Embed Size (px)
Citation preview

7/20/2015
1
Board Review Course & Update
Nephrolithiasis
Orson W. Moe, M.D.
Department of Internal Medicine
University of Texas Southwestern Medical Center
Dallas, TX, USA
July 25 - 31, 2015 | Chicago, IllinoisAcknowledgements and Disclosures
•Research support: National Institutes of Health, American Society of Nephrology
Simmons Family Foundation, Charles and Jane Pak Foundation
•Paid consultations for industry (past 4 years):Abbvie, Allena, Amgen, Ardelyx, Sanofi, Takeda
•Co-inventor of patent (Meta Pharm products):Potassium Magnesium Citrate, Calcium Magnesium Citrate, Synthetic anti-Klotho antibody
Professor G. Elliot Smith, 1901
Calcium oxalate 75%
Magnesium oxalate 9%
Magnesium ammonium phosphate 6%
Carbonate apatite 4%
Uric acid 3%
4800 BCE
Professor S.G. Shattock, 1905
Oldest documented human stone
6700 year old
post-mortem exam
General ConceptsGeneral Concepts

7/20/2015
2
A systemic disease
Kidney stones
OH
OHHO
Nephrolithiasis Nephrocalcinosis≠
Intratubular deposits Interstitial depositsOverlap
Nephrolithiasis Nephrocalcinosis≠Cortical
Medullary
Glomerulonephritis
Alport’s syndrome
Acute cortical necrosis
Hemolytic-uremic syndrome
Tuberculosis
Acute transplant rejection
Pyelonephritis
Medullary sponge kidney
Hypercalcemic states
Hyperparathyroidism
Distal renal tubular acidosis
Furosemide therapy in infants
Bartter syndrome
Ethylene glycol toxicity
Vitamin D toxicity
Over-aggressive phosphate therapy
Primary hyperoxaluria
Medullary sponge kidney
Hypercalcemic states
Hyperparathyroidism
Distal renal tubular acidosis
Furosemide therapy in infants
Bartter syndrome
Ethylene glycol toxicity
Vitamin D toxicity
Over-aggressive phosphate therapy,
Primary hyperoxaluria.
Agenda
• General concepts
• Epidemiology
• Pathogenesis & Etiology
• Evaluation
• Treatment
General concepts
Epidemiology
Pathogenesis & Etiology
Evaluation
Treatment

7/20/2015
3
Epidemiology
Magnitude of the problem
• Annual incidence
• Lifetime risk 10-20%
2-7%• Prevalence
0.6-1.5%
• Geographic variations: Stone belts
World stone belt
USA stone belt
2000Projection:
Pearle et al. PNAS 2009
2050
2095
Magnitude of the problem
• Annual incidence
• Lifetime risk 10-20%
2-7%• Prevalence
0.6-1.5%
• Geographic variations: Stone belts
• Caucasians > Hispanics and Asians > Blacks
•Male > females
• Incidence rising in the USA, EU, and Asia

7/20/2015
4
20051995199019851980197519711965
1 2 3 4 5 6 7 8 9 Decade of life
350-
300-
200-
100-
0-
350-
300-
200-
100-
0-
20051995199019851980197519711965
1 2 3 4 5 6 7 8 9 Decade of life
Romero et al. Rev Urol 2010
Urolithiasis: Increase in time
Pe
r 1
00
,00
0P
er
10
0,0
00
Magnitude of the problem
• Annual incidence
• Lifetime risk 10-20%
2-7%• Prevalence
0.6-1.5%
• Economic impact $2.1 billion(Evaluation and treatment)
• Geographic variations: Stone belts
• Caucasians > Hispanics and Asians > Blacks
•Male > females
• Incidence rising in the USA, EU, and Asia
(N = 322,556)
Without nephrolithiaisis(N = 318,956)
With nephrolithiaisis(N = 3600)
All $3,038 $6,532Age
18-44 $2,809 $6,114
45-54 $3,278 $7,093
55-64 $3,123 $6,525
Gender
Male $2,808 $6,302
Female $3,331 $6,825
Region
Northeast $2,948 $6,442
Midwest $2,962 $6,456
South $3,152 $6,647
West $2,978 $6,472
Saigal et al. Kidney International 2005
Annual expenditure 2000
Melton et al. Kidney International 1998
Stone formers
Non-stone formers
Fractures 11,909 person-years1950-1974
Minnesota study

7/20/2015
5
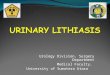
Human kidney stone composition and relative occurrence
Calcareous
Non-CalcareousHydroxyapatite
(20%) Uric Acid
(60%)
(9%)
(7%)
Ammonium Urate
Protease Inhibitors
Xanthine
Brushite (3%)
Calcium Oxalate
Struvite
Cystine
Pathogenesis and Etiology
2. Inhibitor-promoter
imbalance
Renal Tubule LumenRenal Interstitium
3. Calcium
phosphate
deposits
Excessive Solutes1.
3. Nidus for anchor
Crystalluria per se is not a disease
Randall’s plaque
Naked plaque Plaque with small
stones
Large stones
overlaying plaqueUnderlying plaque
after stone removal
Andy Evan, Jim Lingeman, and Fred Coe, U Chicago and Indiana University
Yasue stain of calcium Transmission EM

7/20/2015
6
2. Inhibitor-promoter
imbalance
Renal Tubule LumenRenal Interstitium
3. Calcium
phosphate
deposits
Excessive Solutes1.
3. Nidus for anchor
Rx
Rx
Kidney stones
Pathophysiology
Etiologies
Predisposing
conditions
Condition Stone typeCalcium
oxalate
Calcium
phosphate
Uric acid Struvite Cystine Drugs
Environmental/Dietary
Low urine volume + + + + + +
High protein diet + +
High salt diet +
Metabolic
Primary hyperparathyroidism + +
Granulomatous diseases +
Metabolic acidosis + +
Metabolic syndrome/gout/type 2
diabetes
+
Hyperuricosuric conditions + +
Intestinal diseases +
Chronic diarrheal states + +
Fat malabsorption +
Post Bariatric surgery + +
Idiopathic
Hypercalciuria + +
Hyperoxaluria +
Congenital syndromes
Renal tubular acidosis +
Cystinuria +
Primary hyperoxaluria +
Urinary tract infection +
Medications
Drugs that alter urine chemistry + + +
Insoluble drug +
Evaluation

7/20/2015
7
Do nothing Do everything
EvaluationDo nothing
Recurrence rate
• 10 years ~ 50-65%
• 20 years ~ 70-85%
Blanket Rx
• Drink water
• Decrease salt and protein
• Alkali Rx
Do something
1. Uncover underlying conditions- treatable !
2. Associated conditions that need attention e.g. low bone density
3. Guide prescription- Tailored therapy
4. Follow efficacy of therapy
Evaluation
3. Blood4. Urine
2. Imaging
1. Stone analysis
1. Stone analysis

7/20/2015
8
Evaluation
1. Stone analysis
Stone strainer
CaOx Calcium oxalate monohydrate Ca (COO)2·H2O
Calcium oxalate dihydrate Ca (COO)2·2H2O
CaP Brushite CaHPO4·2H2O
Hydroxyapatite Ca10(PO4)6(OH)2
Uric Acid Uric acid C5H4N4O3
Sodium urate NaC5H4N4O3
Struvite Magnesium ammonium urate NH4MgPO4·6H2O
Cystine Cystine (SCH2CH(NH2)CO2H)2
Others
Condition Stone typeCalcium
oxalate
Calcium
phosphate
Uric acid Struvite Cystine Drugs
Environmental/Dietary
Low urine volume + + + + + +
High protein diet + +
High salt diet +
Metabolic
Primary hyperparathyroidism + +
Granulomatous diseases +
Metabolic acidosis + +
Metabolic syndrome/gout/type 2
diabetes
+
Hyperuricosuric conditions + +
Intestinal diseases +
Chronic diarrheal states + +
Fat malabsorption +
Post Bariatric surgery + +
Idiopathic
Hypercalciuria + +
Hyperoxaluria +
Congenital syndromes
Renal tubular acidosis +
Cystinuria +
Primary hyperoxaluria +
Urinary tract infection +
Medications
Drugs that alter urine chemistry + + +
Insoluble drug +
Evaluation
2. Imaging
3. Blood4. Urine
1. Stone analysis
2. Imaging
Evaluation
2. Imaging
Kidneys Ureters and Bladder X-ray (KUB)
Limited sensitivity and specificity (60-77%). Cannot see UA, xanthine,
and 2,8-dihyroxyadenine (2,8-DHA) stones. Simple. Follow up
Ultrasound
See radio-opaque and radio-luscent stones
Non-invasive. No radiation: children, pregnant women
False positive and negative diagnosis of obstruction.
Computerized tomography
All stones except indinavir stones, visualized by non contrast CT.
High sensitivity and specificity. As small as 1mm.
Significant radiation exposure
Intravenous pyelogram
Use has diminished.
Guide in percutaneous or endoureteral procedures.
Magnetic resonance imaging
Explored as an alternative to NCCT or IVP
Does not deliver ionizing radiation. High cost and limited availability.

7/20/2015
9
Evaluation
3. Blood4. Urine
2. Imaging
1. Stone analysis
3. Blood
Evaluation
3. Blood
Serum Chemistry • Na, K, Cl, HCO2, BUN, Cr, Glucose
• Ca, P, Uric Acid, Mg, Protein
• ALP, ALT, AST, Bilirubin, LDH, CK
CBC • Hb, WBC, Plt
Endocrine • PTH, 25-OH-Vitamin D
Lipid profile • Chol, TG, LDL, HDL
Evaluation
4. Urine3. Blood
2. Imaging
1. Stone analysis
4. Urine
Evaluation
4. Urine
UpH
5.0 5.5 6.0 6.5 7.0
Uric acid RTA Infection
Urinalysis
Cigar
Envelope
Coffin
Polygon
Amorphous

7/20/2015
10
Calcium Oxalate
Monohydrate
Calcium Oxalate
Dihydrate
Evaluation
4. Urine
Evaluation
4. Urine
Calcium phosphate
Evaluation
4. Urine
Uric Acid Cystine
Evaluation
4. Urine
Melamine
Acyclovir
Tyrosine
Sulphonamide
Leucine

7/20/2015
11
Evaluation
4. Urine24 hr urine
Guideline values
Metabolic Risk Factors Environmental Calculated
Volume >2 L Sodium <200 mEq Relative supersaturation
pH 5.5-6.5 Chloride <200 mEq
Calcium <250 mg (6.25 mmoles) Potassium >50 mEq Relative supersaturation
ratioOxalate <45 mg (0.5 mmoles) Magnesium >60 mg
Phosphate <1100 mg (>35 mmoles) Ammonium <45 mEq Saturation Index
Uric acid <700 mg (4.2 mmoles) Sulfate <30 mmoles
Citrate >320 mg (1.7 mmoles) Citrate >320 mg
Cystine <60 mg (0.25 mmoles)
Evaluation
4. Urine
Metabolic Risk Factors Environmental Calculated
Volume Universal. Intake & loss Sodium Calciuria Relative supersaturation
pH UA. CaOx. RTA. Infection Chloride Calciuria
Calcium CaOx and CaP Potassium Alkali intake Relative supersaturation
ratioOxalate CaOx Magnesium CaOx, CaP
Phosphate CaP Ammonium Acid excretion Saturation Index
Uric acid CaOx and UA Sulfate Acid intake
Citrate CaOx. CaP Citrate Acid-base
Cystine Cystine
24 hr urine
Interpretation
ParameterExpected Daily
ValuesInterpretation
Total Volume ≥ 2.5 L Diminishes with low fluid intake, sweating, and diarrhea.
pH 5.8-6.2 <5.5 increases risk of uric acid precipitation commonly found in uric acid stone patients, subjects with intestinal
disease and diarrhea, and in those with intestinal bypass surgery.
>6.7 increases risk of calcium phosphate precipitation seen in patients with dRTA, primary hyperparathyroidism,
alkali overtreatment, repeated shock wave lithotripsy.
>7.0-7.5 indicates a urinary tract infection as a result of urease-producing bacteria.
Creatinine 15-25 mg/kg
body weight
Gauges adequacy of collection. 15-20mg/kg body weight in females and 20-25mg/kg body weight in males.
Sodium 100 mEq Reflective of dietary sodium intake in the absence of excessive sweating and/or diarrhea. Can cause secondary
hypercalciuria.
Potassium 40-60 mEq Reflective of dietary potassium intake in the absence of diarrhea. A marker of dietary alkali intake.
Calcium ≤ 250-300 mg Direct risk factor and precipitating solute for calcium stones. Possible differences between male and female
subjects (higher value in males).
Magnesium ≥ mg Low urinary magnesium reflects low magnesium intake, intestinal malabsorption (small bowel disease), and
following bariatric surgery. Role as inhibitor is controversial.
Oxalate ≤ 45 mg Direct risk factor and precipitating solute for calcium oxalate stones. Seen in intestinal fat malabsorption and
sometimes following bariatric surgery. Values higher than 100 mg/day is suspicious of primary hyperoxaluria.
Phosphorus ≤1100 mg Indicative of dietary phosphorus intake and absorption. High excretion rate may increase the risk of calcium
phosphate stone. Conditions of renal phosphate leak can also lead to secondary hypercalciuria.
Uric Acid 600-800 mg Can contribute to uric acid stones when urine pH is low. Can also increase risk of calcium oxalate stones.
Encountered with the overindulgence of purine-rich foods. Values > 1000 mg may indicate rare enzyme
deficiencies.
Sulfate ≤ 25-30 mmol Sulfate is a marker of the acid content in the diet. Dietary acid intake is important to guide interpretation of urine
pH, citrate, ammonium excretion.
Citrate ≥ 320 mg Principal inhibitor of calcium stone formation. Hypocitraturia is encountered in states with intracellular acidosis
such as metabolic acidosis, dRTA, chronic diarrhea, excessive protein ingestion, frequent strenuous physical
exercise, potassium deficiency, carbonic anhydrase inhibitors and rarely with ACE-inhibitors.
Ammonium 30-40 mEq Ammonia is a major buffer which carries protons in the form of ammonium. Its excretion usually corresponds
with dietary acid load (marked by urinary sulfate). High ammonium:sulfate ratio indicates non-dietary acid load
such as GI alkali loss or high endogenous acid production.
Chloride 100 mEq Usually correspond with sodium intake and excretion. Renal sodium bicarbonate loss may lead to discrepancies
in urine sodium and chloride
Cystine ≤ 30-60 mg Limited urinary solubility at 250mg/L.
Interpretation of urinary biochemical profile
Treatment

7/20/2015
12
Kidney stones
Pathophysiology
Etiologies
Predisposing
conditions
RxDietary Pharmacologicand/or
• Pathophysiologic basis
• Metabolic studies
• Randomized clinical trials
Data
Type Risk Diet therapy Pharmacologic therapy
Calcium stones Low urine volume Fluid -
Hypercalciuria Salt and protein restriction Thiazide, alkali
Hyperoxaluria Oxalate restriction -
Hypocitraturia Protein restriction Alkali
Hyperuricosuria Protein/purine restriction Xanthine oxidase inhibitor
High urine pH * -
Uric acid stones Low urine pH Protein restriction Alkali
Low urine volume Fluid -
Hyperuricosuria Protein restriction Xanthine oxidase inhibitor
Cystine stones Low urine volume Fluid
Cystinuria Methionine and salt
restriction
Tiopronin
D-penicillamine
Low urine pH Protein restriction Alkali
Overview of therapy

7/20/2015
13
Dietary Modification
Fluids
Calcium
Sodium
Protein-acid
Oxalate
Dietary Modification
Fluids
• Pathophysiologic basis
• Metabolic studies
• Randomized clinical trials
The PanaceaThe PanaceaThe PanaceaThe Panacea
Dietary Modification
Calcium
Sodium
Protein-acid
Fluids
Oxalate
Dietary Modification
Borghi et al NEJM 2002

7/20/2015
14
Dietary Modification
Calcium
Sodium
Protein-acid
Fluids
Oxalate
Food Moderate Oxalate:Limit
Rich Oxalate:Avoid
Fruits Apple, Apricots, Peaches, Pears, Pineapple, Plums, PrunesBlack currantsCherries, redOrange, edible portion
Blackberries, Blueberries, Raspberries, Strawberries, Dewberries, GooseberriesConcord grapes, Red currants, TangerinesCitrus peel
Vegetables AsparagusBroccoliCarrots, CornCucumberGreen peas, Lettuce, Lima beansParsnips, Tomato, Turnips
Beans, BeetsTops, Roots, Greens Celery , Chard, Chive, CollardsDandelion greens, Eggplant, EscaroleKale, Leeks, Mustard Greens, OkraParsley, Peppers, Pokeweed, Potatoes, Rutabagas, Spinach, Summer squash, Watercress
Nuts Peanuts, Peanut butterPecans
Miscellaneous Chicken noodle soup dehydratedSardines
Chocolate, cocoaPepperSoybean curd
Bread/Starch CornbreadSponge cake, Spaghetti,
Fruit cakeGrits, white cornSoybean crackersWheat Germ
Beverage/Juices CoffeeCranberry juice Grape juice Orange juice Tomato juice
BeerJuices containing berries OvaltineTea, cocoa
•Hypercalciuria
•Hypocitraturia
•Hyperuricosuria
•Urine pH
Pharmacologic Rx
•Hypercalciuria
•Hypocitraturia
•Hyperuricosuria
•Urine pH
Calcium Urolithiasis
Pharmacologic Rx

7/20/2015
15
Hypercalciuria
Thiazide diuretics
Drug Dosage(s) Comments
Hydrochlorothiazide50mg/day
25mg twice/daySingle dose is preferred
Chlorthalidone 25-50mg/dayMay cause hypokalemia and secondary
hypocitraturia.
Indapamide 1.2-2.5mg/dayLess side effects than hydrochlorothiazide. Rare
occurrence of hypokalemia and hypotension.
Amiloride 5mg/dayPotassium sparing. Lowers urinary calcium but to
a lesser degree than hydrochlorothiazide.
Amiloride/
Hydrochlorothizide5mg/50mg/day
Maintains the hypocalciuric effect of thiazide
while averting hypokalemia.
RCT: Decrease calciuria and stone events
↑ Ca transport
•Hypercalciuria
•Hypocitraturia
•Hyperuricosuria
•Urine pH
Calcium Urolithiasis
Pharmacologic Rx
Hypocitraturia
Citrate3- H+
Calcium phosphate complexes
Low Solubility
Ca2+ HPO42-
H2PO4- H3PO4CaCitrate-
High Solubility
Citrate3-
CO2
3H+
CO2
3HCO3-
Potassium Bicarbonate
Potassium Citrate
RCT: Raises urine citrate and decrease stone events
Dual role of citrate in urine
30-60 mEq base/day
•Hypercalciuria
•Hypocitraturia
•Hyperuricosuria
•Urine pH
Calcium Urolithiasis
Pharmacologic Rx

7/20/2015
16
Hyperuricosuria
Xanthine oxidase inhibitorAllopurinol 200-300 mg/day
Feboxustat 40-80 mg/day
Calcium Oxalate
Calcium OxalateSoluble complex
Calcium OxalateInsoluble complex
Sodium Urate
RCT: Reduces hyperuricosuria and stone events in isolated hyperuricosuria
Hyperuricosuric Calcium Urolithiasis (HUCU)
•Hypercalciuria
•Hypocitraturia
•Hyperuricosuria
•Urine pH
Uric Acid Urolithiasis
Pharmacologic Rx
O
NC
H
NC
C
C N
H
H
NC
O
O9
3
17
H+ -
pK ~ 5.4
Uric acid UrateLow pH
High pH
O
NC
H
NC
C
C N
H
H
NC
O
O9
3
17
H
-Solubility limit
Uric acid nephrolithiasis: A disease of urinary pH

7/20/2015
17
Urine pH
Potassium Bicarbonate
Potassium Citrate
30-60 mEq base/day
RCT: Raises urine pH and decrease stone events
-Solubility limit
•Hypercalciuria
•Hypocitraturia
•Hyperuricosuria
•Urine pH
Cystine Urolithiasis
Pharmacologic Rx
•Chelate cystine
Cystine has low solubilityAmino acid
L-Arginine
L-Lysine
L-Ornithine
L-Cystine
L-Leucine
L-Phenylalanine
L-Histidine
L-Methionine
L-Alanine
L-Tryptophan
N
C158
out
in
II
in
C
C
N
C109C109
IL2-3
EL3-4
1 2 43 5 6 7 8 9 10 11 12
rBAT/4F2 b 0,+ AT
Urine
Amino Acid
xx Autosomal recessive
CSSCInsoluble
pKa COOH NH3
Cystine 1.65 7.85
2.26 9.85

7/20/2015
18
Cys
tin
eso
lub
ilit
y
(mg
/ml)
4 5 6 7 8 9
1200
1000
800
600
400
200
0
Risk of CaP !
pHCysteine or
Cysteine-drug complex
HOOC – C – C – SH
NH2 CH3
CH3
– –
– –
H
HOOC – C – N – C – C – SH
H H– –
–
H
=
O
CH3
CH3
––
Penicillamine α-mercaptopropionylglycine
(Tiopronin)
DSSD + CS DS + CSSD
CSSC + DSSD 2CSSD
CSSC + DS CS + CSSD
D: Drug
C: Cystine
Insoluble
Agenda and take-home points
• General concepts
• Epidemiology
• Pathogenesis & Etiology
• Evaluation
• Treatment
General concepts
Epidemiology
Pathogenesis & Etiology
Evaluation
Treatment
A systemic disease.
Diverse causes converging on abnormal urine chemistry.
Common. Disabling. Expensive.
Urine. Stone. Imaging. Blood.
Medically treatable. Dietary. Pharmacologic.