Embed Size (px)
Citation preview

Geriatric Nephrology and Urology8: 29–44, 1998. 29c 1998Kluwer Academic Publishers. Printed in the Netherlands.
Review article
Nephrologic complications of drug therapy in the elderly
Richard Chan1 & Michael F. Michelis21Assistant Chief, Nephrology Section, Lenox Hill Hospital, New York, New York, Clinical Instructor of Medicine,New York University School of Medicine, New York, New York, U.S.A.;2Chief, Nephrology Section, Lenox HillHospital, New York, New York, Clinical Professor of Medicine, New York University School of Medicine, NewYork, New York, U.S.A.
Accepted 31 December 1997
Key words:aged, contrast sensitivity, drug toxicity, hyperkalemia, pharmacokinetics, renal failure
General concepts
It is well known that the number and proportion ofolder individuals in our society is increasing [1]. Aspatients age, they can be expected to develop a varietyof medical problems which may be treated by an everincreasing number of therapeutic agents. Indeed, it hasbeen noted that hospitalized older patients may receivean average of 8 to 10 different drugs [2]. Unfortunately,the large variety of drugs available can be associatedwith a multitude of uncommon, but nevertheless seri-ous, untoward effects. Some of the untoward effectsseen may occur more commonly in older patients dueto the changes in renal function and drug metabolismwhich may accompany aging [3, 4].
The goal of this review is to explore the cur-rent body of information in regard to the nephrologiccomplications of some of the more commonly useddiagnostic and therapeutic agents in elderly patients.Review of renal functional changes associated withaging and drug handling by older individuals will pre-cede discussions of specific drug problems. These willinclude problems associated with converting enzymeinhibitors (CEI), whose indications now include ther-apy for hypertension, hypertensive cardiomyopathy,and diabetic nephropathy [5]. In addition, the seriouscomplication of hyperkalemia, as it occurs in a vari-ety of therapeutic situations in older patients will bereviewed. Also, complications of therapy with nons-teroidal antiinflammatory agents, interstitial renal dis-ease as it occurs with a variety of drugs,and the toxicityseen with the diagnostic and therapeutic use of radio-contrast material will be characterized.
Changes in renal function which accompany aging
The decreases in glomerular filtration rate and alter-ations in renal tubular function that may accompanyaging have been the subject of numerous studies overthe past several decades [6–8]. It is well recognizedthat glomerular filtration rate, as estimated by creati-nine clearance (CrCl), can decrease with age [8]. Thedecrease in CrCl may not be appreciated by measure-ment of serum creatinine (Cr). This occurs becauseaged individuals generally experience a decrease inmuscle mass, which, in turn, is associated with adecrease in muscle creatinine production. Since thedecrease in creatinine production may parallel thedecrease in glomerular filtration rate, serum Cr mayremain unchanged despite declining renal function.When drugs are prescribed which are excreted by thekidney and which can cause nephrotoxicity at highserum levels, accurate assessment of renal functionby more sophisticated measures is essential for properdrug dosing.
In order to address the necessity for a rapid esti-mate of glomerular filtration rate in aged individuals, avariety of procedures have been proposed. One of themore widely used is the estimate of creatinine clear-ance by the formula of Cockcroft & Gault [9], whichincorporates values for age and body weight as well asa correction for gender:
CrCl =(140� age)�weight (kg)
72� serum Cr
* multiply by 0.85 in females

30
This determination can provide useful information inregard to glomerular filtration rate in older individualsso that the proper dosage of potentially nephrotoxicagents, such as aminoglycosides, can be calculated.
Ideal characteristics of an estimate of glomerularfiltration rate (GFR) in the elderly should include theability to rapidly quantitate renal function with a mini-mum of invasive study and/or data collection. Morerecent procedures for rapid evaluation of renal functionhave included estimates of glomerular filtration ratevia radionuclide techniques [10] which can be usedfor single or serial determinations. Of late, additionalprocedures such as estimate of GFR via data obtainedusing bioelectrical impedance measurements have alsobeen proposed [11].
Aging is also associated with changes in renal tubu-lar function which can complicate drug therapy inelderly patients. These changes include a decreasedability for renal sodium conservation during sodiumdepletion [12], limitation of urinary concentratingand diluting ability [13], and decreased distal tubularcapacity for acid and potassium excretion [14]. In addi-tion to the impaired renal sodium conservation that mayresult from structural alterations in the nephron, hor-monal alterations which may accompany aging such asdecreased renin and aldosterone secretion [15, 16], andincreased activity of atrial natriuretic peptide [17], canalso affect renal sodium handling in elderly patients.
Tendencies for excessive renal sodium loss in agedpatients obviously can complicate diuretic therapy, aswell as render these individuals more susceptible tocomplications from other therapies which may causeuntoward effects in the salt depleted state.For example,antihypertensive drugs may cause hypotension in thehypovolemic patient.
The decrease in urinary concentrating abilityobserved in the elderly occurs, partially, as a resultof renal structural changes which decrease medullaryhypertonicity and limit maximal urinary concentra-tion [13]. Inability to adequately concentrate the urinemay result in increased morbidity during periods ofextrarenal fluid loss. On the other hand, decreases infunction of the diluting segment of the nephron andabnormalities in the regulation of vasopressin secre-tion, may result in inappropriate water retention [18].Previous data have demonstrated higher plasma levelsof vasopressin in older patients when compared toyounger, and decreases in renal excretory capacitymay also limit free water excretion [19]. Inappropriatevasopressin secretion has been noted to occur spon-taneously in older patients [20], and may also occur
Table 1. Changes in renal function with aging
Decreased glomerular filtration rate (variable)
Decreased concentration and diluting ability
Decreased potassium and hydrogen ion excretion
during stress [21], and in association with pulmonarydisease [22], neoplastic disease [23], and with drugsthat stimulate vasopressin secretion [24]. Hypoosmo-lar syndromes often become clinically apparent whenolder patients are given obligatory free water duringintravenous therapy with dilute fluids [25]. Recent datasuggest that stimuli for vasopressin secretion in healthyelderly are dependent more upon nonosmotic factorssuch as hypovolemia, and that osmotic stimuli mayactually not be important for the regulation in vaso-pressin secretion in the aged [19].
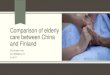
An impairment in hydrogen ion and potassiumsecretion can occur in elderly patients with distalrenal tubular dysfunction. Acidosis secondary to renalhydrogen ion retention has been described in instancesof chronic renal interstitial disease either secondaryto infection or pharmacologic agents [26, 27]. Potas-sium retention can develop either in association withrenal tubular diseases or secondary to the decreasedsecretion of renin and aldosterone which may accom-pany aging [14, 28, 29]. Some data suggest thathyporeninemic hypoaldosteronism may result fromgradual fluid accumulation [30, 31]. Recent studiesare consistent with this hypothesis since some patientswith hyporeninemic hypoaldosteronism, who receivedchronic diuretic therapy, demonstrated increases inplasma renin activity associated with a decrease inatrial natriuretic peptide (Figure 1) [32, 33]. The abovealterations in renal function must be considered whendeveloping specific diagnostic or therapeutic plans inelderly patients with renal disease. This is particularlyimportant when therapeutic strategies are used whichmay be associated with the administration of acid, suchas occurs with parenteral nutrition, or with drugs thatare associated with inhibition of potassium secretionby the distal tubule. The changes in renal function withaging are summarized in Table 1.
Changes in drug metabolism which may accompanyaging
When considering potential nephrologic complicationsof drug therapy in the elderly, the handling of drugsby various metabolic pathways in the aged should first

31
Figure 1. Mean data from four patients with hyporeninemic hypoal-dosteronism are illustrated. In panel A, levels of plasma reninactivity are below the normal range (PRA, open circles) before and60 minutes after captopril 25 mg, while plasma atrial natriureticpeptide (ANP, closed circle) level is elevated. Panel B depictsincreased PRA, response to captopril, and decreased ANP afterdiuretic induced weight loss.
be appreciated. Aging is associated with physiologicchanges which potentially may affect the absorption ofdrugs, but clinically relevant alterations have not beenwell documented in the literature [34]. The gastroin-testinal absorption of drugs in elderly subjects, despitesenescent changes, is generally well preserved unlessconcomitant disease, such as diabetic gastroparesis, isalso present [35, 36].
Decreased secretion of gastric acid may occur inolder patients, especially if concurrent antiulcer med-ications, such as histamine blockers or the newer,more potent proton pump inhibitors are prescribed.This effect of raising gastric pH may potentiallydecrease the absorption of medications such as ironsalts, indomethacin, ketoconazole, and tetracycline,but this usually has little clinical significance [37]. Theconcomitant use of calcium, magnesium or aluminumcontaining antacids may also alter the absorption ofsuch drugs as allopurinol, benzodiazepines, digoxin,and beta-blockers, again with little significant effect[38].
In addition to interference with drug absorptionfrom the gastrointestinal tract, the aging process is alsoassociated with a decrease in the absorptive surfacearea of the stomach and small intestine, and a decreasein overall gastrointestinal mobility, especially if anti-cholinergics or anti-Parkinsonian drugs are also used[37, 39]. Atherosclerosis and cardiovascular problemsmay also contribute to a decrease in splanchnic blood
flow [37]. Despite these age related changes, the gas-trointestinal absorptionof drugs in the elderly is largelyunaltered [36, 39]. Newer methods of drug deliveryvia a percutaneous route of administration, such astransdermal clonidine, nitroglycerin, estrogen, opiates,scopolamine, and nicotine, are not well studied in olderpatients. The pharmacokinetics of these transdermallyadministered drug systems in the aged are unclear[40, 41].
Unlike absorption, alterations in the tissue distrib-ution of drugs prescribed in elderly patients may resultin significant potential for toxic complications. Aftera drug is absorbed, it becomes distributed in bodytissues depending on its properties of water or fatsolubility. When prescribing drugs which are predomi-nantly water soluble, it is important to recognize thataging is generally accompanied by a decrease in leanbody mass relative to fat mass, causing water solu-ble drugs to attain higher levels in that nonfat com-partment. Therefore, drug dosing using body weightalone can result in higher plasma drug concentrationsand toxicity to renal and other tissues. For example,aminoglycosides are distributed into lean tissues anddosages should be appropriately adjusted to accountfor a decreased lean body mass in elderly patients.Further, concomitant use of diuretics, by decreasingextracellular fluid volume, may heighten blood levelsand nephrotoxic risk [42]. Other water soluble (polar)agents include digoxin,aminophylline, cimetidine, andethanol, the use of which should be similarly carefullymonitored in elderly patients.
When lean body mass decreases with aging, theproportion of fat mass increases, especially in women,so fat-soluble (lipophilic) drugs may have a prolongedduration of action due to this expanded reservoir.Examples of lipophilic drugs include the benzodi-azepines, barbiturates, phenothiazines, and phenytoin.For lorazepam and amobarbital, however, the vol-ume of distribution does not appear to change withage [37].
The plasma protein binding properties of drugsalso play a significant role in mediating drug toxi-city, because aging may be associated with a decreasein albumin production and/or binding affinity [43,44]. This can occur due to a variety of factors, suchas chronic illness, or secondary to malnutrition inthe hospitalized or institutionalized geriatric patient.When hypoalbuminemia occurs, the proportion of free(unbound) drug increases, and drug is able to leavethe intravascular space and distribute to target tissues.Monitoring of serum drug levels, which measures the

32
sum of free and bound drug amounts, therefore, maynot prevent potential drug toxicity. Plasma albuminbinds weakly acidic drugs, such as salicylates, war-farin, phenytoin, sulfonamides, theophylline, and bar-biturates. Therefore, low plasma albumin levels willmake more of these drugs available in an unboundstate. The circulating substance�1-acid glycoprotein,aplasma protein, and also an acute phase reactant, bindsweak bases, such as lidocaine and propranolol. Levelsof �1-acid glycoprotein tend to increase with aging,potentially decreasing the availability of affected drugs[45]. Because of the aforementioned physiologic alter-ations in body composition and plasma protein bind-ing with aging, the risk of drug toxicity is heightenedwhen multiple drug regimens are employed in elderlypatients.
The hepatic clearance of drugs occurs via twotypes of biotransformation reactions. Phase I reactionsinclude oxidation, reduction, and hydrolysis, whichmay either decrease or remain unchanged during aging[36]. The Phase II reactions involving glucuronidation,acetylation, and sulfation, remain generally unalteredin elderly patients [36]. While microsomal and non-microsomal enzymes participate in both Phase I andPhase II reactions, measurements of these enzymaticactivities, such as the cytochrome P450 system, in agedindividuals have yielded inconsistent results [46–48].Furthermore, the inhibition of microsomal enzymes bythe drug, cimetidine, is not affected by aging [49]. Thehazardous combination of cimetidine and warfarin,therefore, continues to be a potent threat in elderlypatients.
A decrease in total enzymatic activity respon-sible for drug metabolism would have its greatestimpact on drugs with “low intrinsic clearance,” thatis, those with relatively slow hepatic metabolism. Adecrease in hepatic mass as seen with aging, withconsequence decrease in enzyme activity would slowthe metabolism of such drugs [50]. However, otherfactors, such as cigarette smoking which may stimulateenzymes, may offset the decrease in liver volume inregard to drug metabolism [51]. In contrast to reducedhepatic enzymatic activity, a decrease in hepatic bloodflow, in congestive heart failure, for instance, pre-dominantly affects the metabolism of drugs with “highintrinsic clearance” [52]. The extraction of such sub-stances, such as indocyanine green, is reduced inelderly individuals [51, 52]. The nephrologic impor-tance of reduced hepatic drug metabolism becomesmanifest when hepatically cleared drugs which maycause interstitial nephritis are prescribed in excess.
Table 2. Changes in drug metabolism with aging
Absorption (rarely affected)
Distribution
Decreased lean body mass
Decreased plasma protein
Metabolism
Decreased oxidation reactions
Decreased hepatic blood flow
Excretion
Varies with changes in glomerular filtration rate
Such drugs include the penicillins, macrolide antibi-otics [53], ciprofloxacin [54], and others [55]. Of noteis the CEI, fosinopril, which is the sole member of itsclass to have both renal and hepaticclearance [56]. Thisdrug can be used safely in patients with renal insuffi-ciency, but should be used carefully when concomitantliver decrease is present.
Drug elimination by renal excretion plays the mostcrucial role in geriatric pharmacokinetics. Creatinineclearance, an estimate of glomerular filtration, candecline with aging, as previously discussed [6]. It isimportant to note, however, that subgroups of elderlyindividuals do not demonstrate a decline in glomeru-lar filtration as they age [8]. Therefore, dose selectionand prescribing practices should account for individualdifferences in body mass and serum creatinine. Com-monly employed mathematical formulas, such as thatof Cockcroft and Gault, described earlier in this text,still may overestimate renal function in markedlydebilitated nursing home residents [57]. The accurateassessment of creatinine clearance involving 24-hoururine collection is often impractical, or even poten-tially dangerous if bladder catheterization is employedin certain elderly patients. Until more rapid, precise,and practical methods of assessing renal and hepaticfunction in individual patients are developed, the gen-eral guidelines of using smaller initial drug doses, lessfrequent dose changes, and careful monitoring of ther-apeutic responses, monitoring of serum drug levelsand avoidance of drug interactions, are still paramountin treating aged patients [36]. The changes in drugmetabolism which may occur in aging are summarizedin Table 2.
Finally, it is important to recognize that indepen-dent of drug absorption, the degree of protein bind-ing, metabolism, and excretion, the physiologic effectof drug delivered to target tissues is often alteredin the elderly. Such examples include the decreased

33
responses observed with furosemide [58], and thealtered pattern of cardiac conduction and blood pres-sure response seen with verapamil in elderly patients[59].
Specific drug problems
Nephrologic complications of converting enzymeinhibitor therapy in the elderly
Increasing use of converting enzyme inhibitors (CEI)has been seen to occur over the last decade. A reviewof first line antihypertensive drug choice in the elderly,during 1990, revealed that CEI’s or calcium channelblocking drugs were prescribed four times as often asdiuretics or beta blockers [60]. This occurred despitethe recommendations from the fifth Joint NationalCommittee on Hypertension, which suggested thatdiuretics and beta blocking drugs be used initially,because of their proven efficacy in reducing the mor-tality and morbidity associated with hypertension [61].The increased usage of CEI’s have resulted, in part,from the increase in the indications for the use of thesedrugs. As noted earlier, these agents are now used fortreatment of congestive heart failure [62], reversal ofcardiac hypertrophy [63, 64], protection against dia-betic nephropathy [65–70], and preservation of renalfunction [71, 72] as well as their earlier role in thetreatment of both diastolic and systolic hypertension[5, 73].
The various complications of CEI therapy whichhave been generally recognized include dysgeusia,cough [74], bronchospasm [75], angioneurotic edema[74], exacerbation of psoriasis [76], and neutropenia[5, 37]. In regard to changes involving the kidney,commonly cited problems include the development ofazotemia in association with changes in renal perfusioninduced by CEI’s in patients with renal artery stenosis[3, 77]. This is felt to occur secondary to a decreasein efferent arteriolar tone with resultant decrease inglomerular filtration pressure seen in patients witheither single kidney renal artery stenosis, or patientswith two kidneys and bilateral renal artery disease.Of interest is the observation that even these earlyreports include the finding that the patients describedwith renal artery disease, and who developed azotemiaassociated with the use of CEI’s, often were receivingdiuretic therapy as well.
Review of more recent literature seems to empha-size the important association of decreases in hydration
Table 3. Risk factors for azotemia with CEI therapy in the elderly
Age
Dehydration
Diuretic therapy
Hypotension
Renal artery disease
status often associated with diuretic therapy and theoccurrence of azotemia when patients are treated withCEI’s [78, 79]. Such changes in hydration status canoccur more easily in older patients who may alreadyexhibit decreases in salt and water conservation sec-ondary to the renal tubular dysfunction which mayaccompany aging, as noted earlier in this review.
Although large numbers of patients obviouslybenefit greatly from the use of CEI’s for a variety ofindications, an increasing body of literature is accu-mulating describing renal insufficiency developing inassociation with the use of these drugs [79–81]. Thetypes of problems noted include reversible increasesin blood urea nitrogen levels and serum creatininewhich accompany the use of CEI’s, often in associationwith dehydration, with or without the use of diuretictherapy, and sometimes, coincident with decreases inblood pressure alone [80, 81]. Reversible azotemia iscommonly seen in cardiac patients while on therapywith a diuretic agent and a CEI [78, 81]. Of furthersignificance are the recent observations of changes inrenal function which are either not reversible [82], orwhich have been demonstrated on renal biopsy to beassociated with acute tubular necrosis [79]. The studyby Bridoux et al. described patients with renal insuffi-ciency associated with CEI therapy in which associateddehydration occurred in 77% of cases. When ten of thepatients were subjected to renal biopsy, it was discov-ered that 5 patients exhibited acute tubular necrosis[79]. Risk factors for azotemia with CEI therapy in theelderly are listed in Table 3.
A more recent European study also noted that whenrenal failure occurred in association with CEI therapy,recovery did not always occur [83]. Since varioustypes of renal disease seem to resolve more slowlyin older patients [82], it is not surprising that a pro-longed course of renal failure may occur in associa-tion with azotemia following CEI therapy. It wouldseem prudent that older patients receiving CEI therapyshould have their renal function carefully monitoredand physicians should be particularly attentive to situa-tions where dehydration or negative fluid balance is

34
a possibility. The latter could be expected to occurwhen these patients receive diuretic therapy, but alsomay become significant problems when patients areplaced on oral fluid restriction prior to procedures orsurgery, or when they are given substances such asradiocontrast material which may provoke a diuresisin a patient already marginally hydrated. Avoidanceof CEI-induced renal insufficiency in association withdehydration may be accomplished by discontinuanceor decrease in dosage of either CEI type drugs ordiuretics prior to contemplated procedures, and bymaintenance of adequate hydration during any pro-cedures such patients may require. Further, it wouldseem reasonable that similar recommendations wouldapply to the use of the newer angiotensin II receptorblocking agents.
Hyperkalemia associated with drug therapy in theaged
The changes in renal function which accompanyaging, previously cited, include a tendency toward adecreased GFR [8] and a decrease in distal tubularfunctions such as potassium and hydrogen ion excre-tion. Previously described increases in atrial natriureticpeptide (ANP) in the aged [17], as well as decreasesin plasma renin activity (PRA) and plasma aldosterone(PA) [15, 16], could be consistent with an increasein intravascular volume, perhaps related to decreasedrenal excretory capacity. This increase in volume couldexplain the increase in ANP, the decreases in PRA andPA noted, and also provide a pathophysiologic expla-nation for the tendency to hyperkalemia observed inthe older age group [84]. The importance of volumestatus, and its potential for stimulating ANP, couldthen, in part, explain the observed decreases in PRAand PA, since ANP is known to depress productionof both of these hormones [85–87]. In any case, thechanges in PRA and PA could explain the tendencytoward hyperkalemia observed.
Of interest, is the chance occurrence of the useof a variety of drugs directed toward therapy of car-diovascular and musculoskeletal abnormalities in theelderly, which also can favor elevation of serum potas-sium. Converting enzyme inhibitors given for a varietyof indications cited earlier in this chapter result indecreased aldosterone production, and the commoncomplication of hyperkalemia [88]. Beta blockingagents, useful in the therapy of systemic hyperten-sion, as well as antiarrhythmic, and antianginal effects,result in a decrease in PRA, with the effect that serum
potassium can rise when these agents are used [89].Nonsteroidal antiinflammatory agents, whose associa-tion with tubulointerstitial disease and proteinuria willbe discussed later, also inhibit prostaglandin formation,and thereby have a depressant effect on PRA, whichalso can result in the elevation of serum potassium[90–92].
It is important to recognize, therefore, that thesethree classes of drugs commonly used in older patientshave the combined effect of decreasing the hor-monal regulation of potassium excretion via the distalnephron. Since the distal tubular loss of potassium isthe major route of excretion of this electrolyte [93], itis not surprising that a tendency toward an increase inserum potassium can occur. It is well known that olderpatients commonly receive multiple drug therapy [2],and it would not be uncommon for a given patient tobe receiving more than one, and even all, of the aboveagents. In addition, as stated earlier, an age relateddecrease in PRA and PA as well as a decrement intubular functional capacity associated with acquiredinterstitial disease in an older patient could all com-bine to result in a tendency toward severe, and evenlife threatening, hyperkalemia.
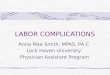
It would seem prudent to carefully obtain base-line serum potassium levels when older patients areencountered, and to carefully monitor these levelswhen commonly used agents associated with hyper-kalemia are employed in the therapy of these indi-viduals. Since some of these patients may exhibit atendency toward some degree of hypervolemia, gentlediuretic therapy with induction of loss of small vol-umes of fluid body weight, may be helpful in decreas-ing intravascular fluid volume with a resultant decreasein ANP, increase in PRA and PA, and resultant facilita-tion of urinary potassium excretion. It should be recog-nized, however, that excessive volume contractioncould result in excessive proximal tubular reabsorptionof filtrate and decreased distal tubular sodium delivery,which could limit distal tubular sodium for potassiumexchange, and have the undesired effect of limitingpotassium excretion and increasing serum potassiumlevels. This untoward effect would only occur whenmore severe levels of dehydration are produced. Twopossible responses to diuretic therapy described aboveare depicted in Figure 2. Careful monitoring of serumpotassium seems, therefore, particularly indicated inolder patients receiving any of the drugs cited above.

35
Figure 2. The figure illustrates the optimal and excessive typesof diuresis that may occur in an older patient with hyporeninemichypoaldosteronism.
Nephrologic complications of nonsteroidalantiinflammatory therapy in the elderly
Nonsteroidal antiinflammatory drugs (NSAID) con-tinue to be used in a wide variety of circumstancesin older patients [94]. Despite the obvious benefitsassociated with the use of these agents, there con-tinues to be much concern in regard to the untowardeffects which also may accompany the use of thesedrugs (Table 4) [3, 95, 96]. These include cutaneouseruptions, hepatic toxicity, and gastrointestinal bleed-ing [97–99]. Despite recent data which suggest thatNSAID’s may not significantly alter renal function inhealthyelderly subjects [100], a variety of renal andelectrolyte disturbances have been described [101].An understanding of the physiologic effects of thesedrugs allows for the prediction of the kind of untowardeffects which may be seen. NSAID’s are known todecrease prostaglandin synthesis, which may in turndecrease sodium excretion and urine volume, resultingin fluid retention and increased blood pressure espe-cially in situations where prostaglandins are acting tomaintain urine flow in a compensatory manner [102,103]. These situations include dehydration, congestiveheart failure, and decreased renal perfusion due to largevessel disease [104]. Decreases in renal perfusion stim-ulate the production of prostaglandins, which in turnmaintain the excretion of salt and water via intrarenalvasodilation [105].
Table 4. Renal complications of NSAID therapy in the elderly
Azotemia
Hyperkalemia
Hyponatremia
Hyporeninemic hypoaldosteronism
Interstitial nephritis
Papillary necrosis
Proteinuria/minimal change disease
Sodium and water retention/hypertension
In addition, prostaglandins are known to stim-ulate increases in PRA and PA, and mitigate theeffects of antidiuretic hormone (ADH) on the collect-ing tubule [103, 106]. When NSAID’s block the effectof prostaglandins, hyporeninemic hypoaldosteronismcan result, with attendant hyperkalemia [107]. On theother hand, NSAID’s facilitate the effect of ADH on thenephron and, during water loading, dilution of plasmaosmolality and hyponatremia can result in associationwith NSAID use. Other effects of NSAID’s includethe occurrence of minimal change nephropathy, withheavy proteinuria when therapy is prolonged,and inter-stitial renal disease, and even papillary necrosis, ina variety of clinical situations [108–110]. The com-bination of glomerular abnormalities with interstitialnephritis has led some authors to suggest that the mech-anism of NSAID induced interstitial disease resultsfrom a pathophysiologic mechanism which is differentfrom that seen in other types of drug induced intersti-tial nephritis [111]. In further support of this concept isthe observation that the characteristic hypersensitivityresponses (fever, rash, eosinophilia, etc.) seen in otherdrug induced interstitial nephritis are often absent inNSAID associated renal parenchymal disease [111].
Recently, Sandler et al. suggested that the risk ofrenal insufficiency associated with the daily use ofNSAID’s was a particular problem in males over 65years of age [112]. An editorial by Wagner, however,pointed out that the data cited were barely statisticallysignificant, there appeared to be no dose responseeffect, and that these complications may occur whenNSAID’s are used to treat medical problems whichmay have renal disease as part of their clinical picture[113].
That serious renal difficulties may be associatedwith the use of NSAID’s in circumstances whereprostaglandins may be exerting protective renal effectsis emphasized in a recent paper by Wen et al., whodescribed two patients who used NSAID’s to treat

36
symptoms which followed excessive alcohol ingestion[114]. Both patients developed evidence of acute renalinsufficiency and one patient received a renal biopsywhich revealed evidence of acute tubular necrosis. Itwas postulated that the NSAID’s interfered with thevasodilatory effects of prostaglandins stimulated by thedecrease in renal perfusion secondary to dehydration.This, in turn, critically decreased renal circulation tothe point where tubular damage occurred. It i s also sig-nificant that the dose of NSAID’s used by both patientscould be considered moderate.
A variety of NSAID’s are now available for clini-cal use [115]. Differences in their pharmacology andmetabolism may relate to the occurrence of renal toxi-city. For example, the metabolism of sulindac may beassociated with a decreased potential for renal toxicity[116, 117]. A peculiar problem to these agents is also aresult of the fact that they are available by prescriptionin the higher dose ranges, but also available as overthe counter drugs in lower doses. Since there is littlecontrol of the frequency of use or dosage of over thecounter agents, it may be expected that some excessiveusage may occur. This may be a particular problem inolder patients who may use excessive amounts eitherdue to forgetfulness or because the drugs are employedto treat chronic conditions which have little chance forresolution. Despite these potential risks, the occurrenceof renal complications of over the counter NSAID’s hasnot been impressive [96, 118, 119].
Drug induced interstitial nephritis in the elderly
With the increase in both prescription and nonpre-scription drug use in elderly patients, the exposure todrug antigens and haptens which may potentially causeinterstitial nephritis has become increasingly common[2]. Both acute and chronic interstitial nephritis sec-ondary to drugs can be observed. Reports of acuteinterstitial nephritis (AIN) have paralleled the intro-duction and subsequent clinical use of virtually everydrug class [120]. For example, observations during thepast three decades have described AIN resulting fromthe use of penicillin type antibiotics [55, 121–123]. Asthe newer cephalosporins, quinolones, and macrolideshave been more widely used, their associations withAIN also have become commonly recognized [53, 54,124–126]. A listing of drugs more recently noted to beassociated with AIN appears in Table 5.
It is believed that the development of drug inducedAIN is related to the effects of immunoregulatory cellsand reactions to immunologically active substances
Table 5. Drugs recently associated with interstitial nephritis (refer-ences provided)
5-Aminosalicyclic acid [179]
Acyclovir [80]
Anti-CD4 monoclonal antibody [148]
Azathioprine [147]
Azithromycin [53]
Captopril [181]
Ciprofloxacin [54]
Diazepam [182]
D-penicillamine [183]
Ethambutol [184]
Indapamide [185]
Omeprazole [149]
Ranitidine [150]
which reside within the renal interstitium [127]. Druginduced AIN is associated with hypersensitivity reac-tions involving antigen presenting cells, T lympho-cytes, complement activation, release of chemotacticfactors, immune complex deposition, and antibodyproduction directed against tubular basement mem-branes [128]. Recently, using sera from patients withantitubular basement membrane nephritis, the glyco-protein gp54 has been identified to be an importantnephritogenic antigen mediating this particular dis-order [129]. The use of lymphocyte stimulation testinghas also been reported to confirm hypersensitivity tospecific drugs in patients with biopsy proven acuteinterstitial nephritis [130].
The migration of eosinophils into the renal intersti-tium in AIN may result from the release of chemotacticfactors by mast cells, T lymphocytes, and other leuko-cytes [131]. Eosinophil major basic protein may thenbe released, and its toxic properties cause further tissueinjury [131]. The detection of urinary eosinophils hasbeen heralded as a noninvasive diagnostic test for druginduced, and non drug induced forms of AIN [132].Because the capability of a standard Wright’s stain todistinguish an eosinophil’s bilobed nucleus and char-acteristic granules is limited, alternate staining tech-niques, using methylene blue and eosin-y in methanol(Hansel’s stain), have been proposed. The use of thislatter technique was said to increase the detection ofeosinophiluria in AIN from 25% to 63% of patientsstudied [132, 133].
However, the patients cited in these studies oftendid not have renal biopsy proven AIN, and when his-tologic findings were available, confounding featuresof acute tubular necrosis were also present [134]. Fur-

37
thermore, eosinophiluria is present in disorders otherthan AIN, such as cholesterol embolization [135] andglomerulonephritis [136]. In a recent retrospectivereview, which, however, may be limited by the paucityof renal biopsy data, the false positive and negativerates of eosinophiluria were too high to serve as adiagnostic test for AIN [136].
The presence of peripheral blood eosinophilia hasbeen associated with the development of hypersen-sitivity reactions in general, and the classic triad ofrash, fever, and eosinophilia may herald the onset ofazotemia secondary to drug induced AIN [137]. How-ever, this triad of findings is present in less than one-third of patients with biopsy-proven AIN [137]. Thefrequency of clinical features which may lead one tosuspect drug induced AIN include: fever (80% cases),hematuria, either gross or microscopic [95% cases),skin rash (40% cases), and, less commonly, unilateralor bilateral flank pain, arthralgia, lymphadenopathy,and other organ involvement secondary to hypersen-sitivity [138]. These responses may be seen less fre-quently and less intensely in elderly subjects with AINdue to changes in immunocompetence which havebeen observed to occur in the aged [139].
The urinary findings in drug induced AINwhich may be observed include hematuria, pyuria,eosinophiluria, and proteinuria. These occur presum-ably because of tubulointerstitial injury [121]. Inter-estingly, urinary erythrocyte casts have also beenreported to appear in AIN [140]. Urinary electrolytesusually demonstrate isosthenuria and elevated urinarysodium concentration (UNa) and fractional excretionof sodium (FENA), although a low UNa and FENA donot exclude the diagnosis of AIN [141].
Hypokalemia, hypomagnesemia, incomplete Fan-coni’s syndrome with glycosuria and aminoaciduriahave also been reported in AIN [142]. In specificpatients, both proximal and distal tubular dysfunctionhave been demonstrated. Some authors, however, sug-gest that injury patterns in AIN preferentially involvethe distal nephron [143]. A review of biopsy specimensusing stereologic microscopy and electron microscopydemonstrated that nephron segments distal to proximalconvoluted tubules were more susceptible to inflamma-tory cell infiltration [143].Other studies, however, noteno difference between the proximal and distal nephronrelative to injury in AIN [121].
Even when clinical data are consistent with thediagnosis of AIN, confirmation by renal biopsy mayoccur in only 50% of patients [144]. This may resultfrom the relatively nonspecific clinical features often
cited as consistent with AIN. In addition, althoughdata suggest that elderly patients can tolerate renalbiopsy well [145], many patients may not have specificbiopsy proven diagnosis due to reluctance by the physi-cian to subject ill patients to yet another potentiallyharmful procedure. Therefore, the overall incidence ofdrug induced AIN in elderly patients is not well docu-mented. Since the aging process is also associated withthe possibility of immune senescence [139, 146], theoccurrence of immune mediated AIN, could actually beless frequent in elderly patients. Nevertheless, biopsyproven, drug induced AIN in elderly patients has beenfrequently reported [147–150]. Since the number ofaged in our population and the use of drugs in theseelderly individuals continue to increase, the prevalenceof drug induced AIN in the elderly should continue togrow [2].
Other diagnostic procedures may also be helpfulfor the recognition of drug induced AIN. For example,gallium uptake scanning may be useful in this regard.Unfortunately, however, positive gallium scans mayalso be obtained in other inflammatory or neoplasticconditions [151].Perhaps the most useful maneuver forboth diagnostic yield and therapeutic benefit is a trialof discontinuance of any possible offending drug. Thisshould be tried even when commonly used agents arebeing given to patients whose renal failure is otherwisenot explained. In regard to elderly patients in particular,the diagnosis of renal insufficiency as a result of vascu-lar disease should not be made unless the possibility ofdrug induced interstitial nephritis is carefully excluded[152]. Other therapeutic approaches, such as the useof steroids, are still quite controversial. Some reportshave observed prompt recovery with steroid use [122,153, 154], while other studies concluded that no benefitwas obtained by steroid administration [120, 155]. Nocontrolled studies have been performed and the use ofsteroids should be considered on an individual basis ineach patient. Whether or not steroids are used, the over-all prognosis of drug induced AIN appears favorable,even if oliguria or the need for hemodialysis occurs[155].
The untoward effects associated with the useof nonsteroidal antiinflammatory drugs (NSAIDs)involving the kidney include the complications of inter-stitial nephritis, as well as profound proteinuria andnephrotic syndrome [108]. These disorders may meritspecial consideration because of the high frequency ofanalgesic use in older patients. The interstitial renalprocess observed with NSAIDs consist of infiltrationby small lymphocytes, as well as some eosinophils

38
[156]. Renal papillary necrosis has also been described.The development of significant proteinuria has beensuggested to be the result of changes in lymphocytefunction following exposure to NSAIDs, which mayalter the permeability characteristics of the glomerularbasement membrane [156]. As with other episodes ofrenal insufficiency where a possible diagnosis of inter-stitial nephritis is being entertained, diagnostic inves-tigation should be initiated, and, in questionable cases,renal biopsy should be considered. Possible offend-ing pharmacologic agents should be discontinued, and,if a high index of suspicion of drug induced intersti-tial nephritis exists in a patient with protracted renalfailure, a trial of steroids may be attempted althougha recent study did not demonstrate this to be of anybenefit [111].
Nephrologic complications of the use of radiocontrastagents in the elderly
The clinical use of radiocontrast agents continues toincrease, particularly in older patients [157]. Therehas been increasing recognition of the renal complica-tions associated with these agents [158]. These includechanges in urine volume due to the osmotic diureticeffect of these substances [159], as well as the develop-ment of significant acute renal insufficiency followingthe use of this material [160, 161]. The type of agentused has changed from the earlier high osmolar agentswith osmolalities in the 1200–2000 mOsm/L range,to substances which are of lower osmolality, in therange of 600–900 mOsm/L. The so called low osmo-lar radiocontrast agents (which are still hypertonic tonormal plasma) are felt to be associated with less renaltoxicity, although several authors have stated that thereal benefit of these agents is seen mostly in diabeticswith renal insufficiency who appear to have a specialrisk for the occurrence of acute renal failure followingthe use of radiocontrast material [162, 163].
The factors that may influence the occurrence ofradiocontrast associated acute renal failure (RAARF)include dehydration, advanced age, underlying renalinsufficiency, diabetes mellitus, history of priorRAARF, and multiple sequential exposures to theseagents (Table 6) [164]. Indeed, a recent study demon-strated that the quantity of dye administered corre-lated directly with the incidence of RAARF in diabeticpatients with renal insufficiency [165]. The pathophys-iologic explanations for the development of RAARFhave included suggestions that vasoconstrictive sub-stances, such as endothelin, may be released from
Table 6. Major factors influencing the occurrence of RAARF
Advanced age
Dehydration
Diabetes mellitus
History of prior RAARF
Radiocontrast dose & frequency
Renal insufficiency
the vascular endothelium of the kidney with resultantintense vasoconstriction and oliguria [166–168]. Fur-ther, a recent study in humans using theophylline asan antagonist to the vasoconstrictor substance adeno-sine, demonstrated that theophylline could preventdecreases in glomerular filtration rate induced by radio-contrast media [169]. RAARF can develop followinga period of increased urine flow associated with theadministration of radiocontrast material [159]. Duringthe period of oliguria,a low urine sodium concentrationmay be observed, in association with a low fractionalexcretion of sodium and progressive elevation of bloodurea nitrogen and serum creatinine levels [170].
Recent studies have shown a low incidence ofthe occurrence of RAARF, and only rarely is dia-lytic therapy required to treat the renal dysfunc-tion [171, 172]. In addition to dialytic therapy forovert renal failure, prophylactic hemodialysis has beenemployed immediately after radiocontrast agents havebeen administered to patients with underlying severerenal insufficiency. It has been suggested that thisapproach may prevent pulmonary vascular congestionsecondary to the mobilization of extravascular fluidinto the intravascular space as a result of the osmoticeffects of the radiocontrast material. This may avoidacute pulmonary edema in some patients, but the inci-dence of this problem is small and such an aggressiveapproach may be required only on rare occasions.
In general, however, problems with RAARF arebest prevented in patients with mild to moderate renalinsufficiency by the maintenance of a high rate of urineflow and the provision of adequate hydration prior tothe performance of the procedure. A variety of mea-sures have been suggested which have included routineadministration of intravenous saline, and/or the use ofvarious diuretic agents concomitant with the adminis-tration of radiocontrast material. These diuretic agentshave included intravenous mannitol and intravenousfurosemide given singly, or even simultaneously [173–176]. A recent study has suggested, however, thatprophylactic regimens using diuretic therapy can be

39
associated with a diuresis whose magnitude may actu-ally result in the development of negative fluid bal-ance following the radiocontrast study, and that this,in turn, may increase the incidence of the develop-ment of RAARF [177]. The preferable recommenda-tion may be, therefore, to avoid the development ofnegative fluid balance when radiocontrast is given, andto replace any fluid losses so that dehydration does notoccur. Further, the question can be raised as to whethersimple hydration with saline alone may be preferableto the prophylactic use of diuretic agents, since thevolume losses with saline alone are less dramatic andthe risk of dehydration is therefore not as great [174,177]. This concept has been fostered by a recent study[178], although the use of 0.45% saline in that studywould raise concerns regarding the development ofhyponatremia.
In regard to the selection of high versus low osmo-lar radiocontrast material (LOCM), many centers havemoved to the use of LOCM to avoid potential legalconcerns regarding possible untoward effects follow-ing these procedures. Of interest, several recent studies[163, 175] have suggested little advantage in regard tothe use of LOCM unless patients already exhibit riskfactors such as underlying renal failure and diabetesmellitus. It would seem prudent that, regardless of thetype of agent used, special attention and follow up beprovided to those patients who appear to be at highestrisk. It should also be appreciated that renal failure inassociation with radiocontrast studies may also haveother etiologies, such as atheroembolic disease, whichmay be more serious and more often, irreversible.Patients with atheroembolic phenomenon may exhibit,in addition to acute renal failure, purple discolorationof the extremities, especially feet and toes, livedo retic-ularis, increases in blood pressure, elevated erythro-cyte sedimentation rate, decreased serum complement,eosinophilia, and eosinophiluria [135].
Conclusion
A variety of diagnostic and therapeutic agents and pro-cedures have become available for elderly patients.Unfortunately, some of these modalities are asso-ciated with untoward effects for which elderly patientsmay be especially susceptible. This review has exam-ined nephrologic complications of several importantmodern therapies. It is necessary to appreciate the spe-cial vulnerability of elderly patients to these agents so
that older patients may maximize the benefits of suchtherapies while avoiding undesirable effects.
References
1. Age Structure of U.S. Population – 21st Century [Statis-tical Brief (SB-01-86)]. Washington, D.C.: U.S. GovernmentPrinting Office, 1986.
2. Amber IJ. Geriatric pharmacology. In: The HospitalizedElderly. Univ. of Utah Geriatric Medicine Publication, 1990:23–29.
3. Lameire N, Verspeelt J, Vanholder R et al. A review of thepathophysiology, causes and prognosis of acute renal failurein the elderly. Geriatr Nephrol Urol 1991; 1: 77–91.
4. Pascual J, Orofino L, Burgos J. Acute renal failure in theelderly. Geriatric Nephrology Urology 1992; 2: 51–61.
5. Gavras I, Gavras H. ACE inhibitors: a decade of clinicalexperience. Hospital Practice July 1993: 117–127.
6. Rowe JW, Andres R, Tobin JD et al. The effect of age oncreatinine clearance in men: a cross-sectional and longitudinalstudy. J Gerontol 1976; 31: 155–163.
7. Epstein M. Effects of aging on the kidney. Fed Proc 1979; 38:168–171.
8. Lindeman RD, Tobin JD, Shock NW. Longitudinal studies onthe rate of decline in renal function with age. J Am GeriatrSoc 1985; 33: 278–285.
9. Cockcroft DW, Gault MH. Prediction of creatinine clearancefrom serum creatinine. Nephron 1976; 16: 31–41.
10. Sanger JJ, Kramer EL. Radionuclide quantitation of renalfunction. Urol Radiol 1992; 14: 69–78.
11. Laboy A, Zabetakis PM, Gleim GW et al. Estimating urinecreatinine excretion and glomerular filtration rate utilizinga bioelectrical impedance analysis measurement of fat freemass. [Abs] NKF Clin Nephrol Meetings Proc pA12, Apr,1994.
12. Epstein M, Hollenberg NK. Age as a determinant of renalsodium conservation in normal men. J Lab Clin Med 1976;87: 411–417.
13. Rowe JW, Shock NW, DeFronzo RA. The influence of ageon the renal response to water deprivation in man. Nephron1976; 17: 270–278.
14. Michelis MF. Hyperkalemia in the elderly. Am J Kid Dis1990; 16: 296–299.
15. Noth RH, Lassman MN, Tan SY. Age and the renin-aldosterone system. Arch Intern Med 1977; 137: 1414–1417.
16. Tsunoda K, Abe K, Goto T et al. Effect of age on the renin-angiotensin-aldosterone system in normal subjects. Simul-taneous measurement of active and inactive renin, reninsubstrate, and aldosterone in plasma. J Clin Endocrinol Metab1986; 62: 384–389.
17. Ohashi M, Fujio N, Nawata H et al. High plasma concentra-tions of human atrial natriuretic polypeptide in aged men. JClin End Met 1987; 64: 81–85.
18. Lindeman RD, Lee TD Jr., Yiengst MJ et al. Influence ofage, renal disease, hypertension, diuretics, and calcium on theantidiuretic responses to suboptimal infusions of vasopressin.J Lab Clin Med 1966; 68: 206–223.
19. Johnson AG, Crawford GA, Kelly D et al. Arginine vaso-pressin and osmolality in the elderly. J Am Geriatr Soc 1994;42: 399–404.

40
20. Goldstein CS, Braunstein S, Goldfarb S. Idiopathic syn-drome of inappropriate antidiuretic hormone secretion possi-bly related to advanced age. Ann Int Med 1983; 99: 185–188.
21. Kennedy PGE, Mitchell DM, Hoffbrand BI. Severe hypona-tremia in hospital inpatients. Br Med J 1978; 2: 1251–1253.
22. Sladen A, Laver MB, Pontoppidan H. Pulmonary complica-tions and water retention in prolonged mechanical ventilation.N Engl J Med 1968; 279: 448–453.
23. Bartter FC, Schwartz WB. The syndrome of inappropriatesecretion of antidiuretic hormone. Am J Med 1967; 42: 790–806.
24. Gardenswartz MH, Berl T. Drug induced changes in waterexcretion. The Kidney 1981; 14: 19–23.
25. DeVita MV, Gardenswartz MH, Konecky A et al. Incidenceand etiology of hyponatremia in an intensive care unit. ClinNephrol 1990; 34: 163–166.
26. Lathem W. Hyperchloremic acidosis in chronic pyelone-phritis. N Engl J Med 1958; 258: 1031–1036.
27. Adler S, Lindeman RD, Yiengst MJ et al. Effect of acute acidloading on urinary acid excretion by the aging human kidney.J Lab Clin Med 1968; 72: 278–289.
28. Tan SY, Burton M. Hyporeninemic hypoaldosteronism. ArchInt Med 1981; 141: 30–33.
29. Nadler JL, Lee FO, Hsueh W et al. Evidence of prostacyclindeficiency in the syndrome of hyporeninemic hypoaldostero-nism. N Engl J Med 1986; 314: 1015–1020.
30. Oh MS, Carroll HJ, Clemmons JE et al. A mechanism forhyporeninemic hypoaldosteronism in chronic renal disease.Metabolism 1974; 23: 1157–1166.
31. Sanjad SA, Keenan BS, Hill LL. Renal hypoprostaglandism,hypertension, and type IV renal tubular acidosis reversed byfurosemide. Ann Int Med 1983; 99: 624–627.
32. Muller FB, Sealey JE, Case DB et al. The captopril test foridentifying renovascular disease in hypertensive patients. AmJ Med 1986; 80: 633–644.
33. Chan R, Michelis MF. The ageing kidney: practical con-siderations in the management of the elderly patient withrenal disease. In: Andreucci VE, Fine LG (eds) InternationalYearbook of Nephrology. London: Springer Verlag, 1992:179–195.
34. Kane RL, Ouslander JG, Abrass IB. Aging and pharmacology.In: Essentials of clinical geriatrics. U.S.A.: McGraw-Hill,1994: 358–371.
35. Bender AD. Effect of age on intestinal absorption: implica-tions for drug absorption in the elderly. J Am Geriatr Soc1968; 16: 1331–1339.
36. Montamat S, Cusack B, Vestal RE. Management of drugtherapy in the elderly. N Engl J Med 1989; 321: 303–309.
37. Williams L, Lowenthal DT. Drug therapy in the elderly.Southern Medical Journal 1992; 85: 127–131.
38. Antacid Drug Interactions. In: Drug Interactions & UpdatesQuarterly. Applied Therapeutics, Inc. Vancouver, Washington1993, Chapter 22, pp. 137–151.
39. Tumer N, Scarpace PJ, Lowenthal DT. Geriatric pharmacol-ogy: basic and clinical considerations. Annu Rev PharmacolToxicol 1992; 32: 271–302.
40. Roskos KV, Guy RH, Maibach HI. Percutaneous absorptionin the aged. Dermatol Clin 1986; 4: 455–465.
41. Armstrong PW. Pharmacokinetic-hemodynamic studies oftransdermal nitroglycerin in congestive heart failure. J AmColl Cardiol 1987; 9: 420–425.
42. Sloan RW. Principles of drug therapy in geriatric patients. AmFam Phy 1992; 45: 2709–2718.
43. Greenblatt DJ. Reduced serum albumin concentration in theelderly: a report from the Boston Collaborative Drug Surveil-lance Program. J Am Geriatr Soc 1979; 27: 20–22.
44. Wallace SM, Verbeeck RK. Plasma protein binding of drugsin the elderly. Clin Pharmacokinet 1987; 12: 41–72.
45. Abernethy DR, Kerznel L. Age effects on alpha-1-acid glyco-protein concentrations and imipramine plasma protein bind-ing. J Am Geriatr Soc 1984; 32: 705–708.
46. Iselius L, Evans DA. Formal genetics of isoniazid metabolismin man. Clin Pharmacokinet 1983; 8: 541–544.
47. Steiner E, Bertilsson L, Sawe J et al. Polymorphic debrisoquinhydroxylation in 757 Swedish subjects. Clin Pharmacol Ther1988; 44: 431–435.
48. Hunt CM, Westerkam WR, Stave GM. Effect of age andgender on the activity of human hepatic CYP3A. BiochemicalPharmacology 1992; 44: 275–283.
49. Vestal RE, Cusack BJ, Mercer GD et al. Age and drug inter-actions. I. Effect of cimetidine and smoking on the oxidationof theophylline and cortisol in healthy men. J Pharmacol ExpTher 1987; 241: 488–500.
50. Bach B, Hansen JM, Kampmann JP. Disposition of antipyrineand phenytoin correlated with age and liver volume in man.Clin Pharmacokinet 1981; 6: 389–396.
51. Wood AJ, Vestal RE, Wilkinson GR et al. Effect of agingand cigarette smoking on antipyrine and indocyanine greenelimination. Clin Pharmacol Ther 1979; 26: 16–20.
52. Wynne HA, Cope LH, Mutch E et al. The effect of age uponliver volume and apparent liver blood flow in healthy men.Hepatology 1989; 9: 297–301.
53. Mansoor G, Panner BJ, Ornt DB. Azithromycin-inducedacute interstitial nephritis [letter]. Annals Int Med 1993; 119:636–637.
54. Bailey J, Trott SA, Philbrick JT. Ciprofloxacin-induced acuteinterstitial nephritis. Am J Nephrol 1992; 12: 271–273.
55. Appel GB, Neu HC. The nephrotoxicity of antimicrobialagents. New Engl J Med 1977; 296: 663–670.
56. Sica DA, Cutler RE, Parmer RJ et al. Comparison of thesteady-state pharmacokinetics of fosinopril, lisinopril andenalapril in patients with chronic renal insufficiency. ClinPharmacokinet 1991; 20: 420–427.
57. Drusano GL, Munice HL Jr, Hoopes JM et al. Commonly usedmethods of estimating creatinine clearance are inadequate forelderly debilitated nursing home patients. J Am Geriatr Soc1988; 36: 437–441.
58. Andreasen F, Hansen V, Husted SE et al. The influence ofage on renal and extrarenal effects of frusemide. Br J ClinPharmacol 1984; 18: 65–74.
59. Abernethy DR, Schwartz JB, Todd EL et al. Verapamil phar-macodynamics and disposition in young and elderly hyper-tensive patients. Ann Intern Med 1986; 105: 329–336.
60. Psaty B, Savage PJ, Tell GS et al. Temporal patterns ofantihypertensive medication use among elderly patients: theCardiovascular Healthy Study. JAMA 1993; 270: 1837–1841.
61. JNC V. The fifth report of the joint national committee ondetection, evaluation, and treatment of high blood pressure.NIH Publication No. 93–1088, 1993.
62. SOLVD Investigators. Effect of enalapril on mortality and thedevelopment of heart failure in asymptomatic patients withreduced left ventricular ejection fraction. N Engl J Med 1992;327: 685–691.
63. Muiesan ML, Agabiti-Rosei E, Romanelli G et al. Beneficialeffects of one year’s treatment with captopril on left ventric-

41
ular anatomy and function in hypertensive patients with leftventricular hypertrophy. Am J Med 1988; 84: 129–132.
64. Pfeffer MA, Braunwald E, Moye LA et al. Effect of captoprilon mortality and morbidity in patients with left ventriculardysfunction after myocardial infarction. Results of the sur-vival and ventricular enlargement trial. The SAVE Investiga-tors. N Engl J Med 1992; 327: 669–677.
65. Keane WF, Anderson S, Aurell M et al. Angiotensin convert-ing enzyme inhibitors and progressive renal insufficiency,current experience and future directions. Annals Int Med1989; 111: 503–516.
66. Bjorck S, Mulec H, Johnsen SA et al. Renal protective effectof enalapril in diabetic nephropathy. British Medical Journal1992; 304: 339–343.
67. Ravid M, Savin H, Jutrin I et al. Long-term stabilizing effectof angiotensin-converting enzyme inhibition on plasma crea-tinine and on proteinuria in normotensive type II diabeticpatients. Annal of Int Med 1993; 118: 577–581.
68. Lewis EJ, Hunsicker LG, Bain RP et al. The effectof angiotensin-converting-enzyme inhibition on diabeticnephropathy. N Engl J Med 1993; 329: 1456–1462.
69. Chagnac A, Korzets A, Zevin D et al. Effect of enalapril onthe microvascular albumin leakage in patients with diabeticmicroangiopathy and normal or mildly elevated blood pres-sure. Clin Nephrol 1994; 41: 144–148.
70. Viberti G, Mogensen CE, Groop LC et al. Effect of captoprilon progression to clinical proteinuria in patients with insulin-dependent diabetes mellitus and microalbuminuria. JAMA1994; 271: 275–279.
71. Palmer BF. The renal tubule in the progression of chronicrenal failure. Journal of Investigative Medicine 1997; 45(6):346–361.
72. Perico N, Lapinski R, Konopka K et al. Platelet-activatingfactor mediates angiotensin II-induced proteinuria in isolatedperfused rat kidney. J Am Soc Nephrol 1997; 8(9): 1391–1398.
73. Materson BJ, Preston RA. Angiotensin-converting enzymeinhibitors in hypertension, a dozen years of experience. ArchIntern Med 1994; 154: 513–523.
74. Israili ZH, Hall WD. Cough and angioneurotic edema asso-ciated with angiotensin-converting enzyme inhibitor therapy:a review of the literature and pathophysiology. Ann InternMed 1992; 117: 234–242.
75. Lunde H, Hedner T, Samuelsson O et al. Dyspnoea, asthma,and bronchospasm in relation to treatment with angiotensinconverting enzyme inhibitors. British Medical Journal 1994;308: 18–21.
76. Gilleaudeau P, Vallat VP, Carter DM et al. Angiotensin-converting enzyme inhibitors as possible exacerbating drugsin psoriasis. J Am Acad Dermatol 1993; 28: 490–492.
77. Hricik DE, Browning PJ, Kopelman R. Captopril-inducedfunctional renal insufficiency in patients with bilateral renal-artery stenoses or renal artery stenosis in a solitary kidney. NEngl J Med 1983; 308: 373–376.
78. Warner NJ, Rush JE, Keegan ME. Tolerability of enalaprilin congestive heart failure. Am J Cardiol 1989; 63: 33D–37D.
79. Bridoux F, Hazzan M, Pallot JL et al. Acute renal failureafter the use of angiotensin-converting-enzyme inhibitors inpatients without renal artery stenosis. Nephol Dial Transplant1992; 7: 100–104.
80. Toto RD, Mitchell HC, Lee HC et al. Reversible renal insuf-ficiency due to angiotensin converting enzyme inhibitors in
hypertensive nephrosclerosis. Ann Int Med 1991; 115: 513–519.
81. Mandal AK, Markert RJ, Saklayen MG et al. Diuretics poten-tiate angiotensin converting enzyme inhibitor-induced acuterenal failure. Clin Nephrol 1994; 42: 70–75.
82. Devoy MAB, Tomson CRV, Edmunds ME et al. Deteriora-tion in renal function associated with angiotensin convertingenzyme inhibitor therapy is not always reversible. J Int Med1992; 232: 493–498.
83. Gentric A, Duquesne F, Cledes J. Incidence, causes, prognosisof renal failure in old patients admitted in an Internal MedicineUnit. Geriatr Nephrol Urol 1993; 3: 151–154.
84. DeVita MV, Han H, Chan R et al. Drug use and the elderlyin relation to changing etiologies of hyperkalemia. GeriatrNephrol Urol 1991; 1: 41–45.
85. Atarashi K, Mulrow PJ, Franco-Saenz R. Effect of atrialpeptides on aldosterone production. J Clin Invest 1985; 76:1807–1811.
86. Obana K, Naruse M, Naruse K et al. Synthetic rat atrial natri-uretic factor inhibitsin vitro and in vivo renin secretion inrats. Endocrinology 1985; 117: 1282–1284.
87. Bahr V, Sander-Bahr C, Ardevol R et al. Effects of atrialnatriuretic factor on the renin-aldosterone system:in vivoand in vitro studies. J Steroid Biochem Mol Biol 1993; 45:173–178.
88. Williams GH. Converting-enzyme inhibitors in the treatmentof hypertension. N Engl J Med 1988; 319: 1517–1525.
89. Buhler FR, Laragh JH, Vaughan FD Jr et al. Antihypertensiveaction of propranolol: specific antirenin responses in highand normal renin forms of essential, renal, renovascular andmalignant hypertension. Am J Cardiol 1972; 29: 633–640.
90. Garella S, Matarese RA. Renal effects of prostaglandinsand clinical adverse effects of nonsteroidal anti-inflammatoryagents. Medicine 1984; 63: 165–181.
91. Clive DM, Gurwitz JH, Rossetti RG. Potassium homeostasiswith indomethacin therapy in normal subjects. Am J Kid Dis1992; 19: 16–21.
92. Pearce CJ, Gonzalez FM, Wallin JD. Renal failure and hyper-kalemia associated with ketorolac tromethamine. Archives ofInternal Medicine 1993; 153: 1000–1002.
93. DeFronzo RA. Hyperkalemia and hyporeninemic hypoaldos-teronism. Kid Int 1980; 17: 118–134.
94. Tomita DK, Kennedy DL, Baum C et al. Drug utilization inthe United States – 1988: 10th Annual Review. Washington,DC: Department of Health and Human Services, November1989.
95. Murray MD, Brater DC. Adverse effects of nonsteroidal anti-inflammatory drugs on renal function [Ed] Ann Int Med 1990;112(8): 559–560.
96. Kafetz K. Nonsteroidal anti-inflammatory drugs and renalfunction in elderly people. Geriatr Nephrol Urol 1992; 1:213–217.
97. Lewis HJ. Hepatic toxicity of nonsteroidal anti-inflammatorydrugs. Clin Pharmacy 1984; 3: 128–138.
98. Carson JL, Strom BL, Soper KA. The association of non-steroidal anti-inflammatory drugs with upper gastrointestinaltract bleeding. Arch Intern Med 1987; 147: 85–88.
99. Griffin MR, Ray WA, Schaffner W. Nonsteroidal anti-inflammatory drug use and death from peptic ulcer in elderlypersons. Ann Intern Med 1988; 109: 359–363.
100. Asokan A, Fancourt GJ, Bennett SE et al. Renalprostaglandins, effective renal plasma flow and glomerularfiltration rate in healthy elderly subjects. Age & Aging 1992;21: 39–42.

42
101. Cooper K, Bennett W. Nephrotoxicity of common drugs usedin clinical practice. Arch Intern Med 1987; 147: 1213–1218.
102. Favre L, Glasson P, Vallotton MD. Reversible acute renalfailure from combined triamterene and indomethacin. AnnIntern Med 1982; 96: 317–320.
103. Clive DM, Stoff JS. Renal syndromes associated with non-steroidal antiinflammatory drugs. N Engl J Med 1984; 310:563–572.
104. Blackshear JL, Davidman M, Stillman MT. Identifica-tion of risk for renal insufficiency from nonsteroidalanti-inflammatory drugs. Arch Intern Med 1983; 143: 1130–1134.
105. Schnermann J, Briggs JP, Weber PC. Tubuloglomerular feed-back, prostaglandins, and angiotensin in the autoregulationof glomerular filtration rate. Kidney Int 1984; 25: 53–64.
106. Anderson RJ, Berl T, McDonald KM et al. Evidence for anin vivo antagonism between vasopressin and prostaglandin inthe mammalian kidney. J Clin Invest 1975; 56: 420–426.
107. Tan SY, Shapiro R, Franco R et al. Indomethacin-inducedprostaglandin inhibition with hyperkalemia: a reversiblecause of hyporeninemic hypoaldosteroinism. Ann Intern Med1979; 90: 783–785.
108. Brezin JH, Katz SM, Schwartz AB et al. Reversible renalfailure and nephrotic syndrome associated with nonsteroidalanti-inflammatory drugs. N Engl J Med 1979; 301: 1271–1273.
109. Katz SM, Capaldo R, Everts EA et al. Tolmetin: associationwith reversible renal failure and acute interstitial nephritis.JAMA 1981; 246: 243–245.
110. Carmichael J, Shankel SW. Effects of nonsteroidal anti-inflammatory drugs on prostaglandins and renal function. AmJ Med 1985; 78: 992–1000.
111. Porile JL, Bakris GL, Garella S. Acute interstitial nephritiswith glomerulopathy due to nonsteroidal anti-inflammatoryagents: a review of its clinical spectrum and effects of steroidtherapy. J Clin Pharmacol 1990; 30(5): 468–475.
112. Sandler DP, Burr FR, Weinberg CR. Nonsteroidal anti-inflammatory drugs and the risk for chronic renal disease.Ann Int Med 1991; 115: 165–172.
113. Wagner EH. Nonsteroidal anti-inflammatory drugs and renaldisease – still unsettled. Ann Int Med 1991; 115: 227–228.
114. Wen SF, Parthasarathy R, Iliopoulos O et al. Acute renalfailure following binge drinking and nonsteroidal antiinflam-matory drugs. Am J Kid Diseases 1992; 20: 281–285.
115. Brooks PM, Day RO. Nonsteroidal antiinflammatory drugs– differences and similarities. N Engl J Med 1991; 324(24):1716–1725.
116. Ciabattoni G, Cinotti GA, Pierucci A et al. Effects of sulindacand ibuprofen in patients with chronic glomerular disease.Evidence for the dependence of renal function on prostacy-clin. N Engl J Med 1984; 310: 279–283.
117. Whelton A, Stout RL, Spilman PS et al. Renal effects ofibuprofen, piroxicam, and sulindac in patients with asymp-tomatic renal failure. A prospective, randomized, crossovercomparison. Ann Int Med 1990; 112: 568–576.
118. Bonney SI, Northington RS, Hedrich DA et al. Renal safety oftwo analgesics used over the counter: Ibuprofen and aspirin.Clin Pharmacol Ther 1986; 40: 373–377.
119. Gurwitz JH, Avorn J, Ross-Degnan D et al. Nonsteroidalanti-inflammatory drug-associated azotemia in the very old.JAMA 1990; 264: 471–475.
120. Linton AL, Clark WF, Driedger AA et al. Acute interstitialnephritis due to drugs. Review of the literature with a reportof nine cases. Ann Int Med 1980; 93: 735–741.
121. Baldwin DS, Levine BB, McCluskey RT et al. Renal failureand interstitial nephritis due to penicillin and methicillin. NewEngl J Med 1968; 279: 1245–1252.
122. Galpin JE, Shinaberger JH, Stanley TM et al. Acute interstitialnephritis due to methicillin. Am J Med 1978; 65: 756–765.
123. Bergman MM, Glew RH, Ebert TH. Acute interstitialnephritis associated with vancomycin therapy. Arch InternMed 1988; 148: 2139–2140.
124. Nguyen VD, Nagelberg H, Agarwal BN. Acute interstitialnephritis associated with cefotetan therapy. Am J Kidney Dis1990; 16: 259–261.
125. Rastogi, S, Atkinson JLD, McCarthy JT. Allergic nephro-pathy associated with ciprofloxacin. Mayo Clin Proc 1990;65: 987–989.
126. Lien YH, Hansen R, Kern WF et al. Ciprofloxacin-inducedgranulomatous interstitial nephritis and Department of Medi-cine, University of Arizona Health Sciences. Am J KidneyDis 1993; 22: 598–602.
127. D’Agati VD, Theise ND, Pirani CL et al. Interstitial nephritisrelated to nonsteroidal anti-inflammatory agents and beta-lactam antibiotics: a comparative study of the interstitialinfiltrates using monoclonal antibodies. Mod Pathol 1989;2: 390–396.
128. Ten RM, Torres VE, Milliner DS et al. Acute interstitialnephritis: immunologic and clinical aspects. Mayo Clin Proc1988; 63: 921–930.
129. Yoshioka K, Hino S, Takemura T et al. Isolation and character-ization of the tubular basement membrane antigen associatedwith human tubulo-interstitial nephritis. Clin Exp Immunol1992; 90: 319–325.
130. John K, Aizawa S, Yamaguchi Y et al. Drug-induced hyper-sensitivity nephritis: lymphocyte stimulation testing and renalbiopsy in 10 cases. Am J Nephrol 1990; 10: 222–230.
131. Ten RM, Torres VE, Kephart GM et al. Localization ofeosinophil major basic protein (MBP) in kidney diseases(abstract). Kidney Int 1987; 31: 339.
132. Corwin HL, Bray RA, Haber MH. The detection and inter-pretation of urinary eosinophils. Arch Pathol Lab Med 1989;113: 1256–1258.
133. Nolan CH, Angel M, Kelleher A. Eosinophiluria: a newmethod of detection and definition of the clinical spectrum.N Engl J Med 1986; 315: 1516–1519.
134. Landais P, Goldfarb B, Kleinknecht D. Eosinophiluria anddrug-induced acute interstitial nephritis. [letter] N Engl J Med1987; 316: 1664.
135. Wilson DM, Salazer T, Farkouh ME. Eosinophiluria inatheroembolic renal disease. Am J Med 1991; 91: 186–189.
136. Ruffing DA, Hoppes P, Blend D et al. Eosinophilis in urinerevisited. Clin Nephrol 1994; 41: 163–166.
137. Cotran RS, Rubin RH, Tolkoff-Rubin NE. Tubulointerstitialdiseases. In: Brenner BM, Rector FC Jr (eds) The Kidney.Philadelphia PA: Saunders, 1986: 1143–1173.
138. Revert L, Montoliu J. Acute interstitial nephritis. SeminNephrol 1988; 8(1): 82–88.
139. Finkelstein MS. Aging immunocytes and immunity. Charac-teristics and significance. Clin Geriatr Med 1985; 1: 899–911.
140. Sigala JF, Biava CG, Hulter HN. Red blood cell casts inacute interstitial nephritis. Arch Intern Med 1978; 138: 1419–1421.
141. Lins RL, Verpooten GA, De Clerck DS et al. Urinary indicesin acute interstitial nephritis. Clin Nephrol 1986; 26: 131–133.

43
142. Braden GL, Germain MJ, Fitzgibbons JP. Impaired potas-sium and magnesium homeostasis in acute tubulo-interstitialnephritis. Nephron 1985; 41: 273–278.
143. Ivanyi B, Marcussen N, Kemp E et al. The distal nephron ispreferentially infiltrated by inflammatory cells in acute inter-stitial nephritis. Virchows Arch A Pathol Anat Histopathol1992; 420: 37–42.
144. Kourilsky O, Morel-Maroger L, Richet G. Renal biopsyin acute renal failure: its indications and usefulness. In:Andreucci VE (ed) Acute Renal Failure: Pathophysiology,Prevention, and Treatment. Boston, MA: Martinus Nijhoff,1984: 201–204.
145. Parrish AE. Complications of percutaneous renal biopsy: areview of 37 years’ experience. Clin Nephrol 1992; 38: 135–141.
146. Dworsky R, Paganini-Hill A, Arthur M et al. Immuneresponses of healthy humans 83–104 years of age. J NatlCancer Inst 1983; 71: 265–268.
147. Meys E, Devogelaer JP, Geubel A et al. Fever, hepatitisand acute interstitial nephritis in a patient with rheuma-toid arthritis. Concurrent manifestations of azathioprinehypersensitivity. J Rheumatol 1992; 19: 807–809.
148. Choy EH, Kingsley GH, Panayi GS. Treatment with anti-CD4monoclonal antibody and acute interstitial nephritis. ArthritisRheum 1993; 36: 723–724.
149. Christensen P, Albersen KE, Jensen P. Renal failure afteromeprazole (letter). Lancet 1993; 341: 55.
150. Gaughan WJ, Sheth VR, Francos GC et al. Ranitidine-inducedacute interstitial nephritis with epithelial cell foot processfusion. Am J Kidney Dis 1993; 22: 337–340.
151. Frankel RS, Richman SD, Levenson SM et al. Renallocalization of gallium-67 citrate. Radiology 1975; 114:393–397.
152. Zucchelli P, Zuccala A. Primary hypertension – how does itcause renal failure? Nephrol Dial Transplant 1994; 9: 223–225.
153. Gilbert DN, Gourley R, D’Agostino A et al. Interstitialnephritis due to methicillin, penicillin, and ampicillin. Allergy1970; 28: 378.
154. Pusey CD, Saltissi D, Bloodworth L et al. Drug associatedacute interstitial nephritis: Clinical and pathological featuresand the response to high dose steroid therapy. QJ Med 1983;206: 194–211.
155. Koselj M, Kveder R, Bren AF et al. Acute renal failure inpatients with drug-induced acute interstitial nephritis. RenalFailure 1993; 15: 69–72.
156. Levin ML. Patterns of tubulo-interstitial damage associatedwith nonsteroidal antiinflammatory drugs. Semin Nephrol1988; 8: 55–61.
157. Detre K, Holubker R, Kelsey S et al. Percutaneous trans-luminal coronary angioplasty in 1985–1986 and 1977–1981:The national heart, lung, and blood institute registry. N EnglJ Med 1988; 318: 265–270.
158. Rich MW, Baird J, Rothstein M, Creceliu CA. Renal risks ofcardiac catheterization in the elderly. Geriatr Nephrol Urol1992; 2: 43–49.
159. Brown PWG, Haylor JL, El Nahas AM et al. The functionaleffects of contrast media on the isolated perfused rat kidney.Contrib Nephrol 1993; 101: 235–240.
160. Harris KG, Smith TP, Cragg AH et al. Nephrotoxicity fromcontrast material in renal insufficiency: ionic versus non-ionicagents. Radiology 1991; 179: 849–852.
161. Taliercio CP, Vliestra RE, Ilstrup DM et al. A randomizedcomparison of the nephrotoxicity of iopamidol and diatrizoate
in high risk patients undergoing cardiac angiography. J AmCol Cardiol 1991; 17: 384–390.
162. Berns JS, Rudnick MR. Radiocontrast media associatednephrotoxicity. The Kidney 1992; 24: 1–4.
163. Koutsikos DK, Konstadinidou IK, Kapetanaki AI et al.Nephrotoxicity of contrast media in persons over the ageof 60. Geriatr Nephrol Urol 1993; 3: 127–131.
164. Byrd L, Sherman RL. Radiocontrast-induced acute renalfailure: a clinical and pathophysiologic review. Medicine1979; 58: 270–279.
165. Manske CL, Sprafka JM, Strony JT et al. Contrast nephro-pathy in azotemic diabetic patients undergoing coronaryangiography. Am J Med 1990; 89: 615–620.
166. Larson TS, Hudson K, Mertz JI et al. Renal vasoconstrictiveresponse to contrast medium. J Lab Clin Med 1983; 101:385–391.
167. Margulies KB, Hildebrand FL, Heublein DM et al. Radio-contrast increases plasma and urinary endothelin. J Am SocNephrol 1991; 2: 1041–1045.
168. Heymann SN, Clark BA, Kaiser N et al. Radiocontrast agentsinduce endothelin releasein vivo and in vitro. J Am SocNephrol 1992; 3: 58–65.
169. Erley CM, Duda SH, Schlepckow S et al. Adenosine antago-nist theophylline prevents the reduction of glomerular filtra-tion rate after contrast media application. Kid Int 1994; 45:1425–1431.
170. Berns AS. Nephrotoxicity of contrast media. Kid Int 1989;36: 730–740.
171. Barrett BJ, Parfrey PS, Vavasour HM et al. Contrast nephro-pathy in patients with impaired renal function: high versuslow osmolar media. Kid Int 1992; 41: 1274–1279.
172. Barrett BJ, Carlisle E. Metaanalysis of the relative nephro-toxicity of high- and low-osmolality iodinated contrast media.Radiology 1993; 188: 171–178.
173. Anto HR, Chou SY, Porush JG et al. Intravenous infusionpyelography and renal function effects of hypertonic mannitolin patients with chronic renal insufficiency. Arch Intern Med1981; 141: 1652–1656.
174. Teruel JL, Marcen R, Herrero JA et al. An easy and effectiveprocedure to prevent radiocontrast agent nephrotoxicity inhigh risk patients. Nephron 1989; 51: 282.
175. Rudnick MR, Goldfarb S, Murphy MJ. Mannitol and otherprophylactic regimens in contrast media-induced acute renalfailure. Coronary Artery Disease 1991; 2: 1047–1052.
176. Weinstein JM, Heyman S. Potential deleterious effect offurosemide in radiocontrast nephropathy. Nephron 1992; 62:413–415.
177. Pfaffle AE, Moses JW, Chan R et al. Negative fluid balanceand the occurrence of radiocontrast associated acute renalfailure. Geriatr Nephrol Urol 1994; 4: 60–64.
178. Solomon R, Werner C, Mann D et al. Effects of saline,mannitol, and furosemide to prevent acute decreases in renalfunction induced by radiocontrast agents. N Engl J Med 1994;331(21): 1416–1420.
179. Mehta RP. Acute interstitial nephritis due to 5-aminosalicyclicacid. Can Med Asoc J 1990; 153: 1031–1032.
180. Rashed A, Azadeh B, Abu Romeh SH. Acyclovir-inducedacute tubulo-interstitial nephritis. Nephron 1990; 56: 436–438.
181. Smith WR, Neill J, Cushman WC et al. Captopril-associatedacute interstitial nephritis. Am J Nephrol 1989; 9: 230–235.
182. Sadjadi SA, McLaughlin K, Shah RM. Allergic interstitialnephritis due to diazepam. Arch Intern Med 1987; 147:579.

44
183. Feehally J, Wheeler DC, Mackay EH et al. Recurrent acuterenal failure with interstitial nephritis due to D-penicillamine.Renal Failure 1987; 10: 55–57.
184. Garcia-Martin F, Mampaso F, de Arriba G et al. Acute intersti-tial nephritis induced by ethambutol [letter]. Nephron 1991;59: 679–680.
185. Newstead CG, Moore RH, Barnes AJ. Interstitial nephritisassociated with indapamide. B Med J 1990; 300: 1344.
Address for correspondence:Richard Chan100 East 77th StreetNew York, N.Y. 10021, U.S.A.Tel.: (212) 794-2117