Embed Size (px)
Citation preview

(Neuro) Informatics Technologies in Ophthalmology: Artificial Retinal Prosthesis
Addabbo G. MD,PhD; Conte E. MD; Sborgia A. MDDepartment of Ophthalmology, St. G. Moscati Hospital,ASL Taranto, Italy.
The human body can be considered as a computer which is related to the surrounding world by the five senses. In this way the human body decodes the reality and allows all the informations to the brain that decodes them giving them a meaning that our body can understand. So our brain can be considered the human CPU.The visual system is that part of the central nervous system which enables humans to process visual detailes, as well as enabling several non-image forming photoresponse functions. It transforms informations from the light for building a representation of the world. The visual system accomplishes a number of complex tasks, including the reception of light and the formation of a monocular vision ; the construction of a binocular perception; the identification and categorization of visual objects; assessing distances to and between objects; and guiding body movements in relation to visual objects.The light passes trough the dioptric media and than it goes on the retina where the electromagnetic waves are transformed in nervous impulses which are sent to the brain. These impulses guide the eye movements too, allowing the binocular vision.Three basical conditions are necessary for visual function which are :-The Light energy (Fig.1)
-A System able to transform light energy into byo-electrical Energy (Fig.2)
-And a System able to decode byo-electrical energy transorming it into vision (Fig.3)
Fig. 1
Fig. 2
Fig. 3
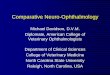
The functional anatomy of visual system is made by the globe, the optic nerve with nervous pathways and the brain.The eye (fig. 4) has three layers: the sclera, the choroid and the retina. The sclera, the most external layer, permits to the eye to mantain the shape. Muscles that control the eye movements are attached to the sclera. Choroid is the middle layer and contains the blood vessels.The cornea is a circle clear area in the sclerawhere light enters the eye. The pupil is a circular opening in the front of choroid. The iris is a colored smooth muscle surrounding the pupil wich adjust the opening according to the brightness of light. The lens is behind the pupil and is a transparent flexible biconvex structure that refracts the light and focuses the object on the central part of the retina that is called macula or fovea centralis. The retina is an extention of the brain.
The rods and the cones which are light sensitive synapse with bipolar cells which than synapse with ganglionar cells. The last one are not light sensitive but however they are able to generate and transmit nervous impulse. Their axons form the optic nerve.Than the stimulus throw the vision pathways goes to the occipital lobe for the interpretation and for processing into the images we see.Rods (Fig. 6-7) are 120 millions, they are positioned mainly in the extramacular area, with an higher concentration in the periphery of the retina. They are light sensitive but not color sensitive.Cones ( Fig. 6-7) are 6 millions and they are positioned in the central area of the retina called macula. They are light and color sensitive.
Most importante is the spatial convergence of the impulse. Infact, starting from
Fig. 4
Fig.5 the ultrastructural aspects of the retina
Fig. 6 Fig. 7
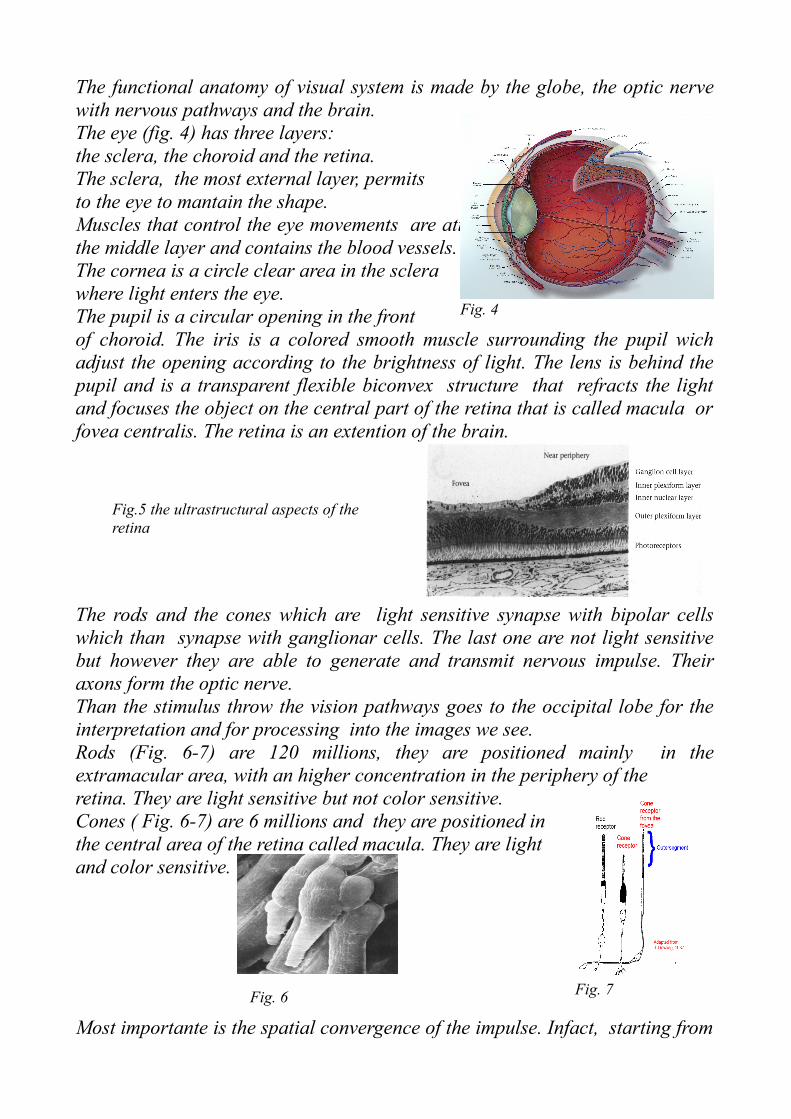
126 millions of photoreceptors, the impulses go trough 1 million and two hundred nervous fibers. Many conditions can cause blindness. In one of these the light can’t arrive on the retina because of the opacity of cornea or lens or vitreous. (Fig. 8)
In the second condition the light can arrive on the retina but the photoreceptors (rods and cones) function is compromised, the visual pathways are good. Hundreds of thousands people around the world have poor or no vision at all due to Age Related Macular Degeneration and to retinal degenerations (Rds) (Fig. 9) like retinitis pigmentosa (RP) (Fig. 10). In both of these diseases, the primary target for pathology is the retinal photoreceptor cells that dysfunction and die. Secondary neurons though are relatively spared.
Another case is when the light can arrive on the retina, the photoreceptors can transform the stimulus from light to nervous impulse but the optic nerve and the visual pathways are compromised or when due to a trauma eyes are removed.At last all stations have a good function but the brain isn’t able to decode the stimulus.The Major retinal prosthesis research groups in the world are :
• Doheny Eye Institute – USC, Second Sight, UC Santa Cruz, Caltech, University of Utah, DOE National Labs
• Univerity of Tuebignen, Retinal Implant Inc • Fraunhofer Institute, Intelligent Medical Implants • MIT, Harvard, U. Luisville, CornellOsaka University• Standford UniversityBionic Vision Australia• I I T Company ( Genova- University of Milan Italy)
Since 1960 many attempts have been made to develop visual prostheses for the blind; most of the devices were based on the production of phosphenes through electrical stimulation with microelectrodes at the retina, optic nerve or brain, but they weren’t able to reconstruct a coherent retinotopic map. Furthermore
Fig. 8
Fig. 9 Fig. 10
they display important restrictions at the biomaterial level that hinder their final implantation through surgical techniques which, at present time, offers more risks than benefits to the patient.To replace photoreceptors function, an electronic prosthetic device can be used such that retinal secondary neurons receive a signal that simulates an external visual image. There are five requirements:
• Works in absence of photoreceptors• Chip electronics do not touch retina no heat damage and electronic
package lasts for decades• Software control important to customize stimulation parameters for
patient• Wireless power and data• Real-Time visual signal processing.
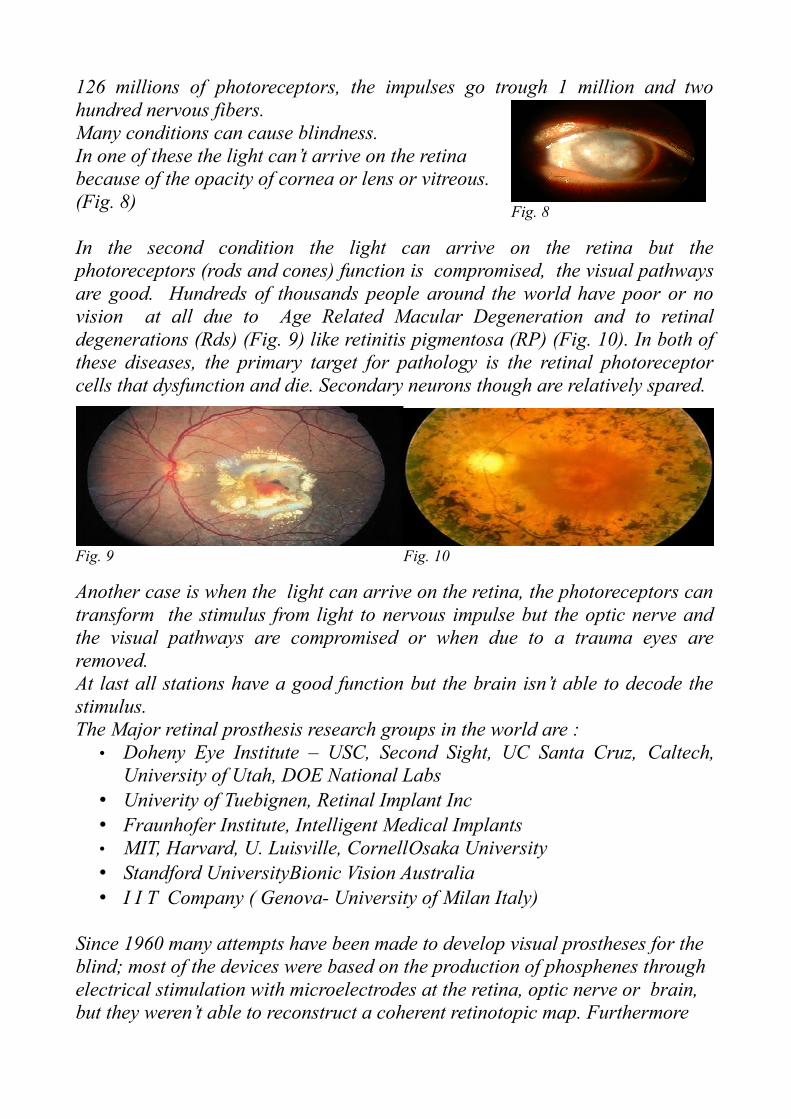
The composite device (Fig. 11) has a miniature video camera mounted on the patient's eyeglasses, which captures images and passes them to a microprocessor that converts the data to an electronic signal. This signal, in turn, is transmitted to an array of electrodes placed on the retinal surface, which transmits the patterned signal to the remaining viable secondary neurons. These neurons (ganglion, bipolar cells, etc.) begin processing the signal and pass it down the optic nerve to the brain for final integration into a visual image.
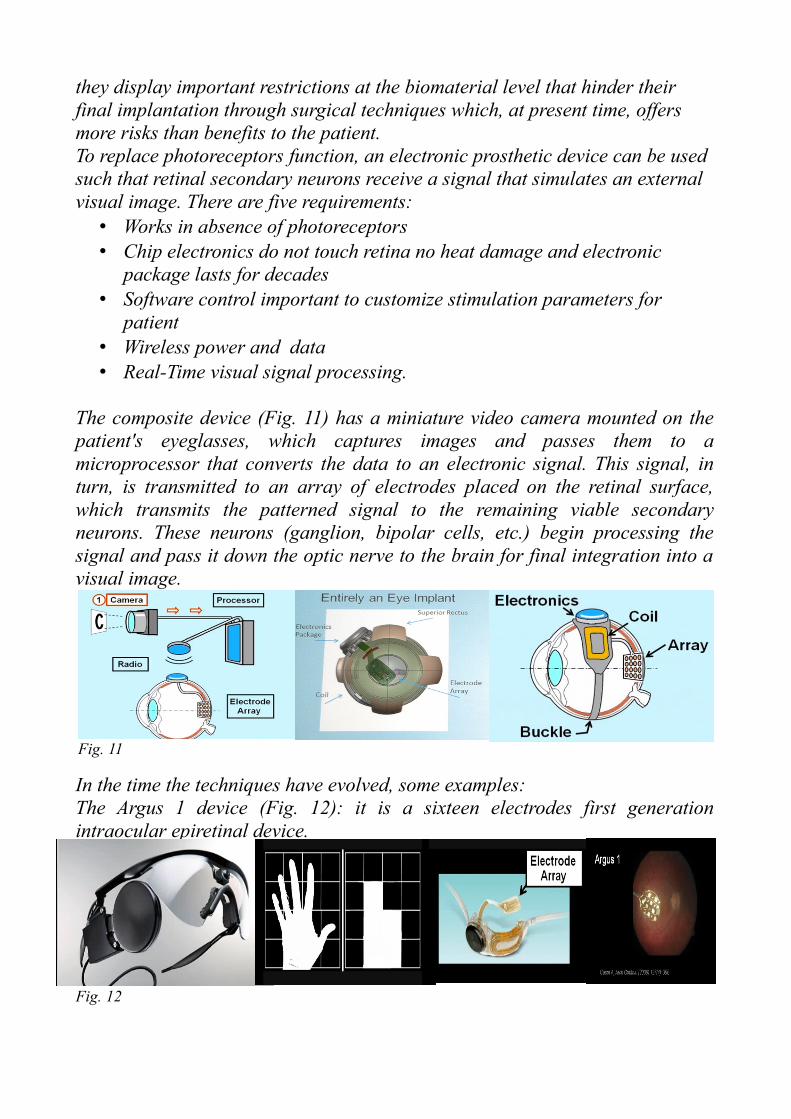
In the time the techniques have evolved, some examples:The Argus 1 device (Fig. 12): it is a sixteen electrodes first generation intraocular epiretinal device.
Fig. 11
Fig. 12
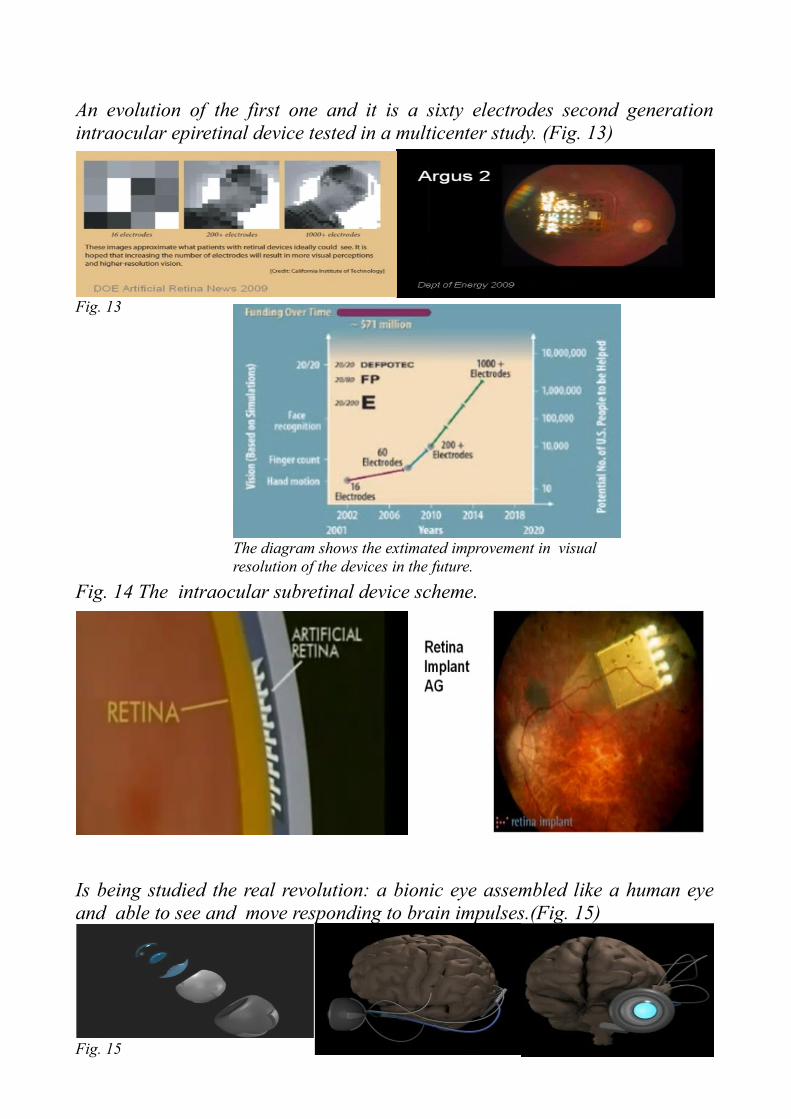
An evolution of the first one and it is a sixty electrodes second generation intraocular epiretinal device tested in a multicenter study. (Fig. 13)
Fig. 14 The intraocular subretinal device scheme.
Is being studied the real revolution: a bionic eye assembled like a human eye and able to see and move responding to brain impulses.(Fig. 15)
Fig. 13
The diagram shows the extimated improvement in visual resolution of the devices in the future.
Fig. 15

Another project of extraocular cam device connecting visual cortex area in the brain.(Fig. 16)
In the end another application of informatic skills to ophthalmology is a CPU assembled on a soft corneal contact lens.(Fig. 17) This lens is able to check serum level of glucose and wireless can control a pump device to inject insulina in diabetic patients according to the serum glucose level. Checks oxigen serum concentration, Cardiac frequence.
In conclusion, from the theoretical modeling, it is estimated that a device with approximately 1000 electrodes could give good functional vision. This could be a reality within 5-10 years from now. No treatmens are currently available for severely affected patients with R.P. and AMD. An electrical prosthetic device appears to offer hope in replacing the functions of degenerating or dead photoreceptors. Devices with new, sophisticated designs and increasing number of electrodes could allow for long-term restoration of functional sight in patients with improvement in object recognition, mobility, independent living and general quality of life.
Bibliography:Weiland, JD. (Jan 2012). Assessment of MRI issues for the Argus II Retinal Prosthesis.. Magn Reson Imaging. DOI:10.1016/j.mri.2011.12.005. PMID 22260934.
Humayun, MS. (Jan 2012). Interim Results from the International Trial of Second Sight's Visual Prosthesis.. Ophthalmology. DOI:10.1016/j.ophtha.2011.09.028. PMID 22244176.
Ahuja, AK. (Apr 2011). Blind subjects implanted with the Argus II retinal prosthesis are able to improve performance in a spatial-motor task.. Br J Ophthalmol 95 (4): 539-43.DOI:10.1136/bjo.2010.179622. PMID 20881025.
Humayun, MS. (2009). Preliminary 6 month results from the Argus II epiretinal prosthesis feasibility study.. Conf Proc IEEE Eng Med Biol Soc 2009:
4566-8.DOI:10.1109/IEMBS.2009.5332695. PMID 19963839.
Yanai D, Weiland JD, Mahadevappa M, Greenberg RJ, Fine I, Humayun MS.: “Visual performance using a retinal prosthesis in three subjects with
retinitis Pigmentosa”, Am. J. Ophthalmol. 2007 May;143(5):820-827. Epub 2007 Mar 23.
Shah S, Hines A, Zhou D, Greenberg RJ, Humayun MS, Weiland JD.: “Electrical properties of retinal-electrode interface”, J Neural Eng. 2007
Mar;4(1):S24-9. Epub 2007 Feb 20
Shah S, Chu A, Zhou D, Greenberg R, Guven D, Humayun M, Weiland J.: “Intraocular impedance as a function of the position in the eye, electrode
material and electrode size”, Conf Proc IEEE Eng Med Biol Soc. 2004;6:4169-71
Xiao X, Wang J, Liu C, Carlisle JA, Mech B, Greenberg R, Guven D, Freda R, Humayun MS, Weiland J, Auciello O.: “In vitro and in vivo evaluation
of ultrananocrystalline diamond for coating of implantable retinal microchips” J. Biomed. Mater. Res. Part B Appl. Biomater. 2006 May;77(2):273-81.
Fig. 16
Fig. 17