Embed Size (px)
Citation preview

Kidney International, Vol. 59 (2001), pp. 230–237
Nephron pO2 and renal oxygen usage in thehypertensive rat kidney
WILLIAM J. WELCH, HORST BAUMGARTL, DIETRICH LUBBERS, and CHRISTOPHER S. WILCOX
Division of Nephrology and Hypertension, Georgetown University Medical Center, Washington D.C., USA,and Max Planck Institute for Molecular Physiology, Dortmund, Germany
Nephron pO2 and renal oxygen usage in the hypertensive rat tubular transport of sodium (TNa) [1–5]. However, thekidney. renal venous pO2 is remarkably high, leading to a small
Background. The kidney has a high rate of oxygen usageand relatively constant arteriovenous gradient for oxy-(QO2) that is closely dependent on tubular Na1 transport (TNa).gen [(A-V)O2] across the kidney [6]. This has been attrib-However, little is known concerning the regulation of the corti-
cal partial pressure of oxygen (pO2). uted to the high rate of blood flow (RBF) that is dictatedMethods. First, the pO2 was measured in the outer cortical by the need to form the substantial glomerular filtrate
proximal (PT) and distal tubules (DT), efferent arterioles[5]. However, despite this very high rate of renal O2(EA), and superficial (SC) and deep cortical (DC) tissues indelivery and low (A-V)O2 gradient across the kidney,normotensive Wistar Kyoto (WKY) and spontaneously hyper-
tensive rats (SHRs) using an ultramicrocoaxial O2 electrode. the measurements of pO2 in the renal cortex averageWe next assessed the determinants of QO2 and tubular reab- only approximately 45 mm Hg.sorption of sodium (TNa) for whether they could account for
A preglomerular shunt pathway for O2 has been in-any differences in renal cortical pO2 in SHRs.ferred from the finding that the pO2 measured in superfi-Results. The pO2 in the EA was reduced 40 to 50% compared
with arterial values but was similar in the two strains (WKY cial cortical (SC) glomerular capillaries of rats is onlyrats 45 6 2 vs. SHRs 41 6 1 mm Hg, P 5 NS). The pO2 value one half of that measured in arterial blood [7]. The firstin the PT, DT, and SC did not differ within strains. All were
aim of these studies was to test directly the hypothesissignificantly (P , 0.001) lower in SHRs (for example, pO2 inthat there is an O2 shunt pathway in the rat kidney. WePT of WKY rats 39 6 1 vs. SHRs, 30 6 1 mm Hg). The pO2
in the renal vein was above that at any site in the EA or the have measured the pO2 at the precapillary site in thecortex, implying a precapillary shunting of O2 from the artery renal cortex within the efferent arterioles (EAs) usingto vein. SHRs had reduced renal blood flow (RBF) leading to
ultramicro platinum-iridium coaxial glass microelec-a reduced (P , 0.05) rate of O2 delivery (WKY rats 42 6 6trodes [8, 9], and compared this with the pO2 measuredvs. SHRs 30 6 1 mmol · min21 · g21) and a reduced glomerular
filtration rate, leading to a lower (P , 0.001), TNa (WKYs 115 6 in the aorta and renal vein. Since the outer cortex is the9 vs. SHRs 66 68 mmol · min21 · g21). However, despite the most well-oxygenated site in the kidney [7], an increase43% reduction in TNa, the renal O2 usage was not significantly
in pO2 in the renal vein above that in the precapillarydifferent between strains (WKY rats 7.6 6 0.8 vs. SHRs 9.0 6arteriole will demonstrate directly an O2 shunt pathway1.0 mmol · min21 · g21). Therefore, the SHRs had a sharp
reduction (P , 0.001) in the O2 efficiency for Na1 reabsorption in the kidney in vivo.(TNa/QO2; WKY rats 15.1 6 1.6 vs. SHRs 7.3 61.0 mmol21). Previous studies with Clarke-type O2 sensors have re-
Conclusions. A precapillary O2 shunt reduces the pO2 ofported a renal cortical pO2 of 40 to 50 mm Hg [10–13].cortical nephrons. The pO2 is reduced further in SHRs becauseHowever, the oxygenation of the nephron has not beenof less efficient O2 usage for Na1 transport.assessed directly in vivo. The second aim was to useultramicroelectrodes with tip sizes of 3 to 5 mm to assessthe pO2 in proximal and distal nephrons. These elec-The kidney has a high rate of oxygen usage (QO2) to
satisfy the metabolic requirement for the high rate of trodes are sufficiently small to allow measurement with-out apparent damage to the capillary blood supply tothe region.Key words: spontaneously hypertensive rat, nitric oxide, erythropoie-
tin, renal blood flow. There is a close relationship in the normal kidneybetween TNa and QO2 [1–4, 14]. The oxygen usage of the
Received for publication April 18, 2000intact spontaneously hypertensive rats (SHRs) is in-and in revised form July 19, 2000
Accepted for publication July 21, 2000 creased [15]. Therefore, the third aim of this study wasto test the hypothesis that renal oxygen usage by the 2001 by the International Society of Nephrology
230

Welch et al: Renal oxygen usage and supply 231
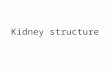
SHR kidney is enhanced because of a less efficient utili- Studies for nephron and tissue pO2 utilized a customdesigned and validated ultramicro, coaxial, recessed-zation of O2 for tubular sodium reabsorption.tipped platinum glass microelectrode shown diagram-matically in Figure 1 [7–9]. The outer tip diameter was
METHODS3 to 5 mm. The tip of the electrode was coated with an
Studies were performed on male SHRs and Wistar- O2-permeable membrane by dipping it in collodion andKyoto (WKY) rats aged 10 to 11 weeks obtained from polystyrene. This electrode was inserted into superficialHarlan-Sprague-Dawley (Madison, WI, USA). Rats proximal (PT) and distal tubules (DTs) and EAs withoutwere maintained on a standard rat chow (Purina, St. Louis, obstructing flow or damaging local blood supply to mea-MO, USA) with a sodium content of 0.3 g21 · 100 g21. sure the intraluminal pO2 values. All of these measure-They were allowed free access to food and water until ments were made while the electrode was visualized inthe day of study. the lumen of the tubule or arteriole. The aim of the
outer cortical measurements was to obtain values fromAnimal preparation and clearance measurements
the interstitium, but this was not so precisely defined.Groups of SHRs and age-matched WKY rats were The micropipette tip was advanced just below the capsule
prepared for in vivo clearance and micropuncture stud- in a space between adjacent tubules. Inner cortical mea-ies, as described in detail previously [16]. In brief, animals surements were obtained in undefined nephron loca-were anesthetized with thiobarbital (Inactin, 100 mg · tions. The electrode was advanced 2 mm below the sur-kg21 intraperitoneally; Research Biochemicals, Inc., Na- face where a pO2 recording was made. The recessed tiptick, MA, USA). A catheter was placed in a jugular vein allowed the measurement of pO2 in rapidly flowing bloodfor fluid infusion and in a femoral artery for the recording in vessels in vivo with an error of ,1.5% (stirring effect).of mean arterial pressure (MAP) from the electrically The electrode was connected to an ultrahigh-impedencedamped output of a pressure transducer (model P23 1D picoammeter (pA6000; WPI, Sarasota, FL, USA). TheStatham Division, Gould, Oxford, CA). A tracheotomy output was subjected to analog-digital conversion andtube was inserted. The animals were allowed to breathe displayed on a computer (Mac-lab 4A; ADInstruments,room air spontaneously. A catheter was placed in the Castle Hill, Australia). This system provides a stable andbladder to collect urine. The left kidney was exposed linear output in response to pO2 across the tested rangeby a flank incision, cleaned of connective tissue, and of 4 to 500 mm Hg.stabilized in a Lucite cup. It was bathed in 0.154 mol/L To validate the accuracy of the electrode, six arterialNaCl equilibrated with air and maintained at 378C. After blood samples were measured by both a blood gas ana-completion of surgery, rats were infused with a solution lyzer (BGA) and the electrode, in random order. Theof 0.154 mol/L NaCl and 1% albumin at 1.5 mL · h21 to pO2 measured by each method was similar (BGA 81.4 6maintain an euvolemic state [16]. Studies were begun 1.6 vs. electrode 79.2 6 1.3; P 5 NS).after 60 minutes for stabilization.
Measurements of kidney function and parameters ofFor clearance, [3H]-inulin (0.1 mCi · mL21; ICN Bio-O2 usagechemicals, Costa Mesa, CA, USA) was added to the
intravenous fluid infusion. Urine was obtained from the These studies were undertaken on 18 WKY rats andbladder, and blood was sampled from the femoral artery 16 SHRs. The O2 content of systemic arterial and renaland renal vein at the end of the clearance period. Renal venous blood were measured in an oximeter (Model 682;venous blood was obtained using a #23 gauge steel needle Instrumentation Laboratories, Lexington, MA, USA)inserted into the renal vein and angled toward the kid- from blood samples (50 mL) drawn from the femoralney. The study period lasted 60 to 90 minutes. During artery cannula and the renal vein. The glomerular filtra-this time, a single renal clearance was undertaken. Values tion rate (GFR) was calculated from the clearance ofof MAP and heart rate (HR) were obtained over 15- [3H]-inulin. The renal plasma flow (RPF) was calculatedminute intervals and were averaged. from the clearance of [3H]-inulin corrected for the mea-
sured renal extraction of [3H]-inulin as described pre-Measurements of arterial, venous, intranephronal, and viously [17]. The renal blood flow (RBF) was calculatedtissue pO2 from RPF factored by 1 hematocrit (Hct). The net tubu-
These measurements were made on 10 SHRs and 10 lar reabsorption of sodium (TNa) was calculated from theWKY rats that were separate from the clearance studies. difference between the filtered load of sodium [calcu-Blood (100 mL) was drawn from the femoral artery and lated from the product of the GFR and plasma sodiumrenal vein at the end of the clearance for pO2 measure- concentration (PNa)] and the renal sodium excretionment. Samples were capped and kept on ice until they (UNaV). Net renal oxygen usage (QO2) was calculatedwere measured, after minimal delay, by a Corning Blood from the product of RBF and (A-V)O2. The measure-
ments of renal venous O2 content were made in the renalGas Analyzer (BGA; Model 525; Boston, MA, USA).

Welch et al: Renal oxygen usage and supply232
Fig. 1. Diagrammatic representation of the tipof oxygen-sensitive coaxial ultramicroelectrodeused to measure the partial pressure of oxygen(pO2) in the renal tubules.
Table 1. Data for body and kidney weights, mean arterial pressure, heart rate and hemoglobin concentration
Body weight Kidney weightNumber HR MAP Hb
Group of rats g min21 mmHg g·100 g21
WKY 18 280611 1.1060.06 366610 11862 15.660.5SHR 16 262610 1.0560.09 37269 15263 17.160.5P value NS NS NS ,0.001 ,0.05
Data are mean 6 SEM values. Abbreviations are: HR, heart rate; MAP, mean arterial pressure; Hb, hemoglobin; WKY, Wistar-Kyoto rat; SHR, spontaneouslyhypertensive rat.
vein after it had exited from the kidney distal to any Table 2 and Figure 2 detail the measurements of theshunt pathway for O2. Therefore, this measure of renal partial pressures of oxygen. There were no significantO2 usage was not confounded by the presence of any A-V differences between SHRs and WKY rats in pO2 mea-shunt for O2 within the kidney. The oxygen efficiency for sured in arterial blood or in the EA. However, the pO2
Na1 transport was calculated from the ratio of TNa:QO2. had fallen substantially by approximately 50% betweenmeasurements in the aorta and the EA. The values for
Statistical methods pO2 did not differ within strains when measured in theValues are reported as mean 6 SE. Analysis of vari- PT, DT, or interstitial space of the superficial cortex.
ance (ANOVA) was applied to data of SHRs and WKY However, the intratubular values were lower (P , 0.05)rats. A post hoc Dunnett’s test was applied where appro- than in the EA in both strains. The outer cortex pO2priate to identify significant differences between groups. was lower (P , 0.05) than EA only in SHRs. Moreover,Values are taken as statistically significant if P , 0.05. values were significantly (P , 0.05) lower by approxi-
mately 25% in the SHRs at each site of measurementin the outer cortex. Measurements of pO2 in the deepRESULTScortex showed a further fall of 25 to 35%, comparedTable 1 details the body and kidney weights, HR,with the superficial cortex. The pO2 values in the deepMAP, and hemoglobin concentration of the groups ofcortex and in the renal vein were both significantly (P ,rats studied in the clearance protocol. As anticipated, the0.05) lower in SHRs than in WKY rats.MAP of SHRs was consistently higher than equivalent
In both groups, the pO2 in the renal vein clearly ex-WKY rats. The hemoglobin content of arterial bloodwas higher in SHRs than WKY rats. ceeded values measured in the superficial cortex. This

Welch et al: Renal oxygen usage and supply 233
Table 2. Partial pressures of oxygen measured in kidney tissue
pO2 mm Hg
Group Number of rats EA PT DT OC DC
WKY 10 45 39a 40a 42 31a
62 61 61 62 62SHR 10 41 30a 29a 31a 20a
62 61 61 61 62P value between strains NS ,0.05 ,0.05 ,0.05 ,0.05
Values are mean 6 SEM. Abbreviations are: EA, efferent arteriole; PT, proximal tubule; DT, distal tubule; OC, outer cortex; DC, deep cortex.a P , 0.05 compared to efferent arteriole
usage, yet a large 43% (P , 0.001) reduction in TNa.Consequently, the O2 efficiency for TNa was reduced sub-stantially by 52%.
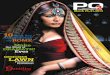
Figure 3 shows individual data for renal oxygen usageas a function of tubular sodium transport. There is asignificant correlation in both groups. The slope of theregression of QO2 on TNa was almost twice as great inSHRs compared with equivalent WKY rats, but bothhad a similar intercept on the y axis. This implies thatacross the range of TNa values studied, the oxygen costof sodium transport is consistently higher in the kidneysof SHRs compared with WKY rats.
DISCUSSION
The main new findings from this study are first, thepO2 in the renal vein is consistently above that in the
Fig. 2. Mean 6 SEM values for pO2 measured in the aortic and renal EAs or outer cortical nephrons. This demonstrates thevenous blood samples and in the efferent arteriole (EA), proximal
presence of an arteriovenous precapillary diffusionaltubule (PT), and distal tubule (DT) with an O2 electrode. Symbols are:(s) data for WKY rats and (d) SHRs data. Compared with WKY; shunt pathway for O2 in the kidney. Second, the pO2 of**P , 0.01. the renal cortex of the SHR is uniformly lower than that
of normotensive control WKY rats. This can be ascribedto an approximately 50% increase in the oxygen costfor Na1 transport in the hypertensive kidney. To ourimplies a diffusional shunt for O2 from arterial bloodknowledge, this is the first demonstration of reducedprior to the EA that bypasses the renal parenchyma andrenal oxygenation in hypertension. Our technique doesdelivers O2 into the renal vein.not allow us to evaluate whether the shunt is quantita-Table 3 details parameters of whole kidney O2 deliv-tively different between SHRs and WKY rats.ery, O2 usage, tubular sodium transport, and O2 efficiency
The high pO2 in blood draining from the kidney, rela-for sodium transport. The O2 delivery was reduced intive to other organs, has been long appreciated. It hasSHRs because of a reduction in RBF that was partially,been attributed to the very high rates of renal corticalbut incompletely, offset by a greater arterial O2 contentblood flow that are required for the formation of a glo-due to a great hemoglobin concentration in the SHRmerular filtrate [5]. This concept predicts that the luxuri-(Table 1). The renal venous O2 content was not signifi-ant RBF would result in a high pO2 of renal corticalcantly reduced in the SHRs, despite the reduced venoustissues. In fact, the redox state of the mitochondrial cyto-pO2 (Fig. 2) because it was offset by a greater hemoglobinchromes of the kidney shows that 25 to 40% is in the(Hb) in the SHRs that enhanced the O2 carrying capacity.reduced form [18]. This suggests that substantial portionsNevertheless, the (A-V)O2 was consistently increased inof the kidney may normally operate on the brink ofSHRs by a factor of approximately twofold. The greateranoxia. The present study confirms quite closely otherA-V difference for O2 did not translate into a significantmeasurements made in rats [7, 11, 12, 19] and dogs [20]increase in O2 usage in the SHRs because it was offsetof an outer cortical tissue pO2 in the normal kidney thatby the lower RBF. The GFR and hence the TNa wereaverages only 42 mm Hg. We found that the pO2 wasreduced significantly in the SHRs by 43%. Therefore,
the SHRs had a modest 18% (P 5 NS) increase in O2 not significantly different within strains in the superficial

Welch et al: Renal oxygen usage and supply234
Table 3. Parameters of whole kidney oxygen delivery, oxygen usage, tubular sodium transport and oxygen efficiency for sodium transport
O2 deliveryO2 usage
Sodium transport O2 efficiencyRBF 3 for TNaRBF AO2 RBF 3 AO2 VO2 (A-V)O2 (A-V)O2 GFR PNa UNaV TNamL · min21 · lmol · lmol · lmol · lmol · lmol · mL · min21 · mmol · TNa/QO2
Group g21 mL21 min21 · g21 mL21 mL21 min21 · g21 g21 L21 lmol · lmol21lmol · min21 · g21
WKY(N 5 18) 5.160.5 8.860.3 41.965.6 7.360.3 1.560.1 7.660.8 0.8260.07 14062 0.4160.16 11569 15.161.6
SHR(N 5 16) 3.160.4 9.860.3 30.461.2 6.960.4 2.960.2 9.061.0 0.4760.04 13763 0.5860.19 6668 7.361.0
P value ,0.005 ,0.05 ,0.05 NS ,0.001 NS ,0.001 NS NS ,0.001 ,0.001
Mean 6 SEM values.
into the perfusate of an isolated dog’s kidney [21]. Theyshowed that O2 reached the renal vein before erythro-cytes, thereby demonstrating an O2 shunt pathway. Theseauthors attributed the shunt to O2 passage between thearteriolar and venular ends of cortical and medullarycapillaries. In a second study, Schurek et al showed thatthe pO2 in surface outer cortical glomeruli of Munich-Wistar rats averaged 46 mm Hg when the arterial pO2
was 90 mm Hg [7]. This strongly supports the conceptof a preglomerular O2 shunt. However, the pO2 in therenal vein was not measured, and therefore, the shuntpathway was not assessed directly. Nevertheless, thevalue for pO2 of 46 mm Hg in outer cortical glomeruliof normotensive Munich-Wistar rats agrees closely withthe value of 45 mm Hg measured in the present studyin EAs in normotensive WKY rats. This suggests thatthe major site of O2 loss is indeed prior to the glomerularcapillaries. The interlobular arteries run for a substantial
Fig. 3. Individual values for whole kidney O2 usage (QO2) as a function distance in direct contact with interlobular veins [22].of tubular sodium transport (TNa). Symbols are: (d) SHRs; (s) WKYThis could be the site for O2 passage from the arterialrats. The equations for lines representing the calculated regressions are
as follows: WKY, y 5 0.048x 1 3.3(r 5 0.65, P , 0.01), and SHR, y 5 to the venous system. The finding that the pO2 falls by0.092x 1 1.9(r 5 0.64, P , 0.01). 40 to 50% between measurements in aortic and efferent
arteriolar blood is reminiscent of results of Duling andBerne in the hamster cheek-pouch preparation [23].They reported that there is a periarterial gradient forPT and DT and the outer cortical interstitium. This sug-pO2 that is apparently caused by diffusion of O2 throughgests that O2 is in diffusional equilibration within thethe walls of distributing conduit vessels. This reduces thesuperficial renal cortex of the WKY rats and the SHRs.pO2 of blood to approximately 20 to 30 mm Hg at theIn contrast, the pO2 in the deeper cortex was consistentlyterminal arterioles. The special aspect in the kidney ap-lower than the superficial cortex by 25 to 35%. There-pears to be the relationship between the intrarenal arter-fore, there is a gradient of pO2 values from outer toies and veins that shunt the O2 leaving the arterial systemdeeper cortex that is preserved in the SHRs. The pO2
into the venous system.in the renal vein consistently and substantially exceedsWe found consistently lower values for pO2 in thethat in the precapillary arteriole in the outer cortex.
cortical nephrons of the SHRs. Calculations from wholeTherefore, the high renal venous pO2 is a tribute notkidney data show that the SHR kidney had a 27% reduc-only to the high rate of RBF, but also to a precapillarytion in O2 delivery, yet a trend toward an increase in O2shunt for O2 from the arterial into the renal venoususage, thereby creating a major mismatch between O2system.supply and demand in the SHR kidney (Table 3). TheTwo previous studies have provided evidence for thegreater O2 demand occurred despite a sharp 43% de-shunting of O2 from the renal arterial to venous system.crease in the net chemical work for Na1 transport. There-Levy and Imperial injected a bolus of blood with a high
O2 tension and containing optically labeled erythrocytes fore, the enhanced O2 demand was related to a doubling

Welch et al: Renal oxygen usage and supply 235
of the O2 cost for tubular Na1 transport. As shown in the SHR kidney might be a reflection of functional NOdeficiency and oxidative stress.Figure 3, the regression of QO2 on TNa was linear through
Physiological concentrations of NO inhibit reversiblythe physiologic range. The slope was almost twice asthe mitochondrial respiratory chain [34]. NO can inhibitgreat in SHRs as WKY rats, yet the intercepts wereO2 consumption in the heart [35] or renal tubules [36].similar. Previous studies in dog and rat kidneys haveAt the pO2 measured in the renal cortex in vivo in ourshown that renal oxygen usage is strongly related to TNa
study, the ED50 for NO-induced inhibition of respirationabove a basal level, indicated by the intercept on the yin rat cortical tubules is 38 6 6 nmol/L. This comparesaxis [4, 5, 24–26]. This relationship holds during increaseswith a calculated NO concentrations in the renal cortexin TNa produced by infusions of hypertonic saline or de-of approximately 30 nmol/L [36]. Therefore, the en-creases by aortic constriction [4].hanced O2 usage by the SHR kidney might be a conse-Two factors have been identified that may contributequence of enhanced tubular respiration because of func-to a decreased TNa:QO2, as demonstrated in the SHRtional NO deficiency. Brezis et al have shown that thekidney. The first is that the efficiency of O2 usage formedullary pO2 in the rat falls sharply after inhibition ofNa1 transport varies between nephron segments. TheNOS [10] and increases after infusion of nitrovasodila-ratio TNa:QO2 is highest in the thick ascending limb oftors [12]. However, the pO2 in the renal cortex was unre-the loop of Henle (TAL), lower in the PT, and lowestsponsive to NOS blockade in their studies [10], perhapsin the cortical or medullary collecting ducts [26]. Thus, abecause of the rather large changes in renal perfusionshift in nephron reabsorption in the hypertensive kidneypressure and RBF. It is not presently clear how O2 usagetoward segments such as the TAL that utilized O2 lesscould become uncoupled from the chemical work re-efficiently could decrease in TNa:QO2. The SHR kidneyquired for NaCl reabsorption by a deficiency of NO.reabsorbs less of the glomerular filtrate in the proximalHowever, the O2 usage of PTs taken from SHRs devel-nephron and more in the loop of Henle, which couldoping hypertension has been found to be uncoupled fromthereby contribute to the increase O2 cost for TNa. How-ATP hydrolysis [27].ever, the pO2 was reduced within the outer cortical PT
Erythropoietin is released in response to a reductionand DT of the SHRs in our study. Moreover, O2 usagein arterial O2 content in the interstitial fibroblasts of thein renal cortical tubules studied ex vivo is increased 15 torenal cortex. Our finding of a reduced pO2 in the renal25% in SHRs developing hypertension [27]. Therefore, acortex in hypertension predicts an increased drive forchange in O2 usage in proximal and distal nephrons oferythropoietin production. This is consistent with ourSHRs presumably also contributes to enhanced O2 utili-findings of an increase in Hb in SHR that confirm otherzation.reports in SHRs or humans with essential hypertension
A second factor that decreases TNa:QO2 is blockade of[37–41]. Collectively, these data are consistent with an
nitric oxide synthase (NOS), which can reduce TNa/QO2 increased drive for erythropoietin secretion in hyperten-in the dog’s kidney by 50% [28]. This is comparable to the sion that could be secondary to relative hypoxemia inreduction seen in the present study of the SHR kidney. the renal cortex.Indirect evidence suggests that the SHR kidney is in a A reduced renal cortical pO2 in hypertension may con-functional state of NO deficiency, despite an increase in tribute to some of the abnormalities in renal regulation.constitutive NOS expression. Thus, the isolated, per- Erythropoietin [39] and increased Hct [42] could contrib-fused afferent arteriole from the SHRs has a diminished ute to increased peripheral vascular resistance. The Kmacetylcholine-induced release of endothelium-depen- for O2 of the cytochrome P-450 4A v-hydroxylase thatdent relaxation factor (EDRF) [29]. The regulation of generates 20-hydroxyeicosatetrenoic acid (HETE) fromtubuloglomerular feedback (TGF) by macula densa- arachidonate is in a range that should be responsive toderived NO is severely curtailed or absent in the SHR the pO2 of the renal cortex measured in this study [43].kidney, despite enhanced expression of NOS in the mac- Studies in the hamster cheek pouch vasculature confirmula densa [30]. There is evidence of oxidative stress in that this enzyme can be an O2 sensor in vivo [44]. Athe kidney of SHRs [31–33]. Functional NO deficiency deficient v-hydroxylase activity in the hypertensive rathas been related to oxidative stress, since the enhanced kidney has been proposed to contribute to altered pres-renal vascular resistance, blood pressure [33], and TGF sure natriuresis in salt-sensitive hypertension [45]. This[31] responses of SHRs can be normalized by administra- could be secondary to renal cortical hypoxia. The genetion of a membrane-permeable superoxide dismutase for vascular endothelial growth factor (VEGF) [46], likemimetic. Recently, we have shown increased expression some other cytokines and growth factors implicated inof nicotine adenine diphosphate (NADPH) oxidase in renal changes of hypertension, contains a hypoxia re-the SHR kidney (abstract; Chabrashvili et al, J Am Soc sponse element that might account for increased expres-Nephrol 10:343A, 1999) that might underlie the renal sion in the hypertensive kidney [47].
In conclusion, the SHR model of hypertension has aoxidative stress. Thus, the increased O2 cost for TNa in

Welch et al: Renal oxygen usage and supply236
18. Epstein FH, Balaban RS, Ross BD: Redox state of cytochromereduced pO2 in the renal cortex that can be ascribed toaa3 in isolated perfused rat kidney. Am J Physiol 243:F356–F363,
an inefficient utilization of O2 for tubular sodium reab- 1982sorption. 19. Lubbers DW, Baumgartl H: Heterogeneities and profiles of oxy-
gen pressure in brain and kidney as examples of the pO2 distribu-tion in the living tissue. Kidney Int 51:372–380, 1997
ACKNOWLEDGMENTS 20. Baumgartl H, Leichtweiss HP, Lubbers DW, et al: The oxygensupply of the dog kidney: Measurements of intrarenal pO2. Micro-These studies were supported by National Institute of Diabetes andvasc Res 4:247–257, 1972Digestive and Kidney Diseases grants DK-36079 and DK-49870 and
21. Levy MN, Imperial ES: Oxygen shunting in renal cortical andby funds from the George E. Schreiner Chair of Nephrology. We aremedullary capillaries. Am J Physiol 200:159–162, 1961grateful to Ms. Delphine Nguyen for preparation of the manuscript.
22. Kriz W: A periarterial pathway for intrarenal distribution of renin.Kidney Int 31:51–56, 1987Reprint requests to Christopher S. Wilcox, M.D., Ph.D., Division of
23. Duling BR, Berne RM: Longitudinal gradients in periarteriolarNephrology and Hypertension, 6th Floor-PHC, Georgetown Universityoxygen tension. Circ Res 27:669–678, 1970Medical Center, 3800 Reservoir Road, NW, Washington D.C. 20007,
24. Klahr S, Hammerman M: Renal metabolism, in The Kidney: Physi-USA.ology and Pathophysiology, edited by Seldin DW, Giebisch G,E-mail: [email protected] York, Raven Press, 1985, pp 699–718
25. Knox FG, Flemming JS, Rennie DW: Effect of osmotic diuresison sodium reabsorption and oxygen consumption of kidney. AmREFERENCESJ Physiol 219:751–759, 1966
1. Kiil F: Renal energy metabolism and regulation of sodium reab- 26. Gullans SR, Hebert SC: Metabolic basis of ion transport, in Thesorption. Kidney Int 11:153–160, 1977 Kidney, edited by Brenner BM, Philadelphia, W.B. Saunders, Inc.,
2. Lassen NA, Munck O, Thaysen JH: Oxygen consumption and 2000sodium reabsorption in the kidney. Acta Physiol Scand 51:371–384, 27. Brazy PC, Klotman PE: Increased oxidative metabolism in renal1961 tubules from spontaneously hypertensive rats. Am J Physiol 257:
3. Barger AC, Herd JA: Renal vascular anatomy and distribution F818–F825, 1989of blood flow, in Handbook of Physiology: Renal Physiology, edited 28. Laycock SK, Vogel T, Forfia PR, et al: Role of nitric oxide inby Orloff J, Berliner RW, Washington D.C., American Physio- the control of renal oxygen consumption and the regulation oflogical Society, 1973 pp 249–314 chemical work in the kidney. Circ Res 82:1263–1271, 1998
4. Deetjen P, Kramer K: Die abhangigkeit des O2-verbrauchs der 29. Ito S, Carretaro OA: Impaired response to acetylcholine despiteniere van der Na1-reschorption. Arch Ges Physiol 273:636–650, intact endothelium-derived relaxing factor/nitric oxide in isolated1961 perfused afferent arterioles of the spontaneously hypertensive rat.
5. Thurau K: Renal Na1 reabsorption and O2 uptake in dogs during J Cardiovasc Pharmacol 20:S187–S189, 1992hypoxia and hydrochlorothiazide infusion. Proc Soc Exp Biol Med 30. Welch WJ, Tojo A, Lee J-U, et al: Nitric oxide synthase in the106:714–717, 1961 JGA of the SHRL: Expression and role in tubuloglomerular feed-
6. Levy MN: Effect of variations of blood flow on renal oxygen back. Am J Physiol 277:F130–F138, 1999extraction. Am J Physiol 199:13–18, 1960 31. Welch WJ, Tojo A, Wilcox CS: Roles of NO and oxygen radicals
7. Schurek HJ, Baumgartl H, Bertram H, et al: Evidence for a in tubuloglomerular feedback in SHR. Am J Physiol 278:F769–preglomerular oxygen diffusion shunt in rat renal cortex. Am J F776, 2000Physiol 259(6 Pt 2):F910–F915, 1990 32. Schnackenberg C, Wilcox CS: Two-week administration of tem-
8. Lubbers DW: Oxygen electrodes and optodes and their application pol attenuates both hypertension and renal excretion of 8-iso pros-in vivo, in Oxygen Transport to Tissue XVI, edited by Ince, New taglandin F2a. Hypertension 33:424–428, 1999York, Plenum Press, 1996, pp 13–34 33. Schnackenberg CG, Welch WJ, Wilcox CS: Normalization of
9. Baumgartl H, Lubbers DW: Microcoaxial needle sensor for po- blood pressure and renal vascular resistance in SHR with a mem-larographic measurement of local O2 pressure in the cellular range brane-permeable superoxide dismutase mimetic: Role of nitric ox-of living tissue: Its construction and properties, in Polarographic ide. Hypertension 32:59–64, 1998Oxygen Sensors, edited by Gnaiger E, Forstner H, Berlin, 34. Brown GC, Cooper CE: Nanomolar concentrations of nitric oxideSpringer-Verlag, 1983, pp 37–65 reversibly inhibit synaptosomal respiration by competing with oxy-
10. Brezis M, Heyman SN, Dinour D, et al: Role of nitric oxide in gen at cytochrome oxidase. FEBS Lett 356:295–298, 1994renal medullary oxygenation. J Clin Invest 88:390–395, 1991 35. Forfia PR, Zhang X, Knight DR, et al: NO modulates myocardial
11. Brezis M, Agmon Y, Epstein FH: Determinants of intrarenal O2 consumption in the nonhuman primate: An additional mecha-oxygenation I: Effects of diuretics. Am J Physiol 267:F1059–F1062, nism of action of amlodipine. Am J Physiol 276:H2069–H2075,1994 1999
12. Brezis M, Heyman SN, Epstein FH: Determinants of intrarenal 36. Koivisto A, Pittner J, Froelich M, et al: Oxygen-dependent inhibi-oxygenation II. Hemodynamic effects. Am J Physiol 267:F1063– tion of respiration in isolated renal tubules by nitric oxide. KidneyF1068, 1994 Int 55:2368–2375, 1999
13. Gunther H, Aumuller G, Kunke S, et al: Die sauerstoffversor- 37. Sen S, Hoffman GC, Stowe NT, et al: Erythrocytosis in spontane-gung der niere. Res Exp Med 163:251–264, 1974 ously hypertensive rats. J Clin Invest 51:710–714, 1972
14. Parekh N, Veith U: Renal hemodynamics and oxygen consump- 38. Gould AB, Goodman SA: Effect of an angiotensin-convertingtion during postischemic acute renal failure in the rat. Kidney Int enzyme inhibitor on blood pressure and erythropoiesis in rats. Eur19:306–316, 1981 J Pharmacol 181:225–234, 1990
15. Walsh GM, Tsuchiya M, Cox AC, et al: Altered hemodynamic 39. Eschbach JW, Davidson RC: Red blood cell mass/erythropoietinresponses to acute hypoxemia in spontaneously hypertensive rats. and blood pressure: Lessons from patients with renal disease, inAm J Physiol 234:H275–H279, 1978 Hypertension: Pathophysiology, Diagnosis and Management, ed-
16. Welch WJ, Wilcox CS: Potentiation of tubuloglomerular feed- ited by Laragh JH, Brenner BM, New York, Raven Press, 1995,back in the rat by thromboxane mimetic: Role of macula densa. pp 389–398J Clin Invest 89:1857–1865, 1992 40. Chabanel A, Chien S: Blood viscosity as a factor in human hyper-
17. Baylis C, Harvey J, Engels K: Acute nitric oxide blockade ampli- tension, in Hypertension: Pathophysiology, Diagnosis and Manage-fies the renal vasoconstrictor actions of angiotensin II. J Am Soc ment, edited by Laragh JH, Brenner BM, New York, Raven
Press, 1995, pp 365–376Nephrol 5:211–214, 1994

Welch et al: Renal oxygen usage and supply 237
41. Chien S: Blood rheology in myocardial infarction and hyperten- in the thick ascending limb of Dahl SS/Jr rats. Hypertension 33(1 Pt 2):419–423, 1999sion. Biorheology 23:633–653, 1986
42. Gaar KA: Erythrocytosis: A key to understanding the hemody- 46. Johnson RJ, Schreiner GF: Hypothesis: The role of acquiredtubulointerstitial disease in the pathogenesis of salt-dependent hy-namic changes in hypertension. Med Hypothesis 27:107–113, 1985
43. Harder DR, Narayanan J, Birks EK, et al: Identification of a pertension. Kidney Int 52:1169–1179, 199747. Wenger RH, Marti HH, Schuerer-Maly CC, et al: Hypoxic induc-putative microvascular oxygen sensor. Circ Res 79:54–61, 1996
44. Lombard JH, Kunert MP, Roman RJ, et al: Cytochrome P-450 tion of gene expression in chronic granulomatous disease-derivedB-cell lines: Oxygen sensing is independent of the cytochromev-hydroxylase senses O2 in hamster muscle, but not cheek pouch
epithelium, microcirculation. Am J Physiol 276:H503–H508, 1999 b558-containing nicotinamide adenine dinucleotide phosphate oxi-dase. Blood 87:756–761, 199645. Ito O, Roman RJ: Role of 20-HETE in elevating chloride transport