Embed Size (px)
Citation preview

DOI: 10.1542/neo.11-7-e349 2010;11;e349-e362 NeoReviews
A. Graham Wilkinson and Sally Wilkinson Neonatal Hip Dysplasia: A New Perspective
http://neoreviews.aappublications.org/cgi/content/full/neoreviews;11/7/e349located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 2000. NeoReviews is owned, published, and trademarked NeoReviews is the official journal of the American Academy of Pediatrics. A monthly publication,
by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

Neonatal Hip Dysplasia: A New PerspectiveA. Graham Wilkinson,
MB, BS, FRCR,* Sally
Wilkinson, MCSP†
Author Disclosure
Dr and Ms Wilkinson
have disclosed no
financial relationships
relevant to this
article. This
commentary does not
contain a discussion
of an unapproved/
investigative use of a
commercial
product/device.
AbstractThis review of neonatal hip dysplasia examines the clinical and ultrasonographicliterature that has guided current practice and discusses the controversies involved indetection and treatment of the condition. We present a view that combines clinicaland ultrasonographic criteria in a simple and effective treatment decision pathway.Enthusiasm, specialization, and expertise in clinical and ultrasonographic aspects, withclear communication and cooperation between these two disciplines, are necessary toachieve an effective screening program.
Objectives After completing this article, readers should be able to:
1. List risk factors for developmental dysplasia of the hip (DDH).2. Describe appropriate neonatal hip examination procedures.3. Discuss initial treatment for DDH.4. Describe ultrasonographic classification of the neonatal hip.5. State the consensus opinion on the role of ultrasonography in screening for DDH.6. List static ultrasonographic warning signs for DDH.
IntroductionDevelopmental dysplasia of the hip (DDH) represents a spectrum of abnormalities thatranges from a minor self-correcting abnormality with no long-term consequences to“congenital” hip dislocation with lifelong disability. Up to 29% of hip replacements inadults younger than 60 years of age are due to DDH. (1) Although genetic and hormonalfactors may play some part, the primary cause is believed to be intrauterine restriction offetal movement in later gestation. (2) Because most fetuses spend the last few weeks ofpregnancy in one position, this is the critical period. The most common position for thefetus at birth is vertex presentation, with the left leg adjacent to the mother’s spine. Thespine, being less compliant than other tissues bordering the uterus, indents it posteriorly,pushing the fetus’ left hip into adduction. In adduction, the hip is less stable and thefemoral head is more easily displaced superolaterally, causing pressure of the upper aspectof the femoral head on the acetabular margin. This, in turn, causes subsequent molding ofthe joint surfaces, which are compliant due to their cartilage not yet being ossified.Distortion of the articular surfaces and the habituation to adduction predisposes to jointlaxity, instability, and dislocation postnatally. Hip dysplasia is more common on the leftbecause this is usually the side compressed by the maternal spine. Other presentations, suchas extended breech, can result in either or both hips being affected.
Risk factors for DDH encompass any cause of intrauterine restriction, including firstpregnancy, oligohydramnios, and breech presentation (especially extended breech), al-though 75% of babies requiring treatment do not have risk factors, other than beingfemale. (3) Female babies are affected four to eight times more frequently than males dueto their sensitivity to the maternal hormone relaxin. There is a relationship of DDH withcaesarean section simply because large fetuses or those that have abnormal lies may need tobe delivered operatively rather than vaginally. There is also a genetic element, with babiesof mothers who have hip dysplasia having a considerably increased incidence. This may be
*Department of Radiology.†Department of Physiotherapy, Royal Hospital for Sick Children, Edinburgh, United Kingdom.
Article musculoskeletal disorders
NeoReviews Vol.11 No.7 July 2010 e349 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

due to a number of factors, possibly including collagendisorders causing hypermobility or pelvic or uterine char-acteristics.
Ortolani is widely recognized as the pioneer of con-genital hip dislocation, publishing the description of histest for hip instability in 1937, (4) but the publicationwas in an Italian journal and received relatively littleattention for a decade. His test relies on the finding thatdislocation in older babies is usually posterior, so whenthe hips are flexed to 90 degrees with the knees together,during progressive abduction of the hips, a dislocated hiprelocates with a palpable sudden movement. In the late1940s, hip dysplasia began to be recognized as a treatablecondition in neonates, with orthopaedic surgeons, in-cluding von Rosen in Sweden (5) and Barlow in theUnited Kingdom, (6) describing diagnosis in the earlypostnatal period using Ortolani’s test or modifications ofit and instituting treatment using a variety of appliancesto hold the hips in abduction. With the hip stabilized inthe abducted position, the femoral head is held securelyin the acetabulum, and joint remodelling occurs within afew months, thereby stabilizing the hip and preventingfuture disability. In the United Kingdom, the incidenceof hip instability requiring treatment was reported ini-tially as about 2.5 per 1,000 births but increased to 6 to7 per 1,000 by the 1970s. (7)
Ultrasonography to assess the morphology of the hipexamination was introduced in 1980 (8) and took severaldecades to become widely accepted. Now it is regardedas an essential component of the diagnostic pathway forbabies who have suspected dysplasia. Approximately 5 to7 babies per 1,000 births now are treated in Scotland.The increase may be due to ultrasonography detectinglesser degrees of dysplasia but also may be related tobabies being placed supine to sleep to minimize the riskof sudden infant death syndrome. (9) Controversy per-sists over the relative merits of clinical and ultrasono-graphic examination in neonatal hip screening.
This article examines the clinical and ultrasonographicaspects of DDH and gives a combined personal opinionof the authors, who colead the hip screening and treat-ment program in Edinburgh, United Kingdom.
Neonatal Hip ExaminationBecoming an expert in neonatal hip examination requiresevaluation of many thousands of hips and awareness ofthe outcomes, with some learning resulting from feed-back. Such expertise requires at least a couple of years todevelop and in our institution is held by specialist pedi-atric physiotherapists, one of whom (SW) coleads thescreening program and exclusively assesses, treats, and
advises on neonatal hip problems. She coordinates all ofthe personnel involved from the maternity unit to theorthopedic outpatient clinic. Rotational junior neonatalstaff are not experts and are documented to miss morethan 50% of abnormal hips. (10) In an era of increasinglitigation, the expertise of the neonatal hip examiner islikely to be subject to more scrutiny than in the past, andthe cost of compensation for missed diagnoses couldprove to be the stimulus for improving screening pro-grams.
In addition to the general neonatal examination per-formed by rotational junior medical staff, the expertphysiotherapists examine as many babies as possible,giving priority to those who have known risk factors forDDH, including big first-born overdue girls, babies whohave features of molding, long babies, and those inwhom the junior doctor is unsure. Nursery nurses areadept at recognizing babies who may be at risk and referthese to the expert physiotherapists.
Neonatal hip examination involves knowledge of anypredisposing risk factor for hip dysplasia, observation ofthe baby at rest and during movement, and tests ofstability. The neonate should be settled, comfortable,and fed prior to the examination. Haste due to earlyhome discharge or an unsettled and “flexed-up” babymakes hip examination a challenge. The examinationstarts at the head, looking for features of molding dueto intrauterine restriction such as plagiocephaly or torti-collis. There may be an asymmetric lie due to scoliosisor foot deformity, particularly calcaneovalgus. (11)(12)The diaper should be removed to allow the essentialobservation of the groin and posterior gluteal creases.The affected hip exhibits more vernix in the inguinal fold,which is deeper than the unaffected side.
Abduction of the hips should be assessed by theexaminer holding both legs with the tips of the fingersoverlying the greater trochanters. The hips are flexed to90 degrees and gently simultaneously abducted to theirfull range. A dislocated femoral head may be felt torelocate with a “clunk” or sliding movement duringabduction.
The Barlow test (6) should be performed on each hipin turn. The pelvis should be cradled in the examiner’shand, which stabilizes the sacrum. With the hip flexed to90 degrees, gentle posterior pressure is exerted along thelength of the femur so any posterior movement of thefemoral head can be appreciated by the examiner’s fin-gers overlying the greater trochanter. A stable hip has afirm end feel, but a subluxing hip can be felt to moveposteriorly and relocate on gentle anterior traction.
musculoskeletal disorders neonatal hip dysplasia
e350 NeoReviews Vol.11 No.7 July 2010 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

A similar push-pull test can be performed in other direc-tions: posterosuperiorly and superiorly.
The Ortolani maneuver is a combination of the twopreviously described tests. With the hip flexed to 90degrees, posterior pressure is applied to the hip, which isprogressively abducted. If the hip is unstable, posteriormovement can be felt, and during the first few degrees ofabduction, the femoral head jumps forwards, relocatinginto the acetabulum with a “clunk.”
An experienced examiner may use a combination ofany of these tests. (13) A hip may be unstable in onedirection only, and the degree of instability varies. Inneonates, hips are rarely dislocated; asymmetric lie, lim-ited abduction, and instability on the Barlow test are themost useful signs.
Inexperienced examiners often apply too much pres-sure and abduct forcefully, so they are unable to appre-ciate the subtle sensation of small degrees of movementcaused by subluxation or relocation of the femoral head.They may not realize that hip relocation occurs withinthe first few degrees of abduction.
There is a group of babies whose position of comfort,due to restriction in utero, is to lie to one side (moreoften the right) with the contralateral (usually left) legextended and adducted. Such babies often are describedas “skew” (meaning oblique, slanting, sideways, or de-formed) in the United Kingdom, but a term such asmolded also can be used. There may be calcaneovalgusfoot deformity on the right and hip dysplasia on the left.During clinical examination of the hip, the femoral headis unstable superiorly but is stable posteriorly during theBarlow/Ortolani maneuver and is easy to miss by aninexperienced examiner.
Babies in whom abnormalities are detected by thephysiotherapist are referred for ultrasonographic exami-nation. In the interval, parents are given positioningadvice to encourage symmetric abduction of the hips.This may include placing a piece of rolled fabric underthe side to which a baby tends to lie or some time spentlying prone in the “frog” position when awake.
DDH seems to be relatively uncommon in pretermbabies, perhaps because of less restriction in utero orbecause preterm babies commonly are nursed in thesupine position in neonatal units. Our practice is to delaydecisions on treatment until the baby is 2 to 3 weekscorrected gestational age.
Initial TreatmentThe decision to treat is based on the clinical and ultra-sonographic findings and the baby’s age. Clinical andultrasonographic findings should agree because they are
simply different methods of assessing the degree of hipinstability. Because instability detected in the neonatalperiod may resolve spontaneously, we rarely start treat-ment before the age of 3 weeks. Treatment involvesapplication of an abduction device to keep the hip flexedand abducted. In this position, the hip cannot subluxsuperiorly or posteriorly, so the cartilaginous labrumceases to be deformed and can develop and ossify nor-mally. The entire process of stabilization and ossificationof the acetabular margin takes approximately 12 weeks.
We use the Pavlik harness, which consists of fourstraps (two on each side) connecting soft bootees to achest band (Fig. 1). The front straps flex the hips andinitially should be adjusted to restrict the hip to a mini-mum 100 degrees of flexion. In this position, when thebaby attempts to extend the leg, the hip does not moveout of joint. After approximately 1 week, the hip stabi-lizes, and thereafter, the safe range is 90 to 120 degreesof flexion. (13) The back (abductor) straps are adjustedso the hip cannot be adducted to less than 50 degrees ofabduction. The range is 50 to 80 degrees of unforcedabduction. Natural posture varies widely, and the harnessmust be adjusted accordingly; no one prescription fits allinfants. The baby’s posture often normalizes within thefirst few weeks of treatment, and the harness is adjustedto accommodate such action.
Upon application of the harness, the parents are in-structed how to care for and position their baby and aregiven an advice sheet (see Appendix in the data supple-
Figure 1. Baby in a Pavlik harness.
musculoskeletal disorders neonatal hip dysplasia
NeoReviews Vol.11 No.7 July 2010 e351 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

ment). Weekly visits in the first 2 weeks are usual andsubsequently in 2 weeks to coincide with the secondultrasonographic examination after 1 month of treat-ment. Improvement in the stability and morphology ofthe hip is expected at this time. The harness is changedby the physiotherapist every 2 weeks, and the baby canbe bathed at that time. The parents must not remove oradjust the harness, which must be worn 24 hours a day.Support is given and treatment rarely causes significantparental distress after the initial fitting. Parents accept theneed for treatment, and noncompliance rarely is a prob-lem. Standard duration of treatment is 12 weeks but maybe less or more, depending on when ultrasonographicexamination shows that the acetabulum is normal.
Great care must be taken not to force the hip intoabduction, which may reduce the blood supply to thefemoral head, (14) causing avascular necrosis that hasbeen reported in 5% of babies treated in Pavlik harnesses(15) and 30% of those treated in plaster spica. (16)Expert application of the device should minimize suchrisk. We have had one case of avascular necrosis out of223 babies with radiologic follow-up available whom wehave treated in a harness at our center. This occurred in ababy who had severe congenital scoliosis in whom agentle symmetric abduction was difficult to achieve. Thehigher incidence of avascular necrosis in other centersmay be due to treatment beginning after 6 weeks of age,when adductor contractures can make abduction diffi-cult. (17) Another complication of screening and treat-ment is parental anxiety, (18) which usually can bemanaged by simple reassurance. Maternal depression andlack of bonding with the baby have been noted in a fewcases, but a causal link with treatment is uncertain. Lackof parental compliance can lead to treatment failure,although this has happened only once in our experience.
Alternative SplintsOther splints, such as the von Rosen (also known as theMalmo) splint, are used effectively in many centers. (19)These more rigid splints have decreased in popularity inrecent years, perhaps because of the perceived risk ofavascular necrosis or the perception by parents that thebaby may be uncomfortable in them. A properly appliedrigid splint, however, is extremely effective, and our useof the Pavlik harness is not a criticism of other types ofdevices; the expertise of the person applying the device ismore important than which device is used. The personapplying the device must be able to examine a hip anddetermine whether it is in or out of joint.
Treatment should begin no later than 6 weeks of age.We do treat babies from other centers whose referral may
be delayed up to the age of 12 to 14 weeks, but this isregarded as suboptimal. Our experience is that treatmentbefore 8 weeks of age leads to a normal radiograph at 1year in 97% of hips and mild abnormality in 3%, but anormal radiograph can be expected in only 66% of thosein whom treatment began at more than 8 weeks of age.Babies presenting later with DDH can be treated withthe Pavlik harness or similar splint up to the age of about16 weeks. Beyond this age, it is likely that closed reduc-tion, possibly with adductor tenotomy, and serial plastercasting will be necessary. Surgery with iliac osteotomy tostabilize the hip may be needed in children presentingafter 1 year of age, but this is a failure of the screeningprocess because a normal hip cannot be achieved.
Ultrasonography: ReviewBackground
Ultrasonography of the neonatal hip has been practicedfor 40 years but is still surrounded by controversy in threeprimary areas: which classification system to use, whichhips to treat, and the role of ultrasonography in screen-ing. Of note, in the infancy of ultrasonography duringthe 1970s, images were poor quality. They were static,not real-time, and had no cine-recall facility. It was usualto display the image in almost black and white contrastwithout much soft-tissue detail. Images were printed onfilm or paper. Unfortunately, many attitudes towardultrasonography have remained unchanged since thattime.
Static ImagingGraf founded the view that the static images producedshould be classified predominantly on angles: the anglethe bony roof of the acetabulum makes with the baselineor lateral side wall of the pelvis (alpha or bony angle) andthe angle the cartilaginous roof of the pelvis makes withthe baseline (beta or cartilaginous angle). (8) A classifi-cation was produced that, in summary, classified hips asGraf type 1 (normal: alpha �60 degrees), Graf type 2a(immature: alpha 50 to 60 degrees), Graf type 2c (defi-cient: alpha 43 to 50 degrees), Graf type 3 (subluxing:alpha �43 degrees), and Graf type 4 (dislocated orinterposed labrum: alpha �43 degrees). Morin and asso-ciates (20) believed that the percentage of the femoralhead contained within the bony acetabulum was a bettercriterion. This was calculated by drawing the baseline (aninferior continuation of the lateral wall of the pelvisthrough the femoral head) and measuring what propor-tion of the diameter of the head lay medial to this line.More than 58% was considered normal, 33% to 58%equivocal, and less than 33% abnormal. A normal ultra-
musculoskeletal disorders neonatal hip dysplasia
e352 NeoReviews Vol.11 No.7 July 2010 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

sonographic image with the landmarks labeled is shownin Figure 2 and without labeling in Figure 3A. Figure 3Bshows the same image with the bony (alpha) angle ofGraf measured. Figure 3C shows the same image withpercent femoral head coverage measured.
Dynamic ImagingWith universal availability of real-time ultrasonographyin the late 1980s, the technique of dynamic ultrasonog-raphy was introduced. (21) It was suggested that the hipshould be flexed to 90 degrees and posterior pressureapplied to the knee to determine whether there was laxityor instability, with posterior displacement of the femoralhead in the acetabulum being detected during transversescanning. Interobserver agreement for dynamic tests,however, is poor, with treatment recommended by radi-ologists varying from 7.4% to 23.9% of babies in onestudy. (22) Interobserver agreement is better, althoughonly moderate, for static methods, (23)(24) and use ofthe Graf classification leads to a large number of indeter-minate results that need follow-up. (25) Throughout thepast 2 decades, while this debate has continued, threepossible approaches were available: classify by angles(Graf method), percentage acetabular cover (Harcke/
Morin method), and dynamic testing. In most centers,one or more of these classifications was used to reportfindings on hip ultrasonographic examinations per-formed by sonographers or radiologists to help ortho-paedic surgeons to decide on management.
Which Hips to Treat?The second controversy of which hips to treat is evi-denced by the considerable variation in practice, withtreatment rates ranging from 2 to more than 20 per1,000 births. Some orthopaedic surgeons took the viewthat only clinically unstable hips (approximately 2 per1,000 births) needed to be treated and that ultrasonog-raphy added little. There was disagreement as to whetherdysplastic but stable hips should be treated. One of a fewrandomized, prospective trials suggested that althoughultrasonographic morphology improved more quickly intreated babies, the outcome, as assessed by plain radio-graphs at 3 months and 24 months, was the same as foruntreated babies. (26) In a similar study of 68 babies whohad “mildly unstable” hips, five failed to improve andrequired treatment at 4 to 5 months of age. (27) The fearwas that treatment of indeterminate hips could be doingmore harm than good because of the complication ofavascular necrosis, (28) and a trend developed to try toreduce rates of treatment as much as possible. (29) Thispolicy might have been harmful by omission becauseindeterminate hips with only mild instability were nottreated when, in retrospect, treatment may have beenbeneficial. Some of these children may present withdislocation later in childhood (30) or with prematureosteoarthritis in adulthood that requires hip replace-ment. The latter may be much more frequent thanhitherto recognized, as evidenced by a recent study fromNorway involving collection of national statistics on hipinstability at birth and arthroplasty. (31) In this report,92% of patients undergoing hip arthroplasty ages 12 to36 years because of prior hip dysplasia were recorded ashaving clinically stable hips at birth. This may be the firstproof of the iceberg under the surface, that is, the un-known numbers of babies who have clinically undetect-able hip dysplasia and develop adult disability.
Consensus on Role of Ultrasonography inScreening
The controversy surrounding the role of ultrasonogra-phy in screening appears to have been settled to someextent, with the consensus going against whole-population ultrasonographic screening. Such screeninghas been successful and cost effective in small areas, but itdepends on local expertise and enthusiasm, which may
Figure 2. Normal hip ultrasonographic image. AM�acetabular margin, AR�acetabular roof, GT�greater trochan-ter, JC�joint capsule, Lab�labrum, LMI�lateral margin ofilium, OFS�ossified femoral shaft, UAC�unossified articularcartilage, UFH�unossified femoral head, YC�Y-cartilage.
musculoskeletal disorders neonatal hip dysplasia
NeoReviews Vol.11 No.7 July 2010 e353 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

Figure 3. A. Normal hip ultrasonographic image. B. Normal bony (alpha) angle. C. Normal percent femoral head coverage ofHarke/Morin (%FHC).
musculoskeletal disorders neonatal hip dysplasia
e354 NeoReviews Vol.11 No.7 July 2010 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

not be widely available, (32) and it has not been generallyaccepted into national screening programs, (33) with theexception of a few countries, including Germany. Thismay be partly attributed to the only moderate inter-observer agreement in performing and interpreting ultra-sonographic scans, (34) which could incur costs inwhole-population screening due to false-positive andfalse-negative diagnoses.
Germany and Austria have instituted whole-population ultrasonographic screening. However,problems, including 8% patient failure in obtaining ultra-sonography and 12% false-negative rates for ultrasono-graphic examination, result in a rate of operation forDDH of 0.26 per 1,000 live births in Germany. (35) Inthe United Kingdom, clinical screening was reported tobe associated with an incidence of first operation forDDH of 0.78 per 1,000 births. (10) It is widely consid-ered that clinical screening with ultrasonography beingperformed only to help manage clinically detected casesis the most cost-effective option. (28)(36) The use ofultrasonography in clinically detected cases can reducethe calculated treatment rate from 8.5 to 4.9 per 1,000births. (37) The cost for each additional case detected bywhole-population ultrasonography has been estimated as£0.3m in the United Kingdom. (28) A systematic litera-ture review for the United States Preventive ServicesTask Force reported simply, “Screening with clinicalexamination or ultrasound can identify newborns at in-creased risk for DDH, but because of the high rate of
spontaneous resolution of neonatal hip instability anddysplasia and the lack of evidence of the effectiveness ofintervention on functional outcomes, the net benefits ofscreening are not clear.” (38)
Ultrasonography: Personal ViewMethodology Concerns
Our own experience has led us to three conclusions thatalter how we assess hips ultrasonographically. First, webelieve that none of the Graf, Morin/Harke, or anterior-dynamic methods described previously is adequate inisolation. Second, we believe that a number of additionalstatic ultrasonographic signs are helpful. Third, we be-lieve that observation of the hip during spontaneousmovement of the baby is much more valuable than theapplied stress test.
Experience has shown that some babies who haveGraf type 1 or 2 hips have needed treatment for deterio-ration or failure to mature on observation, indicating alack of sensitivity of this test in our view. The largenumber of babies who have percentage femoral headcover in the indeterminate range shows that this test lacksspecificity. We have difficulty assessing whether the de-gree of movement of the hip posteriorly during anteriordynamic testing is a reliable arbiter of the need fortreatment; it depends on how much force is used and is
Figure 4. Notched acetabular margin (arrow).
Figure 5. Flattened femoral head, with loss of concavity ofthe acetabular roof.
musculoskeletal disorders neonatal hip dysplasia
NeoReviews Vol.11 No.7 July 2010 e355 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

difficult to measure, even with the benefit of cine recallloops. One study showed that up to 6.8 mm of move-ment can be considered normal in neonates youngerthan 48 hours of age. (39) Examiners frequently use toomuch force, and training and experience are essential toprevent this. (40) We use only the amount of force thatcan be achieved easily by use of the little finger alone. Thehip may be lax in the first few weeks, only to stabilizelater. If the cartilaginous rim at the posterior margin isdeformed by gentle stress when the baby is 6 or moreweeks old, we believe the hip should be treated. Hips alsocan be stressed in the superior direction, but this isdifficult to standardize because the pelvis cannot be fixedeasily.
Static Ultrasonographic Warning SignsSeveral static ultrasonographic warning signs may beassociated with instability and are invaluable. These maybe seen during a hip ultrasonographic examination inwhich the subluxation itself is not observed and are:
1. The notched margin. A hip may be normal and
appear stable but a notch be appreciated at the superiormargin in the sagittal plane. This indicates that the hip is,or has been, unstable. The notch presumably is due topressure of the upriding femoral head on the margin that,due to repeated deformation, prevents ossification. Wenoted this sign independently, and only after severalyears of using it, discovered that it had been describedseveral years previously. (41) It is a warning sign that anotherwise normal hip may be unstable (Fig. 4).
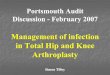
2. Loss of concavity of the acetabulum. This is associ-ated with flattening of the femoral head, (42) so insteadof the concentric hemispheres of the ball-and-socketjoint allowing rotation without movement of the centers,part of the articulation (usually the superior part) be-comes planar and allows superolateral sliding of the headin the acetabulum. This is believed to be due to posturalmolding of the joint in utero, when restriction of thefetus has occurred in the later stages of gestation. It isparticularly evident in extended breech babies (Fig. 5).
3. Thickening and increased echogenicity of the la-brum and joint capsule. This is likely to be due todeformation and stretching, respectively, during sublux-ation of the joint (Fig. 6).
4. The ultrasonographic vacuum phenomenon. Bub-bles of vapor can form in synovial fluid when pressure isreduced below atmospheric due to rotation of adjacentincongruous articular surfaces. Bubbles appear very
Figure 6. Markedly thickened acetabular labrum (arrows).
Figure 7. Ultrasonographic vacuum phenomenon with gasbubbles in synovial fluid (arrows).
musculoskeletal disorders neonatal hip dysplasia
e356 NeoReviews Vol.11 No.7 July 2010 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

bright and can be seen between the striated low echoge-nicity of the femoral head and the homogenous lowechogenicity of the acetabular cartilage (Fig. 7). Fluidwith bright bubbles “sloshing” around in the joint dur-
ing movement of the baby indicates that the hip is actinglike a peristaltic pump because of incongruity (see videoclip 1 in the data supplement). This is an indirect sign ofthe flattening of the articular surfaces.
Figure 8. A. Abnormal hip ultrasonographic finding. Note the deformed labrum (arrow). B. Abnormal bony alpha angle. C. Abnormalpercent femoral head coverage.
musculoskeletal disorders neonatal hip dysplasia
NeoReviews Vol.11 No.7 July 2010 e357 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

Observation of Instability Without StressTesting
Finally, we believe that a formal stress test rarely isneeded; we simply watch the hip with the ultrasono-graphic probe in both sagittal and coronal planes whilethe baby wriggles spontaneously. If there is movement ofthe femoral head with any deformity of the cartilaginousrim either posteriorly or superiorly, the hip should beconsidered unstable (see video clip 2 in the data supple-ment) and treated by the age of 6 weeks at the latestunless it becomes completely stable and morphologically
normal by that age. This has the advantage of observinginstability in physiologic conditions and should be morereliable than an applied test in which the force, direction,and pelvic stabilization vary.
Standard Procedure for UltrasonographicExaminationOur standard procedure is as follows:
1. Perform ultrasonography without reading the clin-ical information to prevent bias.
Figure 9. A. Equivocal hip ultrasonographic finding. B. Equivocal bony alpha angle. C. Percent femoral head coverage within normalrange.
musculoskeletal disorders neonatal hip dysplasia
e358 NeoReviews Vol.11 No.7 July 2010 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

2. Examine the baby in the true lateral position in animmobilizing foam pad.
3. Always starting with the right hip, take a staticimage in the standard plane and measure the alpha angleand percent acetabular cover, which are useful for assess-ing progress rather than for deciding whether the hipneeds treatment.
4. Observe the hip during wriggling both in thesagittal and transverse planes to detect spontaneous in-stability (defined simply as deformation of the cartilagi-nous labrum). If instability is seen, this is recorded as acine clip. If the hip is stable, this is recorded in text on theimage.
5. Look for and record any of the static signs.6. If the hip is not completely normal morphologically
(alpha angle �70 degrees) and no spontaneous instabil-
ity has been detected, perform an anterior dynamic stresstest in the transverse plane (see video clip 3 in the datasupplement) and a longitudinal stress test in the coronalplane (see video clip 4 in the data supplement).
7. Repeat steps 3 to 5 for the left hip.A normal hip has an alpha angle of more than 70
degrees and percent acetabular cover of more than 55%,is stable, and has no static warning signs. If the physio-therapist agrees the hip appears normal, the baby can bedischarged (Fig. 3). An abnormal hip has instabilitydetected on spontaneous wriggling of the baby. If un-equivocal, the baby is treated at the first visit if 2 or moreweeks old (Fig. 8). An equivocal hip has no spontaneousinstability but is not normal morphologically or has staticwarning signs or is lax or unstable on stress testing.Parents are advised to lay these babies prone (whenawake), and they are reviewed at the age of 6 weeks. If thehip is not completely normal at 6 weeks, the baby shouldbe treated (Fig. 9).
The duration of treatment depends on age and paren-tal compliance. If treatment begins at 3 weeks of age,6 weeks of treatment may suffice. Older babies mayrequire up to 16 weeks in the harness. Optimally, weprefer the hips to be completely normal on ultrasonog-raphy before removing the harness, but babies who areolder at the beginning of treatment may not achieve thismilestone.
Joint ViewWe believe that there is potential for miscommunicationbetween the person performing the ultrasonographicobservation and assigning a classification based on angle,percentage femoral head cover, or stability and the per-son deciding on treatment, whose perception of thisclassification may be different. The ideal approach wouldbe if the sonographer simply decided the hip fell into oneof three categories: normal (no need to review), equivo-cal (seek clinical opinion and review after an interval),and abnormal (treat).
It was agreed in our institution that the hip assessmentwould be performed primarily by the specialist physio-therapist. If the result is normal, she discharges the babywithout further assessment. The physiotherapist filterscases and refers for hip ultrasonography only those babiesin whom she suspects hip instability. The hip ultrasono-graphic examinations are performed almost exclusivelyby one radiologist. If both physiotherapist and radiolo-gist agreed the hips are normal, the baby is discharged. Ifboth agree that a hip is unstable, the baby is treatedwithout delay. If the hip findings are equivocal, we
Table 1. Summary of Evaluationand Treatment ProcessNeonatal Ward
All babies who have risk factors or molding and thosewhom the junior medical staff feel concern for anyreason are referred to the specialist physiotherapist.The specialist physiotherapist also examines as manybabies without risk factors as is possible, given timerestraints.
0 to 3 Weeks of Age
First assessment by specialist physiotherapist with 3possible outcomes
● Normal clinical examination: Discharge with nofurther follow-up
● Molded, limited abduction or hip laxity: Positioningadvice and review at 6 weeks of age in the combinedclinic (expert physiotherapist and radiologist)
● Unstable hip or hips: Review in next combined clinic(at age of 3 to 6 weeks)
3 to 6 Weeks of Age
Assessment in combined physiotherapist andultrasonography clinic
● If clinically and ultrasonographically unstable,commence treatment immediately
● If 3 weeks of age and equivocal clinically orultrasonographically, review again in combined clinicat age of 6 weeks
● If 6 weeks of age and still equivocal clinically orultrasonographically, commence treatment
Follow-up
Radiograph at 1 year and magnetic resonance imagingat 5 years for all treated babies and those who wereclassified initially as equivocal
musculoskeletal disorders neonatal hip dysplasia
NeoReviews Vol.11 No.7 July 2010 e359 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

suggest that the parents position the baby as recom-mended by the physiotherapist until the age of 6 weeks.A second clinical and ultrasonography examination isperformed at that time, and unless the both hips arecompletely normal, the baby is treated. We use thecut-off of 6 weeks because, in our experience, treatmentbefore 8 weeks of age leads to a normal hip radiograph at1 year in 97% cases. Such findings drop to 66% if treat-ment is begun after 8 weeks.
In many cases, equivocal hips improve because theparents comply with the physiotherapist’s positioningadvice; almost always the hips are normal at the secondexamination at 6 weeks of age. If the parent does notcomply with positioning advice, the radiologist may seedeterioration or lack of improvement, and almost invari-ably the physiotherapist concurs that the baby continuesto lie to one side or the affected hip remains tight. Suchconcurrence is to be expected because the ultrasono-graphic and clinical assessments simply look at the samephenomenon from different perspectives. A summary ofthe evaluation and treatment process is provided in Table1, and results of the screening program for 2008 to 2009are provided in Table 2.
References1. Furnes O, Lie SA, Espehaug B, Vollset SE, Engesaeter LB,Havelin LI. Hip disease and the prognosis of total hip replacements.A review of 53698 primary total hip replacements reported to theNorwegian Arthroplasty Register 1987–99. J Bone Joint Surg Br.2000;83:579–5862. Hinderaker T, Daltveit AK, Irgens LM, Uden A, Reikeras O.The impact of intrauterine factors in neonatal hip instability: ananalysis of 1,059,479 children in Norway. Acta Orthop Scand.1994;65:239–2423. Bache CE, Clegg J, Herron M. Risk factors for developmentaldysplasia of the hip: ultrasonographic findings in the neonatalperiod. J Pediatr Orthop B. 2002;11:212–2184. Ortalani M. Un segno poco noto e sua importanza perla diag-nosi precoce di prelussazione congenita dell’anca. Pediatria. 1937;45:1295. von Rosen S. Early diagnosis and treatment of congenital dislo-cation of the hip joint. Acta Orthop Scand. 1956;26:1366. Barlow TG. Early diagnosis and treatment of congenital dislo-cation of the hip in the newborn. J Bone Joint Surg. 1962:44-B:292–3017. Jones DA. Principles of screening and congenital dislocation ofthe hip. Ann R Coll Surg Engl. 1994;76:245–2508. Graf R. The diagnosis of congenital hip-joint dislocation by theultrasonic Combound treatment. Arch Orthop Trauma Surg. 1980;97:117–1339. Gilbert R, Salanti G, Harden M, See S. Infant sleeping positionand the sudden infant death syndrome: systematic review of obser-vational studies and historical review of recommendations from1940 to 2002. Int J Epidemiol. 2005;34:874–88710. Godward S, Dezateux C. Surgery for congenital dislocation ofthe hip in the UK as a measure of outcome of screening. MRCWorking Party on Congenital Dislocation of the Hip. Med ResCouncil Lancet. 1998;351:1149–115211. Chapple CC, Davidson DT. A study of the relationship be-tween fetal position and certain congenital deformities. J Pediatr.1941;18:483–49312. Lloyd Roberts GC, Pilcher MF. Structural idiopathic scoliosisin infancy. A study of the natural history of 100 patients. J Bone JointSurg (Br). 1965;47:520–52313. Macnicol MF. The early management of congenital dislocationof the hip. Curr Orthop. 1992;6:245–25114. Bearcroft PW, Berman LH, Robinson AH, Butler GJ. Vascu-larity of the neonatal femoral head: in vivo demonstration withpower Doppler US. Radiology. 1996;200:209–21115. Kalamachi A, MacEwen GD. Avascular necrosis followingtreatment of congenital dislocation of the hip. J Bone Joint Surg(Am). 1980;62:876–88816. Salter RB, Kostuik J, Dallas S. Avascular necrosis of the femoralhead as a complication of treatment for congenital dislocation of thehip in young children: a clinical and experimental investigation.Can J Surg. 1969;12:44–6117. Tschauner C, Klapsch W, Graf R. The effect of ultrasonogra-phy screening of hips in newborn infants on femur head necrosisand the rate of surgical interventions. Orthopade. 1993;22:268–27618. Gardner F, Dezateux C, Elbourne D, Gray A, King A, QuinnA. The hip trial: psychosocial consequences for mothers of usingultrasound to manage infants with developmental hip dysplasia.Arch Dis Child Fetal Neonatal Ed. 2005;90:F17–F24
Table 2. Results of ScreeningProgram 2008 to 2009Birth Rate: 7,000 per year (total 14,000)Percent examined by expert physiotherapists: 33%Percent referred for ultrasonographic examination:
2.3%Outcome (normal radiograph at 1 year): 97% of
treated babiesApproximate cost of screening program: £100,000/yearNumber of known missed hips: 2 (0.14/1,000) (neither
examined by expert physiotherapist)
American Board of Pediatrics Neonatal-PerinatalMedicine Content Specifications• Know the neonatal complications of
abnormal presentations (breech, shoulderdystocia, etc).
• Recognize the clinical features and knowhow to diagnose and manage congenitalanomalies of the lower extremities, such as metatarsusadductus, talipes equinovarus, syndactyly, polydactyly, limbreduction.
musculoskeletal disorders neonatal hip dysplasia
e360 NeoReviews Vol.11 No.7 July 2010 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

19. Wilkinson AG, Sherlock DA, Murray GD. The efficacy of thePavlik harness, the Craig splint and the von Rosen splint in themanagement of neonatal dysplasia of the hip. A comparative study.J Bone Joint Surg. 2002;84-B:716–71920. Morin C, Harke HT, MacEwen G. The infant hip: real timeUS assessment of acetabular development. Radiology. 1985;157:673–67721. Andersson JE, Funnemark P-O. Neonatal hip instability:screening with anterior-dynamic ultrasound method. J Pediatr Or-thop. 1995;15:322–32422. Kaijser M, Larsson J, Rosenberg L, Josephson T. Anteriordynamic ultrasound of the infant hip: evaluation of investigatordependence. Acta Radiol. 2009;50:690–69523. Rosendahl K, Toma P. Ultrasound in the diagnosis of devel-opmental dysplasia of the hip in newborns. The European ap-proach. A review of methods, accuracy and clinical validity. EurRadiol. 2007;17:1960–196724. Roposch A, Graf R, Wright JG. Determining the reliability ofthe Graf classification for hip dysplasia. Clin Orthop Relat Res.2006;447:119–124.25. Finnbogason T, Jorulf H, Soderman E, Rehnberg L. Anteriordynamic ultrasound and Graf’s examination in neonatal hip insta-bility. Acta Radiol. 2008;49:204–21126. Wood MK, Conboy V, Benson MK. Does early treatment byabduction splintage improve the development of dysplastic butstable neonatal hips? J Pediatr Orthop. 2000;2:302–30527. Holen KJ, Tegnander A, Eik-Nes SH, Terjesen T. The use ofultrasound in determining the initiation of treatment in instabilityof the hip in neonates. J Bone Joint Surg Br. 1999;81:846–85128. Dezateux C, Brown J, Arthur R, Karnon J, Parnaby A. Perfor-mance, treatment pathways, and effects of alternative policy optionsfor screening for developmental dysplasia of the hip in the UnitedKingdom. Arch Dis Child. 2003;88:753–75929. Sampath JS, Deakin S, Paton RW. Splintage in developmentaldysplasia of the hip: how low can we go? J Pediatr Orthop. 2003;23:352–35530. Gwynne Jones DP, Dunbar JD, Theis JC. Late presentingdislocation of sonographically stable hips. J Pediatr Orthop B. 2006;15:257–26131. Engesaeter IØ, Lie SA, Lehmann TG, Furnes O, Vollset SE,
Engesaeter LB. Neonatal hip instability and risk of total hip replace-ment in young adulthood: follow-up of 2,218,596 newborns fromthe Medical Birth Registry of Norway in the Norwegian Arthro-plasty Register. Acta Orthop. 2008;79:321–32632. Clegg J, Bache CE, Raut VV. Financial justification for routineultrasound screening of the neonatal hip. J Bone Joint Surg Br.1999;81:852–85733. Holen KJ, Tegander A, Bredland T, et al. Universal or selectivescreening of the neonatal hip using ultrasound? J Bone Joint Surg.2002;84B:886–89034. Rosendahl K, Aslaksen A, Lie RT, Markestad T. Reliability ofultrasound in the early diagnosis of developmental dysplasia of thehip. Pediatr Radiol. 1995;25:219–22435. Ihme N, Altenhofen L, von Kries R, Niethard FU. Hip ultra-sound screening in Germany. Results and comparison with otherscreening procedures. Orthopade (German). 2008;37:541–546,548–54936. Gray A, Elbourne D, Dezateux C, King A, Quinn A, GardnerF. Economic evaluation of ultrasonography in the diagnosis andmanagement of developmental hip dysplasia in the United King-dom and Ireland. J Bone Joint Surg Am. 2005;87:2472–247937. Finnbogason T, Jorulf H, Soderman E, Rehnberg L. Neonatalhip instability: a prospective comparison of clinical examination andanterior dynamic ultrasound. Acta Radiol. 2008;49:212–21938. Shipman SA, Helfand M, Moyer VA, Yawn BP. Screening fordevelopmental dysplasia of the hip: a systematic literature reviewfor the US Preventive Services Task Force. Pediatrics. 2006;117:e557–e57639. Andersson JE. Neonatal hip instability: normal values for phys-iological movement of the femoral head determined by an anterior-dynamic ultrasound method. J Pediatr Orthop. 1995;15:736–74040. Chow YW, Turner I, Kernohan WG, Mollan RA. Measure-ment of the forces and movements involved in neonatal hip testing.Med Eng Phys. 1994;16:181–18741. Portinaro NM, Murray D, Benson MK. Acetabular notch.J Pediatr Orthop B. 1997;6:48–5142. Wilkinson AG. The significance of flattening of the femoralhead on ultrasound for developmental dysplasia of the hip. PediatrRadiol. 2006;36(suppl 1):78
musculoskeletal disorders neonatal hip dysplasia
NeoReviews Vol.11 No.7 July 2010 e361 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

NeoReviews Quiz
1. Developmental dysplasia of the hip (DDH) is a spectrum of abnormalities that ranges from a minor, self-correcting abnormality to hip dislocation with lifelong disability. Of the following, the primary risk factorfor DDH is:
A. Fetal movement restriction.B. Genetic predisposition.C. Hormonal influence.D. Male sex.E. Preterm gestation.
2. The Barlow maneuver for the diagnosis of DDH includes cradling the pelvis to stabilize the sacrum, flexingthe hip to 90 degrees toward the trunk, and applying gentle posterior pressure along the length of thefemur. Of the following, the most useful sign of DDH on the Barlow maneuver is:
A. Clunking sound within the acetabulum.B. Increased vernix in the inguinal fold.C. Leg extension contralateral to the affected side.D. Sensation of posterior movement and relocation on gentle anterior traction.E. Limited abduction of the hip.
3. Ultrasonographic imaging of the hip is being used increasingly in the diagnosis of DDH and in the selectionof newborns for treatment. Of the following, according to Wilkinson and Wilkinson, the bestultrasonographic measure for the diagnosis of DDH is:
A. Andersson/Funnemark measurement of the posterior displacement of the femoral head in theacetabulum by dynamic scanning.
B. Graf measurement of the alpha-angle between the bony roof of the acetabulum and the baseline.C. Graf measurement of the beta-angle between the cartilaginous roof of the pelvis and the baseline.D. Morin/Harke measurement of the percentage of the femoral head within the bony acetabulum.E. Spontaneous subluxation of the femoral head with deformation of the cartilaginous labrum.
musculoskeletal disorders neonatal hip dysplasia
e362 NeoReviews Vol.11 No.7 July 2010 by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from

DOI: 10.1542/neo.11-7-e349 2010;11;e349-e362 NeoReviews
A. Graham Wilkinson and Sally Wilkinson Neonatal Hip Dysplasia: A New Perspective
& ServicesUpdated Information
s;11/7/e349http://neoreviews.aappublications.org/cgi/content/full/neoreviewincluding high-resolution figures, can be found at:
Supplementary Material
s;11/7/e349/DC1http://neoreviews.aappublications.org/cgi/content/full/neoreviewSupplementary material can be found at:
Permissions & Licensing
http://neoreviews.aappublications.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://neoreviews.aappublications.org/misc/reprints.shtml
Information about ordering reprints can be found online:
by J Michael Coleman on August 19, 2010 http://neoreviews.aappublications.orgDownloaded from