Embed Size (px)
Citation preview

Dr Sumesh Thomas
Neonatologist & Clinical Associate ProfessorUniversity of Calgary (Canada)
Director – Southern Alberta Neonatal Transport ServiceAlberta Health Service
MD, FRCP(Edin), FRCPCH, FRCPC
POCUS in Neonatology, Neonatal Transport

Value of early ECHO in ELBW neonates
NEOCON Hyderabad Dec 2019
Dr Sumesh Thomas MB.BS, DCH(UK), FRCPCH (UK), FRCP (Edin), FRCPC – Director SCAN program


>1200 babies admitted to Tertiary Care NICU annually
ELBW babies – 120 annually
22,500 births in Southern Alberta

Foothills Medical Centre

What is ‘value’ to an ELBW infant?


Neonatology -Timelines
1900s – Incubator shows
1950s – Silverman showed benefits
thermoregulation
60’s Basic &
experimental
Focus on lung
Surfactant deficiency identified
70’s
32-36 wks Assisted Ventilation
Establishment of NICUs
80’s
28-32 wks
Surfactant Technologic advances Brain injury
90’s
24-28 wks VentilatorsOutcomes
IVF
Parental role
Post 2000
23-25 wks
Functional outcomes
Cultural diversity
Parent driven
Internet Information

Accepted strategies aimed at Neuroprotection
• Minimal Handling
‘less is better’
• Gentle ventilation
• Optimal growth and nutrition
Avoidance of iatrogenic harm

Typical indications for early ECHO
• Neonatal Hypotension
• Hemodynamically significant PDA
• Pulmonary Hypertension of the Newborn (PPHN)
• Central Line Placement
• Suspected Effusions
• Congenital Heart Disease – cardiologist

POC Neonatal UltrasoundResults: 321 articles – 6 Dec 2019 ( 26 articles on Feb 2014)
1. Investigating the European perspective of neonatal point-of-care echocardiography in the neonatal intensive care unit--a pilot study
Roehr CC et al Eur J Pediatr. 2013 Jul;172(7):907-11
2. Confirmation of correct tracheal tube placement in newborn infants
Schmölzer GM et al . Resuscitation. 2013 Jun 84(6):731-7
3. Utility of targeted neonatal echocardiography in the management of neonatal illnessHarabor A, Soraisham AS J Ultrasound Med 2015; 34(7);1259-63
4. Ultrasound assessment of umbilical venous catheter migration in preterm infants: a prospective study.
Franta J, Harabor A, Soraisham AS. Arch Dis Child Fetal Neonatal Ed. 2017 May;102(3):F251-F255

Targeted examination – ‘minimal handling’
• Evaluate a specific clinical question
• Focused examination with essential views and measurements
Not a ‘fishing’ exercise

Routine ECHO
• Non-focused examination
• Significantly longer examination
Could result in further interventions and or evaluation with limited benefits / potential harm

Neither approach is a substitute for knowledge of ‘neonatal transitional physiology’

PDA – to treat or not to treat?Determining hemodynamic significance (HS)
Indicators of pulmonary over-circulation• Pulmonary hemorrhage• Failed extubation/inability to wean ventilation• Worsening of oxygenation and/or CO2 retention• CXR : cardiomegaly and pulmonary congestion
Indicators of systemic hypo-perfusion• Diastolic BP < 3rd percentile for GA• Systolic and diastolic BP < 3rd percentile for GA with the requirement for
inotropic support• Lactic acidosis unexplained by other causes • Renal impairment with oliguria

Complete Left to Right

Hs PDA
• Identify PDA and determine size
• Determine direction of flow and max velocity across shunt
• Evaluate for left sided volume overload
• Assess end organ perfusion (SMA/CA/MCA)

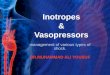
Pulmonary hypertension
Right ventricular hypertrophy
Deviation of IVS to the Left/flattening
Tricuspid regurgitation (TR)
Right to left or bidirectional shunting at PFO / PDA
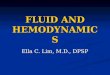
Rt. V systolic pressure calculationBernoulli equation4v2 + Right atrial pressure (~4mmHg),v = maximal velocity of the TR jet in m/s.

RVH / Septal deviation

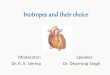
Tricuspid Regurgitation

Peak tricuspid regurgitation (TR) velocity 3.9 m/sec
Bernoulli equation4v2 + Right atrial pressure (~4mmHg),v = maximal velocity of the TR jet in m/s.
Gradient across the tricuspid valve 63 mmHg. Pulmonary artery pressure estimated at 68-73 mmHg
Systemic BP 54/32 Mean 41mmHg

Cardiac Contractility

UVC position

Cardiac Tamponade

Value? – Food for thought

Hemodynamics – changing practices
• Delayed cord clamping when feasible
• Cautious use of inotropes – consider bedside ECHO• hyperinflation and iatrogenic hypotension / raised SVC pressure
• Fluid status / potential insensible water losses
• Cautious use of fluid boluses – consider bedside ECHO if considering >10ml/kg volume in the absence of supportive history

Position
Stimulation
Assessment of breathing at 30 seconds

I need my blood!!

Take home message
• There is a place for early ‘focused’ ECHO examinations – to support clinical decision making and improve procedural success
• Interpretation of ECHO finding requires • In-depth understanding of neonatal transitional physiology
• Recognition of iatrogenic contribution from medical interventions
• Awareness of current controversies regarding treatment options



Physiological changes…in nature
• Infant cries
• Functional Residual Capacity
• Pulmonary Vascular Resistance
• RV Output, PVD & Lung perfusion
• Blood return to LA
• LV filling & output
• PDA flow
• Cord is severed
Net effect systemic perfusion Drawings by A.M. Rudolph Circ Res, 57:811, 1985

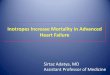
• In the Vent-1st
group, HR and RVO remain stable throughout
Both Groups: HR & RVO
Bhatt et al. J Physiol 2013; 591:2113-26; Figure
courtesy: Dr. Stuart Hooper
“Vent first”
“Clamp first”

Immediate cord clamping
• UV clamped
• Right ventricle (RV) preload
• UA clamped
• Increase in LV after-load
• No lung expansion
• Pulmonary perfusion and pulmonary venous return to LA
• RV output to LA
Net Effect systemic perfusion