Embed Size (px)
DESCRIPTION
ESRD and Dialysis (2014)
Citation preview
NephSAPNephrology Self-Assessment Program
®
Volume 13 • Number 5 • November 2014
End-Stage Renal Disease and DialysisCo-Editors:
Ruediger W. Lehrich, MD
John P. Middleton, MD
EDUCATION DIRECTOR, MAINTENANCE OFCERTIFICATION (MOC)Gerald A. Hladik, MDUniversity of North Carolina at Chapel HillChapel Hill, NC
DEPUTY EDUCATION DIRECTOR,NephSAPJerry Yee, MD, FASNHenry Ford HospitalDetroit, MI
MANAGING EDITORGisela Deuter, BSN, MSAWashington, DC
ASSOCIATE EDITORSMichael J. Choi, MDJohns Hopkins University School of MedicineBaltimore, MD
Linda F. Fried, MD, MPHUniversity of PittsburghPittsburgh, PA
Richard J. Glassock, MDProfessor Emeritus, The David Geffen School ofMedicine at the University of CaliforniaLos Angeles, CA
Stanley Goldfarb, MDUniversity of Pennsylvania Medical SchoolPhiladelphia, PA
Ruediger W. Lehrich, MDDuke UniversityDurham, NC
Kevin J. Martin, MBBChSt. Louis University School of MedicineSt. Louis, MO
John P. Middleton, MDDuke UniversityDurham, NC
Patrick T. Murray, MDUniversity College DublinDublin, Ireland
Patrick H. Nachman, MDUniversity of North Carolina at Chapel HillChapel Hill, NC
Aldo J. Peixoto, MDYale UniversityWest Haven, CT
Asghar Rastegar, MDYale UniversityNew Haven, CT
Manoocher Soleimani, MDUniversity of CincinnatiCincinnati, OH
Charuhas V. Thakar, MDUniversity of CincinnatiCincinnati, OH
John P. Vella, MDMaine Medical CenterPortland, ME
Alexander C. Wiseman, MDUniversity of Colorado at DenverDenver, CO
FOUNDING EDITORSRichard J. Glassock, MDEditor-in-Chief Emeritus
Robert G. Narins, MD
PrefaceNephSAP� is one of the premiere educational activities of the American Society ofNephrology (ASN). Its primary goals are self-assessment, education, and the provision ofContinuingMedical Education (CME) credits andMaintenance of Certification (MOC) pointsfor individuals certified by the American Board of Internal Medicine. Members of the ASNreceive NephSAP electronically through the ASN website by clicking on the NephSAP linkunder “Education and Meetings” tab.
EDUCATION: Medical and nephrologic information continually accrues at a rapid pace.Bombarded from all sides with demands on their time, busy practitioners, academicians, andtrainees at all levels are increasingly challenged to review and understand new and evolvingevidence. Each bimonthly issue of NephSAP is dedicated to a specific theme, i.e., to a specificarea of clinical nephrology, hypertension, dialysis, and transplantation, and consists of aneditorial, a syllabus, self-assessment questions, and core nephrology questions to serve asa self-study device. Over the course of 24 months, all clinically relevant and key elements ofnephrology will be reviewed and updated. The authors of each issue digest, assimilate, andinterpret key studies published since the release of the previous issues and integrate this newmaterial with the body of existing information. Occasionally a special edition is produced tocover an area not ordinarily addressed by core issues of NephSAP.
SELF-ASSESSMENT:Thirty, single-best-answer questionswill follow the 80 to 100 pages ofsyllabus text. The examination is available online with immediate feedback. Those answering75% correctly will receive MOC and CME credit, and receive the answers to all the questionsalong with brief discussions and an updated bibliography. Members will find a new areareviewed every 2 months, and they will be able to test their understanding with our quiz. Thisformat will help readers stay up to date in developing areas of clinical nephrology,hypertension, dialysis, and transplantation, and the review and update will support thosetaking certification and recertification examinations.
CONTINUINGMEDICALEDUCATION:Most state and local medical agencies as well ashospitals are demanding documentation of requisite CME credits for licensure and for staffappointments. A maximum of 48 credits annually can be obtained by successfully completingthe NephSAP examinations. In addition, individuals enrolled in Maintenance of Certification(MOC) through the American Board of Internal Medicine may obtain points towardMOC bysuccessfully completing the self-assessment examination of NephSAP.
CONTRIBUTING AUTHORSC. Blake Cameron, MDShafic El Hindi, MDGentzon Hall, MD, PhDRasheeda K. Hall, MDShashi K. Nagaraj, MDDavid I. Ortiz-Melo, MDJohn K. Roberts, MDStephen R. Smith, MDJohn W. Stanifer, MDSamantha M. Suthar, MDScott G. Westphal, MDDuke University Medical CenterDurham, NC
Andrew F. Malone, MBChBWashington UniversitySt. Louis, MO
James E. Novak, MD, PhDHenry Ford HospitalDetroit, MI
Paul J. Phelan, MBChBRoyal Infirmary of EdinburghScotland
N This paper meets the requirements of ANSI/NISO Z39.48-1921 (Permanence of Paper),effective with July 2002, Vol. 1, No. 1.
NephSAP�
�2014 by The American Society of Nephrology
Editorial311 The State of Peritoneal Dialysis in the United States:
From Inertia to ResurgenceSuzanne Watnick, MD
Syllabus316 NephSAP, Volume 13, Number 5, November 2014—
ESRD and DialysisJohn P. Middleton, MD, Ruediger W. Lehrich, MD
316 Learning Objectives
316 ESRD: Epidemiology and Societal Aspects
316 Trends in Incidence, Prevalence, PatientCharacteristics, Therapy Modality, Mortality,and Morbidity in the US ESRD Population
316 Incidence and Prevalence
317 Patient Characteristics
318 Mortality and Morbidity
318 Therapy Modality
318 Trends in Incidence, Prevalence, Dialysis Modality,and Survival of ESRD Internationally
318 Epidemiology
319 Renal Replacement Modalities
320 Outcomes Worldwide
321 Effect of a Fixed or Bundled Payment Plan onPractice Patterns
321 Anemia Management
322 Bone Metabolism
322 Modality Selection
323 Disparity in ESRD Care
325 Patient Transitions of Care in ESRD
325 Transition from CKD to ESRD Care
327 Conservative Management of ESRD
327 Transition from Pediatric Care to Adult Health CareSystems
328 Transition to End-of-Life Care in ESRD
329 Transition from Failed Renal Allograft to Dialysis
329 Timing of Initiation of Dialysis in the Patient witha Failed Kidney Transplant
330 Whether to Resect the Failed Allograft
331 Immunosuppression Management after Failure ofa Kidney Transplant
331 Geriatric Considerations in ESRD
333 Health-Related QOL
335 In-Center Hemodialysis
335 Determinants of Dialysis Dose, Duration, and Schedule
336 Ascertainment of Dialysis Clearance
336 Frequency of HD Treatments
336 Duration of Hemodialysis Treatments
337 Ultrafiltration and Rate of Fluid Removal
337 Anemia Management
337 Erythropoietin
338 Response and Resistance to Erythropoietin
339 Supplementation of Iron
339 Determination of Target Weight: Bioimpedance andOther Methods
340 Bioimpedance
340 Blood Volume Monitoring
341 Caseload, Physician–Patient Contact, and FacilitySize
343 Hemodialysis Membrane, Constituents of Dialysate,and Clinical Outcomes
343 Evidence for Assignment of Dialysate CalciumConcentration
343 Associations with Dialysate SodiumConcentration
344 Dialysate Bicarbonate and Systemic Acidosis
344 Reuse of Dialyzers and Membrane Permeability
345 Physical Activity in Hemodialysis Patients
348 Home-Suitable Dialysis
348 Choice of Dialysis Modality
349 Clinical Outcomes: Survival, Cardiovascular Events,Hospitalization, and Modality Comparison
349 Comparative Outcomes by Dialysis Modality
349 Modifiable Variables and Outcomes Associatedwith PD
Volume 13, Number 5, November 2014
351 New Approaches to Delivery and Initiation of PD
351 Acute or Unplanned Initiation of PD
352 PD in AKI
352 Psychosocial and Economic Factors AffectingChoice of PD as Modality in ESRD
353 Risk Factors for Necessitating Transition Awayfrom PD
353 Infectious Complications of PD
353 Risk Factors for Peritonitis
354 Outcomes in Peritonitis
354 Treatment of PD-Related Peritonitis
355 Predictors for Relapsing and Recurrent Peritonitis
355 Dialysis Solutions in PD
356 Residual Renal Function
356 Metabolic Indices
356 Peritoneal Transport Properties
356 Peritonitis Rate
358 Patient and Technique Survival
358 Management of PD
358 Testing of Peritoneal Membrane Function
359 PD Access
359 Peritoneal Membrane Pathology
359 Experimental Approach to Peritoneal Fibrosis
360 Encapsulating Peritoneal Sclerosis
360 Diagnosis of EPS
360 Treatment and Outcomes of EPS
361 Home Hemodialysis
361 Vascular Access Issues with HHD/FrequentHD
362 Economics of HHD
365 Management Quandaries in ESRD
365 Uremic Toxins, Biomarkers, and Dialysis
365 Natriuretic Peptides as Biomarkers in ESRD
365 Troponin T as a Biomarker in ESRD
365 Fibroblast Growth Factor-23 as a Biomarker
366 Residual Native Kidney Function and ClinicalOutcome
366 Additional Potential Biomarkers
367 Oxidative Stress and Systemic Inflammation
367 Perceived Quality of Life, Sleep Disorders, RestlessLeg Syndrome, Neuropsychiatric Disorders, andPruritus in Dialysis Patients
367 Sleep Disorders in ESRD
367 Restless Leg Syndrome
368 Mental Health and Depression
368 Cognitive Function in Dialysis
368 Pruritus
368 Pregnancy in ESRD
369 Systemic BP in ESRD and Dialysis
369 BP Variability and Mortality
370 Intradialytic Hypertension
371 Management Considerations
371 Delivered Dialysis Times and BP
371 Nutrition and Obesity in ESRD
371 Body Composition in ESRD
373 Mineral Metabolism, Fractures, and Falls in ESRDPatients
373 Management of Secondary Hyperparathyroidism
374 Hyperphosphatemia
374 Falls and Fractures in ESRD Patients
375 Calcific Uremic Arteriolopathy
375 Stroke, Atrial Fibrillation, and Anticoagulation inESRD
376 Sudden Cardiac Death
377 Definition and Ascertainment of SCD
378 Predictors of Risk for SCD
378 Potential Interventions to Limit Complications ofSCA
379 Cardiovascular Outcomes in ESRD Other than SCD
379 Effect of CKD and Hemodialysis on LeftVentricular Dysfunction
Volume 13, Number 5, November 2014
379 Management of Mineral and Bone Disease andCardiovascular Outcomes
380 Cardiovascular Disease Management andOutcomes
380 Other Interventions and Cardiovascular Outcomes
381 Management of Dyslipidemia in ESRD
381 Vaccination, Hepatitis C, and InfectiousComplications Unique to Dialysis
383 Vaccinations
383 Tuberculosis Monitoring
383 Bacteremia
384 The Microbiome
385 Hepatitis C
389 Advances in Dialysis Methodology
389 High-Efficiency Hemodiafiltration VersusConventional Low- or High-Flux Hemodialysis
391 Frequent HD
391 The FHN Trials
392 Morbidity, Mortality, and Survival
393 Frequent HD, Cardiac Morphology, and CardiacFunction
393 Mineral Metabolism in Frequent HD
393 Nutrition and Body Composition in Frequent HD
394 Vascular Access in Frequent HD
394 Quality of Life in Frequent HD
394 Costs in Frequent HD
394 Wearable Dialysis and Implantable Artificial KidneyDevices
395 Unique Patient Population: Dialysis in AdvancedCongestive Heart Failure
CME Self-Assessment Questions398 NephSAP, Volume 13, Number 5, November 2014—
ESRD and Dialysis
Upcoming IssuesFluid, Electrolyte, and Acid-Base DisturbancesAsghar Rastegar, MD and Manoocher Soleimani, MD
March 2015
Acute Kidney InjuryPatrick T. Murray, MD and Charuhas V. Thakar, MDMay 2015
Cystic Diseases of the KidneyArlene B. Chapman, MD, Michel Chonchol, MD, John F. O’Toole,
MD, Frederic F. Rahbari-Oskou, MD, and Dana Victor Rizk, MD
July 2015
Chronic Kidney Disease and ProgressionLinda F. Fried, MD and Michael J. Choi, MD
September 2015
TransplantationJohn P. Vella, MD and Alexander C. Wiseman, MD
November 2015
HypertensionAldo J. Peixoto, MD and Debbie L. Cohen, MD
Volume 13, Number 5, November 2014
The Editorial Board of NephSAP extends its sincere appreciation to the following reviewers. Their efforts and insights have helped to improvethe quality of this postgraduate education offering.
NephSAP Review PanelAlok Agrawal, MD, FASNWright State UniversityDayton, OH
Mustafa Ahmad, MD, FASNKing Fahad Medical CityRiyadh, Saudi Arabia
Kamal E. Ahmed, MD, FASNYuma NephrologyYuma, AZ
Sadiq Ahmed, MDUniversity of KentuckyLexington, KY
Nasimul Ahsan, MD, FASNNorth Florida/South GeorgiaVA Health SystemGainesville, FL
Jafar Al-Said, MD, FASNBahrain Specialist HospitalManama, Bahrain
Naheed Ansari, MD, FASNJacobi Medical Center/Albert EinsteinCollege of MedicineBronx, NY
Gopal Basu, MDChristian Medical CollegeVellore, Tamil Nadu, India
Mona B. Brake, MD, FASNRobert J. Dole VA Medical CenterWichita, KS
Ruth C. Campbell, MDMedical University of South CarolinaCharleston, SC
Chokchai Chareandee, MD, FASNUniversity of MinnesotaMinneapolis, MN
Dalila B. Corry, MD, FASNUCLA School of MedicineNorthridge, CA
Bulent Cuhaci, MD, FASNAmerican HastanesiIstanbul, Turkey
Kevin A. Curran, MDFresenius Medical Care & US RenalCare Dialysis FacilitiesCanton, TX
Rajiv Dhamija, MDRancho Los Amigos NationalRehabilitation CenterDowney, CA
Christopher A. Dyer, MDUniversity of Texas Health ScienceCenter at San AntonioSan Antonio, TX
Mahmoud El-Khatib, MDUniversity of CincinnatiCincinnati, OH
Lynda A. Frassetto, MD, FASNUniversity of California atSan FranciscoSan Francisco, CA
Claude Mabry Galphin, MDNephrology AssociatesChattanooga, TN
Mohammad Reza Ganji, MDTehran UniversityTehran, Iran
Duvuru Geetha, MD, FASNJohns Hopkins UniversityBaltimore, MD
Carl S. Goldstein, MD, FASNRobert Wood JohnsonMedical SchoolNew Brunswick, NJ
Steven M. Gorbatkin, MD, PhDEmory University,Atlanta, GA
Ashik Hayat, MD, FASNTaranaki Base HospitalNewplymouth, Taranaki, NZ
Ekambaram Ilamathi, MD, FASNState University of New YorkStony Brook, NY
Talha Hassan Imam, MDKaiser PermanenteFontana, CA
Pradeep V. Kadambi, MDUniversity of ArizonaTucson, AZ
Sharon L. Karp, MDIndiana UniversityIndianapolis, IN
Amir Kazory, MD, FASNUniversity of FloridaGainesville, FL
Apurv Khanna, MDSUNY Upstate Medical UniversitySyracuse, NY
Istvan Kiss, MD, PhDSemmelweis UniversityBudapest, Hungary
Nitin V. Kolhe, MD, FASNRoyal Derby HospitalDerby, Derbyshire, UK
Rahul Koushik, MDUniversity of TexasHealth Science CenterSan Antonio, TX
Lalathaksha Murthy Kumbar, MBBSHenry Ford HospitalDetroit, MI
Nicolae Leca, MDUniversity of WashingtonSeattle, WA
Paolo Lentini, MD, PhDSan Bassiano HospitalBassano del Grappa, Italy
Edgar V. Lerma, MD, FASNUniversity of Illinois at ChicagoCollege of MedicineChicago, IL
Orfeas Liangos, MD, FASNKlinikum CoburgCoburg, Bayern, Germany
Meyer Lifschitz, MDShaare Zedek Medical CenterJerusalem, Israel
Jolanta Malyszko, MD, PhDMedical UniversityBialystok, Poland
Christopher Mariat, MD, PhDUniversity Jean MonnetSaint-Etienne, France
Naveed Masani, MDWinthrop University HospitalMineola, NY
Hanna W. Mawad, MD, FASNUniversity of KentuckyLexington, KY
Kevin McConnell, MDJefferson Nephrology, LtdCharlottesville, VA
Pascal Meier, MD, FASNCentre Hospitalier du Valais RomandSion, Switzerland
Ashraf Mikhail, MBBChMorriston HospitalSwansea, Wales, UK
Volume 13, Number 5, November 2014
Tanuja Mishra, MDKaiser PermanenteMid-Atlantic RegionEllicott City, MD
Lawrence S. Moffatt, Jr., MDCarolinas Medical CenterCharlotte, NC
Sumit Mohan, MDColumbia University College ofPhysicians and SurgeonsNew York, NY
Shahriar Moossavi, MD, PhD, FASNWake Forest School of MedicineWinston-Salem, NC
Koosha Mortazavi, MDVista Del Mar Medical GroupOxnard, CA
Tariq Mubin, MDKern Nephrology Medical GroupBakersfield, CA
Narayana S. Murali, MDMarshfield ClinicMarshfield, WI
Thangamani Muthukumar, MDCornell UniversityNew York, NY
Mohanram Narayanan, MD, FASNScott and White HealthcareTemple, TX
Macaulay A. Onuigbo, MD, FASNMayo ClinicRochester, MN
Kevin P. O'Reilly, MDOhio State UniversityColumbus, OH
Carlos E. Palant, MDWashington DC VA Medical CenterWashington, DC
Malvinder Parmar, MB, MS, FASNNorthern Ontario School of MedicineTimmins, ON, Canada
Pairach Pintavorn, MD, FASNEast Georgia Kidney and HypertensionAugusta, GA
James M. Pritsiolas, MD, FASNCarePoint Health Medical GroupBayonne and Chatham, NJ
Paul H. Pronovost, MD, FASNYale University School of MedicineWaterbury, CT
Mohammad A. Quasem, MDUniversal Health Services HospitalsBinghamton, NY
Wajeh Y. Qunibi, MDUniversity of TexasHealth Science CenterSan Antonio, TX
Pawan K. Rao, MD, FASNSt. Joseph HospitalSyracuse, NY
Bharathi V. Reddy, MDUniversity of ChicagoMedical CenterChicago, IL
Joel C. Reynolds, MD, FASNInternal Medicine ClinicMeridian, MS
Brian S. Rifkin, MDHattiesburg ClinicHattiesburg, MS
Helbert Rondon-Berrios, MD, FASNUniversity of PittsburghSchool of MedicinePittsburgh, PA
Bijan Roshan, MD, FASNKidney Associates of ColoradoDenver, CO
Mario F. Rubin, MD, FASNUniversity of ArizonaTucson, AZ
Ehab R. Saad, MD, FASNMedical College of WisconsinMilwaukee, WI
Bharat Sachdeva, MBBSLouisiana State UniversityHealth Sciences CenterShreveport, LA
Mark C. Saddler, MBChBDurango Nephrology AssociatesDurango, CO
Mohammad G. Saklayen, MBBSWright State UniversityBoonshoft School of MedicineDayton, OH
Muwaffaq Salameh, MBBSSt. Martha Regional HospitalAntigonish, NS, Canada
Mohammad N. Saqib, MDLehigh Valley HospitalOrefield, PA
Henry L. Schairer, Jr., MD, FASNLehigh Valley Health NetworkAllentown, PA
Gaurang M. Shah, MD, FASNLong Beach VA Healthcare SystemLong Beach, CA
Nita K. Shah, MDSt. Barnabas Health CenterLivingston, NJ
Arif Showkat, MD, FASNUniversity of TennesseeMemphis, TN
Sandeep S. Soman, MDHenry Ford HospitalDetroit, MI
Manish M. Sood, MD, FASNUniversity of ManitobaWinnipeg, MB, Canada
Susan P. Steigerwalt, MDSt. John Providence HospitalDetroit, MI
Ignatius Yun-Sang Tang, MDUniversity of Illinois Hospital andHealth Sciences SystemChicago, IL
Ahmad R. Tarakji, MD, FASNCollege of Medicine, King Saud UniversityRiyadh, Saudi Arabia
Hung-Bin Tsai, MDNational Taiwan UniversityHospitalTaipei, Taiwan
Anthony M. Valeri, MDColumbia UniversityNew York, NY
Allen W. Vander, MD, FASNKidney Center of SouthLouisianaThibodaux, LA
Juan Carlos Q. Velez, MDMedical University of SouthCarolinaCharleston, SC
Anitha Vijayan, MD, FASNWashington Universityin St. LouisSt. Louis, MO
Shefali Vyas, MDSt. Barnabas Health CenterLivingston, NJ
Nand K. Wadhwa, MDStony Brook UniversityStony Brook, NY
Sameer Yaseen, MDNephrology PCDes Moines, IA
Mario Javier Zarama, MDKidney Specialists ofMinnesota, PASaint Paul, MN
Program Mission and ObjectivesThe Nephrology Self-Assessment Program (NephSAP) provides a learning vehicle for clinical nephrologists to renew andrefresh their clinical knowledge, diagnostic, and therapeutic skills. This enduring material provides nephrologists challenging,clinically oriented questions based on case vignettes, a detailed syllabus that reviews recent publications, and an editorial on animportant and evolving topic. This combination of materials enables clinicians to rigorously assess their strengths andweaknesses in the broad domain of nephrology.
Accreditation StatementThe American Society of Nephrology (ASN) is accredited by the Accreditation Council for Continuing Medical Education toprovide continuing medical education for physicians.
AMA Credit Designation StatementThe ASN designates this enduring material for a maximum of 8.0 AMA PRA Category 1 Credits™. Physicians should claimonly the credit commensurate with the extent of their participation in the activity.
American Academy of Physician Assistants Accreditation Statement (AAPA)This Self-Assessment CME program has been reviewed and is approved for a maximum of 8.0AAPA Category 1 Self-Assessment CME credits by the Physician Assistant Review Panel. Approvalis valid until 10/31/2016. Physician Assistants should claim only the credit commensurate with theirextent of their participation in the activity. This program was planned in accordance withAAPA’s CME Standards.
Original Release Date
November 2014
CME Credit Termination Date
October 31, 2016
Examination Available Online
On or before Monday, November 17, 2014
Estimated Time for Completion
8 hours
Answers with Explanations
• Provided with a passing score after the first and/or after the second attempt
• December 2016: posted on the ASN website when the issue is archived.
Target Audience
• Nephrology certification and recertification candidates
• Practicing nephrologists
• Internists
• Other health professionals
Volume 13, Number 5, November 2014
Method of Participation
• Read the syllabus that is supplemented by original articles in the reference lists.
• Complete the online self-assessment examination.
• Each participant is allowed two attempts to pass the examination (.75% correct) for CME credit.
• Upon completion, review your score and incorrect answers and print your certificate.
• Answers and explanations are provided with a passing score or after the second attempt.
Activity Evaluation and CME Credit Instructions
• Go to www.asn-online.org/cme, and enter your ASN login on the right.
• Click the ASN CME Center.
• Locate the activity name and click the corresponding ENTER ACTIVITY button.
• Read all front matter information.
• On the left-hand side, click and complete the Demographics & General Evaluations.
• Complete and pass the examination for CME credit.
• Upon completion, click Claim Your Credits, check the Attestation Statement box, and enter the number of CMEcredits commensurate with the extent of your participation in the activity.
• If you need a certificate, Print Your Certificate on the left.
For your complete ASN transcript, click the ASN CME Center banner, and click View/Print Transcript on the left.
Instructions to obtain American Board of Internal Medicine (ABIM) Maintenance of Certification(MOC) PointsEach issue of NephSAP provides 10 MOC points. Respondents must meet the following criteria:
• Be certified by ABIM in internal medicine and/or nephrology and enrolled in the ABIM–MOC program
• Enroll for MOC via the ABIM website (www.abim.org).• Enter your (ABIM) Candidate Number and Date of Birth prior to completing the examination.
• Take the self-assessment examination within the timeframe specified in this issue of NephSAP.
• Below your score select “Click here to post to ABIM.”
MOC points will be applied to only those ABIM candidates who have enrolled in the MOC program. It is your responsibility tocomplete the ABIM MOC enrollment process.
System RequirementsCompatible Browser and SoftwareThe ASN website (asn-online.org) has been formatted for cross-browser functionality, and should display correctly in allmodern web browsers. To view the interactive version of NephSAP, your browser must have Adobe Flash Player installed orhave HTML5 capabilities. NephSAP is also available in Portable Document Format (PDF), which requires Adobe Reader orcomparable PDF viewing software.
Monitor Settings
The ASN website was designed to be viewed in a 1024 · 768 or higher resolution.
Medium or Combination of Media Used
The media used include an electronic syllabus and online evaluation and examination.
Technical Support
If you have difficulty viewing any of the pages, please refer to the ASN technical support page for possible solutions. If youcontinue having problems, contact ASN at [email protected].
Volume 13, Number 5, November 2014

Disclosure InformationThe ASN is responsible for identifying and resolving all conflicts of interest prior to presenting any educational activity to learners to ensure thatASN CME activities promote quality and safety, are effective in improving medical practice, are based on valid content, and are independent of thecontrol from commercial interests and free of bias. All faculty are instructed to provide balanced, scientifically rigorous and evidence-basedpresentations. In accordance with the disclosure policies of the Accreditation Council for Continuing Medical Education (ACCME), individuals who arein a position to control the content of an educational activity are required to disclose relationships with a commercial interest if (a) the relation is financialand occurred within the past 12 months; and (b) the individual had the opportunity to affect the content of continuing medical education with regard to thatcommercial interest. For this purpose,ASNconsider the relationships of the person involved in theCMEactivity to includefinancial relationships of a spouseor partner. Peer reviewers are asked to abstain from reviewing topics if they have a conflict of interest. Disclosure information is made available to learnersprior to the start of any ASN educational activity.
EDITORIAL BOARDMichael J. Choi, MD—Current Employer: Johns Hopkins University School of Medicine; Consultancy: GlaxoSmithKline; Editorial Board:
CJASN, Clinical Nephrology, National Kidney Foundation, Board of DirectorsLinda F. Fried, MD, FASN—Current Employer: VA Pittsburgh Healthcare System; Research Funding: Merck (drug donation to Veterans Affairs for
study); Scientific Advisor/Membership: National Kidney Foundation-Steering Committee Kidney Early Evaluation Program (KEEP)Richard J. Glassock, MD—Current Employer: David Geffen School of Medicine at UCLA, Professor Emeritus; Consultancy: Bristol-Myers Squibb,
Novartis, Genentech, Eli Lilly, Sanofi-Genzyme, QuestCor, Astellas, Abbvie, ChemoCentryx, Bio-Marin, Aspreva (Vifor), NIH, UpToDate,American Journal of Nephrology; Ownership Interest: La Jolla Pharm, Reata; Honoraria: Eli Lilly, Bristol-Myers Squibb, QuestCor,ChemoCentryx, Genentech, Novartis, Astellas, Aspreva (Vifor), Sanofi-Genzyme; Scientific Advisor/Membership: Los Angeles Bio MedicalInstitute, University Kidney Research Organization, JASN, American Journal of Nephrology, UpToDate
Stanley Goldfarb, MD, FASN—Current Employer: University of Pennsylvania School of Medicine; Consultancy: Genentech, Ardea Bioscience;Honoraria: Ardea Bioscience, Genentech; Scientific Advisor/Membership: Clinical Nephrology (Editorial Board), Genetech
Gerald A. Hladik, MD—Current Employer: University of North Carolina at Chapel Hill; Honoraria: American College of Physicians through Pri-Med; Scientific Advisor/Membership: Education Director for Maintenance of Certification, American Society of Nephrology
Ruediger W. Lehrich, MD—Current Employer: Duke University Medical CenterKevin J. Martin, MBBCh, FASN—Current Employer: Saint Louis University School of Medicine; Consultancy: Abbvie, Diasorin, Keryx, OPKO,
Amgen; Honoraria: Diasorin, Keryx, Amgen, Abbvie, OPKO; Scientific Advisor/Membership: OPKO, Clinical Nephrology (Editorial Board),Keryx, Diasorin
John P. Middleton, MD—Current Employer: Duke University Medical Center; Research Funding: Eli Lilly, Otsuka, Questcor, Keryx, Bristol-MyersSquibb; Honoraria: NKF; Scientific Advisor/Membership: Editorial Board: Journal of Human Hypertension, Advances in Chronic KidneyDisease, Steering Committee NIDDK CKD Consortium
Patrick T. Murray, MD, FASN—Current Employer: University College of Dublin School of Medicine and Medical Science; Consultancy: Abbott,Argutus, FAST Diagnostics, Mitsubishi Pharmaceuticals, Sanofi, AM-Pharma, GlaxoSmithKline; Ownership Interest: Merck; ResearchFunding: Abbott, Alere, Argutus, FAST Diagnostic Health Research Board (Ireland), Dublin Centre for Clinical Research, Innovative MedicinesInitiative/SAFE-T Consortium; Honoraria: Abbott, Alere, Argutus, FAST Diagnostic, Mitsubishi, A Menarini, Sanofi; Scientific Advisor/Membership: CJASN, Irish Medicines Board, Abbott, Alere, Argutus, FAST Diagnostics, AM-Pharma
Patrick H. Nachman, MD, FASN—Current Employer: University of North Carolina; Research Funding: Alexion (past); Honoraria: HealthAdvances LLC; Scientific Advisor/Membership: ChemoCentryx (unpaid)
Aldo J. Peixoto, MD, FASN—Current Employer: Yale University School of Medicine; Consultancy: St. Jude Medical; Honoraria: American Societyof Hypertension, Society of Critical Care Medicine, St. Jude Medical; Associate Editor: Blood Pressure Monitoring; Editorial Board: CJASN,American Journal of Nephrology, Brazilian Journal of Nephrology, Faculty of 1000 Prime; Society Committees: American Society ofHypertension (CME Committee); Board of Directors: Eastern Chapter of the American Society of Hypertension
Asghar Rastegar, MD—Current Employer: Yale University School of MedicineManoocher Soleimani, MD—Current Employer: University of Cincinnati Department of MedicineCharuhas V. Thakar, MD—Current Employer: University of Cincinnati/Department of Veterans Affairs; Consultancy: ChemoCentryx Cytopherx,
Abbvie, Novartis, LEK Consulting; Research Funding: Hospira, Abbvie, Elcelyx; Other Interests/Relationship: Co-editor, Textbook withSpringer
John P. Vella, MD, FASN—Current Employer: Maine Nephrology Associates, PA; Research Funding: Bristol-Myers Squibb; Scientific Advisor/Membership: UpToDate
Alexander C. Wiseman, MD—Current Employer: University of Colorado at Denver and Health Sciences Center; Consultancy: MKSAP, Astellas,Tolera, Veloxis; Research Funding: Novartis, Alexion, Bristol-Myers Squibb; Honoraria: American Society of Transplantation, Novartis;Scientific Advisor/Membership: American Journal of Transplantation, CJASN
Jerry Yee, MD, FASN—Current Employer: Henry Ford Hospital; Consultancy: Amgen, Vasc-Alert, Alexion, ZS Pharma; Honoraria: Amgen,Alexion, Gerson, Drexel University, University of California at San Diego, ZS Pharma; Patents/Inventions: Vasc-Alert; Scientific Advisor/Membership: NKF: Editor-In-Chief of Advances in CKD (journal); Editorial Board: CJASN, American Journal of Nephrology, DeputyEditor, NephSAP
Volume 13, Number 5, November 2014
CONTRIBUTING AUTHORS:C. Blake Cameron, MD–Current Employer: Duke University Medical Center
Shafic El Hindi, MD–Current Employer: Duke University Medical Center
Gentzon Hall, MD, PhD–Current Employer: Duke University Medical Center
Rasheeda K. Hall, MD–Current Employer: Duke University Medical Center
Andrew F. Malone, MBChB–Current Employer: Washington University at St. Louis
Shashi K. Nagaraj, MD–Current Employer: Duke University Medical Center; Honoraria: Alexion travel grant
James E. Novak, MD,PhD–Current Employer: Henry Ford Health System; Research Funding; Amgen, Eli Lilly; Scientific Advisor/Membership:Advances in Chronic Kidney Disease
David I. Ortiz-Melo, MD–Current Employer: Duke University Medical Center
Paul J. Phelan, MBChB–Current Employer: Royal Infirmary of Edinburgh, Scotland
John K. Roberts, MD–Current Employer: Duke University Medical Center
Stephen R. Smith, MD–Current Employer: Duke University Medical Center; Consultancy: Humacyte, Inc.
John W. Stanifer, MD–Current Employer: Duke University Medical Center
Samantha M. Suthar, MD–Current Employer: Duke University Medical Center
Scott G. Westphal, MD–Current Employer: Duke University Medical Center
EDITORIAL AUTHORS:Suzanne Watnick, MD–Current Employer: Oregon Health and Science University, Portland Veterans Affairs Medical center; Honoraria: ABIM,ASN; Scientific Advisor or Membership: Northwest Renal Network Board of Directors, CJASN Editorial Board, AJKD Editorial Board, ASN DialysisAdvisory Group, ASN Public Policy Board, VA Renal Field Advisory Committee
ASN STAFF:Gisela A. Deuter, BSN, MSA—Nothing to disclose
Commercial SupportThere is no commercial support for this issue.
Volume 13, Number 5, November 2014


EditorialThe State of Peritoneal Dialysis in the United States: From Inertia toResurgence
Suzanne Watnick, MDOregon Health and Science University, Portland Veterans Affairs Medical Center, Portland,Oregon
Between January 2010 and October 2012, monthlyMedicare prevalent counts of patients on peritonealdialysis (PD) increased by 24.0%, whereas prevalentcounts of patients on hemodialysis (HD) increased by 9.6%(1). This remarkable difference seems even more pro-nounced compared with a similar period between 2007and 2009. Prevalent counts for PD remained essentiallyflat, whereas counts for HD patients increased by .8%(2,3). The current acceleration of growth in PD isstriking, particularly in light of the stagnation and declinein PD growth over the period from 1995 to 2005, de-scribed as “inertia in context” (4).
Understanding the forces behind these changesis crucial to establish appropriate policies and care envi-ronments for PD patients in the future. In this editorial,we aim to (1) describe prior United States legislativeand policy incentives that increased PD utilization, (2)summarize current changes in PD use and ongoing im-provement with prior barriers and (3) discuss the futureevolution of care models that may affect PD use as wemove forward.
Prior Legislative and Policy Incentives for PD UseIn this country, PD has been an underutilized
modality. PD advocates report that nearly half of theirpatients are eligible for PD, and providers in the UnitedStates believe that PD use should approach 30%–40%.In 2006, incident rates were 6.2% (5). There is widevariability in Canada regarding the prevalence of PD,which approaches 15% overall and up to 27% in someprovinces—far higher rates than in the United States (6).InMexico and Hong Kong, where “PD first” policies arein effect, .80% of patients are on PD (7,8).
PD is not suitable for all patients with ESRD, but PDdoes offer potential advantages to patients, providers andpayers. As a modality, PD provides greater independence
and greater patient satisfaction (9,10). Studies vary, butmany show that United States patient outcomes duringthe first 4–5 years of PD are no worse than HD (11,12).For providers, PD requires less overhead for equipmentand staffing. For payers, the modality is less costly. In2009, the per-patient payments were $61,588 for PD and$82,285 for HD for the US Centers for Medicare andMedicaid services (CMS) (the payer for .80% of UnitedStates patients) (3).
Given this information, a major question arises:“Why hasn’t PD been more popular?” CMS is and hasbeen the major payer to ESRD care providers, and it isunsurprising that CMS might drive policy changes. In1972, under President Nixon, ESRD became the onlydisease-specific entitlement covered byMedicare. At thattime, home dialysis rates approached 40% (13). In-centerHD units were built to accommodate need, and Medicarerecognized the increased expense of this additional in-frastructure and added incentives for PD, given its in-creased safety, convenience, and decreased cost (14,15).Nonetheless, PD rates continued to decline. Dialysis pro-viders developed more efficient services through in-center HD units that allowed them to decrease costs andgenerate additional profits. This resulted in further growthin the industry (16). In 1983, with an updated model forpayment, consolidation of dialysis patients continued,resulting in marked growth of for-profit HD units. At thispoint, the prevalence of home dialysis (both HD and PD)approached 13.7% (17). In 1985, when the US Renal DataSystem (USRDS) began recording trends in modalityuse, 71% of facilities provided PD services with an in-cident rate of 14%. By 2006, this had dropped to fewerthan half of facilities offering PD with an incidence of6.2% (18).
Because studies have shown that technology ad-vances and patient outcomes for PD patients have
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
311

improved with time (10,11), it was more likely thatnonpatient factors accounted for this change. An analysisof factors contributing to low PD utilization determinedthat lower reimbursement rates, the need to maximize HDchair occupancy, and an affiliation with a chain (largedialysis organization) contributed to lower PD rates dur-ing the period before the prospective payment system(PPS) (4).
The PPS was adopted for multiple reasons. Theprimary stated concern was the “perverse” incentive tooveruse separately billable drugs, yet the governmentalso recognized the incentive to use less expensive dial-ysis modalities. Before the PPS, dialysis payment wascomposed of a composite rate and a separately billablerate. The composite rate covered nursing and other clin-ical services, social services, supplies, equipment, andcertain laboratory tests. The separately billable rate in-cluded certain drugs and laboratory tests that becameroutine after 1983. The injectables included but were notlimited to erythropoiesis-stimulating agents (ESAs), vitaminD and its analogs, iron, vancomycin, alteplase, levocarnitine,and vaccines.
The federal mandate to “bundle” payment for ESRDservices was described in theMedicare Prescription Drug,Improvement, and Modernization Act of 2003, in whichCMS concluded that “this created an incentive to over-use separately billable drugs” (19). The Medicare Im-provements for Patients and Providers Act of 2008legislated to curb expenditures by adopting a single pay-ment to providers for specified dialysis services, whichwould be linked to quality measures (20).
Before the PPS, the clear decrease in incentivesfor PD included a decline in physician familiarity, re-
duced resource allocation and increased comorbiditiesoverall in the ESRD population. Thus, it was more dif-ficult to find adequate resources, providers, and patientsfor PD. Incentives such as CMS coverage for PD patientsat day 1 versus HD at day 90 or similar reimburse-ment for one provider PD visit versus two to three HDvisits were not enough to overcome the inertia of theprior model. When CMS restructured the PPS to pro-vide equivalent overall payment for PD and HD, theattractiveness of the revised model suddenly becameapparent. A recent financial analysis of facility costs forPD and HD patients clearly demonstrated this point.This administrative analysis was modeled for a facilitywith 80 in-center HD patients and 16 PD patients. Be-fore the bundled system, the increased monthly marginto add a HD patient was $76; however, it was a $185loss to add a PD patient. In the new payment system,$86 were gained per HD patient and $201 were gainedper PD patient (21).
A quality incentive program (QIP) was mandatedalongside the PPS to ensure that bundled care did notresult in poorer quality care. Although many of the mea-sures did not apply to the PD patient, this program didnot appear to provide incentives or disincentives to in-crease PD rates.
Current Data Regarding PD in the United StatesPopulation
The goal of the PPS was to decrease overall useof injectable drugs, most specifically ESAs. WeeklyESA use declined by .30% and average hemoglobinvalues declined from 11.3 to 10.6 g/dl from 2011 through2013. The resurgence in PD growth was equally remark-able. The 2013 USRDS Annual Data Report (ADR) re-vealed that PD had grown 22%, primarily in the last3 years, and the growth rate is still increasing. HD prev-alence grew 20%, but the incident rate declined slightlyfor the first time in 3 decades, and overall growth ratesare declining. In this data report, the USRDS researcherswrote, “This change is associated with the new CMSbundled payment system, with its clear incentives forperitoneal dialysis” (22) (Figure 1).
As impressive as this change seemed, these datawere compiled from 2011, the first year of the PPS. Self-reported data from 2014 from large and small dialysisorganizations revealed a continuation of this trend. Thefour largest dialysis organizations reported 35,132 of366,855 patients on PD, which represents 9.6% of the
Table 1. Peritoneal dialysis percent growth by patients:Survey of United States dialysis providers
Dialysis Provider
Percent Growth Rate
May 2012versus
May 2013
May 2013versus
May 2014
Fresenius Medical Care 4.0 4.5DaVita 8.6 5.7Dialysis Clinic Inc 2.0 3.9Totala 6.2 6.0Data are from Neumann ME: 19th annual ranking: moderate growth for providers,but rebasing, ACO participation will impact long-term picture. Nephrol News Issues27: 16–18, 2013; and Neumann ME: 20th annual ranking: a look back, and gettingpositioned for the future. Nephrol News Issues 26: 30–31, 2014.aLargest 10 United States dialysis providers in 2014.
312 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
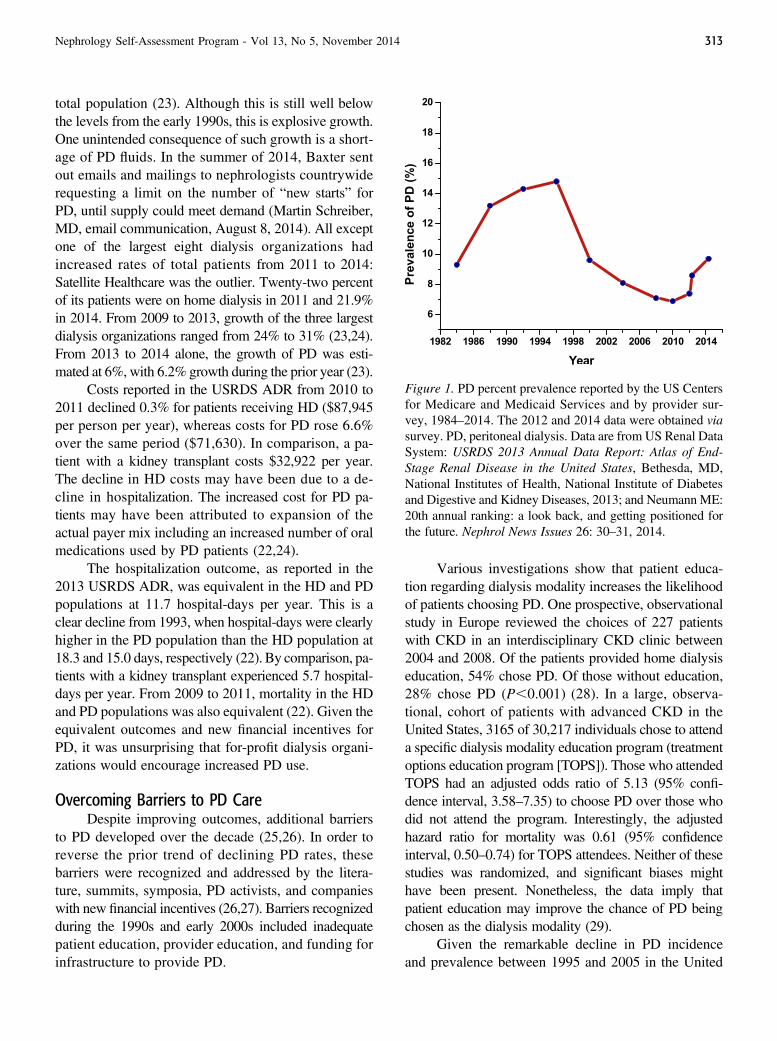
total population (23). Although this is still well belowthe levels from the early 1990s, this is explosive growth.One unintended consequence of such growth is a short-age of PD fluids. In the summer of 2014, Baxter sentout emails and mailings to nephrologists countrywiderequesting a limit on the number of “new starts” forPD, until supply could meet demand (Martin Schreiber,MD, email communication, August 8, 2014). All exceptone of the largest eight dialysis organizations hadincreased rates of total patients from 2011 to 2014:Satellite Healthcare was the outlier. Twenty-two percentof its patients were on home dialysis in 2011 and 21.9%in 2014. From 2009 to 2013, growth of the three largestdialysis organizations ranged from 24% to 31% (23,24).From 2013 to 2014 alone, the growth of PD was esti-mated at 6%, with 6.2% growth during the prior year (23).
Costs reported in the USRDS ADR from 2010 to2011 declined 0.3% for patients receiving HD ($87,945per person per year), whereas costs for PD rose 6.6%over the same period ($71,630). In comparison, a pa-tient with a kidney transplant costs $32,922 per year.The decline in HD costs may have been due to a de-cline in hospitalization. The increased cost for PD pa-tients may have been attributed to expansion of theactual payer mix including an increased number of oralmedications used by PD patients (22,24).
The hospitalization outcome, as reported in the2013 USRDS ADR, was equivalent in the HD and PDpopulations at 11.7 hospital-days per year. This is aclear decline from 1993, when hospital-days were clearlyhigher in the PD population than the HD population at18.3 and 15.0 days, respectively (22). By comparison, pa-tients with a kidney transplant experienced 5.7 hospital-days per year. From 2009 to 2011, mortality in the HDand PD populations was also equivalent (22). Given theequivalent outcomes and new financial incentives forPD, it was unsurprising that for-profit dialysis organi-zations would encourage increased PD use.
Overcoming Barriers to PD CareDespite improving outcomes, additional barriers
to PD developed over the decade (25,26). In order toreverse the prior trend of declining PD rates, thesebarriers were recognized and addressed by the litera-ture, summits, symposia, PD activists, and companieswith new financial incentives (26,27). Barriers recognizedduring the 1990s and early 2000s included inadequatepatient education, provider education, and funding forinfrastructure to provide PD.
Various investigations show that patient educa-tion regarding dialysis modality increases the likelihoodof patients choosing PD. One prospective, observationalstudy in Europe reviewed the choices of 227 patientswith CKD in an interdisciplinary CKD clinic between2004 and 2008. Of the patients provided home dialysiseducation, 54% chose PD. Of those without education,28% chose PD (P,0.001) (28). In a large, observa-tional, cohort of patients with advanced CKD in theUnited States, 3165 of 30,217 individuals chose to attenda specific dialysis modality education program (treatmentoptions education program [TOPS]). Those who attendedTOPS had an adjusted odds ratio of 5.13 (95% confi-dence interval, 3.58–7.35) to choose PD over those whodid not attend the program. Interestingly, the adjustedhazard ratio for mortality was 0.61 (95% confidenceinterval, 0.50–0.74) for TOPS attendees. Neither of thesestudies was randomized, and significant biases mighthave been present. Nonetheless, the data imply thatpatient education may improve the chance of PD beingchosen as the dialysis modality (29).
Given the remarkable decline in PD incidenceand prevalence between 1995 and 2005 in the United
Figure 1. PD percent prevalence reported by the US Centersfor Medicare and Medicaid Services and by provider sur-vey, 1984–2014. The 2012 and 2014 data were obtained viasurvey. PD, peritoneal dialysis. Data are from US Renal DataSystem: USRDS 2013 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, Bethesda, MD,National Institutes of Health, National Institute of Diabetesand Digestive and Kidney Diseases, 2013; and Neumann ME:20th annual ranking: a look back, and getting positioned forthe future. Nephrol News Issues 26: 30–31, 2014.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 313

States, trainees and practitioners had less exposure toPD patients. Despite adequate didactic training, traineesreported decreasing clinical experiences with PD. In2002, Mehrotra et al. reported that trainees in Canadawere spending 21% of their time seeing chronic HDpatients and 10% of their clinical time seeing PD pa-tients. Their counterparts in the United States werespending 20% of their time seeing HD patients and,5% of their time seeing PD patients (30). With rec-ognition of this, PD champions initiated several nationalincentives, including new curricula, free online educationfrom experts in the field, and the development of bench-marks available to nephrology training program directorsand trainees. In addition, the PD population continued togrow by.50% in the last 5 years, leading to an expandedpool of clinical experiences for providers.
Infrastructure requirements have become apparentin the last decades, when resources were scarce. Space,time and nursing support are crucial for a successfulPD program (26). Dialysis organizations have recognizedthese critical elements and allowed for expansion of homedialysis programs when financial incentives aligned withthe burgeoning clinical needs (31).
Future Models and Incentives for PDWith the success of many of the incentives outlined
above, PD has become more attractive to patients. Stream-lining PD initiation also improved the capacity for higherincidence of PD starts. For example, advocates of a “PDfirst” policy have been outlining plans for efficient andeffective care models going forward (32). Many advo-cates believe that 30%–40% of patients on PD is an ap-propriate goal. Interestingly, supply must meet demandfor this to be a reasonable goal. As mentioned previously,PD solutions are now in short supply, with projected res-olution in the first quarter of 2015 (Martin Schreiber,MD, email communication, August 8, 2014).
With CMS’ desire to improve quality by improv-ing outcomes and minimizing costs to the dialysis land-scape, other models of care for dialysis patients are onthe horizon. Will our PD patients benefit and will thesemodels encourage or discourage PD?
The Patient Protection and Affordable Care Actwas signed into effect by President Barack Obama onMarch 23, 2010. The aims included reform of aspectsof the private health care industry and public healthinsurance programs. It aimed to increase coveragefor preexisting conditions and to expand access to.30 million Americans. Accountable care organiza-
tions (ACOs) were part of this initiative. ACOs areprovider-led organizations that manage all care and areaccountable for overall costs and quality for the definedpopulation. The quality measurement component isone of many items similar to the ESRD PPS and QIP(which incentivized PD). CMS has considered creat-ing specialty-specific ACOs to improve quality of care incertain high-cost chronic illness areas. These ESRDseamless care organizations would theoretically reduceduplicative services and expenditures, provide patient-centered care, and improve outcomes and overall CMSsavings. However, after two rounds of requests forapplications, there were fewer applications than desired,perhaps due to no predetermined quality metrics ordefinitions of success. A third round will determinewhether the CMS moves forward with this concept. Inthe continued pursuit of obtaining improved quality,PD would be further incentivized by this care modelbecause it has equivalent outcomes with a lower pricetag.
Significant legislative changes have resulted innew incentives for PD in the United States, and PD rateshave substantially increased. In addition, many of theprior barriers to PD care are being actively addressed.Present and future care models may continue to incen-tivize PD implementation. It will be our community’sresponsibility to ensure that we facilitate expansion ofthe PD patient base at an appropriate rate. Unintendedconsequences must not put our patients at risk for worsen-ing outcomes such as decreased survival and quality oflife. Eventually, we will reach a new steady state of pa-tients receiving PD after this current expansion. Moreproviders will be comfortable with PD. Renewed andrecurrent resources for infrastructure must remain in place,and steps must be taken to maintain a newly expandedpatient population accounting for high PD “burnout”and high kidney transplantation rates. In the interim, thefinancial incentives that were a major driver for thechanges must maintain appropriate checks and balancesto ensure that our patients have adequate resources foroptimal dialysis care.
Disclosures
None.
References1. Collins AJ: Monthly Medicare prevalent counts: All HD and all PD,
Slide 9, 2013. Available at: http://www.usrds.org/2013/pres/Collins_USRDS_ADR_overview_2013.pdf. Accessed August 7, 2014
314 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
2. US Renal Data System: USRDS 2009 Annual Data Report: Atlas ofEnd-Stage Renal Disease in the United States, Bethesda, MD, NationalInstitutes of Health, National Institute of Diabetes and Digestive andKidney Diseases, 2009
3. US Renal Data System: USRDS 2011 Annual Data Report: Atlas ofEnd-Stage Renal Disease in the United States, Bethesda, MD, NationalInstitutes of Health, National Institute of Diabetes and Digestive andKidney Diseases, 2011
4. Wang V, Lee SY, Maciejewski ML: Inertia in health care organizations:A case study of peritoneal dialysis services [published online aheadof print April 23, 2014]. Health Care Manage Rev doi:10.1097/HMR.0000000000000039
5. Mendelssohn DC, Mullaney SR, Jung B, Blake PG, Mehta RL:What doAmerican nephologists think about dialysis modality selection? Am JKidney Dis 37: 22–29, 2001 PubMed
6. Jain AK, Blake P, Cordy P, Garg AX: Global trends in rates ofperitoneal dialysis. J Am Soc Nephrol 23: 533–544, 2012 PubMed
7. Pecoits-Filho R, Abensur H, Cueto-Manzano AM, Dominguez J,Divino Filho JC, Fernandez-Cean J, Ortiz AM, Moretta G, Ramos A,Sanabria M, Sesso R, Paniágua R: Overview of peritoneal dialysis inLatin America. Perit Dial Int 27: 316–321, 2007 PubMed
8. Yu AW, Chau KF, Ho YW, Li PK: Development of the “peritonealdialysis first” model in Hong Kong. Perit Dial Int 27[Suppl 2]: S53–S55, 2007 PubMed
9. Ahlmén J, Carlsson L, Schönborg C: Well-informed patients with end-stage renal disease prefer peritoneal dialysis to hemodialysis. Perit DialInt 13[Suppl 2]: S196–S198, 1993 PubMed
10. Stack AG: Determinants of modality selection among incident USdialysis patients: results from a national study. J Am Soc Nephrol 13:1279–1287, 2002 PubMed
11. Mehrotra R, Chiu YW, Kalantar-Zadeh K, Bargman J, Vonesh E: Sim-ilar outcomes with hemodialysis and peritoneal dialysis in patients withend-stage renal disease. Arch Intern Med 171: 110–118, 2011 PubMed
12. Weinhandl ED, Foley RN, Gilbertson DT, Arneson TJ, Snyder JJ, CollinsAJ: Propensity-matched mortality comparison of incident hemodialysisand peritoneal dialysis patients. J AmSocNephrol 21: 499–506, 2010 PubMed
13. Rettig RA: The policy debate on patient care financing for victims of end-stage renal disease. Law Contemp Probl 40: 196–230, 1976 PubMed
14. Greenspan RE: The high price of federally regulated hemodialysis. JAMA246: 1909–1911, 1981 PubMed
15. Relman AS, Rennie D: Treatment of end-stage renal disease: free butnot equal. N Engl J Med 303: 996–998, 1980 PubMed
16. Nissenson AR, Rettig RA: Medicare’s end-stage renal disease program:current status and future prospects. Health Aff (Millwood) 18: 161–179,1999 PubMed
17. Wiegmann TB, Blumenkrantz M, Layard M, Schmidt RW, Shen F,Stead W: Home dialysis and dialysis treatment modalities in the VAsystem. Am J Kidney Dis 3: 32–36, 1983 PubMed
18. US Renal Data System: USRDS 2008 Annual Data Report: Atlas ofEnd-Stage Renal Disease in the United States, Bethesda, MD, NationalInstitutes of Health, National Institute of Diabetes and Digestive andKidney Diseases, 2008
19. US Government: Medicare Prescription Drug, Improvement, and Mod-ernization Act of 2003, Pub L No. 108-173, 2003
20. US Government: Medicare Improvements for Patients and ProvidersAct of 2008, Pub L No. 110-275, 2008
21. Hornberger J, Hirth RA: Financial implications of choice of dialysistype of the revisedMedicare payment system: an economic analysis. AmJ Kidney Dis 60: 280–287, 2012 PubMed
22. US Renal Data System: USRDS 2013 Annual Data Report: Atlas ofEnd-Stage Renal Disease in the United States, Bethesda, MD, NationalInstitutes of Health, National Institute of Diabetes and Digestive andKidney Diseases, 2013
23. Neumann ME: 20th annual ranking: a look back, and getting positionedfor the future. Nephrol News Issues 26: 30–31, 2014 PubMed
24. Golper TA: The possible impact of the US prospective payment system(“bundle”) on the growth of peritoneal dialysis. Perit Dial Int 33: 596–599, 2013 PubMed
25. Mehrotra R, Kermah D, Fried L, Kalantar-Zadeh K, Khawar O, NorrisK, Nissenson A: Chronic peritoneal dialysis in the United States: decliningutilization despite improving outcomes. J Am Soc Nephrol 18: 2781–2788,2007 PubMed
26. Golper TA, Saxena AB, Piraino B, Teitelbaum I, Burkart J, FinkelsteinFO, Abu-Alfa A: Systematic barriers to the effective delivery of homedialysis in the United States: a report from the Public Policy/AdvocacyCommittee of the North American Chapter of the International Societyfor Peritoneal Dialysis. Am J Kidney Dis 58: 879–885, 2011 PubMed
27. Lacson E Jr: Fresenius expanding INHD programs. Nephrol News Issues25: 29–31, 2011 PubMed
28. Ribitsch W, Haditsch B, Otto R, Schilcher G, Quehenberger F, RoobJM, Rosenkranz AR: Effects of a pre-dialysis patient education programon the relative frequencies of dialysis modalities. Perit Dial Int 33: 367–371, 2013 PubMed
29. Lacson E Jr, Wang W, DeVries C, Leste K, Hakim RM, Lazarus M,Pulliam J: Effects of a nationwide predialysis educational program onmodality choice, vascular access, and patient outcomes. Am J KidneyDis 58: 235–242, 2011 PubMed
30. Mehrotra R, Blake P, Berman N, Nolph KD: An analysis of dialysistraining in the United States and Canada. Am J Kidney Dis 40: 152–160,2002 PubMed
31. Just PM, Riella MC, Tschosik EA, Noe LL, Bhattacharyya SK, deCharro F: Economic evaluations of dialysis treatment modalities.HealthPolicy 86: 163–180, 2008 PubMed
32. Ghaffari A, Kalantar-Zadeh K, Lee J, Maddux F, Moran J, Nissenson A:PD First: peritoneal dialysis as the default transition to dialysis therapy.Semin Dial 26: 706–713, 2013 PubMed
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 315

SyllabusNephSAP, Volume 13, Number 5, November 2014—ESRD and Dialysis
John P. Middleton, MD, and Ruediger W. Lehrich, MDDepartment of Medicine, Division of Nephrology, Duke University, Durham, North Carolina
The ASN Education Director for MOC and the Deputy Education Director for NephSAP would like to thank theDivision of Nephrology at Duke University Medical Center for developing this issue of NephSAP. Nephrologyfellows and faculty from Duke were instrumental in writing this edition under the editorial leadership of Dr. JohnMiddleton and Dr. Ruediger Lehrich. Our intention is to develop and support scholarship among the next generationof nephrologists. We also would like to thank Dr. James Novak from Henry Ford Hospital for his thoughtful reviewand editing of questions published in this issue of NephSAP.
C. Blake Cameron, MD,* Shafic El Hindi, MD,* Gentzon Hall, MD, PhD,* Rasheeda K. Hall, MD, MBA, MHS,*Andrew F. Malone, MD,† Shashi K. Nagaraj, MBBS, MD,‡ David Ortiz-Melo, MD,* Paul J. Phelan, MD,§
John K. Roberts, MD, MS,* Stephen R. Smith, MD,* John W. Stanifer, MD, MSc,* Samantha Suthar, MD,*Scott G. Westphal, MD,* and James Novak, MD║
Departments of *Medicine and ‡Pediatrics, Division of Nephrology, Duke University, Durham, North Carolina;†Department of Medicine, Renal Division, Washington University, Saint Louis, Missouri; §Royal Infirmary ofEdinburgh, Scotland; and ║Department of Medicine, Division of Nephrology, Henry Ford Hospital, Detroit,Michigan
Learning Objectives1. To describe the epidemiology of ESRD in the
United States and internationally and reviewunique transitions in the care for dialysispatients
2. To summarize developments in in-center he-modialysis, home-suitable dialysis, and dial-ysis methodology
3. To discuss management challenges such asanemia, nutrition, cardiovascular disease, preg-nancy, and infectious complications in patientsundergoing dialysis
This issue of NephSAP summarizes significantdevelopments in the field of ESRD and dialysis carepublished between January 2012 and December 2013.A few publications from outside of that time frame arealso referenced if they had bearing on new publications.As in previous NephSAP issues, kidney transplantation,vascular access for hemodialysis, mineral metabolism,and pediatric nephrology are not detailed in this issue.After reviewing the current literature, it became clear
that specific new topics warrant closer attention than inprevious NephSAP issues. This issue acknowledges newobservations regarding the “bundled payment” system fordialysis services, transitions in nephrology care, emergingdialysis technologies, and developing practices and viewson geriatrics and end-of-life care. In addition, peritonealdialysis and home dialysis therapies are reviewed in thesection on home-suitable dialysis therapies.
ESRD: Epidemiology and Societal Aspects
Trends in Incidence, Prevalence, PatientCharacteristics, Therapy Modality, Mortality, andMorbidity in the US ESRD PopulationIncidence and Prevalence. The US Renal Data Sys-tems (USRDS) 2013 Annual Data Report states thatthe number of incident dialysis patients declined forthe first time since the US Medicare ESRD programwas conceived in 1973 (1). The total number of inci-dent dialysis patients decreased by 1.6% compared withthe previous year to around 113,000 in 2011. The prev-alent ESRD population at the end of 2011 consistedof approximately 616,000 patients, 430,273 of whomreceived dialysis therapies and 185,626 of whom hada functioning kidney transplant. The ESRD population
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
316
exhibited an annual growth rate of 3.4%, which wasthe smallest increment in .3 decades.
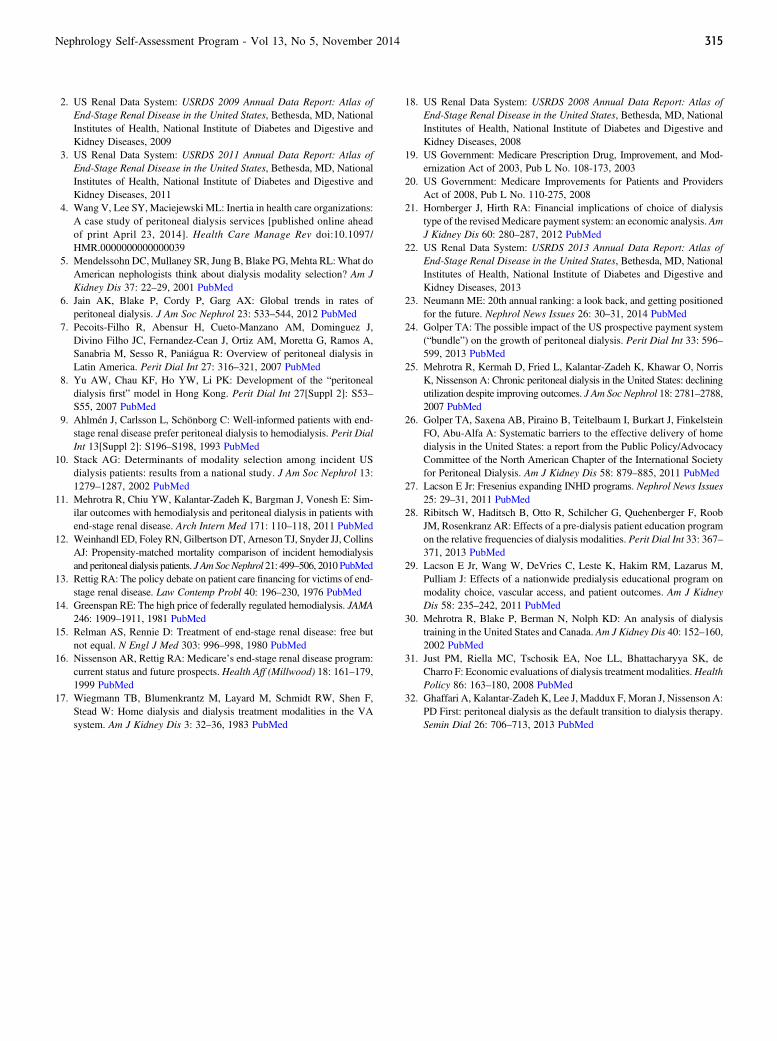
Rosansky and Clark (2) recently postulated thatthe observed increase in the incident rate of ESRDtherapies over the previous decade was due to a trendtoward initiation of dialysis earlier in the course ofCKD. Indeed, early starts, defined as initiation of dial-ysis with an eGFR $10 ml/min per 1.73 m2, increaseddramatically from 19% to 54% of all incident patientsbetween 1996 and 2009 (2). This proportion remainedstable at 54% between 2009 and 2011 (Figure 1). Fur-thermore, the incident count of ESRD rose by 80% inpatients aged .75 years from 1996 to 2005. Early di-alysis starts accounted for most of the rise in the in-cident dialysis population in this age group. However,the increase in incident counts of ESRD patients aged.75 years dramatically slowed. From 2005 to 2010,this segment of the ESRD population only grew by 4%(1,2). This development might in part be due to the factthat the nephrology community and society as a wholeare rethinking how to best manage the elderly popula-tionwith regard to aggressive and life-supporting therapiessuch as dialysis (3).
The burden of disease in the community can bewell characterized by ascertainment of prevalence andincidence; however, these metrics may not be partic-ularly helpful in estimating the risk of developing dis-ease in a given individual. Population characteristicsare also of limited use for the ascertainment of futureresource requirements and for directing public policy.In a recent study, Turin and colleagues (4) estimatedthe lifetime risk of ESRD by sex and baseline kidneyfunction in a large cohort of individuals living in Canada.In this study, approximately 1 in 38 men aged 40 yearswho lived into their 90s developed ESRD. By contrast,this rate was only 1 in 57 for women. If renal functionwas impaired (eGFR of 44–59 ml/min per 1.73 m2), therisk increased to 1 in 13 for 40-year-old men and 1 in 31for women.Patient Characteristics. Diabetes and hypertensionremain the most common causes of ESRD; however,the incident count for ESRD cases due to diabetes hasdecreased by 4.2% from 2010 to 2011 (1). The growthof diabetic nephropathy in the dialysis population variesgreatly by age and ethnicity. Among white patients be-tween the ages of 30 and 39 years, ESRD caused by
Figure 1. Proportion of incident ESRD patient by eGFR (ml/min per 1.73 m2) at start of RRT. Red, 0–4.9; blue, 5–9.9; purple,10–14.9; and green,.15. Patients who started RRT with an eGFR.10 ml/min per 1.73 m2 were considered early starters. Theproportion of early starters increased from 19% to 54% between 1996 and 2008; however, this proportion remained stablebetween 2009, 2010, and 2011. Reprinted with permission from Rosansky SJ, Clark WF: Has the yearly increase in the renalreplacement therapy population ended? J Am Soc Nephrol 24: 1367–1370, 2013.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 317

diabetes only grew by 3.5% since 2000. The numberof African Americans with diabetes aged 30–39 yearswho initiated dialysis from 2000 to 2011 increased 72%.The change in the population of patients with hyperten-sive nephrosclerosis, the second most common causeof ESRD in the United States, also varies by age andethnicity. Incident counts for white 40- to 49-year-oldpatients with ESRD due to hypertension rose by 61%from 2000 to 2011 (1). In African Americans, thisnumber decreased by 5.8% within the same timeframe.The incident count in African Americans who developESRD due to hypertension, however, is 11 times greaterthan in whites. Perhaps as a result of the demographicdifferences and population distribution, marked regionaldifferences persist in the prevalence and incidence ofESRD. The Pacific Northwest (Network 16) has thelowest rate of ESRD, whereas the Southeastern UnitedStates (Network 8) has the highest rate of ESRD.Mortality and Morbidity. Mortality rates in prevalentdialysis patients have declined: Unadjusted mortalityhas fallen from 1996 by 18.3% to 284 deaths per 1000patient-years at risk (1). Any enthusiasm for this favor-able bit of news is dampened by the observation that theadjusted mortality in the dialysis population is 6.5 to 7.9times greater than that for the general population, withthe first year on dialysis being a particularly vulnerableperiod.
The USRDS changed its reporting convention inthe 2013 Annual Data Report. For the first time, theUSRDS computed mortality rates from day 1 of de-clared ESRD (based on Medical Evidence Form 2728)as opposed to day 90, which was the convention inprevious years. The adjusted all-cause mortality in 2010after 2 months on dialysis was 440.2 deaths per 1000patient-years, and 200.5 deaths per 1000 patient-yearsafter 12 months on dialysis. In subsequent years ondialysis, the mortality rate remained relatively stablebetween 185.7 and 219.2 deaths per 1000 patient-years.These data highlight the fact that the first months ondialysis remain the most vulnerable period for dialysispatients.
Trends in survival in the United States ESRDpopulation demonstrated modest improvement over thelast 4 decades across different age categories. For instance,a 50-year-old dialysis patient in 2007 is projected to liveanother 7.9 years as opposed to 7.3 years in 1977 (7%improvement). However, age-specific survival over thelast 4 decades in the general population outpaced theadvances made in the ESRD population: A 50-year-old
individual in the general population was projected to liveanother 27.5 years in 1977 versus 30.9 years in 2007(12% improvement) (5).
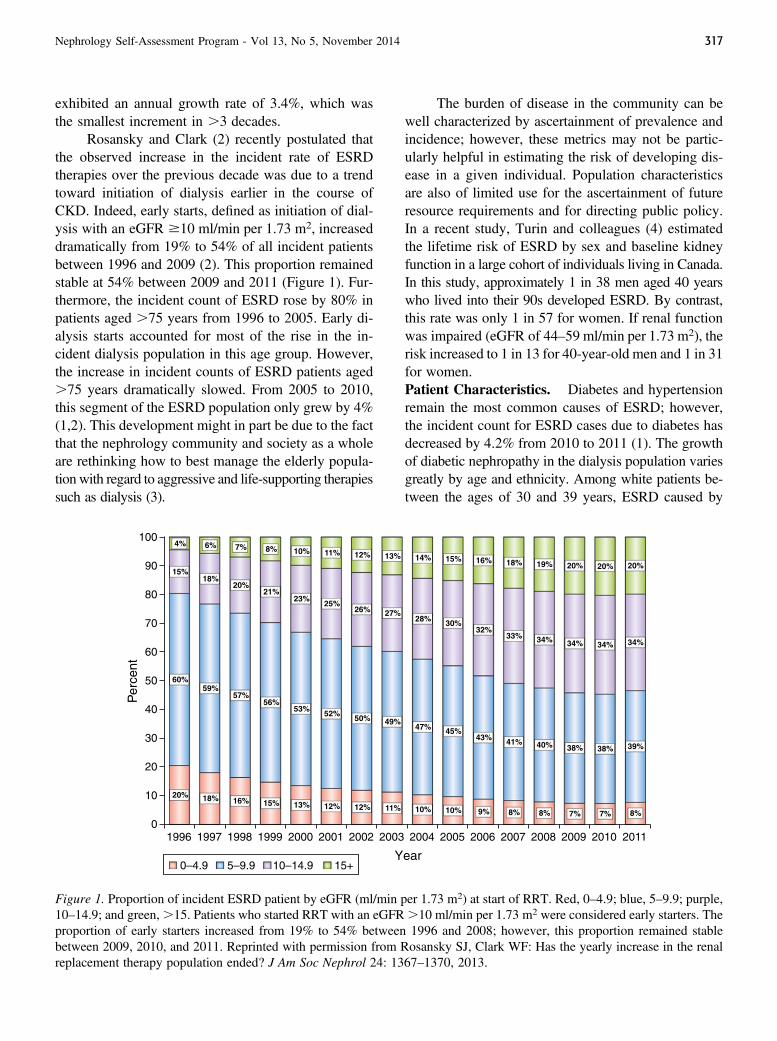
Hospitalization of ESRD patients greatly affectsquality of life (QOL), increases health care costs, andmay herald a precipitous decline in health that ulti-mately ends in death. In a recent study, hospitalizationtrends, as well as laboratory and treatment parametersof 6262 dialysis patients in the United States wereanalyzed (6). Not surprisingly, the rate of hospital-ization increased sharply before death. Laboratory andtreatment parameters were investigated for up to6 months before the index hospitalization. Severaldialysis-specific parameters changed leading up to theindex hospitalization. Intradialytic decline in systolicBP lessened from 11.5 to 10.2 mmHg, interdialytic weightgain declined from 2.76 to 2.67 kg, and effectivedialysis treatment time decreased from 215 minutesto 213 minutes. Of the laboratory parameters, this studydetermined that the hemoglobin concentration decreasedfrom 11.87 to 11.65 g/dl before hospitalization. In patientsultimately hospitalized for infection, the neutrophil-to-lymphocyte ratio increased from 3.7 to 4.5. Serum albuminlevels and predialysis systolic BP also changed (Figure 2).Even though these changes are subtle, the authors suggestedthat the observed changes before hospitalization couldbe used in predictive models.Therapy Modality. A significant change in deliveredESRD therapy is the continued rise in patients who un-dergo peritoneal dialysis (PD) (1). In 2011, a total of7323 patients were placed on PD at initiation of dialysistherapies. At day 90, the number of patients undergoingPD rose to 7887. In 2008, the rate of PD patients permillion population (pmp) was 21.4; this number rose to25.1 in 2011 (17% increase). The number of hemodi-alysis (HD) patients per million population rose onlymodestly from 278.2 to 280 pmp (0.6% increase) from2008 to 2011 (1). Use of PD will likely increase furtherbecause of the newly introduced prospective paymentsystem (PPS) for ESRD care, which provides a mone-tary incentive for growing this segment of the dialysispopulation (7).
Trends in Incidence, Prevalence, DialysisModality, and Survival of ESRD InternationallyEpidemiology. Over 2 million people worldwidenow have ESRD (8), but this prevalence likely under-estimates the extent of the affected population. Inmany developing countries, ESRD is a uniformly fatal
318 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
condition that results in a reported incidence rate that isdiscordant from the prevalence rate. In addition, diag-nostic limitations, lack of registries, and poor accessto medical care result in many cases that are undetectedat the time of death. Even in sub-Saharan Africa, where.22 million people are living with HIV, the potentialfor an overwhelmingly high burden of disease is be-coming conspicuous (9). New evidence suggests that theprevalence of CKD and incidence of AKI in that geo-graphic region approximates or exceeds that of high-income countries such as the United States (9,10).Furthermore, despite the observation that the globalprevalence of maintenance dialysis has doubled since1990 (11), the nearly 80% of the patients who receiveRRT are from five countries. These countries includethe United States, Japan, Germany, Brazil, and Italy,areas that represent approximately 10% of the world’spopulation (12). This is particularly concerning giventhat an estimated 119 million people now have CKDin China alone (13). Similarly, in India, the world’s secondmost populous country, a new health registry indicatesthat the prevalence of CKD has surpassed the UnitedStates, yet ,10% of ESRD patients in India receiveRRT (14).
The cause of CKD differs around the globe. Inhigh-income countries, diabetes and hypertension are re-sponsible for most cases of CKD and ESRD, whereasHIV, hepatitis B and C, GN, and exposure to environ-mental toxins are recognized as common causes in low-income countries (15). Diabetic kidney disease is also asignificant contributor to the ESRD population world-wide, especially in many Latin American and MiddleEastern countries, where prevalence rates of diabetesare often .25% (16,17).Renal Replacement Modalities. In low-incomecountries, prescription of RRT is most likely to occurin patients who present with AKI (18). By contrast,patients who are prescribed RRT in high-income coun-tries are more likely to have ESRD. Patients in low-income countries tend to be young and economicallyproductive persons from within the community (18).The worldwide morbidity and mortality of AKI con-tinue to have highly variable outcomes dependingupon the clinical setting, provider knowledge, and localresources such as access to diagnostic and treatmentmodalities (10). With the transition of patients to ESRD,the role of PD has garnered much attention in the pastfew years as a potentially less expensive, more acces-sible, and more sustainable mode of RRT. In this re-gard, Jain and colleagues recently provided strongevidence that the use of PD is increasing in absolutenumbers. In low-income countries, the rate of PD in-creased from 10.0 to 34.9 pmp, increasing 24.9 pmp(95% confidence interval, 19.2 to 30.6 pmp) from 1996to 2008 (19). Despite this increase in uptake, it is notsurprising that PD use is heterogeneous in global ap-plications. In 2013, van de Luijtgaarden and coworkersreported that at the country level, there was no associa-tion among the reimbursement rates for HD comparedwith PD and the percentage of patients placed on PD(20).
The use of PD is an attractive, if not necessary,option in some locations because it can be managed inlow-technology environments without reliable electric-ity. This likely explains the increase in PD use in a fewlow-income countries in sub-Saharan Africa (21). Chal-lenges such as the availability of supplies, timely diagno-sis, and expertise in PD remain (15), and most patientsin sub-Saharan Africa continue to have little access toany form of RRT.
Broadly speaking, HD remains the preferred andpredominant mode of RRT in Asia and Latin America,but China has seen a 30% annual growth of PD and
Figure 2. Relationship between hospitalization rate, serumalbumin, predialysis systolic BP, neutrophil-to-lymphocyteratio, and ultimately death in ESRD patients undergoing he-modialysis. NLR, neutrophil-to-lymphocyte ratio; SBP, sys-tolic BP. Reprinted with permission fromUsvyat LA, KoomanJP, van der Sande FM, Wang Y, Maddux FW, Levin NW,Kotanko P: Dynamics of hospitalizations in hemodialysis pa-tients: Results from a large US provider. Nephrol Dial Trans-plant 29: 442–448, 2014.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 319
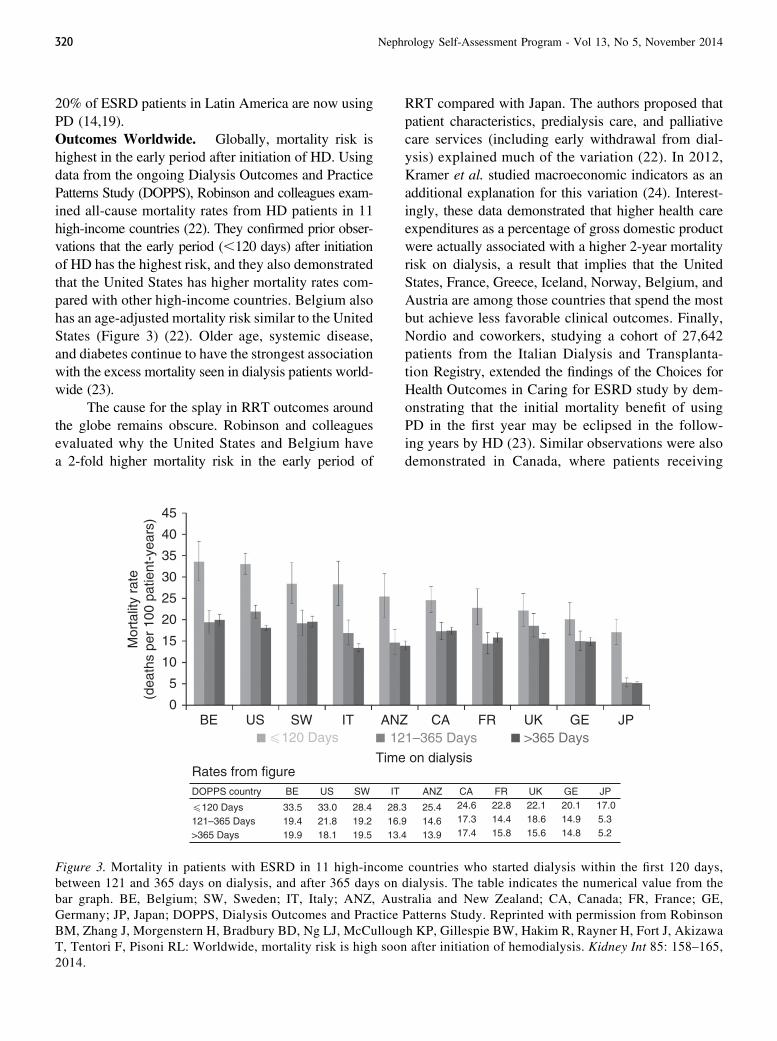
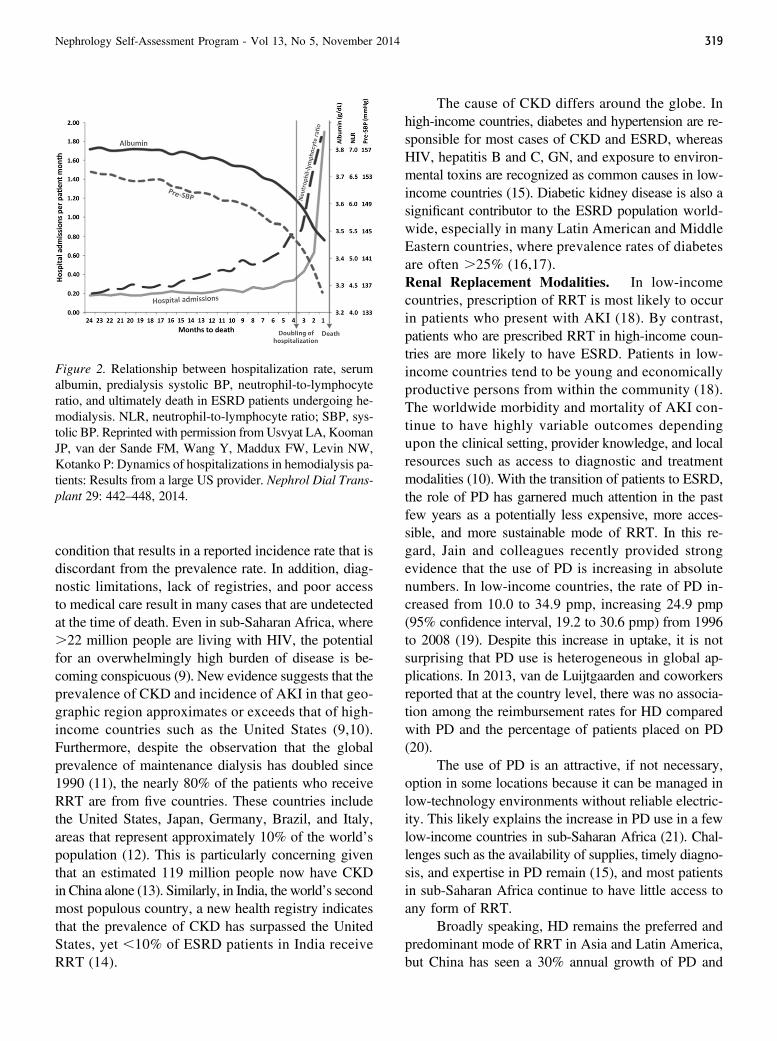
20% of ESRD patients in Latin America are now usingPD (14,19).Outcomes Worldwide. Globally, mortality risk ishighest in the early period after initiation of HD. Usingdata from the ongoing Dialysis Outcomes and PracticePatterns Study (DOPPS), Robinson and colleagues exam-ined all-cause mortality rates from HD patients in 11high-income countries (22). They confirmed prior obser-vations that the early period (,120 days) after initiationof HD has the highest risk, and they also demonstratedthat the United States has higher mortality rates com-pared with other high-income countries. Belgium alsohas an age-adjusted mortality risk similar to the UnitedStates (Figure 3) (22). Older age, systemic disease,and diabetes continue to have the strongest associationwith the excess mortality seen in dialysis patients world-wide (23).
The cause for the splay in RRT outcomes aroundthe globe remains obscure. Robinson and colleaguesevaluated why the United States and Belgium havea 2-fold higher mortality risk in the early period of
RRT compared with Japan. The authors proposed thatpatient characteristics, predialysis care, and palliativecare services (including early withdrawal from dial-ysis) explained much of the variation (22). In 2012,Kramer et al. studied macroeconomic indicators as anadditional explanation for this variation (24). Interest-ingly, these data demonstrated that higher health careexpenditures as a percentage of gross domestic productwere actually associated with a higher 2-year mortalityrisk on dialysis, a result that implies that the UnitedStates, France, Greece, Iceland, Norway, Belgium, andAustria are among those countries that spend the mostbut achieve less favorable clinical outcomes. Finally,Nordio and coworkers, studying a cohort of 27,642patients from the Italian Dialysis and Transplanta-tion Registry, extended the findings of the Choices forHealth Outcomes in Caring for ESRD study by dem-onstrating that the initial mortality benefit of usingPD in the first year may be eclipsed in the follow-ing years by HD (23). Similar observations were alsodemonstrated in Canada, where patients receiving
Figure 3. Mortality in patients with ESRD in 11 high-income countries who started dialysis within the first 120 days,between 121 and 365 days on dialysis, and after 365 days on dialysis. The table indicates the numerical value from thebar graph. BE, Belgium; SW, Sweden; IT, Italy; ANZ, Australia and New Zealand; CA, Canada; FR, France; GE,Germany; JP, Japan; DOPPS, Dialysis Outcomes and Practice Patterns Study. Reprinted with permission from RobinsonBM, Zhang J, Morgenstern H, Bradbury BD, Ng LJ, McCullough KP, Gillespie BW, Hakim R, Rayner H, Fort J, AkizawaT, Tentori F, Pisoni RL: Worldwide, mortality risk is high soon after initiation of hemodialysis. Kidney Int 85: 158–165,2014.
320 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

PD had significantly better survival during the first2 years, but the long-term survival (3–5 years) betweenmodalities was no different in the entire cohort (25). InFinland, Haapio et al. saw no survival differencebetween PD and HD patients in the adjusted analy-sis at any time period or any subgroup, although their datashowed a trend toward worse survival among patientsaged $75 years using PD (26). The global outcomessuggest that the survival of ESRD patients is verysimilar for PD and HD, but clinical outcomes arestrongly influenced by the demographics and medicalcharacteristics of the indigenous population.
Effect of a Fixed or Bundled Payment Plan onPractice Patterns
In the United States, a dramatic shift took placein the last 3 years influencing payment for ESRD-related services. In 2011, the US Centers for Medicareand Medicaid Services launched the PPS for ESRDcare, which expanded the prior composite rate pay-ment to include services that had historically been paidseparately on a fee-for-service basis (27). These newlybundled services included all laboratory tests, intra-venous medications administered with dialysis, bloodproducts, and (beginning in 2016) oral medicationsassociated with ESRD therapies. Physician services,vascular access, and non-ESRD medications will con-tinue to be reimbursed separately as before (27,28).The base rate paid by Medicare to dialysis facilitiesincreased from $135.15 to $229.63 per dialysis treat-ment, with adjustments for geographic wage in-dices, patient age, body surface area, new start ofdialysis (first 120 days), and certain comorbid con-ditions (29). No adjustment was made for race orethnicity. This composite rate was calculated basedon a review of historical Medicare ESRD expendi-tures and service utilization, offset by a global 2%payment reduction. This new payment process shiftedthe financial risk from Medicare to the dialysis pro-viders, and the new policy disincentivized the use ofservices previously paid for outside the bundle. Thispolicy had the potential to prompt a drastic shift in theuse of costly intravenous erythropoiesis-stimulatingagents (ESAs) and vitamin D analogues. The new policyalso linked payments to a quality incentive program toensure minimum quality standards concerning anemiamanagement, dialysis adequacy, vascular access modal-ity, access infections, hospital admissions, patient-reportedsatisfaction with care, and bone mineral metabolism
goals (30). The impact of the PPS on the managementof anemia, bone metabolism and modality selectionare reviewed below.
In 2011 in the United States, the US Cen-ters for Medicare and Medicaid Serviceslaunched the PPS for ESRD care, creatinga “bundled” payment system. This has thepotential for shifting the financial risk fromMedicare to the dialysis providers. This newpayment policy will disincentivize the useof some medications and services in theESRD population.
Anemia Management. ESAs and intravenous ironpreparations are the mainstay of anemia managementin ESRD, but the prescription patterns for these medi-cations stand to undergo seismic changes with the newpayment plans in the United States. Coincident withthis change in reimbursement was evidence that tar-geting high hemoglobin levels by using ESAs causesharm (31,32). A retrospective cohort study examinedpatterns of anemia management in United States hemo-dialysis patients during 2002–2008 using data derivedfrom the USRDS (33). Over the time period studied,use of ESAs decreased and use of intravenous ironincreased, indicating a change in practice patterns thatpredates the expanded bundle.
The DOPPS Practice Monitor noted a decreasein average hemoglobin levels in prevalent United StatesHD patients during the transition to expanded bundlingin 2011 (34) (Figure 4). In this study, it was determinedthat African Americans, compared with other racial groups,experienced a larger decrease in mean hemoglobin levels(0.23 versus 0.04 g/dl) and an increase in percentage ofpatients with hemoglobin levels ,10 g/dl (2.4% versusno change) over the time frame of the study. However, thiswas coupled with a more favorable decrease in the per-centage of patients with inappropriately high hemoglobinlevels .12 g/dl (34.6% to 26.9% in African Americansversus 31.0% to 28.5% in other racial groups) (34).
It is conceivable that implementation of the 2011payment policy in the United States will have partic-ularly difficult consequences for freestanding dialysisclinics and small dialysis organizations (SDOs). TheStudy to Evaluate the Prospective Payment System Im-pact on Small Dialysis Organizations (STEPPS) focusedspecifically on SDOs, defined as stand-alone units or those
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 321
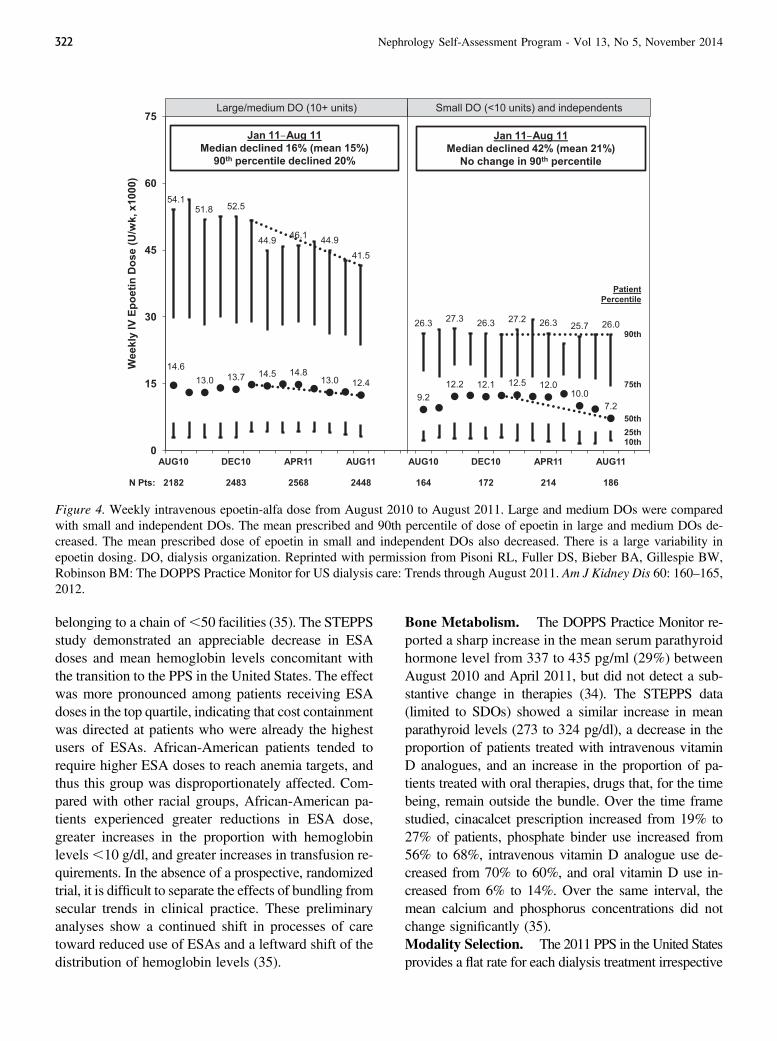
belonging to a chain of,50 facilities (35). The STEPPSstudy demonstrated an appreciable decrease in ESAdoses and mean hemoglobin levels concomitant withthe transition to the PPS in the United States. The effectwas more pronounced among patients receiving ESAdoses in the top quartile, indicating that cost containmentwas directed at patients who were already the highestusers of ESAs. African-American patients tended torequire higher ESA doses to reach anemia targets, andthus this group was disproportionately affected. Com-pared with other racial groups, African-American pa-tients experienced greater reductions in ESA dose,greater increases in the proportion with hemoglobinlevels,10 g/dl, and greater increases in transfusion re-quirements. In the absence of a prospective, randomizedtrial, it is difficult to separate the effects of bundling fromsecular trends in clinical practice. These preliminaryanalyses show a continued shift in processes of caretoward reduced use of ESAs and a leftward shift of thedistribution of hemoglobin levels (35).
Bone Metabolism. The DOPPS Practice Monitor re-ported a sharp increase in the mean serum parathyroidhormone level from 337 to 435 pg/ml (29%) betweenAugust 2010 and April 2011, but did not detect a sub-stantive change in therapies (34). The STEPPS data(limited to SDOs) showed a similar increase in meanparathyroid levels (273 to 324 pg/dl), a decrease in theproportion of patients treated with intravenous vitaminD analogues, and an increase in the proportion of pa-tients treated with oral therapies, drugs that, for the timebeing, remain outside the bundle. Over the time framestudied, cinacalcet prescription increased from 19% to27% of patients, phosphate binder use increased from56% to 68%, intravenous vitamin D analogue use de-creased from 70% to 60%, and oral vitamin D use in-creased from 6% to 14%. Over the same interval, themean calcium and phosphorus concentrations did notchange significantly (35).Modality Selection. The 2011 PPS in the United Statesprovides a flat rate for each dialysis treatment irrespective
Figure 4. Weekly intravenous epoetin-alfa dose from August 2010 to August 2011. Large and medium DOs were comparedwith small and independent DOs. The mean prescribed and 90th percentile of dose of epoetin in large and medium DOs de-creased. The mean prescribed dose of epoetin in small and independent DOs also decreased. There is a large variability inepoetin dosing. DO, dialysis organization. Reprinted with permission from Pisoni RL, Fuller DS, Bieber BA, Gillespie BW,Robinson BM: The DOPPS Practice Monitor for US dialysis care: Trends through August 2011. Am J Kidney Dis 60: 160–165,2012.
322 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

of modality, including home-based therapies. Becausethe calculation of the base rate principally reflects thecost structure of in-center hemodialysis, and becausehome-based modalities use comparatively fewer costlyinjectable drugs, economic analyses suggest that the newPPS will incentivize increased use of PD (7).
Disparity in ESRD CareDespite universal funding in the United States
for ESRD care through Medicare, patient outcomes varywidely across geographic, socioeconomic, and racialgroups (1). The underlying causes of this variation arepoorly understood.
Socioeconomic factors likely contribute to thisdisparity in the delivery of care. In a recent Australianstudy, socioeconomic status predicted need for RRT,with the incidence of dialysis increasing in the mostdisadvantaged areas (36). Similar observations weremade in an analysis of a French data registry (37). Bothof these studies suggested that diabetes predicted thepresence of ESRD and disadvantaged socioeconomicstatus. Similar influences are also likely present in theUnited States, where reported household income ofESRD patients predicted mortality (38). However,socioeconomic influences on outcomes in ESRD some-times run contrary to what might be expected. For ex-ample, patients of black ethnicity with ESRD receivingHD had higher QOL scores and improved survival ascompared with whites (38). This contrasts with reportedQOL and clinical outcomes in other chronic healthconditions in the United States. After adjustment forsocioeconomic factors, the apparent advantage for blackpatients was strengthened. However, when residentialsegregation was identified by use of an instrument calledthe Dissimilarity Index, residential racial segregation pre-dicted mortality in African-American ESRD patients (38).
Geography also plays an important role in dis-parate clinical outcomes in ESRD. In one study, pa-tient survival for urban versus rural dialysis patientswas roughly equivalent, but patients who lived furthestfrom the HD facility (.100 miles) had a substantiallyincreased risk of death compared with those livingwithin 10 miles (39). This observation was supportedin an analysis published by Maripuri and colleagues,who identified higher mortality in micropolitan orrural PD patients compared with their urban counter-parts. This study also identified that rural ESRDpatients were more likely to undergo kidney trans-plantation (40).
Health literacy is an important factor in ensuringdelivery of quality health care. In a recent observationalstudy of maintenance hemodialysis patients, it wasfound that patients with low health literacy as assessedby a questionnaire had increased incidence of misseddialysis treatments, emergency department visits, andESRD-associated hospitalizations (41).
The treatment of undocumented immigrants withESRD poses an ethical and financial dilemma for he-modialysis centers, hospitals, and health systems. Be-cause these patients usually lack health insurance andare ineligible for the Medicare ESRD benefit, indi-vidual states in the United States have pursued carefor ESRD patients in one of two ways: (1) acute hemo-dialysis in an acute care setting or (2) scheduled main-tenance hemodialysis in an outpatient setting. Theprovision of RRT often depends on charity care givenby a sponsoring health organization, the burden ofwhich varies widely based on institutional policies andcatchment area demographics. Some states, such asCalifornia, implemented a state-funded, long-termoutpatient dialysis program for undocumented ESRDpatients. Other states, such as Texas, lack a state-fundedoption completely, and undocumented ESRD patientsreceive only emergency care in an acute care setting(42). Linden and coworkers (43) recently reported re-sults from survey data derived from a single center thatmanaged undocumented ESRD patients. The aim of thesurvey was to investigate whether living donor kidneytransplantation is a cost-effective therapy for ESRD inthis group of patients. The studied population (45 patients)was younger and healthier than their documented counter-parts. Most patients were of Hispanic descent. The averageduration of United States residency was around 12 yearsand more than one half of the patients continued to workwhile on dialysis. When surveyed about thoughts re-garding kidney transplantation, most were interested andreadily identified a realistic potential donor. The authorssuggested that policy makers should consider kidneytransplantation as a cost-effective alternative to dialysisin undocumented ERSD patients. However, as franklystated in the accompanying editorial by Rodriguezand colleagues, “The US nephrology community isparalyzed by the challenges of finding the optimaltreatment strategy for undocumented immigrants withESRD” (42).
References1. US Renal Data System: USRDS 2013 Annual Data Report: Atlas of
Chronic Kidney Disease and End-Stage Renal Disease in the United
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 323
States, Bethesda, MD, National Institutes of Health, National Instituteof Diabetes and Digestive and Kidney Diseases, 2013
2. Rosansky SJ, Clark WF: Has the yearly increase in the renal re-placement therapy population ended? J Am Soc Nephrol 24: 1367–1370, 2013 PubMed
3. Schmidt RJ, Moss AH: Dying on dialysis: The case for a dignifiedwithdrawal. Clin J Am Soc Nephrol 9: 174–180, 2014 PubMed
4. Turin TC, Tonelli M, Manns BJ, Ahmed SB, Ravani P, James M,Hemmelgarn BR: Lifetime risk of ESRD. J Am Soc Nephrol 23: 1569–1578, 2012 PubMed
5. van Walraven C, Manuel DG, Knoll G: Survival trends in ESRDpatients compared with the general population in the United States. AmJ Kidney Dis 63: 491–499, 2014 PubMed
6. Usvyat LA, Kooman JP, van der Sande FM, Wang Y, Maddux FW,Levin NW, Kotanko P: Dynamics of hospitalizations in hemodialysispatients: Results from a large US provider. Nephrol Dial Transplant 29:442–448, 2014 PubMed
7. Hornberger J, Hirth RA: Financial implications of choice of dialysistype of the revised Medicare payment system: An economic analysis.Am J Kidney Dis 60: 280–287, 2012 PubMed
8. Eggers PW: Has the incidence of end-stage renal disease in the USA andother countries stabilized? Curr Opin Nephrol Hypertens 20: 241–245,2011 PubMed
9. Stanifer JW, Jing B, Tolan S, Helmke N, Mukerjee R, Naicker S, PatelU: The epidemiology of chronic kidney disease in sub-Saharan Africa:A systematic review and meta-analysis. Lancet Glob Health 2: e174–e181, 2014 PubMed
10. Lameire NH, Bagga A, Cruz D, De Maeseneer J, Endre Z, Kellum JA,Liu KD, Mehta RL, Pannu N, Van Biesen W, Vanholder R: Acutekidney injury: An increasing global concern. Lancet 382: 170–179,2013 PubMed
11. Thomas BA, Wulf S, Mehrotra R, Himmelfarb J, Naghavi M, MurrayCJ: The rapidly growing global burden of end-stage renal disease – ananalysis of the chance in maintenance dialysis prevalence between 1990and 2010 [Abstract TH-OR135]. J Am Soc Nephrol 24: 32A, 2013
12. Schieppati A, Remuzzi G: Chronic renal diseases as a public healthproblem: Epidemiology, social, and economic implications. Kidney IntSuppl 98[Suppl]: S7–S10, 2005 PubMed
13. Zhang L, Wang F, Wang L, WangW, Liu B, Liu J, Chen M, He Q, LiaoY, Yu X, Chen N, Zhang JE, Hu Z, Liu F, Hong D, Ma L, Liu H, ZhouX, Chen J, Pan L, Chen W, Wang W, Li X, Wang H: Prevalence ofchronic kidney disease in China: A cross-sectional survey. Lancet 379:815–822, 2012 PubMed
14. Rajapurkar MM, John GT, Kirpalani AL, Abraham G, Agarwal SK,Almeida AF, Gang S, Gupta A, Modi G, Pahari D, Pisharody R, PrakashJ, Raman A, Rana DS, Sharma RK, Sahoo RN, Sakhuja V, Tatapudi RR,Jha V: What do we know about chronic kidney disease in India: Firstreport of the Indian CKD registry. BMC Nephrol 13: 10, 2012 PubMed
15. Remuzzi G, Benigni A, Finkelstein FO, Grunfeld JP, Joly D, Katz I, LiuZH, Miyata T, Perico N, Rodriguez-Iturbe B, Antiga L, Schaefer F,Schieppati A, Schrier RW, Tonelli M: Kidney failure: Aims for the next10 years and barriers to success. Lancet 382: 353–362, 2013 PubMed
16. Cusumano A, Garcia GG, Di Gioia C, Hermida O, Lavorato C; LatinAmerican Registry of Dialysis and Transplantation: The Latin Amer-ican Dialysis and Transplantation Registry (RLDT) annual report 2004.Ethn Dis 16[Suppl 2]: S2–S10, 3, 2006 PubMed
17. Shaheen FA, Al-Khader AA: Preventive strategies of renal failure in theArab world. Kidney Int Suppl 98[Suppl]: S37–S40, 2005 PubMed
18. Li PK, Burdmann EA, Mehta RL; World Kidney Day Steering Com-mittee 2013: Acute kidney injury: Global health alert. Kidney Int 83:372–376, 2013 PubMed
19. Jain AK, Blake P, Cordy P, Garg AX: Global trends in rates ofperitoneal dialysis. J Am Soc Nephrol 23: 533–544, 2012 PubMed
20. van de Luijtgaarden MW, Jager KJ, Stel VS, Kramer A, Cusumano A,Elliott RF, Geue C, MacLeod AM, Stengel B, Covic A, Caskey FJ: Globaldifferences in dialysis modality mix: The role of patient characteristics,
macroeconomics and renal service indicators. Nephrol Dial Transplant28: 1264–1275, 2013 PubMed
21. Carter M, Kilonzo K, Odiit A, Kalyesubula R, Kotanko P, LevinNW, Callegari J: Acute peritoneal dialysis treatment programs forcountries of the East African community. Blood Purif 33: 149–152,2012 PubMed
22. Robinson BM, Zhang J, Morgenstern H, Bradbury BD, Ng LJ,McCullough KP, Gillespie BW, Hakim R, Rayner H, Fort J, AkizawaT, Tentori F, Pisoni RL: Worldwide, mortality risk is high soon afterinitiation of hemodialysis. Kidney Int 85: 158–165, 2014 PubMed
23. Nordio M, Limido A, Maggiore U, Nichelatti M, Postorino M,Quintaliani G; Italian Dialysis and Transplantation Registry: Survivalin patients treated by long-term dialysis compared with the generalpopulation. Am J Kidney Dis 59: 819–828, 2012 PubMed
24. Kramer A, Stel VS, Caskey FJ, Stengel B, Elliott RF, Covic A, Geue C,Cusumano A, Macleod AM, Jager KJ: Exploring the associationbetween macroeconomic indicators and dialysis mortality. Clin J AmSoc Nephrol 7: 1655–1663, 2012 PubMed
25. Yeates K, Zhu N, Vonesh E, Trpeski L, Blake P, Fenton S: Hemodi-alysis and peritoneal dialysis are associated with similar outcomes forend-stage renal disease treatment in Canada. Nephrol Dial Transplant27: 3568–3575, 2012 PubMed
26. Haapio M, Helve J, Kyllönen L, Grönhagen-Riska C, Finne P: Modalityof chronic renal replacement therapy and survival—a complete cohortfrom Finland, 2000-2009. Nephrol Dial Transplant 28: 3072–3081,2013 PubMed
27. Feldman RL, Desmarais MP, Muller JS: Orals in the bundle: A policyframework. Clin J Am Soc Nephrol 8: 1043–1047, 2013 PubMed
28. Hirth RA, Turenne MN, Wheeler JR, Nahra TA, Sleeman KK, ZhangW, Messana JA: The initial impact of Medicare’s new prospectivepayment system for kidney dialysis. Am J Kidney Dis 62: 662–669,2013 PubMed
29. US Centers for Medicare & Medicaid Services, US Department ofHealth and Human Services: 42 CFR Parts 410, 413 and 414 MedicareProgram; End-Stage Renal Disease Prospective Payment System, FinalRule. Fed Regist 75: 49030–49211, 2010
30. Maddux FW: Impact of the bundled end-stage renal disease paymentsystem on patient care. Blood Purif 33: 107–111, 2012 PubMed
31. Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S, WolfsonM, Reddan D; CHOIR Investigators: Correction of anemia withepoetin alfa in chronic kidney disease. N Engl J Med 355: 2085–2098, 2006 PubMed
32. Pfeffer MA, Burdmann EA, Chen CY, Cooper ME, de Zeeuw D,Eckardt KU, Feyzi JM, Ivanovich P, Kewalramani R, Levey AS, LewisEF, McGill JB, McMurray JJ, Parfrey P, Parving HH, Remuzzi G,Singh AK, Solomon SD, Toto R; TREAT Investigators: A trial ofdarbepoetin alfa in type 2 diabetes and chronic kidney disease. N EnglJ Med 361: 2019–2032, 2009 PubMed
33. Freburger JK, Ng LJ, Bradbury BD, Kshirsagar AV, Brookhart MA:Changing patterns of anemia management in US hemodialysis patients.Am J Med 125: 906, e9, 2012 PubMed
34. Pisoni RL, Fuller DS, Bieber BA, Gillespie BW, Robinson BM: TheDOPPS Practice Monitor for US dialysis care: Trends through August2011. Am J Kidney Dis 60: 160–165, 2012 PubMed
35. Brunelli SM, Monda KL, Burkart JM, Gitlin M, Neumann PJ, Park GS,Symonian-Silver M, Yue S, Bradbury BD, Rubin RJ: Early trends fromthe Study to Evaluate the Prospective Payment System Impact onSmall Dialysis Organizations (STEPPS). Am J Kidney Dis 61: 947–956, 2013 PubMed
36. Grace BS, Clayton P, Cass A, McDonald SP: Socio-economic statusand incidence of renal replacement therapy: A registry study of Australianpatients. Nephrol Dial Transplant 27: 4173–4180, 2012 PubMed
37. Couchoud C, Guihenneuc C, Bayer F, Lemaitre V, Brunet P, Stengel B;REIN Registry: Medical practice patterns and socio-economic factorsmay explain geographical variation of end-stage renal disease incidence.Nephrol Dial Transplant 27: 2312–2322, 2012 PubMed
324 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

38. Kimmel PL, Fwu CW, Eggers PW: Segregation, income disparities,and survival in hemodialysis patients. J Am Soc Nephrol 24: 293–301,2013 PubMed
39. Thompson S, Gill J, Wang X, Padwal R, Pelletier R, Bello A,Klarenbach S, Tonelli M: Higher mortality among remote comparedto rural or urban dwelling hemodialysis patients in the United States.Kidney Int 82: 352–359, 2012 PubMed
40. Maripuri S, Arbogast P, Ikizler TA, Cavanaugh KL: Rural and micro-politan residence and mortality in patients on dialysis. Clin J Am SocNephrol 7: 1121–1129, 2012 PubMed
41. Green JA, Mor MK, Shields AM, Sevick MA, Arnold RM, PalevskyPM, Fine MJ, Weisbord SD: Associations of health literacy withdialysis adherence and health resource utilization in patients re-ceiving maintenance hemodialysis. Am J Kidney Dis 62: 73–80,2013 PubMed
42. Rodriguez RA, Himmelfarb J, Hall YN: Tragic options and compro-mised care: Undocumented immigrants with ESRD. Am J Kidney Dis60: 335–337, 2012 PubMed
43. Linden EA, Cano J, Coritsidis GN: Kidney transplantation in un-documented immigrants with ESRD: A policy whose time has come?Am J Kidney Dis 60: 354–359, 2012 PubMed
Patient Transitions of Care in ESRD
Transition from CKD to ESRD CareA total of 116,000 patients transitioned from
CKD to ESRD care in 2011 (1). Only one-half of thesepatients had been referred to a nephrologist beforeinitiation of dialysis. The proportion of CKD patientswho receive nephrology care before initiating dialysishas not changed substantially over the past decade (1).One likely outcome of this practice is that hemodialysis(HD) is initiated with a central venous catheter (CVC)in as many as 80% of incident patients as opposed toan arteriovenous fistula (AVF), the preferred accessmodality. No nephrology care before initiating dialysispredicts the type of vascular access chosen for the firstdialysis treatment (1).
It is not clear whether there is an optimal timeto place AVFs in CKD patients. Oliver and colleaguesrecently presented an analysis of a Canadian adminis-trative data set of 1929 patients who underwent AVFcreation (2). Of those patients, 81% initiated dialysisafter a median follow-up of 186 days. However, theremaining 19% never started dialysis: 9% died withoutundergoing dialysis (median observation period of 345days) and 10% remained predialysis (median obser-vation period of 1179 days). The recommended timeframe for AVF creation, estimated to be 3–12 monthsbefore anticipated initiation of HD, occurred in 40% ofpatients studied; 30% of fistulas were created within 90days of starting dialysis, and 30% were created.1 yearbefore initiation of dialysis (Figure 5). Yet 37% ofpatients in this cohort required a CVC within 30 days of
starting dialysis. However, 44% used an AVF as theirfirst access for HD. This analysis emphasizes the in-trinsic difficulty in timing AVF creation correctly andhighlights that nearly 1 in 5 patients with CKD whohave access surgery will likely never need the AVF forHD.
Despite efforts to sufficiently prepare for patientsfor a life with ESRD, survey data suggest that patientsoften feel ill prepared and poorly informed about thedialysis process (3). To address whether populationeducation and screening are effective in optimizing di-alysis starts, Kurella Tamura and colleagues (4) reportedoutcomes from 595 patients who were identified to haveCKD by the National Kidney Foundation Kidney EarlyEvaluation Program (KEEP). Patients who subsequentlydeveloped ESRD were compared with matched CKDpatients who were not enrolled in KEEP. The KEEPparticipants were more likely to have followed with anephrologist, were more likely to have been preemp-tively transplanted or transplant wait-listed, and weremore likely to have chosen peritoneal dialysis. Dis-appointingly, KEEP participants had a similar lack ofpermanent vascular access at dialysis start comparedwith non-KEEP participants. The KEEP program pro-vided improved mortality in an unadjusted analysis;however, this benefit was no longer significant afteradjusting for clinical covariates.
Even if referral to a nephrology specialist takesplace .12 months before initiating dialysis therapies,an ideal clinical outcome is not assured. A retrospectiveanalysis of 436 incident dialysis patients identified sev-eral other important factors causing suboptimal dialysisinitiation, defined as use of a CVC and/or initiation ofdialysis as an inpatient (5). Suboptimal starts occurredin 56.4% of patients, with 65% of this group startingdialysis with a CVC. Patient-related delays (31%), acuteor chronic deterioration in renal function (31%), surgicaldelays (16%), and procrastination (9%) were the fourmost common causes for the suboptimal dialysis initia-tions in this study.
Even with adequate preparation and education,the ideal time to initiate dialysis remains unclear. TheKidney Disease Improving Global Outcomes (KDIGO)Work Group, in its 2012 clinical practice guideline,suggested starting dialysis therapies when “symptomsand signs attributable to kidney failure” are present (6).The work group emphasized that the trigger for startingdialysis typically occurs when the GFR is between 5and 10 ml/min per 1.73 m2. This recommendation was
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 325
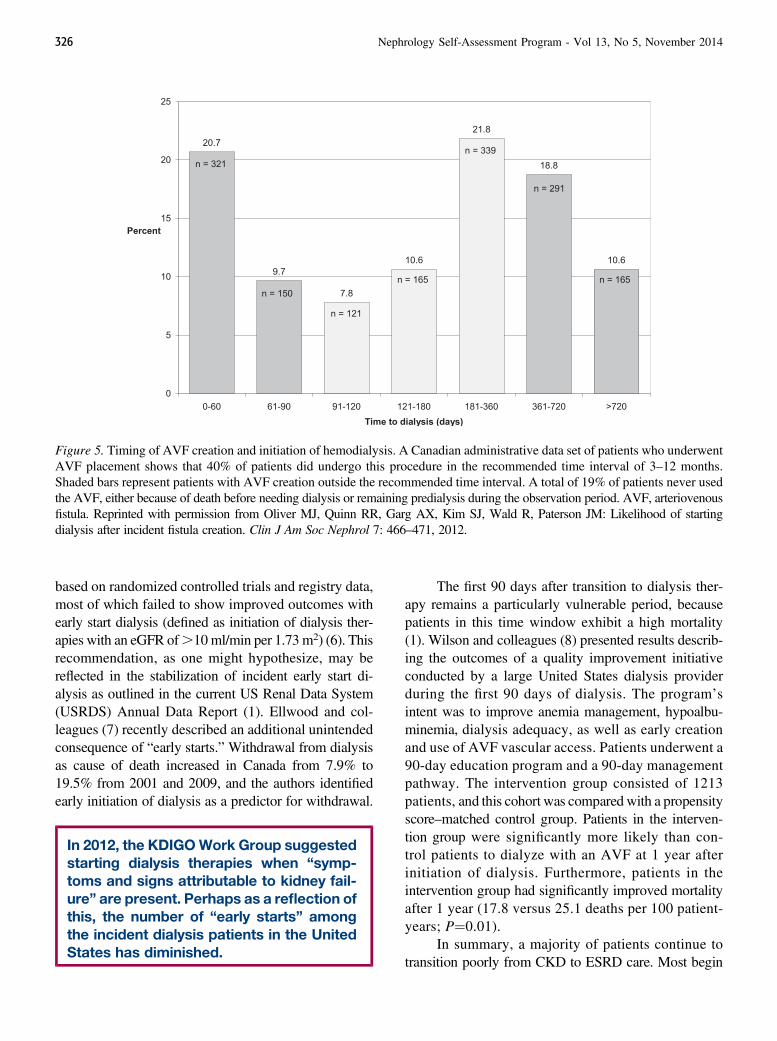
based on randomized controlled trials and registry data,most of which failed to show improved outcomes withearly start dialysis (defined as initiation of dialysis ther-apies with an eGFR of.10ml/min per 1.73m2) (6). Thisrecommendation, as one might hypothesize, may bereflected in the stabilization of incident early start di-alysis as outlined in the current US Renal Data System(USRDS) Annual Data Report (1). Ellwood and col-leagues (7) recently described an additional unintendedconsequence of “early starts.” Withdrawal from dialysisas cause of death increased in Canada from 7.9% to19.5% from 2001 and 2009, and the authors identifiedearly initiation of dialysis as a predictor for withdrawal.
In 2012, the KDIGOWork Group suggestedstarting dialysis therapies when “symp-toms and signs attributable to kidney fail-ure” are present. Perhaps as a reflection ofthis, the number of “early starts” amongthe incident dialysis patients in the UnitedStates has diminished.
The first 90 days after transition to dialysis ther-apy remains a particularly vulnerable period, becausepatients in this time window exhibit a high mortality(1). Wilson and colleagues (8) presented results describ-ing the outcomes of a quality improvement initiativeconducted by a large United States dialysis providerduring the first 90 days of dialysis. The program’sintent was to improve anemia management, hypoalbu-minemia, dialysis adequacy, as well as early creationand use of AVF vascular access. Patients underwent a90-day education program and a 90-day managementpathway. The intervention group consisted of 1213patients, and this cohort was compared with a propensityscore–matched control group. Patients in the interven-tion group were significantly more likely than con-trol patients to dialyze with an AVF at 1 year afterinitiation of dialysis. Furthermore, patients in theintervention group had significantly improved mortalityafter 1 year (17.8 versus 25.1 deaths per 100 patient-years; P¼0.01).
In summary, a majority of patients continue totransition poorly from CKD to ESRD care. Most begin
Figure 5. Timing of AVF creation and initiation of hemodialysis. A Canadian administrative data set of patients who underwentAVF placement shows that 40% of patients did undergo this procedure in the recommended time interval of 3–12 months.Shaded bars represent patients with AVF creation outside the recommended time interval. A total of 19% of patients never usedthe AVF, either because of death before needing dialysis or remaining predialysis during the observation period. AVF, arteriovenousfistula. Reprinted with permission from Oliver MJ, Quinn RR, Garg AX, Kim SJ, Wald R, Paterson JM: Likelihood of startingdialysis after incident fistula creation. Clin J Am Soc Nephrol 7: 466–471, 2012.
326 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

dialysis with a CVC, and a significant proportion beginswithout nephrology care before dialysis initiation. Thefirst 90 days of dialysis remain particularly hazardous.Some patients will not be able to use an AVF created inthe optimal time window before starting dialysis, butmost eventually will. Screening, patient education, andtimely referral to nephrology are generally useful in se-lecting a dialysis modality and improving prospects fortransplantation. Timely creation of vascular access re-mains the Achilles heel of predialysis care. Once pa-tients are on dialysis, structured programs focusing onkey clinical outcomes such as access, nutrition, anemia,and adequacy are beneficial.
Conservative Management of ESRDConservative management of ESRD is increasingly
considered to be an option for patients with ESRD be-cause of the increased incidence of older adults andadults with a high comorbid illness burden who de-velopESRD.To pursue conservativemanagement, nephrol-ogists should engage patients using shared decisionmaking. Shared decision-making can limit the numberof patients who subsequently withdraw from dialysissoon after initiation and increase the number of pa-tients who plan for conservative management (9).
Decisions for conservative management of ESRDhave been studied from the perspective of the nephrol-ogy specialist and from the patient. In 2010, the ne-phrology perspective was examined through a surveydistributed across 11 European countries (10). Conser-vative management was offered to 10% of patients,and the most important factors that influenced phy-sicians’ decisions were patient preference (93%), pres-ence of severe comorbidities (93%), presence of vasculardementia (84%), and low functional status of the patient(75%). In cases that nephrologists initially intended notto start RRT, 10% of nephrologists indicated that patientpreference for dialysis always changed their decisionin favor of providing dialysis therapy. In an Australianstudy of patients with stage 5 CKD, the most commonreason a patient planned for conservative managementwas patient choice (27%) (11). In this study, 14% of pa-tients opted for conservative management. Characteristicsof patients who planned for conservative managementover dialysis included age .65 years, female sex andabsence of private health insurance. Importantly, 65%of patients evaluated in this study received informationabout conservative management as an option. Patientsmost likely to have received this information were aged
.65 years and who were followed by their nephrolo-gist ,12 months.
In order to effectively inform decision making,recent investigations addressed quality of life (QOL)and survival of patients who receive conservative man-agement. In a single-center prospective UK study, 170patients with stage 4–5 CKD were recruited from 2005to 2007, and this cohort was followed through initiationof dialysis or conservative management (12). The pa-tients’ QOL was assessed with the Short Form-36(SF-36), Hospital Anxiety and Depression Scale andSatisfaction with Life Scale every 3 months. Comparedwith patients who chose dialysis therapy, those whochose conservative management had lower scores inphysical health and higher levels of anxiety at baseline.Depression, global satisfaction with life and mentalhealth scores were similar between these groups atbaseline. Over time, satisfaction with life scores weremaintained in the conservative management group butdeclined in those who initiated dialysis. Compared withdialysis patients, patients who received conservativeman-agement had shorter median survival (913 versus 1317days). Adjusted median survival was 13.2 months shorterin patients receiving conservative management comparedwith HD after adjusting for age, Karnofsky perfor-mance score, comorbidities, physical health score (SF-36), and propensity score. The rate of death was morethan three times greater in patients with high comor-bidity burden than those without.
Transition from Pediatric Care to Adult HealthCare Systems
Causes, consequences, and ramifications of CKDdiffer between the adult and pediatric populations, andit follows that the approaches to care among these pop-ulations should be tailored. The most common causesof CKD in children are hereditary nephropathies andcongenital anomalies of the kidney and urinary tract(13). Despite the substantial morbidities associated withthese illnesses, advances in managing these complexconditions and improvement in access to care have re-sulted in 85%–90% of children with CKD survivinginto adulthood. The number of transplants in childrenwith CKD is increasing, and nearly 38% of pediat-ric patients are transplanted within a year of beinglisted (14).
Adolescence is a vulnerable period in life and isassociated with risk-taking and peer-influenced behav-iors, rebellion against figures of authority, and lack of
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 327

insight; these factors are especially relevant to patientswith CKD. Comorbid psychiatric illness such as de-pression is common in children with CKD and the in-cidence increases with the duration of CKD (15,16).Specifically, adolescents and young adults with CKDexhibit poor adherence with medication and clinicfollow-up, resulting in poor health outcomes andearly loss of renal transplants within 36 months aftertransfer to adult units (17,18). Inadequate informa-tion about illness management, unfamiliarity with theadult-based clinics, and lack of communication betweenadult and pediatric units coupled with medicationnonadherence, CKD-associated cognitive impairments,aging out of health insurance, and a lack of a collegeeducation or employment are presumed as factors as-sociated with poor outcomes after the transition process(19,20).
In order to optimize outcomes and achieve thesuccessful transfer of adolescents and young adults tothe adult services, it is important that this transfer oc-curs after the process of health care transition. Adolescentsand young adults should have detailed understanding oftheir CKD and rationale for medications use, assumeresponsibility for their health care, and acquire theskills necessary to manage their illness, while beingcognizant of the available support services and ways toaccess them. This transfer of responsibility needs to beperformed at a measured pace and should be individ-ualized. Adult nephrologists need to have expertise inthe management of CKD that results from conditionsuniquely prevalent in childhood such as congenitalrenal anomalies. Several consensus statements wererecently published on the subject of this transition;however, because of the dearth of evidence, many ofthese recommendations are opinion based (21,22). TheInternational Pediatric Nephrology Association (IPNA)issued a consensus statement outlining the responsibil-ities of health care providers and patients. This includesthe identification of “transition champions” in thepediatric and adult services who have the requisite ex-pertise in educating and providing support to the ado-lescent to master disease self-management (21). Healthcare transition process tools were recently developedto evaluate and objectively measure transition readi-ness (23,24). However, these tools have yet to be validatedin large clinical settings. Currently, the IPNA consensusstatement remains the most comprehensive document,outlining steps necessary to ensure a successful transitionprocess; thus, these guidelines need to be implemented as
best practice guidance until more empirical data andlong-term outcomes are available.
Transition to End-of-Life Care in ESRDTransition to end-of-life (EOL) care and the with-
drawal of dialysis should involve shared decision mak-ing for patients who experience clinical deteriorationand poor QOL. Schmidt and colleagues outlined anobjective approach to manage the withdrawal of dial-ysis, a process that included an assessment of decision-making capacity and an understanding of the clinicalsituation and consequences of treatment discontinuation(25). These authors suggested that patients for whomwithdrawal discussions should be considered includeindividuals with frequent hospitalizations, impairmentof physical function, failure to thrive, nonrenal terminalillnesses, and severe depression. Advanced care planningat the onset of dialysis therapy was also recommendedto assist patients in expressing their goals of care andconsidering how those goals would change if they ex-perienced clinical deterioration (26).
Several studies have examined characteristics of pa-tients who undergo dialysis withdrawal. A large obser-vational study using the Australia and New ZealandDialysis and Transplant Registry (ANZDATA) from1999 to 2008 identified the following risk factors fordialysis withdrawal: older age, female sex, white race,late referral to nephrologist, HD use, increasing numberof comorbid conditions, and diabetes (27). In a USRDSstudy, black patients were 37%–53% less likely to un-dergo dialysis discontinuation than whites, and theserates varied by geographic areas of high versus low uti-lization of EOL services (28). A large Canadian studyof 46,181 incident dialysis patients between 2001 and2009 examined whether older age or higher eGFR atdialysis initiation (.10.5 ml/min per 1.73 m2) was as-sociated with dialysis withdrawal rates (7). The studyrevealed that these two factors were associated not onlywith dialysis withdrawal, but were also associated withshorter time to dialysis withdrawal. Finally, a study of6415 hemodialysis patients identified that higher de-pression scores in the first 3 months of dialysis initiationwere associated with a faster rate of dialysis withdrawalwithin a year compared with patients who lackedsymptoms of depression (29).
New evidence reveals the expected clinical courseof patients who withdraw from dialysis. A large mul-tisite study of 10 hospice units across the United Statesexamined the survival after discontinuation from dialysis
328 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

and hospice admission. The average length of survivalafter hospice admission was 7.4 days (range, 0–40days) (30). Clinical characteristics independently asso-ciated with earlier death include male sex, referral afteran acute hospitalization, lower functional status, pe-ripheral edema, and need for supplemental oxygen.
There are no established methods for measur-ing the quality of care at the EOL in ESRD. Europeaninvestigators designed a list of potential quality in-dicators and assessed EOL care in dialysis patientswho were dying in the hospital setting (31). This meth-odology gathered information about resuscitation at-tempts, the documentation of a “Do Not Resuscitate”order, details of the patient’s care plan, involvement ofpalliative care specialists, effectiveness of symptomman-agement, and quality of death. Less than one third(28%) of these patients discussed EOL care with theirnephrologist within the year before their death. Only64% of patients had a discussion about dying during thehospital admission. These findings serve to identifyareas for improvement in EOL care for nephrologistsand for patients.
Recent studies highlight barriers and solutions toeffective EOL care. One barrier to effectively transitionpatients to EOL care is communication skills. Com-monly, nephrologists do not receive training in com-munication skills to lead EOL discussions. One toolthat could help improve these skills is NephroTalk,a workshop of communication scenarios focused ondelivering bad news and discussing goals of care withpatients (32). In pilot studies, NephroTalk appears toenhance physician preparedness for leading difficultconversations. Another barrier to effective EOL careis fragmented care delivery between nephrology andpalliative care services. The influence of this barrier isevidenced by the fact that hospice services are rarelyenacted by patients with ESRD (26). Renal palliativecare should be considered as a gradual and normaltransition throughout the care process of a patient withESRD (33); however, there is no formal standard toguide delivery and assessment of renal palliative care.
Transition from Failed Renal Allograft to DialysisThe patients who initiate dialysis after a kidney
transplant comprise approximately 5% of all incidentdialysis patients, but the total number of patients issteadily increasing (Figure 6) (34). The initiation of dial-ysis in this setting is associated with a 3-fold increasein mortality compared with patients whose allograft
continues to function (35,36). In addition, mortality isincreased compared with transplant-naïve patients whoinitiate dialysis (37). Key issues in the management ofthe failed transplant patients include the following: (1)timing of initiation, (2) question of resection of the failedallograft, and (3) management of immunosuppressivemedications after the patient has started back on dialysis.
Patients who initiate dialysis after a failedkidney transplant comprise 5% of all in-cident dialysis patients in the United States,and the number is steadily increasing.There are no compelling data to suggestthat a patient with a failing transplant shouldbe managed differently from a transplant-naïve patient with CKD with regard to thetiming of dialysis initiation.
Timing of Initiation of Dialysis in the Patient witha Failed Kidney Transplant. Molnar and colleagues(38) studied the dialysis patients in one large dialysisorganization (from July 2001 to June 2006) who werelisted in the Scientific Registry of Transplant Recipi-ents as having kidney allograft failure within 30 daysof the dialysis initiation date. The 747 patients in-cluded in the study were categorized based on eGFR.10.5 ml/min per 1.73 m2 or#10.5 ml/min per 1.73 m2
at the time of dialysis initiation after the allograft wasdeemed to have failed. In this analysis, earlier dialy-sis initiation was associated with male sex, Medicareinsurance (versus other), diabetes, atherosclerotic heartor peripheral vascular disease, lower total iron bindingcapacity, and lower serum phosphorus concentration.In a multivariable model, there was no significant re-lationship between eGFR at dialysis initiation and death.The authors determined a propensity score based onthe likelihood of starting dialysis earlier or later. Thepropensity score–adjusted model also showed no sig-nificant association between initiation eGFR and mor-tality. On subgroup analysis, there was a trend towardhigher mortality when dialysis was started at a highereGFR in the healthiest and youngest patients and amongwomen.
A study from the Dialysis Outcomes and PracticePatterns Study (DOPPS) compared outcomes among2806 transplant-naïve patients on dialysis who were onthe transplant waiting list and 1856 patients who had
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 329
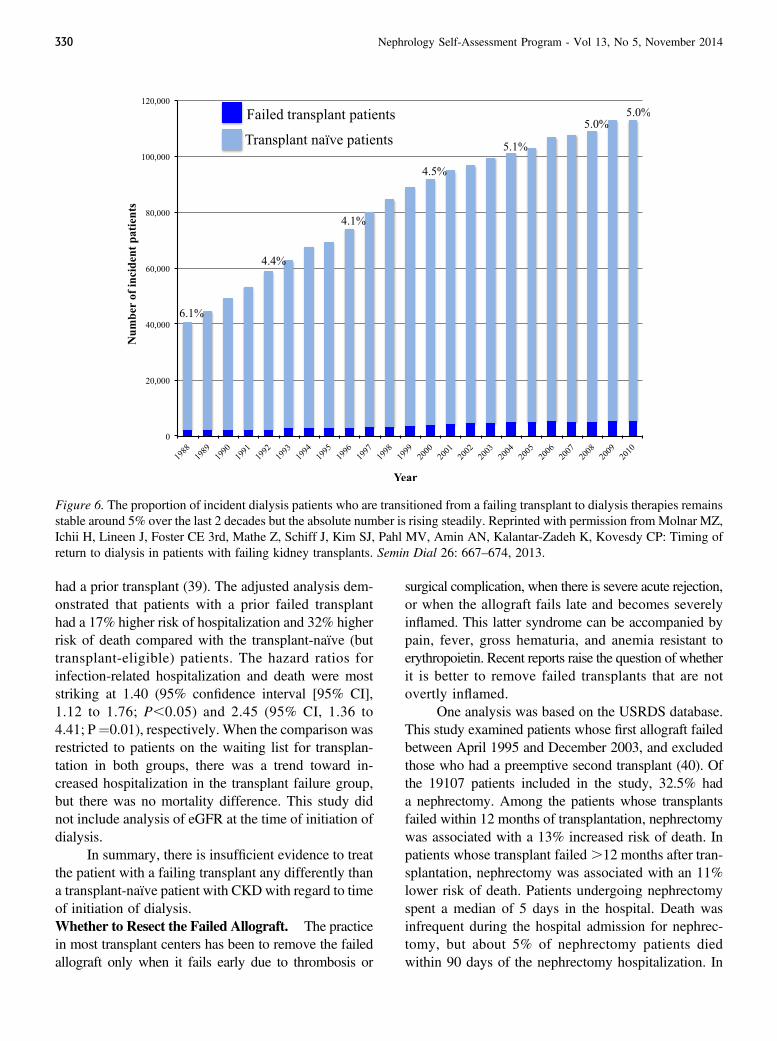
had a prior transplant (39). The adjusted analysis dem-onstrated that patients with a prior failed transplanthad a 17% higher risk of hospitalization and 32% higherrisk of death compared with the transplant-naïve (buttransplant-eligible) patients. The hazard ratios forinfection-related hospitalization and death were moststriking at 1.40 (95% confidence interval [95% CI],1.12 to 1.76; P,0.05) and 2.45 (95% CI, 1.36 to4.41; P¼0.01), respectively. When the comparison wasrestricted to patients on the waiting list for transplan-tation in both groups, there was a trend toward in-creased hospitalization in the transplant failure group,but there was no mortality difference. This study didnot include analysis of eGFR at the time of initiation ofdialysis.
In summary, there is insufficient evidence to treatthe patient with a failing transplant any differently thana transplant-naïve patient with CKDwith regard to timeof initiation of dialysis.Whether to Resect the Failed Allograft. The practicein most transplant centers has been to remove the failedallograft only when it fails early due to thrombosis or
surgical complication, when there is severe acute rejection,or when the allograft fails late and becomes severelyinflamed. This latter syndrome can be accompanied bypain, fever, gross hematuria, and anemia resistant toerythropoietin. Recent reports raise the question of whetherit is better to remove failed transplants that are notovertly inflamed.
One analysis was based on the USRDS database.This study examined patients whose first allograft failedbetween April 1995 and December 2003, and excludedthose who had a preemptive second transplant (40). Ofthe 19107 patients included in the study, 32.5% hada nephrectomy. Among the patients whose transplantsfailed within 12 months of transplantation, nephrectomywas associated with a 13% increased risk of death. Inpatients whose transplant failed .12 months after tran-splantation, nephrectomy was associated with an 11%lower risk of death. Patients undergoing nephrectomyspent a median of 5 days in the hospital. Death wasinfrequent during the hospital admission for nephrec-tomy, but about 5% of nephrectomy patients diedwithin 90 days of the nephrectomy hospitalization. In
Figure 6. The proportion of incident dialysis patients who are transitioned from a failing transplant to dialysis therapies remainsstable around 5% over the last 2 decades but the absolute number is rising steadily. Reprinted with permission from Molnar MZ,Ichii H, Lineen J, Foster CE 3rd, Mathe Z, Schiff J, Kim SJ, Pahl MV, Amin AN, Kalantar-Zadeh K, Kovesdy CP: Timing ofreturn to dialysis in patients with failing kidney transplants. Semin Dial 26: 667–674, 2013.
330 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

patients with a panel reactive antibody level ,30%before the first transplant and who received a secondtransplant, the panel reactive antibody levels were sig-nificantly higher in patients whose first transplant wasresected versus those whose kidney remained in place.This was not true for patients more highly sensitizedbefore the first transplant.
Ayus and colleagues analyzed a similar cohort ofpatients (41). This study analyzed a cohort drawn fromthe USRDS registry; of the 10951 patients studied,31.5% had the failed graft resected. Patients in thenephrectomy group were on average 4.6 years youngerthan those whose grafts remained in place, and thesepatients were more likely to be black, female, or anonsmoker; were less likely to have cardiovasculardisease, diabetes, cancer, or chronic obstructive pul-monary disease, and were more likely to be ambulatory.The patients who had a nephrectomy had higher averageserum creatinine and serum albumin values and wereslightly more likely to have received induction immu-nosuppression. Having the allograft resected was asso-ciated with a 32% reduction in the relative rate of deathover an average follow-up of 2.9 years, after adjust-ing for the propensity score for receiving nephrectomyand other potential confounders. The rate of deathwithin 30 days of nephrectomy was 1.5%. Patients whohad a transplant nephrectomy were more than twice aslikely to receive a second transplant as those who didnot undergo nephrectomy.
These studies indicate that patients who receiveallograft nephrectomy after transitioning to dialysis tendto be healthier than non-nephrectomy patients. How-ever, the substantial improvement in survival associatedwith nephrectomy persisted after statistical adjustmentfor imbalances among the groups. The effect of nephrec-tomy on time to retransplantation and survival after retrans-plantation remains unclear.Immunosuppression Management after Failure ofa Kidney Transplant. Infection is a key contributorto the morbidity and mortality of dialysis patients, andimmunosuppressive medications used in transplanta-tion could influence this complication. The decision totaper immunosuppressive medications with a failing kid-ney transplant is not straightforward. Withdrawal ofthe immunosuppression may precipitate a chronic in-flammatory state with anemia resistant to erythropoi-etin and increased cardiovascular risk, or the need fornephrectomy, a procedure with significant mortalityrisk of as high as 1.5% in a recently published large
study (41). Furthermore, reduction in immunosuppres-sion may lead to increased anti-HLA antibody levels,which might delay or prevent retransplantation. Be-cause repeat transplantation is associated with a signif-icant improvement in survival, this is not an issue to betaken lightly (37).
Controlled trials to guide immunosuppressivemanagement after allograft failure are lacking. Mostcenters taper immunosuppression over a period ofmonths unless there is another functioning solid organtransplant in place, repeat transplantation is thoughtto be imminent, or there is significant residual renalfunction.
Geriatric Considerations in ESRDThe number of older adults who initiate dialysis
is increasing, but older patients often have worseclinical outcomes than younger dialysis patients. Forexample, a study of patients aged $75 years from theANZDATA registry revealed a median survival of only2.3 years (42). In multivariable analyses, factors as-sociated with poor survival in this study included age,comorbidity burden, low body mass index, peritonealdialysis, late referral to a nephrologist (defined as ,3months before starting dialysis), and initiation of HDwith catheter-based vascular access. In addition to poorsurvival, older adults with ESRD are at risk for requiringhospitalization at the time of dialysis initiation.
In a study of 125 elderly incident dialysis pa-tients, nearly 75% of patients were hospitalized at leastonce within 2 years of starting dialysis (43). The mostcommon reasons for hospitalization were cardiac(33%) followed by infectious (18%), and gastroin-testinal complications (12%). Hospitalization at thetime of dialysis initiation and use of a vascular accesscatheter were positively associated with risk for hos-pitalization. The issue of risk associated with a CVCmay not seem to be an epiphany. However, whetherthe commonly applied paradigm of “fistula first” holdstrue for octogenarians was recently studied. A USRDScohort of 115,425 incident patients aged.67 years wasanalyzed according to the vascular access at the timeof initiation of HD (44). The vast majority had CVCs(78.4%), followed by AVFs (18.6%), and arteriovenousgrafts (AVGs) (3%). Not surprisingly, patients who hada CVC at the time of initiation of dialysis did poorly. Inthe entire cohort, AVFs were not superior compared withAVGs. In a mortality analysis stratified by age groups,patients who began dialysis with an AVF had improved
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 331
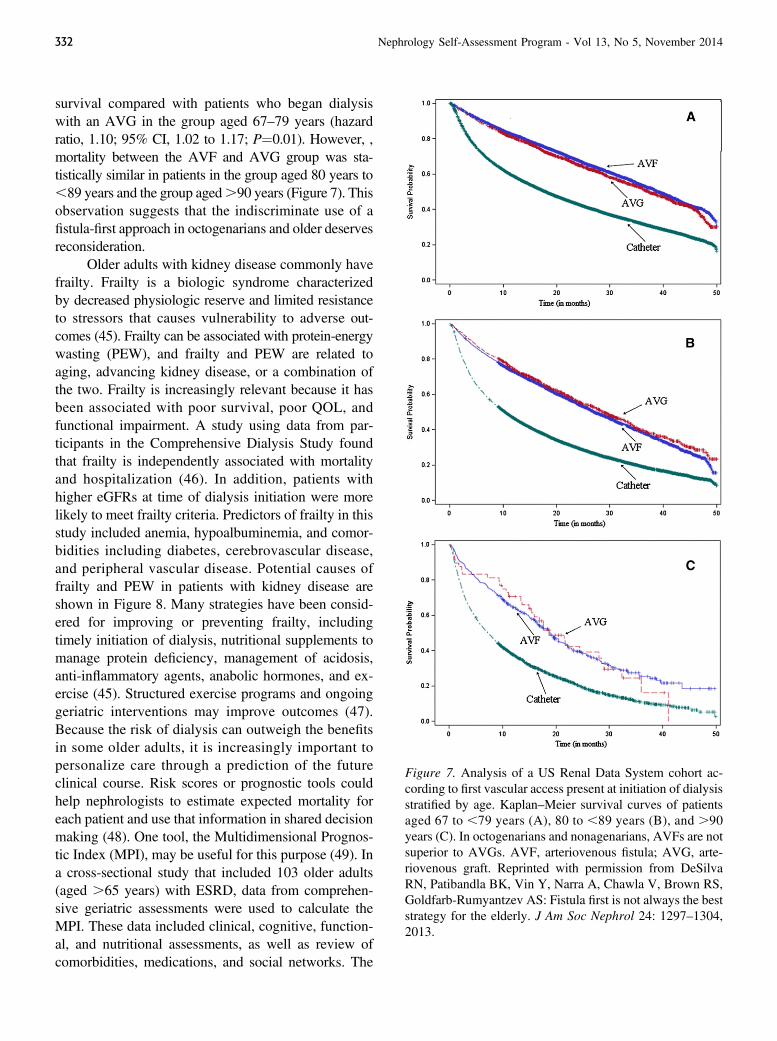
survival compared with patients who began dialysiswith an AVG in the group aged 67–79 years (hazardratio, 1.10; 95% CI, 1.02 to 1.17; P¼0.01). However, ,mortality between the AVF and AVG group was sta-tistically similar in patients in the group aged 80 years to,89 years and the group aged.90 years (Figure 7). Thisobservation suggests that the indiscriminate use of afistula-first approach in octogenarians and older deservesreconsideration.
Older adults with kidney disease commonly havefrailty. Frailty is a biologic syndrome characterizedby decreased physiologic reserve and limited resistanceto stressors that causes vulnerability to adverse out-comes (45). Frailty can be associated with protein-energywasting (PEW), and frailty and PEW are related toaging, advancing kidney disease, or a combination ofthe two. Frailty is increasingly relevant because it hasbeen associated with poor survival, poor QOL, andfunctional impairment. A study using data from par-ticipants in the Comprehensive Dialysis Study foundthat frailty is independently associated with mortalityand hospitalization (46). In addition, patients withhigher eGFRs at time of dialysis initiation were morelikely to meet frailty criteria. Predictors of frailty in thisstudy included anemia, hypoalbuminemia, and comor-bidities including diabetes, cerebrovascular disease,and peripheral vascular disease. Potential causes offrailty and PEW in patients with kidney disease areshown in Figure 8. Many strategies have been consid-ered for improving or preventing frailty, includingtimely initiation of dialysis, nutritional supplements tomanage protein deficiency, management of acidosis,anti-inflammatory agents, anabolic hormones, and ex-ercise (45). Structured exercise programs and ongoinggeriatric interventions may improve outcomes (47).Because the risk of dialysis can outweigh the benefitsin some older adults, it is increasingly important topersonalize care through a prediction of the futureclinical course. Risk scores or prognostic tools couldhelp nephrologists to estimate expected mortality foreach patient and use that information in shared decisionmaking (48). One tool, the Multidimensional Prognos-tic Index (MPI), may be useful for this purpose (49). Ina cross-sectional study that included 103 older adults(aged .65 years) with ESRD, data from comprehen-sive geriatric assessments were used to calculate theMPI. These data included clinical, cognitive, function-al, and nutritional assessments, as well as review ofcomorbidities, medications, and social networks. The
Figure 7. Analysis of a US Renal Data System cohort ac-cording to first vascular access present at initiation of dialysisstratified by age. Kaplan–Meier survival curves of patientsaged 67 to ,79 years (A), 80 to ,89 years (B), and .90years (C). In octogenarians and nonagenarians, AVFs are notsuperior to AVGs. AVF, arteriovenous fistula; AVG, arte-riovenous graft. Reprinted with permission from DeSilvaRN, Patibandla BK, Vin Y, Narra A, Chawla V, Brown RS,Goldfarb-Rumyantzev AS: Fistula first is not always the beststrategy for the elderly. J Am Soc Nephrol 24: 1297–1304,2013.
332 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
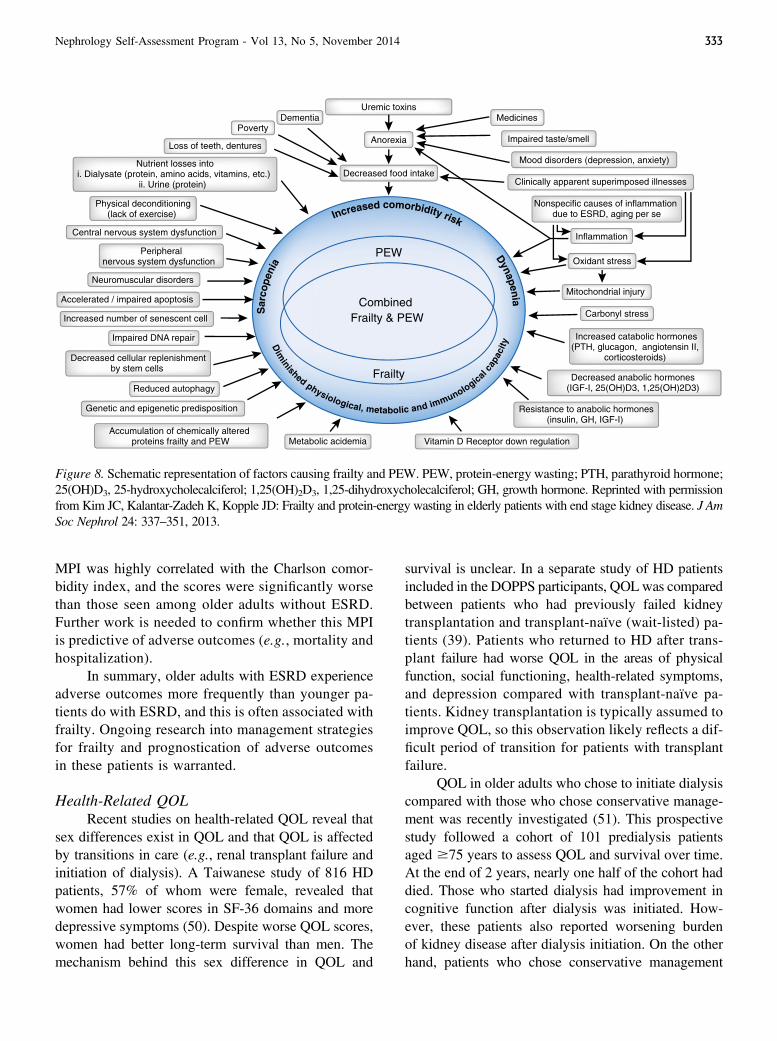
MPI was highly correlated with the Charlson comor-bidity index, and the scores were significantly worsethan those seen among older adults without ESRD.Further work is needed to confirm whether this MPIis predictive of adverse outcomes (e.g., mortality andhospitalization).
In summary, older adults with ESRD experienceadverse outcomes more frequently than younger pa-tients do with ESRD, and this is often associated withfrailty. Ongoing research into management strategiesfor frailty and prognostication of adverse outcomesin these patients is warranted.
Health-Related QOLRecent studies on health-related QOL reveal that
sex differences exist in QOL and that QOL is affectedby transitions in care (e.g., renal transplant failure andinitiation of dialysis). A Taiwanese study of 816 HDpatients, 57% of whom were female, revealed thatwomen had lower scores in SF-36 domains and moredepressive symptoms (50). Despite worse QOL scores,women had better long-term survival than men. Themechanism behind this sex difference in QOL and
survival is unclear. In a separate study of HD patientsincluded in the DOPPS participants, QOLwas comparedbetween patients who had previously failed kidneytransplantation and transplant-naïve (wait-listed) pa-tients (39). Patients who returned to HD after trans-plant failure had worse QOL in the areas of physicalfunction, social functioning, health-related symptoms,and depression compared with transplant-naïve pa-tients. Kidney transplantation is typically assumed toimprove QOL, so this observation likely reflects a dif-ficult period of transition for patients with transplantfailure.
QOL in older adults who chose to initiate dialysiscompared with those who chose conservative manage-ment was recently investigated (51). This prospectivestudy followed a cohort of 101 predialysis patientsaged $75 years to assess QOL and survival over time.At the end of 2 years, nearly one half of the cohort haddied. Those who started dialysis had improvement incognitive function after dialysis was initiated. How-ever, these patients also reported worsening burdenof kidney disease after dialysis initiation. On the otherhand, patients who chose conservative management
Figure 8. Schematic representation of factors causing frailty and PEW. PEW, protein-energy wasting; PTH, parathyroid hormone;25(OH)D3, 25-hydroxycholecalciferol; 1,25(OH)2D3, 1,25-dihydroxycholecalciferol; GH, growth hormone. Reprinted with permissionfrom Kim JC, Kalantar-Zadeh K, Kopple JD: Frailty and protein-energy wasting in elderly patients with end stage kidney disease. J AmSoc Nephrol 24: 337–351, 2013.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 333

had stable physical function and mental function overthe 2 years of observation.
Additional studies evaluated the effect of specificinterventions on QOL in HD patients. With growingevidence on the negative effects of depression on QOLand survival in patients with ESRD, a small, randomizedcrossover trial tested the effect of 3 months of cognitivebehavioral therapy and individual psychotherapy dur-ing hemodialysis treatments in patients with depression(52). Cognitive behavioral therapy improved depres-sion symptoms and QOL in both study groups. Anotherrandomized trial, the Convective Transport Study, ex-amined QOL as a secondary outcome in patients whoreceived either hemodiafiltration or standard low-fluxhemodialysis (53). QOL was not affected by the dial-ysis modality, a result that mirrored the findings fromprior observations on hemodiafiltration and QOL.
Finally, a recent study evaluated whether attain-ing Kidney Disease Outcomes Quality Initiative clin-ical performance targets (e.g., single-pool Kt/V [$1.2],hemoglobin level [11–13 g/dl], vascular access as AVF,phosphorus [2.3–4.5 mg/dl], parathyroid hormone[150–300 pg/ml], and BP [predialysis,140/90 mmHgand postdialysis ,130/80 mmHg]) led to improvedQOL (54). Through a cross-sectional analysis of par-ticipants enrolled in the Convective Transport Study,the investigators found that none of the clinical per-formance targets were associated with better KidneyDisease Quality of Life Short Form responses. In ad-dition, the number of clinical performance targets at-tained (total of six) had no association with higher QOLscores.
Overall, these studies suggest that many dialysis-specific strategies do not significantly affect QOL inhemodialysis patients; however, management of de-pression may be an effective approach to improvingQOL.
References1. US Renal Data System: USRDS 2013 Annual Data Report: Atlas of
Chronic Kidney Disease and End-Stage Renal Disease in the UnitedStates, Bethesda, MD, National Institutes of Health, National Instituteof Diabetes and Digestive and Kidney Diseases, 2013
2. Oliver MJ, Quinn RR, Garg AX, Kim SJ, Wald R, Paterson JM:Likelihood of starting dialysis after incident fistula creation. Clin J AmSoc Nephrol 7: 466–471, 2012 PubMed
3. Song MK, Lin FC, Gilet CA, Arnold RM, Bridgman JC, Ward SE:Patient perspectives on informed decision-making surrounding dialysisinitiation. Nephrol Dial Transplant 28: 2815–2823, 2013
4. Kurella Tamura M, Li S, Chen SC, Cavanaugh KL, Whaley-ConnellAT, McCullough PA, Mehrotra RL: Educational programs improve thepreparation for dialysis and survival of patients with chronic kidneydisease. Kidney Int 85: 686–692, 2014 PubMed
5. Hughes SA, Mendelssohn JG, Tobe SW, McFarlane PA, MendelssohnDC: Factors associated with suboptimal initiation of dialysis despiteearly nephrologist referral. Nephrol Dial Transplant 28: 392–397,2013 PubMed
6. Kidney Disease Improving Global Outcomes (KDIGO) CKD WorkGroup:: KDIGO 2012 Clinical Practice Guideline for the Evaluationand Management of Chronic Kidney Disease. Kidney Int Suppl 3[Suppl]: 1–150, 2013
7. Ellwood AD, Jassal SV, Suri RS, Clark WF, Na Y, Moist LM: Earlydialysis initiation and rates and timing of withdrawal from dialysis inCanada. Clin J Am Soc Nephrol 8: 265–270, 2013 PubMed
8. Wilson SM, Robertson JA, Chen G, Goel P, Benner DA, Krishnan M,Mayne TJ, Nissenson AR: The IMPACT (Incident Management ofPatients, Actions Centered on Treatment) program: A quality improve-ment approach for caring for patients initiating long-term hemodialysis.Am J Kidney Dis 60: 435–443, 2012 PubMed
9. Muthalagappan S, Johansson L, Kong WM, Brown EA: Dialysis orconservative care for frail older patients: Ethics of shared decision-making. Nephrol Dial Transplant 28: 2717–2722, 2013 PubMed
10. van de Luijtgaarden MW, Noordzij M, van Biesen W, Couchoud C,Cancarini G, Bos WJ, Dekker FW, Gorriz JL, Iatrou C, Wanner C,Finne P, Stojceva-Taneva O, Cala S, Stel VS, Tomson C, Jager KJ:Conservative care in Europe–nephrologists’ experience with the de-cision not to start renal replacement therapy. Nephrol Dial Transplant28: 2604–2612, 2013
11. Morton RL, Turner RM, Howard K, Snelling P, Webster AC: Patientswho plan for conservative care rather than dialysis: A national observa-tional study in Australia. Am J Kidney Dis 59: 419–427, 2012 PubMed
12. Da Silva-Gane M,Wellsted D, Greenshields H, Norton S, Chandna SM,Farrington K: Quality of life and survival in patients with advancedkidney failure managed conservatively or by dialysis. Clin J Am SocNephrol 7: 2002–2009, 2012 PubMed
13. Harambat J, van Stralen KJ, Kim JJ, Tizard EJ: Epidemiology of chronickidney disease in children. Pediatr Nephrol 27: 363–373, 2012 PubMed
14. Collins AJ, Foley RN, Chavers B, Gilbertson D, Herzog C, Ishani A,Johansen K, Kasiske BL, Kutner N, Liu J, St Peter W, Guo H, Hu Y,Kats A, Li S, Li S, Maloney J, Roberts T, Skeans M, Snyder J, Solid C,Thompson B, Weinhandl E, Xiong H, Yusuf A, Zaun D, Arko C, ChenSC, Daniels F, Ebben J, Frazier E, Johnson R, Sheets D, Wang X,Forrest B, Berrini D, Constantini E, Everson S, Eggers P, Agodoa L: USRenal Data System 2013 Annual Data Report. Am J Kidney Dis 63[Suppl]: A7, 2014 PubMed
15. Kogon AJ, Vander Stoep A, Weiss NS, Smith J, Flynn JT, McCauley E:Depression and its associated factors in pediatric chronic kidneydisease. Pediatr Nephrol 28: 1855–1861, 2013 PubMed
16. Dobbels F, Ruppar T, De Geest S, Decorte A, Van Damme-LombaertsR, Fine RN: Adherence to the immunosuppressive regimen in pediatrickidney transplant recipients: A systematic review. Pediatr Transplant14: 603–613, 2010 PubMed
17. Watson AR: Non-compliance and transfer from paediatric to adulttransplant unit. Pediatr Nephrol 14: 469–472, 2000 PubMed
18. Harden PN, Walsh G, Bandler N, Bradley S, Lonsdale D, Taylor J,Marks SD: Bridging the gap: An integrated paediatric to adult clinicalservice for young adults with kidney failure.BMJ 344: e3718, 2012 PubMed
19. Groothoff JW, Grootenhuis M, Dommerholt A, Gruppen MP, OffringaM, Heymans HS: Impaired cognition and schooling in adults withend stage renal disease since childhood. Arch Dis Child 87: 380–385,2002 PubMed
20. Andreoni KA, Forbes R, Andreoni RM, Phillips G, Stewart H, Ferris M:Age-related kidney transplant outcomes: Health disparities amplified inadolescence. JAMA Intern Med 173: 1524–1532, 2013 PubMed
21. Watson AR, Harden P, Ferris M, Kerr PG, Mahan J, Ramzy MF:Transition from pediatric to adult renal services: A consensus statementby the International Society of Nephrology (ISN) and the InternationalPediatric Nephrology Association (IPNA). Pediatr Nephrol 26: 1753–1757, 2011 PubMed
334 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
22. Bell LE, Bartosh SM, Davis CL, Dobbels F, Al-Uzri A, Lotstein D,Reiss J, Dharnidharka VR: Adolescent transition to adult care in solidorgan transplantation: A consensus conference report. Am J Transplant8: 2230–2242, 2008 PubMed
23. Ferris ME, Harward DH, Bickford K, Layton JB, Ferris MT, Hogan SL,Gipson DS, McCoy LP, Hooper SR: A clinical tool to measurethe components of health-care transition from pediatric care toadult care: The UNC TR(x)ANSITION scale. Ren Fail 34: 744–753,2012 PubMed
24. Gilleland J, Amaral S, Mee L, Blount R: Getting ready to leave:Transition readiness in adolescent kidney transplant recipients. J PediatrPsychol 37: 85–96, 2012 PubMed
25. Schmidt RJ, Moss AH: Dying on dialysis: The case for a dignifiedwithdrawal. Clin J Am Soc Nephrol 9: 174–180, 2014 PubMed
26. Schell JO, Holley JL: Opportunities to improve end-of-life care inESRD. Clin J Am Soc Nephrol 8: 2028–2030, 2013 PubMed
27. Chan HW, Clayton PA, McDonald SP, Agar JW, Jose MD: Risk factorsfor dialysis withdrawal: An analysis of the Australia and New ZealandDialysis and Transplant (ANZDATA) Registry, 1999-2008. Clin J AmSoc Nephrol 7: 775–781, 2012 PubMed
28. Thomas BA, Rodriguez RA, Boyko EJ, Robinson-Cohen C, FitzpatrickAL, O’Hare AM: Geographic variation in black-white differencesin end-of-life care for patients with ESRD. Clin J Am Soc Nephrol 8:1171–1178, 2013 PubMed
29. Lacson E Jr, Li NC, Guerra-Dean S, Lazarus M, Hakim R, FinkelsteinFO: Depressive symptoms associate with high mortality risk anddialysis withdrawal in incident hemodialysis patients. Nephrol DialTransplant 27: 2921–2928, 2012 PubMed
30. O’Connor NR, Dougherty M, Harris PS, Casarett DJ: Survival afterdialysis discontinuation and hospice enrollment for ESRD. Clin J AmSoc Nephrol 8: 2117–2122, 2013 PubMed
31. McAdoo SP, Brown EA, Chesser AM, Farrington K, Salisbury EM;Pan-Thames Renal Audit Group: Measuring the quality of end of lifemanagement in patients with advanced kidney disease: Results from thePan-Thames Renal Audit Group. Nephrol Dial Transplant 27: 1548–1554, 2012 PubMed
32. Schell JO, Green JA, Tulsky JA, Arnold RM: Communication skillstraining for dialysis decision-making and end-of-life care in nephrology.Clin J Am Soc Nephrol 8: 675–680, 2013 PubMed
33. Davison SN: The ethics of end-of-life care for patients with ESRD. ClinJ Am Soc Nephrol 7: 2049–2057, 2012 PubMed
34. Molnar MZ, Ichii H, Lineen J, Foster CE 3rd, Mathe Z, Schiff J, Kim SJ,Pahl MV, Amin AN, Kalantar-Zadeh K, Kovesdy CP: Timing of returnto dialysis in patients with failing kidney transplants. Semin Dial 26:667–674, 2013 PubMed
35. Kaplan B, Meier-Kriesche HU: Death after graft loss: An important latestudy endpoint in kidney transplantation. Am J Transplant 2: 970–974,2002 PubMed
36. Knoll G, Muirhead N, Trpeski L, Zhu N, Badovinac K: Patient survivalfollowing renal transplant failure in Canada. Am J Transplant 5: 1719–1724, 2005 PubMed
37. Ojo A, Wolfe RA, Agodoa LY, Held PJ, Port FK, Leavey SF, CallardSE, Dickinson DM, Schmouder RL, Leichtman AB: Prognosis afterprimary renal transplant failure and the beneficial effects of repeattransplantation: Multivariate analyses from the United States Renal DataSystem. Transplantation 66: 1651–1659, 1998 PubMed
38. Molnar MZ, Streja E, Kovesdy CP, Hoshino J, Hatamizadeh P,Glassock RJ, Ojo AO, Kalantar-Zadeh K: Estimated glomerularfiltration rate at reinitiation of dialysis and mortality in failed kid-ney transplant recipients. Nephrol Dial Transplant 27: 2913–2921,2012 PubMed
39. Perl J, Zhang J, Gillespie B, Wikström B, Fort J, Hasegawa T, FullerDS, Pisoni RL, Robinson BM, Tentori F: Reduced survival and qualityof life following return to dialysis after transplant failure: The DialysisOutcomes and Practice Patterns Study. Nephrol Dial Transplant 27:4464–4472, 2012 PubMed
40. Johnston O, Rose C, Landsberg D, Gourlay WA, Gill JS: Nephrectomyafter transplant failure: Current practice and outcomes. Am J Transplant7: 1961–1967, 2007 PubMed
41. Ayus JC, Achinger SG, Lee S, Sayegh MH, Go AS: Transplantnephrectomy improves survival following a failed renal allograft. JAm Soc Nephrol 21: 374–380, 2010 PubMed
42. Foote C, Ninomiya T, Gallagher M, Perkovic V, Cass A, McDonald SP,Jardine M: Survival of elderly dialysis patients is predicted by bothpatient and practice characteristics. Nephrol Dial Transplant 27: 3581–3587, 2012 PubMed
43. Schoonover KL, Hickson LJ, Norby SM, Hogan MC, Chaudhary S,Albright RC Jr, Dillon JJ, McCarthy JT, Williams AW: Risk factors forhospitalization among older, incident haemodialysis patients. Nephrol-ogy (Carlton) 18: 712–717, 2013 PubMed
44. DeSilva RN, Patibandla BK, Vin Y, Narra A, Chawla V, Brown RS,Goldfarb-Rumyantzev AS: Fistula first is not always the best strategyfor the elderly. J Am Soc Nephrol 24: 1297–1304, 2013 PubMed
45. Kim JC, Kalantar-Zadeh K, Kopple JD: Frailty and protein-energywasting in elderly patients with end stage kidney disease. J Am SocNephrol 24: 337–351, 2013 PubMed
46. Bao Y, Dalrymple L, Chertow GM, Kaysen GA, Johansen KL: Frailty,dialysis initiation, and mortality in end-stage renal disease. Arch InternMed 172: 1071–1077, 2012 PubMed
47. Ko FC: The clinical care of frail, older adults. Clin Geriatr Med 27: 89–100, 2011 PubMed
48. Kooman JP, Cornelis T, van der Sande FM, Leunissen KM: Renalreplacement therapy in geriatric end-stage renal disease patients: Aclinical approach. Blood Purif 33: 171–176, 2012 PubMed
49. Aucella F, Stoico L, Cicchella A, Gesuete A, Greco A, GrandalianoG, Pilotto A: Comprehensive geriatric assessment in the hemo-dialysis elderly population. J Nephrol 25[Suppl 19]: S85–S89,2012 PubMed
50. Peng YS, Huang JW, Hung KY, Lin BS, Lin CY, Yang CS, Chen TW,Hsia CC, Chen DL, Hsu WD, Chang CF, Wu KD, Lin RP, Tsai TJ,Chen WY: Women on hemodialysis have lower self-reported health-related quality of life scores but better survival than men. J Nephrol 26:366–374, 2013 PubMed
51. Seow YY, Cheung YB, Qu LM, Yee AC: Trajectory of quality of lifefor poor prognosis stage 5D chronic kidney disease with and withoutdialysis. Am J Nephrol 37: 231–238, 2013 PubMed
52. Cukor D, Ver Halen N, Asher DR, Coplan JD, Weedon J, Wyka KE,Saggi SJ, Kimmel PL: Psychosocial intervention improves depression,quality of life, and fluid adherence in hemodialysis. J Am Soc Nephrol25: 196–206, 2014 PubMed
53. Mazairac AH, de Wit GA, Grooteman MP, Penne EL, van der WeerdNC, den Hoedt CH, Lévesque R, van den Dorpel MA, Nubé MJ, terWee PM, Bots ML, Blankestijn PJ; CONTRAST Investigators: Effectof hemodiafiltration on quality of life over time. Clin J Am Soc Nephrol8: 82–89, 2013 PubMed
54. Mazairac AH, de Wit GA, Grooteman MP, Penne EL, van der WeerdNC, den Hoedt CH, Lévesque R, van den Dorpel MA, Nubé MJ,Ter Wee PM, Blankestijn PJ, Bots ML: Clinical performance targetsand quality of life in hemodialysis patients. Blood Purif 33: 73–79,2012 PubMed
In-Center Hemodialysis
Determinants of Dialysis Dose, Duration, andSchedule
Most clinical nephrologists would adopt as axi-omatic that better clinical outcomes will follow fromincreased frequency or longer duration of hemodialysis(HD) in their ESRD patients. However, widespread
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 335

use of prolonged and/or frequent HD is restricted bypatient resistance and by financial constraints. In theNational Cooperative Dialysis Study performed in the1980s, the duration of HD sessions was rejected as amajor determinant of outcome. Yet more recent ob-servations suggest that longer HD treatment times willimprove patient survival. Volume removal and ultra-filtration rate (UFR) are closely integrated with dialy-sis duration. In addition, questions continue to surfaceregarding frequency of HD treatments and the appro-priate measurement of dialysis dose. New literature isbeginning to fill gaps in our understanding regardingthe optimal application of HD.Ascertainment of Dialysis Clearance. Traditionally,the dose of HD is based on urea clearance scaled to thevolume of distribution of urea or total body water (V). Ithas been unclear whether this method applies equally inmale and female patients. One study addressed whetherbody surface area might be a more reliable determinantof dialysis dose than total body water (1). Using a cohortof prevalent hemodialysis patients in the Medicaredatabase, Ramirez and coworkers (1) found that therewas no associated survival benefit associated with single-pool Kt/V .1.7, but the hazard ratio (HR) for mortalitywas progressively lower with higher Kt/Vs if the Kt/Vvalues were normalized for body surface area. This studysuggests that traditional V-based calculations of dialysisdose may result in inadequate HD, particularly in womenundergoing hemodialysis.
Another potential shortcoming of Kt/V-baseddosing of HD was described in a post hoc analysisfrom the Hemodialysis (HEMO) study. McCauslandand coworkers described that HEMO participants whowere randomized to the higher Kt/V goal (targeted to anequilibrated Kt/V of 1.45) were more likely to developintradialytic hypotension compared with those patientsassigned the usual Kt/V goal (eKt/V of 1.05; 18.3%versus 16.8%; P,0.001) (2). The observed differencemay have resulted from the constraints of the HEMOprotocol and also seemed to contrast with the originalintention-to-treat analyses, which demonstrated no ad-vantage to assignment to the higher Kt/V comparedwith usual Kt/V.Frequency of HD Treatments. Past observations havesuggested that provision of daily HD is associated withimproved surrogate clinical outcomes. As reviewed inthe prior issue of NephSAP on ESRD and dialysis, theFrequent Hemodialysis Network (FHN) performed twoprospective randomized trials to examine the effects of
“higher-dose” hemodialysis compared with convention-ally dosed HD. Details of the FHN trials are reviewed inthe section on “Advances in Dialysis Methodology” inthis NephSAP issue.
In contrast with the experience in the FHN trials,one publication from the Dialysis Outcomes and Prac-tice Patterns Study (DOPPS) data explored the otherextreme in HD frequency. Bieber and coworkers re-viewed characteristics of patients in China who re-ceived two (compared with three) HD treatments perweek (3). In stark contrast with other DOPPS countries,twice-weekly therapies were prescribed for 26% ofHD patients in China. Compared with patients di-alyzing three times weekly, patients dialyzed twiceper week in this study were much more likely to beprescribed sessions in excess of 4 hours, yet receivednearly 4 hours less dialysis time per week. The pa-tients dialyzing twice weekly had similar prescrip-tions for erythropoiesis-stimulating agents (ESAs),but were less likely to be prescribed intravenous iron,vitamin D, or a phosphate binder. Whether these dif-ferences were attributable to the frequency of dialysiswas unclear, because the twice-weekly patients alsohad lower socioeconomic status and less health in-surance coverage than their thrice-weekly counter-parts. The authors noted that the limited hemodialysisregimen did not associate with a substantial differencein the quality of life, as captured on the Short Form-12 instrument for assessing physical and mental well-being. Differences in survival for the patients receivingtwo as opposed to three HD treatments per week werenot addressed.Duration of Hemodialysis Treatments. The trends induration of prescribed treatments in the United Stateshave varied over the past decade, perhaps reflectinga lack of conviction about the ideal delivery of HD.The average treatment time peaked in 2006 in theUnited States at 221.9 minutes; however, in 2011, thisvalue had decreased to 217 minutes, the lowest forall participating DOPPS countries (4,5). In a post hocanalysis of the 150 participants in the Dry-WeightReduction in Hypertensive Hemodialysis Patients trial,it was reported that fewer hours of dialysis treatmentwas associated with higher systolic BP, increased pre-scription of antihypertensive medications and a greaterlag time to achieve a lower BP target (6). In a detailedanalysis of the DOPPS participants, longer treatmenttimes were associated with values usually considered tobe favorable, including higher hemoglobin and serum
336 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

albumin concentrations as well as with lower whiteblood cell counts and serum phosphorus concentrations(4). Analyzing results submitted by the countries par-ticipating in DOPPS from 1996 to 2008, every increasein dialysis treatment time of 30 minutes was associatedwith a decrease in all-cause mortality of 6% (4).
A unique study from one of the large dialysisproviders in the United States compared outcomes forpatients who were treated with in-center, nocturnal HDversus conventional thrice-weekly HD (7). In this study,746 nocturnal patients were compared with 2062 pro-pensity score–matched controls. Patients were main-tained in the nocturnal regimen for a median of 401 days,and data were collected for up to 2 years. Nocturnal HDpatients displayed more favorable measurements forinterdialytic weight gain (IDWG), serum albumin con-centration, UFR, systolic BP, serum phosphorus con-centration, and white blood cell count compared with thematched controls. After adjustment for age, body massindex, and dialysis vintage, nocturnal HD was associatedwith a 25% reduction in the risk for death (HR, 0.75; 95%confidence interval [95% CI], 0.61 to 0.91; P¼0.004).Importantly, however, among the active dialysis patientsin the cohort, only 42% of patients remained on thenocturnal regimen after 2 years.Ultrafiltration and Rate of Fluid Removal. Shorterdialysis treatment duration and larger IDWG are as-sociated with increased mortality in maintenance HDpatients (8). However, the relative contribution of eachof these factors along is not clear. Flythe and col-leagues reviewed clinical outcomes from a cohort of.14,000 prevalent HD patients (9). The study ex-cluded patients who had achieved inadequate Kt/V,and it also excluded patients who received ,150 or.270 minutes of treatment time. The analysis com-pared outcomes in high versus low weight gainers(IDWG .3 kg versus #3 kg) and for long versusshorter treatment times (,240 versus $240 minutes),while adjusting for sex, age, vascular access type,and postdialysis weight. This analysis demonstrated a32% increased mortality risk in patients prescribed,240 minutes (compared with those prescribed $240minutes) and a 29% increased mortality risk associatedwith higher compared with lower IDWG. In a similarand related observational study, HD patients prescribeda treatment time ,240 minutes had a 26% increasedrisk of mortality compared with those prescribed$240 minutes (10). This latter analysis excluded thefew patients prescribed ,2.5 or .4.5 hours. Regard-
less, for the patients included in the analysis, the positiveassociation with patient survival was observed across alltertiles of treatment times.
In addition to modifying the dialysis treatmenttime, clinicians certainly realize the importance of in-terventions to minimize IDWG. Reasonable goals thatmight reduce IDWG include minimizing interdialyticsodium and fluid intake and achieving adequate gly-cemic control in patients with diabetes. Because dietand adherence occur for the most part when the patientis out of the clinic, control of IDWG is seemingly outof the control of clinicians. A recent, randomized con-trolled trial evaluated the effect of cognitive behavioraltherapy in patients with a depressed affect (11). Theintervention was done at chairside in the dialysis fa-cility for 3 months. During the intervention, behavioraltherapy was shown to reduce IDWG (D21.2% kg/d;SD 0.2; P,0.001), but this benefit dissipated after 6months. This type of intervention would seem to bewithin the reach of the dialysis clinician.
These recent studies highlight the controversythat persists with regard to the ideal method to replacerenal function in ESRD patients using HD. Purists willawait definitive prospective, randomized controlledclinical trials, but other sources of information, includ-ing the publications reviewed above, suggest that weshould reconsider the duration of prescribed therapies(12). Interestingly, one recent publication suggests thata formal program of physician education can significantlyimprove hemodynamic stability in HD patients (13).Thus, new conclusions and recommendations regardingHD prescriptions can feasibly be applied and may resultin near-immediate improvement in clinical outcomes.
Anemia ManagementErythropoietin. Management of CKD-related anemiahas changed dramatically over the past several decades.Introduction of epoetin-alfa (EPO) in the late 1980sradically reduced the need for red blood cell trans-fusions and limited exposure to blood-borne infectionsand immune sensitization. However, after the nadir forblood transfusions in the mid-2000s, lower hemoglo-bin targets have recently resulted in a slight increase intherapeutic blood transfusions (14). Many of the largeclinical trials involving the use of ESAs and investi-gating target hemoglobin concentrations were summa-rized in a previous issue of NephSAP.
The novel ESA peginesatide was examined in recentclinical trials. The Efficacy and Safety of Peginesatide
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 337

for the Maintenance Treatment of Anemia in Patientswith Chronic Renal Failure Who Were Receiving He-modialysis and Were Previously Treated with Epoetin(EMERALD 1 and 2) examined effects of peginesatidein HD patients already on continuous erythropoietintreatment for at least 8 weeks (15). In the EMERALD 1study, 803 patients underwent randomization at 92 sitesin the United States. In the EMERALD 2 study, 823patients underwent randomization at 39 sites in theUnited States and 47 sites in Europe. Eligible patientswere randomized to receive peginesatide every 4 weeksor to continue on erythropoietin. Patients received in-travenous ESAs in EMERALD 1 and intravenous orsubcutaneous ESAs in EMERALD 2. The primary endpoint for the studies was the mean change in hemoglo-bin from the baseline through the evaluation period. Inboth studies, the prespecified noninferiority criterionwas met. In addition, the proportion of patients receiv-ing a transfusion was similar in the two treatment groups:10.3% in the peginesatide group and 8.6% in the eryth-ropoietin group in the EMERALD 1 study, and 7.7% and9.9% in the two groups, respectively, in the EMERALD2 study. Serious adverse events were reported in 572 pa-tients (53.7%) in the peginesatide group and 309 (57.0%)in the erythropoietin group. This experience promptedapproval of peginesatide by the US Food and Drug Ad-ministration. However, the agency reported the voluntarywithdrawal of peginesatide soon thereafter because ofreports of serious hypersensitivity reactions. Fatal reac-tions were reported in approximately 0.02% of patientsafter the first dose of intravenous administration. Theprevalence of hypersensitivity reactions was approxi-mately 0.2% after 25,000 patients received the drug.
Current practice guidelines recommend usingESAs to avoid hemoglobin decreases ,9 g/dl and toavoid administering ESAs when the hemoglobin con-centration is .10 g/dl (16). These guidelines acknowl-edge that patient quality of life may be improved, insome instances, by dosing ESAs to higher target hemo-globin concentrations. Coyne and colleagues comparedthe quality of life from the Normal Hematocrit Trial(NHT) in the Amgen Clinical Trial Report (ACTR)(17). The NHT trial was terminated early in 1998 dueto a reported increased risk of adverse events in thenormalization arm (hemoglobin target of 13–15 g/dl).Interestingly, the physical function score on the quality-of-life questionnaire after 12 months in the trial in-creased by 0.6 point for each percentage-point increasein the hematocrit (P¼0.03). This contrasted with data
collected in the ACTR, in which the 12-month physicalfunction score was 35.0627.3 in the high arm and35.0627.5 in the low arm, a nonsignificant difference.Although this study did not address adverse effects onquality of life with severe anemia, the ACTR analysisfailed to demonstrate that high hematocrits would furtherimprove patient perceptions of quality of life.Response and Resistance to Erythropoietin. Inflam-mation, nutritional status, hyperparathyroidism, anddrug-induced hemolytic anemia are known to influenceresponsiveness to ESAs (18). Poor response to erythro-poietin also occurs in the setting of malnutrition andsystemic inflammation (19). In a post hoc analysis ofthe FHN trials, Ornt and colleagues evaluated theeffect of frequent HD on anemia management (20). Inthis study, there was no significant treatment effect ofmore frequent HD treatments on ESA dose in eitherthe frequent daily treatments or the nocturnal treatmentscompared with a conventional thrice-weekly schedule.Furthermore, there was no treatment effect on the totalmonthly dose of intravenous iron administered to par-ticipants in the daily HD trial. In the FHN trial, patientsin the six-times-per-week nocturnal treatment arm re-ceived lower amounts of intravenous iron at month 12compared with the conventional group. There was notreatment effect on serum ferritin levels or transferrinsaturation in either trial. Although the FHN programsincluded high-flux HD membranes, follow-up studiesdetermined that these dialyzers do not have a discernibleeffect on ESA dosing or hemoglobin levels comparedwith low-flux dialysis membranes (21).
Responsiveness to ESA has been postulated to bepartially dictated by the adequacy of carnitine stores.Carnitine participates in the remodeling of the erythrocyteplasma membrane, stimulates erythropoiesis, and pro-longs erythrocyte survival in some settings. Carnitine isalso cleared by dialysis; therefore, ESRD patients are atincreased risk for carnitine depletion. In a prospectiverandomized placebo-controlled trial, Mercadal and col-leagues examined whether carnitine (1 g intravenously ateach HD session) would modify the ESA requirementcompared with placebo administration (22). The studyinvolved 92 incident patients, and the primary outcomemeasure was the erythropoietin resistance index (EPO-RI)defined as the mean weekly EPO dose (monthly dose asinternational units per kilogram body weight) dividedby hemoglobin (g/dl). After 1 year, the EPO-RI im-proved in both groups and the mean was not sig-nificantly different between the groups. The plasma
338 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

free carnitine concentration increased in the treatmentgroup and decreased in the placebo group. This studydemonstrated that carnitine replacement is safe in HDpatients, but routine carnitine replacement does notimprove responsiveness to ESAs.Supplementation of Iron. Concomitant with reducedhemoglobin level targets and a shift in the paymentpolicy in the United States, practice patterns for thesupplementation of iron in HD patients are evolving.The prevalence of intravenous iron use was 50% in1999 and increased to 71% in 2009–2011 for the 12countries participating in the DOPPS study (23). In theUnited States, the prevalence of iron use increased from64% in 2002 to 76% in 2008, and the mean quarterlyiron dose increased from 500 mg in 2002 to 650 mg in2008 (24). Several studies explored whether these trendsresulted in improved control of CKD-related anemia. Inthe Heme Iron Polypeptide against Treatment with OralControlled Release Iron Tablets (HEMATOCRIT) trial,the efficacy of oral heme iron polypeptide (HIP) wasreported (25). The novelty of HIP is that it containsa highly soluble heme moiety that contains .1% iron.In this study, PD patients taking darbepoetin alfa for atleast 1 month were randomized to receive oral iron inthe form of either HIP (one capsule twice daily, equiv-alent to 240 mg elemental iron daily) or slow-releaseferrous sulfate (one capsule twice daily, equivalent to210 mg elemental iron daily). The primary outcome wastransferrin saturation (TSAT) after 6 months of treat-ment. There was no significant difference in TSATvalues between the HIP and control groups at any timepoint in the intention-to-treat population. This experi-ence suggests that HIP is a suitable and effective form oforal iron repletion.
Kshirsagar and colleagues examined the effective-ness of different iron dosing strategies (26). The authorscompared a high-dose intravenous iron regimen (.200mg of iron in 1 month) versus a low-dose intravenousiron strategy (,200 mg of iron in 1 month) and a bolusregimen (100 mg intravenous iron on two consecutivedialysis sessions) versus a maintenance intravenous ironregimen. The study used US Renal Data System(USRDS) data to compare results from 117,050 preva-lent HD patients. The authors determined that bolus irondosing was associated with higher average adjustedhemoglobin (10.23 g/dl; 95% CI, 0.21 to 0.26), TSAT(13.31%; 95% CI, 2.99 to 3.63), and serum ferritin(1151mg/L; 95% CI, 134.9 to 168.7), and lower averageerythropoietin dose (2464 U; 95%CI,2583 to2343 U)
compared with maintenance dosing. Similar trends wereobservedwith high-dose versus low-dose iron. This analysisalso suggested that iron sucrose use was associated witha slightly higher hemoglobin concentration comparedwith ferric gluconate.
Questions about intravenous iron protocols alsopersist with regard to safety. Exposure to large amountsof intravenous iron may oversaturate transferrin andrelease free iron into the circulation. Free iron is capableof promoting bacterial growth, at least in vitro; thus, ironhas the potential to aggravate an existing infection.Furthermore, free iron is thought to impair host defenseby decreasing PMN function. To address the safety ofintravenous iron, Brookhart and coworkers carried outa retrospective cohort study of 117,050 HD patients (27).Comparing bolus intravenous iron dosing with mainte-nance intravenous iron dosing, the authors determinedthat the risk of infection was higher in patients who hadreceived bolus iron dosing compared with those who hadreceived maintenance iron dosing (HR, 1.08; 95% CI,1.05 to 1.11) for infection-related hospitalization andinfection-related hospitalization or death. These studiesconfirm that aggressive supplementation of iron is as-sociated with reduced ESA requirement, but cliniciansneed to be aware that one of the potential consequencesof this practice is a slight increase in the risk of infection.
Determination of Target Weight: Bioimpedanceand Other Methods
Volume management and attainment of dry weightwith ultrafiltration are major variables in treatment ofHD patients. Chronic volume overload leads to hyper-tension, left ventricular hypertrophy, cardiac remodeling,and increased cardiovascular morbidity and mortality.However, volume depletion also has deleterious con-sequences such as intradialytic hypotension, end-organhypoperfusion, postdialysis weakness and fatigue, increasedrisk for falls, vascular access thrombosis, and mortality.It is therefore crucial to accurately assess and maintainthe optimal volume status of a HD patient.
Clinicians often determine a patient’s dry weightusing trial and error, or “symptom probing,” adjusting thetarget weight and monitoring the patient during and af-ter the dialysis procedure. This practice may lead to anincreased number of intradialytic events and morbidity.In addition, there is a subset of patients with volume-independent hypertension (28). At the other extreme, in-sufficient removal of fluid can encumber the cardiovascularsystem and increase patient risk. Defining and attaining
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 339

the correct dry weight is therefore important to improvemorbidity and mortality in the dialysis population.
Noninvasive tools can potentially provide objectiveinformation in the assessment of dry weight prescription.These tools include inferior vena cava diameter asses-sment, chest ultrasonography, echocardiography, bio-markers such as atrial and B-natriuretic peptides, andmore recently, blood volume monitoring (BVM) andbioimpedance analysis (BIA). None of these tools arecurrently widely used today in clinical practice, andthere may not be a suitable replacement for a systematicapproach that merges the physical examination, symp-toms, and imaging data. Increased levels of predialysisatrial natriuretic peptide have been found to correlatewith hypervolemia, but postdialysis levels are not a re-liable indicator of euvolemia (29). Vasko and coworkersrecently demonstrated that clinical judgment may still bethe single most important component of volume assess-ment (30). Nonetheless, recent investigations are explor-ing new methods of determining volume status.Bioimpedance. Bioimpedance spectroscopy (BIS) is apotentially useful tool for objective measurement of ex-tracellular volume excess and dry weight. Multifrequencybioimpedance is a technique that passes low-strength al-ternating current at various frequencies (5–1000 kHz)through the skin. Low-frequency current will preferentiallypass through the extracellular fluid space due to its inabil-ity to penetrate cell membranes, whereas high-frequencycurrent can penetrate the extracellular and intracellularspace. By measuring resistance across a spectrum offrequencies and comparing these values with normativevalues in nonuremic patients, total body water, intracellularfluid, and extracellular fluid can be quantified in dialysispatients (31). This technique can accurately measureextracellular volume, and the procedure compares favor-ably with methods such as deuterium oxide, bromidedilution, and total body potassium, classically consideredthe gold standards for quantifying volume (31). BIA canbe performed with whole-body measurements or withsegmental measurements using the calf. The simplicity,relatively low cost, and ability to perform these measure-ments at the bedside make bioimpedance an attractive tool.
Several studies evaluated the use of BIS-guidedfluid management in dialysis. In a prospective analysisof 55 HD patients over 3 months, whole-body BISmonitoring was performed weekly before dialysis, andthese determinations were used to determine weeklytime-averaged fluid overload (TAFO) (32). The TAFOwas projected to account for fluctuations in volume
status in the predialytic, postdialytic, and interdialyticperiods, thus representing the weekly average fluid load.On the basis of BIS measurements, this study showedthat 31% patients were volume overloaded, 47% werenormovolemic, and 22% volume depleted at baseline.Using the measured weekly TAFO, protocol-based ad-justments were made to postdialysis target weights toachieve a TAFO of 0.5 liters. Target dry weight was de-creased if TAFO exceeded 0.5 liters, was not changedif TAFO was at goal, and was increased in volume-depleted patients if the TAFO was ,0.25 liters. Usingthis strategy, TAFO was decreased by 1.2061.32 liters(P,0.01) in the overloaded group, remained unchangedin the normovolemic group, and increased by 0.5960.76liters (P¼0.02) in the volume-depleted group. Thechanges made to dry weight prescriptions did not causean increase in intradialytic events, and every 1-liter changein TAFO was accompanied by a parallel 9.9-mmHgchange in predialysis systolic BP (P,0.001).
Similar findings have been shown in other studiesof BIS-guided fluid management. Hur and colleaguesperformed a randomized controlled trial in 156 dialysispatients comparing whole-body bioimpedance-basedvolume management with conventional therapy (33).The bioimpedance group received BIA twice monthly,and this measurement was used to adjust the targetpostdialysis weight. The goal in the BIA-managed pa-tients was to achieve a TAFO of 0 liters of excess ex-tracellular fluid, which is a measurement that is similar towhat is found in healthy individuals. The control groupreceived standard volume management and dry weightassignment based on the assessment of the roundingclinicians. After 12 months, the intervention grouphad a decrease in TAFO of 20.5 liters (95% CI,20.8 to20.2; P¼0.001) and a significant decrease in left ventric-ular mass index of 10.2 g/m2 (95% CI, 219.2 to 21.17;P¼0.04) compared with the control group. In addition, thebioimpedance group had decreased arterial stiffness andlower BP, with no increase in episodes of intradialytichypotension. It is worth noting that the intervention groupdid have an increased rate in the development of anuria,perhaps due to aggressive volume removal.Blood Volume Monitoring. Online BVM is a clini-cally available tool used to assess relative blood volume.Plasma volume is diminished during ultrafiltration, lead-ing to increased intravascular oncotic pressure. The re-sponse to this change is the expected movement of fluidfrom the interstitial space into the intravascular space, aprocess quantified by the plasma-refilling rate. When the
340 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

UFR equals the plasma-refilling rate, the blood volumeremains relatively constant. Detection of changes in rel-ative blood volume can be monitored continuously duringdialysis to detect intravascular volume changes duringultrafiltration. This can be done using an external opticalsensor to measure serial hematocrits, or by using ultraso-nography to determine blood velocity to measure the totalplasma protein concentration. BVM has been shownto decrease intradialytic hypotension in patients withESRD (34). BVM, however, cannot directly detectwhether there is excessive fluid in the interstitial spaceat the conclusion of a dialysis session. Therefore, BVMis somewhat limited as a tool for the precise determinationof dry weight.
One previous trial that evaluated the use of BVMto adjust volume removal in outpatient dialysis suggestedthat the technique was associated with an increase in all-cause mortality and hospitalizations (35). Consequently,isolated BVM is not a routine part of care. Seibert andcolleagues performed a study to examine the utility ofBVM in HD patients (36). In a cohort of 15 dialysispatients, these investigators combined BVM with contin-uous BIS (cBIS) monitoring of the lower extremity. Inthis study, as extracellular volume decreased with ul-trafiltration, cBIS monitoring detected increased resis-tance until the increase in interstitial fluid was completelyremoved. When excess extravascular fluid was removed,the resistance slope became flatter before the developmentof symptoms, suggesting that the dry weight had beenachieved. By combining cBIS with BVM, however, itwas possible to determine whether any detected decreasein blood volume was due to the achievement of the dryweight or to the UFR exceeding the plasma-refilling rate.In this cohort, the authors demonstrated that as dry weightwas reached by cBIS criteria, further ultrafiltration led toblood volume contraction and the development of symp-toms. Thus, the combination of cBIS monitoring with BVMoffers some promise to improve the ability to determinewhether the plasma volume decrease is due to achievingdry weight versus excessive UFR. Additional studiesare needed to investigate this approach.
Caseload, Physician–Patient Contact, andFacility Size
The population of patients with ESRD continuesto grow in the United States, and the resources tomanage patients on dialysis, namely outpatient dialysisclinics and nephrologists, are limited. Therefore, at-tention must be directed to questions about facility
size, physician–patient contacts, and patient outcomes.Some observations suggest that the caseload for ne-phrologists is associated with patient survival. A retro-spective cohort of 7600 HD patients receiving care atCalifornia DaVita facilities determined that patientstreated by nephrologists who followed the lowest numberof patients had the lowest mortality (37). Conversely,patients treated by nephrologists with the highest dialysiscaseloads had the highest mortality. In this analysis, every50-patient increase in caseload was associated with a 2%absolute increase in patient mortality risk. These investi-gators postulated that higher caseloads had a negativeinfluence on the intensity of patient–nephrologist contact,that clinicians with smaller caseloads were able to investmore time and attention to individual patients’medicalmanagement and complex care coordination, and thatthese negative influences outweighed any benefit as-sociated with greater experience conferred by highercaseloads.
A wide variation exists in the frequency and in-tensity of patient–nephrologist contact and the causes forthis variation are not completely understood. Emerg-ing evidence suggests that patient characteristics explainlittle of this variation (38,39). Increased physician–patient contact is associated strongly with provider andfacility characteristics. Large facilities, urban areas, andincreased nephrologist density explain approximatelyone quarter of the more frequent visits (39). Fixed costsborne by nephrologists who travel to smaller, more re-mote facilities likely exceed any incremental revenueobtained by more frequent visits. There is also substantialgeographic variation, perhaps reflecting regional trainingand practice patterns (Figure 9) (39). The residual three-quarters of the variation in patient–nephrologist outpatientcontacts remains unexplained.
Tremendous variation exists internationallyfor the frequency and intensity of physicianand patient contacts in dialysis facilities.The countries participating in DOPPS re-ported that the mean estimated durationof a typical interaction between doctorand patient was estimated at 7.7 minutes(65.6 minutes), but clinics with physician–patient contacts greater than once perweekwere associated with lower risk of all-causemortality compared with clinics with lowerfrequency contacts.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 341
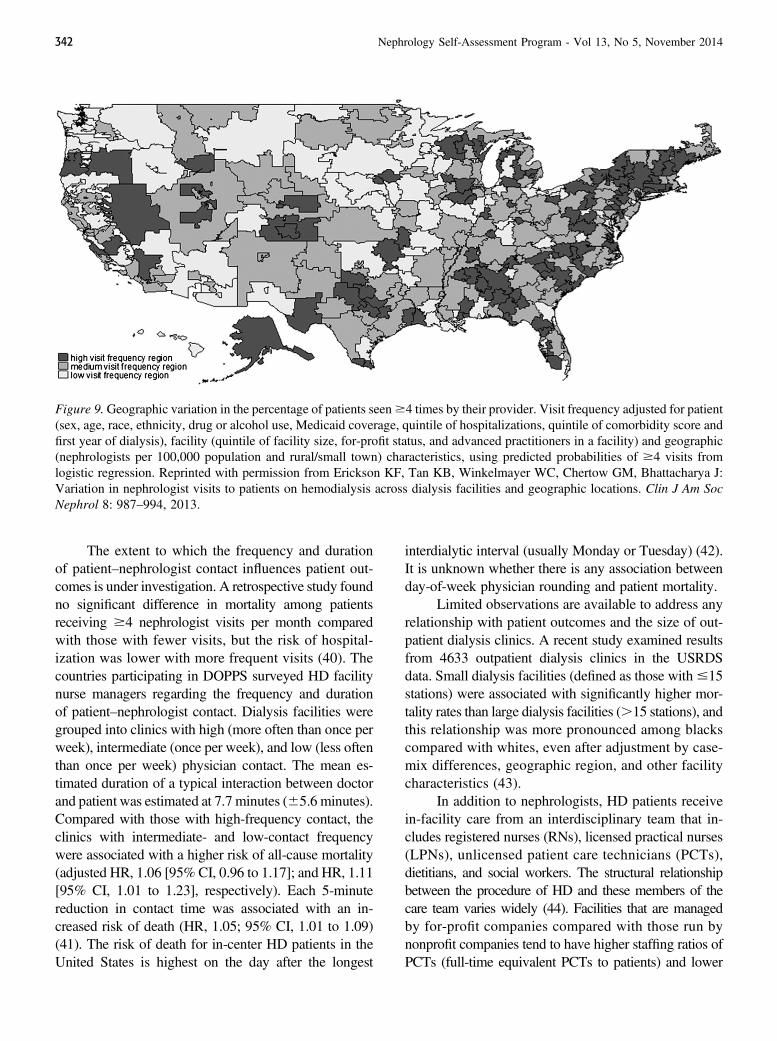
The extent to which the frequency and durationof patient–nephrologist contact influences patient out-comes is under investigation. A retrospective study foundno significant difference in mortality among patientsreceiving $4 nephrologist visits per month comparedwith those with fewer visits, but the risk of hospital-ization was lower with more frequent visits (40). Thecountries participating in DOPPS surveyed HD facilitynurse managers regarding the frequency and durationof patient–nephrologist contact. Dialysis facilities weregrouped into clinics with high (more often than once perweek), intermediate (once per week), and low (less oftenthan once per week) physician contact. The mean es-timated duration of a typical interaction between doctorand patient was estimated at 7.7 minutes (65.6 minutes).Compared with those with high-frequency contact, theclinics with intermediate- and low-contact frequencywere associated with a higher risk of all-cause mortality(adjusted HR, 1.06 [95% CI, 0.96 to 1.17]; and HR, 1.11[95% CI, 1.01 to 1.23], respectively). Each 5-minutereduction in contact time was associated with an in-creased risk of death (HR, 1.05; 95% CI, 1.01 to 1.09)(41). The risk of death for in-center HD patients in theUnited States is highest on the day after the longest
interdialytic interval (usually Monday or Tuesday) (42).It is unknown whether there is any association betweenday-of-week physician rounding and patient mortality.
Limited observations are available to address anyrelationship with patient outcomes and the size of out-patient dialysis clinics. A recent study examined resultsfrom 4633 outpatient dialysis clinics in the USRDSdata. Small dialysis facilities (defined as those with#15stations) were associated with significantly higher mor-tality rates than large dialysis facilities (.15 stations), andthis relationship was more pronounced among blackscompared with whites, even after adjustment by case-mix differences, geographic region, and other facilitycharacteristics (43).
In addition to nephrologists, HD patients receivein-facility care from an interdisciplinary team that in-cludes registered nurses (RNs), licensed practical nurses(LPNs), unlicensed patient care technicians (PCTs),dietitians, and social workers. The structural relationshipbetween the procedure of HD and these members of thecare team varies widely (44). Facilities that are managedby for-profit companies compared with those run bynonprofit companies tend to have higher staffing ratios ofPCTs (full-time equivalent PCTs to patients) and lower
Figure 9.Geographic variation in the percentage of patients seen$4 times by their provider. Visit frequency adjusted for patient(sex, age, race, ethnicity, drug or alcohol use, Medicaid coverage, quintile of hospitalizations, quintile of comorbidity score andfirst year of dialysis), facility (quintile of facility size, for-profit status, and advanced practitioners in a facility) and geographic(nephrologists per 100,000 population and rural/small town) characteristics, using predicted probabilities of $4 visits fromlogistic regression. Reprinted with permission from Erickson KF, Tan KB, Winkelmayer WC, Chertow GM, Bhattacharya J:Variation in nephrologist visits to patients on hemodialysis across dialysis facilities and geographic locations. Clin J Am SocNephrol 8: 987–994, 2013.
342 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

staffing ratios of RNs and LPNs (full-time equivalentRNs1 LPNs to patients) (44). The effect of nonphysicianstaffing levels on patient outcomes is unknown and remainsa subject for future study. Continued research is necessaryto better understand the outcomes of these variations in carepatterns and to guide the formulation of evidence-basedpractice guidelines and regulatory policy.
Hemodialysis Membrane, Constituents ofDialysate, and Clinical OutcomesEvidence for Assignment of Dialysate Calcium Con-centration. Controversy persists with regard to the idealprescription for the dialysate calcium concentration.For centuries, it has been evident that patients withCKD are likely to develop complications related tocalcification of soft tissues. Essentially any organ ortissue can become “ossified” in a patient with CKD, butconsequences of the calcification process are particu-larly grave if it involves cardiac valves or arteries.Given these trends, it would seem ideal, at least in thelong term, to establish a net negative flux of calciumduring the hemodialysis procedure. However, exposureto low calcium dialysate is also associated with intra-dialytic hypotension, cardiac arrhythmias, and second-ary hyperparathyroidism. The lack of consensus on theideal dialysate calcium is manifest by an enormousvariation in prescribing habits around the world, withdialysate calcium concentrations ranging from#2mEq/L(common in the United States) to $3 mEq/L (e.g., inEurope, Japan, and Australia) (45).
The lack of consensus on the ideal dialysatecalcium is manifest by an enormous var-iation in prescribing habits around theworld, with dialysate calcium concentra-tions ranging from #2 mEq/L (common intheUnited States) to$3mEq/L (e.g., Europe,Japan, and Australia). One recent studydemonstrated an association between therisk of in-center cardiac arrest with use oflow (,2.5 mEq/L) calcium dialysate. Theideal dialysate calcium concentration islikely 2.5–2.75 mEq/L.
Part of the difficulty in reaching consensus on thisissue is that patients respond to dialysate calcium invaried ways. In a painstakingly detailed study, Basile andcolleagues determined the net flux of calcium during HD
with a single-pass, batch system with dialysate calciumconcentrations of 2.5, 2.75, and 3.0 mEq/L (45). At allthree concentrations, patients experienced a positive cal-cium balance, but the mass balance for calcium was 2-and 3.5-fold higher with the 2.75 and 3 mEq/L dialysatescompared with the 2.5 mEq/L dialysate, respectively. Incontrast with the results with higher calcium baths, pa-tients dialyzed with 2.5 mEq/L calcium demonstrateda slight decrease in normalized plasma water ionizedcalcium as well as an expected increase in parathyroidhormone (PTH) concentration during the treatment.The authors concluded that the results with the 2.75mEq/L calcium bath were ideal because this conditionresulted in a mildly positive calcium balance, normalplasma ionized calcium concentration, and null effecton in-treatment PTH secretion. In a comparable study,Bosticardo and colleagues calculated the mass balanceof calcium during HD treatments with 2.5 and 3 mEq/Lcalcium levels in dialysate (46). In contrast with earlierstudies, these investigators observed that use of a2.5 mEq/L dialysate resulted in no change in plasmaionized calcium values and in a net neutral calciumflux. However, consistent changes were reported withuse of dialysate calcium .2.5 mEq/L, with short-term increases in serum calcium, decreases in serumphosphorus, and decreases in serum PTH concen-trations (47).
Potential perils associated with use of low calciumdialysate were examined in recent publications. In acase-control study of prevalent HD patients, Pun andcoworkers confirmed that patients exposed to dialysatecalcium ,2.5 mEq/L were more likely to experienceintradialytic hypotension than other patients (48). Thisstudy also demonstrated that use of low calcium di-alysate was significantly associated with increased riskof in-center sudden cardiac arrest (odds ratio, 2.00; 95%CI, 1.40 to 2.90; P,0.001). In addition, the presence ofa calcium “gradient,” determined by the difference be-tween the most recent serum and the prescribed dialysatecalcium concentrations, was also associated with in-creased risk of in-clinic cardiac arrest in this study (oddsratio, 1.40; 95% CI, 1.10 to 1.80; P¼0.002). In sum-mary, these observations suggest that the ideal dialysatecalcium concentration is 2.5–2.75 mEq/L.Associations with Dialysate Sodium Concentra-tion. Uncertainty also reigns with regard to the idealassignment of dialysate sodium concentration and man-agement of sodium balance in maintenance HD patients.A dialysate that contains a sodium concentration that
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 343

exceeds that of the patient’s effective plasma concentra-tion has the potential to reduce symptoms of disequilib-rium and to limit episodes of intradialytic hypotension.However, use of dialysate sodium concentrations thatexceed the plasma sodium concentration tends to producean increase in interdialytic weight gain and predialysis BP(49). A study of nearly 12,000 prevalent HD patients in 12participating DOPPS centers demonstrated a wide rangeof dialysate prescriptions for sodium (50). The mean di-alysate sodium concentrationwas 141mEq/L in the UnitedStates and Italy, and it was lowest (138.4 mEq/L) in theUnited Kingdom and Germany. In the DOPPS participantswho had higher serum sodium concentrations, dialysatesodium concentration was not associated with any dif-ference in patient survival. However, in theDOPPS patientsin the lowest tertile of mean serum sodium concentra-tions, mortality was reduced for dialysate sodium pre-scriptions.140 mEq/L (HR, 0.77; 95% CI, 0.60 to 0.98;P¼0.04) compared with dialysate sodium prescriptionsof 140 mEq/L (50). In patients with mean serum sodiumconcentrations,137 mEq/L, those with dialysate sodiumprescriptions .142 mEq/L had the lowest mortalityrisk (HR, 0.65; 95% CI, 0.47 to 0.91) compared withpatients with dialysate sodium prescriptions of 140 mEq/L(50). The authors suggested that the increase in risk as-sociated with particularly low serum sodium concentrationsmight be abrogated by assignment to a higher dialysatesodium concentration (50).
One interesting finding may also relate to sodiumbalance in dialysis patients. Usvyat and colleagues per-formed a longitudinal cohort study of HD patients indifferent geographic regions of the United States (51).This study demonstrated a rather striking difference inthe observed mortality rate, with 14.2 deaths per 100patient-years in winter months but only 11.9 per 100patient-years in summer months. The apparent increasein mortality was due to cardiovascular events and wasmore pronounced in younger dialysis patients. IDWGs,systolic pressures, and serum potassium concentra-tions were also significantly higher in the study cohortduring the winter months. Although not specificallyaddressed in this study, it is possible that the observedseasonal difference occurred because patients tendedto lose more sodium in between dialysis treatments insummer months. Regardless, these studies support thenotion that the ideal practice would be one that createsa neutral sodium balance. It remains unclear how neutralsodium balance can best be accomplished with tradi-tional HD schedules.
Dialysate Bicarbonate and Systemic Acidosis. MostHD systems allow modification or “modeling” of di-alysate sodium concentration by controlling and adjustingdelivery of sodium bicarbonate. Therefore, modifyingthe dialysate sodium concentration in dialysate is likelylinked to delivery of bicarbonate and acid-base status.One study evaluated the efficacy of correction of acidosisin .110,000 prevalent HD patients (52). In this retro-spective study, 40% of HD patients had serum bicarbon-ate concentration ,22 mEq/L. These lower bicarbonatevalues were associated with an increased risk of all-causeand cardiovascular mortality, compared with the refer-ence group serum bicarbonate of 24–25 mEq/L. Theresults showed that 53% of patients dialyzed with a di-alysate bicarbonate concentration of 30–33 mEq/L hadserum bicarbonate values below 22mEq/L, but even 36%of patients dialyzed with a dialysate bath concentrationof 39–40 mEq/L exhibited these low serum bicarbonatevalues. Interestingly, in this analysis, PD patients evaluatedin the same timeframe had substantially higher serumbicarbonate concentrations than the patients maintainedon HD.Reuse of Dialyzers andMembrane Permeability. Overthe past decade, significant trends are apparent in theprescription, composition, and processing of HD mem-branes. Although they are often not influenced by firmclinical evidence, these practice patterns are oftenguided by overall costs, regional economic conditions,and available alternative technologies. For example, thereprocessing of dialyzers is becoming less common, whilethe use of synthetic and high-flux membranes is be-coming more prevalent (53). Questions also persistwith regard to the ideal characteristics of the membranesused in HD. The HEMO study prospectively examinedwhether patients treated with high-flux membranes hadimproved clinical outcomes. The intention-to-treat anal-ysis of this trial failed to show a significant differencebetween high-flux and conventional dialysis membranes.A post hoc analysis of this trial, however, suggested thatvintage dialysis patients in the HEMO study had reducedcardiovascular mortality when treated with high-fluxdialyzers compared with similar patients treated withlow-flux membranes (54). A randomized prospective trialwas performed in 704 HD patients to determine whetherultrapure dialysate or membrane permeability affectssurvival (55). Patients were followed for a minimum of3 years. In the intention-to-treat analysis, there were nosignificant differences among treatment groups. Thismight seem to lead to a firm conclusion that high-flux
344 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

dialysis membranes do not offer any advantages. How-ever, in a post hoc analysis, high-flux membranes wereassociated with significant improvements in cardiovas-cular event–free survival in patients who had an arterio-venous fistula (adjusted HR, 0.61; 95% CI, 0.38 to 0.97)and patients with diabetes (HR, 0.49; 95% CI, 0.25 to0.94). The ultrapure dialysate intervention was associ-ated with a slight reduction in cardiovascular eventsin study participants who had been on dialysis for.3years. The impact of dialyzer reuse was recently exam-ined by Galvao and colleagues in a meta-analysis thatincluded 14 reported studies of dialyzer reuse that pooledresults from nearly a million patients (53). This study didnot demonstrate significant harm or benefit associatedwith dialyzer reuse compared with single-use dialyzers.
Physical Activity in Hemodialysis PatientsMortality rates in dialysis patients remain high, with
cardiovascular disease being the leading cause of deathdespite ongoing attempts to improve dialysis delivery andmodify risk factors. Physical activity remains a strongpredictor of cardiovascular mortality and may representa potential modifiable risk factor in this vulnerable pop-ulation. It is evident that dialysis patients are very in-active compared with patients without kidney disease, andthe majority of dialysis patients have sedentary lifestyles.In a multicenter, cross-sectional study of 134 dialysispatients, participants wore a device on their wrist thatwas used to monitor energy expenditure, quantify numberof steps taken per day, and determine physical activity(56). In this cohort, 64% of patients were sedentary orwere classified as having a low physical activity level.Factors associated with a sedentary lifestyle in this studyincluded older age, obesity, and diabetes. Higher serumcreatinine was associated with increased physical activity.In addition, physical activity was significantly lower ondialysis days compared with nondialysis days (P,0.001).Diminished physical activity on treatment days may beexplained by postdialysis fatigue, in addition to timeconstraints caused by the dialysis procedure itself.
The Comprehensive Dialysis Study was a multicen-ter, prospective cohort study that evaluated the associa-tion between physical activity and mortality (57). In thisstudy, 1554 incident ambulatory dialysis patients wereadministered the Human Activity Profile, a comprehen-sive survey used to collect information on patients’participation in 94 different activities. This informationwas incorporated in a maximal activity score and anadjusted activity score (AAS). The AAS was interpreted
as a measure of the usual physical activity level and wasused to estimate maximum oxygen consumption (VO2
max). The majority of patients fell into the low fitnesscategory. Patients with low fitness levels tended to haveincreased cardiovascular comorbidities, higher bodymassindex, and lower serum albumin and creatinine levelsthan those with increased estimated fitness levels. Amultivariable analysis confirmed an independent, linearinverse relationship between the AAS level and mortality(adjusted HR, 1.30; 95% CI, 1.23 to 1.39 per 10-pointdecrease in AAS; P,0.001). Patients in the lowest levelof fitness experienced a 3.5-fold increase in risk of death(95% CI, 2.54 to 4.89; P,0.001) compared with thosewith average or above-average fitness. This study couldnot detect a threshold level of activity above or belowwhich greater participation in physical activity was notassociated with survival.
The link between physical activity and survivalwas also demonstrated in a separate, prospective cohortof 202 dialysis patients that showed that increased habit-ual physical activity was associated with a decrease inmortality (58). Patients were monitored with a wrist accel-erometer for 7 days to determine habitual physical activityand the intensity, duration, and frequency of activity.After 7 years of follow-up, this study demonstrated thatincreased physical activity was independently associatedwith increased survival, even after adjusting for demo-graphics and comorbidities (HR for death per 10-minutedaily increase in physical activity, 0.78; 95% CI, 0.66 to0.29; P¼0.002).
Despite the apparent benefit of physical activity,the majority of dialysis patients are not physically active.Dialysis patients are exposed to a number of factors thatmay contribute to this decrease in physical activity.These factors include increased age, bone and mineraldiseases, loss of muscle mass, depression, inflammation,and an increased burden of diabetes and other cardio-vascular morbidities that may limit exercise. In a groupof 270 dialysis patients, it was found that pulmonarycongestion, New York Heart Association functionalclass, diabetes, and impaired mental health were allassociated with worse physical functioning (59).
In a survey of 100 dialysis patients, 98% of pa-tients agreed that a sedentary lifestyle was a health riskand that increasing exercise was beneficial (60). Yet pa-tients in this cohort were very sedentary, with an averagephysical activity of just 25 minutes per week, whichconsisted primarily of walking and light activity. Thisis well below the recommended guidelines of at least
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 345

30 minutes of moderate intensity exercise most (if notall) days of the week. The vast majority of these patientscited at least one barrier to exercise, with nearly one-fifth of patients reporting .10 barriers to physical ac-tivity. The most common barriers noted were dyspnea,lack of motivation, and general fatigue, particularly ondialysis days. Specific barriers that were associated withinactivity included a feeling of helplessness, lower ex-tremity ulcers, excessive medical problems, lack of timeon dialysis days, lack of motivation, and dyspnea.
Increasing physical activity represents one poten-tially modifiable risk factor in dialysis patients. Mortal-ity in these patients remains high, and any interventionthat may improve this should be explored. Tailoringexercise programs to an individual’s unique fitness levelis likely to be more successful than more generalizedrecommendations. Strategies to overcome some of theunique barriers to exercise in individual dialysis patientsshould be applied. One promising option may be link-ing exercise to the dialysis procedure itself, either duringor just after dialysis. Nephrologists should incorporatea regular assessment, discussion, and recommendations re-garding physical activity during routine patient evaluations.
References1. Ramirez SP, Kapke A, Port FK, Wolfe RA, Saran R, Pearson J, Hirth
RA, Messana JM, Daugirdas JT: Dialysis dose scaled to body surfacearea and size-adjusted, sex-specific patient mortality. Clin J Am SocNephrol 7: 1977–1987, 2012 PubMed
2. McCausland FR, Brunelli SM, Waikar SS: Dialysis dose and intra-dialytic hypotension: Results from the HEMO study. Am J Nephrol 38:388–396, 2013 PubMed
3. Bieber B, Qian J, Anand S, Yan Y, Chen N, Wang M, Wang M, Zuo L,Hou FF, Pisoni RL, Robinson BM, Ramirez SP: Two-times weeklyhemodialysis in China: Frequency, associated patient and treatmentcharacteristics and quality of life in the China Dialysis Outcomesand Practice Patterns Study. Nephrol Dial Transplant 29: 1770–1777, 2014 PubMed
4. Tentori F, Zhang J, Li Y, Karaboyas A, Kerr P, Saran R, Bommer J, PortF, Akiba T, Pisoni R, Robinson B: Longer dialysis session length isassociated with better intermediate outcomes and survival among pa-tients on in-center three times per week hemodialysis: Results from theDialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol DialTransplant 27: 4180–4188, 2012 PubMed
5. Arbor Research Collaborative for Health: Achieved dialysis sessionlength, country-specific trends. In: 2012 Annual Report of the DialysisOutcomes and Practice Patterns Study: Hemodialysis Data 1997–2011,Ann Arbor, MI, Arbor Research Collaborative for Health, 2012
6. Tandon T, Sinha AD, Agarwal R: Shorter delivered dialysis timesassociate with a higher and more difficult to treat blood pressure. NephrolDial Transplant 28: 1562–1568, 2013 PubMed
7. Lacson E Jr, Xu J, Suri RS, Nesrallah G, Lindsay R, Garg AX, Lester K,Ofsthun N, Lazarus M, Hakim RM: Survival with three-times weeklyin-center nocturnal versus conventional hemodialysis. J Am Soc Nephrol23: 687–695, 2012 PubMed
8. Singh S, Choi P, Power A, Ashby D, Cairns T, Griffith M, McLean A,Palmer A, Taube D, Duncan N: Ten-year patient survival on maintenance
haemodialysis: Association with treatment time and dialysis dose. JNephrol 26: 763–770, 2013 PubMed
9. Flythe JE, Curhan GC, Brunelli SM: Disentangling the ultrafiltrationrate-mortality association: The respective roles of session length andweight gain. Clin J Am Soc Nephrol 8: 1151–1161, 2013 PubMed
10. Flythe JE, Curhan GC, Brunelli SM: Shorter length dialysis sessions areassociated with increased mortality, independent of body weight. KidneyInt 83: 104–113, 2013 PubMed
11. Cukor D, Ver Halen N, Asher DR, Coplan JD, Weedon J, Wyka KE,Saggi SJ, Kimmel PL: Psychosocial intervention improves depression,quality of life, and fluid adherence in hemodialysis. J Am Soc Nephrol25: 196–206, 2014 PubMed
12. Twardowski ZJ, Misra M, Singh AK: Con: Randomized controlledtrials (RCT) have failed in the study of dialysis methods. Nephrol DialTransplant 28: 826–832, discussion 832, 2013 PubMed
13. Tai DJ, Conley J, Ravani P, Hemmelgarn BR, MacRae JM: Hemodi-alysis prescription education decreases intradialytic hypotension. JNephrol 26: 315–322, 2013 PubMed
14. Gilbertson DT, Monda KL, Bradbury BD, Collins AJ: RBC transfusionsamong hemodialysis patients (1999-2010): Influence of hemoglobin con-centrations below 10 g/dL. Am J Kidney Dis 62: 919–928, 2013 PubMed
15. Fishbane S, Schiller B, Locatelli F, Covic AC, Provenzano R, WiecekA, Levin NW, Kaplan M, Macdougall IC, Francisco C, Mayo MR, PoluKR, Duliege AM, Besarab A; EMERALD Study Groups: Peginesatidein patients with anemia undergoing hemodialysis. N Engl J Med 368:307–319, 2013 PubMed
16. Kidney Disease Improving Global Outcomes (KDIGO): KDIGO clinicalpractice guideline for anemia in chronic kidney disease. Kidney Int Suppl2: 279–335, 2013
17. Coyne DW: The health-related quality of life was not improved bytargeting higher hemoglobin in the Normal Hematocrit Trial. Kidney Int82: 235–241, 2012 PubMed
18. Gaweda AE, Aronoff GR, Jacobs AA, Rai SN, Brier ME: Individual-ized anemia management reduces hemoglobin variability in hemodial-ysis patients. J Am Soc Nephrol 25: 159–166, 2014 PubMed
19. Rattanasompattikul M, Molnar MZ, Zaritsky JJ, Hatamizadeh P, Jing J,Norris KC, Kovesdy CP, Kalantar-Zadeh K: Association of malnutrition-inflammation complex and responsiveness to erythropoiesis-stimulatingagents in long-term hemodialysis patients. Nephrol Dial Transplant 28:1936–1945, 2013 PubMed
20. Ornt DB, Larive B, Rastogi A, Rashid M, Daugirdas JT, Hernandez A,Kurella Tamura M, Suri RS, Levin NW, Kliger AS; Frequent Hemodi-alysis Network Trial Group: Impact of frequent hemodialysis on anemiamanagement: Results from the Frequent Hemodialysis Network (FHN)Trials. Nephrol Dial Transplant 28: 1888–1898, 2013 PubMed
21. Schneider A, Drechsler C, Krane V, Krieter DH, Scharnagl H,Schneider MP, Wanner C; MINOXIS Study Investigators: The effectof high-flux hemodialysis on hemoglobin concentrations in patientswith CKD: Results of the MINOXIS study. Clin J Am Soc Nephrol 7:52–59, 2012 PubMed
22. Mercadal L, Coudert M, Vassault A, Pieroni L, Debure A, Ouziala M,Depreneuf H, Fumeron C, Servais A, Bassilios N, Bécart J, Assogba U,Allouache M, Bouali B, Luong N, Dousseaux MP, Tezenas-du MontcelS, Deray G: L-carnitine treatment in incident hemodialysis patients: Themulticenter, randomized, double-blinded, placebo-controlled CARNIDIALtrial. Clin J Am Soc Nephrol 7: 1836–1842, 2012 PubMed
23. Bailie GR, Larkina M, Goodkin DA, Li Y, Pisoni RL, Bieber B, MasonN, Tong L, Locatelli F, Marshall MR, Inaba M, Robinson BM:Variation in intravenous iron use internationally and over time: TheDialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol DialTransplant 28: 2570–2579, 2013 PubMed
24. Freburger JK, Ng LJ, Bradbury BD, Kshirsagar AV, Brookhart MA:Changing patterns of anemia management in US hemodialysis patients.Am J Med 125: 906, e9, 2012 PubMed
25. Barraclough KA, Brown F, Hawley CM, Leary D, Noble E, Campbell SB,Isbel NM, Mudge DW, van Eps CL, Johnson DW: A randomized con-
346 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
trolled trial of oral heme iron polypeptide versus oral iron supplementationfor the treatment of anaemia in peritoneal dialysis patients: HEMATOCRITtrial. Nephrol Dial Transplant 27: 4146–4153, 2012 PubMed
26. Kshirsagar AV, Freburger JK, Ellis AR, Wang L, Winkelmayer WC,Brookhart MA: The comparative short-term effectiveness of iron dosingand formulations in US hemodialysis patients. Am J Med 126: e1–e14,2013 PubMed
27. Brookhart MA, Freburger JK, Ellis AR, Wang L, Winkelmayer WC,Kshirsagar AV: Infection risk with bolus versus maintenance ironsupplementation in hemodialysis patients. J Am Soc Nephrol 24: 1151–1158, 2013 PubMed
28. Zaloszyc A, Schaefer B, Schaefer F, Krid S, Salomon R, Niaudet P,Schmitt CP, Fischbach M: Hydration measurement by bioimpedancespectroscopy and blood pressure management in children on hemodi-alysis. Pediatr Nephrol 28: 2169–2177, 2013 PubMed
29. Joffy S, Rosner MH: Natriuretic peptides in ESRD. Am J Kidney Dis 46:1–10, 2005 PubMed
30. Vasko R, Müller GA, Ratliff BB, Jung K, Gauczinski S, Koziolek MJ:Clinical judgment is the most important element in overhydrationassessment of chronic hemodialysis patients. Clin Exp Nephrol 17:563–568, 2013 PubMed
31. Raimann JG, Zhu F, Wang J, Thijssen S, Kuhlmann MK, Kotanko P,Levin NW, Kaysen GA: Comparison of fluid volume estimates inchronic hemodialysis patients by bioimpedance, direct isotopic, anddilution methods. Kidney Int 85: 898–908, 2014 PubMed
32. Moissl U, Arias-Guillén M, Wabel P, Fontseré N, Carrera M, CampistolJM, Maduell F: Bioimpedance-guided fluid management in hemodial-ysis patients. Clin J Am Soc Nephrol 8: 1575–1582, 2013 PubMed
33. Hur E, Usta M, Toz H, Asci G, Wabel P, Kahvecioglu S, KayikciogluM, Demirci MS, Ozkahya M, Duman S, Ok E: Effect of fluid man-agement guided by bioimpedance spectroscopy on cardiovascular pa-rameters in hemodialysis patients: A randomized controlled trial. Am JKidney Dis 61: 957–965, 2013 PubMed
34. Santoro A, Mancini E, Basile C, Amoroso L, Di Giulio S, Usberti M,Colasanti G, Verzetti G, Rocco A, Imbasciati E, Panzetta G, Bolzani R,Grandi F, Polacchini M: Blood volume controlled hemodialysis inhypotension-prone patients: a randomized, multicenter controlled trial.Kidney Int 62: 1034–1045, 2002 PubMed
35. Reddan DN, Szczech LA, Hasselblad V, Lowrie EG, Lindsay RM,Himmelfarb J, Toto RD, Stivelman J, Winchester JF, Zillman LA, CaliffRM, Owen WF Jr: Intradialytic blood volume monitoring in ambulatoryhemodialysis patients: a randomized trial. J Am Soc Nephrol 16: 2162–2169, 2005 PubMed
36. Seibert E, Zhu F, Kuhlmann MK, Henson R, Oribello AM, Girndt M,Kotanko P, Levin NW: Slope analysis of blood volume and calfbioimpedance monitoring in hemodialysis patients. Nephrol DialTransplant 27: 4430–4436, 2012 PubMed
37. Harley KT, Streja E, Rhee CM, Molnar MZ, Kovesdy CP, Amin AN,Kalantar-Zadeh K: Nephrologist caseload and hemodialysis pa-tient survival in an urban cohort. J Am Soc Nephrol 24: 1678–1687,2013 PubMed
38. Slinin Y, Guo H, Li S, Liu J, Morgan B, Ensrud K, Gilbertson DT,Collins AJ, Ishani A: Predictors of provider-patient visit frequencyduring hemodialysis. Am J Nephrol 38: 91–98, 2013 PubMed
39. Erickson KF, Tan KB, Winkelmayer WC, Chertow GM, BhattacharyaJ: Variation in nephrologist visits to patients on hemodialysis acrossdialysis facilities and geographic locations. Clin J Am Soc Nephrol 8:987–994, 2013 PubMed
40. Slinin Y, Guo H, Li S, Liu J, Ensrud K, Gilbertson DT, Collins AJ, IshaniA: Association of provider-patient visit frequency and patient outcomeson hemodialysis. J Am Soc Nephrol 23: 1560–1567, 2012 PubMed
41. Kawaguchi T, Karaboyas A, Robinson BM, Li Y, Fukuhara S, BieberBA, Rayner HC, Andreucci VE, Pisoni RL, Port FK, Morgenstern H,Akizawa T, Saran R: Associations of frequency and duration of patient-doctor contact in hemodialysis facilities with mortality. J Am SocNephrol 24: 1493–1502, 2013 PubMed
42. Zhang H, Schaubel DE, Kalbfleisch JD, Bragg-Gresham JL, Robinson BM,Pisoni RL, Canaud B, JadoulM, Akiba T, Saito A, Port FK, Saran R: Dialysisoutcomes and analysis of practice patterns suggests the dialysis scheduleaffects day-of-week mortality. Kidney Int 81: 1108–1115, 2012 PubMed
43. Yan G, Norris KC, Xin W, Ma JZ, Yu AJ, Greene T, Yu W, CheungAK: Facility size, race and ethnicity, and mortality for in-centerhemodialysis. J Am Soc Nephrol 24: 2062–2070, 2013 PubMed
44. Yoder LA, Xin W, Norris KC, Yan G: Patient care staffing levels andfacility characteristics in U.S. hemodialysis facilities. Am J Kidney Dis62: 1130–1140, 2013 PubMed
45. Basile C, Libutti P, Di Turo AL, Vernaglione L, Casucci F, Losurdo N,Teutonico A, Lomonte C: Effect of dialysate calcium concentrations onparathyroid hormone and calcium balance during a single dialysissession using bicarbonate hemodialysis: A crossover clinical trial. Am JKidney Dis 59: 92–101, 2012 PubMed
46. BosticardoG,Malberti F, Basile C, Leardini L, Libutti P, Filiberti O, SchillaciE, Ravani P: Optimizing the dialysate calcium concentration in bicarbonatehaemodialysis. Nephrol Dial Transplant 27: 2489–2496, 2012 PubMed
47. Jean G, Mayor B, Hurot JM, Deleaval P, Lorriaux C, Zaoui E, ChazotC: Biological impact of targeted dialysate calcium changes in haemo-dialysis patients: The key role of parathyroid hormone. Nephrol DialTransplant 28: 176–182, 2013 PubMed
48. Pun PH, Horton JR, Middleton JP: Dialysate calcium concentration andthe risk of sudden cardiac arrest in hemodialysis patients. Clin J Am SocNephrol 8: 797–803, 2013 PubMed
49. Hecking M, Karaboyas A, Saran R, Sen A, Inaba M, Rayner H, HörlWH, Pisoni RL, Robinson BM, Sunder-Plassmann G, Port FK: Di-alysate sodium concentration and the association with interdialyticweight gain, hospitalization, and mortality. Clin J Am Soc Nephrol 7:92–100, 2012 PubMed
50. Hecking M, Karaboyas A, Saran R, Sen A, Hörl WH, Pisoni RL,Robinson BM, Sunder-Plassmann G, Port FK: Predialysis serumsodium level, dialysate sodium, and mortality in maintenance hemodi-alysis patients: The Dialysis Outcomes and Practice Patterns Study(DOPPS). Am J Kidney Dis 59: 238–248, 2012 PubMed
51. Usvyat LA, Carter M, Thijssen S, Kooman JP, van der Sande FM,Zabetakis P, Balter P, Levin NW, Kotanko P: Seasonal variations inmortality, clinical, and laboratory parameters in hemodialysis patients: A5-year cohort study. Clin J Am Soc Nephrol 7: 108–115, 2012 PubMed
52. Vashistha T, Kalantar-Zadeh K, Molnar MZ, Torlén K, Mehrotra R:Dialysis modality and correction of uremic metabolic acidosis: Re-lationship with all-cause and cause-specific mortality. Clin J Am SocNephrol 8: 254–264, 2013 PubMed
53. Galvao TF, Silva MT, Araujo ME, Bulbol WS, Cardoso AL: Dialyzerreuse and mortality risk in patients with end-stage renal disease: Asystematic review. Am J Nephrol 35: 249–258, 2012 PubMed
54. Cheung AK, Sarnak MJ, Yan G, Berkoben M, Heyka R, Kaufman A,Lewis J, Rocco M, Toto R, Windus D, Ornt D, Levey AS; HEMO StudyGroup: Cardiac diseases in maintenance hemodialysis patients: Results ofthe HEMO Study. Kidney Int 65: 2380–2389, 2004 PubMed
55. Asci G, Tz H, Ozkahya M, Duman S, Demirci MS, Cirit M, Sipahi S,Dheir H, Bozkurt D, Kircelli F, Ok ES, Erten S, Ertilav M, Kose T,Basci A, Raimann JG, Levin NW, Ok E; EGE Study Group: The impactof membrane permeability and dialysate purity on cardiovascularoutcomes. J Am Soc Nephrol 24: 1014–1023, 2013 PubMed
56. Avesani CM, Trolonge S, Deléaval P, Baria F, Mafra D, Faxén-IrvingG, Chauveau P, Teta D, KamimuraMA, Cuppari L, ChanM, HeimbürgerO, Fouque D: Physical activity and energy expenditure in haemodialysispatients: An international survey. Nephrol Dial Transplant 27: 2430–2434, 2012 PubMed
57. Johansen KL, Kaysen GA, Dalrymple LS, Grimes BA, Glidden DV,Anand S, Chertow GM: Association of physical activity with survivalamong ambulatory patients on dialysis: The Comprehensive DialysisStudy. Clin J Am Soc Nephrol 8: 248–253, 2013 PubMed
58. Matsuzawa R, Matsunaga A, Wang G, Kutsuna T, Ishii A, Abe Y,Takagi Y, Yoshida A, Takahira N: Habitual physical activity measured
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 347

by accelerometer and survival in maintenance hemodialysis patients.Clin J Am Soc Nephrol 7: 2010–2016, 2012 PubMed
59. Enia G, Torino C, Panuccio V, Tripepi R, Postorino M, Aliotta R,Bellantoni M, Tripepi G, Mallamaci F, Zoccali C; Lung Comets CohortWorking Group: Asymptomatic pulmonary congestion and physicalfunctioning in hemodialysis patients. Clin J Am Soc Nephrol 8: 1343–1348, 2013 PubMed
60. Delgado C, Johansen KL: Barriers to exercise participation among dialysispatients. Nephrol Dial Transplant 27: 1152–1157, 2012 PubMed
Home-Suitable Dialysis
Choice of Dialysis ModalityThe interest in receiving dialysis therapies at home
is growing in many parts of the world. In the UnitedStates in 2011, 8208 incident patients were initiated onhome-suitable dialysis, 9.4% with home hemodialysis(HD) and 90.6% with peritoneal dialysis (PD). This rep-resents 7.4% of all patients who started dialysis therapiesin 2011 (1). The penetrance of PD in the United States ismoderate compared with the international experience,but the incident population is rising as of 2011 for thethird year in a row (1,2). PD is more cost-effective thanin-center HD, particularly after first-year training andstart-up costs are absorbed. Finally, the introduction ofthe new bundled payment system has incentivized growthin this segment of the dialysis population (3).
An important driver of modality selection is pre-dialysis patient education. Patients with advanced stagesof CKD who participate in education programs are morelikely to choose PD as a modality compared with individ-uals who do not participate in these programs. Chanouzasand colleagues (4) identified additional factors that in-fluence modality selection. Survey data from 180 pre-dialysis patients indicated that 70%, 20%, and 10% optedfor HD, PD, and nondialytic therapy, respectively. Pa-tients who chose PD were younger and had fewercomorbid conditions. In addition, demographic factorssuch as being married, being employed, and not livingalone were significantly associated with PD choice. How-ever, there was discordance between the initially chosenmodality and the modality ultimately used for dialysis. Of217 patients who were surveyed after receiving modalityeducation, 57% chose PD and 43% either chose HD orwere undecided. Of the patients who chose PD initially,47% started on PD. This proportion rose to 52% after 91days on dialysis.
In a multivariable analysis, older age predictedutilization of HD (odds ratio [OR], 4.0; 95% CI [95%confidence interval], 1.03 to 15.8; P¼0.05), whereasGN as the cause of ESRD (as opposed to diabetes) (OR,
0.31; 95% CI, 0.95 to 1.0; P¼0.05) as well as beingemployed (OR, 0.16; 95% CI, 0.04 to 0.64; P¼0.01)were associated with the use of PD. Furthermore, 32%of patients who had chosen PD initially required urgenthospital-based initiation of dialysis therapies, which ledto use of HD in most (5).
The socioeconomic status of the patient, either asan influence on the patient or the provider, likely hasbearing on the choice of dialysis modality. Prakash andcolleagues (6) analyzed a prospective Canadian clinicaldatabase to explore whether the socioeconomic status ofa patient’s neighborhood predicted eligibility and choiceof PD. Socioeconomic status was assessed by measuringmedian household income and level of education inmembers of households. Of 1314 patients who enteredinto five renal programs in the province of Ontario be-tween 2004 and 2010, 857 (65% of patients) were deemedeligible for either PD or HD. Of those eligible for eithermodality, 46% chose PD. Socioeconomic status was notassociated with the choice to pursue PD. The three mostcommonly identified barriers that prevented the choice ofPD were general preference for in-center HD (15.4% ofpatients deemed eligible), inability to decide (12.8%), andperceived inability to perform PD (12.6%). In 5.8% and3.5% of eligible patients, “built environment” (defined toinclude “issues such as having a small apartment, spaceissues, and other problems with the built environment[residence/physical space] that would prevent mainte-nance of a PD routine [includes not having space for PDsupplies]; also includes patient self-report of living closeto a hemodialysis or satellite hemodialysis unit”) andfamily/social support, respectively, were cited as barriersmore common in eligible patients in the lower educationand income group. This could represent an indirect influ-ence of socioeconomic status on the PD choice.
Socioeconomic and other factors associated withincreased home dialysis use were also investigated inan observational study in the United Kingdom (7). Pa-tients from an area of lowest socioeconomic status were60% less likely to receive home HD compared with themost affluent patients. Increased distance from a dialysiscenter increased the probability of using home modal-ities. In addition, patients aged 31–40 years were morelikely to use home dialysis compared with younger andolder subsets. South Asian and black patients were lesslikely to use home dialysis compared with white patientsin this analysis from the United Kingdom. A differentstudy from Canada, where conditions of universal payerand provider prevail, addressed these same issues.
348 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

In a retrospective analysis, Hingwala and coworkersdetermined that a strong influence was associated withdistinct individual nephrology practice patterns (8).Interestingly, if the high PD use practice group wascompared with the low PD use group, there was neithera difference in the peritoneal technique survival, nor inthe mortality of patients. The authors of this study arguedthat even if PD was aggressively promoted with patients,the crucial clinical outcomes of technique survival andpatient mortality were not different compared with a lessaggressive approach. This finding is intriguing given theeconomic pressures to reduce costs associated with di-alysis therapies.
Clinical Outcomes: Survival, CardiovascularEvents, Hospitalization, and ModalityComparisonComparative Outcomes by Dialysis Modality. Thedifferent modalities of PD and HD will shape the life-style for the individual, but whether one modality offersa distinct clinical advantage remains an area of scrutiny.In-center HD and PD were compared in numerous ret-rospective studies and demonstrated conflicting results.These retrospective studies are limited by nonrandomallocation of treatment, crossover of modality use, lossto transplantation, and the presence of confounding var-iables. Recent publications attempted to overcome thesemethodologic shortfalls. Lukowsky et al. (9) investigateddifferences in survival according to modality among allincident dialysis patients in a commercial US cohortbetween July 2001 and June 2004. Incident PD patientswere younger, were more likely to switch modality, andwere more likely to receive a kidney transplant com-pared with the incident HD group. Using a marginalstructural model to account for selection bias and time-dependent confounders such as modality switching andtransplantation, the authors found a 48% lower mortalityin the PD group compared with the HD group after 2 yearsof follow-up (hazard ratio [HR], 0.52; 95% CI, 0.34 to0.80). Yeates and colleagues (10) examined a registry of46,830 incident dialysis patients in Canada who initiateddialysis from 1991 to 2007. In an intention-to-treat ana-lysis and a proportional hazards model, mortality upto 18 months slightly favored PD, whereas mortalityafter 36 months favored HD. In a nonproportionalhazards model of the more contemporary cohort (2001–2004), short-term mortality (,2 years) was lower withPD, whereas there was no difference between PD andHD for long-term mortality (3–5 years).
Slightly different results were obtained from studiesof patients in other countries. An analysis of a healthregistry was performed in Finland that evaluated 4754adults who required chronic RRT between 2000 and 2009(11). Similar to the Canadian study, an intention-to-treatanalysis was performed and patients were followed fora median of 2.8 years. Patients who started treatmentwith PD were younger and more likely to already be onthe kidney transplantation waiting list compared withHD patients. After adjusting for 26 variables and cen-soring patients who received a transplant, the study didnot detect a statistically significant difference in mor-tality between the patients on HD and PD. An as-treatedanalysis was also completed in the Finnish study, in anattempt to account for participants who had transitionedfrom one modality to the other. The multivariablemodel for this analysis revealed that patients who wereexclusively on PD had a 17% higher risk of deathcompared with patients exclusively on HD (P¼0.047).Krishnasamy and colleagues (12) used the Australia andNew Zealand Dialysis and Transplant (ANZDATA) Reg-istry to examine the effect of dialysis modality on cardiacand noncardiac death. Over a 10-year period (1999–2008), the timing of cardiac death (day of the week)as a function of dialysis modality was studied in PD(n¼4298), in-center HD #3 times weekly (n¼9503),in-center HD .3 times weekly (n¼251), and home HD(HHD) (n¼573). In-center HD #3 times per week wasassociated with increased risk for cardiac mortality onMondays compared with all other days of the week, asdescribed in several other studies (13). Patients on PD,HHD, and in-center HD .3 times per week had nosignificant variation in cardiac death across all days ofthe week. The causes of cardiac death that drove thiseffect in the in-center HD group were speculated to behyperkalemia and myocardial infarction. These studiessuggest that more frequent dialysis either through PD orfrequent HD can reduce this daily variation on the risk ofcardiac death from hyperkalemia or myocardial infarction.However, these studies do not clarify whether PD or morefrequent HD provides a survival advantage to patients inthe long term.Modifiable Variables and Outcomes Associated withPD. One strategy to improve outcomes for patients onPD is to identify risk factors that the clinician can modify.For example, several observations identify underlyingheart failure as a major risk factor for cardiac death indialysis patients. In a prospective, multicenter, obser-vational cohort in Italy, Gallieni and coworkers (14)
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 349
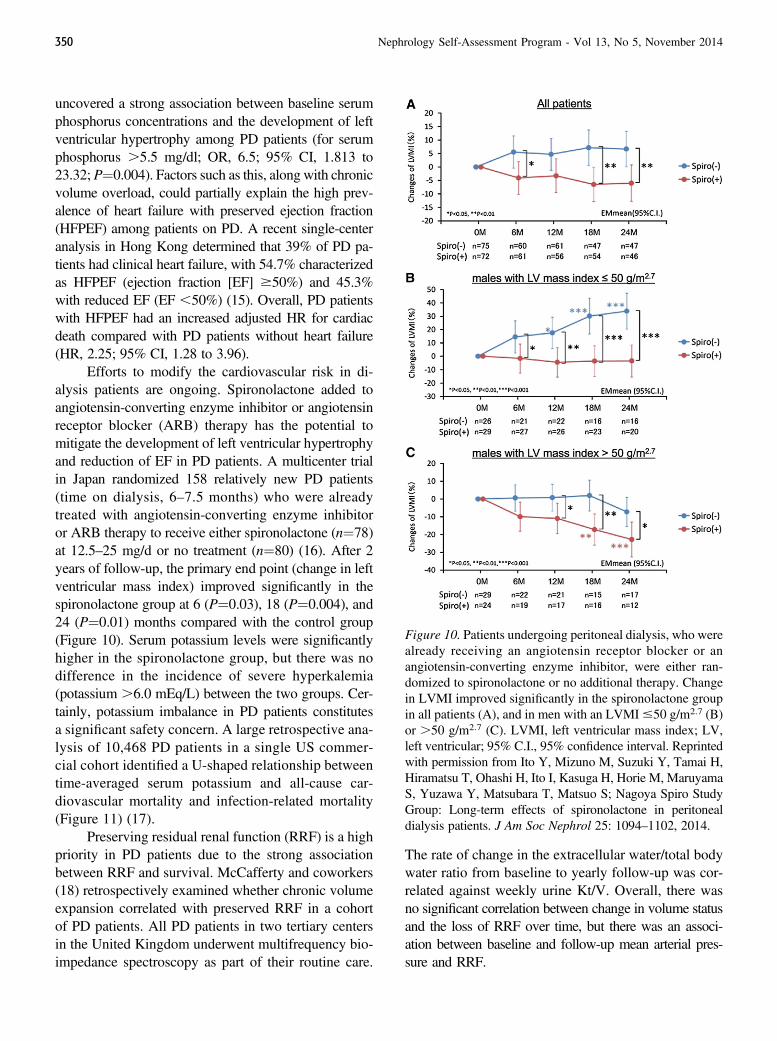
uncovered a strong association between baseline serumphosphorus concentrations and the development of leftventricular hypertrophy among PD patients (for serumphosphorus .5.5 mg/dl; OR, 6.5; 95% CI, 1.813 to23.32; P¼0.004). Factors such as this, along with chronicvolume overload, could partially explain the high prev-alence of heart failure with preserved ejection fraction(HFPEF) among patients on PD. A recent single-centeranalysis in Hong Kong determined that 39% of PD pa-tients had clinical heart failure, with 54.7% characterizedas HFPEF (ejection fraction [EF] $50%) and 45.3%with reduced EF (EF ,50%) (15). Overall, PD patientswith HFPEF had an increased adjusted HR for cardiacdeath compared with PD patients without heart failure(HR, 2.25; 95% CI, 1.28 to 3.96).
Efforts to modify the cardiovascular risk in di-alysis patients are ongoing. Spironolactone added toangiotensin-converting enzyme inhibitor or angiotensinreceptor blocker (ARB) therapy has the potential tomitigate the development of left ventricular hypertrophyand reduction of EF in PD patients. A multicenter trialin Japan randomized 158 relatively new PD patients(time on dialysis, 6–7.5 months) who were alreadytreated with angiotensin-converting enzyme inhibitoror ARB therapy to receive either spironolactone (n¼78)at 12.5–25 mg/d or no treatment (n¼80) (16). After 2years of follow-up, the primary end point (change in leftventricular mass index) improved significantly in thespironolactone group at 6 (P¼0.03), 18 (P¼0.004), and24 (P¼0.01) months compared with the control group(Figure 10). Serum potassium levels were significantlyhigher in the spironolactone group, but there was nodifference in the incidence of severe hyperkalemia(potassium .6.0 mEq/L) between the two groups. Cer-tainly, potassium imbalance in PD patients constitutesa significant safety concern. A large retrospective ana-lysis of 10,468 PD patients in a single US commer-cial cohort identified a U-shaped relationship betweentime-averaged serum potassium and all-cause car-diovascular mortality and infection-related mortality(Figure 11) (17).
Preserving residual renal function (RRF) is a highpriority in PD patients due to the strong associationbetween RRF and survival. McCafferty and coworkers(18) retrospectively examined whether chronic volumeexpansion correlated with preserved RRF in a cohortof PD patients. All PD patients in two tertiary centersin the United Kingdom underwent multifrequency bio-impedance spectroscopy as part of their routine care.
The rate of change in the extracellular water/total bodywater ratio from baseline to yearly follow-up was cor-related against weekly urine Kt/V. Overall, there wasno significant correlation between change in volume statusand the loss of RRF over time, but there was an associ-ation between baseline and follow-up mean arterial pres-sure and RRF.
Figure 10. Patients undergoing peritoneal dialysis, who werealready receiving an angiotensin receptor blocker or anangiotensin-converting enzyme inhibitor, were either ran-domized to spironolactone or no additional therapy. Changein LVMI improved significantly in the spironolactone groupin all patients (A), and in men with an LVMI#50 g/m2.7 (B)or .50 g/m2.7 (C). LVMI, left ventricular mass index; LV,left ventricular; 95% C.I., 95% confidence interval. Reprintedwith permission from Ito Y, Mizuno M, Suzuki Y, Tamai H,Hiramatsu T, Ohashi H, Ito I, Kasuga H, Horie M, MaruyamaS, Yuzawa Y, Matsubara T, Matsuo S; Nagoya Spiro StudyGroup: Long-term effects of spironolactone in peritonealdialysis patients. J Am Soc Nephrol 25: 1094–1102, 2014.
350 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
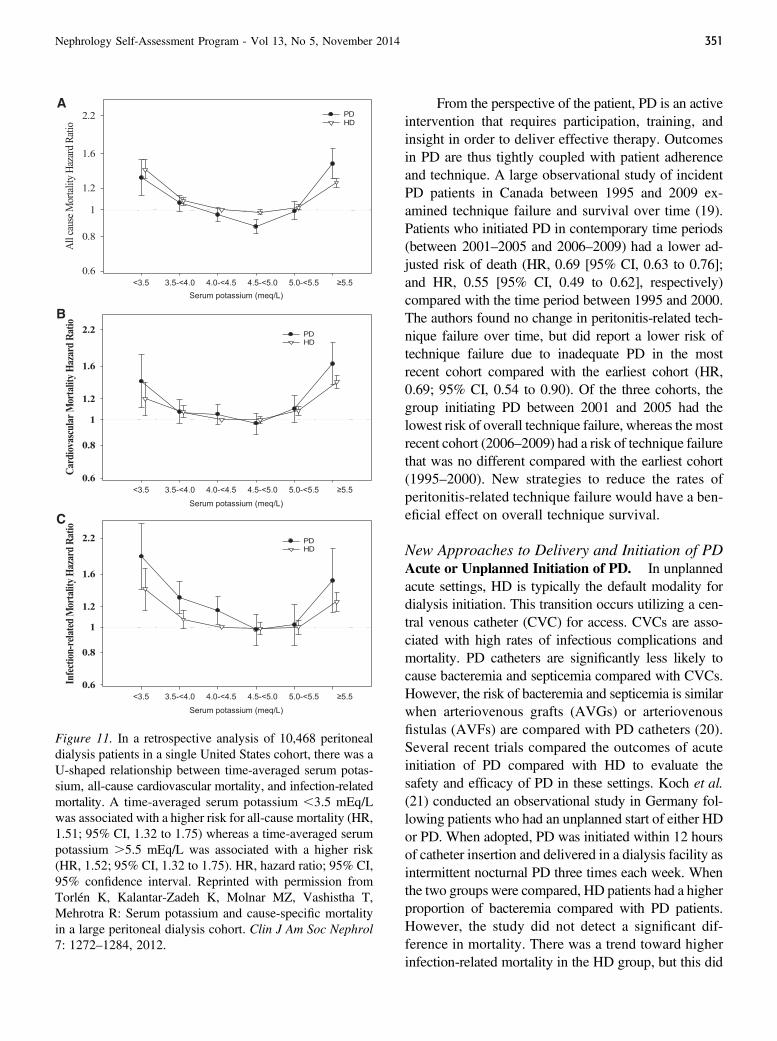
From the perspective of the patient, PD is an activeintervention that requires participation, training, andinsight in order to deliver effective therapy. Outcomesin PD are thus tightly coupled with patient adherenceand technique. A large observational study of incidentPD patients in Canada between 1995 and 2009 ex-amined technique failure and survival over time (19).Patients who initiated PD in contemporary time periods(between 2001–2005 and 2006–2009) had a lower ad-justed risk of death (HR, 0.69 [95% CI, 0.63 to 0.76];and HR, 0.55 [95% CI, 0.49 to 0.62], respectively)compared with the time period between 1995 and 2000.The authors found no change in peritonitis-related tech-nique failure over time, but did report a lower risk oftechnique failure due to inadequate PD in the mostrecent cohort compared with the earliest cohort (HR,0.69; 95% CI, 0.54 to 0.90). Of the three cohorts, thegroup initiating PD between 2001 and 2005 had thelowest risk of overall technique failure, whereas the mostrecent cohort (2006–2009) had a risk of technique failurethat was no different compared with the earliest cohort(1995–2000). New strategies to reduce the rates ofperitonitis-related technique failure would have a ben-eficial effect on overall technique survival.
New Approaches to Delivery and Initiation of PDAcute or Unplanned Initiation of PD. In unplannedacute settings, HD is typically the default modality fordialysis initiation. This transition occurs utilizing a cen-tral venous catheter (CVC) for access. CVCs are asso-ciated with high rates of infectious complications andmortality. PD catheters are significantly less likely tocause bacteremia and septicemia compared with CVCs.However, the risk of bacteremia and septicemia is similarwhen arteriovenous grafts (AVGs) or arteriovenousfistulas (AVFs) are compared with PD catheters (20).Several recent trials compared the outcomes of acuteinitiation of PD compared with HD to evaluate thesafety and efficacy of PD in these settings. Koch et al.(21) conducted an observational study in Germany fol-lowing patients who had an unplanned start of either HDor PD. When adopted, PD was initiated within 12 hoursof catheter insertion and delivered in a dialysis facility asintermittent nocturnal PD three times each week. Whenthe two groups were compared, HD patients had a higherproportion of bacteremia compared with PD patients.However, the study did not detect a significant dif-ference in mortality. There was a trend toward higherinfection-related mortality in the HD group, but this did
Figure 11. In a retrospective analysis of 10,468 peritonealdialysis patients in a single United States cohort, there was aU-shaped relationship between time-averaged serum potas-sium, all-cause cardiovascular mortality, and infection-relatedmortality. A time-averaged serum potassium ,3.5 mEq/Lwas associated with a higher risk for all-cause mortality (HR,1.51; 95% CI, 1.32 to 1.75) whereas a time-averaged serumpotassium .5.5 mEq/L was associated with a higher risk(HR, 1.52; 95% CI, 1.32 to 1.75). HR, hazard ratio; 95% CI,95% confidence interval. Reprinted with permission fromTorlén K, Kalantar-Zadeh K, Molnar MZ, Vashistha T,Mehrotra R: Serum potassium and cause-specific mortalityin a large peritoneal dialysis cohort. Clin J Am Soc Nephrol7: 1272–1284, 2012.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 351

not reach statistical significance. The authors argued thatPD is a reasonable alternative to HD for dialysis ini-tiation in acute or unplanned settings. Ivarsen and col-leagues (22) reported the outcomes of unplanned initiationof dialysis utilizing the Danish Nephrology Registry. Inthe Danish experience, this study did not detect a signif-icant difference in mortality between patients who werestarted on planned PD, unplanned PD, and planned HD inthe Danish Registry. Typically, the PD catheter was used,6 days after implantation in unplanned initiation of PD.The European Best Practice guidelines recommend thatPD be initiated about 2 weeks after PD catheter implan-tation (23). This reduces risk of leakage of PD fluid alongthe catheter and allows for better wound healing. In areview of the literature, Ivarsen and colleagues (22) notedseveral studies showing more mechanical complicationsamong patients with early catheter use, but they did notdiscern a difference in long-term technique survival.Whencomparing populations of patients with planned andunplanned initiation of PD, patients with an unplannedstart tended to be older and have more comorbidities anda higher overall mortality. However, when adjusting forthese characteristics, the difference in mortality was nolonger apparent. Furthermore, the unplanned initiation ofPD did not appear to increase infectious complication, asopposed to an unplanned start of HD in which an increasedrisk of infections occurs compared with planned initiations.
A recent report indicated that unplanned and urgentPD initiations could also become a fruitful policy inthe United States. Using a structured program at asingle clinical center, a total of 18 patients underwenta standardized protocol for modality selection, rapidPD catheter placement, initial prescription, and initialmanagement. Compared with planned starts, the authorconcluded that acute unplanned PD was feasible andsafe (24). In summary, when logistical barriers are over-come, unplanned initiation PD is a safe, efficaciousalternative to unplanned initiation of HD in multipledifferent health care systems. This approach holds theprospect of moving dialysis populations to more cost-effective treatment modalities.PD in AKI. A role for PD is now evolving in cases ofAKI in which intermittent HD or some form of con-tinuous RRT (CRRT) is typically utilized when needed.A recent systematic review investigated the outcomesof patients with AKI treated with PD compared withmore conventional therapy (25). A total of 24 studiesincluding 1556 patients were evaluated. The majority ofstudies were conducted in low-resource regions includ-
ing those in Asia, Africa, and South America. Observa-tional studies of PD compared with HD/CRRT supportfound no significant difference in mortality. When ex-amining the few randomized controlled trials, Chionhand colleagues highlighted several heterogeneousresults. One study suggested greater mortality with PDand three studies demonstrated comparable mortalityrates between PD and the HD/CRRT groups. Thesestudies also suggested conflicting results with regard torecovery of renal function. Given the differences in patientpopulations, it is unclear whether these results will applyto AKI management in other countries.Psychosocial and Economic Factors AffectingChoice of PD as Modality in ESRD. With the risingprevalence of ESRD worldwide and increasing costsassociated with health care, PD may offer significanteconomic advantage. Chui and colleagues (26) inves-tigated costs associated with care in a cohort of dialysispatients in Canada. Over a 3-year span, cumulative costsfor patients exclusively treated with PD were substan-tially lower than in patients exclusively treated with HD.Conversion from HD to PD was also more effective inreducing costs than remaining on HD. PD techniquefailure that required transition to HD had lower costs inthe first year compared with the HD group. By the endof the 3-year observation period, costs were similar inthe patients who transitioned from PD despite the needfor change in modality. Of note, PD patients in the studytended to be younger and healthier than those main-tained on HD. Thus, it is not clear whether PD will pro-vide a cost advantage in older and sicker patients.
Psychosocial attitudes play a large role in selec-tion of dialysis modality. Tong et al. (27) conducteda systematic review investigating the patient perspec-tives of a life spent receiving PD. This study identifiedseveral recurrent themes, highlighting positive and nega-tive characteristics. Many patients easily incorporatedPD into their lives and appreciated the support systemused to sustain the program. Patients valued their senseof control, bodily awareness, and increased under-standing of their condition. Patients also stated that theflexibility of PD allowed them to retain their socialfunctioning. However, other patients emphasized thenegative stigmata associated with PD therapy includingdiminished self-esteem, poor body image, and a sense of“invisible suffering.” Some patients in the survey also notedthat PDwas disruptive and that it posed a significant burdenon families. These sentiments need to be considered whencontemplating PD as a possible dialysis modality.
352 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

Risk Factors for Necessitating Transition Away fromPD. The cessation of PD and the need to transition toHD can result from a variety of reasons. A retrospectiveanalysis by Béchade et al. (28) sought to identify thefactors associated with an early requirement to transi-tion away from PD after failure of PD. Patients whonecessitated early transition were defined as those whoneeded to transfer to HD within the first 6 months ofstarting PD. Patients treated with HD before PD, thosewith peritonitis in the first 6 months of treatment, andthose with failed transplants had a higher risk of tech-nique failure. Transplant patients who required initiationof PD for a failed allograft posed unique problems in thisstudy. Resection of the allograft was associated withsurgical complications, violation of the peritoneal space,and loss of RRF. In addition, continuation of immuno-suppressive medications seemed to enhance the likeli-hood of peritonitis and treatment failure. The study alsonoted that patients who attended dialysis centers with.20 PD patients per year had a lower rate of early transferto HD. This suggests that local expertise will help avoidfailure of the PD technique. The study was not able toaccount for subjective factors associated with individ-ual patients and physicians. In addition, the study hadincomplete data on patient characteristics such as priorabdominal surgeries, socioeconomic status, and RRF.
Psychological and social factors also help deter-mine whether a patient will persevere in a PD program.Patient burnout, fatigue, and loss of functional capacityall likely determine a patient’s fate. One method thatwas recently developed is “assisted PD,” a procedurethat relies on the assistance of healthcare workers orfamily members in the home. A retrospective Frenchstudy evaluated patients undergoing assisted versus self-care PD. Rates of transfer to HD were lower in patientswith assisted PD, although the nurse-assisted subgrouphad less frequent transfers compared with family-assistedpatients. At 24 months, 21.1% of patients in the self-caregroup had switched to HD, but only 15% of patients inthe assisted PD group had transitioned to HD in the sameobservation period (29). An important consideration,however, is that assistance with community nurses iscovered by national health insurance in France but is notnecessarily available in other countries.
Infectious Complications of PDRisk Factors for Peritonitis. Infections associated withPD continue to be a major cause of morbidity and mor-tality. Recent data suggest that peritonitis contributes to
15% of PD deaths and that each episode of peritonitis isassociated with a 4%–8% higher risk of mortality (30).As a result, new methods to prevent the development ofperitonitis and its associated complications persist as ahigh priority in the field.
Exit-site infections (ESIs) at the catheter site increasethe risk of peritonitis via transmigration of organismsfrom the skin via the PD catheter tract into the peri-toneal cavity. A number of observational trials suggesta relationship between ESIs and peritonitis. The Inter-national Society for Peritoneal Dialysis recommendedincreased use of topical antibiotic prophylaxis andmore aggressive treatment of ESIs (31). van Diepenand colleagues (32) described a strong association be-tween recent ESIs and the subsequent development ofperitonitis, with a 6-fold increase in risk. However,organisms isolated from the exit site in this study oftendiffered from those identified from the associated epi-sode of peritonitis. The authors hypothesized that theESI itself may influence immunomodulatory pathwaysand causes an increased tendency toward developingsecondary bacterial infections. Alternatively, because treat-ments used for ESI target skin organisms, other organismsmay flourish, leading to peritonitis with a different patho-gen. Finally, a limitation of exit-site cultures in identifyingthe causative pathogen was postulated to possibly ac-count for the discrepancy between cultures taken fromthe exit site and the pathogen isolated from the PD fluidculture.
PD catheter-associated infections are typically as-sociated with skin flora, including Staphylococcus epidermisand Staphylococcus aureus. However, a recent rise inthe rate of infections related to Gram-negative organisms,including Pseudomonas aeruginosa, was recognized (33).ESIs and peritonitis are reduced by the use of mupirocincream, a compound with broad antimicrobial coverage(34). Gentamicin cream also has excellent activityagainst Gram-negative organisms as well as some acti-vity against Gram-positive organisms, but whether thisprovides a clinical advantage over mupirocin remainsunclear (35). Polysporin ointment has broad-spectrumcoverage, with good bacteriostatic activity against skinflora and coverage against Gram-negative pathogens,and has been successfully used in HD catheter care(36). A recent randomized controlled trial investigatedthe efficacy of polysporin ointment compared withmupirocin (30). The results showed no statistically sig-nificant difference in incidence of overall PD-relatedinfections. The patients who received mupirocin had
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 353
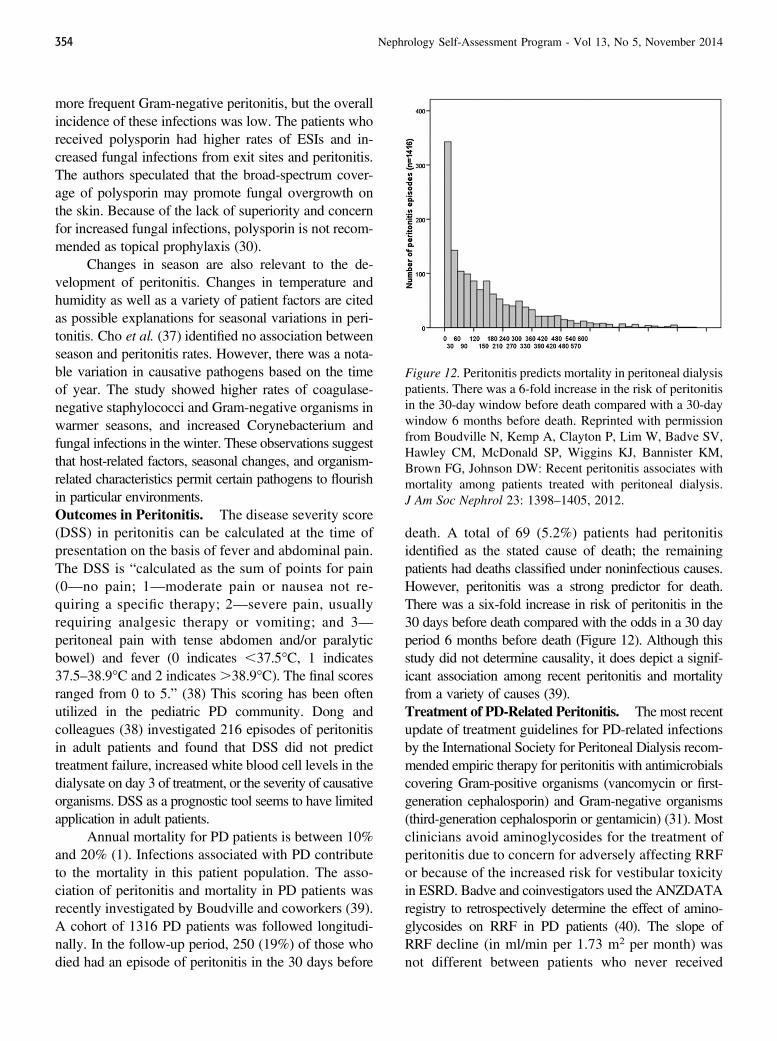
more frequent Gram-negative peritonitis, but the overallincidence of these infections was low. The patients whoreceived polysporin had higher rates of ESIs and in-creased fungal infections from exit sites and peritonitis.The authors speculated that the broad-spectrum cover-age of polysporin may promote fungal overgrowth onthe skin. Because of the lack of superiority and concernfor increased fungal infections, polysporin is not recom-mended as topical prophylaxis (30).
Changes in season are also relevant to the de-velopment of peritonitis. Changes in temperature andhumidity as well as a variety of patient factors are citedas possible explanations for seasonal variations in peri-tonitis. Cho et al. (37) identified no association betweenseason and peritonitis rates. However, there was a nota-ble variation in causative pathogens based on the timeof year. The study showed higher rates of coagulase-negative staphylococci and Gram-negative organisms inwarmer seasons, and increased Corynebacterium andfungal infections in the winter. These observations suggestthat host-related factors, seasonal changes, and organism-related characteristics permit certain pathogens to flourishin particular environments.Outcomes in Peritonitis. The disease severity score(DSS) in peritonitis can be calculated at the time ofpresentation on the basis of fever and abdominal pain.The DSS is “calculated as the sum of points for pain(0—no pain; 1—moderate pain or nausea not re-quiring a specific therapy; 2—severe pain, usuallyrequiring analgesic therapy or vomiting; and 3—peritoneal pain with tense abdomen and/or paralyticbowel) and fever (0 indicates ,37.5�C, 1 indicates37.5–38.9�C and 2 indicates.38.9�C). The final scoresranged from 0 to 5.” (38) This scoring has been oftenutilized in the pediatric PD community. Dong andcolleagues (38) investigated 216 episodes of peritonitisin adult patients and found that DSS did not predicttreatment failure, increased white blood cell levels in thedialysate on day 3 of treatment, or the severity of causativeorganisms. DSS as a prognostic tool seems to have limitedapplication in adult patients.
Annual mortality for PD patients is between 10%and 20% (1). Infections associated with PD contributeto the mortality in this patient population. The asso-ciation of peritonitis and mortality in PD patients wasrecently investigated by Boudville and coworkers (39).A cohort of 1316 PD patients was followed longitudi-nally. In the follow-up period, 250 (19%) of those whodied had an episode of peritonitis in the 30 days before
death. A total of 69 (5.2%) patients had peritonitisidentified as the stated cause of death; the remainingpatients had deaths classified under noninfectious causes.However, peritonitis was a strong predictor for death.There was a six-fold increase in risk of peritonitis in the30 days before death compared with the odds in a 30 dayperiod 6 months before death (Figure 12). Although thisstudy did not determine causality, it does depict a signif-icant association among recent peritonitis and mortalityfrom a variety of causes (39).Treatment of PD-Related Peritonitis. The most recentupdate of treatment guidelines for PD-related infectionsby the International Society for Peritoneal Dialysis recom-mended empiric therapy for peritonitis with antimicrobialscovering Gram-positive organisms (vancomycin or first-generation cephalosporin) and Gram-negative organisms(third-generation cephalosporin or gentamicin) (31). Mostclinicians avoid aminoglycosides for the treatment ofperitonitis due to concern for adversely affecting RRFor because of the increased risk for vestibular toxicityin ESRD. Badve and coinvestigators used the ANZDATAregistry to retrospectively determine the effect of amino-glycosides on RRF in PD patients (40). The slope ofRRF decline (in ml/min per 1.73 m2 per month) wasnot different between patients who never received
Figure 12. Peritonitis predicts mortality in peritoneal dialysispatients. There was a 6-fold increase in the risk of peritonitisin the 30-day window before death compared with a 30-daywindow 6 months before death. Reprinted with permissionfrom Boudville N, Kemp A, Clayton P, Lim W, Badve SV,Hawley CM, McDonald SP, Wiggins KJ, Bannister KM,Brown FG, Johnson DW: Recent peritonitis associates withmortality among patients treated with peritoneal dialysis.J Am Soc Nephrol 23: 1398–1405, 2012.
354 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

aminoglycosides compared with patients who receivedeither one, two, or even three courses of aminoglycosides(P¼0.90). Thus, absolute avoidance of aminoglycosidesin PD patients likely does not translate into preservedRRF in PD patients treated for peritonitis.
A related study evaluated the pharmacokinetics ofintraperitoneal gentamicin. A total of 24 patients withPD-related peritonitis were enrolled, and intraperitonealgentamicin was administered. The plasma and dialysateconcentrations of the drug were measured. The meansystemic absorption of gentamicin was 73%, which washigher than levels previously reported in patients wholacked clinical evidence of peritonitis. The study also sug-gested variation in proportions of systemic absorption ofthe aminoglycoside based on the membrane transporterstatus of the patients; high transporters exhibited a shorterequilibration time. Anuric patients had a longer t1/2 of gen-tamicin compared with nonanuric patients. Thus, the increasein membrane permeability during peritonitis, membranetransporter status, and degree of RRF need to be consid-ered when dosing intraperitoneal aminoglycosides (41).
Peritonitis is treated empirically at time of clinicaldiagnosis, and cultures may remain negative for bacte-rial growth. To remedy the shortcoming between empiricand directed therapy, Lin and coworkers (42) analyzedimmune responses to particular pathogens to identify an“immune fingerprint.” The study demonstrated an asso-ciation between biomarkers such as IL-1b, IL-10, IL-22,TNF-a, and C-X-C motif chemokine 10 with Gram-positive and Gram-negative infections. In addition, adistinct difference in biomarker pattern was noted inculture-negative peritonitis. Further study is requiredvalidate the use of this methodology in clinical practice.Predictors for Relapsing and Recurrent Peritoni-tis. Peritonitis caused by S. aureus and P. aeruginosa isassociated with a high rate of relapse. A predictor forrelapse or recurrence would enable physicians to imple-ment preventative therapy. Prior studies suggested thata high white blood cell count in the dialysate 3 days afterantibiotic treatment serves as a predictor of immediatetreatment failure (43). However, these clinical indicatorshave limited usefulness to predict relapsing and recurrentdisease. Utilizing quantitative PCR assays, bacteria-derived DNA fragments can be found in body fluids. Arecent study addressed whether bacterial DNA fragmentscan serve as predictors of relapse (44). In a study of 143patients with PD-associated peritonitis, DNA frag-ments were compared in the PD fluid of patients withand without relapsing peritonitis (44). Patients with
bacterial peritonitis were followed for 1 year aftercompletion of antimicrobial therapy. Patients weremonitored for relapsing (infection with the sameorganism within 4 weeks), recurrent (different organ-ism within 4 weeks), and repeat peritonitis (infectionwith the same organism after 4 weeks). Measurement ofbacterial DNA fragments demonstrated that patients withrelapsing or recurrent peritonitis had significantly higherlevels of these fragments in their PD fluid 5 days beforeand on the day of completion of the course of antibiotics.Increased levels of these fragments were not associatedwith positive bacterial cultures and were not thought tobe indicative of active infection. This study suggestedthat detection of high levels of DNA fragments can beused to alter treatment strategy, perhaps with pro-longation of antimicrobials or implementation ofalternative therapies. The study was limited by smallsample size, data from a single center, and concernregarding the degree of accuracy in the assays used todetermine DNA fragment levels (44).
Dialysis Solutions in PDThe most commonly used PD solutions in the
United States contain either dextrose or icodextrin toproduce an osmotic gradient to facilitate ultrafiltration.By contrast, newer PD solutions have a more neutralpH, often using lactate or bicarbonate as buffer, andcontain low levels of glucose degradation products.These solutions are considered potentially more “bio-compatible.”A dual-chamber design prevents degradationof glucose while the solutions are in storage.Mixing of thetwo chambers immediately before use produces a neutralpH solution that lacks glucose degradation products (GDPs).In addition, newer, alternative PD solutions are low inglucose and contain amino acids to produce an osmoticgradient. Biocompatible solutions may preserve RRF,improve the systemic metabolic profile in patients withdiabetes, delay peritoneal membrane damage, and alterperitonitis rates. Several published reports recently fo-cused on important clinical end points when comparingconventional with newer solutions.
The use of “biocompatible”PDsolutions, par-ticularly those that limit accumulation of glu-cose degradation products, may preserveresidual renal function, improve themetabolicprofile in diabetics, delay peritonealmembranedamage, and reduce peritonitis rates.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 355

Residual Renal Function. To investigate the effect ofnewer or biocompatible PD solution on RRF, the balANZtrial compared conventional dextrose-based dialysis solu-tion with a neutral pH, low GDP solution (45). A total of185 PD patients were randomly assigned to either con-ventional or low GDP solution and followed for 2 years.The primary end point of the balANZ trial was thedecline in RRF; the secondary end points included timeto development of anuria, fluid volume status, peritonitisrate, technique, and patient survival, as well as adverseevents. The rate of decline in RRF was less in the in-tervention group, but this observation did not meet sta-tistical significance (P¼0.06). The native GFR declinedby 0.22 ml/min per 1.73 m2 per month in the first year inthe intervention group compared with 0.28 ml/min per1.73m2 permonth in the control group (Figure 13). How-ever, time to the development of anuria was signifi-cantly longer in the intervention group (P¼0.01).
Another recent, randomized trial mirrored theseobservations. Three biocompatible solutions based on(1) neutral pH with low GDP, (2) 1.1% amino acids,and (3) 7.5% icodextrin were compared with conven-tional dextrose-based dialysate. Even though the declinein renal function was similar in both groups, the declinein urine volume after 12 months of follow-up was slightlyless in the biocompatible dialysate group (urine output959 ml/d in the biocompatible dialysate group comparedwith 798ml/d in the conventional group; P¼0.06) (46). Asmaller trial with a similar premise conducted in Chinafound that RRF declined at a significantly slower rate inthe patients who underwent PD with a biocompatiblesolution (47).
A recent systematic review by an Australian groupsummarized the literature for neutral pH/low GDP solu-tions on RRF and longitudinal urine output. Seven trialscomprising 520 patients showed larger urine volumeswith the use of biocompatible solutions. Six trials witha total of 360 patients yielded improved RRF after 12months with the use of biocompatible solutions (48).Metabolic Indices. Li and colleagues (49) investigatedwhether biocompatible peritoneal dialysate would im-part a favorable effect on the metabolic milieu in ESRDpatients. This prospective, randomized trial comparedPD with a conventional dialysis solution and a glucose-sparing dialysate in a population of 251 patients withdiabetes. The dialysate in the glucose-sparing group wascomposed of variously reduced dextrose–based solutionssupplemented with icodextrin and amino acids to producean appropriate osmotic gradient. The primary end point
was the reduction of the glycosylated hemoglobin value.The glucose-sparing PD regimen significantly reducedglycosylated hemoglobin (0.5% difference between thegroups; P¼0.01). Other metabolic indices such as theserum concentrations of albumin, triglycerides, very LDL,and apolipoprotein B were also reduced by the interven-tion. Disappointingly, volume status management wassuboptimal in the intervention group. Hypertensive ur-gency and volume overload leading to heart failure weremore common in the intervention group.Peritoneal Transport Properties. In the balANZ trial(as described above), investigators also evaluated whetherbiocompatible PD fluids affected peritoneal transportproperties. In this study, frequent evaluations with theperitoneal equilibrium test revealed that patients whoperformed PD with the biocompatible solution initiallyhad a higher rate of peritoneal membrane transport. Thisrate remained stable over the 2-year observation. By con-trast, patients who dialyzed with conventional solu-tions had a progressive increase in peritoneal membranepermeability (50). In a similar fashion, serial, peritonealequilibrium testing revealed that peritoneal membranepermeability remained unchanged in children who wererandomized to a biocompatible solution, but permeabilityincreased in the control group who dialyzed with con-ventional dialysate. In this study, ultrafiltration capacityincreased over time in the intervention group and de-creased in controls (51). A smaller, retrospective, pediat-ric cohort in The Netherlands concluded that similaradvantages were offered by biocompatible PD solutions(52). A recent systematic review of the literature sum-marized 11 small trials using icodextrin. Improvementof volume management and increased peritoneal ultra-filtration was observed in a total of six trials. Icodextrinwas not associated with a greater risk of adverse eventsin this systematic review (48).Peritonitis Rate. The balANZ trial also investigated theperitonitis rate associated with use of newer PD solu-tions as a secondary outcome. Patients who dialyzedwith biocompatible solutions had lower rates of perito-nitis with 0.30 episodes per year versus 0.49 episodesper year in the control group (P¼0.01) (Figure 14) (45).By contrast, in a retrospective observational cohort inAustralia and New Zealand, the use of biocompatiblesolutions predicted higher overall peritonitis rates as wellas earlier development of the first episode of peritonitis(53). In two systematic reviews summarizing resultswith icodextrin and with neutral pH/low GDP, peritoni-tis rates were not affected with either solution (48,54). It
356 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
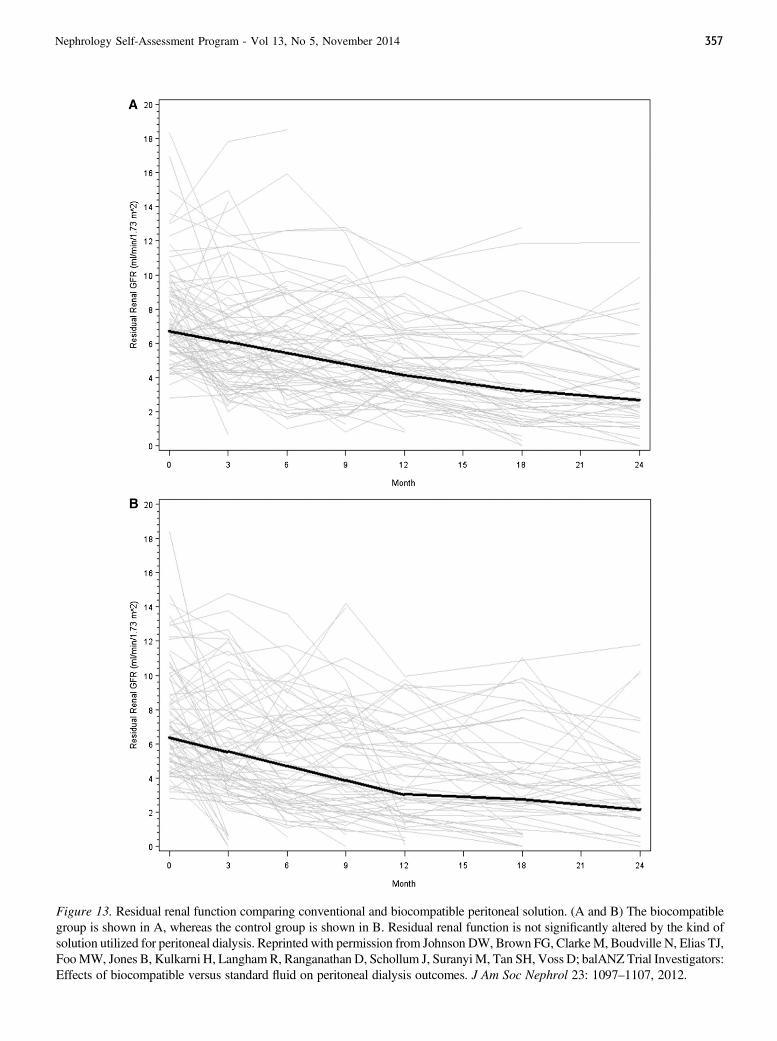
Figure 13. Residual renal function comparing conventional and biocompatible peritoneal solution. (A and B) The biocompatiblegroup is shown in A, whereas the control group is shown in B. Residual renal function is not significantly altered by the kind ofsolution utilized for peritoneal dialysis. Reprinted with permission from Johnson DW, Brown FG, ClarkeM, Boudville N, Elias TJ,FooMW, Jones B, Kulkarni H, LanghamR, Ranganathan D, Schollum J, SuranyiM, Tan SH, Voss D; balANZ Trial Investigators:Effects of biocompatible versus standard fluid on peritoneal dialysis outcomes. J Am Soc Nephrol 23: 1097–1107, 2012.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 357
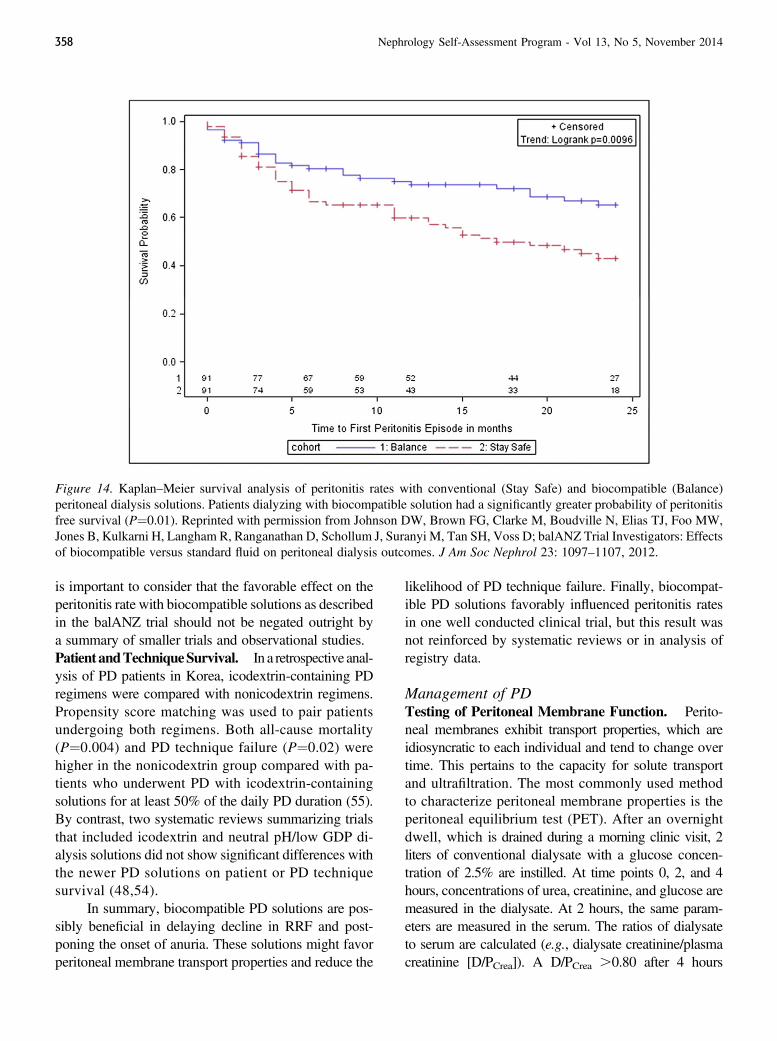
is important to consider that the favorable effect on theperitonitis rate with biocompatible solutions as describedin the balANZ trial should not be negated outright bya summary of smaller trials and observational studies.Patient andTechniqueSurvival. In a retrospective anal-ysis of PD patients in Korea, icodextrin-containing PDregimens were compared with nonicodextrin regimens.Propensity score matching was used to pair patientsundergoing both regimens. Both all-cause mortality(P¼0.004) and PD technique failure (P¼0.02) werehigher in the nonicodextrin group compared with pa-tients who underwent PD with icodextrin-containingsolutions for at least 50% of the daily PD duration (55).By contrast, two systematic reviews summarizing trialsthat included icodextrin and neutral pH/low GDP di-alysis solutions did not show significant differences withthe newer PD solutions on patient or PD techniquesurvival (48,54).
In summary, biocompatible PD solutions are pos-sibly beneficial in delaying decline in RRF and post-poning the onset of anuria. These solutions might favorperitoneal membrane transport properties and reduce the
likelihood of PD technique failure. Finally, biocompat-ible PD solutions favorably influenced peritonitis ratesin one well conducted clinical trial, but this result wasnot reinforced by systematic reviews or in analysis ofregistry data.
Management of PDTesting of Peritoneal Membrane Function. Perito-neal membranes exhibit transport properties, which areidiosyncratic to each individual and tend to change overtime. This pertains to the capacity for solute transportand ultrafiltration. The most commonly used methodto characterize peritoneal membrane properties is theperitoneal equilibrium test (PET). After an overnightdwell, which is drained during a morning clinic visit, 2liters of conventional dialysate with a glucose concen-tration of 2.5% are instilled. At time points 0, 2, and 4hours, concentrations of urea, creatinine, and glucose aremeasured in the dialysate. At 2 hours, the same param-eters are measured in the serum. The ratios of dialysateto serum are calculated (e.g., dialysate creatinine/plasmacreatinine [D/PCrea]). A D/PCrea .0.80 after 4 hours
Figure 14. Kaplan–Meier survival analysis of peritonitis rates with conventional (Stay Safe) and biocompatible (Balance)peritoneal dialysis solutions. Patients dialyzing with biocompatible solution had a significantly greater probability of peritonitisfree survival (P¼0.01). Reprinted with permission from Johnson DW, Brown FG, Clarke M, Boudville N, Elias TJ, Foo MW,Jones B, Kulkarni H, Langham R, Ranganathan D, Schollum J, Suranyi M, Tan SH, Voss D; balANZ Trial Investigators: Effectsof biocompatible versus standard fluid on peritoneal dialysis outcomes. J Am Soc Nephrol 23: 1097–1107, 2012.
358 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

identifies a fast transporter, and a D/PCrea of ,0.55–0.60after 4 hours identifies a slow transporter. A recent po-sition paper from the European Renal Best Practice WorkGroup recommended that the PET be performed yearly orwhen a change in clinical status suggests change of theperitoneal membrane (56).
As conventional dialysate solutions are progres-sively replaced by biocompatible solutions (as describedabove), a classic PET, which uses conventional dialysate,might not be the proper assessment tool in patientswho undergo PD with biocompatible solutions. VanOvermeire and colleagues (57) recently compared PETwith biocompatible and conventional solutions in a smallcohort of PD patients. A total of 19 patients, 9 dialyzedwith conventional and 10 with biocompatible solutions,underwent two PETs 2 weeks apart utilizing either bio-compatible or conventional dialysate. Comparison of thesequential PETs did not reveal a difference in smallmolecule transport rates and ultrafiltration. When D/Pwas assessed for b2 microglobulin and albumin, bothwere transported at a higher rate when biocompatiblesolutions were used. It is not clear why larger moleculestransported differently depending on the PD solutionused during testing, but the authors recommended usingthe same solution in longitudinal comparison. This ob-servation is also important because transport character-istics of larger molecules across the membrane appear tochange in a different cadence compared with small mole-cules. In a prospective cohort of PD patients who werefollowed for a minimum of 4 years, the peritoneal solutetransport rate increased with time, whereas the peritonealprotein clearance remained stable over time (58). Theauthors attributed this finding to different peritoneal evo-lution of large- and small-pore transport pathways.PD Access. With greater utilization and different prac-tices in PD initiation, greater emphasis is being placedon the methods for gaining peritoneal access. Surgicalinsertion, often via a laparoscopic approach, is common-place. Radiologic catheter placement under fluoroscopicguidance is an alternative approach. In a randomizedcontrolled trial, a total of 113 patients were randomizedto radiologic versus surgical placement of PD catheters.The primary end point was complication-free cathetersurvival, which was defined as mechanical or infectiousproblems within the first year. Complication-free cathetersurvival was significantly more likely in the radiolo-gic catheter placement group (42.5% versus 18.1%;P¼0.01). One-year catheter survival was similar in bothgroups (84% for the radiologic group versus 73.7% for
the laparoscopic group; P¼0.27). The authors concludedthat radiologic PD catheter placement is a viable and safealternative to laparoscopic placement. Not unexpectedly,radiologic catheter placement was more cost-effectivethan laparoscopic placement (59).
Radiologic intervention is also a useful method tomodify a nonfunctioning PD catheter. In a single-center,retrospective analysis, 70 radiologic manipulations ofPD catheters were performed because of mechanicalcatheter failure. In 62.9% of cases, manipulations of thecatheter restored function for a mean duration of 469days (interquartile range, 171–865 days). Manipulationsworked best in catheters that were properly positionedinitially and previously functioned well. The authors con-cluded that radiologic manipulation was effective andsafe (60). However, as with radiologic placement of PDcatheters, radiologic manipulation requires great exper-tise by the operator. Surgical placement of PD cathetersand intervention in the case of catheter malfunction is thepreferred method if local expertise is not well verified.
When a catheter is surgically placed, Chen and col-leagues (61) suggest that greater folding of the omentumshould be performed. In a small, prospective, randomizedcontrolled trial, PD catheters were placed openly with orwithout omentum folding. This additional procedure sig-nificantly prevented catheter tip migration and malfunction.
PD catheters vary in several aspects (e.g., straightor coiled intraperitoneal segment, bent or straight sub-cutaneous segment, and single- or double-cuffed, amongother variables). A recent systematic review suggestedthat a surgically inserted, straight, intraperitoneal segmentfavored catheter survival. The number of cuffs and theconfiguration of the subcutaneous segment was not as-sociated with catheter survival (62). However, the authorsof this study advise that local experience and successwith a specific catheter type is the most important con-sideration when PD catheter placement is attempted.
Peritoneal Membrane PathologyExperimental Approach to Peritoneal Fibrosis. Peri-toneal fibrosis is a significant contributor to peritonealmembrane ultrafiltration failure. The cellular and mo-lecular mechanisms that underlie peritoneal fibrosis areincompletely understood. Basic science investigationshave implicated several mediators in the pathogenesisof peritoneal fibrosis, including TGF-b (63) (64), atrialnatriuretic peptide (65), and mineralocorticoids (66). Ex-perimental interventions in animal models to amelio-rate peritoneal fibrosis include N-acetylcysteine (67),
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 359

the vasoactive glycosaminoglycan sulodexide (68),eplerenone (66), as well as glutamine supplementation(69). Mesenchymal stem cell transplantation has shownsome promise in an animal model of peritoneal mem-brane injury and dysfunction (70).Encapsulating Peritoneal Sclerosis. Encapsulatingperitoneal sclerosis (EPS) is a rare, severe complicationof long-term PD. It is characterized by abdominal pain,bowel obstruction, or weight loss (71). Longstandingdamage to the peritoneal membrane can lead to pro-gressive fibrosis and development of EPS. Prolongedexposure to PD solutions is one factor postulated to leadto the development of simple peritoneal sclerosis. Thisusually does not lead to EPS, but the presence of a“second hit,” such as severe peritonitis, discontinuationof PD, or genetic predisposition, may predispose to thedevelopment of EPS (72). Previously identified risk fac-tors for EPS include increased time on PD, younger age,glucose load, and peritonitis (71).
An Italian retrospective review of pediatric PDidentified 14 cases of EPS out of 712 prevalent PDpatients. Increased duration of PD was associated withincreased risk of EPS. This suggested that PD termina-tion should be considered in patients on long-term PD,particularly in those with early symptoms of EPS (73).Despite this risk, data do not support preemptive switch-ing of asymptomatic, long-term PD patients to HD, be-cause not all vintage PD patients will ultimately developEPS. A pediatric study by Shroff and coworkers iden-tified patients who presented with EPS as early as 1.6years and as late as 10.2 years after the beginning PD.This suggested that other risk factors played an im-portant role in the development of EPS (74).
A retrospective analysis investigated the presenta-tions and outcomes of cases of EPS in a referral centerin Germany from 1998 to 2011 (71). A total of 42 pa-tients were included in the study. The patients who hadsignificant symptoms and required surgical interventionwere classified as severe, and the rest were deemed tohave mild to moderate disease. Peritonitis rates in bothgroups were moderate, arguing against the notion thatincreased peritonitis is associated with development ofEPS. This contrasts with the findings of Shroff et al.,who found a significantly higher rate of peritonitis inchildren with EPS compared with those without thedisease (74).
In an observation that is perhaps related, Vidaland coworkers described a high incidence of EPS inchildren with FSGS. This might be related to a similar
proposed pathologic mechanism in both disease processes,namely the upregulation of TGF-b expression (73).Diagnosis of EPS. Diagnosis of EPS is most often madebased on clinical, radiologic, and histologic findings.The clinical presentation of EPS often includes symp-toms of bowel obstruction. A computed tomography(CT) scan can display peritoneal membrane thicken-ing or encapsulation of bowel loops. The most specificfindings on CT scans for this condition are boweltethering and peritoneal calcification. However, the sen-sitivity of CT scans is not always adequate in detectingdisease, particularly in those with early stages of thiscondition (72).
Patients with severe EPS have a median time of5 months from onset of symptoms to a perceived needfor surgical intervention (71). This observation supportsa need for early diagnosis; thus, early peritoneal bi-opsies at the time of any abdominal surgery, such asduring catheter insertion, removal, or repositioning, maybe warranted.
Given a need for early diagnosis, studies to findadditional factors to aid in early identification of pa-tients at risk for disease have been conducted. In a PDcohort in the United Kingdom, the metabolic profile ormetabolome of the PD effluent was examined. Elevenpatients who developed EPS were compared with amatched control cohort. Several metabolites, specif-ically amino acids, amines, short fatty acids, and sugars,were identified to associate with the development ofEPS. Again, these findings were seen in patients beforethe onset of clinical symptoms and diagnosis of EPS.This suggests a potential utility in evaluating the meta-bolome of PD effluent to identify patients at risk beforethe development of EPS (75).Treatment and Outcomes of EPS. A lack of consensusexists for the ideal treatment of EPS, in part due to therarity of the disorder. Tamoxifen is an antifibroticagent, based on its ability to inhibit the production ofTGF-b, and case series suggested that beneficial out-comes can result in some patients taking this therapy.However, the utility of this drug is limited in part be-cause of the associated side effects, particularly the in-creased risk of thromboembolism (72). Immunosuppressiveregimens such as rapamycin and mycophenolate mofetilmay also provide an advantage in patients with EPS,based on animal models of peritoneal fibrosis (76,77).
Surgical treatment may be required when EPS isassociated with an acute abdomen, in the setting ofbowel obstruction, perforation, or hemoperitoneum.
360 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

Surgery is also considered when medical therapies failto reduce symptoms of bowel dysfunction. Surgicaltherapy was historically associated with a high degree ofmorbidity and mortality. However, with the advent ofnew surgical techniques and specialized referral cen-ters, better outcomes are now reported (72). Nonethe-less, EPS remains a devastating clinical consequenceof ESRD and PD therapy. Even though some reportscite comparable mortality rates in patients with EPScompared with the general dialysis population (71),other studies suggest that patients with EPS carry amortality rate of 43% (four times higher than thegeneral PD population) (73).
Home HemodialysisHHD has seen resurgence over the last decade,
and an increasing number of patients are consideringthis modality. HHD offers increased flexibility com-pared with in-center HD as well as the option to performmore intensive HD by increasing dialysis frequency andsession length. More frequent HHD has the potential tolead to improvement in clinical, biochemical, and healthoutcomes, in part due to better volume and BP control,improved clearance of small and middle molecules, andimproved quality of life (78). Frequent HHD can moreclosely mimic the physiology of native kidney function,with less fluid and electrolyte shifts compared withconventional thrice-weekly dialysis. As reviewed inother sections of this NephSAP, patients undergoing in-termittent HD thrice weekly exhibit an increased risk ofcardiac death on Mondays and Tuesdays after the longweekend interdialytic period. This daily variation ofcardiac death is not observed in patients who undergofrequent HHD (12).
No large, randomized controlled trials are avail-able to compare frequent HHD to conventional dialysis,but observational data suggest promising outcomes. AnAustralian cohort of 286 extended-hours HD patients(predominantly home nocturnal), reported 1-, 3-, and5-year survival rates of 98%, 92%, and 83%, respec-tively (79). Selection bias was likely in this study, giventhat patients who participated in HHD program tend tobe younger, healthier, and more independent comparedwith conventional in-center HD. However, full depen-dence on caregiver assistance to perform the HHD, suchas cannulation of vascular access and real-time clinicalmonitoring, does not appear to predict time to first hos-pitalization, technique failure, or death after adjustingfor baseline demographic differences (78).
With proper training and patient selection, HHDis safe, and the serious adverse event rate is reported aslow as 0.060 events per 1000 dialysis treatments (80).Proper training programs and advanced planning areimportant to optimize the success of any HHD program.Although “crash starts” can be successfully transitionedto an HHD program, there may be an increased risk ofadverse events in these patients. A retrospective co-hort study in HHD patients showed that suboptimalinitiation of dialysis (in the hospital or with a CVC)predicted a short interval for first hospitalization, tech-nique failure, and death (81).Vascular Access Issues with HHD/Frequent HD. TheFrequent Hemodialysis Network (FHN) daily trial andthe FHN nocturnal trial raised concerns about an in-creased rate of adverse vascular access events in pa-tients undergoing more frequent dialysis. In the FHNdaily trial, which compared frequent and shorter in-center dialysis with conventional thrice-weekly in-center dialysis, vascular access-related events weresignificantly more likely in the frequent dialysisgroup (82).
In the FHN nocturnal trial that compared homenocturnal dialysis (at least 6 hours per day and sixnights per week) with conventional dialysis, a similarconcern was identified. In this study, the proportion ofpatients using a fistula or graft was 53%. Patients and/orcaregivers cannulated the vascular access at home, and72% used a buttonhole technique (as discussed below)(82). In the nocturnal group, 23 of 45 patients reachedthe primary outcome of a vascular access-related eventcompared with 15 of 42 in the conventional group.Compared with conventional dialysis, the HR for avascular event in the nocturnal groups was 1.81 (95%CI, 0.94 to 3.48; P¼0.08). Although this did not reachstatistical significance, the HR was 3.23 (95% CI, 1.07to 10.35; P¼0.04) in the subgroup of patients with anAVF or AVG. Therefore, similar to the FHN daily trial,the FHN nocturnal trial showed an increased risk ofvascular access–related events in the nocturnal group inpatients using an AVF or AVG for dialysis (82). Asimilar trend was seen in an observational study of 286HHD patients (79). In this study, access event–free survivalat 1, 3, and 5 years was 80%, 68%, and 61%, respectively,and increasing dialysis frequency was associated with anincreased risk of developing a vascular access event (HR,1.56; 95% CI, 1.03 to 2.36: P¼0.04). In addition, access-related adverse events were associated with techniquefailure and mortality.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 361

Traditionally, the rope-ladder technique or rotatingcannulation sites were the standard approach to accessingan AVF. Alternatively, buttonhole needling is anotherapproach to accessing a fistula. Buttonhole needling usesa constant single site for arterial and venous access, andthis method requires the maturation of a tract that can ulti-mately be cannulated with blunt needles. The buttonholetechnique is frequently used in HHD patients because ofthe prevailing sentiment that it is easier to perform, is lesspainful, and is presumably less prone to vascular acces–related complications. This was suggested in the resultsfrom the FHNNocturnal Trial (82). In the FHNNocturnaltrial, participants who used the buttonhole technique hadlonger periods between access complications comparedwith those who used the rope-ladder technique (HR,0.44; 95%CI, 0.20 to 0.97; P¼0.04). However, a recentrandomized controlled trial reached an opposing con-clusion. MacRae and colleagues (83) compared button-hole and rope-ladder needling in a group of patients whoreceived HD in an outpatient facility. A total of 140patients were randomized in this study, and differencesin pain, bleeding, and rates of infection were ascertained.After 8 weeks, the study did not detect a statistical dif-ference in the mean pain score between the two groups;however, a greater proportion of patients in the button-hole group reported excess pain with a high pain score at8 weeks (OR, 2.15; 95% CI, 0.87 to 5.44; P¼0.07). Therate of hematoma formation was higher in the rope-ladder needling group (P¼0.03). However, the rate oflocalized infections was more than doubled in the button-hole group, with rates of 50 per 1000 dialysis sessionsin the buttonhole group compared with 22.4 per 1000sessions in the rope-ladder cannulation group (P¼0.003).The study also detected one episode of S. aureus bac-teremia in the buttonhole group and no episodes ofbacteremia in the control group. After study completionin a 12-month observation period, two more buttonholepatients developed S. aureus bacteremia. This trial waslimited by its relatively small number of patients andbecause it only investigated in-center patients, it did notaddress whether the results were affected by factors suchas colonized bacterial species. Regardless, this studyraises important hazards that may be associated with theroutine use of the buttonhole technique.
The buttonhole technique has been advanced asa possible method to improve primary patency rates.Chan and coworkers, however, found no advantage ofbuttonhole needling over rope-ladder needling withregard to primary patency (84).
Economics of HHD. Whether HHDwill be able to con-tain costs of care compared with conventional in-centerHD is a critical issue, especially given the increasingpopularity of the modality. A recent trial specificallyaddressed the cost issue of HHD in the Alberta (Canada)Nocturnal Home Dialysis trial (85). A cost-utility anal-ysis was performed to compare frequent nocturnal HHD(FHNHD) and conventional HD (including in-center,satellite center, or HHD with a conventional schedule).In this setting, the authors concluded that FHNHD wasmore cost-effective, and demonstrated cost savings of$6700 per year compared with conventional HD. Thecost of HD was greatest with in-center HD, followedby satellite center HD, followed by frequent NHD, andfinally, conventional HHD. There was a higher initialcost with FHNHD, primarily due to the cost of up-front training, but the cost of ongoing maintenance wasconsiderably lower than in-center HD owing to reducednursing and facility costs (85).
In a separate cost-modeling study, the authors sug-gested that FHNHD and conventional HHD were similarin cost to in-center HD during the first year (primarilydue to high start-up costs, home preparation, and train-ing costs), but were less costly after the first year onward(86). Both of these above analyses suggested that HHD,including frequent HHD, can be economically attractive.
References1. US Renal Data System: USRDS 2013 Annual Data Report: Atlas of
Chronic Kidney Disease and End-Stage Renal Disease in the UnitedStates, Bethesda, MD, National Institutes of Health, National Instituteof Diabetes and Digestive and Kidney Diseases, 2013
2. Jain AK, Blake P, Cordy P, Garg AX: Global trends in rates ofperitoneal dialysis. J Am Soc Nephrol 23: 533–544, 2012 PubMed
3. Hornberger J, Hirth RA: Financial implications of choice of dialysistype of the revised Medicare payment system: An economic analysis.Am J Kidney Dis 60: 280–287, 2012 PubMed
4. Chanouzas D, Ng KP, Fallouh B, Baharani J: What influences patientchoice of treatment modality at the pre-dialysis stage? Nephrol DialTransplant 27: 1542–1547, 2012 PubMed
5. Liebman SE, Bushinsky DA, Dolan JG, Veazie P: Differences betweendialysis modality selection and initiation. Am J Kidney Dis 59: 550–557,2012 PubMed
6. Prakash S, Perzynski AT, Austin PC, Wu CF, Lawless ME, PatersonJM, Quinn RR, Sehgal AR, Oliver MJ: Neighborhood socioeconomicstatus and barriers to peritoneal dialysis: A mixed methods study. Clin JAm Soc Nephrol 8: 1741–1749, 2013 PubMed
7. Castledine CI, Gilg JA, Rogers C, Ben-Shlomo Y, Caskey FJ: Renalcentre characteristics and physician practice patterns associatedwith homedialysis use. Nephrol Dial Transplant 28: 2169–2180, 2013 PubMed
8. Hingwala J, Diamond J, Tangri N, Bueti J, Rigatto C, Sood MM,Verrelli M, Komenda P: Underutilization of peritoneal dialysis: The roleof the nephrologist’s referral pattern. Nephrol Dial Transplant 28: 732–740, 2013 PubMed
9. Lukowsky LR, Mehrotra R, Kheifets L, Arah OA, Nissenson AR,Kalantar-Zadeh K: Comparing mortality of peritoneal and hemodialysis
362 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
patients in the first 2 years of dialysis therapy: A marginal structuralmodel analysis. Clin J Am Soc Nephrol 8: 619–628, 2013 PubMed
10. Yeates K, Zhu N, Vonesh E, Trpeski L, Blake P, Fenton S: Hemodi-alysis and peritoneal dialysis are associated with similar outcomes forend-stage renal disease treatment in Canada. Nephrol Dial Transplant27: 3568–3575, 2012 PubMed
11. Haapio M, Helve J, Kyllönen L, Grönhagen-Riska C, Finne P: Modalityof chronic renal replacement therapy and survival—a complete cohortfrom Finland, 2000-2009. Nephrol Dial Transplant 28: 3072–3081,2013 PubMed
12. Krishnasamy R, Badve SV, Hawley CM, McDonald SP, Boudville N,Brown FG, Polkinghorne KR, Bannister KM, Wiggins KJ, Clayton P,Johnson DW: Daily variation in death in patients treated by long-termdialysis: Comparison of in-center hemodialysis to peritoneal and homehemodialysis. Am J Kidney Dis 61: 96–103, 2013 PubMed
13. Foley RN, Gilbertson DT, Murray T, Collins AJ: Long interdialyticinterval and mortality among patients receiving hemodialysis. N Engl JMed 365: 1099–1107, 2011 PubMed
14. Gallieni M, Caputo F, Filippini A, Gabella P, Giannattasio M, StingoneA, Farina M; ROCK-PD Study Investigators: Prevalence and pro-gression of cardiovascular calcifications in peritoneal dialysis patients:A prospective study. Bone 51: 332–337, 2012 PubMed
15. Wang AY, Wang M, Lam CW, Chan IH, Lui SF, Sanderson JE: Heartfailure with preserved or reduced ejection fraction in patients treatedwith peritoneal dialysis. Am J Kidney Dis 61: 975–983, 2013 PubMed
16. Ito Y, MizunoM, Suzuki Y, Tamai H, Hiramatsu T, Ohashi H, Ito I, KasugaH, Horie M, Maruyama S, Yuzawa Y, Matsubara T, Matsuo S; NagoyaSpiro Study Group: Long-term effects of spironolactone in peritoneal dialysispatients. J Am Soc Nephrol 25: 1094–1102, 2014 PubMed
17. Torlén K, Kalantar-Zadeh K, Molnar MZ, Vashistha T, Mehrotra R:Serum potassium and cause-specific mortality in a large peritonealdialysis cohort. Clin J Am Soc Nephrol 7: 1272–1284, 2012 PubMed
18. McCafferty K, Fan S, Davenport A: Extracellular volume expansion,measured by multifrequency bioimpedance, does not help preserveresidual renal function in peritoneal dialysis patients. Kidney Int 85:151–157, 2014 PubMed
19. Perl J, Wald R, Bargman JM, Na Y, Jassal SV, Jain AK, Moist L,Nessim SJ: Changes in patient and technique survival over time amongincident peritoneal dialysis patients in Canada. Clin J Am Soc Nephrol7: 1145–1154, 2012 PubMed
20. Ishani A, Collins AJ, Herzog CA, Foley RN: Septicemia, access andcardiovascular disease in dialysis patients: The USRDS Wave 2 study.Kidney Int 68: 311–318, 2005 PubMed
21. Koch M, Kohnle M, Trapp R, Haastert B, Rump LC, Aker S:Comparable outcome of acute unplanned peritoneal dialysis andhaemodialysis. Nephrol Dial Transplant 27: 375–380, 2012 PubMed
22. Ivarsen P, Povlsen JV: Can peritoneal dialysis be applied for unplannedinitiation of chronic dialysis? [published online ahead of printDecember 17, 2013]. Nephrol Dial Transplant doi:10.1093/ndt/gft487 PubMed
23. Dombros N, Dratwa M, Feriani M, Gokal R, Heimburger O, Krediet R,Plum J, Rodrigues A, Selgas R, Struijk D, Verger C; EBPG ExpertGroup on Peritoneal Dialysis: European best practice guidelines forperitoneal dialysis. 3 Peritoneal access. Nephrol Dial Transplant 20[Suppl 9]: ix8–ix12, 2005
24. Ghaffari A: Urgent-start peritoneal dialysis: A quality improvementreport. Am J Kidney Dis 59: 400–408, 2012 PubMed
25. Chionh CY, Soni SS, Finkelstein FO, Ronco C, Cruz DN: Use ofperitoneal dialysis in AKI: A systematic review. Clin J Am Soc Nephrol8: 1649–1660, 2013 PubMed
26. Chui BK, Manns B, Pannu N, Dong J, Wiebe N, Jindal K, KlarenbachSW: Health care costs of peritoneal dialysis technique failure and dialysismodality switching. Am J Kidney Dis 61: 104–111, 2013 PubMed
27. Tong A, Lesmana B, Johnson DW, Wong G, Campbell D, Craig JC:The perspectives of adults living with peritoneal dialysis: Thematic synthesisof qualitative studies. Am J Kidney Dis 61: 873–888, 2013 PubMed
28. Béchade C, Guittet L, Evans D, Verger C, Ryckelynck JP, Lobbedez T:Early failure in patients starting peritoneal dialysis: A competing risksapproach [published online ahead of print September 26, 2013].Nephrol Dial Transplant doi:10.1093/ndt/gft055 PubMed
29. Lobbedez T, Verger C, Ryckelynck JP, Fabre E, Evans D: Is assistedperitoneal dialysis associated with technique survival when competingevents are considered? Clin J Am Soc Nephrol 7: 612–618, 2012 PubMed
30. McQuillan RF, Chiu E, Nessim S, Lok CE, Roscoe JM, Tam P, JassalSV: A randomized controlled trial comparing mupirocin and polysporintriple ointments in peritoneal dialysis patients: The MP3 Study. Clin JAm Soc Nephrol 7: 297–303, 2012 PubMed
31. Li PK, Szeto CC, Piraino B, Bernardini J, Figueiredo AE, Gupta A,Johnson DW, Kuijper EJ, Lye WC, Salzer W, Schaefer F, Struijk DG;International Society for Peritoneal Dialysis: Peritoneal dialysis-relatedinfections recommendations: 2010 update.Perit Dial Int 30: 393–423, 2010
32. van Diepen AT, Tomlinson GA, Jassal SV: The association betweenexit site infection and subsequent peritonitis among peritoneal dialysispatients. Clin J Am Soc Nephrol 7: 1266–1271, 2012 PubMed
33. Mujais S: Microbiology and outcomes of peritonitis in North America.Kidney Int Suppl 103[Suppl]: S55–S62, 2006 PubMed
34. Chua AN, Goldstein SL, Bell D, Brewer ED: Topical mupirocin/sodiumhypochlorite reduces peritonitis and exit-site infection rates in children.Clin J Am Soc Nephrol 4: 1939–1943, 2009 PubMed
35. Bernardini J, Bender F, Florio T, Sloand J, Palmmontalbano L, Fried L,Piraino B: Randomized, double-blind trial of antibiotic exit site creamfor prevention of exit site infection in peritoneal dialysis patients. J AmSoc Nephrol 16: 539–545, 2005 PubMed
36. Battistella M, Bhola C, Lok CE: Long-term follow-up of the Hemodi-alysis Infection Prevention with Polysporin Ointment (HIPPO) Study: Aquality improvement report. Am J Kidney Dis 57: 432–441, 2011 PubMed
37. Cho Y, Badve SV, Hawley CM, McDonald SP, Brown FG, BoudvilleN, Wiggins KJ, Bannister KM, Clayton PA, Johnson DW: Seasonalvariation in peritoneal dialysis-associated peritonitis: A multi-centreregistry study. Nephrol Dial Transplant 27: 2028–2036, 2012 PubMed
38. Dong J, Li Z, Xu R, Chen Y, Luo S, Li Y: Disease severity score couldnot predict the outcomes in peritoneal dialysis-associated peritonitis.Nephrol Dial Transplant 27: 2496–2501, 2012 PubMed
39. Boudville N, Kemp A, Clayton P, Lim W, Badve SV, Hawley CM,McDonald SP, Wiggins KJ, Bannister KM, Brown FG, Johnson DW:Recent peritonitis associates with mortality among patients treated withperitoneal dialysis. J Am Soc Nephrol 23: 1398–1405, 2012 PubMed
40. Badve SV, Hawley CM, McDonald SP, Brown FG, Boudville NC,Wiggins KJ, Bannister KM, Johnson DW: Use of aminoglycosides forperitoneal dialysis-associated peritonitis does not affect residual renalfunction. Nephrol Dial Transplant 27: 381–387, 2012 PubMed
41. Varghese JM, Roberts JA, Wallis SC, Boots RJ, Healy H, Fassett RG,Lipman J, Ranganathan D: Pharmacokinetics of intraperitoneal genta-micin in peritoneal dialysis patients with peritonitis (GIPD study). ClinJ Am Soc Nephrol 7: 1249–1256, 2012 PubMed
42. Lin CY, Roberts GW, Kift-Morgan A, Donovan KL, Topley N, EberlM: Pathogen-specific local immune fingerprints diagnose bacterialinfection in peritoneal dialysis patients. J Am Soc Nephrol 24: 2002–2009, 2013 PubMed
43. Chow KM, Szeto CC, Cheung KK, Leung CB, Wong SS, Law MC, HoYW, Li PK: Predictive value of dialysate cell counts in peritonitiscomplicating peritoneal dialysis. Clin J Am Soc Nephrol 1: 768–773,2006 PubMed
44. Szeto CC, Lai KB, Kwan BC, Chow KM, Leung CB, Law MC, Yu V,Li PK: Bacteria-derived DNA fragment in peritoneal dialysis effluent asa predictor of relapsing peritonitis. Clin J Am Soc Nephrol 8: 1935–1941, 2013 PubMed
45. Johnson DW, Brown FG, Clarke M, Boudville N, Elias TJ, Foo MW,Jones B, Kulkarni H, Langham R, Ranganathan D, Schollum J, SuranyiM, Tan SH, Voss D; balANZ Trial Investigators: Effects of bio-compatible versus standard fluid on peritoneal dialysis outcomes. JAm Soc Nephrol 23: 1097–1107, 2012 PubMed
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 363
46. Lui SL, Yung S, Yim A, Wong KM, Tong KL, Wong KS, Li CS, AuTC, Lo WK, Ho YW, Ng F, Tang C, Chan TM: A combination ofbiocompatible peritoneal dialysis solutions and residual renal function,peritoneal transport, and inflammation markers: A randomized clinicaltrial. Am J Kidney Dis 60: 966–975, 2012 PubMed
47. Kim S, Oh KH, Oh J, Kim SJ, ChungW, Song YR, Na KY, Oh YK, AhnC, Kim SG, Tan KC: Biocompatible peritoneal dialysis solution preservesresidual renal function. Am J Nephrol 36: 305–316, 2012 PubMed
48. Cho Y, Johnson DW, Badve S, Craig JC, Strippoli GF, Wiggins KJ:Impact of icodextrin on clinical outcomes in peritoneal dialysis: Asystematic review of randomized controlled trials. Nephrol Dial Trans-plant 28: 1899–1907, 2013 PubMed
49. Li PK, Culleton BF, Ariza A, Do JY, Johnson DW, Sanabria M,Shockley TR, Story K, Vatazin A, Verrelli M, Yu AW, Bargman JM;IMPENDIA and EDEN Study Groups: Randomized, controlled trial ofglucose-sparing peritoneal dialysis in diabetic patients. J Am SocNephrol 24: 1889–1900, 2013 PubMed
50. Johnson DW, Brown FG, Clarke M, Boudville N, Elias TJ, Foo MW,Jones B, Kulkarni H, Langham R, Ranganathan D, Schollum J, SuranyiMG, Tan SH, Voss D; balANZ Trial Investigators: The effect of lowglucose degradation product, neutral pH versus standard peritonealdialysis solutions on peritoneal membrane function: The balANZ trial.Nephrol Dial Transplant 27: 4445–4453, 2012 PubMed
51. Schmitt CP, Nau B, Gemulla G, Bonzel KE, Hölttä T, Testa S,Fischbach M, John U, Kemper MJ, Sander A, Arbeiter K, Schaefer F:Effect of the dialysis fluid buffer on peritoneal membrane function inchildren. Clin J Am Soc Nephrol 8: 108–115, 2013 PubMed
52. Raaijmakers R, Coester A, Smit W, Krediet RT, Schröder CH: Freewater transport in children on peritoneal dialysis is higher with morebiocompatible dialysis solutions, higher with older age and declineswith time. Nephrol Dial Transplant 27: 1183–1190, 2012 PubMed
53. Cho Y, Badve SV, Hawley CM, McDonald SP, Brown FG, BoudvilleN, Bannister KM, Clayton PA, Johnson DW: Association of bio-compatible peritoneal dialysis solutions with peritonitis risk, treatment,and outcomes. Clin J Am Soc Nephrol 8: 1556–1563, 2013 PubMed
54. Cho Y, Johnson DW, Badve SV, Craig JC, Strippoli GF, Wiggins KJ:The impact of neutral-pH peritoneal dialysates with reduced glucosedegradation products on clinical outcomes in peritoneal dialysis pa-tients. Kidney Int 84: 969–979, 2013 PubMed
55. Han SH, Ahn SV, Yun JY, Tranaeus A, Han DS: Effects of icodextrinon patient survival and technique success in patients undergoing perito-neal dialysis. Nephrol Dial Transplant 27: 2044–2050, 2012 PubMed
56. van Biesen W, Heimburger O, Krediet R, Rippe B, La Milia V, CovicA, Vanholder R; ERBP Working Group on Peritoneal Dialysis:Evaluation of peritoneal membrane characteristics: Clinical advice forprescription management by the ERBP working group. Nephrol DialTransplant 25: 2052–2062, 2010
57. Van Overmeire L, Goffin E, Krzesinski JM, Saint-Remy A, Bovy P,Cornet G, Bovy C: Peritoneal equilibration test with conventional ‘lowpH/high glucose degradation product’ or with biocompatible ‘normalpH/low glucose degradation product’ dialysates: Does it matter? NephrolDial Transplant 28: 1946–1951, 2013 PubMed
58. Yu Z, Lambie M, Davies SJ: Longitudinal study of small solutetransport and peritoneal protein clearance in peritoneal dialysis patients.Clin J Am Soc Nephrol 9: 326–334, 2014 PubMed
59. Voss D, Hawkins S, Poole G, Marshall M: Radiological versus surgicalimplantation of first catheter for peritoneal dialysis: A randomized non-inferiority trial. Nephrol Dial Transplant 27: 4196–4204, 2012 PubMed
60. Miller M, McCormick B, Lavoie S, Biyani M, Zimmerman D:Fluoroscopic manipulation of peritoneal dialysis catheters: Outcomesand factors associated with successful manipulation. Clin J Am SocNephrol 7: 795–800, 2012 PubMed
61. Chen G, Wang P, Liu H, Zhou L, ChengM, Liu Y, Zhang H, Li J, Sun L,Peng Y, Liu F: Greater omentum folding in the open surgical placement ofperitoneal dialysis catheters: A randomized controlled study and systemicreview. Nephrol Dial Transplant 29: 687–697, 2014 PubMed
62. Hagen SM, Lafranca JA, IJzermans JN, Dor FJ: A systematic review andmeta-analysis of the influence of peritoneal dialysis catheter type on com-plication rate and catheter survival. Kidney Int 85: 920–932, 2014 PubMed
63. Rosengren BI, Sagstad SJ, Karlsen TV, Wiig H: Isolation of interstitialfluid and demonstration of local proinflammatory cytokine productionand increased absorptive gradient in chronic peritoneal dialysis. Am JPhysiol Renal Physiol 304: F198–F206, 2013 PubMed
64. Catar R, Witowski J, Wagner P, Annett Schramm I, Kawka E, PhilippeA, Dragun D, Jörres A: The proto-oncogene c-Fos transcriptionallyregulates VEGF production during peritoneal inflammation. Kidney Int84: 1119–1128, 2013 PubMed
65. Kato H, Mizuno T, Mizuno M, Sawai A, Suzuki Y, Kinashi H, NaguraF, Maruyama S, Noda Y, Yamada K, Matsuo S, Ito Y: Atrial natriureticpeptide ameliorates peritoneal fibrosis in rat peritonitis model. NephrolDial Transplant 27: 526–536, 2012 PubMed
66. Tayama Y, Hasegawa H, Takayanagi K, Matsuda A, Shimizu T,Asakura J, Iwashita T, Ogawa T, Katoh H, Mitarai T: Prevention oflipopolysaccharide-induced peritoneal damage by eplerenone in ratsundergoing peritoneal dialysis. J Nephrol 26: 1160–1169, 2013 PubMed
67. Bui DS, Seguro AC, Shimitzu MH, Schliemann I, Martini D, Romão JEJr, Pecoits Filho RF, Abensur H: N-Acetylcysteine protects theperitoneum from the injury induced by hypertonic dialysis solution. JNephrol 25: 90–95, 2012 PubMed
68. Pletinck A, Van Landschoot M, Steppan S, Laukens D, Passlick-Deetjen J, Vanholder R, Van Biesen W: Oral supplementation withsulodexide inhibits neo-angiogenesis in a rat model of peritonealperfusion. Nephrol Dial Transplant 27: 548–556, 2012 PubMed
69. Kratochwill K, Boehm M, Herzog R, Lichtenauer AM, Salzer E,Lechner M, Kuster L, Bergmeister K, Rizzi A, Mayer B, Aufricht C:Alanyl-glutamine dipeptide restores the cytoprotective stress proteomeof mesothelial cells exposed to peritoneal dialysis fluids. Nephrol DialTransplant 27: 937–946, 2012 PubMed
70. Bastug F, Gündüz Z, Tülpar S, Torun YA, Akgün H, Dörterler E,Düsünsel R, Poyrazoglu H, Bastug O, Dursun I, Yel S: Mesenchymalstem cell transplantation may provide a new therapy for ultrafiltrationfailure in chronic peritoneal dialysis. Nephrol Dial Transplant 28:2493–2501, 2013 PubMed
71. Latus J, Ulmer C, Fritz P, Rettenmaier B, Biegger D, Lang T, Ott G,Scharpf C, Kimmel M, Steurer W, Alscher MD, Braun N: Encapsulat-ing peritoneal sclerosis: A rare, serious but potentially curable compli-cation of peritoneal dialysis-experience of a referral centre in Germany.Nephrol Dial Transplant 28: 1021–1030, 2013 PubMed
72. Stefanidis CJ, Shroff R: Encapsulating peritoneal sclerosis in children[published online ahead of print November 21, 2013]. Pediatr Nephroldoi:10.1007/s00467-013-2672-8 PubMed
73. Vidal E, Edefonti A, Puteo F, Chimenz R, Gianoglio B, Lavoratti G,Leozappa G, Maringhini S, Mencarelli F, Pecoraro C, Ratsch IM,Cannavò R, De Palo T, Testa S, Murer L, Verrina E; Italian Registry ofPediatric Chronic Dialysis: Encapsulating peritoneal sclerosis in paedi-atric peritoneal dialysis patients: The experience of the Italian Registryof Pediatric Chronic Dialysis. Nephrol Dial Transplant 28: 1603–1609,2013 PubMed
74. Shroff R, Stefanidis CJ, Askiti V, Edefonti A, Testa S, Ekim M, KavazA, Ariceta G, Bakkaloglu S, FischbachM, Klaus G, Zurowska A, HolttaT, Jankauskiene A, Vondrak K, Vande Walle J, Schmitt CP, WatsonAR; European Paediatric Dialysis Working Group: Encapsulatingperitoneal sclerosis in children on chronic PD: A survey from theEuropean Paediatric Dialysis Working Group. Nephrol Dial Transplant28: 1908–1914, 2013 PubMed
75. Dunn WB, Summers A, Brown M, Goodacre R, Lambie M, Johnson T,Wilkie M, Davies S, Topley N, Brenchley P: Proof-of-principle study todetect metabolic changes in peritoneal dialysis effluent in patients whodevelop encapsulating peritoneal sclerosis. Nephrol Dial Transplant 27:2502–2510, 2012 PubMed
76. Xu T, Xie JY, Wang WM, Ren H, Chen N: Impact of rapamycin on perito-neal fibrosis and transport function. Blood Purif 34: 48–57, 2012 PubMed
364 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

77. Hur E, Bozkurt D, Timur O, Bicak S, Sarsik B, Akcicek F, Duman S:The effects of mycophenolate mofetil on encapsulated peritonealsclerosis model in rats. Clin Nephrol 77: 1–7, 2012 PubMed
78. Tennankore K, Nadeau-Fredette AC, Chan CT: Intensified homehemodialysis: Clinical benefits, risks and target populations. NephrolDial Transplant 29: 1342–1349, 2014 PubMed
79. Jun M, Jardine MJ, Gray N, Masterson R, Kerr PG, Agar JW, HawleyCM, van Eps C, Cass A, Gallagher M, Perkovic V: Outcomes ofextended-hours hemodialysis performed predominantly at home. Am JKidney Dis 61: 247–253, 2013 PubMed
80. Wong B, Zimmerman D, Reintjes F, Courtney M, Klarenbach S,Dowling G, Pauly RP: Procedure-related serious adverse events amonghome hemodialysis patients: A quality assurance perspective. Am JKidney Dis 63: 251–258, 2014 PubMed
81. Nadeau-Fredette AC, Tennankore KK, Kim SJ, Chan CT: Suboptimalinitiation of home hemodialysis: Determinants and clinical outcomes.Nephron Clin Pract 124: 132–140, 2013 PubMed
82. Suri RS, Larive B, Sherer S, Eggers P, Gassman J, James SH, Lindsay RM,Lockridge RS, Ornt DB, Rocco MV, Ting GO, Kliger AS; FrequentHemodialysis Network Trial Group: Risk of vascular access complicationswith frequent hemodialysis. J Am Soc Nephrol 24: 498–505, 2013 PubMed
83. MacRae JM, Ahmed SB, Atkar R, Hemmelgarn BR: A randomized trialcomparing buttonhole with rope ladder needling in conventional hemo-dialysis patients. Clin J Am Soc Nephrol 7: 1632–1638, 2012 PubMed
84. Chan MR, Shobande O, Vats H, Wakeen M, Meyer X, Bellingham J,Astor BC, Yevzlin AS: The effect of buttonhole cannulation vs. rope-ladder technique on hemodialysis access patency. Semin Dial 27: 210–216, 2014 PubMed
85. Klarenbach S, Tonelli M, Pauly R, Walsh M, Culleton B, So H,Hemmelgarn B, Manns B: Economic evaluation of frequent homenocturnal hemodialysis based on a randomized controlled trial. J AmSoc Nephrol 25: 587–594, 2014 PubMed
86. Komenda P, Gavaghan MB, Garfield SS, Poret AW, Sood MM: Aneconomic assessment model for in-center, conventional home, and morefrequent home hemodialysis. Kidney Int 81: 307–313, 2012 PubMed
Management Quandaries in ESRD
Uremic Toxins, Biomarkers, and DialysisClearance of urea is used as a traditional measure
for the efficacy of dialysis. However, it may not be ap-propriate to rely solely on urea as the primary indexsolute to assess adequacy of dialysis. For example, solutesthat are normally cleared by tubular secretion of thenative kidney (as opposed to glomerular filtration) suchas phenylacetylglutamine, hippurate, indoxyl sulfate,and p-cresol sulfate could serve as markers of effectivedialysis (1). In one study, the predialysis serum con-centrations of these molecules were determined to be41- to 122-fold higher in maintenance dialysis patientsthan in controls who had normal kidney function (1). Thedialytic clearance rates of these molecules were only0.16- to 0.39-fold compared with normal individuals, andclearances were much lower than the rates for urea andfor creatinine. It is plausible, although unproven, thatbetter clearance of substances normally secreted by thetubules will improve outcomes in dialysis patients.
Natriuretic Peptides as Biomarkers in ESRD. Evidenceis growing that cardiac natriuretic peptides will effectivelyserve to identify ESRD patients who have evidence ofvolume excess and who carry excessive cardiac riskburden. The clinical utility of these markers may be thatthe natriuretic peptides serve as alternate measures ofvolume status. Predialysis levels of atrial natriureticpeptides correlate best with volume status, but post-dialysis levels are less reliable. In one recent study ofhypertensive dialysis patients, the concentration ofB-type natriuretic peptide (BNP) failed to correlate withsystematic reduction in the target weight or in decreasesin BP (2). Regardless, related peptides could still serveas risk indicators in dialysis patients. In a recent cross-sectional study of 239 stable hemodialysis (HD) patients,it was found that several peptides including mid-regionalproatrial natriuretic peptide, BNP, and N-terminal-pro-BNPall correlated with age, ventricular systolic dysfunction,and 2-year mortality (3). In a historical cohort of 211prevalent HD patients, BNP was also demonstrated tocorrelate with cardiovascular events, but the cardiac markerdid not associate with clinical events as well as the tra-ditional determinants such as the type of vascular access,serum albumin concentration, or presence of diastolicdysfunction (4). Thus, these cardiac biomarkers may notperform as “standalone” indicators, but they may serve asancillary predictors of clinical outcome.Troponin T as a Biomarker in ESRD. Cardiactroponins are structural proteins that originate from themyocardium, and the concentrations of these proteinsare frequently elevated in ESRD patients. The cause andimplications of elevated troponin levels in this popula-tion are unknown. Concentrations of troponin T were ex-plored in 70 prevalent HD patients (5). In this study,troponin T levels correlated significantly with echocar-diographic evidence for “myocardial stunning” duringthe HD procedure. In multivariable analysis, only ultrafil-tration volume (odds ratio [OR], 4.38; 95% confidenceinterval [CI], 1.01–18.24; P=0.04, for every 1 liter ultra-filtered) and troponin T (OR, 9.33; 95% CI, 1.63–53.43;P=0.01, for every additional 0.1 ng/ml) were indepen-dently associated with myocardial stunning. This obser-vation is potentially important, because intradialyticstunning is proposed as one mediator of cardiac remodel-ing in HD patients.Fibroblast Growth Factor-23 as a Biomarker. Dis-turbed mineral metabolism is a near-universal complicationof CKD, and abnormal components of this metabolismare linked to risks of ESRD, cardiovascular disease, and
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 365
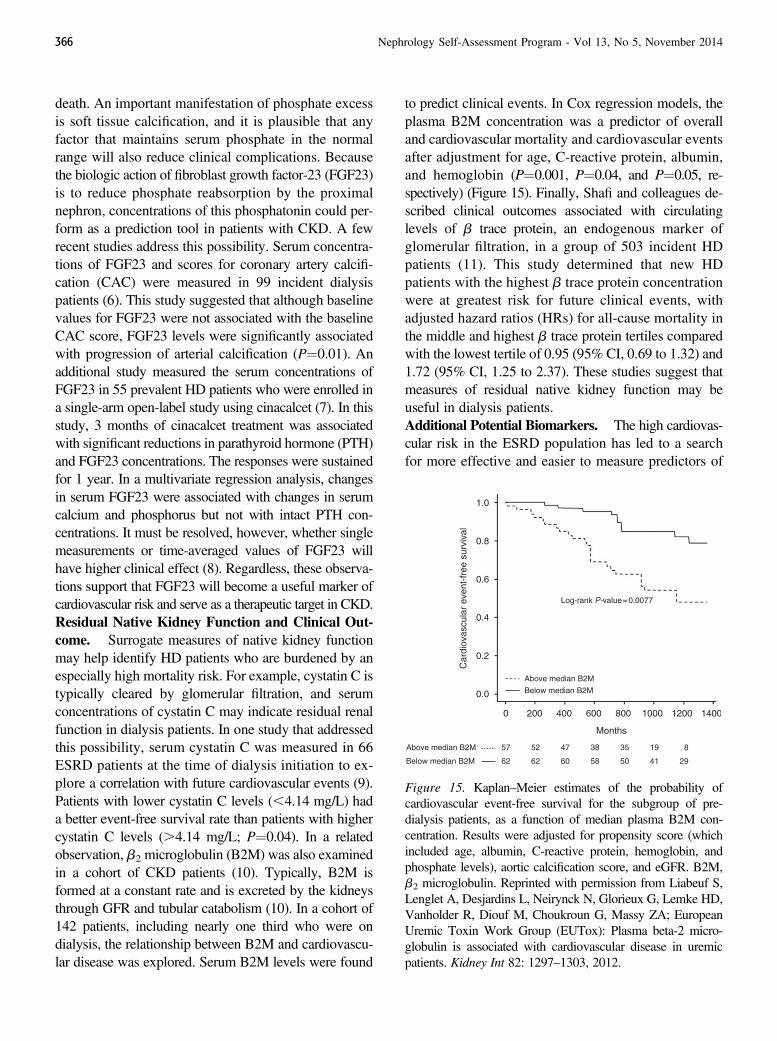
death. An important manifestation of phosphate excessis soft tissue calcification, and it is plausible that anyfactor that maintains serum phosphate in the normalrange will also reduce clinical complications. Becausethe biologic action of fibroblast growth factor-23 (FGF23)is to reduce phosphate reabsorption by the proximalnephron, concentrations of this phosphatonin could per-form as a prediction tool in patients with CKD. A fewrecent studies address this possibility. Serum concentra-tions of FGF23 and scores for coronary artery calcifi-cation (CAC) were measured in 99 incident dialysispatients (6). This study suggested that although baselinevalues for FGF23 were not associated with the baselineCAC score, FGF23 levels were significantly associatedwith progression of arterial calcification (P¼0.01). Anadditional study measured the serum concentrations ofFGF23 in 55 prevalent HD patients who were enrolled ina single-arm open-label study using cinacalcet (7). In thisstudy, 3 months of cinacalcet treatment was associatedwith significant reductions in parathyroid hormone (PTH)and FGF23 concentrations. The responses were sustainedfor 1 year. In a multivariate regression analysis, changesin serum FGF23 were associated with changes in serumcalcium and phosphorus but not with intact PTH con-centrations. It must be resolved, however, whether singlemeasurements or time-averaged values of FGF23 willhave higher clinical effect (8). Regardless, these observa-tions support that FGF23 will become a useful marker ofcardiovascular risk and serve as a therapeutic target in CKD.Residual Native Kidney Function and Clinical Out-come. Surrogate measures of native kidney functionmay help identify HD patients who are burdened by anespecially high mortality risk. For example, cystatin C istypically cleared by glomerular filtration, and serumconcentrations of cystatin C may indicate residual renalfunction in dialysis patients. In one study that addressedthis possibility, serum cystatin C was measured in 66ESRD patients at the time of dialysis initiation to ex-plore a correlation with future cardiovascular events (9).Patients with lower cystatin C levels (,4.14 mg/L) hada better event-free survival rate than patients with highercystatin C levels (.4.14 mg/L; P¼0.04). In a relatedobservation, b2 microglobulin (B2M) was also examinedin a cohort of CKD patients (10). Typically, B2M isformed at a constant rate and is excreted by the kidneysthrough GFR and tubular catabolism (10). In a cohort of142 patients, including nearly one third who were ondialysis, the relationship between B2M and cardiovascu-lar disease was explored. Serum B2M levels were found
to predict clinical events. In Cox regression models, theplasma B2M concentration was a predictor of overalland cardiovascular mortality and cardiovascular eventsafter adjustment for age, C-reactive protein, albumin,and hemoglobin (P¼0.001, P¼0.04, and P¼0.05, re-spectively) (Figure 15). Finally, Shafi and colleagues de-scribed clinical outcomes associated with circulatinglevels of b trace protein, an endogenous marker ofglomerular filtration, in a group of 503 incident HDpatients (11). This study determined that new HDpatients with the highest b trace protein concentrationwere at greatest risk for future clinical events, withadjusted hazard ratios (HRs) for all-cause mortality inthe middle and highest b trace protein tertiles comparedwith the lowest tertile of 0.95 (95% CI, 0.69 to 1.32) and1.72 (95% CI, 1.25 to 2.37). These studies suggest thatmeasures of residual native kidney function may beuseful in dialysis patients.Additional Potential Biomarkers. The high cardiovas-cular risk in the ESRD population has led to a searchfor more effective and easier to measure predictors of
Figure 15. Kaplan–Meier estimates of the probability ofcardiovascular event-free survival for the subgroup of pre-dialysis patients, as a function of median plasma B2M con-centration. Results were adjusted for propensity score (whichincluded age, albumin, C-reactive protein, hemoglobin, andphosphate levels), aortic calcification score, and eGFR. B2M,b2 microglobulin. Reprinted with permission from Liabeuf S,Lenglet A, Desjardins L, Neirynck N, Glorieux G, Lemke HD,Vanholder R, Diouf M, Choukroun G, Massy ZA; EuropeanUremic Toxin Work Group (EUTox): Plasma beta-2 micro-globulin is associated with cardiovascular disease in uremicpatients. Kidney Int 82: 1297–1303, 2012.
366 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

outcome. The impetus for this line of investigation is thepresumption that patients predicted to be at a particularlyhigh risk could be managed in a way that would improvethe odds of survival free from cardiovascular compli-cations. Associations have been demonstrated amongcardiovascular events or mortality and a broad array ofbiomarkers. For example, high mortality was demon-strated to be associated with polymorphisms of a hemeoxygenase (HO-1) microsatellite (12), low serum con-centrations of IGF-1 (13), higher circulating concentrationsof carbamylated proteins (14), and higher resistin con-centrations (15) in certain populations of dialysis patients.However, other possible indicators, such as plasmaconcentrations of a-tocopherol, may lack utility as a bio-marker due to competing coexistent conditions such asmalnutrition (16).Oxidative Stress and Systemic Inflammation. Oxi-dative stress is widely regarded as a key contributor tocardiovascular injury. Therapeutic interventions thattarget chronic inflammation in ESRD patients may leadto improved outcomes. For example, a small pro-spective trial suggested that pentoxifylline 400 mg/d for4 months resulted in significant reductions in serum con-centrations of TNF-a, IL-6, and C-reactive protein com-paredwith placebo (17). Puchades and colleagues examinedmarkers of oxidative stress in patients with CKD andESRD who were treated with either HD or peritonealdialysis (PD) (18). The 160 patients in this study weredivided into control, predialysis, HD, and PD groups.Compared with normal controls, the predialysis, HD,and PD groups demonstrated significantly higher con-centrations of products derived from molecular oxida-tion with a significant decrease in antioxidant enzymes.The PD patients were found to exhibit the best oxidativebalance compared with predialysis and HD patients.
Perceived Quality of Life, Sleep Disorders,Restless Leg Syndrome, NeuropsychiatricDisorders, and Pruritus in Dialysis Patients
Dialysis is capable of prolonging a patient’s life,but the regimen often reduces or impairs the quality ofthat life. The perceived quality of a life spent on dialysisis affected by processes that are often taken for grantedin the general population, including the nature and abun-dance of sleep, the onset of restless leg syndrome (RLS),and symptoms associated with uremic pruritus. Recentstudies evaluated the relationships among these aspectsof daily life and implications on quality of life (QOL),health, and mortality.
Sleep Disorders in ESRD. The association of sleep dis-turbances with symptoms of depression was confirmedin a cross-sectional study involving 168 chronic HD pa-tients (19). Sleep quality (initiation, maintenance, andadequacy) was evaluated using the sleep subscale bat-tery of the Choice for Healthy Outcomes in Caring forESRD Health Experience Questionnaire. Symptoms ofdepression were assessed using the Center for Epidemio-logical Studies of Depression (CESD) scale. Impair-ment in sleep quality was strongly associated withhigher CESD scores, suggesting that dialysis patientswith worse sleep quality were more likely to have symp-toms of depression (19). This same study failed to showany association between sleep disturbances and formalmeasurements of cognitive function. This study did notaddress whether poor sleep quality directly affects sur-vival in ESRD patients. The association of sleep dis-orders and patient survival was recently studied in 128HD patients, in whom 45.6% were estimated to have dis-turbance in sleep based on the Pittsburgh Sleep QualityIndex screening questionnaire (20). The presence of sleepproblems had no significant association between hemo-globin, serum albumin, Kt/V, or patient satisfaction withthe care providers. Moreover, the presence of sleep dis-turbance was not associated with patient survival. Theconclusion of this study contrasts with an analysis of datacollected by the Dialysis Outcomes and Practice PatternsStudy (DOPPS) that seemed to indicate that sleep qualitywas a predictor of QOL and mortality risk (21).Restless Leg Syndrome. RLS is a sensorimotordisorder characterized by uncomfortable or unpleasantsensations and an urge to move the lower extremities.The symptoms are usually incited during periods of rest,are aggravated in the evening, and are at least partiallyameliorated by movement (22). The prevalence of RLSin HD patients is quite high, ranging between 7% and45% (22). The pathophysiology of this disorder remainsunknown. In patients with ESRD, the symptoms of RLSsignificantly improve after kidney transplantation, sug-gesting that uremia may play a role. Several metabolicand hormonal pathways are postulated to be etiologicfactors. These include dysfunction of the dopaminergicsystem, anemia, diminished iron stores, disrupted min-eral metabolism, sympathetic nervous system activa-tion, and peripheral neuropathy (22,23). Recent evidencealso suggests that hyperhomocysteinemia may play a rolein the pathogenesis of uremic RLS. In a study of 52 prev-alent HD patients, a significant positive correlationwas reported between total plasma homocysteine and the
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 367

diagnosis of RLS (24). Pharmacologic treatment mayreduce symptoms of RLS by as much as 60%–75%,depending on the drug used. Current treatment strate-gies include the use of dopaminergic agonists such asropinirole, pramipexole, pergolide, and cabergoline,as well as administration of gabapentin. The nonergotdopaminergic agonists ropinirole and pramipexole arethe first-line agents for the treatment for RLS. Levodopahas a higher side-effect profile and may augment symp-toms of RLS with long-term use. Gabapentin may be ofparticular benefit in patients with insomnia, chronic pain,or peripheral neuropathy. Correction of anemia and de-pleted iron stores, aerobic exercise (especially in patientswith symptoms predominantly during HD sessions), shortdaily home HD, and changing the HD schedule to earlymorning sessions have all been found to aid the treatmentof RLS (25,26).Mental Health and Depression. Depression is the mostcommon psychologic disorder seen in chronic dialysispatients. Although the mechanism is unknown, depres-sion is associated with adverse clinical outcomes andincreased mortality in dialysis. A recent retrospective,observational study of 6415 incident HD patients eval-uated the relationship between depression and mortality(27). In this study, self-reported depressive symptoms(based on two questions from the Short Form-36) withinthe first 90 days of HD initiation were correlated withmortality. After 1-year follow-up, patients who reporteddepressive symptoms had a 32% increase in mortalitycompared with those who did not report these symptoms.The patients with depression were more likely to beyoung and have lower serum concentrations of albuminand creatinine.Cognitive Function in Dialysis. Cognitive impairmentis a common but frequently undiagnosed entity in theaging ESRD population. It is estimated that as many astwo thirds of dialysis patients have moderate to severecognitive impairment, which is a prevalence significantlyhigher than age-matched controls (28,29). Cognitive im-pairment is associated with increased hospitalizationrates, decreased QOL, increased health care–related ex-pense, and increased morbidity and mortality. Unfortu-nately, there is currently no neurocognitive test that hasbeen validated for routine screening of cognitive im-pairment in this population. A recent study attempted toassess the utility of the self-administered Kidney DiseaseQuality of Life-Cognitive Function (KDQOL-CF) scaleas a screening tool for cognitive impairment (30). Thestudy included 168 HD patients, and 24% of the cohort
had a KDQOL-CF score#60, consistent with cognitiveimpairment. However, the KDQOL-CF score had poorcorrelation compared with a more extensive and detailedneuropsychological battery of tests that ascertained a widerange of cognitive domains. This study suggests that thisrelatively simple instrument has limited use in screeningfor cognitive impairment in the dialysis population.Pruritus. CKD-related pruritus, another possible contri-butor to a patient’s sense of satisfaction and well-being,is reported to result from an imbalance in the endog-enous opioid peptides in the central nervous system.Prior studies determined that HD patients complainingof severe pruritus have downregulation of the k-systemof opioid receptors. In fact, the use of the k-receptoragonist nalfurafine for 2 weeks significantly reducedpruritus in 337HDpatients (31).More recently, a prospec-tive, open-label trial was reported in which the use ofnalfurafine was compared with placebo in 211 HD patientswho had severe, refractory pruritus (32). Nalfurafine, ata dose of 5 mg daily, was administered for 52 weeks, andpatients self-assessed pruritus severity using a visual an-alogue scale (100-mm horizontal line score). Nalfurafineassignment was associated with a significant decrease inthe pruritus severity score, from 75.2 mm (95% CI, 73.5to 76.9) to 50.9 mm (95% CI, 47.6 to 54.3) after 2 weeksand to 30.9 mm by week 52. In this study, nalfurafinewas well tolerated and was not associated with psycho-logical or physical dependence.
A prospective open-label trial evaluated the ef-ficacy of gabapentin and pregabalin in the treatment ofsevere pruritus in a cohort of 71 patients with stage 4–5CKD, including patients on HD and PD (33). Gabapentinwas started at 100 mg once daily in CKD and PD patientsand 100 mg after dialysis in HD patients. Pregabalin wasinitiated at 25 mg once daily and 25 mg after dialysis,respectively. In this study, 85% of patients who receivedgabapentin or pregabalin experienced significant reliefof pruritus. In most circumstances, the antipruritic ef-fect was achieved after the first or second doses. Themost common side effect reported in this trial was over-sedation. The usefulness of gabapentin and pregabalin inrelieving symptoms of pruritus in HD patients was alsoconfirmed in a recent smaller trial (34).
Pregnancy in ESRDPregnancy is uncommon in the ESRD population,
particularly in patients who receive HD. The US RenalData System (USRDS) reported a pregnancy rate of 27.5per 1000 years in dialysis patients (35). Unfortunately,
368 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
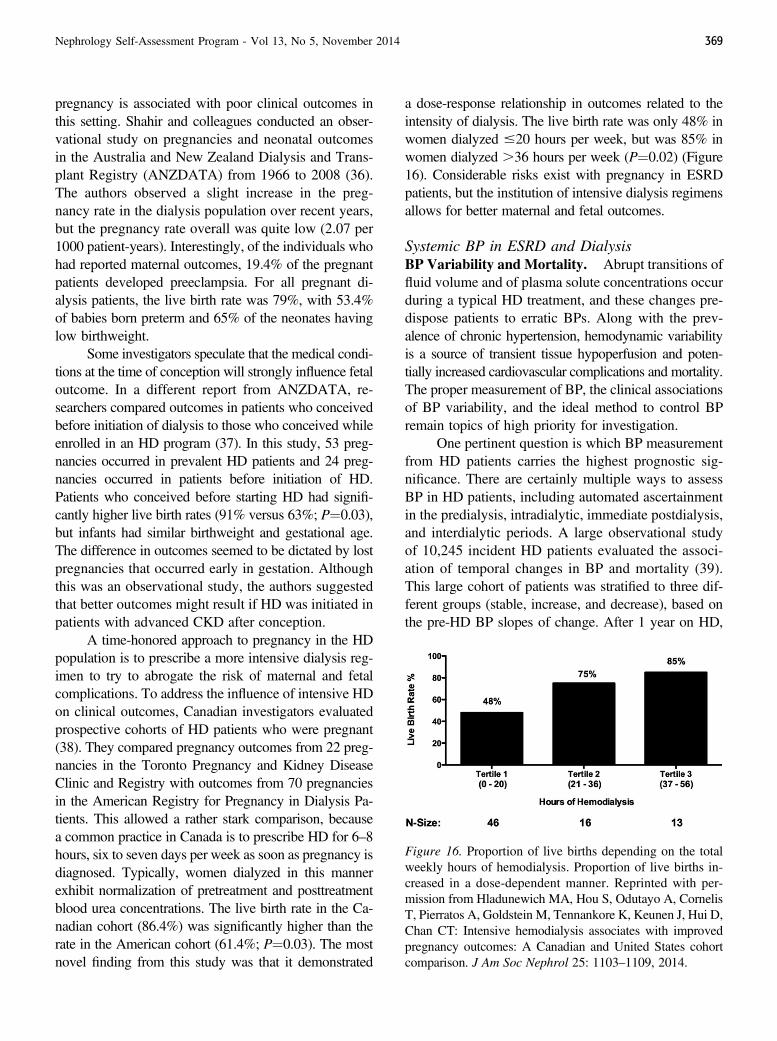
pregnancy is associated with poor clinical outcomes inthis setting. Shahir and colleagues conducted an obser-vational study on pregnancies and neonatal outcomesin the Australia and New Zealand Dialysis and Trans-plant Registry (ANZDATA) from 1966 to 2008 (36).The authors observed a slight increase in the preg-nancy rate in the dialysis population over recent years,but the pregnancy rate overall was quite low (2.07 per1000 patient-years). Interestingly, of the individuals whohad reported maternal outcomes, 19.4% of the pregnantpatients developed preeclampsia. For all pregnant di-alysis patients, the live birth rate was 79%, with 53.4%of babies born preterm and 65% of the neonates havinglow birthweight.
Some investigators speculate that the medical condi-tions at the time of conception will strongly influence fetaloutcome. In a different report from ANZDATA, re-searchers compared outcomes in patients who conceivedbefore initiation of dialysis to those who conceived whileenrolled in an HD program (37). In this study, 53 preg-nancies occurred in prevalent HD patients and 24 preg-nancies occurred in patients before initiation of HD.Patients who conceived before starting HD had signifi-cantly higher live birth rates (91% versus 63%; P¼0.03),but infants had similar birthweight and gestational age.The difference in outcomes seemed to be dictated by lostpregnancies that occurred early in gestation. Althoughthis was an observational study, the authors suggestedthat better outcomes might result if HD was initiated inpatients with advanced CKD after conception.
A time-honored approach to pregnancy in the HDpopulation is to prescribe a more intensive dialysis reg-imen to try to abrogate the risk of maternal and fetalcomplications. To address the influence of intensive HDon clinical outcomes, Canadian investigators evaluatedprospective cohorts of HD patients who were pregnant(38). They compared pregnancy outcomes from 22 preg-nancies in the Toronto Pregnancy and Kidney DiseaseClinic and Registry with outcomes from 70 pregnanciesin the American Registry for Pregnancy in Dialysis Pa-tients. This allowed a rather stark comparison, becausea common practice in Canada is to prescribe HD for 6–8hours, six to seven days per week as soon as pregnancy isdiagnosed. Typically, women dialyzed in this mannerexhibit normalization of pretreatment and posttreatmentblood urea concentrations. The live birth rate in the Ca-nadian cohort (86.4%) was significantly higher than therate in the American cohort (61.4%; P¼0.03). The mostnovel finding from this study was that it demonstrated
a dose-response relationship in outcomes related to theintensity of dialysis. The live birth rate was only 48% inwomen dialyzed #20 hours per week, but was 85% inwomen dialyzed .36 hours per week (P¼0.02) (Figure16). Considerable risks exist with pregnancy in ESRDpatients, but the institution of intensive dialysis regimensallows for better maternal and fetal outcomes.
Systemic BP in ESRD and DialysisBP Variability and Mortality. Abrupt transitions offluid volume and of plasma solute concentrations occurduring a typical HD treatment, and these changes pre-dispose patients to erratic BPs. Along with the prev-alence of chronic hypertension, hemodynamic variabilityis a source of transient tissue hypoperfusion and poten-tially increased cardiovascular complications and mortality.The proper measurement of BP, the clinical associationsof BP variability, and the ideal method to control BPremain topics of high priority for investigation.
One pertinent question is which BP measurementfrom HD patients carries the highest prognostic sig-nificance. There are certainly multiple ways to assessBP in HD patients, including automated ascertainmentin the predialysis, intradialytic, immediate postdialysis,and interdialytic periods. A large observational studyof 10,245 incident HD patients evaluated the associ-ation of temporal changes in BP and mortality (39).This large cohort of patients was stratified to three dif-ferent groups (stable, increase, and decrease), based onthe pre-HD BP slopes of change. After 1 year on HD,
Figure 16. Proportion of live births depending on the totalweekly hours of hemodialysis. Proportion of live births in-creased in a dose-dependent manner. Reprinted with per-mission from Hladunewich MA, Hou S, Odutayo A, CornelisT, Pierratos A, Goldstein M, Tennankore K, Keunen J, Hui D,Chan CT: Intensive hemodialysis associates with improvedpregnancy outcomes: A Canadian and United States cohortcomparison. J Am Soc Nephrol 25: 1103–1109, 2014.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 369

patients with more stable BP measurements surroundingthe HD treatments had a significantly lower mortalityrate compared with those with either a steady increaseor decrease in recorded BP. These findings were in-dependent of absolute BP levels and persisted 2 yearsafter initiation of HD.
Patient adherence to recommended medical anddietary regimens, particularly as it pertains to interdialyticweight gains, influences BP variability. In traditionalthrice-weekly HD schedules, BP variability is highestat the beginning of the week when volume excess is moreprevalent (40). Two recent studies examined whetherBP variability during a HD treatment was associatedwith adverse patient outcomes, specifically all-causeand cardiovascular mortality (41,42). In a retrospectivestudy of 6393 prevalent adult HD patients in the UnitedStates, the risks associated with BP variability wereexplored (41). This study demonstrated that systolic BPvariability that was above the median for the cohort (asmeasured with automated oscillometric devices) wassignificantly associated with all-cause mortality (HR,1.51; 95% CI, 1.30 to 1.76; P,0.001). This associationpersisted after multivariable adjustment for potentialconfounders. The higher systolic BP variability was alsopositively correlated with cardiovascular mortality (HR,1.32; 95% CI, 1.01 to 1.71; P¼0.04).
Similar conclusions were drawn from another re-cent observational study of 113,255 HD patients (42).The authors reported that in a 7-year follow-up, the meanchange in systolic and diastolic BPs after HD was 210and25mmHg, respectively. Large increases (.5 mmHg)and large decreases (,45 mmHg) in BPs during treat-ments were associated with increased all-cause mortalityas well as cardiovascular death, an observation that per-sisted even after different models adjusted for demo-graphics and comorbidities. These U-shaped associationswere independent of predialysis BP levels. The correla-tion between increased intradialytic BP and mortalitywas only present in those patients with a pre-HD systolicBP of $120 mmHg, and many of the patients in thiscategory had a history of cardiomyopathy. By contrast,the correlation of large decreases in BP and mortalitycould be explained by the cardiovascular burden associ-ated with intradialytic hypotension. This observationwarrants consideration of treatment strategies that favorhemodynamic stability during HD, such as decreasingdialysate temperature or increasing HD time.Intradialytic Hypertension. Precipitous drops in BP arequick to gain the attention of clinicians in the HD clinic,
but episodes of BP elevation that occur during treat-ments are also independently associated with increasedhospitalization, adverse cardiovascular outcome, and all-cause mortality (43). The incidence of intradialytic hy-pertension is estimated to be 5%–15% of prevalent HDpatients (44). Several processes likely contribute tointradialytic hypertension, including hypovolemia-inducedactivation of the renin-angiotensin system, sympatheticnervous system over activation, and removal of antihy-pertensive medications during treatment (44). The con-centration of plasma sodium is also a major determinantof extracellular fluid volume, interdialytic weight gain,and BP. A recent study explored the role that the in-tradialytic sodium gradient (the difference between serumand dialysate sodium concentrations) plays in the path-ogenesis of intradialytic hypertension (44). This cross-sectional observational study included 206 prevalent HDpatients, of whom 17% had intradialytic hypertension.An increase in BP during dialysis was associated witha larger sodium gradient compared with patients withno change or decreased BP during HD. Moreover, theblood-to-dialysate sodium gradient was positively corre-lated with interdialytic weight gain. These results indicatethat a larger sodium gradient favors the diffusion of sodiumfrom dialysate to plasma, which in turn leads to higher BPand increased risk of intradialytic hypertension.
Several recent studies implicate a potential role ofendothelial dysfunction in the pathogenesis of intra-dialytic hypertension. A prospective, open-label, 12-weekpilot study enrolled 25 prevalent HD patients with thediagnosis of intradialytic hypertension, defined as an in-crease in systolic BP of $10 mmHg from predialysis topostdialysis (43). Patients were treated with carvedilol6.25 mg twice a day for 8 weeks, titrated weekly, untilcessation of intradialytic hypertension (D systolic BP,0 during $2 consecutive HD sessions) or post-HDsystolic BP was ,130 mmHg in $2 consecutive HDsessions. Endothelial function was assessed by measur-ing changes in flow-mediated vasodilation and by as-saying the number of endothelial progenitor cells in thecirculation, with each patient serving as his or her owncontrol. Treatment with carvedilol was associated withsignificant improvement in endothelial function as re-flected by a 47% increase in flow-mediated vasodilationfrom baseline, despite a nonsignificant change in circu-lating markers of endothelial progenitor cells. Carvedilolwas also associated with significantly lower intradialyticBP, lower interdialytic ambulatory BP, and fewer epi-sodes of intradialytic hypertension. This study supports
370 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

the use of carvedilol in the HD population, and it sug-gests a causative role of endothelial cell dysfunction inthe complication of intradialytic hypertension.Management Considerations. The link between hyper-tension and poor cardiovascular outcomes is well re-cognized in the general population, but there are norandomized controlled clinical trials in HD patients thatdemonstrate treatment of elevated BP improves clinicaloutcomes (45). Moreover, the optimal BP target in HDpatients remains unknown. A recent analysis of 24,525HD patients attempted to identify the optimal BP rangein these patients (45). Using Cox regression models, thisstudy determined that patients who had a pre-HD sys-tolic BP range of 110–119 mmHg had a significantlyincreased all-cause mortality rate compared with patientswith a recorded range of 130–139 mmHg (HR, 1.14; 95%CI, 1.01 to 1.28; P¼0.03). Similar to previous observations,this study did not detect a significant increase in mortalityin those patients with pre-HD systolic BP .160 mmHg.However, when adjustments were made for grouped treat-ments, this study depicted a U-shaped association betweensystolic BP and mortality, with elevated hazards at predial-ysis systolic BP ,130 and .150 mmHg. Patients whoreceived HD treatments at facilities with a higher proportionof patients with pre-HD systolic BP of 130–159mmHg hadimproved survival. By contrast, patients in facilities withpredominant pre-HD systolic BP .160 mmHg had in-creased mortality (45).
At the other extreme, the HD patient with recur-rent hypotension poses unique challenges. Currentstrategies for managing low BP during HD includelowering dialysate temperature, increasing sodium di-alysate concentration, administering the adrenergicagonist midodrine and decreasing the rate of ultrafiltration(46). A recent, randomized controlled trial in 46 prevalentadult HD patients investigated the use of pneumaticcompression devices (PCDs) as a method to reducethe incidence of intradialytic hypotension (46). Poten-tially, PCDs can increase cardiac venous return andcardiac output, and these hemodynamic changes canenhance the central blood volume and reduce the risk ofintradialytic hypotension. In this trial, however, PCDsfailed to show any benefit in the improvement of centralblood volume, cardiac output, systemic vascular re-sistance, or intradialytic BPs.Delivered Dialysis Times and BP. Shorter deliveredtime on dialysis, either due to prescript time on dial-ysis or nonadherence, is associated with increasedmortality (47). A post hoc analysis from the Dry-Weight
Reduction in Hypertensive Hemodialysis Patients (DRIP)trial evaluated the relationship between delivered dialysistimes and BP (47). A total of 150 prevalent HD patientswere divided into two groups based on median delivereddialysis time (3.6 hours per treatment). In the DRIP pro-tocol, the patients who received dialysis less than themedian time tended to receive more antihypertensivedrugs and have higher intradialytic systolic BP. More-over, patients receiving shorter HD treatment times weremore likely to have persistently elevated BP, unless thedry weight was not adequately probed. Thus, an im-portant strategy in HD patients with poorly controlledhypertension is to provide sufficient treatment time thatenables adequate volume removal.
Nutrition and Obesity in ESRDBody Composition in ESRD. Concurrent malnutritionand inflammation is a prevalent condition caused bycoexisting illnesses, genetic predisposition, or expo-sures during the dialysis procedure. This condition hasbeen termed protein-energy wasting or the malnutrition-inflammation complex syndrome (MICS) (48). Tradi-tionally, the serum albumin concentration has been usedas a surrogate marker of the nutritional status of dialysispatients. However, processes such as the retention ofextracellular fluids, overhydration (and subsequent di-lution of blood components), protein losses in urine anddialysate, and shifts among body compartments limitthe value of serum albumin concentration as the solemarker of nutrition state (49). Thus, a subjective globalassessment score, body mass index (BMI) and bio-markers, such as total iron binding capacity or C-reactiveprotein, are often included with serum albumin to assessthe nutritional and inflammation status of dialysis patients(48). An alternative approach uses anthropometric values,such as skin-fold thickness and limb circumference, assurrogate markers for nutritional status. A post hoc analysisof the participants in the HEMO study determined thatdeclining mid-arm circumference and skin-fold thicknesswere significantly associated with all-cause mortality,cardiovascular events, and infection-related hospitaliza-tions (50). The relationship among declining anthropo-metric markers and outcomes was most evident in theHD patients with a BMI #25 kg/m2.
These different measurements allow studies ofthe clinical consequences of the malnutrition-inflammationphenotype. In a large cohort study, HD patients who hadthe poorest response to erythropoietin were found tohave lower serum albumin, higher C-reactive protein,
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 371
and higher IL-6 concentrations along with higher mal-nutrition scores (48). Clearly, there is also significantoverlap of the malnutrition-inflammation complex withphysical frailty, especially in the growing elderly pop-ulation on dialysis (51). A recent study evaluated thelink between body composition and frailty in HD pa-tients (52). In the cohort of 778 patients, 30% werecharacterized as frail, defined by slow gait speed, weakgrip strength, low physical activity, exhaustion, andweight loss. Not surprisingly, patients with frailty weremore likely to be elderly and to have diabetes. In addi-tion, higher fat mass and higher extracellular watermeasurements were also significantly associated withfrailty in this study. By contrast, the simple measureof BMI did not strongly associate with frailty. Thisanalysis suggested that estimates of body compositionmay be more clinically meaningful than either bodyweight or BMI.
A paradox has long been recognized in the HDpopulation. In contrast with the general population,higher BMI may be associated with increased survival.Part of this apparent beneficial effect could merely bethe lack of malnutrition and inflammation in the obesepatient. Regardless, this observation creates uncertaintyabout the best way to manage the obese dialysis patient.A recently reported observational cohort study fromEurope provides some insight to this clinical problem(53). In this study, 6296 prevalent HD patients wereprospectively followed for a median of 24 months. Inthe cohort, 11% of the patients were underweight, but31% were overweight and 16% were obese (BMI $30kg/m2). In follow-up, underweight patients were morethan twice as likely to die compared with normal weightpatients. The overweight and obese patients were sig-nificantly less likely to die in follow-up than their peerswith normal BMI (HR, 0.65 [95% CI, 0.55 to 0.77]; andHR, 0.58 [95% CI, 0.45 to 0.73], respectively, inadjusted models), confirming that obesity in dialysispatients is beneficial. These investigators also showeda significant adverse effect of weight loss over the courseof the study, particularly in the nonobese patients. Inaddition, this study demonstrated that causes of deathwere quite different, with underweight patients morecommonly dying from noncardiovascular causes andobese patients more likely to die from a cardiovascularevent. Consistent results were reported in a meta-analysisin 2012 (54). When combining results from three pub-lished studies and .71,000 dialysis patients, after ad-justments for known risk factors, a BMI .25 kg/m2
compared with individuals with a BMI #25 kg/m2
was associated with a lower mortality rate (HR, 0.94;95% CI, 0.92 to 0.96).
Some observations suggest that the influence ofBMI on survival in dialysis patients may differ in youngpatients (55). In a cohort study of 1749 dialysis pa-tients in The Netherlands, Hoogeveen and colleaguesobserved that obesity was associated with elevated riskfor death in patients aged ,65 years compared witholder patients (56).
Questions persist regarding whether obesity isa surrogate marker for lack of MICS or if being over-weight provides a novel source of protection. Onestudy explored the interaction of body habitus and thepresence of the malnutrition-inflammation phenotype.Kazory and colleagues performed a prospective cohortstudy of 541 prevalent HD patients in France with amean follow-up of 40 months (57). In addition to demo-graphic factors and laboratory variables, C-reactiveprotein and serum albumin were used to identify pa-tients with MICS. In this cohort, a BMI.25 kg/m2 wasassociated with an increased risk of atherosclerotic events(relative risk, 1.68; 95% CI, 1.11 to 3.56) and cardiovas-cular mortality (relative risk, 1.51; 95% CI, 1.07 to 2.13).This study did not demonstrate a significant interac-tion between body weight and MICS for the predictionof adverse events in the overall population. Age, dia-betes, a previous history of cardiovascular disease, highserum concentrations of homocysteine, and MICS werealso associated with an increased risk of atheroscleroticevents.
Adverse clinical outcomes are associatedwith markers of protein malnutrition inhemodialysis patients. Recent studies per-formed in the United States suggest thatprotein supplements provided thrice weeklyto patients with low serum albumin con-centrations are associated with improvedsurvival and hospitalization rates.
Prescriptions that enhance dietary intake of proteinhold some promise in HD patients. Weiner and col-leagues found that malnourished patients with a serumalbumin level #3.5 g/dl who received nutritional sup-plements had a 29% reduction in the HR for all-causemortality compared with matched control patients
372 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

(HR, 0.71; CI, 0.58 to 0.86) (58). Surprisingly, theintervention consisted only of 15 g of supplementedprotein thrice weekly with dialysis. In a retrospectivecohort, the effect of dietary protein supplementation indialysis patients with serum albumin levels #3.5 g/dlwas examined (59). Patients receiving supplementscontaining 14–20 g of protein three times per weekwith dialysis and were compared with matched con-trols. This study demonstrated a modest improvementin mortality in patients who received thrice-weeklyprotein supplementation as opposed to those who didnot (HR, 0.91; CI, 0.85 to 0.98). A potentially morecomprehensive program was subsequently examined(60). Hemodialysis patients who had serum albuminconcentrations ,3.8 g/dl were provided oral nutri-tional supplements (Ensure Plus [protein supplemen-tation of 13 g/d] or Glucerna [protein supplementationof 10 g/d]; Abbott Laboratories) and recommended totake the supplements on a daily basis. Compared withmalnourished patients who did not receive the supple-ments, the intervention was associated with a minimalincrease in serum albumin concentration (0.058 g/dl;P¼0.02) and a 68.4% decrease in the 1-year hospital-ization rate (P,0.01). There was no significant changein mortality risk.
An alternate method to reverse protein wastingin dialysis patients, rather than supplementing the diet,would be to administer anabolic steroids. In a 24-weekprospective trial, 43 dialysis patients were randomizedto receive either placebo or oxymetholone (61). At theend of the study period, patients who received the oralsteroid had improvement in handgrip strength, an in-crease in fat-free mass, and improved physical functionscores compared with those who received placebo.Unfortunately, this study also suggested that patientsreceiving oxymetholone had an increased risk fordeveloping abnormal liver function tests.
The nutrition profile of patients with ESRD differssubstantially from the general population. Patients ondialysis display abnormally low intake of vitamin K andhave evidence of hepatic and vascular vitamin K defi-ciency (62). In addition, the serum from incident dialysispatients contains amounts of long-chain n-3 polyunsat-urated fatty acids that are among the lowest recorded(63). It is attractive to consider that a less complex in-tervention in which a single component of a patient’s dietor a specific nutrition supplement will improve patientsurvival. Taking advantage of a nationwide health pro-gram in Taiwan, Chien and coworkers conducted a
propensity score–matched, retrospective cohort studyto address whether folic acid supplementation was as-sociated with improved outcomes in HD patients (64).This analysis suggested that folic acid use was associatedwith an 8.2% lower mortality rate. A randomized pro-spective placebo-controlled trial was performed inIran to examine the effects of supplementation withselenium (65). In this trial, the dialysis patients whoreceived 200 mg selenium daily for 12 weeks hadsignificant improvements in IL-6 concentrations (P¼0.02),malondialdehyde serum concentrations (P,0.001),subjective global assessment scores (P,0.001), andmalnutrition-inflammation scores (P,0.001) comparedwith those who took placebo.
Mineral Metabolism, Fractures, and Falls inESRD PatientsManagement of Secondary Hyperparathyroid-ism. Multiple observational studies suggest that elevatedPTH levels in patients with CKD are associated with in-creased cardiovascular events and mortality (66). TheEvaluation of Cinacalcet Hydrochloride Therapy toLower Cardiovascular Events (EVOLVE) trial was de-signed to test whether treatment with the oral calcimimeticcinacalcet would reduce the risk of death and cardio-vascular events among HD patients who have secondaryhyperparathyroidism (67). This multicenter, prospective,double-blind trial enrolled 3883 HD patients and ran-domized them to receive either cinacalcet or placebo.The primary composite end point was the time to deathor nonfatal cardiovascular event (myocardial infarction,hospitalization for unstable angina, heart failure, orperipheral vascular event). In an unadjusted, intention-to-treat analysis, cinacalcet reduced serum concentra-tions of PTH. However, the observed associatedreduction in the risk of reaching the primary com-posite end point did not reach statistical significance(95% CI, 0.85 to 1.02; P¼0.11). When the data wereadjusted for baseline characteristics, cinacalcet wasassociated with a significant 12% reduction in risk ofdeath and cardiovascular events. Furthermore, cinacalcetwas associated with a 56% reduction of parathy-roidectomy and a 57% reduction in progression tosevere unremitting hyperparathyroidism. This studywas limited by significant rates of study-drug discon-tinuation (62%) and by the crossover of almost 20% ofpatients assigned to placebo who eventually receivedopen-label cinacalcet during the trial. Overall, the EVOLVEtrial did not provide clear evidence that cinacalcet decreases
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 373

the risk of death, cardiovascular events, or other majorcomplications of mineral and bone disorders; however,the study suggests that any potential benefit of cinacalcetmay have been obscured by an imbalance in patient ran-domization. In addition, HD patients with secondary hy-perparathyroidism have a 24% risk of progressing tosevere unremitting hyperparathyroidism despite therapywith vitamin D sterols and phosphate binders (68) andthe EVOLVE trial suggests that cinacalcet substantiallyreduces this progression.
A smaller, randomized trial examined the effect ofcinacalcet on progression of CAC among HD patients(69). Patients were randomized to receive cinacalcet pluslow-dose active vitamin D (equivalent to a weekly doseof #6 mg of intravenous paricalcitol) or usual dosing ofactive vitamin D as deemed appropriate by the treatingphysician. The results showed that 39% (n¼45) ofpatients in the cinacalcet arm received vitamin D abovethe protocol guidelines. Therefore, the authors per-formed a per-protocol analysis of the remaining pro-tocol-adherent patients to the control group. At 52weeks, the median rise in the Agatston CAC score waslower in the intervention group compared with thecontrol group (17.8% versus 31.3%; P¼0.02). The risein aortic valve calcification was significantly lower inthe intervention group compared with controls (6.0%versus 51.5%; P¼0.02).Hyperphosphatemia. Disorders of phosphorus areassociated with an increased risk for all-cause and car-diovascular mortality among dialysis patients. A recentstudy characterized the intradialytic and postdialytickinetics of phosphorus from data obtained duringthe HEMO study (70). The results showed that pa-tients invariably had decreased serum phosphorus dur-ing the first 60 minutes of HD but that concentrationsrebounded approximately 27% after HD was termi-nated. The investigators calculated a phosphorusmobilization rate that estimated the movement ofphosphorus into the extracellular space. The major de-terminants of higher phosphorus mobilization clear-ances, and thus better phosphorus removal with HD,were low predialysis phosphorus levels, male sex, andlarger postdialysis body weight. Interestingly, the studywas not able to detect an association between phospho-rus mobilization clearance and biomarkers of boneturnover, such as PTH and serum alkaline phosphataselevels.
Oral phosphorus binders are a cornerstone forcontrolling serum phosphorus level in HD patients. A
recent study explored the associations among prescrip-tions for phosphate binders, nutritional status, andmortality in HD patients (71). The main analyses werebased on 23,898 prevalent HD patients from the in-ternational DOPPS prospective cohort. Patients pre-scribed phosphate binders had a lower prevalence ofcomorbid conditions and an overall better nutritionalstatus as measured by likelihood of cachexia and higherserum albumin, serum creatinine, BMI, and normalizedprotein catabolic rate. In Cox models adjusted for num-erous covariates including demographics, comorbidities,nutritional status, and serum phosphorus levels, theuse of a phosphate binder was associated with a 12%decreased mortality rate (adjusted HR, 0.88; 95% CI,0.80 to 0.97). A carefully designed placebo-controlled,prospective trial is needed to better assess whether theuse of phosphate binders is associated with improvedoutcomes.Falls and Fractures in ESRD Patients. Few studieshave examined the prevalence and complications offalls in HD patients. A prospective, single-center studyof 84 HD patients investigated the incidence of falls andrisk factors to predict falls in this patient population(72). The incidence of falls in this study was almost fourtimes higher among HD patients compared with anelderly, nondialysis population. Severe falls, defined asrequiring an emergency department visit and/or hospi-talization, were observed in 28.6% of the HD patients,and more than one half of the cases were complicatedby fractures. Over one half of the falls recorded in thisstudy occurred at home, and almost 38% of these hap-pened within 24 hours after the last HD session. Patientswho had malnutrition, depression, prior history offall, and age.65 years were more likely to experiencea fall in this study. Finally, a fall is associated withhigher mortality in the year after the fall comparedwith the dialysis population who did not fall. Un-fortunately, it is difficult to predict which HD patientsare at risk for falls. In the general population, thePerformance-Oriented Mobility Assessment (POMA)test is a clinical tool used to assess balance and gaitand to predict fall risk, especially in elderly patients.When a modified version of the POMA test wasadministered to a small group of HD patients, the scoredid not function as an independent predictor of severefall risk (72).
The disturbed mineral metabolism prevalent inHD patients likely contributes to the high risk for frac-tures in this population. An analysis of the USRDS,
374 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

which included 935,221 adult HD patients, foundthat the incidence of central (hip and vertebral) andperipheral (arm and leg) fractures requiring hospi-talization progressively increased between 1992 and2004 (35,73). The increased incidence of fractures wasprimarily observed in a subgroup of patients who werewhite, female, and aged.65 years. It is unclear whetherchanges in the use of vitamin D analogues, phosphatebinders, dialysate composition, or calcimimetics will in-fluence the risk of fractures.
Calcific Uremic ArteriolopathyCalcific uremic arteriolopathy (CUA), also known
as calciphylaxis, is a devastating complication of ESRDthat leads to systemic medial calcification of arteriolesand ischemic necrosis of skin and subcutaneous tissues.Up to 4% of dialysis patients are affected, and morbidityand mortality are high, with historical 1-year mortalityrates ranging from 45% to 80%. During the past decade,intravenous sodium thiosulfate (STS) has emerged asa potential treatment for CUA. The precise mechanismof action of STS is not known. An in vitro study ininjured rat aortas demonstrated that STS inhibited softtissue calcification through a mechanism that appearedto be independent of the tissue calcium concentration,pH, or interference with hydroxyapatite formation(74). There are no randomized controlled trials eval-uating the efficacy of STS in patients, but many casereports indicate improvement or resolution of skinlesions after treatment. In this regard, a series of 172dialysis patients who were treated with intravenousSTS for CUA was recently reported and is the largestpublished experience to date (75). Patients treated withSTS had a 1-year mortality of 35%, which was lowerthan historical mortality rates of those who did not re-ceive STS. Among a subset of patients who were sur-veyed, CUA completely resolved in 26.4% of patients,markedly improved in 18.9%, somewhat improved in28.3%, and was unchanged in 5.7%. STS was generallywell tolerated in this series, with side effects such asnausea and increased anion gap acidosis reported at lowfrequency.
The ideal duration of prescribing STS for therapyof CUA remains unknown. A common practice is tocontinue intravenous STS until all lesions are completelyresolved. In a recent prospective cohort study, four pa-tients with CUA were treated with intravenous STSfollowed by an oral STS maintenance regimen (76).Patients diagnosed with CUA had a baseline radio-
nucleotide bone scan to confirm the presence of softtissue calcification. They were treated with intravenousSTS at 25 g three times weekly. Patients were switchedfrom intravenous STS to oral STS maintenance therapyafter clinical response was achieved with the intrave-nous regimen. Interval bone scan results showed thatafter 6 months of oral maintenance therapy, two patientshad further improvement of their lesions, one patienthad stabilization, and one patient had slight progression.The results of this small series were inconclusive, butthe experience suggests that maintenance therapy withoral STS could be considered after successful induction.
The precise components for a successful course oftreatment of CUA are unknown, but a treatment modelthat involves multiple disciplines is commonly used.Along with induction therapy with intravenous STS,a multimodal approach includes wound care, de-bridement, avoidance of tissue trauma, and possiblyhyperbaric oxygen. In addition, empiric reduction ofthe serum calcium and phosphorus concentrations usingnoncalcium-containing binders should be consideredalong with consideration for increased HD frequencywith a low calcium dialysate. Control of PTH con-centrations should also be considered a mainstay ofmultimodal therapy, either with cinacalcet or para-thyroidectomy. Finally, potentially offending medica-tions, such as warfarin and vitamin D analogues,should be avoided. Salmohofer and colleagues dem-onstrated that this multidisciplinary and multilevelapproach can be effective in patients with CUA (77).
Stroke, Atrial Fibrillation, and Anticoagulation inESRD
ESRD patients have an increased incidence ofatrial fibrillation (AF) and a higher risk of stroke com-pared with patients with normal renal function (78–80), and stroke risk may be especially high around thetime of HD initiation (81). A prior issue of NephSAP dis-cussed the risk of stroke associated with warfarin use indialysis patients with AF. Anticoagulation with warfarinfor AF is widespread in the general population and theattendant benefits and risks are better defined than inpatients with ESRD. Since the last NephSAP issue, therehave been no randomized studies of chronic anticoagu-lation in HD patients, but new observations are availableto guide the best choice of therapies. One such studyprospectively followed 60 dialysis patients in Japanwho had AF, and 28 of these patients were treated withwarfarin (82). After 110 patient-years of follow-up
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 375

and after adjusting for Congestive Heart Failure, Age,Diabetes, and Prior Stroke 2 (CHADS2) scores, war-farin use was not associated with a reduced risk ofischemic stroke in the study patients. Major bleeding(fatal or requiring hospitalization) was also not signifi-cantly different between the HD patients who did andwho did not receive warfarin.
Data from the DOPPS study examined factorspredictive of stroke and bleeding in .48,000 HDpatients (83). The use of the CHADS2 score success-fully stratified stroke risk in this dialysis population. Inpatients prescribed oral vitamin K antagonists acrossadjusted models, there was a significant increase inall-cause mortality, cardiovascular mortality, and majorbleeding events. Adding to the safety concerns with oralanticoagulant use in dialysis patients was the finding thatrates of major bleeding substantially exceeded rates ofstroke in all patient groups, even those at highest risk ofstroke. A retrospective cohort study from Canada in-cluded patients aged.65 years admitted with a diagnosisof AF from 1998 to 2007 (84). The cohort included1626 dialysis patients (46% received warfarin) and.200,000 nondialysis patients. In a multivariate anal-ysis, warfarin use in HD patients was associated witha similar risk of nonhemorrhagic stroke but a significantlyhigher risk of bleeding (defined as intracerebral, in-traocular, gastrointestinal, unspecified hemorrhage, andhematuria; HR, 1.44; 95% CI, 1.13 to 1.85). The pa-tients in the analysis who were not on dialysis exhibiteda lower incidence of ischemic stroke with warfarin use,consistent with previous studies done in the generalpopulation.
By contrast, some studies suggest that specifictherapy may aid patients on HD who have AF. Oneobservational study in Scandinavian patients suggesteda benefit of anticoagulation for AF in ESRD. In a largeDanish registry (n¼132,372), warfarin use was exam-ined in patients with renal dysfunction and AF (85).Overall, 3587 (2.7%) patients had CKD and 901 (0.7%)had ESRD requiring RRT. Compared with patientswho had normal kidney function, those with CKDand ESRD had an increased risk of stroke or systemicthromboembolism (HR, 1.49 [95% CI, 1.38 to 1.59];and HR, 1.83 [95% CI, 1.57 to 2.14], respectively;P,0.001). This risk was attenuated in the group of pa-tients treated with warfarin (HR, 0.44; 95% CI, 0.26 to0.74; P¼0.002; for ESRD), but warfarin use was asso-ciated with a higher risk of hemorrhage compared withpatients with normal kidney function. The Swedish
Web-System for Enhancement and Development ofEvidence-Based Care in Heart Disease Evaluated Accord-ing to Recommended Therapies (SWEDEHEART) studydescribed consecutive survivors of an acute myocardialinfarction who also had AF (86). This analysis included24,317 patients with a known serum creatinine value,and 21.8% of the patients were prescribed warfarinat the time of discharge. The primary end point of theSWEDEHEART study was a composite of death, ischemicstroke, and readmission due to myocardial infarction.Warfarin use was associated with a lower risk of theoutcome in every eGFR stratum. For patients with aneGFR ,15 ml/min per 1.73 m2, the primary event ratewas 83.2 per 100 person-years for warfarin versus 128.3per 100 person-years without warfarin (HR, 0.57; 95%CI, 0.37 to 0.86). Moreover, the risk of bleeding was notsignificantly higher in patients with an eGFR ,15ml/min per 1.73 m2 treated with or without warfarin(event rate of 9.1 per 100 person-years for warfarinversus 13.5 per 100 person-years for no warfarin; HR,0.52; 95% CI, 0.16 to 1.65). This study suggested thatwarfarin use in patients who have CKD, including thosewith stage 5 CKD, is efficacious and has an accept-able safety profile. It remains unclear why this patientpopulation seemed to fare so well with warfarin therapycompared with other studies of patients with CKD.Factors such as the exceptionally good control of an-ticoagulation in this population or causes of CKDin Scandinavia could begin to explain the favorableresults in this study (87). Regardless, most otherstudies suggest that patients with CKD, especiallythose on dialysis, exhibit high variability of INR. CKDforms part of the HAS-BLED (Hypertension, Abnor-mal Renal/Liver Function, Stroke, Bleeding History orPredisposition, Labile international normalized ratio,Elderly, Drugs/Alcohol Concomitantly) score (Table1), which predicts risk of hemorrhagic complicationswith warfarin (84,88).
Overall, several studies suggest lower thromboemboliccomplications with warfarin in AF and advanced renaldisease, but other studies demonstrate no benefit orpotential for harm. The decision to anticoagulate mustto be individualized after weighing potential merits anddrawbacks.
Sudden Cardiac DeathIt is increasingly evident that patients with CKD
are exposed to an excess risk of sudden cardiac arrest(SCA) and subsequent death. Sudden cardiac death (SCD)
376 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
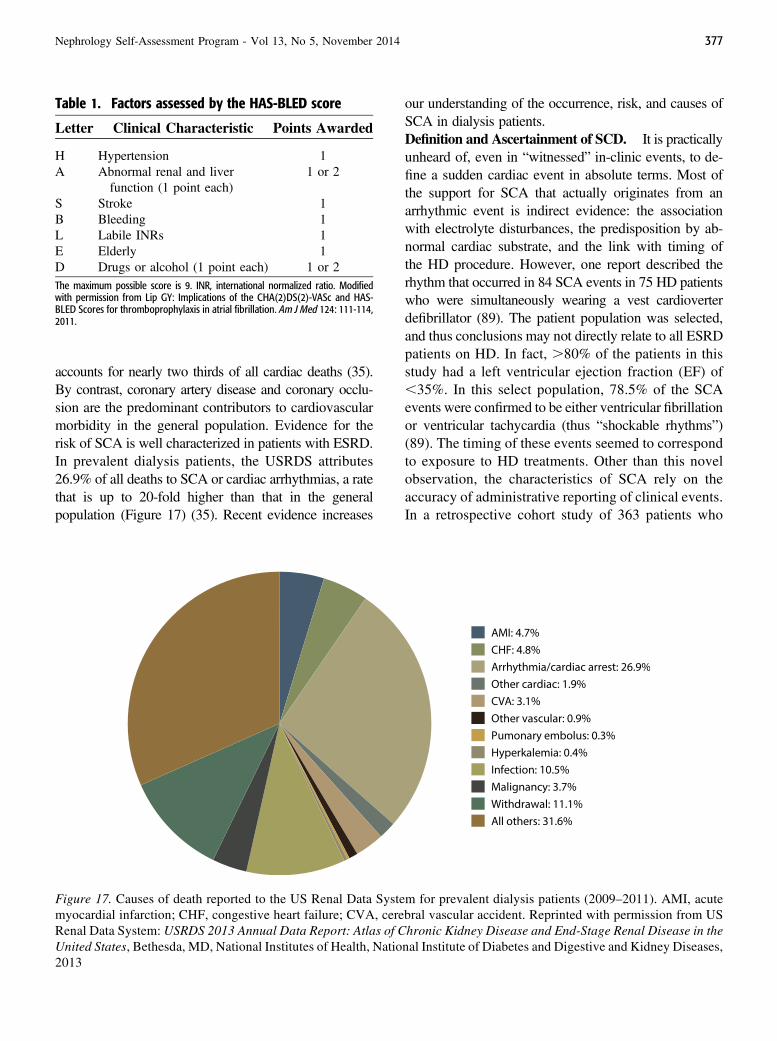
accounts for nearly two thirds of all cardiac deaths (35).By contrast, coronary artery disease and coronary occlu-sion are the predominant contributors to cardiovascularmorbidity in the general population. Evidence for therisk of SCA is well characterized in patients with ESRD.In prevalent dialysis patients, the USRDS attributes26.9% of all deaths to SCA or cardiac arrhythmias, a ratethat is up to 20-fold higher than that in the generalpopulation (Figure 17) (35). Recent evidence increases
our understanding of the occurrence, risk, and causes ofSCA in dialysis patients.Definition and Ascertainment of SCD. It is practicallyunheard of, even in “witnessed” in-clinic events, to de-fine a sudden cardiac event in absolute terms. Most ofthe support for SCA that actually originates from anarrhythmic event is indirect evidence: the associationwith electrolyte disturbances, the predisposition by ab-normal cardiac substrate, and the link with timing ofthe HD procedure. However, one report described therhythm that occurred in 84 SCA events in 75 HD patientswho were simultaneously wearing a vest cardioverterdefibrillator (89). The patient population was selected,and thus conclusions may not directly relate to all ESRDpatients on HD. In fact, .80% of the patients in thisstudy had a left ventricular ejection fraction (EF) of,35%. In this select population, 78.5% of the SCAevents were confirmed to be either ventricular fibrillationor ventricular tachycardia (thus “shockable rhythms”)(89). The timing of these events seemed to correspondto exposure to HD treatments. Other than this novelobservation, the characteristics of SCA rely on theaccuracy of administrative reporting of clinical events.In a retrospective cohort study of 363 patients who
Figure 17. Causes of death reported to the US Renal Data System for prevalent dialysis patients (2009–2011). AMI, acutemyocardial infarction; CHF, congestive heart failure; CVA, cerebral vascular accident. Reprinted with permission from USRenal Data System: USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in theUnited States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases,2013
Table 1. Factors assessed by the HAS-BLED score
Letter Clinical Characteristic Points Awarded
H Hypertension 1A Abnormal renal and liver
function (1 point each)1 or 2
S Stroke 1B Bleeding 1L Labile INRs 1E Elderly 1D Drugs or alcohol (1 point each) 1 or 2The maximum possible score is 9. INR, international normalized ratio. Modifiedwith permission from Lip GY: Implications of the CHA(2)DS(2)-VASc and HAS-BLED Scores for thromboprophylaxis in atrial fibrillation. Am J Med 124: 111-114,2011.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 377
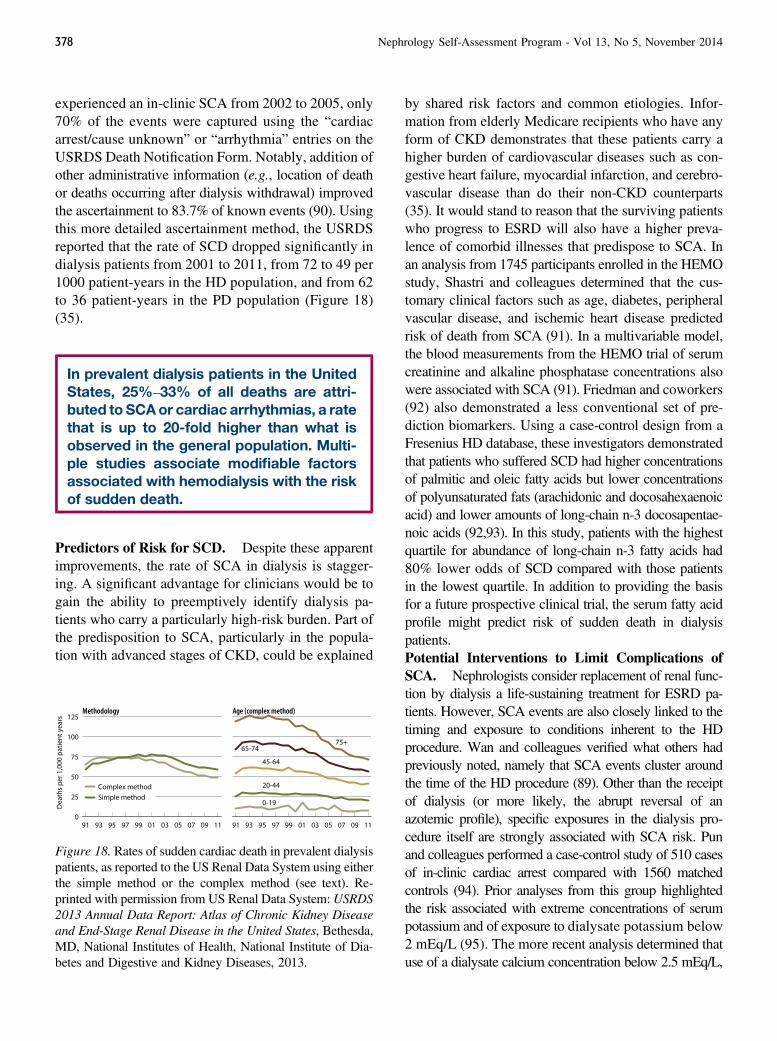
experienced an in-clinic SCA from 2002 to 2005, only70% of the events were captured using the “cardiacarrest/cause unknown” or “arrhythmia” entries on theUSRDS Death Notification Form. Notably, addition ofother administrative information (e.g., location of deathor deaths occurring after dialysis withdrawal) improvedthe ascertainment to 83.7% of known events (90). Usingthis more detailed ascertainment method, the USRDSreported that the rate of SCD dropped significantly indialysis patients from 2001 to 2011, from 72 to 49 per1000 patient-years in the HD population, and from 62to 36 patient-years in the PD population (Figure 18)(35).
In prevalent dialysis patients in the UnitedStates, 25%–33% of all deaths are attri-buted to SCAor cardiac arrhythmias, a ratethat is up to 20-fold higher than what isobserved in the general population. Multi-ple studies associate modifiable factorsassociated with hemodialysis with the riskof sudden death.
Predictors of Risk for SCD. Despite these apparentimprovements, the rate of SCA in dialysis is stagger-ing. A significant advantage for clinicians would be togain the ability to preemptively identify dialysis pa-tients who carry a particularly high-risk burden. Part ofthe predisposition to SCA, particularly in the popula-tion with advanced stages of CKD, could be explained
by shared risk factors and common etiologies. Infor-mation from elderly Medicare recipients who have anyform of CKD demonstrates that these patients carry ahigher burden of cardiovascular diseases such as con-gestive heart failure, myocardial infarction, and cerebro-vascular disease than do their non-CKD counterparts(35). It would stand to reason that the surviving patientswho progress to ESRD will also have a higher preva-lence of comorbid illnesses that predispose to SCA. Inan analysis from 1745 participants enrolled in the HEMOstudy, Shastri and colleagues determined that the cus-tomary clinical factors such as age, diabetes, peripheralvascular disease, and ischemic heart disease predictedrisk of death from SCA (91). In a multivariable model,the blood measurements from the HEMO trial of serumcreatinine and alkaline phosphatase concentrations alsowere associated with SCA (91). Friedman and coworkers(92) also demonstrated a less conventional set of pre-diction biomarkers. Using a case-control design from aFresenius HD database, these investigators demonstratedthat patients who suffered SCD had higher concentrationsof palmitic and oleic fatty acids but lower concentrationsof polyunsaturated fats (arachidonic and docosahexaenoicacid) and lower amounts of long-chain n-3 docosapentae-noic acids (92,93). In this study, patients with the highestquartile for abundance of long-chain n-3 fatty acids had80% lower odds of SCD compared with those patientsin the lowest quartile. In addition to providing the basisfor a future prospective clinical trial, the serum fatty acidprofile might predict risk of sudden death in dialysispatients.Potential Interventions to Limit Complications ofSCA. Nephrologists consider replacement of renal func-tion by dialysis a life-sustaining treatment for ESRD pa-tients. However, SCA events are also closely linked to thetiming and exposure to conditions inherent to the HDprocedure. Wan and colleagues verified what others hadpreviously noted, namely that SCA events cluster aroundthe time of the HD procedure (89). Other than the receiptof dialysis (or more likely, the abrupt reversal of anazotemic profile), specific exposures in the dialysis pro-cedure itself are strongly associated with SCA risk. Punand colleagues performed a case-control study of 510 casesof in-clinic cardiac arrest compared with 1560 matchedcontrols (94). Prior analyses from this group highlightedthe risk associated with extreme concentrations of serumpotassium and of exposure to dialysate potassium below2 mEq/L (95). The more recent analysis determined thatuse of a dialysate calcium concentration below 2.5 mEq/L,
Figure 18. Rates of sudden cardiac death in prevalent dialysispatients, as reported to the US Renal Data System using eitherthe simple method or the complex method (see text). Re-printed with permission from US Renal Data System: USRDS2013 Annual Data Report: Atlas of Chronic Kidney Diseaseand End-Stage Renal Disease in the United States, Bethesda,MD, National Institutes of Health, National Institute of Dia-betes and Digestive and Kidney Diseases, 2013.
378 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

presence of a higher serum calcium concentration, andexposure to a higher blood-to-dialysate gradient werestrongly associated with risk of SCA in hemodialysis(94).
To determine the universal application of theseassociations, the DOPPS study examined dialysis prac-tices and SCD in.37,000 patients in 12 countries (96).In the DOPPS study, sudden death accounted for 33.4%of deaths in the United States, but was as low as 6.8% inSweden. Higher rates of sudden death were associatedwith shorter treatment times, larger ultrafiltration volumes,lower Kt/V, use of lower potassium dialysate, and pre-scription of amiodarone (96). These recent publications,as well as information from prior studies, suggest thatdialysate composition, medications, clearance prescrip-tions, and adherence to dietary recommendations can bemodified to improve the risk and unfavorable outcomesfrom SCA in the HD population.
Death from SCA remains a major problem in di-alyzed ESRD patients, and knowledge of this problemis limited. There is a paucity of well designed, cohortstudies and randomized intervention trials regarding thisissue, and further studies are required to develop moreeffective management practices. The current observa-tions suggest that high-risk patients can be identifiedand that treatment with existing cardiovascular med-ications can mitigate dialysis-related arrhythmic trig-gers. At present, unconventional dialysis modalities andcardioverter-defibrillators should only be considered ona case-by-case basis given the known potential hazards ofthese approaches.
Cardiovascular Outcomes in ESRD Other thanSCDEffect of CKD and Hemodialysis on Left VentricularDysfunction. Exposure to HD can induce reversible,regional myocardial dysfunction, otherwise known asmyocardial stunning. Because left ventricular dysfunc-tion is independently associated with poor outcomes inESRD patients, there has been intense interest in theeffect of the dialysis procedure itself on cardiac function.Assa and colleagues (97) recently described 109 ESRDpatients on HD who underwent serial two-dimensionalechocardiography predialysis, during dialysis, and30 minutes postdialysis. The authors found a significantdecrease in early mitral inflow as measured by mitralearly inflow velocity (E) as well as decreased mean tis-sue Doppler early diastolic flow (e9) which both oc-curred within the first hour of hemodialysis. The change
in E was associated with changes in adjusted volumeparameters such as blood volume change and serumBNP, but not with the ultrafiltration volume and rate.More interestingly, the change in e9 did not associatewith any of the volume change parameters other than asignificant association with the serum BNP 180 minutesinto the dialysis procedure. In a separate analysis, thesame authors described the prevalence and outcomes ofhemodialysis-induced left ventricular systolic dysfunc-tion in the same cohort (98). This study determined that27% of the cohort developed regional systolic dysfunction,with 16% developing this within the first hour of dialysis.Volume parameters, such as ultrafiltration volume, rateand blood volume changes, did not differ between thepatients with and without hemodialysis-induced systolicdysfunction. This study also determined that HD-inducedsystolic dysfunction was associated with higher ad-justed all-cause mortality compared with patientswithout HD-induced systolic dysfunction (HR, 4.6;95% CI, 1.15 to 18.5; P¼0.03). These studies suggestthat hemodialysis-induced cardiac dysfunction is inde-pendent of dynamic changes in volume removal, and thetreatment-related transient changes are a harbinger ofpoor long-term outcomes.
A longitudinal study of 190 patients from theChronic Renal Insufficiency Cohort study evaluatedthe changes in echocardiographic parameters as patientswith advanced CKD progressed to ESRD (99). Overtime, there was no significant change in left ventricularmass index, but there was a significant decrease in themean EF in the cohort EF (53% to 50%; P¼0.002).Alternative measures of left ventricular function, suchas the left ventricular global peak systolic longitudinalstrain ratio was shown to predict outcomes among HDpatients with preserved EF (100). In a small cohort of 88dialysis patients, a less negative global peak systoliclongitudinal strain (less longitudinal shortening of myo-cardium) was associated with higher all-cause mortality(HR, 3.57; 95% CI, 1.41 to 9.04; P¼0.01). Unique riskfactors associated with ESRD such as the chronic uremicstate and intermittent HD likely contribute to the uniquepatterns of left ventricular dysfunction observed.Management of Mineral and Bone Disease andCardiovascular Outcomes. Bone and mineral metabo-lism involves numerous interrelated variables, and tissuecalcification is likely a final common pathway. Thus, anyindependent association between any one variable and anoutcome should be interpreted with caution. Block andcolleagues attempted to overcome this problem by
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 379

performing a retrospective study on a combined data setfrom the USRDS and a United States commercial cohort(101). The authors used a two-stage modeling approachthat allowed them to combine serum calcium, phosphate,and PTH concentrations at baseline to create a singlesummary variable to reflect 36 possible phenotypes ofmineral-bone disease based on Kidney Disease Out-comes Quality Initiative targets. The model compareddeath and cardiovascular hospitalization rates for eachphenotype with the group with normal parameters ofcalcium, target phosphate, and target low PTH con-centrations. The most common phenotypes at increasedrisk for the outcomes were the conditions that includedhigh or target PTH levels combined with high phos-phate and normal calcium concentrations. In addition,phenotypes with target high PTH levels and highcalcium with or without high phosphorus values wereassociated with a higher risk of death or cardiovascularhospitalization. This suggests that a holistic approach tobone and mineral metabolism, rather than focusing onindividual variables, could lead to improved long-termoutcomes.Cardiovascular Disease Management and Out-comes. Patients with CKD have unique risk factors forcardiovascular disease that differ from the general pop-ulation. A better understanding of the underlying causalpathways for tissue calcification, vascular disease, andcardiac dysfunction in HD patients will likely lead toimproved outcomes. A recent post hoc analysis from theAURORA (A Study to Evaluate the Use of Rosuvastatinin Subjects on Regular Hemodialysis: An Assessment ofSurvival and Cardiovascular Events) trial supported priorstudies by showing that nontraditional cardiovascularrisk factors such as serum phosphate, serum albumin,C-reactive protein, and HD vintage were independentdeterminants of major cardiovascular events in HD pa-tients (102). Traditional atherosclerotic risk factors such ashyperlipidemia, BP, and pulse pressure were not associ-ated with outcomes in this population.
Because of different pathophysiology and riskfactor profile, cardiovascular disease in the CKD pop-ulation differs from the general population. Because ofthe paucity of randomized therapy trials in CKD pa-tients, Chang et al. (103) performed a retrospectiveanalysis of 21,981 dialysis patients in the USRDS dataset who underwent coronary revascularization witheither a coronary artery bypass grafting or percutaneouscoronary intervention for multivessel coronary arterydisease between 1997 and 2009. The primary outcome
was all-cause mortality and the secondary outcomewas a composite of death or myocardial infarction. Amultivariable-adjusted proportional hazards model foundthat coronary artery bypass grafting was associated witha lower risk of death (HR, 0.87; 95% CI, 0.84 to 0.90)and death or myocardial infarction (HR, 0.88; 95% CI,0.86 to 0.91) compared with percutaneous coronaryintervention at 5 years of follow-up. Interestingly, Stacket al. (104) used USRDS data to find that the annualprevalence of coronary artery disease significantly in-creased in incident dialysis patients from 1995 to 2004(23.7% to 27.6%; P,0.001). During this same timeperiod, multivariable analysis showed significant yearlyreductions in overall mortality for all racial subgroupsexcept for black patients. These data may indicate thatmanagement of cardiovascular disease in ESRD patientsis improving over time as we selectively apply impor-tant therapies such as revascularization to this high-risk population.
Dialysis patients with coronary artery disease andacute coronary syndrome have historically been lesslikely to receive evidence-based medical therapy. Improv-ing the allocation of appropriate treatments for cardio-vascular disease in ESRD patients is one possible strategyto reduce outcomes. Frankenfield and colleagues ex-amined the use of common cardiovascular medicationsin dialysis patients with the Medicare Part D prescrip-tion drug benefit (105). In a large registry of 158,702dialysis patients with continuous medication coverage,the most commonly prescribed agents were b-blockers(64%), renin-angiotensin system inhibitors (52%), cal-cium channel blockers (51%), lipid-lowering agents(44%), and a-agonists (23%). A majority of patients(76%) qualified for the low-income subsidy. The meanout-of-pocket costs for cardiovascular disease medi-cations per month were $3.44 and $49.59 for dialysispatients with and without the low-income subsidy, re-spectively. For patients without the subsidy, clopidogrelhad the highest out-of-pocket cost at $26.26 per month.Because dialysis patients typically have a high pill bur-den, the addition of medications to reduce cardiovas-cular outcomes (e.g., postmyocardial infarction care)can introduce a greater financial and social burden onpatients, especially those who do not qualify for the low-income subsidy. Strategies to overcome these barrierscan possibly improve long-term outcomes.Other Interventions and Cardiovascular Out-comes. Fish oil contains v-3 fatty acids, which mayprovide anti-inflammatory benefits to high-risk patients.
380 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

One recent prospective, randomized controlled trial exam-ined whether fish oil supplementation would influencearteriovenous graft (AVG) survival or other clinicaloutcomes in HD patients (106). In this trial, HD pa-tients were randomized to either fish oil capsules (four1-g capsules per day) or placebo, starting 1 week afterplacement of an AVG. Cardiovascular outcomes wereassessed as a secondary outcome measure. This studydid not detect a significant difference in the primaryoutcome of graft patency at 12 months, but there wasa substantially lower risk of cardiovascular events inthe fish oil group compared with placebo (HR, 0.43;95% CI, 0.19 to 0.96; P¼0.04). More patients in thefish oil group had a significant reduction in BP recordedand in the number of antihypertensive medications pre-scribed. Because this trial was designed to evaluateAVG patency, the effect of fish oil supplementationon cardiovascular outcomes requires confirmation in fu-ture studies.
Smoking significantly worsens cardiovascular riskin hemodialysis patients. In a post hoc analysis of theHEMO study, McCausland and coworkers found thatcurrent smoking was associated with greater all-causemortality (HR, 1.44; 95%CI, 1.16 to 1.79) (107). Smokingwas also associated with greater cardiovascular hospi-talization rates (incidence rate ratio, 1.49; 95% CI, 1.22to 1.82). Although the effect of smoking cessation oncardiovascular outcomes in hemodialysis patients hasnot been well characterized, it is likely that the benefitsderived from smoking cessation in the general popula-tion apply to patients with ESRD.
Management of Dyslipidemia in ESRDAs discussed above, dialysis patients have an ex-
ceedingly high risk for cardiovascular events comparedwith the general population and patients with earlier stagesof CKD. Therapy with statins consistently decrease all-cause mortality and cardiovascular events in patients withwell preserved kidney function, but the evidence of suchbenefits is less compelling in patients with advanced CKDand those on dialysis (108). Several large-scale random-ized prospective trials over the last decade evaluated theuse of cholesterol-lowering therapies in patients with ad-vanced CKD, targeting an improvement in cardiovascu-lar outcomes (Table 2) (109–111). A recent meta-analysisof 80 randomized trials comparing the effects of statinsversus placebo on mortality and cardiovascular outcome,including data from 7982 dialysis patients, showed thatstatin therapy had little or no effect on all-cause mortality
and cardiovascular outcome in dialysis patients (108).These observations were confirmed by another meta-analysis (112). A possible reason for the apparent lackof benefit of statins is the unique pathophysiologyof cardiovascular disease in the dialysis population. Novelprocesses, such as vascular stiffness and calcification, sym-pathetic overactivity, and cardiacmorphologic changes, areall ongoing in patients with CKD, and these processes arelikely unaffected by statin therapy.
By contrast, another recent meta-analysis sug-gested that statins might offer benefit to patients withCKD. Pooling results from 31 randomized controlledtrials that assessed the effects of statins on cardiovascu-lar outcomes in people with kidney disease, this analysisfound a significant reduction of major cardiovascular eventsacross a range of CKD (113). This study also demon-strated that the benefit of cholesterol-lowering therapieswas significantly modified by kidney function, and thatany beneficial effects were smaller in people with stage5 CKD and those requiring dialysis. Regardless, thisanalysis suggested that intensive statin therapy reducedcardiovascular events by 28% in patients with CKD, andthe number needed to treat to reduce one major cardio-vascular event was 46 in CKD stage 5, 36 in CKD stage 4,and 24 in CKD stages 2–3 (113).
The results of such studies prompted the KidneyDisease: Improving Outcomes (KDIGO) organizationto develop an updated clinical practice guideline forlipid management in CKD (114). Because dialysis pa-tients carry such a high risk for all-cause and cardio-vascular mortality, the KDIGO Work Group no longerrecommends the use of LDL cholesterol for assessingcoronary risk in persons with CKD. On the basis of thenegative results obtained from the 4D Deutsche DiabetesDialyse Studie and the AURORA trial, initiation of statintherapy is not recommended in most prevalent hemodi-alysis patients. In dialysis patients who are already re-ceiving statin therapy at the time of dialysis initiation, itis reasonable to continue this treatment, understandingthat the reduction in cardiovascular events may be relativelysmall.
Vaccination, Hepatitis C, and InfectiousComplications Unique to Dialysis
Even as “specialists” assigned to manage end-stage kidney disease, most nephrologists aspire toprovide comprehensive care for their patients. In orderto achieve this goal, consideration must be given topreventing complications from the legion of infectious
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 381
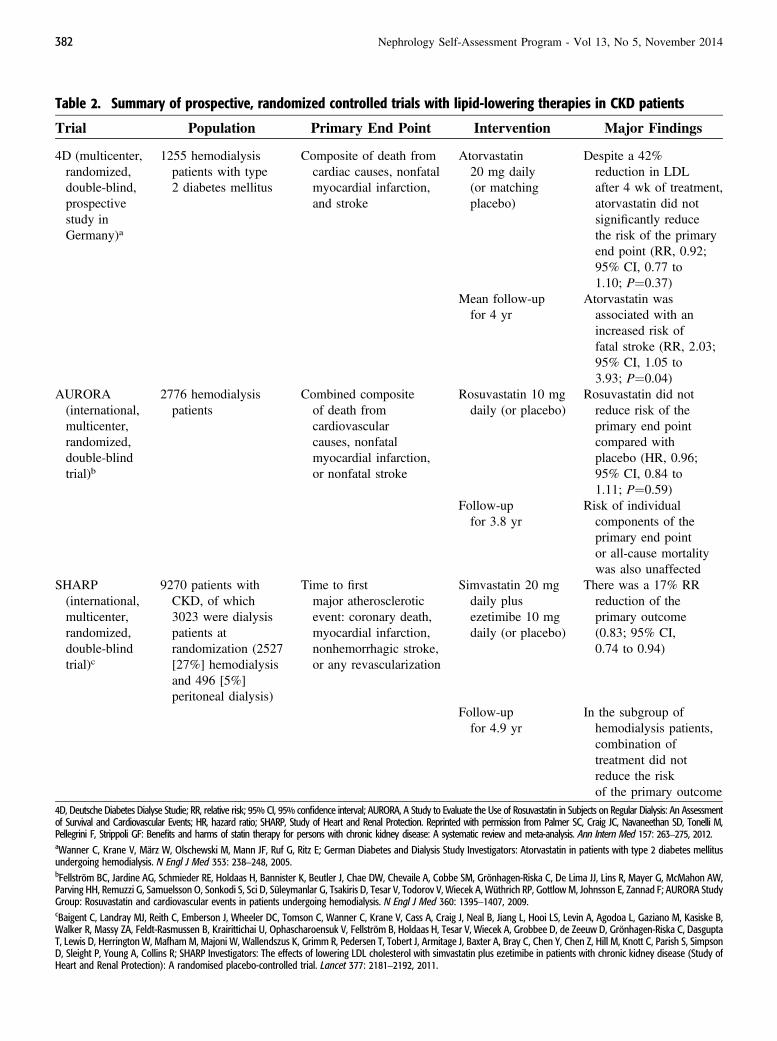
Table 2. Summary of prospective, randomized controlled trials with lipid-lowering therapies in CKD patients
Trial Population Primary End Point Intervention Major Findings
4D (multicenter,randomized,double-blind,prospectivestudy inGermany)a
1255 hemodialysispatients with type2 diabetes mellitus
Composite of death fromcardiac causes, nonfatalmyocardial infarction,and stroke
Atorvastatin20 mg daily(or matchingplacebo)
Despite a 42%reduction in LDLafter 4 wk of treatment,atorvastatin did notsignificantly reducethe risk of the primaryend point (RR, 0.92;95% CI, 0.77 to1.10; P¼0.37)
Mean follow-upfor 4 yr
Atorvastatin wasassociated with anincreased risk offatal stroke (RR, 2.03;95% CI, 1.05 to3.93; P¼0.04)
AURORA(international,multicenter,randomized,double-blindtrial)b
2776 hemodialysispatients
Combined compositeof death fromcardiovascularcauses, nonfatalmyocardial infarction,or nonfatal stroke
Rosuvastatin 10 mgdaily (or placebo)
Rosuvastatin did notreduce risk of theprimary end pointcompared withplacebo (HR, 0.96;95% CI, 0.84 to1.11; P¼0.59)
Follow-upfor 3.8 yr
Risk of individualcomponents of theprimary end pointor all-cause mortalitywas also unaffected
SHARP(international,multicenter,randomized,double-blindtrial)c
9270 patients withCKD, of which3023 were dialysispatients atrandomization (2527[27%] hemodialysisand 496 [5%]peritoneal dialysis)
Time to firstmajor atheroscleroticevent: coronary death,myocardial infarction,nonhemorrhagic stroke,or any revascularization
Simvastatin 20 mgdaily plusezetimibe 10 mgdaily (or placebo)
There was a 17% RRreduction of theprimary outcome(0.83; 95% CI,0.74 to 0.94)
Follow-upfor 4.9 yr
In the subgroup ofhemodialysis patients,combination oftreatment did notreduce the riskof the primary outcome
4D, Deutsche Diabetes Dialyse Studie; RR, relative risk; 95% CI, 95% confidence interval; AURORA, A Study to Evaluate the Use of Rosuvastatin in Subjects on Regular Dialysis: An Assessmentof Survival and Cardiovascular Events; HR, hazard ratio; SHARP, Study of Heart and Renal Protection. Reprinted with permission from Palmer SC, Craig JC, Navaneethan SD, Tonelli M,Pellegrini F, Strippoli GF: Benefits and harms of statin therapy for persons with chronic kidney disease: A systematic review and meta-analysis. Ann Intern Med 157: 263–275, 2012.aWanner C, Krane V, März W, Olschewski M, Mann JF, Ruf G, Ritz E; German Diabetes and Dialysis Study Investigators: Atorvastatin in patients with type 2 diabetes mellitusundergoing hemodialysis. N Engl J Med 353: 238–248, 2005.bFellström BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, Chae DW, Chevaile A, Cobbe SM, Grönhagen-Riska C, De Lima JJ, Lins R, Mayer G, McMahon AW,Parving HH, Remuzzi G, Samuelsson O, Sonkodi S, Sci D, Süleymanlar G, Tsakiris D, Tesar V, Todorov V, Wiecek A, Wüthrich RP, Gottlow M, Johnsson E, Zannad F; AURORA StudyGroup: Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med 360: 1395–1407, 2009.cBaigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano M, Kasiske B,Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U, Ophascharoensuk V, Fellström B, Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Grönhagen-Riska C, DasguptaT, Lewis D, Herrington W, Mafham M, Majoni W, Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, SimpsonD, Sleight P, Young A, Collins R; SHARP Investigators: The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study ofHeart and Renal Protection): A randomised placebo-controlled trial. Lancet 377: 2181–2192, 2011.
382 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
diseases to which dialysis patients are exposed. Thissection addresses new information regarding pre-ventive management of infectious hepatitis, pneu-mococcal infections, tuberculosis, and vascular accessinfections.Vaccinations. The Healthy People 2020 initiative sug-gested that at least 90% of individuals receive approvedimmunization for influenza. Although influenza vacci-nation rates for dialysis patients have risen from 46% in2001 to 65% in 2011, ESRD patients on dialysis are notyet meeting the Healthy People 2020 target (35). Sim-ilarly, the reported rate of immunization for pneumococcalpneumonia in dialysis patients is only approximately25%, and this has not changed over the past 5 years (35).In order to evaluate the consequences of these shortfalls,Bond and colleagues reported results from a survey thatincluded 903 outpatient dialysis clinics and 36,966 pre-valent dialysis patients (115). This study determined thatin 2005–2006, only 41.8% of patients were simulta-neously immunized against both influenza and pneumo-coccal disease. The patients who were immunized wereless likely to be black, were older, and were more likelyto receive HD rather than PD. Immunized patients alsohad higher reported rates of comorbid conditions such ascongestive heart failure, cardiovascular disease, periph-eral vascular disease, diabetes, chronic lung disease, andmalignancy. Perhaps unexpected was the magnitude ofthe survival benefit associated with immunizations inthis study.Multivariable models, fully adjusted for knowncovariates and case-mix differences, showed that the ORfor death was 0.71 (95% CI, 0.65–0.77) for the influenzavaccine and 0.76 (95% CI, 0.70-0.82) for pneumococcalimmunization. This study, even if limited by possibleeffects of unmeasured covariates, contrasts with otherstudies indicating that conventional vaccinations havelimited effectiveness in the ESRD population. For exam-ple, when an analysis was performed comparing dialysispatients who received the influenza vaccine with thosewho did not, the effectiveness of the vaccine is estimatedto be only 13%–30% (depending on the outcome mea-sure) (116). Because the cost of the intervention is low andpotential clinical benefits are profound, it is prudent tocontinue use of vaccines in this vulnerable population ofpatients. However, these observations suggest that alter-nate strategies such as new products, multiple-doseregimens, or high-dose protocols should be investigatedin the future.Tuberculosis Monitoring. Another important healthmaintenance practice, especially in the unique setting
of the dialysis clinic, is the monitoring for tuberculosis(TB) infection. Patients with ESRD have compromisedimmune systems and are therefore estimated to be.50times more likely to develop active TB and to carrya higher mortality from the disease compared with thegeneral population (117). The traditional screening testfor latent TB is the tuberculin skin test, but the sen-sitivity of this test is limited in immunocompromisedpatients. More recently, IFN release assays are beingused to screen for latent TB. ELISAs such as theQuantiFERON tests (Cellestis) or the T-SPOT.TB (OxfordImmunotec) are in vitro assays that measure the responseof sensitized T cells to mycobacterial antigens (117). Arecent meta-analysis compared results for these differenttypes of tests by pooling results from 47 different publishedstudies in ESRD patients (117). This analysis determinedthat compared with a positive tuberculin skin test result,a positive ELISA-based IFN release result was morestrongly associated with radiologic evidence of past TB(OR, 4.29; 95% CI, 1.83 to 10.3; P,0.001) and priorcontact with active TB (OR, 3.36; 95% CI, 1.61 to 7.01;P,0.001). Because of cost differences, the tuberculinskin test will not likely be supplanted, but the clinicianshould be aware of the apparent utility of these newerscreening tests.
Bloodstream infections continue to plaguehemodialysis patients. Because many ofthese infections originate from vascularaccess, a large part of the problem is thelack of patient preparedness before thestart of dialysis. The USRDS reported thatin 2011, at their first outpatient hemodial-ysis session, an astounding 62.6% of in-cident patients had a catheter as their soleform of vascular access.
Bacteremia. Bloodstream infections continue to be amajor source of morbidity in dialysis patients. It is evi-dent that vascular access and complications from ac-cesses are a significant source of bacteremia. Catheterscarry an inordinate risk, but the high incidence of in-fections can also be attributed to permanent vascular ac-cesses of arteriovenous grafts and fistulas. For all accesstypes, implementation of practices that include use ofchlorhexidine, competency training in aseptic techniquefor the clinic staff care and use of vascular access care
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 383
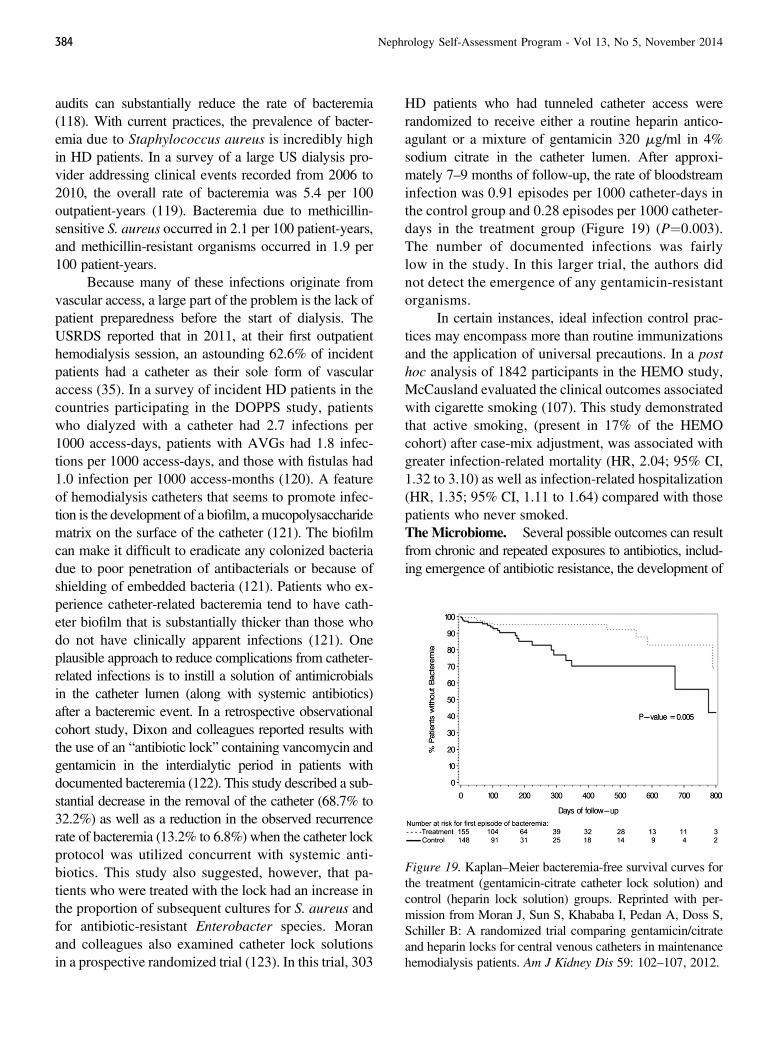
audits can substantially reduce the rate of bacteremia(118). With current practices, the prevalence of bacter-emia due to Staphylococcus aureus is incredibly highin HD patients. In a survey of a large US dialysis pro-vider addressing clinical events recorded from 2006 to2010, the overall rate of bacteremia was 5.4 per 100outpatient-years (119). Bacteremia due to methicillin-sensitive S. aureus occurred in 2.1 per 100 patient-years,and methicillin-resistant organisms occurred in 1.9 per100 patient-years.
Because many of these infections originate fromvascular access, a large part of the problem is the lack ofpatient preparedness before the start of dialysis. TheUSRDS reported that in 2011, at their first outpatienthemodialysis session, an astounding 62.6% of incidentpatients had a catheter as their sole form of vascularaccess (35). In a survey of incident HD patients in thecountries participating in the DOPPS study, patientswho dialyzed with a catheter had 2.7 infections per1000 access-days, patients with AVGs had 1.8 infec-tions per 1000 access-days, and those with fistulas had1.0 infection per 1000 access-months (120). A featureof hemodialysis catheters that seems to promote infec-tion is the development of a biofilm, a mucopolysaccharidematrix on the surface of the catheter (121). The biofilmcan make it difficult to eradicate any colonized bacteriadue to poor penetration of antibacterials or because ofshielding of embedded bacteria (121). Patients who ex-perience catheter-related bacteremia tend to have cath-eter biofilm that is substantially thicker than those whodo not have clinically apparent infections (121). Oneplausible approach to reduce complications from catheter-related infections is to instill a solution of antimicrobialsin the catheter lumen (along with systemic antibiotics)after a bacteremic event. In a retrospective observationalcohort study, Dixon and colleagues reported results withthe use of an “antibiotic lock” containing vancomycin andgentamicin in the interdialytic period in patients withdocumented bacteremia (122). This study described a sub-stantial decrease in the removal of the catheter (68.7% to32.2%) as well as a reduction in the observed recurrencerate of bacteremia (13.2% to 6.8%) when the catheter lockprotocol was utilized concurrent with systemic anti-biotics. This study also suggested, however, that pa-tients who were treated with the lock had an increase inthe proportion of subsequent cultures for S. aureus andfor antibiotic-resistant Enterobacter species. Moranand colleagues also examined catheter lock solutionsin a prospective randomized trial (123). In this trial, 303
HD patients who had tunneled catheter access wererandomized to receive either a routine heparin antico-agulant or a mixture of gentamicin 320 mg/ml in 4%sodium citrate in the catheter lumen. After approxi-mately 7–9 months of follow-up, the rate of bloodstreaminfection was 0.91 episodes per 1000 catheter-days inthe control group and 0.28 episodes per 1000 catheter-days in the treatment group (Figure 19) (P¼0.003).The number of documented infections was fairlylow in the study. In this larger trial, the authors didnot detect the emergence of any gentamicin-resistantorganisms.
In certain instances, ideal infection control prac-tices may encompass more than routine immunizationsand the application of universal precautions. In a posthoc analysis of 1842 participants in the HEMO study,McCausland evaluated the clinical outcomes associatedwith cigarette smoking (107). This study demonstratedthat active smoking, (present in 17% of the HEMOcohort) after case-mix adjustment, was associated withgreater infection-related mortality (HR, 2.04; 95% CI,1.32 to 3.10) as well as infection-related hospitalization(HR, 1.35; 95% CI, 1.11 to 1.64) compared with thosepatients who never smoked.TheMicrobiome. Several possible outcomes can resultfrom chronic and repeated exposures to antibiotics, includ-ing emergence of antibiotic resistance, the development of
Figure 19. Kaplan–Meier bacteremia-free survival curves forthe treatment (gentamicin-citrate catheter lock solution) andcontrol (heparin lock solution) groups. Reprinted with per-mission from Moran J, Sun S, Khababa I, Pedan A, Doss S,Schiller B: A randomized trial comparing gentamicin/citrateand heparin locks for central venous catheters in maintenancehemodialysis patients. Am J Kidney Dis 59: 102–107, 2012.
384 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

medication allergies, and modification of bacterial florathat reside either in the gastrointestinal tract or that arecolonized on the skin. In this regard, data are emergingon the possible pathogenic role of the community ofmicrobes that reside in the gut, called the microbiome.Perhaps due to antibiotic exposures, the ESRD pop-ulation demonstrates differences in the population ofgastrointestinal flora. In a recent study, stool sampleswere analyzed for the presence of certain bacterial oper-ational taxonomic units (124). This study demonstratedthat operational taxonomic units from bacterial familiesincluding Brachybacterium, Catenibacterium, Enterobac-teriaceae, Halomonadaceae,Moraxellaceae, Nesterenkonia,Polyangiaceae, Pseudomonadaceae, and Thiothrix weresignificantly higher in the gut microbiome of ESRD pa-tients compared with normal control patients (124). Itis not clear at this point whether antibiotics, diet, azo-temia, or other medications create these differences inthe microbiome or whether these different bacterialpopulations are associated with complications in CKDpatients.Hepatitis C. New therapies will likely soon result ina shift in the ramifications of chronic hepatitis C in-fection in the CKD patients. Hepatitis C is quite com-mon in HD, from comorbid illnesses, medical exposures,or shared pathogenic factors (125). The prevalence ofseropositivity for hepatitis C in international popula-tions is as high as 51% in Turkey (126). Among the12 countries participating in the DOPPS study, 9.5%of patients were hepatitis C–positive (127). Remarkably,only 1% of the hepatitic C–positive HD patients in theDOPPS study were known to have received effectivetherapies (either IFN, pegylated [peg] IFN, ribavirin, orprotease inhibitors) (127). Part of the lack of penetranceof therapy could be a perceived increase in the compli-cation rate or limited efficacy of available treatments.Because the excretion is limited in uremic patients and isnot aided by conventional dialysis, ribavirin can accu-mulate in the tissues of patients with ESRD and causedose-related hemolytic anemia (126).
PegIFN, a form of IFN linked with a polyethyleneglycol molecule, may be effective when used alone inthese patients. The use of pegIFN-a2a, injected on aweekly schedule for 48 weeks, demonstrated an 84.2%resolution of abnormal liver function tests and a 50%response rate for hepatitis C RNA (126). In a compar-ison of two sequential treated cohorts of HD patients,patients who received combination therapy of pegIFN-a2b/ribavirin had a higher end-of-treatment virologic
response than patients who received monotherapy withthe pegIFN alone (85% versus 62% by intention-to-treatanalysis; P¼0.03) (128). Indeed, this study demon-strated a higher prevalence of severe anemia in thepatients treated with ribavirin. A randomized prospectivetrial performed in Taiwan demonstrated similar find-ings (129). In this study, 205 HD patients with hepatitisC were randomized to receive either pegIFN-a2a withribavirin or pegIFN alone for 48 weeks. Compared withIFN monotherapy, patients assigned to combinationtherapy demonstrated a greater sustained virologic re-sponse rate (64% versus 33%; relative risk, 1.92; 95%CI, 1.41 to 2.62; P,0.001). During the treatment, thepatients who received ribavirin had a significant re-duction in hemoglobin concentrations despite receivingthe higher dose of erythropoietin. It is unclear whetherpegIFN will become used as primary therapy in dialysisunits for hepatitis C. The future holds promise for the useof more effective direct antiviral agents for eradication ofhepatitis C virus infection in ESRD patients without theuntoward effects of ribavirin or IFN pending results ofongoing clinical trials.
References1. Sirich TL, Funk BA, Plummer NS, Hostetter TH, Meyer TW:
Prominent accumulation in hemodialysis patients of solutes normallycleared by tubular secretion. J Am Soc Nephrol 25: 615–622, 2014 PubMed
2. Agarwal R: B-type natriuretic peptide is not a volume marker amongpatients on hemodialysis. Nephrol Dial Transplant 28: 3082–3089,2013 PubMed
3. Artunc F, Mueller C, Breidthardt T, Twerenbold R, Rettig I, Usta E,Häring HU, Friedrich B: Comparison of the diagnostic perfor-mance of three natriuretic peptides in hemodialysis patients: Whichis the appropriate biomarker? Kidney Blood Press Res 36: 172–181, 2012 PubMed
4. Quiroga B, Villaverde M, Abad S, Vega A, Reque J, López-GómezJM: Diastolic dysfunction and high levels of new cardiac biomarkersas risk factors for cardiovascular events and mortality in hemodialysispatients. Blood Purif 36: 98–106, 2013 PubMed
5. Breidthardt T, Burton JO, Odudu A, Eldehni MT, Jefferies HJ,McIntyre CW: Troponin T for the detection of dialysis-inducedmyocardial stunning in hemodialysis patients. Clin J Am Soc Nephrol7: 1285–1292, 2012 PubMed
6. Khan AM, Chirinos JA, Litt H, Yang W, Rosas SE: FGF-23 and theprogression of coronary arterial calcification in patients new todialysis. Clin J Am Soc Nephrol 7: 2017–2022, 2012 PubMed
7. Koizumi M, Komaba H, Nakanishi S, Fujimori A, Fukagawa M:Cinacalcet treatment and serum FGF23 levels in haemodialysispatients with secondary hyperparathyroidism. Nephrol Dial Trans-plant 27: 784–790, 2012 PubMed
8. Seiler S, Lucisano G, Ege P, Fell LH, Rogacev KS, Lerner-Gräber A,Klingele M, Ziegler M, Fliser D, Heine GH: Single FGF-23 measure-ment and time-averaged plasma phosphate levels in hemodialysispatients. Clin J Am Soc Nephrol 8: 1764–1772, 2013 PubMed
9. Shin MJ, Song SH, Kwak IS, Lee SB, Lee DW, Seong EY, Kim IY,Rhee H, Lee N: Serum cystatin C as a predictor for cardiovascularevents in end-stage renal disease patients at the initiation of dialysis.Clin Exp Nephrol 16: 456–463, 2012 PubMed
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 385
10. Liabeuf S, Lenglet A, Desjardins L, Neirynck N, Glorieux G, LemkeHD, Vanholder R, Diouf M, Choukroun G, Massy ZA; EuropeanUremic Toxin Work Group (EUTox): Plasma beta-2 microglobulin isassociated with cardiovascular disease in uremic patients. Kidney Int82: 1297–1303, 2012 PubMed
11. Shafi T, Parekh RS, Jaar BG, Plantinga LC, Oberai PC, Eckfeldt JH,Levey AS, Powe NR, Coresh J: Serum b-trace protein and risk ofmortality in incident hemodialysis patients. Clin J Am Soc Nephrol 7:1435–1445, 2012 PubMed
12. Chen YH, Hung SC, Tarng DC: Length polymorphism in hemeoxygenase-1 and cardiovascular events and mortality in hemodialysispatients. Clin J Am Soc Nephrol 8: 1756–1763, 2013 PubMed
13. Jia T, Gama Axelsson T, Heimbürger O, Bárány P, Lindholm B,Stenvinkel P, Qureshi AR: IGF-1 and survival in ESRD.Clin J Am SocNephrol 9: 120–127, 2014 PubMed
14. Koeth RA, Kalantar-Zadeh K, Wang Z, Fu X, Tang WH, Hazen SL:Protein carbamylation predicts mortality in ESRD. J Am Soc Nephrol24: 853–861, 2013 PubMed
15. Spoto B, Mattace-Raso F, Sijbrands E, Pizzini P, Cutrupi S, D’ArrigoG, Tripepi G, Zoccali C, Mallamaci F: Resistin and all-cause andcardiovascular mortality: Effect modification by adiponectin in end-stage kidney disease patients. Nephrol Dial Transplant 28[Suppl 4]:iv181–iv187, 2013 PubMed
16. Espe KM, Raila J, Henze A, Blouin K, Schneider A, Schmiedeke D,Krane V, Pilz S, Schweigert FJ, Hocher B, Wanner C, Drechsler C;German Diabetes and Dialysis Study Investigators: Low plasma a-to-copherol concentrations and adverse clinical outcomes in diabetichemodialysis patients. Clin J Am Soc Nephrol 8: 452–458, 2013 PubMed
17. González-Espinoza L, Rojas-Campos E, Medina-Pérez M, Peña-Quintero P, Gómez-Navarro B, Cueto-Manzano AM: Pentoxifyllinedecreases serum levels of tumor necrosis factor alpha, interleukin 6and C-reactive protein in hemodialysis patients: Results of a random-ized double-blind, controlled clinical trial. Nephrol Dial Transplant27: 2023–2028, 2012 PubMed
18. Puchades MJ, Saez G, Muñoz MC, Gonzalez M, Torregrosa I, Juan I,Miguel A: Study of oxidative stress in patients with advanced renaldisease and undergoing either hemodialysis or peritoneal dialysis. ClinNephrol 80: 177–186, 2013 PubMed
19. Rodriguez L, Tighiouart H, Scott T, Lou K, Giang L, Sorensen E,Weiner DE, Sarnak MJ: Association of sleep disturbances withcognitive impairment and depression in maintenance hemodialysispatients. J Nephrol 26: 101–110, 2013 PubMed
20. Harris TJ, Nazir R, Khetpal P, Peterson RA, Chava P, Patel SS,Kimmel PL: Pain, sleep disturbance and survival in hemodialysispatients. Nephrol Dial Transplant 27: 758–765, 2012 PubMed
21. Elder SJ, Pisoni RL, Akizawa T, Fissell R, Andreucci VE, Fukuhara S,Kurokawa K, Rayner HC, Furniss AL, Port FK, Saran R: Sleep qualitypredicts quality of life and mortality risk in haemodialysis patients:Results from the Dialysis Outcomes and Practice Patterns Study(DOPPS). Nephrol Dial Transplant 23: 998–1004, 2008 PubMed
22. Giannaki CD, Hadjigeorgiou GM, Karatzaferi C, Pantzaris MC,Stefanidis I, Sakkas GK: Epidemiology, impact, and treatment optionsof restless legs syndrome in end-stage renal disease patients: Anevidence-based review. Kidney Int 85: 1275–1282, 2014 PubMed
23. Pennestri MH, Montplaisir J, Fradette L, Lavigne G, Colombo R,Lanfranchi PA: Blood pressure changes associated with periodic legmovements during sleep in healthy subjects. Sleep Med 14: 555–561,2013 PubMed
24. Gade K, Blaschke S, Rodenbeck A, Becker A, Anderson-Schmidt H,Cohrs S: Uremic restless legs syndrome (RLS) and sleep quality inpatients with end-stage renal disease on hemodialysis: Potential role ofhomocysteine and parathyroid hormone. Kidney Blood Press Res 37:458–463, 2013 PubMed
25. Kutner NG, Zhang R, Szczech LA, Bliwise DL: Restless legs syndromereported by incident haemodialysis patients: Is treatment time of dayrelevant? Nephrology (Carlton) 17: 783–784, 2012 PubMed
26. Jaber BL, Schiller B, Burkart JM, Daoui R, Kraus MA, Lee Y, MillerBW, Teitelbaum I, Williams AW, Finkelstein FO; FREEDOM StudyGroup: Impact of short daily hemodialysis on restless legs symptoms andsleep disturbances.Clin J Am Soc Nephrol 6: 1049–1056, 2011 PubMed
27. Lacson E Jr, Li NC, Guerra-Dean S, Lazarus M, Hakim R, FinkelsteinFO: Depressive symptoms associate with high mortality risk anddialysis withdrawal in incident hemodialysis patients. Nephrol DialTransplant 27: 2921–2928, 2012 PubMed
28. Murray AM, Tupper DE, Knopman DS, Gilbertson DT, Pederson SL,Li S, Smith GE, Hochhalter AK, Collins AJ, Kane RL: Cognitiveimpairment in hemodialysis patients is common. Neurology 67: 216–223, 2006 PubMed
29. Kalirao P, Pederson S, Foley RN, Kolste A, Tupper D, Zaun D, BuotV, Murray AM: Cognitive impairment in peritoneal dialysis patients.Am J Kidney Dis 57: 612–620, 2011 PubMed
30. Sorensen EP, Sarnak MJ, Tighiouart H, Scott T, Giang LM, KirkpatrickB, Lou K, Weiner DE: The kidney disease quality of life cognitivefunction subscale and cognitive performance in maintenance hemo-dialysis patients. Am J Kidney Dis 60: 417–426, 2012 PubMed
31. Kumagai H, Ebata T, Takamori K, Muramatsu T, Nakamoto H, SuzukiH: Effect of a novel kappa-receptor agonist, nalfurafine hydrochloride,on severe itch in 337 haemodialysis patients: A phase III, randomized,double-blind, placebo-controlled study. Nephrol Dial Transplant 25:1251–1257, 2010 PubMed
32. Kumagai H, Ebata T, Takamori K, Miyasato K, Muramatsu T,Nakamoto H, Kurihara M, Yanagita T, Suzuki H: Efficacy and safetyof a novel ĸ-agonist for managing intractable pruritus in dialysispatients. Am J Nephrol 36: 175–183, 2012 PubMed
33. Rayner H, Baharani J, Smith S, Suresh V, Dasgupta I: Uraemicpruritus: Relief of itching by gabapentin and pregabalin. Nephron ClinPract 122: 75–79, 2012 PubMed
34. Solak Y, Biyik Z, Atalay H, Gaipov A, Guney F, Turk S, Covic A,Goldsmith D, Kanbay M: Pregabalin versus gabapentin in thetreatment of neuropathic pruritus in maintenance haemodialysispatients: A prospective, crossover study. Nephrology (Carlton) 17:710–717, 2012 PubMed
35. US Renal Data System: USRDS 2013 Annual Data Report: Atlas ofChronic Kidney Disease and End-Stage Renal Disease in the UnitedStates, Bethesda, MD, National Institutes of Health, National Instituteof Diabetes and Digestive and Kidney Diseases, 2013
36. Shahir AK, Briggs N, Katsoulis J, Levidiotis V: An observationaloutcomes study from 1966-2008, examining pregnancy and neonataloutcomes from dialysed women using data from the ANZDATARegistry. Nephrology (Carlton) 18: 276–284, 2013 PubMed
37. Jesudason S, Grace BS, McDonald SP: Pregnancy outcomes accordingto dialysis commencing before or after conception in women withESRD. Clin J Am Soc Nephrol 9: 143–149, 2014 PubMed
38. Hladunewich MA, Hou S, Odutayo A, Cornelis T, Pierratos A, GoldsteinM, Tennankore K, Keunen J, Hui D, Chan CT: Intensive hemodialysisassociates with improved pregnancy outcomes: A Canadian and UnitedStates cohort comparison. J Am SocNephrol 25: 1103–1109, 2014 PubMed
39. Raimann JG, Usvyat LA, Thijssen S, Kotanko P, Rogus J, Lacson E Jr,Levin NW: Blood pressure stability in hemodialysis patients confersa survival advantage: Results from a large retrospective cohort study.Kidney Int 81: 548–558, 2012 PubMed
40. Kuipers J, Usvyat LA, Oosterhuis JK, Dasselaar JJ, de Jong PE,Westerhuis R, Sands JJ, Wang Y, Kotanko P, Franssen CF: Variabilityof predialytic, intradialytic, and postdialytic blood pressures in thecourse of a week: A study of Dutch and US maintenance hemodialysispatients. Am J Kidney Dis 62: 779–788, 2013 PubMed
41. Flythe JE, Inrig JK, Shafi T, Chang TI, Cape K, Dinesh K, Kunaparaju S,Brunelli SM: Association of intradialytic blood pressure variability withincreased all-cause and cardiovascular mortality in patients treated withlong-term hemodialysis. Am J Kidney Dis 61: 966–974, 2013 PubMed
42. Park J, Rhee CM, Sim JJ, Kim YL, Ricks J, Streja E, Vashistha T,Tolouian R, Kovesdy CP, Kalantar-Zadeh K: A comparative
386 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
effectiveness research study of the change in blood pressureduring hemodialysis treatment and survival. Kidney Int 84: 795–802, 2013 PubMed
43. Inrig JK, Van Buren P, Kim C, Vongpatanasin W, Povsic TJ, Toto R:Probing the mechanisms of intradialytic hypertension: A pilot studytargeting endothelial cell dysfunction. Clin J Am Soc Nephrol 7: 1300–1309, 2012 PubMed
44. Movilli E, Camerini C, Gaggia P, Zubani R, Feller P, Poiatti P, Pola A,Carli O, Valzorio B, Cancarini G: Role of dialysis sodium gradient onintradialytic hypertension: An observational study. Am J Nephrol 38:413–419, 2013 PubMed
45. Roberts MA, Pilmore HL, Tonkin AM, Garg AX, Pascoe EM, BadveSV, Cass A, Ierino FL, Hawley CM; Beta-Blocker to LowerCardiovascular Dialysis Events (BLOCADE) Feasibility Study TrialManagement Committee: Challenges in blood pressure measurementin patients treated with maintenance hemodialysis. Am J Kidney Dis60: 463–472, 2012 PubMed
46. Tai DJ, Ahmed SB, Palacios-Derflingher L, Hemmelgarn BR, MacRaeJM; Alberta Kidney Disease Network: Pneumatic compression devicesduring hemodialysis: A randomized crossover trial. Nephrol DialTransplant 28: 982–990, 2013 PubMed
47. Tandon T, Sinha AD, Agarwal R: Shorter delivered dialysis timesassociate with a higher and more difficult to treat blood pressure.Nephrol Dial Transplant 28: 1562–1568, 2013 PubMed
48. Rattanasompattikul M, Molnar MZ, Zaritsky JJ, Hatamizadeh P, JingJ, Norris KC, Kovesdy CP, Kalantar-ZadehK: Association of malnutrition-inflammation complex and responsiveness to erythropoiesis-stimulatingagents in long-term hemodialysis patients. Nephrol Dial Transplant 28:1936–1945, 2013 PubMed
49. Gama-Axelsson T, Heimbürger O, Stenvinkel P, Bárány P, Lindholm B,Qureshi AR: Serum albumin as predictor of nutritional status in patientswith ESRD. Clin J Am Soc Nephrol 7: 1446–1453, 2012 PubMed
50. Su CT, Yabes J, Pike F, Weiner DE, Beddhu S, Burrowes JD, RoccoMV, Unruh ML: Changes in anthropometry and mortality in mainte-nance hemodialysis patients in the HEMO Study. Am J Kidney Dis 62:1141–1150, 2013 PubMed
51. Kim JC, Kalantar-Zadeh K, Kopple JD: Frailty and protein-energywasting in elderly patients with end stage kidney disease. J Am SocNephrol 24: 337–351, 2013 PubMed
52. Johansen KL, Dalrymple LS, Delgado C, Kaysen GA, Kornak J,Grimes B, Chertow GM: Association between body composition andfrailty among prevalent hemodialysis patients: A US Renal DataSystem special study. J Am Soc Nephrol 25: 381–389, 2013
53. Cabezas-Rodriguez I, Carrero JJ, Zoccali C, Qureshi AR, Ketteler M,Floege J, London G, Locatelli F, Gorriz JL, Rutkowski B, Memmos D,Ferreira A, Covic A, Teplan V, Bos WJ, Kramar R, Pavlovic D,Goldsmith D, Nagy J, Benedik M, Verbeelen D, Tielemans C,Wüthrich RP, Martin PY, Martínez-Salgado C, Fernández-MartínJL, Cannata-Andia JB: Influence of body mass index on the associ-ation of weight changes with mortality in hemodialysis patients. Clin JAm Soc Nephrol 8: 1725–1733, 2013 PubMed
54. Jialin W, Yi Z, Weijie Y: Relationship between body mass index andmortality in hemodialysis patients: A meta-analysis. Nephron ClinPract 121: c102–c111, 2012 PubMed
55. Vashistha T, Mehrotra R, Park J, Streja E, Dukkipati R, Nissenson AR,Ma JZ, Kovesdy CP, Kalantar-Zadeh K: Effect of age and dialysisvintage on obesity paradox in long-term hemodialysis patients. Am JKidney Dis 63: 612–622, 2014 PubMed
56. Hoogeveen EK, Halbesma N, Rothman KJ, Stijnen T, van Dijk S,Dekker FW, Boeschoten EW, de Mutsert R; Netherlands CooperativeStudy on the Adequacy of Dialysis-2 (NECOSAD) Study Group:Obesity and mortality risk among younger dialysis patients. Clin J AmSoc Nephrol 7: 280–288, 2012 PubMed
57. Kazory A, Klein A, Chalopin JM, Ducloux D, Courivaud C: Obesity andatherosclerotic events in chronic hemodialysis patients: A prospectivestudy. Nephrol Dial Transplant 28[Suppl 4]: iv188–iv194, 2013 PubMed
58. Weiner DE, Tighiouart H, Ladik V, Meyer KB, Zager PG, JohnsonDS: Oral intradialytic nutritional supplement use and mortality inhemodialysis patients. Am J Kidney Dis 63: 276–285, 2014 PubMed
59. Lacson E Jr, Wang W, Zebrowski B, Wingard R, Hakim RM:Outcomes associated with intradialytic oral nutritional supplementsin patients undergoing maintenance hemodialysis: A quality improve-ment report. Am J Kidney Dis 60: 591–600, 2012 PubMed
60. Cheu C, Pearson J, Dahlerus C, Lantz B, Chowdhury T, Sauer PF,Farrell RE, Port FK, Ramirez SP: Association between oral nutritionalsupplementation and clinical outcomes among patients with ESRD.Clin J Am Soc Nephrol 8: 100–107, 2013 PubMed
61. Supasyndh O, Satirapoj B, Aramwit P, Viroonudomphol D, ChaiprasertA, Thanachatwej V, Vanichakarn S, Kopple JD: Effect of oral anabolicsteroid on muscle strength and muscle growth in hemodialysis patients.Clin J Am Soc Nephrol 8: 271–279, 2013 PubMed
62. Cranenburg EC, Schurgers LJ, Uiterwijk HH, Beulens JW, DalmeijerGW, Westerhuis R, Magdeleyns EJ, Herfs M, Vermeer C, LavermanGD: Vitamin K intake and status are low in hemodialysis patients.Kidney Int 82: 605–610, 2012 PubMed
63. Friedman AN, Yu Z, Tabbey R, Denski C, Tamez H, Wenger J,Thadhani R, Li Y, Watkins BA: Low blood levels of long-chain n-3polyunsaturated fatty acids in US hemodialysis patients: Clinicalimplications. Am J Nephrol 36: 451–458, 2012 PubMed
64. Chien SC, Li SY, Chen YT, Tsai LW, Chen TJ, Chen TW, Lin YC:Folic acid supplementation in end-stage renal disease patients reducestotal mortality rate. J Nephrol 26: 1097–1104, 2013 PubMed
65. Salehi M, Sohrabi Z, Ekramzadeh M, Fallahzadeh MK, Ayatollahi M,Geramizadeh B, Hassanzadeh J, Sagheb MM: Selenium supplemen-tation improves the nutritional status of hemodialysis patients: Arandomized, double-blind, placebo-controlled trial. Nephrol DialTransplant 28: 716–723, 2013 PubMed
66. Floege J, Kim J, Ireland E, Chazot C, Drueke T, de Francisco A,Kronenberg F, Marcelli D, Passlick-Deetjen J, Schernthaner G,Fouqueray B, Wheeler DC; ARO Investigators: Serum iPTH, calciumand phosphate, and the risk of mortality in a European haemodialysispopulation. Nephrol Dial Transplant 26: 1948–1955, 2011 PubMed
67. Chertow GM, Block GA, Correa-Rotter R, Drüeke TB, Floege J,Goodman WG, Herzog CA, Kubo Y, London GM, Mahaffey KW, MixTC, Moe SM, Trotman ML, Wheeler DC, Parfrey PS; EVOLVE TrialInvestigators: Effect of cinacalcet on cardiovascular disease in patientsundergoing dialysis. N Engl J Med 367: 2482–2494, 2012 PubMed
68. Parfrey PS, Chertow GM, Block GA, Correa-Rotter R, Drüeke TB,Floege J, Herzog CA, London GM, Mahaffey KW, Moe SM, WheelerDC, Dehmel B, Trotman ML, Modafferi DM, Goodman WG: Theclinical course of treated hyperparathyroidism among patients re-ceiving hemodialysis and the effect of cinacalcet: The EVOLVE trial.J Clin Endocrinol Metab 98: 4834–4844, 2013 PubMed
69. Ureña-Torres PA, Floege J, Hawley CM, Pedagogos E, GoodmanWG, Pétavy F, Reiner M, Raggi P: Protocol adherence and theprogression of cardiovascular calcification in the ADVANCE study.Nephrol Dial Transplant 28: 146–152, 2013 PubMed
70. Leypoldt JK, Agar BU, Akonur A, Hutchcraft AM, Story KO,Culleton BF: Determinants of phosphorus mobilization during hemo-dialysis. Kidney Int 84: 841–848, 2013 PubMed
71. Lopes AA, Tong L, Thumma J, Li Y, Fuller DS, Morgenstern H,Bommer J, Kerr PG, Tentori F, Akiba T, Gillespie BW, Robinson BM,Port FK, Pisoni RL: Phosphate binder use and mortality amonghemodialysis patients in the Dialysis Outcomes and Practice PatternsStudy (DOPPS): Evaluation of possible confounding by nutritionalstatus. Am J Kidney Dis 60: 90–101, 2012 PubMed
72. Rossier A, Pruijm M, Hannane D, Burnier M, Teta D: Incidence,complications and risk factors for severe falls in patients on maintenancehaemodialysis. Nephrol Dial Transplant 27: 352–357, 2012 PubMed
73. Wagner J, Jhaveri KD, Rosen L, Sunday S, Mathew AT, Fishbane S:Increased bone fractures among elderly United States hemodialysispatients. Nephrol Dial Transplant 29: 146–151, 2014 PubMed
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 387
74. O’Neill WC, Hardcastle KI: The chemistry of thiosulfate and vascularcalcification. Nephrol Dial Transplant 27: 521–526, 2012 PubMed
75. Nigwekar SU, Brunelli SM, Meade D, Wang W, Hymes J, Lacson EJr: Sodium thiosulfate therapy for calcific uremic arteriolopathy. Clin JAm Soc Nephrol 8: 1162–1170, 2013 PubMed
76. AlBugami MM, Wilson JA, Clarke JR, Soroka SD: Oral sodiumthiosulfate as maintenance therapy for calcific uremic arteriolopathy: Acase series. Am J Nephrol 37: 104–109, 2013 PubMed
77. Salmhofer H, Franzen M, Hitzl W, Koller J, Kreymann B, Fend F,Hauser-Kronberger C, Heemann U, Berr F, Schmaderer C: Multi-modal treatment of calciphylaxis with sodium-thiosulfate, cinacalcetand sevelamer including long-term data. Kidney Blood Press Res 37:346–359, 2013 PubMed
78. Wang HH, Hung SY, Sung JM, Hung KY, Wang JD: Risk of stroke inlong-term dialysis patients compared with the general population. AmJ Kidney Dis 63: 604–611, 2014 PubMed
79. Power A, Chan K, Singh SK, Taube D, Duncan N: Appraising strokerisk in maintenance hemodialysis patients: A large single-center cohortstudy. Am J Kidney Dis 59: 249–257, 2012 PubMed
80. Kuo CC, Lee CT, Ho SC, Kuo HW,Wu TN, Yang CY: Haemodialysisand the risk of stroke: A population-based cohort study in Taiwan,a country of high incidence of end-stage renal disease. Nephrology(Carlton) 17: 243–248, 2012 PubMed
81. Murray AM, Seliger S, Lakshminarayan K, Herzog CA, Solid CA:Incidence of stroke before and after dialysis initiation in older patients.J Am Soc Nephrol 24: 1166–1173, 2013 PubMed
82. Wakasugi M, Kazama JJ, Tokumoto A, Suzuki K, Kageyama S, OhyaK, Miura Y, Kawachi M, Takata T, Nagai M, Ohya M, Kutsuwada K,Okajima H, Ei I, Takahashi S, Narita I: Association between warfarinuse and incidence of ischemic stroke in Japanese hemodialysis patientswith chronic sustained atrial fibrillation: A prospective cohort study.Clin Exp Nephrol 18: 662–669, 2014 PubMed
83. Sood MM, Larkina M, Thumma JR, Tentori F, Gillespie BW,Fukuhara S, Mendelssohn DC, Chan K, de Sequera P, Komenda P,Rigatto C, Robinson BM: Major bleeding events and risk stratificationof antithrombotic agents in hemodialysis: Results from the DOPPS.Kidney Int 84: 600–608, 2013 PubMed
84. Shah M, Avgil Tsadok M, Jackevicius CA, Essebag V, Eisenberg MJ,Rahme E, Humphries KH, Tu JV, Behlouli H, GuoH, Pilote L:Warfarinuse and the risk for stroke and bleeding in patients with atrial fibrillationundergoing dialysis. Circulation 129: 1196–1203, 2014 PubMed
85. Olesen JB, Lip GY, Kamper AL, Hommel K, Køber L, Lane DA,Lindhardsen J, Gislason GH, Torp-Pedersen C: Stroke and bleeding inatrial fibrillation with chronic kidney disease. N Engl J Med 367: 625–635, 2012 PubMed
86. Carrero JJ, Evans M, Szummer K, Spaak J, Lindhagen L, Edfors R,Stenvinkel P, Jacobson SH, Jernberg T: Warfarin, kidney dysfunction,and outcomes following acute myocardial infarction in patients withatrial fibrillation. JAMA 311: 919–928, 2014 PubMed
87. Winkelmayer WC, Turakhia MP: Warfarin treatment in patients withatrial fibrillation and advanced chronic kidney disease: Sins of omissionor commission? JAMA 311: 913–915, 2014 PubMed
88. Lip GY, Frison L, Halperin JL, Lane DA: Comparative validation ofa novel risk score for predicting bleeding risk in anticoagulated pa-tients with atrial fibrillation: The HAS-BLED (Hypertension, Abnor-mal Renal/Liver Function, Stroke, Bleeding History or Predisposition,Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am CollCardiol 57: 173–180, 2011 PubMed
89. Wan C, Herzog CA, ZarebaW, Szymkiewicz SJ: Sudden cardiac arrestin hemodialysis patients with wearable cardioverter defibrillator. AnnNoninvasive Electrocardiol 19: 247–257, 2014
90. Pun PH, Herzog CA, Middleton JP: Improving ascertainment ofsudden cardiac death in patients with end stage renal disease. Clin JAm Soc Nephrol 7: 116–122, 2012 PubMed
91. Shastri S, Tangri N, Tighiouart H, Beck GJ, Vlagopoulos P, OrntD, Eknoyan G, Kusek JW, Herzog C, Cheung AK, Sarnak MJ:
Predictors of sudden cardiac death: A competing risk approachin the hemodialysis study. Clin J Am Soc Nephrol 7: 123–130,2012 PubMed
92. Friedman AN, Yu Z, Tabbey R, Denski C, Tamez H, Wenger J,Thadhani R, Li Y, Watkins BA: Inverse relationship between long-chain n-3 fatty acids and risk of sudden cardiac death in patientsstarting hemodialysis. Kidney Int 83: 1130–1135, 2013 PubMed
93. Friedman AN, Yu Z, Denski C, Tamez H, Wenger J, Thadhani R, LiY, Watkins B: Fatty acids and other risk factors for sudden cardiacdeath in patients starting hemodialysis. Am J Nephrol 38: 12–18,2013 PubMed
94. Pun PH, Horton JR, Middleton JP: Dialysate calcium concentrationand the risk of sudden cardiac arrest in hemodialysis patients. Clin JAm Soc Nephrol 8: 797–803, 2013 PubMed
95. Pun PH, Middleton JP: Sudden cardiac death in hemodialysis patients:A comprehensive care approach to reduce risk. Blood Purif 33: 183–189, 2012 PubMed
96. Jadoul M, Thumma J, Fuller DS, Tentori F, Li Y, Morgenstern H,Mendelssohn D, Tomo T, Ethier J, Port F, Robinson BM: Modifiablepractices associated with sudden death among hemodialysis patients inthe Dialysis Outcomes and Practice Patterns Study. Clin J Am SocNephrol 7: 765–774, 2012 PubMed
97. Assa S, Hummel YM, Voors AA, Kuipers J, Groen H, de Jong PE,Westerhuis R, Franssen CF: Changes in left ventricular diastolicfunction during hemodialysis sessions. Am J Kidney Dis 62: 549–556, 2013
98. Assa S, Hummel YM, Voors AA, Kuipers J, Westerhuis R, de JongPE, Franssen CF: Hemodialysis-induced regional left ventricularsystolic dysfunction: Prevalence, patient and dialysis treatment-relatedfactors, and prognostic significance. Clin J Am Soc Nephrol 7: 1615–1623, 2012 PubMed
99. Bansal N, Keane M, Delafontaine P, Dries D, Foster E, GadegbekuCA, Go AS, Hamm LL, Kusek JW, Ojo AO, Rahman M, Tao K,Wright JT, Xie D, Hsu CY; CRIC Study Investigators: A longitudinalstudy of left ventricular function and structure from CKD to ESRD:The CRIC study. Clin J Am Soc Nephrol 8: 355–362, 2013 PubMed
100. Liu YW, Su CT, Sung JM,Wang SP, Su YR, Yang CS, Tsai LM, ChenJH, Tsai WC: Association of left ventricular longitudinal strain withmortality among stable hemodialysis patients with preserved leftventricular ejection fraction. Clin J Am Soc Nephrol 8: 1564–1574,2013 PubMed
101. Block GA, Kilpatrick RD, Lowe KA, Wang W, Danese MD: CKD-mineral and bone disorder and risk of death and cardiovascularhospitalization in patients on hemodialysis. Clin J Am Soc Nephrol8: 2132–2140, 2013 PubMed
102. Schneider A, Jardine AG, Schneider MP, Holdaas H, Holme I,Fellstroem BC, Zannad F, Schmieder RE; AURORA Study Group:Determinants of cardiovascular risk in haemodialysis patients: Posthoc analyses of the AURORA study. Am J Nephrol 37: 144–151,2013 PubMed
103. Chang TI, Shilane D, Kazi DS, Montez-Rath ME, Hlatky MA,Winkelmayer WC: Multivessel coronary artery bypass grafting versuspercutaneous coronary intervention in ESRD. J Am Soc Nephrol 23:2042–2049, 2012 PubMed
104. Stack AG, Neylon AM, Abdalla AA, Hegarty A, Hannigan A,Cronin CJ, Nguyen HT, Casserly LF: Declining mortality ratesdespite increases in clinical coronary artery disease among USdialysis patients: A national registry study. Am J Nephrol 38: 66–74, 2013 PubMed
105. Frankenfield DL, Weinhandl ED, Powers CA, Howell BL, HerzogCA, St Peter WL: Utilization and costs of cardiovascular diseasemedications in dialysis patients in Medicare Part D. Am J Kidney Dis59: 670–681, 2012 PubMed
106. Lok CE, Moist L, Hemmelgarn BR, Tonelli M, Vazquez MA, DorvalM, Oliver M, Donnelly S, Allon M, Stanley K; Fish Oil Inhibition ofStenosis in Hemodialysis Grafts (FISH) Study Group: Effect of fish oil
388 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
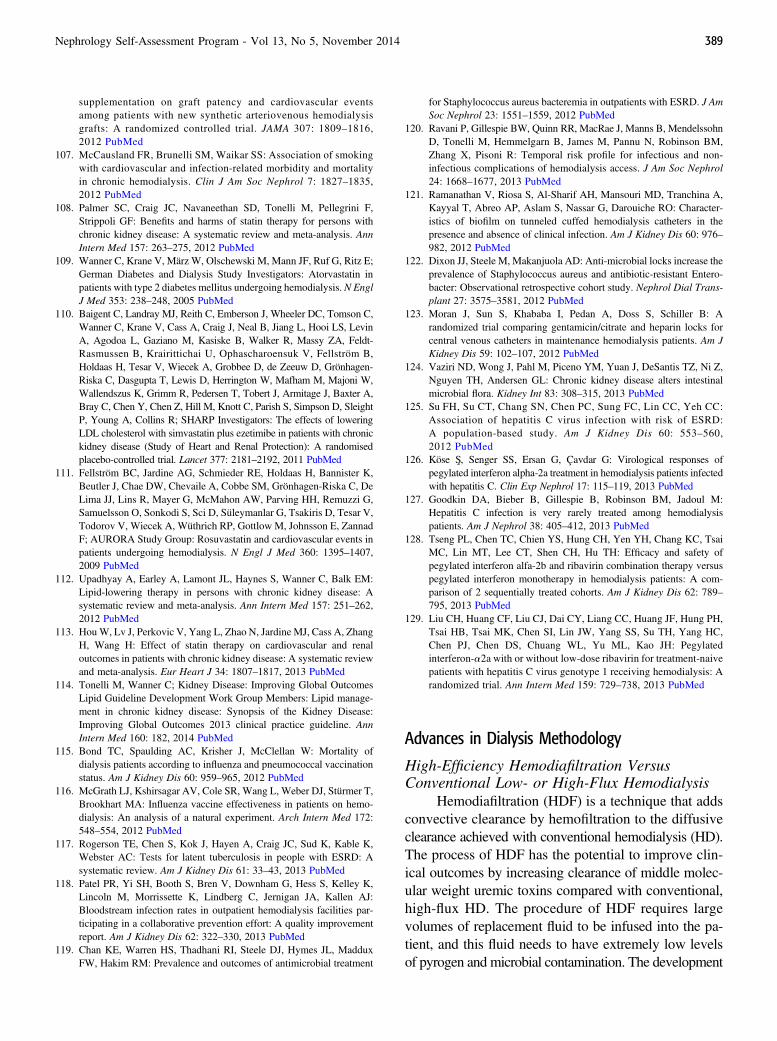
supplementation on graft patency and cardiovascular eventsamong patients with new synthetic arteriovenous hemodialysisgrafts: A randomized controlled trial. JAMA 307: 1809–1816,2012 PubMed
107. McCausland FR, Brunelli SM, Waikar SS: Association of smokingwith cardiovascular and infection-related morbidity and mortalityin chronic hemodialysis. Clin J Am Soc Nephrol 7: 1827–1835,2012 PubMed
108. Palmer SC, Craig JC, Navaneethan SD, Tonelli M, Pellegrini F,Strippoli GF: Benefits and harms of statin therapy for persons withchronic kidney disease: A systematic review and meta-analysis. AnnIntern Med 157: 263–275, 2012 PubMed
109. Wanner C, Krane V, März W, Olschewski M, Mann JF, Ruf G, Ritz E;German Diabetes and Dialysis Study Investigators: Atorvastatin inpatients with type 2 diabetes mellitus undergoing hemodialysis. N EnglJ Med 353: 238–248, 2005 PubMed
110. Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C,Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, LevinA, Agodoa L, Gaziano M, Kasiske B, Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U, Ophascharoensuk V, Fellström B,Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Grönhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham M, Majoni W,Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A,Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, Simpson D, SleightP, Young A, Collins R; SHARP Investigators: The effects of loweringLDL cholesterol with simvastatin plus ezetimibe in patients with chronickidney disease (Study of Heart and Renal Protection): A randomisedplacebo-controlled trial. Lancet 377: 2181–2192, 2011 PubMed
111. Fellström BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K,Beutler J, Chae DW, Chevaile A, Cobbe SM, Grönhagen-Riska C, DeLima JJ, Lins R, Mayer G, McMahon AW, Parving HH, Remuzzi G,Samuelsson O, Sonkodi S, Sci D, Süleymanlar G, Tsakiris D, Tesar V,Todorov V, Wiecek A, Wüthrich RP, Gottlow M, Johnsson E, ZannadF; AURORA Study Group: Rosuvastatin and cardiovascular events inpatients undergoing hemodialysis. N Engl J Med 360: 1395–1407,2009 PubMed
112. Upadhyay A, Earley A, Lamont JL, Haynes S, Wanner C, Balk EM:Lipid-lowering therapy in persons with chronic kidney disease: Asystematic review and meta-analysis. Ann Intern Med 157: 251–262,2012 PubMed
113. HouW, Lv J, Perkovic V, Yang L, Zhao N, Jardine MJ, Cass A, ZhangH, Wang H: Effect of statin therapy on cardiovascular and renaloutcomes in patients with chronic kidney disease: A systematic reviewand meta-analysis. Eur Heart J 34: 1807–1817, 2013 PubMed
114. Tonelli M, Wanner C; Kidney Disease: Improving Global OutcomesLipid Guideline Development Work Group Members: Lipid manage-ment in chronic kidney disease: Synopsis of the Kidney Disease:Improving Global Outcomes 2013 clinical practice guideline. AnnIntern Med 160: 182, 2014 PubMed
115. Bond TC, Spaulding AC, Krisher J, McClellan W: Mortality ofdialysis patients according to influenza and pneumococcal vaccinationstatus. Am J Kidney Dis 60: 959–965, 2012 PubMed
116. McGrath LJ, Kshirsagar AV, Cole SR, Wang L, Weber DJ, Stürmer T,Brookhart MA: Influenza vaccine effectiveness in patients on hemo-dialysis: An analysis of a natural experiment. Arch Intern Med 172:548–554, 2012 PubMed
117. Rogerson TE, Chen S, Kok J, Hayen A, Craig JC, Sud K, Kable K,Webster AC: Tests for latent tuberculosis in people with ESRD: Asystematic review. Am J Kidney Dis 61: 33–43, 2013 PubMed
118. Patel PR, Yi SH, Booth S, Bren V, Downham G, Hess S, Kelley K,Lincoln M, Morrissette K, Lindberg C, Jernigan JA, Kallen AJ:Bloodstream infection rates in outpatient hemodialysis facilities par-ticipating in a collaborative prevention effort: A quality improvementreport. Am J Kidney Dis 62: 322–330, 2013 PubMed
119. Chan KE, Warren HS, Thadhani RI, Steele DJ, Hymes JL, MadduxFW, Hakim RM: Prevalence and outcomes of antimicrobial treatment
for Staphylococcus aureus bacteremia in outpatients with ESRD. J AmSoc Nephrol 23: 1551–1559, 2012 PubMed
120. Ravani P, Gillespie BW, Quinn RR, MacRae J, Manns B, MendelssohnD, Tonelli M, Hemmelgarn B, James M, Pannu N, Robinson BM,Zhang X, Pisoni R: Temporal risk profile for infectious and non-infectious complications of hemodialysis access. J Am Soc Nephrol24: 1668–1677, 2013 PubMed
121. Ramanathan V, Riosa S, Al-Sharif AH, Mansouri MD, Tranchina A,Kayyal T, Abreo AP, Aslam S, Nassar G, Darouiche RO: Character-istics of biofilm on tunneled cuffed hemodialysis catheters in thepresence and absence of clinical infection. Am J Kidney Dis 60: 976–982, 2012 PubMed
122. Dixon JJ, Steele M, Makanjuola AD: Anti-microbial locks increase theprevalence of Staphylococcus aureus and antibiotic-resistant Entero-bacter: Observational retrospective cohort study. Nephrol Dial Trans-plant 27: 3575–3581, 2012 PubMed
123. Moran J, Sun S, Khababa I, Pedan A, Doss S, Schiller B: Arandomized trial comparing gentamicin/citrate and heparin locks forcentral venous catheters in maintenance hemodialysis patients. Am JKidney Dis 59: 102–107, 2012 PubMed
124. Vaziri ND, Wong J, Pahl M, Piceno YM, Yuan J, DeSantis TZ, Ni Z,Nguyen TH, Andersen GL: Chronic kidney disease alters intestinalmicrobial flora. Kidney Int 83: 308–315, 2013 PubMed
125. Su FH, Su CT, Chang SN, Chen PC, Sung FC, Lin CC, Yeh CC:Association of hepatitis C virus infection with risk of ESRD:A population-based study. Am J Kidney Dis 60: 553–560,2012 PubMed
126. Köse Sx, Senger SS, Ersan G, Çavdar G: Virological responses ofpegylated interferon alpha-2a treatment in hemodialysis patients infectedwith hepatitis C. Clin Exp Nephrol 17: 115–119, 2013 PubMed
127. Goodkin DA, Bieber B, Gillespie B, Robinson BM, Jadoul M:Hepatitis C infection is very rarely treated among hemodialysispatients. Am J Nephrol 38: 405–412, 2013 PubMed
128. Tseng PL, Chen TC, Chien YS, Hung CH, Yen YH, Chang KC, TsaiMC, Lin MT, Lee CT, Shen CH, Hu TH: Efficacy and safety ofpegylated interferon alfa-2b and ribavirin combination therapy versuspegylated interferon monotherapy in hemodialysis patients: A com-parison of 2 sequentially treated cohorts. Am J Kidney Dis 62: 789–795, 2013 PubMed
129. Liu CH, Huang CF, Liu CJ, Dai CY, Liang CC, Huang JF, Hung PH,Tsai HB, Tsai MK, Chen SI, Lin JW, Yang SS, Su TH, Yang HC,Chen PJ, Chen DS, Chuang WL, Yu ML, Kao JH: Pegylatedinterferon-a2a with or without low-dose ribavirin for treatment-naivepatients with hepatitis C virus genotype 1 receiving hemodialysis: Arandomized trial. Ann Intern Med 159: 729–738, 2013 PubMed
Advances in Dialysis Methodology
High-Efficiency Hemodiafiltration VersusConventional Low- or High-Flux Hemodialysis
Hemodiafiltration (HDF) is a technique that addsconvective clearance by hemofiltration to the diffusiveclearance achieved with conventional hemodialysis (HD).The process of HDF has the potential to improve clin-ical outcomes by increasing clearance of middle molec-ular weight uremic toxins compared with conventional,high-flux HD. The procedure of HDF requires largevolumes of replacement fluid to be infused into the pa-tient, and this fluid needs to have extremely low levelsof pyrogen and microbial contamination. The development
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 389

of online generation of ultrapure replacement fluid en-ables use of HDF for large groups of patients, a practicecurrently prevalent outside of the United States. In prac-tice, replacement fluid can be infused prefilter, midfilter,or postfilter, but most of the published experiences utilizepostdilution HDF.
Three randomized controlled trials were recentlycompleted examining HDF versus conventional HD.The Convective Transport Study (CONTRAST) randomlyassigned 714 patients to either HDF or to continuous,low-flux HD (1). The HDF group had an increase in Kt/Vurea and lower predialysis b2 microglobulin, a surrogatemeasure of middle molecule clearance. After 3 years offollow-up, the study did not detect a significant differencebetween the groups for the primary outcome of all-causemortality or the secondary outcomes of cardiovascularevents. However, in post hoc analyses, patients who re-ceived higher clearance with HDF (upper tertile of .22liters of convective volume per treatment) exhibited alower all-cause mortality compared with patients as-signed to receive low-flux HD. The Turkish HDF Studyrandomized 782 patients to HDF or conventional high-flux HD (2). After a 2-year follow-up, the composite endpoint of all-cause mortality and nonfatal cardiovascularevent rate was similar between the groups. The post hocanalysis of delivered dose of convective clearance (com-paring those above and below the median achievedclearance of 17.4 liters) suggested that high-dose HDFwas associated with a lower risk of overall and cardio-vascular mortality. From the Turkish experience, it isworth noting that 40 patients in the HDF group withdrewbecause of vascular access problems. Finally, the Estudiode Supervivencia de Hemodiafiltración On-Line (ESHOL)study was a prospective, open-label, clinical trial inwhich 906 ESRD patients in Spain were randomized tocontinue their current modality (mostly high-flux HD)or switch to online HDF (3). After a follow-up of approxi-mately 2 years, the primary outcome of all-cause mortalityoccurred 30% less frequently in the HDF group (mor-tality rates of 18.6% and 27.1% in the HDF and HDgroups, respectively; P¼0.01) (Figure 20). Moreover,analysis of secondary outcomes revealed significantlylower stroke and infectious mortality rates and lower all-cause hospitalizations in the HDF group compared withconventional high-flux HD. It is important to note thatthe ESHOL protocol aimed to provide at least 18 liters ofreplacement fluid per session in those assigned to HDF.Taken in summary, these three recent studies suggestthat HDF, if prescribed to deliver high amounts of total
solute clearance, is capable of conferring a survival benefitin select ESRD patients.
The process of hemodiafiltration has thepotential to increase clearance of middlemolecular weight uremic toxins comparedwith conventional HD. Three recent pro-spective clinical trials suggest that hemo-diafiltration will result in improved survivalof ESRD patients.
A few studies have been performed to attempt torefine the ideal “dose” of convective volume prescribedfor hemodiafiltration. A group of investigators in Spainreported results from 26 young patients with ESRDtreated with HDF who had well functioning arteriove-nous fistulas. Study participants were switched fromthrice-weekly HDF to alternate-day nocturnal HDF (4).A crossover-design allowed comparison of outcomeswith convective volume of 20–30 liters per treatmentwith those for a convective volume of 35–50 liters pertreatment. After 6 months of observation, the nocturnalprogram was associated with significant improvementsin serum phosphate concentrations, BP control, left ven-tricular (LV) hypertrophy, response to erythropoiesis-stimulating agent therapy, and interdialytic weight gain.This study highlights that alternate-day nocturnal HDFis a viable treatment option and that higher-dose HDF(either from longer treatment time or convective clear-ance) may benefit select patients.
How HDF might provide benefit to patients com-pared with conventional HD remains a source of spe-culation. In a small, French clinical trial of 42 ESRDpatients, a comparison was made between patients whoreceived high-flux HD and high-efficiency online HDF(5). Patients who received HDF compared with thoseon HD demonstrated increased brachial artery flow-mediated dilation and carotid artery distensibility,evidence of improved endothelial function. In addi-tion, patients who received HDF had lower predial-ysis b2 microglobulin, serum phosphate concentrations,and protein kinase Cb2 mRNA expression (an endothelialnitric oxide-synthase inhibitor) compared with patientstreated with HD. An ancillary study from the CONTRASTinvestigators (as described above) examined inflammatorymarkers of patients receiving HDF compared with low-flux HD (6). In 405 participants in the CONTRAST study,
390 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
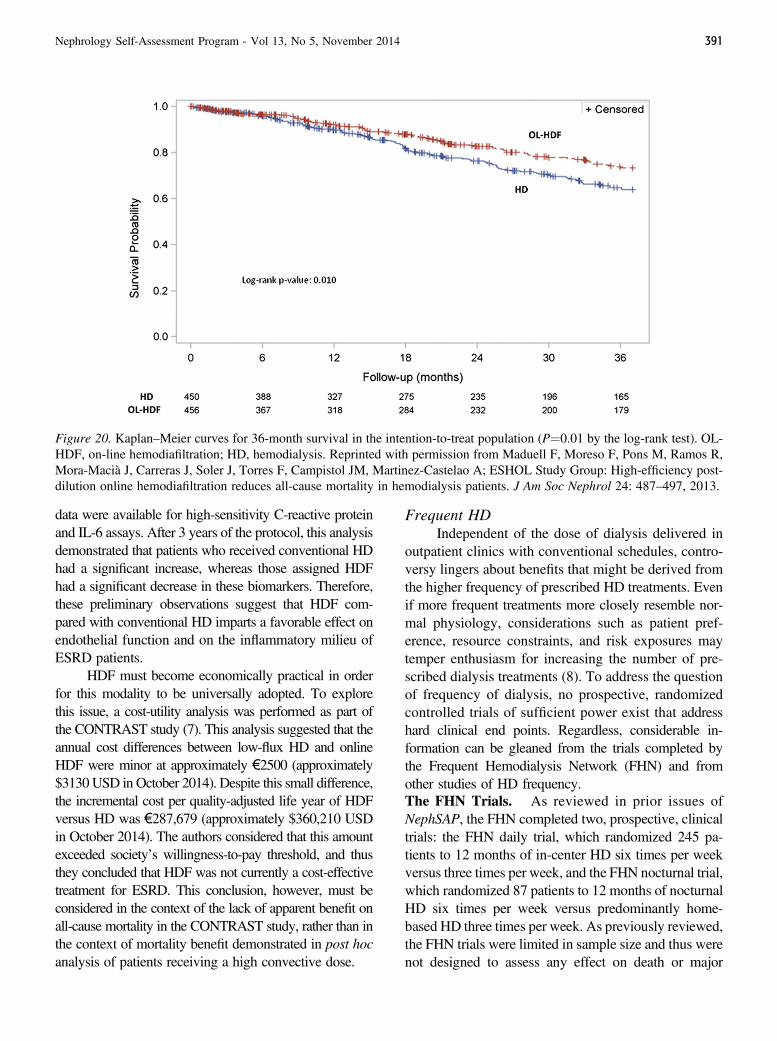
data were available for high-sensitivity C-reactive proteinand IL-6 assays. After 3 years of the protocol, this analysisdemonstrated that patients who received conventional HDhad a significant increase, whereas those assigned HDFhad a significant decrease in these biomarkers. Therefore,these preliminary observations suggest that HDF com-pared with conventional HD imparts a favorable effect onendothelial function and on the inflammatory milieu ofESRD patients.
HDF must become economically practical in orderfor this modality to be universally adopted. To explorethis issue, a cost-utility analysis was performed as part ofthe CONTRAST study (7). This analysis suggested that theannual cost differences between low-flux HD and onlineHDF were minor at approximately €2500 (approximately$3130USD in October 2014). Despite this small difference,the incremental cost per quality-adjusted life year of HDFversus HD was €287,679 (approximately $360,210 USDin October 2014). The authors considered that this amountexceeded society’s willingness-to-pay threshold, and thusthey concluded that HDF was not currently a cost-effectivetreatment for ESRD. This conclusion, however, must beconsidered in the context of the lack of apparent benefit onall-cause mortality in the CONTRAST study, rather than inthe context of mortality benefit demonstrated in post hocanalysis of patients receiving a high convective dose.
Frequent HDIndependent of the dose of dialysis delivered in
outpatient clinics with conventional schedules, contro-versy lingers about benefits that might be derived fromthe higher frequency of prescribed HD treatments. Evenif more frequent treatments more closely resemble nor-mal physiology, considerations such as patient pref-erence, resource constraints, and risk exposures maytemper enthusiasm for increasing the number of pre-scribed dialysis treatments (8). To address the questionof frequency of dialysis, no prospective, randomizedcontrolled trials of sufficient power exist that addresshard clinical end points. Regardless, considerable in-formation can be gleaned from the trials completed bythe Frequent Hemodialysis Network (FHN) and fromother studies of HD frequency.The FHN Trials. As reviewed in prior issues ofNephSAP, the FHN completed two, prospective, clinicaltrials: the FHN daily trial, which randomized 245 pa-tients to 12 months of in-center HD six times per weekversus three times per week, and the FHN nocturnal trial,which randomized 87 patients to 12 months of nocturnalHD six times per week versus predominantly home-based HD three times per week. As previously reviewed,the FHN trials were limited in sample size and thus werenot designed to assess any effect on death or major
Figure 20. Kaplan–Meier curves for 36-month survival in the intention-to-treat population (P¼0.01 by the log-rank test). OL-HDF, on-line hemodiafiltration; HD, hemodialysis. Reprinted with permission from Maduell F, Moreso F, Pons M, Ramos R,Mora-Macià J, Carreras J, Soler J, Torres F, Campistol JM, Martinez-Castelao A; ESHOL Study Group: High-efficiency post-dilution online hemodiafiltration reduces all-cause mortality in hemodialysis patients. J Am Soc Nephrol 24: 487–497, 2013.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 391
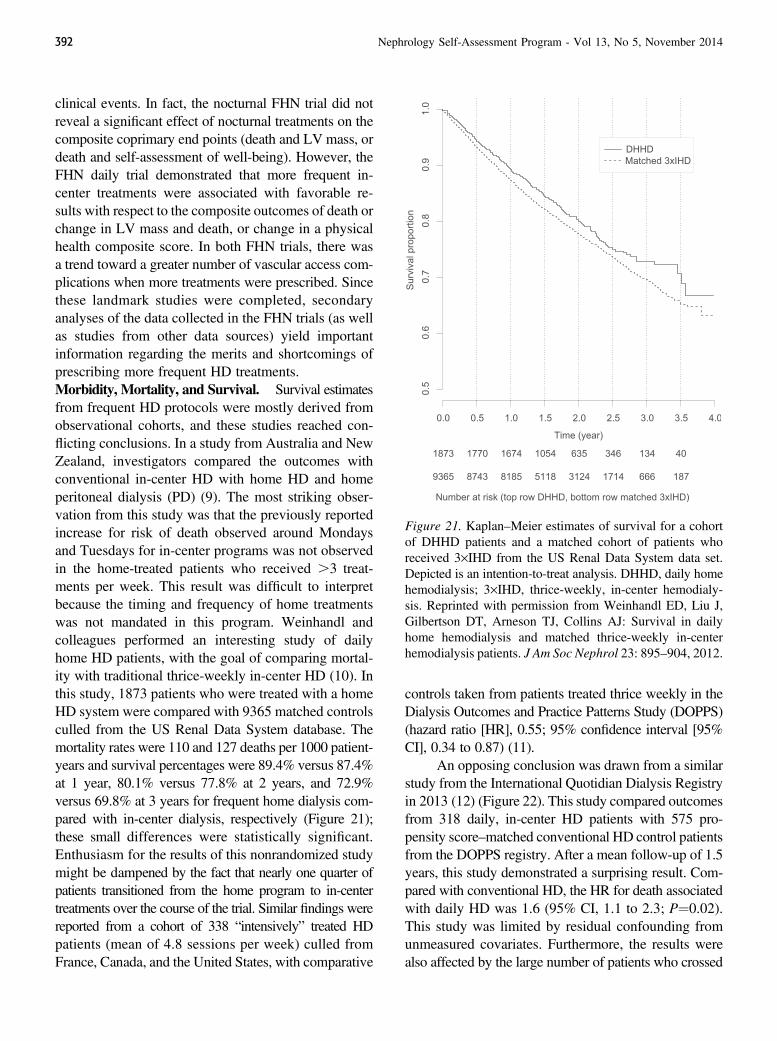
clinical events. In fact, the nocturnal FHN trial did notreveal a significant effect of nocturnal treatments on thecomposite coprimary end points (death and LV mass, ordeath and self-assessment of well-being). However, theFHN daily trial demonstrated that more frequent in-center treatments were associated with favorable re-sults with respect to the composite outcomes of death orchange in LV mass and death, or change in a physicalhealth composite score. In both FHN trials, there wasa trend toward a greater number of vascular access com-plications when more treatments were prescribed. Sincethese landmark studies were completed, secondaryanalyses of the data collected in the FHN trials (as wellas studies from other data sources) yield importantinformation regarding the merits and shortcomings ofprescribing more frequent HD treatments.Morbidity, Mortality, and Survival. Survival estimatesfrom frequent HD protocols were mostly derived fromobservational cohorts, and these studies reached con-flicting conclusions. In a study from Australia and NewZealand, investigators compared the outcomes withconventional in-center HD with home HD and homeperitoneal dialysis (PD) (9). The most striking obser-vation from this study was that the previously reportedincrease for risk of death observed around Mondaysand Tuesdays for in-center programs was not observedin the home-treated patients who received .3 treat-ments per week. This result was difficult to interpretbecause the timing and frequency of home treatmentswas not mandated in this program. Weinhandl andcolleagues performed an interesting study of dailyhome HD patients, with the goal of comparing mortal-ity with traditional thrice-weekly in-center HD (10). Inthis study, 1873 patients who were treated with a homeHD system were compared with 9365 matched controlsculled from the US Renal Data System database. Themortality rates were 110 and 127 deaths per 1000 patient-years and survival percentages were 89.4% versus 87.4%at 1 year, 80.1% versus 77.8% at 2 years, and 72.9%versus 69.8% at 3 years for frequent home dialysis com-pared with in-center dialysis, respectively (Figure 21);these small differences were statistically significant.Enthusiasm for the results of this nonrandomized studymight be dampened by the fact that nearly one quarter ofpatients transitioned from the home program to in-centertreatments over the course of the trial. Similar findings werereported from a cohort of 338 “intensively” treated HDpatients (mean of 4.8 sessions per week) culled fromFrance, Canada, and the United States, with comparative
controls taken from patients treated thrice weekly in theDialysis Outcomes and Practice Patterns Study (DOPPS)(hazard ratio [HR], 0.55; 95% confidence interval [95%CI], 0.34 to 0.87) (11).
An opposing conclusion was drawn from a similarstudy from the International Quotidian Dialysis Registryin 2013 (12) (Figure 22). This study compared outcomesfrom 318 daily, in-center HD patients with 575 pro-pensity score–matched conventional HD control patientsfrom the DOPPS registry. After a mean follow-up of 1.5years, this study demonstrated a surprising result. Com-pared with conventional HD, the HR for death associatedwith daily HD was 1.6 (95% CI, 1.1 to 2.3; P¼0.02).This study was limited by residual confounding fromunmeasured covariates. Furthermore, the results werealso affected by the large number of patients who crossed
Figure 21. Kaplan–Meier estimates of survival for a cohortof DHHD patients and a matched cohort of patients whoreceived 3·IHD from the US Renal Data System data set.Depicted is an intention-to-treat analysis. DHHD, daily homehemodialysis; 3·IHD, thrice-weekly, in-center hemodialy-sis. Reprinted with permission from Weinhandl ED, Liu J,Gilbertson DT, Arneson TJ, Collins AJ: Survival in dailyhome hemodialysis and matched thrice-weekly in-centerhemodialysis patients. J Am Soc Nephrol 23: 895–904, 2012.
392 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
over from daily therapy to conventional in-centertherapy (30% of patients in a median of 10months). Thisstudy suggested that any potential benefits of frequenttreatments (e.g., improved metabolic parameters orBP) might be obscured by other risk exposures such asaccess complications, myocardial stunning, or dietaryindiscretion.
These observations do not allow a definitive con-clusion on whether frequent treatment programs will im-prove survival compared with conventional HD schedules.The published experiences demonstrate that survivalwith frequent HD may be favorable in select patients.Kidney transplantation should still be considered as thebest option for RRT for select patients, but the experi-enced advantages over conventional HD regimens sug-gest that frequent HD programs can be considered asreasonable alternatives to transplantation in some sit-uations (13).Frequent HD, Cardiac Morphology, and CardiacFunction. The FHN experience suggested that increasingthe frequency of HD treatments results in favorablechanges in cardiac structure. The FHN previously dem-onstrated that, compared with conventional HD, frequentdaily treatment results in a significantly greater reduction
in LV mass, as determined by cardiac magnetic reso-nance imaging (14). Chan and colleagues providedadditional information about these changes observed inthe FHN study (15). The nocturnal trial did not dem-onstrate any differences in cardiac structure or function;however, in the frequent daily trial, LV end-diastolicvolume, LV end-systolic volume, and right ventricularend-diastolic volume were substantially reduced com-pared with conventional therapy. Because frequent treat-ments simultaneously decreased LV mass as well as LVend-diastolic volume, the investigators surmised that LVremodeling did not occur with frequent treatments. Thechanges in cardiac morphology with frequent treatmentsmay contribute to the cardiac consequences described,including an increase in the low-frequency heart ratevariability (an estimate of sympathetic modulation), areduction in the QTc interval, or even in the reducedvariation in cardiac deaths associated with days of theweek (9,16,17).Mineral Metabolism in Frequent HD. Patients infrequent HD programs have higher amounts of clearanceof phosphorus, and this may have beneficial effects onhealth of bones and on progressive calcification of softtissues. In the FHN trials, patients in the daily andnocturnal treatment groups had significantly lower serumphosphorus as well as lower prescribed doses of phos-phorus binders compared with conventional HD sched-ules (18). These differences were not associated withchanges in measured serum calcium or parathyroid hor-mone concentrations. These observations differed fromconclusions from a smaller study that did not detecta decrease in serum phosphorus in patients treated withfrequent daily dialysis (19). However, frequent HDcompared with patients treated with thrice-weekly HDprograms was associated with a reduction in fibroblastgrowth factor-23 levels, potentially a sensitive indicatorof phosphorus balance and of risk of calcification (19).In theory, these changes could result in long-term im-provement in bone health or in arterial calcification.Regardless, more frequent HD is capable of controllinghyperphosphatemia and allowing patients less phosphorus–restricted diets with greater freedom from phosphorusbinders.Nutrition and Body Composition in FrequentHD. The FHN programs allowed a careful assessmentof the relationship between the frequency of dialysis andnutritional state. Kaysen and coworkers performed a de-tailed ancillary study to assess the nutrition and bodyweight changes associated with the FHN trials (20). In
Figure 22. Cumulative survival of patients in the Inter-national Quotidian Dialysis Registry who received dailyhemodialysis (.5 times per week) between 2001 and 2010,compared with propensity score–based matched controlsfrom the Dialysis Outcomes and Practice Patterns Study whoreceived conventional (thrice-weekly) hemodialysis. Reprintedwith permission from Suri RS, Lindsay RM, Bieber BA, PisoniRL, Garg AX, Austin PC, Moist LM, Robinson BM, GillespieBW, Couchoud CG, Galland R, Lacson EK Jr, ZimmermanDL, Li Y, Nesrallah GE: A multinational cohort study of in-center daily hemodialysis and patient survival. Kidney Int 83:300–307, 2013.
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 393

the frequent daily trial, there were no significant dif-ferences in the serum albumin concentration or theprotein catabolic rate between groups. The extracellularwater decreased in the group that received HD six timesper week compared with the group that received HDthrice weekly. There were no significant differencesdetected in other measurements of body mass.Vascular Access in Frequent HD. As discussed earlierin this issue of the NephSAP and reported in the FHNtrials, one possible downside to frequent treatments isan increased risk exposure for vascular access. TheFHN daily trial determined a statistically significant76% increase in the risk for a first access event, such asrepair, loss, and access-related hospitalizations, com-pared with the conventional HD group (HR 1.76; 95%CI, 1.11 to 2.79; P¼0.02). The total losses of arterio-venous accesses did not differ between the randomizedgroups. Similar but not statistically significant trends wereobserved in the nocturnal trial (21). The investigatorssurmised that the increased intervention rate was notattributable to increased access surveillance but instead toincreased frequency of trauma at venipuncture sites.Quality of Life in Frequent HD. Patients with ESRDare known to have impaired health-related quality oflife. For all of the potential gain from more frequentHD therapies, intensive HD imparts a significant bur-den on patients. The merits of more frequent HD, in-cluding liberalization of diet and fewer BP medicationsmust be balanced with adverse consequences, such astreatment constraints and burnout. Many studies tookadvantage of the FHN experience. It is well docu-mented that cognitive impairment is common in pa-tients with ESRD, and this condition could affect theperceived quality of life. Despite the suggestion thatmore frequent HD might result in improvements inmemory or verbal fluency, the interventions in FHNdid not result in significant improvements in the trail-making test or in performance on a formal mentalstatus examination (22). With regard to physical per-formance and status, more frequent HD did not appearto improve the short physical performance battery, butwas associated with a significant improvement in a surveyof composite physical health and in the physical func-tioning scale (23).
Because the FHN trials did not detect a significantdifference among the treatment groups with regard toanemia, there was no physiologic reason for a differ-ence in physical function (24). Despite the burden ofmore frequent treatments, daily HD was not associated
with more symptoms of depression. Unruh and col-leagues determined that those assigned to frequentdaily HD had no significant change in their BeckDepression Inventory scores, but study participantsexperienced clinically significant improvements inadjusted mean mental health composite and emotionalsubscale scores (25). The results were similar in theFollowing Rehabilitation, Economics and Everyday-Dialysis Outcome Measurements (FREEDOM) study,an ongoing prospective cohort study of frequent homeHD (26). In this study, the 154 patients who transitionedto a six-times-per-week regimen and were followed fora year reported significant improvements in all eightindividual domains of the Short Form-36. For the pa-tients who completed the 1-year follow-up in theFREEDOM trial (53% of the initial cohort), the per-centage of patients achieving a physical-componentsummary score at least as high as the general populationmore than doubled. These results are not definitive,but the observations suggest that frequent home HDprograms are not an emotional burden to many ESRDpatients.Costs in Frequent HD. Cost assessment will be vitalto determine whether frequent dialysis is a viable treat-ment option in the future. It is difficult to estimate thefinancial impact of these programs implemented in theUnited States, because the FHN trials did not ascertaininformation related to cost. However, costs were mod-eled for nocturnal and frequent daily HD programsbased on conditions in the United Kingdom, Canada,and Australia (27). For all modalities, the first year ex-penditures were significantly greater than subsequentyears due to training and other start-up costs. In sub-sequent years, home therapies were less expensive thanin-center treatments. In the United Kingdom, costs forfrequent home HD were higher than for in-center andconventional home HD. In Australia and Canada, fre-quent home HD was lower than in-center HD andhigher than conventional home HD. In this study, thehigher costs of frequent compared with conventionalhome HD were attributed to consumables. This analysisdid not refute the feasibility of frequent treatments,particularly if they can be delivered in a home setting.
Wearable Dialysis and Implantable ArtificialKidney Devices
Dialysis systems that are capable of providinglengthened periods of solute clearance, either as “wear-able” or implantable devices, are attractive in terms of
394 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

convenience for the patient and mimicry of normal phys-iology. Despite encountering obstacles, which precludeacceptance as a standard of care, researchers are makingsome technical progress in this area.
Technically similar to PD, the Vicenza wearableartificial kidney (ViWAK) is a device that utilizes adual-lumen catheter placed in the peritoneum. A small,battery-powered pump drives flow, and after an initial2-hour dwell, peritoneal dialysate is continuously re-cycled by the passage of spent dialysate through aseries of sorbents such as activated microporous carbon,zirconium, and polystyrene (28). Urease is also includedin series in order to remove urea from the dialysate. Un-fortunately, the ViWAK has no system in place to correctelectrolyte derangements in the recycled dialysate, and itrelies on the use of fresh dialysate each morning. In orderto be successfully used in patients, this device will alsolikely require nighttime exchanges with dialysate con-taining icodextrin. An automated artificial wearable kid-ney (AWAK) has also been developed, and it also sharestechnical features with PD. The AWAK requires asingle-lumen peritoneal catheter and different sorbentcartridges to continuously regenerate dialysate (28).The dialysate is recirculated in a tidal manner, so thatthe solution can potentially be reused for up to amonth. The AWAK system has a chamber that con-tains a disposable cartridge that holds electrolytes,glucose, and lactate to help refresh the regenerateddialysate via a small battery-powered pump, while theultrafiltrate is discarded into a separate bag. The devicealso includes an ammonia sensor to monitor sorbentsaturation. Clinical trials are underway with the AWAKtechnology.
In contrast with variations on PD, a wearableartificial kidney (WAK) is also under development thatmore closely mirrors HD. The WAK 1.0 involves a bloodcircuit with flow powered by a lightweight minipump.Similar to the PD-like devices, the WAK 1.0 systemrequires priming with a small volume of sterile dialysateand regeneration of dialysate by ion-exchange sorbentsand biopolymers (28). Similar to standard extracorporealcircuits, the WAK 1.0 requires provision of antico-agulation in order to be tested in humans. Ideally, thefuture will accommodate the development of an arti-ficial or bioartificial kidney that can be implanted intopatients. It is projected that these devices will be anas-tomosed to the iliac vessels and avoid problems relatedto blood pumps (28). Technology is being developed toaddress the needs of an implantable dialyzer, including
the need for a practical, lifetime device, acceptablepower requirements, and adequate waste removal.
Unique Patient Population: Dialysis in AdvancedCongestive Heart Failure
In addition to facing the fate of progressive kidneydisease, patients with CKD are also likely to be bur-dened by symptoms of congestive heart failure (CHF).In the US Medicare population aged.65 years, 41% ofpatients with stage 4–5 CKD carry a diagnosis of CHF(29). Diminished kidney function appears to have a sub-stantial bearing on outcomes in CHF. If the CHF isrelated to poor systolic function, the 2-year survival is71% for non-CKD patients but only 45% for those withstage 4–5 CKD; for diastolic heart failure, the 2-yearsurvival rates are 72%, and 50%, respectively (29). Inaddition to diminished survival, patients with ad-vanced CHF and CKD suffer from poor quality of lifeand reduced exercise tolerance. Two approaches aregaining popularity in this vulnerable population:placement of ventricular assist devices and ultrafil-tration with RRT.
Continuous-flow LV assist devices (LVADs) canbe effective as a bridge to transplant or as destinationtherapy in patients with advanced heart failure (30,31).Successful placement of an LVAD can improve theduration and the quality of life in CHF, and the devicemay improve objective measures of exercise capacity(31). An intact LVAD can also improve underlying kid-ney function. In a series of 83 patients with CHF whosurvived after LVAD placement, GFR significantly in-creased from admission (53.2621.4 ml/min per 1.73m2) to 1 month after LVAD implantation (87.4627.9ml/min per 1.73 m2; P,0.001). Regardless, 10% of theLVAD recipients who survived required initiation ofdialysis. Unfortunately, maintenance dialysis in patientswho survive after LVAD can be quite complicated, in-cluding concern about risk of hemorrhage, predispositionto infections (particularly with the percutaneous LVADlead line), and monitoring hemodynamic tolerance ofdialysis (30). Once a patient with a functional LVADbecomes clinically stable, it is feasible to consider tran-sitioning to either PD or intermittent HD (32,33).Monitoring of BP by conventional means is often in-accurate, particularly with continuous-flow LVADs (30).However, the equivalent of mean arterial pressure can beobtained with a Doppler device (30). With older LVADdevices, the peritoneum was often violated; however,with newer techniques, PD is a viable option (32).
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 395

Several studies recently examined outcomes afterpatients with advanced CHF were placed on dialysis formanagement of refractory CHF. Some programs ad-vocate ultrafiltration with PD in patients with decom-pensated CHF, frequent hospitalizations, underlyingstage 3 CKD, and no obvious contraindications to PD(34). In a series of 10 patients with end stage CHF whowere not eligible for heart transplantation, initiation ofPD resulted in average weight loss of 7 kg (P¼0.02compared with predialysis), a significant decrease inrehospitalization rate (3.262.5 to 0.160.3 admissionsper patient; P¼0.01), and reduced average length of stay(from 37636.7 to 0.7862.3 days; P¼0.02) (35). Kuninand colleagues evaluated the results from their experienceproviding PD support for a series of 37 patients withrefractory CHF (36). In this study, the median survivalwas only 14 months, and the patients in the lowest quar-tile of survival demonstrated lower serum albumin con-centration (2.8 versus 3.5 g/dl in the greatest quartile;P¼0.003), lower serum sodium concentration (126 ver-sus 137 mEq/L; P,0.001), higher serum leukocyte count(7500 versus 6800/ml; P¼0.03), higher eGFR (39.4 ver-sus 29.9 ml/min per 1.73 m2; P¼0.04), higher number ofhospitalizations before starting PD (3.4 versus 1.9 daysper month; P¼0.003), and lower LV mass index (113versus 137 g/m2; P¼0.04). These prognostic factors canbe considered when planning RRTs in patients with CHF.
References1. Grooteman MP, van den Dorpel MA, Bots ML, Penne EL, van der
Weerd NC, Mazairac AH, den Hoedt CH, van der Tweel I, Lévesque R,Nubé MJ, ter Wee PM, Blankestijn PJ; CONTRAST Investigators:Effect of online hemodiafiltration on all-cause mortality and cardiovas-cular outcomes. J Am Soc Nephrol 23: 1087–1096, 2012 PubMed
2. Ok E, Asci G, Toz H, Ok ES, Kircelli F, Yilmaz M, Hur E, Demirci MS,Demirci C, Duman S, Basci A, Adam SM, Isik IO, Zengin M,Suleymanlar G, Yilmaz ME, Ozkahya M: Mortality and cardiovascularevents in online haemodiafiltration (OL-HDF) compared with high-fluxdialysis: Results from the Turkish OL-HDF Study. Nephrol DialTransplant 28: 192–202, 2013
3. Maduell F, Moreso F, Pons M, Ramos R, Mora-Macià J, Carreras J,Soler J, Torres F, Campistol JM, Martinez-Castelao A; ESHOL StudyGroup: High-efficiency postdilution online hemodiafiltration reducesall-cause mortality in hemodialysis patients. J Am Soc Nephrol 24: 487–497, 2013 PubMed
4. Maduell F, Arias M, Durán CE, Vera M, Fontseré N, Azqueta M, RicoN, Pérez N, Sentis A, Elena M, Rodriguez N, Arcal C, Bergadá E,Cases A, Bedini JL, Campistol JM: Nocturnal, every-other-day, onlinehaemodiafiltration: An effective therapeutic alternative. Nephrol DialTransplant 27: 1619–1631, 2012 PubMed
5. Bellien J, Fréguin-Bouilland C, Joannidès R, Hanoy M, Rémy-Jouet I,Monteil C, IacobM,Martin L, Renet S, Vendeville C, Godin M, ThuillezC, Le Roy F: High-efficiency on-line haemodiafiltration improves con-duit artery endothelial function compared with high-flux haemodialysis inend-stage renal disease patients. Nephrol Dial Transplant 29: 414–422,2014 PubMed
6. den Hoedt CH, Bots ML, Grooteman MP, van der Weerd NC, MazairacAH, Penne EL, Levesque R, Ter Wee PM, Nubé MJ, Blankestijn PJ,van den Dorpel MA: Online hemodiafiltration reduces systemic in-flammation compared to low-flux hemodialysis. Kidney Int 86: 423–432, 2014 PubMed
7. Mazairac AH, Blankestijn PJ, Grooteman MP, Penne EL, van der WeerdNC, den Hoedt CH, Buskens E, van den Dorpel MA, ter Wee PM, NubéMJ, Bots ML, de Wit GA; CONTRAST investigators: The cost-utility ofhaemodiafiltration versus haemodialysis in the Convective TransportStudy. Nephrol Dial Transplant 28: 1865–1873, 2013 PubMed
8. Schachter ME, Chan CT: Current state of intensive hemodialysis: Acomparative review of benefits and barriers. Nephrol Dial Transplant27: 4307–4313, 2012 PubMed
9. Krishnasamy R, Badve SV, Hawley CM, McDonald SP, Boudville N,Brown FG, Polkinghorne KR, Bannister KM, Wiggins KJ, Clayton P,Johnson DW: Daily variation in death in patients treated by long-termdialysis: Comparison of in-center hemodialysis to peritoneal and homehemodialysis. Am J Kidney Dis 61: 96–103, 2013 PubMed
10. Weinhandl ED, Liu J, Gilbertson DT, Arneson TJ, Collins AJ: Survivalin daily home hemodialysis and matched thrice-weekly in-centerhemodialysis patients. J Am Soc Nephrol 23: 895–904, 2012 PubMed
11. Nesrallah GE, Lindsay RM, Cuerden MS, Garg AX, Port F, Austin PC,Moist LM, Pierratos A, Chan CT, Zimmerman D, Lockridge RS,Couchoud C, Chazot C, Ofsthun N, Levin A, Copland M, Courtney M,Steele A, McFarlane PA, Geary DF, Pauly RP, Komenda P, Suri RS:Intensive hemodialysis associates with improved survival compared withconventional hemodialysis. J Am Soc Nephrol 23: 696–705, 2012 PubMed
12. Suri RS, Lindsay RM, Bieber BA, Pisoni RL, Garg AX, Austin PC,Moist LM, Robinson BM, Gillespie BW, Couchoud CG, Galland R,Lacson EK Jr, Zimmerman DL, Li Y, Nesrallah GE: A multinationalcohort study of in-center daily hemodialysis and patient survival.Kidney Int 83: 300–307, 2013 PubMed
13. Pauly RP: Survival comparison between intensive hemodialysis andtransplantation in the context of the existing literature surroundingnocturnal and short-daily hemodialysis. Nephrol Dial Transplant 28:44–47, 2013 PubMed
14. Mishra RK, Dubin RF: The effects of frequent hemodialysis on leftventricular mass, volumes, and geometry. Clin J Am Soc Nephrol 8:2025–2027, 2013 PubMed
15. Chan CT, Greene T, Chertow GM, Kliger AS, Stokes JB, Beck GJ,Daugirdas JT, Kotanko P, Larive B, Levin NW, Mehta RL, Rocco M,Sanz J, Yang PC, Rajagopalan S; Frequent Hemodialysis NetworkTrial Group: Effects of frequent hemodialysis on ventricular volumesand left ventricular remodeling. Clin J Am Soc Nephrol 8: 2106–2116, 2013 PubMed
16. Chan CT, Chertow GM, Daugirdas JT, Greene TH, Kotanko P, LariveB, Pierratos A, Stokes JB; Frequent Hemodialysis Network Daily TrialGroup: Effects of daily hemodialysis on heart rate variability: Resultsfrom the Frequent Hemodialysis Network (FHN) Daily Trial. NephrolDial Transplant 29: 168–178, 2014 PubMed
17. Thomson BK, Momciu B, Huang SH, Chan CT, Urquhart BL, SkanesAC, Krahn AD, Klein GJ, Lindsay RM: Frequent nocturnal hemodial-ysis associates with improvement of prolonged QTc intervals. NephronClin Pract 123: 74–82, 2013 PubMed
18. Daugirdas JT, Chertow GM, Larive B, Pierratos A, Greene T, Ayus JC,Kendrick CA, James SH, Miller BW, Schulman G, Salusky IB, KligerAS; Frequent Hemodialysis Network (FHN) Trial Group: Effects offrequent hemodialysis on measures of CKD mineral and bone disorder.J Am Soc Nephrol 23: 727–738, 2012 PubMed
19. Zaritsky J, Rastogi A, Fischmann G, Yan J, Kleinman K, Chow G,Gales B, Salusky IB, Wesseling-Perry K: Short daily hemodialysis isassociated with lower plasma FGF23 levels when compared withconventional hemodialysis. Nephrol Dial Transplant 29: 437–441,2014 PubMed
20. Kaysen GA, Greene T, Larive B, Mehta RL, Lindsay RM, Depner TA,Hall YN, Daugirdas JT, Chertow GM; FHN Trial Group: The effect of
396 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
frequent hemodialysis on nutrition and body composition: FrequentHemodialysis Network Trial. Kidney Int 82: 90–99, 2012 PubMed
21. Suri RS, Larive B, Sherer S, Eggers P, Gassman J, James SH, Lindsay RM,Lockridge RS, Ornt DB, Rocco MV, Ting GO, Kliger AS; FrequentHemodialysis Network Trial Group: Risk of vascular access complicationswith frequent hemodialysis. J Am Soc Nephrol 24: 498–505, 2013 PubMed
22. Kurella Tamura M, Unruh ML, Nissenson AR, Larive B, Eggers PW,Gassman J, Mehta RL, Kliger AS, Stokes JB; Frequent HemodialysisNetwork (FHN) Trial Group: Effect of more frequent hemodialysis oncognitive function in the Frequent Hemodialysis Network Trials. Am JKidney Dis 61: 228–237, 2013 PubMed
23. Hall YN, Larive B, Painter P, Kaysen GA, Lindsay RM, Nissenson AR,UnruhML, RoccoMV,ChertowGM; Frequent Hemodialysis Network TrialGroup: Effects of six versus three times per week hemodialysis on physicalperformance, health, and functioning: Frequent Hemodialysis Network(FHN) randomized trials. Clin J Am Soc Nephrol 7: 782–794, 2012 PubMed
24. Ornt DB, Larive B, Rastogi A, Rashid M, Daugirdas JT, Hernandez A,Kurella Tamura M, Suri RS, Levin NW, Kliger AS; Frequent Hemodi-alysis Network Trial Group: Impact of frequent hemodialysis on anemiamanagement: Results from the Frequent Hemodialysis Network (FHN)Trials. Nephrol Dial Transplant 28: 1888–1898, 2013 PubMed
25. Unruh ML, Larive B, Chertow GM, Eggers PW, Garg AX, Gassman J,Tarallo M, Finkelstein FO, Kimmel PL; FHN Trials Group: Effects of 6-times-weekly versus 3-times-weekly hemodialysis on depressive symp-toms and self-reported mental health: Frequent Hemodialysis Network(FHN) Trials. Am J Kidney Dis 61: 748–758, 2013 PubMed
26. Finkelstein FO, Schiller B, Daoui R, Gehr TW, Kraus MA, Lea J, LeeY, Miller BW, Sinsakul M, Jaber BL: At-home short daily hemodialysisimproves the long-term health-related quality of life. Kidney Int 82:561–569, 2012 PubMed
27. Komenda P, Gavaghan MB, Garfield SS, Poret AW, Sood MM: Aneconomic assessment model for in-center, conventional home, and morefrequent home hemodialysis. Kidney Int 81: 307–313, 2012 PubMed
28. Fissell WH, Roy S, Davenport A: Achieving more frequent and longerdialysis for the majority: Wearable dialysis and implantable artificialkidney devices. Kidney Int 84: 256–264, 2013 PubMed
29. US Renal Data System: USRDS 2013 Annual Data Report: Atlas ofChronic Kidney Disease and End-Stage Renal Disease in the UnitedStates, Bethesda, MD, National Institutes of Health, National Instituteof Diabetes and Digestive and Kidney Diseases, 2013
30. Patel AM, Adeseun GA, Ahmed I, Mitter N, Rame JE, Rudnick MR:Renal failure in patients with left ventricular assist devices. Clin J AmSoc Nephrol 8: 484–496, 2013 PubMed
31. Leibner ES, Cysyk J, Eleuteri K, El-Banayosy A, Boehmer JP, Pae WE:Changes in the functional status measures of heart failure patients withmechanical assist devices. ASAIO J 59: 117–122, 2013 PubMed
32. Guglielmi AA, Guglielmi KE, Bhat G, Siemeck R, Tatooles AJ:Peritoneal dialysis after left ventricular assist device placement. ASAIOJ 60: 127–128, 2014 PubMed
33. Sosa Barrios HS, Palmer A, Khan T, Banner N, Duncan N: Successfullong-term intermittent hemodialysis in a patient with left ventricularassist device [published online ahead of print July 17, 2013]. ClinNephrol doi:10.5414/CN107894
34. Iadarola GM, Lusardi P, La Milia V, Amici G, Santarelli S, Virga G,Basile C, Bertoli S, Bonofiglio R, Del Rosso G, Feriani M, Galli E,Gallieni M, Gambaro G, Sandrini M, Sisca S, Cancarini G: Peritonealultrafiltration in patients with advanced decompensated heart failure. JNephrol 26[Suppl 21]: 159–176, 2013 PubMed
35. Rizkallah J, Sood MM, Reslerova M, Cordova F, Malik A,Sathianathan C, Estrella-Holder E, Zieroth S: Reduced hospital-izations in severe, refractory congestive heart failure with perito-neal dialysis: A consecutive case series. Clin Nephrol 80: 334–341,2013 PubMed
36. Kunin M, Arad M, Dinour D, Freimark D, Holtzman EJ: Peritonealdialysis in patients with refractory congestive heart failure: Potentialprognostic factors. Blood Purif 35: 285–294, 2013 PubMed
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 397
End-Stage Renal Disease and Dialysis
Claiming Credits and Evaluation Process
Accreditation StatementThe American Society of Nephrology (ASN) is accredited by the Accreditation Council for Continuing Medical Education toprovide continuing medical education for physicians.
AMA Credit Designation StatementThe ASN designates this enduring material for a maximum of 8.0 AMA PRA Category 1 Credits™. Physicians should claimonly the credit commensurate with the extent of their participation in the activity.
American Academy of Physician Assistants Accreditation Statement (AAPA)This Self-Assessment CME program has been reviewed and is approved for a maximum of 8.0 AAPACategory 1 Self-Assessment CME credits by the Physician Assistant Review Panel. Approval is validuntil 10/31/2016. Physician Assistants should claim only the credit commensurate with their extent oftheir participation in the activity. This program was planned in accordance with AAPA's CME Standards.
Original Release Date: November 2014CME Credit Termination Date: October 31, 2016Examination Available Online: On or before Monday, November 17, 2014Estimated Time for Completion: 8 hoursAnswers with Explanations
• Provided with a passing score after the first and/or after the second attempt
• December 2016: posted on the ASN website when the issue is archived.
Method of Participation
• Read the syllabus that is supplemented by original articles in the reference lists.
• Complete the online self-assessment examination.
• Each participant is allowed two attempts to pass the examination (.75% correct) for CME credit.
• Upon completion, review your score and incorrect answers and print your certificate.
• Answers and explanations are provided with a passing score or after the second attempt.
Activity Evaluation and CME Credit Instructions
• Go to www.asn-online.org/cme, and enter your ASN login on the right.
• Click the ASN CME Center.
• Locate the activity name and click the corresponding ENTER ACTIVITY button.
• Read all front matter information.
• On the left-hand side, click and complete the Demographics & General Evaluations.
• Complete and pass the examination for CME credit.
• Upon completion, click Claim Your Credits, check the Attestation Statement box, and enter the number of CMEcredits commensurate with the extent of your participation in the activity.
• If you need a certificate, Print Your Certificate on the left.
For your complete ASN transcript, click the ASN CME Center banner, and click View/Print Transcript on the left.
Instructions to obtain American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) PointsEach issue of NephSAP provides 10 MOC points. Respondents must meet the following criteria:
• Be certified by ABIM in internal medicine and/or nephrology and enrolled in the ABIM–MOC program
• Enroll for MOC via the ABIM website (www.abim.org).• Enter your (ABIM) Candidate Number and Date of Birth prior to completing the examination.
• Take the self-assessment examination within the timeframe specified in this issue of NephSAP.
• Below your score select “Click here to post to ABIM.”
MOC points will be applied to only those ABIM candidates who have enrolled in the MOC program. It is your responsibility tocomplete the ABIM MOC enrollment process.
398
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
NephSAP, Volume 13, Number 5, November 2014—ESRD and Dialysis
1. You are reviewing the monthly laboratory resultsof a 45-year-old female patient who has ESRD at-tributed to FSGS. She has been undergoing peri-toneal dialysis (PD) for 2 years. She is on nightlycontinuous cycling PD (CCPD) with predominantly2.5% dextrose dialysate. She has residual renalfunction with an eGFR of 5 ml/min per 1.73 m2.On physical examination, her BP is 130/80 mmHgand she has no signs or symptoms of volumeoverload. Net daily ultrafiltration is approximately1 liter. Laboratory studies show hemoglobin 10.1 g/dl,potassium 3.2 mEq/L, total CO2 22 mmol/L, phos-phorus 4.4 mg/dl, and calcium 9.1 mg/dl. Her medi-cations include metoprolol succinate 100 mg daily,lisinopril 10 mg daily, and calcium acetate 667 mgone with meals.Which ONE of the following would you rec-ommend to decrease the left ventricular massindex in this patient?
A. Increase the daily ultrafiltration volumeB. Add spironolactone 25 mg dailyC. Increase calcium acetate to 1334 mg with
mealsD. Start darbepoetin 60 mg subcutaneously
once monthlyE. Increase lisinopril to 20 mg daily
2. You are rounding on a group of patients in an out-patient hemodialysis facility and you review themonthly laboratory values with the multidisciplin-ary care team and patients. One of the patients asksyou about his prognosis, and you reflect on hisexpected long-term cardiovascular risk. He is a68-year-old man with a history of ESRD resultingfrom arterionephrosclerosis. He currently receivesthrice-weekly in-center hemodialysis. He smokesone-half pack of cigarettes per day. On physicalexamination, his BP is 138/80 mmHg. A rightcarotid bruit is present. There is loss of hair onthe distal lower legs. The pedal pulses are dimin-ished. Laboratory studies show equilibrated Kt/Vof 1.3, hemoglobin 10.8 g/dl, calcium 9.1 mg/dl,phosphorus 5.4 mg/dl, parathyroid hormone (PTH)586 pg/ml, and LDL cholesterol 110 mg/dl.
Which ONE of the following would have thegreatest effect on favorably reducing his riskfor future cardiovascular events?
A. Smoking cessationB. Reducing serum PTH with cinacalcetC. Switching from conventional hemodialysis
to hemodiafiltrationD. Changing from standard to ultrapure dialysateE. Reducing LDL cholesterol concentration
3. A 46-year-old woman with CKD is admitted tothe hospital with worsening fatigue, decreased ap-petite, nausea, and vomiting. Laboratory values re-veal progression of CKD with a BUN of 75 mg/dland a serum creatinine of 6.2 mg/dl. Serum potas-sium is 4 mEq/L and the total CO2 is 21 mmol/L.The patient had previously discussed with herprimary nephrologist that she prefers PD as hermodality, although she has not yet had a PD catheterplaced.Which ONE of the following approaches offersthe BEST therapeutic option and lowest in-fectious risk for the patient?
A. The patient should have a femoral non-tunneled central venous catheter placed toundergo hemodialysis for the next 2–4weeks.She should also have a PD catheter placedand transition to peritoneal dialysis 2–4weeksafter the catheter is placed.
B. She should have a tunneled central venouscatheter placed and undergo hemodialysis.She should not be switched to PD, becauseshe will likely lose her residual renal func-tion after starting hemodialysis.
C. The patient should be started on sodiumbicarbonate supplementation and antiemetics.She can be discharged and followed closelyin the clinic.
D. The patient should have a PD catheter placedin anticipation of starting PD. She can bedischarged home with plans to initiate PDafter waiting 4 weeks to heal.
E. The patient should have a peritoneal catheterplaced. PD should be started shortly after
399
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014

placement of catheter during this hospital-ization. Low peritoneal dialysate volumes ina supine position for several days should beused, initially in the hospital and subse-quently as an outpatient.
4. A 60-year-old woman with a history of ESRDsecondary to type 2 diabetes mellitus and kidneytransplantation 5 years ago is found to have pro-gressive allograft failure, congestive heart failure,and hypertension. She is seen in the clinic to dis-cuss her transition to dialysis. Her local dialysisunit has a PD population of about 50 patients. Sheis interested in PD, but she would like to knowwhether she would be able to be maintained onthis modality long term.Which ONE of the following is the MOSTlikely risk factor for treatment failure of PD inthis patient?
A. Congestive heart failureB. History of kidney transplantationC. Her ageD. Diabetes mellitusE. Treatment at center with a large population
of PD patients
5. A 45-year-old woman on CCPD for 3 years isevaluated for complaints of erythema at the exitsite of her PD catheter. She denies nausea, vom-iting, diarrhea, or abdominal pain and states thather dialysate has been clear. On physical examina-tion, she is afebrile. The abdomen is soft and non-tender. Erythema measuring 14 mm in diametersurrounds the exit site. Minimal purulent drain-age is present. There is no erythema overlyingthe catheter tunnel and no additional drainage iselicited after milking the catheter. Laboratoryanalysis of the dialysis effluent reveals a cell countof 15 total nucleated cells/mm3with 35%neutrophils.The fluid culture is negative. A culture from theexit site grows methicillin-sensitive Staphylococcusaureus. Sensitivities are pending.Which ONE of the following is the MOSTappropriate treatment for this patient?
A. No additional treatmentB. Intraperitoneal cefazolin plus ceftazidimeC. Oral cephalexinD. Gentamicin cream
6. A 66-year-old woman who has been on PD for thelast 10 years is evaluated for intermittent vague
abdominal pain, nausea, and vomiting. Two weeksago, she had 2 days of bloody peritoneal effluentthat cleared spontaneously. She complains of in-termittent constipation and increased leg edema,but she has not had difficulty with peritonealcatheter function. On physical examination, sheappears chronically ill but is in no acute distress.Her temperature is 37.3�C. Her weight is 60 kg,decreased from 63 kg 1 month ago. The abdo-men is somewhat firm and minimally tender withmoderate pressure. Bowel sounds are present. Thereare no peritoneal signs. There is 11 leg edemabilaterally. Laboratory studies show hemoglobin8.6 g/dl, albumin 3.2 g/dl, and C-reactive proteinof 2 mg/dl (reference range, 0.0–0.8). Peritonealfluid analysis shows 45 total nucleated cells/mm3
with 40% neutrophils. Gram stain is negative.Results of the peritoneal fluid culture are pend-ing. Her most recent peritoneal equilibrium testshowed a dialysate-to-plasma creatinine ratio of0.85 at 4 hours increased from 0.76 6 months agoand 0.62 2 years ago. An upright chest radiographand upright and supine abdominal radiographsshow mild small bowel dilation and an isolatedloop of bowel with an air-fluid level.Which ONE of the following is the MOSTappropriate next step in management?
A. Computed tomography scan of the abdo-men and pelvis
B. Referral for diagnostic laparoscopyC. Empiric vancomycin and ceftazidimeD. Upper endoscopy
7. A 28-year-old woman with progressive stage 4CKD due to reflux nephropathy is contemplatingpregnancy. Her eGFR is 15 ml/min per 1.73 m2,and has decreased by an average of 4 ml/min peryear over the last 5 years. She indicates a con-tinued desire for pregnancy after receiving in-formation regarding the increased risk of morerapid progression to dialysis dependency as wellas the increased risk for adverse maternal andfetal outcomes associated with pregnancy andadvanced CKD. She denies dysgeusia, nausea,vomiting, or anorexia. She asks about how tooptimize her chances of successful pregnancy.Laboratory studies show sodium 138 mEq/L,potassium 4.9 mEq/L, chloride 103 mEq/L, totalCO2 21 mmol/L, BUN 68 mg/dl, and creatinine
400 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
3.6 mg/dl (Modification of Diet in Renal DiseaseeGFR 15 ml/min per 1.73 m2).Which ONE of the following managementstrategies would you recommend to optimizeher chances of successful pregnancy?
A. If she conceives pregnancy, start hemodi-alysis when uremic symptoms develop
B. Start PD now, targeting a weekly Kt/V of.2.0
C. Initiate hemodialysis now, targeting a pre-dialysis BUN ,50 mg/dl
D. Initiate hemodialysis after pregnancy is sus-pected or confirmed, targeting.36 hours ofdialysis per week
8. A 47-year-old man with autosomal dominant poly-cystic kidney disease has been on hemodialysis for4 years after his first kidney transplant failed dueto chronic antibody-mediated rejection. He is nowhighly sensitized. He dialyzes with a low-flux mem-brane 4 hours thrice weekly with a dialysate flowrate of 600 ml/min. His arteriovenous fistula (AVF)has been functioning well and delivers an averageblood flow rate of 500ml/min yielding a single-poolKt/Vurea of 1.6. His predialysis BUN is 48 mg/dland his hemoglobin is 11 g/dl. He has not re-quired treatment with an erythropoiesis-stimulatingagent. He complains of fatigue and pruritus. Hisnephrologist decides to alter his prescription tomaximize middle molecule clearance.Which ONE of the following measures isMOST likely to provide the best middle mol-ecule clearance for this patient?
A. Increasing the treatment time to 5 hoursB. Increasing the dialysate flow rate to 800
ml/minC. Switching the dialyzer to a high-flux
membraneD. Changing to on-line hemodiafiltration
with a convective clearance of 25 liters persession
9. A 64-year-old man with ESRD from polycystickidney disease is evaluated during multidisci-plinary rounds. He has been maintained on hemo-dialysis for 3 years. He was initially resistant tohaving an AVF placed and was dialyzed via acentral venous catheter. A year ago, however, anAVF was placed and he has been using this ac-cess successfully over the past 10 months. He was
one of several dialysis patients in his unit whoswitched from hemodialysis to hemodiafiltrationas part of a clinical trial 6 months ago. He startedweekly cognitive behavioral therapy for depression1 year ago. Last month’s laboratory studies showedhemoglobin 9.4 g/dl (decreased from 9.8 g/dl oneyear ago), calcium 9.2 mg/dl, phosphorus 4.6 mg/dl,and equilibrated Kt/V 1.4. His predialysis BP hasconsistently been ,140/90 mmHg. His KidneyDisease Quality of Life score last month was 6points higher than last year’s summary score.Which ONE of the following is the MOSTlikely factor influencing this patient’s im-proved quality of life score?
A. Hemoglobin 9.4 g/dlB. Predialysis BP ,140/90 mmHgC. Cognitive behavioral therapyD. Switch to hemodiafiltrationE. Functional AVF
10. A 75-year-old man has a history of ESRD due todiabetic nephropathy, and also has a history ofhypertension, chronic obstructive pulmonary dis-ease, and depression. He has been receiving in-center hemodialysis for 4 hours, thrice weekly forthe past 1 year using a 2 mEq/L potassium and2.5 mEq/L calcium dialysate. His medicationsinclude erythropoietin, bolus heparin during ev-ery hemodialysis treatment, paricalcitol, low-doseaspirin, lisinopril, furosemide, and escitalopram. Heoccasionally develops intradialytic hypotension andpalpitations and was recently found to have parox-ysmal atrial fibrillation.Which ONE of the following is true regardingthe use of anticoagulation in this patient?
A. Warfarin has been proven to reduce hisoverall mortality
B. His risk of hemorrhagic stroke is no higherthan matched individuals with normal kid-ney function
C. Warfarin use would be associated with greaterinternational normalized ratio variability
D. Warfarin is not indicated, because hisCHADS2 (Congestive Heart Failure, Age,Diabetes, and Prior Stroke 2) score is low
E. Target hemoglobin should be ,10 g/dlgiven his risk of stroke
11. A 58-year-old man is currently undergoing in-center hemodialysis three times weekly via a left
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 401
upper extremity AVF. He has been treated withhemodialysis for 8 years. His current dialysatehas a potassium concentration of 2.0 mEq/L anda calcium concentration of 2.0 mEq/L. He re-cently developed painful lesions over his prox-imal thighs that have now progressed to necroticulcers. Biopsy of one of the lesions revealed evi-dence of medial arteriolar calcification. On phys-ical examination, he is afebrile. Several 3- to5-cm necrotic ulcers are seen on the medial thighswith overlying eschar. There is no surroundingerythema or purulent drainage. Laboratory stud-ies show potassium 4 mEq/L, albumin 3.7 g/dl,calcium 9.5 mg/dl, phosphorus 7.2 mg/dl, PTH714 pg/ml, hemoglobin 10.4 g/dl, and 25-OH-vitamin D 8 ng/ml. Current medications includecalcium acetate 2001 mg with meals three timesdaily, aspirin, and atorvastatin. Aggressive woundcare is initiated and he is started on intravenoussodium thiosulfate.In addition to replacing calcium acetate withsevelamer, addition of which ONE of the fol-lowing medications is MOST likely to con-tribute to improving this patient’s skinlesions?
A. ParicalcitolB. WarfarinC. CinacalcetD. PrednisoneE. Intravenous vancomycin
12. Which ONE of the following is an advantage ofbuttonhole over rope-ladder needling of AVFs?
A. Decreased incidence of bacteremia and ab-scess formation
B. Decreased pain with cannulationC. Improved primary patency ratesD. Decreased rate of hematoma formation
13. A 62-year-old man with depression, hypertension,diabetes, and ESRD is evaluated for inadequatelycontrolled hypertension. He is currently receiv-ing dialysis three times per weekwith a prescribedtreatment time of 3.5 hours per treatment. Hisinterdialytic weight gains are 2–2.5 kg. Averagepredialysis and postdialysis BPs are 168/94 mmHgand 156/88 mmHg, respectively, with heart rate88/min. He rarely has intradialytic hypotension.Home medications include lisinopril 40 mg daily,amlodipine 10 mg daily, carvedilol 25 mg twice
daily, and aspirin. On physical examination, he has11 pedal edema. The remainder of the examina-tion is normal.In addition to dietary sodium restriction,which ONE of the following is the BESTstrategy to improve this patient’s BP control?
A. Gradually lower the dry weight after in-creasing dialysis to 4 hours
B. Add clonidine to his regimenC. Use blood volume monitoring to help
establish the dry weightD. Titrate the dry weight based on postdial-
ysis atrial natriuretic peptide levels
14. Which ONE of the following is correct re-garding use of biocompatible versus conven-tional PD solutions?
A. Residual renal function after initiation ofPD will decline faster with biocompatiblesolutions
B. Time to anuria is longer when using bio-compatible solutions
C. Biocompatible solutions are associated withhigher peritonitis rates
D. The use of biocompatible solutions willincrease membrane permeability over timeat a greater rate than conventional solution
15. A 78-year-old man is evaluated in follow-up forstage 5 CKD. He has a history of hypertensivenephrosclerosis, and he followed with you in theclinic for the last 15 years. His renal function isslowly declining, and the serum creatinine levelis 5.4 mg/dl (eGFR 9 ml/min per 1.73 m2) todayin the clinic. He generally feels well, has an ex-cellent appetite, and has not lost weight. He re-mains quite active and plays golf on a regularbasis. He attended pre-ESRD education severalyears ago and he opted for in-center hemodial-ysis because he lives alone. He prefers dialysisto conservative medical management. An AVFwas placed 3 years ago and is ready for use. Onphysical examination, he appears well. His BPis 135/80 mmHg. His lungs are clear, and thereis no edema. On neurologic examination, he isalert and oriented. There is no asterixis. Labo-ratory studies show potassium 4.2 mEq/L, totalCO2 23 mmol/L, calcium 9.2 mg/dl, phosphorus4.6 mg/dl, albumin 4.2 g/dl, and hemoglobin11.5 g/dl.
402 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
Which ONE of the following is the MOSTappropriate management?
A. The patient should be hospitalized now tostart hemodialysis
B. The patient should start hemodialysis nowin the outpatient center
C. The patient should start dialysis whenthere are increased signs or symptoms ofuremia
D. The patient should no longer be offered di-alysis given his advanced age
16. Which ONE of the following statements iscorrect regarding the modality of PD catheterplacement?
A. A PD catheter should always be placedwith the laparoscopic approach, utilizinga catheter with a coiled intraperitonealsegment
B. Surgically placed PD catheters have a sig-nificantly greater 1-year survival than docatheters placed under fluoroscopic guidance
C. Radiologically placed PD catheters are asafe and viable alternative to surgically placedcatheters
D. Omental folding during PD catheter place-ment does not prevent catheter tip migration
17. A 52-year-old man with type 2 diabetes mellitusand hyperlipidemia on chronic hemodialysis forthe last 5 years is evaluated because of a mountingurge to move his legs while at rest. His symptomsbegan about 6 months ago and have been ac-companied by marked bilateral leg paresthesias.His symptoms are most prominent at night, makingit difficult for him to sleep, and are partially re-lieved by walking. He denies weakness or myalgias.He recently has become anxious over his continuedinability to sleep. Current medications include insulinglargine, atorvastatin and sevelamer with meals.On physical examination, there is a decreased lighttouch and vibratory sensation up to the level ofthe knees. The remainder of the examination isunremarkable. Laboratory studies show equilibratedKt/Vurea levels consistently.1.3 over the past year,hemoglobin 10.2 g/dl, transferrin saturation 32%,serum ferritin 250 ng/ml, and creatine kinase 200mg/dl (reference range, 30–170). Serum vitaminB12, serum protein electrophoresis, and thyroidstimulating hormone are normal.
Which ONE of the following is the MOSTappropriate management strategy for thispatient?
A. Intravenous ironB. RopiniroleC. GabapentinD. Intradialytic exerciseE. Discontinue atorvastatin
18. A 34-year-old man with ESRD secondary to con-genital dysplasia received a deceased donor kidneytransplant 12 years ago. His maintenance immu-nosuppression consists of tacrolimus, mycophenolate,and prednisone. Allograft biopsy 1 year ago showedextensive tubular atrophy and interstitial fibrosis.His eGFR is 11 ml/min per 1.73 m2, but has re-mained in this range over the past 8 months. He isasymptomatic, works full time, and remains active,exercising on a daily basis. His AVF in the leftupper arm is still patent from before his transplant.On physical examination, the BP is 130/80 mmHg.His lungs are clear, and there is trace pedal edema.Laboratory studies show hemoglobin 9.6 g/dl, po-tassium 4.8 mEq/L, total CO2 21 mmol/L, BUN65 mg/dl, and creatinine 6.8 mg/dl.Which ONE of the following is MOSTappropriate for this patient?
A. Initiate hemodialysis, continue the currentimmunosuppressive drugs, and refer fora second transplant
B. Initiate hemodialysis and refer for allograftnephrectomy
C. Initiate hemodialysis, discontinue tacrolimusand mycophenolate, and refer for a secondtransplant
D. Refer for evaluation for retransplantationand continue to monitor for signs and symp-toms of uremia
19. A 55-year-old woman with history of ESRD sec-ondary to hypertension is currently undergoinghemodialysis thrice weekly for the last 2 years.She had a myocardial infarction 1 year ago re-quiring coronary revascularization. Her medica-tions include sevelamer 1600 mg with meals andparicalcitol 8 mg intravenously with each hemo-dialysis session. Laboratory studies show calciumof 9.8 mg/dl, phosphorus of 6.3 mg/dl, albumin of4 g/dl, and an intact PTH level of 690 pg/ml, allincreased from 1 month ago. You decide to start
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 403
the patient on cinacalcet 30 mg daily. Beforestarting this medication, she asks you to explainthe potential benefits of this medication.Which ONE of the following should you tellthis patient regarding cinacalcet therapy?
A. Cinacalcet has been shown to reduce frac-ture risk
B. Cinacalcet has been shown to decrease therate of parathyroidectomy bymore than half
C. Cinacalcet has been shown to improvemortality
D. Cinacalcet has been shown to decrease cardio-vascular risk
20. A 52-year-old woman with history of type 2diabetes mellitus complicated by stage 5 CKDwas started on hemodialysis 3 months ago. She isreceiving 4-hour treatments three times weeklyvia left upper extremity AVF. She has no priorhistory of heart disease. She is achieving theprescribed dry weight, with no documented epi-sodes of intradialytic hypotension. Her primarycare physician started her on atorvastatin 10 mgdaily based on her cardiovascular risk score. Lab-oratory studies before statin therapy revealed anLDL cholesterol of 130 mg/dl and triglycerides140 mg/dl. A month after initiation of atorvastatin,her LDL cholesterol is 65 mg/dl.Which ONE of the followingMOST accuratelydescribes the effect of continued use ofatorvastatin?
A. A decreased risk of death from cardiac causesB. A decreased risk of sudden cardiac deathC. An increased risk of rhabdomyolysis com-
pared with the general populationD. A persistently high cardiovascular risk de-
spite improvement in LDL cholesterol
21. A 56-year-old African-American woman with ahistory of type 2 diabetes mellitus and ESRD isevaluated during weekly hemodialysis rounds. Herinterdialytic weight gains average 2.2 kg and shehas minimal residual kidney function. She toleratesultrafiltration to the prescribed dry weight withonly occasional fatigue for several hours after dial-ysis. Over the last six treatments, you have receivedcalls from the hemodialysis unit concerning persistentelevations in BP during dialysis treatments. Today, herpredialysis BP is 142/76 mmHg and increases to188/100 mmHg during dialysis. HomeBP readings
average 140–150/80–90 mmHg. Her antihyperten-sive medications are amlodipine 5 mg daily andlisinopril 40 mg daily. On physical examination, thelungs are clear and there is no peripheral edema.Which ONE of the following is the MOSTappropriate next step in management?
A. Increase amlodipineB. Decrease the estimated dry weightC. Add carvedilolD. Increase the dialysate sodium gradient
22. A 60-year-old woman with ESRD treated with in-center hemodialysis is seen during her monthlycomprehensive care visit. She feels generally welland offers no complaints. Laboratory studies showsingle-pool Kt/V 1.65, hemoglobin 11.2 g/dl, PTH432 pg/ml, calcium 8.9 mg/dl, albumin 3.6 g/dl,phosphorus 4.2 mg/dl, and potassium 4 mEq/L.Current medications include calcium acetate 667mgthree times daily, amlodipine 5mg daily, and aspirin81 mg daily. You consider oral supplementationof protein (1 can/d of a liquid protein supplementcontaining 13 g of protein) to improve the serumalbumin in this patient.Which ONE of the following statements re-garding oral protein supplementation in thiscontext is correct?
A. It is a reliable strategy to increase thispatient’s serum albumin level
B. It will improve quality of life as indicatedby an increased score on the Kidney Dis-ease Quality Of Life short form
C. It will reduce this patient’s hospitalizationrate over the next year
D. It usually raises the serum phosphorus leveland will not provide this patient any mean-ingful benefit
23. A 41-year-old man with ESRD secondary to di-abetic nephropathy asks about switching fromthrice-weekly hemodialysis to more frequent he-modialysis six times per week in an effort to im-prove his outcomes.Which ONE of the following should you tellthis patient regarding the effect of more fre-quent hemodialysis on cardiovascular healthand mortality?
A. It will result in more favorable left ven-tricular remodeling
B. It will improve his cardiovascular mortality
404 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014
C. It will reduce the mortality risk associatedwith the 72-hour interdialytic period
D. It will not decrease cardiovascular risk be-cause of QT prolongation
24. A 45-year-old man with ESRD secondary to hy-pertensive nephrosclerosis is undergoing thrice-weekly in-center hemodialysis. He is concernedabout recent trends in his laboratory studies andinquires about daily nocturnal hemodialysis. Hislaboratory parameters are currently as follows:hemoglobin 11.5 g/dl, serum albumin 3.4 g/dl,PTH 523 pg/ml, and serum phosphorus 6.4 mg/dl.His medications include calcium acetate 667 mgwith meals, as well as doxercalciferol 2 mg in-travenously and erythropoietin 2200 units intra-venously with each dialysis treatment.Which ONE of the following should you tellthis patient regarding the effect of daily noc-turnal hemodialysis on serum albumin, phos-phorus, and PTH levels?
A. He can expect no change in the serumphosphate and albumin
B. His serum phosphate and PTHwill decrease,and his serum albumin will increase
C. His serum phosphate will decrease with nochange in serum albumin and PTH
D. His serum phosphate and serum albuminwill decrease
E. His serum albumin will increase and therewill be no change in serum phosphate
25. A 54-year-old man with ischemic cardiomyopa-thy, depression, and ESRD currently undergoingthrice-weekly in-center hemodialysis plans to switchto short daily in-center hemodialysis in the near fu-ture. Successful ultrafiltration has been challengingbecause his BP is chronically low during dialysis.He understands that short daily hemodialysis mayimprove his tolerance of ultrafiltration, but also asksyou to explain other potential benefits and risks ofthis modality.Which ONE of the following should you tellthis patient regarding other potential effects ofshort daily in-center hemodialysis?
A. It may improve physical performanceB. It may improve depressive symptomsC. It may increase the rate of vascular access
complicationsD. It will reduce his erythropoietin requirement
26. You are medical director for an outpatient di-alysis clinic, and your nurse manager asks you toaddress a positive tuberculin skin test on a hospi-talized patient who has started hemodialysis andhas been referred to your center. He is a 68-year-old man with ESRD due to diabetic kidney dis-ease. Detailed chart review reveals that he receivedintravesical Bacillus Calmette–Guérin as a com-ponent of therapy for stage T1 bladder cancer.He does not have fever, cough, night sweats, orknown household tuberculosis contacts. His chestradiograph is normal.Which ONE of the following is the MOSTappropriate action?
A. No further actions are requiredB. Treat with isoniazid for 9 monthsC. Order an IFN-g release assayD. Request sputum for three acid-fast bacilli
smears
27. Which ONE of the following statements re-garding fibroblast growth factor-23 (FGF23)is correct?
A. FGF23 acts in the ascending limb of theloop of Henle
B. FGF23 increases reabsorption of phosphatein the nephron
C. Circulating serum concentrations of FGF23are reduced in patients with CKD
D. Serum concentrations of FGF23 are inverselycorrelated with mortality in patients withESRD
E. FGF23 reduces circulating concentrationsof calcitriol
28. A 55-year-old man has ESRD from hypertensivenephrosclerosis, and has been receiving in-centerhemodialysis thrice weekly for 5 years. He hasa past medical history of polysubstance abuse,coronary artery disease, prior myocardial infarc-tion, hepatitis C, and poor medical compliance.He dialyzes with a native AVF. He is treated withamlodipine 10 mg once a day, ramipril 5 mg oncea day, carvedilol 25 mg twice a day, minoxidil5 mg once a day, a renal multivitamin once a day,calcium acetate 2001 mg with meals, cinacalcet60 mg once a day, ribavirin 400 mg twice a day,and simvastatin 40mg once a day.With his dialysishe receives doxercalciferol 6 mg intravenously anderythropoietin 22,000 units with each treatment. He
Nephrology Self-Assessment Program - Vol 13, No 5, November 2014 405
also receives intravenous ferric gluconate 62.5 mgonce per week. When you review his laboratoryresults you note a hemoglobin 7.8 g/dl, calcium8.4 mg/dl, phosphorus 5.8 mg/dl, PTH 645 pg/ml,ferritin 556mg/dl, and albumin 3.9 g/dl. His single-pool Kt/V was 1.42. Review of the laboratoryresults from the past 3 months reveals that his he-moglobin values have reduced from his baselinevalues of 10.5–10.8 g/dl despite a progressive in-crease in his erythropoietin dose.Which ONE of the following is the BEST op-tion to address his anemia?
A. Discontinue ribavirinB. Administer intravenous ferric gluconate
load of 625 mg divided over the next 10hemodialysis treatments
C. Administer erythropoietin by subcutaneousinjection instead of intravenously
D. Refer him for parathyroidectomyE. Increase his dialysis frequency to five to six
times per week
29. You serve as a member of a patient safety orga-nization and are asked to review a case of suddendeath in a previously stable ESRD patient. Thepatient was a 56-year-old man with a history ofhypertension and FSGS maintained on hemodi-alysis via an arteriovenous graft. The patient livedalone and had been feeling well, but failed toshow for his regularly scheduled dialysis on aWednesday. A family member was contacted anddiscovered that the patient had died at home inbed with no signs of trauma or hemorrhage. Hereceived 4 hours of dialysis three times per weekwith an average blood flow of 480 ml/min anddialysate flow of 800 ml/min. The dialysate hada sodium concentration of 137 mEq/L, potassium1.5 mEq/L, and bicarbonate 33 mEq/L (yieldinga final buffer concentration of 37 mEq/L), andcalcium of 2.5 mEq/L. Review of his dialysis flow
sheets revealed average interdialytic weight gains of1.5 kg, postdialysis weights averaging 62 kg, andaverage postdialysis BPs of 137/78 mmHg. Hismost recent monthly laboratory studies showedsingle-pool Kt/V of 1.6, potassium 5.1 mEq/L, totalCO2 22 mmol/L, calcium 9.2 mg/dl, phosphorus5.2 mg/dl, and albumin 3.7 mg/dl. Medicationsincluded lisinopril, metoprolol, and aspirin.Which ONE of the following factors in thiscase has been shown to be associated withsudden cardiac death?
A. The predialysis serum potassium of 5.1mEq/L
B. Occurrence of his death on a WednesdayC. Metoprolol therapyD. A dialysate potassium of 1.5 mEq/LE. His ultrafiltration volume
30. You are a medical director for an outpatienthemodialysis clinic, and you are reviewing dataduring the monthly quality improvement meet-ing. You note that over the past 6 months, themean interdialytic weight gain increased from2.2 kg to 2.8 kg for the patients receiving thrice-weekly treatments. You are concerned that thistrend might soon result in an increase in the hos-pitalization rate due to recurrent volume overloadin your patients.In addition to measures to reduce dietary so-dium intake, which ONE of the following in-terventions is MOST likely to result ina reduction in interdialytic weight gains inyour patient population?
A. Chairside cognitive behavioral therapyB. An increase in the dialysate sodium from
140 to 145 mEq/LC. An increase in the dialysate bicarbonate
from 30 to 34 mEq/LD. A reduction in the dialysate temperature to
35.5�C
406 Nephrology Self-Assessment Program - Vol 13, No 5, November 2014