Embed Size (px)
Citation preview

Neonatal Resuscitation
Neonatal Resuscitation
ALSO(UK) wish to thank Dr S Richmond for this talk and fully acknowledge the use of material copyright the northern Neonatal
Network, the Resuscitation Council (UK) and the Newborn Life Support course

ObjectivesObjectives
• Select and properly use equipment for neonatal resuscitation
• Perform rapid evaluation of the newborn
• Describe resuscitation schemes and algorithms
• Describe the management of meconium
• Describe the management of the early neonatal period and the most common complications

Stimuli for the first breathStimuli for the first breath
• Cord obstruction
• Cold air
• Physical discomfort

First breathsFirst breaths
Push fluid from airway& alveoli into pulmonary
lymphatics
Push fluid from airway& alveoli into pulmonary
lymphatics
Establishesresting lung volume
Establishesresting lung volume

Sustained (2 second) Inflation BreathsSustained (2 second) Inflation Breaths
First
Breaths
Arterioles Dilate and Blood Flow Increases
Third
Second
Fetal LungFluid
Air
O2
O2 O2

Resuscitation EquipmentResuscitation Equipment
YOU CAN SUCCESSFULLY RESUSCITATE WITH THE FOLLOWING MINIMUM EQUIPMENT &
SKILLS: • Towels to dry and wrap
• Appropriate-sized face mask
• 500ml ventilation bag
• Firm, stable surface (possibly the floor)
• Ability to ventilate appropriately
• Ability to perform cardiac massage

‘Ideal’ Additional Equipment‘Ideal’ Additional Equipment
ClockGas supply and blow off valveGuedel airwaysLaryngoscope & Endotracheal tubesLightingDrugs - Sodium Bicarbonate - Adrenaline - Dextrose - (Volume)Wide-bore suckerScissors and tape

• Dry & cover the baby• Assess the situation• Airway• Breathing - Inflation breaths• Chest compressions• (Drugs)
Basic steps in resuscitationBasic steps in resuscitation

Initial actionsInitial actions
• Start the clock • Dry the baby • Assess
Do you need help ?

Initial assessmentInitial assessment
• Colour
• Tone
• Breathing
• Heart rate

Condition – Group 1Condition – Group 1
• Blue Pink
• Good tone
• Breathing regularly
• Fast heart rate

Dry and coverGive to Mum
Dry and coverGive to Mum
• Blue Pink
• Good tone
• Breathing regularly
• Fast heart rate
ManagementManagement

• Blue
• Moderate tone
• Breathing inadequately
• Slow heart rate
Condition – Group 2Condition – Group 2

• Blue
• Moderate tone
• Breathing inadequately
• Slow heart rate
ManagementManagement
Dry and coverOpen the airwayInflation breaths
Dry and coverOpen the airwayInflation breaths

• Blue or white
• ‘Floppy’
• Not breathing
• Slow or very slow heart rate
Condition – Group 3Condition – Group 3

• Blue or white
• ‘Floppy’• Not breathing
• Slow or very slow heart rate
ManagementManagement
Dry and coverOpen the airwayInflation breathsRe-assessDo you need help ?
Dry and coverOpen the airwayInflation breathsRe-assessDo you need help ?

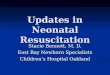
Neonatal Position for Opening the Airway – ‘neutral position’
Neonatal Position for Opening the Airway – ‘neutral position’
Incorrect: Neck Hyperextension
Incorrect: Neck Under Extended
Correct: Neck Slightly Extended

Head flexed by large occiputHead flexed by large occiput

Head in neutral or ‘sniffing’ positionHead in neutral or ‘sniffing’ position

Jaw falling back – obstructing airwayJaw falling back – obstructing airway

‘Jaw thrust’ applied – in neutral position‘Jaw thrust’ applied – in neutral position

• Open the airway - place the child in the neutral position
• If necessary, provide jaw thrust
• Give FIVE initial inflation breaths
Airway ManagementAirway Management

Inflation breathsInflation breaths
Five breaths,each sustained for 2-3 seconds
at 30 cms of water pressure
Five breaths,each sustained for 2-3 seconds
at 30 cms of water pressure

• The heart rate will usually respond to lung inflation
• If there is no heart rate response check for chest movement
Inflation breathsInflation breaths

• Airway reassess
• Breathing reassess - is there a response
?
• Chest compressions reassess
• Drugs
Further resuscitationFurther resuscitation

• If the chest is not moving, it is not being inflated
• Check A & B
• Do not start chest compressions until the chest is being inflated
Chest compressionsChest compressions

ReassessReassess
• If the heart rate is slow and not improving
• Consider chest compressions

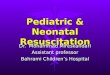
Chest (cardiac) compressionsChest (cardiac) compressions
“Two-thumb” technique is usually preferred

• Indicated when HR < 60bpm after 30 seconds of effective ventilation
• 3:1 compressions:breaths at HR approx 100bpm (Note: EFFECTIVENESS IS MORE IMPORTANT THAN RATE!!!)
• Re-evaluate HR every 30 seconds
• Continue cardiac compressions until HR rising and approx 100bpm (Note: HR USUALLY RESPONDS RAPIDLY)
Chest (cardiac) compressionsChest (cardiac) compressions

Chest (cardiac) compressionsChest (cardiac) compressions
You only need to move oxygenated bloodfrom the lungs to the coronary arteries
Its not that far and won’t take long!

ReassessReassess
• Has the heart rate improved ? No
• Re-check airway• Check chest movement• Check compressions

• Sodium bicarbonate
• Adrenaline
• Dextrose
• (Volume - rarely)
Consider drugsConsider drugs

• Preterm babies care with inflation pressures
• Meconium see next slide
• Congenital abnormality eg diaphragmatic hernia - may make resuscitation extremely difficult
• Delivery outside labour ward cold babies are more difficult to
resuscitate
Special CasesSpecial Cases

MeconiumMeconium
• Suction ONLY IF ‘SOLID’ MECONIUM causing physical block to ventilation use catheter or endotracheal tube with wall suction
• Vigorous infant tracheal suction NOT indicated
• Infant with absent/depressed respirations, HR < 100bpm or poor tone if bag ventilation is inadequate, intubate with 10F
catheter to clear SOLID meconium below cords

• Dry & cover the baby• Assess the situation• Airway• Breathing - Inflation breaths• Chest compressions• (Drugs)
summary neonatal resuscitation summary neonatal resuscitation

Neonatal mortalityNeonatal mortality

Causes of neonatal mortality Causes of neonatal mortality
• Preterm birth
• Asfyxia
• Neonatal sepsis
60-80% of neonatal deaths happen in
low birth weight infants (<2000 gr.)

Preventing neonatal mortalityPreventing neonatal mortality
• All well-responding newborns should be given to their mother immediately after birth and start breastfeeding as soon as possible.
• Skin to skin contact with the mother is the best way of keeping the newborn warm.
• Breastfeeding helps inflate the lungs of the newborn (and prevents the mother from having PPH).
• Do not suction the ventricle

Managing preterm birthsManaging preterm births
• If gestational age below 34 weeks the mother should have corticosteroids:
• Betametazone 12 mg IM twice 24 hours apart
• Reduces risk of perinatal death 68%
• Reduces risk of Respiratory distress syndrome 66%
• Reduces risk of intra-cerebral haemorrhage 54%

Managing preterm or low birth weight neonatesManaging preterm or low birth weight neonates
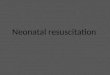
Kangaroo Mother Care (KMC)
• Early, continuous and prolonged skin-to-skin contact between the mother and the baby
• Exclusive breastfeeding
• Initiated in hospital and can be continued at home

Kangaroo mother careKangaroo mother care

Kangaroo mother careKangaroo mother care

Kangaroo mother careKangaroo mother care
Breastfeeding:
preferably mothers milk: if not directly then by cup

Kangaroo mother careKangaroo mother care
Expressing breast milk:

Kangaroo mother careKangaroo mother care
Expressing breast milk:

Kangaroo mother careKangaroo mother care
Breastfeeding:

AsfyxiaAsfyxia
• Early feeding
• Thermal regulation (KMC / SSC)
• Close observation (at risk for sepsis)

Neonatal sepsisNeonatal sepsis
Risk factors:
• Unhygienic procedures
• Prolonged rupture of membranes >24 hours
• PPROM
• Preterm birth
• Asfyxia

Neonatal sepsisNeonatal sepsis
Signs:
• Unable to breastfeed
• Lethargic or unconscious
• Fast breathing
• Severe chest indrawing
• Grunting
• Fever
• Hypothermia
• Umbilical discharge and redness of surrounding skin

Neonatal sepsisNeonatal sepsis
Treatment:
Early feeding
Antibiotics:
• Ampicillin (or penicillin) 25 mg/kg. IV each 6 hours
• Gentamycin 3 mg/kg IV each 12 hours
• Consider antimalarial treatment
Close observation