Embed Size (px)
DESCRIPTION
Nephropathy and Diabetes. Alasdair Mackie Consultant Physician Northern General Hospital. Topics to be covered. Metformin use in renal impairment Microalbuminuria The importance of the CKD classification in Diabetes and Renal Disease. Prevalence of nephropathy in Diabetes Mellitus. - PowerPoint PPT Presentation
Citation preview

Nephropathy and DiabetesNephropathy and Diabetes
Alasdair MackieAlasdair Mackie
Consultant PhysicianConsultant Physician
Northern General HospitalNorthern General Hospital

Topics to be coveredTopics to be covered
Metformin use in renal impairmentMetformin use in renal impairment
Microalbuminuria Microalbuminuria
The importance of the CKD classification The importance of the CKD classification in Diabetes and Renal Diseasein Diabetes and Renal Disease

Prevalence of nephropathy in Prevalence of nephropathy in Diabetes MellitusDiabetes Mellitus
Type 1Type 1 Type 2Type 2
PrevalencePrevalence– Micro-alb (%) Micro-alb (%) 16 (9-21)16 (9-21) 38 (15-60)38 (15-60)– Overt proteinuria (%)Overt proteinuria (%) 15 (18-22)15 (18-22) 15 (5-48)15 (5-48)– At diagnosis (%)At diagnosis (%) zerozero 9 (5-20)9 (5-20)
Annual incidenceAnnual incidence– Overt proteinuria (%)Overt proteinuria (%) 1.2 (0 – 3)1.2 (0 – 3) 1.5 (1 – 2)1.5 (1 – 2)
25 yr incidence (%)25 yr incidence (%) 25 (18-34)25 (18-34) 28(25-47)28(25-47)

Case study 1Case study 1
A 62 year-old lady with Type 2 DM for 12 years. Well controlled HbA1c of 7.2% on a combination of Gliclazide 80 mg bd and Metformin 1g bd.
Also suffers from Hypertension, IHD and ‘empty sella’ syndrome. On Ramipril 10 mg, Bendro-fluomethazide 2.5 mg and Thyroxine 50 μg per day.
Renal function has been gradually deteriorating over two years with serum creatinine now 142 μmol/L. eGFR 48.
You stop her Metformin and her HbA1c rises to 10.3% over the next six months.
What would you do now?When should we withdraw Metformin?

When would you stop Metformin?When would you stop Metformin?
Serum CreatinineSerum Creatinine– 100 100 μμmol/Lmol/L
– 130130
– 150150
– 180180
– 200200
eGFReGFR– Proteinuria and >60Proteinuria and >60
– 45 to 6045 to 60
– 30 to 4530 to 45
– 15 to 3015 to 30
– 15 or less15 or less

Current Clinical PracticeCurrent Clinical Practice
Serum CreatinineSerum Creatinine– Around 130 to 150 Around 130 to 150 μμmol/Lmol/L
eGFReGFR– Around 45 to 60 ml/minAround 45 to 60 ml/min

RememberRemember
An 80 year old lady with a SCr of 100 has An 80 year old lady with a SCr of 100 has an eGFR of 30an eGFR of 30
Whereas aWhereas aA 50 year old man with a SCr of 200 has an A 50 year old man with a SCr of 200 has an eGFR of 45eGFR of 45

ManufacturersManufacturers GDAGDA BNFBNF NICENICE Howlett and Howlett and Bailey Bailey
[NEJM 1999][NEJM 1999]
Renal Renal FunctionFunction
CrCl <60CrCl <60 SCr >107SCr >107 SCr >133SCr >133 SCr >133SCr >133 CrCl <90CrCl <90
Heart Heart FailureFailure
√√ √√ √√ nsns √√
Tissue Tissue HypoxiaHypoxia
√√ √√ √√ nsns √√
Alcohol Alcohol misusemisuse
√√ √√ nsns nsns √√
SevereSevere
liver liver disordersdisorders
√√ √√ √√ nsns √√
Contra-indications to Metformin?

MALA: the evidenceMALA: the evidence
Most studies demonstrate no link between Most studies demonstrate no link between Metformin and Lactate levelsMetformin and Lactate levels– Freemantle Study exception 1.86 v 1.58 mmol/LFreemantle Study exception 1.86 v 1.58 mmol/L
Case reports almost always where renal function Case reports almost always where renal function severely deranged for other cause[s]severely deranged for other cause[s]DARTS-MEMO study: 1 case in 1847 patientsDARTS-MEMO study: 1 case in 1847 patientsSwedish study 1977 to 1991: 2.4 cases of lactic Swedish study 1977 to 1991: 2.4 cases of lactic acidosis per 100 000 patient yearsacidosis per 100 000 patient yearsCochrane database no cases with ~40 000 patient-Cochrane database no cases with ~40 000 patient-years exposure to Metformin.years exposure to Metformin.

Lothian Study of Metformin and eGFRLothian Study of Metformin and eGFR
Diabetes data-base holds 27 259 [3.5%] patientsDiabetes data-base holds 27 259 [3.5%] patients
19 924 Type 2 with a valid SCr measurement 19 924 Type 2 with a valid SCr measurement
11 297 currently taking Metformin11 297 currently taking Metformin
2880 [25.5%] are CKD 3 [GFR <60] or worse2880 [25.5%] are CKD 3 [GFR <60] or worse
No patients taking Metformin with CKD 4 or 5No patients taking Metformin with CKD 4 or 5
Warren et al Diab Med [2007]

Lothian studyLothian study
Local practice is to withdraw Metformin when SCr > 150Local practice is to withdraw Metformin when SCr > 150
If eGFR threshold set at…..If eGFR threshold set at…..
≥≥36 would ‘allow’ similar number to remain on Metformin 36 would ‘allow’ similar number to remain on Metformin and would permit use in SCr up to 180and would permit use in SCr up to 180– 263 [1.3%] with SCr <150 removed263 [1.3%] with SCr <150 removed
– 241 with SCr >150 become eligible241 with SCr >150 become eligible
4040– then 560 [~3%] would have to stop treatment with Metforminthen 560 [~3%] would have to stop treatment with Metformin
– And 102 [0.5%] could startAnd 102 [0.5%] could start
All the newly ineligible individuals female.All the newly ineligible individuals female.
Warren et al Diab Med [2007]

What should we do?What should we do?
Database of all patients on MetforminDatabase of all patients on MetforminAnnual test of SCr [and eGFR]Annual test of SCr [and eGFR]Continue metformin where Continue metformin where ≥ 60 ml/min≥ 60 ml/minStop its use when eGFR ≤ 30 ml/minStop its use when eGFR ≤ 30 ml/minReview cases where eGFR 30 to 60?Review cases where eGFR 30 to 60?– Rate of declineRate of decline– Other co-morbiditiesOther co-morbidities– More frequent monitoringMore frequent monitoring
Consider re-starting where eGFR improves from Consider re-starting where eGFR improves from CKD 4CKD 4

If you were 55….If you were 55….
And developed Type 2 Diabetes Mellitus. Fasting BS 7.6; HbA1c 8.3%.Your blood pressure was measured at 168/84, urinalysis trace protein and SCr 94 [eGFR 75]. Your serum cholesterol is 5.8 mmol/L and LDL 3.2. At Eye Screening visual acuities were 6/6 and 6/9 {R and L}. Fundoscopy – N.
Would you screen your urine for albumin and if so how?What would you do with the result?Under what circumstances would you investigate for Non-diabetic Renal Disease?If you were found to have micro-albumin how tightly would you control
(a) Blood sugar?(b) Blood pressure?(c) And with what agent?(d) Cholesterol?(e) What additional advice would you offer?

How do we measure microalbuminuria?How do we measure microalbuminuria?
‘‘albustix’ - albustix’ - – exclude proteinuric subjectsexclude proteinuric subjects– trace/intermittent positivetrace/intermittent positive
Micral-test stripMicral-test strip
Albumin creatinine ratio: [Albumin creatinine ratio: [first morning or randomfirst morning or random]]
Albumin excretion rateAlbumin excretion rate– timed overnight collectiontimed overnight collection– 24-hour urine24-hour urine– timed ambulant collectiontimed ambulant collection– measured after water loadmeasured after water load[Definition: 20 to 200[Definition: 20 to 200g/min in 2 of 3 timed collections (~8 hours) over 3 months]g/min in 2 of 3 timed collections (~8 hours) over 3 months]

Who should be screened?Who should be screened?
Exclude subjects with proteinuriaExclude subjects with proteinuria
Type IType I– DM developed pre-pubertally - from pubertyDM developed pre-pubertally - from puberty– DM developed after puberty - 5 years onwardsDM developed after puberty - 5 years onwards
Type IIType II– from diagnosis – NICE recommends but ?from diagnosis – NICE recommends but ?
Annual testing?Annual testing?

What are the difficulties?What are the difficulties?
Which sample?Which sample?– Random sampleRandom sample– First morning First morning
How many in what timescale?How many in what timescale?How do we manage the borderline samples?How do we manage the borderline samples?Could it be a false positiveCould it be a false positive– Intercurrent illnessIntercurrent illness– Metabolic decompensationMetabolic decompensation
Should we undertake timed collections?Should we undertake timed collections?If so in whom should we undertake?If so in whom should we undertake?

Screening for Micro-albuminuria
ACR Proteinuria protocol
2+ ACR > 2.5(m) or 3.5(f)
2+ samples < 20 mg/mmol
Retest in one year
Incipient diabetic nephropathy
Determine AER (? No. tests)
> 20-200g/min + No NDRD
Pre-test for protein
+ve-ve
-ve2 more ACR
+ve

Factors interfering with microalbumin Factors interfering with microalbumin screeningscreening
IncreaseIncrease DecreaseDecrease
Poor glycaemic controlPoor glycaemic control ACE inhibitorsACE inhibitors
FeverFever NSAIDsNSAIDs
CCFCCF MalnutritionMalnutrition
UTIUTI
ExerciseExercise
HaematuriaHaematuria

Classification of albumin excretionClassification of albumin excretion
NormoalbuminNormoalbumin MicroalbuminMicroalbumin MacroalbuminMacroalbumin
AER (mg/24 hr)AER (mg/24 hr) <30<30 30 - 30030 - 300 >300>300
AER (AER (μμg/ming/min)) <20<20 20 - 20020 - 200 >200>200
ACR (mg/mmol)ACR (mg/mmol)
MalesMales <2.5<2.5 2.5 - 252.5 - 25 >25>25
FemalesFemales <3.5<3.5 3.5 - 353.5 - 35 >35>35

To screen or not to screen?To screen or not to screen?
Should lead to or be:Should lead to or be:
Identification of a high or higher risk groupIdentification of a high or higher risk group
Predictable prognosis for selected subjectsPredictable prognosis for selected subjects
Intervention improves outcomeIntervention improves outcome
Reliable, accurate and valid measureReliable, accurate and valid measure
Cost effectiveCost effective

“To justify screening for microalbuminuria, there should be evidence that identifying patients withmicroalbuminuria provides a benefit in terms ofan enhanced response to therapeutic interventionsof improved glycaemic and BP control whencompared with treating the population of peoplewith diabetes as a whole, particularly those whoseurine albumin excretion is normal”
Newman et al [2005] Health Technology Assessment

Why do we measure Microalbumin?Why do we measure Microalbumin?
NICE recommendationsNICE recommendations
Diabetes GuidelinesDiabetes Guidelines
We get paid to do so or not….We get paid to do so or not….
Identifies a high risk clinical group e.g.Identifies a high risk clinical group e.g.– Proliferative retinopathyProliferative retinopathy– Progression to Renal diseaseProgression to Renal disease– Vascular disease in Type 2 DiabetesVascular disease in Type 2 Diabetes
Other reason[s]Other reason[s]

Microalbumin screeningMicroalbumin screening
Relationship of micro-albuminuria to outcomeRelationship of micro-albuminuria to outcome– all cause mortality/CVS mortality and CVS events [Type 1 &2] all cause mortality/CVS mortality and CVS events [Type 1 &2] – development of proliferative retinopathy [Type 1]development of proliferative retinopathy [Type 1]– development of proteinuria and ESRD [Type 1 & 2]development of proteinuria and ESRD [Type 1 & 2]
Significant changes in microalbumin statusSignificant changes in microalbumin status– Significant numbers of patients regressSignificant numbers of patients regress
Impact of interventionImpact of intervention– Glycaemic controlGlycaemic control
Type 1Type 1 :No evidence of benefit of improved glycaemic control :No evidence of benefit of improved glycaemic controlType 2Type 2 :Limited evidence in slowing decline of GFR and progression to :Limited evidence in slowing decline of GFR and progression to proteinuriaproteinuria
– Blood pressureBlood pressurePositive benefit in delaying progression to clinical proteinuriaPositive benefit in delaying progression to clinical proteinuriaNo consistent treatment effect of ACEi in slowing decline of GFR No consistent treatment effect of ACEi in slowing decline of GFR

Areas of uncertaintyAreas of uncertainty
What is the benefit of screening and treatment What is the benefit of screening and treatment for those individuals who are normotensive?for those individuals who are normotensive?
What is the value of identifying those who What is the value of identifying those who remain ma +ve despite achieving target BP?remain ma +ve despite achieving target BP?
Does regression of microalbuminuria reduce Does regression of microalbuminuria reduce the risk? the risk?

Algorithm for management of renal diseasein Type II Diabetes Mellitus
Measure urine ACR or [Alb] and Serum creatinine
Is micro-albuminuria or proteinuria present?
> 150mol/l
Yes
No
Yes A1c < 7%BP < 140/80
Higher risk: ACE InhibitorA1c < 6.5 - 7.5%BP < 135/75
Each visit: urine albumin & SCrAggressive cardiovascular RF Rx
Refer
Nice 2002

Why should we not screen for Why should we not screen for microalbuminuria?microalbuminuria?
Many subjects with do not show progressionMany subjects with do not show progression– MicroalbuminuriaMicroalbuminuria
AdultsAdults– RegressionRegression 26%26%– ProgressionProgression 19%19%
AdolescentsAdolescents– RegressionRegression 44%44%– ProgressionProgression 15%15%
– MacroalbuminuriaMacroalbuminuria Regression occurs but lower ratesRegression occurs but lower rates
What is the added benefit of identifying and treating What is the added benefit of identifying and treating those with micro- as oppose to normo-alb?those with micro- as oppose to normo-alb?Risk of under treating those without micro-albRisk of under treating those without micro-alb
Health Technology Assessment - Newman et al. [2005]

A word about PCRA word about PCR
Protein:creatinine ratioProtein:creatinine ratio
Units:Units: mg protein/mmol creatinine mg protein/mmol creatinine
Measured by Clinical ChemistryMeasured by Clinical Chemistry
Measure where ‘dipstix’ positiveMeasure where ‘dipstix’ positive
Random urine – universal containerRandom urine – universal container
What does it mean?What does it mean?– PCR of 100 equivalent to 1g in 24 hoursPCR of 100 equivalent to 1g in 24 hours
– PCR of 50 equivalent to 500mgs in 24 hoursPCR of 50 equivalent to 500mgs in 24 hours
– PCR of >30 approximates to macroalbuminuriaPCR of >30 approximates to macroalbuminuria

Consider Non-Diabetic Renal DiseaseConsider Non-Diabetic Renal Disease
In the absence of Diabetic RetinopathyIn the absence of Diabetic RetinopathyAdvanced renal impairment with low AERAdvanced renal impairment with low AERRapid decline of eGFRRapid decline of eGFRRapid rise in protein excretion or Nephrotic SyndromeRapid rise in protein excretion or Nephrotic SyndromeActive urine sedimentActive urine sediment– VasculitidesVasculitides
Refractory hypertensionRefractory hypertensionSymptoms +/or signs of other systemic diseaseSymptoms +/or signs of other systemic disease– Myeloma/amyloidosisMyeloma/amyloidosis– SLESLE– VasculitidesVasculitides
Marked [>30%] reduction of GFR with introduction of Marked [>30%] reduction of GFR with introduction of ACEi or ARBACEi or ARB

Diabetes and eGFRDiabetes and eGFR
Case Case
ClassificationClassification
CaveatsCaveats
What does it mean for patients?What does it mean for patients?
How to deal with in practiceHow to deal with in practice

Case scenario 3Case scenario 3
An 78 year old lady attends your diabetes clinic. Shehas had Type 2 diabetes for 4 years and is on Gliclazide160 mg bd and Pioglitazone 15 mg. She takes Ramipril5 mg and Amlodipine 10 mg to control her BP, together with simvastatin 20 mg and aspirin 75 mg. Her HbA1c is 8.2% and eGFR 42 ml/min. BP 154/76.
1. What is her CKD status?2. What do you think about her renal function?3. Are there any other tests you may wish to do?4. What, if any, alteration[s] would you make to her treatment?5. What else might you wish to do?

Classification of eGFRClassification of eGFR
CKD 1*CKD 1*normalnormal >90 ml/min>90 ml/min
CKD 2*CKD 2*mildmild 60-9060-90
CKD 3CKD 3 moderatemoderate 30-5930-59
CKD 4CKD 4 severesevere 15-2915-29
CKD 5CKD 5 end-stage or RRTend-stage or RRT <15<15
* Must have other evidence or renal disease, e.g * Must have other evidence or renal disease, e.g proteinuria – haematuria - structural changes proteinuria – haematuria - structural changes

Recent sub-classificationRecent sub-classification
CKD CKD 3a3a eGFR of 45-59eGFR of 45-59
CKDCKD 3b3b eGFR of 30-44eGFR of 30-44
suffixed with p = associated with PCR >100suffixed with p = associated with PCR >100
e.g. e.g. CKD 2pCKD 2p means an eGFR of 60 to 89 with means an eGFR of 60 to 89 with proteinuria [PCR >100]proteinuria [PCR >100]

How do we estimate GFR?How do we estimate GFR?
MModification of odification of DDiet in iet in RRenal enal DDisease [MDRD] Formula:isease [MDRD] Formula:
GFR{ml/min/1.73mGFR{ml/min/1.73m22} = 175 x {} = 175 x {SCrSCr/88.4}/88.4}-1.154-1.154 x x
{{ageage}}-0.203-0.203 x {0.742 if x {0.742 if femalefemale} x {1.210 if } x {1.210 if AfroCaribbeanAfroCaribbean}}

CaveatsCaveatsLess accurate at higher eGFRLess accurate at higher eGFRUnrepresentative in Acute Renal FailureUnrepresentative in Acute Renal FailureLess accurate in those with muscle wastingLess accurate in those with muscle wastingNot validated in certain groupsNot validated in certain groups– childrenchildren– old ageold age– pregnancypregnancy– certain racial groupscertain racial groups
Requires ‘serial’ measurements at least > 3 months Requires ‘serial’ measurements at least > 3 months to determine classificationto determine classification
Don’t forget the clock starts ticking at 40 – GFR declines 1 ml/min/annum

What does it mean for patients?What does it mean for patients?
I have another ‘disease’I have another ‘disease’Increased risk of death and/or cardio-Increased risk of death and/or cardio-vascular diseasevascular diseaseAggressive risk factor managementAggressive risk factor managementMore frequent attendance and monitoringMore frequent attendance and monitoringReferral to hospitalReferral to hospitalReview of medication – MetforminReview of medication – MetforminIntroduction of insulin Introduction of insulin

Clinical implicationsClinical implications
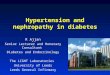
Risk of Cardiovascular Death in 30000 Risk of Cardiovascular Death in 30000 individuals followed up for 5 yearsindividuals followed up for 5 years
CKD 3CKD 3 19.5%19.5% 2-3-fold 2-3-fold ↑ ↑ riskrisk
CKD 4CKD 4 24.3%24.3%
CKD 5CKD 5 45.7%45.7%Keith et al [2004] Arch Int Med

Cardiovascular Event RateCardiovascular Event Rate
0
5
10
15
20
25
30
35
40
>60 45-59 30-44 15-29 <15
Age
-sta
ndar
dise
d ra
te o
f ca
rdio
vasc
ular
even
ts p
er 1
00-p
erso
n ye
ars
CKD Stage 3a 3b 4 5Go et al 2005
GFR ml/min/1.73m2

Address cardiovascular risk to stop them Address cardiovascular risk to stop them dyingdying
Lifestyle , Diabetes, Hypertension, ACE inhibitors, LipidsLifestyle , Diabetes, Hypertension, ACE inhibitors, Lipids
Slow progression of renal disease to delay Slow progression of renal disease to delay the need for dialysisthe need for dialysis
Lifestyle , Diabetes, Hypertension, ACE inhibitors, Lipids Lifestyle , Diabetes, Hypertension, ACE inhibitors, Lipids (specific treatments)(specific treatments)
Avoid harm and be prepared!Avoid harm and be prepared! Medicine managementMedicine management Ensure timely referral and access to pre-dialysis careEnsure timely referral and access to pre-dialysis care
What is the point of knowing about patients with CKD?

ConclusionsConclusions
Be aware of eGFR in patients on MetforminBe aware of eGFR in patients on MetforminStop Metformin when eGFR <30Stop Metformin when eGFR <30Be alert to DM patients [usually Type 2] who may Be alert to DM patients [usually Type 2] who may have non-diabetic renal diseasehave non-diabetic renal diseaseAlways check urine for proteinAlways check urine for proteinConsider the pros and cons of microalbumin testingConsider the pros and cons of microalbumin testingKnow the eGFR of your DM patients and whether Know the eGFR of your DM patients and whether decliningdecliningBe aware of the guidelines for referral to the Renal Be aware of the guidelines for referral to the Renal Unit of your local hospitalUnit of your local hospital

Crude option appraisal: Crude option appraisal: Microalbumin screening in Type 2 DMMicroalbumin screening in Type 2 DMOption 1Option 1
Treat all with ACEi and no screeningTreat all with ACEi and no screeningCost: £6629 per life year gainedCost: £6629 per life year gained
Option 2Option 2Screen all patients for microalbuminuriaScreen all patients for microalbuminuriaTreat only those who are positive with ACEiTreat only those who are positive with ACEiCost: £15157 per life year gainedCost: £15157 per life year gained
Option 3Option 3Screen all not on BP therapy Screen all not on BP therapy Treat positives with ACEiTreat positives with ACEiCost: £5745 per life year gainedCost: £5745 per life year gained

Supplementary CaseSupplementary Case
ZO is 16. She has had Diabetes for 4 years and until recently has hadgood glycaemic control with HbA1c usually <8%. Over the last 12 to 18months control has been less good with HbA1c of 12 to 14.5%. She has had intermittent protein excretion. A recent random PCR was 131.2 with two subsequent first morning levels >100. Her BP is 92/54.
1. What further information would you like to know?2. What further assessment[s] would you make?3. How should she be managed?4. What guidance would you offer her in relation to managing her diabetes and protein excretion?