Embed Size (px)
Citation preview

NEUROANATOMICAL SUBSTRATES OF SOCIALCOGNITION DYSFUNCTION IN AUTISM
Kevin Pelphrey,1,4* Ralph Adolphs,2,3 and James P. Morris4
1Department of Psychiatry, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, North Carolina2Division of Humanities and Social Sciences, California Institute of Technology, Pasadena, California
3Department of Neurology, Division of Cognitive Neuroscience and Behavioral Neurology, The University of Iowa College of
Medicine, Iowa City, Iowa4Duke–UNC Brain Imaging and Analysis Center, Duke University, Durham, North Carolina
In this review article, we summarize recent progress toward under-standing the neural structures and circuitry underlying dysfunctional socialcognition in autism. We review selected studies from the growing literaturethat has used the functional neuroimaging techniques of cognitive neuro-science to map out the neuroanatomical substrates of social cognition inautism. We also draw upon functional neuroimaging studies with neuro-logically normal individuals and individuals with brain lesions to highlightthe insights these studies offer that may help elucidate the search for theneural basis of social cognition deficits in autism. We organize this reviewaround key brain structures that have been implicated in the social cogni-tion deficits in autism: (1) the amygdala, (2) the superior temporal sulcusregion, and (3) the fusiform gyrus. We review some of what is known aboutthe contribution of each structure to social cognition and then reviewautism studies that implicate that particular structure. We conclude with adiscussion of several potential future directions in the cognitive neuro-science of social deficits in autism. © 2004 Wiley-Liss, Inc.MRDD Research Reviews 2004;10:259–271.
Key Words: autism; social perception; social cognition; functional MRI;cognitive neuroscience
Autism is a severe and pervasive neurodevelopmental dis-order whose etiology remains poorly understood. It isdefined broadly by the presence and characteristic de-
velopmental course of deficits in three domains of functioning:(1) social reciprocity and engagement, (2) communication andlanguage skills, and (3) stereotyped, repetitive behaviors andnarrowed interests [DSM-IV; American Psychiatric Association(APA), 1994]. The prevalence of autism is estimated to beapproximately 1 to 2 per 1,000 individuals [Fombonne, 1999]and possibly considerably higher with the inclusion of otherdisorders falling on the “autism spectrum” [Folstein and Rosen-Scheidley, 2001] (Asperger’s syndrome and Pervasive Develop-mental Disorder Not Otherwise Specified). These disorders spana wide range of dysfunctions but share with autism early deficitsin the social and communicative domains. Autism features con-siderable symptom heterogeneity within each of the three coredomains. Variability in the social domain may range from anearly complete absence of interest in interacting with others, to
more subtle difficulties managing complex social interactionsthat demand attention or taking into account social context andother people’s intentions. Similarly, stereotyped and repetitivebehaviors may range from simple motor stereotypies and apreference for sameness to much more complex and elaboraterituals, accompanied by considerable distress when these ritualsare interrupted. Language deficits, while marked in some autisticindividuals who lack basic speech abilities, can be mild andlimited to the presence of pragmatic language deficits in higherfunctioning individuals with autism. In addition to the hetero-geneity in these three key behavioral domains, there is alsoconsiderable variability in general intellect. While the majorityof individuals with autism exhibit mental retardation, IQs canvary from the severe and profoundly mentally retarded range tomarkedly above average.
The heterogeneity in autism and autism spectrum disor-ders is expanded still further by the concept of the Broad AutismPhenotype, which suggests that the genetic liability for autismmight be expressed in individuals who do not meet diagnosticcriteria for autism, but who exhibit phenotypic characteristics ofpsychological functioning that are milder but qualitatively sim-ilar to those seen in autism [Folstein and Rutter, 1977; seePiven, 2001 for a review]. For example, there is evidence forexecutive dysfunction in parents [Hughes et al., 1997] andsiblings [Hughes et al., 1999] of children with autism and socialimpairments and distinct personality characteristics (e.g., aloof-ness and rigidity) in parents of affected children [Wolff et al.,1988; Piven et al., 1994; Murphy et al., 2000]. Parents ofaffected children also exhibit subtle language and communica-tive differences [Landa et al., 1992; Piven et al., 1997] and
Grant sponsor: North Carolina Studies to Advance Autism Research and TreatmentCenter, NIH; Grant number: 1 U54 MH66418. Grant sponsor: NIMH; Grant num-ber: 1 K01 MH071284–0 (to KP).*Correspondence to: Kevin Pelphrey, Duke–UNC Brain Imaging and Analysis Cen-ter, Box 3918, Duke University Medical Center, Durham, NC 27710. E-mail:[email protected] 17 November 2004; Accepted 22 November 2004Published online in Wiley InterScience (www.interscience.wiley.com).DOI: 10.1002/mrdd.20040
MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIESRESEARCH REVIEWS 10: 259–271 (2004)
© 2004 Wiley-Liss, Inc.

experience higher rates of depression andsocial phobia [Piven and Palmer, 1999].
Based on the high concordancerate for monozygotic twins and a recur-rence risk that is greater than the popu-lation rate, there is now considerable ev-idence that autism is a disorder with asignificant genetic component to its eti-ology [Cook et al., 1998; see Bailey et al.,1995 for a review] with heritability esti-mates of 60–70% [Veenstra-VanDer-Weele et al., 2003]. The much higherincidence rate in male compared to fe-male children further suggests a geneticcomponent to the etiology of autism.This could be quite indirect (i.e.,through interactional effects of gonadalsteroids on brain development), but itcould also be more direct, vis-a-vis ex-pression of proteins on the sex chromo-somes in neurons. For instance, Skuseand colleagues [2003] have argued thatimpaired social cognition in Turner’ssyndrome can be traced to genes on theX chromosome (Xp 11.3) and that theeffects of these genes on social cognitionare mediated through the amygdala,which is enlarged in Turner’s syndrome.However, research also indicates a rolefor environmental factors, for example,this is suggested already by monozygotictwins who are discordant for autism.Thus, like most behaviorally defined syn-dromes, autism is very likely to be etio-logically heterogeneous [Rutter et al.,1994]. Roughly 10% of individuals withautism have an associated medical condi-tion thought to play a role in susceptibil-ity to the disease. For example, individ-uals with single gene disorders such astuberous sclerosis, fragile X syndrome;and Smith-Lemli-Opitz syndrome havehigh rates of autism [Baker et al., 1998;Bailey et al., 2001; Martin et al., 2001].In individuals without an obvious associ-ated medical condition (i.e., idiopathicautism), the underlying mechanism ismore likely to be the result of multipleinteracting genes or oligogenic inheri-tance [Pickles et al., 1995; Risch et al.,1999]. Disentangling the precise contri-butions made by genes and by environ-ment in the etiology of autism remains acritical and largely unmet challenge. De-spite this etiological heterogeneity, anddespite complexity in the phenotype, it ispossible that the various factors contrib-uting to the impaired behavior and cog-nition seen in autism exert their effectthrough a circumscribed set of neuralstructures. That is, it might be the casethat the simplest and most compact cor-relate of autism would be found at theneurological or neuropsychological level,
rather than at the genetic or the behav-ioral level.
Advances in techniques for study-ing brain–behavior relationships have ledto an unprecedented and concerted effortin elucidating the neural basis of autismby linking specific social deficits to dys-function in specific brain structures (i.e.,the cognitive neuroscience of social in-formation processing in autism). Theseinclude neuropsychological studies of pa-tients with focal lesions, volumetricquantification of brain structures, ana-tomical pathway tracing, and imaging ofregional brain activation.
fMRI is a noninvasive in vivo im-aging method that takes advantage of anendogenous contrast property of thebrain, blood oxygen level–dependentcontrast (BOLD), to localize changes inblood oxygenation–an indirect measureof underlying neural activity. Since fMRIis noninvasive, does not involve ionizingradiation, can be performed repeatedly,and can be employed to scan relativelylarge samples of individuals, it is an espe-cially appropriate tool to study autism,where large samples are often required totake into account heterogeneity andwhere longitudinal studies of children arenecessary to characterize functional braindevelopment and behavioral change overtime.
Neuropsychological “marker tasks”can provide insights into brain functionand can implicate specific brain regionsthrough comparisons with patients whohave circumscribed brain lesions and/orother neuroimaging techniques [John-son, 1997]. Together with functionalneuroimaging, lesion studies and detailedneuropsychological testing have gener-ated a wealth of knowledge concerningthe neural structures that are the mostlikely candidates for subserving thosecognitive processes that are dysfunctionalin autism. These are exciting times forbasic research because outcomes of theseefforts will prove clinically important inhelping to identify specific neurophysio-logical mechanisms involved in core def-icits in autism, thus leading to an im-proved theoretical understanding fordeveloping and evaluating the effective-ness of novel therapeutic interventions.Emerging neuropsychological models ofautism based on the above techniques arealready beginning to shed light on can-didate mechanisms that may be mediat-ing individual differences in both the ex-pression of autistic symptoms and in theirresponsiveness to treatment. Character-ization of the functional brain pheno-types in autism, as observed throughfMRI, may also lead to a clarification of
the genetic basis of autism. Longitudinalstudies of developmental trajectories andindividual differences will give us a moreaccurate and dynamic picture of autismthan would studies that focus only onadults. Neuroimaging studies focused onchanging brain–behavior relationships inthe developing child may also provideclues to candidate genes in autism, asdevelopmentally important genes beginto be linked to particular patterns offunctional brain development, gene ex-pression, and brain phenotypes.
In this review, we summarize re-cent progress toward understanding theneural structures and circuitry underlyingdysfunctional social cognition in autism.We review selected studies from thegrowing literature that have used func-tional neuroimaging techniques to mapout neurofunctional abnormalities inbrain regions underlying aspects of socialcognition domains in autism. We alsodraw upon functional neuroimagingstudies with neurologically normal indi-viduals and individuals with brain lesionsto highlight how these studies–by pro-viding basic knowledge concerning theneural basis of social cognition–can offerinsights that may help to elucidate thesearch for the neural basis of social cog-nition deficits in autism. We organizethis review around key brain structuresthat have been implicated in the socialcognition deficits in autism: (1) theamygdala, extrastriate visual cortices in-cluding the (2) superior temporal sulcusregion and the (3) fusiform gyrus. Wereview some of what is known about thecontribution of each structure to socialcognition and then review autism studiesthat implicate that particular structure.
In sketching what is known aboutthe role played by specific neural struc-tures in social cognitive processing, wedo not want to imply that such process-ing is localized to a single brain region,nor would we want to suggest that dys-function in a given cognitive process re-sults from dysfunction in a single struc-ture. We have little doubt that each ofthe three structures we will review playsa role in some way in the autism pheno-type, but it remains very unclear howexactly they participate as components ofthe entire neural network and how ex-actly their dysfunction contributes to pa-thology. To give just one example; theamygdala has been implicated in process-ing emotional information from faces,something in which at least some peoplewith autism are impaired. Does their im-pairment therefore arise from pathologyin the amygdala? That conclusion is un-warranted: their impairment may arise
260 MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

from entirely different structures con-nected to the amygdala, and it is in factconceivable that abnormal amygdalafunction is a consequence of having au-tism, rather than a cause of it. The struc-ture–function relationships revealed bycognitive neuroscience often give us onlycorrelative evidence. This is not to saythat researchers are not up to the task, itis only to say that understanding autismwill be a difficult and complex challengeand that approaches from many differentdisciplines must be integrated if we are toavoid serious pitfalls.
NEURAL STRUCTURESIMPLICATED IN SOCIALCOGNITION DEFICITS INAUTISM
Amygdala“Social cognition” refers to our
abilities to recognize, manipulate, andbehave with respect to socially relevantinformation, including the ability to con-struct representations of relations be-tween the self and others and to use thoserepresentations flexibly to guide socialbehavior [Adolphs, 2001]. Different sub-disciplines emphasize different aspects ofthis construct. For example, in social psy-chology, social cognition describes arange of phenomena including reason-ing, stereotyping, and related topics[Kunda, 1999]. In neurobiology, Broth-ers [1990], defines social cognition morenarrowly “as the human ability to per-ceive the intentions and dispositions ofothers.” Definitions of social cognitioncommonly link this construct to socialbehavior and include social perception(the initial stages of evaluating intentionsof others by analysis of gaze direction,body movement, and other types of bi-ological motion), theory-of-mind (theability to make inferences about themental states of others), and attributionalstyle (the way one tends to explain otherpeople’s behavior).
Brothers [1990] proposed that theamygdala is part of a small group of brainstructures (along with the superior tem-poral sulcus and gyrus and orbitofrontalcortices) that form the neurobiologicalbasis of social cognition (see Fig. 1 forneuroanatomical structures highlightedin this review). The amygdala is a com-plex structure comprised of at least 13nuclei located in the anterior medial tem-poral lobe with extensive connections tomany brain regions including the neo-cortex, hippocampus, brainstem, thala-mus, basal forebrain, and claustrum[Amaral et al., 1982; Amaral and Insausti,1992]. Animal models have provided
some of the clearest data concerning theamygdala’s function in several aspects ofbehavior. Studies of rats have demon-strated the involvement of the amygdalain fear conditioning [LeDoux, 1996], theacquisition of fear-related responses to astimulus via its association with a stronglyaversive stimulus. Neurons in the mon-key amygdala respond both to the basicmotivational significance of stimuli[Nishijo et al., 1988] as well as to theircomplex social significance [Brothers,1990; Rolls, 1992]. In humans, amygdalaneurons have been found to respond toemotionally salient stimuli of variouskinds [Oya et al., 2002] including faces[Fried et al., 1997].
Early studies in nonhuman pri-mates indicated that macaques with bilat-eral lesions to the amygdala and sur-rounding medial temporal structures aremore tame than nonlesioned monkeysand demonstrate abnormal food prefer-ences and sexual behaviors [Brown andSchafer, 1887; Kluver and Bucy, 1938,1939]. In an effort to develop an animalmodel of autism, Bachevalier and col-leagues conducted a series of studies withneonatal macaques subjected to bilateralmedial temporal lobe lesions that in-cluded the amygdala [Bachevalier, 1994,1996; Bachevalier and Mishkin, 1994].These monkeys exhibited reduced eyecontact, avoided social encounters, dis-played inexpressive faces, and lackedmany normal play behaviors. They alsoshowed locomotor stereotypies and in-creases in self-directed activities. Thesebehavioral deficits were strikingly remi-niscent of many behaviors observed inautism.
Studies by Amaral and colleaguesexamined adult male rhesus monkeyswith precise bilateral ibotenic acid lesionsof the amygdala, a method that providesa relatively selective way to lesion cellbodies but not axons that may be passingthrough the amygdala. The lesioned an-imals were paired with unlesioned con-trol monkeys during dyadic social inter-actions [Emery et al., 2001; Prather et al.,2001]. Contrary to initial expectations,the adult amygdala-lesioned monkeysinitiated more social approaches and affili-ative behaviors than did the controlmonkeys. The lesioned monkeys also didnot exhibit normal fear behavior in re-sponse to novel and fear-provoking stim-uli (e.g., snakes) and were socially disin-hibited such that they did not exhibit theusual period of reluctance when meetinga novel conspecific. These findings led tothe proposal that a primary function ofthe amygdala is evaluating the environ-ment for potential threats or dangers
[Emery et al., 2001] (see also [Amaral etal., 2003] for more recent findings fromlesioned monkeys and continued theo-retical elaboration). Subsequent studiesdemonstrated that infant macaques, le-sioned at 2 weeks of age, showed anabsence of fear of normally fear-inducingstimuli [Prather et al., 2001]. However,the developmentally lesioned macaquesalso showed more screams and fear gri-maces during interactions with other ma-caques. In human [Fried et al., 1997] andnonhuman primates [Leonard et al.,1985; Nakamura et al., 1992; Rolls,1992], neurons in the amygdala responddifferentially to faces, consonant with thebroader responses of amygdala neuronsthat have been recorded in monkeys inresponse both to the basic motivationalsignificance of stimuli [Nishijo et al.,1988] as well as to their complex socialsignificance [Brothers et al., 1990].Overall, the available animal studiesdemonstrate that the amygdala modulatesmany responses and cognitive processesbased on the emotional significance ofstimuli. A common theme is the abilityto associate stimuli with their emotional/social value.
Behavioral and structural studies inhumans have also clearly pointed to theamygdala’s role in social cognition andsocial behavior. One specific hypothesisof social dysfunction in autism proposesthat this is due to pathology in the amyg-dala (Baron-Cohen), and abnormalamygdala structure has been linked bothto autism (Bauman and Kemper) [Schu-mann et al., 2004; Sparks et al., 2002] aswell as to genetically predisposed abnor-mal social behavior in diseases such as
Fig. 1. Brain structures thought to be im-portant for the cognitive neuroscience of so-cial cognition deficits in autism. The superiortemporal sulcus has been implicated in eyegaze processing, voice perception, and attri-bution of intentionality deficits in autism.The amygdala has been linked to emotionrecognition and theory-of-mind deficits inautism. Hypoactivation of the fusiform gyrushas been proposed as a mechanism underly-ing face processing deficits in autism.
261MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

Turner’s syndrome [Skuse et al., 2003].However, the clearest evidence for theamygdala’s role in social cognition in hu-mans comes from lesion and functionalimaging studies. For instance, clear socialinformation processing deficits, includingimpairments in emotion recognition andsocial judgments, are found in patientswith lesions to the amygdala. Such pa-tients show a relatively disproportionateimpairment in recognizing the intensitywith which facial expressions signal fear[Adolphs et al., 1994] (see Fig. 2c) as well
as a lesser impairment also in recognizingthe intensity of other negatively valencedemotions including surprise and anger[Adolphs et al., 1999]. Subsequent studiesin several additional patients with amyg-dala lesion confirmed an impaired abilityto recognize emotion from faces, despitea normal ability to discriminate faces per-ceptually. Some of these studies found adisproportionately severe impairment inrecognizing fear [Adolphs et al., 1995;Broks et al., 1998; Sprengelmeyer et al.,1999; Anderson and Phelps, 2000],
whereas others found evidence for abroader impairment in recognizing mul-tiple emotions of negative valance in theface, including fear, anger, disgust, andsadness [Adolphs, 1999; Schmolck andSquire, 2001].
Bilateral damage to the humanamygdala has also been found to impairsocial judgments of trustworthiness andapproachability of people based on theirfaces [Adolphs et al., 1998]. Such lesionsubjects judge people to look more trust-worthy and more approachable than do
Fig. 2. Individuals with autism and those with damage to the amygdala make similar abnormal judgments of trustworthiness and approachability fromfaces and make similar errors in emotional expression recognition from faces. Ratings of (a) trustworthiness and (b) approachability from 100 unfamiliarfaces. Shown are mean ratings of the 50 faces that normally receive the most negative ratings (left half of each split graph) and the 50 faces that normallyreceive the most positive ratings (right half of each split graph). Solid black bars are the means (�SD) data from 47 normal controls; three white bars aredata from three individual subjects with bilateral amygdala damage; gray bars are individual data from autistic subjects. All data except for the data fromautistic subjects are from Adolphs et al. [1998]. Norm � normal; Amy � amygdala. Reproduced with permission from Adolphs et al., (2001; Journal ofCognitive Neuroscience). (c) Shows that bilateral damage to the amygdala can result in selective impairment in the recognition of fear. Shown is theperformance of subject SM in rating morphs of emotional facial expressions. The y-axis shows the correlation of SM’s ratings with mean normal ratings,and the x-axis shows the stimuli, which are morphs from happy to surprise and from surprise to fear. Adapted from Adolphs [2003, Annals of the NewYork Academy of Sciences]. Data from Adolphs and Tranel [2000]. (d) Percentage of correct scores for judgments of basic emotional expressions fromfaces in subjects with and without autism. Subjects with autism were significantly worse at identifying anger and fear. Data from Pelphrey et al. [2002,Journal of Autism and Developmental Disorders].
262 MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

healthy controls (see Fig. 1a and b). Thisfinding demonstrates that the role of theamygdala in processing stimuli related topotential threat or danger extends to thecomplex judgments on the basis of whichwe approach or trust other people. Oneproposal [Adolphs et al., 1999, 2000] isthat the impairments across diverse tasksreflect the amygdala’s role in recognizingsignals that indicate potential threat ordanger. But the social impairments dueto amygdala damage may be broader yet:one patient described a film of animatedshapes (normally seen as full of socialcontent) in entirely asocial geometricterms, despite otherwise normal visualperception and intact social knowledge[Heberlein and Adolphs, 2004].
Functional neuroimaging studieshave both corroborated and extendedthese findings and greatly added to ourunderstanding of the amygdala’s functionin neurologically normal humans, partic-ularly with regard to emotion recogni-tion [reviewed in Adolphs, 1999]. Twoearly studies, one using PET [Morris etal., 1996] and the other fMRI [Breiter etal., 1996], found that the amygdala isactivated by facial expressions of emotion(especially fear), even though neitherstudy asked subjects to judge the emotionshown in the stimulus. Other imagingstudies have shown that the amygdala isactivated by facial expression stimuli,even when these stimuli are not con-sciously perceived. For example, Whalenet al. [1998] found amygdala activation tofearful faces that were presented brieflyand backward masked to render theirperception subliminal. These studies sug-gest that the amygdala is engaged in rel-atively rapid and automatic processing offacial expressions. In fact, requiring sub-jects to cognitively label facial expressionstimuli, rather than to watch them pas-sively, may result in deactivation of theamygdala [Hariri et al., 2000].
Other human neuroimaging stud-ies illustrate the involvement of theamygdala in normal social cognition be-yond its role in emotion recognition. Forexample, in a PET study of adult males,Kawashima et al. [1999] observed that
the left amygdala was activated whilesubjects interpret gaze direction whereasthe right amygdala was activated duringeye to eye contact. A recent imagingstudy of subjects’ ratings of trustworthi-ness elegantly corresponds to the lesiondata presented earlier [Winston et al.,2002]. When normal subjects view facesof people that look untrustworthy, acti-vation is found in the superior temporalsulcus, the amygdala, the orbitofrontalcortex, and the insular cortex.
At least three functional neuroim-aging studies of individuals with andwithout autism have explored the role ofthe amygdala in autism (see Table 1 forcapsule summaries). In the first, Baron-Cohen et al. [1999] required participantsto infer the mental or emotional state ofanother person from the expression ofthe eyes alone. In behavioral studies con-ducted outside of the scanner environ-ment, high-functioning subjects with au-tism reliably show deficits on this task[Baron-Cohen et al., 1997]. The superiortemporal gyri, the left amygdala, and theinsula were activated in neurologicallynormal subjects performing this “EyesTask.” Subjects with autism activatedfrontal components less extensively thandid neurologically normal subjects andshowed decreased activation in theamygdala. A second fMRI study exam-ined both explicit (conscious) and im-plicit (nonconscious) processing of facialexpressions [Critchley et al., 2000].While viewing faces, subjects attended toeither the emotional expression (explicittask) or the gender (implicit task) of theface. In contrast to controls, during theexplicit task, autistic subjects did not ac-tivate the fusiform gyrus and during theimplicit task they did not activate the leftamygdala region. Finally, in an fMRIstudy of children and adolescents withautism, Wang et al., [2004] reported thatautistic subjects failed to show normalmodulation of amygdala activation underdifferent task demands (matching versuslabeling faces). During facial expressionmatching, subjects with autism showedsignificantly less activity than the controlgroup in the fusiform gyrus, but greater
activity in the precuneus. During labelingof emotions, no group differences wereobserved. Activity in the amygdala wasmodulated by task demands in the con-trol group but not in autistic subjects.
Some of the most tantalizing (albeitindirect) evidence supporting a role for theamygdala in autism comes from compari-sons of subjects with autism to subjectswith focal lesions to the amygdala on thesame neuropsychological marker tasks. Forexample, Adolphs et al. [2001] adminis-tered a battery of neuropsychological taskspreviously used in subjects with focalamygdala lesions to a sample of high-func-tioning autistic subjects. As illustrated inFigs. 2a and b, the high-functioning adultswith autism made isolated abnormal socialjudgments regarding the assessment oftrustworthiness and approachability in facesthat parallel similar findings from individu-als with bilateral amygdala lesions. Bothgroups exhibited a significant bias towardoverattributing the qualities of trustworthi-ness and approachability to pictures of facesrated by neurologically normal individualsto be somewhat untrustworthy and unap-proachable. Similarly, individuals with au-tism also have difficulty identifying emo-tional features in posed facial expressions[Adolphs et al., 2001; Pelphrey et al.,2002]. The facial expression recognitiondeficits are similar to those seen in patientswith amygdala lesions; both populations areimpaired at judging faces displaying nega-tive affect, especially fear and anger [Ado-lphs et al., 2001] (see Figs. 2c and d). Klin[2000] has found abnormalities in the abil-ity of individuals with autism to attributesocial meaning to ambiguous, moving geo-metric shapes, as is typically done by non-autistic individuals [Heider and Simmel,1944]. The narrations provided by the sub-jects with autism in the Klin study are re-markably similar to those given by patientSM who described a Heider and Simmelfilm of animated shapes in exclusively aso-cial and geometric terms [Heberlein andAdolphs, 2004].
Superior Temporal Sulcus RegionThe functional organization of the
superior temporal sulcus has been studied
Table 1. Functional Neuroimaging Studies Implicating the Amygdala in Autism
Study Stimuli Key Findinga
Baron-Cohen et al. [1999] Inferring mental states from the eyes region Decreased activity in the amygdalaCritchley et al. [2000] Implicit and explicit processing of emotional facial expressions Failed to activate amygdala in the implicit task and
the fusiform gyrus in the explicit taskWang et al. [2004] Face labeling versus matching by emotional expression Amygdala activity not modulated by task demands
aSummary of key finding is made with reference to the primary reported difference between subjects with autism and those without autism.
263MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

extensively in both human and nonhu-man primates. As has been found in stud-ies of the amygdala, some of the clearestfindings regarding the function of thesuperior temporal sulcus have come fromstudies in nonhuman primates. For ex-ample, monkeys use gaze as a componentof facial expressions, particularly as it re-lates to signals of dominance and submis-sion. Monkeys can accurately discrimi-nate small shifts in gaze direction, butthey suffer significant deficits in this taskfollowing surgical removal of cortexwithin the superior temporal sulcus[Campbell et al., 1990]. Two prosopag-nosic patients tested with the same taskused with the surgically ablated monkeysalso showed deficits [Campbell et al.,1990]. Employing single neuron record-ings, Perrett and colleagues [1985, 1989]identified cells in the macaque anteriorsuperior temporal sulcus that selectivelyrespond to cues from head and gaze di-rection. Overall, single-cell recordingstudies in monkeys indicate that cells inthe superior temporal sulcus respond togaze (eye and head) direction [Perrett etal., 1990, 1992], head movement [Has-selmo et al., 1989], mouth movements[Mistlin and Perrett, 1990], hand move-ments [Perrett et al., 1989], and wholebody motions [Oram and Perrett, 1996].Some of these neurons appear to play arole in social attention by signaling thedirection of another person’s visual atten-tion and by processing aspects of the con-text within which actions are observed[Perrett et al., 1990, 1992]. In addition tothe large body of findings concerningaction perception, a polysensory regionhas been described in the monkey supe-rior temporal sulcus (“the superior tem-poral polysensory region”) that integratesaudio and visual components of complexsocially significant stimuli [Cusick,1997].
In humans, the superior temporalsulcus region is defined by Allison et al.[2000] to include cortex within superiortemporal sulcus, to adjacent cortex onthe surface of the superior and middletemporal gyri (near the straight segmentof the superior temporal sulcus), and toadjacent cortex on the surface of the an-gular gyrus (near the ascending limb ofthe superior temporal sulcus). This re-gion (particularly posterior portions inthe right hemisphere) is involved in per-ceiving biological motion [for reviewssee Allison et al., 2000; Decety andGrezes, 1999] including eye movements[Puce et al., 1998; Wicker et al., 1998;Pelphrey et al., 2003a, 2004a]. The STSregion is functionally and anatomicallydistinct from the more posterior and in-
ferior region MT or V5 (MT/V5) that islocalized to the occipitotemporal border[Zeki et al., 1991; McCarthy et al., 1995;Pelphrey et al., 2003b]. Also, portions ofthe superior temporal sulcus region inhumans (as in the monkey) are polysen-sory, responding to audio and visualcomponents of stimuli [Belin andZatorre, 2000; Calvert et al., 2000; Cal-vert, 2001; Wright et al., 2003].
In addition to its role in processingbiological motion, there is evidence tosuggest that, similar to the anterior supe-rior temporal sulcus in the macaque, theposterior superior temporal sulcus in hu-mans is involved in the analysis and in-terpretation of the intentions of other’sgoal-directed movements and actionsseen in other people and is sensitive toother aspects of the context within whichobserved actions are embedded [e.g.,Blakemore et al., 2003; Pelphrey et al.,2003a, 2004; in press]. For example, in arecent series of studies, Pelphrey and col-leagues have investigated the degree towhich eye-gaze–evoked activity in thesuperior temporal sulcus is modulated bythe context of the perceived eye move-ment, that is, when the gaze shift cor-rectly or incorrectly acquires a visual tar-get, or whether the eye gaze conveys theintention to engage in or withdraw froma social interaction. In one study, a strongeffect of context was observed in theright posterior superior temporal sulcusin which observation of gaze shifts awayfrom the target evoked a hemodynamicresponse with extended duration andgreater amplitude compared to gaze shiftstoward the target [Pelphrey et al., 2003a].That study demonstrated that the per-ceived context or intention of a gaze shiftinfluences activity in the human superiortemporal sulcus. Another study demon-strated that the superior temporal sulcusparticipates in the visual analysis of socialinformation conveyed by gaze shifts in amore overtly social encounter (e.g., astranger walking toward the subject andpassing him or her in a virtual hallway).Subjects viewed an animated figure thatwalked toward them and shifted his neu-tral gaze either toward (mutual gaze) oraway (averted gaze) from them. Mutualgaze evoked greater activity in the supe-rior temporal sulcus compared to avertedgaze [Pelphrey et al., 2004a]. These find-ings suggest that activity in the superiortemporal sulcus evoked during observa-tion of others’ eye movements is exquis-itely sensitive to the context withinwhich those actions are embedded (i.e.,approach versus withdraw or goal-di-rected versus non-goal–directed). Theseand other findings have strengthened the
conclusion that the human superior tem-poral sulcus region is involved in socialperception and social cognition in hu-mans via the visual analysis of social in-formation conveyed by gaze directionand other types of biological motion [Al-lison et al., 2000]. This idea is in line withsystems-level frameworks for under-standing the processing of visual informa-tion, which have proposed that regionsof extrastriate cortex including the supe-rior temporal sulcus and superior tempo-ral gyrus are involved in processingchangeable and moveable aspects of faces,whereas regions including the fusiformgyrus process static and structural aspectsof the face.
Given the findings concerning thesuperior temporal sulcus region and as-pects of social cognition and social per-ception, it is not surprising that recentfunctional neuroimaging research has fo-cused on this region in autism (see Table2). The role of the superior temporalsulcus region in eye gaze processing is ofparticular interest. Among the most strik-ing social impairments in autism are def-icits in joint attention (i.e., coordinatingvisual attention with others) and in usinginformation concerning eye gaze to un-derstand others’ mental states and inten-tions [Loveland and Landry; 1986;Mundy et al., 1986; Baron-Cohen, 1995;Dawson et al., 1998; Baron-Cohen et al.,1999; Frith and Frith, 1999; Leekam etal., 1998, 2000]. Behavioral studies haveshown that gaze processing deficits inautism are not based in eye gaze discrim-ination per se, but result from impair-ment in using eye gaze to understandothers’ intentions and mental states [seeBaron-Cohen, 1995 for a review]. In es-sence, individuals with autism perceivechanges in eye gaze direction, but theyfail to attribute the intentions and mentalstates conveyed by eye gaze shifts. Link-ing these behavioral observations withthe demonstrated role of the superiortemporal sulcus in social perception sug-gests the hypothesis that, in autism, ac-tivity in the superior temporal sulcus re-gion is not sensitive to the context withinwhich eye movements are observed. Thislack of sensitivity to context could me-diate deficits in processing social signalsconveyed by eye gaze (and probablyother nonverbal social signals) becausethe superior temporal sulcus region inautism does not properly serve the func-tion of processing the intentionality orsocial communicative value of eye gazeshifts. To date, no published study has yetcompared activity associated with obser-vation of eye movements that conveydifferent intentions in autism. However,
264 MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

an elegant PET study conducted by Cas-telli et al. [2002] offers indirect supportfor this hypothesis. Participants with andwithout autism viewed film segments ofgeometric figures (similar to the films byHeider and Simmel described earlier)moving about in ways that normallyevoke varying attributions of intention-ality. Behaviorally, the subjects with au-tism gave fewer and less accurate descrip-tions of animations that typically evokedattributions of mental states and inten-tions. These behavioral findings are inline with Klin’s previous findings usingsimilar stimuli [Klin, 2000]. Relative tocontrols, subjects with autism demon-strated hypoactivation of the right poste-rior superior temporal sulcus region inindividuals with autism. There was alsoreduced functional connectivity (i.e.,correlation between the time coursesfrom two regions of activation) betweenthe posterior superior temporal sulcus re-gion and a portion of extrastriate visualcortex localized to the inferior occipitalgyrus in the autistic subjects.
This PET study also raised the im-portant question of whether the neuro-biological basis of the lack of differentialsuperior temporal sulcus activity residesin the cortex of the superior temporalsulcus region itself or whether the dys-function is the result of failures in com-munication between the superior tempo-ral sulcus region and other brainstructures involved in social processing.Consistent with the possibility of a pri-mary pathology in the superior temporalsulcus region, a PET study of speechperception reported abnormal lateralityof responses and hypoactivation of theleft superior temporal gyrus [Boddaert etal., 2003] and an fMRI study observedhypoactivation in the superior temporalregion to human voices [Gervais et al.,2004]. Also, bilateral hypoperfusion oftemporal lobe areas has been observed inchildren with autism at rest [Ohnishi etal., 2000; Zilbovicius et al., 2000]. Fi-nally, a recent anatomical study compar-
ing cortical sulcal maps in individualswith and without autism found anteriorand superior displacements of the supe-rior temporal sulcus [Levitt et al., 2003]and Boddaert et al. [2004] recently re-ported abnormal superior temporal sulcusvolume in autism.
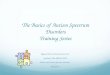
Building upon research to examinepolysensory areas of the superior tempo-ral sulcus region in neurologically normaladults [Wright et al., 2003], the role ofthe superior temporal sulcus region inaudiovisual speech perception was re-cently explored in a small group of high-functioning individuals with autism andneurologically normal controls by com-paring responses to various auditory andvisual speech stimuli [Collins and Pel-phrey, unpublished thesis data]. Fourtypes of stimuli were used to present theauditory and visual components ofspeech in isolation and in combination:(1) auditory speech alone, (2) visualspeech alone, (3) matched audiovisualspeech (i.e., the observed mouth move-ment matched the heard word), and (4)mismatched audiovisual speech (i.e., theobserved and heard words did notmatch). Consistent with a prior report[Wright et al., 2003], the superior tem-poral sulcus region (see Fig. 3) was acti-vated bilaterally during audiovisualspeech perception in both groups of sub-jects. For typically developing subjects,hemodynamic responses from this regionto the audiovisual match condition weregreater than responses to either the audioor the visual components presented inisolation; the audiovisual mismatch con-dition evoked a depressed response con-sistent with the inhibition that is gener-ally observed in paradigms of this type[see Calvert, 2001 for a review]. For thesubjects with autism, there was overallhypoactivation in the superior temporalsulcus region and this region respondedequally to the matching and mismatchingaudiovisual stimuli, suggesting a lack ofsensitivity to the context (matching or
mismatching) of the audiovisual speechstimuli in individuals with autism.
The findings reviewed above areconsonant with a potential disruption inthe superior temporal sulcus region itselfin autism but cannot rule out the alter-native hypothesis that there may be ab-normal functional connectivity betweenthe superior temporal sulcus region andother regions critical to social under-standing. Under this hypothesis, the su-perior temporal sulcus region is criticalfor forming a perceptual representationof socially relevant information regardingthe actions of others and activates initiallyin an obligatory manner when the sub-ject perceives an action (e.g., an eyemovement or hand gesture) made by an-other individual. The representationformed in this region is then fed forwardto higher systems that analyze the goal-directed and intentional components ofthese motions. These higher systems mayengage and maintain activation in thesuperior temporal sulcus region via feed-back when additional processing is re-quired (e.g., when an action violates theviewer’s expectations) and thus contrib-ute to the activation patterns of the su-perior temporal sulcus region. The loca-tions of these putative higher systemswithin this model are unspecified butmay include prefrontal regions and/orthe amygdala. In individuals with autism,the connection between higher-level sys-tems and the superior temporal sulcusregion may be broken, and thus thehigher level systems do not engage andmaintain activation in the superior tem-poral sulcus region. In light of this hy-pothesis, it is interesting to note that arecent fMRI study by Just et al. [2004]found lower functional connectivity be-tween Wernicke’s and Broca’s areas dur-ing language processing in subjects withautism, thereby demonstrating the po-tential value of examining functionalconnectivity in future studies of the su-perior temporal sulcus region and socialcognition in autism.
Table 2. Functional Neuroimaging Studies Implicating the SuperiorTemporal Sulcus Region in Autism
Study Stimuli Key Findinga
Castelli et al. [2002] Viewing animations of geometric shapes that elicitvarying mental state attributions
Reduced activity in the right superior temporal sulcus and reducedfunctional connectivity between the superior temporal sulcus andvisual cortex
Boddaert et al. [2003] Listening to human vocal sounds Reversed hemispheric dominance and hypoactivation of left temporalregions for perception of speech
Gervais et al. [2004] Listening to human vocal sounds Reduced activity in the left and right superior temporal sulci and gyri
aSummary of key finding is made with reference to the primary reported difference between subjects with autism and those without autism.
265MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

Fusiform GyrusA region of human occipitotempo-
ral cortex in the fusiform gyrus is acti-vated in functional neuroimaging studiesby faces (often bilaterally but more reli-ably on the right than on the left) whencontrasted with other objects or scram-bled images [Puce et al., 1996; Kan-wisher et al., 1997; McCarthy et al.,1997], can be modulated by attentionunder some conditions [Haxby et al.,1994], and may be relatively specific forfaces [Kanwisher et al., 1997; McCarthyet al., 1997], although the specificity ofthese regions for face processing is con-tended [Gauthier et al., 2000, 2003]. This
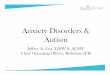
region, unlike the superior temporal sul-cus, may be disproportionately importantfor processing the static features of faces(e.g., those required to recognize identityas opposed to emotional expression oreye gaze) [McCarthy; 1999b]. Fig. 4 il-lustrates face-related activity in the rightfusiform gyrus in a 9-year-old neurolog-ically normal child. During fMRI scan-ning, this child observed faces presentedperiodically within a changing montageof common objects (e.g., kitchen utensilsand hand tools). Bilateral activation ofthe fusiform gyri by faces (yellow-to-redoverlay) is evident, with somewhat moreextensive activation obtained in the right
fusiform. Activation by faces of right lat-eral cortex in and near the superior tem-poral sulcus region is also prominent.
Electrophysiological recordings fromelectrodes placed directly on the fusiformgyrus in patients requiring brain surgeryhave further demonstrated that face-spe-cific evoked activity in the fusiform gyrusoccurs within 200 ms of face presentation[Allison et al., 1999; McCarthy, 1999a;Puce et al., 1999]. Electrical stimulation ofthese same sites has frequently led to tran-sient prosopagnosia (inability to recognizefaces), strongly implicating the discrete re-gions of the fusiform gyrus in face process-ing [Allison et al., 1994; see McCarthy,1999b for a review].
Behavioral studies have providedconsiderable support for face processingdeficits in autism [e.g., Hobson et al.,1988; Loveland et al., 1997], althoughthe precise nature of these deficits hasremained unclear. Thus, the fusiform gy-rus became a focus of initial functionalneuroimaging studies in autism. Table 3summarizes four functional neuroimag-ing studies that have focused on the roleof the fusiform gyrus in autism. Schultz etal. [2000] conducted the first fMRI studyto focus specifically on the fusiform gy-rus’ response to faces in autism. Theyexamined face and subordinate-level ob-ject perception in a sample of high-func-tioning adolescents and adults with au-tism and Asperger’s syndrome and twocarefully matched control groups. Theyfound that subjects with autism spectrumdisorders, relative to controls, exhibit lessface-evoked activity in the fusiform gyrusand recruit regions normally used fornonface object perception to processfaces. Three other fMRI studies have alsoidentified fusiform gyrus hypoactivationin autism [Critchley et al., 2000; Pierce etal., 2001; Hubl et al., 2003]. These find-ings collectively suggest important neuralcorrelates for face processing deficits inadults with autism spectrum disorders.Schultz et al. [2000] suggested a link be-tween amygdala dysfunction in autism[e.g., Critchley et al., 2000] and the lackof the development of a normal face-specific response in the fusiform gyrus(and associated abnormal face perception)in autism, proposing that an early disrup-tion in the amygdala and its connectionsto temporal cortices, including the fusi-form gyrus and superior temporal sulcus,leads to a relative lack of interest in facesand other socially important stimuli andthus to failure of the development of thenormal (activity dependent) specificity ofregions within the fusiform gyrus in au-tism. Longitudinal functional neuroim-aging studies of face processing children
Fig. 3. Results from a study of audiovisual speech perception in autism. Bilateral activity wasobserved in the superior temporal sulcus (STS) and superior temporal gyrus (STG) during audiovisualspeech perception in typically developing participants and subjects with autism. For controls,hemodynamic responses from this region to the audiovisual match condition were greater thanresponses to either the audio or the visual components presented in isolation and greater than theaudiovisual mismatch condition, which led to a depressed response relative to the audio only andaudiovisual matched conditions. In subjects with autism, this brain region responded equivalentlyto matching and nonmatching audiovisual speech stimuli.
Fig. 4. Fusiform gyrus activation to faces in a 9-year-old typically developing child. Face � objectactivations were observed in the (1) fusiform gyri (yellow-to-red overlay) and (2) the right posteriorsuperior temporal sulcus. As illustrated at the right, the child observed images of faces presentedperiodically within a changing montage of common objects in a semiblocked design.
266 MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

with and without autism have not beenconducted but will be necessary to ex-plore this hypothesis.
The above interpretation has re-cently been contended. The debate isspurred in part by findings from eyetracking studies of individuals with au-tism that suggest that autistic people donot look at faces in the same way as doneurologically normal individuals [Klinet al., 2002; Pelphrey et al., 2002]. Forexample, Pelphrey et al. [2002] demon-strated that individuals with autism spendless time visually scanning the core fea-tures of the face, particularly the eyes.These data are illustrated in Fig. 5. Giventhese findings, it is possible that the hy-poactivation of the fusiform gyrus in re-sponse to faces is the result of abnormalscan paths. That is, in the three studiesthat have not controlled for or recordedsubjects’ eye movements, the lack of ac-tivation might simply have reflected lessvisual fixation on and visual attention tothe faces and particularly the eyes. In-deed, intracranial recordings of face spe-cific N200 responses from the fusiformgyrus have shown that full faces evokelarger N200 than do isolated eyes [Mc-Carthy et al., 1999], but the N200 re-sponse amplitude in face-specific sites de-creases progressively in the order of faces,eyes, contours, lips, and noses, suggestingthat, of the internal face parts, eyes carrysignificant weight in driving the fusi-form’s response to faces.
A recent fMRI study directly ad-dressed this issue. Hadjikhani and col-leagues [2004] examined face and objectprocessing in samples of individuals withand without autism. The study used pic-tures of faces and objects and placed afixation point in the center of the stimulito ensure that participants were lookingat and attending to the images in thesame way. With this design, individuals
with autism activated the fusiform gyrusnormally when they viewed faces com-pared to objects. Similarly, in a study thatcombined fMRI and eye-tracking, David-son and Dalton [2003] linked hypoactiva-tion in the fusiform gyrus to inattention tothe eye region. Specifically, in subjects withautism and controls, there was a strongpositive correlation between the numberand length of fixations on the eyes and themagnitude of the response to faces in thefusiform gyrus. In discussing this finding,the authors suggested that it reflects activeavoidance of gaze resulting from auto-nomic hyperreactivity to salient social stim-uli. This hyperreactivity to the eyes isthought to result from dysfunction in affec-tive regulation processes subserved by theamygdala and prefrontal cortices [Davidsonand Irwin, 1999]. Alternatively, both sets offindings (fusiform gyrus hypoactivity andthe correlation between the fusiform gyrusresponses and attention to the eyes) couldreflect a failure to marshal a social responseto the environment, rather than activeavoidance of social interaction. In essence,the individuals with autism fail to look atfaces naturally because the significance ofthe face, and particularly the eyes, is notappreciated by these subjects. Both possi-bilities are worthy of serious future researchand both may be true but perhaps for dif-ferent subgroups of autistic individuals.
SUMMARYWe have reviewed a substantial
body of evidence from neuroimagingstudies of individuals with and withoutautism that indicates important func-tional abnormalities in autism in neuro-anatomical structures thought to play keyroles in different aspects of human socialcognition. This review highlighted threestructures: the amygdala, the superiortemporal sulcus region, and the fusiformgyrus. Studies of typically developing
adults leave no doubt that these structuresfunction in parallel and should bethought of as elements of a broader sys-tem subserving social cognition. For ex-ample, when encountering a socially de-manding situation, the amygdala willprovide a quick and automatic bias withrespect to those aspects of the responsethat pertain to evaluating the potentiallythreatening nature of the situation orwith respect to allocating processing re-sources to those stimuli that are poten-tially important but ambiguous. The fusi-form gyrus will be engaged to the extentthat a perceptual representation of a faceneeds to be made available, perhaps tomake a determination of personal iden-tity. Sectors of the superior temporal sul-cus will be called upon to conduct avisual analysis of socially and communi-catively important human actions, in-cluding movements of facial features andshifts in eye gaze, while other sectors willserve to incorporate auditory and visualcomponents of socially meaningful stim-uli, particularly human speech. The rapidintegration of the functions performed byeach structure would be important toguide social behavior in a typical situa-tion in real life. To date, disruption ineach of the components has been studiedin autism, but their integration has typi-cally been neglected, and probably forgood reason; the initial stages of scientificanalysis often demand a focus on the treesrather than the forest. Future goals willbe to provide a more detailed account ofthe relative contributions that each neu-roanatomical structure makes to socialcognition dysfunction in autism and atthe same time to provide a more integra-tive picture of how functional disruptionin one or more structures in autism mightreflect dysfunction of the entire system.A challenge for the future will be to offera more precise account of the interplay
Table 3. Functional Neuroimaging Studies Implicating the Fusiform Gyrus in Autism
Study Stimuli Key Findinga
Schultz et al. [2000] Face versus object discrimination Greater inferior temporal gyri and decreased rightfusiform gyrus activation during face processing
Critchley et al. [2000] Implicit and explicit processing of emotional facial expressions Failed to activate amygdala in the implicit task andthe fusiform gyrus in the explicit task
Pierce et al. [2001] Viewing faces and objects Reduced activity bilaterally in the fusiform gyrus,increased activity in idiosyncratic regions (e.g.,frontal, occipital cortex, anterior fusiform gyrus)
Hubl et al. [2003] Viewing faces and complex patterns Reduced activity in the fusiform gyrus during faceprocessing and greater activity in the medial oc-cipital gyrus
Hadjikhani et al. [2004] Viewing faces and objects Identified normal activity levels in the fusiform gyrusafter controlling for fixation point
aSummary of key finding is made with reference to the primary reported difference between subjects with autism and those without autism.
267MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

between all of these different processes asa function of the detailed specification ofthe performance demands required by agiven experimental task or by a givensituation in real life.
FUTURE DIRECTIONSFuture directions in research on
the neuroanatomical substrates of social
cognition dysfunction in autism willclearly build upon the findings to date,extend them to broader issues, and at-tempt to resolve some of the currentdiscrepancies and debates. Of specialvalue will be attempts to extend the cur-rent findings, almost all of which comefrom studies of adults, to studies of chil-
dren that incorporate a developmentalperspective (i.e., a perspective involvingearly and longitudinal study of brain andbehavioral development). There are sev-eral reasons why a developmental per-spective on social cognition in autism iscompelling and important.
First, deficits in aspects of socialcognition may originate from primaryimpairments in joint attention and imita-tion, language functioning, and/or theability to disengage and shift attention.Similarly, given the dynamic and recip-rocal relationships between early braininsults and behavioral and cognitive de-velopment, autistic symptoms are at bestindirect reflections of key neurodevelop-mental disturbances. Rather than being adisorder of a specific neuroanatomicalstructure or circuit, it may be that autismarises from subtle and more diffuse earlyneuropathology that ultimately affectsmultiple neural systems, both directly andthrough compensatory experience-de-pendent reorganization.
Second, as a neurodevelopmentaldisorder, autism is a member of a subsetof behavioral and cognitive disorders thatare linked directly to a primary underly-ing neurobiological process, that havetheir onset in the earliest years of child-hood, and that have symptoms thatchange over ontogeny. Although thecore deficits in autism persist throughoutthe lifespan, their actual expression differsdepending on the age of the individual.Neuroimaging studies of autism that takeinto account these psychological and be-havioral continuities and discontinuitiesfrom childhood to adulthood would bet-ter inform us of the neurobiologicalmechanisms in autism than would studiesthat provide only a static picture inadults.
Third, very little is known aboutthe neural correlates of social cognitionin children or about the changes in brainfunction that underlie normative devel-opment in this domain. Thus, fundamen-tal scientific questions concerning thematuration of the brain and its relation-ship to changes in social cognition inhealthy children remain unanswered.This paucity of information is particularlyunfortunate because this basic knowledgeis essential to efforts aimed at understand-ing the neural basis of social cognitiondeficits in autism. Future longitudinalfMRI studies will allow the field to con-struct normal developmental curves forthe functioning of circuits supporting so-cial cognition by age and sex of the childand reveal changes in the circuitry un-derlying developments in the selected as-pects of social cognition during critical
Fig. 5. Abnormalities in visual scanpaths during face processing in high-functioning individualswith autism. Among other deficits in social perception and social cognition, individuals with autismexhibit abnormal scanpaths when viewing faces, typically spending little time on the core featuresof the face, particularly the eyes. The cross marks and lines together indicate the subject’s point ofregard over time during the presentation of the face. Scanpaths are shown from three subjects withautism (left column) and three subjects without autism (right column). Reproduced with permissionfrom Pelphrey et al. [2002].
268 MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

periods of childhood before, during, andafter major developmental epochs. Theavailability of this normative data willfacilitate efforts to characterize atypicaldevelopmental pathways in autism.
Fourth, the early diagnosis of au-tism is an inexact science. Autism is abehavioral syndrome; thus, in contrast tosome other neurodevelopmental disor-ders (e.g., fragile X) no genetic test isavailable to assist a physician in unambig-uously diagnosing autism. Functionalbrain correlates of autism in children mayprove useful in the early identification ofautism. To the extent that the proposedresearch can elucidate developmental tra-jectories of the neural circuitry support-ing pivotal social cognitive skill, it caninform the design of more effective pro-grams for the treatment of autism. Bystarting early, treatments could target de-velopmental pathways of key neural cir-cuits, perhaps shifting them from abnor-mal to normal pathways.
Fifth, a developmental perspectivecan be a useful tool for unraveling theinteraction between seemingly disparatelevels of organization, such as that fromthe molecular biology of gene expressionto the development of cognitive abilities.The human adult brain and the cognitivearchitecture it sustains are composed of acomplex series of hierarchical and parallelsystems that has proven very difficult toanalyze in an exclusively top-down fash-ion. For example, lesions are unlikely tocleanly dissociate different levels of orga-nization or different processes and apply-ing the mapping between brain regionsand functions found in normal adults tounderstanding developmental disorderswill be only partially informative. A de-velopmental approach can allow inde-pendent observation of different levels ofhierarchical control, through observationof how various neurocognitive systemsemerge and integrate over ontogeny.
Finally, by defining functionalbrain phenotypes based on neurofunc-tional/behavioral developmental path-ways, fMRI studies of children with au-tism have the potential to dissect theheterogeneity present in autism as a be-haviorally defined syndrome. Functionalneuroimaging studies of autistic childrencould reveal different brain phenotypesin the circuitry involved in social cogni-tion. These phenotypes might relate tobehavioral outcomes and could suggestnovel and more targeted interventionand treatment strategies. Early and longi-tudinal study will be critical in definingbrain phenotypes in autism because theshape of developmental trajectories ofbrain functioning in specific circuits will
provide more detail on the nature of theabnormalities in autism than will analysisof brain phenotypes in adults. Brain–be-havior studies, particularly those focusedon changing brain–behavior relation-ships in the developing brain, may alsoprovide clues to candidate genes in au-tism, as developmentally important genesbegin to be linked to particular patternsof brain development and gene expres-sion.
Another important avenue for fur-ther studies of social cognition dysfunc-tion in autism is the development ofstimuli and of tasks with more ecologicalvalidity for studying social cognition.Despite the advances reviewed above,progress in the social brain sciences hasbeen slowed somewhat by the lack ofecologically valid social situations thatcan be manipulated and presented in asocially relevant fashion within the con-straint of the testing environments (e.g., aMRI scanner or evoked response poten-tial laboratory). Most studies have imagedsubjects during viewing of simple, staticimages that are confined to a single stim-ulus category. While this strategy hasbeen fruitful for identifying regions of thebrain with functional specificity for par-ticular classes of objects, several questionsremain unanswered about the moderat-ing effects of the context of stimulus pre-sentation on these brain regions. For ex-ample, a key element for successfullyimaging brain regions during social per-ception is that social interactions maydepend upon the “perceived” participa-tion of the individual being tested in thevery scene that is depicted. The develop-ment of naturalistic social stimuli will al-low the field to explore important ques-tions regarding the neural basis of socialperception and cognition–questions thathave gone largely unanswered because ofthe impoverished stimulus environmenttypically used in these studies. Indeed,subtle but important social deficits areoften most evident in high-functioningindividuals with autism when these indi-viduals are faced with relatively unstruc-tured social settings that demand sensitiv-ity to context and the intentions ofothers.
As future studies begin to shift fo-cus from functioning in single regions tointeractions between brain regions (andtheir possible disruptions in autism) in-volved in social cognition, continued de-velopments in techniques for noninva-sive imaging of the human brain willremain key. We will see researchers morefrequently combining data from comple-mentary imaging techniques for examin-ing structure, function, and connectivity
(i.e., multimodal imaging) in the study ofsocial cognition dysfunction in autism.For example, the combined use of diffu-sion tensor imaging (DTI) and fMRI instudies of individuals with and withoutautism holds great promise for studyingthe role of functional connectivity in def-icits that characterize autism. DTI is atechnique that permits the tracking ofwhite matter fiber tracks by quantifyingthe diffusion of water molecules in thebrain. Molecules diffuse less readily acrossmembranes, and part of the MRI processfacilitates the directional mapping ofwhite matter tracts based on this princi-ple. Applying such a technique in autismwould help explicate any differences inthe trajectories and connections of neuraltracts between brain areas. f
REFERENCESAdolphs R. 1999. Social cognition and the human
brain. Trends in Cogn Sci 3:469–479.Adolphs R. 2001. The neurobiology of social cog-
nition. Curr Opin Neurobiol 11:231–239.Adolphs R. 2003. Is the human amygdala special-
ized for processing social information? AnnNY Acad Sci 985:326–340.
Adolphs R, Damasio H, Tranel D, et al. 2000. Arole for somatosensory cortices in the visualrecognition of emotion as revealed by three-dimensional lesion mapping. J Neurosci 20:2683–2690.
Adolphs R, Sears L, Piven J. 2001. Abnormal pro-cessing of social information from faces inautism. J Cogn Neurosci 13:232–240.
Adolphs R, Tranel D. 2000. Emotion recognitionand the human amygdala. In J. P. Aggleton(Ed.), The amygdala. A functional analysis(pp. 587–630). New York: Oxford Univer-sity Press.
Adolphs R, Tranel D, Damasio AR. 1998. Thehuman amygdala in social judgment. Nature393:470–474.
Adolphs R, Tranel D, Damasio H, et al. 1994.Impaired recognition of emotion in facial ex-pressions following bilateral damage to thehuman amygdala. Nature 372:669–672.
Adolphs R, Tranel D, Damasio H, et al. 1995. Fearand the human amygdala. J Neurosci15:5879–5891.
Adolphs R, Tranel D, Hamann S, et al. 1999.Recognition of facial emotion in nine indi-viduals with bilateral amygdala damage. Neu-ropsychologia 37:1111–1117.
Allison T, McCarthy G, Nobre A, et al. 1994.Human extrastriate visual cortex and the per-ception of faces, words, numbers, and colors.Cerebral Cortex 4:544–554.
Allison T, Puce A, McCarthy G. 2000. Social per-ception from visual cues: Role of the STSregion. Trends Cogn Sci 4:267–278.
Allison T, Puce A, Spencer DD, et al. 1999. Elec-trophysiological studies of human face per-ception I. Potentials generated in occipito-temporal cortex by face and non-face stimuli.Cerebral Cortex 9:415–430.
Amaral DG, Bauman MD, Capitanio JP, et al.2003. The amygdala: Is it an essential com-ponent of the neural network for social cog-nition? Neuropsychologia 41:517–522.
Amaral DG, Insausti R. 1992. Retrograde transportof D-[3H]-aspartate injected into the monkeyamygdaloid complex. Exp Brain Res 88:375–388.
269MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

Amaral DG, Veazey RB, Cowan WM. 1982. Someobservations on hypothalamo-amygdaloidconnections in the monkey. Brain Res 252:13–27.
American Psychiatric Association. 1994. Diagnosticand Statistical Manual of Mental Disorders,4th Edition. Washington, DC: American Psy-chiatric Association.
Anderson AK, Phelps EA. 2000. Expression with-out recognition: Contributions of the humanamygdala to emotional communication. Psy-chol Sci 11:106–111.
Bachevalier J. 1994. Medial temporal lobe struc-tures and autism: A review of clinical andexperimental findings. Neuropsychologia 32:627–648.
Bachevalier J. 1996. Brief report: Medial temporallobe and autism: A putative animal model inprimates. J Autism Dev Disord 26:217–220.
Bachevalier J, Mishkin M. 1994. Effects of selectiveneonatal temporal lobe lesions on visual rec-ognition memory in rhesus monkeys. J Neu-rosci 14:2128–2139.
Bailey A, Le Couteur A, Gottesman I, et al. 1995.Autism as a strongly genetic disorder: Evi-dence from a British twin study. Psychol Med25:63–77.
Bailey DB Jr., Hatton DD, Skinner M, et al. 2001.Autistic behavior, FMR1 protein, and devel-opmental trajectories in young males withfragile X syndrome. J Autism Dev Disord31:165–174.
Baker P, Piven J, Sato Y. 1998. Autism and tuber-ous sclerosis complex: Prevalence and clinicalfeatures. J Autism Dev Disord 28:279–285.
Baron-Cohen S, Jolliffe T, Mortimore C, et al.1997. Another advanced test of theory ofmind: Evidence from very high functioningadults with autism or Asperger syndrome.J Child Psychol Psychiatry 38:813–822.
Baron-Cohen S, Ring HA, Wheelwright S, et al.1999. Social intelligence in the normal andautistic brain: An fMRI study. Eur J Neurosci11:1891–1898.
Belin P, Zatorre RJ. 2000. ‘What’, ‘where’ and‘how’ in auditory cortex. Nat Neurosci3:965–966.
Blakemore SJ, Sarfati Y, Bazin N, et al. 2003. Thedetection of intentional contingencies in sim-ple animations in patients with delusions ofpersecution. Psychol Med 33:1433–1441.
Boddaert N, Belin P, Chabane N, et al. 2003.Perception of complex sounds: Abnormalpattern of cortical activation in autism. Am JPsychiatry 160:2057–2060.
Boddaert N, Chabane N, Gervais H, et al. 2004.Superior temporal sulcus anatomical abnor-malities in childhood autism: A voxel-basedmorphometry MRI study. Neuroimage 23:364–369.
Breiter HC, Etcoff NL, Whalen PJ, et al. 1996.Response and habituation of the humanamygdala during visual processing of facialexpression. Neuron 17:875–887.
Broks P, Young AW, Maratos EJ, et al. 1998. Faceprocessing impairments after encephalitis:Amygdala damage and recognition of fear.Neuropsychologia 36:59–70.
Brothers L. 1990. The social brain: A project forintegrating primate behavior and neurophys-iology in a new domain. Concepts Neurosci1:27–51.
Brown S, Schafer A. 1888. An investigation intothe functions of the occipital and temporallobes of the monkey’s brain. Philos Trans RSoc Lond [Biol] 179:303–327.
Calvert GA. 2001. Crossmodal processing in the hu-man brain: Insights from functional neuroimag-ing studies. Cereb Cortex 11:1110–1123.
Calvert GA, Campbell R, Brammer MJ. 2000.Evidence from functional magnetic resonanceimaging of crossmodal binding in the humanheteromodal cortex. Curr Biol 10:649–657.
Campbell R, Heywood CA, Cowey A, et al. 1990.Sensitivity to eye gaze in prosopagnosic pa-tients and monkeys with superior temporalsulcus ablation. Neuropsychologia 28:1123–1142.
Castelli F, Frith C, Happa�e F, et al. 2002. Autism,Asperger syndrome and brain mechanisms forthe attribution of mental states to animatedshapes. Brain 125:1839–1849.
Cook EH, Jr., Courchesne RY, Cox NJ, et al.1998. Linkage-disequilibrium mapping of au-tistic disorder, with 15q11–13 markers. Am JHum Genet 62:1077–1083.
Critchley HD, Daly EM, Bullmore ET, et al. 2000.The functional neuroanatomy of social be-haviour: Changes in cerebral blood flowwhen people with autistic disorder processfacial expressions. Brain 123:2203–2212.
Cusick CG. 1997. The superior temporal polysen-sory region in monkeys. In: Rockland KS,Kaas JH, Peters A, editors. Cerebral CortexVol 12: Extrastriate Cortex in Primates. NewYork: Plenum Press. p 435–468.
Davidson RJ, Dalton K. 2003. Dysfunction in theneural circuitry of emotional face processingin individuals with autism. Psychophysiology40:s3.
Davidson RJ, Irwin W. 1999. The functional neu-roanatomy of emotion and affective style.Trends Cogn Sci 3:11–21.
Dawson G, Meltzoff AN, Osterling J, et al. 1998.Children with autism fail to orient to natu-rally occurring social stimuli. J Autism DevDisord 28:479–485.
Decety J, Grezes J. 1999. Neural mechanisms sub-serving the perception of human actions.Trends Cogn Sci 3:172–178.
Emery NJ, Capitanio JP, Mason WA, et al. 2001.The effects of bilateral lesions of the amygdalaon dyadic social interactions in rhesus mon-keys (Macaca mulatta). Behav Neurosci 115:515–544.
Folstein S, Rutter M. 1977. Genetic influences andinfantile autism. Nature 265:726–728.
Folstein SE, Rosen-Sheidley B. 2001. Genetics ofautism: Complex aetiology for a heteroge-neous disorder. Nat Rev Genet 2:943–955.
Fombonne E. 1999. The epidemiology of autism:A review. Psychol Med 29:769–786.
Fried I, MacDonald KA, Wilson CL. 1997. Singleneuron activity in human hippocampus andamygdala during recognition of faces and ob-jects. Neuron 18:753–765.
Frith CD, Frith U. 1999. Interacting minds: Abiological basis. Science 286:1692–1695.
Gauthier I, Curran T, Curby KM, et al. 2003.Perceptual interference supports a non-mod-ular account of face processing. Nat Neurosci6:428–432.
Gauthier I, Skudlarski P, Gore JC, et al. 2000.Expertise for cars and birds recruits brain areasinvolved in face recognition. Nat Neurosci3:191–197.
Gervais H, Belin P, Boddaert N, et al. 2004. Ab-normal cortical voice processing in autism.Nat Neurosci 7:801–802.
Hadjikhani N, Joseph RM, Snyder J, et al. 2004.Activation of the fusiform gyrus when indi-viduals with autism spectrum disorder viewfaces. Neuroimage 22:1141–1150.
Hariri AR, Bookheimer SY, Mazziotta JC. 2000.Modulating emotional responses: Effects of aneocortical network on the limbic system.Neuroreport 11:43–48.
Hasselmo ME, Rolls ET, Baylis GC. 1989. Therole of expression and identity in the face-selective responses of neurons in the temporalvisual cortex of the monkey. Behav Brain Res32:203–218.
Haxby JV, Horwitz B, Ungerleider LG, et al. 1994.The functional organization of human extra-striate cortex: A PET-rCBF study of selectiveattention to faces and locations. J Neurosci14:6336–6353.
Heberlein AS, Adolphs R. 2004. Impaired sponta-neous anthropomorphizing despite intact per-ception and social knowledge. Proc NatlAcad Sci U S A 101:7487–7491.
Heider F, Simmel M. 1944. An experimental studyof apparent behavior. Am J Psychol 57:243–259.
Hobson RP, Ouston J, Lee A. 1988. What’s in aface? The case of autism. Br J Psychol 79:441–453.
Hubl D, Beolte S, Feineis-Matthews S, et al. 2003.Functional imbalance of visual pathways in-dicates alternative face processing strategies inautism. Neurology 61:1232–1237.
Hughes C, Leboyer M, Bouvard M. 1997. Execu-tive function in parents of children with au-tism. Psychol Med 27:209–220.
Hughes C, Plumet MH, Leboyer M. 1999. To-wards a cognitive phenotype for autism: In-creased prevalence of executive dysfunctionand superior spatial span amongst siblings ofchildren with autism. J Child Psychol Psychi-atry 40:705–718.
Johnson MH. 1997. Developmental cognitive neu-roscience: An introduction. Cambridge, MA:Blackwell Publishers.
Just MA, Cherkassky VL, Keller TA, et al. 2004.Cortical activation and synchronization dur-ing sentence comprehension in high-func-tioning autism: Evidence of underconnectiv-ity. Brain 127:1811–1821.
Kanwisher N, McDermott J, Chun MM. 1997.The fusiform face area: A module in humanextrastriate cortex specialized for face percep-tion. J Neurosci 17:4302–4311.
Kawashima R, Sugiura M, Kato T, et al. 1999. Thehuman amygdala plays an important role ingaze monitoring: A PET study. Brain 122:779–783.
Klin A. 2000. Attributing social meaning to ambig-uous visual stimuli in higher-functioning au-tism and Asperger syndrome: The Social At-tribution Task. J Child Psychol Psychiatry41:831–846.
Klin A, Jones W, Schultz R, et al. 2002. Visualfixation patterns during viewing of naturalisticsocial situations as predictors of social compe-tence in individuals with autism. Arch GenPsychiatry 59:809–816.
Kluver H, Bucy L. 1938. An analysis of certaineffects of bilateral temporal lobectomy in therhesus monkey, with special reference to“psychic blindness.” J Psychol 5:33–54.
Kluver H, Bucy L. 1939. Preliminary analysis offunctions of the temporal lobes in monkeys.Arch Neurol Psychiatry 42:979–1000.
Kunda Z. 1999. Determining what is, what was,and what might have been: Hypothesis test-ing, covariation detection, and counterfactualthinking. In: Ingle DJ, Goodale MA, Mans-field RJW, editors. Social cognition: Makingsense of people. Cambridge, MA: MIT Press.p 111–160.
Landa R, Piven J, Wzorek MM, et al. 1992. Sociallanguage use in parents of autistic individuals.Psychol Med 22:245–254.
LeDoux J. 1996. Emotional networks and motorcontrol: A fearful view. Prog Brain Res 107:437–446.
270 MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.

Leekam SR, Hunnisett E, Moore C. 1998. Targetsand cues: Gaze-following in children withautism. J Child Psychol Psychiatry 39:951–962.
Leekam SR, La�opez B, Moore C. 2000. Attentionand joint attention in preschool children withautism. Dev Psychol 36:261–273.
Leonard CM, Rolls ET, Wilson FA, et al. 1985.Neurons in the amygdala of the monkey withresponses selective for faces. Behav Brain Res15:159–176.
Levitt JG, Blanton RE, Smalley S, et al. 2003.Cortical sulcal maps in autism. Cereb Cortex13:728–735.
Loveland KA, Landry SH. 1986. Joint attention andlanguage in autism and developmental lan-guage delay. J Autism Dev Disord 16:335–349.
Loveland KA, Tunali-Kotoski B, Chen YR, et al.1997. Emotion recognition in autism: Verbaland nonverbal information. Dev Psycho-pathol 9:579–593.
Martin A, Koenig K, Scahill L, et al. 2001. Smith-Lemli-Opitz syndrome. J Am Acad ChildAdolesc Psychiatry 40:506–507.
McCarthy G, Puce A, Belger A, Allison T. 1999.Electrophysiological studies of human faceperception II. Response properties of face-specific potentials generated in occipitotem-poral cortex. Cerebral Cortex 9:431–444.
McCarthy G. 1999a. Event-related potentials andfunctional MRI: A comparison of localizationin sensory, perceptual and cognitive tasks.Funct Neurosci: Evoked Potentials MagnFields 49:3–12.
McCarthy G. 1999b. Physiological Studies of FaceProcessing in Humans. In: Gazzaniga MS,editor. The New Cognitive Neurosciences.2nd ed. Cambridge: MIT Press. p 393–410.
McCarthy G, Puce A, Gore JC, et al. 1997. Face-specific processing in the human fusiform gy-rus. J Cogn Neurosci 9:605–610.
McCarthy G, Spicer M, Adrignolo A, et al. 1995.Brain activation associated with visual motionstudied by functional magnetic resonance im-aging in humans. Hum Brain Mapping2:234–243.
Mistlin AJ, Perrett DI. 1990. Visual and somato-sensory processing in the macaque temporalcortex: The role of ‘expectation.’ Exp BrainRes 82:437–450.
Morris JS, Frith CD, Perrett DI, et al. 1996. Adifferential neural response in the humanamygdala to fearful and happy facial expres-sions. Nature 383:812–815.
Mundy P, Sigman M, Ungerer J, et al. 1986. De-fining the social deficits of autism: The con-tribution of non-verbal communication mea-sures. J Child Psychol Psychiatry 27:657–669.
Murphy M, Bolton PF, Pickles A, et al. 2000.Personality traits of the relatives of autisticprobands. Psychol Med 30:1411–1424.
Nakamura K, Mikami A, Kubota K. 1992. Activityof single neurons in the monkey amygdaladuring performance of a visual discriminationtask. J Neurophysiol 67:1447–1463.
Nishijo H, Ono T, Nishino H. 1988. Single neu-ron responses in amygdala of alert monkeyduring complex sensory stimulation with af-fective significance. J Neurosci 8:3570–3583.
Ohnishi T, Matsuda H, Hashimoto T, et al. 2000.Abnormal regional cerebral blood flow inchildhood autism. Brain 123:1838–1844.
Oram MW, Perrett DI. 1996. Integration of formand motion in the anterior superior temporalpolysensory area (STPa) of the macaque mon-key. J Neurophysiol 76:109–129.
Oya H, Kawasaki H, Howard MA III, et al. 2002.Electrophysiological responses in the human
amygdala discriminate emotion categories ofcomplex visual stimuli. J Neurosci 22:9502–9512.
Pelphrey KA, Mitchell TV, McKeown M, et al.2003b. Brain activity evoked by perception ofhuman walking: Controlling for meaningfulcoherent motion. J Neurosci 23:6819–6825.
Pelphrey KA, Morris JP, McCarthy G. 2004b.Grasping the intentions of others: The per-ceived intentionality of an action influencesactivity in the superior temporal sulcus duringsocial perception. J Cogn Neurosci 16:1706–1716.
Pelphrey KA, Sasson NJ, Reznick JS, et al. 2002.Visual scanning of faces in autism. J AutismDev Disord 32:249–261.
Pelphrey KA, Singerman JD, Allison T, et al. 2003a.Brain activation evoked by perception of gazeshifts: The influence of context.[erratum appearsin Neuropsychologia 2003;41:1561–1562].Neuropsychologia 41:156–170.
Pelphrey KA, Viola RJ, McCarthy G. 2004. Whenstrangers pass. Processing of mutual andaverted social gaze in the superior temproalsulcus. Psychol Sci 15:598–603.
Perrett DI, Harries MH, Bevan R, et al. 1989.Frameworks of analysis for the neural repre-sentation of animate objects and actions. J ExpBiol 146:87–113.
Perrett DI, Harries MH, Mistlin AJ, et al. 1990.Social signals analysed at the cell level: some-one is looking at me, something touched me,something moved! Int J Comp Psychol 4:25–54.
Perrett DI, Hietanen JK, Oram MW, et al. 1992.Organization and functions of cells responsiveto faces in the temporal cortex. Philos TransR Soc Lond B Biol Sci 335:23–30.
Perrett DI, Smith PA, Potter DD, et al. 1985.Visual cells in the temporal cortex sensitive toface view and gaze direction. Proc R SocLond B Biol Sci 223:293–317.
Pickles A, Bolton P, Macdonald H, et al. 1995.Latent-class analysis of recurrence risks forcomplex phenotypes with selection and mea-surement error: A twin and family historystudy of autism. Am J Hum Genet 57:717–726.
Pierce K, Meuller RA, Ambrose J, et al. 2001. Faceprocessing occurs outside the fusiform ‘facearea’ in autism: Evidence from functionalMRI. Brain 124:2059–2073.
Piven J. 2001. The broad autism phenotype: Acomplementary strategy for molecular geneticstudies of autism. Am J Med Genet 105:34–35.
Piven J, Palmer P. 1999. Psychiatric disorder andthe broad autism phenotype: Evidence from afamily study of multiple-incidence autismfamilies. Am J Psychiatry 156:557–563.
Piven J, Palmer P, Jacobi D, et al. 1997. Broaderautism phenotype: Evidence from a familyhistory study of multiple-incidence autismfamilies. Am J Psychiatry 154:185–190.
Piven J, Wzorek M, Landa R, et al. 1994. Person-ality characteristics of the parents of autisticindividuals. Psychol Med 24:783–795.
Prather MD, Lavenex P, Mauldin-Jourdain ML, et al.2001. Increased social fear and decreased fear ofobjects in monkeys with neonatal amygdala le-sions. Neuroscience 106:653–658.
Puce A, Allison T, Asgari M, et al. 1996. Differ-ential sensitivity of human visual cortex tofaces, letterstrings, and textures: A functionalmagnetic resonance imaging study. J Neuro-sci 16:5205–5215.
Puce A, Allison T, Bentin S, et al. 1998. Temporalcortex activation in humans viewing eye andmouth movements. J Neurosci 18:2188–2199.
Puce A, Allison T, McCarthy G. 1999. Electro-physiological studies of human face percep-tion. III. Effects of top-down processing onface-specific potentials. Cerebral Cortex9:445–448.
Risch N, Spiker D, Lotspeich L, et al. 1999. Agenomic screen of autism: Evidence for amultilocus etiology. Am J Hum Genet 65:493–507.
Rolls ET. 1992. Neurophysiological mechanismsunderlying face processing within and beyondthe temporal cortical visual areas. Philos TransR Soc Lond B Biol Sci 335(1273):11–20;discussion 20–11.
Rutter M, Bailey A, Bolton P, et al. 1994. Autismand known medical conditions: Myth andsubstance. J Child Psychol Psychiatry 35:311–322.
Schmolck H, Squire LR. 2001. Impaired percep-tion of facial emotions following bilateraldamage to the anterior temporal lobe. Neu-ropsychology 15:30–38.
Schultz RT, Gauthier I, Klin A, et al. 2000. Ab-normal ventral temporal cortical activity dur-ing face discrimination among individualswith autism and Asperger syndrome. ArchGen Psychiatry 57:331–340.
Schumann CM, Hamstra J, Goodlin-Jones BL, etal. 2004. The amygdala is enlarged in childrenbut not adolescents with autism: The hip-pocampus is enlarged at all ages. J Neurosci24:6392–6401.
Skuse D, Morris J, Lawrence K. 2003. The amyg-dala and development of the social brain. AnnN Y Acad Sci 1008:91–101.
Sparks BF, Friedman SD, Shaw DW, et al. 2002.Brain structural abnormalities in young chil-dren with autism spectrum disorder. Neurol-ogy 59:184–192.
Sprengelmeyer R, Young AW, Schroeder U, et al.1999. Knowing no fear. Proc R Soc Lond BBiol Sci 266:2451–2456.
Veenstra-Vanderweele J, Cook E Jr., Lombroso PJ.2003. Genetics of childhood disorders: XLVI.Autism, part 5: Genetics of autism. J Am AcadChild Adolesc Psychiatry 42:116–118.
Wang AT, Dapretto M, Hariri AR, et al. 2004.Neural correlates of facial affect processing inchildren and adolescents with autism spec-trum disorder. J Am Acad Child Adolesc Psy-chiatry 43:481–490.
Whalen PJ, Rauch SL, Etcoff NL, et al. 1998.Masked presentations of emotional facial ex-pressions modulate amygdala activity withoutexplicit knowledge. J Neurosci 18:411–418.
Wicker B, Michel F, Henaff MA, et al. 1998. Brainregions involved in the perception of gaze: APET study. Neuroimage 8:221–227.
Winston JS, Strange BA, O’Doherty J, et al. 2002.Automatic and intentional brain responsesduring evaluation of trustworthiness of faces.Nat Neurosci 5:277–283.
Wolff S, Narayan S, Moyes B. 1988. Personalitycharacteristics of parents of autistic children:A controlled study. J Child Psychol Psychiatry29:143–153.
Wright TM, Pelphrey KA, Allison T, et al. 2003.Polysensory interactions along lateral tempo-ral regions evoked by audiovisual speech. Ce-rebral Cortex 13:1034–1043.
Zeki S, Watson JD, Lueck CJ, et al. 1991. A directdemonstration of functional specialization inhuman visual cortex. J Neurosci 11:641–649.
Zilbovicius M, Boddaert N, Belin P, et al. 2000.Temporal lobe dysfunction in childhood au-tism: A PET study. Positron emission tomog-raphy. Am J Psychiatry 157:1988–1993.
271MRDD RESEARCH REVIEWS ● NEURAL SUBSTRATES OF SOCIAL COGNITION DEFICITS ● PELPHREY ET AL.