Embed Size (px)
Citation preview

Neonatal Resuscitation – Minimally Invasive Approach
Neil Finer
Professor Emeritus
Division of Neonatology
UCSD Medical School

Conflicts of Interest - N Finer
Dr. N. Finer is a paid consultant for Fisher& Paykel

One and two and three and Breathe !
Delivery Room Resuscitation

When does Resuscitation Begin?Delayed Cord Clamping
Placental blood is the babies blood
Safest blood to give to the infant and easiest
There was a concern that early clamping reduced PPHemorrhage
Recent analyses demonstrate that in Term infants delayed clamping is associated with higher hemoglobin ( + 2.17 g/dl) for up to 6 months and better iron stores, and more need for phototherapy
No change in PPHMcDonald and Middleton, Cochrane Review 2009

Delayed Cord Clamping and Preterm Infants
Rabe et al Cochrane Review 2012
Reviewed studies in preterm infants from 24 to 36 weeks
Delay from 30-180 seconds
Delayed/Milked group needed fewer transfusions for anemia, and had less IVH and NEC, but had higher peak bilirubin concentrations

Evidence supports delayed umbilical cord clamping in preterm infants.
European Consensus guidelines recommend a 30-45 second delay before clamping ( Sweet, 2010)
The single most important benefit for preterm infants is the possibility for nearly 50% reduction in intraventricular hemorrhage.
Raju T, Number 543, December 2012

Time of Cord Clamping – Delaying is much less invasive!!
AAP has endorsed the use of a delay before clamping for preterm infants whenever feasible, and for infants who do not need resuscitation (http://aapnewsde.aap.org/aapnews-open/201304_o/?pg=17#pg17)
However, how do we know at birth if the infant needs resuscitation- I think most of these infants would benefit from the transfusion which is after all fetal blood of up to 30-40ml/kg
Immediate cord clamping never proven to be beneficial by any controlled trials!!

Delayed Cord Clamping and Premature Delivery – Ongoing trials
Australian Placental Transfusion Study – will enroll 1600 infants < 30 weeks - Immediate Clamping vs 60 seconds
Composite outcome = death and/or major morbidity at 36 weeks defined by one or more of the following: Brain injury on ultrasound, Chronic lung disease, Severe retinopathy, Necrotising enterocolitis, Late onset sepsis
Currently 50% complete.
Will evaluate 2 year Neurodevelopmental Outcome

Current Use of Placental Transfusion in USA - Jelin AC et al. Obstetricians' attitudes and beliefs regarding
umbilical cord clamping. J Fetal-Maternal-&Neonatal Med 2013
Only 12% of responders had an umbilical cord clamping policy.
The most frequent response for lack of a policy for optimal timing of umbilical cord clamping, was “don’t know.”
Only cited reason for a delay was the potential for neonatal red blood cell transfusion
The reason to clamp the cord immediately was the risk of delaying neonatal resuscitation!!

Immediate vs Delayed Clamping and Ventilation: Bhatt et al J Physiol
2013;591;2113
Studied lambs (123 days) with catheters and probes in pulmonary and carotid arteries
Lambs were delivered at 126±1 days and:
Clamp 1st -ventilation was delayed for about 2 min (Clamp 1st; n = 6),
Vent 1st - umbilical cord clamping was delayed for 3–4 min, until after ventilation was established

Cord Clamp
Associated with immediate afterload to R and L Ventricle and decreasedR & L Preload
Associated with decreased HR and CO
Increases PVR and decreases PBF
Associated with Increased Carotid artery pressure and decreased blood flow
All may contribute to IVH!
Immediate Clamping

Immediate Clamping and fall of HR and RVO- Bhatt et al
Heart rates markedly decreased within 120 s of cord clamping in unventilated animals and recovered after ventilation.

Delayed Clamping and Early Ventilation -Bhatt et al J Physiol 2013
Immediate Cord clamping resulted in a rapid transient increase in carotid artery pressure, with decreased carotid flow, which then improved over the next minute. Not seen in Vent first animals!

Delayed Clamping and Early Ventilation -Bhatt et al J Physiol 2013
Delayed clamping until after ventilation was initiated maintained HR, and carotid pressure and flow
If Ventilation precedes cord clamping, there is secondary increase in PBF and RVO that persists for at least 30 min after birth.
Abolishes the adverse changes and smooths hemodynamic transition

Rabe H et al Cochrane Database Syst Rev. 2012 Aug 15;8:CD003248.
Subgroup analysis (Delayed Clamping and Cord Milking) : Severe Intraventricular Hemorrhage

PREMOD: PREmature infants receiving Milking Or Delayed
Clamping - Katheria et al
NICHD funded Pilot Study – Sharp Mary Birch Hospital for Woman San Diego
Primary Hypothesis: Milking will improve SVC flow in VLBW infants born by C/S compared to 45 second delay clamp
N= 197 infants (152 C-section, 45 Vaginal)
Milked infants had better Hemoglobins, BP over first 24 hrs, better SVC flow and better RVO

Blood Pressure Premod.
Milked
Delay

Best and First Least Invasive Practice
Provide adequate placental transfusion
If the infant is deemed to need immediate resuscitation – How do we determine this while infant still attached to placenta???- initiate stabilization while still attached to a pulsating cord to open lung and facilitate receipt of placental transfusion (If possible - needs to be proven!)
[http://clinicaltrials.gov/NCT02231411 Katheria et al]
or
Consider Milking and deliver



0
20
40
60
80
100
120
140
160
180
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97
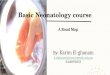
Excessive Facial Pressure Results in Bradycardia
Mask On Off On Off
Pulse Rate
SpO2
Seconds (X2)

Can a Pulse Oximeter Provide Useful Data within 1-2 minutes of Birth?
Gandhi et al, PAS – EPAS2012:4525:344
Retrospective review (June 2010 to December 2011, 50 Preterm Infants
SpO2 values recorded at 1 sample per second (Masimo).
Mean and median time to achieve functioning pulse oximetry was determined.
Gest - 23-35 weeks, BW -360-1445g

Time when Reliable SpO2 Signal Obtained
Mean = 79 ± 42 seconds(range 40-240 s)
Median = 67 seconds(interquartile range 50 – 93 s)

0-30 31-60 61-90 91-120 121-150 151-180 >1810
5
10
15
20
25
30
35
40
45
Time Distribution to working SpO2

Pulse Oximetry – Limitations!!
Now a standard but not easy to get reliable readings before 90 sec and sometimes longer
They probably provide less than accurate readings for initial minute(s)
The Oximeter HR reads somewhat lower than gold standard – ECG but most do not use!
This difference is probably not critical!

Heart Rate Monitoring: UCSD Practice
Auscultation
Continuous Display
Pulse oximeter
EKG leads
– Use for crash CS or known severe fetal compromise
– Use when unable to determine HR by other methods

ECG from Chest electrodes
HR from OximeterApplied

Bag and Mask Resuscitation:A Moving Experience!!
Ensure adequate seal over mouth and nose Use adequate pressure to inflate chest Both Bag and chest should move Commonest problems – leak and airway
obstruction

Does Achievement of Target PIP during Bag and Mask Ventilation Equate to
adequate Ventilation??O’Donnell et al Arch Dis Child Fetal Neonatal Ed. 2005; 90(5):F392-6.
How do you know you are ventilating the infant? Evaluated bagging on a manikin using expired VtThere are large leaks around the face mask. Airway pressure is a poor proxy for volume
delivered during positive pressure ventilation through a mask.
We were concerned that we are not ventilating the infant with every pressured breath!!

Chest Rise as Indicator of Delivered Tidal Volume during Resuscitation-
Resuscitation 2011;82:175 Arch Dis Child Fetal Neonatal 2010;95:393
Performed 2 studies to compare operators assessment of Vt delivered by face mask from Chest Movement compared to delivered Vt
Compared looking at infant from head or beside infant
No good correlation found
For No Vt at all – Actual Vt = 8.3ml/kg
For “not sure” – Actual Vt = 8.6 ml/kg
Estimated Vt was underestimated by > 3.0ml

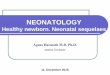
Figure 4 Comparison of expired tidal volume with the operator estimates of chest rise. The horizontal lines show the range of V Te which would provide reasonable ventilation. The y axis represents V Te in ml/kg and the x axis operator estimates of chest rise. The box plots show median values (solid bar), IQR (margins of box) and 95% CI.
Schmoelzer et al Arch Dis Child Fetal Neonatal 2010;95:393
Chest Rise vs Measured Vt during Resuscitation in Preterm Infants

Determination of Adequate Ventilation during Resuscitation
We were concerned that achieving adequate PIP during bagging would not necessarily lead to an adequate delivered breath
Previous work confirmed that reaching PIP was not adequate evidence of an effective breath!
We wanted to avoid complicated instrumentation We looked for a simple method – PediCap was
being used to confirm intubation

Confirming Airway Patencyduring Bagging
Leone et al Pediatrics 2006:118;E202-4
You need an effective breath and a perfused lung!!
No color change forces the team to recheck for airway patency
One Manufacturer now adding such a colorimetric strip to baggers

Failure of Adequate Bagging
Airway obstructed: commonest causes are Tongue against pharyngeal wall Closure of larynx following central apnea Muscle rigidity following fentanyl?
Airway Obstruction – Can create pressure in bagger without gas exchange or chest wall movement
Difficult to appreciate at bedside

Confirming Airway Patency during Bagging
Leone et al Pediatrics 2006:118;E202-4
We started using the Colorimetric CO2 detector during bagging
It will change color if CO2 is detected This is semi-qualitative You will only get CO2 if gas from the lung is
detected and there is pulmonary perfusion!!!

Pedi-Cap Color Ranges
Purple
CO2 <4mmHg<0.5% CO2
Tan
CO2 4-15mmHg0.5-2% CO2
Gold
CO2 >15mmHg>2% CO2

A B C
Top Tracing - Mask Applied, No PediCap® color change till B - Airway pressure increased by operator, Pedicap Changed color at C
Bottom Tracing - Target pressure not being reached with a pressure plateau, and probably represents a significant air leak, no PediCap® color change observed.
Finer et al, Pediatrics 2009;123:865

Airway Obstruction during PPV Finer et al, Pediatrics 2009;123:865
24 VLBW patients reviewed with adequate data
6 had no evidence of color change Of remaining 18, there were a median of
14 obstructed initial breaths(4-37, 10-220 seconds duration)

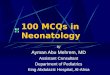
* * *
* p <0.001
Change in HR over Time, N=46.Blank et al, Resuscitation 2014 Sep 15
Seconds
-30 -20 -10 Gold +10 +20 +3050
60
70
80
90
100
110
120
130
140
150

Volume Monitoring in DR
Technology available and reasonably simple using hot wire devices
Adds dead space and resistance
Need education to recognize real exhaled volume and calculation of leak
Newer and simpler devices are being produced to simplify these observations

Respiratory Function Monitor during Resuscitation
Schmoelzer at el, J Pediatr 2012;160:377-81
Percent leak Expired Tidal Volume

Airway Obstruction and Leak during PPVSchmoelzer et al, Arh Dis Child Fetal Neonatal Ed 2011
Jul;96(4):F254-7
Used Respiratory Function monitor
Reported obstruction in 26% beginning at mean of 46 sec, and lasting for a median of 22 breaths – up to 83 consecutive inflations!!
Leak noted in 51% usually starting with first attempted inflation
A median (range) of 10 (3-117) consecutive inflations with a leak >75% were delivered.

Airway Obstruction and Leak during PPVSchmoelzer et al, Arch Dis Child Fetal Neonatal Ed
2011 Jul;96(4):F254-7

Airway Obstruction and Leak during PPVSchmoelzer et al, Arch Dis Child Fetal Neonatal Ed
2011 Jul;96(4):F254-7

Current Controversies in ResuscitationSustained Inflations
TePas et al use longer breaths – 10 sec but study methodology problem –compared with SIB without PEEP! (Pediatrics. 2007;120:322-329)
European Guidelines recommend the use a prolonged inflation of 3-5 seconds before increasing the inspiratory pressure.
Recently demonstrated that SI are ineffective if infant apneic - Von Vonderon et al, J Pediatr 2014

Current Controversies in ResuscitationSustained Inflations
SIs very effective in intubated infant
In other situations when delivering with a mask their effectiveness remains to be proven
They may be associated with increased air leaks
Large study about to begin
I would use for infants unresponsive to PPV with continuing bradycardia and/or desaturation and try to limit to 30 cm and 5-10 seconds duration

Neonatal Resuscitation:The Environment
We cannot change the human condition but we can change the conditions under which we work
Reason BMJ 2003;320:768-70

Leader and Team Problemsduring Videotaped Resuscitations
at UCSD
More than 1 person doing single task (drying) Nobody giving heart rate Nobody assisting with O2 during intubation Nobody calculating duration of intubation attempt Nobody providing cricoid pressure No one coordinating compressions and ventilation No Obvious Leader!!

Preparation for Resuscitation –Led us to Develop a Checklist
Choose a leaderReview relevant NRP guidelines ( ie Meconium)Review each members task(s)Prompt and Support individuals with positive
feedbackProvide objective input (duration of intubation,
coordination of compressions and ventilation)Debrief following with constructive comments
Pre-Resuscitation Checklist
Review each team members role
Discuss any special circumstances – CDH, Anomalies, ELBW etc
Check equipment – and special needs – transilluminator, video laryngoscope, etc
Encourage direct dialogue, and acknowledgement!!
Prepare and Include family if present and have staff


Communication
A pre-brief should include a specific statement, to be read every time, which encourages everyone that if they see something they are not comfortable with, they communicate it to the leader

Post Briefing
Quick huddle in NICU or DR
What did we do well? What did we
do poorly? What can we
do better?

Thank you foryour attention!