Embed Size (px)
Citation preview

NEONATALANDPEDIATRICTRANSFUSIONMEDICINEDr.LaniLiebermanTransfusionCampDay1FridaySeptember17th,2021

Objectives• Highlightspecialconsiderationswhenorderingbloodproductsforneonatesandchildren
• Cases• PRBC• Platelet
• Wewillnotbediscussing• Useofplasma,cryoprecipitateorfractionatedproducts• Intrauterinetransfusions• Exchangetransfusions• Bloodproductuseincardiacsurgery

Whatproportionofbloodsupplyistransfusedtochildren?
TransfusionMedicine2009;19:315–328
4.2%RBC<18yo
1.7%RBC<12mo

Evidencebasedpediatrictransfusion• Limited• Guidelines
• Extrapolatedfromadultdata• Expertopinion• Auditdata
BJH2016;175:784-828

5thingstoconsiderpriortoorderingatransfusionforaneonateorchild
1. Bloodrecipients:similartoadult• Oncology,hemoglobinopathy,OR,ICU
2. Consent-shouldbeobtainedfromchild’slegalguardian(unlessthechildhascapacitytoconsent)
3. Labreferencerangesaredifferentforchildrenandneonates

Newbornlaboratoryvalues
HEMOGLOBIN:168 (137-201 g/dl) MCV:110 fl/cell (adult levels by 9 weeks)
Transfusion2014;54,627-632Blood1987;70:165-72.Blood1988;72:1651–7.

Pediatricresources&Referenceranges
BloodyEasyCBS–ClinicalGuidehttps://professionaleducation.blood.ca/en/transfusion/guide-clinique/neonatal-and-pediatric-transfusion

5thingstoconsiderpriortoorderingatransfusionforaneonateorchild
1. Bloodrecipients:similartoadult• Oncology,hemoglobinopathy,OR,ICU
2. Consentshouldbeobtainedfromresponsibleadult(unlessthechildhascapacitytoconsent)
3. Labreferencerangesdifferforchildren
4. Bloodproductsshouldalwaysbeorderedbyweight

BloodProductsareorderedbyweight(ml/kg)
Product PediatricDose(ml/kg)
RBC 10-15ml/kg
Platelets 10-15ml/kg
Plasma 10-15ml/kg
Cryoprecipitate* 1-2U/10kg
BJH2016;175,784-828

BloodProductsareorderedbyweight(ml/kg)
Product PediatricDose(ml/kg) TypicalAdultDose
RBC 10-15ml/kg 1Unit≈280-300mL
Platelets 10-15ml/kg 1Unit≈250-350ml
Plasma 10-15ml/kg 3-4Units≈750-1000ml
Cryoprecipitate* 1-2U/10kg AdultPool150-200ml
Cryoprecipitate*• Eachunit=8-15ml• AdultPool=150-200ml• 8-10units+50ccNS
Maximumorderfornon-bleeding• Nomorethanadultdose
BJH2016;175,784-828

5thingstoconsiderpriortoorderingatransfusionforaneonateorchild
1. Bloodrecipients:similartoadult• Oncology,hemoglobinopathy,OR,ICU
2. Consentshouldbeobtainedfromresponsibleadult(unlessthechildhascapacitytoconsent)
3. Labreferencerangesdifferforchildren
4. Bloodproductsshouldalwaysbeorderedbyweight
5. Irradiationguidelines–preventTA-GVHD

IndicationsforirradiationIndicationsNeonatesExchangetransfusion PreviousIUTuntil6monthpost
deliverySmallvolumetopuptransfusion Verylowbirthweightinfants
PreviousintrauterinetransfusionCongenitalsevereTcellimmunedeficiencyComplexcongenitalcardiacabnormalities
Hematology/Oncologyindications=sameasadultrecommendations
http://www.nacblood.caNationalAdvisoryCommittee

REDBLOODCELLTRANSFUSIONS

Case:NeonatalAnemia• 25weekpremature–10daysold• Intubated,NGfed,antibiotics,Grade2IVH• Dailybloodworksinceadmission• Hemoglobinhasbeengradually↓ • 150g/L......80g/L

NeonatalAnemia
Widnessetal.NeoReviews2008;9(11)e520

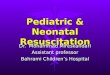
PhlebotomyBloodLossinVeryLowBirthWeight(VLBW)Infants(<1500grams)
16
Cumulative phlebotomy losses typically reach 40-80 ml/kg and, in many infants, will exceed the infant’s blood volume

RBCtransfusionsinELBWinfants• 50-80%ofELBWinfantsreceiveoneormoreRBCTduringhospitalizations
17
Vlalieva et at. J Pediatr 2009; 155 (3): 331-337 Keir et al. Transfusion 2015; 55:1340-6

RBCTransfusion
IncreasedO2supplytobrain
Intraventricularhemorrhage
Necrotizingenterocololitis
Bronchopulmonarydysplasia
Retinopathyofprematurity
Decreased risk of apnea ofprematurity frequency &severity
Christensenetal.JMaternFetalNeonatalMedicine.2013;26(s2):60-63MohamedA,ShahPS.Pediatrics2012;129(3):529-540GhirardelloSetal.AmJPerinatology.2017;34(1):88-95SlidsborgCetal.Ophthamology.2016;123(4):796-803.

NeonatalpediatricRBCtransfusiontrials
19
PINT
Kirpalani et al. J Peds. 2006; 149:301-7 Bell et al. Pediatrics 2005; 115: 1685-1691
IOWA/ BELL
ShorttermNostatisticallysignificantdifference
indeathormorbidity

IowaTrial:SevereIVHandCystic(PeriventricularLeukomalacia)PVL
20

LongTermFollowupData-Cognitive
PINT Bell(Iowa)
Ageatfollowup 18-21months 8-15years
Cognitivetesting BetterinLIBgroup BetterinRESgroup
Whyteetal.Pediatrics2009;123(1):207-213McCoyetal.ChildNeuropsychology,2011;17(4):347–367
Conflictingresults–leadstovariabilityinpractice

22

MethodologyETTNO
Liberalthreshold=492
1013neonates
Restrictivethreshold=521
Triggervariesby:Postnatalage&Criticalstateofhealth
DeathorNeurologicalimpairmentat24months
SecondaryoutcomesOthermeasuresofcognitivedeficitMeasuresofgrowth@D/C&FU
LengthofstayTimefrombirthtodcrespiratory
support,respstimulantgavagefeedsComplicationsofprematurity
RBC20ml/kgLeucocytereducedExclusion
1. Major anomalies (cyanotic heart disease, chromosomal anomalies, syndromes) or malformations needing surgery
2. Lack of viability/comfort car
3. First neonate of multiples pregnancy
InclusionBWt400-999gGA<29wksPostnatal:

Transfusionthresholds(ETTNO)
● Criticalhealth● Exceptionstoguidelineswerepermitted
24

MethodologyTOP
Liberalthreshold
1824neonates
Restrictivethreshold
Transfusionthresholds:
postnatalage&respiratorysupport
Death+/-Neurodevelopmentalimpairmentat22-26months
SecondaryoutcomesOthermeasuresofcognitivedeficit
MeasuresofgrowthSurvivalwithoutcomplicationsof
prematurityNumberofRBCtxns
AdministrationofRBCasperprotocolLengthofstay
RBC15ml/kg
Exclusion 1. Cyanotic heart disease 2. Received IUT 3. Lack of viability 4. Parent with hgbopathy or 5. congenital anemia 6. RBCtxn within 6 hours of
life 7. Twin- twin transfusion 8. Isoimmune hemolytic
disease 9. Concerns re: follow up 10. RBC txn within 6 hours of
life 11. Congenital condition
InclusionBWt<1000g
GA22-29weeksPostnatal:<48
hours

Transfusionthresholds(TOP)
26

Results:Deathorneurocognitivedeficits27
ETTNO
TOPS
NodifferenceDeath
NeurodevelopmentalImpairment
Fewertransfusions

Results28
TOPS
ETTNO
P<0.001
Weeklymedianpre-transfusionHctwas3%higherinliberalgroup
Pre-transfusionmeanHgbdifferentby1.9g/dL
Fewertransfusions

NeonatalRBCthresholdsBottomline• NodifferenceincognitiveoutcomeinneonatesreceivingRBCTinrestrictiveorliberalgroup
• Decreasedtransfusionsforneonatesinrestrictivegroup
Age of neonate
Respiratory Support
No respiratory support
Week 1 110 g/L 100 g/L
Week 2 100 g/L 85 g/L
Week 3 85 g/L 70 g/L
NICURBCTransfusionThreshold(TOPS)

RBCTRANSFUSIONSINOLDERCHILD


TRIPICU
Lowthreshold
Hemoglobin<70g/L
637PICU
Highthreshold
Hemoglobin<95g/L
Nodifferenceinprimary(multiorgandysfunction)Orsecondaryoutcomes44%fewertransfusions
NEJM2007;356:1609-19

RBCThresholdGuidelinesforChildrenPediatricPatienttype Threshold EvidencegradePICU(stable,non-cyanotic) 70g/L 1BOncology 70g/L(typicalpractice)
Insufficientliterature2C
Perioperativenon-cardiacsurgery(stable,non-bleeding)
70g/L 1C
Chronicanemia(DiamondBlackfananemia)
80g/LConsensusbased
2C
Thefollowingshouldbeconsideredforchildrenundergoingsurgerywithsignificantriskofbleeding:
Tranexamicacid(1B)Redcellsalvage(2C)
*Hemoglobinopathies
BJH2016;175:784-828

Case:Pediatricanemia• 22montholdhealthyboy• Symptoms
• Pale• Eatingpaper• Otherwiseactiveandenergetic
• Diethistory–drinks48ozofhomomilk/day;pickyeater• PE:Patientalert,interactiveandchasingbrotherinER,VSS• Hemoglobin=52g/L;MCV=62

Whatistheetiologyofthemicrocyticanemia?
• Thalassemia• Anemiaofchronicdisease• Irondeficiency• Leadpoisoning• Sideroblasticanemia
TAILS

Irondeficiencyanemia(IDA)Who?3.5-11%ofCanadianchildren-COMMONWhy?Multifactorial• Increaseneedsduetorapidgrowth• Inadequateintakeofironrichfoods• MalabsorptionOutcome• Impairsphysicalfunctioning,infantgrowth&developmentandimmunefunction
• ClearassociationbetweenIDAandimpairedneurocognitivedevelopment
Preventionandtreatmentareessential
Abdullah,2011,CanadianPediatricSociety

Howdowetreatit?• Oraliron
• 3-6mg/kg/dayELEMENTALiron• Jinexpensive• L10%absorption,poorcomplianceduetoGIsideeffects
• IViron• Failureoforalirontherapy• Ironintolerance• Needforquickrecovery• Ironsucrose(venofer)=7mg/kg(max300mgdose)• Safebut$$
• PRBCTransfusion–shouldnotbeusedinstablepatient
NEJM2015;372(19):1832-43.

NEONATALPLATELETTRANSFUSIONS

Meds
Cause
AgePrematureOrterm
Bleeding
Thrombocytopenia:Factorstoconsider
Procedure

NeonatalThrombocytopeniaPrematureinfants• Thrombocytopeniaoccursfrequently
• 73%<1000g
• Bleedingiscommon• 30%willdevelopintraventricularhemorrhage(IVH)• Leadingcauseofdeath&disability
• Becauseofincreasedrisk,neonatologistshavebeenliberalwithrespecttoplatelettransfusionthresholds
Pediatrics2009;124:e826–e834

Curleyetal.NEJM2018;380(3):242-251

PLANET2:Methodology
Lowthreshold
Platelet<25x109/L
634neonates<34wkGA
Highthreshold
Platelet<50x109/L
HeadUS<6h
NoIVH
Bleedingassessmentdailyx14d
Headultrasoundweekly
BleedingorDeathat28d
Secondaryoutcomes• Survivalafterbleedingepisode
ProportionsurvivingDChome• Rate/timingofbleeding
• #plateletunitsused• Timetodischarge
• Adverseeventstodischarge• Neurodevelopmentupto2yrs
Curleyetal.NEJM2018;380(3):242-251

PLANET2:Results
Outcome N=331(%) N=329 Oddsratioorhazardratio(95%CI)
Deathtoday28(N,%) 33/330(10) 48/326(15) OR=1.57(0.95-2.55)
Newmajorbleedingepisode(N,%)
35/330(11) 45/328(14) HR1.32(1.0-1.74)
Adverseevents 92in74infants(22%)
94in81infants(25%)
OR1.1495%CI(0.78-1.67)
Atleastoneplatelettxn(N,%)
177/331(53) 296/328(90) HR2.75(2.36-3.21)
Lowthreshold
Platelet<25x109/L
634neonates<34wkGA
Highthreshold
Platelet<50x109/L
Curleyetal.NEJM2018;380(3):242-251

Overallconclusions
● Moredeathsandmajorbleedingoccurredwhenahigherprophylacticplateletcountwasused
Bottomline➢ Inneonates,aprophylacticthresholdof25x109/Lshouldbe
usedpriortotransfusingplatelets

ProposedNICUPlateletTransfusionThresholds
Clinicalstatus Plateletthreshold GradeComment
Majorbleedingorrequiringmajorsurgery(e.g.neurosurgery)
<100x109/L NoRCTinprems
Bleeding,currentcoagulopathy,sx,
exchangetransfusion
<50x109/L
Nobleeding(includingNAITifnobleedingand
FHxofICH)
<30x109/L Grade2C
BJH2013;160:421–433BJH2019;185(3):549-562,
SpecialconsiderationsforNAIT–neonatalalloimmunethrombocytopenia

PLATELETTRANSFUSIONSFORCHILDREN

Pediatricplatelettransfusions• Whoreceivesplatelettransfusions?
• CriticallyillinthePICU,Hematology/oncology,Stemcelltransplant,cardiacsurgery
• Systematicreviewassessedeffectofplatelettransfusionsonplateletcountincrement,bleedingandmorality(only1study)• Prospectivecohort(N=138)foundnodifferenceinmortalitybetweentransfusedandnon-transfusedcriticallyillchildren
• Oncologyandproceduralrecommendations• Basedonadultstudies• Expertopinion
IndianJournalofCriticalCareMedicine,2008;12:102-108NEJM1997;337:1870–1875JCO2001;19:1519-1538http://www.c17.ca

Suggestedplateletthresholdsforplatelettransfusioninchildren
Plateletthreshold(x109/L)
Clinicalsituation
<10 Irrespectiveofsignsofhemorrhage(excludingITP,TTP/HUS,HIT)
<20 SeveremucositisSepsisLaboratoryevidenceofDICintheabsenceofbleedingRiskofbleedingduetoalocaltumourinfiltration
<40 Priortolumbarpuncture
<50 Moderatehemorrhage(e.g.GIbleeding)Surgery,unlessminor(exceptatcriticalsites)
<75-100 Majorhemorrhageorsignificantpost-opbleedingSurgeryatcriticalsites:CNSincludingeyes
BJH2016;175,784-828**expertopinion

Whatistheharm?49
Adversereactions
Supply
$1158

TRIM Transfusion related immunomodulation
Iron overload
TA-NEC

Teachingpoints• Laboratoryreferenceranges(hematologyandcoagulation)specificforneonatesandchildrenshouldbeused
• Alwaysconsidertheetiologyoftheanemiaandthrombocytopeniapriortoorderingatransfusion
• Orderbloodproductsusingchild’sweight

Questions

Keyrecommendationsre:FreshFrozenPlasma(FFP)transfusionsinneonatesNeonatal1. FFPshouldNOTbeusedtocorrectabnormalcoagulation
testinginnon-bleedingneonates(1C)2. FFPmaybenefitneonateswithclinicallysignificantbleeding
orpriortoinvasiveprocedures(highriskofbleeding)iftheneonatehasanabnormalcoagulationprofile(2C)
3. FFPshouldnotbeusedforsimplevolumereplacementorroutinelytopreventIVH(1B)
BJH2016;175,784-828

Keyrecommendationsre:FreshFrozenPlasma(FFP)transfusionsinChildren• ProphylacticFFPshouldNOTbeadministeredtonon-bleedingchildrenwithminorcoagulationabnormalitiesincludingpriortosurgery(2B)althoughitmaybeconsideredforsurgerytocriticalsites(2C)
• ProphylacticcryoprecipitateshouldNOTbeusedroutinelyinnonbleedingpatientswithlowfibrinogenincludingpriortosurgery(2C).
• Prophylacticcryoprecipitatemaybeconsiderediffibrinogen<1g/Lforsurgeryatriskofsignificantbleedingortocriticalsites(2C)
BJH2016;175,784-828