Embed Size (px)
Citation preview

Introduction
H y p o t r i c h o s i s - l y m p h e d e m a -telangiectasia Syndrome (HLTS) is an extremely rare diagnosis with a paucity of literature. We describe a case caused by mutation in the SOX18 gene. Case Presentation
A 41-week-old 3.525 kg boy was born to a 31-year-old Caucasian female who was Gravida 1, Para 0, at the time of delivery. Her prenatal labs were: Blood type A positive, Antibody screen negative, RPR non-reactive, Rubella immune, Hepatitis B sAg negative, HIV negative, GBS negative. The pregnancy was uncomplicated. Delivery was by Normal Spontaneous Vaginal Delivery (NSVD) with epidural anesthesia, with AROM 8 hours prior to delivery productive of meconium stained amniotic fluid. APGARs were 6 at 1 minute, and 8 at 5 minutes. Resuscitation in the de-livery room consisted of drying and stimula-tion, blow-by-oxygen and brief mask CPAP.
The baby continued on blow-by oxygen in the delivery room and could not be weaned, so he was brought to the NICU. Birth weight 3525 g, Length 49.5 cm, Head Circumference 34.5 cm.
Admission Vital Signs: BP 86/44, Pulse 120, Temp 98.2, Resp 77, SpO2 94% on blow-by-oxygen.
Exam: Active baby with strong cry, no sig-nificant distress. HEENT: Anterior Fontan-elle Open and Flat (AFOF), red reflex pre-sent, noted absence of eye brow and eye-lashes, sparse hair on scalp. CV: RRR without murmur, normal pulses. Lungs: Tachypnea with mild coarse breath sounds, equal bilaterally. Abdomen: soft, non-tender, not distended, active bowel sounds. GU: patent anus, normal penis and de-scended testes with b/l hydroceles. Legs: dramatic cutis marmorata with areas of at-
rophy of subcutaneous tissue over the ex-tensor surface of the knee. The lower ex-tremities thighs feel woody from significant edema. Neurological: normal reflexes, slightly increased tone, normal strength, symmetric morrow. Skin: scattered pete-chiae and several areas of telangiectasia.
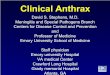
CXR (Figure 1): bilateral hazy lung fields with pleural effusion on the left. Mild cardi-omegaly.
Initial CBC showed WBC 14 with 59 segs, 26 lymphs, 6 monos, 4 eos, 6 bands. ABG o n 1 0 0 % o x y g e n b l o w b y w a s 7.27/47/359/-5. He was placed on a nasal cannula, IV fluids and ampicillin and cefotaxime. Na-sal cannula was weaned off on Day of Life (DOL) #3 and initial left-sided pleural effusion resolved. Cardiac ultrasound on DOL #3 showed mild-to-moderate pulmo-nary hypertension, small pericardial effu-sion, PFO (Patent Foramen Ovale) vs. ASD (Atrial Septal Defect) and a moder-ate to large bidirectional Patent Ductus Arteriosus (PDA). A Genetic consultation obtained on DOL #3 due to skin, hair and dermatologic findings; a diagnosis of probable Hypotrichosis-Lymphedema-Telangiectasia Syndrome was made. On DOL #4-#6 the patient’s respiratory status improved, and he was feeding well.
On DOL #7 his respiratory status worsened, he was placed back on NC oxygen 1L 35%, CxR showed recurrence of bilateral pleural effusions. At this time, he was transferred fromthe Level 2 NICU at the birth hospital to our regional tertiary NICU. He remained on NC for several days, the effusions increased as did his oxygen re-quirement. He was started on furosemide. Serial cardiac ultrasounds showed worsen-ing pulmonary hypertension. He was placed on inhaled nitric oxide at 20ppm and 100% oxygen via 2L NC without improvement in his pulmonary hypertension. iNO was in-creased to 40ppm without any improvement.
NEONATOLOGY TODAYN e w s a n d I n f o r m a t i o n f o r B C / B E N e o n a t o l o g i s t s a n d P e r i n a t o l o g i s t s
Volume 10 / Issue 8August 2015
IN THIS ISSUE
Neonate with Hypotrichosis-Lymphedema-Telangiectasia and Fatal Pulmonary Hypertension By Jane O’Donnell, MD; Casey Cohenmeyer, MD; Crystal Le, MD Page 1
DEPARTMENTS AND COLUMNS
The NPA Advocates for Breastfeeding Support in the Workplace By Raylene M. Phillips, MDPage 5
Medical News, Products & InformationPage 8
Neonate with Hypotrichosis-Lymphedema-Telangiectasia and Fatal Pulmonary HypertensionBy Jane O’Donnell, MD; Casey Cohenmeyer, MD; Crystal Le, MD
Recruitment Ads:Pages: 3, 4, 6, 10, 12
DO ALLSURFAOTANTS
HAVE THE SAMECOMPOSITION?
Find out here

PLEASE READ THIS LETTER ON AN IMPORTANT BILL (ADVANCING HOPE ACT 2015)
THAT IS NOW BEFORE CONGRESS
Extending this act, is a win-win for pediatric patients, physicians and the companies that provide the products and services. After reading this letter, if you agree, download the form letter and send to your Senator.
For additional information, please contact: Saira Sultan, JD, President of Connect 4 Strategies, LLC at: [email protected]
SUGGESTED LETTER (See Links Below to Find your Senator and Download this letter)
On your institutional Ietterhead, if available
[Date] [Recipient][Address][Address][City, State] RE: The Advancing Hope Act of 2015 Dear [Your Senator], As a physician who treats and serves hundreds of premature babies suffering from respiratory distress syndrome, I write to you today with great interest and concern regarding proposed legislation which will affect about 65,000 premature infants each year in the U.S. The Advancing Hope Act is a bill intended to reauthorize and make permanent a priority review program at the Food and Drug Administration (FDA), which will encourage development of new treatments for rare pediatric diseases such as RSD. As a neonatologist at [insert name of your institution] treating these infants, I wanted to write to let you know how much institutions like ours in [insert your state] stand to benefit from additional research in rare pediatric diseases. Historically, our youngest and most vulnerable patients have been underserved and ignored in the drug development arena due to the high risk nature and small size of pediatric patient populations. This is why many drugs used in infants and children have never been tested in these age groups and, therefore, must be used off-label.
As you are surely aware, drug development is expensive and requires many years of effort. The positive impact of an incentive program such as the Pediatric Review Voucher Program is significantly diminished if it is too short-lived or requires frequent reau-thorizations. This is because the value of the incentive is not actually realized until many years after the development process has begun. Small companies like mine, our clinical researcher partners, and our investors, need confidence that approval-related incen-tives like the voucher will still exist when the early-stage discoveries we are developing in the clinic finally make it through the ap-proval process and to the patients’ bedsides.
I hope you will consider supporting efforts to make permanent this voucher program described in the Advancing Hope Act of 2015. This bill will significantly benefit the large, under-served population of infants and children who need new innovative therapies to ensure their best healthcare outcomes. There is a tremendous need for new therapies for these patients, many of which bear a terrible lifelong burden not only for these young patients and their families, but also costs the US healthcare system billions per year to support the infants and children who may continue to require medical support throughout their lives. It is incumbent upon us to work together on behalf of those suffering these enormous challenges to create and promote programs that can benefit their health and potentially reduce overall healthcare costs. Thank you your sincere consideration. Please contact me at [Your phone number or email] if I can be of any assistance on this im-portant issue of making the rare pediatric priority review voucher program permanent. Sincere regards, [Your Name][Your Title]
Find your US Senator: www.senate.gov/senators/contact/Download this letter, fill in the appropriate information in the [brackets] and mail - www.neonatologytoday.net/newsletters/ltr.doc

Sildenafil was started on DOL #10, PGE on DOL #11 to maintain ductal potency in the face of severe pulmonary hypertension, bosentan started on DOL #13, epoprostenil on DOL #13. Despite these measures he continued with persistent severe pulmonary hypertension with continued desaturation episodes down to the 70s. A chest CT was obtained and showed very mild interstitial lung disease with mild thickened interlobular septa. These findings are nonspecific. On DOL #20 his effusions worsened, he was intubated, a chest tube was placed and a large chylothorax drained. He was extu-bated back to NC on DOL #22 with the chest tube left to drain. The patient was gradually weaned off iNO, but he continued to require all other medical therapy for his
pulmonary hypertension. Diagnosis of HLTS was confirmed by genetic testing. The pa-tient was heterozygous, with a mutation in the SOX18 gene, specifically c.541 C>T (p.Gln181Stop). Parents elected to have him transferred to hospice care. He was discharged from the NICU to hospice at 30 days of age. He sub-sequently passed away from pulmonary hy-pertension weeks later under hospice care. Discussion HLTS has been reported to be caused by autosomal recessive and autosomal dominant mutations in the SOX18 gene. This has been described in the literature by Irrthum et al (2003) in a series of three
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 3
Figure 1.
Sign up for a free membership at 99nicu,the Internet community for professionals inneonatal medicine. Discussion Forums,Image Library, Virtual NICU, and more...!
www.99nicu.org
NeonatologistAlbuquerque, New Mexico
• Approximately 3200 deliveries per year
• 3 neos and 2 NNPs, Level III• 38 beds• ADC 29 - 35• 800+ admissions per year• Keep all gestations, all weights• RNs perform PICC line pacement,
NNPs intubate and do chest tubes• 1 physician works each day 0730 –
1700 with 1 NNP who works from 0730 – 1730 and 1 physician works each night from 1700 – 0730
• 24 hour in-house coverage• Have both conventional vents and
high frequency vents• Have sub-specialty support: Cardiol-
ogy, ophthalmology, neurology • The physicians enter their own or-
ders and notes day/night. The hospi-tal has paper medical records but the neos also have to document in Pre-miEHR which is our own EHR. The hospital uses McKesson for order entry.
• ACUITY LEVEL: Level III • REQUIRED CREDENTIALS: Board
Certified in Peds & BC or BE in Neo-natal – Perinatal Medicine
• Full Benefits, Sign on and Relocation• Compensation based on experience,
highly competitive
Preeti Malhotra, Recruiting Consultant TIVA HealthCare, Inc.
1613 N. Harrison Pkwy, Ste. 200 Sunrise, FL 33323
Direct: (954) 858.1027Toll-Free: (800) 506.8482
Fax: (954) [email protected]
www.tivahealthcare.com
<°3nzcI4, Org

families. In animal models, Downes et al (2009) hypothesize that alterations in the SOX18 gene may lead to abnormalities in structural integrity of the microvasculature and lymphatic system. We hypothesize that this abnormal development of the pulmonary microvasculature and lym-phatic system led to this patient’s ulti-mately fatal case of persistent pulmonary
hypertension of the newborn.References
!" Irrthum, A., Devriendt, K., Chitayat, D., Matthijs, G., Glade, C., Steijlen, P. M., Fryns, J.-P., Van Steensel, M. A. M., Vikkula, M. Mutations in the transcription factor gene SOX18 underlie recessive and dominant forms of hypotrichosis-lymphedema-telangiectasia. Am. J. Hum. Genet. 72: 1470-1478, 2003. [PubMed: 12740761].
#" Downes, M., Francois, M., Ferguson, C., Parton, R. G., Koopman, P. Vascu-lar defects in the mouse model of h y p o t r i c h o s i s - l y m p h e d e m a -telangiectasia syndrome indicate a role for SOX18 in blood vessel maturation. Hum. Molec. Genet. 18: 2839-2850, 2009. [PubMed: 19429912].
NT
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 4
“HLTS has been reported to be caused by autosomal recessive and autosomal dominant mutations in the SOX18 gene.... We hypothesize that this abnormal development of the pulmonary microvasculature and lymphatic system led to this patient’s ultimately fatal case of persistent pulmonary hypertension of the newborn.”
2nd Annual Basic & Advanced Fetal Cardiac Symposium and Workshop
Rush University Medical CenterSep 10-12, 2015; Chicago, IL USAwww.FetalCardiacSymposium.com
Corresponding Author
Jane O’Donnell, MDMedical DirectorRCHSD NICU at Scripps La JollaClinical Professor of Pediatrics UCSD School of Medicine3020 Children’s WaySan Diego, CA 92123 USATel: [email protected]
Casey Cohenmeyer, MDMedical DirectorRCHSD NICU at Scripps EncinitasAssociate Clinical Professor of Pediatrics UCSD School of Medicine3020 Childrens Way MC 5008San Diego, CA 92123 USATel: 868.966.5818; Fax: 858.966.7483
Crystal Le, MDRady Children's Specialists of San Diego Medical Practice FoundationAssistant Clinical Professor of Pediatrics UCSD School of Medicine 3020 Childrens Way MC 5008San Diego, CA 92123 USATel: 868.966.5818; Fax 858.966.7483
Neonatology Locum TenensSouthern, AL
• BC-Pediatrics with subspe-cialty in Neonatal-Perinatal Medicine
• 10/1/15 start-up in Dothan, AL
• Must have an Active AL li-cense
• Number of beds in the NICU - 6
• 2-doc model• Week on, week off • Midlevel Support - No• 24-hour shifts; call within a
30 min radius
Preeti MalhotraRecruiting Consultant TIVA HealthCare, Inc.
1613 N. Harrison Pkwy, Ste. 200
Sunrise, FL 33323Direct: (954) 858.1027
Toll-Free: (800) 506.8482 Fax: (954) 851.1861
www.tivahealthcare.com
w voYOUR WAY TO THE ONE
FCS_|“|'}:|‘.\ I . '_._\ |{l'l_| .\(‘ :29M .\Il’()t-‘.Il M In

The National Perinatal Association’s (NPA) mission is to pro-vide a forum for all healthcare providers and those involved in the care of babies, mothers and families in order to com-municate and work together to provide more effective sup-port during the perinatal period. In order to do this we: “Con-vene, Educate, Advocate, and Integrate.” In previous col-umns, I have shared opportunities NPA has provided to Con-vene and Educate. This month I will discuss ways in which NPA participates in Advocacy.
The National Perinatal Association has a long history of ad-vocating for improved perinatal care by taking the lead on issues or by partnering with other organizations to raise awareness and promote support. Advocacy issues NPA has addressed include family support, bereavement, palliative care, quality improvement, promotion of physiologic birth, preconception health, artificial reproductive technology, ac-cess to care, medical liability reform, care of late preterm infant, and breastfeeding as the norm for infant feeding.
This month the NPA joins the WHO and UNICEF in support-ing World Breastfeeding Week and the United States Breast-feeding Committee in celebrating National Breastfeeding Month. The 2015 theme is “Breastfeeding at Work: Let’s Make It Work.” While the Gold Standard for infant feeding is six months of exclusive breastfeeding with continued breast-feeding for one or more years after introducing complimen-tary foods, only 38% of infants are exclusively breastfed for six months globally and less than 25% are doing so nation-ally. Suboptimal breastfeeding contributes to 800,000 infants deaths a year worldwide.
Over 75% of mothers want to breastfeed their babies in the US. One third of mothers return to work by 3 months after the birth of their babies and two thirds are back to work by 6 months. The Surgeon General has called on all sectors of the commu-nity, including employers, to protect, promote and support breastfeeding; yet, only half of mothers have workplace support and the lower a mother’s income, the less likely she is to have breastfeeding support at work. Mothers with breastfeeding sup-port are twice as likely to exclusively breastfeed at 3 months. To support breastfeeding, employers should develop a workplace breastfeeding support policy that includes time and a private space for breastfeeding mothers to pump their milk. Several state and federal laws mandate “Break Time for Nursing Moth-ers.” Mothers should know their rights and talk to their employer about maternity leave and breastfeeding support including lac-tation consults, getting a breast pump, and having a time and place to pump at work.
There are other ways to support breastfeeding for working mothers. Paid parental leave is a hot topic these days. The U.S. is the only developed country in the world that doesn’t guaran-tee paid maternity leave. There are some notable exceptions in our country. Netfix recently announced provision of unlimited paid parental leave for their employees during the first year after the birth or adoption of a child, joining other tech companies who provide 18-22 weeks of paid parental leave including: Google, Apple, and Twitter. Bringing baby to work is an option being trialed by several companies including the Washington Health Department where mothers can bring their infants to work for up to 6 months after birth.
There may be no population needing breastfeeding support more than mothers of babies admitted to the NICU, who often express their milk for weeks or months before being able to actually breastfeed. Many mothers must return to work before their babies are discharged and many have
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2014 5
The NPA Advocates for Breastfeeding Support in the Workplace By Raylene Phillips, MD
Members of the NPA write a regular column in Neonatology Today.
“When physicians and other healthcare providers have a successful breastfeeding experience, supported by their workplace environment, they are much better equipped to provide positive breastfeeding support for mothers in their healthcare practice. By supporting breastfeeding in our own workplace, we are also supporting breastfeeding nationally and globally and helping to fulfill our mission as healthcare providers to heal and serve.”
Q National
Peiinatalssoc1at1onConvene. Educate. Advocate. Integrate.

little or no support at work to provide the milk their babies need for optimal healing, growth, and development.
Another group that often receives less than optimal breastfeeding support is hospital employees, including medical students, residents, and fellows who work long hours with little or no pro-tected time and often no dedicated place to express their milk. We, as a medical profession, must “practice what we preach” and support medical pro-fessionals in training to do the same.
When physicians and other healthcare providers have a successful breast-feeding experience, supported by their workplace environment, they are much better equipped to provide positive breastfeeding support for mothers in their healthcare practices. By support-ing breastfeeding in our own work-place, we are also supporting breast-feeding nationally and globally and helping to fulfill our mission as health-care providers to heal and serve.
In addition to joining the National Peri-natal Association in supporting breast-feeding in the workplace, we invite you to join us in Nashville, TN, this Octo-ber as we explore the art and science of helping pregnant women and their babies deal with drug dependency be-fore and after birth.
NT
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 6
Raylene M. Phillips, MD, IBCLC, FABM, FAAPPresident, National Perinatal Association
Assistant Professor of PediatricsLoma Linda University School of Medicine
Director of Nursery/NeonatologyLoma Linda University Medical Center-Murrieta
Loma Linda University Children's HospitalDivision of Neonatology11175 Campus St. Suite 11121Loma Linda, CA 92354 USA
Office: 909.558.7448Fax: 909.558.0298
Save the Dates
2015 SymposiumSponsored by The National Perina-tal Association (NPA) & The National Advocates for Pregnant Woman (NAPW)
Pregnant Women, Drug Use, and NAS: Experts Share Science & Strategies That Help Women, Babies, and Families
October 2-3, 2015Nashville Marriott at VanderbiltNashville, TN
Download a Save the Date flyer
2016 Annual ConferenceNational Perinatal Association (NPA)
Multidisciplinary and Collaborative Perinatal Decision Making in the 21st Century
April 28-29, 2016Texas Children's Hospital - Pavilion for Women, Baylor College of Medicine, Houston, TX
NeonatologistPanama City, FL
• 8 licensed beds for level 3, and 22 licensed beds for level 2
• Level III NICU• Attendance at delivery for high
risk cases• Physician Hand Off usually occurs
at 8am• 4 MD model, in house coverage
24/7• 4 Vents dedicated to NICU, No
ECMO• Provider involved in transports• ADC 16.7, ALOS 10.3 days• Required Credentials: Board Cer-
tified Peds & BC or BE in Neona-tal –Perinatal Medicine
Preeti MalhotraRecruiting Consultant TIVA HealthCare, Inc.
1613 N. Harrison Pkwy, Ste. 200 Sunrise, FL 33323
Direct: (954) 858.1027Toll-Free: (800) 506.8482
Fax: (954) [email protected]
www.tivahealthcare.com
YOUR WAY TO THE ONE

!"#$%"&#'("&)*+&%,'()(-.
/$("&#()(-.*0.12(3'41
56#(7$%*89:;<*=;:>
!"#$%+("#'"$"#&)?**!**@'&1'<*AB
!"
!!!"#$%&'()*+,-.%+*/-"&%-
01 .$)*'2(*&1&'()*%3%4*+2+01 #$%#'2%3%4*+2+01 &'()*'&1+/(4$%#+01 *#2$#+*5*+2+
01 .6,+*&*'#1'++*+2'#2+01 ')5'#&$)1.('&2*&$1#/(+$+01 7$)+*)$1&3*#*&'31#/(+$+1*#189:;1'#)1:<9:;
01 .$(=/+*%#*+2+01 .$)*'2(*&1&'()*%3%4,1'#)1#$%#'2%3%4,1=$33%!+1
01 .$)*'2(*&1($+*)$#2+
>?@AB>1?;C9B8:BD
,l.lI.J|’Il.IaI"I|3.|-ll-‘I:1 =mmnr- l
u llillllll '3 l I Hi
"' nlluun .- u
IlI
‘fl-I nuu Illlllhn
‘ H ‘ ‘l." min )4 1! Ira ‘
I um U' ' .- . .-!I . .r- '
——v nu ”..l_,,.grnIn.I'-.-l.‘|I'II'I2I.\'l
_....'-2--‘ ‘.a ..a.-...:...a.‘ -—" ' " "“ ' .
2 ‘P 7
‘H. W..- _I- I
.. H‘._;.uI|:I:I.IaI .|'....|‘I n
lna-r = -o s~ - -" I, u. If -1
_1 H 31.“; __H_ ‘“'"".".'. man. Inn: mnaunnun
I'll -—- n " ,. I _n- --"
H‘-‘ ll’
oi.‘
:a
:=
=-.rn
:I:I:I
- .n.-A--u
. l'':: ..' .. «.- .""‘
H"
' I IMI1-:lJI!Ik -_. , N“..., ..
.4
‘H
n_;. [®Z;3TiT,'f'EL«snu-
IHlH
7J.‘lI.'//
1:
TARGET AUDIENCE:g
a..a . — _-; " s
’_;_;Fkf
0 pediatric cardiologists 0 physician assistants 0 perfusionists0 neonatologists 0 advanced practice nurses 0 pediatric cardiology and0 cardiac surgeons 0 bedside clinical nurses in neonatology fellows _
0 intensivists NICU and CVICU 0 pediatric residents.‘.:__5—*s:
T’ V:' www.neocardIsymposIum.com \_
ii
-——‘
. -.- =4.--- :_ _ ,_~_ _:-o in‘ -—_ _- .—c -.
‘’ *
1---:--r '7 W‘ _A. -u—
-21":

Therabron Therapeutics Reaches 50% Enrollment in Phase 2A Clinical Trial for Lead Pediatric Respiratory Critical Care Program - Company on Track to Complete Trial Enrollment by End of 2015
Therabron Therapeutics, Inc., a specialty biotechnology company dedicated to redefining the management of res-piratory disease through innovation, today announced that it has achieved over 50% patient enrollment in the second clinical trial evaluating its lead product candidate, CG100, for the prevention of chronic respiratory morbidities, in-cluding Bronchopulmonary Dysplasia (BPD), in premature infants. This Phase 2A study is supported in part by a $1.6 million grant from the U.S. FDA Office of Orphan Product Development.
“We are encouraged by the progress we have made with patient enrollment in this trial and the interest expressed by the neonatology community in our potentially transfor-mative technology platform. Importantly, our data and safety monitoring board has not observed any unexpected safety or tolerability concerns in the trial to date, allowing
us to now proceed to the highest dosing group in this study” said Dr. Aprile L. Pilon, Founder, Chairman and CEO of Therabron Therapeutics. “CG100 has the potential to provide a significant respiratory health benefit for very premature infants following discharge from the Neonatal Intensive Care Unit.”
The CG100 product candidate is a recombinant human CC10 protein, a secretory protein that is believed to play an important protective role in the lung via maintenance of airway epithelia, delivered by intratracheal instillation in intubated neonates. CG100 has the potential to improve long-term clinical outcomes in preterm infants and signifi-cantly reduce the economic burden beyond the infant’s initial in-patient stay. In a previously completed clinical study (Levine et al., Peds Research, 2005; Therabron data on file), investigators observed suppression of inflamma-tory mediators in the respiratory tract and evidence of re-duced lung injury in CG100-treated infants. Additionally, infant hospitalizations due to respiratory causes, as well as the need for respiratory medications through six months post-discharge, were reduced in CG100-treated infants compared to controls.
Medical News, Products & Information
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 8
Compiled and Reviewed by Tony Carlson, Senior Editor
Choose from 2 Outstanding Meetings in ONE Great LocationHilton Orlando Bonnet Creek
SAVE THE DATE!
®
!"#
$%&
'()* *+
#, %
# - * * % . * * .#/.&(/'
/0)
(1
!"#$%&$'()*+),-()./0123(45(673(893:;39(<336;2=>(;2(
?342@6@A(<3B;C;23
!"#$%&$'()D+),-()./0&2(E2632>;F3(@2B(
G4:H93732>;F3($3F;3I(45(?342@6@A(<3B;C;23
!"#$%&'%#$%()*+$,"%#$%-./0%1"%*2+)$3%$214")5%4#16%7"**2+8&2'%%+$,%"162)%#$,&'1)9%2:;2)1'3%+$,%+*'"%2+)$%<=>?<@>%7)2,#1'A
J1E?((1%$(
G1?KE?%1%L(M%&NEK'(E<8$1O"<"?K(L'<81LE%<(PGMELQ8$"+G1?!"$"?G"(R&'!3S9T@9U()V-()./0
SAVE THE DATE!
FEBRUARY 25-28, 2016
One of the Premier Meetings inNeonatal Medicine
FEBRUARY 23-28, 2016
An Intensive andComprehensive Review of
Neonatal Medicine
Choose from 2 Outstanding Meetings in ONE Great LocationHilton Orlando Bonnet Creek
J N CONTINUOUS QUALITY IMPROVEMENT SYMPOSIUM (CQIS)PRE-CONFERENCE DAY
and other industry experts, and also earn CME/CNE credits. 0 U R February 24, 2016
Join us in Orlando in 2016 to learn, network with colleagues

Therabron anticipates completion of enrollment for the current trial by the end of 2015, with multiple data re-leases in expected in 2016.
About Chronic Respiratory Morbidities in Preterm Infants
Over half a million preterm infants are born in the US every year. Of those infants, about 60,000 are Very Low Birth Weight (VLBW) and experience respiratory dis-tress; and up to 15% of this vulnerable patient popula-tion dies. Of those who survive, up to 15,000 will de-velop neonatal BPD, a chronic lung disorder that pre-disposes the child to potentially life-threatening respira-tory infections and asthma. These infants typically expe-rience repeated hospitalizations for respiratory compli-cations, the need for numerous respiratory medications, and frequent doctor visits throughout their infancy and childhood. An estimated $26 billion are spent annually on medical care during the first year of life in these VLBW premature infants and the emotional cost of fami-lies impacted by having a child with this condition is substantial.
Therabron Therapeutics, Inc. is a clinical-stage biotech-nology company founded in 2007 and located in Rockville, MD. Therabron is focused on the advance-ment of respiratory therapeutics with disease-modifying potential. The company’s product candidates aim to re-store the natural immune balance in the lungs of respi-ratory patients through the administration of recombi-nant human CC10 proteins. The family of CC10 pro-teins, also known as secretoglobins, have the potential to change the course of acute and chronic respiratory diseases, representing large markets into which few truly novel drugs have been introduced. Therabron’s product candidates have the potential to be first-in-class, disease-modifying, breakthrough biologic thera-peutics. For addit ional information, please visit www.therabron.com.
“Tele-Rounding” Robots in the Neonatal Intensive Care Unit
Many hospitals lack the resources and patient volume to employ a round-the-clock, neonatal intensive care spe-cialist to treat their youngest and sickest patients. Tele-medicine—with real-time audio and video communica-tion between a neonatal intensive care specialist and a patient—can provide access to this level of care.
A team of neonatologists at Children’s Hospital Los An-geles investigated the use of robot-assisted telemedi-cine in performing bedside rounds and directing daily
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 9
NEONATOLOGY TODAY Sponsorships and Recruitment Advert is ing
For information on sponsorships or recruitment advertising, contact Tony Carlson at: 301.279.2005
or send email to: [email protected]
Sponsorship
DO ALLSURFAOTANTS
HAVE THE SAMECOMPOSITION?
Find out here

care for infants with mild-to-moderate disease. They found no significant differences in patient outcomes when telemedicine was used and noted a high level of parent satisfaction. This is the first published report of using telemedicine for patient rounds in a Neonatal Intensive Care Unit (NICU). Results was published online first on June 29th in the Journal of Telemedi-cine and Telecare.
“We wanted to determine if robot-assisted telemedicine could be part of daily clinical practice in order to pro-vide care by a neonatologist where one might otherwise not be present—in remote locations, underserved com-munities and at times of limited staff-ing,” said Arlene Garingo, MD, neona-tologist at CHLA and first author on the study. In an earlier study, the team at CHLA demonstrated the feasibility, safety and accuracy of robot-assisted telemedicine in the NICU.
In this randomized study, infants were treated by either an onsite neonatolo-gist who visited the baby at the bed-side during patient rounds, or by an offsite neonatologist who performed daily evaluations of the patient using robot-assisted telemedicine. Twenty pairs of patients were matched by age, weight, diagnosis and disease severity, with one infant from the pair assigned to each treatment group.
There were no differences in average length of stay, age at discharge or hospital charges between the two treatment groups. Nutritional needs, respiratory support, days on antibiot-ics, phototherapy and number of ra-diological studies were also the same between the two groups.
“However, there was a significant dif-ference in time spent at the bedside, with the remote neonatologist requir-ing nearly twice as much time to care for the patient,” said Philippe Fried-lich, MD, MEpi, MBA, Chief of Neona-
tology at CHLA and an author on the study. He explained the additional time was largely due to time required to maneuver the robot, as well as issues of internet connectivity.
At the time of discharge, 45% of fami-lies completed a survey about their experience. All responded that they were comfortable having their baby treated by an offsite neonatologist via telemedicine and would be comfort-able doing it again.
Additional contributors include: Tho-mas Chavez, Linda Tesoriero, MD, Shilpa Patil, MD, and Paige Jackson, MD, Division of Neonatology and the Center for Fetal and Neonatal Medi-cine at Children’s Hospital Los Ange-les; and Istvan Seri, MD, PhD, who was located at CHLA during the study and is now at the Center of Excel-lence in Neonatology, Saidra Medical and Research Center, Qatar.
Children's Hospital Los Angeles has been named the best children’s hos-pital in California and among the top 10 in the nation for clinical excellence with its selection to the prestigious U.S. News & World Report Honor Roll. Children’s Hospital is home to The Saban Research Institute, one of the largest and most productive pedi-atric research facilities in the United States. Children’s Hospital is also one of America's premier teaching hospitals through its affiliation since 1932 with the Keck School of Medi-cine of the University of Southern California. For more information, visit CHLA.org.
Women & Infants Hospital of Rhode Island Receives a $5 Million Grant from National Institutes of Health to Continue Work on Perinatal Biology Women & Infants Hospital of Rhode Island has recently received a nearly
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 10
NeonatologistFort Walton Beach, FL
• BC/BE Neonatologist – great op-portunity for recent graduates (5 years) – to join an innovative team, practicing in a Level II NICU, working on Level III status.
• A 257-bed hospital with a medical staff of over 200 physicians
• 10-12 licensed beds for Level II• Two (2) MD model with 24 hr call
shifts• Attendance at delivery for high
risk cases• Physician involved in transports• Average Daily Census 6.6• Must have current PALS• REQUIRED CREDENTIALS:
Board Certified Peds & BC or BE in Neonatal – Perinatal Medicine
Preeti MalhotraRecruiting Consultant TIVA HealthCare, Inc.
1613 N. Harrison Pkwy, Ste. 200 Sunrise, FL 33323
Direct: (954) 858.1027Toll-Free: (800) 506.8482
Fax: (954) [email protected]
www.tivahealthcare.com
9th International Conference October 1st – 3rd, 2015 newbornbrain2015.com
Fota Island Resort Cork, Ireland
§g§T'i’voYOUR WAY TO THE ONE
BRAINLRNIONITORINGNEIIRUPROTECTION
‘N THENEWBORN

NPA 2015 SYMPOSIUM
Pregnant Women,Drug Use, and NASExperts Share Science &Strategies That HelpWomen, Babies, andFamilies
OCTOBER 2 -3in Nashville, TN Working together
forbetteroutcomes for
PRESENTED in PARTNERSHIP with
National Advocates for Pregnant Women babies’ families’and our
FOR MORE INFORMATION VISIT 5-ommun/1‘)/_www.nationalperinata|.org/Nashville
9 NationalPerinatal
Association
0 -3»
MI i‘=w”I Mad?W7‘. I I ‘g ‘ ‘iJIJL JLJt .4-‘L jig JIL
National Advocatesfor Pregnant Women
NAPW

$5 million grant from the National In-stitutes of Health (NIH) to support an Inst i tut ional Development Award (IDeA) Center of Biomedical Re-search Excellence (COBRE) for Peri-natal Biology. Of the more than 100 COBREs across the country, Women & Infants is the only one specifically focused on developmental research. The IDeA program builds research capacities in states that historically have had low levels of NIH funding by supporting basic, clinical and transla-tional research; faculty development; and infrastructure improvements. Under the leadership of James F. Padbury, MD, Pediatrician-in-Chief and Chief of Neonatal/Perinatal Medi-cine at Women & Infants Hospital and the William and Mary Oh - William and Elsa Zopfi Professor of Pediatrics for Perinatal Research at The Warren Alpert Medical School of Brown Uni-versity, and Surendra Sharma, MBBS, PhD, research scientist at Women & Infants and Professor of Pediatrics at the Alpert Medical School, the CO-BRE team will continue its research in perinatal biology, including studies of fetal and newborn development, pla-cental biology, and reproductive dis-eases including preterm birth and preeclampsia. “Our projects are focused on critical windows of development and repro-ductive life. Environmental distur-bance or other influences during these critical windows can have last-ing effects,” said Dr. Padbury. “Our overarching hypothesis is that under-standing these effects during critical developmental periods informs the mechanisms of health and disease throughout life.” Work supported by the COBRE in Dr. Sharma’s laboratory has identified novel new insights into the pregnancy d i s o r d e r , p r e e m c l a m p s i a , o r pregnancy-induced hypertension. “We have recently demonstrated that
preeclampsia originates from protein misfolding and aggregation. This leads to disturbances in placental function and many of the mother’s symptoms,” explained Dr. Sharma. “Remarkably, transthyretin, the pro-tein we have identified that is mis-folded in preeclampsia, is also dis-turbed in some cases of Alzheimers disease. Our current work is focused on the mechanistic similarities be-tween preeclampsia and Alzheimers disease and whether preeclampsia may be a risk factor for later devel-opment of Alzheimers.” Dr. Sharma and his colleagues are also working to develop a diagnostic test to confirm that preeclampsia can be identified much earlier in preg-n a n c y . H e s a i d , “ I d e n t i f y i n g preeclampsia earlier will certainly lead to new and better treatments.” This is a Phase III award intended to consolidate the formation of the Cen-ter for Perinatal Biology and support the administrative activities of the Center. It will also provide state-of-the-art equipment to support the Cen-ter’s Molecular Biology and Imaging Core. The Center and the COBRE researchers’ laboratories are located in Providence’s “Knowledge District” in the Kilguss Research Institute, the Laboratory for Molecular Medicine and the Coro Research building. Other investigators include: Sunil Shaw, PhD and Shibin Cheng, MD, PhD. Sen-ior investigators also participating in the projects are Ulrike Mende, PhD; Walter Atwood, PhD; Qian Chen, PhD; Pamela Swiatek, PhD; and Karl Kelsey, MD.
Women & Infants Hospital of Rhode Is-land, a Care New England hospital, is one of the nation’s leading specialty hospitals for women and newborns. A major teaching affiliate of The Warren Alpert Medical School of Brown Univer-sity for obstetrics, gynecology and new-born pediatrics, as well as a number of
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 12
International CardiologyNeonatology Symposium
Oct 8-10, 2015InterContinental ! Miami, FL
www.neocardisymposium.com
Neonatal Cardiovascular Program Director – Texas
Children’s Hospital!Texas Children's Hospital in partnership with Baylor College of Medicine (BCM) section of Neonatology, is seeking a Director for the Neonatal Cardiovascular Program. Consis-tently ranked as one of the nation’s top chil-dren’s hospitals and with significant expansion plans for cardiac services, this is an exciting opportunity to join a multidisciplinary team of neonatal experts. This unique program pro-vides high quality, consistent care for neo-nates admitted to TCH for suspected or actual neonatal cardiac conditions including congeni-tal heart disease.
Offering the highest level of care available to newborns, Texas Children’s annually provides care to over 2000 infants in the NICU and approximately 800 children in the Cardiovasular Intensive Care Unit. As the Neonatal Cardiovascular Program Di-rector, areas of responsibilities will include the following:• Participate in the care and lead the coordi-
nation of the neonatology team that pro-vides care to infants admitted to the NICU with cardiac conditions.
• Participate in the care and lead the coordi-nation of care with other specialty teams (cardiac intensive care, cardiology, and cardiac surgery).
A physician dual certified in neonatology and cardiology is ideally suited for this posi-tion but neonatologists or third-year fellows with a strong interest or experience in car-diology are encouraged to apply. The Pro-gram Director will have opportunities to undergo concurrent subspecialty training in cardiology or neonatology, including a for-mal fellowship in cardiovascular critical care. In addition, the successful candidate will be eligible for an academic faculty ap-pointment with Baylor College of Medicine.
If you are interested in learning more about this opportunity and would like to join one of the nation’s largest, most di-verse and most successful pediatric pro-grams, please send your resume to: [email protected].
%.£!%‘.%';i‘1‘§J

specialized programs in women’s medicine, Women & Infants is the 11th largest stand-alone obstetrical service in the country with approximately 8,400 deliveries per year. A U.S.News & World Report 2014-15 Best Children’s Hospital in Neonatology and a 2014 Leapfrog Top Hospital, in 2009 Women & Infants opened what was at the time the country’s largest, single-family room neonatal intensive care unit. Women & Infants and Brown offer fellowship programs in gy-necologic oncology, maternal-fetal medicine, urogynecology and reconstructive pelvic surgery, neonatal-perinatal medicine, pediatric and perinatal pathology, gynecologic pathology and cytopathology, and reproductive endocrinology and infertility. It is home to the nation’s only mother-baby perinatal psychiat-ric partial-hospital, as well as the nation’s only fellowship pro-gram in obstetric medicine. Women & Infants has been designated as a Breast Center of Excellence by the American College of Radiography; a Center of Excellence in Minimally Invasive Gynecology; a Center for In Vitro Maturation Excellence by SAGE In Vitro Fertilization; a Center of Biomedical Research Excellence by the National Institutes of Health (NIH); and a Neonatal Resource Services Center of Excellence. It is one of the largest and most prestig-ious research facilities in high risk and normal obstetrics, gy-necology and newborn pediatrics in the nation, and is a mem-ber of the National Cancer Institute’s Gynecologic Oncology Group and the Pelvic Floor Disorders Network.
Hospital to Create Emergency Experiences Using Virtual Reality: Walk Around Inside Crisis Situations, Educate Medical Professionals
Next Galaxy Corp. recently announced the signing of an agree-ment with Miami Children's Hospital. Next Galaxy will develop immersive Virtual Reality medical instructional content for patient and medical professional education using the Company's VR Model. Per the multi-year agreement, Next Galaxy and Miami Children's Hospital are jointly creating VR Instructionals on car-diopulmonary resuscitation (CPR) and other lifesaving proce-dures, which will be released as an application for smartphones.
Incorporating eye gaze control, gestures, and voice com-mands while "walking around" inside an emergency medical experience or crisis, Next Galaxy's Virtual Reality Model en-gages participants far beyond today's methodology of pas-sively watching video and taking written tests. “Assessments are incorporated directly into the medical VR models. We will design situations where participants are re-quired to make the appropriate decisions about proper tech-niques. The Virtual CPR instructional will measure metrics and provide real-time feedback ensuring participants accurately perform CPR techniques. Further, the instructional will explain
any mistake and prompt users to try again when errors are made. Supportive messages are delivered upon success,” states Mary Spio CEO, Next Galaxy Corp.
The medical VR models will be viewable through smartphones and desktops as 3D, and via VR devices such as Google Cardboard, VRONE and Oculus Rift.
Next Galaxy Corporation is a leading developer of innovative content solutions and fully Immersive Consumer Virtual Real-ity technology. The Company's flagship consumer product in development is CEEK, a next-generation fully immersive en-tertainment and educational social virtual reality platform fea-turing a combination of live action and 3D experiences. Next Galaxy's CEEK simulates the communal experience of attend-ing events, such as concerts, sporting events, movies or con-ferences through Virtual Reality. Next Galaxy is developing entertainment and educational experiences for VR Cinema, VR Concerts, VR Sports, VR Business, VR Tourism and more. In short, Next Galaxy is building the meeting places of the fu-ture. For further information, visit www.nextgalaxycorp.com.
Low Birth Weight and Childhood Infections Predict Ankylosing Spondylitis
The results of a study presented June 11th at the European League Against Rheumatism Annual Congress (EULAR 2015) Press Conference showed that a diagnosis of Ankylosing Spondylitis (AS) can be predicted by low birth weight, having older siblings and hospitalisation for infection between the ages of 5-16 years. These data suggest that these factors play an important role in the pathogenesis of the disease.
AS is a painful and progressive form of arthritis caused by chronic inflammation of the joints in the spine. Prevalence of AS varies globally, and is estimated at 23.8 per 10,000 in Europe and 31.9 per 10,000 in North America.
The cause of AS is unknown. Although AS is strongly associ-ated with the genotype HLA-B27, not everyone testing positive for the marker goes on to develop the disease.
"A link between AS and the HLA-B27 genotype was established more than three decades ago, yet studies on the environmental risk factors are few," said study investigator Dr. Ulf Lindström, Institute of Medicine, Rheumatology and Inflammation Re-search, Sahlgrenska Academy, Sweden. "Our research has identified three factors associated with significantly increased risk of the disease in later life. These data strengthen our un-derstanding of the interplay between genetics and environment in AS, and bring us closer to pinpointing the underlying cause of the disease."
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 13
®
Bar w SyndromeFound G on
Barth Syndrome FoundationSmtoms:
Cardiomyopathy, Neutropenia, Muscle Weakness,Exercise Intolerance, Growth Delay, Cardiolipin Abnormalities
www.barthsyndrome_org

Statistically significant increased risks were observed for birth weight under 3,000g (18% vs. 15%), having older siblings (63% vs. 58%) and for hospitalisation due to infec-tions at age 5-12 (5% vs. 3%) and age 13-16 (2% vs. 1%). These factors have been implicated in other, associated disease; the triggering effect of infections in reactive ar-thritis has been established, birth weight has been shown to predict development of autoimmune disease (diabetes and rheumatoid arthritis), and a link between older siblings and disease risk has been demonstrated in asthma. Data from several Swedish national registers were used for this study, with five matched controls (sex, age, county) identified for each case of AS. Exposures assessed were birth weight, gestational age, type of birth (single/multiple), number of older siblings and exposure to infections.
How Does Human Behavior Lead to Surgical Errors? Mayo Clinic Researchers Count the Ways - Four to Nine Factors Contributed to Each `Never Event’
Newswise- Why are major surgical errors called “never events?” Because they shouldn’t happen — but do. Mayo Clinic researchers identified 69 never events among 1.5 million invasive procedures performed over five years and detailed why each occurred. Using a system created to investigate military plane crashes, they coded the human behaviors involved to identify any environmental, organ-izational, job and individual characteristics that led to the never events. Their discovery: 628 human factors contrib-uted to the errors overall, roughly four to nine per event. The study results were published in the journal Surgery.
The never events included performing the wrong proce-dure (24), performing surgery on the wrong site or wrong side of the body (22), putting in the wrong implant (5), or leaving an object in the patient (18). All of the errors ana-lyzed occurred at Mayo; none were fatal.
The Mayo Rochester campus rate of never events over the period studied was roughly 1 in every 22,000 procedures. Because of inconsistencies in definitions and reporting requirements, it is hard to find accurate comparison data, but a recent study based upon information in the National Practitioner Data Bank estimated that the rate of such never events in the United States is almost twice that in this report, approximately 1 in 12,000 procedures.
Nearly two-thirds of the Mayo never events occurred dur-ing relatively minor procedures such as anesthetic blocks, line placements, interventional radiology procedures, en-doscopy and other skin and soft tissue procedures.
Medical teams are highly motivated and skilled, yet pre-venting never events entirely remains elusive, says senior author Juliane Bingener, MD, a gastroenterologic surgeon at Mayo Clinic. The finding that factors beyond “cowboy-type” behavior were to blame points to the complexity of preventing never events, she says.
“What it tells you is that multiple things have to happen for an error to happen,” Dr. Bingener says. “We need to make sure that the team is vigilant and knows that it is not only OK, but is critical that team members alert each other to potential problems. Speaking up and taking advantage of all the team’s capacity to prevent errors is very important, and adding systems approaches as well.”
For example, to help prevent surgical sponges from being left in patients, Mayo Clinic installed a sponge-counting system and uses that bar code-scanning system and vigi-lance by the surgical team to track sponges. Other preven-tive systems include use of The Joint Commission Health Care Quality Organization’s Universal Protocol, team brief-ings and huddles before a surgery starts, a pause before the first incision is made, and debriefings using a World Health Organization-recommended safety checklist.
To investigate the never events, the researchers used hu-man factors analysis, a system first developed to investi-gate military aviation accidents. They grouped errors into four levels that included dozens of factors:• “Preconditions for action,” such as poor hand-offs, dis-
tractions, overconfidence, stress, mental fatigue and inadequate communication. This category also in-cludes channeled attention on a single issue: In lay-man’s terms, focusing so much on a tree that one can-not see the forest.
• Unsafe actions, such as bending or breaking rules or failing to understand. This category includes percep-tual errors such as confirmation bias, in which sur-geons or others convinced themselves they were see-ing what they thought they should be seeing.
• Oversight and supervisory factors: Inadequate super-vision, staffing deficiencies and planning problems, for example.
• Organizational influences: Problems with organiza-tional culture or operational processes.
In addition to systems approaches and efforts to improve communication, attention should be paid to cognitive ca-pacity, such as team composition, technology interfaces, time pressures and individual fatigue, the researchers say.
The stakes are high for patients, physicians and hospitals, Dr. Bingener says.
“The most important piece is the patient perspective. You don’t want a patient to have to experience a never event. The breach in trust that happens with that is the most im-portant part,” she says.
The study was funded in part by National Institute of Dia-betes and Digest ive and Kidney Diseases grant K23DK93553. The research team included members of the Mayo Clinic Department of Surgery, the Robert D. and Pa-tricia E. Kern Center for the Science of Health Care Deliv-ery, Quality Management Services and Pulmonary and Critical Care Medicine.
Disclosures: Dr. Bingener is supported through an NIDDK research grant, specified research through Nestle and
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 14

Stryker Endoscopy, has received travel support from Intuitive Surgical, and serves on Titan Medical’s Sur-geon Advisory Board. Co-author Su-san Hallbeck, PhD, receives grant funding from Stryker Endoscopy.
Genetic Risk Factor for Premature Birth Found
Newswise — Researchers at the Uni-versity of California, San Diego School of Medicine have discovered a genetic risk factor for premature birth. The risk factor is related to a gene that codes for a protein that the scien-tists have found helps the body’s im-mune cells recognize and fight Group B Streptococcus (GBS) bacteria.
These bacteria are found in the va-gina or lower gastrointestinal tract of approximately 15 to 20 percent of healthy women, but may cause life-threatening infections, such as sepsis or meningitis in newborns, especially those born prematurely.
The study was published online in the May 5th, 2014 issue of the Journal of Experimental Medicine.
“Pregnant women are universally screened for these bacteria during pregnancy and administered antibiot-ics intravenously during labor if they test positive to protect the infant from infection," said Victor Nizet, MD, Pro-fessor of Pediatrics and Pharmacy and co-author. “Our research may explain why some women and their infants are at higher risk of acquiring severe GBS infections than others.”
In the study, scientists identified two proteins on fetal membranes of the placenta that are involved in immune function. One of the proteins (known as Siglec-5) binds to the GBS patho-gen and suppresses immune re-sponse to the microbe, while the other protein (known as Siglec-14) binds to the pathogen, and activates
killing of the bacteria. Siglecs are cell surface receptors found typically on immune cells. They recognize (bind) sialic acids - sugar molecules that densely coat our cells.
“We have one protein that tells the body to attack the pathogen and an-other that tells the body not to attack it,” said Raza Ali, PhD, a project sci-entist in the Nizet laboratory and the study’s lead author.
Scientists believe that the pair of pro-teins together helps balance the body’s immune response to patho-gens, by directing some antimicrobial response without provoking excessive inflammation.
“Identifying the dual role of these re-ceptors and how they are regulated may provide insight for future treat-ments against GBS,” Ali said.
Interestingly, the gene for Siglec-14 is missing in some individuals, and the researchers have found that fetuses that lack the Siglec-14 protein are at higher risk of premature birth, likely due to an imbalanced immune re-sponse to the bacterial infection.
“We found this association in GBS-positive but not GBS-negative preg-nancies, highlighting the importance of GBS-siglec crosstalk on placental membranes,” said Ajit Varki, MD, Dis-tinguished Professor of Medicine and Cellular and Molecular Medicine and study co-author.
For reasons not completely under-stood, GBS infections are not found in any other animals, including chim-panzees, which share 99% of human protein sequences. “The expression of the two siglec proteins on the fetal membranes is also unique to hu-mans,” Varki said. “Our study offers intriguing insights into why certain bacterial pathogens may produce uniquely human diseases.”
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 15
2nd Annual Basic & Advanced Fetal Cardiac Symposium and Workshop
Rush University Medical CenterSep 10-12, 2015; Chicago, IL USAwww.FetalCardiacSymposium.com
NEONATOLOGY TODAY
Sponsorships and
Recruitment Advertising
For information on sponsor-ships or recruitment advertis-ing, contact Tony Carlson at: 301.279.2005 or send email to: [email protected]
' FCSl*‘l+J'l‘.\ I. 1. ;\ [:1 )Lu‘ tauS\’)l[’()Sll..T)l 15

The scientists believe that identifying the mechanisms of siglec protein ac-tion may help in designing therapeu-tic targets against bacterial infections that are becoming increasingly resis-tant to antibiotics and could have important implications for other dis-orders, such as blood c lot t ing, chronic diseases and HIV infections.Co-authors include: Jerry J. Fong, Aaron F. Carlin, Rebecka Linden, Mana Parast, UC San Diego; Tamara Busch and Jeffrey Murray, University of Iowa; Takashi Angata, Academia S i n i c a , Ta i w a n a n d T h o m a s Areschoug, Lund University, Sweden.
Funding for this research came, in part, from the National Institutes of Health (grants P01HL107150 and AI057153).
Disclosure: Ajit Varki has an equity interest in Sialix, Inc., which is de-veloping products based on new dis-coveries of non-human sialic acids and their potential impact on cancer, c a r d i o v a s c u l a r a n d o t h e r inflammatory-mediated disease. He is also a scientific advisor to the company and a member its board of directors.
NEONATOLOGY TODAY ! www.NeonatologyToday.net ! August 2015 16
NEONATOLOGY TODAY
© 2015 by Neonatology Today ISSN: 1932-7137 (digital). Published monthly. All rights reserved.
Publication Headquarters8100 Leaward WayPO Box 444Manzanita, OR 97130 USAwww.NeonatologyToday.net
Publishing Management
• Tony Carlson, Founder, President & Senior Editor - [email protected]
• Richard Koulbanis, Group Publisher & Editor-in-Chief - [email protected]
• John W. Moore, MD, MPH, Group Medical Editor - [email protected]
• Caryl Cornell, Assistant Editor • Virginia Dematatis, Assistant Editor• Loraine Watts, Assistant Editor • Chris Carlson, Web Manager• Rob Hudgins, Special Projects
Designer
Editorial Board
Dilip R. Bhatt, MD; Barry D. Chandler, MD; Anthony C. Chang, MD; K. K. Diwakar, MD; Willa H. Drummond, MD, MS (Informatics); Philippe S. Friedlich, MD; Mitchell Goldstein, MD; Lucky Jain, MD; Prakash Kabbur, MBBS, DCH (UK), MRCPCH (UK); Patrick McNamara, MD; David A. Munson, MD; Michael A. Posencheg, MD; DeWayne Pursley, MD, MPH; Joseph Schulman, MD, MS; Alan R. Spitzer, MD; Dharmapuri Vidysagar, MD; Leonard E. Weisman, MD; Stephen Welty, MD; Robert White, MD; T.F. Yeh, MD FREE Digital Subscription to Qualified Professionals
Neonatology Today is available free to qualified medical professionals worldwide in neonatology and perinatology. Send an email to: [email protected]. Include your name, title(s), organization, address, phone, fax and email.
Sponsorships and Recruitment Advertising
For information on sponsorships or re-cruitment advertising, call Tony Carlson at: 301.279.2005, or send email to: [email protected]
N E O N A T O L O G Y T O D A Y
CALL FOR CASES AND OTHER ORIGINAL ARTICLES
Do you have interesting research re-sults, observations, human interest sto-ries, reports of meetings, etc. to share?
Submit your manuscript to: [email protected]
• Title page should contain a brief title and full names of all authors, their professional degrees, and their institu-tional affiliations. The principal author should be identified as the first author. Contact information for the principal author including phone num-ber, fax number, email address, and mailing address should be included.
• Optionally, a picture of the author(s) may be submitted.
• No abstract should be submitted.• The main text of the article should be
written in informal style using correct English. The final manuscript may be between 400-4,000 words, and con-tain pictures, graphs, charts and ta-bles. Accepted manuscripts will be published within 1-3 months of re-ceipt. Abbreviations which are com-monplace in pediatric cardiology or in the lay literature may be used.
• Comprehensive references are not required. We recommend that you provide only the most important and relevant references using the stan-dard format.
• Figures should be submitted sepa-rately as individual separate elec-tronic files. Numbered figure cap-tions should be included in the main Word file after the references. Cap-tions should be brief.
• Only articles that have not been pub-lished previously will be considered for publication.
• Published articles become the prop-erty of Neonatology Today, and may not be published, copied or repro-duced elsewhere without permission from Neonatology Today.
Upcoming Meetings
9th International Conference on Brain Monitoring and
Neuroprotection in the Newborn - 2015 Symposium
Oct. 1 – 3, 2015; Cork, Irelandhttp://newbornbrain2015.com
NPA & National Advocates for Pregnant Woman -
Pregnant Women, Drug Use, and NAS: Experts Share Science & Strategies That Help Women,
Babies, and FamiliesOct. 2 – 3, 2015; Nashville, TN USA
www.nationalperinatal.org
International Cardiology Neonatology Symposium
Oct. 8-10, 2015; Miami, FL USAwww.neocardisymposium.com

NEONATOLOGY TODAYN e w s a n d I n f o r m a t i o n f o r B C / B E N e o n a t o l o g i s t s a n d P e r i n a t o l o g i s t s
About Neonatology TodayNeonatology Today (NT) is the leading monthly publication that goes to over 3,000 BC/BE neonatologists, Perinatologists, Fel-lows, NNPs, and their NICU teams. Neonatology Today provides timely news and information regarding the care of newborns, and the diagnosis and treatment of premature and/or sick infants. In addition, NT publishes special issues, directories, meeting agendas and meeting dailies around key meetings.
Free Subscription to Neonatologists and their NICU Team MembersNeonatology Today is available digitally worldwide for Neonatologists, Perinatologists, Fellows, NNPs and their NICU teams. To receive your free qualified subscription, simply send an email to: [email protected]. Be sure to include your name, title, organization or hospital, and email to receive your free subscription.
Submitting Manuscripts to Neonatology TodayInterested in submitting a Case Study, Research Results, Hospital News, Human Interest stories, and/or Meeting information? Send it by email to: Richard Koulbanis, Group Publisher and Editor-in-Chief [email protected]. We are often able to publish accepted manuscripts within 1-3 months of receipt.
Sponsorships and Recruitment AdvertisingInterested in receiving information on sponsorship availability or recruitment advertising? There are various sponsorship and recruitment options available. If needed, Neonatology Today will even create the ad for you at no additional cost. For more information please contact Tony Carlson, Founder and Senior Editor, phone: +1(301) 279-2005, or by email: [email protected].
Key ContactsTony Carlson - Founder, President & Senior Editor - [email protected] or call +1.301.279.2005Richard Koulbanis - Group Publisher & Editor-in-Chief - [email protected] W. Moore, MD, MPH, Group Medical Editor - [email protected]
Publishers of CONGENITAL CARDIOLOGY TODAY - www.CongenitalCardiologyToday.com
w w w . N E O N A T O L O G Y T O D A Y . n e t
NEWBORN INTENSIVE CARE UNITS {NICUS} ANDNEONATCILOGISTS OF THE USA & CANADA
DIRECTR? 2011
u...:.
NEONATOL GY TOD
Tetralngv of Fallot in the Nemtata
u;'
_‘
-4" . . . ..=‘ woma I .
n .. ....... -we... A-wuwnn rod»_
a-u.—-a «mu m,«..« «mam -.4 0.
3.. am: -ya-«Jae. -r. .uIn-I\a.'ru4Iuwlk:|-mun:
vliluunnrlnl uum
Imm,-y .. mr .‘c.=. . .. .4-: aw...mm. Lorb-u -um “-3
w|=wurzrIIIwn-':.l9~tII
.r.-u;-—n.—mu -up-.-cg...
an!“I |:rJnl'.IJ-\lnItIIl'|rI:I.u\nJl
. . -. .v n-pr -an-mm-as-..m....
1.-...:.-.........w...... M~_..,;-J-»“\___ W, 451:,..,..., , my ~'¢....-—-,...~v- wt 4- ... _,,,...:v_‘‘,__,.';_
.4.»-*"
. 11."V37: ‘I: W"’4 Farr ”a""’D\°ryM
-.«:.i./.1_r,,,f>”’V-‘r-.-1:9‘, '71
K