Embed Size (px)
Citation preview
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r. com/ loca te / ea r l humdev
Early Human Development (2008) 84, 499–506
BEST PRACTICE GUIDELINE ARTICLE
Neonatal thrombocytopenia: What we do anddon't know☆
Martha Sola-Visner a,⁎, Matthew A. Saxonhouse b,1, Rachel E. Brown c,1
a Drexel University College of Medicine, and St. Christopher's Hospital for Children,Drexel University Neonatology Research at MCP, 3300 Henry Avenue, 7th Floor Heritage Building,Philadelphia, PA 19129, United Statesb Division of Neonatology, University of Florida, PO Box 100296, 1600 SW Archer Road, Gainesville, FL 32610, United Statesc Department of Pediatrics, University of Florida, PO Box 100296, 1600 SWArcher Road, Gainesville, FL 32610, United States
☆ This work was supported by Grant NFlorida/Puerto Rico Affiliate (MS), and⁎ Corresponding author. Tel.: +1 215E-mail addresses: Martha.Sola-Visne
(R.E. Brown).1 Tel.: +1 352 392 4195; fax: +1 352 3
0378-3782/$ - see front matter © 200doi:10.1016/j.earlhumdev.2008.06.004
Abstract
The evaluation and management of thrombocytopenia is a frequent challenge for neonatologists,as it affects 22–35% of infants admitted to the neonatal intensive care unit. Multiple diseaseprocesses can cause neonatal thrombocytopenia, and these can be classified as those inducingearly thrombocytopenia (≤72 h of life) and those inducing late-onset thrombocytopenia (N72 h).Most cases of neonatal thrombocytopenia aremild tomoderate, and do not warrant intervention. Inapproximately 25% of affected neonates, however, the platelets count is b50×109/L, and therapywith platelet transfusions is considered to decrease the risk of hemorrhage. The existing evidence toestablish platelet transfusion triggers in neonates is very limited, but it suggests that transfusingplatelets to non-bleeding neonates with platelet counts N50×109/L does not decrease the risk ofintraventricular hemorrhage (IVH), and that 30×109/L might be an adequate threshold for stablenon-bleeding neonates. However, adequately powered multi-center studies are needed toconclusively establish the safety of any given set of neonatal transfusion guidelines.© 2008 Published by Elsevier Ireland Ltd.
KEYWORDSNeonates;Neonatalthrombocytopenia;Platelet;Transfusions
Contents
1. Definition and incidence of neonatal thrombocytopenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5002. Platelet production in neonates and mechanisms of thrombocytopenia . . . . . . . . . . . . . . . . . . . . . . . . 5003. Causes of neonatal thrombocytopenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 500
o. HL69990 from the National Institutes of Health (MSV), a grant from the American Heart Association,a grant from the University of Florida Children's Miracle Network (RB).842 4960; fax: +1 215 843 [email protected] (M. Sola-Visner), [email protected] (M.A. Saxonhouse), [email protected]
92 4533.
8 Published by Elsevier Ireland Ltd.

500 M. Sola-Visner et al.
4. Approach to the thrombocytopenic neonate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5005. Early-onset thrombocytopenia (Fig. 1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5016. Late onset thrombocytopenia (Fig. 2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5027. Treatment of neonatal thrombocytopenia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 503
7.1. Platelet transfusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5038. Thrombopoietic growth factors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5059. Research directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 505
10. Key guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 506
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5061. Definition and incidence ofneonatal thrombocytopenia
During fetal life, the platelet count progressively increases andreaches a level of approximately 150×109/L by the end of thefirst trimester. Thus, healthy fetuses and neonates at gesta-tional ages≥22 weeks have platelet counts within the normalrange for adults (150–450×109/L), and therefore neonatalthrombocytopenia is defined as a platelet count b150×109/Lregardless of gestational age. However, platelet counts in the100–150×109/L range are somewhat more common amonghealthy neonates than among healthy adults. For that reason,careful follow-up and expectant management in an otherwisehealthy appearing neonate with transient thrombocytopeniain this mild range is acceptable, although lack of quickresolution, worsening of thrombocytopenia, or changes inclinical condition should prompt further evaluation.
The incidence of thrombocytopenia in neonates variessignificantly, depending on the population studied. Specifi-cally, while the overall incidence of neonatal thrombocyto-penia is relatively low (0.7–0.9%), the incidence amongneonates admitted to the Neonatal Intensive Care Unit(NICU) is very high (22–35%). In this review, we will focus onthe common varieties of thrombocytopenia seen in the NICU.
2. Platelet production in neonates andmechanisms of thrombocytopenia
Overall, the mechanisms underlying thrombocytopenia inneonates are the same as in adults: increased plateletconsumption, decreased platelet production, hypersplen-ism, or a combination of these. Unlike in adults, however, theresponsible mechanism(s) are not always clearly identified inneonates with thrombocytopenia, mostly because of thedifficulties associated with performing the gold standardtests (bone marrow biopsy/aspirate and/or radiolabelledplatelet kinetic studies) in sick neonates. The existingevidence suggests that the mechanisms underlying neonatalthrombocytopenia are variable, depending on the etiology.For example, increased platelet consumption underlies thethrombocytopenia of sepsis or necrotizing enterocolitis(NEC), while decreased platelet production is thought tounderlie the thrombocytopenia seen in neonates born tomothers with severe placental insufficiency [1].
Recently, it has beenhypothesized that a relative decrease inplatelet production might contribute to most cases of neonatalthrombocytopenia. In this regard, the rather complex process ofproducing and releasing platelets can be schematically repre-sented as consisting of four main steps: 1) the production of
thrombopoietic cytokines (mostly thrombopoietin, produced inthe liver); 2) the proliferation of megakaryocyte progenitors(the cells that give rise tomegakaryocytes); 3) thematuration ofmegakaryocytes into large, polyploid cells capable of producingplatelets; and 4) the release of platelets into the circulation.Although, in general, these steps are the same in neonates andadults, there are important developmental differences thatmight explain the predisposition of sick neonates to developthrombocytopenia in response to illness. Specifically, megakar-yocytes in neonates are smaller and less mature thanmegakaryocytes in adults, and it is known that smallermegakaryocytes produce less platelets than larger,morematuremegakaryocytes. This developmental feature might limit theability of neonates to increaseplatelet production in response toplatelet consumption, if (like recent evidence suggests)neonates are unable to increase the size and ploidy of theirmegakaryocytes [2]. In addition, preterm neonates seem tohave relatively low levels of thrombopoietin during thrombocy-topenia, which might limit their ability to rapidly up-regulateplatelet production in times of increased platelet consumption.
3. Causes of neonatal thrombocytopenia
In contrast to the limited number of mechanisms thatunderlie thrombocytopenia, there are a large number ofdisease processes that have been associated with thrombo-cytopenia in neonates. In most cases, the underlying etiologyis suggested by the pattern of the thrombocytopenia (time ofpresentation, severity, duration, and response to transfu-sions) and the constellation of presenting clinical signs.Table 1 displays the most common (and some less common)causes of thrombocytopenia among NICU patients, as well asthe typical features of each. For practicing neonatologists,the first step in the approach to the thrombocytopenicneonate is to attempt to recognize a pattern suggestive of aspecific etiology. However, this task can be complicated bythe existence of significant overlap between the differentclinical conditions, and by the frequent co-existence of morethan one likely cause of thrombocytopenia (i.e. the pretermneonate born to a mother with severe pregnancy-inducedhypertension who develops necrotizing enterocolitis).
4. Approach to the thrombocytopenic neonate
Figs. 1 and 2 provide algorithms for the evaluation ofthrombocytopenic neonates with early-onset and late-onsetthrombocytopenia, respectively. In general, thrombocyto-penia identified within the first 72 h of life (early-onset) iscaused by conditions different from those that cause
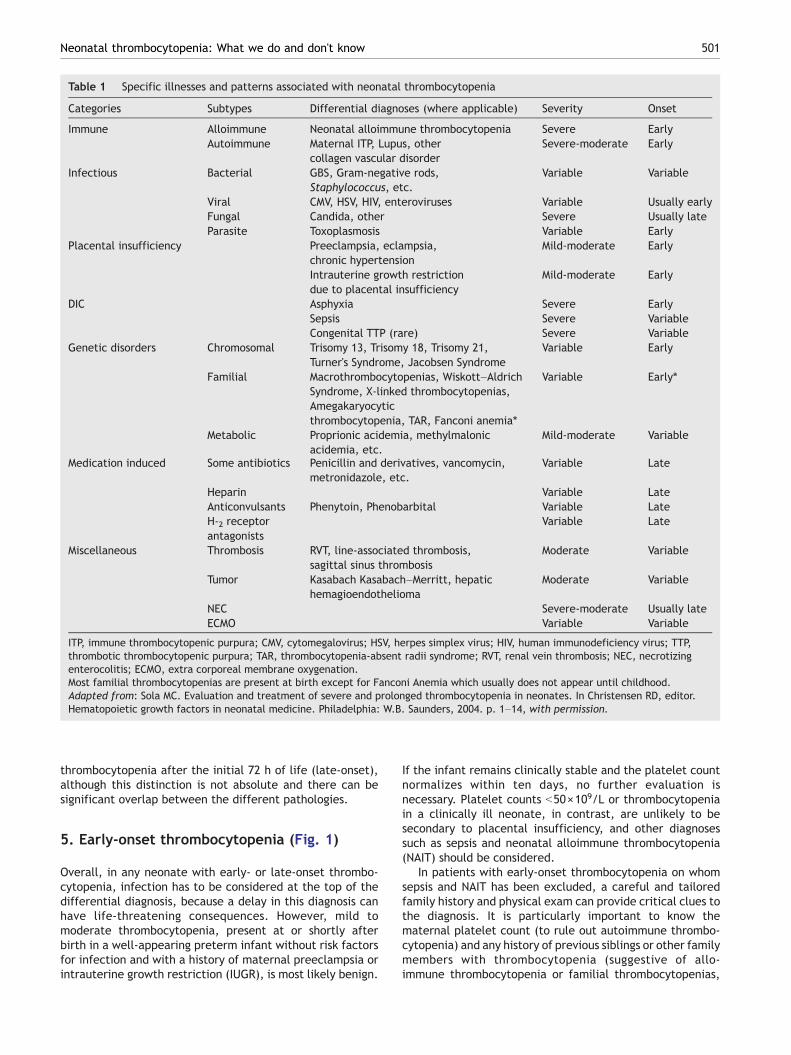
Table 1 Specific illnesses and patterns associated with neonatal thrombocytopenia
Categories Subtypes Differential diagnoses (where applicable) Severity Onset
Immune Alloimmune Neonatal alloimmune thrombocytopenia Severe EarlyAutoimmune Maternal ITP, Lupus, other
collagen vascular disorderSevere-moderate Early
Infectious Bacterial GBS, Gram-negative rods,Staphylococcus, etc.
Variable Variable
Viral CMV, HSV, HIV, enteroviruses Variable Usually earlyFungal Candida, other Severe Usually lateParasite Toxoplasmosis Variable Early
Placental insufficiency Preeclampsia, eclampsia,chronic hypertension
Mild-moderate Early
Intrauterine growth restrictiondue to placental insufficiency
Mild-moderate Early
DIC Asphyxia Severe EarlySepsis Severe VariableCongenital TTP (rare) Severe Variable
Genetic disorders Chromosomal Trisomy 13, Trisomy 18, Trisomy 21,Turner's Syndrome, Jacobsen Syndrome
Variable Early
Familial Macrothrombocytopenias, Wiskott–AldrichSyndrome, X-linked thrombocytopenias,Amegakaryocyticthrombocytopenia, TAR, Fanconi anemia⁎
Variable Early⁎
Metabolic Proprionic acidemia, methylmalonicacidemia, etc.
Mild-moderate Variable
Medication induced Some antibiotics Penicillin and derivatives, vancomycin,metronidazole, etc.
Variable Late
Heparin Variable LateAnticonvulsants Phenytoin, Phenobarbital Variable LateH-2 receptorantagonists
Variable Late
Miscellaneous Thrombosis RVT, line-associated thrombosis,sagittal sinus thrombosis
Moderate Variable
Tumor Kasabach Kasabach–Merritt, hepatichemagioendothelioma
Moderate Variable
NEC Severe-moderate Usually lateECMO Variable Variable
ITP, immune thrombocytopenic purpura; CMV, cytomegalovirus; HSV, herpes simplex virus; HIV, human immunodeficiency virus; TTP,thrombotic thrombocytopenic purpura; TAR, thrombocytopenia-absent radii syndrome; RVT, renal vein thrombosis; NEC, necrotizingenterocolitis; ECMO, extra corporeal membrane oxygenation.Most familial thrombocytopenias are present at birth except for Fanconi Anemia which usually does not appear until childhood.Adapted from: Sola MC. Evaluation and treatment of severe and prolonged thrombocytopenia in neonates. In Christensen RD, editor.Hematopoietic growth factors in neonatal medicine. Philadelphia: W.B. Saunders, 2004. p. 1–14, with permission.
501Neonatal thrombocytopenia: What we do and don't know
thrombocytopenia after the initial 72 h of life (late-onset),although this distinction is not absolute and there can besignificant overlap between the different pathologies.
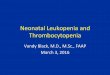
5. Early-onset thrombocytopenia (Fig. 1)
Overall, in any neonate with early- or late-onset thrombo-cytopenia, infection has to be considered at the top of thedifferential diagnosis, because a delay in this diagnosis canhave life-threatening consequences. However, mild tomoderate thrombocytopenia, present at or shortly afterbirth in a well-appearing preterm infant without risk factorsfor infection and with a history of maternal preeclampsia orintrauterine growth restriction (IUGR), is most likely benign.
If the infant remains clinically stable and the platelet countnormalizes within ten days, no further evaluation isnecessary. Platelet counts b50×109/L or thrombocytopeniain a clinically ill neonate, in contrast, are unlikely to besecondary to placental insufficiency, and other diagnosessuch as sepsis and neonatal alloimmune thrombocytopenia(NAIT) should be considered.
In patients with early-onset thrombocytopenia on whomsepsis and NAIT has been excluded, a careful and tailoredfamily history and physical exam can provide critical clues tothe diagnosis. It is particularly important to know thematernal platelet count (to rule out autoimmune thrombo-cytopenia) and any history of previous siblings or other familymembers with thrombocytopenia (suggestive of allo-immune thrombocytopenia or familial thrombocytopenias,
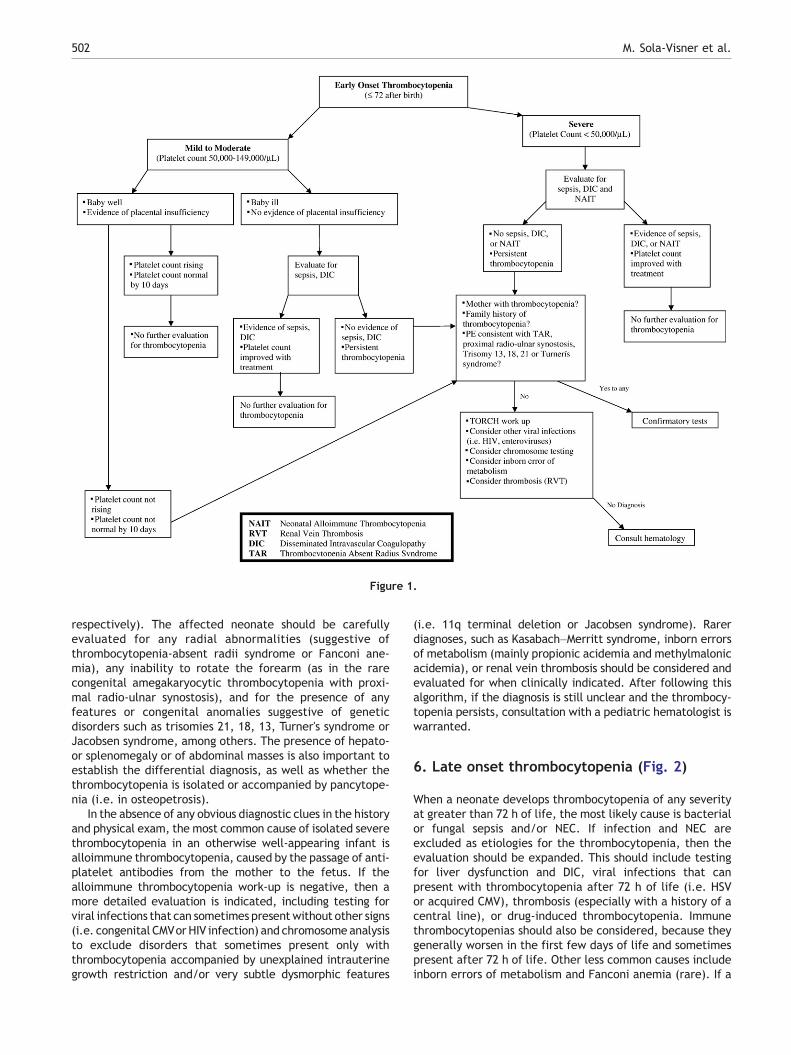
Figure 1.
502 M. Sola-Visner et al.
respectively). The affected neonate should be carefullyevaluated for any radial abnormalities (suggestive ofthrombocytopenia-absent radii syndrome or Fanconi ane-mia), any inability to rotate the forearm (as in the rarecongenital amegakaryocytic thrombocytopenia with proxi-mal radio-ulnar synostosis), and for the presence of anyfeatures or congenital anomalies suggestive of geneticdisorders such as trisomies 21, 18, 13, Turner's syndrome orJacobsen syndrome, among others. The presence of hepato-or splenomegaly or of abdominal masses is also important toestablish the differential diagnosis, as well as whether thethrombocytopenia is isolated or accompanied by pancytope-nia (i.e. in osteopetrosis).
In the absence of any obvious diagnostic clues in the historyand physical exam, the most common cause of isolated severethrombocytopenia in an otherwise well-appearing infant isalloimmune thrombocytopenia, caused by the passage of anti-platelet antibodies from the mother to the fetus. If thealloimmune thrombocytopenia work-up is negative, then amore detailed evaluation is indicated, including testing forviral infections that can sometimes presentwithout other signs(i.e. congenital CMVor HIV infection) and chromosome analysisto exclude disorders that sometimes present only withthrombocytopenia accompanied by unexplained intrauterinegrowth restriction and/or very subtle dysmorphic features
(i.e. 11q terminal deletion or Jacobsen syndrome). Rarerdiagnoses, such as Kasabach–Merritt syndrome, inborn errorsof metabolism (mainly propionic acidemia and methylmalonicacidemia), or renal vein thrombosis should be considered andevaluated for when clinically indicated. After following thisalgorithm, if the diagnosis is still unclear and the thrombocy-topenia persists, consultation with a pediatric hematologist iswarranted.
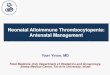
6. Late onset thrombocytopenia (Fig. 2)
When a neonate develops thrombocytopenia of any severityat greater than 72 h of life, the most likely cause is bacterialor fungal sepsis and/or NEC. If infection and NEC areexcluded as etiologies for the thrombocytopenia, then theevaluation should be expanded. This should include testingfor liver dysfunction and DIC, viral infections that canpresent with thrombocytopenia after 72 h of life (i.e. HSVor acquired CMV), thrombosis (especially with a history of acentral line), or drug-induced thrombocytopenia. Immunethrombocytopenias should also be considered, because theygenerally worsen in the first few days of life and sometimespresent after 72 h of life. Other less common causes includeinborn errors of metabolism and Fanconi anemia (rare). If a
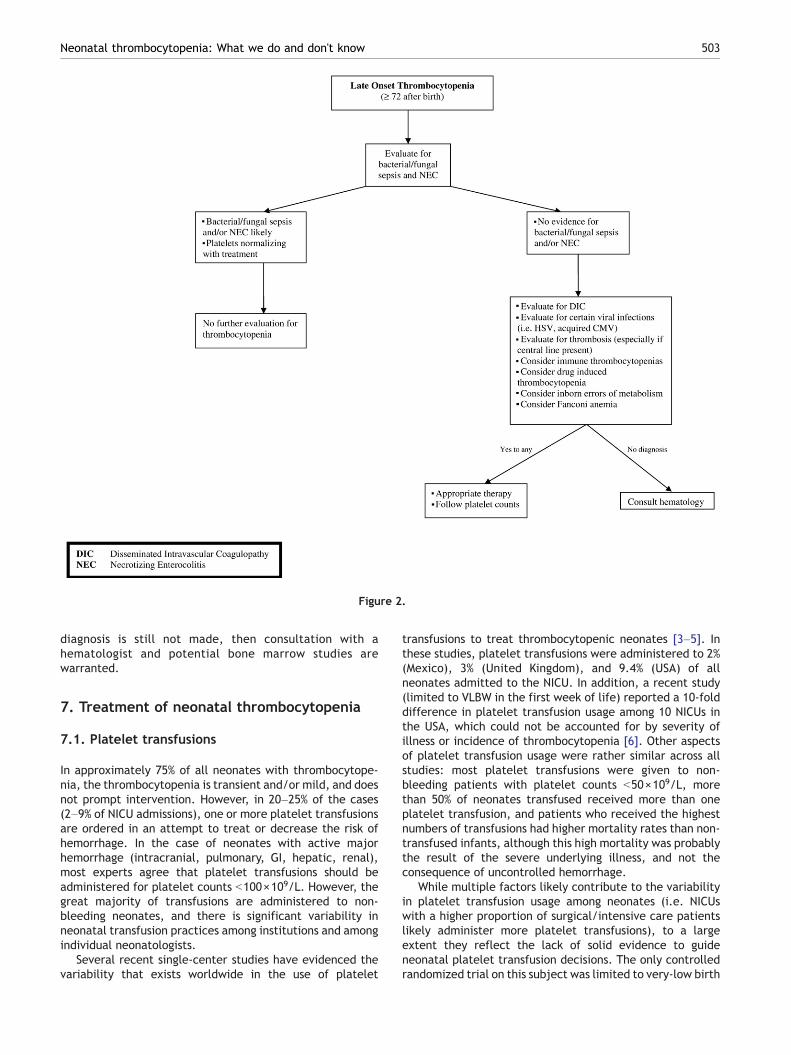
Figure 2.
503Neonatal thrombocytopenia: What we do and don't know
diagnosis is still not made, then consultation with ahematologist and potential bone marrow studies arewarranted.
7. Treatment of neonatal thrombocytopenia
7.1. Platelet transfusions
In approximately 75% of all neonates with thrombocytope-nia, the thrombocytopenia is transient and/or mild, and doesnot prompt intervention. However, in 20–25% of the cases(2–9% of NICU admissions), one or more platelet transfusionsare ordered in an attempt to treat or decrease the risk ofhemorrhage. In the case of neonates with active majorhemorrhage (intracranial, pulmonary, GI, hepatic, renal),most experts agree that platelet transfusions should beadministered for platelet counts b100×109/L. However, thegreat majority of transfusions are administered to non-bleeding neonates, and there is significant variability inneonatal transfusion practices among institutions and amongindividual neonatologists.
Several recent single-center studies have evidenced thevariability that exists worldwide in the use of platelet
transfusions to treat thrombocytopenic neonates [3–5]. Inthese studies, platelet transfusions were administered to 2%(Mexico), 3% (United Kingdom), and 9.4% (USA) of allneonates admitted to the NICU. In addition, a recent study(limited to VLBW in the first week of life) reported a 10-folddifference in platelet transfusion usage among 10 NICUs inthe USA, which could not be accounted for by severity ofillness or incidence of thrombocytopenia [6]. Other aspectsof platelet transfusion usage were rather similar across allstudies: most platelet transfusions were given to non-bleeding patients with platelet counts b50×109/L, morethan 50% of neonates transfused received more than oneplatelet transfusion, and patients who received the highestnumbers of transfusions had higher mortality rates than non-transfused infants, although this high mortality was probablythe result of the severe underlying illness, and not theconsequence of uncontrolled hemorrhage.
While multiple factors likely contribute to the variabilityin platelet transfusion usage among neonates (i.e. NICUswith a higher proportion of surgical/intensive care patientslikely administer more platelet transfusions), to a largeextent they reflect the lack of solid evidence to guideneonatal platelet transfusion decisions. The only controlledrandomized trial on this subject was limited to very-low birth
504 M. Sola-Visner et al.
weight infants in the first week of life, and excluded thosewith platelet counts b50×109/L. In that study, Andrew et al.[7] randomized 152 thrombocytopenic premature infants toeither a treatment group (platelet transfusions for anyplatelet count b150×109/L), or to a control group (platelettransfusions only for clinical indications or for a plateletcount b50×109/L). These investigators found no significantdifferences in frequency or severity of intracranial hemor-rhages between the two groups, and concluded that non-bleeding premature infants with platelet counts N50×109/Lshould not receive prophylactic platelet transfusions. Sinceall neonates with platelet counts b50×109/L were trans-fused, however, this study did not address whether lowerplatelet counts could be safely tolerated. To answer thisquestion, Murray et al. [3] performed a retrospective reviewof platelet transfusions among neonates with platelet countsb50×109/L admitted to their NICU (n=53 over 3 years).Overall, they transfused 51% of these neonates: those with aplatelet count b30×109/L, and those with a platelet countbetween 30 and 50×109/L who had a previous intracranialhemorrhage or were clinically unstable. They did not observeany major hemorrhage in this group, regardless of whetherplatelet transfusions were given or withheld. Thus, theyconcluded that a prophylactic platelet transfusion trigger ofb30×109/L probably represents a safe practice for clinicallystable NICU patients, although they recognized the limita-tions inherent to any retrospective study.
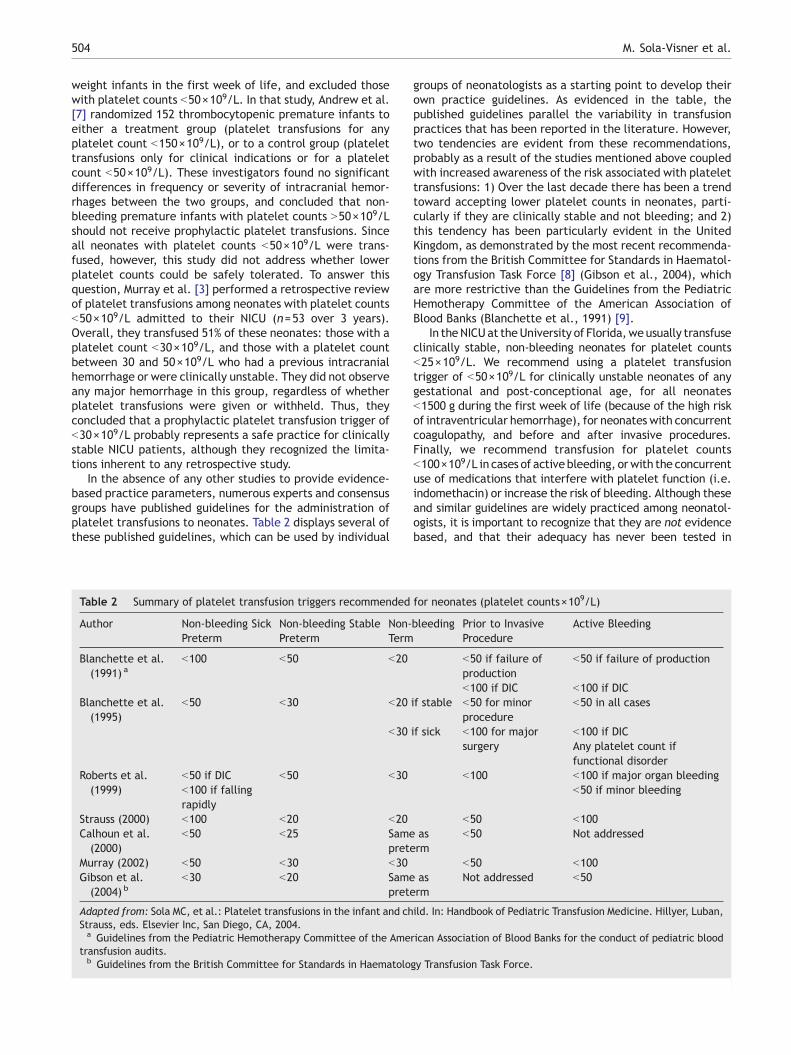
In the absence of any other studies to provide evidence-based practice parameters, numerous experts and consensusgroups have published guidelines for the administration ofplatelet transfusions to neonates. Table 2 displays several ofthese published guidelines, which can be used by individual
Table 2 Summary of platelet transfusion triggers recommended
Author Non-bleeding SickPreterm
Non-bleeding StablePreterm
Non-Term
Blanchette et al.(1991) a
b100 b50 b20
Blanchette et al.(1995)
b50 b30 b20
b30
Roberts et al.(1999)
b50 if DIC b50 b30b100 if fallingrapidly
Strauss (2000) b100 b20 b20Calhoun et al.(2000)
b50 b25 Sameprete
Murray (2002) b50 b30 b30Gibson et al.(2004) b
b30 b20 Sameprete
Adapted from: Sola MC, et al.: Platelet transfusions in the infant and chStrauss, eds. Elsevier Inc, San Diego, CA, 2004.a Guidelines from the Pediatric Hemotherapy Committee of the Ame
transfusion audits.b Guidelines from the British Committee for Standards in Haematolo
groups of neonatologists as a starting point to develop theirown practice guidelines. As evidenced in the table, thepublished guidelines parallel the variability in transfusionpractices that has been reported in the literature. However,two tendencies are evident from these recommendations,probably as a result of the studies mentioned above coupledwith increased awareness of the risk associated with platelettransfusions: 1) Over the last decade there has been a trendtoward accepting lower platelet counts in neonates, parti-cularly if they are clinically stable and not bleeding; and 2)this tendency has been particularly evident in the UnitedKingdom, as demonstrated by the most recent recommenda-tions from the British Committee for Standards in Haematol-ogy Transfusion Task Force [8] (Gibson et al., 2004), whichare more restrictive than the Guidelines from the PediatricHemotherapy Committee of the American Association ofBlood Banks (Blanchette et al., 1991) [9].
In theNICUat theUniversity of Florida,weusually transfuseclinically stable, non-bleeding neonates for platelet countsb25×109/L. We recommend using a platelet transfusiontrigger of b50×109/L for clinically unstable neonates of anygestational and post-conceptional age, for all neonatesb1500 g during the first week of life (because of the high riskof intraventricular hemorrhage), for neonates with concurrentcoagulopathy, and before and after invasive procedures.Finally, we recommend transfusion for platelet countsb100×109/L in cases of active bleeding, orwith the concurrentuse of medications that interfere with platelet function (i.e.indomethacin) or increase the risk of bleeding. Although theseand similar guidelines are widely practiced among neonatol-ogists, it is important to recognize that they are not evidencebased, and that their adequacy has never been tested in
for neonates (platelet counts×109/L)
bleeding Prior to InvasiveProcedure
Active Bleeding
b50 if failure ofproduction
b50 if failure of production
b100 if DIC b100 if DICif stable b50 for minor
procedureb50 in all cases
if sick b100 for majorsurgery
b100 if DICAny platelet count iffunctional disorder
b100 b100 if major organ bleedingb50 if minor bleeding
b50 b100asrm
b50 Not addressed
b50 b100asrm
Not addressed b50
ild. In: Handbook of Pediatric Transfusion Medicine. Hillyer, Luban,
rican Association of Blood Banks for the conduct of pediatric blood
gy Transfusion Task Force.

505Neonatal thrombocytopenia: What we do and don't know
clinical studies. Evaluating these highly variable practices inwell designed randomized controlled trials is critical for theadvancement of neonatal transfusion medicine.
A circumstance that deserves special attention is that ofneonatal alloimmune thrombocytopenia (NAIT). NAIT iscaused by a feto-maternal mismatch of human plateletantigens, and the pathogenesis resembles that of erythro-blastosis fetalis, with the exception that it can affect theproduct of a first pregnancy. As described in the “Approach tothe thrombocytopenic neonate” section, NAIT must beconsidered any time a neonate presents with unexplainedsevere thrombocytopenia at birth. Intracranial hemorrhagehas been reported in 11–21% of cases of NAIT [10], and it istherefore important to provide effective therapy immedi-ately to all affected or potentially affected neonates withvery severe thrombocytopenia (platelet counts b30×109/L).Neonates with any evidence of evenminor bleeding should betransfused for platelet counts b50×109/L, and this thresholdshould also be considered for neonates with a previouslyaffected sibling who had an intracranial hemorrhage (asignificant risk factor for intracranial hemorrhage in thepresent neonate). As with any other variety of thrombocyto-penia, affected infants with severe bleeding should receiveplatelet transfusions for a platelet count b100×109/L.
In the case of NAIT, providing the appropriate product is ofcritical importance, since these patients typically do notrespond well to random platelet transfusions. A recent studyevaluating the records of 1162 cases of confirmed NAITinvestigated in a national referral center in the USAidentified antibodies against HPA-1a (also known as PLA-1)in 79% of these cases, and against HPA-5b in 9% [11]. Based onthis evidence, transfusion with HPA-1a/HPA-5b negativeplatelets should result in an adequate platelet incrementin approximately 90% of cases of NAIT. In England, plateletsobtained from HPA-1a/HPA-5b negative donors are availableon short notice from the National Blood Service, and havebeen shown to induce good platelet increments in most casesof suspected or proven NAIT [12]. This platelet product istherefore the treatment of choice for neonates with NAIT. Incases when there is a long wait for compatible platelets orthese are not available, high-dose IVIG and/or a trial ofrandom donor platelets is indicated. Some affected neonateswill have a response to random donor platelets, which can beexplained by randomly receiving HPA-1a negative platelets,the presence of weak anti-platelet antibodies, or NAITcaused by antibodies against an uncommon platelet antigen(which account for approximately 10% of cases of NAIT).When using IVIG, the usual recommended dose is 1–2 g/kgadministered as 0.4 g/kg daily for 3–5 days or 1 g/kg daily forone or two days [13]. Finally, maternal platelets areindicated in circumstances when a rapid and substantialplatelet increase is required and antigen-negative plateletsfrom another donor are not available. If maternal plateletsare used, these have to be washed (to eliminate thecirculating antibodies) and irradiated prior to transfusion.
8. Thrombopoietic growth factors
Because of the risks associated with blood products, thepotential use of thrombopoietic growth factors has beenexplored as an appealing therapeutic alternative for throm-
bocytopenia. IL-3, IL-6, IL-11, Stem Cell Factor (SCF), andThrombopoietin (Tpo) all support megakaryocyte develop-ment in vitro, and have been touted for their pre-clinicalthrombopoietic activity, but have led to limited plateletrecovery in the adult patient care setting. No trials inneonates have been conducted.
Recombinant IL-11 (rhIL-11) is the only thrombopoieticgrowth factor approved in the USA for the prevention ofsevere chemotherapy-induced thrombocytopenia. Reports ofexperimental benefits for NEC and sepsis in animal modelshave made the potential use of this cytokine in neonatesappealing. However, significant side effects (such as fluidretention and atrial arrythmias), coupled with reports of lackof efficacy in certain varieties of thrombocytopenia (i.e.refractory ITP) [14], have raised questions about its safetyand potential efficacy in neonates. These issues have neverbeen investigated in NICU patients, and its use in theneonatal period should therefore be restricted to well-controlled clinical trials.
The cloning of thrombopoietin (Tpo, themost potent knownstimulator of platelet production) led to a flurry of studies overthe last ten years that quickly progressed from bench researchto clinical trials. Recently, however, several subjects treatedwith a truncated form of recombinant Tpo (PEG-rHMGDG)developed neutralizing antibodies against endogenous Tpo,which resulted in severe thrombocytopenia and aplasticanemia. Ultimately, these complications led to the disconti-nuation of clinical trials involving Tpo. As an alternative,muchinterest has recently been devoted to the development ofthrombopoietin-mimetic molecules. These are mostly smallmolecules that have no sequence homology to Tpo, but bind tothe Tpo receptor and have biologically comparable effects.Among the significant number of thrombopoietin receptoragonists that have been described, AMG-531 (Amgen, Inc.) [15]is currently being evaluated in clinical trials. No in vitro or invivo studies evaluating the potential use of these compounds inneonates have been reported.
9. Research directions
In conclusion, although the majority of cases of neonatalthrombocytopenia are mild to moderate and do not warrantintensive investigation or aggressive treatment, neonatalthrombocytopenia continues to constitute a significantproblem in the NICU and may be the presenting sign of aserious diagnosis. It also appears from recent studies thatneonates might have a relative inability to increase plateletproduction when faced with increased platelet consumption.Further studies to elucidate the mechanisms underlyingthrombocytopenia in neonates with different pathologies areneeded, not only to better understand the predisposition ofsick neonates to develop significant and/or prolongedthrombocytopenia, but also to assess the potential useful-ness of thrombopoietic growth factor therapy in the NICU. Inthis regard, pre-clinical and clinical studies evaluating theefficacy and safety of rhIL-11 and thrombopoietin/thrombo-poietin thrombopoietin-mimetic compounds in neonates areneeded. Previous experience has shown that both thepharmacokinetic and pharmacodynamic properties of hema-topoietic growth factors can be different in neonatescompared to adults, and recent reports suggest that fetal
506 M. Sola-Visner et al.
and neonatal megakaryocytes might have unique biologicalcharacteristics different from those of their adult counter-parts. If, or until, thrombopoietic growth factor therapybecomes a reality in the NICU, platelet transfusions willremain the only treatment for non-immune thrombocytope-nia, and there is very limited evidence to guide ourtransfusion decisions. For that reason, adequately poweredmulti-center studies are critically needed to determine whatconstitutes a safe platelet count in neonates, and to helpneonatologists balance the risks of significant hemorrhagevs. those of repeated blood product therapy in individualsituations.
10. Key guidelines
• Thrombocytopenia affects approximately one third of allpatients admitted to the NICU.
• There are many disease processes that have beenassociated with thrombocytopenia in the neonatal period.These processes can be divided in those that cause early-onset (at or shortly after birth) vs. late-onset thrombo-cytopenia (onset after the first 72 h of life), and in thosethat cause mild-moderate vs. severe thrombocytopenia.
• Most cases of thrombocytopenia are not severe enough towarrant treatment. In approximately 20–25% of patients,however, the thrombocytopenia is severe (b50×109/L)and therapy with platelet transfusions might beconsidered.
• The existing evidence to guide platelet transfusiondecisions in neonates is very limited, but it suggeststhat transfusing non-bleeding infants b1500 g during thefirst week of life for platelet counts N50×109/L does notreduce the incidence of intraventricular hemorrhage, andthat 30×109/L might be a safe transfusion threshold forclinically stable neonates, particularly outside of the highrisk period. Additional studies are necessary to establishthe safety of any set of guidelines for non-bleedingneonates and to critically evaluate the common clinicalindications which frequently prompt neonatologists totransfuse platelets at higher thresholds than above. In thecase of bleeding neonates, most experts agree thatplatelet transfusions should be administered for plateletcounts b100×109/L.
• Recombinant IL-11 and thrombopoietin thrombopoietin-mimetic compounds might become viable therapeuticalternatives for selected groups of thrombocytopenicneonates in the future. Currently, however, their useshould be restricted to well-controlled clinical trials.
References
[1] Murray NA, Roberts IA. Circulating megakaryocytes and theirprogenitors in early thrombocytopenia in preterm neonates.Pediatr Res 1996;40:112–9.
[2] Sola MC, Rimsza LM. Mechanisms underlying thrombocytopeniain the Neonatal Intensive Care Unit. Acta Paediatrica Suppl2002;438:66–73.
[3] Murray NA, Howarth LJ, McCloy MP, Letsky EA, Roberts IA.Platelet transfusion in the management of severe thrombocy-topenia in neonatal intensive care unit patients. Transfus Med2002;12:35–41.
[4] Garcia MG, Duenas E, Sola MC, Hutson AD, Theriaque D,Christensen RD. Epidemiologic and outcome studies of patientswho received platelet transfusions in the neonatal intensivecare unit. J Perinatol 2001;21:415–20.
[5] Del Vecchio A, Sola MC, Theriaque DW, et al. Platelettransfusions in the neonatal intensive care unit: factorspredicting which patients will require multiple transfusions.Transfusion 2001;41:803–8.
[6] Kahn DJ, Richardson DK, Billett HH. Inter-NICU variation inrates and management of thrombocytopenia among very lowbirth-weight infants. J Perinatol 2003;23:312–6.
[7] Andrew M, Vegh P, Caco C, et al. A randomized, controlled trialof platelet transfusions in thrombocytopenic prematureinfants. J Pediatr 1993;123:285–91.
[8] Gibson BE, Todd A, Roberts I, et al. Transfusion guidelines forneonates and older children. Br J Haematol 2004;124:433–53.
[9] Blanchette VS, Hume HA, Levy GJ, et al. Guidelines for auditingpediatric blood transfusion practices. Am J Dis Child1991;145:787–96.
[10] Bussel JB, Zacharoulis S, Kramer K, McFarland JG, Pauliny J,Kaplan C. Clinical and diagnostic comparison of neonatalalloimmune thrombocytopenia to non-immune cases of throm-bocytopenia. Pediatr Blood Cancer 2005;45:176–83.
[11] Davoren A, Curtis BR, Aster RH, McFarland JG. Human plateletantigen-specific alloantibodies implicated in 1162 cases ofneonatal alloimmune thrombocytopenia. Transfusion2004;44:1220–5.
[12] Allen DL, Samol J, Benjamin S, Verjee S, Tusold A, Murphy MF.Survey of the use and clinical effectiveness of HPA-1a/5b-negative platelet concentrates in proven or suspected plateletalloimmunization. Transfus Med 2004;14:409–17.
[13] Blanchette VS, Johnson J, Rand M. The management ofalloimmune neonatal thrombocytopenia. Baillieres Best PractRes Clin Haematol 2000;13:365–90.
[14] Bussel JB, Mukherjee R, Stone AJ. A pilot study of rhuIL-11treatment of refractory ITP. Am J Hematol 2001;66:172–7.
[15] Wang B, Nichol JL, Sullivan JT. Pharmacodynamics andpharmacokinetics of AMG 531, a novel thrombopoietin receptorligand. Clin Pharmacol Ther 2004;76:628–38.