Embed Size (px)
Citation preview
Neuro-Otology:DiagnosisandManagementofDizziness
Ma8hewBoykoReviewedbyDr.SureshSubramaniam
PleaseviewthispresentaDonasaslideshowtolistentotheaccompanyingaudio.Usethearrowkeysormouseclicktomovetothenextslide.
ProsperMénière(1799-1862)
ObjecDves
• Whatisdizziness?• Anatomyofhearingandbalance
• ApproachtohistoryandphysicalexaminaDon
• DisDnguishingcentralvs.peripheralcauses• InvesDgaDonsandtreatment
Dizzy Adjec've|diz!zy|\’di-zē\
:havingawhirlingsensaDonintheheadwithatendencytofall
:mentallyconfused
merriam-webster.com
Inmedicine,dizzinesscanmean…
• Spinning• VerDgo• Lightheadedness• Presyncope• Imbalance• VisualdistorDon• DisorientaDon• Anxiety• Hearingloss• Tinnitus
PossibleEDologies
Peripheral:BPPV,Meniere’sdisease,vesDbularneuriDs,vesDbularparoxysmia,perilymphfistula,superiorcanaldehiscence,otosclerosis,immunerelated(Cogansyndrome,sarcoidosis,lymphoma,carcinomatousmeningiDs),structural(acousDcneuroma,vesDbularschwannoma),infecDous(meningiDs,bacterial/fungal,syphiliDclabyrinthiDs),trauma(labyrinthconcussion),vesDbulartoxicity(gentamicin).
Central:stroke,TIA,MS,epilepsy,migraine,demyelinaDngdisease,tumor,neurodegeneraDvedisorders,rotaDonalvertebralarterysyndrome,familialataxiasyndromes,familialbilateralvesDbulopathy,familialhemiplegicmigraine,posteriorfossastructuralabnormaliDes(glioma,ChiariformaDon,AVM,cavernoma)
Other:orthostaDchypotension,irregularheartrhythm,OA,poorvision
CommonEDologies
• PeripheralvesDbulardysfuncDon(40%)• CentralbrainstemvesDbularlesion(10%)
• Psychiatricdisorder(15%)• Otheri.e.presyncope,disequilibrium(25%)
Epidemiology
• 30%ofpopulaDonhasexperiencedmoderatetoseveredizziness(Neuhaseretal.2005)– 25%ofthesepaDentshadtrueverDgo
• Morecommonamongstelderlyandfemales
• Largeimpactonhealthcare!– 80%ofdizzypaDentsseekmedicalcareatsomepoint
Ear
• Organofhearingandbalance• Threeparts:
1. Externalear"auricleandexternalcanal
2. Middleear"cavityinthepetrouspartofthetemporalbone;connectedtopharnyx
3. Internalear"seriesofcaviDesinthepetrouspartofthetemporalbonebetweenmiddleearandacousDcmeatus

Auricle
Externalauditorycanal
Tympanicmembrane
Ossicles
Innerear
Eustachiantube
Middleear
• TransmitsvibraDonsfromthetympanicmembranetotheinnerear– Tympanicmembrane"malleus"incus"stapes
• Communicateswithmastoidposteriorlyandpharynxanteriorly
Innerear
• Bonylabyrinth:linedwithperiosteumandcontainsperilymphfluid– VesDbule– 3semicircularcanals– Cochlea
• Membranouslabyrinth:conDnuoussystemofductsandsacsthatissuspendedwithinthebonylabyrinthandcontainsendolymph– Semicircularducts– Cochlearducts– Utricleandsaccule(sacs)
Hearing:• Cochlearduct
– AuditoryossiclesconvertairbornewavesfromtympanicmembranetofluidwavesincochleathatsDmulatereceptorcells
Balance:“VesDbularapparatus”• Semicircularducts
respondtomovementintheplaneoftheiranatomicalaxis– Horizontal:“no-no”– Anterior:lateralDlDng– Posterior:“yes-yes”
• Utricle"respondstocentrifugalandverDcalacceleraDon
• Saccule"respondstolinearacceleraDon
VesDbulocochlearnerve[VIII]
• Specialsensoryafferentnerve• Carriesafferentfibers– Cochleardivision"hearing– VesDbulardivision"balance
• ExitstemporalboneviainternalacousDcmeatus"crossesposteriorcranialfossa"enterslateralbrainstembetweenponsandmedulla
• FiberseithersynapseontheVesDbularnucleiorformtheVesDbulocerebellartractanddirectlyenterthecerebellum
VesDbularnuclei
• Locatedintherostralmedullaandcaudalpons• Fournuclei:
1. Lateral2. Inferior3. Medial4. Superior
• Alsoreceiveafferentinputfromcerebellum,spinalcord,andreDcularformaDon
• FormconnecDonswithcerebellum,spinalcord,oculomotorsystem,andcortex
Input:mainlyutricleandsaccule
Input:mainlysemicircularcanals
GoalsofourevaluaDon
#1Definedizziness
#2RuleoutcommonperipheralvesDbularcauses
#3Considerneurologicalcentralcauses
History
1.DefinethesymptomsIfpaDentunable,thenclassifythesymptomsaseither:
1. VerDgo2. Lightheadedness3. Strictlyimbalance(noheadsymptoms)
2.Completeafullhistoryforthesymptoms
3.Determineotherdetails1. Constantvs.episodic?Ifepisodic,duraDonandfrequency?2. Accompanyingsymptoms?3. Howdiditbegin?4. AggravaDngandalleviaDngfactors?5. Triggers?
VesDbulardysfuncDon
ManifestaDonsinclude:• VerDgo• Oscillopsia• Nausea/vomiDng
• Nystagamus
• PastpoinDng• Lateropulsion
GeneralMedicalExam
• Vitals– EspeciallyorthostaDcBP
• Cardiac– Ruleoutarrhythmia
• Pulmonary
• Abdominal
• MSK– ArthriDscanimpairgait
VesDbularPhysiology
AdaptedfromDeJong’s7thEdiDon
GeneralNeurologicalExam
• MentalStatusandlanguage• Cranialnerves
– Importanttoruleoutcentralcauses– Nystagamus– EOM– VAanddynamicVA
• Motor– Bulk,tone,strength,reflexes
• SensaDon– Pinprick,temperature,vibraDon,propriocepDon
• CoordinaDon– Finger-nose,heel-shin,RAMslookingforpast-poinDngandincoordinaDon
• GaitandRomberg– Tandemgait,Fukudasteppingtest
Neuro-otologicalExam
1. VesDbulospinalreflexes– PastpoinDng– Romberg– FukudaSteppingtest
2. VesDbulo-ocularreflexes– Oculocephalic(Doll’seyes)"performedslowlyina
comatosepaDent– Headimpulse"performedquicklyinanawakepaDent– DynamicVA– CalorictesDng(coldwaterstunstonicacDvityfrom
labyrinthonirrigatedside)3. Nystagamus
Dix-HallpikeManeuver
• Performedbyturninghead45degreesthenmovingpaDentfromuprightposiDontosupinewithheadslightlyextended
• PosiDveifup-beaDngandrotaDonalnystagamustowardearthatisdown– DiagnosDcofposteriorcanalBPPV– Nystagamususuallylasts<60secondsandcanfaDgue– Usually<15secondlatencybeforenystagamusisseen
• EsDmatedsensiDvity79%andspecificity75%
Halkeretal.2008
PleaserefertoYoutubeforvideosdemonstraDngnystagamusandtheDix-
HallpikeManeuver
HINTSEXAM
• HINTSincludes:– HeadImpulse– Nystagamus(direcDonchangingineccentricgaze)– TestofSkew(verDcalocularmisalignment)
• NormalheadimpulsewithpresenceofdirecDon-changingnystagamusandskewdeviaDonissuggesDveofstrokewith100%sensiDvityand96%specificity
• Be8erthanMRIwithDWIforrulingoutstrokeinfirst24-48hoursazersymptomonset
• EarlyMRIwasfalselynegaDvein12%ofstrokeswhenperformedwithin48hoursofsymptomonset
Ka8ahetal.2009
PhysicalExamReview
WashingtonUniversityrecommends6specifictestsforvesDbulardysfuncDononphysicalexam:1. Spontaneousandgaze-evokednystagamus2. Extra-ocularmovements3. VesDbulo-ocularreflexes4. Dix-Hallpikemaneuver5. LimbcoordinaDon6. GaitandRomberg
AdaptedfromDeJong’s7thEdiDon
InvesDgaDons
• Tailortothepresumedunderlyingdiagnosis– Electronystagmography
– RotarychairtesDng– Posturography
• UsefultoidenDfycentralcausessuchasstroke• OtherwiseBPPV,Meniere’sdisease,andVesDbularneuriDsdonothaveidenDfiableimagingcharacterisDcs
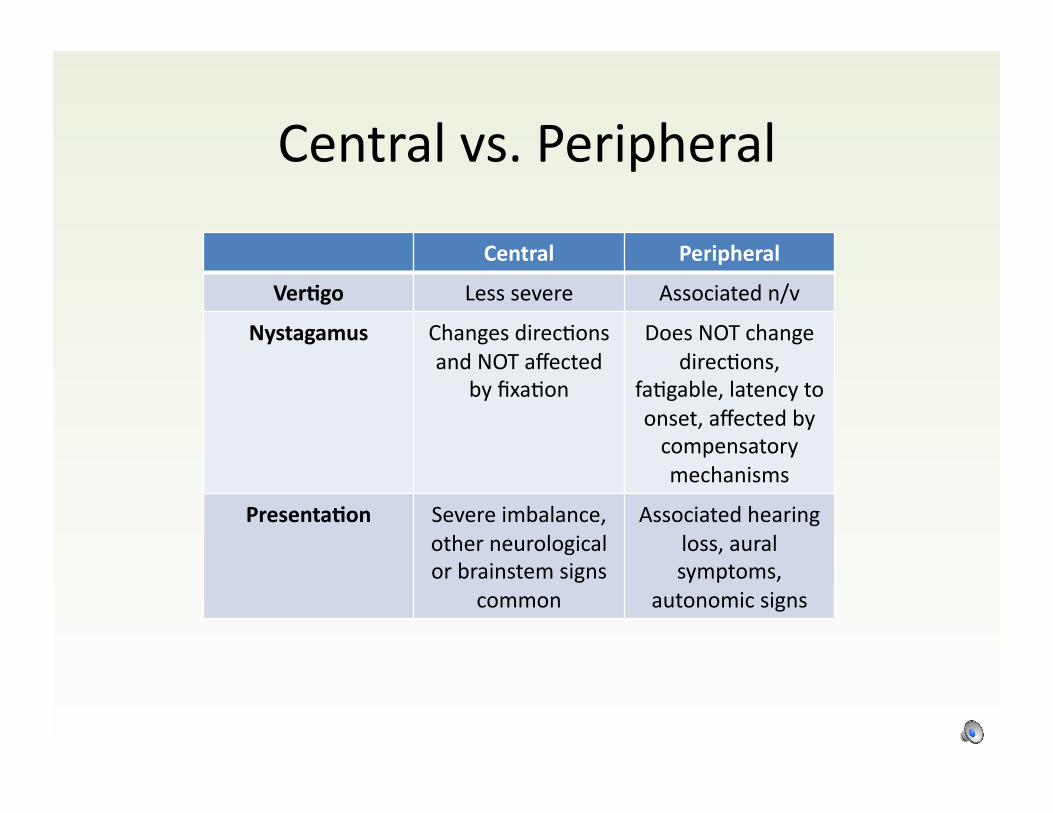
Centralvs.Peripheral
Central Peripheral
Ver9go Lesssevere Associatedn/v
Nystagamus ChangesdirecDonsandNOTaffected
byfixaDon
DoesNOTchangedirecDons,
faDgable,latencytoonset,affectedbycompensatorymechanisms
Presenta9on Severeimbalance,otherneurologicalorbrainstemsigns
common
Associatedhearingloss,auralsymptoms,
autonomicsigns
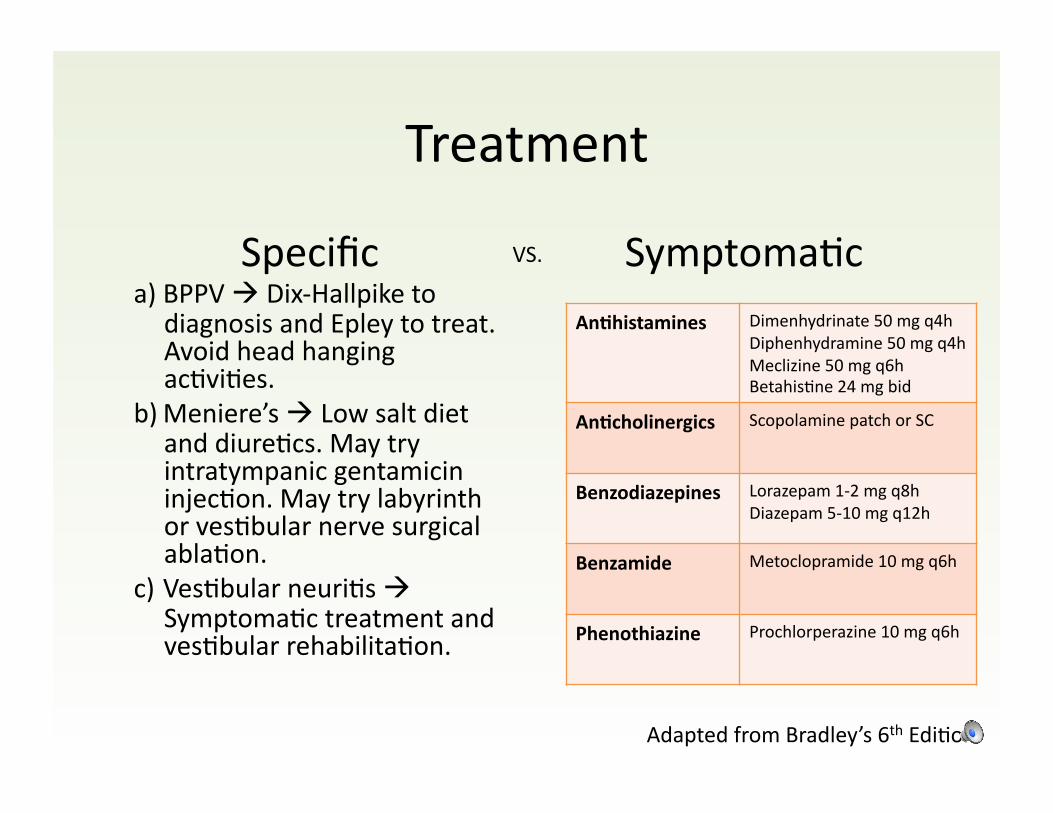
Treatment
Specifica) BPPV"Dix-Hallpiketo
diagnosisandEpleytotreat.AvoidheadhangingacDviDes.
b) Meniere’s"LowsaltdietanddiureDcs.MaytryintratympanicgentamicininjecDon.MaytrylabyrinthorvesDbularnervesurgicalablaDon.
c) VesDbularneuriDs"SymptomaDctreatmentandvesDbularrehabilitaDon.
SymptomaDcVS.
An9histamines Dimenhydrinate50mgq4hDiphenhydramine50mgq4hMeclizine50mgq6hBetahisDne24mgbid
An9cholinergics ScopolaminepatchorSC
Benzodiazepines Lorazepam1-2mgq8hDiazepam5-10mgq12h
Benzamide Metoclopramide10mgq6h
Phenothiazine Prochlorperazine10mgq6h
AdaptedfromBradley’s6thEdiDon
Case#1
86yoFdevelopsacuteonsetroomspinningaroundheruponstandingupoutofbedinthemorning.Symptomslast30secondsthenresolvedbutconDnuetooccureverymorningwhenstandingupoutofbed.
BPPV
BenignParoxysmalPosiDonalVerDgo
• InnerearcondiDoncharacterizedbyverDgowhenheadismovedrelaDvetogravity
• Otolithsbreakfreefromsaccule/utricle,se8leinsemicircularcanals,thenmoveandsDmulatehaircells
• Diagnosis:Dix-Hallpike• Treatment:EpleymaneuverorvesDbularrehabilitaDon
– MedicaDonsrecommendedforusepriortousingparDclereposiDoningmaneuverssuchasanDhistamineoranD-emeDc
– BetahisDne24mgbidx1week
Case#2
40yoMdevelopswarm,fullsensaDonintherightear.AlsomenDonsringinginhisears.OccasionallyhehasassociatedhearinglossverDgolasDngupto1daythatcanbetriggeredbysaltyfoods.
Meniere’sdisease

Meniere’sdisease
• EsDmatedincidence10-1500per100,000• BilateraldiseasecanoccurinuptohalfofpaDents• EndolymphaDchydropsdistendthemembranesofthelabyrinth
– Unclearwhythisfluidbuildupoccurs• Audiometryimportanttoassessforhearingloss• Treatment
– Lifestyle:avoidtriggers(salt<2gperday,alcohol,caffeine,nicoDne),– MedicaDons:AnDhistamines,anDcholinergics,orbenzodiazepinesfor
symptomaDctreatment– RehabilitaDon– IntervenDonaltherapiesforrefractorycases:intratympanic
gentamicin,labyrinthectomy,vesDbularneurectomy,surgicalendolymphaDcdecompression
FunFact!
IndividualsaffectedbyMeniere’sdisease:• EmilyDickinson
• KrisDnChenoweth• AlanB.Shepard• JonathanSwiz• DanaWhite
• VincentVanGogh
Case#3
72yoMwithHTN,T2DM,anddyslipidemiapresentswithacuteonsetverDgothathasnotresolvedsincestarDng.Alsolimbataxiaanddysarthria.
Stroke(centralcause)
Stroke
• Likelyvertebrobasilarstroke• PerformHINTSexam– Wouldexpectnormalheadimpulsetestbutgaze-evokednystagamusinalldirecDonsandskewdeviaDon
• ObtainurgentCT/CTA!
References
• Bradley’sNeurologyinClinicalPracDce6thEdiDon.• Uptodate.com.• Gray’sAnatomyforStudents2ndEdiDon.• DeJong’sTheNeurologicExaminaDon7thEdiDon.• Ka8ahJC,TalkadAV,WangDZ,HsiehY,Newman-TokerDE.
HINTStodiagnosestrokeintheacutevesDbularsyndrome.Stroke.2009;40(11):3504-3510.
• HalkerRB,BarrsD,DavidM,WllikKE,WingerchukDM,DemaerschalkBM.EstablishingadiagnosisofbenignparoxysmalposiDonalverDgothroughthedix-hallpikeandside-lyingmaneuvers:AcriDcallyappraisedtopic.TheNeurologist.2008;14(3):201-204.