Embed Size (px)
Citation preview

Ann. N.Y. Acad. Sci. ISSN 0077-8923
ANNALS OF THE NEW YORK ACADEMY OF SCIENCESIssue: Addiction Reviews 2
Neurochemistry of drug action
Insights from proton magnetic resonance spectroscopic imagingand their relevance to addiction
Stephanie C. Licata1 and Perry F. Renshaw2
1Behavioral Psychopharmacology Research Laboratory, McLean Hospital/Harvard Medical School, Belmont, Massachusetts,USA. 2Brain Institute and Department of Psychiatry, University of Utah School of Medicine, Salt Lake City, Utah, USA
Address for correspondence: Stephanie C. Licata, Ph.D., McLean Hospital/Harvard Medical School, 115 Mill St., Belmont, MA02478. Voice: 617-855-2738; fax: 617-855-3711. [email protected]
Proton magnetic resonance spectroscopy (1H MRS) is a noninvasive imaging technique that permits measurementof particular compounds or metabolites within the tissue of interest. In the brain, 1H MRS provides a snapshotof the neurochemical environment within a defined volume of interest. A search of the literature demonstratesthe widespread utility of this technique for characterizing tumors, tracking the progress of neurodegenerativedisease, and for understanding the neurobiological basis of psychiatric disorders. As of relatively recently, 1HMRS has found its way into substance abuse research, and it is beginning to become recognized as a valuablecomplement in the brain imaging toolbox that also contains positron emission tomography, single-photon-emissioncomputed tomography, and functional magnetic resonance imaging. Drug abuse studies using 1H MRS have identifiedseveral biochemical changes in the brain. The most consistent alterations across drug class were reductions in N -acetylaspartate and elevations in myo-inositol, whereas changes in choline, creatine, and amino acid transmittersalso were abundant. Together, the studies discussed herein provide evidence that drugs of abuse may have a profoundeffect on neuronal health, energy metabolism and maintenance, inflammatory processes, cell membrane turnover,and neurotransmission, and these biochemical changes may underlie the neuropathology within brain tissue thatsubsequently gives rise to the cognitive and behavioral impairments associated with drug addiction.
Keywords: proton magnetic resonance spectroscopy; human; brain imaging; drug abuse
Introduction
Proton magnetic resonance spectroscopy (1H MRS)is a noninvasive neuroimaging technique that hasbecome a useful tool for several applications indrug abuse research. As reviewed herein, 1H MRSis gaining popularity in studies aimed at elucidatingthe cerebral mechanisms underlying drug-inducedneuronal injury and the subsequent behavioral andcognitive changes that can contribute to addic-tion. Beyond simply determining the cerebral con-sequences of drug abuse, however, 1H MRS has thepotential for tracking disease and/or treatment pro-gression. For instance, studies examining the effectof short-term abstinence on the brain of alcoholicsdemonstrated metabolic changes that were indica-tive of neuronal and glial regeneration,1–5 whereas
Streeter et al.6 attempted to correlate changes inneurotransmission with efficacy of candidate treat-ments for cocaine dependence. Recently, Meyerhoffand Durazzo7 proposed the idea of correlating lev-els and patterns of metabolites not only with cogni-tion and behavior but also with genetic informationin order to understand better alcohol use disorder.Taken together, these studies indicate that 1H MRS isemerging as an informative technique that will be-come an invaluable instrument for understandingthe etiology of drug abuse, as well as for monitoringthe long-term recovery from this disease.
Measurable compounds
In 1H MRS, the visible spectrum depends on the en-ergy absorbed by specific organic molecules, which
doi: 10.1111/j.1749-6632.2009.05143.x148 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
Figure 1. Proton spectrum acquired at 4 T from a 16-cc voxel within the parieto-occipital cortex of a 26-year-old healthy male volunteer. Cho/PCho, choline/phosphocholine; Cr/PCr, creatine/phosphocreatine; GABA,�-aminobutyric acid; Glx, glutamate/glutamine; GSH, glutathione; H2O, water; Lac, lactate; mI, myo-inositol;MM, macromolecules; NAA, N -acetylaspartate; NAAG, N -acetylaspartylglutamate; Scy, scyllo-inositol; Tau, tau-rine. [Courtesy of J. Eric Jensen, Ph.D., Brain Imaging Center, McLean Hospital/Harvard Medical School.]
is determined by the number of hydrogen atoms inthe compound as well as in its environment (foran overview of the basic principles of MRS, pleasesee Ref. 8). In the brain, current detection limitspermit the quantification of several chemical peaksin the spectrum once the overwhelming water andlipid signals are suppressed (Fig. 1). Most com-monly reported include peaks for the metabolites N-acetylaspartate (NAA), creatine (Cr), choline (Cho),and myo-inositol (mI). Also visible are the metabol-ically available cellular pools of the amino acids �-aminobutyric acid (GABA), glutamate (Glu), andglutamine (Gln). To some extent, the visible protonspectrum has begun to transform the way in whichdrug abuse researchers think about the mechanis-tic landscape underlying addiction. Neurotransmit-ters that have dominated the literature, such asacetylcholine, norepinephrine, dopamine, and sero-tonin, are of insufficient concentrations to be visiblewith current technology. Similarly, several secondmessengers and ribonucleic acids also are outsideof range. However, a good deal of informationhas been provided by measuring those MR-visiblemetabolites.
N-AcetylaspartateThe most prominent signal in the water-suppressedproton spectrum arises from NAA (for a com-prehensive review on NAA, see Ref. 9). Althoughapproximately 15–25% of this signal is due to thecontribution of N-acetylaspartylglutamate,10 thespectral peak (at 2.02 ppm) is attributable pri-marily to the acetyl groups of NAA. Brain con-centrations of NAA are rather high11 and rela-tively homogeneous,12 although there is signifi-cantly more NAA in gray matter than in whitematter.13 Moreover, Nadler and Cooper14 demon-strated that NAA is localized almost exclusively toneuronal tissue in comparison to glia, thus render-ing NAA a neuronal marker. Reductions in NAAoften have been interpreted as being representativeof neuronal damage and/or loss15–18 or markers forreduction in synaptic density, as well as dysregu-lated neuronal function and/or neurotransmission(see discussion in Ref. 19). Alternatively, as dis-cussed thoroughly in Stork and Renshaw,20 NAAmay serve as a measure of mitochondrial functionbecause of its role in mitochondrial energy pro-duction. Taken together, these studies suggest that
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 149

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
NAA subserves several putative functions within thebrain.
CreatineSimilar to NAA, Cr is distributed evenly throughoutthe brain, with higher concentrations in gray mat-ter.12 The Cr peaks (at 3.03 and 3.94 ppm) are moreaccurately referred to as total Cr, because Cr andphosphocreatine (PCr) are indistinguishable fromone another. Together the Cr–PCr system has beenbelieved to provide a stable source of energy thattypically has been used as an internal reference tonormalize 1H MRS data.21 However, concentrationsof Cr and PCr have been shown to be unstable notonly across disease states,22,23 but it can vary acrossregions of healthy brain and with age.24
CholineWhereas Cho is the precursor of acetylcholinewithin cholinergic neurons, it is the Cho-containingcompounds glycerophosphocholine and phospho-choline that contribute to the Cho peak (at 3.2 ppm).Because both are involved in the synthesis anddegradation of cellular membranes,25 they are foundin higher concentrations within myelin, and there-fore within white matter.12 The distribution of Chothroughout the brain also is regionally dependent12;as a result, the Cho resonance has the potential tovary quite a bit across disease states, particularlywhen membrane turnover has been implicated inthe etiology.25,26
myo-InositolThe exact significance of the mI peak (at 3.56 ppm)is unclear, because there is still much speculationabout the precise function of mI within the brain.It has been suggested that mI is an osmoregulator27
or that it contributes to glucose storage.28 Otherstudies have shown that mI is an integral compo-nent of the calcium-mobilizing phosphatidylinosi-tol second-messenger system,29 and abnormalitiesin this system may contribute to the pathophysi-ology of several psychiatric illnesses.30 Most com-monly though, mI is used as a marker for glialcontent.31
Glutamate, glutamine, and GABAGlu, Gln, and GABA not only maintain an optimalbalance between excitation and inhibition withinthe brain but also work together to regulate neuronal
energy metabolism.32 Although the Glu, Gln, andGABA signals are derived from the large, metaboli-cally active cellular pools, they are notoriously dif-ficult to measure with 1H MRS. Several methodshave been developed to circumvent the complicatedspectral patterns that arise from their overlappingresonances,33 but typically the peak (at 2.4 ppm),which is attributed primarily to resonances arisingfrom both Glu and Gln, is considered “Glx.” Sim-ilarly, the GABA peak (at 3.03 ppm) comprises Crand macromolecules34 as well as homocarnosine.35
Despite a preponderance of evidence supportingcritical roles for altered Glu and/or GABA neuro-transmission underlying drug addiction,36,37 mostspectroscopic studies have restricted their investi-gations to metabolites that are comparatively lesstechnically demanding to measure.
Using 1H MRS to understand illicit druguse
PsychostimulantsAmphetamine congenersAmphetamine (AMPH), methamphetamine(METH), and its derivative 3,4-methylenedioxy-methamphetamine (MDMA, or ecstasy), arehighly abused central nervous system stimulantsthat have been shown to produce long-lastingneurotoxic effects. A wealth of data exists demon-strating that administration of AMPH is toxic todopaminergic neurons, MDMA is toxic primarilyto serotonergic neurons, and METH damages bothdopaminergic and serotonergic nerve terminalswhile also altering the glutamatergic system.38–40
This stimulant-induced toxicity is believed to bemediated by oxidative stress and activation ofapoptotic pathways and subsequently may con-tribute to the observed cognitive, neurological, andpsychiatric disturbances that persist after prolongeduse.41,42
AmphetamineTo date, the 1H MRS studies examining the neu-rochemical effects of AMPH have not been froma drug abuse perspective, but rather, AMPH hasbeen administered as a lithium-sensitive modelof mania.43,44 Specifically, dextroamphetamine wasadministered to healthy volunteers to address thehypothesis that lithium-induced depletion of inosi-tol underlies the antimanic effects of treatment.45,46
150 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
Whereas the results from a preliminary study in-dicated that dextroamphetamine increased levelsof mI (as a ratio of PCr:Cr) in the temporallobe,44 a follow-up study using a sequence opti-mized for mI47 failed to demonstrate any changein mI within the dorsal medial prefrontal cortex.43
The authors concluded that when all things wereconsidered dextroamphetamine had no effect onmI, and thus changes in mI cannot be relied uponsolely to understand the etiology of mania. How-ever, in the context of drug abuse, these data sug-gest that although AMPH is toxic to dopaminergicneurons,39 AMPH-induced reductions in dopaminesynthesis, dopamine metabolites, and dopamineuptake48–51 may not be manifested as glial dis-turbances or inflammatory processes. Of course,the clinical MRS studies mentioned here examinedan acute dose of dextroamphetamine, whereas theother studies cited used a chronic regimen of AMPHadministration.
MethamphetamineMETH has been shown to have long-lasting neu-rotoxic effects in both preclinical and clinical stud-ies. Human neuroimaging studies of METH abusersin particular have demonstrated profound drug-induced changes not only in the dopaminergic52,53
and serotonergic54 neurotransmitter systems butalso in cerebral glucose metabolism,55–57 as wellas the structural integrity of the brain.58–61 Ernstet al.62 was the first group to report alterations inmetabolite concentrations in METH users relativeto healthy control subjects. They found that NAAand Cr both were reduced in the basal ganglia,62
whereas concentrations of Cho and mI were elevatedin frontal gray matter.62 Subsequent studies corrob-orated their findings by reporting both reductionsin NAA/Cr63–65 and elevations in Cho/NAA64,65
within frontal gray matter, frontal white matter el-evations in mI,66 and reduced Cr + PCr/Cho inthe basal ganglia.67 Although together these stud-ies imply that METH exposure leads to subsequentneuronal injury, the literature contains now only afew studies that provide evidence supporting thishypothesis.
Ernst et al.62 also demonstrated an inverse re-lationship between the concentration of NAA infrontal white matter and cumulative lifetime METHexposure, whereas more recently Sung et al.66
showed that NAA was reduced in METH users who
had consumed a “large” cumulative dose relativeto those who had consumed a “small” dose. Thereduction in NAA also was shown to be corre-lated with reduced levels of attentional control asmeasured by interference on the Stroop test.65 Fi-nally, decreased levels of Cr + PCr/Cho were cor-related not only with longer duration of METHuse but also with severity of residual psychiatricsymptoms resulting from METH use.67 Together,these findings suggest a tangible functional relation-ship between METH-induced neurochemical alter-ations and cognitive impairment and/or psychiatricdisturbances.
In addition to the effect that duration of use mayhave on metabolite levels and subsequent neuronalinjury, various durations of abstinence from METHuse may affect reported values of metabolites. Forexample, although reductions in NAA have not beenconsistent across studies, differences in the reportedperiods of abstinence among participants may ex-plain the apparent discrepancies. When abstinenceranged from 0 to approximately 4 months, NAAlevels were reduced compared with those of controlsubjects,62,63,65 whereas NAA was not significantlydecreased compared with levels in control subjectswhen the duration of abstinence was approximately2 years.66 Moreover, NAA was shown to be positivelycorrelated with duration of abstinence, suggestingnot only that metabolite levels may recover but alsothat the neurotoxicity produced by METH may bereversed over time.66 Whereas Nordahl et al.64 con-tradicted this hypothesis by showing no differencesin NAA/Cr between those individuals who had beenabstinent for 1–5 years (long) versus those who hadbeen abstinent for 6 months or less (short), theyreported higher ratios of Cho/NAA in the brainsof “short” relative to the “long” abstinence partic-ipants. These results imply that Cho normalizes asabstinence increases, and they underscore furtherthe hypothesis that the brain may recover fromMETH-induced insult over time. However, func-tional studies demonstrating a reversal in alteredmetabolite levels concomitant with improvementsin cognitive processes and/or psychiatric symptomshave yet to be undertaken.
Recently, Ernst and Chang40 extended theirfindings beyond NAA, Cr, Cho, and mI to in-clude spectroscopic measures of METH-inducedadaptations in glutamatergic neurotransmission.Preclinical studies have shown that in addition to
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 151

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
serotonin and dopamine, Glu levels are altered byMETH,68 which may contribute to the mechanismsunderlying METH’s neurotoxicity.69 Glx was shownto be low in frontal gray matter but not in frontalwhite matter or basal ganglia. Levels of Glx werelowest at the beginning of abstinence (≤1 month),and whereas correlational analysis suggested a nor-malization of Glx over time with progressive absti-nence, a downregulation of Glu and/or Gln duringearly METH abstinence may have potentially signif-icant implications with respect to METH craving.Participants in the Ernst and Chang40 study who re-ported experiencing symptoms of craving had lowerGlx in the frontal cortex than those who did not; thisfinding was in agreement not only with a preclini-cal study that demonstrated reduced levels of basalGlu during cocaine seeking70 but also with clini-cal studies that demonstrated a decrease in drugtaking and cue reactivity when cocaine-dependentparticipants were administered medication to in-crease concentrations of basal Glu in the brain.71,72
Although these findings have not been replicated inMETH users, Ernst and Chang’s report40 providednot only novel evidence of glutamatergic dysfunc-tion associated with METH use in humans but alsoan impetus for improving the methods to permitthe measurement of Glu and Gln separately for usein drug abuse research.
3,4-MethylenedioxymethamphetamineDespite discrepancies between the animal and hu-man literature, the preponderance of evidence sup-porting the toxic potential of MDMA suggests thatthere are residual alterations in serotonergic neu-rotransmission among human MDMA users.73 Theramifications of this putative neurotoxicity includethe emergence of neurological, psychiatric, and so-matic disturbances that have been associated withserotonergic imbalance. Accordingly, case reportssuggest that MDMA use may lead to the appear-ance of a host of problems, such as psychosis, aswell as anxiety, panic, and depressive disorders.74–77
Similarly, more in-depth reports describe MDMA-induced sleep disturbances and cognitive deficits(see references in Ref. 78).
In 1H MRS studies it has been hypothesized thatsimilar to METH, regular users of MDMA exhibitneuronal loss or dysfunction and/or glial activation.Indeed, levels of NAA (expressed as ratios of bothCr and Cho) have been demonstrated to be reduced
in frontal gray matter79,80 and approaching a signif-icant reduction in the left hippocampus,81 whereasmI was elevated in parietal white matter.82 More-over, study participants who had lifetime historiesof heavy use (i.e., taking ≥700 tablets of ecstasy)exhibited deficits in delayed verbal recall that werestrongly associated with the prefrontal reductionsin NAA.79
Most studies, however, have not supported thesehypothesized alterations in NAA and/or mI. In fact,there is little consistency among reports of 1H MRSdata.83 NAA was found to decrease within brainregions that mediate verbal memory in associa-tion with lifetime cannabis use in MDMA polydrugabusers,84 whereas it was unchanged in single voxelsplaced within frontal gray or parietal white mat-ter,82,85–87 neocortex,81 hippocampus,89 or occipi-tal regions.82,85–88 Similarly, mI was unaffected inmany of the same regions.80,84,86–88 Although thesestudies suggest that MDMA does not induce lastingneuronal injury, they evaluated participants whoreported polydrug abuse. In fact, it is difficult tofind pure MDMA abusers within the population,because most also co-abuse cannabis, alcohol, orother stimulants.90 Also, participants reported var-ious estimates of lifetime MDMA exposure. How-ever, data obtained in nonhuman primates demon-strated reductions in hypothalamic NAA afterexposure to a recreational dose of MDMA.91 Fur-thermore, MDMA use in general has been associatedwith impaired delayed memory function even with-out changes in levels of NAA and mI,92 together sug-gesting that the sensitivity of current methods maynot permit the measurement of long-term neuroad-aptations that occur as a result of repeated exposureto MDMA.
CocaineCocaine, like the other psychostimulants, has cog-nitive, neurological, and psychiatric consequencesassociated with prolonged use. These effects maybe due in part to cocaine’s vasoconstrictive ef-fects, which are believed to underlie cocaine-relatedstrokes, intracranial hemorrhage, and persistentperfusion deficits (for more details, please see Ref.93), but they also may be attributed to its ability toincrease intracellular calcium,94 thereby facilitatingseizure activity95 and/or cell death.96 Several studieshave shown that biochemical mechanisms withinthe brain (i.e., alterations in brain metabolites)
152 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
also are associated with cocaine use and may con-tribute to the etiology of cocaine-induced neuronaldysfunction.
Among the changes in brain metabolites believedto result from prolonged cocaine use, alterations inNAA have been the most commonly reported. Ret-rospective studies that examined the effects of co-caine have demonstrated decreased thalamic NAAin current cocaine users19 as well as decreased levelsof NAA in midfrontal gray matter regions amongabstinent cocaine-dependent individuals97 relativeto healthy normal control subjects. However, nei-ther Chang et al.98 nor Ke et al.99 observed anyalterations in NAA when they examined midoccip-ital gray or temporoparietal white matter of absti-nent individuals or the left prefrontal lobe of cur-rent users, respectively. The predominating dogmaregarding the significance of NAA suggests thatalthough levels of NAA may be dynamic and re-flective of ongoing processes within neurons (re-ductions in NAA observed in neurological diseasestates or brain injury have been shown to be re-versible100,101), the decrease in NAA associated withchronic cocaine use may result from loss or damageto neurons, a reduction of synaptic density, or evena cocaine-induced depletion of brain monoamines(see discussion in Ref. 19). Indeed, several imag-ing studies have shown reductions in brain volumeor tissue density consistent with cocaine-inducedinjury.102–104
In contrast, opposite findings have been reportedafter one acute administration of cocaine. A pre-liminary report described a significant increase inthalamic NAA (as well as a nonsignificant increasein Cho) after administration of cocaine to cocaine-dependent participants.105 Similarly, in men whowere only occasional users, an intravenous infu-sion of cocaine resulted in a dose-dependent in-crease in NAA (as well as in Cho) within the leftbasal ganglia.106 Whereas these results are consis-tent with an increase in cocaine-induced phospho-lipid turnover, Christensen et al.106 hypothesizedthat cocaine’s ability to inhibit Na+/K+-ATPase107
may have led to augmented intracellular water con-tent and cellular swelling,108,109 and this subsequentosmotic stress may have affected the transverse re-laxation times (T2
∗) of the NAA and Cho peaks.Although the significance of these collective resultsstill is unclear, NAA may be regulated differentially
by acute cocaine versus prolonged exposure to co-caine over time.
Several other brain metabolites also are believedto be modified after chronic cocaine abuse, such asCr, mI, and GABA. Levels of Cr and mI were shownto be elevated in the temporoparietal white matterof abstinent users and were correlated with the fre-quency and duration of use, respectively.98 A follow-up study examining frontal white matter regions ina younger, less cocaine-experienced cohort foundsimilar results, albeit to a lesser extent.97 Elevationsin mI typically are hypothesized to represent in-creased glial hypertrophy and/or proliferation andmay suggest a reactive process in response to thechronic insult incurred in the brain by cocaine. Glialhypertrophy subsequently may have led to the in-crease in Cr because glial cells contain more Cr thanneuronal cells,31 and Cr levels typically are assumedto remain stable (but see Ref. 110). Further com-plicating matters, Chang et al.97 also reported onsex-related differences in metabolite levels amongcocaine users. Whereas males in that study exhibiteda reduction in NAA (gray matter) in addition to ele-vated Cr (white matter) and mI (both white and graymatter), the only abnormality observed in femaleswas elevated mI in frontal white matter. If thesedifferences in metabolite levels truly indicate differ-ences in cocaine-induced brain injury, then not onlyare they in agreement with previous work show-ing that women experience fewer cerebral perfusiondeficits,111 but they also provide further support forexamining the role of gonadal hormones as potentialtherapeutics.
Two recent studies have shown that cocaine-dependent individuals have lower prefrontal99 andoccipital112 GABA levels than those of healthy con-trol subjects. In the prefrontal cortex, there was a30% difference in GABA between groups,99 whereasthere was a 23% difference in GABA in the oc-cipital cortex.112 The finding within the prefrontalcortex in particular is significant because the pro-found impairments in inhibitory control, execu-tive functioning, and decision making displayed bycocaine-dependent individuals have been localizedrepeatedly to prefrontal cortical regions.113 Interest-ingly, the GABA system has been a promising targetfor therapeutics aimed at treating cocaine depen-dence.114 However it is unclear at this time whetherincreasing levels of GABA, particularly in the
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 153

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
prefrontal cortex, is sufficient to have clini-cal significance with respect to treatment foraddiction.6
OpiatesOpiates, such as morphine and heroin, are powerfulanalgesics with high abuse liability. Synthetic opi-oid compounds, such as methadone, also possesshigh abuse potential, although methadone’s util-ity extends beyond pain relief to include playingan integral role in the process of opiate detoxifi-cation. In addition to the risk of respiratory de-pression, viral infection, and/or liver damage as-sociated with intravenous administration, currentand former opiate abusers tend to display persistentneurocognitive deficits that may result from opiate-induced brain injury.115 Like many other drugs ofabuse, the rewarding effects of opiates are mediatedprimarily by the mesocorticolimbic dopamine sys-tem.116 It is prefrontal regions, however, that havebeen implicated in several neuropsychological stud-ies demonstrating profound impairments in exec-utive functioning,115 as well as in brain imagingstudies demonstrating reduced activity117–119 andcerebral blood flow120–123 in opiate-dependent in-dividuals. Moreover, both T2-weighted MRI124 andvoxel-based morphometry125 in opiate-dependentparticipants have revealed prefrontal white matterhyperintensities and reduced gray matter density,respectively, indicative of neuropathology.
To date, comparatively fewer studies have used1H MRS to study opiate-induced alterations inneurochemistry. The most commonly reported al-teration in metabolite concentration is a nonspe-cific reduction in NAA. For example, NAA wasreduced to a similar extent in both the dorsal an-terior cingulate119 and frontal gray matter126 ofopiate-dependent participants maintained on opi-oid replacement therapy. Case reports also demon-strated cerebellar white matter reductions in NAAamong individuals who suffered from heroin-induced leukoencephalopathy, a toxic spongiformencephalopathy resulting from inhaling heroin va-pors.127,128 That the opiate-induced alteration inNAA is similar to that observed among cocaine97
and METH62 abusers suggests that changes in NAAmay be nonspecific. Indeed, it has been hypothe-sized that reductions in NAA are indicative of thecerebral hypoxic–ischemic events associated withdrug abuse in a more general sense.126
Other notable changes in brain chemistry includean increase in lactate in those patients who sufferedfrom leukoencephalopathy.127,128 Because elevatedlactate levels typically are observed as a result of mi-tochondrial dysfunction,129 this finding was inter-preted to be indicative of abnormal cellular energymetabolism resulting from the neuropathology as-sociated with this particular condition; this changewas not seen in opiate-dependent individuals main-tained on stable methadone or buprenorphine.119 Inaddition to elevations in lactate, opiate dependencealso has been shown to be associated with a de-crease in Glx within the dorsal anterior cingulate.119
Although it is unknown what the subsequent re-duction in neuronal excitability contributes to theprocesses that accompany and/or underlie opiateaddiction, the reduction in Glx may represent ab-normalities in reward-based learning and decisionmaking or in the modulation of dopaminergicneurotransmission.119 Interestingly, despite littleclinical spectroscopic evidence supporting theinvolvement of lactate and Glx in opiate depen-dence, a recent study in the preclinical literaturedescribed similar changes in both the thalamusand somatosensory cortex of rats treated chron-ically with morphine.130 Together, these data in-vite further investigation regarding the role of en-ergy metabolism and neuronal excitability in opiatedependence.
CannabisOf all the illicit drugs of abuse, cannabis causesthe most controversy. Although reports indicatethat cannabis-based drugs provide relief to thosewho suffer from chronic pain or disease-inducedspasticity, there is a vast literature demonstratingimpairment in cognitive function; increased inci-dence of psychotic behavior; and not surprisingly,risk of abuse and/or dependence.131 Moreover, al-though cannabis is believed by many to be harm-less, both preclinical132,133 and clinical134 findingsindicate that chronic cannabis use is neurotoxicand has harmful effects on the integrity of braintissue.
Inasmuch as chronic cannabis consumptionsurely has an effect on neurochemistry, only a fewstudies describe such investigations. Chang et al.135
demonstrated that in the basal ganglia of individualswho had smoked marijuana almost daily for at least1 year, levels of NAA, Cho, and Glu were reduced.
154 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
Glu also was reduced in the thalamus, whereas Crwas elevated in this region.135 In occasional or recre-ational users, NAA was reduced in the dorsolateralprefrontal cortex, but no metabolite changes werefound in the anterior cingulate, striatum, thalamus,or hippocampus.136 The implication of both stud-ies was that the reduction in NAA could be inter-preted as a marker for neuronal dysfunction, al-though the specific functional significance of suchimpairment is unclear. Neuropsychological testingreturned equivocal results because Chang et al.135
did not find any deficits in their participants. Incontrast, the younger cohort examined by Hermannet al.136 exhibited cannabis-related deficits on testsassessing attention as well as short-term memory.Although there was no correlation between thoseneuropsychological results and the dorsolateral pre-frontal NAA decrease,136 it is intriguing not onlythat similar findings have been reported in studiesinvestigating the neurochemical basis of schizophre-nia137,138 but also that cannabis use is believed to bea risk factor for schizophrenia in genetically predis-posed individuals.139 Finally, although these resultsall together highlight the difficulty in drawing infer-ences about brain function from observed changesin brain metabolites, they provide support for theargument that cannabis indeed may have neurotoxiceffects within the brain.
Using 1H MRS to understand licit drug use
AlcoholThe neurotoxicity of chronic alcohol consumptionhas been revealed by imaging and histopathologicalstudies showing significant atrophy in the brains ofalcoholics.140,141 Regions of the brain that appearto be the most sensitive to the effects of chronicalcohol include the neocortex, limbic system, andcerebellum. Subsequently, alcoholics exhibit a hostof cognitive and behavioral abnormalities, includ-ing deficits in executive functioning, learning, andmemory, as well as problems with emotion andpersonality.142
To understand better the neurobiological sub-strates of the profound brain damage commonin alcoholism, other researchers have recently per-formed several 1H MRS studies.7 Reduced levelsof NAA2–5,143–146,148 and Cho2,3,5,143,144,148–150 wereobserved as putative evidence of general neuronaldysfunction in the gray and white matter brain re-
gions of treatment-seeking, alcohol-dependent vol-unteers. Also, levels of mI were elevated, particularlyduring short-term abstinence from alcohol.147 Thisfinding suggests a temporary increase in glial ac-tivation or an attempt to regulate cell volume in astate of alcohol-induced osmotic stress.147 Althoughmetabolite reductions did not correlate necessarilywith specific brain atrophy, recovery of NAA wascorrelated with a gain in global brain volume.1 Therecovery of NAA and/or Cho observed in absti-nence1–5,151 is consistent with a study that found nodifferences in metabolites between healthy individ-uals and those who had been alcohol abstinent for2 years.152 Moreover, the reversal of those metaboliteabnormalities sometimes was correlated with cog-nitive improvements.1,2,5 Together, these findingssuggest that, similar to the alcohol-induced struc-tural and functional deficits that are at least partiallyreversible with abstinence,147 the metabolite abnor-malities associated with those impairments also mayrecover in time.
Metabolite alterations also were observed in stud-ies examining cohorts of active drinkers relative tolight drinkers or treatment-seeking abstinent alco-holics. Active heavy drinkers exhibited lower levelsof frontal white mater NAA than light drinkers, aswell as higher levels of Cho, Cr, and mI in pari-etal gray matter.153 Whereas active heavy drinkersalso exhibited elevated levels of Cho, Cr, and mIacross several gray and white matter regions com-pared with abstinent alcoholics,154 NAA was higherin the current drinkers.154 These slightly differentpatterns of alcohol-induced effects on metabolites inthe actively drinking cohort could reflect any num-ber of factors that may modulate neurochemistrydifferentially (e.g., age, sex, comorbid psychiatricillness, lifetime exposure to alcohol, and withdrawalsymptoms).
Aside from these metabolic alterations, changesin glutamatergic and/or GABAergic neurotransmis-sion have been implicated in the etiology of alco-hol abuse.36,155 Consistent with chronic alcohol-induced GABAA receptor abnormalities and thesubsequent glutamatergic hyperactivity observedduring withdrawal,156,157 Glx and Glu/Cr were in-creased in the basal ganglia150 and the anteriorcingulate149 of detoxified alcoholics, respectively,whereas GABA was reduced by approximately 30%in the absence of any other metabolic changeswithin the occipital cortex.158 Interestingly, Mason
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 155

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
et al.159 found no differences in occipital GABAlevels when comparing alcohol-dependent andhealthy volunteers. However, their data revealed thatduring early abstinence the alcohol-dependent pa-tients who were smokers had significantly lower lev-els of GABA than did the nonsmokers.159 Althougha thorough examination of these data in the contextof the literature regarding GABAergic mechanismsmediating alcohol dependence and withdrawal isbeyond the scope of this review, a brief discussionof the effect smoking has on the neurochemical find-ings in alcohol-dependent individuals is warranted.
NicotineNicotine is the component of tobacco that givesrise to the addictive properties of cigarette smok-ing. Nicotine is an agonist at nicotinic acetylcholinereceptors, and like most other drugs of abuse, ex-erts its reinforcing effects ultimately by increas-ing dopaminergic neurotransmission within themesolimbic reward circuitry.160 A great deal of thenicotine literature has focused on understandinghow nicotine and/or smoking may enhance neuro-transmission within corticobasal ganglia–thalamiccircuits161 to have subsequent effects on learning,memory, and attention,162,163 as well as reward pro-cessing and dependence.164,165 Brain imaging stud-ies in particular have demonstrated that acute andchronic exposure to nicotine and/or cigarette smok-ing results in decreased global brain activity but fo-cal activations within prefrontal regions, thalamus,and the visual system.166 Moreover, nicotine also hasbeen associated with morphological abnormalitiesin frontal subregions and cerebellum.164,165
Preclinical studies have implicated GABA andGlu in the neurobiological effects of nicotine,167
and the clinical literature using 1H MRS supportsthis claim. Nicotine-dependent women exhibitedlower baseline GABA than nicotine-dependent menwithin the occipital cortex,168 and comparisons ofnicotine-dependent women to nonsmoking womenrevealed reductions during the follicular phase ofthe menstrual cycle that could not be attributed todifferences in smoking habits. Although subsequentinvestigations have not followed up on those prelim-inary smoking-related sex differences in GABA, Gal-linat and Schubert169 demonstrated that hippocam-pal Glu was unchanged among smokers, formersmokers, and individuals who had never smoked.In contrast, examination of other metabolites re-
vealed that hippocampal (but not ACC) NAA levelswere reduced when smokers were compared to non-smokers.170 This finding is consistent with a body ofpreclinical work suggesting that nicotine has neu-rotoxic effects on hippocampal neurons.171–173 Tothe extent that NAA is a marker for synaptic den-sity and/or neuronal viability,19 the null result in theACC does not support previous work demonstrat-ing reduced gray matter volume and gray matterdensity within that brain region of smokers com-pared with nonsmokers.164,165 However, involve-ment of NAA has been corroborated by a reportshowing that chronic cigarette smoking was corre-lated with lower midbrain NAA.143 Moreover, thatstudy also demonstrated reductions in Cho withinthe midbrain and cerebellar vermis,143 together con-firming that nicotine and/or smoking has an adverseeffect on neuronal function.
As previously discussed, alcohol has a deleteri-ous effect on the brain similar to that of smoking.Interestingly, upward of 80% of alcohol-dependentindividuals also smoke regularly.174,175 It has beenargued that consumption of alcohol facilitates theconsumption of nicotine, and subsequently, thecodependent population may represent a sub-population having highly specific needs with re-spect to smoking and/or drinking cessation.176
However, whereas chronic cigarette smoking wasshown to be detrimental to gray matter tissue vol-ume and perfusion in alcohol-dependent individ-uals,163,177 most of the studies demonstrating theeffect of alcohol on brain metabolites failed to con-trol for the effects of concurrent nicotine depen-dence.1,2,4,5,144–151 Therefore, the extent to whichthose reported alcoholism-induced metabolite al-terations reflected the effects of the combination isunknown.
Studies in which smokers were separated fromnonsmokers to determine how smoking affectedbrain metabolites and neurocognitive functioningin alcohol dependence found that during the firstweek of abstinence smokers had lower frontal, mid-brain, and medial temporal lobe NAA,143,178 as wellas lower Cho within midbrain143 and medial tem-poral lobe.178 After 1 month of sobriety, smokers ex-hibited less metabolite recovery, whereas their non-smoking counterparts exhibited increases in NAAand Cho, as well as more improved cognitive per-formance.3,178 Together, these findings indicate thatsmoking not only compounds the brain damage
156 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
resulting from alcohol dependence but also influ-ences the brain’s recovery from the chronic alcoholicinsult. Although it is not known how the long-termtrajectory of recovery beyond 1 month is affected bysmoking, these preliminary data support the cam-paign to encourage treatment for both dependenciessimultaneously.
TolueneToluene (methyl benzene) is an organic solvent thatis the main component of many commercial andhousehold products, such as paint, thinner, glue,and lighter fluid. Because it is legal and readily ac-cessible, it is one of the most commonly abused sub-stances among adolescents.179 The adolescent brainis particularly vulnerable to toluene-induced toxic-ity not only because toluene’s highly lipophilic na-ture leads to its accumulation in the lipid-rich whitematter regions of the brain180,181 but also becausethe proportion of white matter is increased duringthis time of neuronal development consequent to anincrease in myelination.182 Accordingly, much of thedamage observed in the brains of individuals whowere exposed to toluene chronically was localized towhite matter regions (in addition to periventricularand subcortical regions)183 and correlated signif-icantly with neurological,184 psychological,185 andcognitive186 deficits.
Although the brain abnormalities as well assubsequent encephalopathy and neuropsychologi-cal deficits associated with toluene abuse in hu-mans have been acknowledged in several publi-cations,187–190 there is no consensus regarding themechanism underlying this damage. However, sev-eral animal studies have demonstrated changesin neurochemistry by measuring levels of acetyl-choline,191 dopamine,192,193 GABA,194 and Glu,195
after administration of toluene. Similarly, the fewstudies using MRS in humans have used this tech-nology as a way to probe the neurochemical pro-cesses underlying toluene exposure in an effortto provide mechanistic substantiation of toluene-induced brain damage. For example, NAA was re-duced within white matter in two individuals (aged19 and 20 years) who had abused organic sol-vents for 6–7 years and who experienced symp-toms of encephalopathy, such as unsteady gait,tremor, diplopia, dysarthria, and impaired IQ rel-ative to that of healthy control subjects.196 Like-wise, young adults (aged 15–23 years) who had
abused paint thinner for 2–3 years had lower lev-els of NAA as well as higher levels of mI in cere-bral and cerebellar white matter, but not in the tha-lamus, relative to their age-matched control sub-jects.197 Moreover, these neurochemical changeswere correlated with the self-reported duration ofuse.197
A reduction in NAA typically has been interpretedto represent a reduction in neuronal number or lossof neuroaxonal integrity in general,9 but these re-sults were interpreted to be indicative primarily ofaxonopathy. Because NAA levels were spared withinthe thalamus, an area with higher neuronal densitythan the white matter and cerebellum, the authorsconcluded that the etiology of toluene encephalopa-thy did not involve the targeting of neurons per se.197
This conclusion is supported by other studies thatfailed to identify neuronal loss or morphologicalabnormalities,183,198 but that demonstrated degen-eration of axons,199 in postmortem tissue. Also, theelevated levels of mI observed by Aydin et al.197 mayreflect toluene-induced gliosis and astrocytic acti-vation rather than neuronal death after chronic ex-posure to toluene. Indeed, glial cell marker proteinshave been shown to be increased, particularly in thecerebellum, of rats exposed to toluene in a chronicdosing paradigm.200–202 Taken together, these datasuggest that axonopathy and gliosis seem to underliethe encephalopathy observed after chronic tolueneexposure.
It has been suggested that in addition to glio-sis, the demyelination observed in postmortem tis-sue183,199 also may underlie the toluene-inducedwhite matter lesions observed with MRI.184 Thishypothesis has been supported by findings in thebasal ganglia showing that levels of Cho/NAAand Cho/Cr + PCr (but not NAA/Cr + PCror mI/Cr + PCr) were elevated among abstinenttoluene abusers relative to control subjects.203 An in-crease in the Cho peak as measured with MRS is in-dicative of an increase in membrane phospholipids,which may be released during membrane decom-position, thereby representing active demyelinatingprocesses.25 However, five of the 12 participants inthis study also were taking neuroleptic medicationto manage their psychiatric symptoms, and Cho hasbeen shown previously to be sensitive to this typeof medication.204–206 Moreover, alterations in whitematter Cho did not reach statistical significancein the results reported by Aydin et al.,197 together
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 157

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
suggesting that demyelination may occur in tolueneabuse, but most probably it is not the primary mech-anism of neurotoxicity.
Synthesis of metabolic changes in drugabuse and future directions
Of all the changes in metabolites (Table 1) andamino acids (Table 2) that have been measured todate, there is considerable overlap across drug classes
(Table 3). Reductions in NAA and elevations in mIwere observed almost universally, thus indicatingthat drugs of abuse in general have a profound ef-fect on neuronal health, energy metabolism, andinflammatory processes. The next-most-commonmetabolite changes involved alterations in Cho andCr, suggesting that METH, cocaine, cannabis, andalcohol influence cell membrane turnover as wellas energy maintenance. METH, opiates, cannabis,and alcohol were found to alter Glx to some
Table 1. Reported metabolite changes with drugs of abuse
Drug NAA Cho Cr mI
AMPHa — — — Increase (TL)
None (PFC)
METHb Decrease (BG, FGM) Increase (FGM) Decrease (BG) Increase (FGM, FWM)
MDMAc Decrease (FGM, HP) — — Increase (PWM)
None (FGM, PWM,
NC, HP, OCC)
None (FGM, PWM,
OCC)
Cocained Decrease (FGM, TH) Increase (BG) Increase (PWM) Increase (FGM, PWM)
Increase (BG, TH)
None (OCC, PWM)
Opiatese Decrease (ACC, FGM,
CBL)
— — —
Cannabisf Decrease (BG, PFC) Decrease (BG) Increase (TH)
Alcoholg Decrease (CBL, FGM,
FWM, TH, TL)
Decrease (PGM, TH, CBL) Increase (PGM) Increase (ACC, PGM,
TH)
Increase (PGM, TL)
Nicotineh Decrease (HP) — — —
None (ACC)
Toluenei Decrease (CBL, CWM) Increase (BG) — Increase (CBL, CWM)
None (BG, TH) None (BG, TH)
ACC, anterior cingulate; BG, basal ganglia; CBL, cerebellar white matter; CWM, cerebral white matter; FGM, frontalgray matter; FWM, frontal white matter; HP, hippocampus; NC, neocortex; OCC, occipital cortex; PFC, prefrontalcortex; PGM, parietal gray matter; PWM, parietal white matter; TH, thalamus; TL, temporal lobe.aMcGrath et al. 2008; Silverstone et al. 2002.bErnst et al. 2000; Nordahl et al. 2002, 2005; Salo et al. 2007; Sung et al. 2007; Sekine et al. 2002.cChang et al. 1999; Cowan et al. 2007; Daumann et al. 2004; de Win et al. 2007, 2008; Obergriesser et al. 2001; Renemanet al. 2001, 2002.dChang et al. 1997, 1999; Christensen et al. 2000; Li et al. 1998, 1999.eHaselhorst et al. 2002; Kriegstein et al. 1999; Offiah et al. 2008; Yucel et al. 2007.f Chang et al. 2006; Hermann et al. 2007.g Bartsch et al. 2007; Bendszus et al. 2001; Durazzo et al. 2004, 2006; Ende et al. 2005; Gazdzinski et al. 2008a;Jagannathan et al. 1996; Lee et al. 2007; Martin et al. 1995; Meyerhoff et al. 2004; Miese et al. 2006; Parks et al. 2002;Schweinsburg et al. 2000, 2001, 2003; Seitz et al. 1999.hDurazzo et al. 2004; Gallinat et al. 2007.iNoda et al. 1996; Aydin et al. 2003; Takebayahsi et al. 2004.
158 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
Table 2. Reported amino acid changes with drugs of abuse
Drug Glx GABA
METH FGM: Decrease (Ernst and Chang, 2008) —
Cocaine — PFC: Decrease (Ke et al. 2004)
OCC: Decrease (Hetherington et al. 2000)
Opiates ACC: Decrease (Yucel et al. 2007) —
Cannabis BG, TH: Decrease (Chang et al. 2006) —
Alcohol ACC: Increase (Lee et al. 2007) OCC: Decrease (Behar et al. 1999)
BG: Increase (Miese et al. 2006) No change (Mason et al. 2006)
Nicotine HP: No change (Gallinat and Schubert, 2007) OCC: Decrease (Epperson et al. 2005)
ACC, anterior cingulate; BG, basal ganglia; FGM, frontal gray matter; HP, hippocampus; OCC, occipital cortex; PFC,prefrontal cortex; TH, thalamus.
extent, whereas GABA was reduced by cocaine,alcohol, and nicotine, together suggesting that drugsof abuse impact neurotransmission. Although notall drugs of abuse were associated with changesin all the metabolites represented, not every studymeasured every visible metabolite. In fact, quan-tifying metabolites with strongly coupled spins,such as mI, Glx, and GABA, requires specific ad-vanced techniques as well as stronger magnetic fieldstrength.47,207 However, as 1H MRS becomes morewidely recognized as a means to evaluate the sub-strates of drug action, the technology has the po-tential to evolve into a more automated and user-friendly procedure.
These 1H MRS data add a new dimension to theexisting wealth of knowledge regarding the detri-mental effects of drugs of abuse on the brain. Specifi-cally, though, what have we learned about addictionfrom measuring brain metabolites? Studies inves-tigating the etiology of other brain diseases have
begun using 1H MRS to probe functional relation-ships between metabolite alterations and other mea-sures of pathology. For example, levels of NAA havebeen shown to correlate with hippocampal volume,memory, and intelligence in patients with medialtemporal lobe epilepsy.208 Similarly, drug abuse re-search has begun to benefit from examining the re-lationships between metabolites and drug-inducedimpairments in neurocognitive function. Correla-tion analyses have revealed associations betweenreduced NAA in frontal regions and attentionalcontrol as well as impaired verbal memory amongparticipants who had histories of abusing METH65
and MDMA,79 respectively. These results are inagreement with other research that has shown acorrelation between levels of frontal NAA and mea-sures of selective attention209 and memory.210 More-over, they agree with findings obtained in alco-holics showing that various measures of learningand memory improved as levels of NAA (and Cho)
Table 3. Overlapping metabolite findings across drug classes (simplified)
Metabolite Decrease Increase
NAA METH, MDMA, cocaine,
opiates, cannabis, alcohol,
nicotine, toluene
Cocaine (acute administration)
Cho Cannabis, alcohol METH, cocaine, alcohol
Cr METH Cocaine, cannabis, alcohol
mI — AMPH, METH, MDMA, cocaine, alcohol, toluene
Glx METH, opiates, cannabis Alcohol
GABA Cocaine, alcohol, nicotine —
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 159

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
recovered during abstinence.3 In general, a great dealof research has shown that deficits in attention211
and memory212 may contribute to processes thatunderlie drug-seeking behavior, thereby necessitat-ing an understanding of the neurochemical mech-anisms mediating those processes and subsequentbehavioral output.
Although other metabolite–behavior relation-ships have been demonstrated (e.g., Ernst andChang40 showed that reduced frontal Glx correlatedwith ratings of craving, whereas Sekine et al.67 corre-lated reduced Cr in the basal ganglia with the severityof residual psychiatric symptoms after use), all to-gether, the information gleaned from 1H MRS stud-ies at this point mostly seems to corroborate decadesof previous research. Moreover, several studies havedemonstrated that metabolite reductions recoverduring abstinence from alcohol1–5,151 or METH,64,66
suggesting that perhaps the long-term neuroadap-tations that maintain drug-seeking and drug-takingbehaviors cannot be explained by the particularchanges in neurochemistry that are measurable with1H MRS. Meyerhoff and Durazzo7 suggested re-cently that in addition to relating metabolite lev-els to cognition, genetic polymorphism data mightprovide an additional piece of information thatcould help not only to elucidate the neurobiolog-ical mechanisms underlying substance abuse dis-order but also to identify risk factors and diseaseseverity.
Indeed, the strength of this technology in drugabuse research may lie in its utility as a diagnos-tic tool to predict treatment matching, to monitorthe progress of treatment, or to prevent relapse. Al-though now 1H MRS is used routinely to monitorthe course of treatment and determine therapeuticstrategies in several other brain illnesses, such as tu-mors, multiple sclerosis, and Alzheimer’s disease,213
the potential of these applications has not been ex-plored thoroughly in the context of drug abuse. Arecent study by Streeter et al.6 demonstrated the useof 1H MRS as a tool for assessing treatment efficacy.The study aimed to correlate changes in the level ofprefrontal GABA with reduced cocaine consump-tion in cocaine-dependent volunteers after 8 weeksof treatment with modest doses of the candidatetherapeutics pramipexole or venlafaxine. Previousstudies had shown that GABA was reduced in the leftprefrontal lobe of cocaine-dependent volunteers99
and that GABA-enhancing drugs reduced cocaine
self-administration in laboratory animals214,215 andhumans.216–219 Although both pharmacologic treat-ments increased levels of GABA significantly relativeto placebo, cocaine use was not reduced in eithertreatment group.6 However, the maximum increasein GABA was still approximately 19% lower thancontrol levels,99 suggesting that dose of drug mayhave been partly to blame. Regardless, this study is aprime example demonstrating the usefulness of 1HMRS within a treatment paradigm.
Although this review focused on metabolitechanges that occur after exposure to drugs of abusein the adult brain, drug abuse may begin in child-hood and/or adolescence, and exposure may occureven in utero. 1H MRS has the potential to be an in-valuable method for studying these vulnerable pop-ulations. The lack of ionizing radiation makes 1HMRS suited for undertaking longitudinal studies,particularly during the more active periods of braindevelopment. In fact, 1H MRS already has been usedto begin understanding the biochemical maturationof the brain not only in terms of specific metabolitesbut also in terms of water content, relaxation proper-ties, and myelination.220,221 In drug abuse, 1H MRSwas used in a small study that used children to ex-amine the neurotoxic effects of prenatal exposure toMETH on the developing brain.222 Findings showedthat despite the absence of structural abnormalities,exposed children (aged 3–16 years) had relativelynormal levels of NAA but elevated levels of Cr in thestriatum relative to age-matched control subjects.222
These results were in contrast to the reduction ofCr (and NAA) observed in this region of adultswho have abused METH.62,67 They suggest that al-though METH-induced biochemical alterations oc-cur in both children and adults, prenatal exposure toMETH can disrupt energy metabolism differentiallyin children, which may have clinical implicationswith respect to cognitive function in these individ-uals as their development progresses.222 Moreover,these results underscore the importance of using1H MRS technology to study the effects of drugs ofabuse in the developing brain.
Finally, 1H MRS may prove to be a useful modal-ity for studying the etiology of addiction in gen-eral. A great deal of research has suggested thatchronic drug abuse shares neurobiological under-pinnings with other addictive disorders, such asbulimia nervosa, pathological gambling, and sex-ual addiction.223 Although to date the findings have
160 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
been restricted to the effects of those reinforcerson the monoamine and opioid receptor system andtheir downstream signaling cascades, it is likely thatother addictive disorders would yield to study with1H MRS just as well. In fact, it would be interestingto determine whether pathological gambling, eat-ing, or sexual appetite reduced NAA to a similarextent as drugs of abuse. Although it is unlikely thatthese nonchemical reinforcers would reduce neu-ronal health and/or viability on their own (inde-pendent of a history of head trauma or some type ofbrain injury), a reduction in NAA would give pausewith respect to its hypothesized function as an out-come measure indicating neuronal viability. Suchresults may hint at metabolite differences as predis-posing factors, although the recovery of NAA duringabstinence from drugs of abuse argues against thatidea. However, 1H MRS studies investigating the ef-fects of natural reinforcers on brain chemistry wouldhelp elucidate some of the neurobiological mecha-nisms contributing to reward and reinforcement ingeneral.
Other spectroscopy methodsWithout going into much detail: in addition to1H, 31P and 13C MRS also hold a great deal ofpromise for in vivo drug abuse research. Phos-phorous spectra contain information regardingphospholipid metabolism, tissue bioenergetics, andpH. Specifically, the major peaks in the spectracorrespond to phosphomonoesters and phospho-diesters, both of which contribute to phospho-lipid metabolism.224,225 Major peaks also corre-spond to high-energy phosphates PCr; inorganicphosphate; and �-, �-, and �-nucleoside triphos-phate. Using 31P MRS, several studies have re-ported abnormalities in phospholipid and bioener-getic metabolism in the brains of cocaine-dependentpolydrug abusers226,227 and heroin-dependent in-dividuals early in their methadone maintenancetherapy.228,229 These results are consistent withthose obtained using 1H MRS, altogether sug-gesting drug-induced changes in cerebral bioen-ergetic states that may shift with increased absti-nence and/or treatment, as well as putative mem-brane changes that may be associated with neuronalviability.19,82,119,126
13C MRS has been developed relatively recently asa noninvasive measure of specific metabolic fluxeswithin the human brain. This technique exploits
the rapid synthesis of Glu, Gln, and GABA by mon-itoring the incorporation of 13C atoms of labeledprecursors (e.g., [1-13C]glucose) into the interme-diate metabolites of the tricarboxylic acid and Glu–Gln cycles.230 Subsequently, 13C MRS provides in-formation regarding the basic mechanisms govern-ing glial–neuronal interactions, particularly withrespect to glutamatergic function.231 Previous 13CMRS studies have demonstrated an inextricablelink between Glu neurotransmission and glucoseconsumption (which undoubtedly has been advan-tageous for interpreting the brain activation ob-served using functional imaging modalities),232,233
but the potential for this technique to be used drugabuse research is untouched. In fact, the use of13C MRS in human psychiatric research in gen-eral is still in its infancy, most likely owing inpart to the tradeoff between long infusion timesof substrate or reduced sensitivity when it is ad-ministered orally.234 However, the need to under-stand better how abnormalities in glia and/or aminoacid neurotransmission contribute to the etiologyof substance abuse (as well as a multitude of otherpsychiatric illnesses), will drive the technology toevolve.
LimitationsWhen considering the 1H MRS findings as a whole,one finds several methodological and technical andlimitations to take into account. First, many ofthe drug abuse studies summarized here relied onself-report of retrospective drug use. Although self-report is a critical aspect of many drug abuse studies,underreporting drug use is common, it varies acrossparticipant populations and with specific drug ofabuse,235 and it can become challenging when thepurity of the drug consumed is in question (e.g.,only 63% of ecstasy pills contain actual MDMA).236
Moreover, MDMA abusers in particular are noto-rious for being polydrug abusers,90 further compli-cating interpretation of any metabolite alterationsin this group of individuals. The retrospective studydesign is problematic in that one cannot draw in-ferences about a causative link between drug intakeand putative neurobiological consequences. How-ever, given the ethical issues surrounding adminis-tering potentially toxic drugs of abuse to human vol-unteers (e.g., cocaine’s effects extend beyond braininjury and include cardiovascular damage),237 moststudies to date have used this design, which while
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 161

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
somewhat dissatisfying is at least consistent acrossstudies.
Although 1H MRS has proven to be an amaz-ing research tool, there are limitations to this tech-nology with respect to the acquisition, quantifica-tion, and interpretation of the spectra. Several ofthese practical issues have been described at lengthelsewhere,238,239 but a few shortcomings stand out.For example, 1H MRS does not have the spatial ortemporal resolution of some other imaging tech-niques. The user must consider employing a single-voxel design versus chemical-shift imaging of aslab across the brain (potentially ≥40–50 voxels).A single-voxel design permits control of localiza-tion, improved shimming and water suppression,and requires shorter measurement times,240,241 butthese advantages are predicated on having chosenthe correct voxel for the measurement of interest.Chemical-shift imaging, on the other hand, cancover a larger region of interest, but as a resultit precludes precise localization, requires a longeracquisition time, and increases field inhomogene-ity.240,241 Importantly, neither design can provideinformation about a specific compartment wheremetabolite changes are taking place. For instance,although the overall concentration of Glu in thebrain is approximately 12 mM, concentrations varybetween gray matter and white matter because ofdifferent rates of synthesis and oxidation across tis-sue.28 Moreover, 1H MRS does not permit differen-tiation between the cytosolic versus vesicular poolswithin those gross compartments.242 Therefore, itis difficult to pinpoint the origin of any metabolitechanges, which ultimately does limit interpretationof spectral changes.
Similarly, regardless of the fact that the chemical-shift approach allows the investigator to obtain mul-tiple spectra simultaneously, whereas the single-voxel approach results in one spectrum, the spectrathemselves are only snapshots of the neurochemi-cal environment during the acquisition. Althoughtemporal resolution is determined in part by thestrength of the magnetic field, even at high fields(≥3 T) data are acquired on the order of min-utes.207 This time frame is acceptable for studiesthat use retrospective or longitudinal designs, butusing 1H MRS for human behavioral pharmacol-ogy during acute drug administration243 may ben-efit from faster acquisition. Taking these findingstogether, although 1H MRS provides a noninva-
sive window into neurochemical changes associatedwith substance abuse, one can still consider it a crudemeasurement.
Conclusions
Neuroimaging techniques, such as 1H MRS, areinvaluable tools for understanding the brain. Thestudies presented here indicate that reduced NAAand elevated mI may be neurochemical hallmarksof drug abuse–induced injury within the brain.Whether these changes are a result of the effectsof the chemicals on the brain specifically or whetherthey reflect the neurobiology driving the addictiveprocess in general (i.e., impairments in motivation–reward, affect regulation, and behavioral inhibition,as reviewed in Ref. 223), is unknown. In additionto giving insight regarding the neurochemical out-comes of drug abuse, 1H MRS also may providean opportunity to match individuals with the mostsuitable treatment, monitor treatment efficacy, andpredict and/or prevent relapse. Consequently, 1HMRS potentially could profoundly affect future drugabuse research.
Acknowledgments
This work was supported by National Institute onDrug Abuse Grants K01 DA023659 (S.C.L.) and K24DA151116 (P.F.R.).
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Bartsch, A.J., G. Homola, A. Biller, et al. 2007. Mani-
festations of early brain recovery associated with absti-
nence from alcoholism. Brain 130: 36–47.
2. Bendszus, M., H.G. Weijers, G. Wiesbeck, et al. 2001.
Sequential MR imaging and proton MR spectroscopy
in patients who underwent recent detoxification for
chronic alcoholism: correlation with clinical and neu-
ropsychological data. AJNR Am. J. Neuroradiol. 22:
1926–1932.
3. Durazzo, T.C., S. Gazdzinski, J.C. Rothlind, et al.
2006. Brain metabolite concentrations and neurocog-
nition during short-term recovery from alcohol depen-
dence: preliminary evidence of the effects of concurrent
chronic cigarette smoking. Alcohol Clin. Exp. Res. 30:
539–551.
162 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
4. Ende, G., H. Welzel, S. Walter, et al. 2005. Monitoring
the effects of chronic alcohol consumption and absti-
nence on brain metabolism: a longitudinal proton mag-
netic resonance spectroscopy study. Biol. Psychiatry 58:
974–980.
5. Parks, M.H., B.M. Dawant, W.R. Riddle, et al.
2002. Longitudinal brain metabolic characterization
of chronic alcoholics with proton magnetic resonance
spectroscopy. Alcohol Clin. Exp. Res. 26: 1368–1380.
6. Streeter, C.C., J. Hennen, Y. Ke, et al. 2005. Pre-
frontal GABA levels in cocaine-dependent subjects in-
crease with pramipexole and venlafazine treatment.
Psychopharmacology 182: 516–526.
7. Meyerhoff, D.J. & T.C. Durazzo. 2008. Proton magnetic
resonance spectroscopy in alcohol use disorders: a po-
tential new endophenotype. Alcohol Clin. Exp. Res. 32:
1146–1158.
8. Moore, C.M., B.B. Frederick & P.F. Renshaw. 1999.
Brain biochemistry using magnetic resonance spec-
troscopy: relevance to psychiatric illness in the elderly.
J. Geriatr. Psychiatry Neurol. 12: 107–117.
9. Moffett, J.R., B. Ross, P. Arun, et al. 2007. N-
Acetylaspartate in the CNS: from neurodiagnostics to
neurobiology. Prog. Neurobiol. 81: 89–131.
10. Pouwels, P.J. & J. Frahm. 1997. Differential distribution
of NAA and NAAG in human brain as determined by
quantitative localized proton MRS. NMR Biomed. 10:
73–78.
11. Tallan, H.H., S. Moore & W.H. Stein. 1956. N-Acetyl-
L-aspartic acid in brain. J. Biol. Chem. 219: 257–264.
12. Pouwels, P.J. & J. Frahm. 1998. Regional metabolite
concentrations in human brain as determined by quan-
titative localized proton MRS. Magn. Reson. Med. 39:
53–60.
13. Inglese, M., H. Rusinek, I.C. George, et al. 2008. Global
average gray and white matter N-acetylaspartate con-
centration in the human brain. Neuroimage 41: 270–
276.
14. Nadler, J.V. & J.R. Cooper. 1972. N-acetyl-aspartic acid
content of human neural tumours and bovine periph-
eral nervous tissues. J. Neurochem. 19: 313–319.
15. Brooks, W.M., S.D. Friedman & C. Gasparovic. 2001.
Magnetic resonance spectroscopy in traumatic brain
injury. J. Head Trauma Rehabil. 16: 149–164.
16. Chen, J.G., H.C. Charles, D.P. Barboriak, et al. 2000.
Magnetic resonance spectroscopy in Alzheimer’s dis-
ease: focus on N-acetylaspartate. Acta. Neurol. Scand.
Suppl. 176: 20–26.
17. Demougeot, C., C. Marie, M. Giroud, et al. 2004.
N-acetylaspartate: a literature review of animal re-
search on brain ischemia. J. Neurochem. 90: 776–
783.
18. Simone, I.L., C. Tortorella & F. Federico. 1999. The
contribution of (1)H-magnetic resonance spectroscopy
in defining the pathophysiology of multiple sclerosis.
Ital. J. Neurol. Sci. 20: S241–S245.
19. Li, S.-J., Y. Wang, J. Pankiewicz, et al. 1999. Neurochem-
ical adaptation to cocaine abuse: reduction of N-acetyl
aspartate in thalamus of human cocaine abusers. Biol.
Psychiatry 45: 1481–1487.
20. Stork, C. & P.F. Renshaw. 2005. Mitochondrial dys-
function in bipolar disorder: evidence from magnetic
resonance spectroscopy research. Mol. Psychiatry 10:
900–919.
21. Bonavita, S., F. Di Salle & G. Tedeschi. 1999. Proton
MRS in neurological disorders. Eur. J. Radiol. 30: 125–
131.
22. Frey, B.N., J.A. Stanley, F.G. Nery, et al. 2007. Abnormal
cellular energy and phopholipid metabolism in the left
dorsolateral prefrontal cortex of medication-free indi-
viduals with bipolar disorder: an in vivo 1H MRS study.
Bipolar Disord. 9(Suppl. 1): 119–127.
23. Yerli, H., A.M. Agildere, O. Ozen, et al. 2007. Evalu-
ation of cerebral glioma grade by using normal side
creatine as an internal reference in multi-voxel 1H-MR
spectroscopy. Diagn. Interv. Radiol. 13: 3–9.
24. King, K.G., L. Glodzik, S. Liu, et al. 2008. An-
teroposterior hippocampal metabolic heterogeneity:
three-dimensional multivoxel proton 1H MR spectro-
scopic imaging-initial findings. Radiology 249: 242–
250.
25. Miller, B.L. 1991. A review of chemical issues in 1H
NRM spectroscopy: N-acetyl-l aspartate, creatine and
choline. NMR Biomed. 4: 47–52.
26. Gonzalez-Toledo, E., R.E. Kelley & A. Minager. 2006.
Role of magnetic resonance spectroscopy in diagnosis
and management of multiple sclerosis. Neurol. Res. 28:
280–283.
27. Nakanishi, T., R.J. Turner & M.B. Burg. 1989. Osmoreg-
ulatory changes in myo-inositol transport by renal cells.
Proc. Natl. Acad. Sci. USA 86: 6002–6006.
28. Ross, B.D. 1991. Biochemical considerations in 1H
spectroscopy. Glutamate and glutamine; myo-inositol
and related metabolites. NMR Biomed. 4: 59–63.
29. Berridge, M.J. & R.F. Irvine. 1989. Inositol phosphates
and cell signaling. Nature 341: 197–205.
30. Kim, H., B.M. McGrath & P.H. Silverstone. 2005. A re-
view of the possible relevance of inositol and the phos-
phatidylinositol second messenger system (PI-cycle to
psychiatric disorders—focus on magnetic resonance
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 163

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
spectroscopy (MRS) studies. Hum. Psychopharmacol.
20: 309–326.
31. Brand, A., C. Richter-Landsberg & D. Leibfritz. 1993.
Multinuclear NMR studies on the energy metabolism
of glial and neuronal cells. Dev. Neurosci. 15: 289–298.
32. Behar, K.L. & D.L. Rothman. 2001. In vivo nu-
clear magnetic resonance studies of glutamate-gamma-
aminobutyric acid-glutamine cycling in rodent and hu-
man cortex: the central role of glutamine. J. Nutr. 131:
2498S–2504S.
33. Mullins, P.G., H. Chen, J. Xu, et al. 2008. Comparative
reliability of proton spectroscopy techniques designed
to improve detection of J-coupled metabolites. Magn.
Reson. Med. 60: 964–969.
34. Behar, K.L., D.L. Rothman, D.D. Spencer, et al. 1994.
Analysis of macromolecule resonances in 1H NMR
spectra of human brain. Magn. Reson. Med. 32: 294–
302.
35. Kish, S.J., T.L. Perry & S. Hansen. 1979. Regional distri-
bution of homocarnosine, homocarnosine-carnosine
synthetase and homocarnosinase in human brain. J.
Neurochem. 32: 1629–1636.
36. Gass, J.T. & M.F. Olive. 2008. Glutamatergic substrates
of drug addiction and alcoholism. Biochem. Pharmacol.
75: 218–265.
37. Torregrossa, M.M. & P.W. Kalivas. 2008. Microdialy-
sis and the neurochemistry of addiction. Pharmacol.
Biochem. Behav. 90: 261–272.
38. Quinton, M.S. & B.K. Yamamoto. 2006. Causes and
consequences of methamphetamine and MDMA toxi-
city. AAPS J. 18: E337-E347.
39. Ricaurte, G.A. & U.D. McCann. 1992. Neurotoxic am-
phetamine analogues: effects in monkeys and implica-
tions for humans. Ann. N. Y. Acad. Sci. 648: 371–382.
40. Ernst, T. & L. Chang. 2008. Adaptation of brain glu-
tamate plus glutamine during abstinence from chronic
methamphetamine use. J. Neuroimmune Pharmacol. 3:
165–172.
41. Cadet, J.L., I.N. Krasnova, S. Jayanthi, et al. 2007. Neu-
rotoxicity of substituted amphetamines: molecular and
cellular mechanisms. Neurotox. Res. 11: 183–202.
42. Lundqvist, T. 2005. Cognitive consequences of cannabis
use: comparison with abuse of stimulants and heroin
with regard to attention, memory and executive func-
tions. Pharmacol. Biochem. Behav. 81: 319–330.
43. McGrath, B.M., R. McKay, S. Dave, et al. 2008. Acute
dextro-amphetamine administration does not alter
brain myo-inositol levels in humans and animals: MRS
investigations at 3 and 18.8 T. Neurosci. Res. 61: 351–
359.
44. Silverstone, P.H., T. O’Donnell, M. Ulrich, et al. 2002.
Dextro amphetamine increases phosphoinositol cycle
activity in volunteers: an MRS study. Hum. Psychophar-
macol. 17: 425–429.
45. Berridge, M.J., C.P. Downes & M.R. Hanley. 1982.
Lithium amplifies agonist-dependent phosphatidyl-
inositol responses in brain and salivary glands. Biochem.
J. 206: 587–595.
46. Berridge, M.J., C.P. Downes & M.R. Hanley. 1989. Neu-
ral and developmental actions of lithium: a unifying
hypothesis. Cell 59: 411–419.
47. Kim, H., R.B. Thompson, C.C. Hanstock, et al. 2005.
Variability of metabolite yield using STEAM or PRESS
sequences in vivo at 3.0 T, illustrated with myo-inositol.
Magn. Reson. Med. 53: 760–769.
48. Melega, W.P., J. Quintana, M.J. Raleigh, et al. 1996.
6-[18F]fluoro-L-DOPA-PET studies show partial re-
versibility of long-term effects of chronic amphetamine
in monkeys. Synapse 22: 63–69.
49. Ridley, R.M., H.F. Baker, F. Owen, et al. 1982. Be-
havioural and biochemical effects of chronic am-
phetamine treatment in the vervet monkey. Psychophar-
macology 78: 245–251.
50. Steranka, L.R. & E. Sanders-Bush. 1980. Long-term ef-
fects of continuous exposure to amphetamine on brain
dopamine concentration and synaptosomal uptake in
mice. Eur. J. Pharmacol. 65: 439–443.
51. Wagner, G.C., G.A. Ricaurte, C.E. Johanson, et al. 1980.
Amphetamine induces depletion of dopamine and loss
of dopamine uptake sites in caudate. Neurology 30: 547–
550.
52. McCann, U.D., D.F. Wong, F. Yokoi, et al. 1998. Re-
duced striatal dopamine transporter density in absti-
nent methamphetamine and methcathinone users: evi-
dence from positron emission tomography studies with
[11C]WIN-35,428. J. Neurosci. 18: 8417–8422.
53. Volkow, N.D., L. Chang, G.J. Wang, et al. 2001. Asso-
ciation of dopamine transporter reduction with psy-
chomotor impairment in methamphetamine abusers.
Am. J. Psychiatry 158: 377–382.
54. Sekine, Y., Y. Ouchi, N. Takei, et al. 2006. Brain sero-
tonin transporter density and aggression in abstinent
methamphetamine abusers. Arch. Gen. Psychiatry 63:
90–100.
55. London, E.D., S.L. Simon, S.M. Berman, et al. 2004.
Mood disturbances and regional cerebral metabolic
abnormalities in recently abstinent methamphetamine
abusers. Arch. Gen. Psychiatry 61: 73–84.
56. Volkow, N.D., L. Chang, G.J. Wang, et al. 2001. Higher
cortical and lower subcortical metabolism in detoxified
164 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
methamphetamine abusers. Am. J. Psychiatry 158: 383–
389.
57. Wang, G.J., N.D. Volkow, L. Chang, et al. 2004. Par-
tial recovery of brain metabolism in methamphetamine
abusers after protracted abstinence. Am. J. Psychiatry
161: 242–248.
58. Chang, L., C. Cloak, K. Patterson, et al. 2005. Enlarged
striatum in abstinent methamphetamine abusers: a
possible compensatory response. Biol. Psychiatry 57:
967–974.
59. Chung, A., I.K. Lyoo, S.J. Kim, et al. 2007. Decreased
frontal white-matter integrity in abstinent metham-
phetamine abusers. Int. J. Neuropsychopharmacol. 10:
765–775.
60. Kim, S.J., I.K. Lyoo, J. Hwang, et al. 2006. Prefrontal
grey-matter changes in short-term and long-term ab-
stinent methamphetamine abusers. Int. J. Neuropsy-
chopharmacol. 9: 221–228.
61. Thompson, P.M., K.M. Hayashi, S.L. Simon, et al. 2004.
Structural abnormalities in the brains of human sub-
jects who use methamphetamine. J. Neurosci. 24: 6028–
6036.
62. Ernst, T., L. Chang, M. Leonido-Yee, et al. 2000. Ev-
idence for long-term neurotoxicity associated with
methamphetamine abuse: A 1H MRS study. Neurology
54: 1344–1349.
63. Nordahl, T.E., R. Salo, K. Possin, et al. 2002. Low
N-acetyl-aspartate and high choline in the anterior
cingulum of recently abstinent methamphetamine-
dependent subjects: a preliminary proton MRS study.
Magnetic resonance spectroscopy. Psychiatry Res. 116:
43–52.
64. Nordahl, T.E., R. Salo, Y. Natsuaki, et al. 2005. Metham-
phetamine users in sustained abstinence: a proton mag-
netic resonance spectroscopy study. Arch. Gen. Psychi-
atry 62: 444–452.
65. Salo, R., T.E. Nordahl, Y. Natsuaki, et al. 2007.
Attentional control and brain metabolite levels in
methamphetamine abusers. Biol. Psychiatry 61: 1272–
1280.
66. Sung, Y.H., S.C. Cho, J. Hwang, et al. 2007. Relation-
ship between N-acetyl-aspartate in gray and white mat-
ter of abstinent methamphetamine abusers and their
history of drug abuse: a proton magnetic resonance
spectroscopy study. Drug Alcohol Depend. 88: 28–35.
67. Sekine, Y., Y. Minabe, M. Kawai, et al. 2002.
Metabolite alterations in basal ganglia associated with
methamphetamine-related psychiatric symptoms. A
proton MRS study. Neuropsychopharmacology 27: 453–
461.
68. Nash, J.F. & B.K. Yamamoto. 1992. Methamphetamine
neurotoxicity and striatal glutamate release: compar-
ison to 3,4-methylenedioxymethamphetamine. Brain
Res. 581: 237–243.
69. Yamamoto, B.K. & M.G. Bankson. 2005. Amphetamine
neurotoxicity: cause and consequence of oxidative
stress. Crit. Rev. Neurobiol. 17: 87–118.
70. Baker, D.A., K. McFarland, R.W. Lake, et al. 2003. Neu-
roadaptations in cystine–glutamate exchange underlie
cocaine relapse. Nat. Neurosci. 6: 743–749.
71. LaRowe, S.D., H. Myrick, S. Hedden, et al. 2007. Is
cocaine desire reduced by N-acetylcysteine? Am. J. Psy-
chiatry 164: 1115–1117.
72. Mardikian, P.N., S.D. LaRowe, S. Hedden, et al. 2007.
An open-label trial of N-acetylcysteine for the treat-
ment of cocaine dependence: a pilot study. Prog. Neu-
ropsychopharmacol. Biol. Psychiatry 31: 389–394.
73. Gouzoulis-Mayfrank, E. & J. Daumann. 2006. Neuro-
toxicity of methylenedioxyamphetamines (MDMA; ec-
stasy) in humans: how strong is the evidence for persis-
tent brain damage? Addiction 101: 348–361.
74. Creighton, F.J., D.L. Black & C.E. Hyde. 1991. ‘Ecstasy’
psychosis and flashbacks. Br. J. Psychiatry 159: 713–715.
75. Fetter, J.C. 2005. Mirtazepine for MDMA-induced de-
pression. Am. J. Addict. 14: 300–301.
76. Pallanti, S. & D. Mazzi. 1992. MDMA (Ecstasy) precip-
itation of panic disorder. Biol. Psychiatry 32: 91–95.
77. Soar, K., A.C. Parrott & H.C. Fox. 2004. Persistent neu-
ropsychological problems after 7 years of abstinence
from recreational Ecstasty (MDMA): a case study. Psy-
chol. Rep. 95: 192–196.
78. McCann, U.D., S.C. Peterson & G.A. Ricaurte. 2007.
The effect of catecholamine depletion by alpha-methyl-
para-tyrosine on measures of cognitive performance
and sleep in abstinent MDMA users. Neuropsychophar-
macology 32: 1695–1706.
79. Reneman, L., C.B. Majoie, B. Schmand, et al. 2001.
Prefrontal N-acetylaspartate is strongly associated with
memory performance in (abstinent) ecstasy users: pre-
liminary report. Biol. Psychiatry 50: 550–554.
80. Reneman, L., C.B. Majoie, H. Flick, et al. 2002. Re-
duced N-acetylaspartate levels in the frontal cortex of
3,4-methylenedioxymethamphetamine (Ecstasy) users:
preliminary results. AJNR Am. J. Neuroradiol. 23: 231–
237.
81. Daumann, J., T. Fischermann, U. Pilatus, et al. 2004.
Proton magnetic resonance spectroscopy in ecstasy
(MDMA) users. Neurosci. Lett. 362: 113–116.
82. Chang, L., T. Ernst, C.S. Grob, et al. 1999.
Cerebral (1)H MRS alterations in recreational
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 165

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
3,4-methylenedioxymethamphetamine (MDMA, “ec-
stasy”) users. J. Magn. Reson. Imaging 10: 521–526.
83. Cowan, R.L. 2007. Neuroimaging research in human
MDMA users: a review. Psychopharmacology 189: 539–
556.
84. Cowan, R.L., J.M. Joers & M.S. Dietrich. 2009.
N-acetylaspartate (NAA) correlates inversely with
cannabis use in a frontal language processing region
of neocortex in MDMA (Ecstasy) polydrug users: a 3
T magnetic resonance spectroscopy study. Pharmacol.
Biochem. Behav. 92: 105–110.
85. de Win, M.M., L. Reneman, G. Jager, et al. 2007. A
prospective cohort study on sustained effects of low-
dose ecstasy use on the brain in new ecstasy users. Neu-
ropsychopharmacology 32: 458–470.
86. de Win, M.M., G. Jager, J. Booij, et al. 2008. Sustained
effects of ecstasy on the human brain: a prospective
neuroimaging study in novel users. Brain 131(Pt 11):
2936–2945.
87. de Win, M.M., G. Jager, J. Booij, et al. 2008. Neurotoxic
effects of ecstasy on the thalamus. Br. J. Psychiatry 193:
289–296.
88. Cowan, R.L., N.R. Bolo, M. Dietrich, et al. 2007. Oc-
cipital cortical proton MRS at 4 Tesla in human mod-
erate MDMA polydrug users. Psychiatry Res. 155: 179–
188.
89. Obergriesser, T., G. Ende, D.F. Braus, et al. 2001. Hip-
pocampal 1H-MRSI in ecstasy users. Eur. Arch. Psychi-
atry Clin. Neurosci. 251: 114–116.
90. Gouzoulis-Mayfrank, E. & J. Daumann. 2006. The con-
founding problem of polydrug use in recreational ec-
stasy/MDMA users: a brief overview. J. Psychopharma-
col. 20: 188–193.
91. Meyer, J.S., M.E. Brevard, B.J. Piper, et al. 2006. Neural
effects of MDMA as determined by functional mag-
netic resonance imaging and magnetic resonance spec-
troscopy in awake marmoset monkeys. Ann. N. Y. Acad.
Sci. 1074: 365–376.
92. McCardle, K., S. Luebbers, J.D. Carter, et al. 2004.
Chronic MDMA (ecstasy) use, cognition and mood.
Psychopharmacology 173: 434–439.
93. Kaufman, M.J., J.M. Levin, M.H. Ross, et al. 1998.
Cocaine-induced cerebral vasoconstriction detected in
humans with magnetic resonance angiography. JAMA
279: 376–380.
94. Du, C., M. Yu, N.D. Volkow, et al. 2006. Cocaine in-
creases the intracellular calcium concentration in brain
independently of its cerebrovascular effects. J. Neurosci.
26: 11522–11531.
95. Meldrum, B.S. 1986. Cell damage in epilepsy and the
role of calcium in cytotoxicity. Adv. Neurol. 44: 849–
855.
96. Schanne, F.A., A.B. Kane, E.E. Young, et al. 1979. Cal-
cium dependence of toxic cell death: a final common
pathway. Science 206: 700–702.
97. Chang, L., T. Ernst, T. Strickland, et al. 1999. Gender
effects on persistent cerebral metabolite changes in the
frontal lobes of abstinent cocaine users. Am. J. Psychia-
try 156: 716–722.
98. Chang, L., C.M. Mehringer, T. Ernst, et al. 1997. Neuro-
chemical alterations in asymptomatic abstinent cocaine
users: a proton magnetic resonance spectroscopy study.
Biol. Psychiatry 42: 1105–1114.
99. Ke, Y., C.C. Streeter, L.E. Nassar, et al. 2004. Frontal
lobe GABA levels in cocaine dependence: a two-
dimensional, J-resolved magnetic resonance spec-
troscopy study. Psychiatry Res. 130: 283–293.
100. Cendes, F., F. Andermann, F. Dubeau, et al. 1997.
Normalization of neuronal metabolic dysfunction af-
ter surgery for temporal lobe epilepsy. Evidence from
proton MR spectroscopic imaging. Neurology 49: 1525–
1533
101. De Stefano, N., P.M. Matthews & D.L. Arnold. 1995.
Reversible decreases in N- acetylaspartate after acute
brain injury. Magn. Reson. Med. 34: 721–727.
102. Fein, G., V. Di Sclafani & D.J. Meyerhoff. 2002.
Prefrontal cortical volume reduction associated with
frontal cortex function deficit in 6-week abstinent
crack-cocaine dependent men. Drug Alcohol Depend.
68: 87–93.
103. Matochik, J.A., E.D. London, D.A. Eldreth, et al. 2003.
Frontal cortical tissue composition in abstinent cocaine
abusers: a magnetic resonance imaging study. Neuroim-
age 19: 1095–1102.
104. Sim, M.E., I.K. Lyoo, C.C. Streeter, et al. 2007. Cere-
bellar gray matter volume correlates with duration of
cocaine use in cocaine-dependent subjects. Neuropsy-
chopharmacology 32: 2229–2237.
105. Li, S.-J., Y. Wang, R. Risinger, et al. 1998. Acute co-
caine administration induces NAA increase detected
by 1H MRS. In Proc. Int. Soc. Magn. Reson. Med. 6:
1714.
106. Christensen, J.D, M.J. Kaufman, B. Frederick, et al.
2000. Proton magnetic resonance spectroscopy of hu-
man basal ganglia: response to cocaine administration.
Biol. Psychiatry 48: 685–692.
107. Lien, R., O.P. Mishra, E. Graham, et al. 1994. Alteration
of brain cell membrane function following cocaine ex-
posure in the fetal guinea pig. Brain Res. 637: 249–
254.
166 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
108. Hertz, L., W.E. Code & E. Sykova. 1992. Ions, water and
energy in brain cells: a synopsis of interrelations. Can.
J. Physiol. Pharmacol. 70: S100–S106.
109. Olson, J., R. Sankar, D. Holtzman, et al. 1986. Energy-
dependent volume regulation in primary cultured cere-
bral astrocytes. J. Cell. Physiol. 128: 209–215.
110. Li, B.S., H. Wang & O. Gonen. 2003. Metabolite ratios
to assumed stable creatine levels may confound the
quantification of proton brain MR spectroscopy. Magn.
Reson. Imaging 21: 923–928.
111. Kaufman, M.J., J.M. Levin, L.C. Maas, et al. 2001.
Cocaine-induced cerebral vasoconstriction differs as a
function of sex and menstrual cycle phase. Biol. Psychi-
atry 49: 774–781.
112. Hetherington, H.P., J.W. Pan, F. Telang, et al. 2000.
Reduced brain GABA levels in cocaine abusers. In Proc.
Int. Soc. Magn. Reson. Med. 8: 523.
113. Aron, J.L. & M.P. Paulus. 2007. Location, location: us-
ing functional magnetic resonance imaging to pinpoint
brain differences relevant to stimulant use. Addiction
102: 33–43.
114. Preti, A. 2007. New developments in the pharmacother-
apy of cocaine abuse. Addict. Biol. 12: 133–151.
115. Gruber, S.A., M.M. Silveri, D.A. Yurgelun-Todd. 2007.
Neuropsychological consequences of opiate use. Neu-
ropsychol. Rev. 17: 299–315.
116. Wise, R.A. & M.A. Bozarth. 1982. Action of drugs of
abuse on brain reward systems: an update with specific
attention to opiates. Pharmacol. Biochem. Behav. 17:
239–243.
117. Ersche, K.D., P.C. Fletcher, S.J.G. Lewis, et al. 2005.
Abnormal frontal activations related to decision mak-
ing in current and former amphetamine and opiate
dependent individuals. Psychopharmacology 180: 612–
623.
118. Forman, S.D., G.G. Dougherty, B.J. Casey, et al. 2004.
Opiate addicts lack error- dependent activation of ros-
tral anterior cingulate. Biol. Psychiatry 55: 531–537.
119. Yucel, M., D.I. Lubman, B.J. Harrison, et al. 2007. A
combined spectroscopic and functional MRI investiga-
tion of the dorsal anterior cingulate region in opiate
addiction. Mol. Psychiatry 12: 611, 691–702.
120. Danos, P., S. Kasper, F. Grunwald, et al. 1998. Patholog-
ical regional cerebral blood flow in opiate-dependent
patients during withdrawal: a HMPAO-SPECT study.
Neuropsychobiology 37: 194–199.
121. Galynker, I.I., S. Watras-Ganz, C. Miner, et al. 2000.
Cerebral metabolism in opiate-dependent subjects: ef-
fects of methadone maintenance. Mt. Sinai J. Med. 67:
381–387.
122. Krystal, J.H., S.W. Woods, T.R. Kosten, et al. 1995.
Opiate dependence and withdrawal: preliminary as-
sessment using single photon emission computerized
tomography (SPECT). Am. J. Drug Alcohol Abuse 21:
47–63.
123. Rose, J.S., M. Branchey, L. Buydens-Branchey, et al.
1996. Cerebral perfusion deficits in early and late opiate
withdrawal: a technetium-99m-HMPAO SPECT study.
Psychiatry Res. 67: 39–47.
124. Lyoo, I.K., C.C. Streeter, K.H. Ahn, et al. 2004. White
matter hyperintensities in subjects with cocaine and
opiate dependence and healthy comparison subjects.
Psychiatry Res. 131: 2229–2237.
125. Lyoo, I.K., M.H. Pollack, M.M. Silveri, et al. 2006. Pre-
frontal and temporal gray matter density decreases in
opiate dependence. Psychopharmacology 184: 139–144.
126. Haselhorst, R., K.M. Dursteler-MacFarland, K. Schef-
fler, et al. 2002. Frontocortical N-acetylaspartate reduc-
tion associated with long-term i.v. heroin use. Neurol-
ogy 58: 305–307.
127. Kriegstein, A.R., D.C. Shungu, W.S. Millar, et al. 1999.
Leukoencephalopathy and raised brain lactate from
heroin vapor inhalation (“chasing the dragon”). Neu-
rology 53: 1765–1773.
128. Offiah, C. & E. Hall. 2008. Heroin-induced leukoen-
cephalopathy: characterization using MRI, diffusion-
weighted imaging, and MR spectroscopy. Clin. Radiol.
63: 146–152.
129. Mathews, P.M., F. Andermann, K. Silver, et al. 1993. Pro-
ton MR spectroscopic characterization of differences in
regional brain metabolic abnormalities in mitochon-
drial encephalomyopathies. Neurology 43: 2484–2490.
130. Xiang, Y., H. Gao, H. Zhu, et al. 2006. Neurochemical
changes in brain induced by chronic morphine treat-
ment: NMR studies in thalamus and somatosensory
cortex of rats. Neurochem. Res. 31: 1255–1261.
131. Murray, R.M., P.D. Morrison, C. Henquet, et al. 2007.
Cannabis, the mind and society: the hash realities. Nat.
Rev. Neurosci. 8: 885–895.
132. Chan, G.C., T.R. Hinds, S. Impey, et al. 1998. Hip-
pocampal neurotoxicity of �9- tetrahydrocannabinol.
J. Neurosci. 18: 5322–5332.
133. Landfield, P.W., L.B. Cadwallader & S. Vinsant. 1988.
Quantitative changes in hippocampal structure fol-
lowing long-term exposure to delta 9- tetrahydro-
cannabinol: possible mediation by glucocorticoid sys-
tems. Brain Res. 443: 47–62.
134. Yucel, M., N. Solowij, C. Respondek, et al. 2008. Re-
gional brain abnormalities associated with long-term
heavy cannabis use. Arch. Gen. Psychiatry 65: 694–701.
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 167

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
135. Chang, L., C. Cloak, R. Yakupov, et al. 2006. Combined
and independent effects of chronic marijuana use and
HIV on brain metabolites. J. Neuroimmune Pharmacol.
1: 65–76.
136. Hermann, D., A. Sartorius, H. Welzel, et al. 2007. Dor-
solateral prefrontal cortex N-acetylaspartate/total crea-
tine (NAA/tCr) loss in male recreational cannabis users.
Biol. Psychiatry 61: 1281–1289.
137. Bertolino, A., D. Sciota, F. Brudaglio, et al. 2003. Work-
ing memory deficits and levels of N-acetylaspartate in
patients with schizophreniform disorder. Am. J. Psychi-
atry 160: 483–489.
138. Molina, V., J. Sanchez, S. Reig, et al. 2005. N-acetyl-
aspartate levels in the dorsolateral prefrontal cortex in
the early years of schizophrenia are inversely related to
disease duration. Schizophr. Res. 73: 209–219.
139. Henquet, C., M. Di Forti, P. Morrison, et al. 2008. Gene-
environment interplay between cannabis and psychosis.
Schizophr. Bull. 34: 1111–1121.
140. Kril, J.J. & G.M. Halliday. 1999. Brain shrinkage in al-
coholics: a decade on and what have we learned? Prog.
Neurobiol. 58: 381–387.
141. Sullivan, E.V. 2000. Human brain vulnerability to alco-
holism: evidence from neuroimaging studies. In Review
of NIAAA’s Neuroscience and Behavioral Research Portfo-
lio (NIAAA Research Monograph No. 34). A. Noronha,
M. Eckardt & K. Warren, Eds.: 473–508. National Insti-
tute on Alcohol Abuse and Alcoholism. Bethesda, MD.
142. Oscar-Berman, M. & K. Marinkovic. 2007. Alcohol: ef-
fects on neurobehavioral functions and the brain. Neu-
ropsychol. Rev. 17: 239–257.
143. Durazzo, T.C., S. Gazdzinski, P. Banys, et al. 2004.
Cigarette smoking exacerbates chronic alcohol-induced
brain damage: a preliminary metabolite imaging study.
Alcohol Clin. Exp. Res. 28: 1849–1860.
144. Jagannathan, N.R., N.G. Desai & P. Raghunathan. 1996.
Brain metabolite changes in alcoholism: an in vivo
proton magnetic resonance spectroscopy (MRS) study.
Magn. Reson. Imaging 14: 553–557.
145. Schweinsburg, B.C., M.J. Taylor, O.M. Alhassoon, et
al. 2001. Chemical pathology in brain white matter of
recently detoxified alcoholics: a 1H magnetic resonance
spectroscopy investigation of alcohol-associated frontal
lobe injury. Alcohol Clin. Exp. Res. 25: 924–934.
146. Schweinsburg, B.C., O.M. Alahassoon, M.J. Taylor, et
al. 2003. Effects of alcoholism and gender on brain
metabolism. Am. J. Psychiatry 160: 1180–1183.
147. Schweinsburg, B.C., M.J. Taylor, J.S. Videen, et al. 2000.
Elevated myo-inositol in gray matter of recently detox-
ified but not long-term abstinent alcoholics: a prelimi-
nary MR spectroscopy study. Alcohol Clin. Exp. Res. 24:
699–705.
148. Seitz, D., U. Widmann, U. Seeger, et al. 1999. Localized
proton magnetic resonance spectroscopy of the cere-
bellum in detoxifying alcoholics. Alcohol Clin. Exp. Res.
23: 158–163.
149. Lee, E., D.P. Jang, J.J. Kim, et al. 2007. Al-
teration of brain metabolites in young alcoholics
without structural changes. Neuroreport 18: 1511–
1514.
150. Miese, F., G. Kircheis, H.J. Wittsack, et al. 2006. 1H-MR
spectroscopy, magnetization transfer, and diffusion-
weighted imaging in alcoholic and nonalcoholic pa-
tients with cirrhosis with hepatic encephalopathy. AJNR
Am. J. Neuroradiol. 27: 1019–1026.
151. Martin, P.R., S.J. Gibbs, A.A. Nimmerrichter, et al. 1995.
Brain proton magnetic resonance spectroscopy studies
in recently abstinent alcoholics. Alcohol Clin. Exp. Res.
19: 1078–1082.
152. O’Neill, J., V.A. Cardenas & D.J. Meyerhoff. 2001. Ef-
fects of abstinence on the brain: quantitative magnetic
resonance imaging and magnetic resonance spectro-
scopic imaging in chronic alcohol abuse. Alcohol Clin.
Exp. Res. 25: 1673–1682.
153. Meyerhoff, D.J., R. Blumenfeld, D. Truran, et al. 2004.
Effects of heavy drinking, binge drinking, and family
history of alcoholism on regional brain metabolites.
Alcohol Clin. Exp. Res. 28: 650–661.
154. Gazdzinski, S., T.C. Durazzo, M.W. Weiner, et al. 2008a.
Are treated alcoholics representative of the entire popu-
lation with alcohol use disorders? A magnetic resonance
study of brain injury. Alcohol 42: 67–76.
155. Vengeliene, V., A. Bilbao, A. Molander, et al. 2008. Neu-
ropharmacology of alcohol addiction. Br. J. Pharmacol.
154: 299–315.
156. Hoffman, P.L. & B. Tabakoff. 1996. Alcohol depen-
dence: a commentary on mechanisms. Alcohol Alcohol.
31: 333–340.
157. Tsai, G.E., P. Ragan, R. Chang, et al. 1998. Increased
glutamatergic neurotransmission and oxidative stress
after alcohol withdrawal. Am. J. Psychiatry 155: 726–
732.
158. Behar, K.L., D.L. Rothman, K.F. Petersen, et al. 1999.
Preliminary evidence of low cortical GABA levels in lo-
calized 1H-MR spectra of alcohol-dependent and hep-
atic encephalopathy patients. Am. J. Psychiatry 156:
952–954.
159. Mason, G.F., I.L. Petrakis, R.A. de Graaf, et al. 2006.
Cortical gamma-aminobutyric acid levels and the re-
covery from ethanol dependence: preliminary evidence
168 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
of modification by cigarette smoking. Biol. Psychiatry
59: 85–93.
160. Leshner, A.I. & G.F. Koob. 1999. Drugs of abuse and
the brain. Proc. Assoc. Am. Physicians 111: 99–108.
161. Alexander, G.E., M.D. Crutcher & M.R. DeLong. 1990.
Basal ganglia-thalamo-cortical circuits: parallel sub-
strates for motor, oculomotor, “prefrontal” and “lim-
bic” functions. Prog. Brain Res. 85: 119–146.
162. Levin, E.D., F.J. McClernon & A.H. Rezvani. 2006. Nico-
tinic effects on cognitive function: behavioral character-
ization, pharmacological specification, and anatomic
localization. Psychopharmacology 184: 523–539.
163. Gazdzinski, S., T.C. Durazzo, C. Studholme, et al. 2005.
Quantitative brain MRI in alcohol dependence: pre-
liminary evidence for effects of concurrent chronic
cigarette smoking on regional brain volumes. Alcohol
Clin. Exp. Res. 29: 1484- 1495.
164. Brody, A.L., M.A. Mandelkern, M.E. Jarvik, et al. 2004.
Differences between smokers and nonsmokers in re-
gional gray matter volumes and densities. Biol. Psychi-
atry 55: 77–84.
165. Gallinat, J., E. Meisenzahl, L.K. Jacobsen, et al. 2006.
Smoking and structural brain deficits: a volumetric MR
investigation. Eur. J. Neurosci. 24: 1744–1750.
166. Brody, A.L. 2006. Functional brain imaging of tobacco
use and dependence. J. Psychiatr. Res. 40: 404–418.
167. Markou, A. 2008. Review. Neurobiology of nicotine
dependence. Philos. Trans. R. Soc. Lond. B Biol. Sci. 363:
3159–3168.
168. Epperson, C.N., S. O’Malley, K.A. Czarkowski, et al.
2005. Sex, GABA, and nicotine: the impact of smok-
ing on cortical GABA levels across the menstrual cy-
cle as measured with proton magnetic resonance spec-
troscopy. Biol. Psychiatry 57: 44–48.
169. Gallinat, J. & F. Schubert. 2007. Regional cerebral glu-
tamate concentrations and chronic tobacco consump-
tion. Pharmacopsychiatry 40: 64–67.
170. Gallinat, J., U.E. Lang, L.K. Jacobsen, et al. 2007. Abnor-
mal hippocampal neurochemistry in smokers: evidence
from proton magnetic resonance spectroscopy at 3 T.
J. Clin. Psychopharmacol. 27: 80–84.
171. Barros, D.M., F.G. Galhardi, J.L. Ribas Ferreira, et al.
2007. The benefits and drawbacks of nicotine exposure
in the cortex and hippocampus of old rats. Neurotoxicity
28: 562–568.
172. Berger, F., F.H. Gage & S. Vijayaraghavan. 1998. Nico-
tinic receptor-induced apoptotic cell death of hip-
pocampal progenitor cells. J. Neurosci. 18: 6871–6881.
173. Trauth, J.A., F.J. Seidler, E.C. McCook, et al. 1999. Ado-
lescent nicotine exposure causes persistent upregula-
tion of nicotinic cholinergic receptors in rat brain re-
gions. Brain Res. 851: 9–19.
174. Burling, T.A. & D.C. Ziff. 1988. Tobacco smoking: a
comparison between alcohol and drug abuse inpatients.
Addict. Behav. 13: 185–190.
175. DiFranza, J.R. & M.P. Guerrera. 1990. Alcoholism and
smoking. J. Stud. Alcohol. 51: 130–135.
176. Littleton, J., S. Barron, M. Prendergast, et al. 2007.
Smoking kills (alcoholics)! Shouldn’t we do something
about it? Alcohol Alcohol. 42: 167–173.
177. Gazdzinski, S., T.C. Durazzo, G.-H. Jahng, et al. 2006.
Effects of chronic alcohol dependence and chronic
cigarette smoking on cerebral perfusion: a preliminary
magnetic resonance study. Alcohol Clin. Exp. Res. 30:
947–958.
178. Gazdzinski, S., T.C. Durazzo, P.H. Yeh, et al. 2008b.
Chronic cigarette smoking modulates injury and short-
term recovery of the medial temporal lobe in alcoholics.
Psychiatry Res. 162: 133–145.
179. Yucel, M., M. Takagi, M. Walterfang, et al. 2008.
Toluene misuse and long- term harms: a systematic
review of the neuropsychological and neuroimaging lit-
erature. Neurosci. Biobehav. Rev. 32: 910–926.
180. Gerasimov, M.R. 2004. Brain uptake and biodistribu-
tion of [11C]toluene in nonhuman primates and mice.
Meth. Enzymol. 385: 334–349.
181. Gospe, S.M. Jr. & M.J. Calaban. 1988. Central nervous
system distribution of inhaled toluene. Fundam. Appl.
Toxicol. 11: 540–545.
182. Giedd, J.N. 2008. The teen brain: insights from neu-
roimaging. J. Adolesc. Health 42: 335–343.
183. Rosenberg, N.L., B.K. Kleinschmidt-DeMasters, K.A.
Davis, et al. 1988. Toluene abuse causes diffuse central
nervous system white matter changes. Ann. Neurol. 23:
611–614.
184. Aydin, K., S. Sencer, T. Demir, et al. 2002. Cranial MR
findings in chronic toluene abuse by inhalation. AJNR
Am. J. Neuroradiol. 23: 1173–1179.
185. Filley, C.M., R.K. Heaton & N.L. Rosenberg. 1990.
White matter dementia in chronic toluene abuse. Neu-
rology 40: 532–534.
186. Yamanouchi, N., S. Okada, K. Kodama, et al. 1997.
Effects of MRI abnormalities on WAIS-R performance
in solvent abusers. Acta Neurol. Scand. 96: 34–39.
187. Ikeda, M. & H. Tsukagoshi. 1990. Encephalopathy due
to toluene sniffing. Report of a case with magnetic res-
onance imaging. Eur. Neurol. 30: 347–349.
188. Lubman, D.I., M. Yucel & A.J. Lawrence. 2008. Inhalant
abuse among adolescents: neurobiological considera-
tions. Br. J. Pharmacol. 154: 316–326.
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 169

Findings from 1H MRS studies in drug abuse research Licata & Renshaw
189. Rosenberg, N.L., J. Grigsby, J. Dreisbach, et al. 2002.
Neuropsychologic impairment and MRI abnormalities
associated with chronic solvent abuse. J. Toxicol. Clin.
Toxicol. 41: 209–210.
190. Zur, J. & W. Yule. 1990. Chronic solvent abuse. 1. Cog-
nitive sequelae. Child Care Health Dev. 16: 1–20.
191. Stengard, K. 1994. Effects of toluene inhalation on ex-
tracellular striatal acetylcholine release studied with mi-
crodialysis. Pharmacol. Toxicol. 75: 115–118.
192. Gerasimov, M.R., W.K. Schiffer, D. Marstellar, et al.
2002. Toluene inhalation produces regionally specific
changes in extracellular dopamine. Drug Alcohol De-
pend. 65: 243–251.
193. Riegel, A.C., A. Zapata, T.S. Shippenberg, et al. 2007.
The abused inhalant toluene increases dopamine re-
lease in the nucleus accumbens by directly stimulating
ventral tegmental area neurons. Neuropsychopharma-
cology 32: 1558–1569.
194. Stengard, K., R. Tham, W.T. O’Connor, et al. 1993.
Acute toluene exposure increases extracellular GABA in
the cerebellum of rat: a microdialysis study. Pharmacol.
Toxicol. 73: 315–318.
195. Win-Shwe, T.T., D. Mitsushima, D. Nakajima, et al.
2007. Toluene induces rapid and reversible rise of hip-
pocampal glutamate and taurine neurotransmitter lev-
els in mice. Toxicol. Lett. 168: 75–82.
196. Noda, S., N. Yamanouchi, S. Okada, et al. 1996. Proton
MR spectroscopy in solvent abusers. Ann. N. Y. Acad.
Sci. 801: 441–444.
197. Aydin, K., S. Sencer, K. Ogel, et al. 2003. Single-voxel
proton MR spectroscopy in toluene abuse. Magn. Reson.
Imaging 21: 777–785.
198. Ladefoged, O., P. Strange, A. Møller, et al. 1991. Irre-
versible effects in rats of toluene (inhalation) exposure
for six months. Pharmacol. Toxicol. 68: 384–390.
199. Escobar, A. & C. Aruffo. 1980. Chronic thinner intox-
ication: clinicopathologic report of a human case. J.
Neurol. Neurosurg. Psychiatry 43: 986–994.
200. Baydas, G., R.J. Reiter, V.S. Nedzvetskii, et al. 2003.
Melatonin protects the central nervous system of rats
against toluene-containing thinner intoxication by re-
ducing reactive gliosis. Toxicol. Lett. 137: 169–174.
201. Huang, J., N. Asaeda, Y. Takeuchi, et al. 1992. Dose
dependent effects of chronic exposure to toluene on
neuronal and glial cell marker proteins in the central
nervous system of rats. Br. J. Ind. Med. 49: 282–286.
202. Gotohda, T., I. Tokunaga, S. Kubo, et al. 2000. Effect
of toluene inhalation on astrocytes and neurotrophic
factor in rat brain. Forensic Sci. Int. 113: 233–238.
203. Takebayashi, K., Y. Sekine, N. Takei, et al. 2004. Metabo-
lite alterations in basal ganglia associated with psychi-
atric symptoms of abstinent toluene users: a proton
MRS study. Neuropsychopharmacology 29: 1019–1026.
204. Ertugrul, A. & B. Ulug. 2007. The effect of clozapine
on neuroimaging findings in schizophrenia. Psychiatr.
Danub. 19: 367–369.
205. Pedata, F., S. Sorbi & G. Pepeu. 2006. Choline high-
affinity uptake and metabolism and choline acetyltrans-
ferase activity in the striatum of rats chronically treated
with neuroleptics. J. Neurochem. 35: 606–611.
206. Bustillo, J.R., L.M. Rowland, J. Lauriello, et al. 2002.
High choline concentrations in the caudate nucleus in
antipsychotic-naıve patients with schizophrenia. Am. J.
Psychiatry 159: 130–133.
207. Di Costanzo, A., F. Trojsi, M. Tosetti, et al. 2003. High-
field proton MRS of human brain. Eur. J. Radiol. 48:
146–153.
208. Sawrie, S.M., R.C. Martin, R. Knowlton, et al. 2001.
Relationships among hippocampal volumetry, proton
magnetic resonance spectroscopy, and verbal memory
in temporal lobe epilepsy. Epilepsia 42: 1403–1407.
209. Grachev, I.D., R. Kumar, T.S. Ramachandran, et al.
2001. Cognitive interference is associated with neuronal
marker N-acetyl aspartate in the anterior cingulate cor-
tex: an in vivo (1)H-MRS study of the Stroop Color-
Word task. Mol. Psychiatry 6: 529–539.
210. Ohrmann, P., A. Siegmund, T. Suslow, et al. 2007.
Cognitive impairment and in vivo metabolites in
first-episode neuroleptic-naıve and chronic medicated
schizophrenic patients: a proton magnetic resonance
spectroscopy study. J. Psychiatry Res. 41: 625–634.
211. Field, M. & W.M. Cox. 2008. Attentional bias in addic-
tive behaviors: a review of its development, causes, and
consequences. Drug Alcohol Depend. 97: 1–20.
212. Robbins, T.W., K.D. Ersche & B.J. Everitt. 2008. Drug
addiction and the memory systems of the brain. Ann.
N. Y. Acad. Sci. 1141: 1–21.
213. Lin, A., B.D. Ross, K. Harris, et al. 2005. Efficacy of
proton magnetic resonance spectroscopy in neurolog-
ical diagnosis and neurotherapeutic decision making.
NeuroRx 2: 197–214.
214. Kushner, S.A., S.L. Dewey & C. Kornetsky. 1999.
The irreversible gamma-aminobutyric acid (GABA)
transaminase inhibitor gamma-vinyl-GABA blocks co-
caine self-administration in rats. J. Pharmacol. Exp.
Ther. 290: 797–802.
215. Stromberg, M., S. Mackler, J. Volpecelli, et al. 2001.
The effect of gamma-vinyl-GABA on the consumption
of concurrently available oral cocaine and ethanol in
the rat. Pharmacol. Biochem. Behav. 68: 291–299.
170 Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences.

Licata & Renshaw Findings from 1H MRS studies in drug abuse research
216. Brebner, K., A. Childress & D. Roberts. 2002. A po-
tential role for GABA(B) agonists in the treatment of
psychostimulant addiction. Alcohol Alcohol. 37: 478–
484.
217. Gonzalez, G., K. Sevarino, M. Sofuoglu, et al. 2003.
Tiagabine increases cocaine-free urines in cocaine-
dependent methadone-treated patients: results of a ran-
domized pilot study. Addiction 98: 1625–1632.
218. Kampman, K.M., H. Pettinati, K.G. Lynch, et al. 2004.
A pilot trial of topiramate for the treatment of cocaine
dependence. Drug Alcohol Depend. 75: 233–240.
219. Winhusen, T.M., E.C. Somoza, J.M. Harrer, et al. 2005.
A placebo-controlled screening trial of tiagabine, ser-
traline and donepezil as cocaine dependence treat-
ments. Addiction 100(Suppl. 1): 68–77.
220. Kreis, R., T. Ernst & B.D. Ross. 1993. Development of
the human brain: in vivo quantification of metabo-
lite and water content with proton magnetic resonance
spectroscopy. Magn. Reson. Med. 30: 424–437.
221. Pouwels, P.J., K. Brockmann, B. Kruse, et al. 1999. Re-
gional age dependence of human brain metabolites
from infancy to adulthood as detected by quantitative
localized proton MRS. Pediatr. Res. 46: 474–485.
222. Smith, L.M., L. Chang, M.L. Yonekura, et al. 2001. Brain
proton magnetic resonance spectroscopy in children
exposed to methamphetamine in utero. Neurology 57:
255–260.
223. Goodman, A. 2008. Neurobiology of addiction. An in-
tegrative review. Biochem. Pharmacol. 75: 266–322.
224. Murphy, E.J., B. Rajagopalan, K.M. Brindle, et al. 1989.
Phospholipid bilayer contribution to 31P NMR spectra
in vivo. Magn. Reson. Med. 12: 282–289.
225. Pettegrew, J., S. Kopp, N. Minshew, et al. 1987. 31P Nu-
clear magnetic resonance studies of phosphoglyceride
metabolism in developing and degenerating brain: pre-
liminary observations. J. Neuropath. Exp. Neurol. 46:
419–430.
226. Christensen, J.D., M.J. Kaufman, J.M. Levin, et al. 1996.
Abnormal cerebral metabolism in polydrug abusers
during early withdrawal: a 31P MR spectroscopy study.
Magn. Reson. Med. 35: 658–663.
227. MacKay, S., D.J. Meyerhoff, W.P. Dillon, et al. 1993. Al-
teration of brain phospholipid metabolites in cocaine-
dependent polysubstance abusers. Biol. Psychiatry 34:
261–264.
228. Kaufman, M.J., M.H. Pollack, R.A. Villafuerte, et al.
1999. Cerebral phosphorus metabolite abnormalities
in opiate-dependent polydrug abusers in methadone
maintenance. Psychiatry Res. 90: 143–152.
229. Silveri, M.M., M.H. Pollack, C.I. Diaz, et al. 2004. Cere-
bral phosphorus metabolite and transverse relaxation
time abnormalities in heroin-dependent subjects at on-
set of methadone maintenance treatment. Psychiatry
Res. 131: 217- 226.
230. de Graaf, R.A., G.F. Mason, A.B. Patel, et al. 2003. In vivo
1H-[13C]-NMR spectroscopy of cerebral metabolism.
NMR Biomed. 16: 339–357.
231. Magistretti, P.J., L. Pellerin, D.L. Rothman, et al. 1999.
Energy on demand. Science 283: 496–497.
232. Mason, G.F., R. Gruetter, D.L. Rothman, et al. 1995. Si-
multaneous determination of the rates of the TCA cy-
cle, glucose utilization, alpha-ketoglutarate/glutamate
exchange, and glutamine synthesis in human brain by
NMR. J. Cereb. Blood Flow Metab. 15: 12–25.
233. Sibson, N.R., A. Dhankhar, G.F. Mason, et al. 1998.
Stoichiometric coupling of brain glucose metabolism
and glutamatergic neuronal activity. Proc. Natl. Acad.
Sci. USA 95: 316–321.
234. Mason, G.F. & J.H. Krystal. 2006. MR spectroscopy: its
potential role for drug development for the treatment
of psychiatric diseases. NMR Biomed. 19: 690–701.
235. Neale, J. & M. Robertson. 2003. Comparisons of self-
report data and oral fluid testing in detecting drug use
amongst new treatment clients. Drug Alcohol Depend.
71: 57–64.
236. Baggot, M., B. Heifets, R.T. Jones, et al. 2000. Chemical
analysis of ecstasy pills. JAMA 284: 2190.
237. Nahas, G.G. 1990. The experimental use of cocaine in
human subjects. Bull. Narc. 42: 57–62.
238. Capizzano, A.A., R.E. Jorge, L.C. Acion, et al. 2007. In
vivo proton magnetic resonance spectroscopy in pa-
tients with mood disorders: a technically oriented re-
view. J. Magn. Reson. Imaging 26: 1378–1389.
239. Frahm, J., T. Michaelis, M. Klaus-Dietmar, et al. 1989.
Localized NMR spectroscopy in vivo. NMR Biomed. 2:
188–195.
240. De Stefano, N., M. Filippi, D. Miller, et al. 2007. Guide-
lines for using proton MR spectroscopy in multicenter
clinical MS studies. Neurology 69: 1942–1952.
241. Hsu, Y.-Y., C. Chang, C.-N. Chang, et al. 1999. Pro-
ton MR spectroscopy in patients with complex par-
tial seizures: single-voxel spectroscopy versus chemical-
shift imaging. AJNR Am. J. Neuroradiol. 20: 643–651.
242. Valette, J., M. Chaumeil, M. Guillermier, et al. 2008.
Diffusion-weighted NMR spectroscopy allows probing
of 13C labeling of glutamate inside distinct metabolic
compartments in the brain. Magn. Reson. Med. 60: 306–
311.
243. Licata, S.C., J.E. Jensen, D.M. Penetar, et al. 2009. A
therapeutic dose of zolpidem reduces thalamic GABA
in healthy volunteers: a proton MRS study at 4 Tesla.
Psychopharmacology 203: 819–829.
Ann. N.Y. Acad. Sci. 1187 (2010) 148–171 c© 2010 New York Academy of Sciences. 171






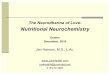

![[MDMA]MDMA Neurochemistry](https://img.pdfslide.us/doc/110x75/577dab601a28ab223f8c57f3/mdmamdma-neurochemistry.jpg)