Embed Size (px)
Citation preview
Neonatal surgical
Emergencies
Dr Prashant Jain
Sr Consultant Ped. Surgery & Ped Urology
Dr BLKSS Hospital
Gastro-Intestinal
Abdominal wall defects
Respiratory distress

Intestinal Obstruction
Bilious Vomiting
Abdominal distension
Failure to pass meconium
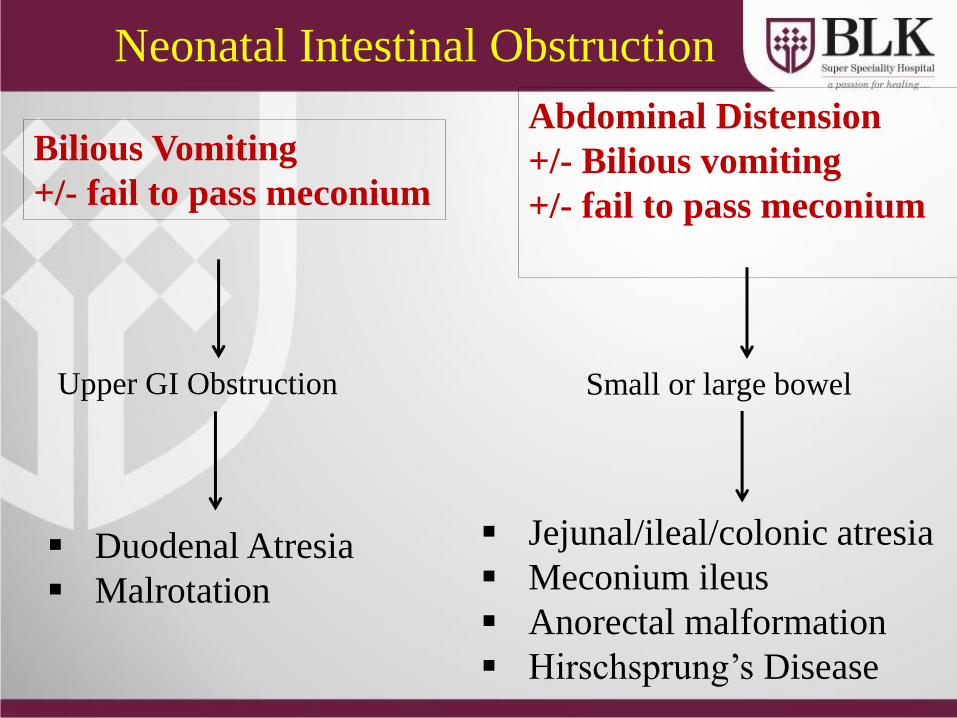
Neonatal Intestinal Obstruction
Bilious Vomiting
+/- fail to pass meconium
Abdominal Distension
+/- Bilious vomiting
+/- fail to pass meconium
Upper GI Obstruction
Duodenal Atresia
Malrotation
Jejunal/ileal/colonic atresia
Meconium ileus
Anorectal malformation
Hirschsprung’s Disease
Small or large bowel
PASSAGE OF MECONIUM
• CANNOT RULE OUT OBSTRUCTION
• CAN PASS EVEN IN CASES OF ATRESIA
Causes
Intestinal atresia
Malrotation with or without Midgut volvulus
Meconium ileus
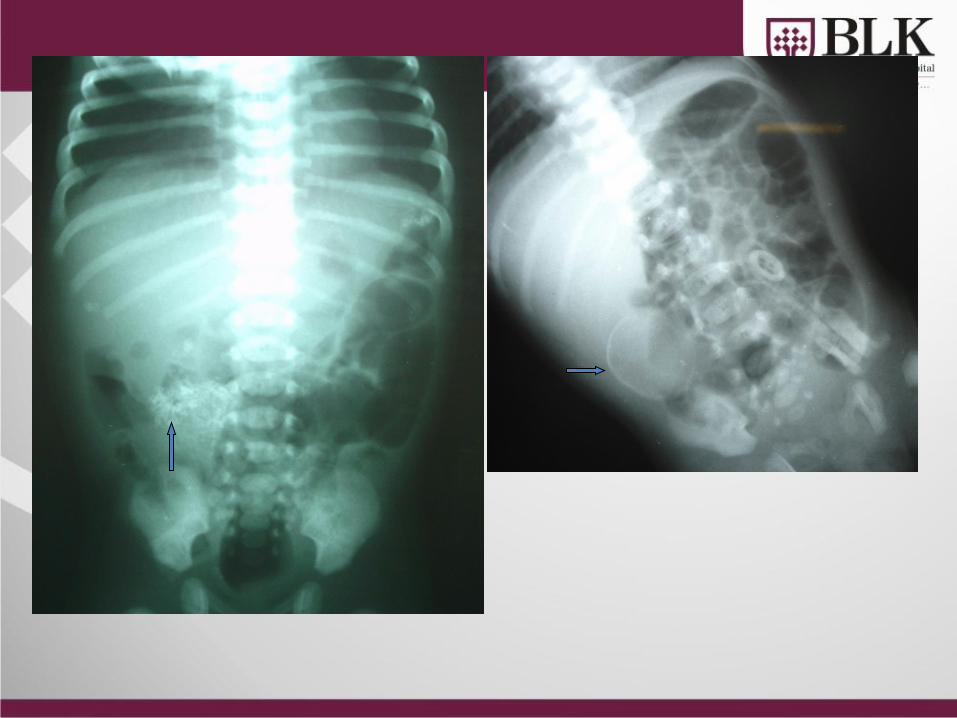
Meconium Peritonitis
Ano-Rectal Malformation
Hirschsprung’s Disease
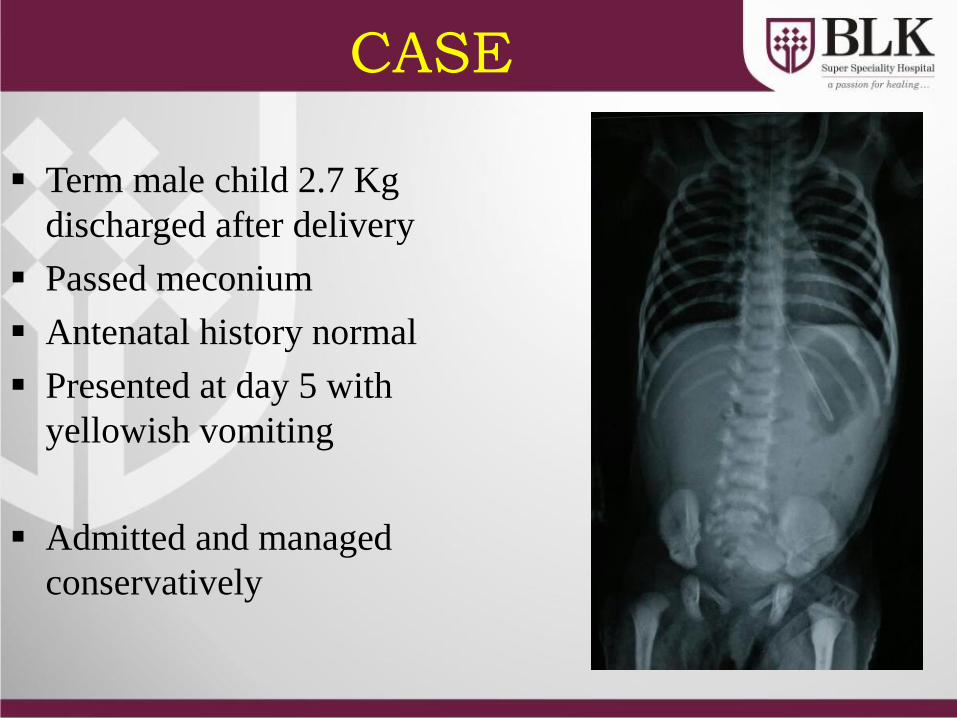
CASE
Term male child 2.7 Kg
discharged after delivery
Passed meconium
Antenatal history normal
Presented at day 5 with
yellowish vomiting
Admitted and managed
conservatively
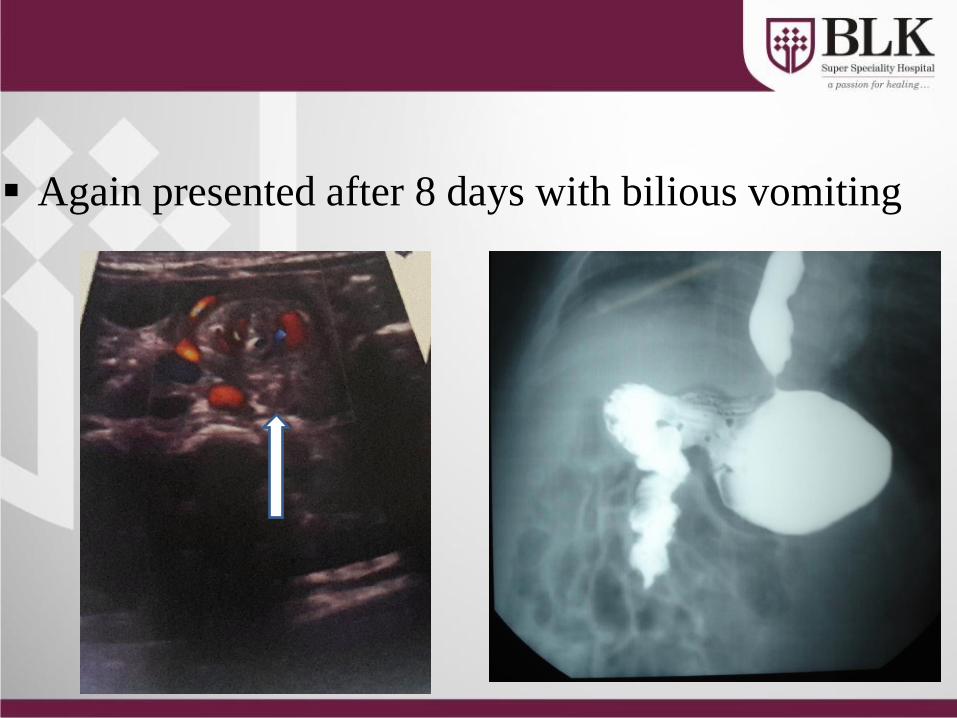
Again presented after 8 days with bilious vomiting
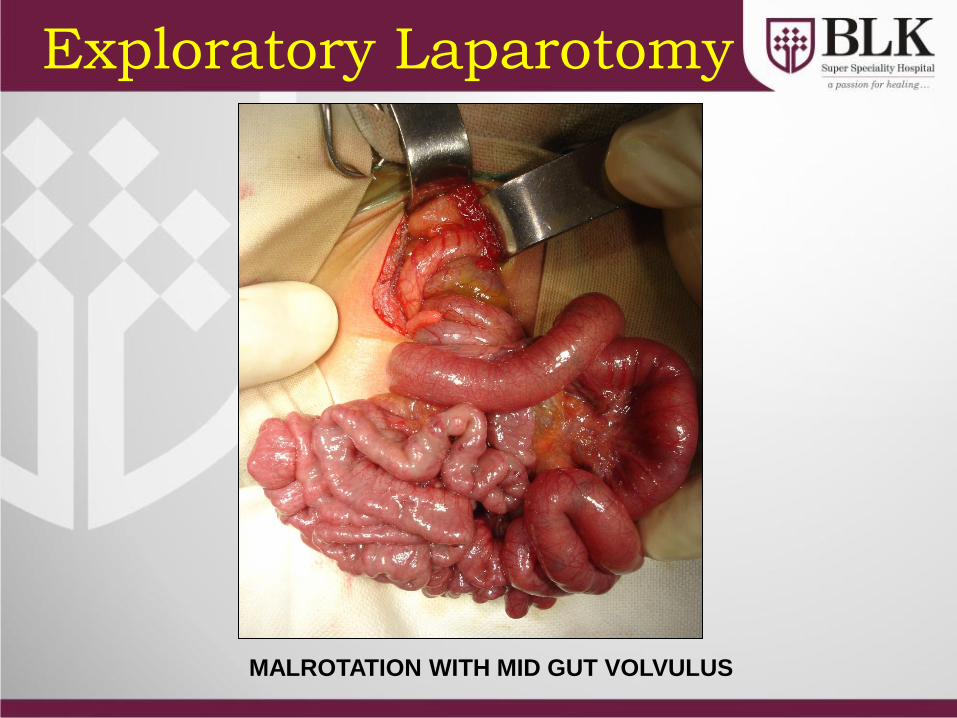
MALROTATION WITH MID GUT VOLVULUS
Exploratory Laparotomy
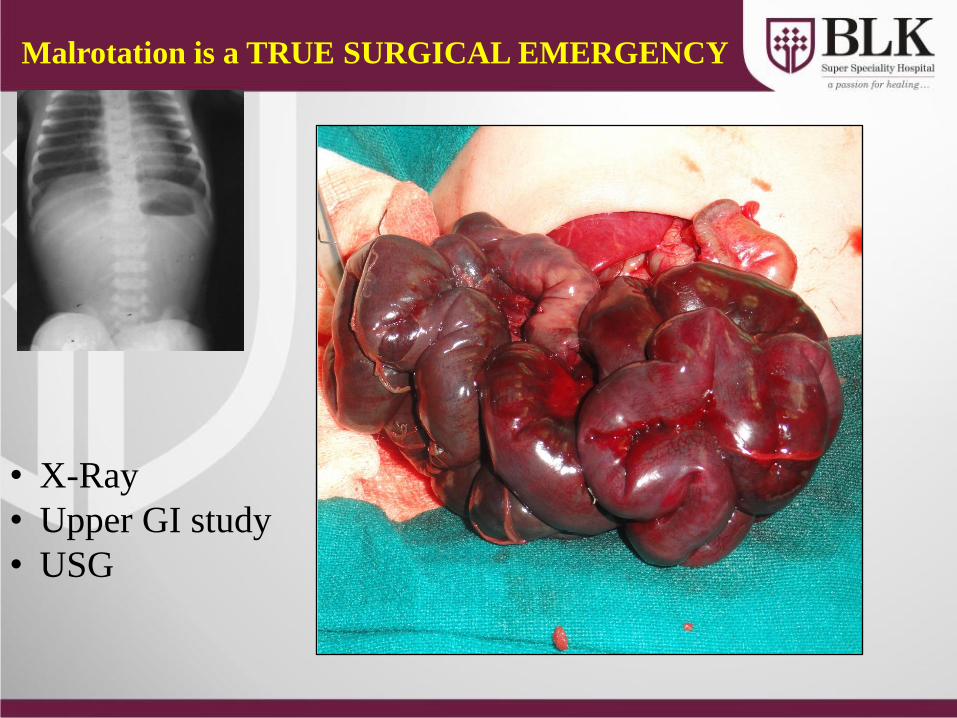
Malrotation is a TRUE SURGICAL EMERGENCY
• X-Ray
• Upper GI study
• USG
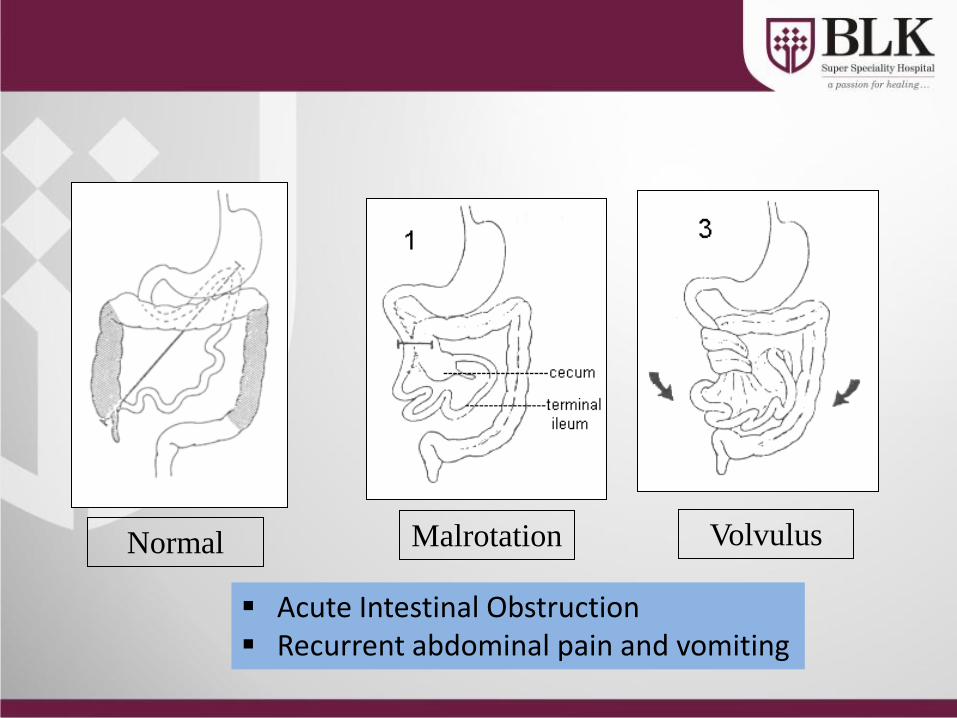
Normal
Acute Intestinal Obstruction Recurrent abdominal pain and vomiting
Malrotation Volvulus
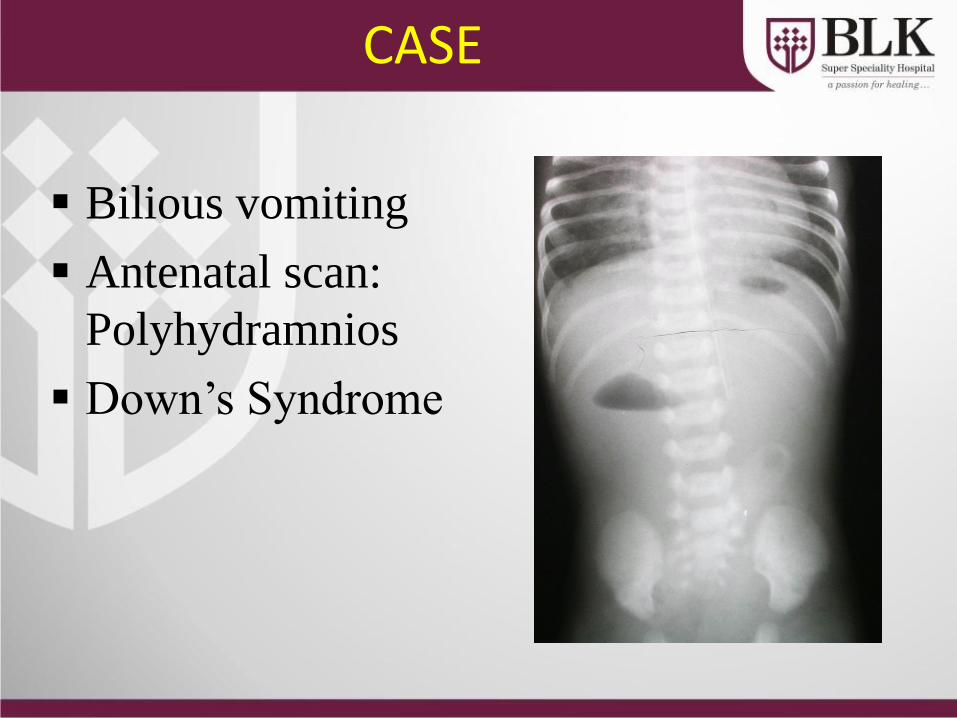
CASE
Bilious vomiting
Antenatal scan:
Polyhydramnios
Down’s Syndrome
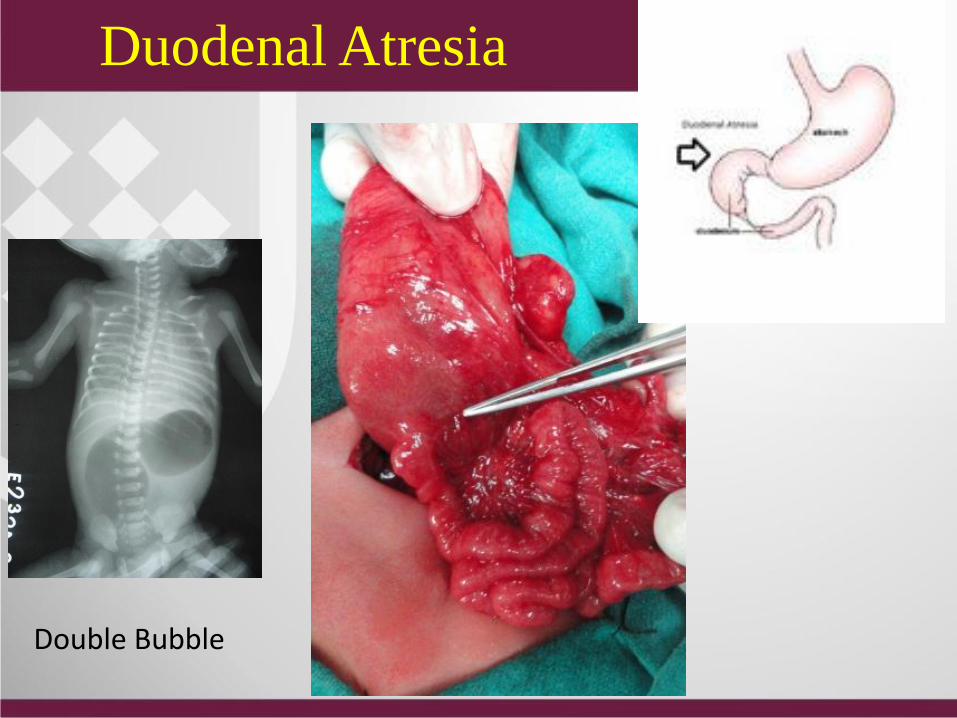
Duodenal Atresia
Double Bubble
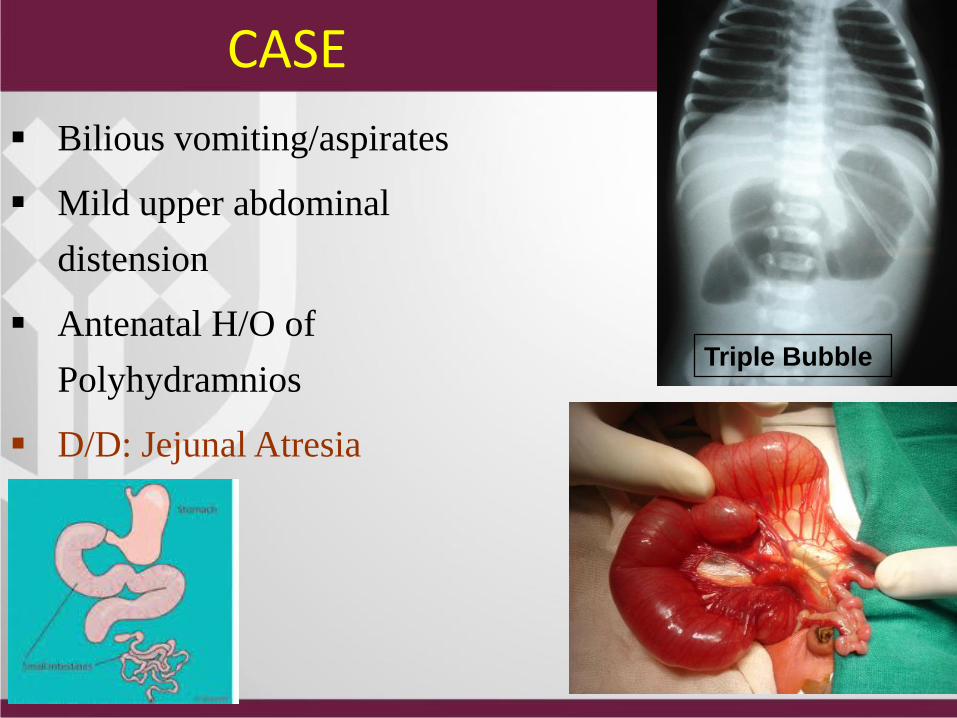
Bilious vomiting/aspirates
Mild upper abdominal
distension
Antenatal H/O of
Polyhydramnios
D/D: Jejunal Atresia
Triple Bubble
CASE
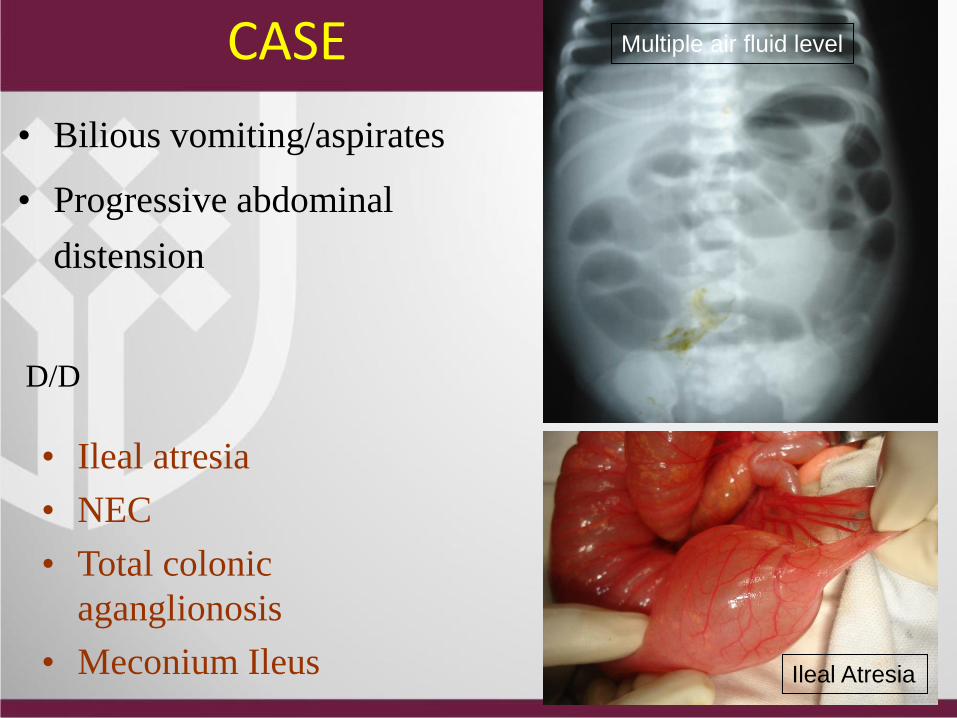
• Bilious vomiting/aspirates
• Progressive abdominal
distension
Multiple air fluid level
Ileal Atresia
• Ileal atresia
• NEC
• Total colonic
aganglionosis
• Meconium Ileus
D/D
CASE
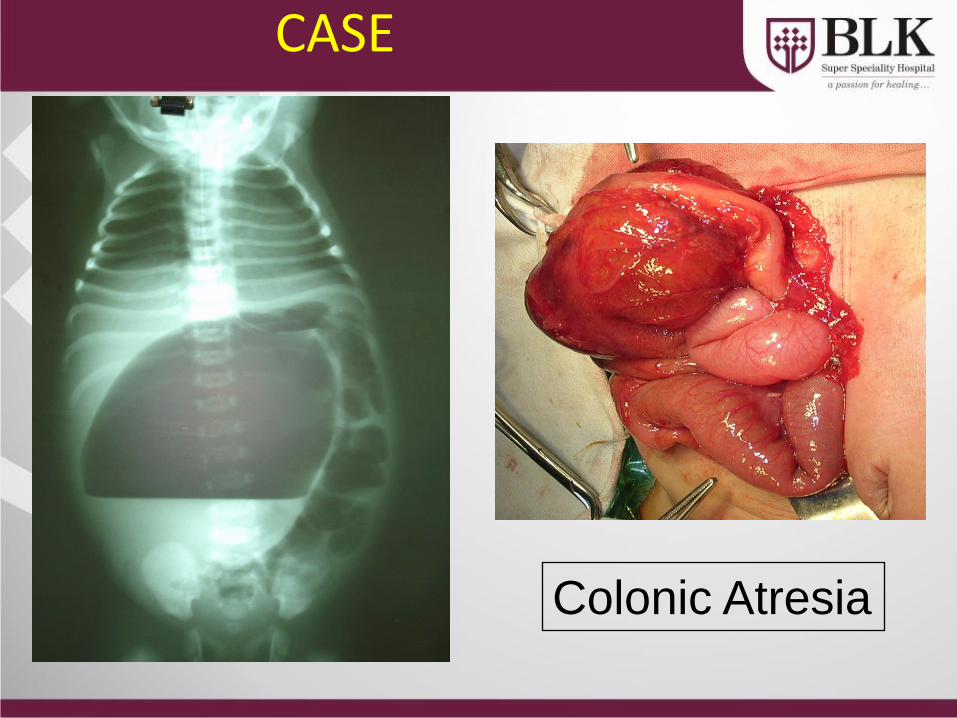
Colonic Atresia
CASE
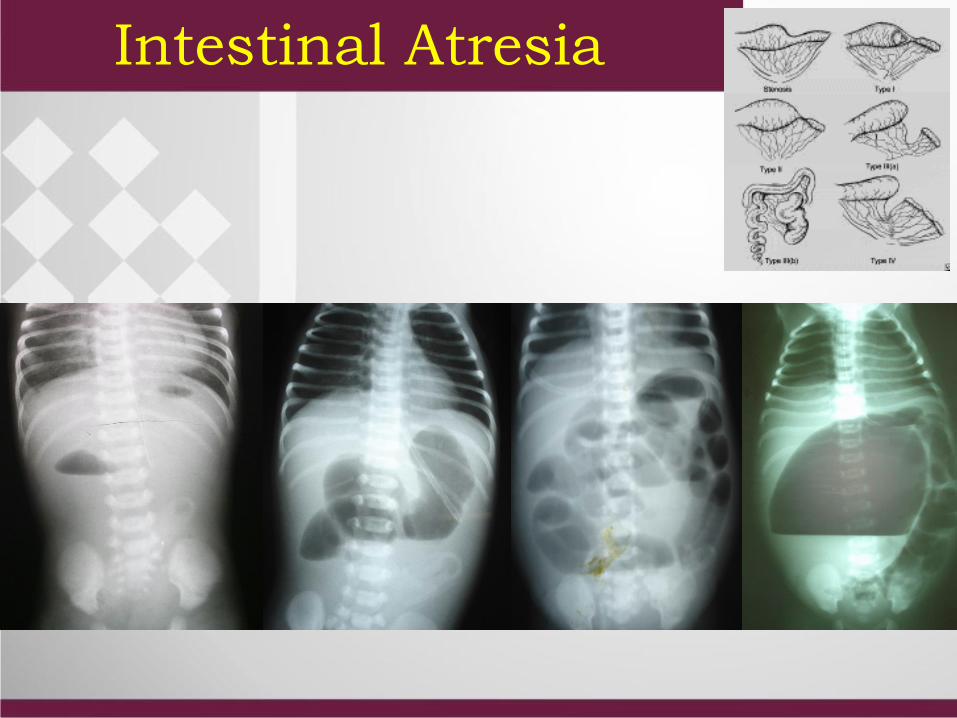
Intestinal Atresia
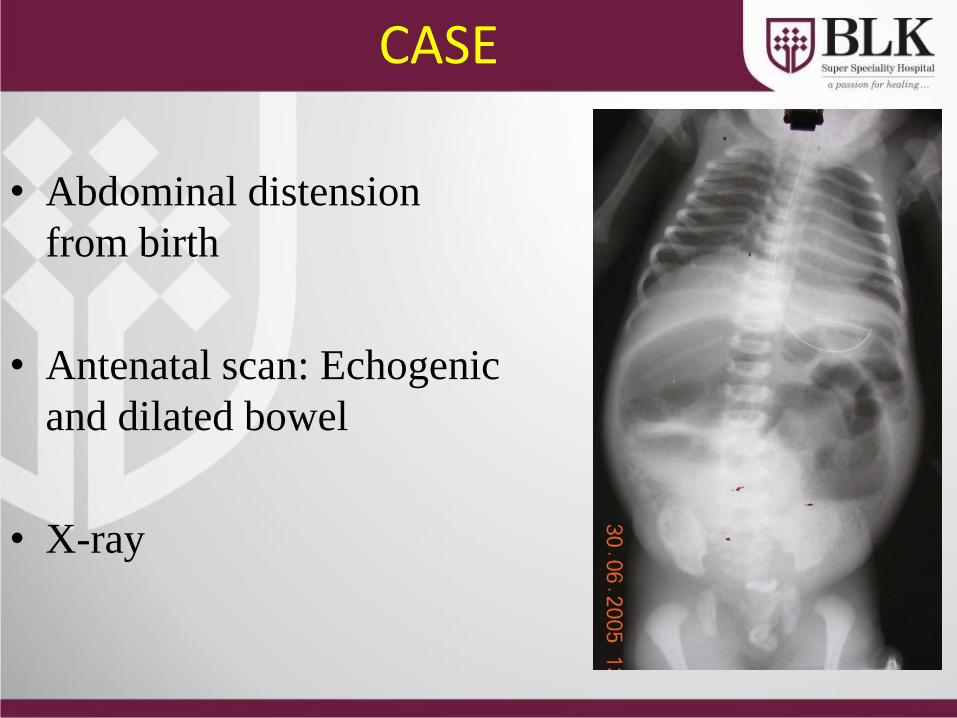
CASE
• Abdominal distension
from birth
• Antenatal scan: Echogenic
and dilated bowel
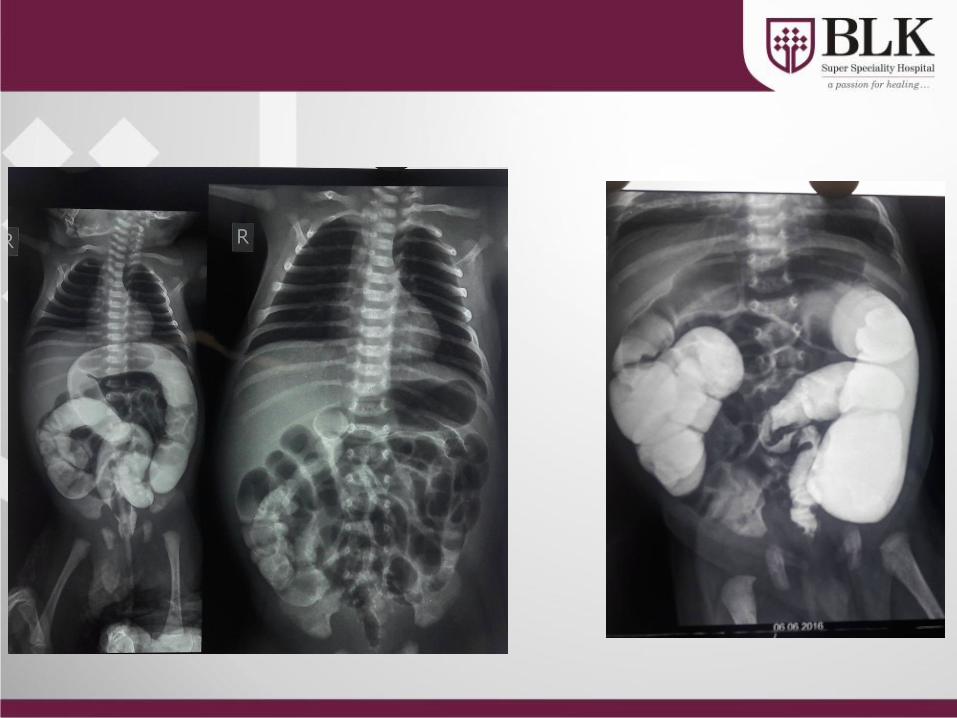
• X-ray
Abdominal distension since birth
Meconium ileus
Meconium peritonitis/ascites
Abdominal lump
Ascites
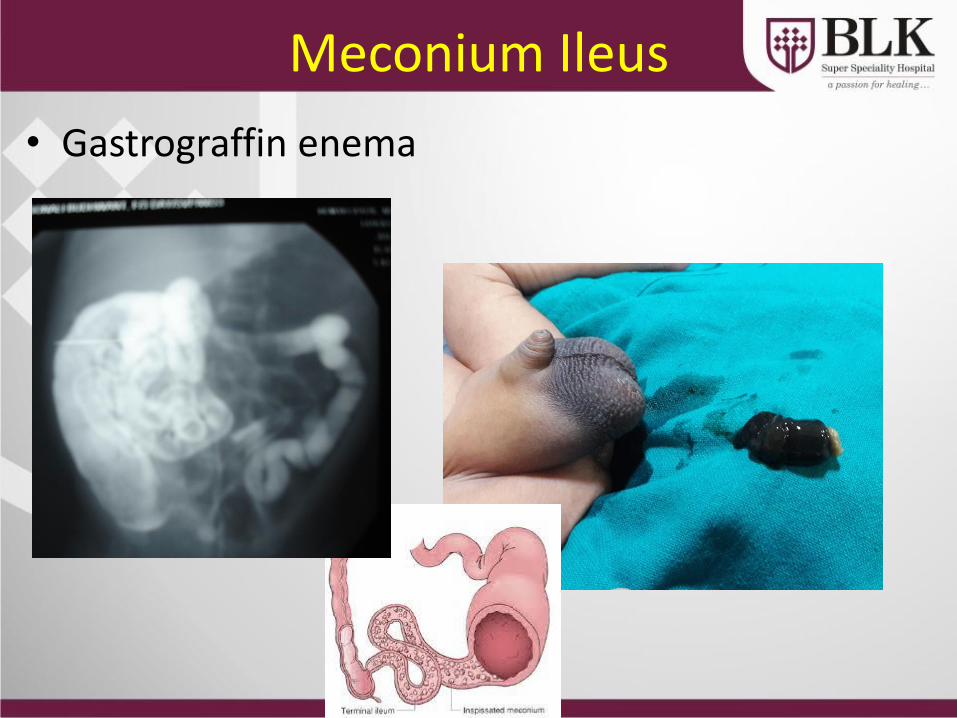
Meconium Ileus
• Gastrograffin enema
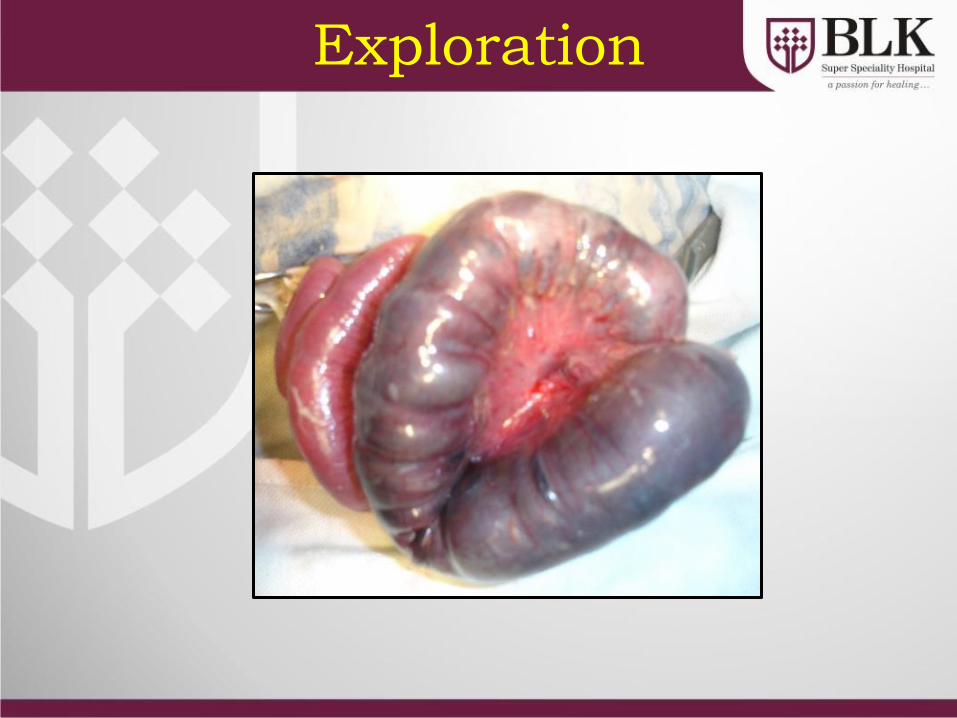
Exploration
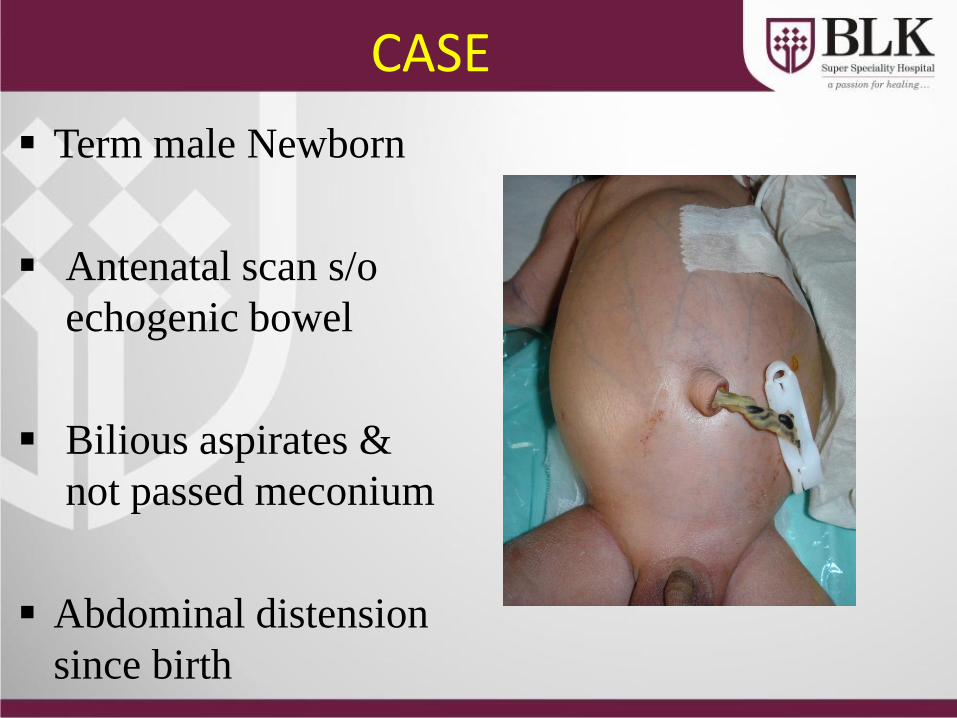
CASE
Term male Newborn
Antenatal scan s/o
echogenic bowel
Bilious aspirates &
not passed meconium
Abdominal distension
since birth
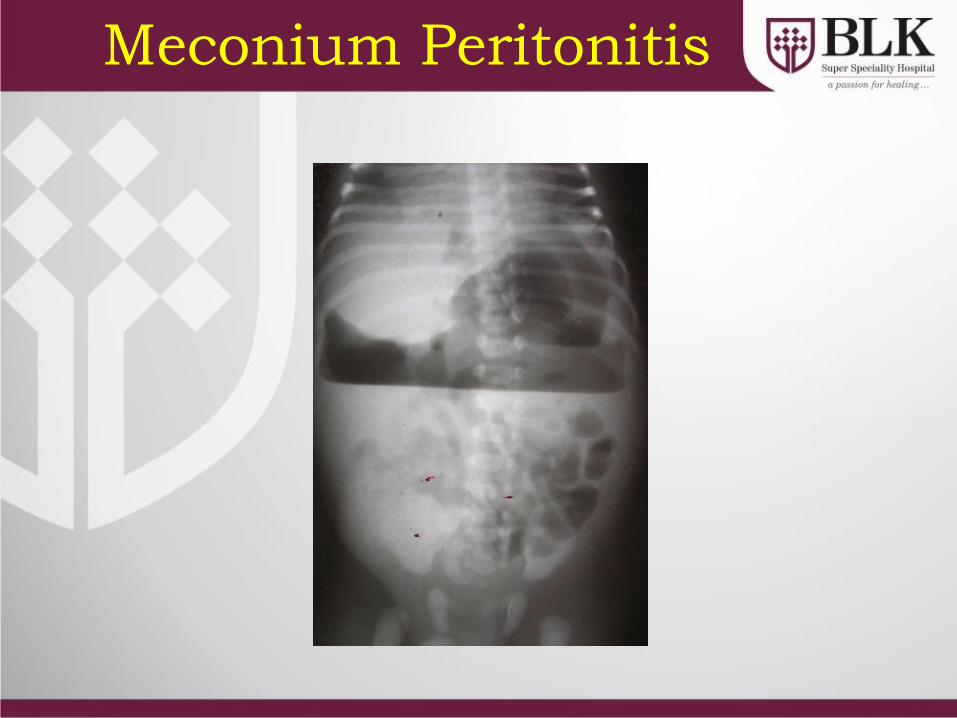
Meconium Peritonitis
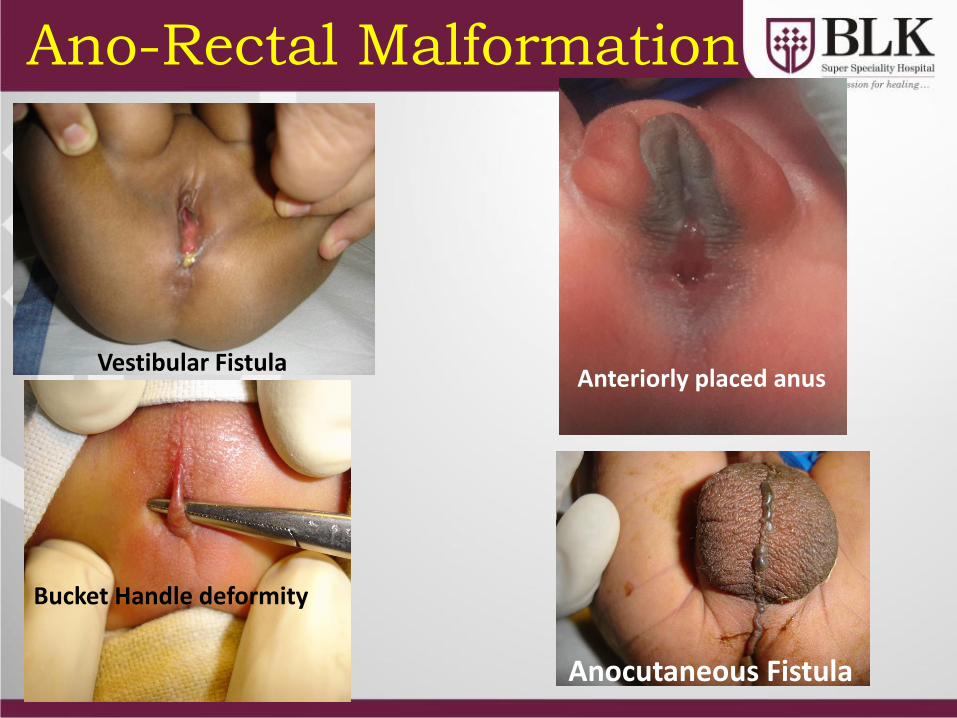
Ano-Rectal Malformation
Vestibular Fistula Anteriorly placed anus
Bucket Handle deformity
Anocutaneous Fistula
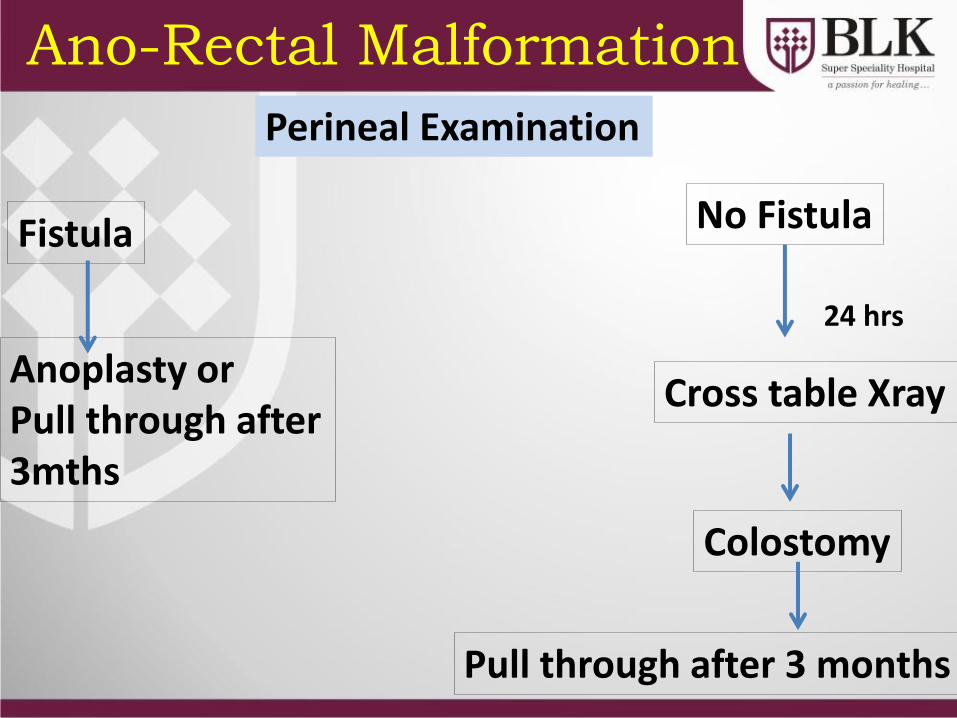
Ano-Rectal Malformation
Perineal Examination
Fistula
Anoplasty or Pull through after 3mths
No Fistula
24 hrs
Cross table Xray
Colostomy
Pull through after 3 months
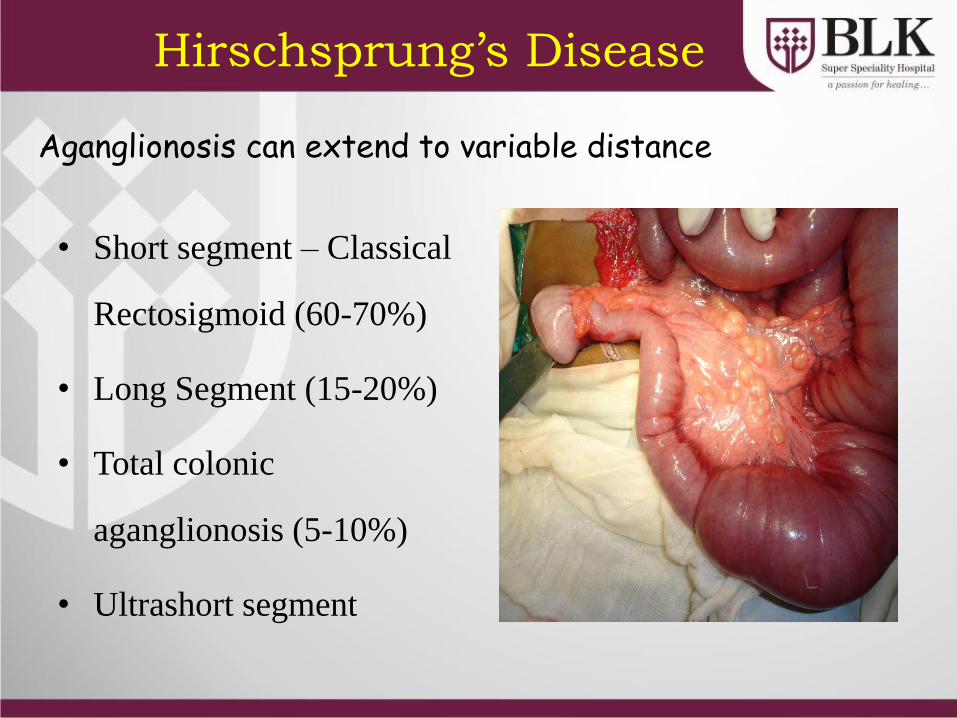
Aganglionosis can extend to variable distance
• Short segment – Classical
Rectosigmoid (60-70%)
• Long Segment (15-20%)
• Total colonic
aganglionosis (5-10%)
• Ultrashort segment
Hirschsprung’s Disease
Presentation
• Characteristically disease of full term newborn
• History of constipation dating back to newborn
period
• 95% of newborns defecate in first 24 hrs
of life
• Abdominal distension
• Poor feeding
• Failure to thrive
Investigations
• Barium Enema
• Rectal Biopsy
Definitive Pull through
for Hirschsprung’s Disease
• Single stage at age 3-6 months
• Two stage at 6-12 months after
colostomy
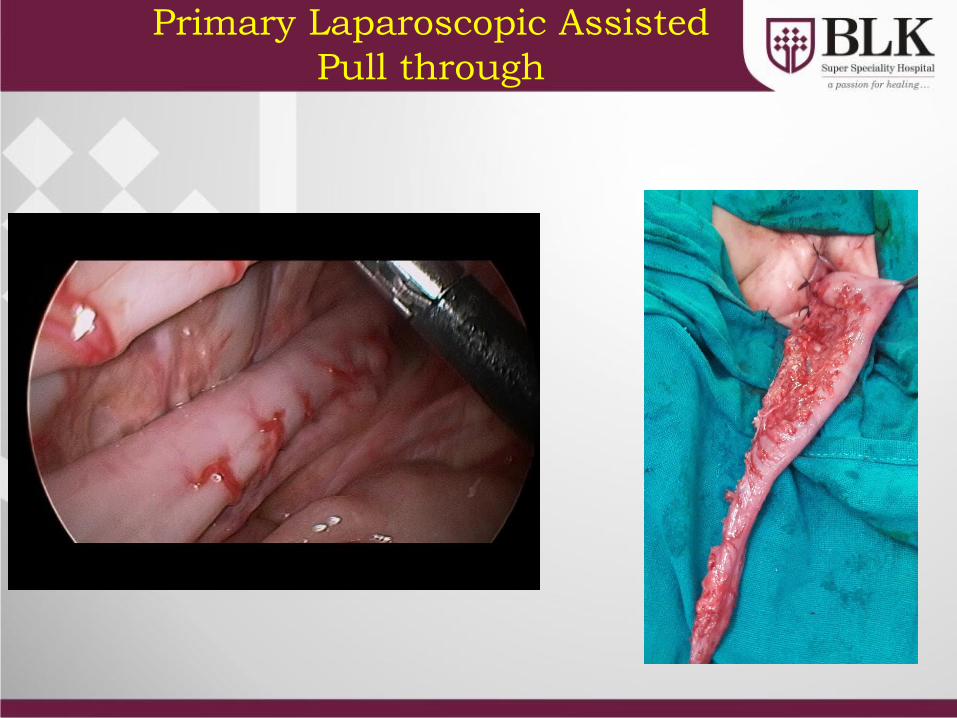
Primary Laparoscopic Assisted
Pull through
Respiratory Distress
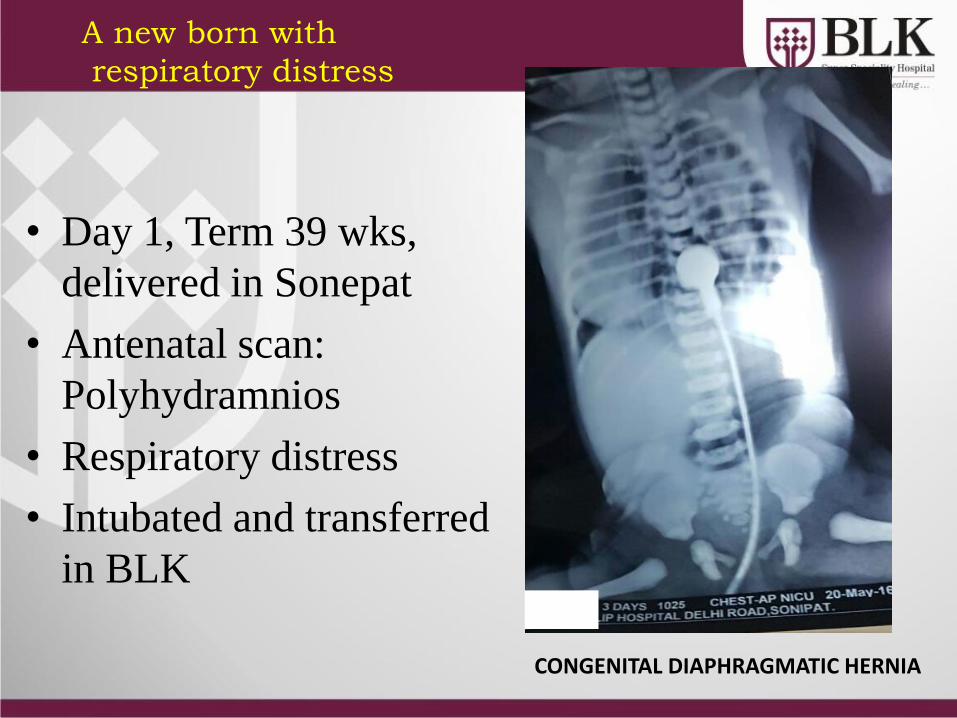
• Day 1, Term 39 wks,
delivered in Sonepat
• Antenatal scan:
Polyhydramnios
• Respiratory distress
• Intubated and transferred
in BLK
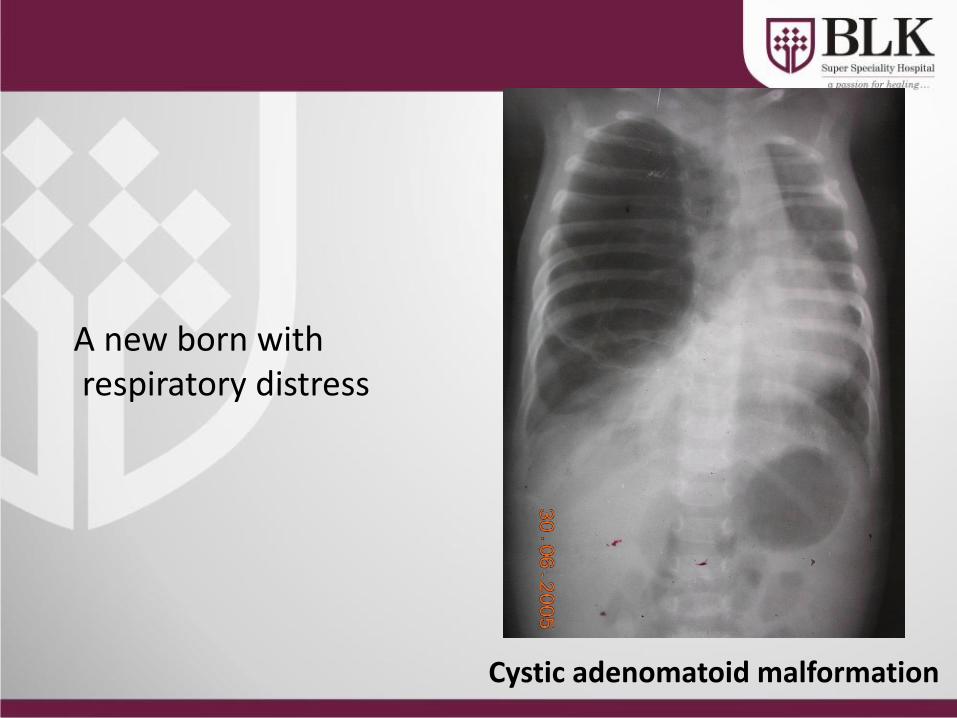
A new born with
respiratory distress
CONGENITAL DIAPHRAGMATIC HERNIA
Congenital Diaphragmatic Hernia
Minimal Barotrauma • Conventional Ventilation • High frequency ventilation • ECMO
Cardio-Pulmonary Stabilisation
(Pulmonary Hypoplasia + Hypertension)
Invasive & Noninvasive monitoring
Day 1
• Respiraory acidosis (Ph 7.26/PO2 118/Pco2 47/Hco3 20.1)
• Assisted control ventilation
– Fio2 100%
– PIP/PEEP: 15/5
• Dopamine and Adrenaline (Mean 50mm Hg)
• Cardiac Echo: Mild Pulmonary Hypertension
Day 2
• One episode of desaturation
• Respiratory acidosis
• Shifted on HFO
MAP 14
Fio2 100%
Delta P 30
• Stable
Day 3
• Desaturated
• Rt Pneumothorax- Drained
• Stable
Day 4(CDH Repair)
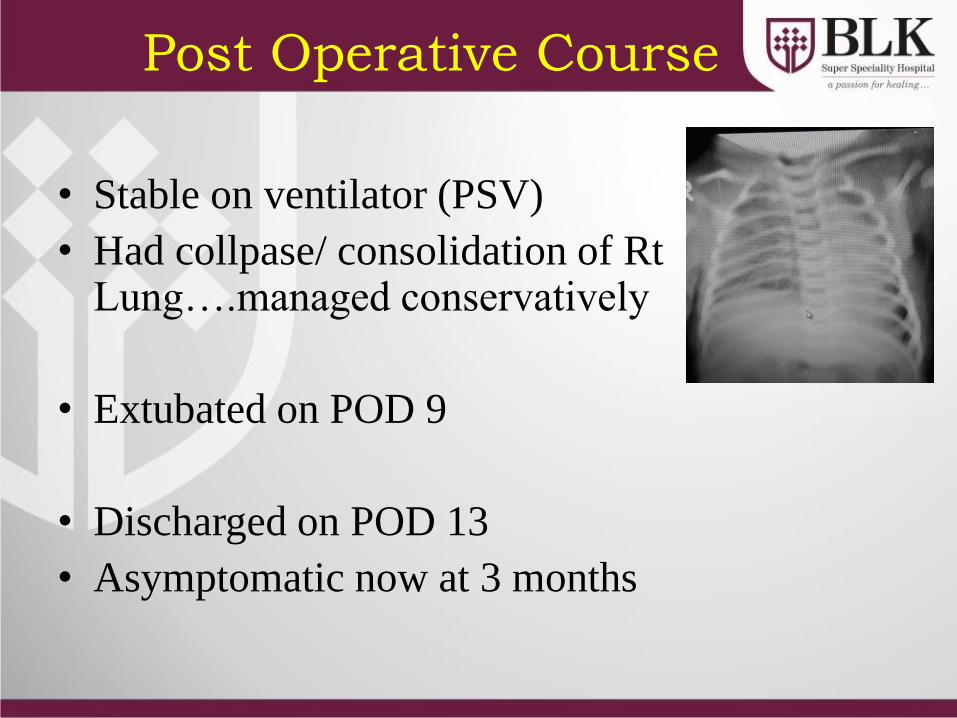
Post Operative Course
• Stable on ventilator (PSV)
• Had collpase/ consolidation of Rt Lung….managed conservatively
• Extubated on POD 9
• Discharged on POD 13
• Asymptomatic now at 3 months
A new born with respiratory distress
Cystic adenomatoid malformation
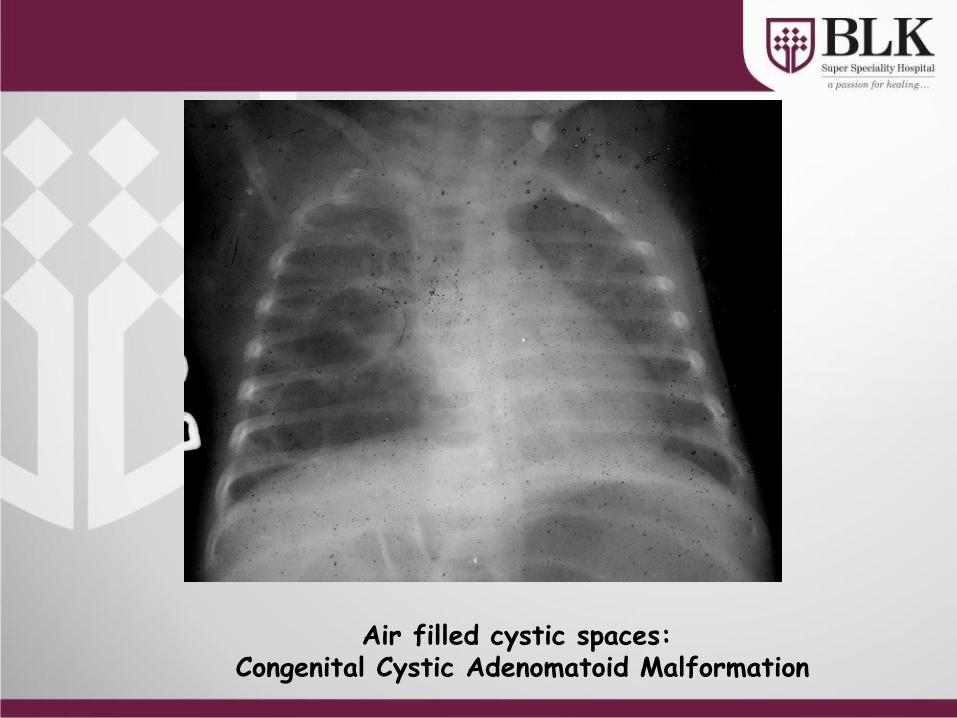
Air filled cystic spaces: Congenital Cystic Adenomatoid Malformation
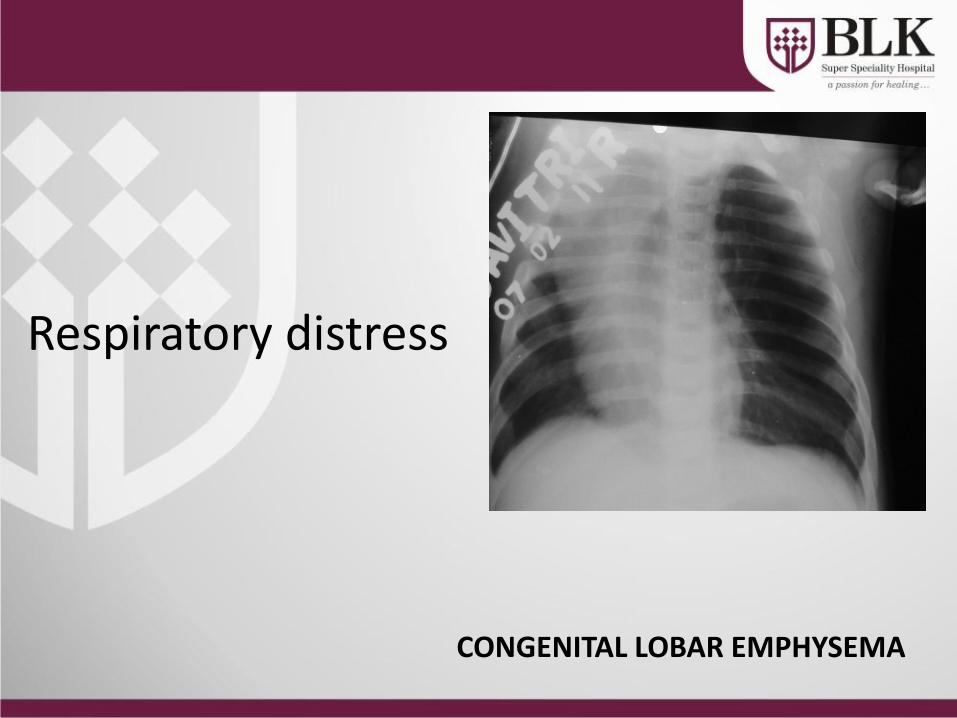
Respiratory distress
CONGENITAL LOBAR EMPHYSEMA
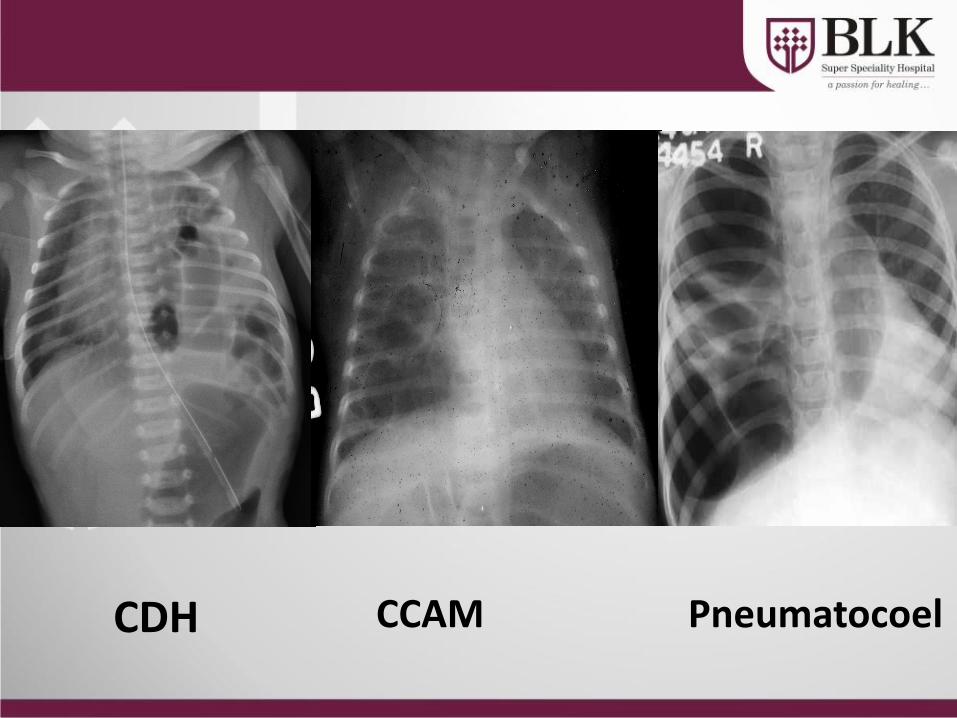
CDH CCAM Pneumatocoel


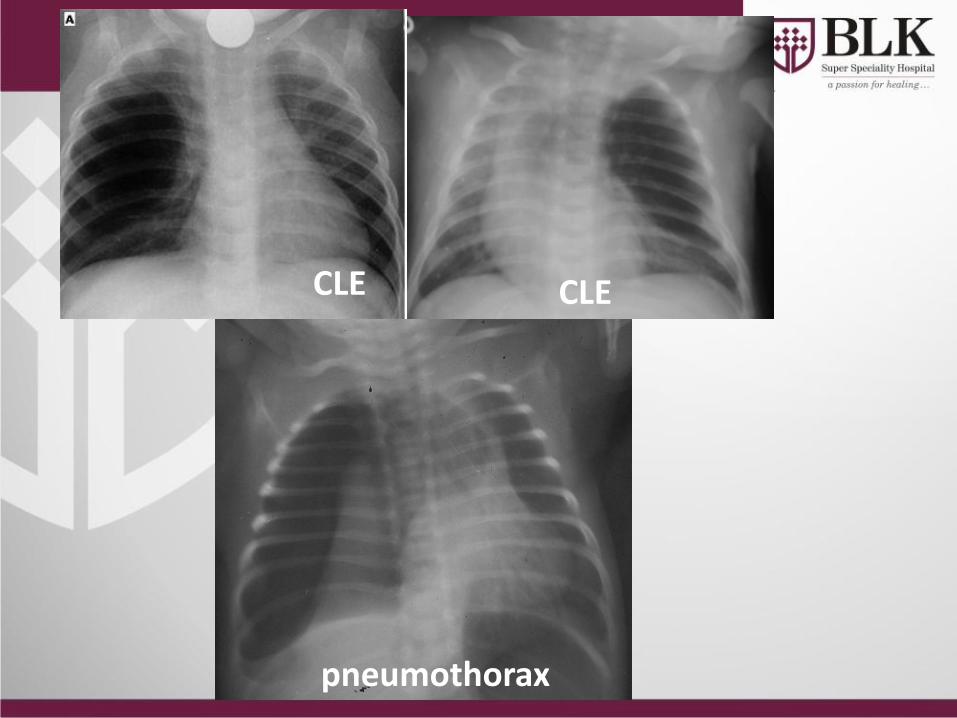
pneumothorax
CLE CLE

![Double Incomplete Pyloromyotomy (A. Ezzat Technique): A ...incidence reported of 1 to 8 per 1000 live births [1] [2]. Projectile non bilious vomiting and its complications are common](https://img.pdfslide.us/doc/110x75/6030a50ce330ab27063bb564/double-incomplete-pyloromyotomy-a-ezzat-technique-a-incidence-reported-of.jpg)