Embed Size (px)
DESCRIPTION
Neurobiology of depression. 01.11.13 Laura Bohleber. Content. Introduction Brief repetition : symptomatology / diagnostic criteria / treatment guidelines We know little Validity criteria : animal models of depression The molecular neurobiology of depression - PowerPoint PPT Presentation
Citation preview

NEUROBIOLOGY OF DEPRESSION01.11.13 Laura Bohleber

CONTENTI. Introduction
1. Brief repetition: symptomatology / diagnostic criteria / treatment guidelines
2. We know little3. Validity criteria: animal models of depression
II. The molecular neurobiology of depression1. Neural circuitry of depression2. The role of monoamines3. Neurotrophins and neurogenesis4. Neuroendocrine and neuroimmune interactions5. Epigenetic mechanisms6. Resilence-related research7. New insights
III. The subgenual anterior cingulate cortex in mood disorders
IV. SummaryV. Journal club

I. Introduction I. Brief repetition: symptomatology / diagnostic criteria /
treatment guidelinesII. We know littleIII. Validity criteria: animal models of depression
II. The molecular neurobiology of depression
1. Neural circuitry of depression2. The role of monoamines3. Neurotrophins and neurogenesis4. Neuroendocrine and neuroimmune interactions5. Epigenetic mechanisms6. Resilence-related research7. New insights
III. The Subgenual Anterior Cingulate Cortex in Mood Disorders
IV. ConclusionsV. Journal club

1. Brief repetition: symptomatology / diagnostic criteria / treatment guidelines
Diagnostic criteria and Symptoms (ICD-10, F3 mood disorders) Major Depression (MDD)
Diagnosis F32 Depressive Episode: mild, moderate, severe, severe with psychotic symptoms (F32.0-
F32.3) F33 Recurrent Depressive Disorder: mild, moderate, severe, severe with psychotic symptoms
(F33.0-F33.3) Symptoms
depressed mood loss of interest and enjoyment reduced energy, increased fatiguability
Bipolar disorders (BD) Diagnosis
F31 Bipolar affective disorder, current episode hypomanic; manic without / with psychotic features; current episode depressed: mild, moderate, severe, severe with psychotic symptoms; current episode mixte; other bipolar disorders (F31.0-31.8)
Symptoms Repeated episodes (at least 2) of disturbed mood & activity level: elevation
of mood and increased energy and activity (mania or hypomania), and lowering of mood and decreased energy and activity (depression)
(a) reduced concentration and attention; (b) reduced self-esteem and self-confidence; (c) ideas of guilt and unworthiness (even in a mild type of episode); (d) bleak and pessimistic views of the future; (e) ideas or acts of self-harm or suicide; (f) disturbed sleep; (g) diminished appetite

Treatment guidelines (Working Group on the Management of Major Depression in Adults, 2008, (leaving psychotherapy aside))
Antidepressant drugs represent a first line of treatment for moderate or severe depression. For mild depression, other therapeutic strategies can be considered before antidepressant drugs.
Comparative Efficacy of Drugs Selective serotonin reuptake inhibitors (SSRIs) -> first choice TCAs are an alternative to SSRIs if a patient has not tolerated at least two
drugs from this group or is allergic to them
Duration of treatment Pharmacological treatment maintained in all patients for at least 6 months
after remission In patients with any previous episode or the presence of residual symptoms,
treatment maintained for at least 12 months after remission In patients with more than two previous episodes, treatment maintained for at
least 24 months after remission
Treatment resistance Switching from an antidepressant to any family, including another
serotonergic. Combining antidepressants. Augmenting the initiated treatment with lithium ECT should be considered as a therapeutic alternative in adults with severe
major depression

S3-Guideline/National Disease Management Guideline, http://www.versorgungsleitlinien.de/themen/depression/pdf/s3-nvl-depression-kurz-engl.pdf

Knowledge about pathophysiology of depression is rudimentary – why?1. Heterogeneous syndromes with heterogeneous etiology -
> weakness of trying to construct a “unifying” theory of depression
2. Observing pathological changes in the brain = difficult, limited techniques available (post mortem, neuroimaging, difficulties in transferring knowledge acquired from animal studies✗)
3. Idiopathy of occurance of depression (various risk factors, no consistent genetic risk modifiers). Interaction of genetic predispositions and environmental risk factors.
Symptom based diagnostic approach poses obvious obstacles
To the interpretation of genome-wide association studies To neuroimaging or post mortem investigation (with typical
heterogeneity in data acquiered from mood disorder samples, often consistent data only in subsets)
2. We know little

✗Preclinical models – interpretation of animal models of depression
Etiological validity (=depression-like behaviour need to be caused by the same etiologies that trigger human depression. BUT: absence of definitive aetiologies for human depression!)
Pharmacological validity (= assays are sensitive to acutely administered known antidepressant compounds. BUT more than half of all depressed individuals do not respond fully to available antidepressants)
Face validity (= behavioral changes brought about by stress or genetic manipulation superficially resemble depressive symptoms. E.g. animal’s decreased sucrose intake after chronic stress ≈ anhedonia)
3. Validity criteria : animal models of depression


I. Introduction 1. Brief repetition: symptomatology / diagnosis /
treatment guidelines2. We know little3. Validity criteria: animal models of depression
II. The molecular neurobiology of depression
I. Neural circuitry of depressionII. The role of monoaminesIII. Neurotrophins and neurogenesisIV. Neuroendocrine and neuroimmune interactionsV. Epigenetic mechanismsVI. Resilence-related researchVII. New insights
III. The Subgenual Anterior Cingulate Cortex in Mood Disorders
IV. ConclusionsV. Journal club

1. Neural circuitry of depression
Mayberg’s model limbic-cortical dysregulation (1997)
Some mechanisms involving limbic structures (Krishnan and Nestler, 2008)
Specific role of the subgenual Anterior Cingulate Cortex (later, Drevets et al., 2008))

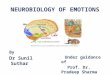
Mayberg’s model of depression: limbic-cortical dysregulation(Mayberg, 1997)
o Sadness + depressive illness:o dorsal limbic & neocortical regions (red)o ventral paralimbic areas (blue)
o Remissiono Reversal of these findingso Inhibtion / activation (black arrows), effect facilitated by fluoxetine
action in dorsal raphe and projection side (dotted lines)o Integrity of the rostral cingulate (yellow) -> required for adaptive
changes -> pretreatment metabolism predicts antidepressant treatment respons
Dorsal (red)Ventral (blue)Rostral (yellow)

Depression and dysfunctional changes in “limbic” regions
Implication of several brain regions and circuits regulating emotion, reward and executive functions:
Structural findings in post mortem studies & neuroimaging: grey matter & glial density in PFC & hippocampus
-> cognitive impairments in depression BUT: findings are not consistent, common problem: co-morbid
diagnosis, medication history -> limited evidence for cause-effect relation
Functional: activity in amygdala and subgenual cingulate cortex correlated with dysphoric emotions
!! Caution with simplistic “localization of function” approach to examine limbic structures

(1)
(2)(3)
(4)
(5)
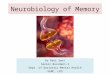
Neural circuitry of depression: some mechanisms involving limbic structures

(1) Deep brain stimulation of
white matter tracks surrounding subgenual cingulate cortex Nucleus accumbens (NAc) (implicated in reward processing & hedonic deficits in depression)
depressive symptoms
More recent findings?
(medial forebrain bundle?)

(2) Increased activity-dependent release of brain-derived neurotrophic factor (BDNF) within the mesolimbic dopamine circuit mediates susceptibility to social stress
-> probably partly through activation of the transcription factor CREB (cyclic-AMP-response-element-binding protein)
BDNF = protein (« neurotrophine » family) acts on neurons in the CNS and PNS helping to support the survival of existing neurons, and encourage the growth and differentiation of new neurons and synapses
CREB = cellular transcription factor, binding to certain DNA sequences called cAMP response (CRE), thereby increasing or decreasing the transcription of the downstream genes, Genes whose transcription is regulated by CREB include: c-fos, tyrosine hydroxylase, and many neuropeptides

(3) Neuroimaging findings : strong implication of the amygdala as an important limbic node for processing emotionally salient stimuli, e.g. fearful faces
(4) Stress reduces concentrations of neurotrophins (such as BDNF), extent of neurogenesis and the complexity of neural processes in the hippocampus -> mediated by increased cortisol concentrations and decreased CREB activity

(5) Peripherally released metabolic hormones, such as gherlin and leptin, produce mood related changes - in addition to cortisol - through their effects on the hippocampus (HYP) and several limbic regions

« monoamine hypothesis »
Decreased monoamine function in the brain Monoamine neurotransmitters and neuromodulators include
serotonine, dopamine, norepinephrine and epinephrine Antidepressant effects of iproniazid (irreversible and nonselective
monoamine oxidase inhibitor (MAOI), discovered in the 1950, originally used as medication against tubercolosis) & imipramine (first tricyclic antidepressant, originally meant to be used as a neuroleptic to treat schizophrenia)
Modern antidepressants = designed to increase monoamine transmission acutely by: Inhibiting neuronal reuptake (SSRIs (selective serotonine
reuptake inhibitors)) Inhibiting degradation (monoamine oxidase inhibitors (MAOI) ->
tranylcypromine (Jatrosom))
2. The role of monoamines

Acute increases in the amount of synaptic monoamines induced by antidepressants may produce secondary neuroplastic changes that are on a longer timescale and involve transciptional and translational changes mediating molecular and cellular plasticity
Monoamine-based antidepressants remain the first line of therapy for depression But: long therapeutic delay and low remission rates
-> search for more effective agents!
E.g. research on the role of P-glycoprotein Several antidepressants serve as substrates (e.g. citalopram) for P-
glycoprotein Human polymorphisms in the gene encoding P-glycoprotein
significantly alter antidepressant efficacy-> value of a pharmacogenetic approach when selecting an
antidepressant

Neurotrophic factors: neurodevelopmentally expressed growth factors that also regulate plasticity within adult brain
« BDNF hypothesis » Brain-derived Neurotrophic Factor = abundantly expressed in adult
limbic structures Preclinical studies show
Several forms of stress reduce BDNF-mediated signalling in the hippocampus
Chronic treatment with antidepressants increase BDNF-mediated signalling
Post mortem data from depressed humans
Decrease in the amount of BDNF in the hippocampusIncrease in the NAc
3. Neurotrophins and neurogenesis

BUT: recent findings suggest that BDNF hypothesis: too simplistic
Knock-in mice that express Met-66 BDNF (Val66Met is a gene variation, a single nucleotide polymorphism (SNP) in the BDNF gene that codes for BDNF) Equivalent response in forced swim test Increased anxiety like behaviour Increased resilience (behavioral and molecular changes) to social
defeat
BDNF-mediated signalling is involved in neuroplastic responses to stress and antidepressants
BUT: effects = region specific and antidepressant-specific and function in the background of potent genetic and environmental modifiers

(a) Hypothalamic-pituitary-adrenal (HPA) axis dysfunction
(b) “Cytokine hypothesis”
4. Neuroendocrine and neuroimmune interactions

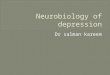
(a) Hypothalamic-pituitary-adrenal (HPA) axis dysfunction
CRH = Corticotropin-releasing hormoneACTH = adrenocorticotropic hormone

Dysfunctional Hypothalamic-pituitary-adrenal (HPA) axis
Chronic administration of glucocorticoides can lead to depression-like symptoms in rodents
Excess in glucocorticoides can reduce subgranular zone profileration (one of two major zones of adult neurogenesis) and produce atrophic changes in hippocampal subregions
this could lead to hippocampal volume reduction seen in depression
Hypercortisolaemia is manifest at many levels in depressed patients
Early adverse experiences play a preeminent role in the development of mood and anxiety disorders Association mediated by corticotropin-releasing factor (CRF)
system? Evidence from preclinical studies (rats, non human primates):
increased CRF may be the persisting neurobiological consequence of stress early in development

Findings in women after sexual and physical abuse in childhood (Heim et al., 2000) 4 groups (healthy, Early Life Stress (ELS) +no Major Depressive
Disorder (MDD), ELS + MDD, no ELS + MDD); psychosocial stress protocol; hormone + heart rate measures
! Note that subjects without early stress experiences showed normal stress reactivity, suggesting differential pathophysiology in subtypes of depression.

Severe stress early in life persistent sensitization of the pituitary-adrenal and autonomic stress response probably a risk factor for adulthood psychopathology
glucocorticoid and corticotropin-releasing factor receptor antagonists as treatment option?
BUT: Divergent findings dependend on depression subtypes
MDD without ELS? Hypercortisolaemia -> only in severe depressive episodes Atypical depression, esp. subtype with hyperphagia and
hypersomnia -> hypocortisolaemia

(b) « Cytokine hypothesis »
Cytokines (Greek cyto-, cell; and -kinos, movement) a diverse group of soluble proteins, peptides, or glycoproteins act as hormonal regulators or signaling molecules at nano- to-
picomolar concentrations and help in cell signaling humoral mediators of innate and adaptive immunity important modulators of mood
Some evidence from clinical and preclinical studies for a role in depression 30% of patients treated with recombinant interferons develop
depression as side effects In rodents: blocking pro-inflammatory cytokine-mediated
signalling can produce antidepressant effects BUT: mechanisms are not yet understood
further research is needed to elucitade the largely unknown neural circuitry involved in the behavioural effects of cytokines and underlying intercellular interactions

Epigenetics -> study of heritable changes in gene expression or cellular phenotype, caused by mechanismes other than changes in the underlying DNA sequence E.g. DNA methylation and histone modification -> alteration of gene
expression without altering the underlying DNA sequence Epigenetic changes -> mechanisms by which environmental
experiences can modify gene function in absence of DNA sequence changes -> might help to explain largely inconsistent genetic association
studies of depression
Epigenetic modifications in the pathophysiology of depression ? Covalent changes to DNA (e.g. DNA methylation) Post-translational modifications of histone N-terminal trials (e.g.
acetylation and methylation) Non transcriptional gene-silencing mechanisms (e.g. RNAs)
5. Epigenetic mechanisms


Depression research has focused on two main chromatin-modifying processes:
1. DNA methylation (of cytosine)
Seems to be important in the influence of maternal behaviour on adult emotional processing
maternal behaviour (licking & grooming) -> anxiety expression of glucocorticoide receptors
2. Histone acetylation Seems to be a key substrate for antidepressant action

The transcriptional potential of genes involved in neuroplastic responses to stress or antidepressant treatments can be regulated through chromatin-remodelling events catalysed by specific enzymes

Humans react very different to stress and adversity
Evidence from animal models: Distinct transcriptional profiles in the Ventral Tegmental
Area (VTA) and NAc in gene expression profiling of stress-vulnerable and stress-resilent mice
Suggesting that resilent behaviour represents a distinct, active neurobiological process (≠ only the absence of vulnerability)
Concerning the neurobiology of stress and the pathophysiology of depression: More research is needed on mechanisms on allostasis (efforts to maintain homeostasis) and antivulnerability processes
6. Resilence-related research

Actions of glutamate (major excitatory NT in the brain)? Limited evidence for dysfunction in specific glutamate
systems BUT: antidepressant effect of ketamine (a non-competitive
NMDA (N-methyl-D-asparte) glutamate receptor antagonist and psychotomimetic (mimics symptoms of psychosis)
Pathways involved in the control of feeding and metabolism and their interaction with substrates of mood Pro-depressant role of MCH (melanin-concentrating
hormone -> regulator of feeding and arousal) ? Antidperessant role of ghrelin and leptin (peptides ->
peripheral metabolic signals) ?
7. New Insights

I. Introduction 1. Brief repetition: symptomatology / diagnosis /
treatment guidelines2. We know little3. Validity criteria: animal models of depression
II. The molecular neurobiology of depression
1. Neural circuitry of depression2. The role of monoamines3. Neurotrophins and neurogenesis4. Neuroendocrine and neuroimmune interactions5. Epigenetic mechanisms6. Resilence-related research7. New insights
III. The subgenual anterior cingulate cortex in mood disorders
IV. ConclusionsV. Journal club

a) Specificity of structural neuroimaging abnormalities in the sgACC
b) Anatomical specificity of sgACC abnormalities
c) Neurphysiological imaging studies of sgACC activity
d) Neuropathological measures: correlations with rodent models of repeated stress
e) Relationship between structural abnormalities in the sgACC and other regions
f) Potential clinical correlates of subgenual prefrontal cortex dysfunction
I. The subgenual anterior cingulate cortex in mood disorders

Introduction & (a) Specificity of structural neuroimaging abnormalities in the sgACC
Ventral ACC -> increasingly has been implicated in the modulation of emotional behaviour (neuroimaging, lesion studies in animals)
MDD and familial BD: reduction of CBF and glucose metablolism in the PFC ventral to corpus callosum: voxel by voxel analysis: peak difference of activation in the sgACC (JC paper, Drevets et al., 1997) Activation differences accounted for by corresponding
reduction in cortex

reduction of grey matter volume in the left sgACC associated with a reduction of glia, but no equivalent loss of
neurons (Ongür, Drevets, et al., 1998) already early in the illness course of MDD and BD, persisting during antidepressent treatment present in manic and depressed phases of bipolar disorder present in psychotic unipolar and bipolar depression and
bipolar spectrum disorders BUT:
high variability findings not always replicated

-> Attempts to enhance sensitivity for identifying neuorbiological markers « familial pure depressive disease » (MDD subject with a first-
degree relative with MDD, but no first degree relative with mania, alcoholism, or sociopathy)
-> volumetric + metabolic differences in sgACC BD with first-degree relatives with BD
-> reduced sgACC volume
o Morphometric MRI studies divided anterior and posterior sgACC (Ongür et al., 2003)

Posterior sgACC reduced in MDD with psychotic features vs schizophrenic patients (Coryell et al., 2005)
GAS (Global Assessment Scale) scores correlated positively with cortical thickness at baseline and volume increase during follow up
-> volumetric abnormalities in posterior sgACC may predict and reflect the course of depression
-> need for further longitudinal studies
o Chronic lithium treatment (exerting robust neurothrophic effects in animal models) has been associated with increasing gray matter volume toward normal in treatment responders in the sgACC and other PFC areas (Caeteno et al., 2005)

(b) Anatomical specificity of sgACC abnormalities
pregenualACC (pgACC - ACC situated anterior to corpus callosum) Abnormalities in MDD concerning CBF/metabolism, tissue
volume, glia cells Part of the ventral “emotion” circuit implicated in affective
illness (Phillips, Drevets et al., 2003) sgACC shares similarities with the pgACC -> the distinctions of
the cortex at the actual sgACC/pgACC interface seem arbitrary Abnormal reductions of glia in MDD extend to the pgACC, as
well as to the orbitofrontal and dorsal anterolateral PFC and the amygdala

(c) Neurophysiological imaging studies of sgACC activity
HOWEVER: distinct functions of the anterior sgACC and more dorsal regions of the pgACC (neuroimaging studies of emotional behavior)
In mood disorders… sgACC activity positive correlation to the severity of depressive
symptomes pgACC activity has more consistently been linked to treatment
outcome Also…
Some evidence for reduction in resting sgACC CBF/metabolism Some findings that metabolic reduction in sgACC presate onset of
clinical symptoms BUT: also contradictory findings (with increased activity in
sgACC) -> due to the interrelationships between deficits in gray matter
volume and physiological imaging data? -> need for partial volume corrections? (sgACC volume
reduction sufficiently prominent to produce partial volume effects in functional brain images

Even… sgACC metabolism is elevated during depressed phase versus
remitted sgACC activity decreases during
Effective antidepressant treatment (Drevets et al., 1997; Drevets et al., 2002; Mayberg et al., 2000)
ECT (Nobler et al., 2001) Deep brain stimulation of sgACC (Mayberg et al., 2005)

(d) Neuropathological measures: correlations with rodent models of repeated stress
Repeated stress results in dendritic atrophy and reductions in glial cells in rodents in regions homologous to areas where grey matter reductions are evident in humans with MDD (e.g. medial PFC, hippocampus) (Bansar et al., 2007; Czeh et al., 2005; McEwan et al., 2001; …)
Dentric atrophy could be reversed by lithium administration in rats (McEwan et al., 2001)
Impaired sgACC function in mood disorders may conceivably contribute to cortisol hypersecretion in depression Major role of glucocorticoid receptors expressed in the
ventral ACC in the negative feedback effect of glucocorticoid secretion during stress (Diorio et al., 1993)

(e) Relationship between structural abnormalities in the sgACC and other regions
Substantial (predominantly ipsilateral) anatomical connections with the amygdala and subiculum Left-lateralized volumetric reductions in these areas might
be related Mixed evidence for volumetric changes (existence and
direction) in mood disorders sgACC projects to the ventromedial striatum and the
accumbens area reported to be abnormally small in a post mortum study of mood disorders
Data suggest that mood disorders are associated with a neuropathological process affecting circuits that involve the sgACC together with anatomically related parts of the orbitomedial PFC, amygdala, hippocampus, striatum, and thalamus

(e) Potential clinical correlates of subgenual prefrontal cortex dysfunction In monkeys and other experimental animals, the homologous
cortex to the sgACC shares extensive anatomical connections with i.e. the amygdala, subiculum, hypothalamus, ventral tegemtal area (VTA) and others -> regions implicated in the modulation of emotional
behaviour -> abnormal synaptic interactions between these areas and
the sgACC might contribute to disturbances in emotional processing or regulation
Evidence from rat studies left ventromedial PFC lesions disinhibit the function of the
right ventromedial PFC, which mediates the heightened sympathetic autonomic, affective, and hypothalamic-pituitary-adrenal axis arousal seen in left lesioned animals
-> in mood disorders, an altered balance between left and right sgACC function conceivably may contribute to the heightened affective, neuroendocrine, and sympathic autonomic arousal seen in depression (e.g. understimulation of parasympathic tone)

Lesions including sgACC (humans) -> abnormal autonomic responses to emotional experience, inability to experience emotion related to concepts that ordinarily evoke emotion, and inability to use information regarding the likelihood of punishment versus reward in guiding social behavior
Role of visceral feedback for evaluating consequences of social behavior? -> visceral feedback mediated through interactions between the ventromedial PFC, hypothalamic autonomic centers, and brain-stem monoaminergic neurotransmitter systems?
ACC may be involved in evaluating the salience of rewards -> role of the ventral ACC in modulating the electrophysiological responses of VTA (Ventral Tegmental Area) dopamine neurons (BA24 of the ACC receives dense dopamine innervation) Decreased sgACC activity (but!!) is associated with diminished
stimulation of mesolimbic dopamine relase, resulting in the absence of behaviour incentive, apathy, and anhedonia



sgACC in conclusion….There is evidence for an
extended anatomical network formed by the neural projections of the sgACC and other areas of the orbitomedial PFC with the amygdala, hippocampus, superior and medial temproal gyri, ventral striatum, mid- and posterior cingulate cortex, thalamus, hypothalamus, periaqueductal gray, and habenula -> implicated in the regulation of evaluative, expressive, and experiential aspects of emotion
Impaired function within this network could conceivably give rise to the clinical signs and symptoms of depression and mania

I. Introduction 1. Brief repetition: symptomatology / diagnosis /
treatment guidelines2. We know little3. Validity criteria: animal models of depression
II. The molecular neurobiology of depression
1. Neural circuitry of depression2. The role of monoamines3. Neurotrophins and neurogenesis4. Neuroendocrine and neuroimmune interactions5. Epigenetic mechanisms6. Resilence-related research7. New insights
III. The subgenual anterior cingulate cortex in mood disorders
IV. ConclusionsV. Journal club

Polysyndromic nature of depression, heterogenous and complex etiology, multilevel processes involved
Many open questions
A multidisciplinary approach is needed to explore the neurobiological bases for depression’s many subtypes
Transfer from preclinical to clinical research and practice ?
RDoC research strategy NIMH http://www.nimh.nih.gov/research-priorities/rdoc/nimh-
research-domain-criteria-rdoc.shtml
What do you think what are the current central research questions?
Which approaches are adequate?
IV. Conclusions…. Discussion!

I. Introduction 1. Brief repetition: symptomatology / diagnosis /
treatment guidelines2. We know little3. Validity criteria: animal models of depression
II. The molecular neurobiology of depression
1. Neural circuitry of depression2. The role of monoamines3. Neurotrophins and neurogenesis4. Neuroendocrine and neuroimmune interactions5. Epigenetic mechanisms6. Resilence-related research7. New insights
III. The subgenual anterior cingulate cortex in mood disorders
IV. ConclusionsV. Journal club

V. Journal club
Drevets WC, Price JL, Simpson JR Jr, et al.
Subgenual prefrontal cortex abnormalities in mood disorders.
Nature 1997;386:824–827.

3rd independant group
« family pure depressed disease »
BF = Blood FlowMrglu= Metabolic rate for glucose
+++ resolution
Methods

Synergistic use of MRI and PET image data

Results

Thank you for your attention!!