A. Rothenberger. (Ed.), Event-Related potentials in children (pp. 257-270). Amster-dam: Elsevier Biomedical Press.
Rothenberger, A. K., S. (1982). Bereitschaftpoten-tial in children with multiple tics and Gilles de la Tourette syndrome. In A. Rothenberg-er (Ed.), Event-Related Potentials in children (pp. 257-270). Amsterdam: Elsevier Bio-medical Press.
Rothenberger, A. K., S., Schenk, G.K., Zerbin, D., & Voss, M. (1986). Movement-related po-tentials in children with hypermotoric behav-iour. In R. Z. W.C. McCallum., & F.Denoth (Eds.), Cerebral psychophysiology: Studies in event-related potentials (Vol. EEG suppl 38, pp. 496-499). Amsterdam: Elsevier (Bio-medical division).
Sallee, F. R., Nesbitt, L., Jackson, C., Sine, L., & Sethuraman, G. (1997). Relative efficacy of haloperidol and pimozide in children and ad-olescents with Tourette’s disorder. American Journal of Psychiatry, 154(8), 1057-1062.
Sanavio, E. (1988). Obsessions and compulsions: The Padua Inventory. Behaviour research and therapy, 26(2), 169-177.
Saxena, S., Gorbis, E., O’Neill, J., Baker, S. K., Mandelkern, M. A., Maidment, K. M., et al. (2008). Rapid effects of brief intensive cog-nitive-behavioral therapy on brain glucose metabolism in obsessive-compulsive disor-der. Mol Psychiatry, 14(2), 197-205.
Schuerholz, L. J., Baumgardner, T. L., Singer, H. S., Reiss, A. L., & Denckla, M. B. (1996). Neuropsychological status of children with Tourette’s syndrome with and without atten-tion deficit hyperactivity disorder. Neurology, 46(4), 958-965.
Schwartz, J. M., & Begley, S. (2002). The mind and the brain: Neuroplasticity and the power of men-tal force. New York: Harper Collins.
Seignot, J. N. (1961). [A case of tic of Gilles de la Tourette cured by R 1625]. Ann Med Psychol (Paris), 119(1), 578-579.
Shapiro, E., & Shapiro, A. K. (1986). Semiology, nosology and criteria for tic disorders. Revue neurologique, 142(11), 824-832.
Shapiro, E., Shapiro, A. K., Fulop, G., Hubbard, M., Mandeli, J., Nordlie, J., et al. (1989). Controlled study of haloperidol, pimozide and placebo for the treatment of Gilles de la Tourette’s syndrome. Archives of General Psy-chiatry, 46(8), 722-730.
Singer, H. S., Hahn, I. H., & Moran, T. H. (1991). Abnormal dopamine uptake sites in postmor-tem striatum from patients with Tourette’s syndrome. Ann.Neurol., 30(4), 558-562.
Singer, H. S., Szymanski, S., Giuliano, J., Yokoi, F., Dogan, A. S., Brasic, J. R., et al. (2002). Elevated intrasynaptic dopamine release in Tourette’s syndrome measured by PET.

50 LAVOIE ET AL.
American Journal of Psychiatry, 159(8), 1329-1336.
Sowell, E. R., Kan, E., Yoshii, J., Thompson, P. M., Bansal, R., Xu, D., et al. (2008). Thinning of sensorimotor cortices in children with Tourette syndrome. Nat Neurosci, 11(6), 637-639.
Steketee, G. (1994). Behavioural assessment and treatment planning with obsessive-com-pulsive disorder. Behavioral Therapy, 25, 613-633.
Stoetter, B., Braun, A. R., Randolph, C., Gernert, J., Carson, R. E., Herscovitch, P., et al. (1992). Functional neuroanatomy of Tourette syn-drome. Limbic-motor interactions studied with FDG PET. Advances in Neurology, 58, 213-226.
Sutherland, R. J., Kolb, B., Schoel, W. M., Whishaw, I. Q., & Davies, D. (1982). Neuropsycho-logical assessment of children and adults with Tourette syndrome: A comparison with learning disabilities and schizophrenia. Adv.Neurol., 35, 311-322.
Swain, J. E., Scahill, L., Lombroso, P. J., King, R. A., & Leckman, J. F. (2007). Tourette syn-drome and tic disorders: a decade of prog-ress. J Am Acad Child Adolesc Psychiatry, 46(8), 947-968.
Taylor, S. (1995). Assessment of obsessions and compulsions: Reliability, validity, and sensi-tivity to treatment effects. Clinical Psychology Review, 15, 261-297.
Thibault, G., Felezeu, M., O’Connor, K. P., Todo-rov, C., Stip, E., & Lavoie, M. E. (2008). Influence of comorbid obsessive-compulsive symptoms on brain event-related poten-tials in Gilles de la Tourette syndrome. Prog Neuropsychopharmacol Biol Psychiatry, 32(3), 803-815.
Thibault, G., O’Connor, K. P., Stip, E., & Lavoie, M. E. (2009). Electrophysiological manifes-tations of stimulus evaluation, response inhi-bition and motor processing in Tourette syn-drome patients. Psychiatry Research, 167(3), 202-220.
Tourette Syndrome Study Group. (1993). Defini-tions and classification of tic disorders. Ar-chives of Neurology, 50(10), 1013-1016.
Walkup, J. T., Leckman, J. F., Price, R. A., Hardin, M., Ort, S. I., & Cohen, D. J. (1988). The relationship between obsessive-compulsive disorder and Tourette’s syndrome: A twin study. Psychopharmacology Bulletin, 24(3), 375-379.
Wilberg, T., Dammen, T., & Friis, S. (2000). Comparing Personality Diagnostic ques-tionnaire-4+ with Longitudinal, Expert, All Data (LEAD) standard diagnoses in a sample with a high prevalence of axis I and axis II disorders. Compr Psychiatry, 41(4), 295-302.
Woods, D. W., Himle, M. B., Miltenberger, R. G., Carr, J. E., Osmon, D. C., Karsten, A. M., et al. (2008). Durability, negative impact, and neuropsychological predictors of tic suppres-sion in children with chronic tic disorder. Journal of Abnormal Child Psychology, 36(2), 237-245.
Woods, D. W., Miltenberger, R. G., & Lumley, V. A. (1996). Sequential application of major habit-reversal components to treat motor tics in children. J Appl Behav Anal, 29(4), 483-493.
Yeates, K. O., & Bornstein, R. A. (1994). Atten-tion deficit disorder and neuropsychological functioning in children with Tourette’s syn-drome. Neuropsychology, 8, 65-74.