-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
1/36
Neonatal
Hyperbilirubinemia
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
2/36
Jaundice
Yellowish discoloration of skin +/- sclera ofnewborns due to
bilirubin
Affects nearly all newborns Peak: 48-120 hours, typically 5-6
mg/dL,
usually does not exceed 17-18 mg/dL
Pathologic: TSB exceeds age (in hours)specific 95th percentile
according to Bhutaninomogram
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
3/36
Effects of
hyperbilirubinemia Bilirubin toxicity
Toxicity due to unbound (free) form
Focal necrosis of neurons and gliaAcute bilirubin
encephalopathy
Chronic= kernicterus
Most often affects basal ganglia and
brainstem nuclei Movement disorders
Impaired upward gaze
Auditory abnormalities
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
4/36
Effects
Bilirubin toxicityAt risk when TSB > 25-30 mg/dL
Premature and sick infants
Albumin level
Drugs- silfisoxazole, moxalactam, ceftriaxone
Acidosis
Near term (35-37) weeks
Breast fed Hemolytic disease
Discharge before 48 hours
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
5/36
Manifestations
Phase one- 1st few days Lethargy, hypotonia, poor suck, high
pitched cry Phase two- end of 1st week
Irritable, hypertonia, retrocollis,opisthotonus
Phase three- after 1st week Stupor, coma, shrill cry
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
6/36
Evaluation
Transcutaneous bilirubin
Total serum bilirubin
End-tidal carbon monoxide
Blood type, direct Coombs test
CBC, peripheral blood smear Reticulocytes, G6PD screen
Serum albumin
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
7/36
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
8/36
Special circumstances
Jaundice in 1st 24 hours
Frequently due to hemolysis
Require immediate evaluation and closesurveillance
Other reasons for increased bilirubin
production Cephalohematoma, extensive bruising,
conjugation disorders
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
9/36
Management
Phototherapy Mechanisms
Structural isomerization Photoisomerization
Photo-oxidation
Irradiance
Initiation if bilirubin exceeds the 95thpercentile for
hour-specific TSBconcentration and risk category
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
10/36
Risk categories-
phototherapy Lower risk: at least 38 weeks gestation, no
risk
factors >12 mg/dL at 24 hours, >15 mg/dL at 48 hours,
>18
mg/dL at 72 hours
Medium risk: at least 38 weeks with risk factors or35-38 weeks
without risk factors >10 mg/dL at 24 hours, >13 mg/dL at 48
hours, >15
mg/dL at 72 hours
Higher risk: 35-38 weeks with risk factors >8 at 24 hours,
>11 at 48 hours, >13.5 at 72 hours
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
11/36
Management
Rate of decline of TSB
Irradiance
Surface area
Initial TSB
Discontinuation
TSB level below 95th percentile for age
Is less than 13 mg/dL
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
12/36
Management
Exchange transfusion Hyperbilirubinemia unresponsive to
phototherapy Especially useful with immune-mediated
hemolysis Removal of circulating antibodies and
sensitized RBCs For TSB > 25 mg/dL
Presence of bilirubin neurotoxicity
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
13/36
Risk categories-
exchange transfusion Lower risk: at least 38 weeks gestation, no
risk factors
>19 mg/dL at 24 hours, >22 mg/dL at 48 hours, >24 mg/dL
at72 hours
TSB/Albumin>8.0
Medium risk: at least 38 weeks with risk factors or 35-38weeks
without risk factors >16.5 mg/dL at 24 hours, >19 mg/dL at 48
hours, >21 mg/dL at
72 hours TSB/Albumin>7.2
Higher risk: 35-38 weeks with risk factors >15 at 24 hours,
>17 at 48 hours, >18.5 at 72 hours TSB/Albumin>6.8
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
14/36
Summary
Assess for jaundice every 8-12 hours
Assess risk factors
If discharging, appropriate follow-up isnecessary
Treatment should be initiatedimmediately upon
identifyingsignificant hyperbilirubinemia
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
15/36
Approach to themanagement ofHyperbilirubinemia in
Term Newborn Infant
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
16/36
2004 AAPGuidelines
Management of Hyperbilirubinemia in theNewborn Infant 35 or More
Weeks ofGestation
Subcommittee on HyperbilirubinemiaPediatrics
2004; 114;297-316
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
17/36
Prevention
Breastfeeding
Should be encouraged for most
women Separate AAP guidelines
8-12 times/day for 1st several days
Assistance and education
Avoid supplements in non-dehydratedinfants
Do not decrease level & severity ofhyperbili
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
18/36
Prevention
Ongoing assessments for risk ofdeveloping severe
hyperbilirubinemia
Monitor at least every 8-12 hours
Dont rely on clinical exam
Blood testing
Prenatal (Mom): ABO & Rh type, antibody
Infant cord blood Mom not tested, Rh (-): Coombs, ABO, Rh
Mom O or Rh (+): optional to test cord blood
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
19/36
Laboratory investigation
Indicated (if bilirubin concentrations reachphototherapy levels)
Serum total or unconjugated bilirubin concentration
Serum conjugated bilirubin concentration
Blood group with direct antibody test (Coombstest)
Hemoglobin and hematocrit determinations Optional (in specific
clinical circumstances)
Complete blood count including manual differentialwhite cell
count Blood smear for red cell morphology Reticulocyte count
Glucose-6-phosphate dehydrogenase screen
Serum electrolytes and albumin or proteinconcentrations
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
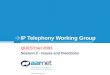
20/36Co ri ht 2004 American Academ of Pediatrics
Subcommittee on Hyperbilirubinemia, Pediatrics
2004;114:297-316
Nomogram for designation of risk in 2840 well newborns at 36 or
more weeks'
gestational age with birth weight of 2000 g or more or 35 or
more weeks' gestational
age and birth weight of 2500 g or more based on the
hour-specific serum bilirubin
values
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
21/36
Risk Factors for SevereHyperbilirubinemia
Major risk factors
Predischarge bili in high-riskzone
Jaundice in 1st 24 hrs Blood group incomp with +
direct antiglobulin test, otherknown hemolytic disease (eg,
G6PD deficiency) Gestational age 3536 wk Previous sibling
received
phototherapy Cephalohematoma or
significant bruising
Exclusive breastfeeding East Asian race
Minor risk factors
Bili in high intermed-risk zone Gestational age 3738 wk Jaundice
before discharge Previous sibling with jaundice Macrosomia infant
with
diabetic mother
Maternal age 25 Male
Decreased Risk Bili in low-risk zone
41 wks gestation Exclusive bottle feed Black race D/c from
hospital > 72hrs
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
22/36
Discharge
Assess risk Predischarge bili
Use nomogram to determine risk zone
And/or Assessment of risk factors
TSB Zone Newborns(%)
% with TSB>95th %
High risk 6 39.5High intermed 12.5 12.9
Low intermed 19.6 2.26
Low 61.8 0
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
23/36
Discharge
Close follow-up necessary
Individualize based on risk
Weight, % change from BW, intake,voiding habits, jaundice
InfantDischarge
Should be Seenby
< 24 hours 72 hours
24-48 hours 96 hours
48-72 hours 120 hours
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
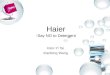
24/36Co ri ht 2004 American Academ of Pediatrics
Subcommittee on Hyperbilirubinemia, Pediatrics
2004;114:297-316
Algorithm for the management of jaundice in the newborn
nursery
-
7/29/2019 Neonatal Hyperbilirubinemia2009 Modified for
Presention
25/36
Phototherapy
Mechanism: converts bilirubin to watersoluble form that is
easily excreted
Forms Fluorescent lighting
Fiberoptic blankets
Goal is to decrease TSB by 4-5 mg/dL or