Embed Size (px)
Citation preview

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 1/177
Geneticsatl)(.|uman
With the completion of the human genome sequenceand the hap-
lotype map, investrgaciveand diagnostic tools are available to
determine the qenetic contributions to both uncommon and
common disordirs. Information about the genetic aspects of all
pedi ric diseaseshas grown rremendously and is readily avail
able n mufti ple websitesand in other locations Table78-1).
TH E BURDET{ F GENETIC ISOBOEBSN CHI[0H000. Although
mr-rltifacrorialgenetic condition was a major contributor to pedi-
atric hospital admissions (in 1978) in approximately 257o of
patients. The majority of chronic diseases n children has an
obvious genetic component or is influenced by genetic suscepti-
bility. Thirty-four percent of deaths of hospitalized childten are
associatedwith an underlying genetic disorder. Major categories
of genetic disorders rn chrldren include singlegene,chrornosomal,
an d multifactorial condit ions.
lndividualll', single-genedisorders are rare, but collectively they
representatr rmportanccontribution to childhood disease. he y
includedisorders uchas sicklecell anemiaan d cystic6brosis,as
rvell as a myriad of extremely rare conditrons thar have been seen
rn only a few families. Srngle-genedisorders tend to occur when
mutations have a pro{ound effect on function of the gene product.
Sucheffects include product (structural protein, enzyme, rnetabo-
lite) denciency as wellas oss or gain of fLrnction,The phenotypes
associaredwith single-genedisorders can be variable and modi-
6e d by the action of other genesor the envrronment.Th e hall-
cases this is due to rhe founder effect, in which a mutalion
achreves elarively high frequency in population derived from
a small number of Founders hat rem ns closed to rnterbreeding
lvith those outside the populatron- Thrs is the casefor Tay-Sachs
disease n Ashkenazi Jews and French Canadians. Other muta-
resistanceo malaria,Chromosomal disorders such as Down syndrome are assocl_
ated with rhe presenceof an extra copy (trisomy) of chromosome
21 . Only a fe w trisomies ar e compatible with live birth (chro-
mosomes 13. 18. and 21, as well rhe X and Y chromosomes)j
most lead to early miscarriage as a result of severegenetic imbal
ance. Subtle changes of individual chromosome srructure
(rnicrodeletions) hate also been rdentified. Many of these are
associated with disrinctive phenotypes thar can be recognized
clinically; some produce nondescrrpt phenotypes of developmen
ral impairment wirh variable effects on intellect as well as growth
an d physrcalappearance.
Multifactorial inheritance occurs when multiple genesor gene-
environmental effecrs cause a disorder Multifactorial inheritance
in pediatrics is seen with certain congerriral anomalies, such as
spina bifida or cleft lip/palate. These trairs may clusrer rn fa
lies but usually do not segregate n accordance w'ith mende
domrnant or recessive inheritance. The responsrble genesunknown, and genetic counseling is based on empirical data. T
conceot of mulcifactorial rnheritance extends to common dis
ders, iuch as asthma and diabetes mellitus.
THE CHANGINGPARADIGMOFGENETICSN IIiIEDICINE, CIAIi
few genecic disorders were amenable to treatment in the p
management was focused largely on prevention and managem
of chronic illnesses . nborn errors of metabol ism &'ere the f
genetic disorders to be recognrzed; many are amenable to tre
ment by dietary manipulation (seeChapter 84), These condirr
result from genetically determined deficrencyof specific enzym
leading ro the burldr.rp of coxic substrates and/or defciency
crirical end products. The expansion of newborn genetic
metabolic screening includes a much larger array of sc ree
disorders, made possrble by the use of tandem mass spectro
try, permirting detection of a wide vanety of metabolites
a single, inexpensive assay. Expanded newborn scree
will dramatically increase he number of metabolic disor
in children that are amenable to rrearmeflt (see Chapcer
and 94i.ln addit ion co available creening rograms,more therapie
in development for the treatment of many lysosomal storage
orders that were lerhal or associated wrth intracrable chro
illness. The basis or rreatment in this case s enzyme replacem
usrng specially modified enzymes that are administered
intravenous nfusion and are then taken up by cells and inc
purared nto ly'osome:. Condit ions such a, Gau.her drsea.e
Fabry diseaseare rouonely treated; rreatments for others suc
Pompe disease nd mucopolysaccharidosis re in developm
This places an added responsibiliry on the pediatrician to esl ish an early diagnosis,which is a challengegiven rhe ra
of these disorders and relatively nonspec ific naturc of esvmDtoms.
Tlrerapeutic advances are extending to other nonmetabgenetic drsorders as we)1. mprovemenrs in surgical treament
congenitalanomalies uchas hearrdefectsar e excending he vival of children with birth defects or conditions such as Do
syndrome. The life expecrancy of those rvirh cystic fibrosis
steadily ncreased, argely owrng to improvements n antibi
therapy as well as the managementof boch chronic pulmon
drseaseand malabsorpcion. A malor consequenceof th
advances s that affecced ndividuals survive inco adulthood,
aring a need o transirioncare rom pediatric o adult provrd
Gene replacement therapies have long been anticipared, tho
there have been major challenges rn developmenr of safe
effective approaches for the insertion of genes inro disea
rrssuesand achievement of physrologically meamngful level
geneexpression. The advent of therapeutics based on use of s
cells also offers the possibilrtv of rrearmenc for previo
rntractabledisorders.
Longsrandrng and highly successfulcarrier screeningprogra
have existed for disorders such as Tay Sachs disease and m
orher rare, single-genedisorders rhat are prevalent in specifrcp
ulations. Couples are commonly offered screening for a var
of conditions, in parr based on ancestry (Tay-Sachs dise
hemoglobinopathies, ysdc 6brosrs).Couples ound to be at
can be offered prepregnancy or prenatal testing, rvhich is ba
on gen€tic tests aimed at detecrion of specific mutarions.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 2/177
486x PARTX F HumanGenetics
WEBADDSTS5
h!ta://"wi.ndi
nln rlfrQat
http /twi.rabt ninntltqat-/Anin
n :// ,hti.n(bi.nitni q,r/Ee\ncp
t ttp:/,\t,tvi. (b.nin nth cvlLb/eenbankI ti ,r' tii.n b .nn n tqtl tl. ga
hiP: t\twNge 6t : aq
hilpf/ww q?nekteKattr
hitp:r'ttwwotlq.a.g
hryJ vt /tw0 . g V5l n e 1 h n
D ect0rif(ns and b orielrg fgenetird50r6et5
Te gandounselaqdaE
Heilt lr,( lnlcal, lega,50(,ardth ssueiArcican oderyf Humaneftt6 fe[cmntee nGenelicfrhe mefn Aaadem/f
Pediata6ited!catnalened15om oundium|Jedh5upesiscnuldelinescr mmcneneti(cs0rle6
DAIA AIE
6eneiaiRhretueaintainedy ,lalicnaiibraryfMedne
0n neMendel,rnhertaicelnlin Nlrcmely5efulfof ncansorerl0,000entresofqenetlciraitsinderedy eneamp,tmplonrs,and0crthJ
Generaere|lce0 ffenteifortslo aphe lrnanqen0nle
tearchabeposcryrfaDNAequenceataGncereforunalomyrcF:tlletondl(ai(er
l|rsttute)Ilat nal umrne.Dmeei€archslute!ebSe
(usefunfomdtorboutlLrmanenelit5nde l. c,r 5
hilp,//w,t/rwcn.ntuiJuw(n/ng/hgnd0.htni HunarGpn?Mutationdtdba5e5earchabhdex i
a deso enmuQtonghLrmanenesth
Plrenot!ff5ndele ntet
ro lc i f l all aspectsof pediatric pracfice. Genctic variationenzyrnes involved iLr drr.rg mctabolisrn underhe differcnccthcrapeunceffecran d roxiciry,arrdshould bc taken lto acci l rhe determinationof clrugdosage.Basecl n their gerlotrl
ferent ndividuirls vil l respond diifcrcnrly to specif icdrugsLoring trearment ro individual variations in clrug rnetaboresponsiveness,nd susceptibil ity o coxiciq rvil l leacl o pe
aiizatronof rnedrcal rcatment. Genetic ests vil l c()nre () nn
lic a high proporcion of all medical decisions an d rvi l
scamlessll ncorporatcd rDto rourine medical care. (ieneric
r- i lLalso be used n predicnve esting br predisposit ion o chro the exteri! lhirt such tesrine can lcad to strafe.qies o llredisease r improve outcome (secChapter 8j).
6EMrlCS ANDPEOIAIRICRACTICE enetics rofcssiooalsT78 2) includcph,vsicians'h o complcre csidenciesn genericarc cerrified by rhc American tsoard of l\.'ledical icrLcrics, enized bv rhc American Board of N' lcdjcalSpecial, ies.GecoLrnselofsccelve l1raste]-'scgrcc n generic ou[s,: l ingardccrtif iedhy rhe \merican Board of (ieneticCouuselitrg. hcr
:1lsonursc-gcneticists ho rccoiveadr.arced rairin.g n gcn
lblLou,ilg complerrono{ nursing educarron.Fo r rare singlc-genedisorders, rhe pcdratriciarru' i l l r
closell rvith specialisrsn many disciplines Tablc 711-3).
agerneur ' i l l focus on achievinga correct diargnosiri,ounsthe family regardingnatural hisroryan d managernelrof theorder as wclL as recurrencc isk, anrl implemenradcn oi a maq r tnc r r t r r r . i l ea t rncn r l rn . A . t he s .o f ' c , ' i t e r r r t r i t eincreases.he pediacrician vill be ncreasingly chelk:ngcd oognize elativcl,vare clisordershat arc amcnable o tr earnreto identifv chiLdren ,! 'ho re ar risk on rhe basisoi f:rrnil) 'hisrvho ma,v of !e t dispLay ymptorns f disease. csrin panelsbe developed or conmoLr, conplex problems.sucl as devmental delav. Somedisorders or lvhich eallv rreafrnenr s ccal nray bc added to novborn or earl,v childhood scrccpatels; ochcrs ,r.rl l e the subjccf oi clinical practice guidc
Fanrily historl n'rll be an incrcastnglv r.aluablc rool to recogchilclren r risk. rvho can be esredend thcn oFiered ersonaapproachesro preventx)r of managemenr.Cicnetic resrs
Lrcreasingly Lndcrlielar
fo ddv treatmcnldccisions or comdisordcrsnor rradit iorrall,v icrvcd as genefrc.
ETHICAI-SSUESGcnctic tescing, iagnosis, rrrd rearmcnt nbe performcd rvirh a hr._ehegree of confidcntialitl. rvojdirg srig,ma or fhe paficnr. (lenetic clscriminafion shorrld bc ilbecause ubdc or nor so subtle elfectsof havine,a persorlfrmil,v gcncrrcdiagnosisma y occasionall_1ffect employrneth c ebilir), ro obtarn healrh or life insuralce. Norhing is sosoual as one'r genetic natcrial.The decision o Lln(ler[ lo ctcsl lng s complicarcd. he tlecisron bout whethcr !() pcfiof
naral tesrirg ls aLsooffered for chromosorral clisordcrssuch
as Do$'n syn(lrome. wich !rn increasing numl)cr of affecredpregnanclcs erng ecognizcd y nonirlvasive clccnl l ls esfs uc h
as matcfl)aiserllnlmarkcr screening Dd cra]ulrrasound.Prenara l diagnosis al be conlirmcd by anuiocenccsis r l6-18 rveeks
er chorionic vil lus sampling at l0-12 weeks. Prcimplantation
gcneticdiagnosis PCD) of earll ' cmbfTos Lr,v nalvsisof srngle
blastorneres an selcctonlv ullaffectcdcmbrvos or implantarron.
Approaches o notrlvasile prcnaral cliagnosis ry samplng ofletal cclls or fefal I)\A in maternal blood are also being devcl-oped irr spccialized aLroratorics.
(;enefic tcstinS s increasingl,v vailable br:r u' ide variety of
borh rerc and rclati! 'clJ cornmon gcnctjc Jlsorders Testingcan
resolve Lrnccrtalnry egardiI1gdiagnosis, pror.rde r basis forgcncticcounseljrrg, lnd, n some lrsrirnces,erve ls r prcludc for
specif ic renrrncnt.C;eretic esting ' i1L lav an ncre:rsinl:Lycrtral
FR0FE5S|0||AL RAllllll6 (Emltl(ATlotl
Mel]:al enprliist MD ndeldency AmericanodrCfmedi(alEener5 lledallJenets
[e1a. i cunlef
q r L L l
lI n lcrar 51
Ph|)rMD,rnd'yrrcI0\451r
AdvdnredraC(eNu6e6encit5
imastertr[enet6,n,ctNLrrsebarcalaureate)
Anrerlcanoad F
Ge1e| (
fuun5eg
Amer:anBo,lrdl
[4eitalGeret5
6ene, ( u6 inq
L€denraling
[ommi55ion
ROIE
Daqno5and
iaraqementofp,rtenEthqenelttc50I0e6
6eneticoun5ellng
l:ale
5upervi5ionflahatoryrenn9 {yt0qenei(s,
lrochemaqenelia5,
,tndmc ru rqeftt6
Nu6 q a'eolpatent5
w thqeneri(i5l]rdeis
TYPEOTOISONDTR
Rire5ingleqeft0r(hmmosoma
d50mer
Lommon
multfa(Ioia
c 50T0eT
PTOIATRIflAN
Reco!n€9ign9.ndympl0ms,
rnaKetleflat;supp0rrraf;manaqenaudra/e
Useeneiresstoqu0erca[neni
5PICIAUST
r'Ianaqe
5pecalty'
5peri(prcDl,Alrl
LlSeeIetrr
te5boguide
fieamgn]
MTDI$IGTNETI(
Pertcrmagnoi,(tJn
andorq i tLdlar
alv5e n nterpre
of re i l re iu15;d
!leneli:a5eCher
De59nrd nrerprct
mald(ecmp x 2
perfornarnjly
aoJlntng;0cLs5
gefet Fred ner

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 3/177
seletic test on a child is evenmore drfficult, becausehe child
-annot al*ays participate n d iscussions bout the testtng.The
uftimatedecisionhingeson how the resultsoi the test will help
or harm the child. The interestof rhe chrld s always oremost;
thus, open discussionof rhe pros and cons of testingshould
alwayscenreron the chrld's nterests.Molecular diagnosticcests
are often used to diagnosemalformation syndromes,mentalretardation,or orher disabilirieswherein here s a clear benefitto the child. In other cases, he decisronwhether o test a child
is more difficult.Policies egardinggeneric estingof children have been ssuedjointly by the American Societyof Human Genetics nd Ameri-can Collegeof Medical GenetrcsAmerI Htm Genet 1995;57:.1,233-1,241,)nd by the AmericanAcademyof PediatricsPediatr
2001,;107:1,451-1455).he AAP recommendationsnclude the
following:
l. Btablirhedewborneenin{etttthouldeeviewedandevaluatedPedodi(allyto€mit
nodifGtionf heprogramraliminationf neffectiveompon€ntt.henlroductionf
ne* newbom(eeninger$should€ ondudedhrc0gharcfullyonitotedctcarh
ptoto(olr,
2. Ceneti(ertt ikemost iagnostkorarapenk ndeavo6fordildren,requitepn(est I
infomedarentalonrentnd heolder ild3astent.e{,bom(e€ning rogransre
enouragedoevalu.teroto(oknwhkhnfomedntent rom aPnttsobtained.hefirquenq f nfomedefugahhouldemonitored.egeardo mprovefieeffdenq nd
effectiveneltf nfoflnedonrentornatbont(recningt warnnted,
3. The APoer otupportfiebroadi4of adet etting r5(eeningndildrefl radoles-(entr. dditional€readl eedtobe ondwtedn ar d iteening[ dildrcn nd doles'(entr,he rk andbenefittf (adet meningn hepediatti(opulationhoulde
evallatedn(ar€fullymonitoredini(al alsb€t0ret ir offered na hoad ale (arier
irceninqorpregnaltdoles(entrt ot oneadolesrenEntid€nggrcgnanq ay e
appropriate.
L Geneti(eatingoradult-onsetonditiofi enerallyhouldedefertedntil duhhoodr
untilan dolescentnterertedn erting at evelopeduturc edtion'malingap.dtiet.
The APelievesh.tgeneti(testingofdildtenanddoleg(enttoptedictate-ontetitor'
der r nappop tewhenh€geneti(nfomationas ot e€nhowno cduce otbidity
andmortalitythrroughnterventionrnitialedn t ldhood.
5, Becaureeneti((rcelingnd eslinq ay otbewell nde6tood,ediatftianteed0
prcvidearentghe eaessarynformitionnd@unrelingbouth€ imittofgenetknowl'€dge nd reatmentapabilitiei,hepotenthlarmhatmiybedone ygailng ertnin
geneti(ntonnatioDndudingheportibilitietotPty(hologicalanh,tigmatitation,nd
dircrimination,andedi(alonditiongnd itabilitynd otentialrcatmeiBnd eryi(e!
fordildrciwith eneti(onditiont-ediatftiantnnbe 5sittednninaging any f h€(omplex!ru6 nvolvedngenetk€tting , (ollaboBtionith enetkittg,amtkoun_
reloE,nd renatalcarercvideE.
5. The APupporbhe lp.nsion[educationalpportunitietnhumanenaticotmedi(il
rtudents,esidentr,nd radi(ingiytidantnd heexpantioif rainingrogtamtor
g€neti( rcfegtionab.
Borighr AP, Kere J, SchererSw: The generics f childhood disease nd deveL-
opment, A serres f review ardcles.?eddtr Res2003;53:4-9.
Braude P: Preimplanration diasnosrs br seneticsusceptibjliry.N Ersl / Med
2006;355:541-541.
Burton PR, Tobin MD, Hopper JL: Key concepts n genericepidemjology.
Lancet 2005;366:941-9 50.
creety HT: Bannrnsseneticdiscrimjnarion-N Ezgl l Med 2005;353:865-867.
Gu$macher AE, Collins FS: Genomic medicine--A ptilller N Ensl ! Med
2002;347.1572-1520.
Hall lC, PowersEK, Mcllvaine Rl et al: The frequencl.and inancial br.rrden
of senericdisease n a pedialric hospital. Az / Med Geftet 1978;11417.
McCandlessSE, Brunser Jw' Cassidy SB: The burden of genetic diseaseon
inpatienr care n a children's hosplral.Au.,f H!l,n Cenet 2004;7+121 127
StevensonDA, Care-v C: Contribudon of malformations and senecicdisor-
ders to mortatity in a children's hospital. Az l Med Cerct A
2004r126:393-337
Chapler 9 r TheHumanGenomo
Knorvledge f the structureand funcrion of DNA ushered n era of molecularbiologn with arr ncreasingly ich undersraing of the processes f DNA replication, ranscription, ran
tion, and protein processing.Many genetic disordersunderstood t the molecular evel, esulting n specifrc iagnotestsand appropriace reatments. he Human GenomeProjculminating n che equencing f the humangenomejmade t psible o studyvirtually any humangeneand to explore he roof senesn both rare and common disorders. t has also becapparent hat the genome ncludes ar more than a coded stof informatron o produceproteins.
The human genomehas approximately25,000 genes,whare the individual units of heredityof all traits.Reproductivgermlinecellscontain one copy (N) of this generic omplemand are haploid, whereassomatic(non-germline) ells contrwo completecopies 2N) and are diploid, The genesare ornrzed nto long segments f DNA, which, during cell division,compacted nto inrricarestructureswith proteins o form ch
mosomes.Each somatrccell has 45 chromosomes 22 oairsaurosomes,r non-sexchromosomes.nd I pair of se i chmosomes XY in a male, XX in a female]).Germ cells (esperm) ontain 22 autosomes nd 1 sexchromosome,or a !oof 23. At fertilization, he full d iploid cbromosome omplemof 46 is again ealized n the embryo.
Mosc of the geneticmaterial s contained n rhecell'snucleThe mitochondria thecell'senergy-producingrganelles) onttheir own uniquegenome,The mitochondrialchromosome sistsof a double-strandedircular pieceof DNA, which conta16,568 ase airs bp )of DNA and s completelyequencedproteins hat comprise he mitochondriamay eicherbeproduin the mitochondria (from information contained n the mchondrial genome)or produced rom information containethe nucleargenome nd transporred nto the organelle.All michondria are maternallyderived(becar.rseperm do not usucarry mitochondria nto fertilized eggs);different mitochonwithin a singlecell with a variety of genomeseflect he manal ines rom which heydescended.
FUNDAMENTATSF M0LECUIAB ENETICS-he cenrral enemoleculargenericss that rnformationencodedn DNA predoinantly locaced n the cell nucleus s transcrjbed nto messeRNA (mRNA),which s then ransportedo the cytoplasm, ,'ir is rranslatednto proteil. A gene s a unir that rncludes rulatory regionand a coding region hat stores nformation cresponding o the sequence f amino acids n a specrfic rore
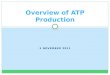
DNA consistsof a pair of chainsof a sugar-phosphateabone inked by pynmidineand purine bases o form a douhelix (Fig.79-1). The
sugar n DNA is deoxyribose. he pynidinesare cvtosine C) and thymine (T); the purinesare guan(G ) and adenine A) . The bases re inkedby hvdrogen osuch hat A alwayspairswith T and G with C. Each strandthe double helix has polariry,wirh a free phosphate t one e(5')an dan unbonded ydroxylon thesugar t theorher ndThe cwo srrandsare oriented n oppositepolaritv in the douneltx.
The replicarion of DNA follows the paring of bases n parenrDNA strand.The original two strandsunwind by breing rhehydrogen ondsbetween ase airs.Freenucleotides,sisting of a base attached ro a sugar-phosphate,orm nhydrogenbondswith their complemenrary aseson rhe parsuand; ne&' phosphodiester onds are created by the enzyDNA polymerase.Replicarionof chromosomes eginssimu

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 4/177
488 r PABI X I HumanGenetics
- Adenine
Thymine
'fl=, GuanineCytosine
Fisure 79 1. DNA double helix, nrrh sugarphosphatebackbone and nitroge
nous bases. From lorde LB. Carey JC, Bamshad v!, et al leditorsl: Medical
Cenetics, nd ed. St. Louis, lv{osby,1999, p 8.)
neously ar multiple sites, orming replication bubbles that expandbrdirectionallyunril the entire DNA molecule (chromosome) s
repllcated. Errors in DNA replication, or mutations induced by
environmenral mutagens such as irradiation or chemicals, are
detected and potentially corrected by DNA repair systems,
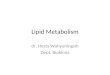
A procotl'pical gene consrsts of a regulatory region, segments
called exons thar encode the amino acid sequenceof a protein,
and intervemng segmentscalled introns (Fig. 79-2). Transcription
srarts at the promorer region and contmues through the enrire
length of the gene to form mRNA. The introns are then removed
and the exons spliced together to form a marure message,which
is then exported to the cyroplasm. There the mRNA is bound to
ribosomesand ffanslated nl o protein.
Transcnptron is iniriared by attachment of RNA polymerase to
rhe promoter site upstream of the beginning of the coding
sequence.Specificproteins bind to the reglon to either reprederepress ranscription by opening up the chromatin, whichcomplex of DNA and histone proteins. It is the productio
these regulatory proteins (transcription factors) that determwhen a gene is turned on or off. Some genes on specific cmosomes rn defined areas are turned off more or lessoermanby epigeneticmerhylarionol cyrosinebaser hat are adjaceguanines (CpG bases).Gene regulation is flexible and responwith genes being turned.on or.off during developmento
responseo envlronmenralsllmulr,Transcriprion proceeds rhrough the full length of the gene
thesizingmRNA in a 5'to 3'direccion. RNA, hke DNA,
sugar-phosphate chain with pyrimidines and purines. The sin this case s ribose; uracil replacesthymrne rn RNA. The Rreads off one strand of DNA to copy a complementary R
sequence. A "cap" consisrrng of 7-methylguanosine is adde
the 5' end of the RNA rn a 5'-5' bood and. for most lranscseveral hundred adenine basesare enzymaticall y added to cend after transcriprion, mRNA processing occurs in rhe nuand consists of excrsron of the inrrons and splicing togerhlhe exons. Soeci6cseouencesat the start and end of introns mrhe sires where the splicing machinery wil l act on the transcIn some cases, here mav be tissue-specificpatterns to splicinthat the same primary transcript can produce multiple dis
protelns.The processed transcript is next exported to the cyropl
where it binds to ribosomes, which are protein-RNA compleThe genetic code is then read in triplets of bases,each tnplet
responding wrth a speciGcamrno acrd or provrdng a signal
terminates translation. The triplet codons are recognize
transfer RNAs (tRNAs) rhat include complemencary "codons" and bind the corresponding amino acid, delivering
the growing pepride. A new amino acid is enzymatically atta
to the peptide; each time an amino acid is added, the ribos
moves one rflplet codon "step" along che nRNA. Event
a stop codon is reached, at which point translation endsthe peptide is released, In some proceins, there may be p
translational modifications such as attachment of sugars (g
sylatron); the protein is then delivered to its destination withi
outside the cell by trafficking mechanisms hat recognize portof the peptide.
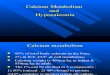
GENETIC ARIATI0N.The processof production of protein
a gene s subject o disruption at mult iple Jevels wing ro a
ations in rhe coding sequence .Ftg.79-3).Changes n rhe
moter region can lead to altered gene regulatron, inclu
increased or decreased ares of rfanscrlptron, failure of gene
va t ron , r ac r i va t ion f rhegene r napp rop r ia reim es r i n i
propriate cells. Changes in the coding sequence can lea
substitution of one amino acid for anorher (missensemutat
or creation of a stop codon in the place of an amrno acrd co
Some srngle-base hangesdo not affect the amino acid, since
may be several codons thar correspond with a single amino (silentmutarion). Amino acid subscitutionsmay havea profo
effecr on protein function if the chemical properries of the slituted amino acid are markedly differenc from the usual
substitutions may have a subtle or no effect on protein func
if the substituted amino acid rs chemically similar to the orig
one.
Genetic changesmay also include insertions or deletions. I
rions or deletions of a non-integral multiple of three bases
rhe coding sequenceeads o a frameshift,altering chegrou
of bases into triplets- This leads to translation of an rnco
amino acid sequence nd usuall y the eventualproduction
srop codon. Ioserrionor deletronof an inregralmuhiple of t
bases into the coding sequence will insert or delele a c
sponding number of amino acids rom the protein. Larger
insertions or deletions can disrupc a coding sequenceor resu
compleLe elerionof an entire Henc )r group ol genes.
"'1-
I
E
E:
II
III

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 5/177
Fi l i tsrc 9.: . Summarv f thc steps eading ron DNA b pr o
teins Rephcaoon nd transcr ipt ion .cur in thc cel l nucleus
The nRN-A is rhen transportedk) thc crroplasm, rvhete rans-
lar ion ol ' the mRNA rnto amino rcid sequencesomposrng
protein oc.urs. (l.rom Jorde l.B. alarey (i, Bamsh.td 'U. er al
led;tots):Medrcdl Ce etirs,2nd ed Sr louis, Mosbl. 1999, p
1 2 1
Mutations usuallycan be classif ied s causinggain of function
or loss of fulrcnon. A gain-of-functionmuration can resulr n an
increase n the abilicv of a proteiD molecule o perform one or
more normal functions!or , more comm()nl)' , r can result u ovet-
expression r inappropriareexpression i a geneproduct. Gain-
ofliuncti{)n mutations most frequentl,v produce aurosomal
dominant disorders (see Chapcer 80). Charcot-Marie-Tooth
disease, ype lA, or peroneal muscular atroph)' . the most
common form of chronrc peripheral neuropath-y f childhood,
resulcs rom dup[cation of rhe gene for penpheral m,velin protein
22 , rcsult ing n ovetexpression f rhe geneproduct. The gain-of-iunccion murarion in achondroplasia, he rnost comrnon of rhe
shorc inTbed keletaldysplasias, xernplif ies he enhanced unc-
rion of a normal ororein. Achondroplasia resuLtsrom a muta-
rion in f ibroblast growth recepror 3 (FCFR3). w'hich eads to
acti\.arion f the recepror, ven n the absence f 6bnrblasrgrou rh
iacror (FGF).Loss-of-functionmutations are frequendvobserved
in autosomal recessive isorders n rv hich loss of 507" enzyme
activity n th e heterozygote ontinues o allow fbr normal func
tion. A lternativell. , oss of funccionmutations can result n con-
dirions in which 50% of the gere product is insuff icienc or
normal function (haploinsuff iciencv). oss of-function rnutations
can have a dominant negarive ffect ,r,henhe abnormal protein
product actively rnterferes v irh rhe function of rhe normal protein
produo.
Cha[ter79 r TheHomanGenome
Anochercategorvof mLltationsma]' ' onfer a novel propertfhe protein sy'nrhesized,,vichouraltering the proteins norfernctions. n sickle cell disease,an amino acrd is subsciinto the hemoglobin rnoLeculebat has no effect on the abof che protein to transport oxvgen. Howeve! unlike norheruogLobin. nder condicions f deoxygenation, icklehemoLrinchains aggregare! ormrng fibers that deform the red cA 6nal caregorl'o( mutations results n abnormaLexpressja gene over spaceand time. Many cancercausinggenes ogenes)are normal regularors of cellular proliferation du
devel<:pment;when expressed n adulc l i fe, and in cellrvhich they usually are not erpressed, thev may resulreoplasla.
l)elerionscan varl in rheir extent and, even rvhennot viat the cytogenetic er.el, an involve several enes; hese re otenned microdeletions. 81. a variety of rearrangemencs, corions eterred o as contiguous en esyndromesma y be generTh e clinician ma1,be alerted o this poss ibil itv bv an unusdiversearray of chnical earures n any indrvidualor thc presof addirional eatures o a known condit iol. For example,ouro the closeph,vsical roximicl' of a series f genes, ifferent drions nvolving he shorr arm of cheX chromosomecan prodinclividualswith various combinationsof the followine Fear ih th r , , . r . ,Ka l l rnann l r rd rom e , iu la r a lb rn i rm ,m cn ( ; l re larion, chondrodysplasia unc!ata,and short srature.The rnd

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 6/177
490 PAnTX I HunanGeneticg
Promoter
Filwe 79-3- Various types of inrragenic mucations. Promoter mutarions alrer rate of transcription or disrupt gene reguLarion.Base chang€swithin e
can havevarious effects!as shown. Mutations within Lntrons an lead ro inclusion of some nrronic sequencen the final processedmRN-A" or can lead to e
skipping.
ual eaturesn each ase epend n the nvolvement fthesegenes
and the ossof DNA sequencesn the underlyilg reaffangement.Many other chromosome deletion syndromes have beendescribed n humans, including Smith-Magenis,Rubinstein-Taybi, DiGeorge, 0illiam, and Prader-Willisyndromes.
Rearrangemenls uch as translocationsalso take place insomaticcells.The best understoodare the rearrangementshatoccur in lymphoid cells.Some earrangements re required orthe formation of funcrional immunoglobul in in B cells andantigen-recognizingeceptorson the T cell, Large segments fDNA, which code or the variableand the constant egionsofeither immunoglobulin or the T-cell receptor, are physically
joinedat a specilic tage n the development f an immunocom-petert lymphocyte.The rearrangemenrsake placeduring devel-opment of the ymphoid cell lineagen humansand result n theextensive iversiryof immunoglobulinand T-cell eceptormole-
cules. t is as a result of rhis post-germlineDNA rearrangementrhat no t'vl'o ndividuals,not even dentical wins, are really den-tical,because ature ymphocltes rom eachwill haveundergonerandom DNA rearrangemenls t theseoci.
Studiesof che humin genomesequenceeveal thar any twoindividualsdiffer in about one basen a thousand.Someof thesedifferences re silent;some esult n changeshat explainPheno-typic differenceshair or eye coloq physicalappearance); omehave medicaL ignif icance, ausingsinglegenedisorders uch as
sicklecell anemiaor explainingsusceptibility o commondisor-derssuchas asthma.Genetic ariantswithin the samegeneoccur
commonly in the population and are referred o as polymphisms.Thesemay be silenr or subtleor have signilicantphetypic effects.
GEI{OTYPE-PHENOTYPEORREI.ATIONSN GENETICDISEGenotype s the geneticconstirutionof an individual and reto whichparticularalternative ersion allele)of a genes preat a specfic ocation (locus)on a chromosome. henotJpesobserved tructural,biochemical, nd physiologic haracterof an individual, determinedby the genotype,and refers o obsepedstructuraland functionaleffectsof a mutant allelespecific ocus.Many mutations esult n predictable henoty
Therefore, dentificationof a specilicmutation in an individ
ofren can be used o predict clinicaloutcomesand plan appriate treatmentstfategles.
The ong QT syndrome xemplifies disorderwith predictgenotype-phenotypeorelations (seeChapter435.5). Longsyndrome (phenotype) an be causedby mutadons n sevgeaes(genotypes),whicb are designatedLQT1, LQT2, LQT3, all encodingcardiac on channels,The risk for carevents syncope, borted ardiacarrest,or sudden eath) s higwith mutations ̂ t the LQTL locus (53%) or the lQT2 lo(46y.) thar amongsubjectswith mutations at the l8T3 lo
{ 8o/o).n addition, hosewith LQfl mutarions xperienceof thei r episodes uring exercise nd rarely during rest or slthosewith LQT2 ar.d QT3 mutationsare more ikely to h
episodes uring sleepor rest,and rarely during exercise.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 7/177
l \ ' lutations n the 6bnllin-1 geneassocialed ' ith Marfan syn-
diome reptesent another example of predictable genorype-
phenotypecorrelations seeChaprer 700). Marfan syndrome rs
charactenzed v the combination of skeletal,ocular,an d aorric
manifestarions, vith the mosc devastacing utcome being aortic
root djssectron nd suddendeath. Sixcy-five xons make uP th e
fibril l in 1 gene,an d mutations have been ound in almost all of
rhese exons. The locatron of the mutarion within the gene (geno-
lung diseasecaused by mutations in the CF transmembrane con
duccance regulator (C}-TR) gene. More than 1,000 different
mutations harrebeen dentif ied; he most common is the AI508
mutation, which accounts for 707" of all mutalions and is asso-
ciatedwith severe isease. everalmulations associatedvirhmrld
disease ave been denrif ied, ncl uding 3272-25A+G, 3849+10
kb C-+T, IVSS-5T,and 2789+5GrA. Patienrs 'rrh at leaston e
3272-26A-+G alleleand a second mutaced allele (compound het-
erozygote) associated rvirh severe disease are more likely to be
diagnosed ater and have berter ung function, a lower incidence
of Pseudomonas aeruginosa colon:tzatton,and normal pancreatic
funcrion. Homozl,gotes or rhis mutarion are no! obseruedan d
may nor have clinical disease. Conversel)', lhose with
2183AA-+G mutations, eicher homozygous or heterozygous ,rvrth
another CF muration, are more lik ely to have early-onset, evere
disease. hose wich this mutation tended o have severe ancre-
aric involvement, failure to thflve, varrable lung Involvemenc, and
relativelyearly death.
With any given mutation! modifrer genes for a different gene
producl may altenuate th e murared gene'sphenotvpe. W'hen
srcklecell anemia is co-inherired rl'irh the gene or hereditary per
srstence f fetal hemoglobin, he sicklecel l phenotypicexpression
is less severe. Modifrer genes in CF may rnfluence the develop-
ment of congenitalmeconiu ileus,or colonizationwith P aerlg-
fuosa. -Nlodifer genes ma also affect rhe manifesrations of
HUMANGEN0ME B0JEGT. en emapping s performed by genetic
linkage analysis, hich is basedon the principle that Leles t
t\r'o genetic loci thac are located near one another rvill gregate
together i a family unless they are separated bv genetic recom-
bination, he fre<luercyof recombinarionbetween he loci is a
measureof physical distance.A set of polvmorphic generic oc i
is dentif iedand is closely' paced long be entirehuman genome
and eou ld be used o map an r gc t t e t t era i t .
Phy mapping of the genome nvoLvessolation of segmenrs
of rhe an genomewith lengths rom hundredsor thousands
to a ferl million basepairs and placing them in micloorganisms
su!h a\ hacrerir or )ea\I. AuronratedseqLren(ingvstem\ pcrmit
the base sequenceof these segments o be decermined The seg-
ments could chen be pieced togerher by examining !he sequence
of overlap regions and by relacing rhe sequenced segments to
sequencing be fragments,an d rhen using a compllter to order
the fragmentsbasedon overlappingsegments.
Analysis of the human genome has producedsome surprising
resulcs s well. The number of genes s str l l not known preciselY
but appears o be around 25,000. This is fewer rhan had been
ChaDter9 a TheHumanGenome
of alternarive promoter regions in some genes, alternatite sp
ing, and post cranslationalmodrfications.
Ic is a lso apparent ha t moscof rhe genomedoes no t encprorein ( lesschan5% is rranscribed nd translared).Many tr
scribed sequences are not translated but represent genes t
encodeRNAs that servea r egulatory role. A high proporcio
th e genomeconsistsof repeatedsequenceshac are interspe
among chegenes.Someof theseare ransposable eneric lem
rhat have he ability ro move from placeco place n lh e geno
Others are stacicelements hat Eere exoanded arrddisoerse
rhepa r t du r rnghum anevo lu r ion . rhe i repea redequen (e \
play a struccural tole. There are also regions of duplicationgenomic regions.Such duplJcations re substrate br evolutallowing geneticmocifs o be copied an d modif ied to servenroles n the cell. Duplicarionsma v also form rhe basis or ch
mosomal rearrangement,permitring nonhomologous chrom
some segments o pair during merosrsand exchangemate
This is another sourceof evolutionarvchanse.an d also serve
a p ' t rn r ia l \ ou rceo l ch rom u \o rna lns tab i l i i yead ing o cong
ital anomaliesor cancer
Availability of the genome sequencepermits the stud,v of la
groups of genes, ooking for patterns of gene expres siogenomealteration.N,licroarra]s av e beendeveloped ha t per
tensor hundredsof thousandsof gencs o be anaLyzed n a smglasschrp. Pat terns of geneexpressionprQvidesigcatures for p
ticLllardisease tates, uch as cancer,or rn response o ther(F rg .79 -4 j .

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 8/177
492 PAnT I Humrn Gnotics
ChristensenK, Murray JC: whar genome-wideassocia.ionstudiescan do for
medicine. N Engl J Med 2007;356:1094-1097.
Cordefl HI, Clayton DG: Genetic association sfidies, Ldn et
2005i366:1121-1130,
Hatrersley AT, Mccarthy Ml Wlrat makes a good geneticassociarion rudyl
Lancet 2005 366 1315-L323.
JarvisJN, CentotaM: cene-expression rofiling: Time lorclinical apphcation?
Lancet 2005 3651199100.
Lander ES, Linton LM, Birren B, er al, Initial sequencing nd analysisoI rh€
human genome.Naturc 2001;4091.6822):860-921.Mcchee SA, Mccabe ERB: Genome-wide esrhg: genomicmedicine. PedrTtt
Res 200660243-244 .TeareMD, BarreftJH: Genetic inkage studies. -rncet 2005i36611036-r044.
VenrerJC, Adams MD, Myers EW, et al: The sequence { the humangenome.
Science 001 2911S5O7 l 3O4.
FAmltY HISTORY IUDPEDIGREEl0TAnOfl. The farnily historyremains he most important screening ool for pediatricians nidentifyinga patient's isk for developinga wide range of dis-eases,ncludingmultifactorialconditions, ike diabetes nd atten-tion defrcitdisorder, o s ingle-geneisorders uchas osteogenesisimperfectaand cystic ibrosis,Through a detailed amily historythe physician an ascertain he modeof genetic ransmission ndthe risks to family members.Because ot all familial clusteringof diseases due ro geretic actors,a family historycan also den-tify commonenvironmental nd behavioral actors hat influencethe occurlence f disease. he main goal of the family history sto identifygenetic usceptibili ty, nd he cornerstone f the familyhisrory s a systematicnd srandardizededigree.
A pedigree rovidesa gaphic depictionof a famrly'sstructureand medicalhisrory. The person providing the information is
termed the proband, and is typically designated by an artow- his important when raking a pedigree o be systematicand usestandardsymbolsand configurations Fig. 80-1) so that anyonecan read and understand he information. A three-eenerationpedigree houldbe obrained s an iniri alscreenor iue.y ne *patienr to identify possiblegeneticdisorderss€gregating ithinthe familn the inheritancepattern, and rhe risk to the patient.The closer he relationshipof rhe proband to the person n thefamily with the geneticdisorder, he greater s the sharedgeneticcomplement. irst-degreeelatives, uchas a parent, ull sibling,or child,shareY, heir genetic nformation on average; stcousinsshareY5. ometimes diseasen a more distant elativemay createa greater isk; for thar reason, more extendedpedigreemay beneededo identify risk for certaindisorders.A hisroryof a distantmaternally elaredcousinwith mental retardationdue to lragi le
X syndromemay have itde significanceor the male nfant youare examining,or it may mean har this child is ar elevated iskfor fragile X syndrome.
MEITIEtIAl{ NHEBITAI{CE
There are threeclassic orms of genetic nheritance: utosomaldominant.autosomal ecessive. ndXJinked. Theseare referredto asmendelian nheritance orms,after GregorMendel, he 19thcenturymonk whoseexperimentsed to the laws of segregationof characteristics,ominance, nd ndependent ssortment. heseremain he oundationof single-genenheritance.0ith mendelianinheritance,a singlegene'seflect rs necessaty nd sufficieflt ocausea particular phenotype.This is in conttast to oth€r forms
f tttare
I Femate
Sexunspecified
ra |,1$'.:1,',::i#""lO,qfiecteo
r. il:lH::[3$ffi'"XT;Obligala arder, il lnotmanifest isea$s
Proband
Deceasedndividual
sti bidh
Adoptednto amily
Adopted d ol family
Marriag€ r union
Divorced
Consanguinity
Monozygoticwinsff
EO
TFj/.
trl
Dizygoticwins
Twinsot unknownzygosity
Nootfspring
lvlultiplenions
Figur€ 8O-1. Peati4reenotation. Symbols commody used ir pediSree cAlrhough there s no uniform syst€mof pedi8ree otation, the symbolsshere are according o recent recommendationsmade by professionals
6eld of geneticcourselhg, (From BennettRL, SteinhausKA, LlhrrchSBRecommendations or standardizedpedigreenomenclatve. I Genet Co1995A:267-279.1
of geneticallydetermined raits, such as impriotirg condittriplet repeatdisorders, nd multifacto rial raits, in which ofactors nfluencewhether he disease ill bepresent n somwho carries he genetic hange.
AutosomalDominantnhoritance. utosomal dominant intance s determined y thepresence f one abnormalgeneon
of the autosomeschromosomes
-22), Thegenes
n thesemosomesexist in pairs, with eachpatent contnbufing one c!7ith an autosomaldominant trait, one of the pairedgenean effecton the phenotype hat dominateshe effectof rhe oof the pair.Phenotype efersnot only to physicalmanifestabut also o behavioral haracteristics r to differences eteconly through aboratory ests, uchas biochemical bnorma
The pedigree or an autosomaldominant disorder(Fig,8demonstrates ertain characteristics,1) The disorder s trmitted n a vertical (parent o child) pattern,appearingn mple generations. his s rllustratedby individual .1 (see ig 8passing n the changed ene o IL2 and II.5. (2) An affectedvidual has a 50% (1 in 2) chanceof passingon the deletegenesor eachpregnancn nd hereforeof havinga child affeby the disorder.This is referred o as the recurr€nc€isk fo
disorder.3)
Unaffected ndividualsfamily
memberswho domanilest he !:.aitldo not pass he disorder o their childreMales and females re equally affected.Although nor a chteristicper se, 5) the inding of male-to-maleransmissiontially confirms autosomal dominant inheritance. Vertransmission analsobe seenwith X-linked raits.However,a father passes n his Y chromosome o a son, male-totransmission anno t be seenwith an X-linked trair. Theremale-to-male ansmissioneliminat€sXlinked inheritanceoossible xolanation.While male-to-malelansmission an owith YJinkid genes swell, there arevery ew Y-linkeddisocomparedwith thousands aving he autosomal ominant nrtanceDattem,
Although parent to child transmiss ion s a characte risautosomal ominant nheritance,or manypatrefltswith an a

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 9/177
somaldominart disorder here s no history of an affected amily
member. hereare several ossibleeasons,irst, hepatienrmayrepresen!a new mutation; second,many autosomaldominantconditionsdemonsrratencompletepenetrance,neaning hat not
all individualswho carry the mutationhavephenotypicmanifes-
tations. n a pedigreehis may app€a!as a ek ipped eneration,n
which an unaffectedndividual links two affectedpersons Fig.
80-3). There are many potential reasons hat a disorder mayexhibit incompletepenetrance,ncluding the effect of modifier
Benes,nvironmental actors,gendeq nd age,Third, individuals
with the sameaurosomaldominant mutation will manifest hedisorder o different degrees. his is termedvariableexpression
and is a characteristic f many autosomaldominantdisorders.Founh, somespontaneous eneticmutationsoccurnot in the egg
or sperm hat forms a child but rather n a cell n the developingembryo. Such eventsare referred o as somaticmutations.The
resultingphenotype aused y a somaricmutation can bevaried,but it is usuallymilder than if all cellscontain the mutation. Ingermlinemosaicism,he mutation occurs n cells hat populate
the gernline that produceeggsor sperm.A germlinemosaicwillhaveno manifestations f the disorderbut will producemultipleeggsor sperm hat carry the mutation.
AutosonalRecessivenheritance. utosomal recessivenheri-tance nvolvesmutations n both copiesof a gene.Examplesofautosomal recessive iseases re cysdc fibrosis and sickle cell
disease.Characteristicsf autosomal ecessiveraits (Fig. 80-4)
include(1) horizontal transmission,he observation f multipleaffectedmembersof a kindred in the samegeneration,but noaffected amily members n othergenerations;2) recurrenceiskof 257o or parentswith a previousaffected hild; (3) malesandfemales eingequallyaffected, hough some raits exhibit differ-ent expr€ssionn males and females ovariancancer,hypospa-dias); (4) increased requencyof consaDguinity,articularlyfortate tratrs.
The chance hat any two parentscarry an identical mutantallele s increasedf the couple s consanguineous.onsanguinityis relationshiobv descentrom a common ancestor. onsanguin-ity between arinrs of a child with a suspected eneticdis;rderimplies (but does not prove) aurosomal ecessivenheritance.
Although consanguineous nions are uncommonin Western
society, n other parts of the world (southern ndia, Japan, he
ChaFor I P|ttor[!ol Gonoticrsnsmislio
l l t 1 2
Fture 80-3. Incomplete penetrance.This family segregates familial csyndrome, familial adenomatouspollposis, Individual II.3 is an ob
carrleq but there are no findings to suggest he disorder. She s rermedpenerranr.
Middle East) heyarecornmon.The risk of a genetic isordethe offspring of a first-cousinmarriage 6-8%o)s about dothe risk n thegeneral opulation (3-4"/.), Therearesomegersolates small populations separatedby geography, eliculture, or language)n which rare recessive isordersare mcommon than in the generalpopulation. Even though conguinity may not be increased n thesepopulations,becaulimited mate choice, he chanceof a couple from an isogenetic egion havinga child wirh an autosomal ecessiveotion may
be as high as that observed n first-cousinmarriScreening rogramshave beendevelopedn suchgroups o
Figure 80-2. Autosomal dominant pedigree.Pedigree howing ryprcal nheritanceof a form of sensorineural eafness DFNAS/ inhedted as an aurosomainant trait, Blue. affecredDati€nts.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 10/177
Fisurc ti(}4. ,qurosomat ecessive edigreex.ith parental consanguinitr. Purple, carriers; Red, afl'ected
494 r PARTX ! HumanGonrtics
tect heterozygotes t rrsk for having affected hildren,A varietyof autosomal recessive onditions are more common among
Ashkenazi ews hann
thegeneral opulacion.Natronalpractice
guidelines ecommend creening symptomaticAshkenazr ewsfor rhe neurodegenerative rsorder Tay-Sachsdisease,andCanavandisease arrier screening or other disorders Fanconi
anemia,Gaucherdisease, ystic ibrosrs, amilial dysautonomia,nesidioblastosis)s under considerationor this population.
The prevaLencef carriersof certainaulosomal ecessiveenesin sorneargerpopr-:lationss unusuallyhigh. In suchcases, et-erozygoteadvantage s postulared.The carner frequencies fsicklecelldiseasen cheAfricanpopularionand of cystic rbrosrs
in thenorthernELrropeanopulationaremuchhigher han would
beexpected rom new mutations. t is possiblehat heterozygous
carriershave had an advanragen terms of surv ivaland repro
ducrion over noncarriers.n sickle cell disease,he carrier stale
may confer some resrstanceo malaria; in cystic fibrosis, rhe
carrier statehas beenpostulated
co confer resistanceo cholera
or enteropathogenicscherichia oh rnfections, opulation-based
carrierscreeningor cystic ibrosis s recommendedor individu-als of northern European and AshkenaziJewish background;population-basedcreeningor srckle ell diseases recommendedfor individualsof African background.
If the irequencyof an autosomal ecessive iseases known,che requencyof lhe heterozygote r ca rrier statecan be calcu-lated rom cheHardy-Weinberg ormula:
p:+2pq+q' 1
wherep is the frequencyof one of a pair of allelesand 4 rs chefrequencyof the other. For examp , if the frequencyof cysticlibrosis among white Americanss in 2,500 (p2), hen the fre-
quencyof cheheterozygote2pq an be calculated:f pr = Ythenp=|ro an dq = a'7t,,2pq= x Ysoxa%o,or pproximt/2.
lo r 3.921").Every human probably has several are, harrnful, recesgenes.Becausehesemutantgenes re frequendynot identifiaby laborarory ests, he heterozygous dult usually earnsabtheseharmful recessive enesafter the birth of a homozyg(and thereforeaffected)child. Relatedparentsare much mlikely to be heterozygousor the sameharmful recessive ebecausehey have a common ancestor
Ps€udodominantnheritance, seudodominantoheritarrceeto rhe observation f apparentdominaflt(parent o child) cramissionof a known autosomalecessiveisorder Fig.80-5).Toccurs 'hena homozygous ffected ndividualhasa parrnerwis a heterozygous arrierrand it is most likely to occurfor retively common trarts,such as sickle cell anemia or congendeaFnessue o connexin26 en emutation,
Xiinked lnheritance.Characteristics f X-linked inherita(Fig.80-5) nclude he following: (1) Males aremore commoand more severely ffected han females. 2) Female arriersgenerally naffected, r if affected, heyare affectedmore milthan males. 3) Affecredmaleswill have onLvcarrierdaughtThey have no chanceof havrng an affectedson (male-to-m
transmjssion xcludes -linkageand s seenwith aurosomal oinant and Y-linked nheritance). 4) Carrier women havea 25risk for havrngan affecred on, a 257. risk for a carrier dauter, and a 507o chance or a child rhat does not inherrt mutated X-linked sene.
A femalemay oicasionallyexhibit signsof an X-hnked t
similarly to a male. This may occur owing to nonrandominacrivarion,homozygosiryor an X l inked trait, or presenc
a sex chromosome bnormality 45,X or 46,XY female).

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 11/177
Fisurc 80'5. Pseudodominanrinherirance. Red, alfected(deaf ) .
GhoDter{l r Pon.msotceletic Tr6nsnission
Of specialnote s rhepseudoautosomalegiorton the Y chmosome, hesmall egionof bomologychat s sharedby bothand Yp- Very few genes eside n this region. One of the feSHOX. Hererozygous SHOX mutadofls cause Leri-Wdyschondrosteosis,rareskeletal ysplasia hat nvolvesbilatbou.ineof the forearmswith dislocarions f the ulna at the wand generalized hort stature.Homozygousmutationscausemuch more severe angermesomelic war6sm.
0lGENlCNHERITANCE.igenic inheritanceexplains he ocrence f retinitispigmentosa RP) n childrenof parentswho ecarry a different RP-associatedene.Both parentshave norvision,aswould be expected, uc he offspringwho were douhererozygotes eveloped RP Digenic pedigees (Fig. 80exhibit characceristics f both autosomal dominant (ver
transmission) nd autosomal ecessivenheritance 1 in 4 rerence isk). A couple n whrch the two partnersare carriersrwo different genesmay have affected children. Anv chhowever,might transmit both mutations o an offspring, adommant nherltance,
PSEUD0GENEC NHERITANCENDFAMlt lA[CIUSTERINGhare nongenetic easols or the occurrence f a diseasen muple family members; hesecan mrmic genetic fansmissron.sible explanations include environmental factors, teratoexposure,and as yet undetermined nd undefined actors.Mtiple srblingsmayhaveasthmadue o exposureo cigaretre mfrom rheir parents.A woman may have multiple children wsmall size,developmental elay,and unusual acial appearowing to her useof alcohol during pregnancl'. hernatively
diseasemay be very common n the generalpopulatiol- Brcancerwill allect 1|Yo of all womenr t is oossible hat sevwomen n a familywill develop realr ancer ecause|; erutermined faccors. t rs usually possible o differentiate amwith generrcally etermined igh-riskcancersyndromes, ucthat associated ith a BRCAI mutation, by their earlier agonsetof breastcancer n multiple family members.
NONTRAOITIONATNHERITAIiIGE
Sone eenetic disorders are inherired in a manner that doesfollou.classical mendelian oatrerns. This nontraditional inh
tance partern includes mitochondrial disorders, triplec repexpansion diseases,and rmpnnting defecrs.
X chromosomenactivationoccursearly n development ndinvolves andom and irreversible nactivationof most genes non eX chromosomeyeach el l Fig.80-7). n some ases, pre-ponderanceof cells may inactivate he sameX chromosome,resulting n phenotypicexpression f an Xlinked mutation if it
resideson the activechromosome.This may occur owng to
chance r to selection gainst ells hat have nactivated nolmal
X if the other X carriesa structural earrangemen!.Thereare someX-linked drsorders, alledX-linked dominant,
in which female a iers ypically manifesr bnormal indings An
affectedman rvill ave only affecteddaughtersand unaffeced
sons, and half of rhe offspring of an affectedwoman will be
affecred1Fig.80-8). Some X-linked dominant conditions arelethal in males. An example is incontinentia pigmentl (see
Chapter651). The pedigree howsonly affecred emales, nd an
overall ratio of 2 : 1 females o maleswich an increased umberof miscarriagesFig.80-9).
Y-I|NKED NHEBITANCE.here are few Y-linked craits, These
demonstrate zly male-tomale raDsmission , nd only malesareaffected Fig.80 10). r{ostYJinkedgenes rerelated o malesex
decermination nd reproduction,and are associated ith rnfer-
tility. Therefore, c is rare to see amilial transmrssion f a Y-
linked disorder Advances n assisred eproductive echnologresmay makepossible amilial lrarismission f male nfertiliry
Figure 80-6. Pedigreedemonsnating Xlinked recessivenheritance- (From
Nussbaum RL, N'lclnnesRR, Vitlard HF, ThorllPson & Tboh'Pson Gehetics
in Medidne,5th ed. Philadelphia, rB Saurders, 2001.)
TI

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 12/177
496 PAETX r HumanGerctics
IB f f i g H,xe x-x" X.Xo X.Xo
/ ' \
/ \
H HX.Xp x*4
H Bx.x" x-x, X.X
H Bx.xo x_x"
X X, X-XU X.X.X.X,
x.xo x,xo x.x x.x, X.Xo X.Xo
X. X., X.XN X.X. X.X,,
Figure 80-7. X inactivation.
Mitochondrialnhelitance.An individual's mitochondrialgenome s entirelyderived rom the mother (Fig,80-12). Spermcontarn ew mitochondria,most of which are shedupon fertil-ization. Mirochondrial disordersexhibit maternal nheritance;woman with a mitochondrial geneticdisotder will have onlyaffected ffspringof eithersex,while an affected ather will haveno affectedoffspring (Fig.80-13).Although suchan inheritancepatternca n be explained y autosomal ominantor X-linkedinheritance, t suggescs mitochondria l basis Table80-1).
The mitochondriaare the cell! suppliers f energy, o that theorgans hat are most affectedby the presence f abnormalmito-
Figure 80-8. Pedigreepatrern demonsrratingx-linked dominanr inheritance-
lFrorn Nussbaum RL, Mclnnes RR, Wrllard Hr: Thompson It Thonptu11
Geneti.s n Medicine,6rh ed. PhiLadelphia,WB Saunders, 001.)
chondria are rhose that have the greatest energy requireme
such as the brain, muscle, heart, and liver (see Chapters 8
358, and 598). Common manrfestationsnclude developm
delal seizures,cardiac dysfunctron, decreasedstrength and c
as well as hearing and vision problems. Examples include MEL(myopatby, encephalopathy, lactic acidosis, and stroke
episodes), MERRF (zryoclonic epilepsy associated with rag
red flbers), and Kearns-Sayre syndrome (ophthalmoplegia,
mentary retinopathy, and cardiomyopathy) [see Chapter 5
Mitochondrial drseases an be hrghly variable in clinical mfestatrons. Cells may contain a mixture oI mutant and nor
mitochondria, referred to as heteroplasmy. Unequal segrega
of mutant and normal mirochondria (rephcative advantage)
result in signilicant drfferences n expression of a mirochond
trarr ,n the ovum and different cel ls of an individual or diffeoffspnng of a carrier mother. Becauseof rhis, the mother nia
asl'mptomatic. In affected offspring, diseasemanifestations t
ro occur when 50-507o of mrtochondria carry a single large d
non or when 80-c0o/ohave a poinl murarion.
TriFletRepeatExpansionDisordeis. Triplet repeat expansron
orders are distinguished bv the special dynamic nature of
diseasecausrng mutation. Triplet repeat expansion disor
include fragrle X syndrome, myotonrc dystroph)', Huntir8t
disease, spinocerebellar disorders, and several others (Table
21. These disorders are caus€d by expansion in the numbe
three-base-pair repeats.The fragile X gene, FMRI, normally
between .5and 50 CGG rriplets. An error in replication can re
ln expansion of thar numbeq referred to as premutation.
fragile X, premutation comprises 50-200 repears. Individ

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 13/177
ChdFe.m . Prltemsol G6r6ticTlrlsnissiol r
Figur€ 80-9. Pedigree f an X-link€d dominant disord€r with male lethaliry, such as incontinenla pismenn-
with a premutationareat risk for having hegeneexpand urtherin subsequentmeiosis,crossing nto the range of full mutation.In fragile X, that boundary is above 200 repears.Wirh rhisnumber of repeats, he FMR1 genebecomes ypermethylated,
and protein production s lost. Somemale carriersof the premu-tation develop a syndrome as adul ts characterized y ataxia,tremoq and cognitivedecline,
The effectof theexpansions different n othergenes.n Hunt-ington disease,he expansion auseshe geneproduct o haveanew, oxic effecton the neuronsof rhe basalganglia,For most
tripler repeatdisorders, here s a clinical corelation to theof rheexpansion, ir h a greater xpansionausingmoresand/or earlier ageof onset or rhe disease. he observatiincreasing everity f disease nd earlyageof onset n subse
generalionss termedgeneticanticipationand is a deliningcacteristic f triplet repeatexpansiondisorders Fig.80-14).Geletic mp ntittg.The two copiesof most genes re func
ally equivalenr. n a small number,only one of the pair isscribed.The activegenewill be that inherited from a spparent,and the other copy is silenced ssociated ith met
Figure 80-10. Ylinked inheritance.Blue, aflecredpadenr.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 14/177
498 r PARTX r HunanGenelics
F'igurc80-ll. Digenicpedigre€.
tion of DNA (epigeneticmodification of a gene not due to a DNA
mutation). In imprinting, gene expression is dependent on the
parent of origin of the chromosome (seeChapter 81). Imprinting
disorders result from an imbalance of accive copies of a given
gene, which can occur for several reasons- Prader-Willi andArgelman syndromes, whrch are two distinct di sorders associated
with developmental impairmenr, are illustrart ve. Borh are associ-
ated rvith microdeletions of ch(omosome 15q11-12. The
microdelerion n Prader-Wrllisyndrome s always on the pater-
nally derived chromosome 15, u'hereas n Angelman syndrome ic
is on the maternal copy. UBE3 is rhe specific gene for Angelman
syndrome, and as expected, rhe paternal copy of UBE3 is tran-
scriotionall v silenced in the brain.
Uniparental disomy (UPD), the rare occurrence of a child
inheriting boch copies of a chromosome from the same parent, is
another senetic mechanism thar can cause Prader Willi and
Angelman syndromes. Inheriting both chromosomes 15 from the
mother is fuflctionally the same as deletion of the paternal 15q12
and will result in Prader-rJ7illisyndrome. About 30% of casesof
Prader-Villi syndrome is caused by paternal UPD15, whereas
macernal UPD15 accounts for only 3lu of Angelman syndrome(seeChapter 81).
A mutation in an imprinted gene is another cause. Mutations
m [IBE3 account for almost 307. of patients with Angelman syn-
drome and also result in familial transmission. The most uncom-
mon cause is a mucation in t he imprinting center, which resul ts
rn an inability to set the imprint. In a woman, the inability to
reset the father's chromosome 15 imprint will result in passing
oo ro active copies of UBE3, and the child will have Angelman
syndrome,Besides 15q12, other imprinted regions of clinrcal interest
include rhe short arm of chromosome 11 (where the genes for
Beckwith-Wiedemann syndrome and nesidioblastosrs map) and
che ong arm of chronosome 7 (maternal uniparental disomy of
7q has been associatedwith some casesof idiopathic shorr stature
and Russell-Silversyndrome).
Imprinting of a gene may occur during gametogenesisor earlv
embryonic development (reprogramming). Genes may become
rnaclive or active by various mechanisms inc|.rding DNA methy-
lation or demethylation (or histone deacytylation) with different
patterns of (de)methylacion noted on paternal or maternal
imprintable chromosome regions. Some genesdemonstrate tissue
specific rmprinting. There is an increased ncidence of imprinting
disorders ssociated ith in vitro fertilizatron r intracvtoolassperm injecrion (Beckwith-Viedemannnd Angelmansdrome). Retinoblastoma as also been reported n associawith assisredeproducriveechnologies.
MULTIFACT0RIAUPOIYGENICNHERITANCE.ultifactorial inhetance efers o traits thar are causedby a combinationof inhited, environmental, and stochastic factors (Fig. 80-1Multifactorial traits differ from polygenic nheritance,whrefersro traits thar result from rhe additive effectsof multigenes.Multifacrorial traits segregate i thin families buc do nexhibit a consistent r recognizablenheritance attern.Charteristics nclude he following:
l. Iherei a imilarate f €(uen(etypitally-5%)mongll st-degreeelaliverpariblingg,off5pdngI he ffertedild).lt r un|llualtondasubrtaltialnfie e n kl
rclativegelatedore ittnntlythannd eg.eeo he nder a5e.
2. lhedrk fn(ufien(er related0 he nddeftefthe ise e.
3. SomeirodeE ave s€x edilection,r ndiaatedy nunequalale emalen(id
Pyloft eno9k moreommon0males,herearongenitalislo(ationfthe iprirm(ommonn enaler.Whereherer analtepd lx la1i0,hedrk 9higheror he elativ
an ndex(deinthele$connonlyaffectedtex.Ihedsktohe onofanf{ededemal
infdntileylod(lenoeis318%ompandith fie5%uk or he on fanaffe(ed
lhe emalear asrednagreaterenetku(eptibility0hpr ffrpng.
4. lhe ikelihoodhat othdentiolwins illbe ffectedith he ame alfomatior
than 00%ut u(h reaterfianhe hancehat otfinembeBofaonidenli(alwin
willbe ffeftd.lherequen(yf(on(odan(eor denti(.ltwinrngetfioml%to6
Thit ittdbutionontras$ithhat fmendeliannhe an(e,inwhi(hideaticiltw
thare dkorderuato ingle utantene.
5. Ihe rhl of rc(u[en(er increaredhenmultipleamily nembersre af{e
therengtaneale oftenhe mortproblenatkor dirtinquirhingnuhifactol f
mendeliantiology.simplexanpl€r that he igk frc(ufienceorunilaterale
and alates496ora(ouple,ithone ff€ctedrildand nsea'tr o 996 ith rvoaffe
d\ildren.5, Theiikof eorren(e ay e nater henhedisodermoreevere,henfant h
long-tagmentlirsdlrprungireaseas greateran(e fhavingnaffe.tedibling
the nfant fio utshort-regmQntiuchsFungieease.
There are two cypesof multifactorial traits. One exhibits co
tiriuous variation, with normal defined by a statistical range, a
outliers of that range, usually two standard deviations, are co
sidered "abnormal" {intelligence, blood pressure, heigbr, he
circumference). Offspring represent a modified average of th

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 15/177
Ch|[to.8o . P.ttornsol Genolic ransmiision
Aminoglycoside-inducedeaf ess12S RNA
s€nsorineuraleatness (A1555G)
12S RNA \ \(A7445G)
\v. l 12s
T
P
I\,1ELAS,PEO 16 5IRNA'E' \
(A3243G) \L
NDl
t Q
M
ND 2
ND 5
LSH
Nna - NADHdehydrogenase" Subunrt
CO 11 G(Arg34 0His)
A6
'NARPand Leigh iseaseATPase ubunit
(Leu15 6Arg,Leu 156Pro)
c o l
co A8
S
D KI
I/lERRFtRNALY"
(A8344G,T8356G)
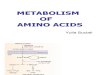
Figure 80-12. The hurnan mirochondrial DNA rnolecule,showing rhe tocation of genesencoding22 rRNAs, rwo rRNAs, and 13 proreinsof the oxidacivep
phorytarion (OXPHOA) complex. Some of the most common disease-causjnBubstitutions and deletions n the mtDNA genone are also illustrated. OH
OL are the origins of rep)icarionof the two DNA strands, respecrively;12S, l2S ribosomal RNA; 165, 15S ribosomal RNA. The tRNAs are indicated b
single etrer codefor rheir correspondingamino acids (e.9.,L for leucine,K for lysjne).The 13 OXIHOS polypepridesencodedby mrDNA includecompo
of complex I: NADH dehydrogenas€ND1, ND2, ND3, ND4, ND4L, NDs, and ND5); cornplex [: cytochrome 6 (Cyt ,)i cornplex V cytochrome c oxI, or Cyr c (COI, COII, COn); and complex V ATPase6 (ATP-6, ATP'8). SeeTabl€ 80 I for representadve iseases.Adapted from ShoffnerJM, \gallace
Oxidative phosphorl.lariondrsease.n Scriver CR, BeaudetAL, Sly wS, er al [editors]: Tbe Metabolic and.Molealar Basisof lnheti4d Disease,Tth ed.
York. Mccraw-Hrll, 199-9; nd Johns DR: Mirochondnal DNA and dise se.N Ensl I M?i 1995;333:638-544. Frorn NussbaumRL, Mclnnes RR, Willard
Thomfrson 0 Thoh'bson Ceneti.s in Medici'e,6th ed, Philadelphia,WB Saunders, 001 )
Fisu.e 80-11. Pedigree of a mitochondrial disorder exhibi.ing
marernal nheritance. Btu€, affecredPatient.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 16/177
DlStASt PI{EN0IYPE M05I ntQUEllT UTATlotlll MTDNA,!ott(Utt Holtl0PLASMYvStftnoPrAsMY l]HfRITAN(t
Leba! e'ed;rI.rtir neu[rFih.v
icLrt e eectmrranslortctiinjot'retonrpr
n 55en5eru.a rr5
NANqeqh 5ea5e
METAS
5m > PARTX 4' HumanGenetics
l,tumpath!tax ret t , qmenl]!i,Eveloprnil Po imJtalionsnAlh5e . ir 16qene |]eteropsr l,4atena
dea); , ienta.a ai01 ct i i ai l . .mi
,1.1ahoncrlpni.phalom/olitii;ldrt ,( d0! , rnd Poifim aiionn q:iA" |].teropsft Matemal
nrokelikep odei;nav ar n cn ardirbetes
rne I'J5MERBf ,{1!oc)nrr p Fy' ,rqqed€l] lbersf mu5rle,tax , Poifim taticnn R\A' |]etfi0psh Matema
!ensoreuraledlxe!
Deafnei! rroq|e!!'ve5en5orcuralean.'55,oftencLtedy A15556inut]tonlT5rRNA |]0roplasmii L4atena
am oglrc5ident olcs
llonsyndrom5en50reuraleaFnesj(hmni(ror_tresl/e {sna ?:ogrl]s!:vehraines5le)lta0(urmu(ej
cphthalmopeqraaPl0)
Ai445Gutdton ll! rRNA |]olropl;s mi.
The(ormonIELASclr irJta1i0nn RNA arqp |]eter,lpa5mr
0clProirsi .niaro 55
PBa6cnynCmme
L4atel|a
L4atenJpc1t
t rLi l i0n5
5po,adromatr L
!pordc5onati.Lri
Panxeaii(n5ufticiet\ipan(ylopen, (( ardolj Larqee lron5ielercpla5Tiiearnsryrl incomeK!5i Pi l ]ofei r lonserLlr lhhe, t rtb0(k.relnagmetal icn h. k5 r_cee t n
| , . imN-'bz[ IRL'! t | i |$iR! ' lLidt | i 'et |o| \ )|h|N\0, ln|11h'npJrn| : |4l l r.J] i ,1cf6€,5rh?dPhadehh,r\ ' l8rd| [ ]0] ,p;46
p a r e n t s ! wi t h l t U t r i t i o na l a n d c n \ .l r ( D m e ] 1 ta l i a c t o r s p [ ay i l r g a n t r i L l t r ri o r l | l i l b i | i t y
inportanr role. popuianorr. Lrdivjdurls wh o cxceed a thrcshold liabiliry
l(ith other muLrifactorial rl irs, thc discinction )er$-cen onnel affectcJ bi the treir.
anclabnormal s clearer pyloricsrcnosis, curirl uL)e lefect5,(Jn-' l 'hc
h.rl-rLr..hrnr.rr ' grrr.rre nnd Lvir()nlnental actor
gcnitalheart dele*s, al<l cleft l ip, clefi palacc). Lrchrarts ollorv clenronstratecll neural rube defects.Cleneric acrors are ima fhreshold nodel (t-ig. 80 l6). Thcrc is postulareclo be a clrs- cated bv fhc increascd ccrrrrcnce isk for partrrts of ln affe
DIsEAST
Category
iluxInqlDn51:aja
lpni i r i bulbi ,r! (ul i r: t ruphy
5p orereber trxa iF l
5pnorereber tJra lpr2
Sp otereber rirxnlE.l
iMd.hddco5ephs€a5e)
5p o,:ereberdtax,rlp€6
5p o(erebelirtaxa tpe
tp notereber taxa ypel
Defi;t. rbrala co rirdrl
aircpfy/|]ir ,rarl"ndrfle
Gtegory2
P5edoa(fnd'rpi5a/nrIe
erPry!e;Y, l ] i i r
0(uloiha'ynqeal J5(Lrr JlrrcphI
I erdotlardilpaja
9ynpol)da(I'!
tategorY3
L'ryotcndlslropflDl,1ftr,rmc5rme9)
Liy1rhn.Itrcthl Dl"1]:
drr,rml)itnrclFrednh atarD
Fr;rqrle: !f di.re rFAXAl
lrdqile PllAXf)
!t norarcbi]r tirJ rypc!t)noaireberr raxa pc ll
5rnl]rer€beratra rype2
Prcgrej51,e)',rcf c ep :p5l'
tIlre
0$(ntPTt0N
Lo55fr0otor01rc1,derenta,aff$llyf5orcer
Ad',ri n5etrlolor'r.'rroleaieas5o(aRdr:h
anrlml lenn5eBl, l t i
ProEetsivera.\ii,lsa"hr , )'5Teir
Poqrer5iveraxia,yldthr l
D)A n , i5Lrlmr5iur; t roph)la.ar,erte a
opr ln2mopeqraPogre!srrl]::r;,dysanhr,ny51iqfl5
ProgrelsiwiarE,dlsanhra,rctna?ceneratr0nPmqrpssNflrri;, emenr, Bdyke5L,dismet(a
[erbclartophIaiaria,tc( ni( pep!)1
chorenatletosi5,emenl
5ho[ Lilne,Jointxrt!, Eenerilive0n,di5e,re
Pro{qa irnb e;lne5t y5pfqia,r0!i5
Sh0fr5tdtJr,open5k!r ture5vr-hbulq lngcallara rv udrhyp0pa5.,h0r1€ned
ln!eI'derta nomalies
Pcyda(tyl/ancj'nda.ryl
l/,15t1055.adaarfi!'1hr ,catira6mntil
balClly'rsr osi,G'd;adr!'1hl'1,catrratt5,tonial
baliingPrcqresli\rmbaiaria,dysanhr, ype(ophrl
c,rrc0mFpalh,{pycmdae;kne55eqs
lvientaetdrdal0n,igee,rfinc,ar]j,f'ric'corahidr\mma i
lvld nefia r.crditof
AdJ cn5ettar ,Ct5,lrthr, ny5taqmusAiaxiaff eIurc5
ACXE,eyaofirnentcclc€r5,7a-;l]aq? l
cn5et
l I rel i re r\ . "1t01vt0n5,myDinr tdeFen
PAREII]NWHOM
EXPAIISIONSUAtTYCCURS
|!broien rolqh iherlb e1rjtenhrorqhaihel
i c€.t|rn hroLrghather
[hr rflenhrouqhithef
i,1crefleIh,ouqhaihcf
ibr olten|ot|!halhel
LOCAlIONf IXPAN
Exrn[r]n
Exirn[xcnExcn
ExoI
Exon[xcn
REPEAT5tQUEE
iAGiAG
iA6IAGtA6
tA6r-Ac0c
GA '
6ar:[t6, r:l6iA
6al.,C(lGarl
o6
afla
NORMAIA 6I,
AENOR[4ATAfiGE
6l4, l r i 100. 'rroi l
| 14,40 l
6 l 9 ; 4 ' S 1
r! 29,15 9
1i l6;68 t
4 15)", )r-
7-l5tl8 /ila29 4l ;4755
i' 25;49 8
i: 6 I
6 , i ' , 1
li 2l (expi|.in b5ered
n 01? lr1 l
15i22 5
5 17;100o5e'.irt
</5t75 l,l0r'r
)j ),1009il0 no-e
6 52;100.000! 'mo,e
6 15;>100
l 6 l 7 ; 1 0 7l /
l r ' 6 ; 8 0 0 5 0 0
,r l8;66 S
Fxon
l 'untr; rsJtede! r
l 'untrJn5ateleq 1
5 ' u n t ; r 5 i t e l{ o l
5'un[ ; f5arclcq]r
l 'Lrntr: f5atedeq n
lnfrox
J'untraIJtede! n
5'IntEr\aleilc! ]r
Ircn
Excn
[66
[(
irtheraren!bJtrpan5]1 o
a01lena 0mrlr0uqf 0thcr
Auto5onac.ei5veher.r1e,lljdseoreallei rri rnherrdfior1r0.n arli5
1r !5veIlhro[of lothPr
Ill]rcoftenlhiouqhrhl]r
l c|e henhrulh rothe-Ilcrirftenh,cLrqhilhef
fUI0t0nat(eii e nler?'rie,50
lranrm.ted,vb0.ha|eltr
06AJI'(A6
i. riidr ,B,l,rr!L,Ermrh;dirl,r\,i R ,r.1dmerrfr.,ldl r rLr L1]lU1llll5,p?

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 17/177
A41 yl
Figure 80-14. A, Myotonrc dysrophy pedigree llustrating anricipation ln rhis case, he age of onser or family
membersaffectedwrth an autosomaldominant diseases lower in rnore recentg€nerations.Blue, affecredparients.
B, An autoradiogram frorn a Sourhernbtot analysisof rhe myoronic dystrophy gene n three ndividuals. Individ
ual A is homozygous or a 4- ro s-repeat rllele of 175 repeats; his indrvidual has myoronic dystrophp lndividualC is also affecredwith myotonic dysnophy and has onenormal alleleand a disease ausingallele of approximately
900 repea6. (4, Counesy of Drs. Kenneth and Elaine Lyon, Universityof Utah Health Sciences enter.From JordeLB, CareyJC, BamshadMJ, et aL Medical Genetitr, 3rd €d. sr. Louis, Mosby, 2006, p 81.)
child compared o the generalpopulation.This risk is 3%, less
than what would be expectedf the trait was caused y a singlegene.Further emphasizinghe role of nongenetic nvironmentalfactors s that the recurrence isk can be owered by vp ro TOyo
Cho olm . Prnemsof Genelic lansmission
if the mother-to-be akes olic acid at 4 m9lday starting 3prior to conception-Another example s that a sequencetion in the nterferon egulatory actor 5 gene sassociatedafl increasedisk for cleft lip and palate.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 18/177
502 PAnTX r HumanGenelics
Nalure snurture
FiBure80-15. The progressive ecreasen the genecicoad contributing ro che
developmenrof a disease reatesa smooth transitron rn the djsribution of ill-
nesses n an etiologic diagjam. In theory,no diseases re completely ree rom
the influenceof both genetrcand environmental facrcrs. (From Bomprezzi R,
Kovanen PE, Marrin R: New approaches o Inveshgating heterogeneiry n
compl€x rraits. Med Genet 2003t4U553-559. Reproducedwith permissron
from the BMJ Pubtishing Group.)
HighLiability
Figur€ 80-16. Typical hnear erythemr and bliscering n a female nfanr with
incontinentiapigmenrj.As the child grows older, he skin lesionswill become
flattened,pigmenredstreaks. (Photographcourtesy of Mrginia Sybert, Uni-versity oI\0ashingron, Seatrle. romNussbeum RL, Mclnnes RR, Wrllard HFr
Thompson d Tbompson Genetics b Med.icine,6th ed. Philadelphia, WB
Saunders. 001.)
Many adult-onset iseasesehaveas f causedby multifacial inheritance.Diabetes,coronary artery disease, nd schphreniaare examples.
Allegrucci C, D€nning C, Priddle H, et aJ:Srem-ceJl onsequences f emb
epiLgeneticdeferts. Lancct 2004;364 206-208.Bomprezzi R, Kovanen PE, Marnn R: New approaches o rnvestrgating
erogeneity n complex tfttts. I Med Genet 2003;40:553-559.
Clayton-Snirh J: Genornic imprinting as a cause of disease. B
2O03;327 1121-1122.Gosden RG, F€iDbersAP: C€neticsand epjsenetics-naore's pen-and-p
ser N Engl l Med 2007;3561731-733.
Jacob S, Moley KHr Gam€les and embryo epigenenc eprogramming af
developmenraloutcome: mplication for assisred eproductive echnoto
Pediatl Res 2005,5 *437 446.
JacquemonrS, Hagerman RJ, Leehey MA, et al: Penetranceof rhe fra
X-associated remor/ataxia syndrome n a permutatroncarrier populat
JAMA 2004:291:460468.
Maher ER, Brueron L\, Bowdin SC, et al: Beckwith-Viedemann syndr
and assisted eproducrjon technology(ART). .l Med Geftet 2003i4U62-
Teebi AS, El'Shanti H: Consanguinity: mplications for practice, esearch
oolicy. IaRcet 20061367'9 7 0-97 1.
Clinicalcytogeneticss thestudyof chromosomesiheir structinheritance, and abnormalities. Chromosome abnormaloccur n approximately% of livebirthsand are esponsiba largeproportion of early fetal losses,multiple congenitalmformations,and cases f mental retardation.They havea sigicant role in the development f neoplasias.
Chromosomeanalysis s indicated n dre child with multicongenitalanomalies nd/ordysmorphic eatures, t is indicafor the pregnantwoman with advancedmarernalage >35yr)
is also warranted n patientswith (1) two major malformatiand/or threeminor malformations; 2) problemsn earlygrowand developmenr,ncludingambiguous enitaliaor mental edatioo; (3) fertiliry problemsor recunent miscarriage )3), sbirth, andneonataldeath; 4) a first-degreeelativewith a knoor suspected tructuralchromosome bnormaliry.
METH0DS F CHR0MOS0MENALYSIS. ytogenetic tudiesusually performed on peripheralblood lymphocytes; ultufibroblastsmay also be used.Prenalalchromosome tudi€sperformedwith cellsobtained rom the amniotic luid, choriovillus tissue,and fetal blood,or in preimplantationdiagnosisanalysisof a blastomere.Cytogenetic tudiesof bone marrhavean mportant role in tumor surveillance, articularlyamoDatientswith leukemia.
Chromosome nomaliesncludeabnormalities f number astructureand are the resuhof errols in cell division. Theretwo typesoI cel l division:mitosis,which occurs n mostsomcells, and meiosis,which is limiced o rhe production of gecells,
In mitosis, wo geneticallydenticaldaughter ellsareprodufrom a singleparentcell.DNA duplicationhas alreadyoccurduring interphase, o at the beginni[g of mitosis the chromsomesconsistoI two DNA strands oined together at the ctromere.Mitosis as oursrages:rophase,ne;phase, naphand telophase. rophases characterized y condensation f DNA. Also during prophase, he nucleai membraneandnucleolus isappear nd he mitotic spindle orms. n metaphthe chromosomesare maximally compacted and are clea
Low -
Environmentalffect

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 19/177
Figurc 8l-1. A, Centromereposition determining the rhree types
of chromosome seen n rhe normal human karyorype-metacen-
tric, submetacentric,and acrocentric.B, MorphoLogic landnarks
use{ul n chromosome d€nrification.
Chapter l . Cytogonolics
fi=ifuxSatellites
I- secondary onstriction-i
ttSecondaryonstrictions
ii.. l- /''1 I 1 6
B
I
I
l sfltt
Metacentric
Submetacentric
l AAcrocentric
vrsibleasdistinctstructures. he chromosomeshgnac he center
of the cell an spindle ibers connect o the centromere f eachchromosome nd extend to centnolesat the two poles of the
of two chromatids, n meiosis,a diploid cell (2n = 46 chromo-somes)divides to form haploid cells (n = 23 chromosomes).Meiosisconsists f two major roundsof cell drvision. n meiosisI, eachof the homologouschromosomes air preciselyso thargenetic ecombination, nvolving exchangeberween wo DNA
itrands (crossing ver),may occur,This restrltsn a reshuffling f
alleleson rhe recombined hromosomes. acbdaughtercell henreceivesone of each of the 23 homologouschromosomes.n
secondpolar bodn eachwith a haploid (z = 23 chromosomes)set.Consequenrly, eiosis ulfills rwo crucialroles: t redrlceshechromosome umber from diploid (45) to haploid (23) so that
upon fertiliza tion a diploid number s restored, nd it allows for
genetrc ecombination.Two errorsof cel l divisioncommonlyoccur duringmeiosrs r
mitosis,and both can resulc n an abnormalnunber of chromo-somes.The lirst is nondisjunction, n which cwo chromosomes
fail to separate nd thus migrate rogether nto one of the new
cells,producingone cell wrth two copiesof the chromosome nd
another with no copy, The second s anaphaseag, in which a
chromatidor chromosomes lost becauset fails o movequickly
enoughduring anaphaseo becomencorporated nro oneof the
trypsin-Giem which producesG- or GTG-bandrng, uniquecombinarion dark (G-posirive) nd Lighc G-negatrve) ands
Many other banding techniques and special stains includ
qurnacrrne Q-banding), everse R-banding), nd cencromer
bandrngl are available for use in certain circumsta
Metaphase chromosome spreads are 6rst evaluated microsc
cally, then thei r images are capcured by a video camera and sto
on a computer Homologous chromosomes from a metaphspread can be paired and arranged sysrematicall y into a ka
orype. The chromosomes are arranged by size n pairs, the lar
autosome being designated chrornosome l and the sma
chromosome 22. The sex chromosomes (X and Y) make up
23rd pair A description of the karyorype includes two or th
parts: (1) th e number of chromosomes, 2) the sex chromos
constitution, and (3) any abnormalities noted. A normal ka
otype is 45,XX for females and 45,XY for males (Fig. 81-3
present, abnormalities are noted after the sex chromoso
complement.
While the internationally accepred system for human chrom
some classificatron relies largely on the length and band
Daughter ells..> -oo
Miloticnondisjunction
ZySote\
..> -?tQfigurc 61'2. Formation of mosaicism.The X and Y chromosomesare
ro illusrrace wo common errors eading o chromosomaltyabnormal cell
ulations. In normal mitosis /topl, duplicared chrornosomes separate
become ncorporated nro daughrercells. f one replicatedchromosome
to separate,mirotic nondrsjuncdonoccurs zrtldlel. Occasionall-v,ormal
aration occurs, bur one member fails to misrate. This is knorvn as anap
l^E (bottom) (Used,wirh perm;sion, Iron wxnrewski LP, Hirschhorn
Glide to Huffian Chromosome Defec*,2nd ed. Whjre Plains,NY, Nlarc
Dimes Birth DefectsFourdation, Birth Defects:Orieinal Articl€ Series, o
'ec 6. 1980. )

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 20/177
504 PARTX r HumanGenetics
of the 24 differcncchtomosomepaints s labcled$.irh a clit fe
coflbinarion of the -i f luorcscentdyes (u'hich cmir ar diifcn'avelengrhs). lch oi th e 2. 2dutosomes.nd the X an d Y crnosornes ave fheir otvn Lrnique pectraof \\ 'avelengths f fresceDce. pecial i lfers.clnteras, and imageprocessing ofrwar c requireclo iclcnrif.vach chromosonrc.SK Y and M-Fl5Hespeciaily useful for rdenrifl'rng tire complex chr{}lDosrearran[jemcntsoLlnQ ll manv tumors.
Comparative genonrich,vbridization CGH) is a FISH bmethod fhar call be usedas a Henome-&'idecreen () neasur
ierencesn copy uLrrnbcr f a particular )NA sequence r cmosomirl segmcnl beru.cen u'o diffcrcnt DNA samples.tcchnique nvolvcs.li lferenrially abelin!ipatrerltDN A u'irh a
orescent le (green an d normal reference )NA rvirhanotheorescent ye (red).F-qual mounts of the tr,vo abelDNA sa|nare mixed and fhen lsed es a painting probe for FISH r
nornal met.lphase hromosolllcs. he ratio of grcen o red ffescences measured long cach chromosome.Regionsof amfication of patient DN A u,ouJd ciisplay a exccss oi gliuorescencc,vhi lc regrors of loss of paticnt D\A rvould sexcess ed f luorescence.f parient and control D^_A are eqlreprcscrltcd, hc green-to-red ario would bc 1 : I rnd th c cmosornes \\1)r.rldappear yellow
High rcsolrrrion (-(iH-bascd microarr:rys (alrlv (l(lH) hth e probe preparatioD hrt is dre same es rra(lit ionel CGH,
rether thrrr hybridizing th e probe to rnelaphase hrornossprcads, arge' inscrtclones (such as bacrerialart if icidl chro
somcs; lACls) pottedon nicroarrays serveas rh c targcr. hc
oluoon of array ( lGl l is Limited nl _v y thc sizeoi thc inscrt
thc distancc bcrrveen lones, vhcreirs hromosomc CCH h
resolutioDof only -5-ltJMb. Targeredarray basecl lGH is
Ijgu.c 31-3.(arvotvpcf norrnalnale ithchronrxonresn ht e prophxre.Lhc hromosomesre onger,r|rd greirer unrb.f oi b^ndsft.s.endrtrn
wherchronxxomesrephorogrephcrlr nrcraphrsc
pattern of each chrol' lrosome.he posif ion oi thc ccntromere el
atir.c o fhc cnds of rhe chromosomealso s e usetul distinguish
ing Fcature (scc fig. l l1-1). l 'he centrrnere divides rhe
chromosornc n trvo, rvirh the short arnr designared s fhe I ar mand rhe ong arnr designated s rheq ann. A plus or minus signbeforc the nrLrnbcr f a chromosome n(licafes haf rhere s ane\tra or nlissing chronrosome, cspcctii,cLy. aLrlc ll-1 shows
somc of thc abL)re\'ranons sed or the descnption oi chromosomesand rheir abnormalit ies.A rnccaphaschromosomcsprcdd
will usuallv shorv.150-500 balds. Prophase nd pronefaphase
chf(rnos(xnes are k)nge! are less condensed.and ofren shorv
500 850 bands. High resolution analysis s uscfLrl or dercctirg subtle chromosomc abnormalirics he r mrghr ofherwisc l jounrecognlzcd.
The fluorescencen situ hybridization (FISH) rechnrques uscd
ro ideLrrify he presence, bsence,or rearrangemcnrof specif icDN A segmenrs. ISH involves using a unique f)NA sequence
labelcd rvith a f luorescent d1e, rvhich is exposed ro single
srrandedDNA on a microscopeslide-Th e probc pairs rvirh i ts
complementarl D\A scqucnce nd call be visualizedbv lluores-cence mcroscopy Fig. I | 4). In interphase cLls. hc number ofcopies of a parricu)ar f)NA segment can be dcrcrmined. Innletirphasc hromosome spreads, he number of copies of theDNA sequence s \ 'ellas he exactchromosornaLocation of cachprohc copv .an be documenfed.FISH is particularlr uselul forderecting erl. smxll deletions hat might escnpe olicc wirh C;-
band anirl-"sis.{r i rh high-rcsolutionchromosome anal,vsist isi 'ery dif l icult to rccognrze elenons ess hal 5-10 miLlion hasepl irs {5 10 \1b) in sizc; FISH can reLiablt derecr delerionsas
small a 1 Nlb. This has allorvcd checlinrcalcharacrerizarion f a
number of njcrodelcrion svndromcs. n addrtion to laenc-or
locus specif icprobes.complex mixturcs of DNA from irne part
of a chromosomearm, an elt ire chromosomearL-n, r an entirechromos()me re available or f luorescencerainingof largechromosomeseclions r entire chromosomes- he prohe mixturcs arcrcfcrrcd to as chromosomepaints (lig. 81--5).
Spcctral aryotyping (SKY) and mult icolor FISH (N4 FISH) aresimilar molecular c-vtoljencticechliques that use.].4 difterentchrom()some ainting probesand -5 luolochromcs o simuirancousJl' ,Jsuali zc velv chrdnosome in a metaphase pread. -ach
\
.l6
tq
r t
l iE a l
l 8
"
f . li . I t l ; ' r .; ; i i ? lr i i : : i f t
7 I 9 1 0 1 1
i l . :r a G li . i I a r t J
. j i ; : t ' t
: ,
3 1
9 ){ ,; l
6
! ta a
t 3
f :1 9
1 4 1 5 1 6 r /
' aa l
20 21 22
XX Female
IY [,lale
l i i l Nurnber{ tot(e 5
ten [ef0ome0del Deetion
der Dervaiive
dJ! Dup,ld1ron
nJ Inse{on
nv Inyercn
eh Lr'euphaseilsP
i,l( 5h lnterphasels|]
nat L,laer
m05 lrmia|{
c0NDm0tl
lla'malema hr',1]i,ne
Nordlrale a'yotype
NJmberfr e 5 ed(h1]
5epardteine' fdone5ftmalewrhr omy ll\ ale /th oonosoml'l
kf
+
5hortamrLonqrnRinq(hmmolome
Ilansloction
Termninal5a5htuin fL0s5l

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 21/177
Chapter8lr Cnogenetics
ChromosomalNAon sltde
Denaturaln
-- ,r-
cGTT _ A
A _ T
c - G
A _ TcG
B
-
Renaturationi lhtluorochrome-labelled
DN Aprobe
c
TT
Gc
cG
Probehybrid ation
D C
o n c i r g e n t t i c s l i d e p r c p a I , l ] o n s 1 A ] i n t o s i l r g l e - \ t r l n d e d D N A 1 B T h t
c o p i e s o f a s n r g ] e s r r J n C | e d , i l u o l l c h l r n r e L a b e l e d D ^ v A b , l s e p [
BangsCl), ct al : FISJln
Dtsaf t lercn At lolesrents rate f rhe Art Rerlews Adolescenr ' lerl ieinc ht ladelphLr, rnler an d Bel fus, 002,pp 105 i1. ] )
2 ] - s p c c i f c p r o b e I h c 3 r e d s r g n a l s n r a r k r h e p r c s c n c e o i . ] c h r l n o y m e s ] 1 t . } I s H e n a 1 v s r s o f a r r r e r a p h a s e c h r o m r l v l l c s p r e a d i r o n l r c n i c a |
rndlvrdual using a rvhoLc-chromosome a
Chromosome ilhfluorescentprobestgnal

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 22/177
5m r PAnTX I Human orelics
NormalGhromosome21.8
1.51.2
0.9
0.6
0.30.0- 0,3.0 .6
- 0.9- 1.2. t.5. {.8
DiGeorge yndromedel(22Xq1.2q1 .211
0.30.0
.0.3
.0.G
.0.9
.1 .2
. t .5- 1.8
Figure 81-5, Representative rray CGH plocs rom a norrnal control and frorn an indMdual with the 22q11,2 deletior seen n Diceorge syndrohe. Each c
is arranged along the *-a-'ris according to i* LocatioR on the clEomosome *'ith th€ mo6t distalhelomeric p-arrn clones on the left and the most disraVtelomq-arm clones on the right. The blue line plots represent the ratios from the fust slide (control Cys/patient Cy3), and the pink plots represent the ratios obtai
from the second dide in which the dyes have been reversed (pati€nt Cy5/control Cy3). The mp panel is a norrnal plot for chromosome 22. Th€ lower plo
fron an individual with DiGeorge syndrome ir whom clones in the critical del€tion region a-redeleted (dt/ou). (Plots cou{tesy o[ BA Beiiani and LG ShaSrgnatureGenomic Laborarories,LLC.)
ocE=
ooGt
tJ
6coo-
ooGu
I
,t.81 .51 .2
0,90.6
effective and efficient techniquefor detecting cryptic chromoso-
mal aberrations, hich rnaybe an mportantadlunct o FISHandconventional hromosome nalysis Fig.81-6),
ABNORMATMESFCHROMOSDIIIE{UIDERAnsuploidy nd Polyploidy. uman cells contain a multiple of
23 chromosomesz = 23). A haploid cell (n) has23 chromosomes(ovaor sperm) . f a cell'schromosomes re an exact multiple of23 (46, 69,92 inhumars), the cell s referred o aseuploid.Poly-ploid or heteroploidcells are euploid cells with more than thenormal diploid numberof 46 (2n)chromosomes, hilepolyploidconceptionsare usually not viable, the presence f mosaicismwith a karyotypicallynormal ine mayallow for survival.Abnor-mal cells hat do not containa multiole of 23 chromosomes retermedaneuploid ells.Aneuploidy sihe mosrcommonand cUn-
ically significant ype of humanchromosome bnormality, cc
ring in at lea6t3-4% of all clinicallyrecognized regnancieTiiploid cells, hos€with three setsof chromosomes3n),
viable n a mosaic orm. Trioloid inlants can be livebornbutnot survive ong. Triploidy ii frequendy heresultof fenilizatby fwo sperm dispermy). ailureof one of the meioticdivisioresulting n a diploid egg o! sperm,can also result n triploiThe phenoqpeof a triploid conceptiondepends n the originthe extrachromoso$eset. f the exua set s of patemaloriginwill result n a hydatidiform mole.Those hat have an extraof marernalchromosomes re soontaneously borted.
Aneuploidies suallyconsistoi monosomy nd risomy.Monsomy,which may be completeor partial, occurswhen only oinsteadof the normal two chromosomess present n an othwisediploid cell, n humans,a1l omplete utosomalmonosom

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 23/177
Chapler 1 . Cytogenetics
appear ) be Le rha l a rh in deue lopm enr ;u rv iva l s poss iL r l . ' i n
mosaic orms, An enccption s monosomy for fhe X chronlosonte
farlure of chronosorres to disjoin normally durtlg mcit>stsse e
Fig. 81-2). No n di s r.LnctLonan occur durilg mclosis I or l l or-
dur ng nirosis. Aitcr meiotic nondrsjunction, hc result inggrnlctc
eirLreracks a chrornosome r has 2 copies, esult ing u e nrttncr
\ r m l L , 1 ' i n ' r n l r \ B ' , r e . ' c ' l \ l ' l l \ ( l ! ,Trisom,r., haracrcrizccLr the prcsclce of 3 instead ol thc
cel lsor ir may bc in mosarc orrn. N'{osrndividuals ' tth tr strrnr
exhibit a consisrcntand spccilic phenolypc depen<1irrgrr thc
chromosonrc nvolved. FISH rs c()mrtonly r.rlcd r rhc l)rendreLdetectionof fetal aneuploid,v nd rn tLre apid diagnosisof neu'
borns suspectcd o have a crtsotny,
Th c major nu c'ncal lisordcrsof chromosonres re -l rtLrtoso-
rn l l t r i so rn rest r i l om y l , u i son ty l l , t r i som y 3 ) , and 4 f l pes
of scx chrcrnTosornal neuploidics:I irrner
s,vndrone iusuallv
45,X); Klinetelter s\ 'ndrorne 47.XXY); 47,XXXr and'17,XYY
B,v ar the ilost conmon type oi rrisun-v n livehorr infants is
frisonly 21 lkaryotypc 47.XX,+21 or 47,X\+21) or Dou'[ s-vn
drome.' lr isom-v 1li irncl risorny li are also rclativeLY ornnlou
and are associared ' ith a characcerisricer of congcnital r[onr
al icsald nental rctardarion (Tablc t1-2).l)own syndrome s rssociated vith cognirivc mpairncnr en d
characterist icacial and orher dtsnorphic fearures Figs i l l -7 ft )
81-9). Affecred ndividLrals re nore prone to congcniralheart
defeccsatrior.entricul;rr eptaicletecrs, cnrrtcuLat eprdlciefects.
isolared ecunclum trial scpraldefecrs, DA. rerralogyoi fallor).
sY[DRo
Tr50myl,PataLl
5yndrome
I[ 5omy8, dmri]s
iyndrcme
[{cDt}tG
1/10,0{00fth5
l/6,000hs
Ir 5omy,mo5asm l /20, 000ifrh!
(trilt(ALANtFtsTAIt0lrS(leftlo lfrenmdlin,otflexednge6wihp0/da,:1y,J4tua
hypoteorm,bulbouroJe;w e tmalfomlpdar9
abn0Imakur;(ercbrdlfralfomat0n,e5pe
holo | ) ro5en(eohay;nrrophf l d,cdrdra(maf
icalp ei?cB;hyp0plrsrorab5enbs,vi5(erandgeni lalafomale5
Low thwl:igh[,c05edstiwlrrndex nger\€rapp
ld cal
andhe th 9{ cvrddpog he th, arcw
\rft |m pi labdLjctrcn,5hoernum,r0rker-bo
1r(mrepl;)' , romenicdput,m oqnath, dbc
r€namaiomaton5,dndmertactrdat0n;95%0
are than he l yr
Hypolonia,atlace.upl/lardxd dntedalpebiass!e5
epicinthfolds,speakledrue5Erushield$0n5);$rdeEeesi nentalandm!Vthiardirof;dysp! cf
Flv 5,l:adDr alfomatirnr,andinanredse;sh
handl,hyl)opgiafnr dle haanIi5th ing4du
aftesa,a"dqhar(hedaale:596fpatient5!rthDc
tndromerehe esull0faft!solntcn (l4q2lq
(l5q2lq),and{llq2lq)- i wi ch he hen0t}Ts
s,rmes ruomy?1own/ndmme
Longa(e,ghprorheqlorehead,\{,ideprurnei0jer
everted0llrPl ,mlooretruqnalhia,wsettars,gh
arched,50metme5:lell a te;0iteDdrtcufanornd
(0mm0n,mooetaleenla lanlit n
Ir5oni r,Down5yndlonr
t/5cc 00Dtnnl

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 24/177
500 PARTX r Human enetics
Figure 1-8. Characterisri cerrnal anerns f thepalmof a childwirh Downsyndrome, single lexioncreasesirnian rease), xial tlnadills (anol!) indislalposirion, patrern rea n rhepalrnbetweenhe hird and ourthdigirs,andulnar oopson all 10disjts. FromNussbaurn L,Mclnn€sRR,WillardHl Thoftpsob6 TbonpsonGenetics Medkire, 6rh ed.Philadelphia,rBSaunders,004, 160.)
gastrointestrnal anomalies, leukemia, Alzheimer disease, mmune
dysfunctroo, hypothyroidism, diabetes mellitus, ard problemswrth hearingand vision {Table81-3),Most maleswith Down syn-
drome are sterile; some females have been able to reproduce. Indi-
viduals with Down syndrome often bene6r from programs aimedat stimulation, development, and education. They also benefitfrom anticipatory guidance, which establishes the protocol for
screening, evaluation, and care for patients with generic syn-
dromes and chronic disorders. The lile expectancy for childrenwith Down syndrome is approximately 50 yr,
Down svndrome is the most common chromosome disorder
and the single most common genetic cause of moderate mentalretardalion. The incidence of Down syndrome in live birrhs rsapproxrmatel;r 1 rn 750; the incidence at conception is more
than rwice that rate, The occurrenc€ of tr isomy 21 as well asother autosomal trisomies increaseswith advanced maternal aee
12J5yrl. Due to this rncreased isk, women at thir age should 6eoffered genetic counseling and prenatal diagnostic tools (serum
screening, ultrasonograph)', ammocentesis , and chorionic villus
sampling) [see Chapter 96].Even though younger women have a lower risk, they represent
half of all mothers with babies with Down syndrome becauseoftheir higher overall birth rate. All wornen should be offeredscreening or Down syndrome in rheir second ffimester by meansof 3 maternal serum tests (free p-hCG, unconjugated estriol, andc.-fetoprotein), Even more efficient, with a detection rate of 95ol",is a method of screening using maternal age and fetal nuchaltranslucency (NT) chrcknessalong with maternal serum p-hCG,
PA?P-A (pregnancy-associatedplasma prorein-A), unconjugatedesrriol. and o.-fetoDroteln. Increased levels of maternal serum cr-
Figure 81-9. Prehensile oor in a l-mo-old child.(Frorn
WiedemannKunze J, Dibbern H: Atlas of Clinical Syndrones: A visual Cuide to D
, 'osrr,3rd ed. Sr.Louis,Mosbl ;1989.)
fetoprotein MSAFP)are also inked o orherabnormal etalcditions, ncludingopenneural ube defects nd defects f thetrointesrinal ystem nd genirourlnary ystem,
In approximately95lo of the cases f Down syndrome hare 3 copies f chromosome 1. Theparentalorigin of the sunumerarychromosome 1 is marernaln 977o of the casesresult of errors in meiosis. The maionw occurs rn matemerosis (78%). Approximately 1% of individualsare moswith somecells having 45 chromosomes, hile anorher47
individuals havea translocation hat involveschromosomeThe majority of translocationsn Down syndromeare fusionthe centromere etween hromosomes 3, 14, 15, or 21, knoas Robensonian raoslocations.The cranslocations an benovo or rnherited.Veryrarely s Down syndrome iagnosedparienrwith only a part of the long arm of chromosome triplicate (partial trisomy). Down syndromepatientswithouvisiblechromosome bnormaliryare he leastcommon.
&

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 25/177
ChapterSl Cylogenetics
DISORDENARYO]YPT
l$omy 4],XX/XX+8
\lanlg 1/,XXIX'1,+9
Irsomy6 47,XX/XI+16
Tetrarrmy 7,XX/XX+(12p)
(Ltr{tcArAfittsTATroxs
Grorrh ndmentalell(ienryre arrablehemallrrtyfpaten15
diem05a,Ihe
ptesen(efdeepaknarfld dntarfu,ovA
lt (naEcteI5l:c
Ihen40r{ydi rtr€rti ar6 oeirs (l,licaicatuts rilrde(an0fad3hiqhoreheadmi(mphthdlm,lowrel dl[orme,l
ea6, ulb0,rsoielandkelelaj0ifi onraturea)altornalnl
dnd eJrt efecls6096)
Them05tftequenty0b5erven,ruto50nilaneLrploldyspontaneous
abonronsheeturenelsk nElige(rownd5Pal inerl lnrtndrome5paxelnierf frapharr ,
eldrcw5,nd ye ihe5,ominentoPhead,hubbyheek5,nq
ph1rurn h hDupperpdndrpd bowonfiqurdror
Polydacryand reaksfhyper/hvcop!rnenlationavee€f
reFrreo
I t is not possible o disr inguish he phcnotypesot inLli\ ' r( lua
u' ith full tr isom,v l ald rhose \ ' ifh a lransl()cetiorr. xtlcntswb o
are nosaic tcnd ro havc r mikler phcnotvpe.(lhrorrosome arallsis is rnclicatcdn indivrdualssrLspectedi
havitg Dou'Lr ,vndronre.f a rranslocarion s idcnril ied,plrenral
chromosomesrucljesmrLstbe periorrned to deccrnrrne vherhcrone ol the parcLrtss:t translocatiol cirrrier, vhich carrrese hrgh
recLrrrenceisk ior havilg another rifccted child. Thar parerrt
lnirt dlso have orhcr farnrly nlenlhcrs af risk. Trarslocetiorr
l-11;21) afriers havc r l{)0'ra reclr'rcn.c risk lbr a chromoso
nrallv abnorrral chiL,:1. cnomic dosage rnbalanceconcribures
through direcran J indJrecr arhwa.vs r rhc l)or'n syodrorne hc
notype and it s phenotlprc variatior.
TebLes81 4 arrrl l l l-5 providc urorc trrfotnrariol on othct
aneuploicLiesnd parraL autosomalancrrploidies l ig s li I lt) rrr
l. t - l.
ABNOBM ATIT IESTCHFOMOSOMETsUCIURE
Translocaiions. ransloclt ions, r,vhLch rvolr'c the tralsfer oi
rnltcri: l frrur one chrorrosonre o aLrofhcr, ccur wrfh r trc
quenc' of 1 in 500 livcl.or:nhunran nfalrs. Thq mav l.e inhcr
TRISOMY] Tfl150['tY8
I , 'l l r i , Facrr lappcarancc i .1 .ht ld wrfh rr l somy 13 (From Wnrrnn I l { . KnDrcJ,DibhenrH. ,1/ ld. , , /Ol t rtLLalyndromes: Ysual (
n, l ) r r ! !osrs . rct .d St l -ouLs, osb! . 1989
Headndira Sc;p efe.r5eq,(utiapldl ) Smaind rem,rturerppearanie
M lophlhdia,orneabnomar5 llghtpapebra55Lrnl
[kfr pa u dalen 6096-80%fci5e5 Na.mw05e]nd ypoplarna5dlae
Miiro(epy
llcrochtharia
5otn9 thead
Ho po5en(ephrlyft nen(ephaiy)
[ar ]4ry emanqnmas
Deafnel5fhesl Ccnge,r13ea ni5ed5eeg,/ iD,PDA,
and ICJrn0% fcae!
Th rpot teicrD5m!5nqib5l
Erlftmrte5 0vedaooq 0fh0qer5ndce5dincdactyy)P|)ydanyly
lypopd5t(d ,hypPrc,invera,
Proff entoccul
1,4oliafi a
l :el po r a te
Mlc|o(ephaly
l.orEenil hed( 5ea5e9,V5D,lA.
and !D)
5hl]nternum,smallrpdP5
Lr|red ipabdu. rof(l'rodacryind verappingirlE15
ndex\rr d, 5ih ver ,c iei h5t
ffoil3f-botomeet
Hnooast(Jr l r
[enerd seveftpvelopmenla]delaysnd nnaEl ser'erelve pmentael 5.rdprctur:
and rlsinarairowthetardalcn and stm(a rouh elarcalon
Refalbnoimalities Premdt,r,?th, 0yhyd?Tniosi i lcrcarpmlei t$rsineuvophrls fqJrni lorabdo|I ' , ] lhernia5
f ty t% veofger lhdnrn o 0n1y5%rwonqerrhanlwa'
nomhb.mdRt,(kqrirnl!1l?iJcnfJrflrrollftdr,rrfteiPh delphi,WB5r!nde62002l4i A5D,dLridepl;]
delerr,DA"aknLu(L!:rter 5ur5D.nmolirtla denr
rfed t 'rom a carricr parc t or i lppcar'de novo, n' ith ncr orf iected fanril\ ,mcrnbc. Translocationsmal, be elther recjpror roircrtsonian lig. lJ1 1,1).
Reciprocal translocations rrc thc rcsLrltof brc:rks l nornrokrgous hrornos<nnes,lth reciprocalexchange f the bro\egrrlents. larricrs oi e rcciprocal rransk>catiou re usuallyllorvprcaLl}'nornlxlbur.re lt irn rncreased isk both for misriagcdu c ro unbalxnced ccipr<>cirlranslocatior and for beachronrosoarallyabnornral olfsprng. Unbalanced rans]oca.| e rhe resLrlt f xbnoromlit ies r rhe secregatiortcrossovertreLrslocirf lonarrler chtonlosornesn rhc gcrrn ccLls,
Robertsonian ransJocationsnvoh'c trvo acrocentricchro5orncs chro[losorDes .], 14, 1.1.21,ancl22) that fuse neirccnfrorneric egion wirh e subsequcnt oss 01 the shorr elJecausehe shorr arrnsol r l l -5pairsof acroccntric hrornoshave mult ipLecopresoi gcLresor ri l,osomal RNA. loss of
!h(rrt rrrr of 2 rcr()cenrnc hronosonteshas no deletcriotLsfThe resulring arvotvpe hr s on1y,1-i hromosomcs,ncludingrrnnslocntcd hromosome har is macleup of rhe oig lrm ofrn'o tused hronrosorne!. )rricrs of Roberrsonidn ranslocairrc sua]lv phenof,vpicalll orLrel. lotvever, he,v rc at increrrsL irr niscarriage nd u bdlinccd aLrnormal ffspring.
Inversiolts \ lt xlversion re(lurres hJt a single cbromosbreak et tu<r poinrs; he broken piece s rhcn nvertedan d jo
llrt(J the s;lnrc chronr(Jsorne,nversioLrs ccur ln 1in 100
l>rrr lrs. hcre are t\\1) types of rnversions: e.icentric and p
ccntric. lr pericentric nversions, he hreaksar c in the trv<>
srtc arnls of lhe chromosonre rnd rrclude hc ccntr()mere..1reLrsualLy iscoverecl ccausc hc_v hrnge rhe posirion ofccnrromcre. I he bre:rks n palacentric nvcrsionsoccur i[

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 26/177
510 PARTX r HumEn enetics
Figure 81-11. Trisomy l8; overlapping ingers and hypoplasricnails- (From Wiedemann HR, KunzeJ, Dibben ft Atlds of Clinrcal Syk*omes: A visual C
to Diagnosis,3rd ed. St. Louis, Mosby, 1989.)
one arm. Carriers oI inversions are usually phenotypically
rormal, but they are at increased risk for miscarriages and chro-
mosomally a bnormal offspring.
Deletioffi ald Duplications. Deletions may be simple, wich a
piece of the chromosome missing, or rhey mav occur along with
a duphcation of another chromosome segment, resulting in an
unbalanced reciprocal chromosomal translocation. The latter is
r-:suallydue to abnormal crossover or segregation n a tra[sloca-
t10n ot lnvetslon carrlet
Deletions may be located at the end of the chromosome or in
interstitial segments,A carrier of a deletion is monosomic for the
generic nformatior of the missing segment. Deletions are usuall,v
associatedwith mental retardation and malformations- The most
comrnonly observed deletions in routine chromosome prepara-tions ioclude 1p-,4p-, 5p-, 9p-, 11p-, 13q-, 18p-, 18q-, and 21q
(Table 1 5 andFig.81-15). eletions aybeobservedn rouchromosome preparations,wich deletions and t ranslocalarger han 5-10 Mb usuallyvisiblemicroscopicalll'.
High-resolutionbanding echniques, ISH, and DNA stucan revealdeletions hat are too small o be seen n ordinarroutine chromosome preads.Microdeletionsare small chrosome delerions, he largesrof rvhich are dececrable nly wprophase hromosome tudiesand./orDNA probes.For sucroscoprc eletions,he mrssing iececan only be detected FISH or DNA-imolecular tudies.
The presence f extraSeneticmaterial rom the same hrosome s referred o as duplication,Duplicationsor partial (mental) trlsomles are less frequent than rvhole trisom
Duplicationsmay be sporadicor result frorn abnormalsegLion n translocationr inversion arriers.
Fisure 81-12. Trisomy 18: rocker-bottom feet lprotruding calcanei). Frorn V/iedemann HR, KunzeJ, Drbbern H: Atlas of Clinical $,ntuomes: A Visual G
t^ DMEh^<t<.rd ed.St .Lous. Mo\bt . lc8'

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 27/177
Chapter 1 . Cytogeneficr
Figure81-13.Male nJentwirh trisomy78 ar age4 days.Norepromin€ni
occiput,mlcrognathia, ow-s€l earsrsholt stemum,narrow pelvjs'prominent
calcaneus,nd ler.ion bnormalitiesf the ingers.
E
A
13 ta
Ids(13;t.l)
BFigur€ 81-14. A, khematic djj?.F/zm left) and panial G-banded karyotpe (ri8ht) ot a rcciprocal Eanslocarion between chromosome 2 (blue)and chromo
8 (pink). The breakpornmare on the long (q) arm of both chromosomesat bands 2q33 and 8q24.1 with the reciprocal exchangeof material between he
ative (der) chromosomes2 and 8. This translocation s balanc€d,with no net gain or loss of malerial. The nomenclature or this aychange s t(2;8)(q33:q
B, khenetic d|agr^m (W) and paftial c-banded ka.yorype (ight) of a Robensonian translocalion between chromosomes 13 (blue) and 14 (pink). The b
points are at rhe cnrromere (band q10) of both ckomosomes with tusion of the long arms into a single derivative chromosome and lo6s of the shon (p
mac€rial.The nomenclature or rhis exchange s der(13;f4)(q10;q10).

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 28/177
512 PARTX r HumanGenetics
\
cFisureSl-l5.A,Chi ldwi thvelocardiofacialsyndromc{delet ion22ql l .2).B,Chi ldwi thl r: rdeGVit l is,vndrome(delet ionl5ql l -13) C, Chi ld wnh A nge
syndrone deledon iql1-13). D, Chi ld ui th \ i l l ia mssvndrome delerion ql1.23). Fronl Lln RL. CherryALI, BangsCD. et al ; Flsrl ins for ansrver
use of moJecular -vrogenericechniques n adolescentmedicnc practice. n I{yme HE, creydanus D [edirorsl: Ceneti. Disoders in Adolrsrent' Srafeof rhe
Re' ie\r 's. dolescenr edicine.Phj ladelphia, an leyand Bel fus,2002, t 305-31i . )
N'Iicrodelerions ard microdupl ications usDally involve regions
rhat include several genes,so that the affected indivrduals have adisrrnctive phenotype. When such a deletion involves more than
a single gene, the condirion is referred to as a contiguous gene
svndrome(Table8l-7).
Subtelomeric regiofls are ofien involved in chromosomal
reauangements that cannot be visualized using routine c_litoge-
netics.Telomeres, 'hich are the distal endsof the chromosomes,
ar e gene-rich egrcns,Small subtelomericdeletions/duplicacions
or rearrangements translocations,nversions)may be relatively
common in nonspecific mental retardation wirh mjnor anomalies.Subrelornericearraneements ale been found in 3-7?. of chil-
dren r.r'ichmoderare to mild mental rerardation and 0..5% of chrl
dren rvirh mild menral retardarion. Clinical iearures >30includeshort stacure,microcephah;hypertek>rism, asalaod
abnormaliries,and cryptorchidism m males. Thrs group is acharacterized y' 'a iamiLy hiscory of mental retardarion andincreased Likelihood of retarded gro\4'th beginning in the pre
tal period. Both rhe suhtelomeric rearrangements and
microdelecion/microduplication yndromes are diagnosed
FISH or other molecular means.Insettions. Insertions occur rl.hen a piece of a chromoso
broken ar trvo poincs is incorporared inro a break rn another p
of a chromosome.A total of threebreakpointsare then requiand thev mav occur bet\\,'een llo or vvithin one chromosome
form of lonreciorocal translocation. insertions are rare. Insert

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 29/177
carriersar e ar risk of having offspring wirh delerionsor duplica-
t ions oi rhe rnsetted ellrnent.
lsochromosomes.sochromosomcs onsistof two copresof rht
same chrornosomearnl loined through a singlecenrrolnerealtd
lbrning rnirror images of one another. Th e most frequcntlr '
reported aurosomal rsochronlosones cnd b involvc chronro
solneswi!h sma]l arms. Sone of chcmote colnnr()n hromosome
arms nvohed in thjs formation Lnclude p,8p, 9p, l2p, lt ip, rnd
sornic or the genespresent n thc isochronosorne.
MARKER ND BINGCHR0MOSOMES. arker chrornosonres rc
rare and are usual[ychromosome ragmelrs tbar ar c f(x) sn]all c
be idenrif iedbv bondedc,vtogenericslhc yusually occur rn addi
t l(r1 ro the normal .1 6chrontosomes. ' lost arc sporadic (709i,);
Lnosaicisms often (.50%)nolcd becatseof th e mirocic rtscabi[-
ity of rhe marker chromosonle.The incidence n neu horn infants
is 1 in.l, l00. and rhe ncidencc rr ndividuals vith nrelrt ir l erar-
dation is 1 in l(10. Their phenotvpe rarlgesho m normal lo
s rve re lv bno rm a l .
of a chrornosorne re delcrcdand the endsar e he n oincd to f irrrrr
a ring. Depcnding on rhe atnount of chromcrsomc narerial haris lacking or in erccss (i i rhe ring is in cddit ion ro the nornral
chromosomes),a patient wirh a ring chrotnosolrte an afl)ear
normai or nearl-ynormal or may have mental retarc]arron nd
multipie congcnitalanorll.r l ie .
SEXCHR0M0S0ME NEUPLOI0Y.bout 1 i n ,100 ta lcs nd 1 rn
6-50 cmales hare some lorrn of sex chrotrosome abnlrrntalitr"(-onsidereclogerher, ex chromosonrc bnormaljtres,rrc he uosf
connron chromosonreabnornrlit ies seen in lireirorn rnlents,
childrer, and adults.Sexchromosorleabnorrnaliftes ln b.'erther
Chapter 1 r Cytogenetics
MRYOTYPT APPNOIIMAITI.I(IDEIJORDTR
Ki ehllerFdrcfire
IYYilndrcmeOtherorYchmmc4omeabnolnalle5XXmaes
Tumeriyndofire
TrisomyX
47,XXY48,XXXY0lher48,XXYY,9,IXXYt
m0$1rt47,XYY
46,XX
45,X
1/5/5-li ,000l,lar
li 50,000/80,000lvidb
l/80C ,0lllNb 5
I / 500,rld s
l/20,011[4alrJ
l/2,50J1/5,C00;ema
0lher hmmosomebnomtaiel
XYenae5 46,XY
Variail5nd rolai(s47,UX l/1,000emales48,UXXnd 9,XXXXXRarc
l/1,000malesl/20,000ulralet
stmcturaL or numerical and can be prcsent in all cells or i
rrosaic form. Those aficctcd rvirh theseabrrormaliriesmav h
r L u r r r r r , l h r , s r r , r l' r J c r c . ' p m e n r . r lr o h l e r n sl . r h l e l - t r .
TurnerSyndrome. urncr slndrome, a coldit ion charactc
Lrr rhr complere or partial aLrsence f rhe sccondsex chro
some. s definedb- va conrhinationof phenotypic eaturcs T
81 9t . Hrlf oi rhc patienrs rvirh Turnel syndromehave a 4chronrosorne omplelrrenf. he other h:llf cxhibits nosaicrsnrane.l stmcfural abnorrrir l ir ics oi the X or Y chromoso
I)arentalage s not a factor in the 45,X abnornahty; its vari
occur rn approxintately I in .5,000 ernale rve hirrhs. n 7-l%
prrLenrs, he lost chr()mos()mes of parcrrralorigrn, 4-5.X s
of rhc chromosorrc a[.normalit ies rrrost frcquentl,vassoc
rrirh spontancoLrs borrion. lt has been esrimared hac 9-5-9
ol ,15.Xconceprions rre rniscarrieclTh c phenotype irr rh e ncrvborn can includc shott stat
prr)rnrner!eirrs,ucbhing of rhe neck. and edema of thc ha
Dtttltoil
lpl65ql56p257q1'1.))
JY DNOMI
lpdeldion
-bto550%)
Axenfed-Riegel
8D1l
rype
9ql4 eeton
D6eoqe
Poro([-5haffer
ldoDsen
Pradef-Wii
Ar4eman
l5q2ldel..tlon
Fubin5rein-Taybi
sfiith Magerf
t{llerDeker
Al iqi le5yndrome
Ve (ardEfa(idDGeorgeyndmme
cL r(AtMAl, tSlAIl0N5
Growthretardaran,dysmorphr(fearurc5wlhflatndiabdqe,,rbrcrmaear,deep-iereyet0yergrohlh,acrocphaly,aqe andind€pl islinrtiwa(idlearures,ieftal isabilric5Arenfudieqeralfornrdton,eannqrs,r0ngenrlaearldefe.ttdent?n0ma5,develo!menhldeay5,fadal5morphi!$
RaUndfac€WithfL]LChe€l5ancipl'5teldtepafefn|r'$labhmL]5,5|]po\'J|V!ar.]0I| it5temmtalrtardatn,l ndpeBonalty
Kallmansyndrcme2,5phem(ylosr5,mLrtrpeongenrla,rnomaie5,mefiaretard,itron[,1i(rcepha, ewlopnrentaleld]5,SD.VSDulmonrrteno5i5,nqenibehdvclabnormater
pir tum. r,lpaotrudg a6,md en(a elalrjatn
Ilu ple ,]5ael(arclnomas,odontoqenrreratol:y(!dlmopantari$ , ( ficatonak erebr
DI l ln(facW]lh5/nophry5, lnlevaledndIe5'tentedupperiDprot |LldingtongUe,mrdfatehypopa5id,
l\/lanyofhpCiGeorqelndvelocardi0facalfeatLrres
Multiphxo5toses,nlargedareldlforamd,(dn 5yn0sfo5fucla ysmorDhi5m,e0c aid :ap
N}peinephromdlW|mslUnrol),anrda'ma|eqent i |hyoopa5iaoIvaringdegees,gonadob|a{0rna'on
0to!r5,e,rkedo3e,lowet corlyoimedun( s,menlaeiada{on
Meniand rowtterardat;oi,ordarnd qit nonrlie5,hmmboqlopen
Seterehyp0t0nratbnh,obesrry,5h0rtitatJrere5pon5iveoqrowlhormoI1e),s,naandsndeet,ypogoiladr'r, entalrcladaiicn
HypoIonla'fai|ha|I'midb(ehypop|a5d,pm9n.]lh5m,5ezUre5'jeiqa1axitm4emefl'unconI@llab|eb0U]5o
Gmu]lhtadaton,aked 05e,rhupperip,5mailhandsId e4ment]leladalron
l\,1.forephal)1tori5,eaked05e ithowlynq h Irunr,roadhLrmb5ndargelrs,mentaletardalr0n
Brachxephaly,drar lhrpopla5d,pralndthm,myop,deh a tg$o( alure,ehavoraroblem5,enDlretadat0n
l.,1(|orPph,r|y,i59enGphay,padygyra'nar|oWlofheadhyp0p|anicma|eeX|erna|ge01a9,9lot{hre|ard
Bkdu(paucqwf{ho|e5i ]55;heande|ec| l 'pani0|ar|ypLrmoadIydt teIyJteno5i5;o(ulalabncmaitelo
ru(h 5 unerllyeltebneinq 05e hbmad id-nole
Hyp1jpa5iaofa9ene5i5oi lFethymL]5andNrdthyroidq|a0d5'hypopd5iofaui(eandextema|a]drIy
5hoatiaturc,ehavrocioberns
Hypoion,dpvel0pmentildey,n0rmaior((eehledmwth,ptori5,dyspft tornas,abnormilea[,poinledhin
Du(henneuscurdystrophy,ltl1iipigrnento5a,adrenalhypoFla5ia,menbetrrdatn,gly(erclkna5ede6oenq
dthyosi5,ai in 5yndtorne,efa eudat 0,cho0dr0dy5Dtapun(ati
lUcro0hthalrna,Lnedrikindereds,p0rkl0dem,r,i:ooqenihlhedrtdefe(1s,sezureS,mentaetadatn
Spl l
8p2l
8q24ql4 l l
9q22
tt4l0pl2'plll l p l l 2 -p l4l lp l l
11q24lllqlel15q11'q1lar )l5qllq1 l ma U
15q21l6plll1/Q1111/pll20p12
22qll
22q1l.le t,orXp21'p2txp .) )lIl/t1 ltl r0llldlrr4 l- hPardet''I\Vl5)

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 30/177
51 4 ' PARTX r Human enetics
:|l0rtrlrture
Lonqenitdmphedemi
Paiela5oct cn
ncrea5edryinqanqle];ebcw
illaielLlrgef0rmiyrh0ndrcdysps cfdina dalep hy56)
[onqei : i lhdJc(aron5ro r5'y'/
de5preadpFe!5hedheet
Eedundantfui [ ,1( r uiproiy$i lE ]0rnd)
Lcw o5terrha ne
[oardal0nlao{a
Ei(u5pido' i {a e
Lardr ordLrrtonbnotrute5
Fyp()plaqi{Pir ea'irfdrorel
:0radaidt\!leire!ilinil'l)1pindrlamenorrhea)[0nad0bl{ lmal 'Yihomo5cFremrieridlpreserl )
Lean q b rrll]snonverbaaceprudcrornd 5105pd1:alk15ln 70%]
ie!eloprnentalea)"n 10%)
ioca dL!klvddre55
iypothyrcd5ma.qu,,.d15 l]-lr6)Ii0e2ddbete5el ur{riurn et6lal)ej
5trJbriLrj
[aia,r(
Red reenclcioIndnessa5n n; ejlReaurien:trtlm'd,l
serioxn.rn Parnqss
Inflamm?toryowe sei5e(, ,8(l i reasg?
a n d f e e f , ) t m r ) n c $ ' h o r n s a f c f h c n o ! \ . p i c a l l v r r o r m a l l l g . l J 1 -'|
61. Oldcr chi lcl rerr rnd adul ts have shorr s tacure anc l exh ib i t var i
able d,vsnorphr c ieatures. (i rngrni tal hcart dcfccts (40%) anr l
5 t ruct r r r i r l renai d.omal ies (607.) are coLunolr Thc most
connon heart defects are bicuspid aorr i c r ,ahcs. coarctat ion ol
th c aorta, lorric srcrrDsis) nd mit ral valve proLapse.The gorrrds
are gereral l , \ 'st re aks of l ibrous t issuc (gonadal dysgenesjs). Ihere
is pr imarv aurenorrhea and lack of seconclarv scxual characrer ist ics. These chi ldr en shoLrid recerve re l lu lar endocr inr>1ogic cst ing
isee Chapter 587). Pat ienrs tend rcl be of normal inrel l igcnce bu r
are at increased risk for beh ar. ioral problcms ancl clcl iciencies n
spat lal an(l mofor fercelron.(iuidcl incs for hcr l rh supen' ision
ior chi ldren u'rfh' l i rner sl rrdrome arc publ ishcd br' the AAP
Approximarcly l0% of pdtienfs wirh 4-5,X,/46,XYmosa
have extemal geniralLahar are crthcr ar.lbiguots or femalercmxining 90-9i' v i l l have nornaL appearin[jcxternal n1.rletalia. I his va.raLlf s esrirnared rcprssent pproxinately 6prrt icnlswith nrosricTurLrer _vndromc.om cofthe patienfs'Iurner
sl.ndromephenor,vpe nc la Y cell l ine lvil l exhibrr culinizatiorr. Phcnocyprc lnaLes rvirh 4.5,X/46,XY irosaihave a 15 .10')1,lsk of clcvclopine onadoblastoma. hc ris
fhe patients i ' ifh a nele ph.notlpe an d exfern.ll testes sso high. but funlor sLrrvcillarcc s nevertheless ecomrne
The A,A.P :rs ecornmer(Le.lhc usc of FISH anaLrsis t) L(x
Y-chromosorre mosaicism n lll 4-5.X patients. I i Y chrosornc mntcr rl is idcnrii ied. laparoscopic gonadectom
rccom m ct )oeo ,
\oonan syndromc s arr aLrtosorlal lominanrclisorcler usolnepatienfs 609i,) tr a rnulation in PTPN/, n-hich elcodnon recep to rv ros inc inase SL l l ' - 2 ) n ch rom oso r re 2q
Features onmon to \oonal s,vndrornertclr.rclehorf starureposrcrior hxirl ir rc, shicld chesr,cougenitaL eart discirsc,
sho r ro r r vebbed eck I lab le 8 l - -10 ) . l con f r r s f o I u rne r. l r r r r c .N , ' , ' r . . \ r , d n , n r cr i t c c r ' . , r h r r . ' , r ' d \ . r , . r d i i lpaftern of coLrgeniral eart diseasc-
KlittelelterSyndro e. F.ighrl-percenr i childrerr$' ith l(hn
ter syndrorrc hevc a m,rlc karyotype n'rrh an exfra ahromosX-47,XXY1 thc rcrnainlng 09i,havea higher grrdc oi scr cm osom e i l r l cL rp lo id r , 43 ,XXXI ' 18 ,XXYY; 49 ,XXXX
mosaicisrr 46.XY/.17,XXY1,or srrLrcrlrrall_r-bnorrnal X cmosomcs.Thc grcalcr rhc dnetlploidy, he more scvcre he seand rncntal impairnrcnt arrd dvsnlorphisrn. Indivicluals
5M[5tat",re
Fa ' reo hrive
tpcntha cidr
fuo\i5
nypenef!m
Low a5dlbrdqe
DoLlnladlanlinqa ebri5iu.€5r,lpp
\ynaqtrr$-0w-5elaLllaes
Denla dDrilLl5on
Lowosrerio,a r
Snorrebbedc(k
5hieliht5t
P€rius(ov3iumrGanaiumS(olosi5
[ub us aq$
PLironJfyalveteio!i
llypertrophkrdiomyocahy
Atdlseph elerl (A-iDl
lelriloqyf r ot(ry!rcrchrrSmal e is
Bhednq trde[, (irdng tromboqt
Nfrgi , l ,VtJ2004i1.51:12 2--. -12i8 oplr ighr O20r)4 \ . lassrchrLsc trs.{edr. : r locrei}Al l r iel i ts cscricf

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 31/177
Klinefelterar e male; his syndtome s the most common causeot
hypogonadisman d nfertil ity in malesand the most common sex
chromosomeaneuploidy n humans (seeChaprer 584). The rnci-
dence s approximarely1 in 575 liveborn males.Errors in pater-
na l nondisjunction n meiosis (MI) account or half of the cases.
pr()gnosis for testicular function. Although individuals with
Klinefelter do not have a reduced intellect. rle)'show deEcits in
language and executive funclions.
47,XYYThe incidence of 47,XYY is approximately I in 800 to
1,000 males,with many cases emainingundiagnosed, incemosl
affected individuals have a normal aDDearanceand normal fer-
I igencebu t are at nsk for learning disabilit iesan d hyperacrive
behavror
fBAGltE SITES.Fragile sices are regions of chromosomes that
show a tendency or separation,breakage,or aftenuation under
parricular growth conditions. They appear as a gap in the stain-ing- At least120 chromosomal oci! many of rhem heritable,have
bein idencrfied as fragile sites in the human genome (seeTable
80-1). One fragile site hat has clinical signif icances that on the
distal long arm of chromosome Xq27.3 associatedwith tbe
fragile X syndrome. Fragile X accounts for 37" of the cases of
males wich merrtal retardanon. There is another fragile sitc on
the X chromosome FRAXE on Xq28) that ha s also been mpli
cared with mild menral retardacion.The FRA11B (11q23.3)
breakpoinrs are associatedwirh Jacobsen svndrome- Fragile sires
may also play a role in tumorigenesis.
The main clinical manifestations of fragile X syndrome rn
affecred males are mental retardation, autist ic behavjor,
macroorchidism, large size, and characterisdc facial fearures.The
macroorchidismma y not be evidentuntil pubertp Th e facial ea
tures, which include a long face and prominent jau', become moreobvious with age. Females affected wich tragrle X shorv varying
degrees f menral retardatronand/or learning disabilicies- iag-
oosisof fragileX is possible y irs molecularcharacterizarion nd
by the observation hat rr is associatedwirh an expandedDN A
segment. The expansion involves an area of the gene thar con-
rains a variable number of trinucleocide CGG) repeats.
MOSAICISM, {osaicismdescribes n individual wrth 2 or more
different cell lines derived from a single zygote and is usuaLly he
result of miroric nondrsjunction seeFig 81-2). Scudyof placen
tal tissue from chorionic villus samples collected at or before the
10rh wk of gestationhas shown rhat 27o or more of all concep-
trons are mosaic for a chromosome abnormalitt-. !(/ith the excep
tion of chromosomes 13, 13, and21, compJete aurosomal
trisomiesare usuallynonvrable; he presence f a normal cell in e
early embryogenesis, osaicismmay be present n some trssues
but not in orhers.Germline mosaicism,which refers o lhe Pres-ence of mosaicism rn the Eerm cells of the gonad, is associated
with an increased risk for recurrence of an affected child.
PallisteFKill ianSyndrome,This disorder rs characrerizedby
coarse facies, pigmentar,v skin anomahes, localrzed alopecia,
diaphragmatic hernias, cardiovascular anomalies, supernumerary
nipples,and profound mental retardatjon.Th e svndrome s due
to mosaicism for isochromosome 12p. The presence of the
isochromosome 12p in cells gives four copies of 12 in the
affected ceils. The isochromosome 12p is preferentially r.rltured
Chopter8l Cytogenolics
from fibroblasts and is seldorn present in lymphocltes.
abnormalit iesseen n affecred ndividuals probably reflecpresence f abnormal cells dunng early embryogenesis.
Hypomelanosist lto. This entity is characrerized y unila
or bilateral macular hypopigmented whorls, streaks, and pat(seeChapter 652), Abnormalit ies of the eyes, musculosk
sysrem!and central nervous system may also be present. Pat
wirh hypomelanosis of lto have rwo genetically distinct cell l
The mosaic chromosome anomalies that have been obse
involve both aulosomesand sex chromosomesand have
demonsrratedn about 507o of patients.Th e mosaicismmay
be visible in lymphocyte-derived chromosome studies ; it is m
lkely ro be found r .yhen chromosomes are analyzed lrom fibroblasts. The drstinct cell lines may not ahvays be duobservable chromosomal anomalies but to single gene mutat
or other mechanisms.
CHBOM0SOMENSTABIIITY YNDBOMES. h.omosome nsta
iry syndromes, formerly knou'n as chromosome breakage
dromes,are characterized y an increased rsk of malignanc
specificphenot,vpes.They display autosomal recessivenhenta
and have an rncreased requency of chromosome breakagear
rearrangement, r,r,'hether pontaneous or induced. Thev r
from specific defecrs n DNA reparr, cell cycle control, and a
tosis.The result ing hromosomal nstabilicl ' eads o he ncrerisk of developrngneoplasms, he classic hromosome ns
ity syndromes are Fanconi anemla, ataxia celangiec
Nijmegen svndrome, ICF (immunodeliciency, centromere in
brlrty., and facJal anomalies) syndrome, Roberts svndro\ferner syndrome, and Bloom syndrome.
UNIPARENTAIlS0MY Uniparenral drsomy (UPD) occurs w
both chromosomes of a pair of chromosomes ilr a person w
normal number of chromosomes have been inherired from
one parent. Uniparental isodisomy means lhat che cwo chro
somes are identical, whereas uniparental heterodisomy m
rhat the two chromosomes are different members of a pair.
o[ which were nherired rom nne parent. l he phenorypical
of UPD varies according to the chromosomeinvolved,
rhepa
who contributed the chromosomes, and whether it is isodrs
or heterodrsorny, Three types of phenotypic eifecls are see
UPD: (1) those relared to imprinted genes, hal is, the absena gene that is expressedonly when inherited from a parent
specificgender, (2)rhose related to autosomal recessivedisordan d (3) rhose related to a vestigial aneuploid produ
mosaicism se eChaoter 80).In unipareocal isodisomn boch chromosomes (and thLr
genes) n tbe pair are i dentical. This is particularly impo
when the parent is a carrier of an autosomal recessivedisoIf the offspring of a carrier parent has uniparental disomyisodisomv for a chromosome that carries an abnormal gene
abnormal gene will be present In rlr.o copies and the pheno
wrll be rhat of the autosomal ecessrve isorderi he chrld ha
autosomal recessivedisorder even though one parent is a ca
of tha! recessivedisorder. It is esrimated rhat all human becarrl 5 to 8 abnormal autosomal ecessrveenes. he autos
recessivedisorders sprnal musctrlar atrophy, cystic 6brosis, clage-hair hypoplasia, cr- and p-thalassemias, nd Bloom
drome have occurred because of uniparental disomy'.possibil ity of uniparenral sodrsomyshould also be considrvhen an individual is affected with more than one recessivorder because the abnormal genes for both disorders coul
carried on the same isodrsomic chromosome. Uniparental i
som-v s a rare cause of recessively nherited disorders.
Matemal uniparental disomy involving chromosomes 2, 7
and l5 and paternal uniparental disomy involving cbromoso
6, 11, 15, and 20 are associated ith phenotypic abnorrna
ofgrou'th and behavior.UPD maternal7 is associatedwitha

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 32/177
516 PAnT t HumanGon€tics
J--- +-.'-
Figure 81-17. In pediBrees uggesrive f parernal mpnnnng, phenorypiceffects occur only when the gene s transmitred rom the mother but not when tr
nnred frorn the facher.Equat numbers oI matesand femalesare affectedand not affectedphenotypically n eachgeneration.A non manifesring ransmitrer
a ctue co rhe sexof the parent 11hopasseshe expressed enetic nformation; in other words, in paternal mprinrinB, here are "skipped" non manilesting em
notype similar to Russell-Silver yldrome with intrauterinegrowchresrriccion.Thesephenotypiceffectsmay be related oimprinting (see mprinting, below).
UPD for chromosome 5 is seen n somecases f Prader-!7illi
syndromeand Angelman syndrome. n Prader-Willi syndrome,abow 60o/" of cases ave maternalUPD (missingche paternalchromosome 5). n about 5% of individualswith Angelman yn-drome,paternalUPD of chromosome 5 s observedmissinghematernalchromosome 5). The phenotype or both Prader-!(illisyndromeand Angelmansyndrome n cases f UPD is thoughtto be due to the lack of the functional contribution from a oar-ticularparentol rheirchromosome 5. These indings uggesrtherearedifferencesn functionof certain eeions fchromosome15 .dependingn wherher t s nheritedroir rhemother r fromtbe father,
Uniparentaldisomymost ikely ariseswhen a pregnancy tartsoff as a trisomy.Most trisomiesare ethal,and rhe etussuryivesonly if a cell hne osesone of the extrachromosomeso becomedisomic.One hird of che ime, he disomiccell ine s uniparental.
Usually the viable cell ine outgrows he trisorniccell ine.Whenmosaic risomy ls foufld at prenatal diagnosis, are should betaken o determinewhetheruniparentaldisomyhas resultedandwhether he chromosomenvolved s one of the disomies nownto be associatedwith phenotypic abnormalities.There mustahvaysbe concern hat some esidualcells hat ar€ trisomic willbe presenrn some issues,eading o malformatiols or dysfunc-tion, The presence f aggregaresf trisomiccellsmay account orthe sDectrum f abnormalities een n individualswith UPD,
IMPBINflNG.Genomic mprinting occurs when the phenotexpression epends n the parentof origin for certaingeneschromosome egments.Whether hegeneticmaterial s expredepends n the genderof theparent rom whom rt was deri
Genomic mprinting s suspectedn the basisof a pedigreeF8L-1.7and 81-18)with unusual ransmission.mprinting probly occurs n many differentparts of the human genomebuthought to be particularly mportant in geneexpressionelto development, rowth,cance.,and behavior.
Imprinting in humans s noted by phenotypicdifferencesrn Prader-Williand Angelmansyndromes,which are assocwith deletionand uniparentaldisomyof the same egionof chmosome15. Thus, in uniparentalmaternaldisoml chere s lack of rhe parernal segme[t of chromosome15, resultinPrader-Willi syndromeas well, In Prader-Vill syndromedeletion,when t occurs, s alwaysof thepaternallyderived hmosome15, suggestinghat thephenotype f Prader-\(illi sto a lack of paternallyderivedgeneticnformationcarriedon tsegment f chromosome 5. In contrast,when there s a del
chromosome 5 n Angelman yndrome,he deleted hromosis alwaysmaternal n origin, and he JPD s alwayspaternal,is, there s lack of maternal nformation.There are ikely tomany other disorderswith this type of parent of origin effec
ACOUIREDYTOGENETICBN0RMAUTIES.cquired clonal)geaetic hanges an be found in most tumor cells.Chromosanalysiss an mportant tool for the classilication f manyherologicdisorders.Most leukemias isplaynumerical hromos
-+--r--.,-l---.''-.'
Figurc 81 18. lD pedigrees uggestive f maternal imprinting, phenotypic effects occur only uhen the gene s transmrtted rom the facher but not when tr
mitced from rhe morher Equal numbers of males and fernalesare affecredand not affectedphenowpically in each gener3tion.A non-manifesting ransm
grvesa cJueco the sex of the parent *ho passeshe expressed enetic nformacionj n orher words, in mateinal imprindng, rhere a.e "skipped" non rnanife

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 33/177
abnormalities, structural rearaanSemenrs mairrly trans]ocations),
or borh (see Chaprer 495). Many of rhe chromosomal abnor-
malities are nonrandom and have been shou'n to be useful in
diagnosing rhe leukemia subtype afld predicting treatmenr
outcome, This has been especrally rue in the case of acute lym-
phoblastic eukemia (ALL).
PREI{ATAL IAGN0SIS.Prenaral diagnosis is indrcated q'hen there
rs a familial, marernal, or fetal condition that represents an
rncreased rrsk for malformation, chromosome abnormalitn or
genetic disorder. Advanced maternal age (235), whrch is associ-ated with an increasedrisk for aneuploidies, rs chemost common
reason for prenatal diagnosis. Chromosome analysis and genetic
counseling are also warranted in the event of (1) an abnormal
screening result; (2) a chromosome abnormality in a previous off-
spring, parent, or close relatrve; (3) a previous offspring with mul-
tiple congenital anomalies on whom no chromosome study was
obrained; 4) th e need or fetal se x determjnation n pregnancies
ar risk for serious X-linked disorders for which speciflc prenatal
diagnostic tests are nor available (seeChapter 83).
Prenatal diagnosis usrng cell or rissue samples for chromoso-
mal, biochemical, or molecular genetic str.rdiesmay be performed
using a number of technrques, ncl:ding transabdomin amnio-
centesis, chorionic villus sampling {CVS), fetal blood mpling,
and preimplantation genetic dia8nosis (PGD). In addirion, fetal
cells and free fetal DNA have been detecred n the mother's cir-cularron and can aid rn the prenatal diagnosis of fetal condirions(seeChaprer 96).
Alfirevic Z, Neitson JP: Antenatal screening or Down\ svndrome BM"/
2004;329:811 812.
Anronarakis SE, Lyte R, De.mnzakis ET, et al: Chronosorne 21 and Dorvn
syndrome, From genomics to parhophysiolog-v. Ndt Rev Cenet
2004;5:725-738.
BandyopadhvayR, Heller A, Knox DuBois C, el at: Parentalorigin and timinB
of de novo Robertsonian rranslocarion formation. Am I Hun Ceflel
2002;71:7456 1452.
Beiiani BA, Srleki R, Ballit BC, er at: Use of targeredarray-basedCGH lor the
ctinical diagnoslsofchromosornal imbatance:k lessmorcl Am I Med Genet
2A05:r34A:259267
Bondv CA, Van PL, Bakalov VK, et al: Prolongation of checardiacQTc
inter-
val in Tu.ner svndrome.Medicine 2006,8s:7S-81.
Caine c.. faftbv AE, Parkin CA, et al: PrenataL eteclion of Down's svndrome
by rapid aneuploirly resrins bf chronosones 13, 18, and 21 by FISH or
PCR without a full karyotype: A cyrogenetic .rsk assessmenr La,.ef
20O5;366:'t23-128.
Carrel AL, Moerchen V Myers SE, er al: Grolr'rh hormone improves mobil-
iry and body composirion in infan$ and coddterswirh Praderwilli syn-
&ome. I Pediat 2004:145:744-149
Cicero S, Bindra R, Rembouskos G, et al: Inregrated ulrrasound and bio'
chemical screening or trisomy 21 using feral nuchal rranstucency, bsenr
fetal nasal bone, {ree 0 hCG and PAPP-Aat 11 co 14 weeks Pleut Diagn
2003i23:306-310.
CrolJaJA, Youings SA, Ennis S, et aLrSLrpernumerary arker chromosomes
in man: Parenralorigin, mosaicismand maternal aee rcvtsied. Eur I Hum
C enet 2OO l 3 7S4-l 60.
CuDnrffCr American Acad€mvof P€dialricsCornmitreeon Genetics;Prenaral
screeningand diagnosis or pediarricians.Petlahics 2004\114:889-894De Vries BBA, LeesM, Knisht SJ,et rl: Clinical studiesof submicroscopic ub
telomericrearrangenents:A checklist. Med Gezar 2001;j8:145-150
Douglas SD: Down svndrome: mmunologic and €pidemiologjcass,xiarions-
Enismasrenaln../ Ped,.rtt 2005;r47:723-725 .
Dyken ME, Lin'Drken DC, Poulron S, et al: Prospective olysomnographic
analysiso{ obstructivesleepapnea n Down synd ome.Arch Pediztr Adolesc
Med 2003 1. 7 655 460.
Garrison MNl, Jeffr;esH, Christakis DA: Risk of death for children with
Down syndromeand sepsis. Pediatr 2005;147:748-752.
Gibson PA, Newron RW, Selby K, et al, L:ngitudinal srudy of rhyroid func
rion in Down\ svndrome in rhe first rwo decades.Arch Dis C,h d
2005r90:574-578.
cicquel C, RossignolS, Cabrot S, et al: Epimutarion of the telomeric mprinr
ing center r€gion on chromosome 1lplJ in Silver Russ€ll syndrome. Nat
C e le 2O05 J7 :100 3-7oo7
Chapter12 r Genetics ol Common0isorders: 0iagnosis and Management r
Heffner LJ: Advanced marernal age How old is roo old? N Eflsl -l2004t3 5l:1927 -1929 .
J€cquemontS, Hagerman RJ, Hrgerman PJ,LeeheyMA: Fragile X synd
and fragile X associated rernor/araxia syndrome: rwo faces oI F
Ldaret Neurol 2007:'6:45^5 .
KLeefsrra , Yntema HG, Nillesen \(/M, et al: MECP2 analysis rn me
.etarded patients: Implicarions for routine DNA dta9nos.j'cs. ur JGenet 2004112124-28
Lanfranco 4 KamischkeA, Zirzmann M, ec al: Klinefeiter'ssvndrome. d
2004.,364..273-283.
lvlalone FD, Canick JA, Ball RH, et al: Firsr trimester or second-rrim
screening, or both, for Down's syndrome. N Ensl J M€d 200.52001-2010
MassaC, Verlinde De Schepper , er a| Trends n age at diagnosisoI T
syndrome.Arci D,s CDild 2005;90)67-268.
Mazzan.i L, Cicognani A, BaldazziL, er al: Gonadoblascoma n Turner
drome and Ychromosome derived marerial. Az I Med Genet 2005t1
150-1 i4
NeiLson JP: OptiDlsrng prenatal diagrosis of Doon's syndrome.2005;332:433-434.
Rappold GA, ShanskeA, SaengerP: All sbook up by SHOX deficie
Pedi * 2005 147 422424.
Rio M, Molinari I HeuertzS, et al: Aucomared luorescent enotypingd
10% of crypric snbretomeric earrangemenrsn idiopathic s,vndromicm
rel€ldarion. I Med Cenet 2002:39:166-270.
Robin NH, ShprinrzenRJ: Defining the ctinical spec(um of delerjon22q
J Pediatl 20Q5t147 90-9 6.Roizen NJ, PatrersonD, Downt syndrorne Laftcet 2003\36111281-12
Schubbert S, Zenker M, Rowe SL, er al: Cermline kR,4S mutarions
Noonan svndrome. ar Cer€t 2006:38:331- 336.SchwartzS, Graf MD: Microdelerion svndrom€s:Characteristics nd dia
sls.Methods Mol Biol 2002;704127 -290.S,vberrVP, Mccaulet E: Turner\ syndrorne. N Engl J Med 2004
1227-7238.
Tarraglia M, Pennacchio A, Zhao C, €r at: Crin-of-tunL-tionSOSI mL,r
causea distinctiveaormoiNoonan syndrorne.Nat Genetics2007,39:75
VissersLELM, van RavenswaaiiCMA, Admiraat R, et al, N.lutations n a
rnember of the chromodomajn een€ amily causeCTLA.RGE lDdromeCenetZ0D4: j6195-957
Watter S, Sandig K, Hinkel CK, er al: SubtelomereFISH in 50 childrenmental retardarion and minor anomalies, denrifiedby a checklist, selerearrangementsncludinga de novo balanced randocation ofchromos17p13.3and 20q13.33.An I Me d Genet200411284:364-373.
Vhpner R, Thom E, SimpsonJL, er al: Fi.st-trimesterscreening or rris
21 and 18. N Ersl.J Med 20033411405-1412.V'arburron D, Dallaire L, ThangaveLuM, e! al: Trisomy recurrenc€:A r
sideration based on Norrh American d^a. Am t Hhm C2004:75:376-385.
Yagi H, I'urutani ! Hamada H, et al: Role of TBX1 in human de122syn&ome. Lan.zt Z[0i;362:l jri6-1 37
Youings S, Etlis K, Ennis S, er a| A srudy oI reciprocal rranslocarioninv€rsionsderected y lighr microscopywirh specral eference o originregation! ard r€currenrabnotmaltties.Am J Med Genet 2O04i126A14
Zenker M, Gemor BDheitelG, Rauch R, et al, Genor.vpe-phenotvpeo
tions in Noonan sy\dror^e. I Pediatr2004:14+368-374.
Geneticstudiesare useful n diagnosingand trearing are patric conditions,ofrenalleviaring uffering,e)rTendingife, anthe case f neonatalmetabolic cre€ning,reventingnjury besymptomsdevelop,Ceneticstudiesmay also rdentify he caof more commondiseasesuchasasthmaafid obesiry,An unstanding of the complex and potentially multiple pathwleading o disease s crucial ro rhe development f appropprevenlion strategies including screeningof presymptomparents), s well as effectrve nd specific herapies.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 34/177
518 PARTX r Humon onotics
Commonpediarricdiseases re often multifacrorial,with thecombinationof manygenes nd eflvironmental actors riggeringa complexsequencef events eading o disease. ach ndivrdualhas variations n his or her set of genes;he interactionsof theindividual'sgenevariantswith eachother and with the environ-ment determinesusceptibilrty o disease. he complexiry n thecombinationoI facrors ncreaseshe challenge f iinding genericvariants hat causedisease.Genetic ools include he completedhuman genomesequence, ublic databases f genericvariants,and the human haplotypemap. The incorporationoI these oolsinto largewell-designed opulatronstudies s the field of geneticepidemiology.
82.1 MAJORGEI{ETIGPPROACHESOTHESIUDYOFCOMMONEDIATRIGISORDERS
A model for the genetic conuibution to health is shown in Figure
82-1. Genetic liability is present from conceprion in all persons.
Sometimes this liability rs predominant and results in a srngle-gene disorder such as cystic librosis or si ckle cell anemia, In most
the liability is latent at binh but over time contributes to theemergenceof spec ific medical conditions, particularly upon expo-
sure to envrronmental factors. The goal in medical genecics s toidentify the generic factors in che hope of preventing the occur-
rence of disease,erther by avoiding inciting environmental factors
or by instrturing trearmenrs that reduce risk. For individuals who
cross the threshold of disease, he goal is to better understand theparhogenesis n rhe hope that this will suggest better approaches
to rrearmenr.
A srarting pornt in the genetic analysis of a complex trait is to
obtain evidence n support of a generic contriburion and co esti-
mare the relacive strengrh of genetic and environmental factors(Fig. 82-2), This rs done by determining u'hether a trait clusters
in famrlies and is seen amons related individuals more often chan
in the general population. Possible nheri tance models are delin-
eated by such segregation analyses, The relative st rength ofgenetic and nongenetic risk factors can be estimated by variance
compoflents [alysis,atld the amountof variabilityof a rrai tis due to inherited factors s termed the heritabilitv of a tChromosomalegions irh geneshat mayconrribuieo dissusceptibility an be ocatedwith lintage mapping,which locregionso{ DNA that are inherited n families with the spdisease. enedc ssociation tudies eek o determine elativeof diseasen individr:alswith specific enetic ariants.Dereof the modesteffect of eachvariaff and inreractionswith eronmental actors eouireswell-oowered tudies.
Both linkagemapping and association tudies equiremaralong heDNA rhatcan be ascertained, r genotyped, ith lascale aboratory echniques.Markers that are typically usein the form of microsatellites nd single-nucleotide olymphisms (SNPs) Fig. 82'3]. rVhile humans all have the sgeneticmaterial, everyperson'sgenome s shghtly differencomparison f any two copiesof the same egion of genomereveal that about one in every 1,200 baseswill be diffeusually n the form of a SNP Most SNPs dentifiedby comirtg two chromosomes re common and areessentiallyhe eqalencof geneticdialect,or random differencesn coding withsignificance r functionalconsequence, few of thesepolvmphismswill alter the biologic unctionof a gene,either by afing the structure of the protein or by altering rhe locaamoun!.or time atwhich theorotein s made.Some f these tional alterationsmay affect usceptibllty !o disease.
Outcomes n genetic tudies reclinicalphenoqpesand caa clinical iagnosisf a diseaser a discrete easurementr related o disease. phenotype an be measured y the presor absence f a disease s aquahtative rait, or by usinga maof disease, uch aspulmonary function tests n asrhmaor bmass ndex in obesiry as a quantitative rait. A homogenphenorypes ideal to avoid conflicting esults rom rhe scua trait that has tt'o or more etiologies.Geneticheterogerefers o a trait resulting rom more than onegeneticmechanThe develooment f a trait or diseaserom a differencmecharesults n iphenocopy, the occurrence f which would dininthe detectibilityof theresponsible ene,A pafticular genevarmay not cause he sameoutcome,and rhis pleiotropiceffeeachvariant depends n other geoetic ffectsand environmexposures.
t . iguIe82-l .Model fortheinf luenceofgenetrcsonheal th.Everyoneinheri rssomegenet icl iabi l i ty{ordiseas€risk,buriornut t rfactorialdisordersthist
ficienr ro produce disease n its own. Over time, exposure o environmencal acrors eads rom a presymptomaticco a disease tate. dentificatron of rhe g
responsible or risk can lead to orevenrionstrateeres r treatments.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 35/177
Chalter82 r Genetics f Common isorders
GeneticEnvironmental 4easurementvariance variance variance
v P : v A + v D + v E + v t + c o v c E+ v M
VA=Addit iveenetic a anceVD Devialionue odomindnce ndepistasisVE=EnvironmentalarianceV :lnteraction arianceCoVcE:Covarianceot genelicsand environmenii igu,c S2 L Heri t ibi l i ry cr)ncept henoqvpic ar iance an be part r -
ttuned into gererrc uararce, ervrronmentalvariance,rhe covanance
benveel rhe tlvo. and measurement ariance. Genericvariarce can
Lreurrher partitnrncd nro addirrveatfectsand gene gere interactrons(epjstasist invi ronmental anance an ikervtse e pant r ioned nro
addnive atrd nreracriveeffecrs.HerLtabilitv s defined as the propor
tion of phcnotlplc veri:rn.e dc.ounred ior by genenc variance. One
caD esrimate hentabilirv in the ndrfow sense ron corrclation of .t
quanrirarive .ait betrveen elatives,as sho*'n in the table
There are many factors that may colnplicate scgrellarion and
heritability srudres.Many disedseshat are found to crack n fam-
ilies rna,vappear to skip a generation; a person could inherit an
allele (inherired unir, DNA segorent, r chromosome)and not
show any sign of the disease, phenomenon called ncomplere
penetraflce. om edLseases anifesrsignsonly larer in li fe, u'hile
orhersbecome es sobvious as rhe child grows olderi study pa r
ticipanrscould be misclassi6ed s unaffected gho actuallv have
the d ise . r se - l r ' r duc rngcne . M a r rv L " m nru r rd rsease \m d t r l t e \ t
with varying severit,vl families,and this variable expressivitys
another actor that could causemisclassif ication f People.Tb maximjze rhe ability ro derecra genewirh disease ssocia-
tron, environmelral exposures need ro be measured andaccoulted for in a populatlon.The interactionberween enes nd
Relationship
i,lonozygoticwins
Sib-sibor Dizygotic wins
One parenFOne offspring
l\,'!dparenFOtfspring
Firsl cousins
Uncle-Nephew
Hedtability
h2:2r
h2:2r
h2= 105=to.7o71
h2=8r
h2:41
the environment s called cpjstasis.Epistacic f lectscould a
the expressivity f a rrait as well as rhe penetrance. n era
of this is G6PD deficiency. n individual could carry the algene aod be deficient n l he enzyme.1e r would never hahemolyriccr is isunless xposed o an oxidative stress. eople
inherited propensity for malignant melanoma lr.ho live in dageographic egionsor limir their sun exposuremay neeercxth e phenoc,vpef cance. Asthma in some susceptible eople
developonly afl er exposure o cerlaln antigensor pollucanLinkageMapping.Linkage studies rvere used in the pa
isolare eneshat cause are genetic vndromes;modrfiedmehave been used to identi$ chromosomal regions linked to
common diseases. rnkagesrudies nvolve taggrngsegmenperson'sgenomewith markers thar allow identil ication of
Whal s an SNP?
Differentpeoplecan have aditferenlnucleotideor base ala given ocationon a chromosome
What san SNPmap?
GGTAACTG
GGCAACTG
Figu.c 81.-:i. Ditfercrt combinarions oa single nucleoljde
polymorphisrns SNPs)are found in different indn'iduals.
The locations oi rheseSNlrscrn be pinpointed on Drps oIhumangcnes. ubsequerr t l ) ,hev an beused o creet tpro-
files that are assocjrred rvrrh difference Lrr esponsckr i
drug, such as eificacv and nonei6cac-v.Adapted rt{,m
RosesA l'hafmacogenerics nd the prd.hce ot rnedrcrne-
Ndt'/zd2000;40J 857-865 Copvrishr 2000 Rcprinred b1
permission or Llacmillan Publ,shersLrd )
iff,llii""t'^l["
fi EHow can an SNP mao be used o oredictmedicine esoonse?
oction f SNPgqnoype rof
T|_ImTIlmatientsYi,ith llicacyin clinicalials
Patientswithouteff cacyin clinicalrials
Predictive f efficacy
Predictive f no etficacy

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 36/177
520 PARTX r Hurnan enelics
menls that bave been inherited through the famrly along wrth
disease, The markers are typically microsatellites or SNPs that
define u'hich tvpe of an allele any person carries. The type of an
allele is referred ro as a genotype. Linkage anal,vses f commondiseaseshave shorvn inconsistent results. Facrors sucl as hetero-generty,plerotropy, variable expressivitl'. and reduced penetrance
in addi tron ro varrabiliry in envrronmencal exposures \l,eaken theporver of linkage studies in complex craits.
GeneticAssociation. or mult ifactorial common diseases, sso
ciation analyses mav be better suited to detect small effects than
linkase studies. Genetic assocratron srudies are simrlar ro rradi-tronal disease ssociation tudies,with a person's enoc,vpeeing
used as a predictor of a disease or trait. The goal is to identifv
the actual allelesat a locus that confer the risk f or a disease.Three
basic designs re used: 1) a case-coltro] design,with a compar
ison of che frequency of an allele in affected people compared
with unaffecced people, (2) a population based studl', in u'hich
an inc rea \en J quan l r la l r vera r to r con t inuousmea\urement\
correlated with genotype, and (3) a family-based test, in which
cransmission f alleles o affecred and unaffected offspring is
cested. hjs lasc ype of anah'sis,known as a transmission ise-quilibrium rest (TDT), looks for an allele hat is cransmictedo
an affected person more often than rhe other allele. lf there is nc>
assocrarron etween an allele and disease, he transmrssionof
eachalleleshould be equaL,with eachhaving a 50/50 ratio. If an
allele confers risk of disease, he rransmission rario rvill be drs-rorted, u.irh one allele showing higher transmissron ro affeced
chrldren,The uccess f all 3 typesof associatxrn nalvsrs epends
on the desiEn f a well-poweredstudn wrrh enoughsub;ects, nd
atr accuratelymeasured rait ro avord misclassif icatron ue tovariable expressivit,v r reducedpenetrance nd ro minimize th e
effect of genecic heterogeneitv and pJeiotropl.. In large popula-
tion-based studies, confounding bv erhniciry or population strar-
ificarion could distort results. Some senenc varlanrs are more
lrequentlr round rn people rom a p.rrricularethnicgroup. rvhich
could causean apparent association f a r.arianrwrth a disease,
when the disease ate happens ro bc higher in that group. This
association would not be a true associalion betrveen ao allele and
a djsease,as the association *'ould be confounded bv ethnicitl',rl,'hich s oftel re(erred to as population strarification. The famil,v-
based cestsusing the TDT are immune co population stratificatiofl because he association s rot wich a soecif ic l lele.bu t rvith
a d is ro r r ion l r ran \m i \ \ i on n a t f e . t edpeop le i rh ina t . rm i l1 .
Assocrarion srudies should be a powerful rool to find genecic
variation that confers isk ro an rndividualt rhe effecrof any one
genetic varianr rvill be a verv small conrrlburion ro the complex
diseasepathrvay. Genetic variants have been found that impl icate
a novelgene n a process,modvating more in-depth esearchnr o
svstems hat &'ill affecr diseaseoutcome. Assoc iations such as theApoE4 variant with an increased risk of Alzheimer drseaseare
nored by many sr udies.Many published association esultsar enot reproducible; insuflicient pow'er and stratl6cation may
account fo r rhe inconsistencies.
Genetic discovery is also possible by focusrng on specrfic can-
didate alleles. There are 5 10 million SNPs across the genome,
far more chancan be cestedn any singleassociarion tudy'.Can-didare SNPsar e identrf led rom genes hat are suspected o con-
tribute to risk, perhaps because of a known phvsiologic or
biochemical role in che disorder A major limitarion is that unex -pected genetic contributions will be missed, leading to fai lure to
take advancage of the potencial power of rhe generic associalion
approach to uncover ner! 'disease mechanisms.Sequencing feach rndividual's genome u.ould detect all variants but is rmprac-
tical and expensive. However, by using known patterns in thegenome, lhe rnajoflty of vaflants can be assessed or each individual rapidly.
SNPs are arranged n the genome on blocks of 10,000 basepairs or more that have nor been interrupted by recombinatron
through generations;he SNPs n a block iorm an inheritedunit
called a haplotvpe. The HapMap proiect has delined these bloin four populations around the world, providing measurem
of the relationship betrveen SNPs in the blocks. This al lowsrhe selection f SNPs hat are proxies or "tags" for a haploblock. Genotyprng chis smaller subset of SNPs captures mos
the common variarion in a regon with far fe*er genoty
Current estimares show that 500,000 SNPs are sufficient to resent about 907n of variation in th e human senome. HapMap is a ra r lab le : a pub l i t Ja raba ' e . . ; l uab le res .for the design of association sudies that can be tailored to s
crnc Popularrons.
82.2 CURRENTrrrorRsrnnorrucFGENErrcsFCOMMONIsoROrRsNCHITDREN
The impacr of generic scudies of common pediarric diseas
being reahzed. Prevention and incervention may soon be poss
usingval id genecic ssociation esults o identif,v hildren at rThreeexamplesof diseases nder ntense crutiny or genetic
factors are tvpe I dlabetes mellitus, asthma, and obesit,v.
TYPEDIABETESELTITUS
Type I diaberesmellirus T1DM) is the best characterized f poJygenic,mult ifactorial pediatric llnesses sceChapter 590is a common diseasewith a well-defined phenotype and evide
of environmental and geneticcomponents. Linkage studiefamilies vith an affectedchi ld yield many loci thac appear o
consistently inked to rncreased isk for Tl DN{. A |:ewgenevants have been found rhat confer risk for disease,and some eronnental factors have been idencilied includrne vrral infecti
rriggering rhe autoimmune process.While rheie are rare '
dromic forms, such as Wolfram syndrome, resulting liom knomonogenicmutations,most childrendiagnosed vith T IDN{ ba currently unidentrfied etiology.
Heritability estimates for T1Dtr'l are cst imated bet\r' een 6and 72o/., u.irh trvin concordance of 307. to 50%. Althou
these studies ma,v be confounded by shared environmenr, ievident that, at least in part, there is an inhericed componen
T1D1!{ risk. The relative risk to a child in chegeneral populat
is 0.47", whereas or the sibling of a child with drabetes r rs
trmes higher ar 67". The Type 1 Diabetes Consortr(wtuw.tldgc.org) has undertaken a meta-anal,vsrsof all of
l inkage dara. They have also devised a uniform nomenclas1'stern, uch that promising linkage regions have been assignumbers, designated DDN{ 1-18. lt ' {any early scudies etelinkage at the MHC locus on chromosome 6p21 u.ithin the Hgene region. A meta-analvsis f these inkage studiesshonevery srrong [nkage signal wirh a LOD score of 65 at this locnhich has beendesignated DDM1,
'$(rhrlerhe HLA-{DDM1 locus has been studied extensiveJ
presents many chalJenges n dececting causal genetic alteratro
Many of the genes n the region have sjmilar functions and in coflcett in tbe Th2 immune system, The region also has h
linkage disequilibrium (LD); many of the proposed risk alleles
inherited together, making it di fficult ro isolate a srgnal from
one as being drrectl,v responsible for the rncreased risk. Thpercent of children diagnosed with TlDNI have rhe combrnac
of ailelesac rhis locus hat code for HLA-DQ2/DQ8 (genoc
Cornbinatrons of alleles (haplorypes) at two loci in the Hregion ar e risk alleles;none of these has pinpointed discinccausalvarlants.
The IDDM2 locus encompasseshe insulin 11NS/gene.Asciation studies idennfied varianrs rn this sene thar conferred
f o r T ID \ | . A r rpeat reg ion kno t rn a ' r VNTR. or va r i
number tandem repeat) near the INS gene has been associ

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 37/177
with diabetes risk, with a longer repeat correlated with increased
risk for T1DM. The mechanism of gene dysfunccion due to the
repeat is unknown, an it rs very likell, that rt is in LD with
arother \.ariant thar do alter funcoon or inreraccion to predis-
pose an individual to diabetes.
A varianr of the CTLA4 gete is found in the coding region of
this gene, suggesting hat a firnctional change n the protein could
cause suscepribility. Additional studies found a variant in rhe 3'
untransLated region in LD with the coding SNP ro be an even
better predictor of risk. Thrs SNP was in chepromoter region of
th e gene,whjch could also suggest functional role in ttanscription regulation. The mechanism by which alterations in this gene
increases susceptibiliry ro TIDM reguires a thorough search for
regulatory genes hat may interact with rhe promoter region.
OBESITY
Childhood obesity n rhe UntcedStates s increasing t an alarm-
ing rate (seeChapter44). Obesity s a multifactorialdisease, ith
man-v of che conrributing factors still unknolr'n. Ic is likelv a het
erogeneous phenorl.pe resulting from dysfunction many dif
ferent parhways. Concributing factors ma,v inclu a modern
environment of plentiful calories and low phvsical activitn whrch
combined rvirh inherited risk genes esults in obesiry
Prevrousll.,childhood obesity was rare enough that a severel)'obese child warranted consideration of rare syndromes such as
POMC (proopiomelanocortin) deficiency,Prader-rJ0illis,vndrome,
an d Bardet-Biedlsyndrome.A few studieshave suggested hat
childhood obesrty s due to rare geles lhat act as a recessiverait
and can explain a larger fraction of tAe variation in body mass.
Melanocortin 4 receptor (MC4R) rs an exampleof a genewrth
recessive urations hat are found in 3% of children with severe
early-onset obesity. Polymorphisms in MC4R have not been
found to be associatedwith more common polvgentc obesity
observed n th e generalpopularion.
Common forms of obesiqv show a complex pattern of family
segregation. Family srudtes and twin studies yreld estimacesof
heritabrlrty ranging from 3Oo/" o 70y", $.ith the t,vpical estimate
at 5070, meanjng hat about half of the variation in body mass
within apooularion
is due to inherited factors-Body mais index (BMl) is a phenotype obtained in many
cohort collecnons. Whole genome linkage studies have shown
evidence i l inkage egionson everychromosomeibu r a number
of regrons ave beendeteced n several tudies ha t hold promise
for genes associated with common obesiry. Linkage studies in
children have resulted in the discovery of rare mutatrons in genes
such as leprin and melanncorrin thaf account for some of rhe
severe arly-onset besity; hesegenes av enot beenconsrstenrlv
found ro conrribute to comrlon obesrt)..
Studies have also focused on candidare genes thougbr to be
involved in obesity-related athways, such as tnsulin signaling,
fatty acrd oxidation, an d appetire regulation, N{ore than 10 0
genetrc assocrationswith obesitv have beenreported in posirional
and funcnonaLcandrdace genes, ier verv few of these indings are
reproducible; none have led to a novelprevention or therapv for
common obesity. Haplotypes in rhe ghrelin recePtot, ENPPI,
leprin. and insulin signalingprotein 2 are reported o he rssoei
ated with. common obesrty', et only rhe /NSIG2 finding has been
repllcareo.
ASTHMA
Asthma is a common childhood condit ion; rr is increasrng t an
epidemic rate (seeChapter 143). In rhe United Srares,asthma is
more orevalent in Hispanic and African American chiLdren.
Atopy and aschmaare heritable. Asthma is a heterogeneousdrag
nosrs and is delined as reversrble airway narrowing with obs-
truction associated wirh small airlt'av bronchospasm and
Chapter 2 r Genelics f ComnonDi$o.deF
inflammation. It mav resuft from dysregulation of the Th2 infla
macory cells with hrgher serum levels of IgE . Children with
parents affected with asthma have a 507o increased risk of atoThe odds of asthmadragnosis n children aged 3 to 6 yr incr
by 2-fold in children u'ith two rather than one affecred par
Twin studies rn S$,eden and Finland bave found asthma h
tability esrimates of 80%, ',r.ith much hrgher concordancemonozygocic twins than in drzygotic rwins. Children of asthmmothers have a higher risk than those wirh aschmatic athers,
gesting the possibilit_vof in ureto mechanisms nfluencing risk
deveJopingdisease.In utero exposure to tobacco and maternal aslhma are ass
ared with jncreased IgE leveLs n infants and a higher rate
asthma. Early pulmonary infectrons wrth respiratory synry
virr.:s (RSV), rhinovrus, and Chlamydia pneumonia have
been mplicated in rhe developmenr of asthma. Associations h
been demonstrated wrth enviionmental exoosures such as en
to r in , . ock roach nddusrm r tean r rgens .ndd ie te l a r r i c les
lack of exposure to a differenr set of pathogens has been shoto inctease mmune deregularion and asthma, as proposed in
hygiene hypothesis. Exposure to parasites n early childhood beeo correlated with prorection against asthma and atop,v.
Asthma has quantifiable markers such as pulmonary functcests, inkaee studiesof asthma an d its markers have dem
srratedsomi overlap of DN A regronson chromosomes5q,
12q, and 13q. Linkage ro 20p13 ha s motivated associastudies n the geneADAM3.3 la member of the a disintegrinmetalloprotease domain farnily); this finding has not been re
ducible. ncerleukins and 13 are associated ith rncrease
levels. ,rhrle L-4 and l0 are assocrared ith airway rersra
as measured bv FEV,. Increased TNFo levels in bronchral se
tions led ro a str-rdyof polymorphisms in that gene wrth le
and asthma severitv.ln childhood asthma rhere is great variability in respons
medications. arge cohorc srudies n children (suchas he Chhood Asrhma Managemenr Program and che Tucson ChildreRespiraroryStudy)have provided evidence f subgroupsof cdren with asthma that drffer in the natural historv of the disas w.ellas in drurg response. Cbildren vary greatlv in responsleukotriene inhrbrtors and corticosteroids, another hetero!!en
aspect of rhe asrhma phenotype. Varratron in the []j-receptorbeen shou'n to influence response ro $ agonist therapy with particular genotype in rhe receptor causing reslstance o the
bi[zrng and dilating effecc of the drug.
SUMMABY t is clear that there is much yet to be discorcred abthe common drseasesffectingmosrchildren.Successfulheraand prevention strategies will depend on the dissectioncomplex pathways in whrch many small changesan d envimenlal interaction\can acl rn urder for a per*on fo enc(,unthreshold for drsease development. Gene therapy techniqcould be applied as treatmen! focused on modif,ving rhe acgenetjc risk facro! bur will reqr.rire dentilication of specilic tarin diseasepathwal's. Efforrs rn the past to supply a gene to tth e placeof a mulated geneha d some success, ut were lim
bv hrrst re;ection of the vectors. New discoveries promise mprecrse modulation of gene products using techniques suchRNAi (RNA interference) with synrhetic RNA molecules tar
ted for specific genes.
Th e ne w tools available o researchers ave allowed detecof a number of novel genesand pathways for common diseaand the adveot of whole genome association studies promise
acceleration f these esults. nteractionsbetw.een eri6ableallelesan d environmental actors as uell as epistaric nteracwiii be increasingly possible. Whole genome association stuwill provide vast amounts of data, requiring new anal,vtrc
to dissect the true effects and inreractrons, Whole senome ac ia r ion e \ f ingp rom iseso h igh l igh tmany gene l i ca r ian r \ lin relation to each other and environmental factors wrll eluci

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 38/177
522 PARTX . HumanGenotics
the pathlvavs leading to common disease, eading to rreatment
and ultimately preventiol of disease.
Al6huler D, er al: A haplorype map of rhe human genome. N'atere
2005;437:r299-1320
Balicki D, Beuder E: Gene therapy oi human disease. Medirme
2002181:69-196.
Bracken NlB, Belanger K, Cookson ViO, et al: Genetic and perinatal risk
facrors br asthmaonsetand severiry:A reviewand rheoreticalanalysjs.pi
demia Rer 2002,24,L75-1 89.Carroll W, ,{sthma generics:Pit{alls and triumphs. Paediatr Resph ReN
2005;5:6874.
Cavazzana'Calvo 1, FrscherA: Efficacy of gene therapt for SCID is bejng
conf'tmed. Ltln.et 2004\364:27 5J1 56.
Escolar DM, ScacherjCC: Pharmacologicand genedc herap). or childhood
musculardvstrophies.Cwt Ne rol Newosci R€p 2001,,11158-174.
Ferry N. Heard J\.{: Liver direcred gene rransfer veaors. Hum Gene Ther
1998..9:1.975-1981
Frsch€rAr Gene herapy oI tympboid prinary rmmunodeficiencies. rr Opi'
Pediatr 2000,12:s57-552.
Crimm D, Kay MA: TherapcutLc ho.t hanpin RNA expression,n the liver:viraL argetsand lectots. Ce11e henpy 2006j13(rt):563 575.
High KA: Gene transter as an approach ro rreating hemophilia. Cil. Rrs
2001i88:137-144
Hirschhorn JN: Genetic epidemiolosv of qpe 1 diabete!. Pediatr Diabetes
2003;4:87-100.
Kaiser J: Seekins he cause of induced leukernras n X SCID trial- Sciezce
2003j299:495
Kozarsky KF: Gene herap_vbr cardiovasculardiseaseAtrr Opin Pbarmacol
2001;1:'t97-202.
Krvon Hl,, BelangerK, Bracken MB: tffect of pregnancy and stage oi preg-
nanc,v on asrhma severity: A systematic revie$,. Al, / Obstet Gynecol
2004;190:1201-1210
Lyon HN, Hirschhorn JN: Genetics of comnon forms ol obesiry: A brief
ove ie\ i1Al z / Cr, Nrt / 2005;82:2155-2175.
Liu I Huang L: Developmentof non viral vcctors or systemicgenedeLivery.
J Control Release C02;18:259-256.
McCormick F: Carcer genederapv: Iiinge of curting edge)Ndt ReL Cd'1cer
2001;1:130-14r.
Onengut Gurnuscr:S, Concannon P: The genecics I rype 1 diaberes:Lessons
learnedand furure challenges.J Atutoi'11nun2005;25:S34-S39.RichardsonPD, Kren B! SteerCJ: Cen€ epair in the nerv ageolgene therapy.
H€pdtolosl 2002,15:512-.t18.SchmidtY/otf CD, Schmidr-Y/olf IG: Immunomodularory gene therapy for
haematologicalmalignancies Br J Haenato! 2002111/-:23 32.
Thornas CE, Ehrhardt A, Kav MA: Progress nd problemswrth the useofviral
vectors or gene hetapv.Nature Reltiew Ceretr.s 2003i4(5):146-358.
\X:eis S! Rabv BA: Asrhna genetics 001. Hrm Mol Gezel 2004;11(SpecNo
1):R83-R89
Yoon lw, Jun HS: Recentadvancesn insulin gene herapy or rype I diabetes.
Ttends Mal lvled2002;8-.62-68.
GENETIC ESTING.Genetic testing involves analysis of genetic
material to obtain information related to an individualt health
status using either chromosomal analysis (see Chapter 81) orDNA-based re5ring.
0IAGN0STICTESTING.Diagnostic generic resting helps explain aset of signs and/or symptoms of a disease. The li st of disordersfor which speciEc genetrc tesrs is avajlabLe is extensrve. The,Nebsrte Lrtu)ta-gefietests.orgrovides a database of available tests.
Single-genedisorders can be tested by two approaches: hlkage
analysis aod direcr mutation analysis. The former rs used if the
responsible gene js mapped bur not yer identified, or if impraccical ro frnd specificmurations, usually becauseof chesiTe and Iarger number of differenr murarion' in some gDrrect mutation analysis rs Dreferred and is facilitated ahuman genome sequence s ftrrther elucidated a[d cechnofor mutation analysis improve.
Linkage testing involves tracking a genetic trait rhroufamily using cJosely inked polymorphic markers as a surrofor the trait (Fig,83-1). t requires escing n exrended amily
is vulnerable rc' 5sveral pitfalls, such as genelic recombina
genelic hererogeneirr,,and incorrect diagnosis in che probGenetic recombination occurs betrveen any pair of loci, thequency being proportional to the distance between them. problem can be amehorated b,v che use of very closelv li
markers, and, rf possible, using markers that flank the spgene, Genetic heterogeneity can be problemaric for a linkbased test rf there are multiple distrnct loci that can caus
same phenotype, resulting in risk that the locus tested rs noone responsible for disease n the family. Incorrect proband
nosis also leads to tracking the wrong gene. Linkage ceremains useful for severalgenetic conditions. I! is critically imtant that genelic counsehng be provided to the familv to exrhe complexities of interpretatron of test results.
Direct mutation testing avoids chepitfalls of linkage restir
detection of the specilic gere muration. The specilic appr
used s customized ro the biology of fhe gene beingtested. In sdisorders one or a few distincc mutatrons occur in all affe
individuals. This is the case in srckle cell anemia, in which
same single base substitution occurs in everyone with the d
der In orher conditiols, there may be many possible mutat
that accoun! for the disorder in different individuals. Cfibrosis is an exampler over a lhousand distinct mutathave been found rn the CFTR gene. Mutalon analysis wichallengrng becauseno single cechnique will decect all pos
mutations.Direct muratlon tescsare interpreted in llght of 3 factors:
lytical validrry clinical validiry, and clinical utilitl-. Analyvalidity is test accuracy-does the lest correctly derect the
enceor absenceof mutation? Most genetic tests have a very
analvtical vahdity, assuming that human error such as sa
mix-up has not occur red. Such errors are possible, and u
Diseasegene
2 2 2 4
Figurc tll-t. Use of linkage analysis n prenaral diagnosis oI an aurorecessive isorde.. Both parents are carriers, and rhey have one alfecre
The numbers betow the symbols ndicate allelesar 3 polvnorphic Loci:
and C. Locus B resjdeswithin rhe diseasesene The aflecredson inherne
1-2-2 chrornosone from his facher and the 2-1-2 chromosome fror
mother.The fetus has nherited rhe samechrornosome rom the father, b
3-2-4 chromosome ron chemother,and rheretore s mosr ikely to bc i ca
c
2 2

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 39/177
most medrcal tests, a genetic cest s unlikely ro be repeated, since
ir rs assumed hat rhe resuft will not change over time Therefore,
human ettors may go undetecced or long periods.
Clinical validity is the degree ro which the test correctly pre-
not prove rhat rt is the causeof the individual's disorder Various
lines of evrdence are used to establish pathogeniciry These
include: finding rhe variant only in ffected individuals; inferring
that the variant alters rhe funcrio of the gene product; decer-
mining whether che amino acid alcered y the mutatron is con-
served in evolution; and determinin rvhether tbe rnuca
incidental.
False-negative results reflect n inability to detecr a mutation
in an affected indrvidual, Thi occurs principally in disorders
gene, since mutarions can be varied both in locatron *'ithin the
genean d rype of mutatron,Direct sequencing ill missgenedele-
t ions or rearrangements, nd mutations ma y be found wrrhrn
noncodingsequences uch as ntrons or the promoter; a negalive
DNA tesc does not necessanly exclude a diagnosis.
Clinical utility is the degree ro which cheresults of a test guide
clinical management. For generic testing, clinical utilitv includes
establishinga diagnosrs hat obviales che need for addit ional
workup or guiding surveillance r treatment.Test results may
also be usedas a basis or genetic ounselingThere ar esomedis-
orders for which genetic rescing s possible but in whrch the test
resultsdo not add ro the clinical assessment.f lhe diagnosis nd
genetic implications are already clear, it ma,v not be necessary o
pursue geneltc tesnng.
PREDICTIVE ESTING.Predictive genetic testirg involves perfor-mance of a tesr rn an individual who is at risk of developinga
genetic drsorder (presympromatic), all,von the basis oi family
hisrory; yet does not manrfest signs sl/mptoms. This is usually
done for disorders thar display age-dependent penetrance; the
likehhood of manifesting ignsand symptoms ncreases"ith age,
concern hat a posit iveDN A restma y reslrlt n stigmarizationof
an rndividual and may not as yec provide ioformation that rvi l l
guide medical managemenr. Stigmatization might include psl'
chologJcal tress,buc could also include discrimination, ncluding denral of heafth, ife, or disabil itv rnsurance r employmenr
(seeChaprer 78). lt is generally agreed har predictive genetic ests
should be performed for children if the resulcs of the rest will
beneft the medical management of the child. Otheru'rse, che est
should be deferred until the child has grot'n up to the point of
underscanding rhe risks and benefirs of resting arrd can provide
rnformed consenc. ndivrdual states offer varyrng degreesof pro-
rection from discrimination on che basisofgeneric resting; federa)
legrslation as noc yet passed hrough the U.S. Congress.
PREDISP0SITI0NAtESTING.t i s expected ha cgenetic estsma y
becomeavarlable ha t will predict nsk of disease. ommon dis-
orders are multifactorial in etiology; there may be many differ
Chapter 3 r Integration f Gerelics ntoPodiatricPraclico
ent genes that contribuce to risk of any speciflc condrtlon
Chapter 82). Mosr of rhe genetic vananrs that have been fo
to correlate wrth risk of a common diseaseadd small increm
of relatrve risk, probably in most cases oo little to guide m
agement. lc is possible, however, that further discovery of g
lhar conLribute !o common disorders will reveal examples of
ants thar convey more significant levels of risk. It is also pos
that testrng several genes ogether will provide more informa
about risk chan any indrvidual gene variant would confer.
rationale for predispositional cesting s tbat the results would
ro srrategiesairned ar risk reducrion. Thrs mighr include av
ance of environmental exposures that would increase ris
disease,medical surveillance, or, in some cases,pharmacolog
lreatment. The vah.reof predispositional tescing r'ill need t
cfltically appraised through outcomes studies as these tesr
deveLoped,
PHABMAC0GENETICESTING. olymorphisms in drug metabo
genes may result in distinctive pacrerns of drug absorp
mecabolism, excretion, or effectiveness seeChapters 56 and
Knowledge of individual genotypes will guide pharmacolog
therapy, allowing customuation of choice of drug and dosa
avoid roxiciry an d prurrde a rherapeulic esponse.
83.1 GENETICOUNSELII{G
Genetic counseling is a cornmunicarron process in rlhich
genetic contribudon to health is explarned, along with sp
risksof transmissionof a trart, and options !o manage he
dit ion and ts inheritance Table83-1).Tb e counselor s exp
to oresenr nlormation in a neutral. non-direcrive nanner an
pro,ride support to che individual/f amily to cope with deci
t|lat are made.
Genetic counseline has evolved from a model of care that
devek;ped n the contexr of prenatal diagnosis and pediacrics
Table 83-1). Fo r prenatal diagnosis, he task is to assessis
a couple of havrng a child with a genetic condrtion and a
the couple about options to manage that risk, including reductive options such as artiEcial insemrnarion and prenala
preimplanration genetic diagnosis. In pediatrics, the task
establish a diagnosis in a child, provrde longicudinal care fo
chrld. and advise he Darenrs bouc isk of recurrence s r.e
options to deal with that risk,The generic counseling role has expanded, particularly
advances n understanding the geneticsof adult-onset or com
disorders. Genetic counselng has a major role in risk asses
for cancer,especially breasr and ovarian cancer or colon ca
for which rvell defined genenc tests are avai lable to assess is
an irdividual.
TAIKING T0 FAMltlES. The type of information provided
family depends on the urgency of the sit uation, che need to m
decisions, and the need ro collect additional informatThere are 3 srtuations in which genetrc counseling is parhcu
rmPortant.
The lirst is the prenatal diagnosis of a congenital anomagenetic disease. The need for information is urgent becafamill musr ofcen decidewherher to continue or to termin
pregnancy. Risks to the mother must also be considered.
second rvoe of situarion occurs when a child is born wit h a
threaremng congenital anomaly or genetic disease. Deci
must be made immediacely with regard to holv much sup
should be provided for the child and whether certain type
therapy should be artempred. The rhird situation arises lat
life rvhen (11a diagnosiswrth a genelic mplication is rnad
a couple rs planning a family and there is a family history

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 40/177
524 PABTX r HumarGenetics
(onranguinity
Terat0genxposureo(upational,bure)
Repeatedregnancyors rinfe ility
Pregnancy(reeningbnolmality
MitenJl5e:ufrletcpr,rn
MatemalIi ! ( r?enr ,J l ] f lhJi . , i tltlal ullaronoErfiy
fetd aryotipe
Heterozygotecre€ningased n€thnk itlS d , . a l i r e m d
IJr. ;clt aJrrir!ar,JL(h.{ aiia!
Iha 5gem5
F0llow-upo abnormale0natalenetkesting
genctic pfoblem. includrng rvhethcr on e member oi a couplecarriesa translocationor is a carrier of an abllorlna]gene or anautosomaL ccessive r X-Llked disordcrl i3 ) ao adolescent ryoung adulr has a family historv ot an adult-onser cnelicdisor-de r iHuoringtoo disease, reastcancer); 4) unrlslral eaturesar e
presentand a (llagnosis s wanting or not possiblet rf ld (5)thereis suspecred xposure o a loxrc subsrance r tcratogen. f is oftennecessirrvo have severalmcetings vicha famiJl. n this third cat-egorl' . - lrgcnc,vs ooc as much of an issucas being sure hat the,vhave as much iniormation and as many options as are available.
GENETIC 0UNSEtING rovrdrng ccuratc nformacion o familiesrequires (1) raking a careful famrly historl. and constructing lpedigree rhat l ists rhe patrenr! relatives (including abortions,sril lbirrhs,deceasedndividuals)n ith tlreir sex, age,and stateofhealrh, up ro and ircluding rhird-degree clativcs; 2) garhering
informatjon from hospital recordsaboLlt he affecred rdividual(irr sorne cases,ahout orher famiLymembers); 3) d()curnenringpreretal, pregnancl; :rnd delverl.histories; (4 ) rcvierving chelarestavailablcmcdical. aborarory., nd genetic n[ornratioucon-
cerning the disordcr; i5) careful phvsical cxamilarion of rhealfected ndividual (photographs, neasuremenrs) nd of apparentl)runaffecrcd ndividuals n rhe amily; (6 ) establishing r con-firming the <iiagnosis v the diagnosrrc esrsavailable;17 )grvingrhc family informatron abolrt sLrpport roups; (8 ) providing neu'information to the family as it becomesavailable a mechanismi i ' r upd r t ingneeJ ' . ' h r < .Lab l i rhed ) .
Counseling essrons us! include the folkrt ' ing information:Th e Specif icCondit ion r Condit ions. f a specilicdiagnosis s
rnadc and confirmed, that should be drscussed ' ith che familynnd inlbrmation provided in wrrtrn€!, However. ofcen the disor-de r firs ittto a spectrum (1 of manv types of arthrogryposis)orrhe diagnosis s clinrcal ather rhan aboratory based. n thosesi ruarions, the famil,v needs to undersfand fhe limits oi preseDt
knou-ledgcand rhrr addit ional research vill probabll, leabetcer nformation i n th e future.
Knowledge f he Diagnosis l the Pa.ticularCondit ion. lrhoit js not aiu.ayspossible o ll lake an exact diagnosis,havinaccuralea diagnosis s possible s important. Esnmates |: ercnce risk ir|r.ariorLs family mernbers depend on an accudiagnosis. 0hen a specilic iagnosis annot lle made (a s n ncasesof mult ipie .ongen ta anomalies), he vari<>us iiferediagnosesshould be discrLssed ' irh the iamilv and empiin [u rm ar io r
5 ' r
r rded . f ' p cL f i d ragn , ' soc , " , t r r re" t r ' l "thcv should be discussed.
NaturalHistoryof the Condilion. t rs very important to disthe natural history of the specif icgeletic disorder n the famA le r ed nd i l i du r . l nd t he r r am i l i es i l l ha . . t uc , r inn . estng hep roAn ( , \ l s l | dpo fen t i J lh r r Jp \ rh . l t . l n b r r , \ c rcdwith knorvledge of fhe ritlrral hiscor,v. f rhele are other posdrffercntial iagnoses,heir naturalhistory ma,vdlso be disculf rhe disorder s associaredvith a spectrumof clinical ourcoor complications, he worst and best scenarros, s \,r 'ell s trmen! and referral to thc appropriate specialist, shouJaddressed.
Genetic Aspects o{ the Csndition and BecurlencB Eisk. Tinformation is ilrrporfant for the family because all farmernbersnecd ro bc mate of their reproductivechoices.generics f rhe drsorder an bc explarned virh visual aids
figof chromosornes).c s inrportant coprovide accurare ccurrand recutrence lsks for various members of rhe farnill ' , nciLrg naflectcd ndividuals. f a de6nitediagnosis annot Lr cmir is recessary to use empirical recurrence risks. CounseshouLdgivc th e individuais the necessarynfonnarion to rrnscancl he varrous oprioos and let th e patientsnake their oinfonned dccisions regarding pregnancl,, adoptr<>n, rri6inseminarion, renrraldiagnosis, cr eening, arrierderectionlennlnatiol of preenancv. It ma,vbe necessar,vo hirve more fone counseling essi()n.
PrenatalDiaqnosis nd Preventi0n.r. ' lan,viffercncmerhodprenatalcliagnosis re available, epending n drc specilic endisordcr seeChaprer95). The useof ultrasonography l lovr.snatal dia8nosis of auatornic abnormalit ies such as congeheart defccts.Amniocentesrs ld chorionic vrllus samplinqus . ' d u oh t . r in e r , r l r ' . u c t . r . rna l l s i i ' f ch |on ro .on r i labmaliries, biochemicirl disorders, and DNA studies. Mateblood or s erumsampling s used or some ,vpcs f scr eenrng.cells can be rerrieved from the urnbilical cord or from matebltxrd or tcsting.althoughnothers may harbor cells rom all vrouspreSndncreS,
Thetapies nd Beferral.A number of genericdisorders eqlhe careof a specialisr.ndividualswirh Turner s,vndron,tesuneed R) be evaluated y an endocrrnologist, reventionof knoconlpLcations s a priorir,t. The psychologicadjusrmenrof family may require speci6c ntetveDtron.
SupponGroups.A large number of communitv Iay supgroups have been iormed ro provide informarion and to fresearch n specif ic eneric nd nongenetic oldit ions. An imptanr par! o| .genetic ounselil1gs to glve nformarion rl)oLrt hgroupsro individualsand to suggest contact person or the fi l ies. Many groups have establishedwebsitesu' ifh ver,vhclrntormatron.
Follow-up.Families shorl]d be encouraged o continoe to questionsand keep up u' irh ne w information about thc spedisorder. Nerv developnents oitcn influence the diagnosistherapv oi specilicgenericdisorders.Lay supporr !(roupsagood sourceof nerv nfornation.
NondirectiveCounseling.ienetic counseling s usually norecrive; hoices bout reproducrionare eft to the familv to dewhat is t ight for thern. Ttre role oi rhe coulselor (physic
gencuccounsel()r, urse,medical geneticistl s ro provide inmation in undersrandable erurs nd outline the ranseof oDtavaiiable

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 41/177
83,2 MAI{AGEMENTt{DTREATMENTF
GENETICISOBDERS
Genetic onditionsareoften chronicdisorders;ew are amenable
ro curativeherapies. evertheless.herear emanymanagement
oprronsavailable. ll individuals/familieshouldbe provided
rnformation about the disorder,genetrc ounseling, nticrpatory
manrpulations, uchas avoidaace fphenylalanineor indrvidu-
al s with phenylkeronurra;oenzymeuPplementarionor lomeparients ir h merh lm aon cacidemal provision { substrateso
ixcrete ammoniafor thosewith urea cycledisorders;bisphos-phonate rearment or rhosewirh o\teogenesismperfeccao
ieducebone racrures; nd avoidance f cigaretre moking or
PHAffMACOLOGICHERAPIES.any physiologic therapies use
it is highly effective n rreatmentof CML and severalother
malignancies.
REPTACEMENTHERAPIES'Replacement rherapies include
reDlacement f a missingmetabolite,an enzyme'an organ, ol
evena specific ene.Enzyme eplacements a comPonent f the
rreatmenc f cy'itic6brosis o manage nteslinalmalabsorPlion.
Chaptor } | htegralioft l GeneticsntoPodiatricPractice
Pancreatrcenzymesare easily administered orallJ, since rhey m
be delivered to che gastrointestinal tracr. Enzyme replacem
strategies are effective for some lYsosomal storage disorde
Enzymes are targeted for the lysosome by modification w
mannose-5-phosphate, which binds to a specific receptor T
receptor is also present on the cell surface, so lysosomal enzym
wirh exposed mannose-6-phosphate residues can be tnfused in
the blood and are taken into cells and EansDotted to lvsosom
olism, and hematologic or rmmunologic disorders A succes
rransplant is essent ially curative, though there may be signifi.c
risks and side effects (seeChaprer 134).
Replacement of a defective gene (gene herapy) may offer a
invasive means of achieving a cure of a genetic disorder (
Chaoter 82).
Alliance of Genaic Supp rt Gtovps Directory of Ndtio,Bl Genetic Volun
Orsonizatiots, 35 Wisconsin Circle, Suite 440, Che\'! Chase,
20815-70r5.BarrelsDM, LeRoy BS, Mccarrhy 4 et at: Nondirecdvenessn genelicco
seling: A survey of practilione..s.Am J Med Genet 1997;72:172-179
Bowles'Biesecker , Marteau TM, The fuure of geneticcounseljng:An in
national persp€ctive,Nat Cenet 1999;22:133-137.
Burke w: Genetic tesrins.N Engl I Med 2002i347:1867-1876
Farrell MH, Certain LK, Farrell PM, Genericcor:nsetingand risk conmu
cation services f newborn screeningprograms.Arcb Pediatr Adolesc M
2001r155:120-125.
Frver AEr Clinicatgenetic ervicesr criviry, outcome,eff€ctivenessnd qua
Summary of a report of rhe Clinical Genetics Commifte€ of the R
Coljege of Physicrans- Roy Coll Physidans Lond 1997\3r:624-621.
ceneclinrcs:[email protected].
Hayflick SJ,Eiff, M?, CarpenterL, et al: Primart care Physicians'ut,liza
and perceprionsof genetics ervices.Genet Mea 1998\1:13-21
Holornan NA, Watson MS: Prornoringsafeand effectivegeneric esting n
United Srates:Final report of the rask force oD geDetjc esting, Bethe
MD, Human Genome Resea.ch nsrilute, 1997.
Hubbard R, Lewontin RC: Prrfalls of genetic testins N t,gl / M
199ti:3i4:1192-1194-
Preimptantationgeneticdiagnosis-For or a8ainst humamty? Ldn.et 2O
364:1729-1730.
PressN, Brown€r CH: Characterrsrics f wornen who refusean offer of
natal diagnosis:Dara from the California marernal serurnalpha fetopro
blood tesr experience.Am I Med Geftet 1998;781433445.
Sermon K, Van SteineghemA, Liebaers : Prermplantariongenetjcdiagn
Laicet 2004,363 1633-l 640.
ve.linsky Y, Rechitsky S, SharapovaT, et al: PreirnpLantationHLA tes
I AMA 2O04;291:2O79-2085
Ve.linskv ! Rechrtsky S, Verlinsky O, er al: Preimplantat,ondiagnosj
sonic hedgehogmutation causing amilial ho{oprosencephaly r" EzglJ
2001r348:1449-1454.
1
v

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 42/177
Part(.Vletabulic
errorsof metabolism.Most mutations are clinically inconseguenlral nd represent
may never ause linical iseasen e lifenme f the ndividual.
Potencialpsychosocial mplicatio of such findings can be
der.astatingand deservesserious consideratrons.ntrauterine
diasnosisf mosrgenetrconditionssnot' feasiblendha sbeen
usei routinel-vo Jetecraffected erusesn the population ar risk(seeChaprer 6) .
Childrin with inbornerrorsof metabolism ay present ithone or moreof a largevarier-v f srgns nd symptoms. hesemay
includemetabolic cidosis,ersistencomiting, atlure o rhrive,
diagnosis.
NEONATAf-ER|0D.nborn errors of mecabolism ausing linical
findings are usuallv nonspecificand simiLar o lhose seen n
infants ..ith epsis.n inbornerrorof metabolismhould econ-
sideredn the differennal iagnosis f a severelyll neonatalinfant,and special rudies houldbe undertakenf the ndexof
susprcions high(Fig.84 1).Infantswichmecabolicisorders re usualLy ormalat birrh;
I seasBscalcium and response to intravenous injection of glucose
calcrum usually establish hesediagnoses.Becausemost inb
errors of merabolism are inherited as autosomal recessive ra
a history of consanguinitvand/or death in cheneonaralpe
should increase suspicion of rhis diagnosis. Some of these di
ders have a high incidence rn specific population grou
Tyrosinemia 1'pe1rs nore common among French-Canad
of Quebec than in the general population. Therefore, knowle
of the echnic background of the patient may be helpful in d
oosis. Physical examination usually reveals nonspecifc 6ndin
with most signs related to rhe central nervous s,vs
Hepatomegaly is a common finding rn a variety of inborn er
of merabolism. Occasionally, a pecuhar odor may off-eran rnv
able aid to the dragnosis (seeTable 84-3). A physician caring
a sick infant should smell the patient and his or her excretr
for example, patients with maple syrup urine disease have
unmisrakableodor of maple syrup in their rrrine and on t
DOOleS.
Diagnosis usually' requires a variety of specrfrc laborat
st dies. Measurements of serum concenlrations of ammo
bicarbonate, and pH are often very helpful initialLy in differe
acingmajor causes f metabolicdisorders seeFig. 84-1). El
t ion of blood ammonia is usuall y causedby defecrs f urea c
enzymes. nfanrs with elevatedblood ammonia le"els from u
cvcle defecrscommonly have normal serum pH and bicarbon
values; rvirhouc measurement of blood ammonra, they m
remain undrasnosed nd succumb ro their disease,Elevatio
,...,. u-.oii" is also observed rn some infants with cer
organic acrdemras.These infants are severelyacidocic becaus
accumulationof organic acids n body Ouids.
When blood ammonia,pH , and bicarbonate aluesar enorm
other aminoacidopathies (such as h,vperglycinemia) or ga
tosemia should be considered;galaccosemic nfants may
manilest cataracrs, epatomegalr' , scites, nd jaundice.
Most inborn errors of merabolismpresenting n the neon
penod are lethal il specific redtffient is not iniriated rmmedia
Specilic diagnosrs, even in an infant in rvhom death se
inevitable, is of great importance for genetic counseling of
familv (seeCbapter 83;. Every effort should be made co de
mine the diagnosrs while the infant is aiive; postmortem exa
narion is noc ah,r'avs helpful, A specr6c diagnosis may
esrablished -v measuremenrof abnormal metabolices n b
flurds, bv assay of the specific enzyme activit-vror by identil
r ion of chemutant gene.
CHILDBEN FIER THE NEONATAIPER|0D.Most inborn errors
metabolism rhat cause symproms in the 1sr ferv days of
exhibit milder varianc brms chat have a more insidious onThese forms may escape detecrion during tbe neonatal per
and the diagnosis may be delayed for months or even years. E
clinical manifestations in children wrrh rhese orms are commo
nonspeci6c and may be attributed to perinatal nsulcs.
Clinical manifestations, such as mental retardation, m
delicits, developmental regressron,convulsions, m,vopathr', e
rent emesis, and cardromyoparhy are the common finding
older children. There may be an eprsodic or intermiftent paft
with episodes of acure clinical manrfesrationsseparate
periods of seemingly disease-free tates.The episodes are usu
An inborn error of metabolism should be considered in anv c

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 43/177
5Ag PARI r MebbolicDi$€rs€6
Initial indingBncludeoneor moreot the ollowing:a) Poorfeedingb) Vomitingcl !'BthargY . Nor r€sDonsiveoo) uonvuElont intrave;ous lucose r calciume) uoma
Nomal
IObtain
bloodpHandCO2
Figure 8+1. Clinical approach co a new
infant wirh a suspectedmetabolic disorderschema s a guide ro rhe elucidadon of so
rhe metabolic disorders in oewborn inAlthough rome exceprjonq o rhis schemair is appropdate for most cases,
r-rr--l
Obtain
High
Obtain
bloodpHandCOz
Normal Normal niongap

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 44/177
with one or more of rhe following mani{estations:-rnexplained
mental etardation,developmenral elay ot regression, r motor
deficitor convulsions; nusualodor,particularlyduring an acute
illness; ntermittentepisodes f unexplained omiting, acidosis,
menral deterioration,or coma; hepatomegaly;enal stones;or
muscleweakness r cardiomyopathy.
Grosse SD, Dezateux C: Newborn screenirg for jnherired metabolic disease
Lancet 2007;369:5-6.Marsden D, Larson C, Levv HL: Neit'born Screenihs o. rnetabolicdisorders'
J Pediatu2006;148 51 7 5 84
McBryde KD, Kershaw DB, BunchmanTE, er 1, Renal replacemenr herapv
in rhe rreatment of confirmed or suspected born errors of rnetabollsm.
Pediatr 2006;L 48:7 7 0-7 7 8.
Warsbren SE: Neuborn Screening for merabolid dtsorders -/AMA
)006;29 6:993-994
85.1 PHENvIALAI{INE.ra i Bezvani
viduals was found to be close o that of normal subiectswhen
Ch6pler5r Delgstin Metabolisnl ArDiro cids
studiedby magletic resor]ancepecroscopy MRS)and imag(MRI) echniques.
CtASSICPHEt{YLKETONURIA(PKUl.evere yperphenylalanin(plasma henylalanineevels>20 mg/dl-), f unrreated'nvariaresults n the development f signsand symptoms fclassicPKexceot n rare unDredictable ccasions
ClinicalManitestations.he affected nfant is rormal at biMental rerardation may develop gradually and may not evrdent or the 1st few months. It is usually severe, nd m
patients require institutional care if the condidon remaunreated. Vomiting, somerimes evereenough co be misdnosed as pyloric stenosis,may be an early symptom. Olunreared children becomehyperactive,with purposeless oments. hyrhmic ocking, nd arhetosis,
On physicalexamination, hese nfantsare ighrer n theircoplexion han unaffected iblings.Somemay havea seborrheeczematoidash,which s usuallymild and disappearss he chgrows older.Thesechildren have an unpleasant dor of phelacetrc cid,which has beendescribed s mustyor mousev. hare no consistentEndings on neurologic examination. Minfanrs are hypertonic wirh hyperactivedeep rendon refleAbour 25% of childrenhave seizures, nd more han 507" helectroencephalographicbnormalities.Microcephaly, rominrnaxiJlawith widelyspacedeeth,enamelhypoplasia, ndgro
rerardationareother common indings n unueated hildren TclinicalmaniFesrationsf classicPKU are rarelyseen n thcountries n which neonatal creening rograms or the detecof PKU are n effect.
MITDER OBMSO' HYPEBPHENYI.ATAI{EMIA" ION-PKU YPPHENYIAIANII{EMIAS.n any screeningprogram for PKUgror-:pof infants are identilied in whom initial plasma ccentrations of phenylalanine are above normal (2 mg/120 pmoleil) but <20 mgidl (1,200pmole/L).These nfantsnot excretephenylketones. linicalln rhese n{antsmay remasympromatic) ut progressive rain damagemay occul gra
ally with age,Thesepatientshave milder deficiencies f phealanine hydroxylaseor its cofaclor retrahydrobiopterin B
than rhosewith classicPKU. AftemDtshavebeenmade o c
sif,vhese atienrs n differentsubgro sdepending n thedeof hyperphenylalaninemia,ut such practicehas ittle clinor therapeutic dvantage. s with classicPKU, defciencyof Bshould be nvestigatedn all infants with milder forms of hypphenylalaninemiasee ater).
Diagnosis. ecause f gradualdevelopment f clinical mantarions of hyperphenvlalaninemia,arly diagnosiscan onlyachieved y mass creening f all newborn nfants(seeater)infantswith positive esults rom the screenor hyperphenynrnemia, diagnosrs should be confirmed by quanticameasurement of plasma phenylalanine. Idenctficationmeasurement f phenylketonesn the urinehas no place n screening rogram. n countriesand placeswheresuchprograre not in effect,however, dentificationof phenylkeconesn
urineby ferricchloridemay ofler a simple est or diagnos
infants with developmental nd neurologicabnormalities.Othe dragnosis f hyperphenylalaninemias established,eficieof cofacror BHa)should be ruled out rn all affectednfants wproper studies rer).
Neonatsl cre for Hyperphenylslaninonia.ffective ndatively inexpensivemethods for mass screeningof newbinfantshavebeendeveloped nd areused n the UnitedStatesseveral ther countnes.The bacterial nhibition assav f Guthwhich was the 1st method or thepurpose,has been eplacemoreprecise nd quanritativemerhods fluorometricand canmals specrrometry).ll thesemerhodr equire fe* dropblood,which areplacedon a filter paperand mailed o a cenlaboratory or assay. loodphenylalaninen affectednfantsw
PKU may se to diagnosticevelsas earlyas 4 hr afterbirth e

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 45/177
530 PARTX Metabolic iseasos
Protein ynthesis
I
in the absence f protein feeding. t is recommended, owever,that the blood for screemns e obtained n the 1st24-48 hr oflife after feedingprotein rJreduce the possibilityof false nega-tive results,especiallyn rhe milder forms of the condition.
Treatment,hegoalof therapy s to reduce henylalaninen thebody; formulas ow in or free of this amino acid are availablecommercially. he diet should be startedas soonas diagnosissestablished.t is generallyaccepted hat infantswirh persistentplasma evelsof phenylalanine 6 mg/dl (360 pmole/L) shouldbe reatedwith a phenylalanine-rescrictediet similar to that forclassicPKU.No dietary estriction scurrently ecommendedor
- Fumarylacetoacetate
Protein ynthesis
Succinylacetoacelate
iSuccinylacetone
Fumarate Acetoacetate
infants whose phenvlalanine levels are between 2 and 6 mPlasma concentradons of phen;rlalanine n treated patients shbe maintained as close to normal as possible. Becausephenynine is not synthesized by the body, overtreatment rnay leaphenvlalanine deficiency manifested by lethargy, failu(e !o thanorexia, anemia, rashes,diarrhea, and deathi moreoveq tyrobecomes an essential amino acid in this disorder and its adeqrntake must be ensured. Controversies exist regarding the "alable" degree of residual hyperphenylalaninemia rn trepatients. It is generally believed that plasma phenylalanine lshould be maintained between 2 and 6 mgldl- (120-350 prno
It
I
co2 + H2o
Fjgur€ 85-1 Parhwaysof phenylalanineand ryrosin€ metabolism. nborn effors are depided as bars crossing he reaction ato1r,(s). Path*'ays for synrhcofactor BH, are shown in rrlpl?. PKU. refen to defectsof BFli metaboLsm hat affect rhe phenvlalanine, yrosine,and tryprophan hvdroxylases seeFig2 and 85-5). Enzlmes: (1) phenylalaninehydroxylase,(2) carbinolamjnedehvdratase, l) d,hydrobioprerin reducrase, 4) 6,pvruvoylrerrahydroprerinsyn(J) guanosine rjphosphate(GTP) c-vclohydrolase,6) tyrosine aminotransferase, 7a) intranolecular reaffangernent, 7+7a)4-hydro4?henylpvruvare dio
nase,8)
homogentisicacid dioxygenase, 9) rnaleylac€toaceraresomerase, 10)fumaryLacetoacecateydrorylase.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 46/177
alanine-restricted iet for l ife.
Oral adminisrration of the cofactor tetrahydrobiopterin (BH.)
through a regional reatmentcentet
Pregnancyn Womenwith HyperphenylalaninemiaMaternal KU).
nraiata-iledon a phenylalaninc-restrictediet before and during
ch e us cdescribed ongeniralanomahes n therr offspring
HVPERPHENYLATANINEMIARO MDEFICIENCYTTHE COFACTOR
BHa. n 1 2% of infants t ith hyperphenylalaninemia,he defecr
resides n one o{ rhe enzymesnecessatYot producoon or recv
transmitrersdopamine se eFig. 85-2) and serotonin seeFig. I l5-
Chaprer 5 r Delectsn Metabolism l AminoAcid$ .
5). BHr is also a cofactor for nitric oxide s-lnthase,hich
al,vzeshe generationof nirric oxide from arginine.Patientsw
BH1 delicienc,v re diagnosed er,v arl-vn life because llparie
u'ith PKU and hvperphenylalanirremja are rested or the poss
ir,vof this cofactor deliciency.
BH. is svnthesized rom guanosine triphosphare thro
severalenz-vmatic eactions (sce Fig. 85 1). Four enzvme d
ciencieseading o defectrve Hq fbrlnacionhave beendescr
.\{ore than half oi the reportedpatienrshave had a deflcien
6 pvrur.o,vhetrahydropterinynthasc PTPS).
Clinical Manifestations.nianrs with cofactor deficiencyidencif ied uring screening rograms or PK U because f evid
of hvperphenvlalaninemia. Lasma henylalanine evels may
as high as rhose in classic t'KU or in rhe range of nilder fo
of hvperphenylalaninemia. NeurologJc manifestations, such
.loss f }ead c ontrolr truncal hl,potonia (f loppy baby), drool
su.allowing diflicufties, and myoclonic seizures, develop a
3 mo of agedespiteadequare iecary-herapv.
0iagnosis. BHa deficiencv and the responsible enzyme de
mav be dragnosed by rhe following tests: measuremen
neoprerin (oxidarive product of dihydroneoprerin riphosph
and biopterin (oxidative producr of dihydrobiopterin
retrahydrobiopterin) n body fluids, espectallv nne (seeFig.
1). n patientswirh guanosine riphosphate GTT) cvclohvdro
defciency, urinary excretion of both neopterin and biopteri
very lorv. In patients wirh 6 pyruvo,vhetrahydropterin syntdeficienc,r', here rs a marked elevation of neopterin excretion
a concomiraot decrease n biopterin excrelion. In patienrs
dihydroptcridine reducrase eficiency, eoptern is normal,
bioprerin rs verv high. Excretion of biopterin rncreasesn
enzylrre deficiency because rhe quinonoid dih,vdrobiopt
cannot be rec,vcled nto BHa. Patients u.ith carbinolamine d
dracasedeficiency excrete 7-bioprerin (a n unusual isome
bioDrerin) n their urinc.llt{r l.OADlN-c I-I l5 . Ar oral dose of BH4 (20 mg/kg)
malizes piasma phenylalanine n parients * ' ith BHa defici
rr. ithin 4 to 8 hr The blood phenylalanine bould be elev(>400 gmole/L) to enable nterpretarionof che esults.This
be achievcd by discontintJng diet rherapy for 2 da1's before
tesr or by administering a loading dose of phenylala
1100mg/kg) 3 hr before tlre tesr.t\ lYN'll l ASSAY,The acci rity of dihydropreridine educ
can be measured n chedr,v blood spocson the filter paper u
Tyrosinase
DOPA
Tyrosinase
M elanosom e- - - - - -
Tyrosine
3,4,dihydroxy-
phenylalanineDOPA)
1 6 t
Dopamine
l oNorepinephrine
l ^| ( 4 1
Epinephine
HO cH2-cH cooHNH z
Tyrosine
DOPAQuinone
Pheomelanin(yellow-red olymer)
It
Eumelanin(black olymer
IThyroxine
L
Fieure 3 j t. Orher Frthwa"s in'olving t_vrosine etabol ism. KtJ' i rdrc . r re !hyperpheu,v la lancLrraut ro retrah,rdrobioptermBH!) dcl iciency sc
8j 1) [nzymes: t] r_vnrs ine_vdrrxi lase,2) arcm.ric L-aminoacr< l ccarboxr laseAADC), (3) dopamrnc vdrox l lase, 4) phenyLerhanolamlnem
!ranst i rasePNN{T).

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 47/177
532 PARTX MetaholicDisoases
for screening purposes. 6-Pyruvovltetrahydropcerin synthaseactivity can be measured in the liver, krdneys, and eryrhrocvtes.Carbinolamine dehydratase activity can be measured in the liverand kidneys. GTP cyclohydrolase activify can be measured in theliver and in cvtokine {interferon-y) stimulared mononuclear cellsor fibroblasrs (the enzyme activity is normally very low in unstimulated cells).
Ireatneol. The goals of therapv ate to correct hyperphenylalaninemra and to reslore neurotransmifter deficlencies n cheCNS.
l he con r ro lo f h lpe rpheny la lan inem ias m po r tan r n pa t ien rs
n'ith cofactor defciencl., because high levels of phenylalanineinterfere with che rransport of neurotransmifter precursors (cyro-sine, tr,vprophan) inro the brain. Plasma phenylalanine should bemairtained as close to normal as possrble (<6 mg/dl). This canbe achieved bv a combinarion of a low phenylalanine diet andoral supplementation of BHa, Intbnts with GTP cyclohydrolaseor PTPS deticiencies respond more readrly to BHa rherapy (5-10 mg/kgiday) than those with dihydropteridine reducase defi-crencl', In the latt er patient s, doses as high as 20 mg/kg/day maybe required. BHa for replacemencrherapy is commercially avail-able, although r rs expensive.
Adminisrration of defrcient neurorransmirrers iL-dooa and 5-hldroxvtryprophant ir recommended ve n when rrear;ent wirhBHr normalizes ptasma levels of phenylalanrne. BHa does norreadily enrer the brain to restore neurotransmitter production.
Supplemenration wirh folinic acid is also recommended inpatients \:r,lth dihydropteridine reductase de6ciencl..
Hyperprolactinemia occurs in patients with BHa deficrencyandmay be due to dopamine deficiency lwhich is the major prolacrininhibiting factor) rn rhe hypothalamic region. Measurement ofserum prolactin levels may be a convenient method for monitor-ing. adequac,v of rreurotransmitter replacement in affectedpanents,
Some drugs such as trimetoprin sulfamethoxazole, methofiex-atet and other antileukemic agents are known to inhibit dihy-dropteridine reductase enzyme activity and should be used withgrea! caurion in patients with BHa deficiencv.
Genetics and Prevalence. AIL defecrs causing hyperphenylala-
ninemra are inherited as autosomal recessive rairs. The oreva-len ie o i PKU in rhe Un i redSta res s es r im a red t l / 14 ,000 ru
1/20,000 live births. The prevalence of non-PKU hyperpheny-lalamnemia is esrimated ar 1/50,000. Th e condit ion is morecommon in whrtes and Native Americans and less prevalent inblacks,Hispanics,and Asians.
The gene for phenylalanine hydroxylase is located on chromo-some 12q24.1 and many disease-causing urations have beenidencified in drfferenr families. The majority of parients are com-pound heterozygotes for rwo different mulaflr alleles. The gene
for PTP synthase, the most common cause of BH4 deficiency,resides on chromosome 71q22,3-23.3, the gene for dihy-dropteridine reduclase is locared on chromosome 4p15.3, andthose of carbinolamine dehydratase and GTP cycLohydrolaseareon 10q22 and 14q22.1-22.2, respectively. an y disease-causrngmutations of thesegeneshave been rdenrified. Prenaral diagnosisis possible using speci6c geneuc probes in cells obrained from
chorionic vil l i hiopsl' .
TETNAHYDROBIOPTEBII{EFECTSITHOUTHY CRPHEIIYTALANII{ETJIIA
IIEREDITAEYROGBESSIVEYSTOI{IA,UTOSOMATOMIIIAIITooPA-sEsPol{srvEysToNrA,EGAWA|SEASESEEArS0GHAPTER 9t.3). Thrs rare form of dystonia, 1st described in
Japan, is caused bv GTP cyclohydrolase deficiency. t is inheriredas an autosomal domrnan! ffaic and ts more common tn femalesthan males (4:1)
Clinical manilestations usually occur around 5-6 yr of age andare heralded bv dystonia of the lorver Lmbs, which may spread
to all extremities wichin a few years. Torlicollis, dystonia oarms, and poor coordination may precede dystoma of the l
becoming worse by rhe end of the dav and improving with sParkinsonian signs may also be present or develop subsequwith advancing age.Patients may be misdiagnosed as havingbral palsy. Late presentation in adult [fe has also been repo
Laboratory findings shou. no hyperphenylalaninemia,reduced levels of BHr and neoptenn are found rn rhe spinal
Dopamineand t r s m erdbo l i re \hom ovan i l l r c c id ) m ly a lreduced in the spinal flLrid. lt is believed that the enzymeciency in this condition is less severe han that of rhe autosrecessive orm of GTP cyclohydrolase deficiency, which rs ciated wirh hyperphenylalaninemiase e arlier].The existenasymptomatic carriers indicates that other factors or genesplay a role in parhogenesisof the phenorype. The asymptomcarrier mav be rdentified by measuring the rario of plasma phlalanine to tyrosine after an oral dose of phen,vlal(100 mgikg); the ratio increases significantlv (=3 times ano fm a l va lueat 2 h r ) i n the asvm p lom a t t ca r r ie r .
Diagnosis may be confirmed by reduced levels of BH4neopterin in rhe spinal fluid, by measuremenrof the enzyme airr. and by idenrif icarion i rhegenedefectLsee arlrer].Clinicthe condirron should be differentiated fuom orher causesof
t on ias nd ch i ldhoodPark inson ism ,spec ia l l v) o \ ine hvdlase (seeChapter 85.2) and aromatic amino acid decarboxdeficiencies.The sriking diurnal partern of dystonra is an imran t c l in rca l nd ing n tavo ro i CTP cyc lohyd ro lasee f i c ie
Treaiment wirh L-dopa in conjunction with a peripheral ddecarboxylase inhibitor usually produces dramaric improvem
85.2 TyRosrNEGrant . Mitchell ndlraiBezvani
Tyrosine, obtained from ingesced proteins and synthe
endogenously from phenylalanine, is used for protein synthand is a precursor of dopamine, norepinephrine, epinephmelanin, and thyroxine- Excess yrosine is metabolized to cadioxide and warer (see Fig. 85 1). Hyperryrosinemia is obsewith de6ciencies of r_vrosne aminorransferase, 4 hvdroxvphpyruvate diorygenase (4-HPPD), or fumarylacetoacetate h1lase (FAH). Deficiencies of other enzymes involved in rvrodegradation cause iftle or no increase n blood levels of tyrosAcquired hypertytosinemia may occur tn severe hepatoceldys func t ion l i re r la i l u re t , cu rvy v r t am inC i r rhe o fac roche enzyme 4-HPPD), and hyperthyroidism; hyperc,vrosinema common artifact in blood samples obtained soon after eaThe clinical specrrum of heledltary byPertyro*nemias is not
wBosrNrMrAypE {wBosr osts, HEREDTTABYyB0stNH€PAT0RENALYE0S|NEMlAl.n this condition,caused y a ciencyof the enzymeFAH, a moderateelevarionof serum rsine s assocrated ith severe nvolvementof the liver. kidnan d peripheral erves. hese indingr may be due ro amulation of metabolites of tyrosrne degradation, espesuccrnylacetone.
ClinicalMaoifcstations. he affecred nfant rypically prebetween and 6 mo of agebut rarely may become ympromas earlyas 2 wks o{ ageor may remainseemingly ealthy or1st vr of life. The earlier hepresentation,he poorer rs hepnosis. The l yr morcality,which is abour 60y. in infantsdevelop5y11p1o-.6efore2 mo of age,decreaseso 47o rn nfwho become ymptomaticafter 5 mo of age.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 48/177
The major organs affected are the liver, peripheral nerves, and
kidneys. An acucehepatic crisis commonly heralds the onset of
the diseaseand is usually precipitated by an intercurrent illness
that Droduces a catabolic state. Fevef, irritabiliry, vomirrng,
hemoirhage, hepatomegaly, jaundice, elevated levels of serum
transaminases, and hypoglycemia are common. An odor resem-
bling boiled cabbage may be present, due ro increased methion-
ine metabolites. Most heparic crises resolve spontaneouslt but
may progress ro liver failure and death. Berween the cnses,
varying degreesoffarlure
tothrive, hepatomegaly, and clotttng
abnormalties often persist. Cirrhosrs of the liver and, eventually,
heparocellular arcinomaoccur with increasing ge ;carcrnoma ''
unusual before 2yr oI age.
Episodes of acute peripheral neuropathy resembling acute por-
Dhvria occur in =407" ol affected children These ctises, often
iriggered by a minor nfection, are characterized by severepain,
often in the legs,associacedwtth hypertonic postunng of the head
and trunk, vomiring, patalytic ileus, and, occasronally, self-
induced injuries of the tongue or buccal mucosa' Marked weak-
nessan d paralysrs ccur rn =307oof the episodes, hich may lead
to resprratory farlure requiring mechanical ventilation. Crisescyp-
icallv lasr I to 7 daYs.
Renal involvement rs manifested as a FanconiJike syndrome
with normal anion gap metabolic acidosis, hyperphosphaturia,
hyp.,phosphatemia,nd vitamin D-resistanL ickets.Nephrome-
giiy an d .ome degreeof nephrocalcinosi' , re often found by
ultrasound examination.
Hypertrophic cardiomyopathy is occasionally seen in these
lnfants.Laboratoty Findings. In untreated patients, liver function tesrs
are perturbed in a characterisnc fashion. c feroprorein level is
incriased, ofcen markedln and liver-synthesized coagulation
factors are decreased n most parients; serum levels of transaml
nases are increased, parlicularly during acute heparic episodes.
Serum concentration of bilirubin is increased with hver failure.
Increased evels of cr-fetoprotein are present in rhe cord blood of
affected infants, indicaring intrauterine liver damage Plasma
ryrosine level is dependent on diet; tyrosine level has less diag-
nosdc value than that of succinylacetone (see ater) Elevations rn
serum concentratiorlsofmethionine and other amino acids, char-
acreristic of liver farlure, may also bepresent. HyperphosPhaturia
and hypophospharemia are common. Generalized aminoaciduria
mav occur. The urinary level of 5-aminolevulinic acrd is elevated
(due to inhJbition of 5-aminolevulinic hydratase by succinylace-
tone). The presenceof elevated evels of succinylacetone n serum
an d urine is diagnoscic seeFig. 85-1).
Diagnosis is usually established by dernonstration of elevated
levels of succinylacetone in urine or blood. Neonatal screening
methods detect h;rpenyrosinemra; only a minority of patjents
wirh ryrosinemia type I ate identrlied by these methods. Succ iny-
lacetone, whrch is not detected by the current screening methods,
rs rhe preferable initial metaboLite tested. Tyrosinemia rype I
should be differentiared from other causes of hepatitis and
hepatrc failure in infants, including galacrosemia, hereditary fruc-
toie intolerance, neonalal iron storage disease,giant cell hepatl
t is, and citrull inemia yp e II (seeChapter 85 11)
Treatmentand outcome. A diet low in phenylalanine and tyro
sine can slow down but nor halt rhe progtession of the conditjon.
The treatment of choice is nitisinone (NTBC, 2-(nitro-4-trifluo-
romethylbenzoyl)-1,3-cyclohexanedione), which inhrbits tyrosine
degradation at 4-HPPD {seeFig. 85-1), Thls treatment prevents
acute hepatic and neurologic crises. Patienrs treated wich nrtisr-
none are also prescribed a diet low in phenylalanine and tvro-
sine, Ahhough nrtisinone stops or greatly slows progression of
the disease, much preffeatment liver damage is noc reversible.
Therefore, patients must be followed for development of hepa-
rocellular carcinoma. On imaging, the presence of a liver nodule
usually indicates generalized crrrhosis. Accurace distinction
between benign nodules and malignant ones is difficult to obtain
ChaDter5 oelectsn Metabolisml Amino cids
through maging.Liver ransplantationsan effectiveherapyaalleviates he risk of hepatocellular arcinoma.The impacnitisinone rearmenton the need or liver transplantation s under study but dependson the stageof the drsease t whtherapybegins.
Genetics ld P]evalence. yrosinemia ype I is an aurosorecessiverait. The gene or FAH has beenmapped o chrosome15q;nunerous mutationshavebeen dendfied.DNA ansis is useful or molecularprenataldragnosis nd for rescingroupsat risk for specificmutationssuchas French-Canafrom the Saguenay-Lac aint-Jeanegion of Quebec.Tvronmra ype is panethnic;ack of FrenchCanadianor Scandinaancesrrydoes not exclude he diagnosis.The prevalence f condition s estimated o be 111,846ive births n the SagueLac Sarnt-Jeanegion.The worldwide prevalences estimarebe 1/100,000o 1/120,000. renatal iagnosisasbeen chiby measurement f succinylacetonen amniotic flurd, by enzymeassay n amniocyresor chorionic villi biopsv, andDNA analvsis.
TYROSINEMIAYPE I {RICHNER.HANHARTYNOBOME,GUTTANE0US B0SINEMIA).his rare aucosomalecessiveisois causedby deficiencyof ryrosine aminotransferase nzywhich results n palmar andplantar hyperkeratosis, erpetif
corneal ulcers,and menral retardation (seeFrg. 85 1). Ocmanifestations f excessiveearing, redness, ain, and phophobia ofrenoccur beforeskrn esions.Corneal esrons re psumed o be due to tyrosine deposirron. n contrast o herpulcers, orneal esions n tyrosinemiaype I stainpoorly withorescrn nd often are brlateral.Skin lesions,which may devlacer n life, includepainful, nonpruritic hyperkeratoticplaq
on rhe soles,palms, and fingertips.Mental retardation, whoccursn <507oof patients,s usuallymild to moderate,
Abnormal aboratory indingsare imited to significant ytyrosinemia 20-50 mg/dl; 110-2,750pmole/L) and tvroiluSurprisingly, -hydroxyphenypyruviccid and ts merabolitealso elevated n urine desprtebeingdownstream rom the mbolicblock see ig .85-1).This s presumedo be due o shing of ryrosinevia other transaminasesn rhe presence f h
ryrosine oncencrations,he condicrons due o the deficienche cyrosolic raction of hepatic tvrosine amrnofiansferascontrast o tyrosinemia ype , liver and kidney unction, asras serumconcentratlons f other aminoacids,are normal.
Diagnosis s established y assayof plasma yrosrnecontration.Susrained ypertyrosinemia n a nonrestncted iet s aseen n liver failure; the level of plasma yrosine is hrghetyrosinemia ype l and oculocu!aneous anifestat ions reabin liver fail-rre.Diagnosis f rype I ryrosinemramay beconfirby assay f ryrosineaminorransferasectivity n liver or bv Dana)ysis f the mutant EeDe.
Treatmen! wjth a diet low io tyrosine and phenylalaimproves he biochemicalabnormalitiesand may result n dmatic healing of the skin and eye lesions.Some observasr.rpporthe easonable laim rharmental erardationmay be
ventedby earlv dietary estrictionof t,vrosine. he gene or rsineaminotransferases mapped o chromosome 6q and sevdisease ausinemurarionshave been dentilied.About haltreported aseJare f Italiandescent.
rYR0SltlEM|AYP Ell {PRIMARYEFICIENCYF -HPPDl. nfew cases avebeen eported;most weredetected v amino adeterminations erformed or vatrousneurologic indings.This doubtas ro whether his enzyme eficiencyauses ny clinabnormalities. ge of onsethas been rom 1 to 17 mo, Devemental delan seizures,nrermittenr ataxia, and self-desrrubehavior are reDorted. No liver or renal abnormaliriespresent.Asymplomatic nfants have been dentilied n neonscreenlnSrograms,

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 49/177
53{ r PARTX MetaholicDiseases
The diagnosis is suspected n chrldren with sustained moder-ate iflcreases n plasma levels of tyrosine (350-700 pmole/L) andthe presenceof 4-hydroxyphen,vlpvruvic acid and rts metabolites(4-hvdroxvphenyllaccicand 4-hvdroxyphenylacecicacids) inurine. Diagnosis ma,v be confirmed by denonstration of lowactivir,vof 4 HPPD enz,vme n li ver biopsv or presenceof muta-tions rn the 4-HPPD gene.
Given rhe possibleassocrarion rith neurologrcabnormaliries,dietary reduction of plasma tyrosine levels s reasonable. It i s alsological co atrempt a trial of vitamrn C, the cofaccor or 4-HPPD.The condit ion is inhericedas an aulosomal recessive rait. Th egene for 4-HPPD rs mapped co chromosome 12q24-qter
TBANSIENT YR0SINEMIA F THENEWBORN.rl a small numberof newborns, plasma cvrosine may rise co as high as 60 mg/dl(3,300pmole/L)d uring r he 1sr 2 u'k of l i fe. Most affected nfanrs
are premature and are receiving high-prorein diets, The condition
is presumablydue to dela,redmaruratronof 4 HPPD enzyme see
Fig. 85-f). Lethargl' ,poor feeding,and decreasedmoror acrivityare noted in some patients; most are asympromatic and come tomedical attention becauseof a high blood phenylalanine evel,rendering rhe screening rest for PKU posirir.e. Laboratory find-ings rncludemarkcd elevationof plasma vrosinewlth a moder-ate increase n plasma phenylalanine,Th e presence i markedhyperty rosrlemia ditferenciates this condition from phenylke
tonuria. 4-H_y-drox),phenylpyruviccid and irs metabolires (4 -
hydroxyphenyllacticand 4-hydroxl'phenylacetic crds)are alsopresent n rhe urine. HypertJ'rosinemia sually resolves ponta-neously n th e 1sr mo of l ife. The condirion is often cottectedprompdv by reducing the amount of protein in the dier (t o
2 Elkg/24 htJ and by administering vitamin C (200-400 mg/24
hr). Mild incellectual ellcitshave been eporred n some ull-term
infanrs lr.ith this disorder, but rhe causal relationship to hyperc,v-
rosiiemia is nor conclusivelv scablished,
HAWKINSINURIA. his rare condit ion (named after the 1staifecced amily) is causedby a mutant 4-HPPD enzyme har car-alyzesa partial reactiolraDd releases n intermedrate ompoundused for diagnosis (seeFig, 8-5-1).This rntermediare s eitherreduced rcl li:rm 4-hydroxycyclohex,vlacetic acid (4-HCAA) orreacts with glutathlone to form the unusual organic acidhawkinsin (2-L-cysreine-S-y1-1-4-dihydroxvcvclohex-5-en-1-yl
acetic acid); secondarv glutachione de6ciency may occuf.Individuals vich hisdisorderbecome vmptomaticonl,vdunng
infancl'. The symproms usualLyappear after u.eaning from breasr-Feedingvith rhe nrroductionof a high-proteindiet. Severemeca-
bolic acidosis, erosrs, ailure to f ir ive, mil d hepatomegah;an d
an unusual odor (of a s&'imming pool) are described. N'lental
developmenr s usually normal.
Affected children and adults excrete the organic acids 4-HCAA, 4-hldroxyphenylpyruvic acid and its merabolites(4-hvdroxvphenyllaccrc and 4-hydroxyphenylaceric acids),.5-oxoprotine owing to secondarl glutathione deficiency),an dhawkinsil in rheir urine.Plasma ,vrosineevel s usuallynorma[.
Treatmcnt consrsts f a lor-protein drer breasrmilk) or a dietlorv in phenylalanineand t,vrosine.A trial rvi th large dosesoivLtamin C (u p ro 1,000 mg/24hr) rs also recommended. Notherap,v s needed after 1 yr of age. The same mutation, a substr-tution of threonine or the normal alanine codon a! posit ion 33of the 4-HPPD gene,has been dencified n unrelated patients wirhharvkinsinuria.
ALCAPT0NUfiIA. his rare (incidence =1/250,000) aurosomalrecessivedisotder is due to a deliciencl' of homogencisic acidoxidase, ra'hrch causes large amounts of homogentisic acid toaccumulate in the body and lhen lo be excreted il the urine lseeFie. 8-5-' l l.
tlinical manifestations of alcapronuria consist of ochronosisand archritis, rvhich occur in adufthood. The only sign of rhe dis
order in children is a blackening of the urine on standing.rs caused by oxidatron and polymerization of the homogenacrd. Urine uirh acrd pH may not darken even affer man,v hThis sign may never be noted, delaying rhe diagnosis unrrl ahood. Ocbrcxosis, seen clinrcail y as dark spots on rhe scleear cartilage, results from rhe accunulation oF the black polof homogentisic actd, Arthritis can be disabling and occualmost all affecredsubjeccswrth advancing age. t involvelarge oints (spine,hip, and knee) and is usuallv more sevm a le r . i l e rhsum a to id r rh r r t i s , he a r rh r i c i r
a 'acu re
\abations, buc the radiologic {indings are typical of osceoarthwith characteristic narrorving of the jornt spacesand calcificof the ntervertebra discs.High incidences f hearrdiseasem
an d aortic valvulris, calcif icarion f rhe heart valves, nd m,vdiaL nfarction) have been noted.
The diagnosis is confirmed by finding massive excretiohomogentisrc acid in urine. The enzl,me is expressed onl;' inliver and kidneys. Th e gene for alcapronuriamaps ro chrosome3q and several iseases-causingutations have beenti6ed, Alcaptonuria s most common in the Dominican Repand Slovakia.
There is no effecrive reatrnent for this disorder Nitisinonetreatment of tyrosinemia rype I) inhibrrs homogentisicprorioni its administration to patrents rvitb alcapronuria bplgment deposirionma1' be useful n prevention
ofarchntis
TYROSINE YDROXYTASEEFICIENCYINFANTITEARKINSOAUTOSOMATBECESSIVEDOPA-RESPONSIVEYSTONIACHAPTER 97.31. yrosine hydroxylase calalyzes thc formatioL-dopa from tyrosine (seeFig. 85-2). Deficiencr.of this enhas been reported in a felv chrldren r.ith dystonia and pa
sonism. The clinical picture resembles the aurosomal domidystonia due to GTP cyclohvdrolase deficrencv (see Cha85.1). The spectrumof the condit ion is nor full,vappreciat
Clinical manifestations such as jerky movemenrs of the lleading to spasriciry ard muscJe rigrdiry, expre$sionless ptosis,drooling, oculogyriccrises, nd parkinsonismmav sraearly rnfanc1.. Psychomotor rerardation has been secn in sparients. No diurnal variation of the svmproms has been uo
Laboratory indings nclude educed evels f dopamJne nmerabolice onovanrll ic acid (HVA) and normal concenrraof retrahydrobiopterinand neopterin n the spinal f luid. Sprolactrn evelsare usually elevated.
Diagnosisshould be considered n an y patients vichdysand parkinsonism. GTP cyclohydroxylase defrcienc,vshoulruled out bv proper studies seeearlier).Diagnosis s establbv che aboratory f indings (seeearlier)an d genestudy.
Treatment with L-dopa resufts in a dramatic improvemPatients unresponsrve to L-dopa have recentlv been repohora'ever,The cofldition is inhericed as an autosorlal recetraic. The gene for tyrosine hl.droxylase is rnapped to chrosome11p.
AIBlNlSM. Albinism is due to defecrs n the biosvnthesis andtribution of melanin (Table ll5-1). N{elanrn s synthesizemelanocyres rom tyrosine in a membrane-bound ntraceorganelle, the melanosome. Melanoc,vres originate from embr,vonic euralcrestand migrate ro the skin, eyes choroid
iris), and hair foll icles.The melanin n the eye s not secretethe adjacent issues,whereas he pigmenr n skin and hair fcles s secreted nto the epidermis and the hair shaft. The ramelanogenesis s ver,v low in the eye and very hJgh in cheand hair The bios-vntheticparhnay for melanin synthesis iscomplerelyelucidared seeFig. 85-2). The end products arepigrnetts: pheomelanin, which is a yellov,red pigment;
euffieldnin, a brown-black pigment.
Clinical rnanifesratiolls common in generalized albinismhvpup igm en ra r ronf t hesk inand ha i r .Pa t ren rs i rh nvo l r m

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 50/177
85-1), Attempts o differentiate ypesof albinismbasedon the
mode of inheritance, tyrosinase activity, or the ettent of
hypopigmentarion ave ailed to yield a comprehensivelassifi-.rtion. The followine classifications basedon the distributionof albinism n the body and the qpe of rnutatedgene.Not all
conditions associatedwith albinism are discussed nterested
readersare referred o more comprehensiveources see efer-
ences),0culocutaneousGenerslized)Albinism0CA). ack of pigment s
generalized, ffecringskin. hair, and eyes.Threegenerically is-iincr ormsexisr:OCAI, OCA2, nd OCAj. The ac kof pigrnent
is usuallymore severen patientswith OCAI; these ypesmay
nor be distinguishable linicalln however,becauseoI a great
in theseparients esidesn the tyrosinase ene,which is located
on chromosome 1q. Many mutant alleleshave been dentifred.
Most affected ndividuals are compoundheterozygoteor twodifferent mutant alleles.The condition can be subdivided o
OCAI A and OCAI B basedon enzymeactiviry and, to a lesser
er.:tent, linicalmanifestations.OCAI A (Tyrosinase-NegativeCA), A numberof mutations
in the tyrosinasegenerender the enzymecompletely nactive'Individualswith this form usuallyhave he most seve!€ as€ofgeneraUzedlbinism, linically,ac kof pigmenrn che ki n milky
whire),hair (whitehair).and eyes re dgray ridesl s evident tbinh and remainsunchangedhroughout life. They do not tan
and do not developpigmentednevi or freckles.OCA1 B. These mutations in the tyrosinasegene result in
enzymeswith some esidualactieities.Clinically these ndividu-
als, although completelydepigmented t birth, are capableof
GhaDtol86 Defccrsr llslrtolilm d Amino cids
developing omepigmentwith ageand become ight blond wlight blue or hazeleyes.They developpigmented evi and frlesand they may an. Thesepatients,depending n the degrepigmentation, trereonce subdivided nto different groupswere hought to begenetically ifferent.One nteresting ormthe temperature-sensiti ve lbinism in which the tyrosibecomesmore active n coolerpans of the body such as imThese ndividualshave no pigment n the scalpand uunk developsomepigment n arms and legs.
OCA, (TYROSINASE-POSITM OCA). This is the m
common orm of generalized lbinism. t i s particularlycomin African blacks.Clinicallv. hese ndividualsdemonstrate pigmentation f the skin and eyes t birth andcontinue o copigment hroughout their lives. The hair is yellow at birth may becomedarker with age. They have pigmentednevi frecklesbut do not tan. They may be clinically ndistinguishfrom OCAI B. These ndividualshavenormal ryrosinase ctiThe defect s in the p (pink-eyed ilution) gene,which is locon chromosome 15q. This gene produces the P proleinmelanosomemembraneprotein, the function of which is completely nderstood, atientswith Prader-Williand Angelsyndromeswho havedeledonoI chromosome 5 lack one cof the OCA, gene nd havemild pigmentary ilurion(seeCha80).
OCA3 (RUFOUSALBIMSM). This form has been dent
only in AIricans,African-Americans, nd natives f New GuiPatientshave eddishhair with reddishbrown skin as an adThe color of the skin is peculiar o this form. In the youngmanifestationmay be confusedwith that of oCAr. PatientswOCA3 can make pheomelanine ut not eumelanine. he mtion is n the tyrosinase elatedprotein 1 (TYRP1)gene, he furion of which is nor understood.
HERMANSKY-PUDLAK SYNDROME. This is a group oforders,eachcaused y mutation of one of the seven enesHto HPS7. Thesegenesare necessaryor normal sfiucturefunction of lysosome-derivedrganellesncluding melanosand plateletdensebodies. n most forms, a tyrosinase-poOCA of highly variableseverity s associated ith plateletfunction (owing to the absence f plateletdense odies)anaccumulation I a ceroid-likematerial n tissues, he cond
is transmittedas an autosomal ecessiverait and is mostprlent in Puerto Rico (types1 and 3, frequencyabour 1:2,0Bleeding endencies, ften manifesredas epistaxisand alonged bleeding imer are common. The ceroidJike materihistochemically imilar o that found in neuronalceroid ipocinosis.The accumulationof this material in tissues esulresrictive lung disease, nflammatory bowel disease,kidfailure, and cardiomyopathyn the 3rd or 4th decade f life.majoriry of patientshavemutations n IIPSl, which s locatecn
ASHI SYNDROME. Patientswith this autosomal ecessiveondition havepartial albinismand susdbility to infectionwith the presence f giancperoxidase-polysosomalgranules n granulocytes see Chapter 129), Tpatienashave a reducednumber of melanosomes, hich
abnormally large (macromelanosomes).atienrs who suearly childhood may develop a lympho{ollicular malignaMutadons in CHS1 gene locatedon the long arm of chrosome ) have been dentified n thesepatients,
0cularAlbinisn 041,Albinism s imited o the eyes.All th€frndingsof albinism see arlier)arepresent.The Xlinked resive orm (OAr) has beensegregated s a separate ntity. Mcases f autosomal ecessive cular albinism are Ielt to be mvariantsof OCA2.
OCULAR ATBINISM 1 (OA, NET'TLESHIP-FALLS TYOnly the hemizygotemale has he completemanifestationwsomeabnormal refinal pigmentation may bepreserf in hete-gore female carriers. The gene for this condition is locon the short arm of rhe X chromosome.An X-linl<edoc

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 51/177
536 PART r Metabolic isga6ss
albimsm with lare-onsetsensorineural eafness as also beenreporled.
Localized lbinism.This disorder s characterized y locahzedareas f hypopigmenration f skin and hair,whicb may bepresentat brth or developwith time,
PIEBALDISM. In this autosomaldominant inherrredconditron. che ndividual is usually born with a whrte forelock. Theunderlying skin is deprgmented.n addition, there are usuallywhite macules n the face, runk, and extremities. hewhite hairlock and che depigmented underlying skin are devoid of
melanocytes.Mutatlons in the KIT genehave been shown inaffecred atients.
\\,AARDENBURC SYNDROME. In this syndrome, aceraldrsplacement f inner canthi, broad nasalbndge,heterochromiaof irides and sensonneural eafness re associated ith a whiteforelock,This condirron s inheritedas an autosomaldominanttrart. !'our typesof this syndromehave been dentilied,Patiencswith rype have displacemenr f inner canthi, The condrtion scausedby mutations n rhe PAXJ gene.Type ll patientshavenormal innercanchi,and mutations n the MITI genehavebeenshown n somepatients.Patientswith type ll havealL he find-iogs seen n individuals with rype I, plus hypoplasiaand con-tractures of rhe upper limbs. The geneabnormalitv rs in thePAX3, Type IV is assocraredvrth Hirschsprungdisease,s het-erogeneous, nd mutat ions Lndifferentgenes EDN}, EDNRB,
or SOXl0) havebeen dentified n differentpacients.
85.3 METHIoNINE.lraiezvani ndDavidS.Bosenhlaft
The normal pathway for catabolism of methionine, an essentialamino acid, produces S-adenosylmethionine, whrch serves as amethyl group donor for methylation of a variety of compoundsrn the body', and cysteine, which is formed rhrough a series ofreacnonscalled rrans-sulfurarion Fig. 85-3).
H0M0CYSTINURIAH0M0CYST|ilEMlA). ost homocysteine,an
intermediate compound of mechronine degradation, is normallyremechy'lated o methronine, This mechionine^sparing reaction iscatalyzed by the enzyme methionine synchase,which requires ametabolite of folic acrd (5-rnethyltetrahydrofolare) as a methyl
donor and a metabolite of vitamrn Br2 (methylcobalamin)as acofactor (see ig. 85-3). Only 20-30% of r otalhomocvsternean d
ics dimer homocystine) is in free form in rhe plasma o{ normalindividuals. The rest is bound to proterns as mixed disulfides.Three major forms of homocystinemia and homocystrnuria havebeen rdentiGed.
Homocysliruria ue o Cystalhionine-Syntha$eCBS)Deliciency(Classic Homocvstinurial.This is the mos! conmon rnborn errorof methionine metabolism. About 40% of affected patients
respond to hrgh dosesof vitamin B{,and usuall,vhar.e milder clin-i ca l m an i f es ra r ion rhan hosewho a re un respons iveo v l t am in
B, rherapy. These patients possesssome residual enzl'me activiry-Infants rvith this disorder are normal at birth. Clinical mani-
festarions during infancy are nonspecifc and may include failureto thrive and developmental delay. The dragnosrs s usually madeafrer 3 yr of age, when subluxation of the ocular lens (ectopia
lentis) occurs. This causesseveremyopia and rridodonesis {quiv-ering of the iris), Ascigmatism, glaucoma, staphyloma, cararacts,retinal derachment, and optic atrophy may develop larer in life,Progressive mental retardation is common. Normal intelligence,however, has been reported. In an international survey of >600patients, IQ scores anged from 10 to 135. The higher IQ scoreswere noted in viramin 86 responsive patients, Psychiatric andbehavioral disorders have been observed in >50% of affectedpacients. Convulsions occur in =207o of patienrs. Affected indr-
viduals with homocystinuria manifest skeletal abnotmalresembling those of Marfan syndrome (see Chaprer 700);are usuaUy tall and thin, with elongated limbs and araodactyly. Scoliosis, pectus excavatum or carinum, genu valgpes cavus, high arched palate, and crowding of the teeth are cmonly seen. These children usually have fair complexrons,eyes, and a peculiar malar flush. Generalized osteoporosis, ecially of the spine, is the marn roentgenographic finding, Thrboembolic episodes involving both large and small vesespecially those of the brain, are common and may occur at
age. Optic acrophS paralysis, cor pulmonale, and severe hytension (due to renal infarcts) are among the serious consequeof thromboemboli sm, whrch is caused by changes n the valar walls and increased plarelet adhesivenesssecondary to vated homocl'stine levels.The risk of thromboembolism rncreafter sr-rrgical rocedures. Sponraneouspneumothorax and apancreatitis are rare comphcadons.
Elevations of both merhionine and homocystine (or homoreine) in body fluids are rhe diagnosric laboratory findiFreshly voided urine should be cested or homocystine, sincecompound is unstable and may disappear as che urine is stoCystrne rs low or absent in plasma. The diagnosis may be elished by assay of the enzyme in liver bropsy specimens, cultufibroblasts, or phytohemagglutinin-strmulated lymphocytes oDNA analysis.
Tieatmentwith high dosesof vitamin Bs (200-1,000 mg/2causesdramatic improvement in most patients who are ressrve to this therapy. The degree of response to vrtamin 86 trment may be different in different families. Some patrents
not respond becauseof folate depletion; a patient should noconsidered unresponsive to vitamin Bo until folc acid (1-5
24 hr) has been added to the ffealment regimen. Resrrictiomethionine ntake n conyunctionwith cysteine upplementis recommended for parients who are unlesponsive to vitaminThe need for dietary restrictrcn and its extenc remains conversial in patients with vitarmn 86 responsive form. ln sparients wrth this form, addition of betaine may obviate the nfor any dietary restncrion. Betaine (trimethylglycioe, 6-9 yJ2
for adults or 200-250 mg/kg/dav for children) lowers homoteine levels in body flurds b1' remethylatrng homocysteine
methionine (seeFig. 85-3); this may resuk in further elevadoplasma methronloe levels. This treatment has produced clinimprovement (preventrng vascular events) ln patients who unresponsive o vitamin 86 therapy. Cerebral edema has occLin a patient with vitamin 86 nonresponsive homocysrinuria dietary noncomphance dunng betaine rherapy. Administracionlarge doses of vitarnin C (1 giday) has improved rhe endothfunction; lonB-term clinical efficacy is not known.
More than 100 pregnancies n women wich the classic formhomocystinuria have been reported with favorable outcomesboch mothers and infants, The majoricy of infants were full tand normal. Postpartum thromboembolic events occurred few morhers. All but one of the 38 affected male patients hasnormal offsprrng.
The screening of newborn infants for classrc homocystinu
has been performed worldrvrde and a prevalence of:t/200,0001/350,000 has been estimared, The condition seems mcommon in Neu.South Wales,Australia {1/60,000)and IrelEarly trearment of patients idencified by the screening processproduced favorable results. The mean IQ of 16 patients wvitamrn Bu unresponsive form treated in early infancy lvas 94. Dislocation of the lens seemed to be prevented in spaflents.
Homocvstinuria is inherited as an autosomal recessive The gene for cystathionine p-synthase s located on chromoso21q22.3. Prenaral diagnosis is feasible by performing an enz
assav of cultured amnrotrc cells or chorionic villi or by D
analysrs. Many disease-causingmucations have been identifie
different famihes. The majorrty oF affected paciencs re compo

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 52/177
Chapter 5 r oelects n Metabolisml AminoAcids r
NH'
IcH3-s-(cHr)2 cH-cooH
'Methionine-\| M"thi",fi;A
o \,
-----* oilgiflt s-Adenosyrmethronrne/ glycrne \
c , l
t'/
I
ioS-Adenosylhomocysteine
- Homoserine Cysteine
/ J \\
/ l \I Glutathione
Sultite
Sulfate
cblc,D, E,F, Gvit B'rz ------- ll-- MethylCbl
Cyslathronrne
Cystathioninemiat ^
T \l/
d-Ketobutyricacid
iPropionic ci d
III
Succinic cidIt
co2 + H2o
Figurt 85 3- parhways in rhe metabolLsm f sulfur containing arnrno acids. Enzymesr 1) methronine adenosyttraDsferase,2) adenos-vlhomoc),steineydro
(i)cysrarhion svnrhase, 4) cyrrathionase, 5) sulfite oxrdase, 5) betainchomocysreinenethvltransferase, 7) merhylene er.ahydrofolare eductase.
hererozyg,' teror tw o ditfercnt allele' ' .Heterozygoutcarriersar e
u .ua l l . a ' tm p t< rm ar i . ; h rom bocm ho l i ceven tsand c , ' r ona r '
he.rrt disease r" rno." aoarrrrn rn rhere rndrvrduals han in rh e
Methylcobalamin is rhe cofaccor for the enzyme methioninc syn-
thase, which catalyzes remethylation of homocysteine to methio-
nrne. There are at least iive distincr defects in the inlracellular
metabolismof cobalamin ha r may interferewirh the formation
of methylcobalamin.To better understand he merabolism of
cobalamrn,se emerhylmalonicacidemia (seeChapler 85.6 an d
amjn is impaired (s e ChaPter85.6).
Patients *.rrh cblE nd rblG defeccsare unable to form methyl-
cobalamin and develophomocysrinuria virhout methl' lmalonic
laurine
acidemia {seeFig. 85-4); fewer than 40 patients are known *
each of thesediseases.
The clinical manifestations are similar in patients wich al
rhese defects. Vomrting, poor feeding, letharg,v, hypotooia,
developmental delay may occur in the 1st fer,..months of life. O
patient \r.ith rhe cblG defect was not symptomatic (exceptmild developmental elay)until shewas 21 yr old, horvever,
she developed difficuJty in walking and numbness of the han
Laboratory findings include megaloblastic anemra, homocys
uria, and hypomethioninemia.Th e presenceof megalobl
anemia differenciates these defects from homocysrinuria du
merlvlenetetrahydrofolate reductase deicjency {see later).
presenceof hvpomethioninemia differentiates borh of these c
dirions from cystachionine -synthase eEciency se eearlier)
Diagnosis is establishedby complementacion studiesperform
in cuhured ibroblasts.Prenataldiagnosis as beenaccompli
by studies rn amniotic cell cukures. The gene for c6lE (MTR
is mapped to chromosome 5p15.3-p15.2 and that for c
(MTR) is mapped lo chromosome1q43; severaldisease-ca

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 53/177
538 PAnTX Motatolic iseases
(Dielaryom)Biolin-C N Prolein
o
Acetoac€lc acid + Acelyl CoA
I
(;
cbro cbrcI
oHcbr+3
,Proteinsynthesrs
\
i" ..t f", I \ cHscH3-cH cH cooH cHr-cH,-cH
?HCOOH CHI-CH-CH' CH COOH
-NHz NHz ,ln
cYt*ol
V.lin. lsolsuclne Lsuclne
2-Keto-3-n€lhylval€riccid 2-Ketoisoca proic cid
l$lf -*'*' ir'i".."e'f l#;:?:Hf"l I rr'a'i"ee
lsobutyryl-CoA 2-Methylbutyryl{.A lsovaleryl4oA
1 f r"*a.l"-lI I T I acidsmia I
Melhacrylyl-CoA Tiglyl.CoA
i |3-Melhylcrolony-coA
r i co, -.l \ g-gvo,o*rl"-"r.rc""io-fryfioryisobulyrrl-CoA 2-Merly-3-fydroxybutyryLcoe l
Tr----ffi;6;-] N\--oddchan I| -^ , : ^_, - | | \ ' \ r r8$yac |os t-I acid€mra
|-\)i;;"",";
Il3-Hld,.']+l"9ihvrffii|l'
\ 'Mehon,ne
Methytcttncacd'cBestercl
l\
fTiil;Gii"d,-l
-+ -,-.1F- Melhyl cbl
Fffi;Hcu-l
Figur€ 85-4. Pachwaysn the metabolismofthe branched-chain mino acids,biorin, and vrramin BD (cobalamin).MMA, methylmalonicacidemE; HCU,c1'stinuria;CbJ,cobalamin; OHCbl, hvdroxycobalamin; cbl, defect n merabohsmof cobalamin; TC, rranscobalamine.
vary from apnea, seizure, microcephaly, coma, and deatdevelopmental delan ataxia, and motor abnormalities or psychiatric manifestations, Premarure vascular diseaseor per
eral neuroparhyhas been reporred as che only manitestairthis enzyme deficiency in some patients. Adults with seenzyme defrciency may even be completely asymptomatic. Esure to the anesthetic nitrous oxide (which inhibrts methiosynthase) n patients wirh MTHFR deficiency may result in rologic deterioration and dearh.
Laboratory fndings include moderate homocl'stinemiahomocystinuria. The methionine concentration is low or normal. This findine differertiates this condition from cla
mutations, ncludrnga common missensemufation (P1173L) nthe MTR gene,havebeendescribed.
Tlearmentwith vitamin 812 n the form of hydroxycobalamin(1-2 m9l24 hrl is used ro coffect the clinical and biochemicallindings.Results ary among both diseases nd sibships.
Homocystinuria ue o Deficiency t MethylsnetotrahydrololateBeductaseMTHFBI.his enzyme educes -10 methylenecetrahy-drofolate o form S-methyltetrahydrofolate, hich provides hemethyl group needed or remethylation of homorysteineromerhioninese e ig .85-3).
The severir,v f the enzymedefectand of the clinicalmanifes,tationsvariesconsiderablyn different amilies.Clinical findings

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 54/177
homocystinuria caused by cvstathionine synrhase defrciency.
Absence of megaloblasric anemra distingurshes chis condition
from homocysdnuria caused by merh,vlcobalamin formation (see
earlier). Thromboembolism of vesselshas also been observed in
tion in the MTHR gene.
A number ofpolymorphisms have beendescribed n the MTHR
sene.T'"!o of these 677C > T and 1298A > C) may affecr evels
ofplasma toral homocystein€ and have been studied as possible
risk factors for a wide variety of medical conditions, ranging from
birrh defects to vasculal diseaseand even risk for cancer, ProS-nosrs for survival in leukemia, and risk for Alzheimer disease.To
po l lm o rph i .m i . w ide lu ava i lab le , t s p red rc r i re a lue n ny
g iven nd iv idua l as er to be de re rm ined .-Treatment of severeMTHFR deEcrencywitb a combinatio of
folic acid, itamin 85, vrtamin Br2, methionine supplementanon,
and betain has been ried. Of rhese,early treacment with betaine
seems o have the mosr beneficial eftecr.
The condition is inherited as an autosomal recessive raiti tfie
gene or rhe enzlme has been ocatedon chromosume pl 6 J and
iranu drsease-causrng utarion\ have been reported Prenalal
diagnosis can be offered by measuring N{THFR enzyme activrty
in cultured chorionrc villi cells or amnioc],tes, by linkage anal,v-
sis in informative families, or by DNA analysis of the muration
HYPERMETHI0NINEMIA.econdary hypermethioninemia occurs in
liver disease, qvrosinemia type I, and classic homoc,vstinurra.
Hypermethionrnemia has also been ound in premarure and some
full-term infanrs receiving high protein drets, n whorn it ma,v ep-
resent delayed maruration of the enzyme methionine adenosyl-
rransferase. Lorvering the protein inrake usually resolves rhe
abnormaliry Primary hypermethioninemia caused by the de6-
ciency of hepatic metbionine adenosyltransferase (seeFig. 85-3)
has been reported in a few patients. The majority of thesepatrencs
have beendiagnosed in the neonaral period rhrough screening or
homoc,vstinuria. Affected individuals wrth residual enzyme acliv-
rr).remain asymptomatrc throughour life despirepersistent hypermethroninemia. Some complain of unusual odor to cheir breath
(boiLedcabbage),A few patients with complete enzyme deficiency
have had neurologic abnormaliries related to demyelination
( ntal retardarion, dystonia, dvspraxia). The gene for merhion-
i adenosyltransferases on chtomosome 10q22 and several
hypermethroninemia,
CYSTATHI0NIt{EMIACVSTATHI0NINUBIA). econdary cystathion
inuria occurs in pahents with viramin Br or Brz deficiency, liver
drsease partrcularlv damage caused bv Balactosemia), thvrotox
icosis, hepatoblastoma, neuroblastoma, ganglioblasroma, or
defecrr n remethtlatronoF homocysfeine.
Cystathionase defciency results in massive cystathionlnuria
and mild to moderare cystathroninemia; cysrarhionine is not nor-
mally detectable in blood. Deficiency of this enzyrne s inherited
as an autosomal recessive ralt and rts prevalence is estrmated co
be about l/14,000 live births. Affecred subjectswith a wide
variery oF clinical manifestations have been reported. Lack of a
consiscentclinical picture and the Presenceof cystathionrnuria in
a number of normal persons suggesr hat cystathionase denciency
thionase is located on chromosome 16.
Ghapter 5 r Doloctsn Metabolism l AminoAcids |
85.4.CysrElNVCvstNtlrajRezvani
Cysreine is a sulfur-containing nonesseDtial amino acid tha
synrhesized from methronine (seeFig. 85-3). ln rhe presenc
oxygen! two molecules of cysteine are oxidized to f orm cys
The mosc common disorders of cysteindcystine metaboli
cyscinuria seeChapter J47) and cystinosis se eChapter 529
are discussedelsewhere.
SUI.TITE XIDASEDEFICIENCYMOIYBOEI{UMCOFACTORClEltlCY). t the lasr srep n cysteinemetabolism, sul6te is oxidi
to sulf ate bv sul6te oxidase. and the sulfate is excreted n the u(see Fig. 85-3). This enzyme requires a molybdenum-p
comDlex named molvbdenun cofactor, This cofactor is also
essaiy for the function of rwo other enzymesrn humans: xanth
dehydrogenase (which oxidizes xanthine and hypoxanthine
uric acrd) and aldehyde oxrdase. Three enzymes, encodedbv th
drfferent genes,are involved rn the synthes is of the cofactor
genesar e mapped to chromosornesL4924,6p21.3, and 5q
Deficiency of any of the rhree enzymes causescofactor deflci
wirl jdentrcal phenotype. Most patrents who were origrn
diagnosed as having sullire oxidase deficrency have been pro
to have molybdenum cofactor deficrency. Both conditions
ioherited as autosomal recessive raits.
The enzyme and the cofactor deficiencies produce idenclinical manifestations. Refusal !o feed, vomiting, se
intractable seizures (ronic, cLonic, myoclonic), and severe de
opnental delay may develop wirhrn a few weeks after birth. B
eral dislocation of ocular lenses s a common finding in pati
\4ho survive the neonaral period.
These children excre!e large amounrs of sullire, thiosulfate
sulfocysterne,xanthine, and hl,poxanthrne in their urine. Urin
and serum levels of uric acid and unnarv concentratio[ of su
are dimrnished. Fresh r-rrine hould be used or screeningpurpo
and for quantitative measurements of sulfite, because oxida
at room temperature may produce false-negative results,
Diagnosis is confrrmed by measuremenr of sulfite oxidase
molybdenum cofactor in fibtoblasrs and liver biopsies, res
rively- Prenaral diagnosis is possible by performing an assa
sul6re oxidase activi ty in cultured amniotic cells or in samplechorionic villi.
No effective treatnent is available, and most children di
the 1st 2,vr of hfe. The prevalence of neither of the deficien
ls known.
85.5.TRYPToPHAN.raiRezvani
Tryptophan is an essential amino acid and a precursor for n
tinic acid and serotonin (Fig. 85-5). Presumeddeicienciesvariecy of different enzymes involved in tryptophan cacabo
have been epor ted, but no distinct clinical entity has yet emer
Hartnup disorder causes disturbance in trvptophan absorpti
HARTNUP IS0RDER.n this autosomal ecessive isorder, a
after che 1st reporced famill there is a defect in rhe transpor
monoamlno monocarboxylic amino aclds (neutral amino a
by the intestinal mucosa and renal tubules. Mosc children
Hartnup defecr remain asymptomatic. The major clinical m
festation in the rare symptomatic paoenr is cutaneous photo
sitivit,v.The skin becomes ough and red afrer moderate expo
to the sun! and with greater exposure, a pellagra-like rash
develop. The rash may be pruritic, and a chronic eczema
appear The skrn changes have been reponed in affected inf
as young as 10 days of age. Some patients ma,vhave inrermit
acaxia manifested as an unsceady,u'ide-based gair. The at
may last a few days and usually recovers spontaneously. Me

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 55/177
540 PABTX Metabolic iserses
Protein ynthesis
Figure 85 5. Pathwa)-sn rhe merabolismof tryprophan. PKU. indicareshyperphenvlatanemia ue co tecrahydrobiopterindeficiency see 'ig. 85 ll. Enzt(1) tr-vptophanhvdroxylase,{2) aromadc L-amino add decarboxylase A-qDC), (3) monoamineoxidase (MAO).
ln vitro
development is usually normal. Two indrviduals in the originalkindred were menlally retarded, however Episodic psychologic
changes,such as irritabilit)', emotional instability , depression, andsuicidal tendencies,have been observed; thesechangesare usuallyassociated r,r.ithbouts of ataxia. Short starure and atrophic glos-
sitls are seen rn some pallents.
Mosr chrldren diagnosed with Hartnup disorder by neonatalscreening have remained asymptomatic. Thrs indicates thac otherfacrors are also involved in parhogenesrsof the clinical conditron.
The marn laboratory finding is aminoacrduria, which isrestricted to neutral arnino acids (alanine, serine, threonine,valine, leucine, isoleucine, phenylalanine, tyrosine, rryprophan,histidine).Urinary excretionof proline,hvdroxyproline,and argi-nine remains normal. This findrng differentiates Hannup disor-
der from other causes of Eeneralized amrnoacrduria, such asFanconi syndrome, Plasma concentrations of neutral amino acldsare usuaLlynormal. This seemingly unexpecred flndrng is becausethese amino acids are absorbed as dipeptides and rhe transportsvstem for small pepcides s ntact in Hartnup disorder. The mdolederivarives (especially ndican) may be found in large amounts rn
some patients, owing to bacterial breakdown oi unabsorbed rryp-topnan ln the lntestrnes.
Diagnosis is established by the striking intermiment nature ofsymptoms and the yust described urinary findings.
Treatment rvich nicotinic acid or nicorinamide (50-300 me/24 hrr and a hrgh prorcrn dier resulrs n a tavorable espon.. ins).[lptomatic patients. Becauseof rhe mtefmitlenr nature of theclinical manifestations, the efficacy of thes€ treatmeols is drfnculr!o evaluate. The orevalence of the disorder ls estimated to be
1/30,000.Normaloutcome both Ior mother and fetus s reportedin affected pregnant lvomen. The gene for rhis condition has notvel been rdentified.
85.6oVATINE,EUGINE,SOTEUCINE,NDRELATEDORcnrtc clDEMlAslrai Rezvani ndDavid$. Eosenhlatt*
The early steps n the degradation of these three essentralaminoactds, the branched-chain amino adds, are similar (see Fig. 85
*DavidS.Rosenbla|tontributedo rhesection n merhvlmaloniccidemia.
5-OH-indoleacetic cid(5 H|AA)
4). The intermediate metabolites are all organic ac rds, and ciency of any of the degradative elzymes, except tbr the transinases,causesacidosis; n such instances, he organic acids bethe enzymatic block accurnulate in bod;r fluids and are excrin the urine. These disorders commonly cause metabolic acsis, which usualll/ occurs rn the 1st few days of life, Althomost of the clinical lindings are nonspecific, some manifestatrnay provide imporrant clues to the nature of the enzyme dciencv. An approach to infants suspected of having an orgacrdemia is presented in Figure 85-6, Delinirive diagnosr:sually established by identifying and measuring specilic orgaacids in body fluids (blood, urine), by the enzyme assal andrdenrification of the mutant gene.
Organic acrdemras are not limited co defecrs in the catab
pachways of branched-chain amino acids. Disorders cauaccumulalion of olher organrc acids include chose derived flysme (seeChapter 85,13), those associatedwith Iactic acidChapter 87), and dicarboxylic acidernias associated with detive fany acid degradation (seeChapter 86.1).
MAPTE SYBUP URI E DISEASE (MSUD). Decarboxylationleucine, isoleucrne, and valine is accomplshed by a compenzyme system (branched-charn c-kecoacid dehydrogenase)uthiamine pyrophosphate (vitamin 81) as a coenzyme. This mchondrral enzyme consists of four subunits: E1", E'p, E., ndThe E3 subunit is shared wrth two other dehydrogenase inbodl namelv p;rruvare dehydrogenase and or-ketoglutarate dedrogenase. Deficiency of this enzyme system causes MSUDFig, 85-4), named after rhe sweet odor of maple syrup found
body fluids, especially urine. Based on clinical findings response to rhramine administration, five phenotypes of MShave been denri6ed.
Classic MSUD. This form has the most severe clinical manitations. Affected infants who are normal at bir th develoD Dfeeding nd vomrting n rhe lst wk ot l ite; ethargyand coma mensue wrthin a felr, days, Physical examinarion reveals hytonicity' and muscular rigidity with severeopisrhoronos. Perof hypertonicity may alternate with bouts of flaccidity. Neulogic findings are often mistaken for generalized sepsis meningitis, Cerebral edema may be present; convulsions occumost infants, and hypoglycemia is common. In contrast to mhypoglycemic states, correction of the blood glucose concenrion does not improve the clinical condition. Rouline laborat
Formylkynurenine
III
Nicotinic cid

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 56/177
Chsplor 5 r oelocts [ Motabolisnol AminoAcids I
Common eatureg
Flelusalo eedVomitingAcidosis
DehydrationNeutropenaa
Hypoglycemia
Ketosis
r___-_-r
Fisu.e 85-6. Ctinical approach o infancswith organic acidemia Asrerils indicare
2). MSUD, mapte syrup urine dis€ase.
findingsare usuallyunrernarkable, xcept or metabolicacidosis.
Death usuallyoccurs n untreatedpatients n the 1st {ew weeks
or monrhsof life.
hrgher han thoseof the orher hreeamino acids Urine containshigh levelsof leucine, soleucine, nd valineand their respective
keioacids. Theseketoacids may be detectedqualitatively by
addinga few drops of 2,4-dinitrophenylhydrazineeagent.(0.17"
in 0.aN HCI) to the urine; a yellow precipitateof 2,4-dinitro-
measuredn leukocytes nd cuhured ibroblasts.Treatmentof the acutestate s aimed at hydrarionand quick
removalof thebranched-chain mino acidsand theirmetabolites
lasix, or hypertonicsaline.Trearmentafter recovery rom the acutestate equiresa dier
low in branched-chainminoacids.Syntheticormulasdevoidof
leucine, isoleucine, and valine are available commercially.Becauseheseamrnoacidscannot be synthesized ndogenously,
disard€rs n which patients ha"e a characterisric dor (se€ ext and Table
small amountsof rhem shouldbe added o the diet; he amoshould be ticratedcarefully by performing requentanalysethe plasmaamino acids,A clinical condition resemblingadermatitisenteropathica ccurs n affected ofantswhosepla
isoleucine oncentration ecomes ery ow; additionof isoleuto the diet causes rapid and complete ecovery.PatientswMSUD should emainon the diet for the rest of their lives.Lrransplantatron as beenperformed n a smallnumberof pati
with classicMSUD with promising esults.Thesechildrenhbeenable o roleratea normal diet.The long-termprognosis f affected hildren emainsguar
Severe etoacidosis,erebral dema, nd deathmay occurduany stressful ituation suchas infectionor surgeryr speciamid-childhood, Mental and neurologic deficits are com
sequelae.Intemitt€nt rlSUD. n this form of MSUD, seemingly or
chrldrendevelop omiring,odor of maplesyrup,ataxia, ethaand coma during any stressor catabolicstate such as infecor surgery.During theseattacks, aboratory findings are inringuishablerom thoseof the classicorm, and deathmay ocTreannenr f the acuteattack of intermitrentMSUD is srmrlthat of the classic orm. After recovery, lthougha normal ditolerated,a diet low rn branched-chain mino acids s rec
mended.Activity of dehydrogenasen patientswrth the ntertent form is higher han n che lassicorm and mayreach5-2of the normal activity.
Mild lhtennediate)MSUD. n this form, affected childdevelopmilder disease fter the neonatalperiod. Clinical mfestations re nsidiousand imited o the centralnervous ys
Patients avemild to rnoderatemental etardarion usuallya5 mo of age) with or without seizures. hey have he odo
maple syrup and exctetemoderateamounts of the branccharn amino acids and rheir ketoacidderrvarivesn the uPlasma oncentrations f leucine, soleucine, nd valinearem
erately increasedwhereas rhose of lactate and pyruvatenormal. These hrldrenare commonlydiagnosed uringan ncurrent llnesswhen signsand symptomsof classicMSUD
No ketosis r mildketosis
1.3-Hydroxy-3-melhylglularicaciduria
2.AcylCoAdehydrogenasedaficiency
3. HMGCoAsynthetasedeficiency
No skinmanifestations
1. rethylmaloniccidemia2. Propionic cidemia3. Ketolhiolaseefciency

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 57/177
542 PARTX MotabolicDiseases
occur The dehydrogenase activiry is 3-30% of normal. Sincepatients wirh rhiamine-responsive MSUD usually have manifes-tatrons similar to those seen n the mild tbrm. a trial of thiaminetherapy is recommended. Diet therapr., similar ro that of classiclvISUD, is needed.
Thianine-Sesponsiye MSUD. Some children wrth mild or inter-mediate forms of MSUD who are ueated with hish dosesof thi-am ine havc d ram ar icc l in i ca l and b iochem rca lm o rovem enr .AJthough some rerpond ro rrealmenr with rhiamine ar l0mg/24 hr, others rnay require as much as 200 mg/24 hr for at least 3
wk before a favorable response s observed- These patienrs alsorequire drets deficient in branched-chain amino acids. The enzy-matic activity in these oatie[ts is 2-407o of normal.
MSUD Due o a 0efici;ncy ot ErSubunit (Dihydrolipoyl Dehydroge-nasel. This is a very rare drsorder Patients develop lactic acido-sis in addition to signs and symptoms simrlar ro those ofintermedrate MSUD because he E1 subunit is also a componentof pyruvate dehydrogenase and o-ketoglutarate dehydrogenase.Progressrve neurologic impairment manifested by hypotoniaand developmental delay occurs aIrcr 2mo of age. Abnormdmovements progress to atax ia. Death ma,v occur in earlychildhood.
Laboratory findings include persistent actic acidosis wirh highlevels of plasma lactate, pyruvate, and alanine. Plasma concen-trations of branched-chain amino acids are moderatelv increased.
Patienls excrete large amounfs of lacrate, pvruvate, cr-glutarate,and the three branched-charn ketoacids in rheir urme.No effeccive treatment is available. Dietary resrtrction of
b ranched -cha inm ino rc rds and r reaLm enr. r r rh i eh doses frh iam ine . io t in .and ipo icac rdhasbeen ne f fec t i re .
Geneticsand Preyalenceof MSUD.All forms of MSUD are nher-ited as an autosomal recessivecrait. The gene for each subunitresides n dil lerenr chromosomes.The E1, gene s on chromo
different disease-causine mutations have been idenrified inpatrents with different forms of MSUD. A given phenocl,pe iscar:sed by a variety of genotypes; patients from different pedigrees u'ith the classic forrn of MSUD have been shown co havemLllations rn 64enesor E1", Ern, or E2. Most paciencsare com-
pound hererozygotes nheriting tlvo different mr.rtant alleles-The prevalences estimatedat 1/185,000.The classic orm ofMSUD is more prevalent in the Old Order of Mennonires in theUnrted States, with estimated prevalence of 1/358, Affectedpatients rn this population are homozygous for a specific muta-tion (Y394N) in the Ero subunit gene.
Early detection of NISUD is feasible by mass screening ofnewborn infants. Prenatal diagnosis has been accomplished byenzyme assayof the cultured amniocytes, cultured chorionic villitissue, or direct assay of the chorionic vrlli samples and by identrfication of che mutant eene-
Several successful pregnatr.re" have occurred in women wirhdifferent forms of MSUD. No ill effects have been observed inthe offspring of rhesepatients. Episodes of metabolic decompen-sations have occurred rn rhe mothers during pregnancy and the
postpartum perlod.
IS0VALEBIC Cl0EMlA. This rare condrtion i s due to the delicrencyo f r sova lc ry l oenzym e lCoAt deh ld rogenasesee ig . 8s -51 .
Clinical manifestations rn the acute form include vomiting andsevereacidosis in che 1st few days of life. Lethargy, convulsions,and coma may ensuer and death may occur if proper therapy rsnor rnitiated. The vomiting may be severe enough to suggestpyloric stenosis. The characterisric odor of "sweaty feet" may' bepresent (seeFig. 85-6). Infants who survive rhis acure episode wrllgo on to have the chronic ntermitten! form later on in life. Amilder form of the disease (chronic intefinittent form) also exists;rn rhis, the 1st climcal manifescation (vomicing, lechargy, acido-sis or coma) may not appear unrrl the child is a few monrhs o. a
few;lears old. lo both forms, acute episodesof metabolic depensacionsmay occur during a catabolic state such as an intion. Sen rive methods for newborn screenng have identifieda m i lde r nd po ten f ial l ) ' a \ ym p tom ar ichenotvpe f rhe cotion; a few older siblings of these affecred newborns were foto have identical genotype and biochemical abnormawithout any clinical mamfescations.
Laboratory findings during the acute attacks include ketodosis, neucropenia, thrombocytopenia, and occasionally patopenia. HypocaLcemia, hyperglycemia, and moderace to se
hyperammonerma may be present in some parients. Increasplasma ammonia may suggest a defect in the urea cycle. Incycle defects the infant is noc acidotic (seeFig. 85-6).
Diagnosis is esrablished by demonstrating marked elevaof isovaleric acid and its metabolites (isovalerylgft.crne
hydro:':aisovaleric acid) in body fluids, especiallyurine. The mcompound in plasma is isovalerylcarnitine, which can be msured even in a few drops of dried blood on a filter paper. lvsuring the enzyme in cultured skin fibroblasts confirmsdiagnosis.
Treatment of the acute attack is aimed at hydrarion. reveof the catabolic state (bv providrng adequare caloties orallyintravenously), corre ion of metabolic acrdosis (by intusodium bicarbonate). nd removal of the excess rsovaleric aBecause sovalerylglycinehas a high urinary clearance, adm
rradon of glycine \250 mglkg/24 hr) is recommended ro enhformation of rsovalerylglycine. L-carnicine (100 mg/kg/2orally) also increases emoval of isovaler acid by formrng valerylcarnirine, which is excreted in the rine, In patients
s ign i f i can t ype ram m onem iab loodam m on ia 200 ; rM r . msures thar reduce blood arnmonia should be employedLhap re r 85 ,1 l ) . Exchange rans l : us ionnd pe r i t onea l iama,v be needed if the just described measures fail to induceni6canr clinical and biochcmical imDrovemcnr.Alrer reco
tine supplemenrs. Pancreatitjs (acute or recurrent forms) has breported in survivors. Normal development can be achieved r€arly ano proper rreatment,
Prenatal diagnosis may be accomplished by measuring
valerylglycine in amniorrc fluid, by enzyme assay in cuhuamniocytes, or by Ldentification of the mutanr gene. Succepregnancy wich favorable outcomes both for the mother andinfanr has been reported. Mass screening of newborn infanrrn use in the United Srates and othet counrfles. lsova
disease-causingmutations have been dentilied. The prevalencrhe condirion is estimated from 1/52,500 (io parts of Germato 1/250,000 (in the United States).
MUtTtPtECARBoXYIASEEFtCIE'{CIESDEFECTSN UTIUZA0F BlOTlt{1.Biotin is a water-soluble vitamjo that is a cofactorall four carboxylase enzymes rn humans: pyruvate carbox_vacetyl CoA carboxylase, propionyl CoA carboxylase, and
methylcrotonyl CoA carboxylase. The latter two are involvethe metabolic pathways of leucine, isoleucine, and valine (see
85-4).
Dietary biotin is bound co proteins; free biotrn is geoeratethe intestine by the action of digestiveenzymes, by intestinal bteria, and perhaps by biotinidase. The latter enzyme, v.hicfound in serum and most tissues n the bodr', is also essentiathe recvcling of biotin in the body by releasing rt from the apozymes (carboxylases, seeFig. 85-4). Free biorin must form a colent peptide bond *'ith the apoprotein of the four carboxylato activate them (holocarboxylase). Thrs binding is catalyzedholocarboxylase svnthetase.Deficiencies n thrs enzyme or intinidase result in malfunction of all the carboxvlases andorganic acidemia.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 58/177
of biotin.Treatment rvich biotin (10 mg/day orally) usually results in an
imDrovement n clrnical manifestatton\an d ma y normalize thebiochemical abnormalit ies. Early diagnosis and treatment ar e
related to cheourcome lemains unclear.
ciency. Infants q'ith this defictency may de lop. clinical
maniiestations similat to those seen in infants lth holocar-
ChaDter6 r Defsctsn ltle{abolism f AminoAcids r
The orevalenceof this aucosomal recessivecrait is estimated
1/60,000. The gene for brotinidase is located on chromoso
3p25 and manv disease-causingmutations have been dentif ied
different families. Prenatal diagnosis is possible by the measu
ment of rhe enzyme actrvity in the amniotic cells or by ident
cation of the mutant gene.
Mult iple Carboxyl6s;DeficiencyDue o DietaryBiotin Delicie
Acquired de6ciency oI biotin may occur in infants receir.ing lo
parenreralnurrit ion without added biorin, in parienrs ecei
prolonged antrconvulsant drugs (phenycoin, prirnidone, car
mazepine) or in children wrth short bowel s1'ndrome or chrodrarrhea who are recervrng formulas low in biotin. Exces
ingestion of raw eggs may also cause biotin defictency beca
the protein avidin in egg white binds biotin and makes it unav
able for absorption, Infants with biotin deficiencv develop d
matitis, alopecia, and candidal skin infections.
ISOTATED.METHYTCROTONYTOACARBOXYTASEEFICIThisenzymes oneof fourcarboxylasenzymesn the bodyrequire iotinasa cofacrorsee ig.85-4).An solated eliciof this enzvme musc be differentiaced from disorders of bio
metabolism (multiple carboxylase deficiency), which causedrm
ished actrvity of all four carboxylases, 3-Methylerotonyl CoA c
bo:'ralase is a heteromeric enzyme consisting of cr (bio
containing) and p subunirs.Clinical manifestations are highly variable, ranging from fa
neonatal onset wrth acidosis, severe hypotonra, and seizure
asympromatic adults. In the severe form of the condition,
affected in{ant who has been seemingly normal de.'elops an ac
episode of vomiting, hypotonia, lethargy, and convulsions afte
ninor infection. Death may occur during the acute episode.
Laboratory findings during acute episodes nclude mild to m
erate acidosis, ketosis, severe hypoglycemia, hyperammonem
and elevaredserum levels of liver transaminases. Large amou
of 3-hydroxyisovaleric acid and 3-methylcroconylglycine
found in the urine. Urinary excretion of 3 mechylcrotonic aci
not usualh' increased n this condition because he accumula
3-merhylcrotonyl CoA is converted to 3-hydroxvisovaleric a
Severesecondarv carnrtrne deficiency is common. The condit
should be differenciated biochemically from multiple carboxyldefcrency (seeearlier) in which lactic acid and metabolites of p
pionic acid are present in body fluids in addition to 3-hydro
isovaleric acid. Diagnosis rnay be confirmed by measuremen
the enzyme activity in cultured fibroblast s, Documentation
normal activities of other carboxylases is necessary or delim
diagnosis.Aggressive treatment of acute episodes with hydration, in
venous infusion of glucose, and alkali is recommended. Th
parienrs are unresponsive to biorin therapy. Parients who
earlier reporrs were found to be t' iotin fe\ponsrve were mprobably suffelng from muftiple carboxylase deliciency due
biotinidase defrciency (seeearher). Long-term treatm€nt inclu
a dier rescricced n leucine in conjuncrion with the oral admi
tration of L-carnitrre (7 5-100 m{k{24 hr) and the preven
of catabolic states.Normal growrh and development are expecin thesepatlents.
The condition is inherited as an autosomal recessive rait.
gene for cr subunit (MCCI ) is located on chromosome 3q25-
and rhar for the p subunir \MCC2) is mapped to chromoso
5q12-13. Mutation in either of these enesmay resulc n the d
ciency of rhe enzyme activity. Srmilar phenoqvpe may be cau
by different genotype. Severaldrsease-causrng utations rn ei
gene have been idennfied in different families. Newborn scr
ing programs using tandem mass specrrometry have identifred
unexpectedl;r high number of infants with 3-methylcrotonyl C
carboxylase deficiency (1:50,000), suggesting hat this condit
may be one of the most common organic acidemias in cer
ooDulatl()l1s.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 59/177
544 PARTX MetabolicDiseases
546 PART r Metabolic isrosas
during acure artacks.Diagnosismay be confirmedby enzymeassayn cuftured ibroblasts, eukocytes, r liverspecimens r byidentificationof the mutant gene.Prenacal iagnosrss possibleby the assay f the enzyme n culturedamniocytes r a chorionicvilli biopsy or by DNA analvsis.
Treatmentof acute episodes ncludes hydratron, nfusion ofglucoseo control hypoglycemia, rovisiono{ adequate alories,
and adminisuationof bicarbonareo correct acidosis.Hyperam-monemia hou ldbe r reared rompt ly seeChaprer 5.11) .Exchange ransfusionand peritonealdialysismay be required npati€ntswirh severe yperamrnonemia, estrictionofprotein andfat intake is recommended or long-term management.Oraladministrationof L-carnitine 50-100mg/kg/24hr) prevents ec-ondarycarnitinedeficiency. rolonged astingshouldbe avoided.One child died after routine immunizarion. The condition isinheritedasan autosomal ecessiverait. Theeeneor HMG-CoAlyare resides n chromosome prer-p33and several rsease-causingmutationshavebeen denrified n different amilies.Thegenedefectappears o be more common n the Arabic popula-tion, especiallyn SaudiArabia.
SUCCINYt 0A:$KETOACID0ATRAiISFERASESc0T)DEFICIENCY
This enzyme s necessaryor the metabolismof ketone bodies(acetoacetarend 3-hydro:r1'butyrate)n peripheral issue (seeFig. 85-7). A deficiency f this enzyme esults n the underuti-lization and accumulationof ketone bodies and ketoacidosis,Only a few patientswirh SCOT deficiency ave been eportedto date; he condirion may not be rare becausemany cases reundiagnosed.
The presentation s an acute episodeof unexplainedsevereketoacidosisn an infant who had beengrowing and developingnormalh'.About half of rhepatientspresent n the 1st wk of lifeand all before2 yr. The acureepisode s oftenprecipitated y anintercurrent infection or a catabolic state. Death may occurduring hese pisodes. chronrc uhclinical erosis sually er -sis!sbetrveen heattacks,Developments usually normal.
Laboratory findingsduring the acute episodeare nonspecific
and includemetabolicacidosis nd ketonuria with hieh evelsofaceroacetatend J-hydroxyburyraren bloodand urini. No orherorganicacidsare ound n the blood or in the urine.Bloodglucoselevels reusuall) ormal,bur hvpoglycemiaar been eponedntwo newborn infants rvirh severeketoacidosis,Plasmaaminoacidsareusuallynormal. Diagnosis an be established y demon-stratinga deliciency f enzymeactivity n cultured ibroblastsorbv DNA analvsis.
Treatmentof acuteepisodes onsists f hydration,correctionof acidosis, nd theprovisronof a d iet adequaten calones. ong-term treatment vith a high-carbohydrare iet and avoidance fcarabolicstates s recommended. his condition sbould be con-sideredn any nfant tuith wnexplamed oatsof hetoacidosis.hecondition is inherited as an autosomal ecessiverair, The eenefor rhis enzlme s locared n chromosome plJ, and .eieral
drsease-causingutationshavebeen ound in different amrles.
MEVAL0NICCIDUBIA. levalonicacid, an incermediatemetabo-lite of cbolesterol ynthesrs,s converted o 5-phosphomevalonicacid by tbe action of the enzymemevalonate inase seeFig. 85-7). Based n clinical manifestations,wo formso{ this condirionhavebeen ecognized.
Mevalonic Aciduria, Seyere Form. Clinical manifesrarionsincludemencal erardation, ailure to thrive,growth rerardation,hypotonia,ataxia,hepatosplenomegalnataracts, nd acialdys-morphrsm dolichocephaln ronral bossing,ow-setears,down-ward slanringof the eyes,aod long eyelashes). ecurrenc rises,characterizedby fever, vomiting, diarrhea, arthralgia, edema,lymphadenopathy',urther enlargement f liver and spleen,andmorbrlliform rash have been observed n all patients. These
eprsodesast 4-5 days and recff up to 25 times/yr Deathmayoccur durine these rises.
Laboratory findings include marked elevation of mevaacid n urme; he concentrationmay be as high as 56,000pmmole of creatinine(normal <0.3). Plasma evelsof mevaacid are alsogreatly ncreasedashigh as 54 pmole/dl; nor<0.004).This is the only abnormal organic acid found in tpatients,The levelo[ mevalonicacid tends o correlarewithseverityof the condition and increasesuring crises.Serum
Iesterol oncentrations normal or mildlv decreased. erumcentrarionof crearinekinare 1CK1 s markedly increSedimentationate and serum eukotriene-4 re ncreased uthe crises, erial xamination f rhe brain by MRI revealsgressjverrophv f the cerebellum,
Diagnosismay be confirmed b,v assayof mevalonate inactivity in lymphocytesor in cultured fibroblasrs.No effetherapy s available,Tieatment with high dosesof predm
12mg/kEl24 r) causesmprovement f the acute rises. he cdition is inheritedas an autosomal ecessiveuait. Prenataldnosis s posribleby measuremenrf mevalonic cid inamniotic luid, by assay f theenzyme crivity n culturedamcytesor chorionicvilli samples r by demonstration f lhe mugene.The gene or mevalonate inase MVK) is on chromos1,2924.
Pe odic Fever with Hyperimnunoglobulinemia {MevaAciduria,Mild Form).Somemutarionsof mevalonickinaseetMVKt causemild deficienciesf rhe enzyme nd producclinicalpicture of periodic everwith hyperimmunogobulinD. Thesepatientshaveperiodic bouts of fever associatedabdominal pain, vomiting, diarrhea, arthralgiaj arthrhepatosplenomegaly,ymphadenopathy, nd morbiliform r(evenpetechiaand purpura) which usually start before 1]'rage. heanacks an beproduced v vaccinarion, inor rauor stress;usually occur every 1-2 months and last 2-7 dPatientsare free of symptomsberween cute attacks.The dnostic aboratory inding is elevationof serum rmrnunoglogammaD (lgD); IgA is also elevatedn 8070 of patients.Duacute attacks, Ieukocvtosis, ncreasedC-reactjveprotein,mild mevalonicaciduria may be present,High concentratio
serum IgD differentrateshis condition from familial \4edranean ever.
Tieatment of acuteartacks emainssymptomaric.The cotion s nherited san aurosomalecessirerairrmostoafienwhirean dar e rom western uropean ountries60'i, ar eeiDutch or French).The enzymeactivity is usuallyabout 5-1of normal. The parhogenesis f the condition remainsuncSeveral isease-causng utationsof the gene locatedon cmosome12q24) havebeen dentifred, ut one mutation (V3is present n 807o of pacrents. ong-term prognosis s usugood,bu t amyloidosir asoccurredn a teu parienrs.
PBOPIOI{IG CIDEMIA PROPIONYT OA CABBOXYTASECIENCY).Propronic acid is an intermediate merabolite
isoleucine, ahne, hreonine,methionine,odd-chain ary acand cholesterol atabohsm.t is normallvcarboxvlatedo metma lon ic c idby rhemr rochondr ia lnz lme rop ionv l oA boxylase,which requiresbiotin as a cofactor(see ig. 85-4).enzymes composed f rwo nonidentical ubunits, and p. Biis bound o the cr subunic.
Clinical indingsarenonspecific.n the sel'ere orm of the cditior, patientsdevelopsymptoms n the 1st few days or weof life. Poor feeding, omiting,hypotonia, etharg,r', ehydraand clinicalsignsof severe ecoacidosisrogress apidlv to coand deach. eizures ccur n =307oof affectednfancs.f an rnsurvives he 1st attack, similar eprsodesma,yoccur duringintercurrent nfecrionor colstipation or afrerrngestion f a hprotein diet, Moderate o severemental retardattonand nelogicabnormaliries uchasdystonia, horeoathetosis,emor,
pyramidalsignsare common sequelaen the older survivorthe milder forms, the older rnfant nay havemental retarda

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 60/177
without acute attacks of ketosis. Some affected chrldren mav hat'e
episodesof unexplained se,'erekeroacidosis separated by periods
oi seemingly noimal health. Mass screening of newborns- has
identified milder forms of rhe condition; a few of theses nfants
were complerely asl/mptomatic at diagnosis. The seleriry of cln-
ical manifestartons may also be variable wirhin a familv; io one
kindred, a brother was diagnosed at 5 yr of age whereas his
13 yr old sister, wirh the same level of enzyme deficiency, was
and oreviouslymenrionedorganic acids usualll persisL erueen
the acureanaik,. ( T rcan and MRI oF he brain mar revealer
Chapter 5 r oefucls [ Mdtabolisn l AminoAcids r
tered (10 mg/24 hr orally) to all infants during the 1st attack a
until the diagnosis is established.
Long-rerm treatment consists of a low-protein diec (1
1.5 dkg/24 hr) and admrnisrradon of L'carnicine (50-100 mg/
24 hr orallyr. Synrheticproteins deficienr n propionare prec
sors (isoleucine, aline, methionine,an d threonine)may be u
to increase he amount of dietary protein (ro 1.5-2.0 g/kg/24
rvhile causing minimal change in propronate productron. Exc
sive supplementarion wich these proteins may cause a defrcie
of the essenrialamino acids. To avoid rhis problem, natural p
reins should comprise most of che diecary protein (50-75%Some patienrs may require chronic alkaline therapy to corr
chronic acidosis. The concentration of ammonia in the blo
usually normalizes between attacks, and chronic trearmen
hyperammonemia is not usually needed. Carabolic srates t
may trigger acute attacks (rnfections, constipation) should
treared promptly and aggressively.Close monitoring of blood p
amino acids, urinary content of propionate and its metaboh
and growth parameters is necessary o ensure the proper bala
of the dret and lhe successof therapy.
Long-term prognosis is guarded. Deach may occur during
acute altack. Normal psychomotor developmenr is possible, es
cially in the mild forms identrfied through screening program
mosr children identified clini cally manifest some degree of p
manent neurodevelopmental deficit such as dystonia, chorea, a
pyramidal signs despite adequate therapy. These neurologic liings may be sequelae of a metabolic stroke occunng duringacute decomoe[sadon seeearlier).
Prenatal diagnosis is achieved bv measuring the enzyme ac
ity in c uhured amniotic cells or in samplesof unculturedch
onic villi, by measurement of methylnitrate in amniotic fluid,
by identi6cation of the murant gene.
The condition is inherited as an autosomal recessive rait a
can be identified by mass screeningof newborns. Ic is more pre
lenr n S audi Arabia (1 :2,000 co 1 :5,000). The gene or th
subunit (PCCA gene) s located on chromosome13q32 and c
of rhe p subunit (PCCB gene) rs mapped to the chromoso
3921-q22. Many mutations in either genehave been dentified
differenr patients. Pregnancy with normal ourcome has b
reporred in affected females.
METHYIMAI0I{|C ACIDEMIA. Methylmalonic acid, a structuisomerof succinicacid, s normally derived rom propionic aas part oI the catabolicparhwaysof isoleucine, aline, hreonmethionine,cholesterol, nd odd-chain att) 'acids. Two enzy
are involved in the conversion of D-methvlmalonrc acid to s
crnjc acid: methylmalonfl CoA racema'e, rthich iorms rheisomer; and melhylmalonyl CoA mutase, rvhich converts L-methylmalonicacid to succinicacid (seeFig. 85-4). The la
enzyme equiresadenosylcobalamin, metaboliteof vitaminas a coenzyme. Deficiency of either the mutase or its coenzycauses he accumularion of methylmalonic acid and its prec
sors-in body fluids. A defrciency of rhe racemase has not bconnrmeo.
At least tr.o forms of mutase apoenzyrne deliciencieshave b
identified. These are designared muttt, meaning no detectenzyme actrvrty, and muf, indicating residual, alrhough abnmal, mucaseactivity. The majority of reporred patients.rmethylmalonrc acidemla have a deficiency of the mutase apozyme mult or m / ). The\e patienrs re nor respon\ive o vitaB12 herapr'. In the remarning patients with methylmalonrc aemia, the defecr resides n che formarion of adenosylcobalam
Defectsn Metabolism lVilaminBu (Cobalaminl. ietar_v ita812 equires rntrinsrc factor, a glycoprotein secreted by the gasparietalcells. for absorption in the terminal i leum, It is traported n the blood by 6apcocorrin TCI) and transcobalam(TCII). The complex of rranscobalamin l-cobalamrn(TCII-C
is recognized by a specific receptor on the cell membrane enters the cell by endocytosis. The TCll-Cbl complex

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 61/177
550 PARTX Metaholiciseases
l{eonatalHypelglycemia. his is the most common form ofNKH. Clinical manifestations evelop n the lst few daysof life(between6hr and 8 daysafter birth), Poor feeding, ailure tosuck, ethargy,and profound h1'potoniamay progress apidly toa deep coma, apnea, and death. Convulsions, especiallymyoclonicseizures nd hiccups,are common,
Laboratory indings evealmoderate o severe yperglycinemia(as high as eight rimes normal) and hyperglycrnuria.Theunequivocal levationof glycineconcentrationn the spinal luid(15 to 30 timesnormal) and the high ratio of glycineconcentra-tion in spinal fluid to that in plasma (a value >0.08) are diag-nostrc of NKH, SerumpH is normal; plasmaserine evelsareusually ow
About 30% of affected nfantsdie despite upportive herapy,Thoservho sun' ive developprofound psychomotor etardationand lntractable seizuredisorders myoclonicand/or grand malseizures).Hydrocephalus, equiring shunring, and pulmonaryhypertension avebeennoted [ somesurvlvors.
Inlatttile lKH. Thesepreviouslynormal infants developsignsand symptomsof neonaralNKH (seeearlier) after 6 mo of age.Seizures re he commonpresenting igns.Thiscondition appearsto be a milder form, infantsusuallysurvive,and mental etarda-tion is not asprofound as n the neonatal orm.
laboratory findings n these atientsare rdentical o he neona-tal lorm.
Late-OnsetlKH,Mild Episodic orm. rogressivepastic iplegia,optic atroph]'.and choreoathetoticmovemenls re he main clin-ical manifestations, ge of onserhas beenbetween2 and 33 yr.Symptoms f delirium,chorea,and verticalgazepalsymay occurepisodically n somepatients during an intercurrent nfection.Mental developments usuallynormal, but mild retardationhasbeen eported n somepatienrs.Seizures ave occurred n onlyone parieqt.
Laboratory indingsaresimilar o but rtot aspronouncedas nthe neonatal orm.
TransientNKH. Most clinical and laboracory manifestationsof thrs form are indistineuishablerom those of the neonaralform. By 2 to 8 wk of age,however,he elevated lycine evels nplasmaand cerebrospinalluid (CSF)normalizeand a complereclinical recoverymay occur.Most of thesepatientsdevelopnor-mally with no neurologicsequelae, ut mental retardationhasbeen noted in some. The etiology of this condition is notknown, but it is believed o be due ro immaturity of the enz:/mesvstem.
Atl formso{ NKH shouldbe differentiatedrom ketotichvoer-glycinemia, -glyceric ciduria se e arert,and ingestion f val-proic acrd.The latter compound causes moderate ncreasenblood and urinary concentrations f glycine.Repeatassays fterdiscontinuation f the drug shouldestablishhe diagnosis.
Diagnosis an be established y assay f theenzymen liver orbrain specimens r by idenrifcation of the mutation. Enzymeactivity n the neonacalorm is close o zero,whereasn the otherforms,some esidualactivitv s present. n mostpatientswrth theneonatal orm, the enzymedefect residesn the P protein; thedefect n the T protein accounts or rhe rest. The enzymeassayin three patients with rhe infantile and late-onset orms hasrevealedwo patientswith the defect n the T protein and one nthe H protein.
No effectivereatment s knorm, Exchangeransfusion, ietaryrestrictionof glycine,and administrationof sodium benzoate rfolate havenot altered he neurologicoutcome.Drugs hat coun-teract he effectof glvcineon neuronalcells,suchas strychnine,diazepam,and dexuomethorphan,have shown some beneficialeffeccs nly in patrentswith the mild formsof the condition.
NKH is inherited as an autosomal ecessiverait. The oreva-lences nor known.bur high requency f the disorder ai beennoted n northern Finland (1/12,000).The gene or P protein slocaredon chromosome p22. The gene or H protein s mapped
to chromosome 6p24and that for T protein s mapped o chro-
mosome3p21-p21,1.Several isease-causingutarionshbeen dentified.Prenatal iagnosis asbeenaccomplished yIorming an assay f the enzymeactivity in chorionic villi biospecimens r by identifrcation f the murantgene.
SARC0SIIEMlA.ncreased oncentrations f sarcosineN-meglycrne) reobservedn borhbloodand urine.but no consi
clinicalpicture
hasbeenattribuced o this melabolicdefect.Tis a recessivelynherited nborn error involving sarcosine drogenase,he enzyme hat converts arcosineo glycine see85-8).The gene or this enzymes ocaredon chromosome qq34.
D-GIYCEF]CCl0UBIA. -glycericacid s an incermediate etalite of serine nd fructosemetabolism see ig. 85-8).At leastforms of this rare condition have been dentrfied, n one foclinical manifestationsof severeencephalopathy hypotoseizures, nd mentaland motor deficits)and the laborarory irngsof hyperglycinemia nd hyperglycinuriawere suggestinonketotichyperglycinemia. hesepatientsexcreted arge qutitiesof o-glycericacid(thiscornpounds not normallv detecin urine). Enzyrne studies ndicated a deficiencyof glyce
kinase n one pacienrand decreased ctivity of o-glycericdedrogenasen another.In the other form, the major findrngsare persistentmetab
acidosis and developmentaldelay, This infant excreted aamountsof p glycericacidwithout hvperglycinemia. he enzdefect n this patient s not known.
No effectrve rherapy is available. Resrncrion of frucimprovedseizuresn one pacient.
TBlMEttlYLAMlNUBlA.rimetiylamine is normally producethe ntestine rom the breakdo*'nof dietarycholineand trimelamine oxide by bacceria. ggsand liver are the main sourcecholine, and fish is che major sourceof trimethylamrne xTrimethylamines absorbed ndoxidized n the iver bv uimetlamine oxidase flavin-containingmonooxygenases)o trime
lamineoxide,which s odorless nd excreted n the urine (see85-8). Deficrency f rhis enzyme esults n massive xcretiotrimethylamine in urine. Severalasymptomaticpatients wtrirnethylaminuria ave been eponed; here rsa foul body othar resemblesha! of a rottefl lish, which may have signifisocial and psychosocialamifications.Restrictionof fish, eIiver,and other sources f choline suchas nutsand grarns) ndiet significantly educe he odor The gene or trimethylamoridase asbeenmapped o chromosomeq23-q25,
HYPEROXURIAAND XAt0SlS.Normally, oxalic acid s dermostly from oxidation of glyoxylic acid and, to a lesser egfrom oxidation of ascorbicacid (seeFig. 85-8). Glyoxylic acformed from the oxidation of glycolic acid in the preoxisoThe source of glycolic acid remainsunclear.Foods containoxalic acid, such as spinachand rhubarb, are the main exonous sourcesof this compound, Oxalic acid canlor be furtmetabolized n humansand is excreted n the urine as oxalaCalcium oxalate s relatively nsoluble n water and precipitin tissueskidneysand oints) f its concenuation ncreasesnDOOy,
Secondary yperoxaluriahasbeenobservedn pvridoxinedciency cofactor or alanine-glyoxylareminotransferase,ee85-8) after ingestionof ethyleneglycol or high dosesof vitaC, after administrationof cheanesthetic gent methoxyflur(u'hrch oxidizes directly to oxalic acid), and in patients winflammaroryborveldisease r extensive esection f the bo(entetichyperoxaLarlal. cute, fatal hyperoxaluriamay deveafter ngestionof plantswith a high oxalic acid conten! sucsorrel.Precipitationof calciumoxalate n tissues auses l?oc
cemia, iver neclosis, enal arlure,cardiacarrhythmia,and de

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 62/177
The lethal dose of oxalic acid is esrimated to be berween .5 and
3 o gPrimary hlperoxaluria is a rare genetic drsorder in wbich large
amounts of oxalates accumulate in the body. Two tvpes of
peroxrsomes se eFig. 85 8).
There is a wide variation rn rhe age of presentarion. The major-
ity of patientsbecomesymptomaticbefore5 yr of age. n =10%
of cases, s,vmptoms de"elop before 1vr of age (neonatal
oxaluria). The inicial clinical mariifestations are related to renal
as gout becauseuric acid is usually elevared n patients wirh rype
I hyperoxaluria. Late forms of the disease presenting during
adulihood have also been reported. Crystalline retinopathy and
optic neuropath,v causing visual loss have occurred in a fe*
patlenrs.
A marked rncrease in urinary excretion of oxalate {normalexcrerion 10-50mg/24 hr) is the most important laboratory
fiading. The presence of oxalate crystals in urinary sedimenr rs
rarely helpful for diagnosis becausesuch crystals are often seen
in normal indivrduals. Urinary excretion of glycolic acid and gly-
oxylic id is rncreased.Diagnosis can be confirmed by petform-
ing an say of the enzyme in hver specimensor by identification
of the mulant 8ene.Medical trearment has been largely unsuccessful. In some
patrents, administration of large doses of pyridoxine redu s
urinary excretion of oxalate. Renal transplantation in patie s
with renal failure has not improved rhe outcome in most cases,
because oxalosrs has recurred in rhe transplanted kidney. Com-
bined liver and kidnev transplanrs have resulted in a sLgnificant
decrease n plasma and urinary oxalate in a few patients, and this
this condit ion. The most common muracion esults n the mis-
targeting of the enzyme to the mitochondria instead of the per-
oxiiomes. The in vicro enzyme activi!y in thesepatients may reach
the level found in obligate heterozygotes. n vivo function remains
defectrve, owever About 30% of parientswith hvperoxaluria
type 1 are estimaled to have this defect.
Prenatal diagnosishas been achievedby the measurementof
fetal hepatic enzyme activiry obtained by needle biopsy or by
dition is due to a deficiency of D-glycerate dehydrogenase
(hydroxypyruvate reductase)/glvoxylate reductase enzyme
complex (see rg .85-8).A deficiencyn the activrtyof rhis enzyme
resu[|s in an accumulation of two intermedrate metabolites,
hydroxypyruvate (the ketoacid of serine) and glyoxylic acrd. Both
these compounds are further metabolized by lactate dehydroge-
nase(LDH) to L-glyceric acid and oxalic acid, respectrvely.About
307' of reporced patients are from the Saultear-rx-Oiibway
Indians of Manicoba.
Clinically, chesepariencs are rndisc inguishable rom those with
hyperoxaluria type I. Renal stonespresenringwith renal colic and
hemarr.rria may develop before age 2 yr. Renal failure rs less
Ch60ter 5 . 0elects n Motabolism l AminoAcids r
comrnon in this condition than rn hyperoxalurra type [; the ur
concains large amounts of L-glyceric acid in addition to h
levels of oxalate (L-glyceric acid is not normally present n urin
Urinary excretion of glycolic acid and glyoxylic acid is
increased.The presenceof L-glvceric acid without increased e
of glycolic and glyoxylic acids in urine differentiates this ty
from type I hyperoxaluria. The gene is mapped to chromoso
No effective therapy is available.
CREATINEEFICIENCYreacine s synthesized n th e liver, p
creas, and kidneys from arginrne and glvcrne (Fig. 85-9) and
rransported to muscles and the brain, in lr'hich there is high c
atine kinase activitl'. Phosphorylation and dephosphorylation
creatine by this enzyme in conjunction with adenosine diph
phate and triphosphate (ADP/ATP) provide high-energv ph
phare reactions in rhese organs. Creatine is nonenzymatrc
metabolized to crearinine ar a constanr daily rate and is excre
rn the urine. Three eenetic conditions are known !o cause cr
tine defciency in rissues,Two are due to deficiency of the enzym
involved in the biosynthesrs of creatine. The enzymes
arginrneglycineaminotransferaseAGAT) an d quanidinoace
methyltransferase (GAIIT) (see Frg. 85-9). Borh conditio
respond well to creatine supplementation. The third condition
caused by the defect in the creatinine transporter(CRTR)
annot resoonsir ro crearinineadminisuation.
Cliniial mani{estations of the three defects are similar, re
to the brain and muscles, and rnay appear in the 1sr few we
or months of hfe. Developmental delan mental retardati
speech delal and serzures are common. Dystonic hyperkine
movements are seen n severe GAMT deficiencv.
Laborarory f indings nclude decreased rearineand crearn
in blood and urine in patients with AGAT and GAMT defe
Marked elevations of guanidinoacetare in blood, urine, and es
cially in CSF are diagnostic of GAMT defects,Low level
suanidinoacetate are found wirh rhe AGAT defect. Absence
ireatine and creatine phosphate (in all three defects) and h
levels of guanidinoacetare (with GAMT defects) can be dem
strated in the brarn by MRS. MRI shows signal hyperintensiry
the globus pallidus. Diagnosis of AGAT or GAMT defects m
be confirmed by measurement of th€ enzyme n the livert cuftu
Gbroblascs,or srimulated lymphoblasts or by DNA analysis
rhe gene. Diagnosis of CRTR is confirmed by genetic analysis
creatrne uptake b;i libroblasrs.
Treatment with creatine monohydrare (350 mg-z g/kg/d
orally has resulted in a dramatic improvement in muscle tone
overall mental develooment and has normalized MRI and e
rroencephalographic 6ndings in pacients wich AGAT and GAM
defects. It is believed that early treatment may assure norm
development. No therapy rs available for the CRTR defect.
AGAT and GAMT defects are inherired as aulosomal reces
traics. CRTR rs an X-hnked rrait. The orevalence of the enzvdeficrencys nor known: lour patientswrrh CA\lT derecr,,rh
from one family) were identified among 180 insticutronal
patients with severe mencal handicap. This condition must
considered in any patienc with brain and muscle disorders, s
treatment calr produce a dramatic response.
85.8.SrRttr raiRezvani
Senne rs a nonessenrial amino acid synthesized rom glucose
glycine (seeFig. 85'9).
3-PH0SPH0GLYCEBATEEHYDR0GENASEEFICIENCY elicie
of this enzyme causes deficiencies of serine and glycine in
body. Clinical manifestations, which are developed in the 1st
months of life, include microcephaly, severepsychomotor re

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 63/177
552 PAFIT I Met6bolicDiseases
3-Phosphoglyceraledeficiency
Glucose
II
3-Phosphoglycerate
l ^I "
Sarcosine
clyoxvlate I
\ l\:ryutrre -
Arginine ------|
\ /-:\Ornithine --4 \9/
IGuanidinoacetate
3-Phosphopyruvate
Serine - 3-Phosphoserine
Figure 85 9. Pathways or the svnthesisof serin
cre3tine.Enzymes:1) 3-phosphoglycerateehydr
as€,(2) guanidinoacetaremethyltransferdseGA
(3) arginine:glycineaminorransleraseACAT).
hydroxyproline (dipeptides nd tripeptidescontaininghydroproli[e) reflectscollagen u.nover and is iflcreasedn drsoof accelerated ollagen turnover, such as rickets or hypa!alhyroidism.
HYPERPR0IINEMIA.wo types oI this rare autosomaLececondition have beendescribed. ype hypetprolinemia s dra deficiency f proline dehydrogenase,nd type II is duedefect n A'-pyrroline-5-carboxylrc cid dehydrogenasenz
(Fig.85"10).Neither type causes ny specific linical manifetion attributable o hyperprolinemia.ncreased lood concetions of proline (morepronounced n rype I) and prolinuriafound in both types. Hydroxyproline and glycine areexcreted n abnormal amounts n the urine because f the sratjon of the commofl nrbular reabsorprionmechanismbymassiveprolinuria. The presenceof ALpyrroline-S-carboacid in plasmaand urine d ifferentiates ype II from rype L treatment s recommendedor the affecred ndividuals.
The gene or prolinedehydrogenases mapped o chromos22q11.2 and several isease-causrngutationshavebeen de6ed;somemutationshavebeenassociated ith an ncreasedof schizophrenia.vlicrodelerion f chromosome 2q11.2cavelocardiofacial DiGeorge,Shpritzen) syndrome. n a steightout of 15 patientswith this syndrome lso had type hy
prolinemia. It has been suggested hat patienrs wirh hyprolinemia be screened (by FISH analysis) for presof rnicrodeletronof chromosome22q11.2. The gene forpyrroline-5-carbor.1.liccid dehydrogenases mapped ro cmosome:1p36,
PR0IIDASEDEFICIENCY uring collagen degradation,dodipeptidessuchasglycylproline) re eleased nd arenorrncleaved y tissueprolidase.This enzyme equiresmanganesits proper activity. Deficiency f prohdase, vhich s inherirean autosomal ecesslvetait. results n the accumulationofdodipepridesn body fluids.
The clinical rnanifestations f lhrs rare condirion and rheat onsetar e quitevariable 19mo to 19yr) and nclude e
S-noenosVlmethionine6{
S-AdenosylhomocysteineJ
Creatine+ + CreatinineI
IUrine
darion, and intractable eizures. ther findingssuchas ailure othrive, spastic etraplegia, ystagmus, ataracts, ypogonadism,and megaloblastic nemiamay also bepresent.
Laboratory indings nclude ow lel'elsof serineand glycine nplasma and very low levelsof serineand glycine n CSF Noabnormalorganicacid s found in the urine. Magnetic esonanceimaging of the brain shows significant attenuation of whitematter and incompletemyehnation.
Diagnosiscan be confrrmedby measurement f the enzyme
activity in cultured ibroblastsand by DNA analysis.Tieatmentwith serine 200-600mg/kg/24hr, orally) alone or
in conjunctionwith glycine (200-300mg/kg/24hr) normalizesthe serine evels n the blood and CSF.This rreatmen!producessignificantmprovement n all clinical rndings xcept or thepsy-chomotor etardation;seizure ctivity subsides ithin a few daysof therapyand may be haltedcompletely.Microcephaly mprovesin young affectednfants. There s evidenceo indrcate hat psy-chomoror etardationmay bepreventedf rhe rearment tarrs nthe 1st few daysof hfe.
The condition s inheritedasan autosomal ecessiverait. Thegene for 3-phosphoglycerateehydrogenase nzyme has beenmapped o chromosome q12 and a few disease-producinguta-tions have been dentified n different amilies,Prenataldiaeno-si sha sbeen chievedy DNA analysisna familywith previously
affectedoffspring; administrationof serine o the mother cor-rectedmicrocephalyn the affected etusas evidenced y ultra-sound imagrng.The favorable response f this condition to asimple reatmentmakes his dragnosis n important considera-tion in any child with microcephaly nd neurologicdefects uchaspsychomotordelayor a seizure isorder
85.9 PR0LINElrai Rezvani
Prolineand hydroxyprolineare found in high concentrarionsncollagen.Neitherof theseaminoacids s normally found in urinein the free form except n early infancy. Excretionof "bound"

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 64/177
Chaoter 5 . Doloctsn l{otabolism l Amim Acids .
\.)A'-Pyrroline- Glutami
acrd
!-igure 85-10. Pathways n rhe mecabohsmof pro
line. Enzymes: 1) proline oxidase, (2) ^lpyrroline
l-carboxylic acid dehydrcgenase,3) hydroxyproline
5-carboxylicacrd
i+
Ornithine
A'-Pyrroline-+ Pyruvic ++hydroxy-s- acid
carlgoxyliccid
19Glyo
acHydroxyproline
Hyd.oxyprolinemia
rent, parnful skin ulcers, which are rypically o hands and legs.
Other skin lesrons hat may precede ulcers by veral years may
include scaly erythematous maculopapular rash, purpura, and
telangiectasia. Mosr ulcers become nfected Healing of the ulcers
mav iake 4 to 7 mo. Mild to severe mental and motor deficits
an d suscepribil ity o infecrionsar e also present n morr patients
(recurrent otitis media, sinusitis, respiratory infection,
splenomegaly). Infection is rhe cause of death.Some patients may
have some craniofacial abnormalities such as ptosis, ocular prop-
cosis, and prominent cranial sutures. Asymptomatic cases have
also been reponed. Development of systemrc upus erythernato-
sus {SLE) has been nored in affected children of one family; young
patients wrth SLE should be screened for prolidase defrciency.
iligb leuels of urinary excretion of imidodipepcides are dragnos-
tic. Enzyme assaymay be performed in eryrhrocytes or cultured
skin 6broblasts,
Oral supplementation wrth proline, ascorbic acid, and man-
ganese and the topical use of proline and glycine result in an
improvement in leg ulcers. These reatments have not been found
consisrently effective in all patients.
The gene for prolidase enzym has been mapped to chtomo-
some 19cen-q13,11and several isease-causing utations have
been identified in drfferent families,
85.10. turAMtcclD lraiRezvani
Glutarhione (y-glutamylcysternylglycine) is the major product of
glutamic acid in rhe body. This ubiquitous tripepcide is synthe-
sizedand degraded through a complex cycle called the y-glutamyl
cycle (Frg.85'11). Because f irs free sulfhydryl (-SH) group an d
its abundance in the cell, glutathione protects other sulfhydryl-
containing compounds (such as enzymesand coenzyme A) from
oxidation. It rs also involved in rhe detoxification of peroxides,
including hydrogen peroxide, and tn keeprng the cell content in
a reduced stare. The common consequence of glurathione defi-
ciency is hemolytic anemia. Glutathione also partrctpates in
amino acid traflsport across the cell membrane through the 1-glutamyl cycle.
GIUTATHI0NEYNTI|EIASEEFICIENCYFlG.85-11).hree orms of
this condition have been reported. In the severe form, whrch is
due to generalzed deficiency of the enzyme' severeacidosis and
massive S-oxoprolinuria are the rule. ln rhe mild forrn, in which
the enzyme deficiency causesglutathione deficiency only in ery-
throc;tes, neither 5-oxoprolinuria nor acidosis has been
observed. A moderate form has also been observed rn which the
hemolytic anemia is associaredwith variable degrees of acidosis
and 5-oxoprolinuna. In all forms, patients have hemolpic anemia
secondary to glutathione defictency.All forms are rare (a coral of
55 patients have been reponed).
Gldathione Synthetase Deficiency, Severe Form (Pyiogluta
Acidernia, Severe 5-oxoFrolinuria) and Modelate Form, Clin
manifestations of thrs rare condition occur in rhe 1st few day
life and include metabolic acidosis, jaundrce, and mild to m
erate hemolytrc anemra. Chronic acidosis continues after rec
ery. Similar episodesof li fe-threatening acidosis may occur dugascroenteritis or an infection or after a surgical procedure.
gressive neurologic damage manifested by mental retardat
spastic tetraparesrs, ataxla, tremor, dysarthria, and seiz
develops with age. Susceptibrlir y ro infection, presumably dL
granulocyte dysfunction, is observed in some patients. Pati
wirh rhe moderate form have milder acidosis and less 5-oxop
linuria than with the severe orm; neurologic manifestations
atso aDsenc.Laboratory frndings rnclude metabolic acidosis, mild ro m
erate degreesof hemolytic anemia, and 5-oxoprolinuna. H
concenrations of 5-oxoproline are also found in blood. The
tathione content of erythrocytes is markedly decreased. ncrea
svnrhesis f S-oxooroline n this disorder is believed o be
!o the conversiol of 1-glutamylcysteine to 5-oxoprolne
the enzyme lglutamyl cyclotransferase see Frg. 85-11)
Glutamylcysteine production Increases greatly because
normal inhibitory effect of glutathione on thelglutamylcysresynthetase enzyme is removed. A deficiency of glutathione
rhetase has been demonstrated in a variety of cells includ
erythrocytes.
teatment of acute attack includes hydration, corr€ctionacrdosrs (by infusron of sodiurn brcarbonate), and measure
correct anemia and hvoerbilirr-rbinemia. Chronic adminisrra
of alkali is usually needed indeGnitely. Administration of l
doses of viramins C and E has been recommended. Drues
oxidants thar are known to causehemolvsir and stressfulbolic srares hould be avoided,Oral adminisrrationof elutarhanalogshas been ried wirh variablesuccess.
Prenatal diagnosis can be achieved by the measurement o
oxoprohne in amniotic flurd, by enzyme analysis in culru
amnrocytes or chronic villi samples, or by DNA analysis of
gene,Successfulpregnancy rn an affecred female (moderate fo
with favorable outcomes for both mother and rnfant has b
reported.
GlutathioneSyniheiaseoeficiency, Mild Form.This form has b
reported in only a few patrents. Mild to moderate hemo
anemia has been rhe only clinical finding in these patie
Splenomegaly has been reported in some patrents. Mental de
oDment is normal: metabol ic acidosis and increased concen
tions of S-oxooroline do not occur Thrs condrtion is due
mulations in tle gene chat encodes for glutathione synthe
enzyme, These mutations, however, presumably render
enzyme unstable but wirh normal catalyti c function. The e
dited rate of enzyme turnover caused by these mutations is o
consequence or all tissues with normal protein synthesis ex
for erythrocltes rn which the absenceof protein synthesis re

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 65/177
554 PABTX MotabolicDiseasss
Glutathioneynth€la6€deficiency
Vitamin 86 dependency
_.--Glutathione(GSH\
. //,,''\\ -Glulafi]'ylcysteinylglycine
,' Aminoacidoutsidethecell
"y-Glutamyl mino acid
Succinicacid
@
LysrneHistidineProline-Histidine*-Prcline.' tOrnithine/
mylcysteine
Glutamica(
Glutamyl
,? 61 ,nz' r
Figure85-11. The glutamylcycle. De
of the glutarhione slnthesis and degr
rj<,n are nored. Enzymes: (11 ysluca
transpeptidase, 2) rglutaDryl cyclotr
ferase, J) s-oxoprolinase,(4) lslutamcvsteine svnthetase,(J) glutathione
thetase,(6) gluramjc acid decarboxy(7) G,{BA transaminase,8) suc.inic s
aLdehyde ehydrogenase.
5-Oxoproline(pyroglutamiccid)
@
@GABA Succinicci d
semialdehyde
III
t-Hydroxybutyricacid
in a serious deficiency of glutathione. Treatment is that of
hemoll.ric anemia and avoidance of drugs and oxidants rhat can
trigger the hemolytic process.
All forms of the condition are inherited as an aulosomal reces
sive trait. The gene for rhis enzyme ls located on chromosome
20q11.2. Several disease-causingmutations have been identifed
in different familiess-0xoprolinase 0eficiency {s-0xoplolinurial. The main cause of
massive 5-oxoprolnuria is glutathione synthetase deficiency lseeearlier). Moderate 5-oxoprohnuria has been found in a variety of
metabolic and acquired conditions, such as n patients with severe
burns, Srevens-Johnsonsyndrome, homocystinuria, urea cycle
defects, and tyrosi lemia type I.
A few individuals with moderate 5-oxoprolinuria (4-10 g/day)
due to 5-oxoprolinase deficiency have been denti6ed. No specific
clinical picture has yet emerged. Modera!e !o severemental retar-
darion has been reported in two patients. Asymptomatic individ-
uals with the enz-vme deficiency have also been identifed,
holvever. It is, therefore, not clear r-herher S-oxoprolinase de6-
ciency is of any clinical consequence. No treatment has been
recommenoeo.
T-Glutamylcysteine Synthase Defciency. Onl)' a few patients
with this enzyme deficiency have been reported. The most con-
sistent clinical manifestation has been rnild chronic hemolytic
anemia.Acureart.rck,, f hemolysishaveoccurredafter expoiure
to sulfonamides. Peripheral neuropathy and progressive spin-
ocerebellar egenerarionavebeennoted n tlvo siblings n adhood. Laboratory findings of chronic hemolytic anemia wpresentn all patients.Generalized rninoacidurias alsoprebecausehey-glutamylcycle s involved n amino acid transpin cells(seeFig. 85-11). Treatmmt is that of hemolvtic aneand avoidance of drugs and oxidants that may triggerhemolytic process.The condition rs rnheritedas an autosorecesslvetatt.
GIUTAIHI0NEMIAT-GTUTAMYI BANSPEPTIDASEGGTjDClEl\lCYl,his enzyme spresentn any cell chathas secretorabsorptive irnctions. t is especiallyabundant n the kidnepancreas,ntestines, nd liver. The enzyme s alsopresent nbile. Measurement f thisenzymen the blood is commonlypformed to evaluate iver and bile duct diseases.
Deficiency f this enzyme auses levation n glurathionecentrations n bodv fluids. but the cellular evels emain normOnly a few patieniswrth enzymedeficiency avebeen eportherefore, he scopeof clinical manifestations as not yet bdelined.Mild to moderatemental retardationatrdsevere ehioral problemswere observed n threepatients.One of the tsisterswith this condition had normal intelligence s an adhowever, nd the other had Prader-Willisyndrome.
Laboratory indings ncludemarked elevationsn urinary ccentrations f glutathione up o 1 g/day),lglutamylcysteine,acysteine.None of rhe reported patients has had genera

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 66/177
aminoaciduria,a 6ndrng hat would have beenexpeccedo occur
in this enzyrnedeficiency seeFig. 85-11).
Diagnosis can be confirmed by measuremenc of rhe enzyme
activirr- in leukocytes or cultured skin fibroblasts No effective
tr€atment is available.
The condicion s nhetited as an autosomal ecessiverair' Th e
enzyme GG T is a complex prorein an d is encoded by at least
sevengenes.
INBoRN8[0BS t METABoLISMt
IAMINoBUTYFICClo
(GABA).Decarboxylation of glutamic acid by glutamic acid decar-
boxylase (GAD) the main biosynthetrc pathway for GABA pro-
duction in the b n and other organs, especially the kidneys and
th e p cells oi the pancreas.Thrs enzyme requires pyridoxine
to chromosome2q31. Knockour of rhe gene or CAD"' in mice
causes left palare; he associarion f mutacions n GAD6' gene
rvhich rs presumably caused by decreasedactivitv of GAD The
maio clinical manifestation of thrs condition is seizures, which
usually occur in rhe 1sc ew hours of life and are unresponsive to
conventional anticonvulsanr cherapy. Adminlsrratioo of vltamin
86 in large doses (10-100 mg/kg) usuallv results in a dramatic
improvementof both serzures nd electoencephalographicbnor
malities. Late onset forrns of checonditton (as ate as 5 yr of age)
have been reported. A trial wirh vitamin 86 therapy has, there-
fore- been recommended n anv infant with intracrableseizures-
The dependency is usually hfelong. Other neurologic findings
such as delayed speechhave been noted in some parients.
Laboratory studies bave revealed increased gluramate and
decreasedGABA levels in the brain and in rhe spinal fluid.
Th e parhogenesis f this condirion remains unclear Alrhough
an increase in che Km of the GAD enzyme for its cofacror
(viramin 86) in the brain seemsa logical explanation, no abnor-
mality in the GAD activicf in the bram has been documented.
DNA studres of rhe gene for GAD* and GADer have likewrse
revealed no mutations. Linkage studies have mapped che condi-
t ion ro rhe long arm of chromosome5q31,2, a locus completely
different from loci of GAD genes.
Treatment wich high daily doses of vitamin 85 is necessary
indelinitell'.
GABA Transarninase eficiency, This is a very rare autosomal
recessivecondition that has been reported rn three infants from
tu,'o different families, Clinical manifestarions include severepsy-
chomotor retardation, hypotonia, hyperreflexia, lerhargl, and
refractory seizures. Increased linear growth was present in the
ofiginal report of two siblings but not in the third patien
Increased concentrations of GABA and B-alanine are found i
the spinal fluid. Evidence of ler.rkodystrophy u'as noled in thepostmortem examination of the brain. GABA transaminase deli-
ciency is demonsrated in the brain and lymphocytes. No effec-
tive treatment is available. Treatment rvith vitamin B; has been
ineffective. The gene for this enzyme is located on chromosome
deficiency (see Frg. 85-11) have been reported. Clinical
manifestarions, which r:sually begin in early infancl rnclude mild
to moderate mental retardation, delaved speech. marked hypo
tonia, ataxra,and seizures-Other associacedindrngsare oculo-
moror apraxia, choreoarhetosis, utist ic €aluresr nd aggressrve
behavior.Ataxia may improve with advancemenc f age,
ChaDter5 | oelects n Metabolism l AminoAcids .
Laboratory studies reveal marked elevarions in 1-hydroxvbtyrrc acrd concenrrations n the blood (u p co 200-fold), sp
fluid (u p to 1,200-fold),and urine (u p to 800-fold). There is
acidosis. Urinary excretion of y-hydroxyburyric acrd decrea
wirh age. ncreased oncentrations f glycinemay also bepres
in pJasma, rine, and spinal f lLrid.
Diagnosis can be confirmed by measuremenr of the enzy
activi!]' in lymphocvtes. Prenatal diagnosis has been achieved
measurement of 1-hydroxybutyric acid in the amniotic fluid
assayof the enzyme activity in lhe amniocytes of in biopsy sp
imens of chorionic vil l i,Treatment has been largely ineffective; vigabatrine has p
duced some improvement !n ataxia end mental status n so
Patlents.The condicion s inheritedas an autosomal ecessiverait, T
gene for succinic semraldehydedehydrogenase has been map
to chromosome 6p22; several disease'causingmutatrons h
been identilled in drfferent families.
The role of 1-hydroxyburvric acid in the pathogenesis of
condit ion remains unclear and somewhat confusing beca
admrnistration f this compound to humansand animalsha sp
ducedsomeopposireeffects,1-Hydroxy-bur,vrateGHB) has b
used ll i cit ly as a recreationaldrug with anesthetic ffecr an
on e of th e dare-rape rugs (seealso Chaprer 113).
Congenital Glutanine Deficiency. This uncommon disorde
du e to a deliciency f glutaminesynthase.Glutamine s absenplasma, urine, and CSF but plasma levels of glutamate rem
normal. Manifesracions nclude cerebralmalformations (abn
ma l gyration, u.hire matter esions),multrorgan arlure ncltrd
respiratory ailure, and neonataldeath. t may be nhericedas
autosomal rart; the gene s mapped o chromosome 1q31.
85,11 UREAvclrro Hvprnamnirolrtsr(Anetrne, ITRULUNE,nlrutrurl lrai Rezva
Catabolism of amino acids resulrs rn the production of
ammonia, u'hicb is highly toxic to the central nervous s,vs
Ammonia is deroxif ied to urea lhroueh a seriesof reactkno rvn as rhe Krehs-Hen .e le i tr u rea cyc le F ig .E5 -12 t .
enzymes are required for the synchesisof urea: carbam,vl ph
phate synthetase (CPS), ornirhine transcarbamylase(OT
argininosuccinate ynchetaseAS), argininosuccinateyase (A
and arginase, A sixth enzyme, N-acetylglutamate s,vnthetas
also required for synthesis of N-acetylglutamate, which is an a
vator of the CPS enzyme. Individual deficienciesof theseenzy
have been observed and, r'ith an overall estimated prevalenc
1/30,000 live births, they are the most common genetic cause
hyperammonemia n infants,
GENETICCAUSES0t HYPEBAMMONEMIA.n addrtron to sen
defectsof rhe urea cycle enzymes.a marked increa.e n pla
level of ammonia is observed in other inborn errors of meta
lism (Table85-2).
Ctll{l0At MANIFESTATI0t{S F HYPERAMMONEMIA.n the neo
tal period, symptoms and signs are rnostly related to brain d
function and are simrlar regardless of the cause of
hvoerammonemia. The affected infant is normal at birth
beco-es sympromatic within a few days of protein feed
Refusal to eat, vomrtinB, rachypnea, and lethargy quic
progress o a deep coma. Convulsions are common. Phy
examination may reveal hepatomegaly in addition to rhe ne
logic signs of deep coma. In infanrs and older children ac
hyperammonemia is rnanifested by vomiting and neurolo
abnormalicies uch as ataxia, mental confusion, agrtation,
tabilit l, and combativeness. hese manifescationsmay alcer

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 67/177
556 PABT I MetabolicDiseases
Benzoate
I
Glycine+ BenzoylCoA
.. Glutamate' . +
A m m o n i a + c o 2 + A T P Phenylacetate
Acetyl CoA+
Glutamicacid
Putrescine
oTc
Citrulline
Citrulline
.. OrnithineU ea+--__\
I\ ^
r--------------- l(5)I A ' s i n i n e m i a | { v- \
Cylosol
Arginine
,,.*".-\q"i:?#;;.
\JnthetaseI I ,
del lLiency | 1_
I f - N-Acetyl-glutamiccid NAG) *^+ | cps oeficiency | -- IA (1)l
_J phenytacetyl
V, \, I glutaminephosphale
l-cl,----;".t'.phy-l- Glutamic acid
'y-semialdehyde
Argininosuccinicaciduria
f isrrcgi- l l . t t reacycle:larhways tr ammonrrdisposal ndorni thinemerabol ism. eact ions ccurringn rhemitochondria redepictcdn rwPl" Rea.
shown whh i,,crruptud anoars are rhe afternarepathways or rhe disposal of ammouia. Enzyncs:(l
) carbamll phosphatesynthetaseCPSi,
2) onrthine trc a r b a m y l a s e ( O T C ) , l ] ) . . g i n i n o s u c c i n j c a c i d s V n t h e t a s e ( A s ) ' i 4 ) a r g i n i n o s u c c n l i c a c i d 1 y a s e l A L ) , i j ) a I g i n a s e , ( 6 ) o r n i t h i n e 5 - a m l n o r agluranletc NA(;) synthctasc. 'HHH syndrome. yperammonrnra-hvperorni thinemiaomocrrrul l inemia.
u.rth periodsoi lechargvand somnolence bar may progres
coma.Routine laboratory studies sholv no spec ifrc findings u'
hyperamrnonemia rs due to defects of rhe urea cycle enzymBLoodurea nirrogen s usually ow SerumpH is usuall-v or
or mrldly elevated. In infants with organic acidemiirs, hvper
monemia is commonlv associated vith severe acidosis. NewbinFants vichhyperammonemia re ofren misdiagnosed s ha
sepsis; hev may succumb vr.ithouta correct diagnosis.CT m
reveal cerebral edema iFig, 85 13). Autopsy is usually umarkable, t is imperative o measure lasma ammonia leve
any il l infant q.hoseclinical manifestations annot be expla
by an obvious infection.
DlAGtloSlS. The main cflterion for diagnosis is hvperammo
mia. The plasma ammonia concentration in the ill infan
usuallv >200 ptmole/I. (normal values <35 pmole/L).
approach to the differeotial diagnosis of hyperanmonemia rn
newborn nfant is l lustrated n Figurc 85-14-Patienrswith a d
crency of CPS or OTC have no specific abnormalities of plas
amino acids except for increased levels of glutamine, aspa
acid, and alaninc secondary o hyperammoncmia. A mar
incrcase n urinary orotic acid in patients with OTC defici

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 68/177
Figure 8-s 11. Compurer axiat tomographic scansof rhe head oI hyperamnonemic encephalopathy n the composite case of ornirhine transcarbamylascjency.A, Imagedone on admissioD o the community hospital. B, Image done 24 hours larer denonstrates bilateral hemispheric€dem, with eff.cemenr of
brospinal fluid spaces. From Brusiloe SV/: HyperammonemicencePhalopathv.Medicine 2002;81:240 )
NoacidosisIIt
Obtain
Transienihyperammonemi
of henewborn
Figure 85-14. Cljnical approach to a newborn infant lvirh symptonatic hyperammonemia.CPS, carbamyl phosphate synthelaseiHHH syndrom€, hyp
monemra-hvperornithinemia'homocrtrullinernia;AG, N acetvlSluramateiOTC' ornrrhin€ uansarbamvlase
Specificaminoacid elevation
Chrpler 5 r Delocls [ Motabolism l AminoAci& r
Nospecilic minoacidelevation
IObtain
urine oroticacid
Normal r elevated
I
High
I oic--lI oeticiency

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 69/177
55t r PAR|IX MerEboliciseasos
differentiateshis defect rom CPSdeficiencv, atientswith a deli-ciency of AS, AL, or arginasehave a marked increase n theplasma level of citrulline, argininosuccinicacid, or arginine,respectively. ifferentiation between he CPSdeficiency nd theN-acetylglutamateNAG) synthetase eficiencymay requireanassay f the respective nzymes.Clinical mprovementoccurringafter oral administration of carbamylglutamate, oweveqmaysuggest AG synrhetase eficiency.
TREATMENTt ACUTEYPERAMM0T{EMlA.cure
hyperammone-mia should be treatedpromptly ard vigorously.The goal oftherapy s !o removeammonia rom chebodyand o provideade-quate caloriesand essential mino acids ro halt further break-down of endogenous roteins (Table85-3). Adequatecalories,fluid, and electrolytes hould be provided intravenously. ntra-venous ipids (1 ElkglL4ht providean effectivesourceof calo-ries.Minrmal amountsof protein (O.25gkgl24 hr), prefetably nthe form of essential mino acids,should be added o the intra-venous luid to preventa catabolic tate.Oral feedingwith a low-protein forrnula \0-5-7.0glk9lz4 fu) rhrougha nasogastricubeshould be srartedas soon as sufficient mprovement n lhe clinical condition s seen.
Because he kidneysclear ammoniapoorly, its removal fromthe body must be expeditedby formation of compoundswirh ahigh renal clearance. odium benzoateorms hippuric acid withendogenous lycine (seeFig. 85-12). Each mole of berzoareremoves1 mole of ammoniaasglycine,Phenylacetateonjugareswith glutamine o form phenylacetylglutamine, hich is readilyexcreled n the urine.One mole ofphenylacetateemoves molesof ammoniaasglutamne from the body (seeFig. 85-12).
Arginine adminisrration s effective n the rreatmentof hyper-ammonemia hat is due to defectsof the urea cycle (except npatients&'ith arginasedeficiency)because r supplies he ureacyclewith ornrrhrneand NAG (seeFig. 85-12). n patientswithcitrullinemia,1 mole of arginine eactswith 1 mole of ammonia(as carbamyl phosphate) o form citrulline. In patients wirhargininosuccinic cidemia,2 moles of ammonia (as carbamylphosphareand aspartate) eact with arginine to form argini-nosuccinicacid. Crrrullineand areininosuccinic cid are far less
roxicand more readily excreted
6y the kidneyshan ammonia.
In patientswith CPSor OTC deficiency , rginineadministrationis indicatedbecause rginrnebecomes n esseotial mino acid nrhesedisorders,Patientswith OTC deficiencybenefit rom crt-rulline supplementarton200ng/kEl24 hr) because moleof crt-rulline can accept1 moleof ammonia asasparticacid) ro formarginine.Adminrsrratronof arginine or ci trulline is contraindi-cated n patiencswith arginase eficiency. rginasedeficiency sa rare condition n which acutehyperammonemiaarely occurs
as a presenting ign, n patienrswhosehyperamrnonemias sondary o organicacidemias,reatmenrwirh arginine s not incated becauseno beneficialeffect from such theraov canexpected.n a newborn nfant with a lsr artackoi'hyp.rnmonemia, arginine should be used until the diagnosisestabhshed.
Benzoare,phenylacetate, nd arginine may be administetogether or maximal therapeutic ffect.A priming doseof rhcompounds s followed by continuous nfusion until recovfrom the acutestateoccurs seeTable85-3). Both benzoatephenylacetate re usuallysuppliedas concentrated olut ronsashould beproperly dlluted(l-2yo solution) or intravenousThe recommendedherapeutic osesof bochcompounds elia substantial mountoI sodium o the patient hat shouldbe cculated s parrof the daily sodium equirement. commepreparationof sodium benzoateplus sodium phenylacetaavailable or intravenous se(MedicisPharmaceutical orpocion,wwwmedicis.com),Benzoare nd phenylacetacehouldused wirh caution in newborn infants with hyperbilirubinebecausehey may displacebilirubin from albumin (seeChap102,4). n infants at risk, it is advisableo reducebilirubin tosafe evel beforeadministering enzoate r phenylacetate,
If the foregoing therapies ail to produce any appreciachange n heblood ammonia evelwithin a few hours,hemodysisor peritonealdialysisshould be used.Exchangeransfushas little effecton reducing otal body ammonia. t shouldusedonly if dialysiscannot be employedpromptly or when tpatient s a newborn nfant wrth hyperbilirubinemia see arliHemodialysis, lthough the most effectivemeasure or remoof ammonia, s technicallydifficr:lt to perform and may notreadil;' available.Peritonealdialysis s the most practical aexpeditiousmethod or treatmentof patients vith severe ypammonemia; here s usually a dramaticdecreasen the plasammonia level withrn a few hours of dialysis, and in mparients, he plasmaammonia eturns o normal within 48 hrinitiarion of peritoneal dialysis. n a patrent whose hyperamonemia s due ro an organicacrdemia, eritonealdialysiseffttvely removesboth the offending orgamc acid and ammofrom the bodv.
To curtail the possibleproduction of ammonia by rntestbacteria,oral adminisrrationof neomycinand lactulosehroua nasogastricube shouldbe nitiatedvery early n the coursetherapy.There may be considerableag betrveenhe normalition of ammoniaand an mprovementn the neurologic tatusthe patient.Several aysmay beneeded efore he nfant becomfully alert.
Long-Tern horspy.Once rhe nfant is alert, therapy shouldtailored to the underlyingcause of the hyperammonemiageneral,all patienls require some degreeof protein restrict(1-2 glkg/24hi) regardless f the enzymaticdefect. n pariewith defectsn the wea cycle. hronic administrarion f benzo(250-500rng/kg/2a r), phenylacetate 250-500mgikgl2ahand arginine 200-400mglkg/24hr) or citrulline(in patientswOTC deficiency, 00a00 ngfl<g124 r) is effective n maintaing blood ammonia evelswithin the normal range. Phenyl
tyrate may be used n placeof phenvlacetate,ecausehe patiand the family may not accept he latter owing to its offensodor.A commercial reparation f thecompound s availableoral use(Buphenyl,Medicis Pharmaceutical orporation).Cnitine supplementations recommended ecause enzoateaphenylacetate ay cause arnitinedepletion; he clinical beneof this compound emain o be proved.Skin lesrons esembacrodermatitisentropathicahave been noted in a few patiewith differenr ypesof ureacycledefects, resumably ue o deciency of essentral mino acids, especiallyarginine, causedoverzealous ietary protein restliction. Carabolicstacesrigging hyperammonemia hould be avoided. n patientswith CPOTC, and AS deficiencies, cute hvperamrnonemicttacksmbe precipiraredy vaLporatedministration.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 70/177
CARBAMYLPHOSPHATE YNTHETASECPS)AND fl.ACEIYI.GI.UTA-
MATE NAGISYNTHETASEEFICIENCIESSEE lG.85-12}Deficien-
cies of these two enzymes Produce slmilar clinical and
biochemical manifestations. There is a wide varianon in severit,v
of symptomsa in the ageof presenta!ion.Most commonl), rh e
affected rnfant comes symPtomatic durrng rhe 1st few days of
byperammonemia intelspersed wirh bouts of acute h-vperam
molemia have also been observed.
term therapy of rhe condicion s oullined earlier (see able 85-3).
ParientsvvrthNAG synthetasede6ciency benelir from oral admin-
istratron of carbamylglutamate. It is therefore important to dif
ferentiate betrveenCPS and NAG synrhetasedelicienciesby assay
dicion is not known.
OBI{ITHINE TBANSCAREAMYIASE OTC) DEFICIENCY SEE FIG.
85-12). n tbis XJrnked partially dominant disorder, lhe hemrzl'
gote males are rno severelyaffected than heterozygote females-
The heterozygous males may have a mrld form of the disease,
but the majonty 757o) are asymptomatrc.This is the most
common form of all rhe urea cycle disorders
Clinicalmanifesrations in a male newborn infant are usuallv
rhose of severehyperammonemia (seeearlier) occurring in rhe 1st
ferv days of life. Milder forms of che condirion are commonl)
seen n heterozygous females and in some affected males. Mild
forms characterrsrically have episodic mamfesrations, t'hich may
occur at any age (usually after infancy). Episodes of hvperam
monemia (manifested by' vomiting and neurologic abnormalities
survivors; the mechanism remains unclear
The maj laboratory finding during rhe acuceatrack is hvper-
ammonem without an increase n any specificamino acid rn the
blood. Elevatronof cheplasma concenlrationsof glutamine and
alanine are secondary to hyperammonemia A marked iocrease
tare in urine as gravel or stones. n the mild form, these boratory
abnormalities may revert to normal between artacks. hrs form
should be differenriated from all the episodic conditions of child-
hood, ln parcicular, lysinr:ric prorein inrolerance (see Chapter
85,13) mimics the clinical and biochemical characterist ics f
OTC deficiencl', ncreased urinary excretions of lysrne, ornithine,
and rginine and elevated blood concentrations of citrulline,'w'hic are salient features of lysinuric protein intolerance, are not
seen n patrents with OTC deEciency.
Chalter85 r Delectsn Metabolism t AminoAcids .
The diagnosisma,v be confir med b1-performing an assa
enzyme aclivity that is nonnally presentonly in che iver or
identif ication of tbe murant gene. Prenatal dragnosishas b
achieved by means of fetal hver biopsl' or by DNA studie
chorionic r.illi samples. An oral protein load, u'hich incte
plasma ammonia and urinary orotic acid levels , may iden
asympromatic heterozygous female car'riers. A marked incre
rn urinary excrecion of orotidine after an allopurinol loading
also detects obligate female carriers. Mild cerebral dysfunc
may be present n asymptomacic emalecarriers.
Treatment of acute hyperammonemic atracks and the lo
term therapy of the condirion is outlined in earler pages of
chapcer. Citrulline is used in place of arginine in patients w
OTC deficrency.Lrver transplantarion is a successfuland def
treatmenr for patients with OTC delicrency who have been
conrrolledand have avoided mult ipte hyperammonemrc ris
The gene for otnithine transcarboxllase has been mappe
X chromosome (Xp21.1). N' lany disease-causingmutac(>200) have been identified in different patients. The degre
enzyme deficiency and rhe genotype dictate the severitv of
phenorype in most cases,Mothers of affected nfants are expe
ro be carriers of the mutant gene, A rnother rvho gave birth
rwo affecred male offspring vas found to have normal genot
suggestinggonadal mosaicism in the mother.
ARGININOSUCGINATEYNTHETASEAS) DEIICIENCYCITRUt
MlAl [SEEFlG.85-12]. wo clinically and genetically distinct fo
of citrulUnemiahave been dencif ied. he classic orm (type
due to the deflciency of rhe AS enzyme, The adult form (typ
is due to deficiency of a mitochondrial transport plotein na
crttrn,
Citrull inemia ype (ClassicCitrull inemia, TLN'l). his cond
is causedby the deliciencyof AS (seeFig. 85-12) and has v
able clinical manifestation depending on the degree of the enz
deficiencv. Two maior forms of che condition have been ide
fied. The severe or neonatal form, which ls the most comm
form of rhe condition, appears in the lst few days of life w
sign and synptoms of hyperammonemra (seeearlier). In rhe
acute or mild form, clinical findings such as failure to thri"e,
quent vomiting, developmental delay, and dr1 brittle hai r ap
gradually after 1 yr of age. Acute hyperammonemia, triggere
an inrercurrentcatabolic stace,may bring the diagnosis o li
Laboratory findings are similar to those found in patients w
OTC deficrency except thar the plasma cicrulline concentratro
markedly elevared (50-100 rrmes normal) in patients with
rull inemia ype I (seeFig. 85-14).Urinary excretionof orotic
rs moderarely increased; crystalluria drLe o precipitation of
rates may also occur The diagnosis is confirmed by perform
an assayof the enz-vme ctii,it,v n cuhu.ed fibroblasts or by D
analysrs. renaraldiagnosis s accomplishedby th e assayof
enzyme activit], in cultured amniotic cells or by DNA analys
cells obtained from chorionic vilh bropsv.
Treatment of acute h,vperammone[lic attacks and the lo
term rherapy of the condition are outlned in rhe earlier pag
rhis chapter Plasma concentration of citrulline remains elev
at all times and may increase urther afrer administration ofnine. Although prognosis is poor for symptomatic neon
patients with the mild disease usually do rvell on a prot
restricted diet in conyuncdon with sodium benzoare and argi
therapy. Mild to moderate mental deGcrenc,v s a com
sequela, ven n a rvell-treared acient.
Citrullinemia is inheflted as an autosomal recessive rait.
gene rs located on chromosome 9q34. Several disease-ca
mulations have been identi{ied in differenr families. The ma
icy of patients are compound hererozygotes for two diffe
alleles. The prevalence of rhe condrtiol is not known,
Cilrurullinemia ue o CitrinDeficiencyCitrull inemia ype l. C
2), Citrin is a mitochondrial transport protein ercoded by a
(SLC25A13) located on chromosome7q21.3. One of the f

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 71/177
560 PARTX. MGtaboliciseas6r
tions of this protein s ro transport aspartaterom mitochondriato cytoplasm;aspartate s requrred or convertingcitrr:llne toargrninosucciniccid see ig. 85-12).Citrin deficiency auses is-ruption of the urea cycle.AS activity is deficient n the liver ofthese atients,but no mutatron n thegene or AS hasbeen ound,It ispostularedhar crtrin deficiency r its mutatedgenenterfereswith translationof nRNA for AS enzymen the liver.Mutatronin the gene or citrin produces wo distinct clinical entities,Thecondition s reportedalmost exclusivelyn Japan.
NeonatalntrahepaticholestasisCitrullinemia
yp el-Neon8talFotm).Clinical and laboratory manifestations,which usuallystarts at 3 mo of age, nclude cholestatic aundrcewith mild tomoderate direct (conjugared) hyperbilirubinemia, markedhypoproteinemia, lottrng dysfunction (increased rothrombintrme and partial thromboplastin times), and increasedserum
lglutamyltranspepridase (GGTP) and alkaline phosphataseactiviues; llver transaminasesare usually normal. Plasmacorcentrationsof ammoniaand crtrullineare usuallynormal, butmoderateelevations re reporled.Theremay be also ncreasesnplasmaconcentrations f merhionine, yrosine,alanine,and thre-onine,Elevation n serumgalactoseevelshasbeen ound n somepatlents; all enzymes nvolved in galactosemetabolism arenormal. The reason or hypergalactosemias not known. Markedelevation n serurn evelof c-fetoprotein s also present.Thesefindings esemblehoseof tyrosinemia ype , but unlike he attercondition, uilnary excretion of succinylacetones not elevated(seeChapter85.2), Liver biopsyshows arty nfiltration, cholesta-srswith dilatedcanaliculi,and a moderatedegree f 6brosrs.Thecondition is usually selfJimicing and the majority of infantsrecoverspontaneously y 1yr of age with only supportiveandsymptomatic reatment.Hyperammonemra nd hvpercitrullinemia, f present, houldbe treatedwith low-proreindiet and otherappropriatemeasuressee arlier).Hepatic ailure requiring ivertransplantation as occurred n a few cases. lthough the condi-tion is almost exclusively een n Japan,chediagnosis hould beconsideredn any neonatalhepatirissyndromewrth cholestasis.Data on the long-termprognosrs nd the natural history of thecondition are imrted:develoomentnto theadult orm of thecon-drtion (see ater) after seueril yearsof seemingly symptomatichiatus has beenobserved.
CitrullineniaType l, Adult Fo n {Adult-onselCilrullinemia, it-rullinemia ype l-Mild Form). his form stans suddenly n a pre-vrouslynormal individual and manifestswith neuropsychiatricsympromssuch as disorienration,delirium, delusion,aberrantbehavior, remors, and frank psychosis.Moderate degreesofhyperammonemia nd hypercitrullinemia represent. he ageofonsets usually etween 0 and40 yr (range 1 o 79 yr).Patientswho recover rom the 1st episodewill have ecurrentattacksandmost will die within a few yearsof diagnosismarnly from cere-bral edema. Pancrearitis,hyperlipidemia, and hepatoma aremajor complicatrons mong he survivors.Medical reannenthasbeen mostlv ineffective or oreventionof future attacks.Livertransplantation s the most eifective herapy.
Several isease-causingutationsof the genehave been den-tified in affected amilies in
Japan.The pathogenesis f cit-
rullinemia rype I (neonaral nd adult forms) remarns nigmatic.Although the frequencyof abnormalgene s quitehigh in Japan(1;20,000homozygosity),he clinical condition has a frequencyof onlv 1:100.000. his rndicateshat a substantial umberofhomozygous ndivrduals emainasymptomattc.Only a few non-
Japanese atientshave been dentified.
ARGININOSUCCINATEYASEATIDEFICIENCYARGININOSUCCINIC
ACIDURIAISEEFlG. 5-12]. he severityo{ rhe clinical and bio-chemical manifestationsvaries considerably, n the neonatalform, signs and symptoms of severe hyperammonemia seeearlier)develop n the lst few daysof lile andmortaliry s usuallyhigh. Infantswho survive he lst acuteepisode ollow the ctini-cal courseof chesubacuteorm. In the subacute r lare orm. the
major finding is mental retardation,which is associatedwfailure to thrive and hepatomegaly. bnormahtiesof rhe hcharacrerizedy dryness nd britdeness re of specialdiagnovalue.Gallstones avebeenseen n someof the survivors.Acattacks.. f severehyperammonemia ommonly occur durincatabollcsrate.
Laboratory findings ncludehyperammonemia,moderatevations n liver enzymes, onspecilicncreasesn plasma evegluramineand alanine,moderate ncreasen plasma evelsof rulline (less han that seenn citnllinemra), and marked ncrein plasma evelsof argininosuccinic cid (see ig. 85-14). n mamino acid analyzers, rgininosuccintc cid appearswithrn isoleucine r methionine egion,which may cause onfusiothe diagnosis,Argininosuccinic cid can also be found in laamounts n urine and sprnal luid. The levels n the spinal flare usuallyhigher han those n plasma.The enzyme s normpresentn erythrocytes,he iver,and cultured ibroblasts,Pretal diagnosis s possibleby measurernent f the enzymeactiin culturedamnioticcellsor by identificationof the mutanr geArgininosuccinicacid is also elevated n rhe amniotic fluidaffected etuses.
Tieatrnentof acute hyperammonemic ttacks and the loterm thelapy of the conditionare outlmed n the earlierpagethis chapter Mental retardation,persistenthepatomegalywmild increasesn liver enzymes, nd bleeding endencies ueabnormalclotting factorsare common sequelae f rhe diseThis def iciency s rnheritedas an autosomal ecessiverait witprevalence f =1/70,000 ive binhs. The gene s locatedon chmosome cen-q11.2
ARGTNASEEFTCTET{CYHYPEBARGTNtNEM|A)SEEFrG. 5r2]. Tdefect s inhentedas an autosomal ecessiverait. There are tgenetically istinctarginasesn humans.One scytosolic A1) ais expressedn the liver and er;throcytes,and rhe other (A2found in rhe renaland brainmitochondria.The gene or cytolic enzyme,which is the one deficient n patientswith argindeliciency,s mapped o chromosome q23, The role of the mchondnal enzyme s not well understood;ts activity ncreaspatienls with argininemiabut has no protec ve effect.Sevdisease-causing utations have been identified in differmm tes.
The clinical manifestatiomof this rare condition areouire ferent rom rhore ol: other urea cycleenzymedetects. he onis insidious; he infant usuallyremainsasymptomatrcn thefew months orr sometimes, earsof life. A progressive padiplegiawith scissoring f the ower extremities, horeoarhernovernenrs,nd ossof developmentalmilestonesn a previonormal infant may suggest degerierative isease f the cennervoussystem.Two children were fteated for several earcerebral alsybefore he diagnosis f arginase eficiencywascfirmed. Mental retardation s progressrve;eizures re commbur episodes I severe yperammonemia re nor usuallyseethis disorder Hepatomegalymay be present.The acuteneonform with intractable eizures,erebral dema, nd deathhasabeen eported.
Laboratory findings nc ludernarkedelevationsof argininplasma nd CSF se e ig. 85-14).Urinaryoroticacid s modately ncreased. lasma mmonia evelsmay be normal or milelevared.Urinary excretionsof arginine, lysine, cystrne,aornithine are usually ncreased, ut normal levelshavealso bnoted. Therefore,determrnationof amino acids in plasma cri tical step in rhe diagnosisof argininemia,The guanidcompourids {a-keto-guanidinovalenc cid, argininic acid) markedly ncreasedn urine.The diagnosiss confirmedby aslng arSrnasechvrtym erytnrocytes,
Treatmentconsisrsof a low-prorein diet devoid of arginAdministration of a synthericprotein made of essential macids usually resulls n a dramatic decreasen plasmaarginconcentralionand an improvement n neurologicabnormali

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 72/177
gooo conlrol.
TBANSIENTHYPERAMMONEMIAF THE NEWBOBN.Althoughplasma levels of ammonia in normal full-cerm infants are within
normal limits, very low birthweight rnfants may have a mild ran-
sient hyperammonemia (40-50 pmole/L), which lasts for about
5-B wk. These infants are asymptomatic! and follow-up studies
up to 18 mo of age have not revealed any signifrcancneurologrc
delicirs.
Severe transient hg>erammonemia has been observed in
newborn infants. The maioriry of affected infants are premaLure
and have mild respratory drstress syndrome HyPerammonemic
coma may develop within 2-3 da1'sof life, and the infanr may
succumb to the drsease f treatment rs not started immediately.
Treatment of hyperammonemia sbould be initiated promptly and
contrnued vigorously (seeearlier). Recovery without sequelae s
common, and hyperammonemia does nor recur even wirh a
normal protein diet.
oRNITHINE,Ornithine is one of the intetmediate metabolites of
and converts ornithtne to Putrescine (seeFig. 85-12) Two genetic
disorders result in hyperornithinemia: gyrate arrophy of the re
rina and hyperammonemia-hyperornithinemia-homocirrulline-
loss of peripheral vision, and postelror subcapsulal cataracts.
These eyi changes start betweel 5 and 10 yr of age and Progress
to complete blindness by the 4rh decade of life. Atrophrc lesions
rn the retina resemble cerebral gyri. These patients usually have
normal inrelligence.There is a 10- co 20-fold increase rn plasma
levels of ornithine (400-1,400;rrnole/L). There is no occurrence
of hyDerammonemia nd no increasesn any other amino acids;
pla"ma levelsof gluramare.glutamine. ysine,crearine. nd crea-
iinine are moderarelydecreased. om epaLients e*pond partially
to hieh dose' uf pyridoxine 1 00 - I 00 0 mg/24 hr). Argrnine-
res r r i ; t ed ie r n cun iunc r ion i t h .upp lem en ra lys rne . ro l ine .
and creatine has been successful tn leducing plasma ornithlne
concentration and has produced some clinical imProvemen s The
gene for ornithine 5-aminotransferase is mapped !o chromosome
10q26.M"ny (a t least 60) drsease- ausrngmutations have been
identifred in drfferent famrlies
HYPERAMMONEMIA.HYPEBORNITHINEMIA-HOMOCITRUTLINEMIA{HHH}SYNDR0ME,n hts are utosomalecessivelynheritedrs -
Chaoler 5 r oelecL in Motobolisn l AminoAcids r
order, the defect is in the transport sysrem of ornirhine from
cytosol into rhe mitochondria, which causesan accumulatio
ornithrne in rhe cytosol and a defciency of ornithine inside
mitochondria. The former causes hyperormthinemia and
latter resuks n disruprrono{ the urea ycle and h} peramm
mi a (seeFig. 85-12). Homocirrull ine s presumably ormed f
the reacrion of mitochondrial carbamyl phosphate with lys
which occurs because of the intramitochondrial deficienc
ornithine. Clinical nanifestarions of hyperammonemra
develop shortly afrer birch or may be delayed until adultho
Acute episodes of hyperammonemia manrfesr as refr.rsal o f
vomiring, and lethargy; coma may occut during infancy.
gressiveneurologic signs, such as lower limb weakness, ncre
deep cendon reflexes, spasticitn clonus, seizutes, and var
degreesof psychomotor retardalion may develop if the condi
remains undiagnosed. No clinical ocular f indings have b
observed in rheseDatients.Laboratory findings reveal marked increases n plasma le
of ornirhine and homocirrull ine n addrtion o hyperammone
Rescricrion of protern inrake improves hyperammone
Ornrthrne supplementation may produce clinical improvemen
somepatients.The gene or rhis disorder(SLC25,415) s loc
on chromosome 13q14.
85,12. rsrtDtNEraiBezvani
Histidine is an essentral arnino acid only during infancy
biosynthetic palhway in older children and adults is po
understood. Hrstidine is degraded through the urocanic
pathway ro glutamic acid. Severalgenetic ondit ions invo
rhe degradative parhway of histidine hav been reported,
none has any clinical consequence.
85.13.vstt ' tt raiRezvani
The major pathway n the catabolismof lysine nvolves ts
densarionwirh ct-ketoglutaric cid to form saccharoprnecharopine s then degraded o o-aminoadipicacid semialdand glutaric acid. These lst two steps are catalyzed baminoadipic semialdehyde ynthase,which has two activlysine-ketoglutarateeductase; nd saccharopine ehydrog(Fig.85-15). n a mrnorparhway or ysine egradation,ysrransaminated6rst and rhen condensed o the cyclc fpipecolicacid.This s the maior pathwa), or Dlysine in rheban d or the L-lysinen the brain se e ig .85-15).
Hyper$sinemia, a-aminoadipic acidemta and a-ketoaacidemia arethree condicions har are due to rnborn erromembolsm of lysine. Individuals wirh these conditionsusuallyasymptomatic.
GIUTAEICCIDURIAYPE Gluraric acid s an intermediatendegradation f lysrne see ig. 85-15), ydroxllysine, ndtophan.Glutaric aciduria ype , a disordercaused y adefrcof glutaryl CoA dehydrogenase,hould be drfterentiatedglutaric aciduria ype Il, a distinc t clinical and biochemicaorder causedby defects n the electron transport systemChaocer5 ,1 ) .
ClinicatManifestations, ffected nfants with gJuraricacrrvpe may developnormally up to 2 yr of hfe; macrocepha common6nding n these nfancs.Symptoms f hypotoniaof head control, choreoathetosis, eizures, eneralized igopisthotonos,and dystoniamay occur suddenly n a seemnormal infant after a minor infection. Recover-vrom th
anack usuallyoccurs lowly,but some esidualneurologic bmalicies, specrally ystoniaand extrapyramidalmovements

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 73/177
562 PABT r MetabolicDisoases
Protein ynthesis
o-N-acelyl-lysine
NH2-(CH2)4 CH-COOH
Pipecolicacrd
........- Piperidine-6-carboxylic cid
persist.Addidonal acuteepisodesesembling he 1st one usuallyoccur during an intercurrent nfecrion. n other patients, hesesignsand symptomsmay developgradually n rhe 1st feu,'yearsof life andhypotoniaand choreoathetosis aygraduallyprogressinto rigid iry and dystonia.Acuceepisodes f metabolc decom-pensarionwith vomiting, ketosis,seizures, nd coma also com-monly occur in thesepauentsafter infectionor other catabohcstates.Death usually occurs n the 1st decade f life during oneof theseepisodes. he intellectualabilities usually remain rela-tir..el) 'normaln mostpatienrs.
Laboratory indings. uring acute episodes,mild to moderatemetabolicacidosis nd ketosismay occur Hypoglycemia, yper-ammnnemia ,nde leva t ionsl se rumransamrna lesreseennsomepatients.High concentrations f glutaric acid are usuallyfound n urine, blood, and CSF, -Hydroxyglutaricacid may alsobe present rn the urine. This frnding drfferentiatesglutaricaciduria ype from rype I. In glutaricaciduria ype I, 2-hydrox-yglutaric rather han 3-hydroxyglutaricacid s elevated.lasmaamino acrdconcentrations re usuallvwithin normal hmrts,Lab-oratory findirrgsmay be unremarkable etween t tacks.Severelyaffected children wrthout elutaric aciduria have also beenreported. n someof thesepiriencs, he glutaric acid s elevatedonly in tbe spinal fluid. In any child with progressive ystoniaand dyskinesia, ctivity of the enzymeglutaryl CoA dehydroge-nase houldbemeasuredn leukocytes r cultured ibroblasts.CTand MRI of che brain revealmacrocephaiy, ilated lateral ven-rricles, cortical atrophy', fibrosis, and atrophy of striatum(putamenand caudate).
Treatnent.A lou-protein diet (especially diet restricted nlysine and trvptophan) and high doses 200-300mg/24hr) ofriboflavin (che oenzymeor glutaryl CoA dehydrogenase)nd L-carnitine (50-100mg/kgl24 u orally) produce a dramatic
1 r-N-acetvFlvsine
I s "I ln,/
o
Glutamicacrc
cr-Aminoadipicactd
6-Semialdehyde
Pipecolicacidemialx-Aminoadipic
acro
t'igurc 8s-1s- Parhwavs n che netabolismo{ lysrne ErzFnes: (1) lysine keroslutarate eductase, 2) sacchrropinedehvdrogenase,3) d-aminoad,pic acjd rraftrase, (4) a-ketoadipic acid dehydrogenase,s) glutaryl CoA dehvdrogenase,6) o-anlnoadipic semialdehyde xjdase.
decrease n the levels of giutaric acid in body fluids, but the clical effect has been variable. The addrtion of a GABA anathaclofen)and valproic acid to the therapeuric egimenprodu
improvement in some affected children,
The condition is inherited as an autosomal recessive rait. Tprevalence is not known. The condrtion is more prevalentSweden and among the Old Order Amish population in
United States. The gene rs located on chromosome 19p13.2 amany disease-causiflgmutations have been reported in drfferfamilres, A single mutat:on (A421V) accounts for all the patie
from Lancaster County Old Order Amish.Prenacal diagnosis may be accomplished by demonstrat
rncreasedconcentrations of glucaric acid in amniotic fluid, by assay of the enzyme activit], in amniocytes or chorionic vsamples, or by idencification of the mutant gene.
tYslNURtc RoTEINNTotEBANGEtAMtUAtPR0TE|NNTotAITCE).his rare autosomal ecessive isorder s due to a defin the transportof the cationicamino acids ysrne, rnirhine,aarginine in both kidneys and intestine.Unlike patients rvcystinuria,urinarl. excrelion of cystine s not increasedn lhpatients.About half ofthe reported ases avebeen rom Finlawhererheprevalence as beenestimatedo be 1/60,000.
Clinical manifestationsonsistof refusal o feed.nausea. vs ion upro te in ,omi r ing .ndmi ldd ia r rhea .h ichmay esufailure to thrive, wastrng, and hypotonra. Breasr-fed nfausually remain asymptomaticuntil shonly after u,'eaning.may be due to the low protein contentof breastmrlk. Episoof hyperammonemia ay occur after ngestionof a high-protdiet. Mild to moderate epatosplenomegaly',steoporosis, pabrirtle hair, thin extremicies ith moderate entripetaladiposand growth tetardationare commonphysical rndings n patie

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 74/177
whose condition has remained undiagnosed. Mental development
patients and may cause death-Laboratory findings may reveal hyperammonemi and an ele-
vated concentration of urinary orotic acid, rrvhich evelop only
afcer protein feeding- Fasting blood ammonia and urinary olotic
acid excretion ar e usually normal. Plasma concentlations of
l ys ine . rg in rne , nd o rn i t h ineare ucua l l vm r ld lydec reased .ur
urinary lerels oi rheseamino 66i615.specralll vsine,ar e S,reatlrincreased. The mechanism producing hvperammonemia rs not
clear All enzymes of the urea cycle are normal. Hyperammone
mia ma-v be related co a disturbance of the urea cycle secondary
to a deEciency of arginine and ornithrne. In patjents rvitb c1'strn-
uria rvho also have defects in the transporc of l,vsine,arginine,
and ornirhine in both intestine and kidneys hyperammonemia is
not observed. Piasma concentrations of alanine, gJutomine,
serine, glycine, proline, and citrulLne are usually increased.These
abnormaliciesmay be secondary o hyperammonemia nd areno t
specific to thrs disorder.
N{ild anemia and increasedserum levelsof ferritin, laccic deh,v-
ated from hyperammonemia due to urea cvcle defects (see
Chapcer 85,11), especrally n heteroz,vgousemaleswith OTC
de6ciency'. ncreased unnary excretion of l,vsrne,ornithrne, and
arginine and elevated blood levels of cicrulline are not seen in
mented with citrulline (3-8 g/day) has produced biochernrcal and
the management of acute pulmonary conplications
The gene for l,vsinuricprotein incolerance SLCTAT) is mapped
to chromosome 14q11.2 and severaldisease-causing utations
have been identified in different families, Pregnancies n affected
morhers har.e been complicared by anemia, thrombocytopenia,
toxemia, and bleeding, but offspring have been normal.
85,14. ASPABTICgD (CAI,IAVANTSEASE}
Reuhen .Matalon
N-acet,vlasparricacid, a derivacive of aspartic acrd, is synthesized
tn the brain ard is found In a high concentrarion, similar to that
of glulamic acid. Its function is unknown, but excessiveamounts
of N-acetylaspartic acid rn urine and deficiency of the enzyme
aspartoacylase !hat cleaves he N-acetyl group from N-acetylas-
partic acid are associaled rvith Canavan drsease.
Chroler95 . Doloctsn Mctabolism l AminoAcids r
CANAVANDISEASE.Canavan drsease,an autosomal recessrv
order characterized by spongy degeneration of the whire ma
of the brain, leads to a severe orm of leukodystroph;'. lt rs m
prevalent in individuals ofAshkenazi Jewish descent han in o
ethnlc groups.
Etiology snd Palhology,The deficrency of the enzyme aspar
cylase leads to the accumulation of N-acety lasparric acid in
brain, especially in white marter, and massive urinary excre
of this compound. Excessiveamounts of N-acetvlaspartic acid
also present n the blood and CSF.There is striking vacuoliza
and astrocytic srvelling in white matter. Electron microscreveals distorted mitochondria. As the diseaseprogresses! he
tricles enlarge, ow'ing to cerebral acrophy.ClinicalManiteslations. he severityof Canavandisease o
a $'ide spectrum. Infants Lrsuallyappear normal at birth and
not manifest symptoms of the drseaseuntil 3-6 mo of age, u
they develop progressive macrocephaly, severe hypolonia)
persistenr head lag. As rhe infant grows older, dela)'ed mil€sto
become evrdent. These children become hyperreflexic and hy
tonrc; joinr sriffness mav be encountered. As they grow o
seizures and opric atrophy develop, t-eeding difficulti es, p
weighc gain, and gastroesophageal eflux may occur in the 1
of life; swallowing deteriorates in the 2nd and 3rd yr of life,
nasogastric feeding or permanen! gastrostomy may be requi
lVIost parrents die i[ the lst decade of life; rvith irnproved nur
care, they may survive through the 2nd decade.AtypicalCanavan isease.Somepaoenrswith Canavandis
ma!,have a mild allele (Y288C), a substitution of ryrosine
cysteine or (R71H) substitution, or arginrne u'ith histidine. S
patienrs have very mild delays and are no! suspected of ha
Canavan disease.Th e excretion of N-acecvlasparticaci
increa.ed moderately in urine, whrch rarses hi que.rru
Canavan disease and the MRI of the brain shorvs a diffe
image,no r globalwhite matter drsease, ut increased rgnal n
sities with che basal ganglia, rvhich may be confused with rn
chondnal drsease.Diagnosis. CT scans and MRI reveal diffuse white ma
degeneratron, primarily in the cerebral hemispheres, with
involvement in the cerebellum and brainstem (Frg. 85-
Repeated evaluations may be required. N1RS performed at
time N1RI is done can show the hrgh peak of N acetylaspacid, suggesting Canavan disease. The differential diagnosi
Canavan disease should include Alexander disease, rvhic
anorher leukodystrophy wirh macrocephal,v. Progressio
usua)ly slorv ra Alerarder disease; hypotonia is not as
nounced as it is in Canavan disease.Brain biopsy shows spo
degeneration of the myelin livers, astrocytic swelling, and e
gared mirochondria. Defi^rtrve diagnosis can be establshed
6nding elevacedamounrs of N-acetylaspartic acid in the unn
blood. A deliciency of aspartoacyclasecan be found in cultu
skin flbroblasts. The biochemrcal method is the preferred ch
for diagnosis. Levels of N-acetylasparcic acid in normal urine
only trace amounts (24 i 16 pmol/mmol crealinine), r,|.here
patients with Canavan disease hey are in the range of 1,44
873 pmol/mmol creatinin€. High levels of N-acetylaspartic
in plasma,CSF,and brain lissuecan also be derected. he airy of aspartoacylase n the libroblasrs of obligate carriers is a
half or lessof the acrivitv found rn normal individuals,The gene for asparroacvlase s cloned, and mutations lea
ro Lana\an disease re idenrrf ied. here are tu.o mutarion\
dominant in che Ashkenazi Jewish population. The 1st is
amino acid substituoon (E285A) in which glutamrc acid is
sriruted to alanine, This muration i s che most frequenr
eflcompasses 3% of 10 0 mutanr allelesexamined n Ashke
.lewish parients. The second common murarion is a change f
tyrosine ro a nonsensemutation, ieadi[g to a srop in the co
sequence Y231X). This mutatron accounts or 13% of the
mutant alleles, n the non-Jewish population, more diverse m
cions have been observed; the two mutarions common in Je

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 75/177
564 PART r M€tabolic iseares
Fieure 85-16. Axial T werghted MRI of a 2 yr old patienr with Canavan
disease. xrensivehicl iening f the uhi te maner s seen.
peopleare rare. A different mutation (A305E), substitution ofalanine or glutamicacid,accounts or 40/ of 62 mutant allelesin non-Jewish atients.Wirh the diagnosis f Canavandisease,tis mportant o obraina molecular iagnosis ecausehiswill leadto accurate ounseling nd prenatal or the family, f the muta-
tions are not known,prenatal
diagnosis elieson the evelof N-
acetylaspartic cid in the amniotic fluid. In AshkenaziJewishpatients, he carrier frequency an be as high as 1:36, which isclose o that of Tay-Sachs isease. shkenazi ewish ndividualsmay need o be screenedor Canavandisease,
Treatment nd Prevention. o specific reatment s available.Feedingproblemsand seizures hould be fieated on an individ-ual basis.Geneticcounseling, arrier testing!and prenataldiag-nosisare the only methodsof prevention. njection of liposomeswith the human aspartoacyclase enewas introduced to the ven-tdcles of two children with Canavandisease, he resultsof thisgen€ herapy haveno! beenencouragrng.
General
Crombez E, Koch R, Cederbaum S: Pitfalls in newborn screeniq. I Pediatr
2005;147:r19-120.
Holtzman NA: Expanding newborn screenng. /A MA 2003;290:26O6-2608.
McKusick VA: Online Mendelian lnhentance in Man (OMIM), Available ar
www.ncbi.nlm.nih,gov/entrez/qu€ryfcg?db-omim
Morioka D, KasaharaM, Takada Y, et al: Living donor liver transplantation
for pediacricpadentswjth inheritablemerabolic disodlrs. Am I Tlansplant
2QO5;1r:27 417 63
Na|owicz M: Newborn screening-Setting evidence-basedolrcy for prorec-
rron. N Engl l Med 2005;353:857-870.
SchulzA, Lindner M, Kohlmuller D, et al: Expanded newborn screening or
inbom efiors of metaboLism y electrospray omzation-tanden mass spectrom€try: Results, outcome, and impltcarions. Pediatrics 2OO3;l1l
1399-1406.
Scriver CR, BeaudecAI. Valle D, et al (eds): The Metabolic and Molec
Basisof Inheited Disellse,8th €d. New York, McGraw-Hill, 2001.
\0aisbrenSE, Albers S, Amato S, et al: Effec of expandednenborn scree
for biomedical genetic disorders on ch d outcomes and parental st
IAM A 2003:290:25 64-2 572.
Phenylalanine
Blau N, Koch R, Matrlon R, et al: New de"etopment in phenylkero
and tetrahydrobiopr€rin rescarch.Mol Genzt Mektb (S"ppl 1) 2C)01-156.
Blau N, SeriverCr N€r,r' pproaches o trearPKUt l{ow I arc wel Mol G
Merab 2O04i81:1-2.
Crone Mr, van SpronsenFJ, Oudshoom K, et al: Behavioural ac.ors rel
to m€tabolic control in parientswith phenylkerofltia. I lnherb Metab
2O05;28$27437.
Desviat Lr, PerezB, Belanger-Quintan,A, et al: Tetrahydrobiopt€r;nres
siveness:Resulrsof the BH4 loading tesr n 31 SpanishPKU patienrs
correlationwith their genc't:fie.Mol GefletMetab 2004j83:157-152.
Gassio R, FusteE, Lopez-SalaA, er al: khool performancern early and
trnuously created henylke.ontlrrr..Pediatr Neurol 2005;33:267 27 1.
Koch Rr Maternal phenylketonuria:The imporcanceof early control du
pregnancy.Arch Dts Ch'ld 2005;901114-115.
Koch R, de )a Cruz F, Az€n CG, €t al: The maternal phenylketonuriaco
orative study: New dev€lopmenrs nd the need or new strat€gies. edid
2003;1 2(Suppl):1513-1584.kvy HL, GuJdbergB Guttler F, et al: Congenital hearr
phenylkeronuria: Repon {rorn the matemal PKUPediafi Re 2001 49 636-4 42.
Matrlon R, Koch R, Michals-Matalon K, er al: Biopterin responsiveph
lalaninehydroxylasedefr.\ency.Cenet Med 2004;627-32.
Munrau AC, RoschingerW, Habich M, er al: Tetrahydrobiopterinas an anrtiv€ treatm€nt for mild phenylkeronuria. N Eflgl J2002;347:2122-2132.
Segwa M, Nomura I NrshiyamaN: Autosomal domhant guanosine ripphate cyclohydrolase I deficiency (Segrwa disease). Ann Ne
2003;54:S32-545.
WaisbrenSE, Hanley W Lera HL, et al: Outcome at age 4 years n o{fsp
of women wrth maternal phenylk€tonuna:The maternal PKU collabora
study. JAMA 20OO;283:756-762.
Waher JH, $ghite FJ, Hall SK, et al: How practical are recommendarion
dietary control in phenylketon[ia? La/'.et 2002;350:55-57.
Tyrosine
Cerone R, FantasiaAR, CastellanoE, et al: Pr€gnancyand tyrosinaemia
. I Inherit Metab DE 2002i5:317-318.
Crone J, Mostinger D, Bodamer OA, er al: Reversibiliryof ci-rrhotic ege
ative iver nodulesupon NTBC trearment n ! child with ryrosinaemia
l. Acta Paediatt 2003;92:625-628.
Dionisi-Vivi C, Hoffmann GF, Leuzzi V, et a| Tyrosine hydroxylasr deficie
with severe lmical course:Clinical and biochernical nvestigations nd omizarjon of therapy..l Pediitr 2000t136:560-562.
ELlaway CJ, Holrr}e E, Standing S, a al: Outcome of tyrosinaemia type l
lnherit Metdb Dis 200l;2+824-832,
Furukawa Y Updare on dopa-responsive ystonia: Locus hererogenerty
biochemicaf earures.Ad, Ne,rcl 20O4i94:127-138.
Hefd PK: Disorders of tyrosine catabolism"f
Mol Genet Me
2006;88:103-r06.
Mag€.a MJ, Cunawardena ND, Hahn SH, et al: Quantirative determina
of succinylacrion n dried blood spots or newborn screening f tyrosineqp< L J Mol Genet Metab 2006t88tr6-?1.
Macsar MS, SchwarrzTL, Hinkle D, er a| Tyrosinemia yp€ II: Nine cas
ocular signsand symprom$ Am I Opbthalmot 2001.t132:522-527.
Madan V Gupta U: Tyrosinaemia ype I with diftuse planrar keratode
And self-mutilation. Cli, E p Dermatol2006t3L154-56.
Moller LB, RomstadA, PaulsenM, et al: Pre-and postnataldiagnosisof t
sine hydroxylase defrcietrcy. renat Diagn 200 5t25 677-675.
Phornphutkul C,Introne !0J, PerryMB, et al: Natural history ofalkapronu
N Engl J Med 2002;347:2111-2121..
Russrll'Eggin I: Albinisfl, Ophthabnol Clin North Am 2001;14:533-546
Schiller A, Werers RA, Steenb€rgenGC, et al: Long-term course of L-d
responsiv€dystonia caused by tyrosine hydrorylase deliciency.Newol
20M;6J:1524-1526.TechakrtrirojC, Cunningham A, Hooper PF, et al: High protein dret mim
hypertyrosinemia in newhon infants. ! Pediatl 2o05t1461281-282.
disease n mate
collaboracive st

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 76/177
Tomita Y, Suzukj T: G€necics f pigmenca.y disorderc.Am I Med Cenet C
Se,nn Med Genet 2004;131C:75-81
Vrn SpronsenFJ, Bijleveld CM, van Maldegem B! wiiburs FA: Hepatocel
lular carcinoma in hereditary ryrosinemiacyPe desprre -(2 nitro-4-3 trr-
fluoromerhylbenzoyl)-1,3-cyclohexanedione treatment. I Pediatr
Gastrcentetol Nul'' 2005i40:90-93
Methionile
Carmet R, GreenR, RoesnblaftDS, Watkins D: UPdateon cobalamin, folate'
and homocysteine.Genericdiseases nd potymorphisms Hematologj Am
SocHema I Educ Program 2003;62-,37Larvson-Yue A, Levy HL: The use of betaine n the tr€atment of elevated
homocysteine.l Mol Csrlet Metab 2006;88:201)07
I ee SJ,Lee DH, Yoo H\v, er al: Idenri$carionand funcrional analvsisot cvs-
rarhionine beta synthasegenemutations n patienrswith homocvsrinuna J
H&m G enet 200 5 501648-6 5 4
Lerner- sJP,Tnone JC, PaweLek D, €i al: Identificationofthe Sene espon-
sible merhylrnalonicaciduria and homocysrinuria, rlc rvpe Nat Cenet
2006;38:93-100.
Morel CR Scotr,P, ChristensonE, et a| Prenataldiagnosis or severemedyl
en€tetrahydrofolate eductas€d€ficiencvby tinkage anatvsisand enzvmaoc
^ss^y.Mol Genet Metab 2005;85:115-120.
SelzerRR, RosenbtattDS, Laxova R, Hogan K: A erseeffectof nitrous oxide
in a chitd with 5,10 methylenerertahydrofolate ductasedefciencv.NE@
J Med 2003;i49:45-50
SibanrS, kclerc D, rWeisbergIS, er atr Characrenzationof mulations i' severe
nerhylenetetrahydrofolate educr:se deficiency reveals an FAD r€sponsive
m:utation.Hun MBt 2003;21:509-520Topaloglu AK, SansaricqC, SnydermanSE: nfluenceof metaboliccontro
growth in homocystinuria due ro cystarhionine p-synrhase deficie
Pediafi Res200 1 49:7 96-7 9 8
Ueland PM, Holm, PI, Hustad S: B€ta,n€:A key modutacor of one-carbon
metaboLismand homocysreine status Cli, Cb€m Lab Med 2005;43:
1069-L075.
VilasecaMA, CuarceroML, Marrinez de SalinasM, et aJ:Two successful reg-
nancies n pyridoine-nonresponsive hornocysrinuria. f lzDerit Metub Dis
2004l'27:77 -777 .
tarhionine beta-synrhase CBS) defici€ncy Am I Med Cenet 2002|.108:
s7-63.
tathionine beta-st'nthase eficiency. Inheit Metab Dis 200724:437447-
Cysteine/Cystine, Tryptophan
Karakas E, Wilson HL, Graf TN, et al: Structural nsights nro suifire oxidase
defrd.en.y. Biol Chen 2005;280:lJ 505-3 35 5
Kleta R, B€rnardini I, Arcos Burgos M, et al: Mol€cular basisof the Harrnup
dtLsordetMol Genet Metab 20O5;84:225.
Leirnkuhler S, CharcossetM,latour P,et al: Ten noveLmurations D he molvb
denum co{actor genesMOCSI and -MOCS2 and rn"nro
characterizatron
of a MOCS2 mutation that abolishes he binding ablhry of molybdopterin
synrha 'e .Hazz Gp4pt200i ; l l ' : t65-570
Tan V/H, Eichler FS, Hoda S, et al: lsolated suJfire xidase deficiency:A case
report with a novel mutation and revi€w of rhe hrcrarufe. Pediat/lcs
2O0 ;llt5:7 57 7 6r i
Valine, Leucine, Isoleucine, and Relared Organic Acidemias
Acquaviva C, Benorst R Call€baur , et al: N219Y, a neiv trequ€nrmDraoon
among zal forms of merhylmalonicacidernia n Caucasjanpatienrs ElrJ
Hu,fl Ceflet 2007,,577-582.
Anikster Y, Klera R, ShaasA, et al: Type II 3-methylglutaconicaciduria(optic
atrophy pJussyndrome, or Cosceffopric arrophy st'ndrome): denri6carion
of the OPAI geneand ns founder m'rrarion n Iraq; Jews.Am J Htm Genet
200169:12 L8-1214
BarshopBA, Khanna A, Domino heparic ransplantarion n maPles)'fuF urine
d\sease.N Engl J Med 2005;353:2410-2411
Barrh PG, Valianpour F, Bowen VM, et at: X'linked cardioskeletalmyopathy
and neurropenia (Barth syndrorne): An update. An I Med Cenel
20Q4;126 :349-i 54.
Baumgatner MR' Molecular nechanism of dornrnant expression in 3-
merhylcroronyl CoA carboxatase deEcrency. f Inhe t Metab Dis 2005;
28:301-309-
ChEptsr85 r Delocls ir Metabolism ot ArninoAcids r
Bodner LeideckerA, WendelU, SaudubrayJM, et al: Branchedchain L-a
acid metabolism n ctassicalmaplesyrup urine disease lter orthotopic
tJanspl^nj3tiotr. I l,'hetn Metab Dis 2000;23:805-818
2002;140:261 263.
Danta' MF, Suormala , RandulphA, er a l: I Methylcrotonyl-CoA ar
lase deficiency:Mutation analysis n 28 probands, 9 svmproDadc an
derectedby newborn screeninP,Hum Mutut 2005;261164.
Desviat LR, Perez B, Perez-CerdaC, et al: Propionic acidemia: Muta
updareand tunctional and srrucruraleflectsofthe varianr alleles Mol G
Metab 2004.8328-37 .D'Osualdo A. Picco P. Caroli F. er al, MVK murarions and associacedt
fearures n kalian patients affecredrvirh aucoinflammatorydisorder
recurrent ever. E,r.l HLln Cenet 20OSi1Jt3'14-32O.
Lncenauer , vock leyI, Wi l lard l. €t al : A (ommon murar ion s a 'srx
witb a mild, porennally asymptomaticphenoryp€ n patientswrth iso"
acidemia diagnosed by newborn scr€enine. A,fl J Hum G
2O04;7 :11i6-1't47.
I -ukao scr iverCR, Kondo N. er l :The L l inrcal henot.pe nd outco
mirochondriai acetoacetyl-CoA hiolax deficienc). beta ketothiolaseo
deficiency) n 25 enzymaricallyprov€d and muBrion-de6ned patients
GenetMetrb 200t i72tL09-lr4Harding CO, Pillers DA, SreinerRD, et al: Porendal for misdiagnosisd
lack of combined rnerhytmalonicaciduria/hyperhomocystein€miac6
the neor, rc.I Petitatol 2003 23:384-3 86.
Hoffrnann B, Hetbling C, SchadewaldtP, WendelU: Impact of longrtu
plasma leucine levels on rhe intellectuat ourcome in patjents w,th c
MSUD. Pedt t/ Res 2006t59:17-20.Houren5M. Frenkel , R' jker\ G . et dl : Temperarureependencef m
mevalonate inase activq as a parhogenjc acror n hyper{gD and pe
fever syndrome.Hzz Mol Geflet 2002t2213115-3174.
HymesJ, StanleyCM, V/olfB: Mutarion in BTD causinsbiotinidasedefic
Hutk Mutat 200111*37 5-3131.
Kavser M: Disord€rsofk€tone production and udliz tion. J Mol GenetM
1006;87:281-283
KoeberlDD, Millington DS, Smnh r0rE,er al: Evaluation of 3-merhylcro
CoA carboxylasedeficiency etectedby !andemmassspectrometrynew
sqernhg. J lflherit Metab Dis 200326:25-35.
Lerner-EllisJB Gradinger AB, Watkins D, er al: Mutation and bioche
analysisofpatients beLonging o th€ trl B complementarion lassofvit
Br:-dependent methvlmalonrc aciduria. Mol Genet Metab 200
219,225.
Lonso N, Fukao ! Slngh R, er al: SuccinyfcoA:3 kecoacid trans
ISCOT) de6ciency n a new parienthomozysous or an R217X mumd
Inheit Metnb Dis 2004;27:691492.
Mardach R, Verity MA, CederbaDmSD: Clinical, parhological,and bro
icai studies n a patienr wirh prcpionic acidemiaand fatal cardiomyop
Mol Cenet Metab 2005:85:286 290.
Morel CR Scotr P, ChJistensen , er al: Prenaral dragnosis or severem
eneteuahydrofolate educrasedeficiencyby linkage analysisand enzy
assalJ. ol Cenet Metdb 2005;85:115-120.
tvlorel CF, watkins D, Scott B et al, Prenatal dragnosis or mechylrn
acidemia and inborn errors of vimmin B,r metabolism and transport
C enet Metzb 200S 86:1 60-171.
Morrone A, Malyag,a S, Donari MA, et al: ClinicalEndings and bloche
and rnolecular analysis of lour patienrs with holocarboxylase synt
deficiency. A,n I Med Genet 20r)2;lrr:70-78.
Morton DH, Stfauss KA, Robinson DL, er al: Diasnosis and creatm
maple syrup disease: study of 36 parienrs.Ped dtrics 2002t1o9:999-
Modinger D, Muhl A. SuormalaT, et el: Mol€cuLarcharacterizationand
ropsychological outcome of 21 patienrs wnh profound biorinidasciency derected by newborn screeningand lamily srudies. F.w J P2003;162:545-S49.
Nellis MM, ksinski A, Carlson M, er al: R€ladonship of causarivesmutations in maple syrup urine diseas€wirh rheir clinical expressio
Ge,et Me ab 2003 80:189-19S.
Prasad C, Nurko S, Borovov.l, Korson MS: The importance of gut m
in the metabolic control of propionic acidemia. ./ P
2004;144:532-.535.
Prietsch V Mayateper E, Krastel H, et aL Mevalonate kinase defic
Enlarging the cljnical and biochemical spectrum. Pediatics 2003
258,261.
Sass O, HofDann M, Skladal D, et al: Propionic acjdemia €visited:A
shop report. CIis Pedi4, (Phila) 2004;43:837-84J.
ValianpoDr 4lx/aners RJA, Overmars H, er at: Cardiolipin deficie
Xlinked cardioskeleral myoparhy and neutropenia (Barth synd

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 77/177
566 PABT r Metobolic iseases
MIM 302050):A stud,vn culturedskin fibroblasts. Pedia 2002;1411729-733.
VarvogliL, RepertoGLI, Waisbren E,et al: High ccgnirive urcomen anadolescent ith ,r'4r merh)'lmaloniccidenia.An J Med Ge et 20OQ\96 192-195.
Y/olfNI, Rahman ,Claycon I' Zschocke: Mjtochondrial luc-CoA sl,nrhase eliciency:dencificalionf trvo {urrherparjents arrfing ttro novelm[Janons..ur ] Pedidtr 003,162.2/-9-280.
\0organLC, NilesK, TironeJC, et aL The spectrum f murarionsn m rme vl'naloni. acidemiaand jdenrificationof a comnon Hispanic mut.tionand haplorype. Hrn Mutat 2006;2t-:3143.
Yoriluji T, Muroi J, Uematsu {, et al: Living relaredJiver ransplantation tbrneonatal-propionicacjdemia.I Pediatu2.000;13V572 574.
Glycine
Almeida LS, Verhoeven NM. Roos B, et atr Creatine and guanidinoacerate:
Diagnostic markers or inborn erro.s in creatinebiosynrhesis nd cransport.
Mal Genet lvletdb 2004;82:2 \ 4-21,9
Caldeira Araujo H, Smir U/, VerhoevenNi.f, et al: Guanidinoacerare nethyl-
uanslerasedeficiency dentified in adulrs and a child wifh mental retarda
tlon. A,t1 Med Cenet A 2005i133:122-127.
Cochat P, Nogeeria PCK, Mahmoud lVA, et al, Primarv hyperoxaluria
in jnfants: l!{edicoethical and economic issnes. Pediatr 1999;135:746-750.
Darnpue CJ: Molecular etiologr of primary hyperoxaluria rype 1: Ne\,!
directions or trearrnent.Am J Nephd 2005t25:303-3 t0.
Dinopoulos A, Varsubara Y, Kure S: Arypical vrriants of nonketoric hyper
gl_vcinemia. oI Ge,er Metab 2005t86:61-69.Hoover Fong JE, Shih S, Van Hove JL, et al: Natural hisrory of nonketotic
hyperglycinemian 6J pat ien.s. e,r/o/os]2004;53:1847-1853.
JamiesonNV European PHI TranspJantationStudy Group, A 20-vear expe-rienceof combined liver/kldnev transplantarion or primary hyperoxaluria
(PH1): The European PH1 transplanr regisrry experieDce984-2004. Am
I Nephrcl 2005i251282 289.
Mitliner DS: The prirnary hvperoxalurias:An algoflrhm for diagnosis,Arn /N eph c 2005 Zr l 5 4-1,60.
RosenbergEH, Atmeida LS. Kleefstra ! et al: High pr€valenceoI SLC6A8
deficiency in X linked mental retardarion. A,n I Han Genet
20O4;7 :97-10 5
SellnerL, Edkins E, Greed L, Lewis B: Derectionol mutations in the glycine
decarboxylasegene in prtients ivilh nonkerotic hvpergl-vcinaemja.,VIol
Cenet Metab 20Os184:767171.
StroinberserC, Bodairer OA, SrocklerJpsirosluS:Ctinical characteristics nd
diagnosric clues in inborn efrors of creatine metabolism.J Inhetu Merab
Dis 2O03;26:299-308.
Verhoven NIU, Salomons GS,Jakobs C: Laboratory diagnosisof defectsof
crearinebiosvnthesls nd uansport Clt Cbin Acta2005;361:1 9.
Serine
de Koring TJ, Klcmp LW Serlne-deficiency yndromes. Cutr Opin Nearcl
2004;171197 204.
de Konins TJ, Klomp LW! van Oppen AC, er at: Prenataland earl).postnatal(eatment in 3 phosphoglycerate ehydrogenase deficiency. Lracer
200413 4:2221)222.
PolLitcRJ. Sharard N.fJ:T.eatins rare inborn errors o{ metaboLism.Lrr.ef
2004i364:2158-2160
Proline
ForLino A, Lupi ,A.,Vaghi P, €t al: l.Iu|ation analysis of 6ve new parientsaffecred by prolidase deficiency: The lack of enzyme activir-v c.uses
necrosisLike cell death in culrured fibroblasts. Hum Cenet 2002,'l1ll
314-t22.
Lupi A, DeRrso A, Torre SD, et al: Characcerizationof new PEPD altele
causing prclidase denciency n r\r'o unrelated patientsi Natural-occufrent
mutations as a tool ro investigatestructure uncrion rclad'onship. Hum
Genet 2004;41500-506.
Gluramic Acid
Cordon N: Succinic sernialdehvdedehydrogenasedeficiency TSSADH) (4-
hydroxybutyric aciduria, gamma hydroxvbutyric a.ciavti^\ Eul I Paediatr
Neutul 1004;8:261J55.
HaberleJ, corg B, Rutsch R et al: Congennal glutamine deficiencywith gJu'
ramrnc ynrhetase utat ions.N EzAl l M?d 2005;353:1926-1933.
N'ledinaKauwe LK, Tobin AJ, DeMeirleir - et al: 4 AmLnobutyrare minorferase GABA fansarninaseldefrcienc\l.Inbetu Metdb Dis 1999224144
Njalsson R: Glutathione synrhetasedeficiency.Cell Mol Life Scz 20051939-194S.
Njalsson R, Ristoff E, CarlssonK, et al: Genowpe,enzymeactivirl'!glutrrh
level, and clinical phenotype n patienrs wirh gLutathionesyntherase.iet\cv.Hum Cenet 2005 r16384-389.
Pearl FL, Gibson KN{: Ciinical aspects f rhe disordersof GABA netaboin chrldren. Crzr Opm Newol 2004i171107-113.
Pearl PL, Cibson KN.I,Acosta MT, et al, Clinical spedrun of succinic saldehydedehydrogenase eiciencr. N'errolr;gy 2 0O3 0.74 73-7417.
Ristoff E, Larsson {: Oxidative stress n inborn errors of metabolism:kssIrom slutathione deiciercy. J Inheit Metnb Dis 200225:223-226
Wong CG, Bottislieri T, SneadOC III: GABA, samma-hydroxybur_vricand neurological disease.Afln Neurcl 2003\54s3-512.
Urea Cycle
Anadions G, Ierardi Curro L, Kaplan PB, et al: Ornithine transcarbamdeficiencl and pancreatnis I Pedia, 2001l'1381123-124.
Arvio P, Arvio N,l: Progressrve ature of aspartylglucosaminuria.Arta Pa
dtr 2002191255-257Brusilo\r' SW: Hlperamnonenic encephalopathl Medicifte (Bdhim
2002\811240 249 .
Cronbez EA, Cederbaun Slr: Hyperargininemia due to liver arginase dcienct. Mol Cenet Metal' 2005;84:2:13-251.
EnsenauerR. Tuchman M, El YoussefM. et al: I\'Ianagemenr nd ourcomneonatal-cnsetornithine transcarbamvlase eficiencyaollowing iver rra
planration ar 60 days of liIe. Mol Ceset Metdb 200J;84:363-355.Gropman AL, Ba6haw ML: Cognitive outcome in urea cvcLe isorders.
Genet Metab 2004 81 S 8-S62.
Habede J, Koch HC: Genericapproach to prenaral diagnosis n urea c
detec$. Prcnat Diagn 2004;24r378-383.
Honlen SP, McCouan TC, Goertzen TC, er al: Isolated hcparocyre raptantation rn an infant with cycle disorder. Pedia
200i;L1.L:1262 L267
Kaiser Kupfe. l!{I, Caruso RC, Valle D: Gvrare arrophy of the choroid
retira: Further experience 'irh long"term reduction of ornithine leve
children. Arrn Ophtbabnol 2002t120:146-153.
KaiseFKupfer vll, Caruso RC, Valle D, ReedCF: Use of an arginine-resrr
diet to slow progressionof visual oss n patientsrvith gyrateatrophv.A
Ol, hthd tuol 2004 229 82,-9 4.
Kleijer U1, Garrisen VH, Linnebank lvl, et al: Clinical, eDzynadc, and m
cular geneticcharacterizationof a biochemicatvariant type of arginino
cinic aciduria: Prenatal and postnataldjasnosjs n five unrelated arnilie
Inberir Metub Dts 2C02;25:49 -410.
Kofman SH, Kanaza{'a N, Abu-Ljbdeh B, et a): Hyperornirhinemia, hv
ammonemia, and homocitrullinuria syndrome r1th evidenceoi mitoch
drial dysfuncrion u€ o a novelSLC25A15 ORNT/)sene mutarion
Palest inianami ly./ rNel l rol cr2004;218:53 8.
t.rnnebankM, TschiedelE, H3berleJ, et al: Argininosuccinare asc (ASL)d
ciency: Murarion anal).sis n 27 patientsand a compLeted t.uctur€ of
human ASL gene H n Cenet 2002t171:350-3s9.
LfcBride KL, Llitler G, Carier S, er at: Developmental outcomeswith e
orthotopic liver uansplanration for inlants {.ith neonatal-onser rea c
defecrs nd a femalepatienc vith late onserorniihine rranscarbanylase
c;ency.Pedid r .s 2O0 I 74 e 23-e526.
Morioka D, Kasahara ,I, Takada Y, et al: Current rule oi 1i"er transpla
tion for the treatment of urea cvcle disorders:A review of che rrtrLdw
English lirerature and 1l cases ar Kyoto Universir): Lircr Tlan
2 0 0 5 ; 1 1 :3 3 2 - l 4 2 .
Nagasaka H, Komatsu H, Ohura T, et aL:Nitric oxrde syntheris n ornithtranscarbamvtase eiciency: Posslble nvotvement of lorv no svnthes
clinical manifestarionsof urea cycle defect. Pedidtr 2004\145:259 262
Nicolaides P, LiebschD, Dale N, er al: Neurological outcome of patienrsw
ornirhine carbamo,vlrransferaseeiciency. Arcb Dis Child 20018654-5
PickerJD, Puga AC, Lery HL, et al: Arginase deiiciency vith ledral neon
expression: Evidence for rhe glutamine hyporhess of cerebral edem
Pediatt 2003 r 42349-3 52.
Robininath T, Costello DJ, Lynch I et al: FataL resentationof o.nithine tr
scarbarnylase eficiency n a 52'vear-old man and farnily studies./ lnr
Metab Dt 2004i27:285 288.
SahekiT, Kobayashi K, Iijima M, er al: Metaboiic derangemenrsn deficie
of citrin, a ljver-typemitochondrial aspartare-glutamarearrier H"pdtol
2 0 0 5 ; 3 3 : 1 8 1 - 1 8 4 .
SahekiT, Kobayashi K, Iijima M, et al: Adutt onsec vpe II cnrulline'nia
idiopathic neonatalhepatitrs ausedby citrin deficiencv: nvoLvement f

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 78/177
asparraregtutamatecarrier for urea synthesisand maintenanceol rhe ur€a
year follo*-tp. I Inhent Metab Dts 20O4;27:787-196
ScagliaF, O'Brien WE, HenrvJ, er al: An integraredapproachrothe dia o-
sis and prospectivemanagementof parrial ornithine rranscarbanvlase fi-
ciency.Pedia*rcs Z0D2;109:150-152
Summar M, Tuchman M: Proceedings f a consensus onferenceor rhe man
ra l inuahepatic cholestasis ausedby citrin defrcjenc,v:ase epons from 15
Metab 2004i81 585-59L.
o'rccome. Pediatl 1997;131:44G-443.
Lysine
BjugstadKB, Goodman SI, FreedCR: Age at symptom anset predrctssever
ity of mocor impajrment and clinical outcome of glutaric aciduna tvpe I .f
Pedia l 200O\l37 681 6 86.
Kolker S, Rarnaekers I, ZschockeJ,er al, Acure encephalopathy espLte arlv
rherapy in a padenr wirh homozvgosny for E365K in the slutamyLcoen
zvmeA dehydrogenase ene.I Pediatu20O1t138:277279
PalacjnM, Bertran J, Chi aron J, ec al: Lysinuric Prorein ntolerance, vlech-
anismsof parhophysioloEy.Mol Genet Metab 2004;81 527-S37.
SperandeoMB Annunziara P, Ammendola V, er al: Lysinuric prorein intoleF
ance: Identification and functional analvsis oI mutations ot rhe SLC7A7
gene.Hum Mutat 2005;'25:410.
StraussKA: Cluraric aciduria rype 1: A cJinicjant vlew oI progress.Brarz
2005;128:697-699.
StraussKA, PuffenbergerEG, Robinson DL, Morton DH: Tvpe I gluraric
aciduria, pan 1: Natural hiscory of 77 p^tienrs An I Med Gnet C Semin
Med C enet 2003;121138-5 .
Aspartic Acid
Leane P.Janson CG, Bilianuk L, ec al: Asparroacylase ene transfer to rhe
mamnalan central nervous system wirh lherapeutic imPlications for
Canavan isease. ra Neurcl2o00t48' 27 38 .
N{ataton R, Mjchats K: Molecuiar basis of Canavandisease.E1i I Paedidtl
Neurol1998t2t69 76 .
l,latalon R, \{ichals-Matalon K: Spongydegeneratjonof rhe brain, Cana"an
disease, iochemicatand molecular indings frozt Bios.i 2000lj:301-311SurendranS, BamforrhFJ,Chan A, et al, Mitd elevationof N-acerylasparic acid
and macrocephaly:Diagnosricprobtem./ Clld N2nol 2003;18B09-812
Tacke U, Olbrich H, Sass O, et at: possibtegeneotype-phenotypeorrelatrons
in children wirh mild clinical course of Canavan dlte^se Neurcpedidtl'cs
2005;36:252-25i .
Topcu M, Erdem G, Saatsi , ec al: Clinical and masnericresonance masins
featuresof L 2 hydroxygluraric aciduria: Report of threecases n compari-
son with Canavan disease. Chil,1Neurol 1.996;11:373-377
Yalcinkaya 1,Benb; G, SalomonsGS,et al: Atypical MRI findinss tn Canavan
disease:A parienr wirh a mtld colrse. Neuropediarl;rr 2005;36:316-339
86.1 DTSoBDERSFMtrocHoNDRtALATTYclD
B-0xlomono Charles . Stanley ndMichael . Bennett
lvlitochondrial l-oxidationof faay acids s an essential nergy-producingpathrvay, t is a particularly mportanrpathwayduring
Chapt€r6 Defectsn MotobolismfLipids
prolongedperiodsof starvalron,and during periodsof reducaloric ntake due to gastrointestinalllnessor increased nexpenditureduring febrile illness.Under these conditronsbody switches rom using predominantlycarbohydrate odominanrlyacas csmajor uel.Facry cidsar ealso mporfuels or exercising keletalmuscle nd are he preferred ubsfor the heart. n these issues,actl' acidsare completelyoxidro carbon dioxide and water The end products of hepfatry acid oxidarion are the ketone bodiesp-hydroxybuc
an d These cannot be oxidized by che liver
serv€ as important fuels in peripheral tissues, particularlybrarn.
Genetic defects have been identified in nearly all of the kno
steps n the fatry acid oxidation pathway; all are recessively nh
ited (Table86-1).
Clinical manifestatiozs characterisncally involve lhe tiss
with a high p-oxidation flux including Iiver, skeletal, and card
mr:scle. The most common presentation is an acute episode
life+hreatening coma and hypoglycemia induced by a period
fasting due to defecrivehepatic ketogenesis.Other manifestat
include chronic cardiomyopathy and muscle weakness or e
cise-induced acute rhabdomyolysis. The fatty acid oxidat
defects can be asymptomatic during periods when rhere is
fasring scress.Acutely presenrrng drseasemay be misdiagnose
Reve syndrome or, if fatal, as sudden unexpected infant de
Facty acid oxrdation disorders are easily overlooked becauseonly specific clue ro the diagnosis may be the frnding of in
propriately low concentrations of urinary ketones in an in
who has hypoglycemia. Genetic defects in ketone body util
uon may be overlooked because kecosis s an expected find
with fasting hypoglycemia, ln some circumstances, clinrcal m
rfestations appear to ar ise from toxic effects of fatty acid rneta
lites rather than simply rnadequate energy production. Th
include disorders (LCHAD, CPT-IA, SCAD, TFP; see larer
which the presence of an af fected fetus (homozygous) incre
rhe risk of a life-threatening rllness n che helerozygote mot
resultrng in acute fatty liver of pregnancy or preeclampsia rHELLP (hemolysis, elevated liver enzymes, low platelets)
drome. Malformations of the brain and kidne;rs have b
described in severe electron rransfer flavoprotein (ETF),
dehydrogenase (ETF-DH), and carnitine palmitoyltransferas(CPT-ll) deficiencres har might reflect ir utero toxiciry of f
acid metabolites. Progressive retinal degeneration arrd chrprogressive liver drseasehave been identifred in LCHAD
ciency. Newborn screening programs using ta[dem mass s
rromerry (MS/MS) detect characterisric acylcarnicines seemany of these disorders and permir presymptomatic diagnScreeningprograms have provided evidence thar all the fatry
oxidation disorders combined are among the mos! comminborn errors of metabolism.
Figures 85 1 and 86 2 outline the steps nvolved in the ox
tion of a rypical long-charn fatty acrd. In the carnitine cycle,Iaclds are transported across the barrier of the rnner mitochon
ial membrane as acylcarnrtine esters. !(Iithin che mitochond
successive urns of the four-srep p oxidation cycle convert
coenzr,nteA (CoA)-activated fatty acid to acety'lCoA units. to three different chain length specific soenzymes are neede
each of these p-oxidation steps to accommodate the differ
sized farty acyl CoA species. The electron r ransfer path
carrres electrons generated in the 1st P-oxrdation step (
CoA dehydrogenase) to the ele.trorl ttufispol t .hdin for ad
sine triphosphare (ATP) produccion,while electronsgene
from che third step (3-hvdroxyacyl CoA dehvdrogenase) e
the respitatetry chain ac the level of complex 1. Most of
aceryl CoA generated from hepatic p-oxidation flows throthe pathway of ketogenesis to form p-hvdroxybutyrare
acetoacelale.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 79/177
568 PAnTX Melabolic iseases
EI{IYMETFIOTNfl GINE
airllinelnnsporter AJM
Longlra ar,vcioanrpofrer {Irl6lam r?p,]lroylttilil.rase GL-i
ftIIII(ATPHENOTYPT
[a-iion)'op,rtlry,kr ehl i '0pdth]r,ver ease,udceneafiendo(adiaFbr0easl l ]5s, ln1; t ,ndl lB(r ren inqdiaqn05rrepnted
Fare,aru '€, /erfaluainrhldhoodrequrrngveri ran5platal icI
Lverf i re.slclpiavopalhIrenaubulopathy.andsuddeldedthenatalandNBsoeenlqCraqn05se|orted,rnaterndlre?tampsa,H[iLP5ynd'0me;llocalon
des(nbedn fuhpatcnlJ
[rrcni( o-cr55r./everrr,9,p€r5sreft'lfr, iipertrophcrd myopathy
idfyafd;te rnsalpes ,r?r ure, i(epta paihrrdi0noparhit
al l( riharqes,NErceflg aEnoi53oled
funEn o eyer€rese1tdtr0n,0 nc de n(ephaiopdthic5€aierpr0qftsslve
my0pdthy.Brpenrnqragnt!po5se,male'narl]ecampsa,HL:LPsyncrofie
a5so03:1 8ftb,od fgwrdt,ent5
Hypo!i,Gnia,ep,rtencephaE h,; rddeneathBscftninqaqnosircr5€matara reeCimpria,IEL5ynlmme550ridt0nesc,ibedarely
D dleda icmy0patrrt,rd)thnrs. ypogefiia,ano ppau.erlogrs
Ldte-on5et,5tr5sduapd'habdomyoy5i5,eps0dirn]yopaihy.Prena:rndNB5CreeqlqdBqno!i ril5 ie
Nonctot(;st 9hlprq/(enr ,conqeFalanomas,m erorm5f verd ase,GdiornpFthlanck. t, nvopdtlly
\onkeloti(altr.aypoql)rem, on-cenrultonal 5. erdisea5e,(;rdmyopath\1afdsiprtaly0oethi lso eic,ibed
fu n! ypog.,/(em, orgeniralrunas. vEdiseasqard myopatl.y,ndkelera
myopallry6o es(red|]/Dq emia,yper5, nenidadomyopathtllyopaihy.BsftenlqC cnol
po55ibhl{B ftrnin! driqncirs5rbh,maternalrelanF6 ,HEL[)indfo1le,dnc,\F.P
arso(iirn de5dbedrcquen'
9eve.erard,r(andlkeeta.n)opafry,hypoglycema,a(d05s,hype.N|1, ,suddendeaih,
eelrtediveren4,me5,relcpatliy.l\,1dterftree(ldmpj, ]ELLPyrdrome,ard
neuroFlhyrdeary edtiaE0nserre5enrsirhm/opath/iatemalpredampsia,HIii-Plfdr0me5s0c],rtonLrent
lr yone 6tent6cxbed,ypolon4 de newbom,may ererekeetalmyotathl
dfd:e5pctorya ur€ ]/poqi)tefirL]re
:lypcket0sirnd ftr-a iem , ;re r)€pithl
i yprket05i5nd ypoqrem, ardv y0p,rthl
TTBORATORYINOI}IGS
J irrrl ndiee 'nit e, offnaay;mitineiclqltr e,3ndqa a(d
lcrraior lreecdnLlinr,elelateiir et\tlrdhniiid,ncoi5ttefabnoma(ll(arneprcle
Normalortreern ,re,fpasmar.r,ir clcrD he
fpa5Fra,-:r
Ireediy ( j
acikam,t,nesNo |](ea5edat0ofacyo .ecm n,,,1rceaq
0N arnitine5
\ 0 1 a 0 + h F e r i r f e l d y l ] l r p " n t t . a t o 0 ' f J L r ' e o r q d
a(csdno ryql0ne5
itl)blani may E ogno5li.
irrr nrerabolrc leconlpensaflol f cxposcclo suf6ciert peli()d
iesring.
Lahoratory indin(Js.)uring acutc cpisocles, ypogl-vcc'mnsualll prcscnt. Plesma enrl urirrary <etone onceorrati()l linappropri:rrclv or.r {hyp6ks161ic ypoglycemia),Bccausc l
rclati\ .ch\ pokct{)nemii, here s l i t r le or no metaLrolic crde
Tcsrs of lircr iLrnctiou ruc atrnorrnal, widr cle\rt i(nrs oi l
enzymes AI l. , \S' l), eLcvatecl lood ernnronia,an d prolon
prothrombin 1Pf) arrl pertiei t lxornhoplastin i rcs LPTT).hiopsl, at f inles of rcufe il lness shows rnicrovcsjculr
mecrovcsicular cearosisLr eo trigl,vcerlde ccurnulatjon. )ur
fastingstrcss r dt t iurcsoi:rcLlte lltess,uriLrarv rganrcacid p6lcs by gl s chromirrogr.lphy/rnasspectronctlv shorv indp
priateLy rrv concenrrationsof keroncs an d clcvaccd cvel
rlrcdiuDr-chain licarLrrxl. l ic ci t ls ladipic, suberic. lr)d seb
ecicls)har dcri!e ironr microson.rl an.1perorrsonrrl onrcgl r
danon o{ iarrl acids l)Lasma nd rissuccorceDtfationsol t
. irr it inc ;rrc rcduced ) l j .50lzu l normal. and the liaction
total esrerif ierl irnrf ine is increased This pattcrn () t lccond
carnit ine dcficicncy s secn n alrnostall thc frtty acjd oxrdrt
clcfccts nd fcflccfscl)rr)peflt ion .crnrcn incrcascddcvlcrrni
lcvcls end frcc c ^rnirinc rlensport lt the plesrnanrenrbr:rrre
r i ic l l l r te\ccpfr(ns to fhis r-Lrle re rhe llesmd rncmbrlnc cr
Iinc rrdnsporfer (IPTIA .lrd p h-vdrox-v-13-urcthyLglur,r
iH\. iC C.oAl svrrth:rsc cficrencies.
(drftfl: fari oca5e(dmimea
itcy ran5feraje
5hcfr hin a!! aoA
dehlcroqera5e
lvhdiunrha dd l-!A
celyorogl:ndje
VerIofq ha aril[1rA
d?hydroqena5e
:Tfdehld'cEeidie'
flecttofranspcrt
I e(tftnrdn5port
fia,Jopr,iredShrri-(hdint'ltdrcrfdr)
ao,qeh)'d'casna!eLonq{hjir I qrror)"aql
[oAdehydrogefa5e
MitochondiianfuNrcnapr0le
-I)llg-(hdin-ketorcloA
rhicdse
2,4Di..noylol rect(raie
Hl\,161-oAsyntietise
Hlil6uA \tse
'A50lniu,nrq Fr. :dtnr;ne
G(i(Pt
!
'[AD
[)t(R1
HM6l5)iI16t
MU!
t/'i(AD
tLt-'tt1
tEli
SGID
(HAA
LIOI
|]Lttlh?mr!,ie.ukd jvfl$zimc5,0w,rte trNB, ewl}r|n
DEFECTSNTHE -0Xr0ATr0NYCTE
MEDIUM HAIN CYICOA EHYDBOGINASTMCAD)DETICIENCYM(lAD clcficicncrs hc rnostconrmon f fhe eftv acido\i( l,r-tiorr lisorclers.
lhe Jisorderhor,r 'sstrone,()un(ler ffecri nost
patieDf havc il l()rrl l\ ,vcsrcrn uropei] lr lncestrv. nd rhe major
irv of paricnrs are homozvgous krr a sing,le ()mrlon orisscrrsc
nutariol! en,,\-(i trensirion rt cDNA posirion 9il-5 har chalges
d lvs ine o g u taLn i r c r ( l r r r s rduc 29 iK l29 t - ) .
ClinicalManilestahDIs {f iecred pafrenr\usuall-v rcscnr n rhe
lsr 3 nro I rr of l i ic rlith episodes I acure rllness rrggcrcdby
prolong,c.l ,rsring asring onger rhan 12-16 hr. SigLrs nd slmprorns in.ludc vonlit i lrg end lerhargv,u'hrch rapicLlv rog,rcsso
co]rra or seizulesand cardiorcspirarorycollapsc.SuddcLt rex
pected ntaDf deathmal occur. I 'hc ivcr mav bc slightly enJlrged
rvirh far rleposit ion.Affacks are rare until rhc infant is beyorrcl
rhe st few monthsoi l i ic, presurnablyJue o nrore requenr ced-
irrgsar a younger:rge.Affeoed oider intinrs are ar higher risk of
il lnessas rhc,vbcgin nr iast thlough th e rright or ale erpose.l cr
iasting strrss rllrring an rntercurrenr hrlJhood iLlness. rcscLrra-
t ion in rhe irt clrvs of l ifc has bccn rcporrcd irr rrcq.borns hat
r,vcrc astcd lradrerrentlybelirre successhrl least ieerfil lg.Dieg-
nosisol Nl(-AD hls occasjonall-vccn r](rcrrrncnrcclrr prrcvir;LrsJv
hcllrhl tcerage antl acLulr ndivirluals. indrcirt ing t lrrr even
prrt icnrs vho h.rvcbeenasymptomatic u inaency rc strll .r t r isk

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 80/177
Chapter 6 . Delectsn Metabolism t Lipidsr
Carnitine
Plasmamemb
Lcaclrctrl:le
Outermitochondrialmembrane
brane bv carnitine/acylcarnitine randocase(TRANS). and rhen reconvcned nro , ton8 chain fany acvl CoA bv carnitine palmrtoyltransferase"Il CP
undergop-oxidarion. r;ery long chaln acvLCoA dehydrogenaseVLCAD/LCADi leads o tbe prodLrctionof (C15-l0i 2,3 eDoylCoA. Trifunctional protein
conrains rhe acriviries of enoyl CoA h,vdrarasehvdrataset,3 OH-hvdrox,vacyl CoA deh;rdrogenase3'OH-ACD), a|d P ketorhiolase(thiolase) Acervl
FADH. and N,iiDH are produced.Medium, and shorr-chain aay acrds C8-.+lcan enrer he Inrrochondnal matri\ independenrof rhe carnitine c-vcle.{ed
chain acyl Q,A dehvdrogenaseMCAD), short-chaiuacyl CoA dehydrosenrsc SC,{D). and shorr chain h,vdrcrv ac-vlCoA dehydrogenaseSCHAD) are req
Acecyl CoA can rhen enrer rhe Krebi tl CAI cycle. Electronsare rranspoir.d fro'1 FADti ro rhe respirak).y chain via the eJecrron rnnsfer lavoprore,n h-T
rhe eledron ugnsfer 0avoprorein dehydrogenaseET}--DH). NAI)H mrers rhe electron ra'rspo( chain through compLexL Acervl CoA can be converre
h_vdroxymerhylsltrrar_vlHMCI) CoA bv 0 hvdrcx,'-0 merhvlglutaryl CoA svnthase HNl(; GiA svnthase)and rhen r,be erone body acetoacerate -v hc a
of p hydrory'p-merhl lgluraryl CoA lvrse (HMG CoA lyase)
Dtagnoscicmarkers include increasedplasma Cro, Crl,o,an d
C101 acylcarnit ine specresan d increased urinary ylglycines
including hexanovl-, suberyl- an d 3-phenylpropio glvcines.Newborn screening programs using tandem mass spectrometry
can diagnosepresymptomatic nfants basedor the detectionoi
the abnormal acylcarnit ines n 6lter paper blood spots. n many
cases, he diagnosiscan be confirmed by f inding the common
A985G mutacion.A second ommon mutalion. T199C, has been
detecred n infants with characterisric cylcarnitrnesn nervborn
screening esrs. nterestingll, this allele has not been seen to
date in symptomatic N{CAD patients; ic may represent a miLd
mutatron.Treatrenl. Acure i llnesses should be promptl]' treated \r'ith
inrravenous luids containing 107" dexrrose o treat or prevent
hypoglycemra nd !o suppress ipolysisas rapidly as possible se eChapter 92). Chronic therapv consistsof avoiding fashng. This
usually equrres imply adjusting he dier to ensure hat over
fascingperiodsare limiced o <10-12 hr Restncting dietar
or treatment wilh carnit ine is controversial.The necessiactive theraDeutic ntervention for individuals u.ith the T1
murarion has not yet beenesrablished.
Prognosis. p to 257. of unrecognized atienrsmay die du
rheir ls r attack of i l lness.There is frequendv a histor,v f a
vious sihhngdearh due ro unrecognizedMC,{D deficrency.patienrsmay developpermanenrbrain injurv during an attaprofound hypoglvcemia.Th e prognosis for survivors rvit
brarn darnage is excellenr becausemuscle weakness or
diomyopathy does nor occur in MCAD deficiency, asting
ance mproveswith ageand the risksof rl lness ecreases.s m
as 509. of affected patienrs have never had an episode; there
testing of siblings of affected patienrs is imporrant to d
asvmDtomatrc familv members.
Long-charnree atty acid (C16'palmilate)
\

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 81/177
Palnitate
Iv
Cr5 CO-CoAI
l c P r - 1Y
C15-CO carnit ineInnerm i tochond r ia l I __^ .
; ; ;b ; ;__- . -__ _____I_TBANS_____
Cj5 CO-carnit ine
Jcer.,
CanitineCycle
ElecironTransfer
Electronransponcharn
C1s CO-CoA
ErF-DHrF rno .1 ^^^*- -- rao14
^""
R CH2-CH:CH-CO-CoA
I uyorataseV
R CH2-CHOH-CH-CO-CoA
NA D.js_oFt_nco
NADH+
R CH2-CHO-CH2-CO Co AncetvtCoA--y' Thiolaset
C1s-CO-CoA,J
AcetylCoA<--1
C11-CO-CoA
nceVrcoe --{
Ca-CO-CoAA
AcetylCoA<--1
C7-CO CoA
AcervlCoA<-4- v
Cs-CO CoAAcet/ Con+{
Ca-CO-CoA
Acetvl on.-{
AcetylCoA
13-OxidalionCycle
KetoneSynthesis
I HM G oA synthasef
Leucine->' -+ HydroxymethylglutaryloA
Iuuccooy"""i
Acetoacetate
i{
13-Hydroxybutyrate
570 I PABT r MetabolicDiscases
f igurc l t6-l Pnthwarof ni tochondriaL xrdarxrn f palmrratc, rvpical16
carkrn Longchain firly alid. Fnz)'lne sleps rt{rt1r tarnitinc palmrtorltr:ns
f t rase CPT] I anJ 2, carri tmc/ecl lce rninne. rnsbcase TRANSI. electron
trans{er lavop<,re (FTt ) , ETF deh}drogrnascET}-DHt. rcv l t :bA dehy
drcscDaseA(lD), enovl CoA hydratast hvdrarasc) .l -hydn)\-v cyJ Co A
clehvdrogenasei OH ACD), p-kctorhiolasethLolase),P h_vdrox l methl l '
glutarrl CoA iH\4c CoA) syntlase, and lvase.
VEFY IONG CHAIN ACYI. COA DEHYDROGENASEVI"CAD)OCIENCYVLCAD deficiencyu'as olginally termed LCAD dciency be{ore rhe existence of the inncl mirochondmembranebound VLCAD lvas knorvn.,A.ll paticnts prevro
d i . rgnoseJ. hav ing ( \D , l r6 . ien . ' hav . \ ' L t \D enzvmccienc,v.No patient s with isolated LCAD dcliciency have bdescribed nd the rolc o1 LCAD i human fattv acid oxidariou rknown . P i t re r r t ' , t r rh r l LAD r lehc ienc t r r u .uc l l r rnseverely afiecced than rhose with MCAD dcficiencl', prcsenearlier n infanc]'- nd having more chromc problems virh mu
,,r;caknessr episodes f musclepain and rhabdomyolysis.Cdromyoparhymay'bepresentdurmg acuteattacksassociatedfasting. The left vencricle may bc hypertrophic or dilatedshow poor contractility on echocardiograph,v.Suddenunexpecdeath has occurred in severalpatients, b$r most lvho surviledinitial eprsodeshorved improvement, including normalizatroncardiac unctjon. Other ph1'srcal nd routine laboratory learare similar to those of -\.ICAD deficiency, ncluding secondary cnirine deliciency'- The urinary' organic acid pro6le shownonkctotic dicarboxylic aciduria. Increased levels of (
dicarboxylic acrdsmay be noted in the urine. Diagnosisma,suggested ,v an abnormal acylcarnit ineprofile n' ith plasma
blood spor C1111a6ac-vlcarnicinepecies, ut chespecif icdiag
sis requires assay of enz,vmeactivities of VLCAD in culrufrbroblastsor direct mutarional analysis of thc VLCAD ge
Treatment is based primarily on avoidance of fasts for >112 hr. ContinuousrntrallastrLceeding s usefu) n somepatie
SHORT_CHAINCY TCO AOEHYDSOGENASESCAD} EFICIEN
small number of paticncs vith tu.o clear null mutaoons in
SCAD gene have been described u.ith variable phenor,vpe.Mpaticnts classifredas being SCAD deficienr have been shor,vhave polymorphic DNA changes rn the SCAD gene and hresidual activity. he ru<r common polymorphisms are Gl8and R147Vi Currenth, i t is believed hat rhcs eare susceptibchanges, rvhich require a 2nd, as vet unknor-r.rt,genetic mutat
!o express a clinical phenotype. These indrviduals do nor pres
rvith hvpoketoric hypoglycemia. Skeleral myoparh,v secms o p
dominate. br:r a consistent clinical ghenot,vpe has not hccn id
ri6ed. Somepatientshave severemetabolic acidosis.Ncurolo
signs are present in most patientsr although mildly aftccted in
vidualsma v be asympcomatic. iagnosis s indicatedby eleva
levelsof butyr,vlcarnirine n blood spotsor plasma and increa
excrerioi of urinary erh,vlmalonic cid and butvrvlglycine.Thmetabolic abnormalit iesare most pronounced in paoents w
null murationsan d variably presenrn parrenrs 'ho are homogous or th e polymorphisns. Confirmacionof dragnosis equ
mutacion analysls.Some of the clinical featuressuggesc toxity s,vndrome. erhapsowing to accumulationof short chain fa
acid merabolites.One reported pariencha d nornal ketogcn
irnplving chat there is no irnpairmenrof longer chain farrv a
oxidation.Treatment is lirnitarion of fastrng strcss and dierary far.
IONG_CHAIN -HYDROXYACYTOA OEHYDROGENASETCHMITOCHONDRIATRIFUNCTIONAT ROTEIN TTP} DEFICIE
LCHAD deficienc,v s the second most common of the fatty a
oxidanon disorders.The LCHAD enzyme s part of a mitoch
drial crifuncrionalprorein (TlP), which also contains two ot
stcps n B oxidation, long chain enoyl CoA hvdrataseand lo
chain p-kerorhiolase.r rs a hetero-occameric rotein compo
of 4o and 4J3 hains hat dcrive iron disnncr contiguousgc
wirh a common promoter region. In somc paricnrs,onlv
LCHAD acivity of the TFP is affected (LCHAD dedcienrvhereas chershavedeficiencies f all three acriviries TF P d
cienc,v).Clinical manilestations include rtracks of acute hypo
toric hvpoglycemia similar ro MCAD deficiencv;patientsof
shou' e1'161s...1 m.rc severedisease, nclucling cardiomyopat

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 82/177
mav also be associared l'ith malernal lllness.'ireatmenr
is similar to that for MCAD or LCAD/VLCAD defi-
ciencn thac is, avoiding fasring stress. Sorne invescigators have
suggested hac dietary suPplements wirh medium-chain trrglyc-
eride oil and docosahexaenoic cid (DHA) may be useful Liver
tlansplantariondoesnor ameLorate hemetabolicabnormalicies.
SHORT_CHAINHYDROXYACYI._COAEHYDBOGENASESCHADI
DEFICIENC y few patrents with rhis inborn error have been
described. frvepatientswith proven mutatronsof SCHADhave been reported. Four cas in three families wirh recessive
mutarions of SCHAD presen d with episodesof hypoketotrc
hypoglycemra that was shown to be due lo hyperinsulinism ln
contrast !o patients wlrh other forms of fatty acid oxidation dis-
orders, these cases equired specific therapv for hyperinsulinism
to avoid recurrent hypoglycemia. A Sth child presencedwith ful-
minant hepatic failure at age 10mo and was compound her-
erozygous for two different SCHAD mutations. Orher reports
include a child wrrh attacks of fascing h,vpoglycemia and myo-
globinr,rria associated wrth deficiency of SCHAD in muscle but
not in cultured fibroblasrs, three children with fatal liver disease,
and an rnfant wbo died suddenly and unexpectedly.Thrs variable
phenotvpe may be due lo genetic heterogeneitv.Specificme bolic
markers for SCHAD deficiencv have not yet been ide i6ed,
making this a particularly dif6cult diagnosisco establish.
DEIECTSNTHE ABNITINEYCLE
PTASMA MEMBRANE CARNITINETBANSPOBTDEFECTPEIMARYCABNInNEOEFICIENCY).rimary carnit ine deficrencys the only
gene c defecr in rvhich carnirine de6ciency is the cause, rather
than he consequence,of imparred fatcl' acid oxidation. The mosr
colrlrlron presentalio is progressive cardtomyopathy wirh or
w i rhou t ske le ra l u ' e weakness eg inn ing t l - 4 ' r o f age.A
smaller number of patients may present rvith fasring hypoketotic
hypoglvcemra in the lsr yr of life before the cardromyopachl'
becomessymptomatic. The underlying defect involves the plasma
membrane sodium gradient-dependent carnitlne uansporter that
is present n heart, muscle, and kidney. Th:s transporter rs respon-sible botb for maintainioe ntracellular carnit ine concenrratrons
20- to 50-fold trigher than plasma concentracions and for renal
conservallon or carnlrlne.
Diagnosis of the carnirine cransporter defect is aided by rhe fac
that patients have extremely reduced carnitine levels in plasma
and muscle (1-27o of normal). Hereroz,vgoteparents have plasma
carnitine levels =50% of normal. Fasting kerogenesis may be
normal because iver carnitine transport is normal, but ir may be
irnpaired if dietary carnirine intake is interrupced. The fascing
unnary organic acid profle may show a hypokecocicdicar-
box,vlicaciduria pattern if heparic fatty acid oxidation is impaired,
but it is orherwise unremarkable. The defect in carnitine trans-
porl can be dem,rnstrated linicallr by severe eduction n renal
Chapter 6 r oefecls n Metabolism f Lipids
carnitine threshold or in vilro by assav of carnitine uptake u
cultured 6broblascs or lvmphoblasts. Mutations in the orga
carion/carnitine transporler (OCTN2) underlie this disor
Treatment of chis disorder with pharmacologic doses of oral
nitine (100-200 mg/kg/day) is highlv effective in correcting
cardiomyoparhy and mlrsc le weakness as well as any impairm
in fascing ketogenesis. Muscle total carnitrne concentrati
remarn 5ozo l no rm a l on l rea lm en t
CAEI!ITINE PAIMITOYLTRANSFERASE_IACPT_IA} DEFICIE
Several dozen infancs and children have been described wrtdeliciency of the liver and kidney isozyme of CPTIA. Clin
manifestations include fasting hypoketotic hypoglycemia, o
sionally ';r'ithmarkedly abnormal Iiver funcrion rests and, rar
rvith renaltubular acidosis- he heart arld skeletalmusc]eare
involved because the muscle isozyme is unaffected. Fas
urinary organic acid profile shows a hypoketotrc Cr-Cr: di
box;rlicaciduria but may be normal. Plasma acylcarnione an
sis demonstrates mostly free carritine with r.ery littLe acyla
carnitine. This observarion has been used to esrablish CPT
diagnosis on newborn screening by tandem mass spectrome
CPT-IA deliciency is the only fatty acid oxidation disorde
rvhrchplasma otal carnit ine evelsar e elevated o 150-200%
normal. This may be explained by the fact rhat rhe inhibit
effects of long-chain acylcarni tines on the renal rubular carnr
rransporter are absel! in CPT-L{ deficiency. The enzyme decan be demonstrated in cukured fibroblasts or lvmohobla
LPT.IA deficiencyn th e fe tus has beenas'ociaredwrth icute f
liver of pregnancy rn the mother in a single case report. Tr
ment is similar to rhat for N{CAD defc iencl' with avoidanc
situatrons where fasting ketogenesrs s necessary.
CARNITINE_ACYTCABNITINERANSTOCASE CACI) DEFICIE
This defect of tie rnner mitochondrial membrane carrier pro
for fatcy acylcarnirines blocks the entry of long-chain fatqv a
inco che mitochondna for oxidation. The clinical phenotyp
this disorder rs charactenzed by a severeand generalized imp
ment of farty acid oxidation. Most neu'born patrenrs present *
acracksof fasting-rnduced hypoglycemia, hyperammonemia,
cardrorespiratory ollapse.All symptomatic newborns have
evidence of cardiomyopathy and muscle $eakness. Sepacienrs with a partial rranslocase deficiency and milder dis
wirhout cardrac involvemenc have also beeo idenrified. No
cincciveurinary or plasma organic acids are noted, althoincreased evels of plasma long-chain acylcarnitines are reporDiagnosis can be made using cultured fibroblasts orphobLasts. he human genehas beencloned,and mutarions h
been identilied in affected parienrs. Treatment is similar toof other farty acid oxidacion disorders-
CARITIITINEATMITOYTTRANSFERASE_IICPT_II)DEFICIEIIIGYh
forms of CPT-II defrciencv have been described. The antenpresenlation of this drsorder rs associatedwirh a profo
enzyme deficiencl and neonatal death has been reported
several newborns with dysplastic kidneys, cerebral malfortions, and mild facial anomalies- A severedeficienq' of enz
activity is assocrated w'ith an infantile-onset form. This fshares all the clinical and laborarory features of CACT deGciA milder defect is associated with an adult presentationepisodic rhabdoml'olysis. Th e 1s t episode usually does
occur until late childhood or early adulchood. Attacks mayprecipitaced b,v prolonged exercise. There is achrng muscle
and myoglobrnuria that mal be severe enough to caus€ r
farlure. Serurn levels of c reatine kinase are elevated to 5,0
100,000 UiL. Fasting hypoglycemia has not been describedfasring may contribure to attacks of myoglobrnuria. N{u
biopsy shows rncreaseddeposition of neutral fat. The myopa
Dresenration of CPT ll deficiencv is associated with a com

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 83/177
572 r PAnTX Melaholic iseases
mutanon 5113L. An intermediare form of CPT-II deficiencv ore-sents in intanc)/early chrldhood wirh fasrrng-induced epancfailure, cardiomyopathy, and skeletal my'opathy with hvpoketo!ichypoglycemia but does not have the severe developmentalchanges seen n the neonatal presentation. This pattern is morelike that seen n VLCAD de6ciency and management is identical.Patiencs are generally heterozygous for one of the severe rnuta-
tions and one of rhe milder mutations.Diagnosis of all forms of CPT-II deficiency can be made by
demonstrating deficient enzyme activity in rnuscle or other ti ssues
and in cultured 6broblasts. Mutation analysis rs available.
DEFECTSI{ ETECTROIINAilSFERATHWAY
ETECTBONSANSFEB TAVOPROTEINETf)AND ETECTROTRANS.FER TAVOPROTEII{EHYDROGENASEETF{H I DEfICIENCIESGI.U.TARIGACIDURIA YPE . MUTTIPTECYLCOADEHYDROGTNATIONDEFICIENCIES).TF and ETF-DH funcrion to transfer elecrronsinco the mitochondrialelectronrransoort chain from dehvdro-genationeacrionsaralyzedy VLCAb. MCAD. and SCAD,aswell as glutaryl CoA dehydrogenasend at least four enzymesinvolved n branch-chainamrno acrd oxidation. Deficiencies fETF or ETF-DH produce llness hat combines he featuresofimpaired any acid oxrdation and impairedoxidatronof severalamino acids.Completedeliciencies f either protein are associ-
aredwith severellness n rhe newbornperiod,characterized yacidosrs, ypoglycemia, oma, hypotonia, cardromyopathy, ndan unusualodor of sweaty eetdue co sovalerylCoA dehydro-genase nhibition. Somealfectedneonateshavehad facial dys-morphia and polycystic kidneyssimilar to that seen n severeCPT-II deliciencl',which suggesrshat toxic effectsof accumu-lated metabolitesmay occur n utero
Diagnosis an be made rom the urinary organicacid pro6le,which showsabnormalities orrespondingo blocks n oxidationof fatty acids etbylmalonacend C6-C,6dicarboxylic cids),lysine (glutarate),and branched hain amino acids (rsovaleryl,isobutvryl-,and q-methylbutyryl-glycine). osr severely ffectedinfants do flot survive he neonatalDeriod.
Parlraldrhcrencresl L ll ' .rnd rF-DH oroduce disordertharma ' mrmrcMCADde6crenc lr orhermj lder a t ry c id x i -
dation defects. hesepatientshaveatracksof fasringhypoketoticcoma.The urinary organic acidprofile revealsprimarily eleva-cions of dicarboxylic acids and ethylmalonate,derived fromshort-chain artv acrd rntermediates. econdarv arnitine de6ciency s present.Some atientswirh mi ld forms of ETF/ETF-DHdeliciencybenelit rom treatmentwith high dosesof riboflavin,which is a cofaclor for the pathwayof electron ransfer.
DEFECTSN KETOTIEVNTHESISATHWAY
F-HY0R0XY-p-METHYTGT.UTARYT.oA{HMGCoA)SYNTHASEDEFICIENCY MG CoA synthase is the rare-limiti ng step in the
conversion of acetyl CoA der ived from fatty acid p-oxidation in
the liver to kerones. Severalpatrentswith this defect have recently
been identified. The presentation is one of fasting hvpoketotichypogJycemia withor:r evidence of impai red cardiac or skeletal
muscle function. Urinary organic acid profile showed only a
hypoketotic dicarboxylic aciduria. Plasma and tissue carnitine
levels are normal, in contrast to all the other drsorders of fatty
acid oxidarion. A separate synthase enzyme, present in cytosol
for cholesterol biosynrhesis, s not affected. The HMG CoA syn-
thase defect is exoressed onlv in the liver and cannoc be dernon-
strated in cultured fibroblasts, The gene has been cloned, and
mutations in rhe affected patients have been characterized. Avoid-
ing fasting is usually a successful reatment.
p-HYDR0XY-P-I/IETHYLGLUTA8YLOA TYASE EFIGIENCYeeChaoter 5.6.
IIEFECTStI KETOTIETILIZATIOI{
The ketonesP-hydroxybutyrateand acecoaceratere rheproductsof hepatic fatt;t acid oxidation and are importanmetabolic uels or the brain during fascing. wo defects nlization of ketones n brain and other peripheral issuessent as episodesof "hyperketotic" coma, with or withnypoglycemra.
SUCCIYI-COA:ilKEI0ACID COA TBAIISFEBASESC0T}CIENCYSeveral parients with SCOT deficiency havereported. Characeristic presentation is an infanc q'irh recurepisodes of severeketoacidosrs induced by fasting. Plasma acarnirine and urine organic acrd abnormalities do not distingufrom other causesof keroacidosis.Tieatment of eoisodes eouinfusion of glucoreand largeamount' of bicarbonateunril mbolically stable, All patienrs exhibit inapproprrate hyperketomia even between carabolic episodes. SCOT is responsrbleactivating acetoacelate n peripheral tissues using succinyl Cas a donor to form acetoacetyl CoA, Deficient acrivity candemonsrrared n brain, muscle, and f ibroblasts lrom affepatients. The gene has been cloned, and numerous mutati
have been characteflzed.
P-{GT0TH|OLASEDEFICIENCY.ee Chapter 85.6.
Andresen BS, Dobrowolski SF, O'Reillt, L, et al, Medium chain acrfC
dehydrogenaseMCAD) muratrons dentified by MS/MS-basedprospe
screeningof newborns differ frorn rhose observed n patients wrrh cli
svmptoms, denrificarionand charact€rizarionof a new, prevalentmuta
thar results in mild I{CAD deficiencv. Az I Htm C
2001i68:1408-1418.
Bonne{onrJP,Djouad, 4 Prip-BuusC, et al: Carnitine palmitoyltransaera
and 2: Biochemical, molecular and medical aspects. Mol Aspe.ts
2004;25:495-520.
Clayton Pl Earon S, Aynsley Green A, et al: Hyperinsulinism n short-c
L 3-hydroxvacyl-CoA dehvdrogenase eficiency eveals he impcrtanc
beta-oxidation n insulin secretion. Clin Inuest 2001;1081457465.
Den Boer MEJ, Dionisi-\ricj C, Chakapani A, et ai: lviitochordrial tilu
cionalprotein deficiency,A severe ady acid onidation disorderwirh carand neurologic rn"olvenent. I Pediatr 2003i142r684-s688.
Den Boer MEJ, WandersRJA, Monrs AAM, er al: Long-chain 3-hvdro
cyfcoA dehydrogenase e6ciencl.:Clinical presentarionand follow u
50 paienl.s PeAdtri.s 2002;109:99-104.
tslpelegON, Hammerman C, SaadaA, et al: Antenatal presentarionof c
tine palmitoylrransteraset deiclency.Affi J Med Geftet 2001'102:183
Fukao I Mrcchell GA, Scng XQ, ec al: Succinyl-CoA:3-ketoacidCoA u
ferase SCOT): Cloning oI th€ human SCOT sene! e{dary structuraLm
eling of the human SCOT monomer, and characrerization of t
pathosenicmuradons. Geaomics 2000i681144 151.
GregersenN, Andresen BS, Corydon MJ, et al: Mutation analysis n m
chondrial fany acjd oxidation defects:ExemplJfiedbv acyt-CoA dehy
genase eficrencres, ith special ocus on genotype-phenorvpeelation
Hun Mutat 2001t181169 189.
Klose DA. Kolker S. Heinrich B. ec al: Incidenceand short rerm outcom
children rvith symptomatic pr*entarron of organic acid and iany acid
dation djsorders n Germ^ny. Pediat/ics2002t110:1204 1210.Mathur A, SimsHn, Gopahkrishnan D, et aL,MoJecularheterogeneiryn v
long-chainacyl-CoA dehydrosenase edciencv ausingped,atric cardio
oparhy and suddendeath. Cir.ulatioh'19999911337
1343.
Shekhawat PS, Marern D, StraussAW: Fetal fatty acid oxidacion disor
rheir eifecr on maternal health and neonatal outcome, Impact of expa
newborn screening on their diagnosis and management. Pedntr
2005;57:78R-85R.
StanleyCA, Bennett MJ, Mayatepek E: Disorders of mitochondrial fatty
oxidation and relatedmerabolicpath.*ays. n: FernandesJ, SaudubmyJVan den Bergh C, Walter JH (eds). nborn Metabotic Djseases:Drasn
and Trearment4rh edidon: Heidelberg:SpringerVerlag,2005 pp. 175-
Wllcken B, Haas M, Joy P, et al: Our come of neonaral screening or med
chain acyl-CoA deh-vdrogenase eficiency in Ausualia: a cohorr st
Lancet 2007359:3742.
DD

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 84/177
Yar lsZ. Yxmrd, t . Zhro \ et aL: ' ,ospect , le cr c. . ,ng or pedr-r t r rerr i r
chordrrrL roreLr let tcts npregrrr r i cscompl icared ) |vcf drscase.. 11.1
2 0 0 2 ; 1 8 8 r 2 1 62 1 6 6
86.2. DtsoRorRSFVERYoNG HATNlrrv Actosa
PEROXISOMAIISORDERS
' fhepcroxisomal diseases re genetiaallt derermined clisorclcrs
catLsed ither by rhc faiLr.rreo f()rrn or maiLrtarrrhc pero\Ls()nrc
in chiidhood ard r>ccur- ror'c rcquentll and prcscnt e ulder
rlngc of phelotvpe rhen h:s becLr ecognrzedn rhe past
[Tl0l-0GY l'eroxisonraldrsordersare subdivided nto t\\ 'o n]. jor
ca tego r ieslab le 86 2) .
In categorvA, the pcroxisomalbiogenesir isorders PBD), rhc
basicdefcct s rhe ailure ro irnport one or morc protetls inro fbe
orsanellc- ln category Il, defeccsaffect a single peroxisonralprotcin 1h e peroxisorrc s prcsent n all cellscxcepr natLrrcer \
drrocvtes.rud is a srLbcellul;rrrrganclle urroLrnded y e singlc
membrlnc; >51) peroxisr:rmalcnzYmes erc identif iccL Sorne
c z!nrcs ere rnvolved n the pro(luctron dn d dcconposLtiorr )f
hldrogcn pcr<>xide; thers nrt conceruedwlfLr iPid ald rrnrno
ircid metabolsn. N4osr croxisonralenzy cs rrc I sr sl nrhesrzed
rn their Inatllre forrn,rn lree prrlyribosornes url enter t ltc cyro-
plasrn.Proteirts hat arc destirled or the perorisorne onfarnsp e
ci l ic perox;somc argeting seqLrencesPTS).N' losf peroxi\orrrirI
rnarrix proterns contain PTSI. a 3-amino .rcLd equrenccrr rhc
carboxyL ermilus. PTS2 is an rrrlno-ternlindl seqLrcncehir i \
cricical or the xnport oi elzvnlts rnvt>lved rt phsnalog,cn rntl
branchcd-charn farty lcid nr. 'raltolisnr. lDport oi pr(rtcins
involves a complcx serres t rellcrons thar rnvolvesat least . l
Chapter 6 r Defectsn Metabolism f Lipidsr
A:DlS0nDtnSfPtnoxl$Mt |[4PoRT
Allell$Pgertndrome
A2r eonatdldrenoukodyitroply
AlinfantkRel5umtease
A4rRhomer(hondrcd)5pia5iauKtata
B:DEFECsF lL6l.EEno)($oliAttlZYME81lt-link€ddr00leukodyforhyB2rAcyl[oAxi(id5eef( ncy
8l:BrFLrn(ina nzymeeficienr/B4:Peroxsolrah laseefrcnry85 a5i ir ebumseaseB6:2ethllary0A (emaseen[ien(y87i fAP ry ansferaiePnoenq88:Ay CHAPynthaseefi(iei(y89:lvlevalonk( uda810:6lutrk(iduriaypeEllHIEro$luiaype812 (ata5emia
distnrct proteins. These proteins are referred t() as pero
cncodc.l by PF.X gcnes IaLrle86--i sumrnarizes he / ' lX g
rhrrr rrc delective n hunrar discase rarcs.
tPlDEMl0L0GY.Excepr for X-linkccl odrcnoleukodlstrophAl.L)), elL he peroxlsomal :lrsorclerslr TaLrlel6-2 are autosrcccssirc raits- X AII) is th e rnosf comiroll pcroxisorrral
dc ( r t r rhan cs t im a tcdrc idcncc f 1 /17 ,000 - he co rnb incderce ol the other peroxrsomal djsorders Ls esfirrated ft / 0 ,000.
PAIH0t0GY Absenceor reduction l rhc number of peroxisis parhognonrorticor disorders f peroxrsonebroqenesis.r
disorrlcrs, hcrc irre mefilbrinoLrs acs har confain peroris
integr-llnrcrrbralc proteins. vhich ac k chenorrnal complcoi nntrir protcins; these re pcr()\ isonre "ghosts." Parho
charlges re observed n nran! ()rt!: lns nd include proiound
ch.rr.rcrerrsrrcefecrs n neuronal migrdtioni micronodultf
(OMPTEMEilTATIO}IROUP I,IO ATITNRTUIXIDT(I(I
PTROTIN#
l
)
(HARACTTRISTI(
]1I Kd AA IPAIC
[]H[.zna nd q nleqc]peroxsomdembTdnerole 5 5l kd
51 52kd nielra eox crulmembke ole l
21-24 d emri5omdlas5octed biquitn-.0nju9ar,r9nzyne
Pis riepiof
ll 27koAAA IPe5€PIS re(eplcr
7l 8- kdPerlxisomrl3ssa{atedrotein
42-kC tegc eorjsomalembrdierolein
trfC zne-bindinqteEalpeoxr50maembraner0lein
ll-12 ld Penrxi5omalmembonerotenvnved per0x5omarolfeftllon
48-kd,f(r ?jnc rnd9 n1egraemxomal emEne rote
lfl I cont; nq 0 41kdperox5ori;nteqralperc](iicmaernbrdftrotern
4l kc nreqra enbrdnemlern
48+Cfo5o r prole
-19c Pephec erox50ma]membranemtein
:i-10 kdhrcxi5cmallnlr sc rnernbraneroler
l5 39 d Per0xi5ornalembrdneroleznr inger rtrf
Percxisrmaen ranerotern,pffylateo
1Dockrnqailoror or1p nd er6p
(KI PHT{OTIPT ftROM
99 15,ALD.IRD 7q11)2 A
|((I IAPAN AMs
t E )r 0 F 5
l l
2 li,r,rALDA,IALDRIDP
zs,\AL!l
li,i,rALSl Dz5,iiAt. i)
A
AA,NAsD, DA
r & 1 16p216qn 4
8q210
r23
t
1 8t9
15
5
5
)
im5.Amnerdim|(l,erned/nEe, ri'tutpI cmMoler V, enntF-phei0r)p€orcla r5i d 0de6 fFe.mome ll?ritt l,1rt edt!lr b 19959316

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 85/177
Pe'odio4lesb5ent0 cduredn lumber
574 r PART r Mehbolic Diseases
(aala5e ''tosol
lnireasedrioaryKretion
rhosisof the iverl enal cyscs; hondrodysplasia unctata; orneal
clouding, congenitalcataracts, laucoma, and recinoparh,v;ongeniralheart diseaser nd dysmorphic earures.
PATH0GENESIS.r is Lkelv that all pathologic changesare sec-
ondarl co che peroxisome defect. N'tultiple pero)(isomal enzymes
fail co function in the PBD (Table86 4). The enzymes har are
diminished or absent are s)-nthesized uc are degradedabnor-
malll. fast because hey mav be unprotectedoursideot the per-
oxisorne. t is not clear how defective eroxisome uncrions ead
to the rvidespread arhologic manifestatrons.
The PBD are associated t'ith geneticall,v deternined import
defects. he PBD have beensubdivided nro 12 complementarion
groups. The molecular defeccs ave been defincd n l0 of these
gror,rpsse eTable 86 3). Thc pattern and severityof pathologic
features var-v virh the nature of the tmporr defeccsand the degree
to rvhich mport is mpaired. Thescgcncdcfects ea d o disorders
that were named before rheir relationship to lhe peroxisome
\{'as recognized.namell' , Z,elhl'cgcrs,vndrome ZS), neonatal
adrenoleukodystrophv NALD), infanrile Refsun disease lRD),
an d rhrzomelic hondrod,vsplasiaunctara RCDP).The 1st hree
disorclers re no\\ ' considered o form a clinical continuum, with
ZS rhe mosr ser.ere, RD rhe leasr severe, and NALD itcermedi
ate. The,v can bc caused b,v 11 diiferenr gene defecrs,u'hich
invoh'emainly rhe inporr of proteins hat contain the PTSI tar-
gecing rgnal; hc genedefects annot be distingLrishedn the basis
ofclinicalieatures. he ciinical ser.eriry ariesv' ith the degree o
v'hjch prorein mport is impaired.Mutations thar aboLishmporr
reraincd, eads o the somewhat mildet phenotypes.A defect n
PEX7, r'hich involves he import of proteins that util i ze PTS2,
rs associatcdwith RCDP -PEX7 defects har leave mporc par-
cially ntact are assocrared ith milder phenotypes, om eof u'hich
resemble lassicRefsum disease.
Th e geneticdisorders har involve singleperoxisomalenzymes
usualJy ave clinical manifestations ha! are rnorc rcstrictedan d
relaccd to thc biochemical defect. The primar,v adrenal insuf6-
cienc,v f X Al-D is causedb, vaccumulationof ver,v on g chain
fatty acidsVLCtA)
in rheadrenalcorrex, and the peripheralneu-
ropath,v n Refsum disease s caused b,vrhe accumulation of phy
r rn r . . r . i d n 5 .h t tann ce l l s r r Jm l r l rn .
PBDwith Milder or AtypicalPhenotypes. ervborn rnfancs . 'r.rth
Facialappearance high forehead, unslanringpalpebral issures,
hrpopJasric upraorbital ridges.and epicanrhal olds; Fig. 86 31,
severeweakness nd hyporonia,neonatalseizures, nd e,ve bnor-
malit ies (cacaraccs,laucoma,comeal clouding,Brushfieldspots,
pigmenrary rccinopatht-,arrd nerve d,vsplasia). ccausc of chc
hvpotonia an d "mongoloid" appearance. o*'n svndrome may
be suspected. nfants rrrrh Zelhveger s,vndromc rarelY live more
than a ferv months. More than 90ot" shou' poscnatalgrorvth
failure. Table ll6--5 sts he rnain clinical abnormalit ies.
Patients vith neonatalALD shor.r' ferver nd, occasiooalldvsmorphic features.Neolatal seizures ccur frequenrly.S
degreeof psvchomorordevelopmenr s present; unction rem
in ch eseverelyor proioundl,v etarded range, and developm
mav regressafrer 3-5,vr of age, probabl,rr rom a progres
leukod,vstroph,v.el'eral atienrsare now in a stable,albeit
abled, sate in their 3rd or 4th decade. Hepatomegaly, impa
liver unction, pigmelrary degencration fthe retina,and seve
impaired hearingar e nvariabl,v resenf.Adrenocorrical unc
is usuallv imoaired. but overt Addison disease s rare. Cl
drodvsplasia unctata dnd renal cystsare absenr.
Patientswith infantile Refsumdisease ave survived o rhe
decadeor longer.Thev are able to walk, afthough gair may
ataxic and broad based. Cognicive funcrion is in the seve
retarded ange.A1 1 ave sensorineural caring lossan d pigm
tarv degenerarion f the retina. They have moderatel,v ,vsphic fearures hat nal include epicanrhal olds, a f lar bridg
the nose, and lo.rv-ser ars. Earlv h.lpotonia an d hepatome
rvirh rmpaired function are common. Levels of plasrna cholest
and high and lou'densit l ' l ipoprorein are often mocler
reduced.Chondrodvsplasia uncrataand renal cortical cvsts
absenr. Postnlortem studv in infantile Refsum drsease er
mrcronodular ir.ercirrhosisand small hvpoplasricadrenals.
brain sholvs no malformations,except or severebypopLas
the cerebellar ranule ayer and ec()pic locati{)ns f the Purk
cells n the moleclrLar dyerTh e mode of iohenhnce is auc
mal rccesslve-
Iigtrr. ll(. I lilrr tatients $irh Zellu'eger cerebrohepatorcnalsvndr
Note thc hlgh forehead,ep'icrnrhal o1ds, nd h,vpoptasia f nrpmorbit.l ri
and rnrdiace (t-ourtes! of Han\ Zellweser. N{Di

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 86/177
ftom eflds HA!Grcbo-heorm:eia/elwetsi yrdrcmenta indb0thim ilonsequerrerdpen!50"41fu(rl,rni it1r5.lne6O0fAmnerd;m,1984
Some prricnts u' idr PtsD drsordcrshave milder ancl rr\pic:lI
phcnortpe:,. lhev rral prcsent with periphcrel netlroPith) {rl
rvirh retinop:rrh,-.urparrecl ision,or cafaracfs n chilr lhootl.adrr
lescence,r rclult ltoodenrl hevebcendragnoscdo hare Ch.rrcot
l\. larieToorh disease rr Llshcr svndrc>rne. onrc parieors hare
Chapter 6 t oelecls n Metaboli srn l Lipids
srLrvrvedo rhe -5rhclecade. elects r PEX7, which rnost
rronlv lead ro dre I{CDP phenotype. nirv.rlso ead ro a m
phenorlpe rvrrh cLinicaL anlfest. lt i()ns inrilar o thoseof c
cal Reisurndrseaseph,vranovlCoA hvrlroxvlase e{icicncv
Rhrzon re l i cho f ld rodysp las iarnc ta ta HCDP) h is d iso r
cher.rcrerizecl y rhe preserrce f stippled ioci of calcif icwirhrrr rhe h,vrline carrilagc and is associatcd vith cfi,v
carar.rcrs72' llol.and rrulr;. lc rnalformations ue o contrac
Vcrtcbral bodicshrvc'a coronal clcft l i l led Lr,v arnlage rha
result of an ernbrl,onrc rrest, l)rsproportiorrafeshort st
.rffccts hc proxinral parts of fhc cxrrcnrrt i.-s I i ig. 86-4i). RoLrgic.lbnormaLiries onsrsrof shorteLrrni{f the proxunal
boLres,netaphlseal upping. tnd drsturhedossilication Fig'1ll i. Height, u'eight. rnd hc.rl circumfercncc re es s ha n h
percentile, nd these hildrcurc levcrcl) rcrardedmcncalb'
changessuch as those observed Lr chrhyosliorm erythrod
af c lrcsent in =2.5!6of f itrtnts.lsolatedDelectsol Peroxi sonral attyAcid 0xidation.
lhc d
dcrs rbclcd R1 through tli isecTablc S6 2) cech nvoLve l
rhrceenzl.rnesnvolverl n per<>xisomalarrv acrdoxidanon.'
c l r r i ca l nen i f es ta t ro ls csc rnb le hose of thc Zc l lwcgc rclronrc/rconaralALD/Inienrile Rcisum disccse ontinuum;cirrrbe clisrirrgursheclon r disorders i pc.r'orisonreiogenelel-.or.rnrrv csts. Dciccts oi biiuncrionel cnzvmc erc c() r
rnrl dre found in =li ' l i, () f patrenrr rvirh rhe lellwe
svl t l lme/neora al ALL)/irridnfile l{elsunr diseasephenoPirricr)ts irh isoldtccl .\ L .o A oricl:rscdcficicncvhavea s$+it nrilder phenot,vpc hrrt rcsernblcshar of nconatal i\LD
ls0latcd Defectsof PlasmalogenSynthesis.Plasmakrge
lLp id ; n wh ich rhc ls r ca rbono i g l , vcc ro ls inkcd o an a lrrrth.r th.n a iacryacid Thcy rre s ynthesized hrougha com
serreroi leactions, rhc lst two steps of rvhich ale cefrllze
th c peroxisomaLenz\mes dihydroxvacetonc phos|h:rte
trrrtsieraseaiJ s\nthrsc. L)eliciencv )i elfhef oi fheseenzr L r . lr n l t i r n L r l l , s . - l c r d ' , , f r ( r ' \ ' r \ l c l ' r r . . l i n
inclisrirrgLrishale ironr rbe peLorrsornirl rnport rl isorclerRThLs etrcr disorder s crru\edb_v dcft-ct n PFX7, thc .cckrr pcr ()\ i\onrc targcrirrqsclluelce 2 l t shares he severecrencr of plasnaloeers \vrth disordersB.trand 85 but. in
(Ast li vfir(HII{fORMATIONAEOUTII{EfTATUREWASAVAttAEtt
GJEsINWHI(HTHE TITURTIVAS RT5ENI
ABI'IORMATTATURE Nt)
|lgh ore|le,rd 6l
Flal ri:pui 16
Largeon nel is).lideLriun5 tt-
Sh aow drd l rdqes ll
Low/bro,rdaa bridqe 2l
Eocal thus ]6
Hgh ,{hedF dte l1-
Exiernrarilefolmrty 411
llcrognalhia 18
lieCundantkinfoldrfne(k 1l
Erushhedpots 6
[a]a.arl/(rdyorneJ l5
Gaucotu 1)
Abnolmairern,rqmerrdt$n 15
Optc s(palr r 2l
SeveEypo:ord 95
AbncnalMcrutspon5e )t
Nypcrsllexarareflexa 57
Poolucklnq 11Gavaqeieding )t
:pripi isezrles 6 l
liyihomorcfretrrd,rton 45,mptred earlnq ll
fystaqmus 3'.
% N0.
5 ] 5 Et4 l l50 5529 ,rl20 ill2 l lt2 l5l5 l9t6 18t] t, l5 5
lt l0I il l 620 li8l 947l )65C 55
68 i4ll 2554 55l9 451 8 9l2 lJ
91
8 l
r00r009)9i9rlilrl1i08l86:t411
t[096
96l1l09i
t0 l408t
r . l : , r '. . A. Nc\vborn i , r t . l t r ! " , r I hrzonlc lL. .hondrod!s
pld i r , r fun. t r t . r lRr : l l ) l ) r \ofe rh . !L\ . f r 'hor tenr lg of the pro\
rnr , l l Lnl - .s . he dep.es leLJ rLc lgc i rhc rosc , hvpcr ons,n. . rn.1
lv idcs tnead sct r lurg L n lLsrNs- 11. ( , tc rhe nrnrk€d s l rorre. ng
oi rhc humcrur arrd eprphvseal 5r t t lnq r t t l ic rhouLder . r j r l
e lborv ;o,nts . iCour : r ' r ot lohn ] ' ] . )o,s r . \ ' l l ) r

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 87/177
576 PARTX MetabolicDiseases
rion, has defecrs of phytanrc oxidatit>n.'l
he fact rhat disordcrs
84 and 85 are associrtedu-irh he full phenrxlpe of RCIDPsug-
gests hat e delicrency f plasmakrgenss sliEcrenr o producc r-
ClassicRelsumDisease. he defectrve nzyme phvtaLroyl ir, i\
oxidase) s iocalized o the peroxisorte. Thc nranifestationof
classicRefsurndiseasencludes mpalredvision irom retinirispi g
merrrosa, chchyosis, elipherll n.uropathy, irrarir. and, occa-
sionaLly. ardiac arrhyrhmias. ln conrrast to rnfanrile Refsum
drsease, ogrit iue funcrion is rrorrrdl and there are rro congenital
malforrnarions. lLassicRefsum disease frcn does not rnanifcsc
unol youLrgadr.rlthcx>d,ur visual disturhancessuch as nighrblindness, chthyosis, nd peripheralneuropadrynray rlreaclvbe
present n chrldhood and adolescence. arll cliagnosiss impor
tallt lrecause nsritution of i phvfarlic acid resrric rrd dier can
rcvcrsc hc pcripheral neuropadrvan d prevent he p()grcssio of
rhe visLral nd ccntr'al rcrvous ysternmanifcsterions. hc classi
ca l Rcfsum discascphcnoc-vpcra v :rlsobc causcdhv dciccrs n
PI..X7.2-MethylacylCo AHacemase eliciencf- his cli sorder s caused
by en enzvme clelict that lcrds to thc accunrrrlationol the
branched-chain attv acids ph,vtarican d prisranrc cicLlr.nd i. le
acids.Paticnrsprcscntwith adult typc pcriphcral ncuroparhvan d
may also havc li!r, lne[tdry degenerati<>n:i rhe rerrDa
IAIIORAI0RY lN0lNGS. aboracorl cests bI pcroxrsonraldisor
ders cen bc vicwcrl ar rhrcc cvcLs f cornllcxirv.l-evel1: Docs he PalrentHavea Peroxisomal isortlet? his can
he resoh'ed bv noninvasivc tcs[s that a.c generallv availablc
(fable Eri 61. \4ersurenrent f plasrnaVI CIFA s th c nrostcorn
rnonlv usedassay Wbereasphsna VLCFA levelsarc ele!ated i
mn[,\ 'paticnts vith peroxisomal chsorclers,his s n<x:rJrvayshe
casc.The most i rrpt)rtant excepfLonsre RCL)P. n"vhich
VLCFA
lcr.els re lormaL, but plasma phyranic acid lcvclsar c incrcascd
al d rcd l>loodccll plasmalogen evelsare reduced. n sorneofher
peroxrsomal drsorders, hc biochcmicirl abnormaliries are strll
nrore resfricfed.Therefc:re, panel o1 tests s rcconrrnended nd
inciLrdes hsnrr lcrcls of Vl-(lFA al d of phvtanic,pristanic,ancl
pipccolic acids ancl levels of p)asmalogerrsn red blood cells
Tandenr Lrass sfectronrctry techniqucs also permit c<;trvcnicnr
quan t i r i r t i ( )nib l l c : r c ids n p lasm a nc l r rL re . h i spane l f t e : i r s
cau bc pcrfi)rmcd on 2 nr[. samples f ven<>us]ood in(l pernirsdeteccionoi nrosr pcroxisomal chsorclers.nd ornal results
nakc thc prcsence f a peroxrsomaldisorder unlikclr ' .
[euel i Whfit s he PreciscNotureol the Peroxrsonlal isoder]
Table 86 6lists thc main biochemical bnormalit ies n rhe varior.rs
peroxisomaldisordcrs.Whcr combined u'Lth he clinical presen
tation, thc jLr5t nenrioned alel of tests s ofrerr utf icient o iderr
t it ,v the precisenarure of the defect-ElcvarL'dplasma VL(-FA
levelspermir thc frccise diaglosis of X ,AI ) ir rrralepctients.
-\4arked reduction of err,throc,vrc lasoralogcn evelscombired
lr-ith clevaredplasma phytanic acid perrnrtsprccrscdiagnosJsn
a patierrr vidr thc clinical featuresof RCL)lr. Classic Refsunl
disease an be di.rgnosed l demonstrationoi rncrcascd lasrna
phyranic acicl corrbincd rrith normaLor rcrluced evelsof pris-
crnic acid levels, vhile n D bifunctional enzrrne deficiencl aLrd
2 merhylacv CoA raccrnasc cficiencl' ,he leveJs f prisranrc ndphyranrc acid rle bodr incrcascd.Precise clenri6cation f some
peroxisonal disordersmay r'equiremorc cxccnsil 'e tudres rrcul-
rured skin libroblasts.This mal bc rcqrLrrcd or rhe driferenria-
tion of PBD trorlr dcf-ects n biiunctjonal elz,vne. In PBf), rhe
pacierrc's erorisomcs rrc absenr an d catalase s rD rhe solult le
fraction,whcrcas n bifunctronalenzvmedefecr!peroxisomcs rc
present and catalase s in the particrrlatc racriol. l ibroblasr
stLrcliesre requircd ro idcntifv rhe nature of rhe rnoleculardelect
in PBI). V'hether such specialrzedturlicserc clinjcaLlvvarranred
depencls n indrvic|.ral ircurnsranccs. r'ccisc clinjrion of rhe
defecr Ln a probard may improre th e precisicn of prcnatal
diagnosis n at risk prcgnancics,alci ir rs requrred for carrier
derection. It is also oi value il ;ert irrg progrrosis. Prccisc
Fbrob 5tJ
AtD,adren0hLrhd\qr0rhyYtifAer 0i9i"anfaqa.d5
characterizarorr s of prognosric value iir patjcnrs wirh PF
detects. hrs deiecr s prcscnt n =60?i of PBD paricrrrs, ntl abhali of thc PI:Xl clefe*s have rhe G843D allele,which is ass
ulqcl1r' idr signrficanrly ri lcler henotype han is lound i n ot
mutatron5.LcvelS:What s the Molecul;rrDetqct? able86 3 shoq.s hat
m<>lecularefects n rroscof the PBD har'c bccn dcfincd. Dcl
rion of rhe rnolecular efect n the probalcL, vhich s rolr 'ofier
in scvcr al aborarories, sessentialor carner rlefectiot and sp
prenatalclr gnosrs.
DIACN0SIS Ihere ar c scvcral noniuvasivc aLrorator,vests
pcrnrir prcciseand earlr ciiagnosis 1 pelorrsonraldisordcrs
Iable 36 5).-fhc
chalLeng,en PBD is to clriferenriatehe fr
thc largc varictv of orher condit ions thrt cerr causc hvpoto
DISTASI ISSAY
Zelvq{ersyndrome Pa5maNeonatdl
adrenol*odystmphylnfantheBumiseaie
Rhizcmelc Ph5ma{hondrody5pla5apun(ata RBls
fibtublan5
X nkedLDhemuy,Jona5mafibftrbla5i5
]/L(FA
Pnytanadd
ft 5tanacdPpmliracrd
Be & d
Pasmaoffnvel5
v(FA er'e
VfFA xddtion
Fla5nalen yntieri5
Fh!,1dni{.r anl( xdat n
Gtaia5ecdlizatioi
lmmunoqn(i€m,r(ry[omplelllettalton
DNA
Ph/t in(a(id
VLTFA
PlasmaqeIevel5
Plalrralcgenynihe5i5
PhIanacc xidaton
ON A
VLIFAve
vLIFA](idatonALDP rrn,lrearrvrtl
DN A
VL[FA
!L[FA !el5
ALDP munoreartvity
DNA
VL(FAPhytan(addDTnan iod
Srearid5VLFAievels
Pr 1ana(dDxdatoD
[ata seori zation
Inryme
Vt(IA
/L(FA veVl(FAxcation
Enzyme
Pr5tandi ld
thicdr
PrL$rLL(aaid{iditloi
Enrlme
Phfani(rd
Prst ina(d
Inr/me
FINDING
,nctea5e0
Aqe ependentin
Aqe egendel-:t(rca
r[rea5ed
fcreasedabrorm
Vamby eireased
nrftased
0efta5ed
DerEa5eC
D$r..aseC
lytosoli.
Ferox0me5blent
5e abh86- l
seeTabh86-1
lnfta5ec
N0mal
Decreased
De(reasedDe(rea5el
Pf,Yl eteo
n(rcaied
Derrea5edAb5e[f70%
,4tarimutit,of
Varableaed!en85
Vardblercredse90
VarableP(rease
,1ffO1nutatiorjncea5ed
nctr5ed
nateaSedrf ,ra5e4,rbnorma
fftaiedDe(rcaied
D-bifurctronalclen
l]efirenq
n('a\gd
n(r,.a5edDereised
A.f ftA iiCa5r efu
lnrreaied
lncreaied,bncrfl pa
0ereaged
h,leih)" cy tA ori
dehallndeaied
Decr..a5eCPh)'lancyloA cfi en
NB(e,Fibrobia5E
Bfunctonanzyme P 5madete(
X nkedAlDnererozyq0rc
Ary tA oxdaie
deh(ien(y
Pla5ma
iil'obiJ6
Phrma
FbrobranJ
2'Vetrrlary:oA Pbirnrracemai,!eliaen(y
FibrobLarts
l:a5:i(eEum5edie Pliina

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 88/177
seizures, failure to thrive, or dysmorphic features. Experienced
clinicians can readtly tecognize classic Zellweger syndrome by
its clinrcal manifestations. PBD patrents often do not show the
full clinrcal spectrum of disease and may be identifiable only by
laboratory assays.Clinical fearures that mav serve as indicatrons
for rhese diagnostic assays nclude severepsvchomotor retarda
tion; weakness and hypotonia; dvsmorphic features; neonatal
seizures; retinopathn glaucoma, or cataracts; hearing de6crts;
enlarged liver and impaired liver function; and chondrodysplasia
ounctata. The Dresenceof one or more of these aboormalities
increases rhe li[elihood of this diagnosis. Arypical mrlder forms
presenting as peripheral neuroparhy have also been described.
Some patients wrth the isolated defects of peroxisomal farry
acid oxidation (group B) resemble those wrth group A disorders
and can be detected by the demonscratton of abnormally high
levels of VLCFA.
Patients with RCDP must be distinguished from patients with
olher causes f chondrodysplasia unctata ln addit ion to war-
farin embryopathy and Zellweger syndrome, rhese disorders
include the milder autosomal dominant form of chondrodyspla-
sra punctata (Conradi-Hunermannsyndrome),which is charac-
terized by longer survival, absenceof severe imb shortening, and
usually inract intellectl an Xlinked dominant form; and an X-
linked recessive orm assocratedwith a deletion of the terminal
Dortion of the short arm of the X chromosome. RCDP is s -
pected clinically becauseof rhe shor tness of limbs, psychomo r
retardatioo, and ichthyosis. The most decrsrve aboratory tes s
the demonstration of abnormally low plasmalogen levels in red
blood cells and an impaired capacity to synthesize plasmalogens
in cultured skin fibroblasrs. These biochemical defecrs are not
present in orher tvpes of chondrodysplasiapunctata. Chon
drodysplasia punctata may also be associated s'ith a defecr of
3$-hvdroxysteroid-As,Atisomerase, n enzyme involved in
biosynchesisof cholesterol,
COMPLlCAT|0NS.Patienrs wich Zellweger cerebrohepatorenal
r ynd rom ehavem u l r ip le i sab i l rnesnvo l r ingm usc le one . wa l
lowing, cardiac abnormalities, liver disease,and serzures.These
conditions are treated symptomaticall-v,but the p.ognosis is poor,
and most patients succumb in the 1sr few months of life- Patients
wirh RCDP may developquadriparesis wrng to compre5sion I
rhe base of the brain.
PBEVENTI0N.eeChapters83 and 84.
TBEATMENT. he most effective therapy is the dietary treatment
of classic Refsum diseasewith a phytanic acid-restrrcted die!.
For patients with rhe somewhat milder variants of rhe peroxi
some import disorders,considerable uccess as been achieved
with multidisciplinary early incervention, including physical and
occupational therapl hearing aids, alternative communication,
nurrition, and support for the parents. Altbougb mosr patients
continue to function in the profoundly or severely erarded range,
some make signilicant gains in self-help skills, and several are in
srable condition in their teens or even early 20s.
Srudies to mitigate some of the secondary biochemical abnor
malities include the oral administration of docosahexaenoic acid
in a dosageof 50-100 mg/24 hr eirher as the ethyl ester or in rhe
in tbe peroxisorne, There are anecdotal reports of ctinicaL
improvement. The oral admrnisrracion of choLc acid and chen-
odeoxychoLc acid in a dosage of 100-250 mg/24 hr, wirh the aim
of reducing the levelsof presumably toxic brle acid intermediares,
may be effective.
Chapter6 Delectsr Motabolisml Lipids
GENETIC0UNSEIING,ll the peroxisomal isorders, xhyperoxaluria ype 1, can be diagnosed renatally n the ls2nd trimester.The tests are similar to thosedescribedor pnatal diagnosissee able86-5)and usechorioric villus samor amnioc)tes.More than 300 pregnanciesavebeenmonitoand more than 60 aflecred eruses ave been dentifredwithdiagnosrrc rror Because f the 257o ecurrenceisk,coupleswan affectedchild must be advisedabout the availability ofnalaldiagnosis. eterozygoresanbe denti6edn X-ALD anrhosedisordersn which the moleculardefecthas been dent(see able86-3).
ADRENOTEUKODYSTROPHYX.TINKED}
X-ALD is a genetically determrned disorder associated with
accurnularion of saturated VLCFA and a progressive dysfunc
of the adrenal cortex and central and peripheral nervous svs
white matter.
ETI0L0GY The key brochemical abnormality is the tissue amulatron of unbranched saturated VLCFA. with a carbon c
length of 24 or more. Excesshexacosanoic ci d (C26:0) rsmost striking and charactenstic feature. This accumulation
fatty acids is caused by genetically deficient peroxisomal dedarion of fatty acjd, The kev biochemical defect involves
impaired function of peroxrsomal hgnoceroyl CoA ligase,
enzyme lhat catalyzes the fornation of the CoA denvativeVLCFA. The gene that rs defective (ABCDI ) codes for a per
somalmembrane ALDP). More than 400 distinctmutationsh
been idenrif ied, and most familes have a mutation tha"privare" (uniqueco hat kindred) and areupdaredon the we
http://wwwx-ald.nl. The gene has been mapped to chromosXo28. The mechanism by which rhe ALDP defect leads ro VLC
aciumularion and the pathologvof X-ALD is unknovvn.
EP|DEM|0L0GY he mrnimum incidenceof X-ALD in mal
1i21.000. and the combined ncidenceof X-ALD males anderozygous females in the general population is estimated to
1n7,000- All races are affecred. The various phenotypes ooccur in members of the same krndred.
PATH0L0GYCharacteristic lamellar cvroplasmic inclusions ca
demon',rratedwith the electron mic.osc,rpe n adrenoco
cells, escicularLeydig cells, and nervous systemmacroph
These inclusions probably consist of cholesterol esrerified w
VLCFA. They are most prominent in cells of rhe zona fascicu
of the adrenal cortex, which ar 1st are distendedwith Jipidlater arroPny.
The nervous system can display two types oI lesions. In
severe childhood cerebral form and in the rapidly progres
adulr forms. demyelination is associated with an inflamma
responsemanifesied by the accumulati.rnof perrra.cr., lar
phocytes that is most mtense in rhe pariero-occipital region
rhe slowly progressive adult form, adrenomyeloneurop(AMN), che main finding is a distal axonopathy rhat affects
long tracrs in the spinal cord. The inflammatory response s m
or absent.
PATH0GENESIS.he adrenal dysfunction is probably a direcr
sequence of the accumulatron of VLCFA. The cells in the z
fasciculata re distendedwirh abnormal l ioids. Cholesteroli6ed wirh Vl-.Cl'A is relativell resirtant o adrenocorlicothormone (ACTH)-stimulated cholesterol esrer hydrolases,this limits rhe capacity to convert cholesterol to accive srerln addition, C26:0 excess ncreases he viscosity of the pla
membrane and thrs may interfere with receptor and other c
lar functions.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 89/177
570 PARTX MeraholicDiseases
There is no correlation between the neurologrc phenotype and
the nature of the mutation or the selrrity of the biochemical
defecc as assessedby plasma levels o{ VLCFA or berween the
deeree of adrenal i nvolvemenc and nervous svstem involvement.
lhi severiryof the illnerr an d rareof progression orrelarewith
the lnlensltt/ of the inflammatory response, The inflammatory
response mav be cytokine mediated and may involve an autoim-
mune response triggered in an unknorvn way bv rhe excess of
VLCFA. A CD I l ip id anligen has been mplicared. Nlitochondr
ral damage and oxidatrve stress also contribute. Approximatelyhalf of the paciencsdo not expenence the inflammatory response.A modifier gene that sers he "rhermostar" for the rnflammatory
response s postulated.
CtlNlCAt MANIFESTATI0NS. here are five relatively distrncr phe-
notypes, three of which present in childhood r,r.ithsymptoms and
signs. In all the phenotypes, development is usually normal in the
1st 3-4 yr.
In the childhood cerebral {orm of ALD, sy-mptoms are 1st
noted mosl commonly between he ages f 4 and 8 yr (2 1 months
is the earLest onser reoorted). The most common initial manifes
tations are hvperactivicl', rvhich is often misraken for an artention
deficrt disorder, and u.orsening schooI performance in a child u hohad previotLsly been a good student. Auditory discriminarion is
ofren impaired, although tone perception ispreserved.
Thrs maybe evidenced by difficulty in using the telephone and greatly
impaired performanceon inrelligenceests n items that are pre-
sented verball,v.Spatial orienration is often impaired. Other rnrtial
symptoms are disturbances f vision, acaxia,poor handu,'rrt ing,
seizures, nd strabismus.Msual disrurbancesar e often due to
involvement of the cerebral cortex, which leads to variable and
seemingly nconsistent vrsual capacit;', Seizuresoccur Jn nearly allpalients and ma).represent he 1st manifestatronof the disease.
Somepatientspresent vith increasednrracranialpressure r with
unilareral mass esrons. mpared cortisol response o ACTH stimulation is present n 857o of patients,an d mild hyperpigmenta-
tion is noted. In most pariencs uith this phenotype, however,
adrenald,vsfuncion s recognized nlv afrer he condit ion s diag-
nosed because of che cerebral s,vmptonrs. Cerebral childhood
ALD tends to progress rapidly with rncreasing spasticity andparalysis, isual and hearing oss, and loss of abili rv ro speakor
su'allow. The mean rnrerval berv'een the 1st neurologic symDcom
and an apparentl,vvegetative state s 1.9 yr Patients ma1' conrm this apparentlyveg€talive tate or 10 yr or more,
Adolescent ALD designatespatients rvho experienceneurolsymptoms between he agesof 10 and 21 yr The manilesraresemble chose of childhood cerebral ALD excepr that prog
sron is slowerAbout 10% of patients present acuteJywith scatusepilepti
adrenal crisis, acute encephalopath,v,or coma.
Adrenomyeloneuropathy 1st manifesrs in late adolescencadulthood as a progressive paraparesis caused by long tdegeneration n the spinal cord. Approximately hali of palienls also have rnvolvement of the cerebral \,\.hltematter
The "Addison only" phenotype is an important and undiagnosed condrtion. Of male patients with Addison disease,2may have the biochemrcal defeccof ALD. Many of rhesepati
have intact neurologlc systems, *ereas others have subtle nelogrc signs, Many acquire adrenomyeloneuroparhv in adulcho
The term "asymptomaticALD" is applied o persons vho hrhe brochemrcal defecr of ALD bur are free of neurolosicenducrinedisrurhancqs,Nearly al l personr wirh the gene
-d
eventually become neurologrcalll' symptomatic- A few hremaned asymptomatic even in che 6th or 7ch decade.
Approrimatelv 50'o of female heterozlgotcr acquire adrome rhat resembles drenomyeloneuropachJut is mrlder
of later onset. Adrenal insufficiency is rare.
IAB0BATORY ND RADI0GRAPHICINDINGS. he most spe
an d rmportaor aboratory inding s rhe demonstrationoF ab
mallv high levels of VLCFA in plasma, re d blood cells , or
tured skin libroblascs.The test should be performed i
laboratory that has experience with this special ized proced
Positive results are obtained rn all male patients with X-ALD
in =85% of female carriers of X-ALD. Mutation analysis ismosr reliablemerhod for che dentif icatron f carriers.
CT and MRl. Parienls ,vrth childhood cercbral or adolesALD show cerebral *hite matter lesions that are characterrvith respect to locatjon and attenuahon parrerns on MRI
807o of parienrs, he lesions ar e svmmetric and rnvolv eperiventricular whire matter in the posrerior parietal and oc
tal lobes.About 50% sholv ocacionof a earlandof accumucon t ras rm a te r ia lad jacen f nd an te r ,o . , , t he po r te r ior h r
dense esions Fig. 86-.5,4). hi s zone corresponds o rhe zonc
Fisure86- i . ,4, Conuast enhanced t abmalitics in adrenoleukodrsrophy IALD)q'pical parietcoccipital location, shor.ing metric biJareral ypodense nactive zones H
The enhancing active periphery zone of hdensirv s demarcarcdby arrt*rs Conpareanterior zone of hvpodensry (drrouheads)
that on the MRI in B. CC, corpDs caLlosu
MRI oi the samepatternand area shown b,
NIRI T2 r,r'eighted nage shows a high-inte
signaL i rhe abnormall,vbrighr parieto-occwhite matter. Subcordcal nvolvement is b
identified on MRL SeparatronoI acrive z
ma_v e bener apprecJated y C! because
inacrive and acrive zonesare seenar high s
areasorr N'IRL k is assumed. ou'ever, hat
najor disdndions afforded hy CT rt'ill als
demonsrrablewhen IV enhancement prram
netic enhancement)becones readilv avail
Nore e },lpoden\e involverne|r of CT 1aheads^nd dttotus n A) .ompared !$rh rhe
resolved esioDs n MRI in B (From Kuma
RosenbaumWE. Naidn S, et al: Adrenoleuk
srrophy: Corresponding N{R irnaging srrh
Rad a ogt 19 /',165 497 504.)

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 90/177
incenseperrvascular l1'mphocytic infiltracion where the blood
brain balrier breaksdown. In 127o of patrents, he nrtial lesions
are irontal. Lnilateral lesions hatproduce a masseftect ugges-
tive of a brain lumor may occur. MRI provides a clearerdelin-
eation of normal and abnormal white matcer rhan does CT and
by CT (Fig. 86-58).
857o of patientswith the
evels of ACTH in plasma
an d a subnormalnse of cortrsol evels n plasma ollowing inrra
venous injectron of 250pg of ACTH
{Cortrosvn)
DIAGN0SIS ND 0lFFEBENTlAtlAGN0SlS The earhestmanifes-
rations of childhood cerebral ALD are diflicult to disringuish
from the more conrmon artentron deficir disorders or learning dis-
tarion during the neonaralperiod.
Cerebral orms of ALD mav presen!as increased ntracranral
pressureand unrlateral mass esions.Thesehave been misdrag-nosed as gliomas, even after brain biopsy,and severalpatients
have received radiotherapy before the correct dragnosiswa s
made. Measuremen!of VLCFA in plasma or brain biopsy speci
mens s rhe mo.r reliabledifferenriaring esr.
Adolescentor adult cerebralALD can be confusedwith psy-
chiarric disorders,dementingdrsorders, r epilepsy The 1s cclue
to the dlagno s of ALD mav be rhe demonstration of whicc
mafter lesions y CT or MRI; assaysof VLCFA are conlirmarorl'.
ALD canno be distinguished clnicaLly from other forms of
Addison drsease; t is recommended that assaysof VLCFA levels
be oerformed in al l male Datients ,rth Addison disease Al-D
parientsdo not usuallyhave anribodies o adrenal issue n their
plasma.
C0MPI-ICAT|0NS.n avoidablecomplication s the occurrence fadrenal Jnsufliciencl '. The most diflicult neurologrc problems are
those elated o bed resf,contracture, oma, and swallowrngdi s
turbances.Other complicarions nvolve behavioraldisrurbances
and injuries assocratedwith defeccs of sparial orientation,
impaired visron and hearing,and seizures.
TREATMENT, orticosteroid replacement for adrenal insuf6cienc;,
or adrenocorticalhypofunction is efleccive se eChapter -576). t
Eone Marrow Transplantation. one marrow transplantation
(BMT) benefits parients who shov early evidenceof th inflam-
macory demyelinarion that rs characteristi c of the rap lv pro-
gressiveneurologic
disability in boy and adolescents rvirh the
cerebral X-ALD phenotl'pe, BMT is high risk procedure, and
patients must be seleccedwith great care, The mechanism of
the benelicial effect is incompletely understood. Bone
marrow-derived cells do express ALD! the protein rhat is deli-
cienc n X-ALD; =507oof brarn microglial cel lsare bonemarrow
denved. It is possible that replacement of affected cells bv cells
that conrarn lhe normal genechanges he brain mtlteu suffrcientl;;
ro correct the brain merabolic disturbance. The favorable effect
may also be caused by modificarion of the brain inflammatorv
response. Five co 10 yr follow-up of boys and adolescents who
had earlv cerebral involvement has shot'n stabilizacion and, in
some instances, rmprovement. On the other hand, BMT has not
shown favorable effecrs n patients who had already severebrain
involvement and may accelerate diseaseprogression undet these
Chapter 6 r Defectsn Mol.holismof Lipids
circumstances. The nonverbal IQ has been found to be of
dictive value, and transplant is not recomnended in patients
nonverbal IQ significand,v below 80. Unfortunateh! in more
half the patienrs who are diagnosed becauseof neurologic sy
loms, the illness rs so advanced tha! they are not candldates
transplant.
Consideration of BMT is most rele\.anl in neurologic
asymptomatic or mildly involved patients. Screeningar-rrsk
tives of svmpromatic palients idenrilies rhese parients most
quenrly. Screening by measurement of plasma VLCFA leve
patienrs wrth Addrson disease may also idenr if,v candidace
BivIT. Because of rrs rrsk (10-20% mortality) and the fact
up to 50% of untreated patrenrs with X-ALD do not dev
inflammatory brain dem,veLinatron, ransplant rs not re
mended in patients who are free of demonstrable brain invo
menc.The MRI rs also of key rmportance for the crucjal dec
of *'hether transDlan! should be oerformed. MRI abnorma
precedeclinically evidenr neurologic or neuropsychologic ab
rnalitres. The brain MRI should be monitored at 6 mo to
intervals in neurologically asymptomaric boys and adoles
becrveen he ages of 3 and 15 yr, If the MRI rs normal, BN
not indicated. If brain MRI abnormalties develop, the pa
should be evaluated ar 3 mo intervals to determine if the ab
malicy is progressive, n combinacion rvith careful neurologic
neuropsychologrc evaluacionl and if earl,v progressive nvo
ment is conlirmed, transplanr should be considered.Mag
resonance pectroscopl improver the capacil\ lo derer
whether rhe brain involvement is progressive. It is nor kn
whether BN{T has a favorable effect on the noninflamma
spinalcord involvement n adults with the adrenomyeloneu
th y phenotype.
Lolenzosoi l Therapy. he administration of Lorenzo's o
asymptomatrc boys reduces the rrsk of developing the childh
cerebral phenocypeby a factor of two or more. Lorenzo(4:1 mrxture of glyceryl trioleate and glycer,vJ rierucace)
bined rvich a dietary regimen is recommended for neurologi
asvmDtomatic bovs rvho have a normal brain MRI and
younger than 8 yr'old, but must be supervrsedcarefully. Adr
funcrion and brain MRI must be monirored. Patients
develop progressive lvlR[ abnormalities are evalualed
hemaropoietic stem cell cransplant wheo changes are still m
early phase.Lorenzo's oil has not been shown to alter di
progression n patientswho alreadyhave cerebraI nvolvem
OtherTherapies. nterferon-p and immunosuppressive ther
have not been found to be effective. Therapies r.ith lovas
and with 4-phenylbutyrare have been proposed and are b
rested in clinical trials. Gene rherapy has shown promise in
tured cells and the mouse model of X-ALD buc is not yet a
able for human trial.SupporliveTherapy.The progressive behavioral and neuro
disturbances associated with the childhood form of ALD
exrremely difiiculc for che amill'. ALD patienrs require the e
lishmenr of a comprehensive management program and par
ship among the family, phvsician, visiting nursing staff, sc
authorit ies,and counselors, n addrtron,parenl support gr
are often helpful (United Leukodystroph,v Foundatron,
HighJand Drive, Svcamore, L 60178). Communicacion
school authorit ies s imporrant because nder rhe provisio
Public Law 94-142, children with ALD qualifv for speciavices as "other health impaired" or "mult ihandicap
Dependingon rhe ra!e of progression f the disease, pecialmrght range from relatrvely lowlevel resource se ices with
regular school program to home- an d hosprtal-based ea
programs for children who are not mobile.
Management challengesvary with the stage of rhe illness
early stages are characterized by subtle changes n affect, be
ior, and attention span. Counseling and communication
school authonties are of prime importance. Changes n the s
wake cycle can be benefited b.v the ;udicious use ac nigh

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 91/177
580 PABTX Metabolic isoaros
sedatives uch as chloral hydrate (10-50 mg/kg),penrobarbital
{5 me/ke), or diphenhydramine2-3 mglkg).As the leukodysuophyprogresses,he modulation of muscle
tone and support of bulbar muscular unction are malor con-cerns.Baclofen n gradually ncreasrng oses 5 mg bid to 25 mgqd) is the most effectivepharmacologic gent or che reatmentof acuteepisodicpainful musclespasms.Other agenrsmay alsobe used,wrth careberng aken o moni tor the occurrence f srdeeffectsand drug interactions,As the leukodystrophyprogresses,bulbar muscular control is lost. Although initially thrs can bemanagedby changrng he dier to soft and pureed foods, moscpatients eventually require a nasogastric ube or a gasrrost-omy. At least one third of patients have focal or generalizedseizureshat usually eadily respond o scandard nriconvulsantmedications.
GENETICOUNSETINGt{D PREVEI{TI0N.eneticcounselinsandprimarv and secondary rerentionof X-ALD are of ciucialimportance.Excendedamily screening hould be offered o allat-risk relatives f symptomatic arients;one program ed to theidentificacron f more han250 asymptomatic ffectedmalesand1,200 women heterozygous or X-ALD. The plasma assaypermits eliable dentificarionof affectedmales n whom plasmaVLCFA Levels re ncreased lreadyon the day of birth. Identifi-
cation of asymptomatic male5 permits instirution of steroidreplacementherapy when appropriateand prevents he occur-renceof adrenalcrrsis,which may be fatal. Nloniroringof brainMRI also permits rdentiEcation f patientswho are candidatesfor BMT at a stagewhen this procedure as chegreatest hanceof success. lasmaVLCFA assav s recommendedn all malepatientswith Addisondisease. -ALD has beenshown o be hecauseof adrenal nsufliciency n >25% of boys with Addisondisease f unknorvncause. denti6cationof womenheterozygousfor X ALD is more drfficuk than that of affectednales. PlasmaVLCFA levelsare normal in 1-f-20% of heterozygous omen,and ailure o nore hishas ed ro serious rrors n senetic ,.run-seling.f Vl CFA evels renormalborh n plasmalnd culturedskin frbroblasts, he risk of false-negativeesults s reducedbutnor eliminated.DNA analvsrsDermitsaccurate dentilicationof
carriers,provided hat the mutarionhas beendefined n a familymember. nd s cheorocedure ecommendedor the dentificationof heterozygouswbmen. Mucation analysis s available on aseffice basls.
Prenaral iasnosis f affeccedmale etuses an be achieved ymeasurementf VLCFA levels rr cultured amniocvres r chori-onic villus cells and by mutation analysis. Vhenever a newpacientwith X-ALD is identified,a detailedpedigree hould beconstructedand efforts should be made to identilr all at-riskfemalecarriersand affecredmales.These nvestigations houldbe accompanied y carefuland sympatheric ttention o social,emotional,and ethrcal ssues uring counseling.
Peroxisomal Disorders
Baumganner MR, Poll-The B! VerhoevenNM, et al: Clinical approach to
inherited peroxisornal disorders: A series of 27 pztients. Ann Ne rol
1998;44:720-730.
FerdinandusseS, Yliantrila MS, Gloerich J, et al, Mutarional speccrurn f D-
bifuncnonal protein deiciency and structure based genotypephenotype
anAlysis, ,r1 Hr'11 Geset 2006t78:112-124.
Maninez M. Pineda M. Vidal R. et a| Doco$hexaenoic acrd-A new thera-
peutic approach ro peroxisomal-disorderpatients: Exp€rience with two
cases.Nerlolos] 1993 4 1389-1397
NIoserHW: Genorypephenorypecorrelarions n disordersof peroxisone bio-
&enesis.Mol Genet Metab 1999;68,316-327.
Modey AM, Brites P, Gerez L, et al: MDrarional specuum in lhe PEXT gen€
and funcrional analysis of mutanr alleles n 78 parients with rhizomelic
chondrodysplasiapuncrat^ rype 1. ,1m J tu1ft Genet 2002;70:612424.
PreussN, Brosius U, BiermannsM, er al: PEXI mutarions in complem
non group 1 of Zellweger spec m patLentscorrelate rvirh seven
disease. Pediatr Res 2002;51,:706-714.
SteinbergS, Chen L, We, L, Moser A, er al: The PEx genescreen:Molecdiagnosisof peroxisome biogenesisdisorders n rhe Zellweger synd
spe.JJtm. Mol Genet Metab 2004.83252163.
Valter C, GoorjesJ, Moojjer P.{: Disorden of peroxisome biogenesis umutations n PEXI: Phenorypes nd PEXI proteln levels Am J H tft G
2OO1;69:3 48 .
WandersRJ, JansenGA, SkjeldalOH: Refsum disease, eroxrsomes nd
tanic acid oxidationi A review I Neurooathol Exo Ne
2001;60:1021-1031.
Adrenoleukodystrophy (X-Linked)
BezmanL, Moser AB, Raymond cV, er a| ,{drenoJeukodystrophy:ncide
new Duration fare, and fesulrs of extended amily screening.Azn Ne
200r;49:5r2-517.Boehm CD, Cuttins GR, LachrermacherMB, et al: AccurateDNA basedd
nostrc and carrier resring or X linked adrenoleukodvstrophy.Mo/ G
Meab 1999;66:128-136,
Kemp S, Pujol A, V/rrerham HR, et al, Xlinked adrenoleukodystrophvm
tion database: Rote in diagnosis and clnical correlations. Hun M
2001;18:499-5r .Moser AB, Kr€irer N, Bezman L, et al: Plasmavery long chain fatw aci
3,000 peroxisome disease patients and 29,000 concrcls. Ar'n Ne
1999;45:100-110,
Moser FIri(, Lo€s DJ, Melh€m ER, er al: X linked adrenoleukodyscrOvervrew and prognosrsas a tunction ol age and brain magnetic eson
irDaging abnonnali.y: A srudy involving f72 parients. Ne"rcpedia
20O0;3r:227 -239 .
Moser HW, Raymond GV Dubey P, AdrenoleukodysFophy: New approa
to a neurodegenerative isease.,JAMA2005j294:3131-3134.
Moser H\v, Raynond CV, LD SE,er al, Follow-up of 89 lnrenzo's Oil tre
asymptomaric adrenoJeukodysrrophy parients. Arch Ne
2005j62: l073-1080.petersC, CharnasLR, Tan Y, et ai, Cerebral X linked adrenoleukodystro
The inte.national hematopoieticcell transplanlation experience rorn 1
to 1999.Blool 2004;104:881-888.
SrephensonDJ, Bezman L, Raymond GV Acute presentarjono{ childh
adrenoJeukodystrophy. ewopedia*i.s 20003r:293-297.
Van Geel BM, AssiesJ, Haverkon EB, et al: Prosressjonof abnorrnaliri
adrenornyeloneuroparhy and neurologicallv asymptomatic X-lin
adrenofeukodystrophydespite treatment ivirh "Lorenzot oil." J Ne
Ner/osarg Psychiatry 7999,67 290-?99.
86.3. orsoR0EBsFLlpopfiorElNEtrsor-rsnrNTRAt'rsPoRrWill iamA. Neal
EPIDTMIOTOGYF TOODIPIDSNDCARDIOVASCUI-ARISEASE
The relationship betweendietary fat consumprionand placholesterolwas demonstratednearlJ'a century ago. ! ellAmericans ad higher atesofcoronary heartdiseaseCHD) tDostlr.arEurooeanswho subsisred n limited rations.The Se-ountries Studyof geographic, ocialclass, nd ethnicdifferern CHD around the world found strong associations etwaveragentakeof saturated ats, plasmacholesterol, nd mority from CHD. In 1950, the mear total blood cholesrerol eamongAmericanse'as 20 mg/dl. By 1991, che eveldeclinea mean of 205 mg/dl-.
ln 1977, the Cooperative Lipoprocein Phenorl'prngStshowed chat her€ s an inverse elationshipbetweenHDL CHD. Clinical trials of dietary and drug inrerventionsdirecowardmodulation of cholesterol evelswere begLrn uring1970s, ultimately providing rhe basis or screening nd trement standardsas promulgated by the National Choles

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 92/177
Educarion Program (NCEP). l'urther refinement of the molecu-
lar basis of l ipoprorein merabolism has better characterized
phenotypic aboormalit ies an d more directed inrerventional
sffategte
Of all ommon chronic diseases, one is so clearlv nfluenced
male gender, hough it is increasrngly apparent that hearr disease
is under recognized in women. Tobacco use confers a twofold
higher liferime nsk. Sedentary activiry and high intake of satu-
rated fats, leading to adrposity, increase risk through differencesin th e plasma evelsof hpoproreins hat ar e atherogenic Famil,v
history is a reflecnon of the combined rnfluence of lifescyle and
geneticpredisposit ion o earlv hearcdisease.Risk of premature
heart disease ssociated it h posirive amily historJ is 1.7 trmes
hieher rhan in families with no such histor,v.
The pathogenesis of atherosclerosis begins durrng childhood.
Korean and Vietnam war casualties rvere noted to have surprrs-
inglv advanced afty streak rn dplaque ormati.,n rn rh ecoronarr
arieriesan d aona. Th e lohn' Hopkinc PrecursorrStudv demon-
srraced that white male medicaLstudents with blood cholesterol
levels in the lowest quartile showed only a 107o incidence of
CHD three decades ater, whereas those in the highest quartile
had a 40% incidence. The Pathobiological Determinants of
Atherosclerosisn Youth (PDAY) Srudy demonstrateda signi6-
canc relarionship berween tbe weight of the abdomind lat pacl
and the extent of atherosclerosis found at autopsy on subiects
15-34yr of age. The BogalusaHeart Study of >3,000 black
and whire children an d adolescentsha s provided the most
comprehensive longitudrnal data relaring the presence nd
severicy of CHD risk facrors wirh semiquantiliable severi of
arh€rosclerosrs,
Th e "feral originshvpotbesis" s basedon rhe observation ha r
babies born wrth lorv birthweight have a higher incidence of heart
disease s aduhs-Epidemiologic tudies upPorr he dea hat pre-
natal and earlv poscnatalcondit ions ma v affecr adult health
starus. Children *'ho are large for gesratiooal age at birch and
exposed to an intrauterine environment of eirher diabetes or
maternal obesicy are at increased nsk of eventually developing
rhe "metabohc syndrome" (insulin resistance,yp e lI diabetes,
obesrty, CHD). Breasc-feeding preterm infants confers a long-
term cardioprotectivebenelit 13-16 yr laret. Those adolescents'w.howere breasr-fedas infants had lower C reactive prorein con-
centratiors and a 141" lower LDL to HDL ratro compared to
those fed infant formulas,
Poverty is also associatedwirh numerous negative health oLrt-
comes. The Younq Hearts Proiecc n Northern I reland has shown
rhat behavioral ;isk factors are influenced bv socioeconomic
status. and they are well established by adolescence,even rhough
no biologic differences are apparent.
Chaptei 6 r Delectsn Metabolism l Lipids
ETOODIPIDSITD IHEROGEI{ESIS
Numerous epidemiologic rudres ave demonstrated he ass
tion of hypercholescerolemia, reierring to elevated total b
cholesterol, rvith atheroscleroric disease.Advances in clinical
oratory rechniqLres or measurement of orher selected ipopro
parricleshave increased ur understanding f the role of b
lipids in relation to hearr disease. he ability co measure
components wirhin classesof lipid parhcles, as $'ell as mar
of rnflammation,have further elucrdared he processof ath
genesis nd plaque upture leading o acutecoronary syndro
Atherosclerosis ffecrs primarily th e coronary arteries but
often involves the aorta, arreries of the lower extremities,
carotid arteries.
The early s tage of development of alherosclerosisrs choug
begin with vascular endothelial dysfunction and intima rn
thickness, which has been shown to occur in preadolescent
dren with risk factors such as obesity or familial hvperch
terolem,a. The complex process of penetration of the int
lining of the vesselmay be due to a variety of insults, inclu
the presenceof highly toxic oxrdrzed LDL particles. Lymphoc
and monocytes perterate the damaged endothelial lining, rv
tbey become macrophages laden wrth LDL lipids and
become foam cells. Such accumularron s counterbalance
HDL partrcles apableof removing iprd deposicsrom tbe v
wall, Fundamental to plaque formatron is an inflamma
process elevatedC-reaciiveprotein) nvolving macrophage
ch earrerialwall. Th e deposit ionof l i pid withrn the subend
lial l ining of the arterial wall appearsmacroscopicallyas
screaks,'hich ma y to some degreebe reversible.A later sra
plaque developmenr involves disruption of arterial sm
muscLe ells stimulated by rhe releaseof t issue cytokines
growrh facrors. The atheroma is composed of a core of fatty
stance eparated rom the lumen by collagenand smoorh mu(Fig. 85-5). Growth of the atheroscleronc laque mav resu
rschemia of the tissue supplied by che arcery, Chronic inflam
tion within the atheroma, perhaps caused by infectrous ag
such as Chlamydn pnebmonite, results rn plaque inslabiliqv
subseouen! ruoture. Placeletadherence eads to clor formatio
the sire of rupture, resulting in myocardial infarctron or a c
Dtovascular venl.
PTASMA IPOPROTEINETAEOTISMIfOTRAI{SPORT
Abnormalitres of liooorotein metabolism are associatedwith
betes mellitus and premature arherosclerosis, ipoproteinsoluble complexes of lipids and proteins rhar effect transpo
fat absorbed from the diet, or syorhesjs by the liver and adi
Adventitia
fisurc 86-6. The early stage oI developrnentof
atheroscle.osisbeglns rvrrh penetrarion of rhe
incimal lining of rhe vessclbv innamDitory ceLls
Deposrtion of lipid {jthin the subendothelial
Lrnrng f the artcrial *'all e"entualty leads o drs-
ruprion o{ smoochmusclecells co form an sthero
matous hpid core thar impitges on the lumen.
Chronic inflanmation leads ro plaque instabilitv,
setring he srage or plaque rupture and complete
occiusionoi the vessel umen by clor lormahon
Monocyte/Macrophage
lnt ima
Tunica medra
Subendlayer
Endolheli
Lipid core

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 93/177
Ei
582 PABT . MetabolicDiseases
tissues,or utrlizationand storage.Dietary ac s transportedromthe small ntestine schylomicrons. ipids synthesizedy the iverasvery ow densrty poproteins VLDL) are catabolized o inter-mediatedensity ipoproteins IDL) and low-density ipoproreins(LDL). High-density lipoproteins (HDL) are fundamentallyrnvolved n VLDL and chylomicronmerabolism nd cholesteroluansport, Nonesterifiedree atty acids FFAs)are metabolicallyactive lipids derived from lipolysis of triglyceridesstored inadipose issuebound to albumin {or circulation in the plasma
(Fie.86-7).Lipoproteinsconsrst f a centralcoreof triglycerides nd cho-
lesteryl sters CE)surrounded y phospholiprds,holesterol, ndproteins Fig.85-8).The densityof the several lasses f lipopro-teins s inversely roportional o the rario of lipid to protein (Fig.86-9) .
Phospholipid
Figule86'7. The exogenous, ndogenous, nd reverse hole
pathways. The exogenousparhway transports dietarl far
rhe small intesnneas chylomicrons o rhe peripheryand the
The endogenouspathway denores the secretion of verldensiry ipoprotein (VLDL) from rhe liver and its caraboli
inrermediaredensity lipoprotein (IDL] and lo$ density lipo
tein (LDL). Trigiyceridesare hydrolyzed frorn rhe VLDL pa
bythe action oflipoprotern lipase LPL)in rhe ascular bed,ving free fatty acids (FF.\s) or utilization and storage n m
and adipose rssue.Hish-densiry lipaprotein (HDL) merab
is responsible or the transporr of excesscholesterol from
perlpheral cissuesback to rhe liver {or excrerion in the
NascentHDL-3 particlesderived from the Lver and small i
dne are esteriied to more macure HDL-2 parriclesby enz
mediaced novemenrof chvlomicron and VLDL into the
core, n'hich is removed rom the circularion by endocvtosi
Constiruent roteinsare klown as apolipoproteins Table7). They are responsibleor a variety of metabolic unctionaddition o thefuscructural ole, ncludingcofactorsor inhibof enzymatic athways,and mediatorsof lipoprotein bindincell surface eceptors.ApoA is the major apoliprotein of HApoB is present n LDL, VLDL, IDL, and chylomicrons.Ap100 rs derived rom the liver, whereasapoB-48comes iomsmall ntestine.ApoC-I, CJI, and CJII are smallpepcidesmtant ir lriglyceridemerabolism. ikewise,apoE,which rspre
in VLDL, HDL, chvlomicrons, ndchylomicron emnants,an important role in the clearance f triglycerides.
Uuerterifiedcholeslerol
1 20
1 1 0
1.06
1 .O2
1.006
1.00
E
'a
c
oo
#HDL
5 1 0 2 0 4 0
APOB-100
Low-Density ipoprotein
Figure 86-8. Schematicmodel of low-density ipoprotein (LDL). Lipoprotein
consistsoI a central core of cholesrerylesrers, urrounded by phospholipids,
cholesrerot. nd Drorein.
80 1
Diameter, m
Figure 86-9. The densir-v f the severalcLassesf lipoprotein is inversely
portionat ro th€ ratio of lipid to protein. As lipid is less dense ban pro
rhe more lipid contained in the parcicle ncreases ts size and decreas
density. HDL, high-densir.vpoproteinj LDL, lorv-densiq' lipoprotein;
int€rmediatedensity ipoprotein; VLDL, very low densitl lipoprotejn.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 94/177
Chapter 5 . Defectsn Metabolism f Lipids
(oMPO$Tn
LIPOPROTTIN-
I|llomoo15
[hyom n remfan$
ttD-rD lLlt
HDt
$unclrte$ e[hylomkonrLivetifienineVLDI!tDr[iwr,ntenineLDLthylol|]i(ont
'i po!rteB.rn! q Df ertn 0E of
ft{, hqh.lenlry p0prctn Dl, rFrmed ledmr y Fpnir n;LDl,0w le$ ty poprrtn]VLDt,?ry o,,v enritvQopote
LIPIO
98-ts9 l %909l89194l-68
AP0umPRoTgt{5
( , i , t I , ,A ,A ,AB48,tI J . [ , t , t ]
3100l-,r- ,A-r\r,a , D
srorage n rnuscleand adipose issue.Hvdrol,vsrs t =80% o
TG presenc n VLDL perriclesproduces f)l- partrcles onta
.ur equal amounr of cholesterol nd TCI-The remarning en
IDI- is conr.erted o I I)L h)r deliverr ro pcripheral issueso
rhe liver.ApoE is artacheclo the reulnant DI- particle ro a
l. inding to the celLan d srLbsecluentncorporacion nro rhe
some lndividLralswith deficienc,v f eicher apoE2 or he
trigl'ceride lipase HT(iL) accuntulereDI - in rhc plasma.
I DI particlesac.olrnt for =709i, oi thc plasma choleste
normal jndividuals. l.Dl reccprors re presentoD the surfac
Lre.rrly l l cells.N' losrLDL rs taken up b,v he liver, and rhe
is rrrnsported ro peripher'alissLrcsuc has the adrenalglandgonrds iol steroid synrhesis.Dlslipidcmia is grearlv rrf lue
bi LDL-R activirv The cif iciencvu' irh rvhichVLDL is conv
t r r r r , D l r s . r l . o m p n r t , t n rr r r p r . l , ' n t e o s r a s i ' .
HD LAN DREVEBSEH0LESTER0tRANSP0RT.s hcparicsecr
of hpid parricles nto ch e bile is rhe onll mcchirnisrn v u
cholesterolcan be removcd fronr rhe hodv. lransporr of e
cholesrerol rom the peliphcral cclls rs a r.rtall,vmportent
t ion of IIDL. HDL is hcavil-v aclenq.rth apo,A. conra
lLp.opr,rceins,vhrch rs nonarherogenrcr contrast to B llp(
rcins (iholescerol-por)r irsacntHDI- parricles secrefedby
lrter end small nrestireare esterii ied o more nratr.rrc DL-2
riclesbv rhe actiorrof rhc cnzvnc leci rhin-cholesrerol cyL
tcrasc L(lAI). u'hLch .rcrlitaresnorernenrof chvlomicron
VLDL rnto the HDI corc. HDL-2 mav trarsfer choLesrcrybacl to lpoB lipoproreiLrs redilted bv cho)estcryl ster ra
proteir (CE1P), of the cholcsteKt-richparriclenay bc rcrn
irrm rh e plirsnrahy endocytosis. omplering reverscchole
rrrrrl port.Low I ID L rnai be gerrericdeficcnc,v apoA-I) o
ondar. to i ncreased lasna TCi.
HYPEBLIPOPROTEINEMIAS
HYPERCHOLESTEBOTEMIATABLE6.8)FamilialHypercholesterolemiaFH). H is a monogenrc u
nal co dominarrrdisordcrcluseclb,v nurarions ffecting he
SlZt(nm)
i301,20010 1t0l0-8025-3518255)0
DtNtlIY9/rrLl
<095<t 01106095-10C6r11x-r 191019 061I 125 r0
PR()IAN, : l
6"87,10't l
)1t2 57
TRANSP0BTF EXOGENOUS0IETARY)lPIDS All dietarv iar rvith
th c exceprionof r uedium-chain riglycendes s cflicieLlrLt rrried
tissuc. Free fattv acids are oxidized. resterif ied br storage as
the chylolnicron, apo(i parrrcles:rre ecirculatedLrack o HDL
Thc subsequcnr oltribr.rriol of apoE from ll l)L to the re rli lnr
meal, an exceptionbeing ndividuals with a disorderof chrLomi
cron rnetabolism.Posrprandial vperlipidemras a risk frcror ior
arhrrosclerosis. bnormal transport of chvlomicrons an d therr
ren'rnantsra v rcslrLtn their absorpfion n() rhe blood ves.cl.vll l
as oam ccLls. ausecl v rh e rngescion f CF-bl macroPhlges, he
carliesrsrirgc n rhe developrnenr i fatt,vsrreaks
TBANSPORT0FND0GEN0USlP lDS BOM HE IVEB ' fhe k r r rn r
t ion and secretiorr f VLI)1 frrrm the liver dnd irs carabolisnr rr
IDL and I-DL parrcles des.ribe lhe eldogenous lipoprorcirr
path\\ 'ay.Fatq- acicls rsecl tbe hepatrc brmation ol ! ' l Dl rrc
ancl r consrsts f trglyccricles, holesrervl srcrs, hospholipicls.
and apoB 100. Nascentparnciesoi \rLD[- secrccd into rhe cir-
culatit>n ombrne r' ich llo]iprorei
Vl-DI particle is dctermineJ l.tr
prcsent,prrrgrcssivel,vhrinklng rn
th e :rctiorl oi l.PL. yielding frcc
imi ahypercho5lerolemi,rimiial, lele(veApoB00Autosomrcces5i\€yp.orch0l€5tercleitDSltoiteroemhlyqenhypedohneonEtunllaombinedyperlipldemt(HL)
fam lal $betalipoproteinemiafuflrdl h.v mrunerniaFreder(ksonrypeFamilqpertrI re.idemiaFrc,ieftksonype V)fumi lhyperlry.eddemiaFredericKonype lfumil lhecircpaseefeicy
11!04
t l tai ] i l
< N.llll,i)0-i)
<ti I,llll:l. ll
t i ! '
t// lut/ 'I],]clt'/"ll0,llll:l' /5l l
< r ill!',l la
L}L
L]L
Llrl
LD L
LDtLDL,TCtDt,r.GrctT16116ttVtDL
Tendonanthorna5,I|JtTendonanthomas,I|1DTendonaflhomrs,l-|1D.Iendon
)(dnrhomas,IHDtf D(rlD
iubaerupliveanthoma5,eripheraa5curdisea5eirupnveanth0,Ta5,ep,rtorpn0meqaly,,rncredt5l(l]ihnlh|rmast{HDi|])
ADAD
ADAD
ADADAF
AD, iu|05omadonnant ,Afa! Io9m.rResve]LH! , r0r0| ' ] r iedl |df3R]LJ i ,0wnel l5 ly |pDEm, I6, l f ) f

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 95/177
584 PARTX Metaboliciseasss
Figure 6 10. Achillesendon anthoma hererozygousamilialhypercholes-terDlemia).FromDurringtonP: Dydipidaemia. an.et2O03;j6Z7l7-731.1
receplor. ft is characterized by strikingly elevated LDL cholesterol, premature cardiovascular disease,and tendon xanthomas.
Molecular studies have identified five classesof mu!ations affect-
ing the ability of LDL cholesterol to bind with the LDL receptorOf the nearly 800 murations described, some result in failure of
syflthesisof rhe LDL receptor (receptor negative) and orhers cause
defecrive binding or releaseat the lipoprotein-recepror rnterface.
Receptor negative mutations result in more severe phenotypes
than recepror defecti ve mutations.
HomozygousFH. FH homozvgotes inherit two abnormal LDL
recepror genes! esulting in markedly elevated plasma cholescerol
levels ranging between 500 and 1,200 mg/dl. Tnglyceride levels
are normal to mildly elevated, and HDL levels may be shghdy
decreased. he condit ion occurs n 1/1,000,000persons.Receptor negative palents have <2o/o rrortr].al LDL receptor activ ir,v,
whereas those who are receptor defective may have as much 257o
normal activirr and a bener prognosi(.
The prognosrs rs poor regardless o{ the specific LDL receptor
aberration, Severeatherosclerosrs nvolvins the ao.tic roor andcoron.rryarreries r pre\ent by early ro mid-;hildhood. These hil-
dren usually present with xanthomas, which may cause hicken-
ing of the Achilles tendon or extensor tendons of the hands, or
cutaneoLrs esions on che hands, elbows, knees, or br:trocks (Figs,
85-10, 86-11, and 86-12). Corneal arcusmav be presenc. amil,v
Fisure 36-11. Srria€ palnar xanrhomata. (From Dulljngron P: DysliFi-
daemia Lancet 2003;362:7L7 7 37.)
history is informarrve becausepremature heart disease s stronprevalent among relatives of both parents, The diagnosis may
confirmed bv measuring LDL recepcor acivity in cultured s
fibroblasts. Pheoo4prc expression of the disease may also
assessedby measuring receptor activity on the sulface of l)phocytes bv using cell sorting technrques.
Untreated homozygous patients rarel_r- urvive !o adultho
S;rmproms of coronarv insufficiency may occur; sudden deat
common. LDL apheresis o selectively emove LDL particles fr
rhe circularion is recommended for many children and has bshown to slow the progression of atherosclerosis. I-iver t raplantation has also been successful n decreasing LDL cholest
lerels. but complicarions related ro immunosuppression
common. HMG CoA reductase inhibitors are ofren effec
depending on the specific class of LDL receptor defecc presCombination therapy with ezetimibe, selectively blocking cho
terol adsorption in the gut, usually results in further mod
decline in LDL levels; t has largely replaced tbe use of bile a
sequestra11ts.
Heterozygous H.Heterozygous FH rs one of the most comm
single gene mutations associared with acute coronary syndrom
and atherosclerotic CHD in adults. Its prevalence is =1/500 in
viduals worldwide, but the frequeoc,vmay be as high as 1/250
selected popularions such as French-Canadians, Afrikane
and Christian Lebanesedue to the founder effect of unique n
mutatio11s.Heart disease accounts for more than hall oi all dearh
Western society, The pathogenesis of CHD is both environm
Figure 86-12. F,ruptivexanthomata Dn ertensor surftce of forearn. lFDurrington P: Dyslipidaemia.Lakcet 2003;362:717-731 )

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 96/177
Chrlter 06 | Dolocls n mdabolism ol LiDidsr
An estimated10 million peoplehave FH worldwide. Symptoms
of CHD usuallyoccurat themeanageof 45-48 yr in males,and
a decadeater in females,
oarenta hypercholesterolemia. Plasma evels f LDL cholesterol o not allow unequivocal
Holland. The diagnosiswithin well-definedFH families s pre-
ability of FH, verified by molecular genetics,s derived frorn
a U.S. population cohort and may not be applicable o othercounttles.
(LDL-C155 ngidl).Treatmentof childrenwith FH shouldbeginwith a ratherrig-
orous low-far diet (see ater). Diet alone s rarely sufficient or
decreasing lood cholesterolevels o acceptableevels LDL-C
<130 mg/dl). The Expert Panelon Blood CholesterolLevels nChildren and Adolescents (National Cholesterol Educarion
by 20-30 mg/dl. Thismedicationhasnot beenevaluated y c
trolled clinical trials n children.HMG CoA reductasenhibihave become he drug of choice or treatmentof FH becautheir remarkableeffectivenessnd acceptableisk profile, Tis sufficient linical experience ith this classof drugs n chilro document hat they are aseffective n children as adults,the risks of elevated epaticenzymes nd myositisare no grethan in adults(seebelow).
FamilialDefective poB-lm {FIIE}. DB is an autosomaldonant condition that is indistinguishablerom heterozygouLDL cholesterol evels are increased, riglyceridesare noradults often develop endon xanthomas,and premature Coccurs.FDB s caused y mutation n the receptorbinding e
of apoB-100, he ligand oI the LDL receptor,with an estimfrequency f 1/700peoplen Western ultures. t is usuallycaby substitutionof glutamine for arginine n position 350apoB-100,which results n reducedability of the LDL recero bind LDL cholesterol,hus mpairing ts removal rom theculation.Specializedaboratory estingcan distinguishFDB fFH, but this is not necessary, xcept n research ettings,treament is the same.
Autosomaliecessiye yp€rchol€stsrolemiaARH}, his rare dition, caused y a defect n LDL receptormediatedendoclin the liver, clinically presentswith severe ypercholesteroat levels ntermediateberween hose ound in homozygouheterozygous H. It is dispropoJtionately resentamongdinians,and s modesdy esponsiveo treatmentwirh HMG reductasenhibitors.
Sitosterolgmia. rare autosomal ecessiveondition charaized by excessiventestinal adsorption of plant sterols,sterolemia s causedby mutations n the ATP-binding castransportersystemwhich is responsible or limiting adsorof plant sterols n the small ntestineand promotesbiliary erion of the small amounts adsorbed,Plasmacholesterol emay be severely levated,esulting n tendonxanthomasandmature atherosclerosis. iagnosis an be confumedby meing elevated lasmasitosterol evels,Treatmentwith HMG reductase nhibitors is not effective,but cholesteroladsorinhibitors such as ezetimibe and bile acid sequestraneffecrive.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 97/177
586 PABT r MetabolicDisoases
small effects of many genesare impacted b; environmental rnflu-ences (diet), Plasma cholesterol evels ar e modescly elevated;triglvceride levels are normal. Polygenic hypercholesterolemiaaggregates rn families sharing a comrnoo lifestyle but does notfollow predictable hereditarl' pafterns found in single genelipoprotein defects,Treatment o( children with pollgenic hvper-cholesterolemia is directed tou.ard adootion of a healrhv liFescvle:reducedo ta land \ f l t u ra ted at on rum p t ro r r nd a t l ea r t h i , ' fphysical activitl, dail;'. Cholesterol lowering medication is rarelynecessal)'.
HYPERCHOI-ESTEROIEMIAITH YPERTRIGTYCEBIDEMIAfamilial onbinedyperlil idemiaFCHI).hi s s an autosomal
dorninant condition charactenzed bv moderate elevation inplasma LD L cholescerol nd trrgll.c erides, nd reduced plasmaHDL cholesterol. ft is the most commol primary lipid disorder,occurnng rn =1/200 people. No single metabolic aberration hasbeen identilied linking FCHL wich atherogenesis, but it is rvelldocumented thac =20o/. of individuals who develop CHD bvo0 ' r o i aHe ha re FCHL . fam i l r h i s ru r ' ' , f p rem aru rehea r rdisease s t,vpically posrtrve; the formal diagnosis requir€s that atleasc $o lirsr-degree relatives have evidenceof one of three r.an-anrs of dvslipidemia: (1 ) >90th percentilepLasmaLD L choles-rerol; (2 ) >90th percentiLe-DL cholesterol nd trigll icerides; nd(3) >90tb percentile rngl,vcerides. Individuals su.irch from one
phenotype to another. Xanthomas are not a feature of FCHL.Elevated plasma apoB levelsrvith increasedsmall dense LDL par-
t icles support the diagnosis.
Chrldren and adults with FCHL have co existing adiposi4.,
hypertension, and h,vperinsulinemia, suggesting the presence ofthe metabolic syndrome. Formal diagnosis of this multipler s,vn-drome as defined bv the NCEP's Adulr Treatment Panel III {ATPIII) idenrifres six major components: abdominal obesicl', athero-genic dyslipidemia, h1'pertension, insulin resistance w.ith orwirhour impaired glucose olerance,evrdence f vascular nflam-mation, and hvpercoaguabiliry t is escimatedhar 30% of overweight adults fuliill criteria for rhe diagnosis of metabolicsyndrome, including rwo rhirds of those rvith FCHL. Hispanicsan d South Asians from rhe Indian subcontinentare especially\ u \ cep th le .
The mechanisms associating visceral adiposity with che nera-bolic s,vndnrmeand type II diaberes are not full,v understood. Aplausrble unifying principal is that obesiry causes endoplasmictetrculum scress, eading to suppression of insulin receptor sig-naling and thus insulin resiscanceand heightened inflammatoryresponse. Hor,! thi s relaces to atherogenesis is unclear lt rsassumed that hypcrcholesterolemia and, rvith less certainty,h-vpertrigl;-ceridenia confer risk for cardiovascular disease inpatients wrth FCHL. When features of rhe metabolic syndromeare ncluded in logistic modelssharedenologrc earuressuch asincreased isceraladiposir,v ecomeapparent.Visceraladrposityincreaseswith age and its importance in chrldren as a risk facrorfor heart disease nd diabetes s Lmired by th e relative paucrtyofdara. Though longicudinalmeasurement f lvaist circumferenceand rhe presence f incra-abdomrnalat as decermined v MRI is
being conducred n tbe research etcng, body mass ndex (BMI)remains the surrogate for adipositv in the pediatric clinicalsertlne.
The metabolic syndrome is a dramatrc illustrarion of che nter-accion oI generics and rhe environmenc. Geletrc susceptibilit,v sessenrial s an exolanation tbr Drematureheart disease n ndi-
viduals rvith FCHL. Unhealthy lifesq,rle,poor diet, and physicalinactivity contribute ro obesitl and atrendant features oi themetabolic syndrome,
The cornersconeof management is lifesc_vlemodificatron. Thisincludesa diet low rn saturated ats, trans fats, and cholesterol,as well as reduced consumption of sirnple sugars- Increaseddietary rnrake of fruits and vegetables s importanr, as rs t hr ofmoderate phvsical accivitv darly. Compliance among children and
their parents is ofcen a problem, but small incremencal stepmore likely to succeed han agglessivew.eighcJoss rrategiesverv importanc that the child's caregivers partrcrpate inprocess.Plasma rrigl,vceride evels are usuall,vqurte responsidietary restriction, especially reducrion n the amount of srened dnnks consumed. Blood cholesterol levels mav decrea
Fanilial DysberalipoproteinerniaFDBL, ype ll Hyperlipopromia).FDBL is caused y mLrtationsn th e gene or apolipopr
E (apoE), rvhich when exposed co environmental influencesas high fat, high calonc diet, or excessrvealcohol inrake, rein a mixed rvpe of hvperlipidemia. Patients cend o have elevplasma cholesteroLand trigl,vcerides o a relativelv similar deHDL cholesrerol s rypically normal in conlras! !o orhet caof hvpetriglyceridemia associated u.ith low HDl,. This rareorder affecrs=1/10,000 persons-ApoE mediates emovaL f lomicron and \rLDL remnants from the circulation bv bindinheparrc uriace receptors- he poll m.rphic apof g"n" .*pr.in three isoforms: apoE3, apoE2, and apoE4. E4 is che "normallele present in the majority of rhe population. The a1isoform has lower affnic,v for the LDL receptor and its frequis =7%. About 1% of the population is homozygousapoE2/E2, che mosr common mutarion associated with FDbut onl,v a minority express rhe disease.Expression requires
crpitating iJlnesses uch as diabetes,obesity; renal drseashvpothyroidism. Indir.iduals homozygous lor apoE4/E4 arrr:k for l are-onset lzheimer disease.
\Iost parrencs .irh FDBL present n adulthood wirh distincxanthomas. Tuberoeruptive xanthomas resemble small grape
clusters on the knees, burtocks, and elbows. Promrnent orare l low d rsco lo ra t ion f the c rea ' e ' o l rhe hands pa lm arthomas) s also ypicallypresent.Atherosclerosis, ften presewith peripheral vascular disease,usuallv occurs in che 4rh ordecade,Children ma;''present u.ith a Less iscinctrve ash and erally have precipitatrng llnesses.
The diagnosis of FDBL is established by lipoproteJntrophoresis, r'hich demonsttates a broad beta band conrairemnant Lpoproteins.Direct measuremenr f VLDI- by ulcratrifugation can be performed in specialized ipid laboratorie
VLDL/total triglyceride ratro >0.30 supports the dragnosis. Agenotyping for apoE2 homozygosity can be performed, conling rhe diagnosis in rhe presenceof the distinctive ph1'sical
ings.A negative esuk does ro! necessarily ule out che disa \ o ther mura t ion \ in aF ' , f m av caL r \e \ en m ore semanilesrations.
PharmacoLoeic reacmenco1 FDBL is necessarv o decreasl i ke l ihood f . i rp ,o - rL ' . a the ro \ c le ro \ i sn aJu l r \ . HM C (
reductase nhrbitors,nicotinic acid, and f ibraresare all effecFDBL is quJrc esponsive o recommendeddietary rescrictio
HYPERTRIGIYCEBIDEMIAS.he familial disordersof crielvcer i ch l i pop ro te in , nc lude , r t hcommon and ra re v . r r ian r , lFrederickson classification sysrem. These include chylomicromi a (rype ), famrhalhypertriglyceridemiatvpe V) , and chem
severe combined h,vpertriglyceridemia and chylomicrone(t,vpeV). Hepatic lipase (HL) deficiency also resulrs Ln a simcombinedhyperlipidemia.
tamilial ChylonicronerniaType Hyperlipidemia}.hrs are sigenede lec t , i kc f am i l i a lh lpe rcho les t c ro lem ia ,' du r r ' , mtions a{fecting clearance o{ apoB-contaimng lipoproteins. Dciencv or absenceof lipoprotein lipase (LPL) or i ts cofaapoC-ll, which facilitates lipolvsis by LPL, causes severe elrion oi crigllceridenc h plasma chylomicrons.HD L choleslevelsare decreased. s clearance f theseparticJes s markdela,ved, he plasma is noted to have a rurbid appearanceafter prolonged asrrng Fig. 86-13). Ch,vlomrcronemiaauseLPL deficrency is associated wlrh modesr elevation in trigerides. u.hereasrhis is not the case vhen rhe cause is deficien

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 98/177
Chapter36 Deleclsn MetabolismfLipids
c\ac\! i\ c corrsLtrn|i{Jnoi io(1.1fr(l ()thcr !r 'cctcrlccl lr inkr,r i c ( ) 1 i1 r ( ) I lo en . ( )L ln f r r aop lc h ( r ( l . rnL L rpe rs izcdr iL
r r ru l rp l c 2 oz r ' r r r s i : t ce rcnc . l rL r jnk . . r i l r ' l cssenono f
l)r.r.f.c'()itcn resLrlrs]l drrnritre fa L rr rigl-vcerideevclsas
.' . i \ \ 'crghf l rrron!l hose who .trc oltcsc. lDL cLlrlcstcrol
\ \ r l f r nJ t o r i scas l \ ' l l s t aL r i l i zcs
l)cil irtr ic dise:rsesdssocirteJ *itI hvperlipidenri. inc
h r po th r o ic s r l , neph ro t i c v r r c i ro r r ra .i l i a rv a r res ia , l , v
\ror ,rtc diseirse,Nienrann-l\ck cliseitsc. .rv'Sechs liscitsc
fcl)ric lI l-\LrservtherndtosL]s! epanris, lrtcl artorcxie Lre
i l . r l , l L r> l { ) ) .( . c r reLnm ed ica r io rs cx i r ce rh r teh rpc r l i p rde r l r r , r c l r
rsorrerinoin ,Accutanci. hiezrLlc iur crics, ()r.t l cof frirccfrrcroidr, j3 blockers. rrrnrurlo\Lrppressi s. xnd pro
nhrl-.Ltorsse(l in th c trcaoncnr ol HI\ i
Ire.rrnrcnr f hyl-ertrgLr crirlcnri,r Lrchrlclrcrr ereh re(l
nrcrll. .rrioLrLrnless cvcLs >1.00() rri l, /dl-persist aftcr die
r.!tri! tr(nr of iars, sugars, 1nal .rfLroh\ rafes.accompaDi
incrc,r.cdphysicaL cti\ ' ltv. n \uch eascs. he airr rs to prc
.l-rr\orles f pdDcrextit is. he uornnton Lrsc f l ibratesan d n
rr r. lulrs u,irh hvpelniglr.endenria is rrot rccommended n
Llrcn H\' lCi (loA reclucrascrhrhrtori rre rcasonilbLy flect
Iruerrrrg tr ' igl,vcerrdeerels. rd thcrc is coLrsidcrlbl,v ore e
ncnec docuurcncing he sirtcrr rrrd cif icecv >f h is classof lorrcrin!, rneclicatiorrsn .hllJrcr
HcpaticLipase0elicrerrcy Hcpirric lrprsc rledciency s a r i l r . irrrrosomdl ecessrtecouclit ion caLrsing le\,ation D
t. i.r\nri cholesterol rn.i rri i{ lrccrJeJ. Hcparic lipaserrilr,r l,zcs rriglvcerides nc l phos]'holiprclsn Vlf)1, remn
r rnc l L )1 . , r cvcn t ing he i r o r \ c r \ i ( ) r rn r LDL . l l l ) 1 . cho le
lcrc s rcnd to be ucrelscLl . lrrher d1.1n ecreascd, uggesti
i l i lgnosrs. I-ahorarory conlifmafr()f lt ,- 'srablishedbt nreas
i l l : r c t i v i t yn hcpa r inLze r ll r sn r r
O ISORDLBSFHDTM ETABOISM
PflrnaryHypoalphirliproteireoriasoi:rtcclou HI)1. chole
s .r i. lrr i lr.r lcondit ion rhrt oircn follorvsa patterrrsullir,cs
ru:,rsoLD:rI omtnlnr ir lherrt.rnce ut lri]v occur indepc Llc
irrnrlr hrstorf. It is rh c nrosrcoDrnorr lisorcler f HDI- mc
li:nr k rs lefinecl isHDI cholcsrelrl <ll.)fh pcrccnlle lor gc
i - , ,1 - . r r i l lLlh plasr: ra orr prr ienr rrh rcute. rL ' .Lomi rr . i' . r rn l r r r r
l )Lrr r i rsrorr : )rsl i rrr. laerria- ; r rdJ l r l () l rra' l r l7 t j l l
a [ rscrr t a ] - . ( )C ll. Borh arc i rurosoLre l raccsslve aondi f l ()rr\ \ \ ' i !h i
f r c q u e n o o f - 1 . 1 1 . ( l ( 1 0 . 0 0 t 1 .I e d i s c a s eL r s L r i r l l \ r c r c r r r \ ( i L L r i n g
chrlclhoot l u' i th rrcute pirncrc.rt i r is. Fi rLLptJr'c anthorrri ts orr thc
i l r ls! k ccs, anLl L)L l r ( )a l (5 l l i t r l . )e prescnt . al1(l thcfc nr i l ! [r r
por tar l vcDoos s!src| l r rr] i l \ i lLrl lxrcrt ! olel f l t intake, i l r ld , l ( l l l l l l l
israrion of f ish oi ls r l r i r\ .1lso bc b encf icial
Fan i l i a t Hype r t r ig l ycenden r iaF l jTG, ype V l l ype r i i p idem ra '
l i {T ( i i s r r . l u tosom r j on r rnen t l i so r t le r f L r l l Lno$rc t io loS \ .
t L r i ch occLL rsn . - l . r . i i ) 0 nd iv idL r r l ; .r i . ch l rac t c r r zc . l' r l l c l r
t iorr oi pLasrrrarighcericlcs>' l(Jrh
l-.crccntilc2.5(l-l.0ll i) rrrq, 'ct l
(l .qcl. )ltcrracc()nrF;rrr;( ' { l'r . l jghr r' levarjon ll plasrllrr lolts
rerol rnd <>rv [)[-, l: ] l l( i docs rrot Lrslrellvna.llc\t Llnnl r(1L1ll
hoocl. hough ir 1scxprerse.l rr =10')i, ol eiiecrccL hllclrtn- lrr
collt fesf o F(-l l l , , l H'I (, is rror hought ttr bc highlr .rthcr )gcrrre-
It is rnosr ikely causecl rrd.ic.ri!c brcekdorvnof Vl L)l or less
degrcc relativc wirh h!pcrrrLgl\ ' . : tr idcmra.-HT(i shoLrld -'c lr.
Jisc,rse. hc cli ifcrentiation s r.rir l l)- ossrL.len cl i l ic l l sfotLnd\'
r r rha tLoucr I ) l - cbo lc ' t c ro l c rc l srccom p lnv l l f ( i . hL r r r c . r
su rc r re r t o i nonna I i ] l ( J l l e rc l r i n l t lT ( l rna - r . e hc l l - i L r l r r
levclsoi c rr lornicrons ls wcll es Vl-l)l l ' .rr ic lcs (ljreclcrcl'on
r lpc \ r ) r r r r \ occas io l l t b c c r t co r rn fe rcc l .r i g , l l ce r i . l cc rc l . . r r r '
o i t cn>1,000n rg / t l L . he , -1 isc , r res i r r . ' l v cen l ch l ld re r r 'r rco r r -
f r -as t( Jchv lo rn rc ro r rc rn i rl r cL l . r i . ks ( ) r r!Pc l ) , I l ' l - o r r l ( ) ( . l l
dcficiencl is ro r pfeseur Thc\e L..rtrcnrs ifcrl dcvcl{rPcrrrfr \r
x i l r f hon l r s r r ac lu l rhoo r l .hc r -casypc IV hvpe r t r t g ,hec r, l c r l l i , r
indivi,JLrlls lo no f Acure pirrcrc.rrit is nrt be dr e frc\cnfrrrsi l l ness .As w i th od rc r hypc r r ig l ' ce r rde rn i ' r \ ,xccss i \ c .1 l . oh ( ) l
c()nsul] lption ncl e.rr-ogcnLrcrilIr catl e\rccrbafc thc diseesc-
Secrrnclalv .rusc:oi rrltrsicrrrhvpertriglvccridertiir horrlt l tc
lu l cc lou t bc f i r r cn r i r kLng ( l rdc r r ( r s rsf tHT(1 . A c l i c rh igh i r r
criJenri.t. Adolcscerts iur! l adulrs rhoulcl bc qtrcstiorrcLllr()ttt
I {: . ?
HYPMCHOTTSTEROLEi$IA-lpctiyrcdrjmrrPlfr!r:i itni'cme
i i .e! t i5ri
ll Lrq5:prcqeneonqllnxel,qret0,ilr05p0te
HYPTRTRIGTY(ERIDEMIA
01:! t l
l!oe drar.'te5
i,l$ nq yndroni)r.,qf,rnq
"epa0l5a0i irrclea5infhilcfJ
-rrJqtf rbo atend!,p 0cie5,e5Lroqen,r1zrtdj
REDU(EDDL
tnol fit
0r:J !
T!" i . l ldr:bi t$
Druqr Blxike15,anibc5iPr:r5

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 99/177
588 PAnTX Melaboliciseases
and agewith normal plasmauiglyceridesand LDL cholesterol,r00hethert is assocrared ith more rapid athetosclerosiss uncer-tain. It appears o be related o a reduccion n apoA-I synthesisand ncreased atabolism f HDL. Secondary auses f low HDLcholesterol, uch as the metabolicsyndrome,and rare diseasessuch as LCAT deficiency nd Tangierdiseasemust be ruled out.
FamilialHyperalphalipoproteinemia.his is an unusual condi-tior conferrirg deceasedisk for CHD among amily members.Plasma evelsof HDL cholescerol xceed80 mddl.
Familial poA-lOeficiency.uration\ n rh eapoA-l genemay
result n complere bsence f plasmaHDL. NascentHDL is pro-duced in the liver and small intestine.Free cholesterol romperipheral cells is escerified y LCAT, enabling formation ofmarureHDL particles.ApoA-I is required or normal enzymaricfunctioningof LCAT. The resultantacctrmulation f free choles-terol m rhe circulation eventually eads to corneal opacities,planarxanthomas, ndprematureatherosclerosis.omepatients,however, ay havemurationsof 4poA-1 hat result n very rapidcatabolism of the protein not associatedwith atherogenesrs,despiteHDL cholesterolevels n the 15-30 mg/dl range.
TangicrDisease.This is an autosomal co-dominanr diseaseassociated rth levelsof HDL cholesterol 5 mgldL- t is causedby mutations n ABCAI, a protein thar facil itares he binding ofcellular cholesrerol o apoA-L This results rn free cholesterolaccumulation n the reticuloendothelial ystemmanifestedbytonsillar hypertrophy of a distinccive orange colo! andhepatosplenomegaly,ntermittenr peripheral neuropathy mayoccur from cholesterol ccumulation n Schwann ells.Diaeno-si sshouldbe suspectedn childrenwirh enlarged range onsil*and extremely ow HDL cholesterolevels.
FamilialLecirhin-GholesterolcyhransteraseIGAT)Deficiency.Mutations affectrng CAT interferewith theesterification f cho-lesterol, berebypreventing ormation of mature HDL partrcles.Thrs is associated ith rapid catabolismof apoA-I. Free circu-lating cholesteroln the plasma s greatly ncreased, h ich leadsto corneal opaciries and HDL cholesterol evels <10 mgldl,PartialLCAT deficrencys known as"fish-eye"disease, ompletedeficiency auses emolyticanemiaand progressiveenal nsuffl-ciency early in adulthood. Thrs rare disease s not thought rocause premature atherosclerosis. aboratory confrrmation is
based n demonstration { decreasedholesterol sterificationnrlreprasma.
Cholesteryl stelTranslerProtein CETPI efciency.Mutationsinvolving the CETP geneare localized o chromosome16y21.CETP facilitates he transfer of lipoproteins rom mature HDLro and from VLDL and chylomi-ron anicles.hus ulrimatelyregulating he rateof choles terol ranspon to the iver for excre-tion in the bile.About half of matureHDL2 particlesare directlyremoved rom the circulationby HDL receptorson the surfaceof the iver.The other half of cholesteryl stersn the coreof HDLexchangewith triglycerides n the core of apoB lipoproteins(VLDL, IDL, LDL) for transport o the liver Homozygousdeli-ciencyof CETP has beenobserved n subsets f the Japanesepopulation with extremely high HDL cholesterol levels(>150meidL).
GONDlTlOlls SS0CIATEDITH OW GHOIESTER0t.isordersofapoB-conrarning lipoproteins and intracellular cholesterolmetabolismare associated ith low plasmacholesterol.
Ahetalipoproteinemia.his rare autosomal ecessive iseasescaused y rnutations n thegeneencodingmicrosomal riglyceridetransferprotein necessaryor the cransfer f lipids o nascent hy-lomicrons n thesmall ntestine nd VLDL in the iver Thisresultsin absence f chylomicrons, LDL, LDL, and apoB,and very owlevelsof plasmacholesterol nd triglycerides. at malabsorption,diarrhea,and failure to thrive present n early childhood. Sprn-ocerebellar egeneration,econdaryo viumin E deficiency, an-ifests n loss of deep endon reflexesprogressing o ataxia andlower extremiry spasticityby adulthood. Patientswirh abeta-
lipoproteinemiaalso acquire a progressive igmenled ednthy associated ith decreased ight and color vision and etual blindness. heneurologic ymproms nd retinopachymamistaken or Friedreichataxia. Differentiation rom Friedrataxia is suggested y the presence f malabsorptionand athoc;tosis on peripheralblood smear n abetalipoproteinMany of the clinicalmanifestations f the disease re a resumalabsorption f fat-soluble itamins,suchas vitaminsE, A,K. Early treatmentwith supplemental itamins,especiaJly, msignificantly slow the development of neurologrc sequVitamin E is normally ransported rom the small ntestine oliver by chylomicrons,where t is dependent n the endogeVLDL pathway for delivery nto the circulationand periphtissues. Parents of children with abetalipooroteinemiahnormalblood ipidan dapoB evels.
Fanilial Hypobetalipoproteinemia.amilial homozygoushybetalipoproteinemias associated ith symproms ery similathose f abetalipoproteinemia,ut the rnheritance attern s asomal co-dorninant.The diseases causedby mutations ngeneencoding poB-100 ynthesis.L i s disringuishableabetalipoproteinemian that heterozygous arentsof probahave plasma LDL cholesteroland apoB levels ess than normal.There are no symptomsor sequelae ssociated ithheterozygousondirion.
The selectivenability to secrere ooB-48 rom rhe small ntine resulls n a condition resemblingabetalipoproteinemhomozygous ypobetalipoproteinemia.ometimeseferred oAndersondisease,he failure of chylomicron absorptioncasteatorrhea nd fat-soluble itamin deficiency. he blood e"eapoB-100,derived rom normal hepatocyte ecretion,s norin this condition,
Smith+enlH)piE SyndmmeSLoS).Patientswith SLOSohave multiple congenital anomaliesand developmentaldcausedby low plasmacholesteroland accumulated recur(Tables 5-11 and 86-12).Familypedigree nalysis asreveits aucosomal ecessivenheritanceDattern. Mutations inDHCRT1t dehydrocholesrerol-A-educrase)ene esulr n dciencyof the mrcrosomal nzymeDHCR7, which is necessacompete he linal step n cholescerol ynthesis.t is not knowhy defecrsn cholesterol ynthesisesult n congenitalmal
mations,but as cholesterols a major componentof mvelin,n

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 100/177
CEI{TMLIERVIX'sYsT[TIkonralbe ypopla5iaEn rqedentride5Aqmesi5l Dlpusallo5um(ereb€lhrypopasiaHolopm5en(ephdly
CANDIOVASOI.ARAl',rrrventli(ularana
se(Undumtr seplaeh(t%tentuclu5rte 5u!llembranou5ertdolarpplalefeo
URINARYTNACTReMlypoplasiaf apLrsiaRenalord(aly5t!
fiydmnephrosisllreteclupcalion
GASTnotrT6TllllLHirschsprungi5ed5ePylofCeno5sReiBctofy5motifilyl:ho16lafi(ndondolenatcrogc55iveivelisedse
PUullot{AnYPulmonaryypoplasia
Abnomalbationfi.lDofttt{E
Adrenansuffrdenry
ko. Pad D, lLE R offmann f: nh€dl€i sodeE fdd?]ko bi6,nlh{n \AnpedidrE l:f\l,tl1l 111
somcrvhathigher frequency n Hispanicsand lolver Lrcideocc n
indrvidualsof Airican descenr.
vival rs unlikel,v 'ben the pLasma holesrerol evel s <20 g/dl.
Laborirtor-vneasutcment shoLrldbe performed bv ga chr,r
macography, s standard echniquesor lipoprotein assa-v cludc
-"naut.rrr" lt t oi cholesterolPrecursors, vhich na v vield ialsc
posit ive esult.N4ilder ases nay nor preseur nril late chiJd
Pheoorypic ariance anges r<)mmicrocephal,v.ardiacan d
malforniarion, an d ruult iplc organ sysrem ailure to onll
dysmorpbic teaturesand mild Jevelopmentaldelav Treacntenc
Chapter 6 r Defectsn Melabolism l Lipids
includes upplemental ictar-v holesrerol eg gvolk) and pr>ss
H\lC; CoA reductasenhibirion to pre!ert rhc svnthesis f ro
prccu15ors roximal to thc cnzyrnarrc lock.
DISOBDERSF NTRACELLUTARHOI.ESTEROLETABOLISM
Cerebro(endinousanthomatosis.his aLltosomal ecessivc
orrlcr presentschnically in latc adolescence vith tendon xa
fhorrls. cttaracts, an d progressrveneurodc.qenerarion.t
ceusedL-v issueaccumLrlation f bile acLd nternrediateshun
into cholestanoLesult ing rom nlutations rn the ecne fol ste
27 hrdrox,vlase. Ihrs enzymc s neccssarl or normal mirochclrral "nrhesis f bile acids Lr be iver.Early rcatmenrwirh ch
oJeoxrcholic acid reducescholesrerol cvels aLrdprevents
de-velopment f sy.rnptoms.
Wolman Diseaseand Choleslerol sterSl0rageDisease CE
Thcsc autosomal ecessive isordersare causedby lack of ly
sonralacid lipase,Afrer LD[- cbolesterol s incorPorated nto
cell bv endocytosis, r is deli"ered lo lvsosornesu'here ic
hydrol'zed b,v ysosomal ipase.Failure of hycLnrlvsis ecaus
conDlere absence f the enztme causes ccumularionof cho
teryl csters vvithin thc cells, Hepatosplenornegall, teacorr
aLrd arlure o thrive occur during early infancl, lcading ro de
hr , rhe age of 1y'r. ln CESD, a l ess severe orm rhrn Wolm
discasc, here s lou but derectable cid lipaseacrvicv,
Niernann-PickDisease ypeC'fhrs
is a disordcr of inrrace
Ier cholcstcrol transporf charac[erizcd b,v accuntulation.h r l c . r c r , ' l anJ ' ph rngon r t c l ' n n lh . ( cn t r J l nc r t ' , u t a
rcticuloendorhelial -vsten1s.eath froru this autosomal eces
ncurologic disease :suallyoccursbt adolescence.
||POPR0TE|N ATTERNSN CHILDRENND AD0LESCENTS-a
l l6- l i , derivedprimaril,v rorn the Lrpid ResearchClinics Po
lanon Studies,shoo.s thc disrnbution of Jipoproccin evel
Anencan youtb at various ages. btal plasma cholesterol
r.rpidh lionr a mean of 6i 3mg/dl ac birrh co a level appro
nrarcLr wice fhar by rhe end of the neonaral ptri ' rd. A v
gradu:rl r ise in cotal cholesterol evel occurs unfil puberty
rvhich rine the mean levcl reaches160 mg/dl, Total cholesr
falls cransicnrly uring pubertv. n malcs due to a snall decre
in HL)L cholesterol. nd in femalessecondar,vo a slight fal
LDL cholesterol.Blood cholesrerol e' .els rack rcasonably
as individuals age,High blood cholesterol ends o aggrega
fanilies. a reflecrion i eeneticaDd environmental nfluences
Ar :rcceptable oral iholesteroLanrong children and ado
cents is <170 mg/dl,; borderline is 170-199 mg/dl; and h
>200 Lr/dL. An acceprable DL cholesterol s <110 mg/dl; b
tof,i-oEilstUPoPnfiHil GflttxStTYP0PftorE0t0ttsrEflot
MTH 95TH IOTH 25TH
0{0tEsTrR0t
MTAN
79
roTrl Hor.t$tnotioDr)MTAN 75TH 9OTII
TOTALTFI6UGNDE
5rH
4) 103 11 - 5 0
5TH
1 l
9
6
75IH
r09|0
109l
t17 129 t8 42 49 56 112J r40 t6 t8 4/ 5l /
111 tn v 40 46 5t 11 1 6 B 6 ] 7 q 4 5 5 2
lrl J0 J0 1,1 l9 ^6 6)9 117 t5 l8 4l t t
61 9l68 r0{
64 9168 9l
6t 9459 96
95TH sIH5TH
84
t/0 r90 2011/3 r88 200
168 181 r89116 r90 191
r7t 188 242t7l 191 20 5
168 t8l l9l176 198 )01
68 85 99 114lq 95 112 112
58 /0 85 12574 10 1 126 111
14 94 ll l 12485 10.4 r20 125
88 r25 143 ll885 fl2 126 r8
68
155156
155
160r60
r5 l159
l4
56
t
6l7)
t87l
29t4
28l2
33l9
38l6
l5-19rMaeFema
l:ord
1 4 y lMale
[imale
5 9 y rlvlalefumdle
l0-14rlvalefumah
r0l5
'Notedardiftercnte(flt e5 rcllFdmr iDi.h0eltem
l1,16,d|d]inIa|)q?seaft0n'(5[wtl0ran,udk5D0laWrDl1'|l'ePRfEf.?Ji!d'NNp!bLkalirnM80]527Wi'hil1!l0n'0(l1aI0rrhi|fF5dH$h[l9&

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 101/177
590 PABTX. Metabolic iseases
derlJne110-129 mg/dl; and high >130 mg/dl.. HDL cholesterolshould be >40 mg/dl.
Bt00D GHOLESTER0ICREENINc. CEP's Expert Panelon BloodCholesrercl Levels n Children and Adolescenrs established suide-l i ne ' , o r cho le , , re ro l ea \u fem en rha r we rep r . rb l i shedn 199 l .The panel recommended a sele.tiue approach to screening basedon the follo\a1ng critena:
Saeenildren nd dolescentshore arcntrrgrandparenttave o(umentedoronaryarterydiseareeforche qe f55 r.
Screenheoffspringf a parcnt hohas eenoundo hav.a blood olegterolevel f>240mg/dt.
Smen(hildnnnd dole(entsforwhomfamilyhistoryr unobtainable,pattkuladythosewith
otherir* adors,
The American Academy oI Pedrarricsand rhe American HearrAssocration (AHA) have endorsed rhese criterra. Application ofthese criteria will result in the screenins of 2J7o of Americanyou lh . rep fe \en r ingho\e m os t r ke l l ro ha le a f am i l i a lba r i s o rtheir hypercholesterolemla. predicted 597" of children wirhelevated levels of blood cholesterol will avoid detecrion becauseof che ack of universal screening, and rherein lies the source of
>240 mgldL is considered by some to be coo insensirjve and dif-ficult to apply.
The rationale is basically sound, lhough admirredly the guide-lines are fraught rvith problems of compliance. lf familv his-rory of n'idespread premature arherosclerotic heart disease tsobtained, offspring are Jndeedat signilicandv greater risk of dys-lipidemia than children without such family' history..The converseapplies to children who do not fulfill criceria for screening; theyare not likely to have a suong genedc predisposition ro heartdisease. The 59% of children with hypercholesterolemia notde rec ted 1 l i n i . i an ' f o l l ow ing hegu ide l rnesre I i ke lv o haveonly modest elevacion of cholesterol due to environmental influ-ences such as diet and sedenrar)' lif€style. Pr imary preventionstrategies pplicable o the population as a whole include daily
physical activicyand a diet low in saturated ats. Children an dadolescents or whom there may be consideration of using cholesterol lowering medication rvill nearly always be correctly ident rFedb1 io l l ow rng u r ren r u ide l ine ' .
Early dragnosrsand treatment of individuals rvho are at risk ofpremature CHD becauseof genetic susceptibrliq is an importantpublic health strategl It is esrimated that no more than 2070 ofpeople with heterozygous familial hypercholesterolemia are diag-nosed,and <10% are being adequately reared. detailedstud_vfrorn the United K ingdom has established the cost-effectivenessof "cascade screenng," which means tracking and tesrrng amilymembers of FH probands. Ic is even more cost-effecti ve to screenvounger people becauseof more life y€ars gained attet preventrveffeatment.
It is well documented that many parents are unaware of their
o$.n cholesrerol levels, making the use of that criterion problem-atic. The evidence that cholesterol screening of children maycausepsychological harm to the child is less han compelling, asis the concern that universal screening mighc lead to overuse ofcholesterol lowering medrcation, The n'orrisome eprdemic ofchrldhood obesity, approaching 50% in some disadvantagedhigh risk populations, supports broader screening to identif).those with the metabohc syndrome- A fasting lipid profile rarhertban nonfasting total blood cholesterol measurement is indicaredif screening s beiog conducted becauseof obesity as a risk facror
not specrfy he age at which at-risk children should be tesred.Five
-yearsof age is a reasonable age !o screen since dietary intetven
tions for those children with hypercholesterolemia can be sapplied at chrsstage of neurodevelopment.
RISKASSESSMENTND TBEATMENT FHYPERTIPIOEMIArecommends nsk assessmen! ased on LDL choles ol levels86 -14 ) . he f o l l ou .up n te rva l nd m od i f i ca r ion d ie r s dmioed by the sevelry of dyslipidemra. Borderline hyperchterolemia {LDL 11,0-129 ngldLl should prompc iniriation ochild on the AHA Step I diet:
(aloriesonrum.dt at hooldot x(eed096ftotal(aloderonrumeder ay.(alorie!onqrmedr atlntedatshouldot xeed lD6ftotalcalorieter ay.Totalholcrterclntakehoold e initedo<300 g/dlper ay.
Instruction regarding avordance of other risk lactors for disease such as tobacco use should be provided. and the sh<'uldbe reevaluatedn I yr .
Persrstenceof elevated LDL cholesterol >130 ms/dL indicthe need or more comprehen\ile elaiudtion an life.rvle mf i ca t ion . H rs to ry and phys ica l exam rna r ion nd . rdd rIaborarory tests aimed at rulng out s€condar,v causehyperlipidemra seeTable 86-10) should be performed. Ofamily members should have blood cholesterol screening. I
LDL cholesterol level does not achieve the rmnimal eoa. | ]0 mgidl. the AHA Step l drer*hould be recommendeddiet allows lhe same average fat consumption of no more307" of total calories, bur restricts saturared Iats to <7-87toral alories and cholesrerol intake to <200 mg/day. Follollab c ts, meastrremenr of height and weight for the calculaof body mass ndex (BMI), and dieta._vhistory should be sculed at 3-6 mo intervals.
The 2004 revision of the NCEP ATP III raised rhe mrnacceptable eveLof HDL cholesterol from 35 mg/dL to 40 mgIf low HDL cholesrerol Js present, counseling directed rowweight management, tobacco avoidance, and daily physical aitv shor:ld be orovided.
No restricrion of fac or cholesterol is recommended for inf<2 yr of age becauseof rapid grorvth and development, espe
rnvolving he cenlral netvous systemand the possibil iq of doping failure to thrive. Overfeeding should be drscourahowever, as, increasingly, infants and toddlers are exceeu,'eight for height standards published by the U.S. CentersDisease Control and Prevention- The myth that "a bigger bis a healthier baby" persists.
of poor growth or compromised nutritional status. The prosrive, well-controJled Dietarv Irtervention Srudy in Child(DISC) compared chrldren consuming a low-far Step I diet sublectsconsuming che"Lrsual" dier, containing 33-34o/" ol ries as fat and 137. as saturated Iat. No differences betw
groups wlth regard to height, weight, micronurrients, or psylogic well being were observed. Children on the lor-fat dietlower LDL cholesterol levels.
The Commrtee on Nutrition oI the American AcademPediatrics suggests hat as children >2 yr consume fewer calofrom far. thev should ear more grain pi oducrr, {ruirs. regeralow-fat milk produclsr beans, ean meats, poultry, frsh, and oprotern-rich foods. Low-carbohydrate, high-fat diets becomepopular in th e lascdecadeas a means o achieveweredr.rction.Unlimiced fat intake is strongly discouraged, as s ustricted sugar and carbohYdrate consLlmption. Carbohvdrshould comprise --55% of calories, achieved b,v consumcomplex carbohydra!es such as pasta, cerrain vegetables, ptoes, e8umes,and whole grain cereals nd bread.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 102/177
Chapter6 oelectsn Metabolisml tipids
BiskAssessmenlPosiliveamily istoryl Parentalig hBloodCholesterolr Premalure VD
l igurc l iL l1. l low chart of chssLi ical ion,
educatiol, .rnd f<,lli,w up oi chilclrenb.rsed n
l o r d e - s r ' l , n o o r o r e r l D l ." ' r ,
r , ' | l
levels.CVD, cardiovascular isease;HDL.
high'dcnsi t -!ipoprotcin. FrornVi lLrans CL .
HagmanLL, Danrcls R,er al : Cardbvascular
henkh io chi(dhoorl. Cir.:rlarr)" 1001i106:
1,+l-16t)
frozen vegctables rrd soupsshould be selected or l orv sodiurn
conrent,
the entjrc iamilv rarher fhan cn ildjvidual child -r\ regular irne
Th e rise n sedentar,vclrvity emong oLlryouth is conlributing
"lf low HDL cholesterols deiected, hen patientsshouldbe counseled egarding igarettesmoki
low saturated at diet,physicalactivity,and weighl management if overweighl).
tFor patients 10 yr old andwithLDL-C> 19 0mg/dL or >160 mg/dLwithaddit ional sk actor
diet does nol achieve he goal, hen pharmacologicntervention houldbe considered
hypertension,Thc Narional Associarion or Sport and Ph,
EdLrcatior NASPE) recommends hat children should acc
lare ar leasr 60 minutes of age-appropriate hysicalaclivit
nlost daysof rheweek. Extendedperiods >2 hr ) of daYtime
tivif\r are dlscouraged, s is >2 hr of televr sionand other f
of scrcen rme,DrugThelapy Tables 6-14 nd 86-151, he NCEP ExpercP
fo r rllhiidrenand Adolescents ecommends hat considerati
f ion, at leasr 6 mo, has not achieved herapeDticgoals
rherapvshould be considered vhen:
' LDLholesterolcmains190mg/dl'LDLdole(erolremains>16{mg/dLandthereitaPotit ivefemi
di0va(ulariseareCVD)before5 tofage t wo rmore thet sk adolsot
presentfler igorourttempttt ifestyl. odif(ation.
Thesearbitrarv but sensible uldelines re basedo[ lhe s
Repeat ipoprotein nalysis
wilhin5 yr .Provideeducationon recommendedeatingpatternandrisk actor reduction.
Repeatlipoproteinanalysisandaverageprevrousmeasurements
Risk actor advicelProvideSlep-OneDiet andother risk actor nterventioRe-evaluate tatus n one y
Doclinical valuationhistphysical xam,ab ests). Evaluateorsecondarycauses.
. Evaluateor amilial isorScreen ll amilymembersIntensivelinicalntervenStep-One,henStep-TwoSetgoalLDLcholesterol:. Minimal:13 0mg/dL. ldea l : 110mg/d l

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 103/177
59 2 PABTX Metaboliciseases
MECIIANISMFAOION
|1MCoA cduxa!enhibftoE5tarn5)
Bie (d5eq,testants:
iiole5lranine[ohntpc
l,icclnac
ii|ft arid edvt,ve5:6emfbroz
F 5 h o 5
ft ohnerc biorptionnhrbit|)|l
fuelamibe
t!l-lowenriuxp'olantLfL,0rrft pa5e,iG,Iq}teide]VtDt,lrrylowdmsirypDler
ar e encouDtered nd family hi story oi early cor-onarv iseasc sprevalenr-
Corsiderable experienccwith drug therapl. rn childrcn an d
cacy. D fhe pasr. rhe mainst; lv of drug rherapl wa s bile asequcstrarttsLrch s cholesFralnincan d cholesripolbecaLlsehrverenot sysrcrr icalll ' rhsorLred.rterruption of the enrerohepcrrcLrlatiorr i Lri]e crds promotessvDrhesisn thc lir.cr oi nbile:rcicls ronr cholesterol.Gastroinrcstinal ide eff icrs and tefe\ultcd in less han desirable ornplrance. \ren vheD here ,t eu . v iab le p rons .
HN'lG CoA rerluctasenhibrtors,knorvn as statins,are rcma
abl,v cifecrive n lorvering LD[, cholcsrcrol evelsand rcducplaque nflanlmation, hereb,vcducilg rhe ikelihood of a sudcoronery event iLr an at-risk adult lr ' irhirr u,eeksof srart ingmedication. As a class, hey u'ork I ' t blocking the intrahcpbiosynthcsis l cholesrerol, herebvstimullt ing th e proclucrionlote Lf)L recel)rors n thc ccll lLlrface.The N(IEP ATP accafes rllgrcssivc orvcring ol l-DL ro <70 rng/cll in indiviclurvith knowr coronary he:rrtdiscese. his informarion is rclcrbecause hildrcn u'ho iulf i l l crrterra or considcratron f choterol lowering rnedicanon \rll allnost alwai,s hrvc inheflreclcondrfi(u ironr ()ne pnrcnr Not urfrequentll ' , vhcn pro"idicare or l l1echild. questjons o re up abont screening ncl rcment of parentsor grandparcnts.Statinsare equallv cficccivchildren,capableof lou'ering -DI cholesterol evels ,r half wlnecessar,v.hey also effect nlodesr eduction n rrigl,vccridcs
incortsistent ncrcase in HI)l cholesrerol. Sratins have beshown to impr(rve ntirne-nrcrlia hickness n crrotid irrterie
failLrre, hould bc rakcn nto considerationbcforc prescribiDgdrug. Thcre has beel no evidence o datc, ho,"vever,har compcatrons are aLr,v nore lrcqucnt in children than in adLrlts. skeLeralnrLrscle iscorriort seens r() bc sornervhat ess ofproblern.Stiltrnsare concraindicarcdn pdtienrs vith acti!c l i( l lsease nd during prcgnarrcvalrd lactarion. Childrerr shohave liver enzyrnes lolirored rcgularll, anclcreatirc plr(rsphinasc (CPK) measnred i musclc ache or weakness ccurs I iverzv rcscar be allowed o rise rhreeioldbcfore discolt inuing drug. It should be reernphasizedhr r children rvirh nroclcst vations n cholesrer()1,Lrch s that sccn n polvgelic h_vper
lcstcrolemia, re nor candidates or stetins as a rule becausthcir sideeffet profile.
()thcr cholescerolou'eringmedicariols such as r'r icofurrc ancl f ibrareshave heen used ar lcssoften iu chrlt lrer thrn bacid scqucstrants nd stxtins-Nicorinic acid has been usecl etivcly in children u'rth rrarked hvpcrtriglycendeLria r risk facute pancrearif is, holgh dictary resfrlcrionof complcx srrgand cirri)oh)drates usrrallv resulrs in signif icant lo,,verugrriglycericle er.cls.
F.zctjnibe s useful n the pediirtricpopularron beceuscof ei6cacr' an d lo w side effect pro6le. F-zctirnibc educes plasl. l)t- cholesrerol v bloci. ingsrerolabsorprion n elteroc,vtes.drrrg,s nratketecl s an adjuLlct t) starins$,hen adulr subjectsnor achievingsuff icienrblood lipJd orrerirrg \, ith stauns rlo
Jt eiterolandV|DLrynthesis1|1 ar|( IL c(eflcBTB andexrrelon
J HeparVLDLynthees
'l
rPrJVLDLJ VL)Lrodudion
J lnrcninab5orptio[hr] 5lerol
['lDt(ATt0t{
tlevated0l
FlevaiedDL
Ekv?teil0i
TPVatPdG
!levared16
EPVated;6
te,/atedDL
STARTTD
5-80 q qh
4-12 Ca'5 4C l aJrl]2,000
600 q d
I 10 aail
lC |rg aily
DRUGftD|lE nIYPEr FfE(T frrfi
sIAT[iSikn RarhNervo!5y5iern
Lver
GJ$mintea r,r(lMus(5
lmmune5y5temPmteinindrng
Lcssf oftentorioi,rep Ltudaia, ead&he,enpheral
neilr0pa(ny
Hepilil,lo55bppetiie,wehlcsr nd roeaie5iI serum'"l rotrdrrhras.\_0,^4Io 'periffer,' .ppq n o[_1"ncmallan!le
Ab0ofitlndld ,mii5ea,iairhea
4(5aled cfwedknel5,yorri5u5Lralyrth er,Jinleatine
i{nase 1,000/L),habdrrny0y5w th |rnaurlure
Lupu5likendromeol/artatn,5"r!ana1rn,0rl!va5ta)
Dir i fpd i l l T 0f ! "drr L! 'd\ ldrr., r :a : r. l i lvd'rdrnl
BITIA(IFBINDINGESIIIS
l;astroleii0a ra( Abdomnalfulns5s,nau5ea,tlas,(on(ipaton,hemo4hoidl,anaistLrre,tiatlo aid!e( tul1ltdmi0 hedbsorlii0nfyiiirnin n hiden
M d\p _ro-1rorrJr ' 'p ldep,dlrol ! i ; th,dn[eerdb".c
by 0nr0maFIrealmpntr h a tatin
In(Ieaieslnemmr!iy(erideif=10%greatprn(ed5esnpatem5ith ypet ycerdemia)
f rpprr' Dr r a(d0.i h !h drFo1d ".i" .,\,,.f eldl a Lr
kholesfycmine)Eindingfwafan, l!ox , haide ruret('hymxine,rciins
Flu5hrng,drykin, rur{1r5,(hthyosis,rantho5i5iqr n!
[on]unctivt,!,ryJtoda(u redema,et dldetaihment
Na5arJIufline5l
5,.pra\,entrUlarIhythrnj
|Jerfbur, cors owsllroveme0$tdiarheii id rn(ei9e1 eruTnmLn0irdnsfenses,hepatitirith arrsea
anCIa(LcUe
lt4yorilhLly0q!:Ir1i{in(dene\h \iJhpn pd,tp,t.tha.dbae,t.
lnLfea5eof0% erLlmr(aiid
Fash
510mrrhpiet,ab,roitnaain(rnaryqemFbrozi),ch0eslerol
5aiufttedie,inrreareofl% ngalsmnen(denceftecliley5fun(1i0nrna y doibote)
Myos5w i impad rendlfun.llon
nterfercncev/nhindinqfwarldnn,qu nq edudronn l.e
dosefwdrfariny 10%
urrcdsede'umm oiran(era5e5
ljver
Metabcic5yrtem
lhffo yle5
0ruq ieraclionr
t(oTtNt(ACrD5 k i
EyesRe5pihll)ryra(tHeart6afonlestinatmatLver
l/lusceslt4elabolic|$en
fIBRATES5kn(a5trointenal ECt
6encudnarycrlNllx 5Pblmarctein5
Lvef
fomhop! RdDtuqrcrmFfi f ,iid order fntl/#e, 1999t1.11985l2

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 104/177
Largeclinical rials of ezet imibe sedasmonotherapyn children
havi not beenconducted. everthelessherearesufficient eports
in the iteraturedocumenting he impressive ffectivenessf this
medicationu'iihout worrisomesideeffects hat the cliniciancan
<L30 mg/dl or, more deally,<110 mg/dl. There s no reason o
push LDL levels ower as s recommendedor high-riskadults'
2004tl60421429
De lonsh \, Os e L, sramosi . et i l : f f fcacy an d safewof ' tat in therapv n
.ttitai.n wirh familial hvpercholesterolemia. Crcularion
2002;1Q6:2231-2237.
DemerathE, Muratova V SpanglerE, et al: School-based besitvscreeningn
ral Appalachia.Preu Med 2003;37.553-560.
Durringron P, Dyslipidaemia.Lancet 2003;362:717 37
coldberg AC, Aditi S, JLL, et at: Effcacy and safetyof ezecimibe oadminis-
teredwith simvastarinn Pati€nrswirh Primary hyPercholesterolemia: ran-
domized, double-blind, placebo controtted vl:.l Mavo Clift Pto'
20O4t79:520-629
crundv SN{. Hansen B, Srnith SC, er al: Clinrcal managemenroI metabolic
syndrome:ReporcoI rhe AmericanHeart Association4'{anonalHeart, LunB,
Itlood Instrtute/American Diabetes Association Conferenceon kientific
IssuesRelatedro ManagemerJ:.Circul|tioll 2004;109:551-556
H ins PN, Heiss G. Ellison C, et al: Coronary arrerv disease isk in famil-
cornbrned hyper)ipidemia and famitiat hvP€rtriglyceridemia,A case
control comparison irom the National Hean, Lung, and Blood Insricure
Gmet 2004;66:483487.
Merkens LS, Connor WE, Linck LM, et at: Effecrsof dietarl cholesterolon
plasma lipoproterns in Smith-l€mli-OPitz syn&ome Pediat Res
2O04l,56:726-72.
Raitakari OT: Arrerial abnormalities in children with familial hvpercholes-
ftrcmi?, Lan et 2004\363:342-343Sinshal A, Cole TJ, Feffir€ll M, et al: Breast milk feeding and lipoProrcin
profile in adolescents orn pretermr Follow up of a prospective andornized
st)d\. Lan et 2O04i363,1571-15 8.
wiesman A, Hult€n BA, de Groot E, et al: Effcacy and safetvoI stat rherapv
in children wrth familial hypercholesterolemia fAMA 2004;292: 1-331
86.4.LlPlDosEs.argaret . McGovernndBobert , Desnick
fhe lvsosomalipid storage iseasesre diverse rsordersac h
du e o a n inheriLede6ciincy f a lysosomal ydrolaseeadingto che ysosomalaccumulationof the enzyme's articular sub_
strate iable 85-15).With the excePrion f Wolmandisease nd
cholesterolester storagedisease, he lipid substrates hare a
common structure hat includesa ceramidebackbone 2-N-acyl-
.ohineosine)ro mwhich hevarrous phingolipidsrederived y
subrriuLion f hexose",horphorylcholine.r oneor moresiahc
acid residueson the terminal hydroxyl gror:p of the ceramide
Chaderm . oefectsn Metabolisrnl Lipids 5
alterationsand characteristic linical manifestations f rhe ip
storagedisorders see able 86-16).Progressiveysosomalaccmularion of glycosphrngolipidsn the cenrral neflous systeleads o neurodegeneradon,hereas toragen visceral ellsca
lead o organomegaly,keletalabnormahrres,ulmonary nliltr
tion, and other manifestations. he storageof a substrate n
specific issue s dependent n its normal distribution n thebodDiagnosticassaysor the identificationof affectedndividua
relyon the measurementf rhespectficnzymaric ctivit ' In is
lated leukocltes or cultured fibroblasts, For mosr disorde
carrier dentifrcatron nd prenataldiagnosis re available;a spcrfic iagnosissessentialo permrt enericounseling.he chacterization f thegeneshat encode hespecific nzymesequirfor sphingolipidmerabolismpermit the development f therpeuticoptions,suchas ecombinant nzyme eplacementheraas well as he potentialof gene herapy. dentilicationof specdisease-causingutations mproves iagnosis, rena!aldetectiand carrier dentificatron. or somedisorders Gaucherdrseait has beenpossible o make genotype-phenotypeorrelatiorhatpredicr iseaseeveriryndallowmorePreciseenetic ou
seling. nheritance s autosomal recessive xcep! for X linkFabrydisease.
GM1GAt{Gtt0SlD0SlS. M1 gangliosidosismost frequentlypr
sents n early nfancy (type 1 disease) r-rt as beendescribed
patientswith a juvenileonser type2). Both areautosomal ecsive raits; each esults rom the deficientactivity of F-galactdase,a lysosomalenzymeencodedby a geneon chromosom(3p21.33). lthough he disorder s characterizedy patholo
accumulation of GM1 gangliosidesn the lysosomesof bo
neural and visceral ells,GM1 ganglioside ccumulations mo
marked n the brain. n addrtron, eratansulfate,a mucopolys
charrde, ccumularesn lirer and rs excreted n the urineparientswith GM1 gangliosidosis. he p-galactosidaseeneh
been solatedand sequenced; utationscausingeither ype 1
rvpe2 disease ave been dentified.'iheclinical madfestationsof the infantile form of GM, ga
gliosidosis type 1 disease)may be evidenr n rhe newbornlrepatosplenomegaly, dema, and skin eruptions (angiok
atomata), t most tequentlypresentsn the 1st 6 mo of life wi
developmental elay ollowed by progressive sychomotot etadation and the onsetof tonic-clonrcseizures. wpical faciecharacterizedv low-ser ars, rontalbosring. depresseda
bridge, and abnormally ong philrrum. Up to 50% of paciehavea macular cherry ed spot. Hepatosplenomegalynd sketal abnormalities imilar o chose f the mucopolvsaccharidoincluding anterior beakingof the venebrae,enlargement f t
sella urcica,and thickeningof the calvarium,arepresent.By t
end of the 1st yr of life, most patientsare bhnd and deaf, wsevere eurologrcmpairrnent haracrerized y decerebrateigitv. Death usually occurs by 3-4 I'r of age.The juvenile-on
form of GM1 gangliosidosistype2) is clinically distinct, 'ithvariable age at olset, Affected parientspresentprimar y wneurologicsymptoms nclLrding taxia, dysarrhna,mental refdarion. ndspasticity. eterlorations slowipafienr(ma ysur\
chrough he 4th decadeof life. Theseparients ack the visceinvolvement. acial abnormalicies. nd skeletal eaturesseentype 1 disease. here rs no spec ific featment or either ormGM 1gangliosidosis,
The diagnosisof GM' gangliosidosis hould be suspecteinfanrs with typical clinical featuresand is confirmed by tdemonstrationof the deficiencyof p-galactosidase ctivrtyperipheral eukocytes r cultured skin fibroblascs.Orher disders that sharesomeof the featuresof the GM1 gangliosido
include Hurler disease mucopolysaccharidosisvpe I), I-cdisease,ndNiemann-PickiseaseNPD) yp eA, whrch anebe distinguished y rhe demonsrration f their specific nzymdeiiciencies.Carrrersof che disorder are detectedbv the msuremenrof the enzvmaticactrvitv n white blood cel ls or c

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 105/177
5S4 PABT Metabolic iseases
L+l
i+) +(+)
+ +
+ + +(+l
ft(]MEN(LATURE
MUOLIPIDOSTS
l urol ) o5e!,l r d5Ei ierlu.o d.r5i Llj5tudolr4e:
i uao $! ! t
SPtlll'lG0LlPlD0StS
fubr/Cie25e
fdderdr€ase
6i datl]ra .rJ
6^r,g:qqidcris
6Mrgirg5dcsi5T;y irh5 rseaeq!ardh0'i
0r5edsei
[,rucherlpe
iaurl.:rlyp3
Nendnrr( r ) -p .=A&B)r,,lcta.hrcn.:| .Ll.di5trph!
UPtDST0RAGEt50n0tnS
Nlerdnn(k lF L1=i&D)
!io man isea!e(p'cd |olir{n05,5,infdnthtrntayJox
f lantal('i0d pofLrnir ,h:e iinte(lanskl
Be5rhlr! i5[y)
a?r0 ipofL.(,(r .iuvenieSpieFr?yef''rcqt)
Gmd polul rncrj . ;dri (r i j , fur/ j
0LtGosA(ftARtD05tsArpJrlylErici:mur
Furc!rdoi t
3 i{;nioidor
)[i ndErd ear?
l i r f t i51
5ii ccis
TNZYMIFIIO
,'[Aaeiy r05ary hcjphotrrn!L:ri$/i AieiI,l (Diar yJfl];l]hotr:riarri5c
d Gad(1c5d;\e
tetaTtiie
tsaaacrosLlas!arLddr?
Faaictosiar\i
P lexcsarnida5aJAri I
(' u.c(ercbm5il.5.
ourcrerubrc55. '
durocePl]rl]\d;!!
)Prrq0mlea:eAry ullirta5.p 6; airi]iertr'lddr..
nfrrelu;rahr nr,o ran5p()rt
Ai l piie
Pal iol !r1r1:rhoE5t€nre[.N]i
Papt3iinn5erjlire..nidue (l:L\l)
t r, i rni5 t nhiC i-N5l . l rke)
(iLNTl.ariai iaL\ ,6)lLfll,rembranerotein
(lN4, rabablyerD1rerroLr!
r5parry! Jianr nare
0 lVafn,rldJjs
d-lfAcetilqicrjrn r ii,e
5r; da5i
5r; dar.'
l+l+ l+l
- i+i ]r
1+ + (+ l- 1+l
- ++ -+ -
- # .
1+) -
+
(a )
(+)
- + +
+ l+)f . -
1+l +
1+l +l+t +l+l
+ +
l+) -
l+l -
+;
1+)(+)
l+)
l+)
++I
++
- +
+ rn.re.lt+,me_ p isnl,[+1, :rnrtrrfi'rilllg ile: n_ad5fi(t r.u n nrr lsln,tA(.,i .tiim riq)r;rt
|,1td1?dflNof-dn[:tilh.0$L,l5(hNk!],etaJido,eL]]0,d4/il,
+ (+)
l+ i*)+ (-)
1+ii + t +
tur-e(lskin hhrobLastsr renatal dragnosis s rccourplishc.l by(leterlnination i thc cr)zvDa c acfir. it ,vn ctrlrurcd rrlr locr tes or.ho r io r i c \ r l l r -
I t i i 1 l l 1 , i t r i : r i r ' lS rL l l lS !5 he ( iN41 a rg l i l l s i c los . ' sc l rLch a r -Sachsdiscese rrrI Sandhoff discasc: lch risults irorn th(- Llcfictenc! ol [3hcrosarrriDiclase criv]tv end t hc 1r-sosorrelac(urlrLr|rLron r (i\ '12 galgiiosides, pirt iculir lr rr t rhe ccnnalnervoLrs s\stenl. Eorh disorders have becn ci.rssif ierl nt oirt i lrt i le-, jrLvenile.and adulf onser f i)frns barccion fre aqe atonset f lnd clinical fcanrres. B llerosaminicl;rsc ().cLlrs s ttv()isoz-vrues:B hcxosarnirrit lase, r,r 'hichs cornposcrl f ole u andon e l i s b nir, an.l B herosarninrclasel, rvhich hrr t.r,o J3 ub ,Lr ifs. F Hexosamiljr lasc dcficicncl esLrltsrom nrirr:rt iorrs th cn subul)itard causcs' lrri,Sirchs lisease,vhcre:rs rurrrrionsr tlre
B srbuLritgelc rcsult r the rle6cielc,v f both p lrcrosr lr inril:rscsA ald B :rnd ceuseSandhoff diseasc.Borh rre aLrfosonr.rlccc!silc rr:rits,u,rrh T.ry-Sachs iscascharrng a preclilccrion l rhe
.\rhkelazi jcwish popLrlunon,wherc rhc cerrier t iequcnr Lrour1/25
l\ '1ore han i(l rLrtarols have beel iclentif iedi t(rsr rre.r.rtcd rvirh rh c iLrfenriLcorurs oI cliseasc. hr.ec rrurr
irc.oLrnror >.lSll; of nrutarltalleles rnongAshkc az i ]crvisr crsof la.v-Sachs iscirsc.rclurlng one allclcassocrareclvrrlclrrlt olser forrr. \ ' f tLterLonshat carr se he subacutc rr chkrrnrs result i l enzy.nre)r()tcinswifh resi drLal nzrrrrrt ic at r ' , . t l r c I . \ , , " r r 1 ' . r ' r r c l r t c, , i r hh s r r t r r r . , l r , d ,
l)arcrts rvith rhe rlannlc form of Ta1'Sachs listaschrr..ical manilestations n rLriercyof loss ri not()r skll1s, ncrs(rrt le re.tction.and rllecularpaLloratrcl eti nal chcrrv red
isccTab le86 16) .A f iec t . ' Jn ianLs sua l l , ,l cve l rp o r rna l l4 j rno oi erc rvhcn decreased vc corltocl t1ldaD exi!,ftcsr.rrrlc cspor;c to noise thyperacusis) rc lroted.Macr-ocenor rssociared virh hvrJftrcephalus,rr y rlevelop. n rhe Lrol lr le. seiztrres equlrine rnlicorvu)sant rherapv dcvclop.rodegencratior s fclr ' rrlcss,wirh Jearh occltrlng by rhe ag

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 106/177
pNAcgal-a l -
l aNANA
Neuraminidaseceramide-------> gal- NAcgal
ChaflEr 6 r Dstoctsn Met.bolism l Lipids
B-Hexosaminidasei|ooarsS8ndhofi,and others)
- glc-ceramid€
Polysialogangliosides
PC-ceramide
Sphingomyelinase
Niemann-Pickisease
NANA
II
Gmgangliosideeuraninidase
*gal - glc-ceramide
Tal
I
Lactosylceramide-galactosidase
gangliosklosis,.abbe isease
Flgure 86-15. parhwaysin the maabolism of sphingolipids ound in nervous issues.The name of the eruyme caralyzingeach reaclion is given wrth the n
of the subsrrace credon. Inborn errors are depictedas bars crossingcbe eacdonsarrouts, ar'd the narneof the associated efect or deleccss Siven n lhe ne
6on. The gangliosidesare named eccording to che nomenclarureof Svennerholm.Anomeric configurations are gtven only ar the largest staning a compo
cal, gabc;s€] glc, glucose;NAcgal, N acerylgalactosamine; ANA, N-acetvlneuraminicacid; PC, phosphorvlcholine
or 5 yr. The iuvenile-onserorm initially presents ith alaxia and
dysaithriaand mayno! be associated ith a macula!cherryred
spo!.The clinical manifestations f Sandhoffdisease re similar to
A and B determination, ndeed, or Tay-Sachs isease, artrer
screening f all couplesn which at leastonemember s of Ashke-
naziJewishdescents recommended efore he nitiation of p
nancy o identifycouples t risk. Thesestudies anbe conduby the derermination f the levelof $-hexosaminidase acl
in peripheral eukocytes r plasma.Molecular studies o identhe exact molecular defect n enzymatically dendfied car
should also be performed o permit more specificdenrificaof carriers n the amily and o allow prenaul diagnosism atcouples by both enzymaticand genotypedeterminations
incidence f Tay-Sachs isease as beenmarkedlyreduceds
the introduction of carrierscreening rograms n the AshkeJewishpopulation.Newborn screeningmay bepossible y msuringspecific lycosphingolipidmarkers.
GAUCHERISEASE.his diseases a multisystemiciptdosiscacterized y hematologicproblems,organomegaly, nd skeinvolvement, rhe laner usually manifestingas bone pain

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 107/177
596 PARTX MotabolicDiseases
c r p p p pfuc- gal NAcglc- gal- glc ceramide
l " INAcgal
BloodgroupA glycosphingolipid
.t-galactosaminidaseq-galactosidase
NAcglc- gal-glc- ceramide
I etooosrouposty""-:-i,j::3
TI
-]jj"'""rT!I 8)
g-galactosidase
GMIgangliosidosis
GMa angliosidosis,ertainypes
d g pNANA gal-glc- ceramide
Pc-ceramide--_-_-] l--------------+-eramide F sphingosine fattyacid
Niemann-Pickisease IT",b", rseas"1
blood cells.Seealso the legend or Figure 86-15.
ga l NAcglc- gal- glc-ceramide
Trihexosylceramidea-galactosidase
Figure 86-16. Parhways n the degradarion of sphingolipids ound rn visceralorgans ,nd red or whirefucose;h-Acglc, -- acetylglucosamine.
juvenileor Norrbotcnian orm. All areaurosomal ecessiveraits.Type 1, which accou ts tor 99lo of cases, asa strikingpredilec-tion for Ashkenazi ews,with an ncidence f about 1/1,000anda carrrer requencyof 1/18.
Gaucherdiseaseesults rom the deficientactivrtvof the lvso-somalhydrolase, cid p-glucosidase, hich is encodedby a genelocatedon chromosome q21-q31.The enzymaticdefecr esuftsin the accumulation f undegraded lycolipid substrates, artic-ularly glucosylceramide,n cellsof the reticuloendolhelial ystem.This progressive eposition results n infiltration of the bonemarrow,progressive epatosplenomegaly,nd skeleral omplica-tions. Four mr:tadons-N370S, L444P, 84insG, and IVS2-account or =957o of mutanr allelesamong AshkenaziJewishpatients, ermittingscreeningor this disorder n this population.Genotvpe-phenotypeorrelations avebeennoted, providing hemolecular basis or che clinical heteroseneity een n Gaucherdiseaseype l. which has a wide rangeof ieverityand agearonset, Patientswho are homozygous or the N370S muration
Lactosylceramide-galactosidase
GM1 angliosidosis,rabbe isease
glc-ceramide
o p p p pfuc- gal- NAcglc- gal-glc- ceramide- - fuc-gal-
t ^
gal I Fabry iseaso
Blood roup glycosphingolipid
P . ' S PNAcAal- gal- gal-glc- ceramide
I cnmsroe
_Lq-hexosaminidaseand B
GM2 angliosidosisSandhoff) NAcglc gal- glc-ceramide
tend to have later onset, with a more indolent course tpatients with one copy of N370S and another common allel
Clinical maoifestations of type 1 Gaucher diseasehave a vable age at onset, from early childhood to late adulthood, w
most sympromatic patients presenting by adolescence.Atsentation, patients may have bruising from thrombocytopenchronic fatigue secondary to anemia, hepatomegaly withwithout elevated liver function test results, splenomegaly,bone pain, Occasional patie[ts have pulmonary involvementhe time of presentatron. Patients presenting in the 1st decadequently are not Jewish and have growth retardation and a mmalignant course. Other parients may be discovered fortuitouduring evaluation for other conditions or aspart of routine exinations; these patients may have a milder or even a bencourse. In symp[omatic padents, splenomegaly s progressive
can become massive, Most patients develop radiologic evideof skeletal involvemenr, includrng an Erlenmeyer flask defotmof the djsral femur.Clinrcallyapparenrbony involvemenr,wh
gal gal glc-ceramide--_ll--------------r-at- gtc-ceramide
GM 3 angliosideneuraminidase
Sphingomyelinase

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 108/177
Fisure 6-17. Cells rom hespleen f a pacient irh Gaucher isease. char-
acteristicpleen ell s shownengorged ith glucocerebroside.
lieence are normal.-Thepathologic hallmark of Gaucher diseases the Gaucher cell
in the reticuloendothelial system,particularly in the bone marrow
(Fig. 85-17). These cells, which are 20-100 pm in diameteq have
a characteristic wrinkled paper aPp€arance resulting from che
presenceof irltracltoplasmic substrate inclusions. The cytoplasm
of the Gaucher cell reacts strongly positively with the periodic
acid-Schiff stain. The presenceof this cell in bone martow and
tissue specimens s highly suggestiveof Gaucher disease,although
it also may be found in patients with granulocltic leukemia and
myeloma.
Gaucher disease ype 2 is much lesscommon and does not havean ethnic predilection. ft is characterized by a rapid neurodegen-
erative course with extensive visceral involvement arld dearh
within the 1st 2 yr of life. It presents in infancy wi th increased
tone, strabismus, and organomegaly. Failure to thrive and stridor
caused by laryngospasm are typical. After a several-year period
of psychomotor regression,death occurs secondary o respiratory
compromise. Gaucher disease type 3 presents as clinical mani-
Iestations that are intermediate [o those seen n rypes 1 and 2,
with presentation in childhood and death by age 10-15 yr. It has
a predilection for the Swedish Norrbottnian population, among
which the incidence is 1/50,000. Neurologic involvement is
present but occurs later and with decreased severiry compared
with type 2 disease.Type 3 disease s further classified as types
3a and 3b based on the extent of neurologic involvement and
whecher there is progressivemyotonia and dementia (rype 3a) orisolated supranuclear gaze palsy (type 3b).
Gaucher diseaseshould be considered in the diflerential diag-
nosis of parients with unexplained organomegaly, who bruise
easily, have bone pain, or have a combination of these conditions.
Bone marrow examination usually reveals the Presence of
Gaucher cells. All suspected diagnoses should be confirmed by
determination of the acid p-glucosidase activity in isolated leuko-
crtes or cultured fibroblasts. The identification of carriers can be
achieved by enzymatic assa5 wirh confirmation of results by mol-
ecular resting in most Jewish families. Testing should be offered
to all family members, keeping in mind that heterogeneity, even
among members of the same kindred, can be so gleat that non-
symptomatic affected individuals may be diagnosed. Prenatal
ChaDter6 D.tectsr ile{.holism fLipids
diagnosis s available by dererminationoI enzyme activitychorionic villi or culturedamniotic fluid cells,
Treatmentof patientswirh Gaucherdisease ype 1 incluenzyme eplacement herapy,with recombinanracid l3-gludase (imiglucerase).Most extraskeletal symptoms (orga
megaln hematologicndices)are reversed y an initial debulkdoseof enzyme 60 IU/tg) administered y intravenous nfusevery other week. Monthly maintenance nzyme replacemimprovesbone structure,decreasesonepain, and induces opensarory rowth n affected hildren.A smallnumberof patie
have undergone onemarrow transplantation,which is curabut results n significantmorbidity and mortality from the pcedure,making the selectionof appropriatecandidatesimiAlthough enzyme eplacement oesnot al ter the neurologicpgression f patientswith Gaucherdiseaseypes2 and 3, it beenused n selected atientsas a palliativemeasure, articulin type 3 patientswith severe isceral nvolvement.Alternatrealments,ncluding he useof agentsdesigned o decreassyrthesis of glucosylceramide y chemical inhibition of g
coslceramide ynthase, re being evaluatedand efforts are aunder way to developgene herapy or type 1 disease.
NEIMANI{-PICKISEASENPD}. he original descriptionof Nwas what i s now known as type A NPD, a fatal disordeinfancy characterized y failure to thrive, hepatosplenom
and a rapidly progressive eurodegenerativeourse hat leaddeath by 2-3 yr of age.Type B is a non-neuronopathic oobservedn childrenand adults.Type C is a neuronopathicothat results rom defective holesrerolransport.All the subtyare inherited as autosomal ecessiveraits and displavvariaclinical earuresse e able86-15).
NPD typesA and B result from the deficientacrivity of asphingomyelinase, lysosomalenzymeencodedby a genechromosome1(11p15.1-p15.4).heenzymaticefectesuthe pathologc accumulation f sphingomyelin, ceramide hpholipid, and other lipids in the monocyte-macrophageysthe primary pathologicsite.The progressive eposrtion f spgomyelin n the central nervoussysrem esults n the neurogenerative ou$e seen n type A, and in non-neural issue nsystemic iseasemanifestations f type B, includingprogres
lung diseasen someparients.The acid sphingomyelinaseensequenced, nd a varietyof mutations hat cause ypesA anNPD are known.
The clinical manifestationsand course of rype A NPDunrform and is characrerized y a normal appearance t b(ahhough rhe newborn period is sometirnes omplicatedprolonged jaundice). Hepatosplenomegaly,moderate lphadenopathn nd psychomotor etardationareevidentby 6of age, ollowed by neurodevelopmentalegression nd deat3 yr. Wirh advancing ge, he ossof motor function and he drioration of intellecrual apabilit ies reprogressively ebilitaand in later stages, pasdcityand rigidity are evrdent.Affeinfanrs oseconractwirh their environment. n con trast o stereotyped ype A phenotype, he clinical presentationcourseof patientswith type B disease re more variable. M
are diagnosedn rnfancyor childhood when enlargemenr fliver or spleen,or boch, s detectedduring a roucinephysexamination.At diagnosis, ype B NPD patientsusually hevidence f mild pulmonary nvolvement,usually detectedadiffuse reticular or finely nodular infiltration on the chest ograph, Pulmonarysymptonrs suallypresent n adults. n mpatients,hepatosplenomegalys particularlyprominent n chhood, but with increasing inear growth, the abdominalpr
berancedecreases nd becomes ess conspicuous, n miaffectedpatients, he splenomegaly ay not be noted until adhood, and rheremay be minimaldiseasemanifestations.
ln some ypeB parients, ecreasedulmonarydiffusioncauby alveolar nfiltration becomes vident n late childhoodor eadulthoodand progresses irh age.Severely ffected ndivid

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 109/177
598 PAnTXr Mebbolic Dise€ses
may experience significant pulmonary compromise by 15-20 yr
of age. Such pacientshave low PO2 values and dyspnea on exer-
tion. Life-threatening bronchopneumonras may occur, and cor
pulmonale has been described. Severely affected patients may
have liver involvement leading to life-threatening cirrhosis, portal
hypertensron, and asc ites, Clinicall,v significant pancytopenia due
to secondary hypersplenism may require partral or complete
splenectomy; this should be avoided if possible becausesplenec-
tomy frequently causesprogressron of pulmonary disease,which
can be life-threatening. In general, type B patients do not have
neurologic involvement and have a normal IQ. Some patientswirh type B diseasehave cherry red maculae or haloes and subtle
neurologic symptoms (peripheral neuropathy).
Type C NPD patients often present with prolonged neonatalyaundice, appear normal for 1-2 yr, and then experience a slowlvprogressive and variable neurodegeneratlve course. Their
hepatosplenornegaly s lesssevere han tbat of patients with types
A or B NPD, and the-v may survive into adulthood. The Lrnder-
lying biochemical defect in type C patients rs an abnormality rn
cholesterol t.ansport, leading to the accumulalion of sphin-gomyelin and cholesterol in their lysosomes and a secondaryparrial reducrion in acid sphingom,velinaseactivi!y (seeChapter
86 .3 .In type B NPD patients, splenomegaly is usually the 1st man
ifestation detected. The splenic enlargemenr is noted rn early
childhood; however, in l'ery mild disease, be enLargement ma,vbe subtle and deteccionmay be delayed untrl adolescence r adult-
hood. The presenceof the characceristic NPD cells in the bonemarrow aspirates supports the diagnosis of type B NPD. Parients
\.rth type C NPD, however, also have extensive inliltration of
NPD ceLls n the bone marrorv and, thus, all suspected cases
should be evaluated enzymatically to confrrm the clinical diag-
nosis by measuring rhe acid sphingomyelinase acrivity level in
peripheral leukoc,vtes,cultured fibroblasts, or lymphoblasts, or a
combination of rhesecells. Parients with tvpes A and B NPD have
m arked l l dec reasedeve ls l - l 0 " i , r . whe r iaspa r ien rs i rh rupe
C NPD have someu.hat decreasedacid sphingomyeJinaseactivi-
lies, The enzymatic identification of NPD carriers is problemaric.
In families rn which the specific molecular lesion has been identified, ho\a.ever, amily members can be accurately tested for het-
erozygote status by DNA analysis. Prenatal diagnosrs of types Aaod B NPD can be made reliably by the measurement of acid
sphingomvelinase activif_y rt cultured amniocytes or chorionic
villi; molecular analys is of fetal cells can provide the speci fic diag-
nosrs or serve as a confirmatory test. The clinical diagnosis ofqvpe C NPD can be supported by the demonstration of filipin
stain positivicy in cultured libroblasts and./or by idendfying a spe-
ci6c mutation in rh e NP C gene.
There is no specific treatmert for NPD. Orthotopic liver trans-plancation in an infant with type A disease and amniocrc cell
transplantation in several type B NPD patients have been
atrempted rvirh little or no success.Bone marrow ttansplantation
in a small number of trpe B NPD patients has been shown to be
successful n reducing rhe spleenand liver volumes, he sphin-gomyelin content of the liver, rhe number of Nlemann-Prck cells
in the marrow, and radiologically detected infiltration of thelungs. ln one patient, horveve! liver biops ies taken up to 33 mo
post transplantation showed only a moderate reduction in stored
sphingomyelin. To date, lung transplantat ion has not been per-
formed in any severelv compromised patient with cypeB disease,
although two patients who underweflt whole lung lavages with
variable results have been reported.
Future prospects or treatment of rrpe B disease nclude enzyme
replacemenr and gene therapy. Treatment of rypes A and C
disease s presently precluded by the severe neurologic involve-
ment,
FABRYDISEASE, his condition is an inborn error of glycosphin-
golipid netabolism characterized by angiokeratomas(relang-
rectatic skin lesions), hypohidrosis, corneal and lenticuLar op
nes! acroparesthesias,and vascular diseaseof the krdnel', he
and/or brain (seeTable 86-161. The drsease s an X-linked re
srve rart tha! is maflrfested n affected males and has an estimprevalence of =1/40,000 males, Later-onset affected males w
residual c-galactosidase A activity may present with car
and./or renal disease ncluding hyperrrophic cardiomyopathyrenal failure. Heterozvgous females for the classrcphelotype
be asymptomatic or as severely affecred as the males, the vabihtv due to random X-i[activation. The disease results f
the delicient activity of cr-galacosidase A, a lysosomal enzencoded by a gene ocated on the long arm of the X chromoso(Xq22). The enzymatic defecc eads to the systemic accumulaof neutral glycosphingolipids, primarily globocnaosylceramparticularly in the plasma and lysosomes of vascular endoth
tion, leading to the major diseasemanifestations. The CDNAgenomic sequences encoding c-galactosidase A have identimore than 200 differenr mutations in the d-galactosrdaseA g
that are responsible for this lysosomal storage disease, nclud
amrnoacid substitutrons, gene earrangements, and nRNA srng oetecls,
Affected males with the classicphenotype have the skin lesiacroparesthesias, hypohidrosis, and ocular changes, whe
males wrth the later onset phenotypes lack these frndingspresent with cardiac and/or renal drsease rn adulthood-classic angiokeratomas usually occur in childhood and ma,v
to early diagnosis, They increase n size and number wi rh age
range from barely visible to several mm in diameter The les
are puncta[er dark red to blue-black, and flat or slightly rai
They do not bJanch with pressure, and the larger ones may sh
shght hyperkeratosis. Characteristicall]', the lesions are m
dense between the umbilicus and knees, rn the "bathrng tru
area," but may occur anywhere, incLrding the olal mucosa.hips, thighs, buttocks, umbilicus, lower abdomen, scrotum,glans penis are common srfes, and there is a tendency towsymmetry. Variants without skin lesions have been describSweating is usuall y decreased or absent. Corneal opacitiescharacteristic lenticular lesions, observed under slit-lamp exa
nation, are present n affected males as well as n =707. of asl'tomahc heterozygotes. Conjunctir.al and retinal vasc
tortuosity is common and results from the systemic vasctnvolveme11t.
Pain is the most debilitating symptom in childhood and a
lescence. Fabry crises, lasting from minutes to several d
consist of agonizing, burning pain in the hands, feet, and pro
mal extremiries and are usuall,v associatedwith exercise, atigfever, or a combination of these facrors. These painful aparesthesias usually become less frequent in the 3rd anddecades of hfe, although in some men, they may become mfrequent and severe.Attacks of abdominal or flank pain may s
ulate appendicitis or renal colic.The major morbid symptoms result from the progres
involvement of the vascular system. Early tn the course of
disease, casts, red cells , and lipid inclusions with characterbirefringent "Maltese crosses" appear in che urinary sedim
Proteinuria, isosthenuria, and gradual deterioration of renal fu
tron and development of azotemia occur in the 2nd through
decades. Cardiovascular f indings may inc lude hvpenension,
ventricular hvpertroph,v, anginal chest parn, myocardral ischeor infarc tion, and heart failure. Mrrral rnsufficiency rs the m
common valvular lesion. Abnormal electrocardiographrcechocardiographic findings are common, Cerebrovascular mfestations result from multifocal small vessel nvolvement. Ot
features maf include chronic bronchit is and dyspnea, lyphedema of the legswithout hypoproteinemra, eprsodic diarrhosteoporosls, retarded growth, and delayed puberry Death m
often results ftom uremia or vascular diseaseofthe heart or br

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 110/177
Before hemodialysis or rena transplantation, the mean age at
death for affected rnen was 1yr' Later onset cardiac varianis
with resrdual u-galacrosidaseA activiry have cardiac diseaseand
may have mild proteinuria but usually have normal renal func -tion for age, Thi cardiac manifestations include hyperrrophy of
the left ventricular wall and interventricular septum, and elec-
trocardiog hic abnormalities consislent *ith cardiomyopach,v-
Others ha had hypertrophic cardiomyopathy or myocardial
angiokeracornasof the scrotum (Fordyce disease)or from angiok-
eratoma clrcumscriptum. Aogiokeratomas identlcal to lhose of
Fabry disease have been reported in fr.rcosidosis,asparryJgly-
cosaminuna! Iate-onsecGMr gangliosidosis, galactosialidosis, cr-
N-acetylgalactosaminidase deficienry, and sialidosis. Latel onse!
variants have been rdentified among chronic hemodialysis
pacients. Like the cardiac variants, these renal varianrs lack the
early classic manifestations such as the angiokeratomas, acro
paresthesias, vpohidrosis,and corneal opaclt ies The dragnosis
of classic and variant patients is confrrmed biochemicall,v by the
demonstrarron f markedly decreased t-galactosrdase activit,v
in plasma, isolated leukoryces, or cultured fibroblasts or
lymphoblasts.
Heterozygous iemales may h e corneal opacines, solated skrn
lesions, and intermediate activi s of cr-galactosidase in plasma
or cells. Rare female heterozvgotes may have manifestarions as
severe s rhose n aifectedmales.Asymptomatic at-rtsk females
in families affected by Fabry disease,however, should be opti-
mally diagnos by the direcr analysis of their family's specifrc
mutarion. Pre tal detection of aftected males can be accom
plished bv chedemonsrration of defrcient o-galactosidaseA activ-
ity or the family's specrfic Sene mutarion in chorionic villi
obtained in the ls! trimester or in cultured amniocltes obtained
by amnrocentesis n the 2nd rrimester of pregnancn Fabry disease
ca n potentidlly be dececred newborn screening.
Tieatment for Fabry drse was once nonspecific and limired
of 1mg/kg er.ery other week.
FUG0SlD0SlS.his is a rare autosomal ecessrve isordercaused
by the deficrent accivity of c fucosidase and the accumulation
oi fucose-containrng glycosphingolipids, glycoproteins, and
type, with the most severely affected patients presentng rn the
1st yr of life with developmental delav and somatic fearures
similar to those of the mucopol;rsaccharidoses.These features
rnclude frontal bossing, hepatosplenomegall', coarse facial fea-
tures, and macroglossra. The central nervous system storage
results in a relentless neurodegenerative course, with deach in
childhood- Patients lr'ith milder diseasehave angiokeratomas and
longer survrval, No specific therapv exisrs for the disorder, which
can be diagnosed bv the demonsrration of deficrent cr-fucosidase
activity in peripheral leukocytes or culcured fibroblasts. Carrier
Chatter 6 . Delscb n Metabolism l Lipids
identif ication rudies nd prenataldiagnosis repossible y d
mination of the enzymacic cciv ity.
SCHIN0tERDISEASE. his is an aLrtosomal ecessrve eurode
eratrve disorder that results from the defrcienr accivitv of
acetylgalactosaminidasend the accumulationof sialylate
asialoglycopeptidesnd oligosaccharidesse eTable 86-15)
gene for the enzyme is mapped to chromosome(,22913 1-1.3 2), The disease s clinically heterogeneous,and
major phenotypes have been dentr6ed. Type I disease s an mlile-onset neuroaxonal dystrophy. Affected infants have no
development for the 1st 9-15 mo of life followed b,va rapid
rodegenerarive course that resuhs in severe psychomotor r
daoon, corcical blindness, and frequent myoclonic seizures.
l[ drseases characterized y a variable age al onset!mrld r
dation, and angiokeratomas. There is no specific therapy
eicher form of the disorder, The diagnosis is by demonstr
of the enzymatic deficiency in leukocytes or culcured
fibroblasts-
METACHR0MATIC EUK0DYSTR0PHYMLD).This is an autos
recessivewhite matter disease caused by a deficiency of arv
fatase A (ASA), which is required for the hydrolvsis of sul
gl,vcosphmgolipids. Another form of MLD rs caused b,v a
cienc;r of a sphingolipid actrvator protein (SAP1), rvhirequired for che ormation of rhe subsffate enzyme complex
deEciency of this enzymatic activiry results in the white m
storage of sulfated glycosphingolipids, which leads to dem
nation and a neurodegenerativecourse. The ASA gene s on
mosome22 (22q13.31qter); pecif icmutations are knou'n t
inro rwo groups rhat corlelate with diseaseseverity,
The clinical manifestatiors of tbe late inlantile form o{ M
which is most common, usually presents between 12 and 1
of age as irritabilitJ', inabrlity to walk, and hyperextension o
knee, causinggenu recurvatum.Deep tendon reflexes re d
ished or absent. Gradual muscle wasting, weakn€ss! and h
tonia become evident and lead to a debilitated state. A
diseaseprogresses,nystagmus, myoclonic seizures,optic atro
an d quadriparesis ppear,wirh deach n the 1scdecade f lif
Table 86-16).Th e iuvenile orm of the disorderhas a more lent course with onset rhat may occur as late as 20 yr of age
form of the diseasepresencsas gait dJsturbances,mencal de
ration, urinary inconrinence, and emotionat di fiicultres. The
form, which presents after rhe 2nd decade, s similar to the
nile form in its clinical manifesrations, althou8h emotxtnal
culries and psychosis are more prominent features. Deme
seizures,diminished reflexes,and optic atrophy also occur in
rhe juvenile and adult forms. The pathologic hallmark of M
rs che deposition of metachromatic bodies, which stain str
positive with periodic acid-Schiff and alcian bLue, n rhe w
matter of the brain. Neuronal rnclusions may be seen n the
brain, pons, medulla, recina, and spinal cord; dem,velin
occurs in the peripheral nervous syslem. Bone marrolv t
plantation has resuhed in normal enzymatic levels in p
heral blood buc no clear evidence for clinical efficacy in of che neurologic coursei support ive care remains the pri
rntervenuon.
The diagnosis of MLD shor,rldbe suspected o patients wit
clnical fearures of leukodvs trophy. Decreasednerve condu
velocit ies, ncreased erebrospinal lui d protern, metachro
deposics n sampled segmentsof sural nerve, and metachro
granules n urinary sedrmenr re all suggestive f MLD. C
marion of rhe diaenosis is based on the demonstracion o
reducedactivity of ASA in leukocyces r culturedskin librob
Sphingolipid activaror protein deficiency is diagnosed by
suring the concentrauon of SAP1 in cultured fibroblasts us
specific antibody to the prorein. Carrier deteccion and pre
diaenosis is available for all (orms of the dtsorder.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 111/177
m0 r PARTX MctabolicDiseases
MUITIPLESULF SE DEFICIENCY his is an autosomal recessivedisorder that results from the deficiency of three enzymaric acdv-ities: arlrlsulfatasesA, B, and C. Sulfat ides, mucopolysaccharides ,steroid sulfates, and gangliosides accumulate in the cerebralcortex and visceral tissues, resulting in a clinical phenotype withfeatures of leukodysrrophy as well as those of rhe mucopolysac-charidoses. Severe chthyosis may also occur. Carrier testng andprenatal diagnosis by measLrrement fthe enzymaric activities canbe performed. There is no specific treatmenr for multrple sulfa-tase deficrency other than supportive care.
KRABBE 0ISEASE. This condition, also called globord cellleukodysrrophn is an autosomal recessive fatal disorder ofinfancy. lt results from che deficiency of the enzymatic activity ofgalactocerebrosidaseand the whire matter accumulation of galac-
rosylceramide, which i s normally found almosr exclusively in chemyelin sheath. The galactocerebrosidasegene is on chromosome14 (14q31), and specif icdisease ausing mulalions are known.The infantile form of Krabbe disease s rapidly progressive andpatrerts present in early infancy wich irritabil ity, seizures, andhypertonia (seeTabJe85-16). Optic atrophy is evident n th e lstyr oI hfe, and mental development is severely impaired, As thediseaseprogresses,opcic arrophy and severe developmental delal'become apparent; affected children exhibit opisthotonos and die
before 3yr
of age. A second, ate infantile form of Krabbe diseasealso exisrs and patients present atter the ageof 2 ;'r Affected indi-viduals have a diseasecourse similar to thar of the earll, infantile
form. Bone marrow cransplantation has been attempted in severalpatrents wirh later onset disease but without signifrcanc results,Umbilical cord blood transplantation of presymptomatic parients
in the 1st 2 mo of life results in ensraftmenr and normal bloodgalactocerebrosldase evels. Developrnental milestones, cerebralmyelination, and cognitive funcrion up co 3 yr of age have beennear age-appropriate expectatrofls. Nonetheless, some patien!sdemonsrrate mild ro noderate language delays and mild to severegross motor deLavs.The diagnosis of Krabbe disease elies on thedemonstration of the specrficenzymaric defrciencv n u'hite blood.e l l s , , , r u l t u red k i n f ib rob las t r . a r r ie r den t i f i ca r ionnd pre-
natal diagnosis are available.
FABBER ISEASE. his is an aulosomal recessive isorder thatresults from the deficiency of the lysosomal enzyme ceramidase
and the accumulation of ceramide in various tissues, especiallyrhe joints. Symptoms can begin as early as the 1sr yr of life withpainful jornt srvellingand nodule formation (Fig. 85-18), whichrs sometimesdiagnosedas rheumatoid arrhrit is. As che diseaseprogresses, nodule or granulomatous formation on the vocalcords can lead to hoarsenessand breathing difficulties; failure tothrive is common, In some patients, moderate central nervoussystemdysfuncnon s presenr seeTable 86-16).Parientsmay dreof recurrent pneumonias in their leens; there is currently no spe-cific therap,v-The diagnosrs of this disorder should be suspectedin patienrs who have nodule formacion over the loints but noother lindings of rheumatojd arthritis. In such patrenrs, cerami-
dase activrt,vshould be determined in cultr-rredskin fibroblasts orwhite blood cel ls. Carrier deteccion and Drenatal diaqnosis areavailable.
WOIMANDISEASENDCHOI.ESTEROLSTERTOBAGEISEASE(CESD). hese are autosomal recessive ysosomal storage diseasesthat resulr from the deficiency of acid lipase and the accumula-non of cholesterol estersand triglycerides in hrstiocytrc foan cellsof most visceral organs. The gene for lysosomal acid lipase is onchromosome10 (10q24-q25). (/olmandiseases !he more severeclnical phenotlpe and is a fatal disorder of infanc,v.The clinicalfeatures of che disease become apDarert in the 1st rvk of life andinclude failure to thrive, relentliis vomiting, abdominal distention, steatorrhea,and hepatosplenomegaly see Table 86-16).
Figurc 86-18, Forerrm of an 18 rno old girl wich Farber disease.Note tpainful joint sweiling and the nodule formarion. The infanr rvassuspecte
having rheumatoid arthritis
There usr.rally s hyperliprdemia. Hepatic dysfunction and Iibrsis ma,v occur. Calcification of the adrenal glands is pathognmonic for the disorder. Death usuallv occurs wirhin 5 mo.
Cholesterol ester storase disease s a less severe disorder thmay not be dragnosed un;il adulrhood. Hepatomegaly can be tonly detecrable abnormaliq., but af fected individuals are at snificant risk for premature atherosclerosis. Adrenal calcilicatiois not a feature.
Diagnosis and carrier identification are based on measuriacid lipase actrvity rn leukocyresor cultured skin fibroblasts. Prnaral diagnos is depends on measunng decreasedeozyme levels
cultured chorionic villi or amniocytes. There is no speci6c heraavailable for either disorder, although pharmacologic agents suppress cholesterol synrhesrs, rn combination lvith cholestyrmine and diet modilication, have been used in patients with chlesterolescer toragedisease se eChapter 86.3).
Charrow J, Andenon HC, Kaplan P, et al, Enzyme replacemenr herapy a
monitorins for children wirh rvpe r Caucher d,sease:Consensus ecomendationsI Pediatr 2004;144:112 120.
Clark JTR: Naiiarive revier': Fabry disease.An lflten Med 2007;14
425433.
Desnick Rl, Brady R, Barranser J, er al: Iiabry disease,an under recogr z
multi systemic disorder: Experc recommendadans or diagnosis, mana
ment, and enzvme replacemenr therapy. Arz lnten Med 2003.13
t38-345.Elstein D, Abrahamov A. Hadas Hrlpern I, et al: Cauchcr's lisea,\e. dn
2001;358:324 37
Escolar ML, Poe N{D, ProvenzaleJM, et aL:Trarsplantarion of umbilicafcoblood in babies with inhntile Krabbet disease. N Ehgl I M
2005i20:2069-2080.
Johnsor V/G: The clinicat specrrum of hexosamrnidase eiciency diseaNewolosy 1981i3r tl4 53 1456.
Kaplan B And€rson HC, Kacena KA, YeeJD: rhe clinicaLand dcnograph
characrerisrics f nonncuronpathicGaucherdisease n 887 children ar dianosis Arch Pedidtl A.lolesc Med 20O6;16U603-608
Meikle PI, Ranien E. SimonsenH, et al, Nervborn screening or lvs(xomsrorage disorders: Clnical evalDation of a rrvo tier straregl Pedidr2004i114:909-916
Mistry PK, Abraharnov A: A practicalapproach ro diagnosisand manasem
of Gaucher'sdisease.BaillieresClin Hdenatol I997;I0:8] .-8l8

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 112/177
SchuchmanEH, Desnjck RJ, Types A and B Niemann Pick drsease n Scriver
CR. BeaudetAL, Sty rWS.er al leds)tThe Metabolic and Mole.ulat Bases
of lnherited Dsease, 8rh ed. New York, Mccraw Hill, 2001
Wilcox wR, BanjkazemiM, Guffon N, et al: Long rerm safetvand efficacvcf
enzyme replacement therapy for Fabry djsease. Am I Hun Cenel
20O4t7 ;65-74.
Chaplert r oelects r Metabolism l Carbohydrates 6
Carbohydrate synthesis and degradation provide the ener
required for mosr metabolic processes.The importanr carboh
drates include three monosaccharides-glucose, galactose, afructose-and a polysaccharide, glycogen. The relevant br
chemical pathways of these carbohydrates are shown in Figu
87-1. G|,rcose s the principal substrare of energy melabolism,
conrinuous source of glucose from dietary mtake, Sluconeogesrs, and glvcogenolvsis of glycogen maintarns normal blo
glucose levels. Metabolism of glucose generates adenos
triphosphate (ATP) via glycolysis (conversion of glucose or glyc
gerr o pyruvate), mitochondrral oxrdative phosphorylation (co
version of pyruvate to carbon dioxide and water), or bot
Dietary sources of glucose come from ingesting polysaccharid
primarrlv starch and disaccharides, including lacrose, maltos
and sucrose. Oral intake of elucose s rntermirtent and unreliab
Glucose made de novo from amino acids , primarily alanine (g
coneogenesis) contribures to maintarning the euglycemic sta
but this process requires time to be acrive. The breakdown hepatic glycogen provides the rapid release of glucose, whi
mainrains a constanc blood glucos€ concentratlon. Glycogen
also the primarv stored energy source rn muscle, providin
glucose for musc le activity during exercise. Galactose and fru
!ose are monosaccharides rhat provide fuel for cellular metab
lism; their role is less significanc than chat of glucose. Galacto
rs derived rom lactose galacrose glucose),which rs found
milk and milk pruducrs.Calactose s an imporrant energl 'our
rn rnfanrs, but i t is 1st merabolized ro glucose. Galactose (exog
nous or endogenously synthesized rom glucose) s also an impo
tant component for cenain glycolipids, glycoprotetns, a
glycosaminoglycans . The dietary sources of fructose are sucro
(fructose + glucose, sorbirol) and fructose itself, lvhich is fou
in fruits, vegetables,and honey.
Defects in glycogen metabolism rypically cause an accumution of glycogen in the tissues,hence rhe name g/lcogen stora
disease Table 87-1). Defects in gluconeogenesisor rhe glycoly
pathway, includng galacrose and fruccose metabolism, do n
resulc n an accumulation of glycogen (see Table 87-1). T
defects n pyruvare rnetabohsm in rhe parhv-ay of rhe conversi
of pyrr-:vate to carbon dioxide and water via mrtochondr
oxidarive phosphorylarion are more often associated rvirh lac
acidosisand some issueglycogenaccumulation.
87.1 Gr-vcocrr ToRAGETSEASESPriya .KishnanindYuan-Tsonghen
The disorders of glycogen metabolism, the glvcogen storage deases (GSDs). result from de6ciencies of various enzymes
transport proleins in the pachways of glycogen metabolism (
Fig. 87-1).The glycogen ound in thesedisorders s abnorma
quanrrq; quality, or borh. GSDs are calegonzed by numeric ryin accordance with the chronologrc order in which these en
matic defects lvere identified. This numeric classification is s
widely used, at leasr up ro number VlL The gJycogenstorage d
eases can also be class i6ed bv organ inr.olvement and clinic
manifestations into liver and muscle glycogenoses (see Ta
87-rJ.There are more than 12 forms of gl,vcogenoses,lucose
phosphatase eficiency type l), lysosomal acid cr-glucosideficiency type Il), debrancherdeliciency type III), and liv
86.5 Muc0LlPt0osEs.ar$aret . McGovernandRobert. Desnick
I-cell disease mucolipidosis II [MLl!) and pseudo-Hurler poly-
dystrophy (mucolipidosis III IML-IU) are biochemically related'
rare autosomal recessive disorders that share some clinical fea-
activities. The enzyme that catalyzes the lst step, the UDP-N-
enzymatic levels n cultured skin fibroblasts. Direct measuremenc
of the phosphotransferase accivitv is possible. Prenatal diagnosis
and carrier identificaoon studies are available for both disorders
by measurenent of lysosomal enzymaric activities rn cultured
cells. Neonatal screening by tandem mass spectroscopy may
detect -cell disease.
l-CEtt DISEASE. his disorder shares many of the clinical mani-
festations of Hurler syndrome, although there is no mucopolysac-
chariduriaand the presentadon s earlier seeTable 86-16).Some
parienls ave clinical features evident ar birth, including coarse
facial fe ures, craoiofacral abnormalities, restricted joint move-
ment, and hypotonia. Nonimmune h1'dropsmay be present n the
fetus. The remainder of patients present in the 1sr yr wich severe
psychomotor retardation, coarse facial features, and skeletal
manrfestations that include kyphoscoliosrs and a lumbar gibbus.
Parients may also have congeniral dislocation of t he hips, inguinal
hernias, and gingival hypenrophy. Progressive, severe psy-
chomotor retardation leads to death in earlt' childhood No
lreatment is available.
PSEUD0-HURtEFP0tYDYSTR0PHY- seudo-Hr-rrlerpolydystrophy
is a less severe disorder than I-cell disease,with later onset and
survival to adulchood reported. Affected children may present
around the age of 4 or 5 yr wich joint stiffness and short starure.
ings include corneal clouding, retinopathy, and astigmatism;
visual complaints are uflcommon (see Table 85-15). Some
patients have learning disabilities or mefltal retardation. Treat-
menr, which should include orthopedrc care, is symptomaric.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 113/177
\
Debrancher
./'o*' Galactos€
l l - - -__-_-- . - - - , - -_-_-- -
1-P Uridvl Enslerase
t+ Phosphohexoseisomerase
{otc-o ase
Glucose Fruclose_1,6+J phosphotrucbkrnaseotpnospna€se r
F-1,.6-P, F-1-P<- Fructl l
Aldoiase 5.\G lyceraldehyde 'l Aldolaser - '
Glyceraldehyde-3-P- Dihydrcxyacelone-P
tlPhosphotrioseisomerase
ll Glyceraldehyde-3-Pehydrooenas€
l,3.Bisphosphoglycerale
f{ ehosphostycerate inase
3-Phosphogiycerate
llPhosphoglycerate utase
2-Phosphoglycerat€
1+ Enoiase
Phospho€nolpyruvale
I Pyruvate imse
I Lactaledehydrog€nas€Pytvale . . _ Laclale----Z'-\-
GSa=z csb
UDP-Glc
6m r PABTXT Metabolic iseases
phosphorylase kinase deficiency (t-'-pe X) are the most common
that rypicallv presenr n early childhood; myophosphorylase de6-
ciency (type V, McArdle disease) s the most common in adoles-
cenrs and adults. The frequenc,vof all forms of GSD is =1/20,000
live births.
TIVERTYCOGENOSES
The GSDs rhat principally affect the liver include glucose-5-phospharase deficiency (type I), dehranching enzvme deficiency(type Ill), branching enzvme deliciency (t,vpe V), liver phospho-
rvlase delicienc,v t),pe VI), phosphorylase kinase deficiency (type
IX, tbrmerly rermed GSD VIa), glycogen s,vnrherasedelicienc,v(type 0), and glucose transporter-2 defect. Because heparic car-
boh,vdrare merabohsm is responsible for plasma glucose home-
oscasis, rhis group of disorders typically causes fasting
hypogl,vcemiaand hepatomegalv. Some(rvpe III, tvpe IV, tvpe IX)
caD be associaredu.ith crrrhosis- Other organs can also be
fiBure E7 t- Parhlvav elated ogen storagedlseases nd galacto
tructose disorders GSa, aclivegen synrhetase;CSb, inactLvefl,vsvntherase;Pa! actLvephospho
Pb, nactive phosphorylase; 'aI.
phorylase a phosphatase;Pb(a.
phosphorylase kinase;PbKb, in
phosphor,vlase kinase; G, gly
rhe primer for glrogen synrhesi
uridine diphospharc; CLUT-2, g
rransporrer 2; NADA,'ADH, nnamide-adenrnedrnucleotide (
fied from Beauder AR: Gly
slorage disease n IsselbacherKl
lcdsl Haltison s PtinctpLes f In
Medi.ine, 13th ed. \ew
McGraw-Hill, 1994 Rcprcduce
permission ot The McGrar
Companies.)
involved and may manifest as renal dvsfunction in type Imyopathy (skeletal and/or cardiomyopathy) rn types Ill an
as rvell as in some rare forms of phosphorylase kinase deficr
TYPE GLYCOGENTORAGEISEASEGLUCOSE,6"PHO
0RTRANSL0CASEEFICIENCY,ONGIEBKEISEASEI.vpei . causedhv rhe absence r deficiencroi gluco'e-o-ph,r'ph
activity in the liver, kidney, and intestinal mucosa. It cadivided inro trvo subtypes: type Ia, in vr'hich the gluco
phosphataseenzyme is defeccive;and rype Ib, in u'hich a tra
case that transports glucose-5-phosphate across the microsomembrane is defeccive.The defects in both tvpe la and rvp
lead to inadequate hepatic conversion of glucose 6 phospha
glucosechroughnormal glycogenolysis nd gluconeogenes
make affected individuals susceptible o fastrng h,vpogl,vcem
Tvoe I GSD is an autosomal recessivedisorder. The srruc
gene or git cose 6 phosphatase s located on chromosome 17
th e gene for rranslocase s on chromosome 11q23. Com
mutarions responsible for the disease are koown. Carrier d

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 114/177
Chapter8 7 D e fe c ts n M et a bo l is m f C a .b o hv d ra t es
0t50nDER5
L|vEn tY(06E1.105t5
Type/Commoname1.1\r,rnerk
tc
lla/(or r orber
0
VlAfda5ef
l l er5
PlLrjpho 5ek a5e9ii !n{!
6li.cqen yr helir5ePir nq
tan(cn B1:€ 5yndron-'
MUs(trLYC06tt{05ts
Typ./(ommonlame
qi]L t
Ddnonl5edSe
PRKA[]eh(enq
!/t1:Adle
\il/T::ui
Pho$hoql)'cerdtend!ee']i?rq_
Phojphcql/aerdt€rrajeeh( nrl
La(ire ehidqsriie eh:i?niI
GAIACTOSTISORDtRS
Gala(mJernvr h ?15ferneeh(1e1:y
Gid(ok aie ehferar
G?f€ftlzedl03 dpi05r.dte!,lbilcie+epir!G5c ei( fc!
FNUOO5EISORDERS
l55en.druo.riLrri
Heied.ri l l ruf tserl ]erince
DtSonDERSt GtU(0Nfff Ntsls
F((ore 6 drpho5phatd5eeh( nq
Ph0sphoefpyevaterblxl 1iiedehtieltl
DISONDERSf PYRUVATEITABOTISM
ryruvileihldrcqer;se0n etdefe.t
ry vaie rbrrlirccefief.l
lerpifttor)"l; I d.fet hx dit!e
cros!horili:orjea\!)
DIsOROERSNPTI'/TO5ETTAEOTISM
r;n!aldcb5eeF(re1ay
1bo5e phcrphaLetner?Jeeh(re1iy
BI5I(OEFECTs
a LriD5eplrojcha.i5t
a ucoie -pl05chal?rani ]t;5e
lypr rd mL5c:eebranthefieF(nr l
i ;m! .1,5 lu(051ft !el
LYsrebEnderelcenay,nom.
mi( een,ymi atvy
Erir.trgen2/,ie
L e 'pho5phorya5c
Pf05phoryasena5e
6 oqenynrhetaie
6 .ose rdsporteri6!tT l
Ardd qr(osdaseicd a ta5el
A.do quto5dd5e( d li tasel
A(doqJri5ldse(i (dala5elyjcScmal50taLe0elnDIaft
irlole ILAMPl)llVPa( \'atedrorek'r?5e
\l)'opno5prorybrPIr!phlrfruftk!!ePhir5phoqlycerdlea5e
\l rubure0tph05rhoqlie'dlenutare
M ub!r cf 3ctateetyCmgemre
aalarlo5e-pf $haterdylranft 5e
i,rhftkndJe
llIdrnepftspMie a]:tlcre
epTlera5e
FrJiroir-l-plosc[ale,rcare
Fru.r$E,6-dphctph;Ieie
Piosphoenclpyruvale.itortkrna5e
PyrLViredehydruqenr5e
fltv;tP car00rya5e(crnp r toV:mafyl toooldra
DllA urar!fi
L xtu o5e lrita5e
Tri f !al loaieRbirP ixc5phareornerdse
(urlrctt Pflt5tNTATj0N
:r,n,rrhrarda0on,hepailrmeqd,hlpoglyen;e vrteCloci
d(?le,(ra 5ftrcl,triqc4de,ancr i( d eveh
!;nea5 ipeh tr:haddr[00and E5 lneutroEnianiinpr re(]
nerLnpflLrdr0n
:h dfl]nd epJtcrrre_cal)'!rcvJthrrrdatonu5(ew€akre55,
h]'poqy:em;,lylenpdema,elevsieolranlamina5eve5verrymptcn;nprcvewlm,rqe
Lyart f rplcf i5dn?s n lp e a;f0mue5ymolom5
f. ure0 hr",a,h/iroronr;,epalcriela!;5prrome,qdly,roEe5\
arf ihci5ldeat l '5,dly"eforc5lhyI),elevaredrlan5anrnr5eve5
N.,p,Iomegdl,rlJhyiroqcnB. yperpderia,nc el0sl5
Heoatrn{r}n id 'rp0EicrD,lyffripide b,dndei [
[ary ,irn1q o\r5 esj fd ?tque,fa5tn!ypoqlycem,a [eto5i5
to e - r r . r . ^pp:r ' . o eqo)i l r! )4. ef aLlLld
dydun(i0rpa rd qur0send a ct05eti atorr
(a,l0meg.t/'y0rlonrr,llep,rlorieit,rlt0n5elJTthro
l'1pp:rhIdr .i rd nlcparh)"in5ahidhcod
l'1!0palh\1re5pGor!suli(en(yicnleradulthoodfllrertropnG(lrJm/ipdtrl
flyce(lphL:adr0lr0rirt,
:xer(!e 0ler;,ra,rrJ5ia(Irmp5xersedatgabi,vie. F .0h . r , i r0 [P d] d e1d.r/o0l 'b 'o
Aswrrl'lir?,]
Alwrt i ycet
1 '.
r 1 q ( " r - r - t / . d t d i , d r ' 1 d , d . ' d . d i . : J . "
iatardr5
! r rri. trdf5fera5eejiien(lwlrhcd 0nalfindq5 fhrpcmn
;fd nerYicrafnet
LlxnaiJi iLrbstan(eAC.reom fg,rwe;r €mJqy
ahrcni.:fdre.nhr e,epatr(fai lle
[p od hypoqlt(en,apner,aodl]j
Hipnqirn , fapdlcmPgai iripoton,fd,ureD hlve
!eie.a'atiecnai,r r ld tiorrt, a(t,cardo5is,psyclornotor
rcLlrcalcn, , lndrJrec f r 'e
)i l te; lacc\ 'eHei..raqpfec05!itl multi5)51:mvclvennt
UrneEluanqr"in;nie
La (r h0sri:iil r ure adon/,rpathy
Proqresgrrl?r(cena?phdll]parhldrrorerplerdeur0pdthy
(O/IIMENTS
[ormon,sererclpo_q'yi?F]
l0% l l lpe
fornon,nt€rmedateevet/ 0fiypc!t(er
l5%rlr ipe
Rlr neLfomu5iula,aranl!r t
[3.:,Denrqnyioqef05i
:ormcf,benF y(t lef 5!
Dftredseder y(ogentcre
:LtT eipressedv.tk,lrel,,ancreas
ntetIn..
i0m|Iaf,iird0r5pctor)"t c eading0d
Dy ge yr
Fe5dir?n iyre (t ly
Fejd,rdn4r ida(YUFarc,Inked
Arlosoral on:dnt
[]mrai ralep',"i1]minan(e
Pre$lentnJipane5snd shkenarle$l
Rdre,Xnked
FJrema ltyotpalrentsrc [ (znAme:r
Jre
Afr anAmercn ateIli ifd c haveiilCe
synflcmJ
B q r
Abeniqnarantlsc i!s
3enon
)roqnc55q00dl.h ruitosecitrctiorl
tcc0proq105r,avca5tnc
Rai?
\fon cn'mondrr o ] o hrnrt, .fert]i
Rare,dut,isonae(eri e
M ochoxdriaherit1t:
Be ln
Attcilma ies5lve
f ion and Prendlll (Li3Bn()srs1r c Lr()ssrble'rfh rhe I)N'\_l- 'ased
il theueonatalperiud virh hr prri: lvccmia rld acuc acidosisr he v
an.l proruherantabdomen Lrat ; .1ue o nlassive cpatomegelt:
rhc krdrevs ere also eniargcd, rrlcfcJs the spLeen nd heart are
norma .
Th c Lriochemical allrnarks of rhe discascerc hypoglvce
lacnc acrrlosrs, hypcr rriccnria. ,urci hvperlipicJerlia. Fl-
gLycernrand acricaci. losis aLr levelopeffer shorr ast.Hy
ur ceLria s prcscnr n voung children;guLrr arclv clcvelops e
f.Lrbertr.Dcspitc rnerked hepatoLregaLy,hc 1it,cr ransanr
letcl. er c usuall,v orLn.rlor onlr slighdv clcvarcd. ntenur
dilrr hea nra,v c.Llr tthe Llecherrisrns urrknorvn) liasy bru
:rnJ eprstaris lrc c(nrn()r1 rrJ rr-eessociatcd virh n prolor
blceding rrme as u ;esulr rrl inrp.rircil l ' l3rclef aegrcgirt ion
e.ihesion.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 115/177
6lN r PARTX MetabolicDis€ases
The plasma may be "milkv" in appearance as a result of a strik-ing elevauon of rrrglyceride evels. Cholesterol and phospholipids
are also elevated, but less promrnently. The lipid abnormaliryresembles type IV hyperlipidernia and is characterized byincreased levels of very low density Lpoprorein, low-densitylipoprorein, and a unique apolipoprotein profile consisting of
increased levels of apo B, C, and E, wirh relatrvely normal orreduced levels of apo A and D, The histologic appearance of theIiver is characterized by a universal distention of heparocytes byglycogen and far. The lipid vacuoles are particularll' large and
prominent. There is litde associared ibrosis,All these findings apply to both rype Ia and wpe Ib GSD, but
type Ib has addrtronal features of recurrent bacterial inlecrionsfrom neutropenia and impaired neutrophil funcrion. Oral andintestinal mucosal ulcerarron and inflammatory bowel diseasearecommon. Excepronal casesof rype lb wrthour neutropeniaan dtype Ia with neulropenra have been reported.
Although tvpe I GSD affects rnarnly the liver, multiple organsystems are involved. Pubert,v is often delayed. Virruallv allfemales haye ultrasound lindrngs consiscent with polycystic
ovaies; other features of polycystic ovary syndrome (acne, hir-sutism) are not seen. It is uncerrain whether rhis affects long-
term ovularion and fertilicy. There have been mutiple reports of
successfulpregnancy in adult rvomen with GSD I. Symptoms ofgout usually srart around pubertl' from long-term hyperuricemia.
Secondary co the hpid abnormalities, there is an increased nsk ofpancreatitis. The dyslipidemia, together with elevatederyrhrocyceaggregation, predlsposes these parients to atherosclerosls. Pre-mature arherosclerosis has rtot yec been clearly documented
except for rare cases. rnpaired platelet aggregation and increasedanrioxidatrve defense o prevent lipid peroxrdation may function
as a Drotective mechanism to helo reduce the risk of atheroscle-
rosis, Frequent fractures and radiographic evidence of osteopenia
are common; bone mineral content is reduced even in prepuber-
tal patiencs.
By the 2nd or 3rd decade of life, mosr patienrs wirh rype I GSDexhibit hepatic adenomas that can hemorrhage and, in somecases,become malignant, Pulmonary hypertension has been seenin some lons term survivors of the drsease.
Renal disiase is another complication, and most pacients with
type I GSD l,/ho are >20 yr of age have proteinuria. Many alsohave hypertension, renal stones, nephrocalcinosis, and alteredcreatimne clearance. Glomerular hyperfiltrarion, increased renalplasma flov; and microalbuminuria are often found in the early
stagesof renal dysfunction and carl occur before the onset of pro
teinuria. ln younger patienls, hyperfiltration and hyperperfusion
may be the only signs of renal abnormalities. With the advance-
men! of reflal disease, focal segmental glomerulosclerosis and
interstitial fibrosis become evident. In some patierrtsj renal func-
cion has detenorated and progressed o failure, requiring dialvsis
and transplancerion. Other renal abnormalities include amyloi-
dosis, a Fanconr-like syndrome, hypocitraruria, hypercalciuria,
and a distal renal rubular acidification defect.Diagnosis.The diagnosis of rype I GSD rs suspectedon the basis
of clinical presentacron and the laboratory findings of hypo-
glycemia, lactrc acidosis, hyperuricemia, and hyperlipidemia.Neutropenia is noted in GSD Ib pacienrs, typically after the 1st2-3 yr of lile- Administracron of glucagon or epinephrine resultsin litde or no rrse n blood glucose evel, buc the lactare level risessignificantly. Before rhe glucose-6-phosphatase and glucose-5-phosphate rranslocase genes were cloned, a definitive diagnosisrequired a liver biopsy. Gene-based mutation analvsis now pro-
vides a floninvasive $'ay of diagnosis for mosr patients with typesIa and Ib disease.
Taealmenl. Treatment is desrgned to maintain normal bloodglucose levels and is achieved by continuous nasogastric infusion
of glucose or oral administration of uncooked cornstarch. Naso-gasrnc drip feeding can be introduced in early infancy from rherime oi diaenosis. It can consist of an elemental enteral formula
or containonly glucose r aglucose olvmer o providesuffrcglucose o maintain normoglycemia urrng the night. Freqfeedingswith high-carbohydrateontentaregiveoduring he d
Uncooked ornsrarch ctsasa slow-releaseorm of elucosecan be ntroduced r a doqe f t.6 g/kgevery hr foi rnfantyr of age.The response f young nfants s variable.As the cgrows older, the corns tarch egrmencan be chaoged o ev6 hr at a doseof 1.75-2.5g/kg of body werght,Becauserucand galactoseannotbe converted irectly o glucosen GSD I, these ugars re restrictedn the diet. Sucrosetablesugar,
sugar, rher ngredients),ructose fruit, juice,high fructoses;rrup), actose dairv foods),and sorbitol shouldbe avoidelimited, Due to thesedietary resrrictions, iraminsand minesuchas calcium and viramin D may be deficientand supplemration is required to preveflt nutritional deficiencies.Dietherapy mproveshyperuricemia, yperhpidemia, ndrenal ution, slowing he developmenr f renal ailure.Thrs herapy ahowever, o normalze bloodurrc acidand ipids evels omplein some ndividuals,despitegood metabolic control, especafter pubeny,. he control of hyperuricemia an be further amenredby the use of allopurinol, a xanthine oxidase nhibiThe hyperlipidemiacan be reducedwith lipid-lowering drsuch as HMG-CoA reductasenhibitors and fibrate(seeCha861.Mic roa lbuminur ia .near lynd ica to rf rena l ys funcrrype disease,s treatedwith angiorensrn-convertingnz
(ACE) inhibitors. Citrate supplementscan be beneficialparienrs with hypocitraturia by preventing or amelioranephrocalcinosrsnd development f urinary calculi.
In patientswith r1'pe b GSD, granulocrte and granulocmacrophage olony-+timulating actorsare successfuln corring the neutropenia,decreasing he number and severirbacterial nfections, and improving the chronic inflammaboweldisease.
Orthotopic liver transplaltation is a potential cure of typGSD, but the inherenrshort- and long-termcornplicarionsethis as a treatm€nrof last resort, usually or patientswith limalignancn muhiple liver adenomas,merabolicderangemrefractory !o medical management, nd/or liver failure. Laadenomas >2cm) that are rapidly increasing n size andnumbermay requirepartial hepatic esecuon.Smalleradeno
(<2 cm) can be trearedwirh percutaneous thanol njectiontranscatheter rterial embolizatron.
Beforeany surgical rocedure,he bleeding rarusmust be euated and good meraboliccontrol established. rolongedbleing times can be normalizedby the use of intensive nlraven
glucosenfusion Ior 2448 hr beforesurgery.Useof l-deami8-o-argininevasopressinDDAVP)can reducebleeding omcations. Lactated inger solution should be avoided becaucontains actateand no glucose,Glucose evelsshould be matained in the normal range hroughout surgerywith the use107o dextrose.
Prognosis. reviously,many patientswith rype GSD died young age, and the prognosiswas guarded or chosewho svived.The ong-rerm omplications ccurmostly n adultsu'hdisease as not adequatelyreatedduring childhood.Early d
nosis and effectiveEeatmenthave moroved he outcome: edi*ease nd lormationof heparic denomas rL hporenriafor malignantrransformation emaln serious omplications.
TYPEII GIYCOGEN TOBAGE ISEASEDEBRANCHEREFICIEtlMlT DEXTBINOSIS).ype III GSD is causedby a deficiencglycogendebranching enzyme activity. Debranching enzytogetherwith phosphorylase,s responsibleor completededationofglycogen. (hen debranchrngnzyme s defective, lygen breakdown s incompleteand an abnormal glycogenwshort outer branchchainsand resemblineimit dextrin acculares. Deficiencyoi glycogendebranlhing enzvme cahepatomegaly,hypoglycemia,short stature, variable skemyopathy, and variable cardiomyopathy.The disorder usu

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 116/177
involves both liver and muscle and is termed tvpe IIIa GSD. In
=157. of patients, the disease appears to involve only liver and
Droaressiveweaknes. and waslinS. Myopathy does no t follow
any-parricularpatrern of involvementlboth proximal and distal
-uril"t ,t" involved. Electromyography reveals a widespread
mvopathyi nerve conduction srudiesmay be abnormal. Venrric-
ular'hypenrophy is a frequent finding, but overt cardrac dv s
funcdon is rare. Hepatic symptoms in some patients may be so
mild that rhe diagnosis is not made until adulthood, when che
develoPmenr n a pati€nt wrrh tvpe IIIb glycogen
nt has debrancherdeficrencv n livs but normal
d, he had hepatomegalv, vpogtvcemia, nd growth
he no lonsef bad h€patomegalvor hvpoglvcemia'
s normal He had lro muscleweakn€ssor atroph,vi
this is in contrast to rvpe IIIa pari€nts, n whom a progressivemvopathv rs
ChaDter7 r Dolectsn Metabolism l Ca.bohydroles
patients show symptoms and signsof neuromuscular disease.T
initial diasnosis has been confused with Charcor-Marie-Too
disease.Polycystic ovaries are common; fertilrt,v,however, is
reouceo.
Hypoglycemra and hyperliprdemia are common. In contras
rype I GSD, elevation of liver transaminase levels and fas
ketosis are Drominent, but blood lactate and uric acid conc
trations are usuallv normal. Serum creatine kinase levels can
useful to identify patients with rnuscle nvolvemenr; normal le
do nor rule out muscle enzyme deficiency.The adminrstration
glucagon 2 hr after acarbohydrare meal provokes a nor
increase n blood glucose; after an overnrgh! fast, glucagon m
provoke no change in blood glucose level.
Diagnosis.The hisrologic appearance of the liver is charac
has been seen n some patienrs with GSD lII.
Parienrswith mvopathy and liver symptoms have a general
enzyme defect (type IIla). The deficient enzyme activity can
demonsrrated not only in liver and muscle, buc also in o
tissues such as heart, erythrocl/tes, and cultured 6brobla
n btype asslgnmenr in the maioricy of patienrs.
Dietary management is less demanding than in
I nts do not need to restnct dietary inrake of fruc
rhan recommendinga high-protein diet and an exerciseplogr
Liver transplantation has been performed in pariencs with
stage cirrhosis and/or hepatic carcinoma.
TYPEV GLYCOGEl{TOBAGEISEASEBRANCHINGNZYMECIENCY,MYLOPECTIN0SIS,8 ANDERSENlSEASEl eficof branching enzyme activity results n accumulatior of afl ab
mal glycogen with poor solubiliry. The disease s referred t
type IV GSD or amylopectinosis because he abnormal glyco
has fewer branch points, more q. 1-4 linked glucose u
and longer ourer chains, resulting in a structure resemb
amvloDectln-TyF IV GSD is an autosomal recessivedisorder The glvco
branching enzyme gene is located on chromosome 3p21. M
tions responsible for rype IV GSD have been identified, and
characterization in indrvidual patients can be useful in predic
the clinical outcome. Some mutations are associacedwith a g
mosr common and classic form is characterized by progre
cirrhosis of the Lver and is manifested in the 1st 18 mo of lif
hepatosplenomegaly and failure to rhrive. The cirrhosis
gresses o portal hypertension, ascites' esophageal varices,
liver failure that usually leads to death b-v -51'r of age.
patients survive without progression of liver disease
A neuromuscular form of the disease has been repo
Patients may present at brrth wirh sevete hypotonia, mu
atrophn and neuronal involvement with death in the neo
period; others may present in late childhood wirh myopath

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 117/177
606 PARTX Melaholiciseases
cardiomyopalhy;or presentas adults with diffuse central andperipheralnervoussystem ysfunctionaccompanied y accumu-lation of polyglucosanbody drseasen the nervoussystem so-calledadult polyglucosan ody disease). or adult polyglucosandisease,eukocyte r nervebiopsy s neededo establish hediag-nosisbecausehe branchingenzyme eficiencys lrrmted o thosettssues.
Diagnosi$. issuedeposrionof amylopectinJikematerialscanbe demonsrratedn liver, heart, muscle,skin, inrestine,brain,spinalcord, and perrpheral erve.The hepatichistologic indingsare characterized y micronodular cirrhosis and fa inrly srainedbasophilic nclusionsn thehepatocl.res.he nclusions onsistofcoarsely lumped, toredmarerial hat is periodicacid-Schiffpos-itive and parcially resistant to diastase digestion. Electronmrcroscopy hows,n addition o theconventional and p glyco-gen parcicles, ccumulationo{ the fibrillar aggregationshat aretypical of amylopectin.The drstirct staining propertiesof thecytoplasmic nclusions, s well as electronmicroscopic indings,could be diagnostrc. owever,polysaccharidosesirh histologicfeatures emrniscent f type IV disease, ut without enzymaciccorrelation,havebeenobseryed. he definitivediagnosisestsonthe demonstration f the deficientbranchingenzymeactivity inliver, mu..1., cultured skin fibroblasts,or leukocytes.Prenataldiagnosis spossible y measunng he enzyme ctivity n culturedamniocytes r chorionicvilli.
Treatnent, here s no specificreacmentor type V GSD.Livertransplantation as beenperformed or patientswith progressrve
hepatic ailure, but becauser is a multisystem isorder nvolvingmany organ systems,he long-term success f liver transplanta-tion is unknown.
TYPEVI GTYCOGENTORAGEISEASEI.IVER HOSPHORYTASEDEFIGIENCY,ERS ISEASE).here are few patientswith docu-mented llver phosphorylasedefcrency.Such patients have abenrgn ourseand presentwith hepatomegaly nd growth retar-dation in early childhood. Hypoglycemia,hyperliprdemia, ndhyperketosis re usuallymrld if present. actrcacid and uric acidlevels are normal. The heart and skeletal muscles are notinvolved. The hepatomegalyand growh retardation rmprovewith age and usually disappeararound puberty.Treatment s
svmptomatic.A high-carbohydrate iet and frequent eedingareefiectire n preventing ypoglycemia; osrpalients equirenospecific reatment.GSD VI is an autosomalrecessive isease.Diagnosis estson elzyme analysis f the liver biopsy.The liverphosphorvlase ene (PYGL) is on chromosome74q21-22 andhas 20 exons.Many mutationsare known in this gene,a splicesite mutation in intron 13 has been dentified n the Mennonitepopulatlon.
TYPEX GI.YCOGENTOBAGEISEASEPHOSPHORYTASEII{ASECYl.This disorder epresents heterogeneousroup ofoses, Phosphorylase, he rate-limiting enzyme of
glycogenolysis,s activatedby a cascade f enzymaric eactions
kinase. he latterenzyme as ou r subunicsn, p, 16), eachencodedb;' differentgenes n differentchromosomes nd differ-entially expressedn various issues. his cascade f reactions sstimulared rimanly by glucagon.This glycogenosisould be heresult of any enzymedefciency along thrs pathlvay; the mostcommon s the deficiency f phosphorylase inase.
The numenc classiflcarion f phosphorylase inasedefrciencyis confusing, anging rom rypeVIa to VIII to IX. It is advisableto refrain from sucha designation nd to classify he variousdis-ordersaccording o organ nvolvement nd mode of inheritance.
X-tlNKEDUVEBPHOSPHOBYLASEINASE EFIGIENGYlinkedliver phosphorylase rnasedeficiency s the most common form
of liverglycogenoses.n additron o live! enzyme ctivitycanbedelicient n erythrocytes nd eukocyces;t is normal n muT1'pically, 1-5 yr old presentswith growth retardarionanrncrdentalindingof hepatomegaiy. holesterol, nglycerideliver enzymes remildly elevated. etosismay occurafrer asLactateand uric acid evelsare normal. Hypoglycemia s mipresent.The responsen blood glucose o glucagon s norHepatomegaly nd abnormalbloodchemistries raduallybenormal with age.Most adulcsachreve normal 6nal heighare usually asymptomaricdespite a persistentphospho
kinase deficiency. iver histologic appeatance howsglycodistendedhepatocltes.The accumulatedglycogen p partrosette orm) hasa fra;,'ed r burstappearancend s ess omthan the glycogenseen rn type I or type III GSD. Fibseptal formation and low-grade rnflammatory changesbe oresenc.
fhe strucruralgene or the common iver soform of rhepphorylase inase ubunit, iver crsubunrt s ort he X chromo(rrl- at XpZZ.2).Mutations of this geneare known.
AUTOSOMALIVERANOMUSGTEHOSPHORYTASEINASEGlEilCYSeveral atientshavebeen eportedwith phosphorkinasede6ciencyn liver andblood cellsand an autosomalmof inheritance.As with the X-linked form, heparomegalgrowth retardationapparent n eadychildhood are rhe pred
inant symptoms.Somepatientsalso exhibit musclehypotI(/hen measured n a few cases, educedactivity of the enha sbeen emonstratedn muscle.Murations ausine uto:ll y rransminedrverand rnut.|"nhosphorvlaseinaiedeficare for-rndn the autosomalp subunitgeneof rhe PK gene cmosome 6q12-q13).
AUT0SOMAI-IVEBPH0SPH0RYLASEINASEDEFICIENCform of phosphorylase inasedeliciency s due to mutarrothe testis/liversoformof rhe7 subunit of the gene TL, PHKIn contrast o the benign ourseof XJinked phosphorylaserdefrciency,atienrswich mutatronsn the PHKG2 genehavemsevere phenotypes wrth recurrent hypoglycemia and odevelopa progressiveiver cirrhosis.PHKG2 maps ro chrosome16p12.1 and many disease-causingutationsare kn
IOr tirls gene
ilUSCtE-SPECltlC PH0SPH0RYLASE INASE DEFICIENCYA casesof phosphorylase krnase deficiency restricted ro muscleknown. Patients, both male and female, present either wmuscle cramps and myoglobrnuria with exercise or withgressive muscl€ weakness and atrophy. Phosphorylase kinactivit't is decreased n muscle but normal in liver and blood cThere is no hepatomegaly or cardiomegaly. The structural gfor muscle specifrc form q subunlt (crM) is located at XqMr-rtationsof this genehave been ound in male patients with disorder. The gene for muscle l subunit (1M, PHKG1) is on cmosome 7p12 (29). No mutations in this genehave been reposo far
PH0SPHORYI-ASEINASE EFICIENCYlMlTEDT0 HEABT.patients resentwith cardiomyopathyn infancyand rapprogresso heart ailureand death.Phosphorylaseinaseciency is demonstrated in the heart with normal enz_vme ctirn skeletal muscle and liver.
Diagnosis. Definitive diagnosis of phosphorylase kinase dciency requires demonstration of the enzymatic defecr n affetissues.Phosphorylase kinase can be measured in leukocyteserythrocytes, but because the enzyme has many isozymes,diagnosis can be missed withour studies of l iver, muscle, or htn certain rnstances,
Tteatment.The treatment for liver phosphorylase kinase dciency includes a hrgh-carbohydrate diet and frequent feeding

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 118/177
lase kinase deficiency other than healt transplafltation.
ctYcOcEN SYIIIThErASE EFlCltttloYGSD0}. Deficiency of hepacic
glycogen synthetase eads o a marked decreaseof glycogen srored
in the li"er The patients Present in infancy with early-morning
(before eating breakfast) drowsiness, pallor, emesis, and fatrgueand sometimis convulsions associated with hypogll'cemia and
cated on chromosome 12p72.2-fteatmett
consists of frequenr
eals, rich in prorein, and nighttime supplementation wich
uncooked cornstarch.
HEPATIC GIYCOGEI{OSISWITII RENAT FAIIICONI SYNDROIIIE
and small meals with an adequate caloric intake may Implove
grol\,'th.
MUSCTETYCOGEI{OSES
Chapter? Detects[ Mel.bolistnf Calbohydrates6
theseatter enzyme eficiencresan alsobeassocrated ith a copensaced emolysis,suggestinga more generalizeddefectglucosemetabolism.
WPE l GtYCOGEl{TORAGEISEASEtYS0S0MAtACID r1,4-G
C0SIDASEEFICIEI{CY,OMPE ISEASE}.ompedisease, referred o as GSD type II or acid maltasedeficiency,s caus
This enzymedefect esults n lysosomalglycogenaccumulat
in multiple tissuesand cell types, with cardiac, skeletal, a
smoothmuscle ellsbeing he most serrously ffected. he dise
is characterized y accumulationof glvcogen n lysosomesopposed to its accumulation rn cyroplasm in the orhglycogenoses.
Pompediseases an aurosom recessive isorderwith an rn
denceof =1/40,000 ive births. he gene or acrdq-glucosid
rson chromosome-q25.2. Multiptepathogenic utations a
been dentifred hat could be helpful in delineatingchephetypes. n sitemutation IVS1-13T-"G), omonly see enrsof caucasian escent.
Clinicat e disorder ncompa\ses range
appearance," eeding difficultres, macroglossia, epatomegand a hypertrophiccardiomvopachyollowed by dea from cdiorespiratory ailure or respiratory nfectronusuall by 1yr age.Juvenileand adult-onsetdisease late-onsetorms) is chacterized y a lack or absence f severe ardiac nvolvement
The clinicalpicture s dominatedby slowly progressive roxim
muscleweaknesswith truncal involvementand gteater nvolment of the lower limbs than the upper imbs. The pelvicgird
paraspinalmuscles, nd diaphragrnare the musclegroupsm
seriously ffected.With disease rogressiol,patlentsbecome ofined cowheelchairs nd requireartrficialventilation.The init
sympromsn
somepatientsmay be espiratorynsufficiencyma
ifestedby somnolence,mornrflgheadache, rthopnea,and extional dyspnea, which eventually lead to sleep-drsordbreathingand respiratory ailure.Respiratory ailurers the caof significantmorbrdrtyand mortality in this form of the diseThe ageof deathvaries rom early childhood o late adulthodependingon the rate of disease rogression nd the ex tenresDiratorvmuscle nvolvement.
laborrtoryFindings, hesencludeelevatedevelsof setumcatine kinase,aspartate mrnotransferase,nd lacratedehydronase. In the infanrile form a chest x-ray showing mascardiomegalys requently he 1st symptomdetected. lectrodiographic indings nclude a high-voltageQRS complex anshortenedPR interval. Echocardiographyeveals hickeningboth ventricles nd/or he ntraventricular eptumand/or eft vricular outflow tract obstruction.Musclebropsy hows heprence of vacuoles thac stain positively for glycogen; aphosphatase s increased,presumably from a compensaincrease f lysosomal nzymes. lectfonmi(ro\copy re\eglycogenaccumulationwithin the membranous ac and in cytoplasm.Electrornyographyevealsmyoparhic eatureswexcessive lectrical rrirability of muscle rbers and pseudootonrcdischarges. erumcreatinekrnase s not alwayselevain adultpatients.Depending n the muscle ampled r testedmusclehrsrologicappeara[ceon electromyographymay not
abnormal. c is prudent o examine he affectedmuscle.nosrs of Pomid cr-elucosiskin fibrobla

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 119/177
6mr PARTX Metabolicisaasas
dried blood spots, eukocyces, r blood mononuclear ellsusngmahose,glycogen, r 4-methylumbelliferyl-a-D-glucopyranoside(4MUG) as a substrare,Deficrencys usually more seyeren rheinfantile form than rn the juvenile and adult forms. The skrnfibroblastassay s usuallypreferred o musclebiopsybecausetis less nvasiveprocedurewith rhe advantage f maintainingace line for future use and providing information on residualenzyme activit)'. Blood-basedassayshave the dvantageoI arapid turn-around ime. A musclebiopsycan yi d faster esultsand provide addrtronalnformation aboutglycogen ontentand
site ofglycogen
storagewichin and outside the lysosomes fmuscle ells.A mayor imitarion of a musclebropsy n late-onsetpatients s the variablepathologyand glycogenaccumulation ndifferentmuscles nd withrn muscle6bers;musclehistologyandElycogen ontentcanvary depending n the siteof muscle ropsy.There is also a risk from anesthesia. renatal diagnosisusingamniocytesor chorionic villi is available n the fatal infantileform.
Treatmentoptions were once imited to supportiveor care. Clinical trials of enzyme eplacementherapy(E beenpromisingand ERT with myozyme s availablefor treatmentof Pompedisease. ecombinant cid cr-glucosidaseis capableof improving cardiacand skeletalmuscle unctions(Frg.87-3). For patientswith the late-onset orm of rhe disease,a high protein diet may be beneficial.Nocturnal ventilatory
support, when rndicated, hould be used. t has beenshown toimprove he quality of life and is parricularlybeneficial uring aperiodof respiratorydecompensation.
GIYCOGEI{IOBAGE ISEASES IMICKING YPERINOPHTCAR-DI0MY0PATHY.eficrencies f lysosomal-associatedembraneprotern 2 (LAMP2, also called Danon disease)and AMP-activatedproteinkinasey2 (PRKAG2) esult n accumulation fglycogenn the hean and skeletalmuscle.Thesepatientspresenrprimarily as a hypenrophiccardiomyopathy, ur can be distin-guished rom the usual c sesof hypertrophiccardiomyopathydue to defecrsn sarcome prorein genes y their electrophvsio-logic abnormalities,particularly ventricular pre-excitationandconduction defects.The onset of cardiac symproms, ncludingchestpairi, palpitation, syncope,and cardiac arrest,can occlrr
between he agesof 8 and 15 yr fo r LAMP2 defrciency',othan the averageage for patients u'ith PRKAG2 defiwhich is 33 yr, The prognosis or LAMP2 deficiency swith progressiveend-stageheart failure early in aduhCardiomyopathydue to PRKAG mutations s comparibllong-term survival, although some patients may necethe implantarion of a pacemakerand aggressive ontarrhythmias.
TYPEV GIYCOGEflTORAGEISEASEMUSGTEHOSPHO
DEFICIENCY,CARDTEISEASE).his rscaused y rhe defiof musclephosphorylase crivity. Lack of this enzymemuscle ATP generationby glycogenolysis,esults in glyaccumulation, nd rs he prototypeof muscle nergydisorddefrciency f myophosphorylasempairs he cleavage f glmolecules rom the straighrchainof glycogen.
erancewith muscle ramps/pain.wo rypesof acLiviryecause ymptoms:brief exercise f grear ntensirysuch assing or carryingheavy oads;and less ntensebut sustainediry suchas climbingstarrsor walking uphill. Moderateexsuch as walking on level ground, can be performed bypatients or long periods.Many patientsexpetience chaistic "secondwind" phenomenon. f they slow down o
brieflyat the lst appearancef muscle ain. rheycan eexercisewrth more ease, Due to the underlying myothese patientsmay be at risk for statin-inducedmyositrhabdomyolysis.
About half repon burgundy-colored rine afrerexerciseis the consequencef exercise-induced yoglobinuriasecoto rhabdomyolysis.ntensemyoglobinuriaafter vigorousexmay causeacute enal failure. In rare cases, lecromyogfindingsmay suggest n inflammatorymyopathy and thenosis anbe confused irh polymyosiris.
The levelof serum creatinekinase s usuallyele.\'atedand increasesmore after exercise.Exercisealso increaslevelsof blood ammonia, nosine,hypoxanrhine,and uricThe latterabnormalities reattlbuted to acceleratedecycmuscle urinenucleorideswing o insufficient TPprodu
Pre-treatment Post-treatment
Fisure 87-3. Chestx-rav and musclehistotogy indan infanrile-onsetPompe diseaseparient before fnafter fEl enzyme eplacement herapy.Nore rhe de
in heart sizeand musle slycosenwirh rhe rherapy.i6ed Irom Amalfitano A, Beneur AR, Mone R?,Recombinant human acid alpha-glucosidase etherapy' for Lnfannle gtycogea storage disease yResults of a phase VII cljnical trial, Genet2001i3:132-138.)

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 120/177
Type V GSD is an aulosomal ecessive isorder.The gene or
muscle hosphorylasePYGM)hasbeenmapped o chromosome
described,rcise est offers a rapid diagnostic
sc mecabolicmYoPathY. ack of an
in s and exaggerated lood ammoniaelevations ndicatemuscleglycogenosis nd suggest defect n
the conversronof muscleglycogenor glucose o lactate. The
abnormal ischemrcexercise esponses not limrted to type V
GSD. Other muscle defects in glycogenolysisor glycolysis
producesimilar results deficiencies f musclephosphofrr-rctoki-
nase, phosphoglycerate inase, phosPhoglyceratemutase, or
lactatedehydrogenase).Phosphorusi"gn.tr. t".onuttc" imaging(31PMRI) allows for
rhe nonrnvasive valuationof musclemetabolism Patientswith
typeV GSDhaveno decreasen incracellular H and haveexces-
sive reduction n phosph<xrearinen responseo exerciseThe
diagnosis houldbi confirmedby enzymatic valuation f muscle.
A cbmmonnonsensemutation R49X in exon 1 is found rn 907"
of white patients,and a deletionof a singlecodon n exon 17 is
found in 51% ofJapanese atrenrs.Other commonmutatrons nwhrres G204Sn exon5 and K542T in exon 14 ) makeDNA-
baseddragnosis nd carrier tesring or McArdle disease ossrble
fbr the 2 populations.Treatmeni. voidance f strenuous xelcise levents he svmp-
toms;however,egularand moderate xercises recommendedo
improve exercisecapacity.Sucrosegiven before exetcisecan
-"ik"d1y i-ptou. tolerancen these atients.A high-prorein ier
may ncreasemuscle ndurance ndcreatine upplement asbeen
shown o improvemuscle unction n someparients. ongeviry s
not generallyaffected.
TYPE II GTYCOGENTORAGEISEASEMUSCTEHOSPHOFRUC-
TOKINASEEFIGIENGYABUT ISEASEI.ype VII GSD rs caused
sible n is population.Clinic Manile$tations, ix features f rypeVII are distrncrive:(1) Exercise ntolerance,usually evidenr n childhood, is more
severehan in typeV disease ndmay be associated ith nausea,
vomiting, and severemuscle ain; vigorousexercise auses evele
m.,scle tamps and myoglobinurra (2) A compensated emoly-
sis occursas evidenced y an rncreasedevel of serumbilirubin
Chaptei7r D.lectsn Metaholismf Calbohydiat
because lucose nhibits lipolysis and rhus deprivesmuscfatty acrdand ketonesubstrates.n contrast,parientswirhV drseaseanmerabolize lood-borne lucose erived rom eliver glycogenolysis ! exogenous lucose; ndeed,glucose
sion mprovesexerciseolerance n type V pattents. 6) Thno sDontaneousecond-wind henomenon ecause f the in
ity to metabolizeblood glucose.Two rare rype VII variants occur. One variant prese
infancy with hypotonia and limb weakness nd proceed
rapidlv progressivemyopathy rhat leadsco death by 4 yr o
The other variant presents n adults and is characterizeslowly progressive,ixed muscleweakness ather than crand myoglobinuria.
Diagnosis. o establisha diagnosis,a biochemicalor hchemrcal emonstrarion f the enzymaric efecr n the musrequired.The absence f rhe M isoenzyme f phosphofrunase an alsobe demonstratedn blood cellsand fibroblas
Trcatment.here s no specific featment,Avoidance l scous exercise s advrsable o prevent acute attacks of m
crampsand myoglobinuria.
OTHER USCI.E TYCOGEI{OSESITHMUSCTE NERGYMMENI Six additional defects in enzymes-phosphoglykinase,phosphoglyceratemutase, actate dehl'drogenasetose-1,6-biphosphateldolaseA, musclepyruvatekinase,a
enolase in the pathway of the terminal glycolysis-symptoms nd signs f muscle nergympairmentsimilar o of typesV and MI GSD.The failure of blood actate o incln responseo €xercises a usefuldiagnostic esrand can bero differentiatemuscle glycogenosesrom disorders of mecabolism, uch as carnrtinepalmitoyl transferaseI defi
and very long chain acyl-CoAdehydrogena deficiency,walso causemusclecrampsand myoglobinur Musclegly
levels an be normal in the disordersaffecting erminal gly
sis and assaying he muscleenzymeacrivity ts needed o mdefinirediagnosis. here is no specifrc reatment, voidanstrenuous rercisepreventsacuteattacksof musclecrampmyoglobinuria.Avoidanceof drugs suchas statins,and mnant hypenhermiaprecaulions or patientsundergoingansia should be followed.
87.2. DEFEGISNGATACTOSEETABOTISMPriyaS.Kishnani ndYuan-Tsonghen
Milk and dairy products ontain actose, hemajor dietarysof galactose. he metabolismof galactose roduces uel foh-rlarmetabolism hrough its conversion o glucose-L-pho(seeTable 87-1). Galactose lso playsan important roleformation of galactosides, hich includeglycoproteins,iprds, and glycosaminoglycans. alactosemia enotesrhvated evel of galactose n the blood and is found in 3 dinborn errors of salactosemetabolismdefecriven 1 of rh
lowing enzyrnes:alacrose-1-phosphateridyl transferasetokinase, and uridine diphosphategalacrose-4-epimeraterrngalactosemia, lthoughadequate or the deficienciesof thesedisorders, enerally esignareshe transferaseefr
GAIACTOSE-1-PHOSPHATEBIDYTTBANSFERASEEIIC
GAIACT0SEMIA,wo forms of the deficiency xisr: nfantcomplete r nearcomplete eficiency f theenzyme classic
tosemia)and those with partial transferase eficiencyCgalactosemias a seriousdiseasewith onserof symptomcallv bv the 2nd half of rhe 1st wk of !fe, The incide1i50,0d0.The newborn nfant receives igh amountsof la(up to 40% in breastmilk and certain ormulas),which co

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 121/177
610 PABT r MetabolicDiseases
of eqLralparrs of glucose and galactose. firhout the transferaseenzyme, the infant is unable ro metabolize galacrose- -phosphate,
the accumulation of which results in injury ro krdne_v, iver,and brain. This injurv may begin prenatally in the affecred fetusby transplacental galactose derived from the diet of the her-efozygous mother or bv endogenous producrion of galactose rnffre lerus.
Clinical Manilsslations. The diagnosrs of uridyl transferasede6-ciency should be considered in newborn or young infants wirhany of the following fearures: aundrce, hepatomegaly, vomrting,
hypoglycemia, convulsions, lethargn irritabilirl, feeding dif6cul-tres, poor weight gain or failure to regain birth weight,aminoacidurla, nuclear cataracts, vitreous hemorrbage, hepaticfaiLure, liver cirrhosis, ascites, splenomegaly',or mental retarda-rion. Symptoms are milder and improve when milk is temporar-ily withdrar,r.n and replaced by intravenous or lactose-freenutrition, Patients wirh galacrosemia are at increased risk forEscberichia coli neonatal epsis ; the onset of sepsisoften precedes
the diagnos is of galactosemia.Death from liver and kidney failureand sepsis may follow within days. \X/hen che diagnosis is normade at hitth, damage ro the liver (cirrhosis) and brain (mental
retardatron) becomcs ncreasingly severeand irreversible.Partial translerase deficiency is generally asympromatic. ft is
more frequen! than classic gaLacrosemia and rs diagnosed innervborn screening because of moderatell' elevated blood galac-tose and./or ow rransferaseactivit-v'.Clalactosemiashould be
con-sidered for the newborn or young infant who is not rhriving orwho has any of the preceding 6ndings, Light and electronmicroscopy of hepatic tissue reveals farty rnfiltrarion, che orma-tion of pseudoacini, and eventual macronodular cirrhosis. Thesechanges are consistent with a metabolic disease but do noc indi,cate the Dreciseenzvmatrc defect.
Diagnosis. he prehminary diagnosisof galactosemias madebv demonstrating a reducing subsrance n severalurirte specimenscollected while the patien! is receiving human mrlk, cow's milk,or any other formula containing lactose, The reducing substancefound rn urine by Clinitest (glucose, galactose, others) can beidentilied by chromarography or bv an enzymatic test specific forgalactose. Galacrosuria is present, provided che lasr milk feeddoes nor dare back more chan a fer,,'hours and rhe cbild is norvomiting excessively. Chnistix urine test results are negarivebecause he res t matenals rely on the action of glucose oxidase,t'hich is specific for glucose afld is nonreactive with galactose.
O$.ing to a proximal renal tubular syndrome, however, theacurely rll babv may also excrere glucose together with amino
acids. Because galacrose is injurious to persons with galacto-
semra, diagnostic challenge tests dependent on administeringgalacrose orally or intravenously should noc be used. Directenzvme assay using erythroc,vtes establishes the diagnosis. Oneneeds to confirm that the Danent did not receive a blood trans-Iusron before the collection of the blood sample, as a diagnosiscould be mrssed. Deficient activit,' of galactose-l-phosphare
uridyl cransferase s demonstrable in hemolysatesof eryrhrocytes,which also exhibit increased concentratrons of salactose-1phlsphate.
Genetics. Transferase deiciency galacrosemla rs an autosomalrecessivedisorder. There are several enzymatrc variants of galac-tosemia. Tbe f)uarte variant, a single amino acid substitution(N314D), has drminished ed cell enzymeactrvirybu t usuallynoclinical significance. Some Afrrcan-American pacienrshave mildersymptoms despice he abselce of measurable rransferaseactivityin erythrocytes; these parienrs retain 107o enzyme activity in Jiver
and inrestinal mLrcosa,.,vhereas os t white parients have nodetectable activity in any of rhese issues. n African-Americans,
62% of allelesare represenred y cheS135L mutation, a mura-tion tha! is responsible for a milder diseasecourse. In the whitepopulation, 70% of alleles are represenred b,v the Ql88R andK285N missensemutations an d are associatedwich severedisease.Carrier tescingand prenatal diagnosis can be pertbrmed
by drrect enzyme analysis of amniocytes or chorionic vil li; rescirn a[5o be DNA basrd.
Trealrnent and Prognosis. Because of newborn screening galacrosemia.parienrr ar e berng identrf ied and rreared iaVa r iuus m i l k suh l i ru r ( \ a re a ra i lab le (ca .e in hyd ro lysso,vbean-based ormula). Elimination of galactose from the dreverses growrh failure and renal and hepatrc dysfunctioCataracts regress,and most parients have no impairment of esrght. Early diagnosis and treatment have improved the prognsis of galactosemia; howeve! on long-term follor-up, patie
still manifest ovarlan failure wich primary or secondarv arnenrhea, decreasedbone mineral densit,v,deveJopmenral delali alearning disabilities that increase n severit,v virh age. Most milest speech disorders, whereas a smaller number demonsrrpoor growth and impaired moror function and balance (r,r,'i
wrthout overt araxia). The relative control of galactosephosphate levels does not alwa,vs correlate with long teoutcome, eadingco he belief hat orher faccors, uchas clevagalactitol, decreased uridine diphosphate galactose (UDP-gal
tose, a donor for galactolipids and proteins), and endogenogalactose production may be responsible.
GALACT0KINASE EfICIENCYThe deficient enzvme is ealactonase. rhrch normallv caralyzes he phosphorvlaiionof
'g.rlacr
The principal metabolites accumulated are galactose and gala
tol. Tu'o geneshave been reported to encode galactokinase: Gchromosome 1r-q24 arrd. GK2 on chromosome 15. Cataraare usually the sole manifestation of galactokinase deficienpseudotumor cerebri is a rare complicarion. The affected infais othenvise asymptomacic. Heterozygore carriers may be at rfor presenile cataraccs.Affected patienrs have an increased cocentration of blood galaccose evels, provided they have been a lactose-containing formula. The diagnosis is made by demostraung an absence of galactokinase activiry in erylhrocytes fbroblasrs. Transferase acrivrty is normal. Treatment is dietarescriccionof galactose.
URIDINEDIPH0SPHATE AtACT0SE-4-EPIMERASEEtICIENCY.abnormalJy accumulated merabolites are simrlar ro those n tranferase
deficrency; ho.w'ever, here is also an increase in celluUDP-galactose. There are 2 drstinct forms of epimerase deciency. The 1st is benign form discovered incidentally throuneonatal screening programs. Affected persons are healthy ar.ithout problems; the enzvme deficiency is limlted to leukocyand eryrhrocytes- No rreatmenr is required. The 2nd formepimerase deficrency s severe, and climcal manifestations reseble transferasedeficiencl r.r'ith he additional symptoms of h;rpconia and nerve deafness. The enzyme defciency is generaliz
and clnical symptoms respond ro restdction of dietary galactoAlthough thrs form of galacrosemia s rare, it rnust be considein a symptomatic patient wirh measurable galatose-1-phospha
who has normal transferase activity. Diagnosis is conlirmedthe assayof epimerase n erythrocytes.
Patients wrth rhe severe form of eDimerasedeficiencv cannsynthesize alactose rom glucosean d ar e galactosedependBecause alactose s an essentral omponent of manv nervosystem structural proteins, patienrs are placed on a galactorestricted diet rather rhan a ealactose free diet.
Infants with the mild {orm of epimerase deficrency have nrequ r redfea tment .t j * adv isab le, ' f o l l ow u r ine pec im ensreducing substances and exc lude aminoaciduria within a feweeks of diagnosis while the infant is still on lactose-containiformuia.
The gene for UDP-galactose-4-epimerase s located on chrmosome I at 1p36. Carrier detecrion is possible by measuremeof eprmeraseactivity in the er)'throcyles. Prenatal diagnosis frh e severe orm ui eprmerase e6.iencl. using an enzymeassof cultured amniotic fluid cells. is oossrble.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 122/177
87.3 DEFECTSNFBUCTOSEETAEOLISMPriya .KishnanindYuan-Tsonghen
DIFICIENCYTTRUCTOKINASEESSENTIATRBENIGN BUCTO-SURI cyof fruccokinasesnot associatedith anyclin-rcal ons. ft is an accidentalinding usuallymade
becauseheasvmptomaticatient's rine ontains reducingub-
stance. No treatment is neiessaty and the prognosis is excellent
Inheritance is autosomal recessive with an incidence of
1/120,000. The gene encoding fructokinase is locared on chro-
mosome2p23.3.
Fructokinase catalyzes the 1st step of metabolism of dietary
fructose: conversion of frucrose to fructose 1-phosphate (seeFig
87-1). Without this enzyme, ingested fructose is not metabolized.
Its level is increased in the blood, and it is excreted in urine
because here is practically no renal threshold for fructose. CIin-
itesr resLrlts eveil the urinary-reducing substance,which can be
identilied as fructose by chromatography.
DEFICIENCY OF FRUCTOSE.I,6.8ISPHOSPHATETDOTASE
5 uctute'The true incidence of hereditarY
f unknown but maY be as high as
Chapler 7 . D.lects n Metaholism f Calbohydiates
An intravenous fructose tolerance tesc, admrnisceredwith gr
caution! is 1 step in facilitating diagnosis. The fructose challe
will cause a rapid fall, lst of serum phosphate and then of blo
glucose,and a subsequentncreasen uric acid and magnes-A n,rral rolerance e*i should not be perfurmed becau:epati
can become acutely ill. Definitive diagnosis is made by assa
fruccaldolase B activiry in the liver' Gene-baseddiagnosis is av
able for most patients with thrs disease;a common mutation (s
sticution of Pro for Ala ar position 149) accounts for 537. of H
alleles worldwide.
Treament Treatment consistsof the complete elimination o
sources of sucrose, rucrose, and sorbirol from the diet. Ic may
difficult because these sugars are widely used additives, fou
even in most medicinal preparations Wirh tleatment, l
and kidney dysfuncrion inproves, and catch-up in grorwh
common. Intellectual development is usually unimpaired. As
patient matures, symptoms becom milder evell after fluct
ingesrion; he long-termprognosis1 good. Because f volun
diilary avoidanceof suciose,affec d patientshave lew de
canes.
87.4. DEFEcrsN INTERi|EDIARYARB0HYDRMETABoUsMss0ctATED|TH Acrlc cto0st
PriyaS.KishnanindYuan-TsonghenLactic acrdosrs ccurswirh defects f carbohydratemetabochacnrerferewith the conversion f pyruvate o glucose ia
respirarory haindefeccs,ndpyruvate arboxylase e6ciencdrsordersn the pathway of pyruvaremetabolism ausing a
acidosis,Lactic acrdosis an also occur in defectsof fatty oxrdacion, rganicacrdurias se eChapters856, 85.10,
86.1),or biotin util izadondiseases.hesedisorders re e
distinguishable by the presenceof abnormal acylcarnprofiles and amino acids in the blood and unusual org
acids in the urine, Blood laccate,pyruvate, and acv lcarnprofiles and lhe presence f theseunusual urine organic a
ihould be determined n infants and children with unexpla
acidosis,especially f there is an increaseof aoion gap
Chapter 5) .Lactic acidosisunrelated ro an enzYmaticdefect occu
dosis s shown n Figure87-5
DISORDERSFGLUCONEOGENESIS
DEFICIENCYF GTUCOSE-G.PHOSPHATASEWP E I GTYCGSD is the only glycogenosis sacidosis.The chronic metabolic
lien!s to osteoPenia; fter proloted wirh hypoglycemias a life-th
ening ondition se eChapter 7.1).

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 123/177
612 r PABT r MetabolicDis€as€s
dehydrogeMse'
El active
Acetyl-coA\-> Cilicacid ycle
\______: "_ r ,H:U
I'igurc 87-1. Enzvmatic reachonsof carbohydrate metabolsn, deliciencies f u'hich can gjve rise ro lactic acidosrs,pvruvate elevarions,or hypoglycemiapvruvaredehydrogenase onplex comprises, n addition to Er, Fr, and E:, an exfia lipoate containingprorein (nor shown), calledprotein X, and p_vruvar
orogenasenospnarase.
fBt CTOSE-1,5-DIPHOSPHATASEEFICIENCYruccose- 6 diphos-
pharase efieiencl mpairs rhe formarion ol glucose ro m al l glu-
cooeogenic precursors, including dietary fructose. Hypoglycemia
occurs when glycogen reservesare limited or exhausted. The clin-ical manifestations are characterzed by life-rhreatening episodesof acidosis, hypoglycemia, hyperventilation, convulsions, andcoma. ln about 7. of che cases, he deficiency presents n the 1stwk of life. In infants and srnall children, episodes are triggeredb1' febflle inlections and gastroenterrtis if oral ibod inrakedecreases.The frequency of the attacks decreaseswith age. Lab-orarory lindings include low blood glucose, bigh lactate and uricacid lerrls. and metabolic acidosrs. n contrast to bereditary fruc-rose intolerance, rhere is r-rsuallyno averslon to s\{'eers; renalrubular and liver functions are normal.
The dragnosiss established y demonstratingan enzymedefi-
ciency in erther liver or intestrnal biopsl', The enzyme defect canalso be demonsrrated in leukocytes in some cases. The gene
eodrng or frucro.e-1. 6dipho'phata'e rs ocatedon chromosom.9q22; mutarions are characteriz-edmaking carrier detection andprenatal diagnosis possible. Treatment of acute attacks consistsof correction of hypoglycemia and acidosis bv inrravenousglucose infusion; the response is usually rapid. Avoidance offasting, aggressivemanagemenr of infections and reslriclion offructose and sucrose from the diet can Dreve[r further eDisodes.For l, 'ng-1er6preventionof hyp'glycemia. a slowll rele.: ied ar-bohydrate such as cornslarch is useful. Panents who survivechildhood develop normallv.
PHOSPHOENOTPY8UVATEARBOXYKINASEPEPCK} EFIGIENCYPEPCK s a key enzyme n gluconeogenesis.t catalyzes hecon-versionof oxaloacetate o phosphoenolpyruvateseeFrg.87-4).PEPCKdefrciencys both a mitochondrialenzl'me eficiency nda cytosolicenzyme eficiency, flcoded y 2 distinctgenes.
The disease as been eportedJnonly a few cases. he clinicalfeatutesare heterogeneous,ith hypoglyc€mia,accicacidemia,hepatomegaly, ypotonra, der.elopmental eJay,and farlure cothrive as the major manifestations. here may be multisysceminvoLvemenc,wlth neuromuscular deficrts, hepatocellulardamage, enal dysfunction,and cardiomyopathy. he dragnosisis based n the reducedacrivityof PEPCK n liver,6broblasrs, r
lymphocytes.Fibroblastsand lymphocytesare not suirabldiagnosinghe cl,tosolic orm of PEPCKdeficiency ecausetissuespossessorly mirochondrial PEPCK. To avoid hglycemia,patientsshould be treated virh slow-releasearbdratessuchas cornstarchand fascing houldbe avoided.
DISORDEBSFPYRUVATEETABOTISM
Pyruvate is formed from glucose and other monosaccharfrom lacrate, and from alanine. It rs metabolized through 4 menzyme sysrems: lactate dehydrogenase, alanine aminouaferase, pyruvate carboxylase, and pyruvare dchydrogecomplex. De6crency of the N{ subunit of lactate dehydrogecauses exercise intolerance and myoglobinuria (see Cha87.1). Genetic deliciency of alanine aminotransferase hasbeen reported in humans.
PYBUVATE EHYDR0GENASE0MPL€XDEFICIENCY fter entethe mitochondria.pyruvafe s converted nt o acetylcoenz\m(acetyl CoA) by the pyruvate dehydrogenase complex (PDH
*'hich catalyzes the oxrdation of pyruvate to acetl'l CoA, .rv
then enters the tricarboxylic acid cycle for ATP production.
complex comprlses 5 components: E1, an cr-keto acid deboxylase; E2, a dihydrolipoyl transacylase; E1, a dihydrolipdehydrogenase; protein X, an extra lipoate-conraining prot
and pyruvate dehydrogenasephosphatase. The most commoa defect in the Er (seeFiE- 87-4).Deficiencv of the pvruvate dehydrogenasecomplex is the m
common of the disorders leadine ro lacric acidemia and cennerrr'ous system dysfunction. Tlie cettttrl nervous syscem funccion s because he brain obtains irs energy primaril l, fr
oxrdation of glucose. Brarn acetyl CoA is synthesrzed neexclusively from pyruvate-
The E, defects are caused by mutations in the genecodingE1a subunit, which is XJinked. Although X-Lnked, i ts deficieis a problem in both males and females, even thor.rghonlyo allele n femalescarriesa mutatiorr.
ClinicalManilestations.he disease as a r,r. ideoectrumof \entations rom the most severeneonataloresenrariono a m

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 124/177
FanyAcld OxidationOetects
Chapter , I Dof.crs o lo|lholi lm ol Carbohydrates
Metabolic cidosis
Skin ash/Alopecia
lncreased
3 HydroxyButyraie:Acetoacetale
Propbnic acidemh l
MEthylmalonic cidomb iOtherorganic ac*furia i
BiotinidassHolocarborylase
Eynlhetasedslicbncy
Diabetesmellitus
Normal02saturation
Normalo low3 HydroxyButyratelAcetoacoialeyp€rglycemia
NormalGlycemiaNo Ketosis
late-onset orm. The neonatal onset is associatedwith lethal lactic
acidosis, white matter cystic lesions, agenesisof the corpus cal-
losum, and the most severeenzyme deficiency. nfantile onset can
be lethal or associatedwith psychomotor retardation and chronic
drogenaseomplex,but also n thecr-keto lutarateand brancchainketo acid dehydrogenaseomplexes. yruvate ehydrasephosphatase eficiency as also been eported.TheseoPDHC defectshave clinical manifestationswithin the varspectrumassociated ith PDHC deficiency ue o E' deficie
TrestnentThe general rognosis s poor except n rare cawhich mutation is associated ith altered affinity for thiapyrophosphate,which may respond o thiamine supplemtion. Because arbohydrates an agglavateactic acidosis, keenicdiet is recommended. he diet has been ound to lowe6lood lactate evel,but limited or no long-termbenefit s sepotential reatmentstrategy s to maintain anyresidualPDHits active orm by dichloroacetate,n inhibitor of Er kinase
UrineOrganic cidsplEsmaacylcamitineprofi19
Decr€aa€dor normalpyruvaieincreased aclale/pyruvalo alio
Multisyslem nvohEment"RaggedRed Fibei
in musde biopsy
FiBure 87-5. Algorithm of the drflerentiaj diagnosjsof lactic acidosis.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 125/177
614 PABT r MebbolicDiso.so6
eficial effects n controlling postprandial actic acidosisn somepatientshave beenshom,
DEFICIENCYFPYBUVAIEABBOXYTASE-vruvate arboxylasesa mirochondrial.biotin-conraining tuyme essential n theprocess f gluconeogenesis;t catalyzes he conversionof pyru-vate o oxaloacetate. he enzymes also essentialor Krebscyclefunction as a providerof oxaloacetate nd rs nvolved n lipoge-neslsand formation of nonessential mino acids.Clinical rnani-festationsof this deficielcy have varied from neonatal severe
lactic acidosisaccompanied y hyperammonemia, itrulhnemia,and hyperlysinemiatypeB) to late-onsetmild to moderate acticacidosis nddevelopmental elay typeA).In both types,patientswho survivedusually had severe sychomotor etardationwithseizures, pasticicy, nd microcephal,v.omepatientshavepatho-Iogic changesn the brainstemand basal ganglia hat resembleLeigh disease. he clnical severityappears o correlatewrth thelevelof the residualenzyme ctivity.A "benign" form of PC defr-ciency charactenzed y recurrentattacks of lacric acidosisandmild neurologicdeficits as alsobeendescribed. aboratory ind-ingsare characterized y elevated evelsof blood lactate,pyru-vate, alanine, and ketonuria. In the case of type B, bloodammonia, citrulline, and lysine evelsare also elevated,whichmight suggest primary defectof the ureacycle.The mechanismis likely causedby depletronof oxaloacetate,which leads to
reducedevelsof aspartate, substrate or argininosuccinateyn-rhetasen the ureacycle seeChapter85.11).Trearmentconsistsof avoidanceof fasring,and eatinga carbohydratemeal beforebedtime,During acuteepisodes f lactic acidosis, atrents houldreceivecontrnuous ntravenousglucose.Aspartate and citratesupplements estore he metabolic abnormalities;whether thisfieatmentcan prevent he neurologicdeficits s not known. Livertransplantation asbeenattempted;ts benefit emainsunknown,Diagnosis f pyruvatecarboxylase eficiencys madeby themea-surementof enzymeactivity n liver or cultured skin frbroblastsand musr be differentiated rom holocarboxylase ynthetase rbiotinidasede6ciency.
DCFICIEI'ICYFPYRUVATEARBOXYI.ASEECOIIOARYO DEFI-CIENCYOF HOTOCARBOXYIASEYNIfiETASE R BIOTIT{IDASE.
Deficiencyof either holocarboxylase ynthecaseHCS) or bio-tinidase,whrchare enzymes f biot in metabolism, esult n mul-ciple carboxylasedefrciency pyruvate carboxylaseand otherbrotin-requiringcarboxylases nd metabolic reactions)and inclinical manifestations ssociated ith the resDectiveeficiencies.as well as ra'h, iacricacrdosis.nd alopeciJse ealsoChaprer85.6). The courseof HCS or biotinidasedeficiency an be pro-tracted,with intermitten!exacerbation f chronic acticacidosis,failure to thrive, seizules,and hypotonia leading to spasticity!lethargy,coma, and death. Late-onsetmilder forms have alsobeen reported, Laboratory findings include metabolic acidosisand abnormalorganicacids n theurine. n HCS deficiency, iotinconcentrationsn plasmaand urinearenormal. Diagnosis an bemade n skin libroblastsor lymphocytes y assay or HCS activ-ity, and in the caseof biotnidase, n the serumby a screening
blood spot. Treatment consistsof biotin supplementation, -20 mg/day,and rsgenerally ffectivef treatment s startedbeforethe developmentof brain damage.Parients dentifred hroughnewbornscreening nd trearedwrth biotin have emained symp-tomatic.
Both enzymedefciencies re autosomal ecessiveraits. HCSand biorinidaseare locatedon chromosome2'1q22and 3p25,respectively. thnic-specific utations n the HCSgenehavebeenidentified.Two commonmutations del7lrns3 nd R538C) n thebiotinidase eneaccount or 52lo ol all mutant alleles n symp-tomaucparen15 irh biorinidaseeficiency.
MrTocHoNoRtAr ESPTRAToRYHATNEFECTSoX|DATTVEHoS-PHORYIAflONISEASE).he mitochondrial esoiratory haincat-
alyzes heoxidation of fuel molecules nd transfershe electto molecularoxygenwith concomitantenergy ransductionATP (oxidativephosphorylation). he respiracory hainprodAT? fiom nicotnamide-adenine inucleorideNADH) or FADand ncludes5 specific omplexesl: NADH-coenzymeQ redtase; I: succinate-<oenzyme reductase; II: coenzymeQcytochromeQ reductase;V cltochromeC oxidase;V: ATP srhase).Each compJex s composedof 4-35 individual prota[d, wrth the exceptionof complex I (which is encoded oby nucleargenes),s encodedby nuclearor mitochondrial D
(inheritedonly from the mother by mitochondrial nhertanDefects n any of these omplexes r assembly ystems rodchronic actic acidosis resumably ue o a change f redoxswrth increased oncentrations f NADH. In contrast ro PDor pyruvatecarboxylase e6ciency',keletalmuscleand hearusually nvolved n rhe espiratory hain disorders; nd n mubiopsy,"raggedred fibers" (rndicatingmitochondrialproliftion) are often see[ (seeFig.87-5). Because f rhe ubiquinatureof oxidativephosphorylation,a defectof the mitochdrial respiratorychain accounts or a vast arrayof clinical mifestations nd should be consideredn patients n all agegropresenting with multisystem involvement. Some dencieresemble eighdisease, hereas therscausenfantilemyopatsuchasMELAS (mitochondrialmyopathy, ncephalopathy,aacidosis, nd strokelikeepisodes),MERRF (myoclonusepile
with ragged ed frbers),and Kearns-Sa1re;rrdrome (exteophthalmoplegia,acidosis, retinal degeneration,heart blomyopathy,and high cerebrospinallr.rid rorein) [Table87-2alsoChapters 98.2an d610.4].Diagnosisequires easureof enzyme ctivitiesn tissues r analysis f mitochondrialD(mtDNA) mutation, or both (Fig. 87-5). Analysis of oxidaphosphorylationcomplexes -IV from inraccmitochondrialated from fresh skeletalmuscle s the most sensitive ssamitochondrialdisorders.Specific riteria may assist n makindiagnosis Table87-3). Treatment emains argely symptomand does not significantlyaller the outcomeof disease.Spatients,however,appear o respond o cofactor supplemtypicallycoenzymeQ10 plusL-carnitineat pharmacologic o
TEIGHOISEASESUBAGUTEEGROTIZTNGIICEPHALOMY
THY).Leigh diseases a heterogenous er:rologicdiseaseremainsa neuropathologic escription haracterized y demnation, gliosis,necrosis, elativeneuronalsparing,and capilproliferation in specific brain regrons. n decreasing rdeseverity, he affectedareasare he basalganglia,brainsrembellum, and celebralcortex (seeChapter 598). The classicpse ation is of an infant who presentswith centralhyporodevelopmental egression r arrest, and signsof brainstembasal ganglia involvement.The clinical presentation s higvariable.Diagnosiss usuallyconfrrmedby radiologicor palogic evidence f symmetric esionsaffecting he basalganbrainstem,and subthalamicnuclei. Patientswith Leigh dishave defects in several enzyme complexes.Dysfunctioncl.tochrome C oxidase (complex IV) is the mogt commoreported defect, followed by NADH--coenzvmeQ reduc
(complex ), PDHC, and pyruvatecarboxylase.Mutations nnuclearSURF1gene,which encodes factor involved n the genesrs f clrochromeC oxidaseand mitochondrialDNA mutions in the ATPase6 coding region, are common molecfindings n patientswith Leigh disease.
87.5. DEFEGTSNPENTOSEETABOTTSMPriya .KishnanindYuan-Tsonghen
Abour 90% of glucosemetabolism n the body is via thecolytic pathway, with the remaining 10% via the hex

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 126/177
Chapter7 . Deleclsn Metabolisml Carbohydrates
(IAIITDITETIONSN
mtDlia
MUTATIONNTNASFERNA MUlAlloNN lBoS0lilALNA MUIAIION}IMES5TIiGEfllNA
]I4ELA5
+
L:r:
MTRRI
+
(5S Pt0 P5
+
AID LHIARPsYltlPTol$5,16N5,ND l G0ll{Gs
GNTRALTTRVOUsY5T[M
5e Lrre!
P5ydo,irotoreladaiDn
fuy(,romotorcqre55of
HPnrpa5 dndemanop
li1!c ne-ke e3da.hes
Dvsloni,
PtRIPHtRAt{ERVoUSYSTEI!,!DeripheraIeu'oFthf
MUsttt{'eakne55rdexelc5ent0leran(a
lrph:ha op ! a
EYtP,q,renIry,:ln0pdlry
ilplr. tropfy
BLOOD
5dercba5l(, lnemlafliD0Gt tSYSTEM
Dabelelel ru5
5h0rl1tat!"
HypoparaiYro r5m
IIEARI
[cndu(roro' le '
G(lDmy0paIri
GASTROINTISTII{AI,YsTTM
E[c(xe0,]rcreat0isnrn(I|ln
rlestn;preudoD5tru(lon
TAR, OSLAIIDHROIT
!eIs(lIeul,rlearq oisi
KIDNTY
LABORATONYNDINGSLait (;aooi
Ragqeid frber5nmLr5aeoPiY
MODET NHIRITANCE
[']ate||al
Sporad.
E
+-
+
++BI
E
E E +
++
'ih,rxrnrn r oi.kl ,r or rf !tmpr0mind !ni rcbr|!d
frm I r,liu :.j(hcn iA [l i.oir
++
+
E]
l{
t . t
E]
I$AJORIIENIA
r:inii t lcil! romplelea rcephar)'opalhyr; iritodcnor;ytap,rth'lrehned:!'rLn(l
alll |f$e folio,,{c'
>l9i raqqeded bpr!Rifl r5keetaulde
ayt..a1llmc0rca5ee-,titeiroerj| fe5icuaal l ofan ( 0mp )i ]li6 1i.' r:
<ll% fJ(e ne,or<10%l ,r r clr t ssur:!
tbroba5lAl fInd'e5i5ate5>l)bel0w ea r
NuceirrnLDl,iALltatrcnlrfc spLteoatroqen!_
MINOR(RITTRIA
!,ymlr|nn5l)nrat,beW]fi nL ce'e('
mrhrrrmbe'50[ fFi f )!Al \ ' l ,or{d. 'Jr. radie(i ronma:oi icpyabr0rm
lf L 0d, i5ej e crfi 0r lar Ra ekt 0r?5cL,rl(t y:t 0j n Raomp x 0 l0-i6
tr!!ire,-lrl09;r Jis In!,rirja 4ll% l ,ir rore,551,€5norcbh5LATplrrhe!ri l f5 ri Ibebwme:r,0' l ibr0bd56undbeloqn$nqfluiearl nrt,lNArtrtrf,'iI0b;r EpJl rrlenrnl!
l ra i r crc ehbnI qdi idrcrJcf0] t€d rtdb0r(r r (cn
r !lc!oq)"
: f r/mDciy
\ foecuar
l,.lctabc
, \ l l "dcre. id! rc !ner 'phc5rhaLe. l r - ! ipnLr I rh i ,_,5JAr ' . t rb!d(0enmia(( i ! ,Lonn10i0fda
ioimet;hil. id{5 h,w bp:fPrdlded"r!
pn0n.rPen q
| n m j i a ! | . r | h \ r | t ] A 1 t q n \ ' ] e L l | | : 3 l l e | . r m _ o l b d 1 l . r . d ' 0 1 a . ! n l ] ] p e r i j | l i : p ? J ] d h m

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 127/177
616 PARTX Metabolic isEosos
Figure 87-6. Murations jn the human mitochondial genome hat are known to causedisease.Disorders har are {requentlyor prominenlty associated ith
tions in a parricular geneare shown in 6old. Diseases ue Eomutations $at imparr mitochondrial prorein synthesis re sholvn h rl&e. Diseases ue to
tions in prot€in-coding genesare shown in raL ECM, encephalomyopathyiFBSN, amilial brlateralstnatal necrosisiLHON, l,eber hereditary optic neuro
LS, LeiSh syndJonq MELAS, rnirochondrial encephalomyopathr lacrc acidosis, and srrokelike episodes;MERR4 myoclonic €pilepsy with ragged-red
tvlll-S, maternally nherited Leigh syndrome; NARB neuropathy,ataxia, and retinrtis pigmentosa;PEO, prog€ssive external ophthalmopl€giaiPPK,palmo
tar keratoderma; and SIDS, sudden infant dearh syndrome. (From DiMauro S, Schon EA: Mirochondrial respirarory-chain disesses.N Engl J2003;348:2656-2668. Copyright @ 2003 MassachusettsMedical Societt All flghts reserved.)
monophosphatepathway. The hexose monophosphateshunrleads o formationof pentoses, swell asprovidingNADH. Oneof the metabolites s ribose-5-phosphate, hich is used n thebioslnthesis of ribonucleotides and deoxTribonucleotides.Through the transketolaseand cransaldolase eactions, thepentose phosphatescan be converted back ro fructose-6-phosphateand Blucose-6-phosphate.
ESSEIIflAL EIIITOSUBIA.ssential entosurias a benigndisorderencountered rincipally n Ashkenazi ewsand is an autosomal
trair, The urine contains L-xylulose, which is excreteincreased mounts because f a block in the conversionoxylulose o xylitol due to rylitol dehydrogenaseeficienccondition is usually discovered ccidentally n a urine tesreduci[g substances;o treatment s required.
IWt SAIO0|ASEDERGIEXCY.o date, only 2 pati€ntsreported;1 presentedwith liver cirrhosisand hepatosplenaly in early nfancyand rhe other presented ith severe eohepatopathy and cardiomyopathy,Biochemical abnorma

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 128/177
revealedelevatedevelsof arabitol, ribitol, and eythrirol in the
urine. Enzyme assay n the lymphoblasts/fibroblastsemon-strared ow transaldolasectivity,which was confirmedby muta-trons n the transaldolase ene.
RIBOSE-5-PHOSPHATES0MEBASE €FlClEt{CY nly I casehas
been eported.The affectedmale had psychomotor etardationfrom early n li fe and developed pilepsyar 4 yr of age.There-after, a slow neurologicregression eveloped,with prominent
cerebellar taxia,somespasricity, ptic atropht and a mild sen-sorimotorneuropathy.MRI of the brain at ages11yt and 74 yr
showed extensiveabnormalitiesof the cerebralwhite rnatterProton magneticresonance pecffoscopy MRS) of the brainrevealed levatedevelsof ribitol andD-arabitol.Thesepentitols
were also increasedn urine and plasmasimilar ro the patient
found in transaldolase eficiency.Enzyme assays n culturedfibroblastsshoweddeficient ibose-5-phosphatesomerase ctiv-iry which was confirmedby a molecularstudy.
Amatnrano A, Bengur AR, Morse RP, €t al: Recombinanthuman acid alpha
glucosidase nzyne cherapy or infanrile glycogen storagedisease ype Il:
Resulrsof a phaseVII clinical vial. Genet Med 2001;3:132-138.
Arad M, Maron BJ, Gorham JM, er al: Glycogen storage dis€asepresentlng
as hypertrophic cardiomyop thy. N Ensl J Me.l 20O5352:362-372BachrachBE, gehstein DA, Otbo Melander M, et al: Glycogensynrhase efi-
ciency(glycogenstoragedis€ase ype O) presentingwrth hyperglycemiaand
glucosuria: Report of rhree new mutarions..l Pedatr Z0n2;1401781-783
Bosch AM, GroorenhuisMA, Bakker HD, er al: Living wrh classicalgalac-
rosemiai Heal${elrt€d qualiry of life consequences. Pel,dtli.s
2004;1I3:e423€428.
Chamoles NA, Niizawa G, BlancoM, et a| Glycogenstoragedisease ype II:
Enzymat,cscreenins n dried blood spors on fiher paper, CIn Arn Acta
20A347:97-s1tJ2.
Ch€n YT: Glycogenstorasediseases.n krjver CR, BeaudetAL, Sly WS' Valle
D leds). The Metabolic and Molecular Bases of lnherited Disease, 8rh ed.
New York, Mccraw-Hill, 2001, pp 1521 1551.
Cnmi M, Papadlnitrious A, Galbiati S, er al: A new mitochondrial DNA
muracion r ND3 genecaustngsevereLeis.hsyndrornewjth early lerhality
Pediatl Res 2004;5 S:842-846.
D€ Menleir L: D€Iecrsof pyruvate merabolisrnand the Rrebs cycle.J Child
Ne/rol 2002j17(Suppl3):l526-iS34.
Den Boer MEJ, Dronisi-Mci C, Chakrapani A, et al: Mitochondrial trifunc'
lional protein d€fici€ncy:A xvere fany acid oxidation disorder wrth cardiac
and neurologic nvolvement.I Pediatr 2003.742:68a489.
DiMauro S, Schon EA: Mitochondrial respirarory-chaindiseases.N Engi /Med 2003 348:26 6:2668
Elpeleg O: Inherited mitochondrial DNA depletion. Pedia, Res
2003;54:153-159.Franco LM, Krishnamurrhy V, Bali D, €t al, Heparocellujar carcinoma in
glycogen storage disease rype la: A case series. lftheit Metab Dis
200Ji28:153-162.
carcoa-Cazorla A, De Lonlay ! NassogneMC, er J: l]]n8-tetm follow-up of
neonaral rnirochondrial cytaparhies: A study of 57 parients.Pedhttics
2O05t116:1170-1777 .
Haller RG, VissingJ: No spotrraneous econdwind in musclephosphofruc-
tokinase deficiency.Neurclogy 2004\52:82-85.
Holton JB, WaherJH,Tyfield IA, a al: Galacrosemia.n ScriverCM, Beauder
AL, Sly wS, ValleD (eds):TheMetabolic and Molecular Basesof lnherited
Diiersd, 8rh ed. New York, Mccrrw-Hill, 2001, pp 1551-1J87
Huck lH, VerhoevenNM, StruysEA, er al: Ribose-s-phosphatesomerase e6-
ciency:New inborn error in rhe pentost phosphateparhwayassociar€d ith
a slowly progressive leukoencephalopathy: Am J Huft Genet
2004'74:745-751.
Hunrsman RJ, Sinclair DB, BhargavaR, Chan A: Atypical presentatioflsof
Leigh syndrome:A case eries nd re"rew,PedratrNeroi 2005;32:33+-340.
K,shnani PS, HowelL RR: Pornpedis€ase n irfants and children. I Pediarl
2004;144:Sl5-S43-
LivingstoneC,.\l Riyalri S,Wilkins P,FernsGA: McArdle's dneasediagnosed
followrns statin inducedmyositis. Affi Clin Biocben 20O4i41tJ38-340.
ScasliaR Toqbin JA, Craieehr0q, ec al: Clinical spectrum, morbidity, and
mortality in 113 pediatnc patients with mitochondrial dtsease.Pediattics
2004;114:925-931.
Chapte.07 r Dol.cls ir Mdabolisn ol Carbohydrates
Scheers, BachyV StephenneX, SokalEM: Risk of hepatocellular arc
rn liver rnicochondrial resprratory chain disorders. ,f Pediatr 200
4t4417.
ShenJJ,ChenYT: Molecular characrerization fglycogen storagedisea
IIL CUn Mol Med 2002t2:r67-175.
Shoffn€rJM: Oxidarive phosphorylationdiseases.n ScDverCR, Beau
Sly wS, Valle D (edt:
"r€Metabolic and Molecutu Basesof tnh
Diseds?, rh ed, New York, Mcc.aw-H'll, 2001, pp 2367 2423.
StrcpoolePw, Keff DS, BarnesC, et al: Controlled Clinical trial of dic
a€€tate or rr€atment oI congenital lacric acidosis n children. Pe
2006i117:1519-1531.
UusimaaJ, Finnila S, RemesAM, et al: Molecular epiderniologvof ch:mitochondrial encephatomyopathresn a Finnish population: Se
analysisof entire mtDNA of 17 children revealsheteroplasmicmurat
rRNA Arg, tRNAGIU, and IRNA l-eu(UUR) Eenes.Ped.iafti.s200
443-450.
Van den Hout JMP,KamphovenJHJ,Winkel LPF,et a| Long-term ntra
rr€atmencoI pompe diseasr with recombinant human cr-glucosida
mtlk. Pediarlrcs2O04;113:e448-<457.
VerhoevenNM, Wallor M, H''ckJH, etal:A newborn wrth severeiver f
cardromyoparhy and transalodase deficrency, / Inhelit Meta2005128:169-179 .
VissingJ,Haller RG: The effectoforal sucrose n exercise olerance,np
with McArdle's disease.N Ensl I Med 2OO3i349:2503-2J09.Webb AL, Singh RH, Kenn€dy MJ, Elsas LJ: Verbal dyspraxia and
rosemi^.Pediatr Res Z00J;53:396-402.
W€ber P, Scholl S, Baunganner ER: Ourcome n parientswith profoun
iinidas€deficiency:Relevance fnewborn screening.Deu Med.Child
2004\46r''81484.Winkel LP, Van den Hout JM, Kamphoven JH, et al: Enzyme repla
rh€rapy n late-onsetPomp€t dis€ase:A three-year ollow-rp. Ann
2004r55:495-502.
Zeviad M, Di Donaro S: Ifrcochondridl disorders. Brain 200
21s31172.
87.6. DISORDERSFGTYGOPROTEINEGRAOAAND TRUCTUREMargaretM. McGovern n
Robert . OesnickThe disordersof glycoproteindegradation nd structure nseveralysosomal torage iseaseshat result rom defectscoproteindegradation, nd the congenitaldisorders f glyctein (CDGs), which are pathophysiologically unreGlycoproteins remacromoleculeshat arecomposed f oligcharidechains inked to a peptidebackbone.They are ssized by 2 pathways: he glycosyltransferaseath\ray, ws''nthesizes ligosacchandesinked O-glycosidically o or lhreonine r€sidues;and the dolchol, lipid-linked patwhich synthesizes ligosaccharidesinked N-glycosidicaaspafaSrne.
The glycoprotein ysosomalstoragediseasesesult fromdeficiencyof the enzymes hat normally participare in
degradationof oligosaccharidesnd include sialidosis, asialidosis, aspartylglucosaminuria,and c-mannosidossome nstances!he underlyingabnormality hat leads o gprotein accumulationalso results n abnormal degradacofher c)asses f macromoleculeshat cortain similar oligcharide inkages,suchas certainglycolipidsand proteoglIn these nstances,he underlyingenz)'matic eficiency esthe accumulationof borh glycoproteinsand glycolipidsclassiEcation f these ypesof disordersas liprdosesor gproteinoses s dependenton the nature of the predomistoredsubstance.n general,he glycoproteindlsorders reacterizedby autosomal ecessivenheritanceand a progrdisease oursewith clinical features hat resemble hosesthe mucooolvsaccharidoses.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 129/177
618 r PARTX MelabolicDiseEse$
SlALlD0SlS ND GAIACTOS|AI|D0SlS.ialidosis s an aurosomalrecessivedisorder that resuks from the orimarv deficiencv of neu-ram ni dase ue ro murarions n thegene har encodes hi sprorein.which is locared on chromosome 10. In conrrast. salacrosialido-' i s sdue o thede f i c ienc ) l2 t ysos , 'm a lenzyme . .eu ram rn ida reand p-galactosidase.The loss of these enz_ymaoc criv ities resultsfrom mutations in a gene ocated on chromosome 20 tbat encodesprotective protein/cathepsin A (PPCA), which funcrions to stabi-lize rhese eozymatic activiries. Neuraminidase normally cleavesterminal sialyl linkages of several oligosaccharides and glycopro
teins. Its deficiency results in rhe accumularion of oligosaccha-r ide ( , . l nd rhe u r ina r t e \ c r . t i on o f s ia l i c ac id re rm ina loligosaccharides and sialylglycopeptrdes. Examrnation of tissuesfrom affected individuals reveals pachologic srorage of substratein many rissues ncluding liver, bone marrow, and brain.
The clinical phenotype associated with neuraminidase defi-ciency s vanable and includes type I sialidosis which usually pre-sents n the 2nd decade of life with mvoclonus and the oresence. , f a ehe r ry cd sp , , r . hese a r ien r r p i ra l l y eome o j t t en lon
secondary o gait disturbances,myoclonus,or visual complaints.In contrast, type II sialidosis occurs as congenital, infanr e, and
;uvenile forms, The congenital and infantile forms result from iso-lated neuraminidase de6ciencn t'hereas the juvenile form resultsfrom boch neuraminidase and B-galactosidase deliciency. Thecongenital type II disease is characterized bv hydrops fetalis,
neonatal ascites, hepacosplenomegaln stippling oi the epiphyses,periosteal cloaking, and srillbirth or death in infancy. The type IIinfantile form presents n the lst,vr of life with dysosrosis mulri-plex, moderate mental recardation, visceromegall, corneal clouding, cherr ;r red spot , and seizures. The juvenile type II form ofsialidosis, which is somerimes designatedgalactosialidosrs, has avariable age of onsec ranging from infancy to adulthood. Ininfanc;i tbe phenotvpe is similar co thar of GMr gangliosidosis,u.ich edema, ascites, skeleral dysplasia, and cherrv red spot.Parienrs virh laler-onsetdisease ave dvsostosismulriolex. vis-
ie rom ega l l .m en r , r l e ra rd . l i on . y m orph ism . o rnea l loud ing ,progressive neurologic dererioranon, and bilateral cherry redspots. No specific therapv exists ior any form of rhe disease,although s tudies in animal models have demonstrated improve-ment in the phenotypeafter bone marrow rransplantacion. he
diagnosisof sialidosisan d galactosralidosiss achieved by thedemonstration of che specific enzymatic deficiency. Prenacaldiag-nosis using cultured amnioric cells is also possible.
ASPARTYLGIUC0SAMI|'IUR|AAGU). This is a rare autosomalrecessive ysosomal storage disorder, except in Finland, where thecarrier frequency is estimaced at l/36. The drsorder results fromthe deficient activity of aspartylglucosaminidase and rhe subsequent accumulation of aspartylglucosamine, particuLarly in theliver, spleen, and rhyroid. The gene for the enzyme has been ocal-ized to tbe Longarm of chromosome 4 and the cDNA has beencloned and sequenced. n the Finnish population, a single muta-oo n in th e gene (C153S) accounts for most mutaor alleles,rvhereasoutside of Finland, a large number of privare mulationshave been described- Affected individuals with AGU typicallv
present in the 1sc 1r of life w-ith recurrenr infecrions, drarrhea,and hernras.Coarseoingof the faciesan d short stature usuallydevelop later, Other features include jornt laxity, macroglossia,hoarse voice, crystal-like Lensopacities, hypotonia, and spascic-iry. Psychomocor der.elopmenr is usually near normal untrl theage of 5 when a decline rs noted. Behavioral abnormalities aretypical and lQ values in affected adults are usually <40. Survivalto aduLthood s common, with most earlv deathsarcributable opneumoniJ or o ther pu lmonarv cau .es . DeEn i r r ve iagnns isrequires measuremencof the enzyme in peripheral blood leukocytes. Molecular diagnosrsby analysisof DNA for the C163Smutation is possible or Finnish patien!s.Severalparientshaveundergone allogeneic bone marrotr,' cransplants, but rhisapproach has not been proven effective and no specific treatment
rs available. PrenataLdiagnosrs by the determinatron of the leof asparcylglucosaminidase n cultured amniocyres or chorionvilli has been reported.
aS-MANNOSIDOSIS.hi s autosomal recessivedisorder resufrom the delicient acnvity of q-mannosidase and rhe accr.rmtion of mannose-rich compounds. The gene encoding the enzyhas been localized o chromosome 19p13.2-q12, although tcDNA has not been cloned. Affected patjents wich rhis drsord
drsplay clinical heterogeneicy.There rs a severe nfantile form,type I disease, nd a milder juvenilevarianr, type II disease.parients have psychomotor retardation, facial coarsening, adysosrosismultiplex. The infantile iorm of the disorder, hou'evis characterized by more rapid mental deteriorarion, with deaoccurring betrl,'eenhe agesof 3 and 10 yr. Parienrs.rvich he infatile form also have more severe skelecal involvement ahepatosplenomegaly. The juvenile drsorder is characterized onser of symptoms rn earll' childhood or adolescencewirh mildsomanc features and survival to adulthood. Hearins loss. destrur i ve , , ynov i t i s , an i \ ropen ra . nd .pa . r i . pa r rp leg ia ave bcreported in type II patients, No specific therapv exists for the dorder The diagnosis is made b1' the dernonstrarion of the decieocy of q-mannosidase actrvity in white blood cel ls or culturefibroblasts, and prenaral diagnosis has also been achieved.
CONGENITAL ISORDEBS f GLYG0SYLATI0NCDGS). hese areheterogenous group of aurosomal recessivedisorders tbac resfrom defects rn tbe processing and svnthesis of the carbohydramoiety of glycoprotetns.
There are at least 22 jdentiliable disorders; rype Ia is the mocommon (Table 87-4). One main group includes those rvdefects in biosynthesis or transfer of sugar chains from a lipihnked oligosaccharide precursor to a nerv protein in rhe endpLasmic eticulum (group Ia to IL). Group II (I la ro IIf) characcerjzed by defects in N linked sugar chain Golgi proceing. Undefined disorders are cemporarily assigned o group X.
A distinctive brochemrcal marker of che disorder r s the preence of carbohydrare deficient transferrin in serum and cebrospinal fluid. The most consisrent clinical t-eatures of t
disorder include psychomocor retardarion, which varies in sevity, and facial d1'smorphic fearures that rnclude a prominent )aand ears and inverted nipples. l'requenc neurologic Endings infancy include cerebellar atrophy lFiS. 87-7), hypotonia, weaness, hyperreflexia, and strokelike episodes,
In chrldhood, ataxia, muscle atrophl, decreaseddeep cendreflexes, toe r',alking, and continued strokelike episodes aobserved. The latcer events may be related to coagulopathjcharacterized by reduced factor XI, protein C, and ancithrombIII. Strabismus is a consistenr finding and retinitis pigmenrosacommon. Growth failure, liver dyslunction, retinal degeneratioand skeletal abnormalities have also been described. The skelefeatures can include contractures, kyphoscoliosis, and peccuscainatun, all of which ma y be secondary o rhe neurologiceifeof the disorder Pericardral effusion in older patienrs and hvoe
t roph icobs r rucL rv ra rd rom yupa rh tn rhe n lanra l " o occu iTransferrin studies ha.'e also revealed rhar infantile olivooon
tinecerebellar trophy is e revcre form ol LDC. Lrpudv'rropu'ith prominent fat pads on the buttocks is a dishnchve featurThe disorder should be considered in patients u.ith mental retadation, cerebellar hypoplasia, heparic dysfunction, and episodscrokelike pisodes, nd in parienrswith vari ous combrnationsrhe features detailed in the previous paragraph. The diagnosis cabe confirmed by analysis of the transferrin patrern by rsoelecrfocusing. Although prenatal diagnosis by analysis of transferrhas been attempted, rt has not proven reliable. Trcatment of thedisorders rs symptomaric, except for CDGIb. whrch respondsoral mannose (100-150 mgikgiday ever,v 4 6 hr), and possibCDGIIc, whrch may respond to oral fucose (25 mg/kg/day nd)

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 130/177
chapter 7 r Defectsr l{otEholism f carbohydrdes

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 131/177
622 " PARTX MetabolicDiseases
MPS-I MPS-tlPahcnts vrrhv in(nrs rr ,pes i mucopolrsrceharoscs :
r l i scasc.( l r |l VI : Nlrr)t . ru\ I t rnrv rs€; rse.t yr
MPS-|il tvtPs-tv MPs-vlHurlcr (hsers. . r fi I l : Llurrrr dis. isc. 1l yri l l l i S.rnl i ppo disersc, ! r: lV: Nlor.
t{P5
TI/PTl
FPOIIYMPfdundler-Hurel
t khee
|]S |]Lrilerhee1l funtr
lll A irnr:ppo
l l B sanfippoll ( lant ppo
I D sanflippo
! B lvlo:quo3
!l lviaroraaurJm/
6ENE
JNHERITAN(IHflOMOSOMEAR ,D14p163
DtttotvtNzYMt0 L dJ'cnift5e
cuonateullaler J,atasc
|]eparan'5ufim a5e
N.ircd-g oifll r dise
Aa tA ! uroam ce N
aaeryiran!lera!.!
l,l-d(-qluoJarninine
5ullileJljitJ5e
N-aclaacll]sanrne
5ullnt5JJalare
P a,rlactlr5idar
MIM
ASSAI NUM',tA(i/ 251
5U0!,tAi,aV 607
i,tAqav 60i05,tAl ioq {
L,[Ar,i\' 25260\ l
s,[At,i, )ti ,F,A. lt 9
MAttJLr (ALtArUnt5leyerelurer hercttpe.mentaldehaieni)1orea0ud g, edlh5!alyjef0rc
,rDf,t)€arJ
!r i l0nlr. i l )nredoLrdfo,dort i iydl !edi5ed5e,rcimal inteen(e,5urv!eto
aljr hcodPrefoiypptermedateet\reenfland ;
5e!ercouBesimlditolbLrdeali0rrea51i]douIee55prr]n0L,riedeaturc5,
atcrmJn.iegLat0r,rLn,rrlr0du hcd,{th m 0 ornl]mentdlieii(enlyBe,rv0o1prcbem5,rleeprqdsorder,aqg| t5r0n,pnqreslvedemerrJ,n
dr'9morphi5m,ii]aIeJil earaornl]as,suruallc dullfooc05lrblg
lA l
l",tl(,Iv
)(R
AR
AR
Ati
IDA pl64
iAA4p16
DJXq2, ' l28
,5l7q25
NA6LU'tQ1
H..juAi
8p1lq1 l
6 5I2q'14
6111516q24l
,1tl lpll ll
5h0rLrunldwarl inineorfeapdrtei , f taf t (er5. i iboneC)6pa5,r; lndlI'eighl 125 m
5i ear A, utm , leri luh. .0h1>l l l ]r
Vfi st rlRX flya roxdd5eeioenry AR
,4rid q: c .l Hurle'henoipewith arkei orneal0udqbut ornr,rlnteqefire;tld l] at qa r:0i nrne l"l,A(ridprirterd ?vererpE55ionndlffercfitfarn,e5 4 sulfden'atdre
litI5L irhsel6il5iJlq7111 tbf)ingfmmeGlf)dopr0mlCl'rno?h,Jn,erJs du!.ni nlrrnuloq'i.! tsgLliLlroni&\! 5,;Ar,(yHlALl )1) PErrtiola, d55e5.o ]ir,hphenotlpe |]yailmnca5et r
Li 9
6076
i:l tl
l 5 l 3
l lL.5
l5l2
)t 7
60' 4
l c 1 . . r e i a m . i 0 t t c ! ' A l , ; m! 1 r | | d ; i , l t h I m t ' ' . l t !a c ' ] r 0 j i J l ] l ' e " i $ , | l l / ' ! t d ! e

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 132/177
HurlerDisease. hi s fbrm of MPS I (lvlPs -H) rs a severe, ro -
arrery narrowing. Obstructive airway isease, nocably during
sleep, may necessicate racheotomy Ob ructive air',vav disease,
respiratory infection. and cardrac compl atiols are the common
causes f death.
Most chrldren$'tth Hurler s)'rdrome acquireonlv limited lan-
'r.r'irhdentigerous cysts,
Chapler 8 | Mucopolysaccharidoses
HurlerscheieDisease. he clinrcalphenotypeof NIPS IVS
incermediace ecweenHurLer and Scheiediseases nd is char
rerized by progressive somalic in\.olvemenr, including d,vsost
mult iplex with litr le or no intellectuaIdysfunction.The onse
symproms s usuallvobserved etrveen and 8 vr of age;surv
ro adulrhood s common. Cardiac nvolvemeotan d upper airu
obstrucrioncontribute ro cli nical morbidicy.Somepariencs a
spondylolischesis,vhich nay cause ord comptession.
Scheie0isease.N{PS -S s a comparativelymild disorderch
accerized v jornr stiffness, ort ic vah'e disease, ornealcloudi
and mrld dysostosismultiplex. Onset of signiGcant ymptomusually after the age of 5 vr, rvith diagnosis made betu'een 10 a
20 vr of age. Patients with Scherediseasehave normal rntellige
and srature but har.e significant joint and ocular involvement
carpal runnel syndrome ofren develops. Ophthalmic featu
include corneal clouding, glaucoma, and retinal degenera
Obstruccive airway disease, ausing sleepapnea) developsrn so
patients, necessrtating tracheotomy. Aortic valfe disease(L ,mmon nd ha r requ i red a lve ep lacementn somepa t ien
MUCOPOLYSACCHARIDOSISl. Hunter dis€ase MP S II) i s an
linked disorder caused by che de6cienc,vof iduronate 2-sulfat(tDS). Th e gene encoding DS is mapped o Xq2ll. Point mu
tionsof rhe DS genehavebeenderecredn abouc807o of patie
wirh \4PS IL Major delerions or reatrangements of the IDS ghave been found in the resr; these are usuallv associaredwlth
more severeclinical phenotype (seeFig. 88-2). Hunter dise
manifestsalmoscexclusrvely n males; t ha s beenobserved
ferv fernales and this is explained by skeu'ed rnactivarion of
X chromosomecarrying the normal gene.
\.larked molecular hecerogeneiw explains the rvrde clini
spectrum oi Hunrer disease.Paciencs'rth severeMPS II have f
I r ist 'c88. ] 'D-v5ostosismuhiplex.A,sanl i l ippodiseasc,4l r:TC, Hurler discase, 8 mo:.nterior supetx)r ypoptasia f l - -1 resul t rngn hooL-shaped ppearance

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 133/177
624 r PABTX MetabolicDiseases
cFigurc 88-4. Dysosrosismu[iplex. A, Mucopolysaccharidos,s MPS) I'H, 10 yr. The inferior porrions of the jlia are hypoplastic with resufting liac flar
shatlo{' ace|abular ossae.The femorat necksar€ in valgus position. B, MPS I-H, 4 yr . Metacarpalsand phalangesare abnormally shorr, wide, and defo
uith proxlmal pointing of the rnetacarpalsand bullet shap€dphalanges.Bone trabeculation s coarseand the cortices are thin. C, MPS l-S, 13 yr . The c
bonesare smalJ eading o a V-shapedconfguration of rhe digits. The short tubular bonesare well rnodeled.Flexion of the middte and dLstalphalanges I
causedbv ioint concractures.
B
tures simllar to those of Hurler disease xcept or rhe lack ofcorneal clouding and t}le somewhat slower progressionofsomatlc and CNS deterioration, Coarse acial features,short
staturerdysostosismultiplex, )oint sriffness, nd menral etarda-tion manifestbetween and 4 yr of age. Groupedskin papulesare present n somepatients.ExtensiveMongolian spots havebeenobservedn African and Asian patientssincebirth and maybe an early marker oI the disease.Gastrointestinal toragemayproduce chronic diarrhea. Communicatilg hydrocephalus ndspasticparaplegiamay developdue to thickenedmeninges. nseverelyaffectedpatienls,exrensive! lowly progressive euro-logic involvement recedes eath,which usuallyoccursbetween10 and 15yr of age,
Patientswith the mild form havea prolonged ife span,minimalCNS nvolvement, nd slow progression f somaticdereriorationwirh preservation f intelligence n adult life. Survival o ages65 ar'd 87yr has been reported; some palients had children ,Somatic features are Hurler-like but milder wi th a greatly
reduced ate of progression.Adult height may exceed150cm,Airway involvemen!,valvular cardiac disease, eating impair-ment, carpal tunnel syndrorne,and joint stiffnessare commonand can result n significant ossof function n both the mild andsevele orms.
MUCOPOLYSACCHARID0SISll. Sanfilippo iseaseMPS II) makesup a generically eterogeneousut clinically sirnilar group of 4recognizedypes.Each ype s caused y a differentenzyme e6-ciency nvolved n thedegradation f heparan ulfate see ig. 88-1), Mutatlons havebeen ound in all the MPS III disorders orwhrch the senes ave been solated.
Phenotypic ariation exists n MPS III patientsbut to a ldegree han m other MPS disorders.Patrenrswith Sanfidrseaseare characterizedby slowly progressive, evere
involvementwith mild somatic disease.Such disoroportirnvolvemenrf the CNS s unique o MPS ll, Onsettf clifeatures suallyoccursbetrveen ar'd, yr in a child who pouslyappeared ormal.Presentingeaturesncludedelayedopment, hyperactivity with aggressivebehavior, coarsehirsutism, leep isorders, nd mild hepatosplenomegalyse88-2),Delays n diagnosis f MPS II arecommondue o thephysical eatures,hyperactivity,and slowly progressive elogic disease. evere eurologjc ereriorarion ccurs n patientsby 5-10 yr of age, accompanied y rapid deteriorof socialand adaptiveskills. Severe ehaviorproblemssucsleepdisturbance, ncontrolledhyperactivity, emper antrdestructive ehavior,and physicalaggression re common.found mental retardationand behaviorproblemsoften occpatientswith normalphysical trength,making managemen
ticularlv difficult.
MUCOPOIYSACCHABID0SISV Morquio disease(MPS IVcaused y a deficiency f N-acetylgalactosamine-5-sulfataIV-A) or of p-galactosidaseMPS V-B). Both resuft n the dtive degradarion f keratansulfate.The geneencodingN-acgalactosamine-5-sulfatases on chromosome 16q24.3 andgeneencodingp-galactosidase, lBl, on chromosome p2:p-galactosidaseatalyzesGNogangliosiden addition to kersulfare,and mos! mutarionsof GlBl result n generalized

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 134/177
intelligence.MPS IV-A is usuallymore severe han MPS lV B,
*ith idult heightsof <125cm in the former and >150 cm in the
latter.There s considerable ariability of expressionn both sub-
rypes, owever.heappearancefgenua alga. yphosis. rorvthriiardaLion it h shorr runkan dneck, ndwaddling ar twnh a
tendency o fall are early symptomsof MPS IV (seeFig. 88-2)
Extra skeletalmanifestationsncludemild corneal louding,small
MUCOPOTYSACCHARIDOSISl Maroteaux-Lamy drsease N{PS
VI) is caused y mutations f rhe,4RSB en eon chromosome5q11-13 encodingN-acetylgalactosamine-4ulfatase arylsulfa-
taseB). It is characterizedy severeo mild somatrcnvolvemenr,
as seen n MPS I, but with preservationof intelligence The
somatic nvolvemenr f the severe orm of IVIPS l is character-
ized by cornealclouding, coarse aci features, ornt stiffness,
valvular eart isease,ornmunicating drocephalus,nddysos-
rosismultiplex se e rg. 8-21.n the severe.,rm.growthcan be
norma l o r rhe s t fewyears l ' l iFe u t seemsi r tua l lyo srop
after aee5-8 yr The mrld to intermediateorms of Nlaroteaux
Lamy Jiseasern be easily onfusedwirh Scheie yndrome,Spinal
cord compressionrom chickening f the dura in the upper cer-
vical canalwith resultantmyelopathv s a flequentoccutrencen
palienrswirh IVIPS l.
MUC0P0LYSACCHABID0SISll Slysyndrome MPSVll) is caused
by mutatrons f the GUSB en eocacedn chromosomeq21.11.
Mutations esuk n a deficiencyf p-glucuronidase,ntracellular
srorageof glycosaminoglycanragmentsand a very wide range
of clinical nr.olvement. he most severeotm Presenls s lelhal
nonimmune eralhydropsand may be detectedn uteroby ultra
dysostosismultiplex but normal incelligence nd usual cleal
corneae. hey may be found incidentallyon the bastsof bloodsmear hat showscoarsegranulocvtic nclusrons.
MUC0P0LYSACCHABIDOSISX.The disorders caused ;ra muca'
acetabulae ere rheonly radiographic indings.
ChspterSS Mucopolysaccharidos
DIAGI{OSISNDDIFFERE]IITIATIAGl{OSIS
Radiographs f chesr, pine,pelvis,and handsar usefulcodearlv igns f dysostosrsultiplex se e igs. 8-3 nd 88-4)quantitativespot tescs or increased rrnary GAG excretio
ably be diagnosed n serum using monoclonal antibodkeratansulfate.Any indivrdualwho is suspected f an MPorder basedon clinical features, adiographic esults,or uGAG screeningests houldhavea definitivediagnosis stabby enzyme assay,Serum, leukocytes,or cultured fibroare usedas the tissuesource or measuring ysosomalen(see Table 88-2). Prenatal diagnosis s available fomucopolysaccharidosesnd is carriedout on culturedcellsamniotic luid or chorionicvillus biopsy.Measurement f Gin amniotic fluid is unreliable.Carrier testing n Huntedrome,an X{inked disordeq equiresanalysis f 1DSgenthe specificmutation or chromosome t.angementn the funder consideration s known. Molecular analysis n Pawith other mucopolysaccharidosesr rn known carriers ea specrficationale.Attemptsare beingmade o developmetor routrnenewDornscreenlng-
Mucolipidoses nd oligosaccharidosesanifesrwith theclinical and radiographic eatures s mucopolysaccharidoChapters 6,4an d 86.5). n these onditions,he urinarytion of glycosaminoglycanss not elevated.Hurler-hke acirures, oint contracture!. ysostosismulriplex,and elurinary GAG excretiondilferentate the mucopolysacchafrom other neurodegenerativend dwarfing conditions.
TBEATMEI{T
Bone marrow transDlantarion from related or unrelated dor cord blood transplantation results in significant c
improvement of somatic drsease n MPS I, II, and Vl, C
effects include increased life expecta[cy, resolution or imp
ment of growth failure, heparosplenomegaln joint stiffness,
appearance, pebbly skin changes in MPS II, obstructive
apnea, heart disease,communicaring hydrocephalus, and h
loss. Enzyme activity in serum and urinary GAG excretion
malize. Transplantation does not significant ly improve the
ropsychologic ouccome of MPS patients if there is irnp
mentation at the time of transplaoration. This is true for M
H, II, and III. Patients with MPS I who have undergone
plantation befbre 24mo of age and with a baseline m
derrelopment ndex >70 have improved long-rerm or:rcome
transplantation in MPS Il may have the same effect. Tran
tarion in MPS VI stabili zes or improves cardiac manifestaposlure, and joinr mobility, Stem cell transplantalion do
correct skeletal and ocular anomabes; they have to be t
with appropriare orthopedic and ophthalmologic proce
Cord blood lransplantalion is the therapy of choice in ch
with MPS I-H, and possibly MPS lI, before the age of 2 y
transplantation-related dearh or primary graft failure,
occurs in =307o of the patients, must be weighed against
therapeutlc optlons.
Enzyme replacement uslng recomblnant enzymes is app
for patrents with MPS I, MPS II, and MPS VI. It re
organomegaln ameliorates rate of grouth and joint mobiliry
reduces rhe number of episodes of sleep apnea and urinary

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 135/177
626 PABT r Metrbolic iseos.s
excretion.The €nzymes o not cross he blood-brainbarrieranddo not prevent deterioration of neurocognitive nvolvemeot.Consequently, rhis therapy is the domain for patients withmild centralnervous nvolvement.To stabilize€xtlaneuralman-ifestations,t is also ecommendedn young patientsbeforestemcell transplantation.The combination ol enzyrne eplacementtherapy and stem cell transplan tationmay oIf€r the best reat-m€f,t. Recombinart iduroflate-2-sulfatasemeliorates he non-newologic manifestations f Hunter disease, nd recombinantN-Ac-gal4-suUataseas beensuccessfullyested n patientswith
MPS VI.Prirnary prevention through Beneticcourseling and tertiafy
preyention o avoidor treat complications emains he mainstayof supportivepediaric care,Multidisciplinary attention o respi-ratory and cardioyascular omplicatiofls,hearing loss, carpaltunnel syndrome,spinal cord compression, ydrocephalus, ndotherproblems angreatly mprove hequaliryof life for patientsand theL families (Tabte88-3). The progressive atureof clini-cal involvementn MPSpatientsdictates he need or sp€cializedand coordinatedevaluation.
Allen JL: Treatmenr of respiratory syst€m(not just lung) abnormaljtiesmucopofysaccharidosis I. J Ped.iatr 20n4;144:561-562.
BeesleyCE" Meaney CA, Greenland G, et al: Mucational aralysis of mucopolysaccharidosis ype I families: Frequ€ncy of known mu[arjoidentincation of 17 norel mulacions and in viro expression of misse
muratioff, Hrrtt Genzt 2O0(;1O9:5Q3-511.
BroadheadDM, Kirk JM, Burt d er al: Full expressionof Hunrer's diseas
a femalewith an X-chromomme deletion eading to non-random rnact
ti,on. CIin Gerret 1986i30:392-39 8.
Cheng Y, V€rp MS, (nui€l I Hibbard JU: Mucopolysaccharidosisy?e all
a cause of recu-trena non-immune hydrops fetalis. J Pettwt M
2003i31:535-537,
Fuller M, Rozaklis T, Ramsay SI. et al: Disease-specinc markers for
mucopolysaccharidoces. PeAafi Res 2004\561733-738.
Grewal SS,Wnn R, Abdenur JE, et al: Safery and effrcacy of enzyme repla
menr rherapy in combitration with hematopoietic stem cell transplantatioin Hr:rlet syndrome. Genet Med 2005;7t1,43-146.
Harmatz P, Ging[ani R, Schwartz I, et al: Enzyme replacemenr thera
for mucopolysaccharidosis M: A phase 3, randomized, double-blinplacebo-concrolled, multinational study of recombrnant humanacetylgalactosamin€+sulfatase (recombrnant human arylsulfatase B
RHASB) and fofLow-on, openlabel extension study, J Pediafi 2006;14533-539.
Harmarz 4 Whitley CV, Waber L, et aJ: Enzyme replecemeot rherapy
mucopolysaccharidosis VI (Maroteaux-lffy syr.&ome). I Pedi
2004;144574-580,
Hershkovitz E, Young Er Cmper A, et al: Bone marrow transpLantatior Maroteaux-Lei$y syndrome.J b herit Metab Dis 1,999t22r5}4z
Ito K, Ochiai T, Suzuki H, et al: The effect of haematopoieticsrem cell traplant on papuleswith
'pebbly'app€rence in Hunter's syndrome. BrJ D
matot 2004;15 1 207 271,
Meilde PJ, Ranien E, SkLmonsen , et al: Newbom screening or lysoso
srorage disordersr Clinical evaluetion of a two-trer stategy. Ped.iat2004i714:9O9-914.
Muenzer J: The rnucopolysaccharidoses: heterogeneous roup of disordwith variablepediatric prcse$tations./ Pedidt200444:527-533.
on J, Crowhursr J, Carey B, Greed L: Incidence of rhe mucopolysa
charidoses n V€srern Australia, An J Med Genet A 2003;123A:31
313.Ochiai I lto K Okada T, et aL Significanc€ f ext€nsiveMonBolian spors
Hunter's syndrome.8r / Defltutol 2003t148t1173-1178.
Robeftson SB Idug GL, Roge6 JG: Cerebrospinal luid shunts n the ma
agement of behavioural problems in Sanflippo syndrome (MPS I )
Pediatr 1998\157 953-65 5.SouillecG, Guffon N, Maire I, et al: Ourcome of 27 patienrswith Hurle
syndrome ransplanted rom eirher elatedor unrelat€dhaemaropoietic t
cell sources.Bonc Marrolr Traflsplant2003;37:1105-1117.
Saba SL, Escolar MI. Po€ vt er al: Cord-bJood ransplanrs tom unrela
dono$ in pati€$ts with Hurler's syndrome. Nea, Engl I Med 2004135
1960-1969.
Tomatsu S, Okamura K, Tak€rani T, et al: Development and testrng of n
screening method for kelatan sulJate in mucopolysaccharidosis IVA. Pel,d
Res 2004;55 592-597Triggs-RaineB, Salo TJ, Zh^nE 4 et ^L Mutations in HYAU, a member
a taademly distibured mubigene femily €ncoding disparate hyaluronid
activities, cause a newly describ€d ysosomal disorder, mucopolysacch
dosis IX. Pnc Ndt Acad Sei U S A 199996:62964300 .
VeJlodi A, Young E, Cooper A" et a| lrcng-term follow-up following bo
marrow transpfantatiotr for Hunler dtsease. J Inheit Meab D
1999i221638-548.
Vihox \(R: Lysoeomal storage disc,rders: The need for beBer pedianic reco
nrtion and comprehursive czre. J Pediav 20041,144: S3-S14.
WrairlJE, Clarke LA, BeckM: Enzyme epLac€menth€rapy or mucoFolys
charidosis I: A randomized, double-blinded, placebo-controlledrnLrlttional study of recombiaant human o-jduronidase \LaronidaseJ. J Ped.
2004j144:581-588.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 136/177
The inherited disorders of purine and pyrimidrne metabolism
Purines are involved rn all biologic processes;all cells require
a balanced supply of purines for growrh and survival. They
orovide th e ptimary sourceof cellularenergy hrough adenosine
irrphosphate ATI-) and. Logetherwirh pyrimidines' proride rhe
source or the RNA and DNA that stores, tlanscribes, and trans-
lates qenetic information. Purines provide the basic coenzymes
(NAD-, NADH) for metabolic regulation and play a ma,or role
in sisnal transduction (GTl cAMP, cGMP) Metabolically active
nucliotides are formed from heterocyclic nitrogen-contarning
Urlc acid is not a specific drseasemarkeq so the cause of its ele-
vation mus! be determined- The level of uric acid present at any
time depeflds or the size of the purine nucleotide pool, which rs
derived from de novo purine synthesis, catabolisrn of tissue
nuclerc acids, and increased rurnover of preformed purines. Uric
acid is poorly solubl€ and must be excteted continuously to avoid
ro{ic accumulations in the body. Its renal excretion involves lhe
following components: (1) glomerular filtration, (2) reabsorption
in rhe proximal coavoluted cubule, (3) secretion near the lermF
Chaptoi 9 r Diso.doFof Puiine nd Pyrimidinolelabolism.
nus of rhe proximal tubule, and (4) limited reabsorption
these secretory sites. Thus, renal loss of uric acid is resu
renal rube excretion and ls a function of serum ull acid
centration and a homeostatic mechanism to avoid hyperurice
Because renal rubule excretion is greater in chrldren tha
adults, serum uric acid leve.lsare a less reliable indicator of
acid production in children than in adults, and conseque
measurement of the level in urine may be required to determ
excessiveproduction. Clearance of a smaller portion of uric
is via the gastrointestinal tract (biliary and intestinal secret
Owing to poor solubrlrty of uric acid under rrormal circstances,uric acid is near the maximal tolerable limrts, and s
alteratrons n production or solubility or changes n secret ion
result in high serum levels. In renal nsufficiency, urate excre
is increased by residual nephrons an by the gastrointestinal tr
lncreased production of uric acid is found in malignancv; R
syndrome; Down syndrome; psoriasis; sickle cell anemia; c
otic congenital hearr disease; pancreatic enzyme rePlacem
glycogen storage disease ypes I, I[, IV, and V1 hereditary f
lose ifltolerance; acyl coenzyme A dehydrogenasedeficrency
eout.The metabolism of both purines and pyrirnidines can
drvided into two biosynthetic parhways and a catabolic pathw
The 1sr, the de novo parhway, involves a multrstep biosynth
of phosphorylated ring structures from precursors such as C
glycine, an glutamne. Pr-rrineand pyrimidine nucleolidesproduced om nbose-S-phosphate or carbamyl phosph
respectively.The second, a single-step salvage pathwav, reco
purine and pyrimidine basesderived from eicher dietary intak
th e cataboLcpathway {seeFigs. 89-1, 89-2, and 89-3). n rh
novo pathway, the nucleosides guaoosrner adenosifle, cylid
uridine, and thymidine are formed by' che addition of nos
phosphate to the purine basesguanine or adenine' and to
pyrimrdine bases cytosine, uracil, and thymine. The phosph
Iation of these nucleosides produces monophosphale, dip
phate, and triphosphate nucleotides. Under usual crrcumsta
the salvagepathway predomrnates over the biosynthetic path
Synthesis is most active in trssues with high rates of cel
turnover, such as gut epithelium, skin, and bone marrow.
Phosphoribosylpyrophosphate(PRPP)synthetase
o ol l lP-O-P-O
OH O
l ' ' tsurc 1) . Ea r v xeps rn hebiosln the ' rs frhe purine ring.
Phosphoribosyl--pyrophosphate
(PRPP)
c
c
OHIc\
N/
N
cH <-nr Num€rouseactions
Inosin€-5rphosphate(lnosiniccid,MP)
D-ribose hosphate
5-Phosphoribosylamine

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 137/177
628 PART I Motabolic iseases
DNAsynthesis - dGTP
+I
RN A I
Feedbackinh ib i t i on - - - - -
De novo---> synthesis
DN AdATP-----t- synthesis
I
II RN A
Feedbackinhibit ion
synthesis -
Guanosine
II{o
GT P
tAdenosineeaminase
deficiency
q F- Adenosine
--------->synthesis
Adenine hosphoribtransteraseef cienc
ATP
1Inosiniccid
(rMP)
IY
-+ -----+ --_-r- Adenylicacic
Hypoxanthine-guanrnePRPP
lransferase
Hypoxanlhineriboside(lnosine)
+ PRPP + PRPP
NH ,t -
Adenine
+ Phosphoribosyl--pyrophosphatePRP
tI
II
Hypoxanthine
_lXanthine xidaseT
I
o Y oI
Ribose-s-phosphateA
H
Xanthine
Figurc89-2.Parhwaysn purinemerabolismndsaLvaBe.
third pathway is catabolism.The end product of the catabolcpathwayof thepurines s uric acid,whereas atabolism f pyrim-idinesproduces itric acid cycle ntermediates. nly a small rac-tion of the purines turned over each day are degradedandexcreted.
lnborn errors n the synthesis f purinenucleotidesnclude: 1)phosphoribosylpyrophosphatesynthetase superactivi!y, (2)adenylosuccinaseefrciencnand (3) 5-amino-4-imizolecarbox-amide (AICA) riboside deficiency AICA-ribosiduria).Disordersresulting from abnormalities n purine catabolism ncluder(4)muscleadenosinemonophosphate AMP) deaminase eficiencn(5) adenosine eaminase eficrency,6) purine nucleoside hos-phorylase eficiency, nd (7) xanthineoxidoreductase eficiency.
Disorders esulting rom the purine salvage athway ncluder 8)hypoxanthine-guanine hosphoribosyltransferaseHPRT) deli-ciency, and (9) adenine phosphoribosyltransferaseAPRT)Genclency,
Inborn errors of pyrimidine metabolism nclude disordersofp1'rimidine ynthesis nd of pyrimidine nucleotidedegradation.Disorders nclude: (1) hereditary orotic aciduria {uridinemonophosphace ynrhasedeficiency), (2) dihydropyrimidinedehydrogenaseDPD)defrciencl',3) dihydropyrimidinaseDPH)deficiencS 4) p-ureidopropionase eficiency, 5) UMPH-1 defi-ciency (previously pyrimidine S'-nucleoridase eficiency),(5)pyrimidine nucleosidedeplerion and overactivecytosolic 5rnucleotidase,7) thymidinekinase2 defrciency,nd (8) thymidinephosphorylase efi iency.
H
Uric acid
GOUT
Gout presentswith hyperuricemia,uric acid nephrolithiand acute inflammatory arthritis. Gouty arthritis is duemonosodiumurace rystaldepositshat result n nflammatiojoints and surrounding issues.The presentation s most cmonly monoarticulai, ypically n the metatarsophalangeaoof the big toe.Tophi,deposrts f monosodium ratecryscals,occur over poirits of insertionof tendonsar the elbows, knand feet or over the helix of the ears.Primarygout, ordinaoccurring n middle-agedmen, results rom overproductiouric acid,decreasedenalexcretionof uric acid,or both. The b
chernical tiologyof gout is unknown for most of thoseaffecand it is consideredo be a polygenic rait. When hyperuriceand gout occur n childhood, t is mostoften secondary out,result of another drsorder n which there s raprd tissue bredort'n or cellular urnover eading o increased roducriodecreased xcretion of uric acid. Gout occurs n any condithat leads o reduced learance f unc acid: during therapymalignancy or wrth dehydration, actic acidosis,ketoacidstarvation, diuretic therapy, and renal shutdown. Excespurine,alcohol,or carbohydratengestionmay ncrease ric atevels,
Gout is associated ith hereditarydisorders n rhreediffeenzyme isorders har result n hyperuricemia. hese ncludesevere orm of HPRT deficiency(Lesch-Nyhandisease)

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 138/177
Chapter 9 r oisoiders l Purin.andPydmidineMet.bolisn r
cooHI
NH, CH,t - t -c-:o-Hc-cooH
NH
/*Carbamyl-L-aspartaie
OH
Nz"'cH.--------->
| |-
O:C.rr.,C$!O"
UMPSynthase(Orotidyliccid
, decarboxylase)+1f-
Feedback
inhibiiionor
rcpress|on
Iriboss hosphate
orotidine-5honophosphale (OMP)
OHI
*zc-c"t t l
O:C\N,,-C-cooH
Dihydrooroticacid
. , \ n u
co2+ I ll- vn
Iribose hosphate
uridine '-monophosPhateUlvlP)
IY
Orotic cid
UTP RNACTP l--------+anddCTPI DNAdTTP synthesis
Figure 89-3. Pathways n pyrimidine biosynthesrs.
diminished renal excretion of urate. Glycogen storage disease
types III, Y nd VII are associated with exercise-inducedhyper-
uricemia, th consequenceof rapid ATP urilization and failure to
regenerate t effectively during exercise(seeChapter 87 1). Auto-
somal dominant iuvenile hyperuricemia, goury arthritis,
ulin-associated kidney disease IJAKD) has beenproposed. Unlike
the three inhented purine disorders that are X-linked and the
recessively nherited glycogen storage disease, hese are autoso-mal dominant conditions. Familial iuvenile gout or familial juve-
nephropa hy.
Treatmentof hypenricemia nvolves he combinarionof aurinal (a xanthine oxidase nhibitor) to decrease ric acidduction.probenecido increase ric acidclearancen thosenormal rinal function, alkalinizationof the urine to increa
solubiliw of uric acid. and increased luid intake to reducconcentrationof uric acid.A low-purine diet, weight reduand reducedalcohol nrake are recommended.
ABiIOBMALIIIESNPURII{EATVAGE
LESCH-NYHANISEASElJ{D}.This is a rare Xiinked disordpurine metabolism that results from HPRT deficiencyenzymes normallypresentn eachcell n the bodn but its hiconcentrations n the brain,especiallyn the basalganglia.ical manifestationsnclude hyperuricemia,ntellectualdisadystonic movement disorder that may be accompanichoreoathetosisnd spasticiry, ysarthricspeech, ndcornp
self-biting,usuallybeginningwith the eruption of teeth,There are severalclinical presentations f HPRT delicHPRT levelsare related o the extentof motor symptoms,presencer absence f self-injury, ndpossibly o the evelofnitive function. The majority of individuals with classichave ow or undetectableevels f the HPRT enzyme. artiaciency n HPRT (Kelley-Seegmilleryndrome)with >1.5-2enzyme s associated ith hyperuricemia nd variableneurodysfuncrion neurologicHPRT deliciency).HPRT defrcienclevels 87o eads o a severeorm o{ gout,with apparently ocerebral unctioning HPRl-relaredhyperuricemia) lthougnidve deficitsmay occur.Qualitarivelysimilar cognitive dorofileshavebeen eported n both LND and variant casesints produced sco.is that are intermediateberween ho

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 139/177
630 PARTX Mdabolic Diseases
patients u'lth LND and normal controls oo nearly everv neu-
ropsychologic measure tested.
Genetics. The H?RT gene has been localized ro the long arm
of the X chromosome (q26-q27). The complete amino acrd
sequence for HPRT is known (=a4 kb; 9 exons). The drsorder
appears in males; occurrence rn lemales is excremelv rare and
ascribed to nonrandom lnactivation of the normal X chromo-
some. Absence r.:f HPRT prevents che normal merabolism ofhl.poxanthine resulting in excessive uric acid producrion andrnanifestations of gout, necessltating specilic drug treatmenr
(allopurinol). Because of the enzyme deficiency, hypoxanthineaccumulates n the cerebrospinal fluid, but uric acid does not; uric
acid rs not produced in the brain and does nol cross the blood-brain barrier, The behavior drsorder is no! caused by hyper-
uricemia or excess hypoxanthine because patients with partial
HPRT deliciencl rhe variant$ with hyperuricemia, do not selfi-
injure and infants having isolared hyperuricemia from birth do
not develop self-iniurious behavior-
The prevalence of the classic Lesch-Nyhan disease has been
estimatedar 1/100,000 co 1/380,000. The rncidenceof partial
variants ls no! known. Those with classic LND rarely surwive hetr d decadebecau"eof renal or respirator) compromise.Th e l i ie
span rnay be normal for patiertts with partial HPRT deficiency
without severe enal involvement.
Parhology.No specific brain abnormality rs documented after
detailed histopathology and elecrron mrcroscopy of affected brainregrons.Magnetic resonance maging has docunenred reductions
in the volume of basal ganglia nuclei. Abnormalities in neuro-
transmitter metabolism have been idenri6ed in three autopsied
cases.All three patients had very low HPRT levels (<1ol" rn stri-
atal tjssue and 1-2Y" of control n thalamus and cortex). There
was a functional loss of 65-90% of che nigrostriatal and
mesolimbic dopamine terminals, although the cells of origin rn
rhe substantia nigra did not show dopamine reduccion. The brain
regions primarily involved were the caudare ntrcleus, putamen,
and nucleus accumbens. It is proposed chat the neurochemical
changes ma,v be linked to functional abnormalities, possrbly
resulting from a djminution of arborization or branching of den-
drites rarher than cell loss. A neurotransmitter abnormalrty i s
demonsrrared by changes in cerebral spinal flurd neurotransmit-
ters and their metabolites, and confrrmed bv posrtron emissiontomography scans o[ dopamine {unction. Reductions in vrvo in
the presynapric dopamine transporrer have been documented in
rhe caudatean d putamen of six individuals.
The mechanism whereby HPRT leads to the neurologic and
behavroral symptoms is unknown. Borh hypoxanthine and
guanine metabolism is affected; guanosine triphosphate {GTP)and adenosinehave substantial effects on neural tissues. There is
a functional link betra'eenpurine nucleotrdes and the dopamine
system that involves guanine, the precursor of GTP Dopamine
brnding to its receptor results in either an activatron (Dr
receptor) or an inhrbition (D2 receptor) of adenylcyclase. Both
receptor effects are medrated by G proreins (CTP-binding
proteins) dependenc on guanosine diphosphate (GDP) in the
GDP/GTP exchange or cellular activation. Dopamrne and adeno-
sine s,vstemsare also linked through the role of adenosine as aneuroprotective agent ln preventi[g neurotoxiciry Adenosrne
asonists mimic the biochemical and behavioral actions of
d6pamine antagonrsts, whereas adenosine receptor antagonists
act as funcrional dopamine agonist s. Dopamine reduction in
brain is documented in HPRT deficienr strains of mutant mice.
Clinical Mani{estati0ns. At birrh, infants wirh LND have no
apparent neurologic dysfunction. A fter several months, develop
mental delan intellectual disabilicy, and neurologic s igns become
apparenl.Before he ageof 4 mo. hyporonia. ecurrentvomiting.
and difficulty r,'ith secretions may be nored. By =8-12 mo,
extrapyramidal signs appear, prirnarily dystonic movemenrs. In
some cases!spastrcity may become apparent at this time or, in
some instalcest later in life.
Cognirive function is usually reported to be in che nild-moderate range of rntellectual disability, alchough some indruals test ln che low normal range. Because est scores mayinfluenced by drfficultv m tesdng rhe sub,ects owing to t
movement disorder and dysarthric speech, overall inrelligemay be underestimated.
The age of onset of self-injury may be as early as 1 vr aoccasionally, as late as rhe teens. Self-injury occurs, althoughsensory modalities, including pain, are intact- The self inluriobehar.ior usually begins with sel{-biring, although other patte
of self-injunous [rehavior emerge wrth time. Most charactercalln the fingers, mourh, and buccal mucosa are mutilated. Sbiting is intense and causes issue damage and may result ln amputation of fingers and substanrial loss of rissue around lips (Frg. 89-4). Extraction ol primary reerhmay be required.biting parrern can be asymmetric, with preferentral mutilation
the left or righr side of rhe bodl'. The cype of behavior is dif
ent from rhar seen in other intellecrual disability slrndroinvolving self-rnjury; self-hitting and head banging are the m
common initial presenrations n other s)'ndromes.The inrensi rthe self-injurious behavior generally requires chat the parient
restrained.When restrajnts are removed, the individual rvitl LN
may appear erfified, and stereot)?icalll' placea 6nger in chemouThe patient may ask for restraints to prevent elbow movemwhen the resrraintsare placed or replaced, he patrent may app
telaxed and better humored. Dysarthlc speech may cause rnpe$onal commumcation problems; chehigher-functioning childcan express hemselves ully and participate in verbal rherap1.
The self-mutilation presenrsas a compulsive behavior thatchild tries to conrrol bur frequently is unable to resis t. Older rn
viduals may enlist the help of others and notify them when t
are comfortable enough ro have restuaints removed. In so
instances, the behavior may lead to deliberate self-harm. In
viduals with LND may also show compulsive aggressron
inflict injur,v to others through pinching, grabbing, or hittingby using verbal fotms of aggressron.Afterwards thev may ap
ogize, stating that rheir behavior was out of their concrol. Or
maladaptive behaviors include head or lrrnb banging, eye pokiand psvchogeoic vomiting.
Diagflosis.The presenceof dystonia along wirh self-mutilat
of the mouth and frngers suggests Lesch-Nyhan disease. Wpartial HPRT deficiency', ecognition is linked to either hypuricemia alone or hyperuricemia and a dystofllc movemenr
order. Serum levels of uric acid >4-5 ms uric acid/dl- anurine uric acrdrcreatininr atro oi 3:4 or more are highly sugtive of HPRT deficrenc%particularl)' when associatedwirh n
rologic symptoms. The defininve diagnosis requires an analof che HPRT enzyme. This is assayed n an erythrocyte lys
Individuals wrth classicLND have near 07o enzvme activity a
rhosew iLhp . r r l i J l a r ian rshuw va lues etween . iq . and 60
The intact cell HPRT assal' rn skin fibroblasts offers a good c
relation benveen enzyme acrivity and the severity of the diseM-olecular cchniqr-resre used br genesequencrng nd rhe d
trfrcatton ot catflers,Di{ferential diagnosis includes other causes of i nfanhle hy
tonra and dystonia. Children with LND are often initially increctly diagnosed as having athetoid cerebral palsy. !' hendiagnosis of cerebral palsy is suspected n an infanr with a normprenatal, perinatal, and postnatal course, LND should be c
sidered. Patial HPRT deliciency may be associated u.ith ac
renal failure in infancy; therefore, clinical awareness of par
HPRT deficiency i5 of parricular importance.
An understanding of che molecular disorder has led to ef
tive drug treatrnent for uric acrd accumulation and anhritic toprenal srones, and neuroparhy. Reduction rn uric acid alone d
not rnfluence the neurologic and behavioral aspects of LN
Despire rreatment from birth for uric acid elevation, behavroand neurologic sydptoms are unaffected. The most srgmfic
complications of LND are renal farlure and self-mutilatxrn-

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 140/177
Figurc 89-4. SelI-iniurv in Lesch-
Nyhan disease. issuedamaBe o the
lip 1Al and fineers fBl was selfinflicr€d. Managernent o{ rhis
problem requires covering any dan-
gerous porcions of rhe wheelchair in
combinarion with Protectrveresuaints fcl. (From VisserJL Bar
PR, Jinah HA: Lesch-Nyhandisease
and the basalganglia.BlaillRes Rer
2000;32:449a7)
ChoDter9 Diso.d€FofPuiineendPyrimidino otabolism
alone, usingoperalt conditioning approaches, ave nor pro
ro be an adequate eneral r€atment.Altl,ough behavioralpcedureshave had some selecti*'e uccessn reducingself-injgeneralization outside the experimental setting limits tapproachand palientsunder stressmay revert o their previself-injunous ehavior.Behavioral pproachesmay also ocusreducing the self-injuriousbehavior rhrough the treatmen
phobic anxiety associatedwith berngunrestrained,The rn
common techniquesare systematicdesensitization, xtinctand differentral rernforcementof other (competing)behavStressmanagement as been ecommendedo assistpatieDtdevelop noreeffecrive opingmechanisms.ndividualswith LNdo not respond o contingentelectricshock or sirnilar averbehavioralmeasures. n increasen self-injurynay be obsewhen aversivemechods re utilized.
Restrainr day and night) and dentalprocedures te commmeans o preventself-injury.The time in restraints s linkedthe ageof onsetof self-injury.Childrenwith LND canparticipin makingdecisionsegarding estrairtsand he typeof restraThe time n resrraintsmay potentiallybereducedwrth systembehavior reatment rograms.Many patientshave eethextracro prevent self-injury. Others use a protective mouth gudesigned y a dennst.Most parentssuggesthat stress educand awareness f the patient's ne€dsare the mosc effectivreducing elf-injury.Positrve ehavioral echniques f rernfor
lppropriate behavior are rated effectiveby almost half of taml11es,
ADENINEPHOSPHORIBOSYTTRANSFERASEAPRTIDCFICAPRI a purine alvagenzyme,atalyzeshe synthesisf Afromadenine nd5-phosphoribosyl-1-pyrophosphatePP-nP),The absencef this enzymeesultsn the nabihty o utadenine and accumulated adenine being oxidized by xanth
dehydrogenase co 2,8-dihydroxyadenine, which is extrem
Treabnent.Medical management of this disorder focuseson the
ble. Self-mutilation is reduced through behavior management and
the use of restraints, removal of reeth, or boch. Injection of borulism toxin into the masseter muscles was useful in one patient.
Pharmacologic approacbes to dectease anxiety and spasticity
rvith medication have mixed results. Drug cherapy focuses on
svmptomaricmanagementof antrcrpatoryanxiery,mood srabil-
irarion, and reduction of self-iniuriousbehavior.Diazepamma y
be helpful for anxiety symptoms' and calbamazePine ol
gabapentin for mood srabilization.Each of these medications
may educe self-injuriousbehavior by helprng o reduceanriery
and srabilize mood.
the birth of an unaffected male infant.
Both the motivation for self-injury and its biologic basis must
be addressed n creatment programs. Yet behavioral techniques

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 141/177
GPI PABT r Metabolic iseases
rnsoluble.APRT deficrency s presenr from birth, becomingapparentas early as 5 mo and as ate as the 7rh decade.Genet-ics:The disorder s anautosomal ecessiverait with considerableclinical heterogeneicy.he AIDRT ene s locatedon chromosome16 q(16q24.3) nd encompasses.8 kb of genomrc NA , Thereis an APRT knockout mousemodel that replicares he diseaseprocess.Clinical manifestationsnclude urinary calculus orma-tion rvichcrystalluria,urinary tract infecrions,hemaruria, enalcoLic, ysuria,and acute enal ailLrte. he presence f brownishsporson the infant'sdiaper or of yellorv-browncrystals n the
urine is suggestive f the diagnosis, aboratory indings:Urinarylevels f adenine, hydroxyadenine,nd 2,8-dihydroxyadenineare elevated,vhereas lasmauric ac id rs normal.The deficiencymav be complete type ) or pardal (type I); rhepartial deficiencyis reported n Japan.The diagnosiss madebasedon che evelofresidualenzyme n erythrocyte ysates.The renal calcuJi,com-posedof 2,8-dihydroxyadenine,re radiolucent,soft, and easilycrushed. Thesestones are not distineuishable rom uric acid\tone\ hv routine esrsbur requirehigh-pressureiquid chromatographv HPLC), ultravroletor infrared radiation detection,mass pectroscopyMS),x-ray crysrallography,r capillaryelec-trophoresis or diagnosis, articularly o distinguish rom stonesin HPRT defrciency.
Treatment ncludes igh fluid intake,dietarvpurineresrnction,and allopunnol,which inhibits the conversionof adenine o irs
metaboltes,urther ,8-dihydroxyadeninexcrerion,nd uftherstone formation. Alkahnization of tbe urine is ro be avoided,because,nJike hat of uric acid, he solubiJity f 2,8-dihydrox-
,vadenrne oes not increase up to a pH of 9. Shock-wavelithotnpsy has been reported to be successful. he prognosisdepends n renal function at the rime of diagnosis.Early treatment is critical rn the preventionof stonesbecause evere enalinsuffrciencymay accompanvate recognrtron.
DISORDEBSINKEDOPURINEUCTEOTIDESYNTHESIS
PHOSPHORIBOSYTPYBOPHOSPHATEPBPPISYNTHSTASEUPEB-AGTIVITY.RPPs a substratenvolvedn the synlhesisf essen-trallyall nucleotidesnd rnportant n rhe egulation f rhedenovoparh!{'aysf purineand pyrirnidine ucleotide vnthesis.This enzymeroduces RPProm rjbose-S-phosphatend ATIasshownn Figures 9-1and89-2-PRPPs he 1scntermediarycompound in the de novo synchesis f purine nucleotides rhat lead!o the formatron of inosine monophosphace. Superactivrty of theenzyme results in an increasedgeneration of PRPP BecausePRPPamidotransferase, the 1st enz;.me of the de novo pathwan rs notphvsiologically saturated by PRPP, the synrhesis of purinenucleorides increases,and, consequently, the production of uricacid is increased. PRPP s;rnthetasesuperactlvity is one of the fewhereditar;,''djsorders in which there is enhancement of the acrrv-rty oi an enzyme.
Genetics: Phosphoribosylpyrophosphare synthetase (PRS)
superactivity is inherited as an X-linked rrait and presencswithtwo clinical phenotypes with varying degrees of severicl'. Threedrstinct PRS cDNAs have been cloned and sequenced.Two forrnsare X lrnked to Xq22-924 ar'd,Xp22.2-p,22.3 (escapesX inacri-vation), respectively,and are widely expressed; he third maps tohuman chromosome 7 and appears to be transcribed only in rhetestes.Even though the defect is X linked rt should be consideredin a child or voung adult of either sex with hyperuricemra and/orhyperuricosuria and normal HPRT acrivrty in lysed red cells.Clinical manifestatioos in the more severe vDe in affected hem-izygousmales rncludr signsof uric acid overproductron har ar eapparent n infancy or early childhood, neurodevelopmental
ior have been described.Heterozygous emale rriersalsodevelopgout and hearing mpairment.The la juvenearlv adult onset ype s found in maleswho show gour oac iduro l i rh ia r rsur no neuro log ic : igns .mechan i .moneurologicsymptoms s unknown. Laboratory findings: Buric acid may be two to three times normal values,anurinary excretion of uric acid is increased.The diagrequires nzyme nalysis f erythrocytes nd cultured6brob
This disorder must be drffe rentiated rom partial HPRTciency nvolving he salvage arhwanwhich also esulrs nr:ologicHPRT deficiencyor hyperuricemiawithout neurleatures,
Treatment s wirh allopurinol,which nhrbitsxanthineoxithe ast enzymeof the purine catabolicpathwav.Uric acrdduction is reducedand is replacedby hypoxanthine,whimore soluble, han xanthine. The initial dose of allopuri10-20 mg/kgl24hr in children and is adjusted ro mainormal unc acid evels n plasma.Occasionalln anthinecmay form. Consequently, low-purine diet (one free of omeats,dried beans,and sardines), igh llurd intake,and alkrzahonof the urine ro establish urinary pH of 6.0-6.5 rses.ar).Thesemea'urt's onrrol rhe hypiruricemia nd neuropathybut do not affect he neurologicsymptoms- h
no known treatmenr or the neurologiccomplications.
ADENYT0SUCCINATEYASEADSt)DEFICIENCY.his s an iired deficiency f de novo purine synthesisn humans.Adesucclnaseyase s an enzyme hat catalyzes wo pathwaysrovo synthesis ndpurinenucleotide ecycling. hese re heversion of succinvlaminoimidazolecarboxamide rib(SAICAR) rnto aminormidazole arboxamrde botide (AICin the de novo synthesis f purine nucleotides, nd the cosion of adenylosuccinareS-AMP) nro adenosinemonophare (AMP); the latter is the 2nd step in the conversiinosinemonophosphatellvlP)rnto AMP in the purinenuclecycle.ADSLdeEciencyesults n rhe accumulationn urine,
brospinal luid, and, ro a smaller extent, n plasma,of SAribosideSAICAT) nd succrnyladenosineS-Ado), ephoslated derivatives f SAICAR and S-AMP, espectivel)'. enThrs is an autosomal recessive isorder; the gene hasmapped o chromosome2q13.1-q13.2nd =20genemutahavebeen dentified. aboratory nvestigationshor,r,.he prein urine and cerebrospinalluid of succinylpurines, hicharemally undetectable.
Clinical manifestarionsncludevarying degrees f psychror retardation, generallyaccompaniedby a seizure disand/or aulistic ike behaviors poor eye contacr and repebehaviors).Neonaral seizuresand a severe nfantile eoiencephalopathyreoften he lsLmanifestarionsf thi. disOthers demonstratemoderate o severe ntellectual drsa50metimess.ociared irh growth erardarionnd mu,ele
ronia.One reportedcase, girl, tested n rhe mild rangeof ilectual disability.The form with prolound inrellectualdisahasbeendesignatedype , the variant casewirh mild intelledisabrliryas ype II. Other patientshavean intermediate lisymptompattern with moderatelydelayedpsychomotordopment,seizures, tereorypies,nd agiration,Pathology:CTMRI of the brain may show hypocrophyor hypoplasiaocerebellum, articularly hevermis, t is proposed hat rarherbeingcausedby purine nucleotidedeficiency,he symptomdue co the neurotoxic effectsof accumulating uccinylpurThe ratio of S-Ado/SAICAT asbeen inked ro phenotypeity suggestinghat SAICATs the more toxic compoundandS-Ado might be neuroprorective, he laboratory diagnobased n the presencen urine and cerebrospinalluid of SA

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 142/177
and S-Ado; both are usually undetectable. No successtul tfeat-
ment has beendemonstrared for this disorder Prenatal diagnosis
has been reporced, Systematic screening lvrth the Brarcon-Mar-
shall test isiuggested in infancsan d children with unexplarned
psychomotor retardation and/or seizure disorders
5-AMlt{0-4-lMl0Az0tf ARB0xAMIDEAICA) IB0SIDEEFICIENCY
by chebifunctionalenzymeAICAR transformylase/llvlPycLohv-
diolase (ATIC). The transformylases deficienr n fibroblasts n
this disorder.Genetics: hts is an inborn error of purine biosyn-
thesis aused y amurationof ATIC geneeffectingAICAR trans-
form'la'eactrvitl. n a reported ase, ICAR ran'formyla'e aspro found lye6c ienr ,herea .he MP cyc lohydro laseeve l a t
407" of no.-"I. Clinical features:The disorder s describedn a
der No successfulreatment s described.
OISOROERSESUTTINGROMBiIORMATITIESNPURIiIEATAEOTISM
MYOADENYTATE EAMII{ASEOEFICIENCYMUSCtE AOENOSINE
MOItI0PH0SPHATEEAMlf{ASED€FlClEf{GY). yoadenvlare deam-
inase rs a muscle-specific isoenzyme of AMP deaminase that is
active in skeletal muscle. Dunng exercise! lhe deamination of
AMP leads to increased levels of IMP and ammonia in propor-
ical manifestarions are, most commonly, isolated muscle
weakness, fatrgue, m,valgrasafter moderate to-vtgorous exerclse'
or cramps.Myalgias may be assocrared it h an increased erum
creatinekinase evel and derecrabLelecrromyelographic bnor-
tion durrns muscle contraction. lt is unclear how individuals mal'
carry the Jencit and be asymptomatic. n addit ion to muscledys-
function, a mutation of liver AMP deaminasehas been proposed
as a cause of pflmarv gout, leading to overproductron of uric acid.
The inherited form of rhe disorder is an autosomal recessrve
vart. AMP-DI, the gene responsible for encoding muscle AMP
deaminase, s located on the short arm of chromosome 1
(1p13 2l). Population rudres eveal that chis mutanc allele s
found at high frequenc in Caucasian popLrlations. The disorder
Chapter9r Disordersl Purinr ndPyrinidine etEbolis
mav be screenedor by performing he orearm schemic xtest.The normal elevationof venous lasmaammoniaaftercise hat s seen n normalsubjectss absent n AMP deam
deliciency. he 6nal diagnosrss made by histochemicalchemrcal ssays f a musclebiops,v. he primary fotm is dguishedby the linding of enzyme evels<2% $,'ith ittle immunoprecipirable nzyme.Affe ed individualsare adviexercisewith caution to prevenr habdomyolysts nd mybinuria-Although rhereare no documelted ully effectivements, ir has been proposed thac enhancing the ra
replenishment f the ATP pool might be beneficial.Usinrationale, reatmentwirh ribose(2-60 gl24 hr orall,v,n d
doses) r xylirol, whrch s converred o nbose,has been epto improve endurance nd musclestrength n somecasesineffecciven others, Geneticapproachesma-vbe leasiblefuture for inherited cases,whereas reatmentof the Lrndcondition s essentialn secondatvascs.
A0EN0SINEEAMINASEEFICIENCYeeChapter 25.1
PURllttEUCtEoSIDEH0SPHoRYIASEEFICIENCYeeCht25 2.
XANTHII{EOXIDOREDUCTASEEFICIEiICY EREOITARYANUBIAAI0tYBDEt{UM 0FACTOBEFICIENCYanthine oxductase XOR) is the catalyLc enzyme n che rnal step purrnecatabolicpathwayand oxideshypoxanthine o xaandxanthrne o uric acid.Because OR exisrs n rwo formsthine dehydrogenase nd xanthine oxidase, the deficiealso referred to as xanchine debydrogenase/xanrhrne(XDHD(O) deficiency. anthrne, he rmmediate recursoroacid, rs esssoluble han uric acid n urine and de6ciencyenzymeresults rn xanthinuria. Xanrhine oxidoreductascienc-vmay occur n ao isolated orm {xanrhinuria ype l)combined orm involvingxanthineoxidoreductase eficienaldehydeoxidasedeficiency xanthinuria rype Il), or in a
bined orm with deficrency f xanthineoxidoreduccase,ldoxidase,and sulfite oxidase(molybdenumcofacror defrcThe isolated orm resul ts n an alrnost otal reDlacemenac idbv h lpoxanrh inend anth rne .a t ien rs anox id izurinol ro oxypr:rinalvia aldehyde xidase.Parientswith thlared orm are usuallyasymptomaricr havemild symhowe,.er,enal stones, ften nor visibleon radiography, refor renaldamage nd may appear t any age.Crystallinthine deposrtsn musclemay resut in musc le ain ollowingtion. Rarely,xanthine sloneshar.ebeen eported as a reallopurinol administrarion.n rype I, the clinicalpresentsimilar to rype . Type l patienrsare deficient n borh oxand cannot metabolizeallopurinol. Molybdenum cofactociency failure o s)'nthesizehe molybdenumcofacror) nall three molybdoenzymes nd, like isolatedsr.rlfite xidas
ciency, esults n neonatal eediogproblems,
neonatalseincreased r decreased uscle one,ocular ensdislocationintellecrualisabilicy,nd death n earlychildhood.
The inherirance f types and II is autosomal ecesshumanXOR gene s ocatedon chromosome p22. n bothof the deEciency,he diagnosiss madeby measuring lasmcenrrations f uric acid;plasmauric acid s lorv (<1 rng/dxanthine s elevatedn plasma nd urine.Urinary uric areduced, being replacedbv xanthrne and hypoxanthimoLybdenum ofacrordeliciency, here s, rn addrtion,ansive excretionof sulfiteand other sulfur-containingmetabEnzyme iagnostic easuremen!equireseyunal r l iverbecause hese re the only human tissueshat containapble amountsof xanthineoxidoreducrase. ulfiteoxidasea

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 143/177
63{ r PARTX MelabolicDise8ses
mol,vbdenum cofactor can be measured in liver and libroblasrs.Although rhe isolated deficiency is generally benign! treatmentwith a low purine dret and increased fluid intake are recom-mended. Allopurinol has been recommended for chosewith residual xanthine oxidoreductase activiry It completell blocks theconversion of hypoxanthine into the far less soluble xanrhrne.The prognosis for molybdenum cofactor deficiency rs very poor,
DISORDERSFPYRIMIDINEETABOTISM
The pyrimidines afe the burlding blocks of DNA and RNA andinvolved n the formarion of coenz,vmes,as active inlermediaresin carbohydrareand phospholipid metabolism,glucuronidationin decoxification processes, and glycocylation of proreins andlipids. Pvrimidine synrhesis drffers from thac of purines in thatthe single pynmrdine ring is 1st assembled and then linked toribose phosphate to form uridine 5rmonophosphate (UN{P), Thepyrimrdines uracil and thymine are degraded in four steps, asshown in Figure 89-3. Eight disorders of pyrimidine metabolismare revrewed-Purine metabolsm has an easily measurableen dpomt in uric
acid;however,
there is no equrvalen! compound inpvrimidine metabolism. The 1st defect, heredrtary orotic aciduria,is in the de novo synthetic pathwal whereas the other disordersinvolve overacrivitl' (in one syndrome) or defec ts in rhe pvriml-
dine degradation pathway. Degradation disorders may presenrasanemra, neurologic disorders, or rnultisystem mitochondrial drs-orders. The 1st three steps of the degradacion parhways forthymine and uracil make use of the same enzymes (DPD, DPH,and UP). These three steps result in the corversion inco p alaninefrom uracil. There rs ncreasing evidence chatpyrimidrnes play animportant role in the regulation of the nervous system. Reducedproduction of the neurottansmitter function of p-alanine ishypothesized to produce clinical symptoms. Clinicalll., theserare disorders may be overlooked because symptoms are norhrghly specrfic; however, chey should be considered as possiblecauses
of anemia and neurologic diseaseand are a conrraindica-tion for treatment of cancer patients with certain pyrimidine
analogs.
HEBEDITARYROTIC CIDURIAURIOII\IE ONOPHOSPHATEYN .THASETYPE1 DEFIGIENCY).hrs is a disorder of pyrimidine syn-thesis assocrated v,ith deficient acrivity of the last two enzymesof the de novo pyrimidine synrhetic pathway, ororare phosphor!bosyluansferase (OPRT) and orotidine--5!monophosphate decar-boxylase (ODC). The ac tivities of rhese two enzvmes reside rnseparate domains to a single polypepride coded by a single gene.This bifuncrional protein, r.rridine5'-monophosphate (UMP) syn-lhase, catalyzes the two step conversion of orocrc acid co UMP,via orotidine monophosphate (OMP). Hereditary
orotic acidunaresults in the excessiveaccumulation of orotic acid. Genetics: Thisdisorder is autosomal recessive. Two functional domains areencoded on a single gene. The gene for UMP synthase s locatedon the long arm of chromosome 3 (3q13). Genecic metabolicdefects that nvolve four of rhe six enzymes associared with theurea cycle mav result in orotic acrduria secondary ro PP-ribose-Pdepletion resulring from a substantial increased lux rhrough thede novo pathwal', Clinically, patients with hereditary oroticaciduria (UMP synthas€ type 1 defciency) have a macrocytichypochromic megablastic anemia lhat ls unresponsive to theusual forms ol rherapy (iron, folic acid, and B1r) and may haveleukopenia. Onset is usually rn the 1st months of life. Untreated,
rhis disorder can lead to developmencaldrsabilirl', intellectual dability, failure to chrive, cardiac disease,strabismus, crysrallurand occasional urereric obstruction. Renal unction is eeneranormal. Heterozygolesmar' havemild orotr aciduriabuf ar. n
pharmacologic agents (5-azauridine,allopurinol) produce sondary ororic aciduria and orotidrnuria by specilically inhibiciODC. Orotic aciduria rnay also occur in association with penteral nutritionr essenrial amino acid deficrency, and R e sy
drome, The enz\mat rc de fe . t m ay be dem ons t ra red l r "lvmphoblasrs, erythrocytes, leukoc,r'tes,and cultured skin fibrolasts. A carrier detection test is available, as s prenaral diagn' is. ln OD( deficiencl rUVP synrhase yp 2 deficiencyl, clinical symptoms show neurologic abnormaliti u'ithout megloblastic anemia, In reported cases,both orotid una and oroaciduria were found.
impror.ement and reduction in orotic acid excrerion. Lifelot f ea rm en t\ requ i red . rac i l i s ne f f e r r i vee iause , n i kepu r inpy r im id ine a lvage ccu rs r rhe nuc leos ideu r id ine l . ve l . llong-cerm prognosis in uncomplicated cases is good; howev
DIHYDIOPYRIMIOII{EEHYDROGINASEDPD)DETICIENCYPcatalyzes the initial and rate-hmiting step in the degradationthe pyrimidine basesuracil and thiamine. DPD has been idenfied in most tissues, rvith the highest acrrvrty being in lymphq'tes. Genetics: DPD deficiency s an autosomal recessivedisordmapping to chromosome 1p22 wirh ac leasr 32 pol,vmorphismdetected. It is estimated tbat the frequency of the heterozygomay be as high as 3%. The clinical manifestations in childremay rncLudeseizure disorder, inrellectual disabilit_v.and motdelay. Lrs. frequenrar e grourh rerardation,microcephalv.autisrrc-like behavior and ocular anomalies. Others do noc shodevelopmental abnormalities but may have milder neurolog
symptoms and language disorder. In most cases, here is an initiperrod of normal psychornotor developmenr, followedsubsequent developmental delays. Sympcoms may be linkedaltered uracil, chymine, and p-alanine homeostasis. DPD is thinitial and rateimiting enzyme in the catabolism of the neoplatic drug S-fluorouracil (5 FU), being responsible for u07o of catabolism. Patients wrrh a partial deliciency of this enzymare at risk for developing a severe s-Fu-associared toxici adult paciencs,neurotoxlclty (headache.somnolence, visua lsions, and memory impairment) linked ro pyrimidinemia after FU treacmenr for cancer is reported in prevrously healtrndividuals.
Prenatal diagnosis has been reported. Laboratory findingDPD deficiency s characterized by a varrable phenocypeand dianosed by che accumulation of thramine and uracil in urinplasma,
and cerebrospinal fluid and no activit], in fibroblastDiagnostic tests use high-pressure liquid chromatograph(HPLC) or gas chromatography-mass spectroscopv (GC-MS
Alternarively, DPD defciency mav be conlirmed by measuring thenzyme in cultured fibroblasrs and leukoblasts. Uric acid levehave been reporred to be normal. BecauseB-alanine is a strutural analog of y amioobutl.ric acid (GABA) and glycine, it hbeen proposed rhat it na1' affect inhibirorl.neurotransmissionThere is no established treatment for this disorder: Datienrs rviseizures o rerpond to annconvulsanLmedirations. arienrs rrDPD deliciency should not be given 5-FU, and thrs deficienshould be suspected when neurologrc symptoms emerge aftcancer rreatment wlth 5-FU,

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 144/177
DIHYDBOPYBIMIDINASEDPH}DEFICIENCYDIHYDROPYRIMIDIN-
maDDedo chromosome q22 ln one studn therewas no signif-
icani differetrcen residualactivirv betweenmutationsobserved
in symptomaric nd asympromaticndividuals.Populationpreva-
lenie in a Japanese ample s 0.1% Clinical manifestationsnthree unrelatadaffectedcasesncludesetzures ith dysmorphrc
testswith uracil, dihydrouracil, thymine, and drhydrothymine
havebeenused o differentiacehis disorder rornDPD deliciency-
Io symptomatic casesi teatment with p-alanine has been
attemDt;d with equivocal results. Although ir has not been
reported, nc.eased ensitiviryo fluorouracil s expected ecause
of its role in pyrimidinemecabolism.
N-CABBAMYt-g-AMlN0AclDuRlA(DEHCIE -URElD0Pfio"
PIONASE).he pyrimrdinebases racil and aredegraded
via rhe consecutive ctionof threeenzym anineand p
aminoisobutyric acid, respectively. he chird enzyme in the
patiway is p-ureidopropionaseUP) and its deficiencyeads co
N carbamyl-p-amino ciduria.Urinary analysisn a reported ase
showedelevatedevels f N-carbamyl-p-alaninend N-carbamylp-aminoisoburyric cid,The enzymes expressednlf in the iver
andno activrtyof p-ureidopropionases derectedn a iver biopsy.
Genetics: luorescencen situ hybridization ocalized he human
treatment or UP deficiency.
URlDlt{E 0N0PH0SPHATEYDR0LASEDEFICIENCYPYRlMlDll' lE
5'-l{UCtE0TIDASEEFICIENCY).rythrocvte aturationsaccom-paniedby RNA degradation nd he release f mononucleotides,
PyrimidineSlnucleotidases tbe 1st degradative nzymeof the
pyrimidinesalvage ycleand catalyzeshe hydrolysisof pyrimi-
dine Srnucleotides o the correspondingnucleosides. nzymedeficiencv esults n the accumulationof high levelsof cytidine
and urid'inenucleotides n the erythroc;tes of those affected,
which results, n turn, in hemolysis.Defi encyof pyrimidine 5:
nucleotidases atleast n par! compensate n vivo by othernucle-
osidasesor perhaps other nucleotide metabohc pathways.
Genetics: his s an aurosomalecessiveisorder nvolvrnga gene
Chapter 9 r Disorders f Plrin. .nd PyrinidineMetoboliEm
pvrimidine S'-nucleocidase and assessmentof lead levels sh
te included whenever rhe hemolltic anemia, p,vrirnidrne
nucleotidase deficiencn and basophilic strpplng are fo
rogerher. Diagnosrs requires demonstration of a complete
ciencv of the major isoenzymeuridrne monophosphate hydrol
1. The enzyme defect should be suspected in parients w
nonspherocytic hemolytic anemia with basophilic stipplng
anemia is usually moderate, and transfusions are rarely neces
There is no specific treatment. Splenecromv has not prove
be an effective treatment. Lead-induced acquired pyrimid
S'-nucleotidase delicienc;; is treatable, unlikeche conge
deficiency.
PYflMTDINE{UCTEOSIDEEPTETIONNDOVERACTIVEYTO5,-NUCLE0TIDASE.yrimidineucleosideepletion ndover
tion in the activiry of pyrimidine S'-nucleoridase in fibrobl
with both purine and yrimidine substrates. nvestigarion in
tured fibroblasts der ed from these patients showed no
incorporation of purine bases into nucleorides but decre
incorDoration of uridine and orotrc acid. Clinical manifestat
include developmenLal elay. serzures. taxia. recurrent in
tions, severe anguage deficit, hyperactivity! short atcention sand agg ssive behavior appearing in the 1st feu' yr of
Affected atients show electroencephalogram (EEG) abnorm
ties. Metabolic testing is normal except for persisrent hypour
suria. It is proposed that increased catabolic activiry
decreased pyrimrdrne salvage cause a deficiency of pyrimid
nucleotides. Treatment is with oral uridine, based on its ef
on reversing rncreased nucleotide catabolism. AII repo
patients rreated wich uridrne show improved speech and be
ior. decreased seizure activitv with disconrinuation of se
medications, and decreased requeocy of infections.
THYMIDtNEPH0SPHORYLASECFICIENCY hymidine phosph
lase catalyzes the conversion of thymidine to thymine.enzyme is also known as platelet-derived endothelial cell gro
factor due to its angiogenic or "gliostatin" properties, indica
its inhibitory effects on glial cel l proliferarion. Ic has been im
cated in mitochondlal nucleoside metabolism. Plasma thvmi
level is increased>20-fold in paciencs ompared to controls.
of funcnon of thymidine phosphorylase causes mirochond
neurogastrointestinal encephalomyopathy (MNGIE), an au
mal recessive disorder rvith mitochondrial DNA alterat
Geoeticsr It rs an aulosomal recessive disorder, and che
encoding thymidine phosphorylase has been identified as
MNGIE gene and mapped to chromosome 22q13,32-
Clinical manifestations of MNGIE rnclude prosis, progre
external ophthalmoparesis, gastrointestrnal dysmotility
malabsorption, cachexia, peripheral neuropathv, skeletal m
myoparhy, and leukoencephalopathy.Laboratory find
Muscle biopsies typically reveal mitochondrial abnormal
The diagnosis is made by assayof thvmidine phosphorylase a
ity in penpheral ler-lkocytes.ncreased hymidine may causem
chondrial nucleotide pool imbalance resulting in mitochon
DNA alterations through a mitochondria-specific rhym
salvage pathu'ay. Supportive treament is indicated.
THYMIDINE INASE (IK2)DEFICIENGYhymidrnekinase2 (
is a key enzyme rn micochondrial DNA (mtDNA) precursor
rhesis. TK deficienciescause tissue-specif icdepletion oi mcD

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 145/177
636 PARTX.Metaboliciseas6s
TK2 normally phosphorylates eoxlthymidine, deoxycytidine,and deoxyundine.Genetics: he gene s locatedon chromosome16q22- Clinically, in TK2 delicienry,affected ndividuals haveseveremyopathyand depletionof muscularmitochondrialDNAin infancy.No specific reatment s available,Supportive reat-ment is indicated.
Augoustid€s-SavvopoulouP, Papachrisrou 4 Farrbanks LD, er al: Parrial
hypoxanthineguanine phosphoribosyluansferase efciency as the unsus,peded causeof rena) disease pannrng hreegenerations:A cauhonary tale.
Pediafiics 2O02ilO9E17
Caneron J5, Moro R SimmondsHA: Gour, uric acid and purine metabolisrD
in paediarric nephrology,Pediatr Nepbrcl 1993;7 '105-118.
Cameron JS, Simmonds HA, Hereditary hyperuricemia and r€nal dis€ase.Setnin Nefihrol 200525:9-78.
Dabrowski E. SmathersSA. Ralstrom CS. et al: Botulinum toxin as a novel
rreatment for self-mutilation in Lesch-Nyman Syndrome.Det Med ChildN eutol 2005 47 636-639.
Jinnah HA, De Gregorio L, Harrrs JC, et al: The spectrumof inherited muta-
tions causing HPRT deficiency: 7i new casesand a review of 195 prevr
ously reported cases.Mutat Res 2000t463:309-326.
Loffler M, Fairbanks LD, Zameitat E, et al: Pyrimidine pathways in health
^nd diselse,Mol Med 2005t1,1,:430437.
Marinaki AM, EscuredoE, DuleyJA, ecaI Geneticbasrsof hemolytic anemia
cau*d by pyrimidine 5'nucleorjdasedefrciencr lood 2O01;97:3327-3332.
Nrshino I, SpinszzolaA, Hirano M: MNGIE: From nuclear DNA to mito-
chondrial DNA. Nearorfluscul Disotd 2001l'1117-10.
Nyhan Ii/L: Disorders of purin€ and pyrimidine metabolisn. Mol GenetMetab 2O05;86:2s-33.
Nyhan Vl, Vuong LU, Broock R: Prenataldiagnosisof Lesch'Nyhandisease.
P etrdtDiag" 2003,23 1807809.
RaceV, Marie S, Vincent MB et al: Clinical, biochemicaland moleculargeneric
correlations in adenylosuccinate lvase deficiency. Hum Mol Cenet
20O0;9:2159-2165.
SchredenDJ, Harris JC, Park K, er al: Neurocognitive furctioning in Lesch-
Nyhan disease nd partial hypoxanrhrne-guanine hosphoribosyltransferase
deiciency. I Int Neu/opsychol Soc 2001i7:8O5-812.
SchretlenDJ, Vard J, M€yer SN{, er al: Behavjoral aspectsof ksch-Nyhan
disease nd its varianrs. DeLj Med Child Newol 2O05t47:673-677.
Scriver CR, BeandetAL, Sly WS, et al ledsl The Metdholic ad Molecular
Bask of Inbe ted Diseasa Vol. 2, 8th ed. Nell York, Mccraw-Hill, 2001,
pp 2513J7O2.Sinmonds HA, Duley JA, Fairbanks LD, et al: When to inv€stigareor purine
and pyrimidine disorders: nrroduction and review of cLinicaland labora'
rcty ,ndlc tions. I lftherit Metab Dis 19972O:214-226.
van Gennip AH, van Kuilenburg AB: Defectsofpyrimidine degradarion,Clin-
ical, nolecular, and diagnostic aspeccs.Adz Ex.p Med Biol 2000t486:
233 241.
Wons DR Hafiis JC, Naidu S, et al: Dopamine transponers are markedly
reduced n l*sch-Nyhan diseasen vivo. Pror Natl Acad SciU S A 1996193:
5539-5543.
Progeria'smost striking eature esembles ccelerated ging,Thisrare syndrome,also referred o as the Hutchinson-Gilfordprog-eria syndrome (HGPS), has an incidence of -118,000,000.
Affected children do not become exuallymature or reDroduceasa result f \fvere aiJureo rhrive; arenr-ro-childransmissionhas not beenobserved. he clinical diagnosis f HGPS s basedon recognition f commonclinical eatures ndexclusion f other
syndromeshat haveoverlapping eatures.Mutations in IMNthe geneencoding amin A-/C,are the only mutationsknowbe associatedwith HGPS. Approximately 90% of individwith HGPS havehad an identifable MN/ mutation,
C NICAI MANIFESTATIONS.hildren with progeria usuappearnormal in early nfancy,but manifestarionsuch asmfacial cyanosis, sculptednose,"and "sclerodema"mav sugthe exist€nce f the syndromeat bi rth. Profound growrh {a
occurs n the 1styr of life. Thecharacterisricacies, lopeciaof subcutaneousat, abnormal posture, stiffnessof joints,bone andskin changes sually become pparenr n the 2nd ylife (Fig,90-1). Moror and mental developments normal.dominant clinrcal manifestations ncludeshort stature; wedistinctly ow for heighr;diminishedsubculaneousar; headproportionately arge for face; micrognathia; prominenr sveins;generalized lopecia;prominent eyes;delayedand abmal deDtition; pyriform thorax; short, dystrophic clavi"horse-riding"stance;wide-based hufflinggait;coxa valga,limbs,and prominent,stiff joints;and failure to complece ematuration.
Featuresrequentlypresenr reskin hat is thin, taut, dry,wkled, and brown-spotredn various areas;sclerodermatousover the lower abdomen,proximal thighs,and buttocks;pro
nerrtsuperficial eins; ossof eyebrows ndeyelashes;ersistpatent anterior fonranel; sculpted, beaked nasal tip; fnasolabialcyanosis; hin lips; protruding ears; absence flobules; hin, high-pirched oice;dystrophicnails; and progsive radiolucencyof the rerminalphalanges nd distal clav(acro-osteolysis).ifferentialdiagnosisncludesmandibularadysplasia,Cockayne syndromerHallermann-Streiffsyndroand neonatalprogeroidsyndrome \(riedemann-RautenstrWernersyndromes anotherdisease f premarureagingduedominantly o murations n the DNA helicase ene Table90
Figure 90-1. A 4.5yr old Bnl with height of 1.75yr and bone age of(From Wilkins L: Diaposrs and Treatmmt of Endocine Disordets in Chood and Adolescetce,3rd ed. Springfield, L, CharlesC Thomas, 1965

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 146/177
FIIIURE
Mll',|unberGuratraeftis)60netks0rset|lairg0yingiidtIl055
tlin hinniru
Sub(utaneou55tueos5SkiI iklfrcationAnkleheritioHA,:*eralostsOtaracls5honsraturc(0)GYalgd
2771tnr/RN,UfiAAu [Re!5|veYoungduhhood+Maleaftem+
++++++
11fr70
SpoEdir,utosooalomindnl(hibhod
+ToEl+
-
++
WmltnsnDmfllt HUTCHItI$lt{ltFoBDSYl{)mMt
Chaplerl i ThePorphyrias
muscular dyscrophy1B, Charcot-Marie-Toothiseasemandibuloacraldysplasia,and atypical Werner svndromeTable90 1).
PR0GN0SIS.hildrenwith progeria suallv av ese"ere thsclerosis,nddeath ccurs sa result f complicationsf caror cerebrovascular isease, enerallybet*'eenage 5 and 20wirb a medranif e spanof =13yr Cataracls nd tumorshinfrequenclv been noted, but many changes associated
normal aging n adults, uchas presbycusis,resbyopia,senils, osteoarthricis, enilepersonalitychanges, r Alzhedisease,reno t found,
TREATMENI o specific reatment or thisconditronexists.This a progena foundarion (u.wrv.progeriaresearch.org),hmainrains ProgeriaRegisrry o help with diagnosis nd o dernoreclearlv he incidence nd molecularbasrs f chedisord
Bro$'n VT, Gordon LB, Collis l-S: Hutch,nson-G,lford progeriasyndron
a;cnc Rev,ewsat Ccnc Tesrs:N.ledlcalCenerics nformarion Rescurce
baseonlinel AvallabLe c hrrp://r'w$'senerestsors/(updaredAnsust 20
CapeUBC, Erdos VR, Madigan ll', er al: lnbrbinng farn€sylationof proprerents he characteristicnuclear blebbing of HLLrchinsonGilford pro
syndrone ProzNari Acad S./ U S A 200i ;102:12879 12884
Chen I, t-ee ., KudLow A, et al, lMr\H mutarions n atypical Werner\
drome. I-!,r.el 2003j-163r44(H45.
Eriksson.1v1, rol.n V! Cordon LB. ct al: Rccurrenr de novo point m
lions in lamin A cause Hurchnrson Cilford progeria syndrome. N
2001;423,293-298.
Hegele RA: DrawjnB rhe l ine rn progena svndromcs Larcer 2003
416417.
Porphyrias are metabolic diseases esufting from deficienciespecific enzymes of the heme biosynchetic pathu.a-r T
elzymes are most active n bone marrou'and [ver. !?hen tdiseasesare manifesr, accumularion of 1 or more intermedi
occurs nit ially in I ofthese t issues. r,vthropoietic orphyria
rvhich overproduction of heme path*ay intermediates occursmarily in bone marrorv erythroid cells, usually present at birt
in early childhood u.ith cutaneous photosensitiviry, or in the
of congeniraler\throporetic porphyria. even in utero a\ nu
mune h,vdrops..Nlost orphyrias are hepatic, with overpro
cion aod init ial accumulatiorr of porphyrin precursor
porphvrins occurring 1st n the liver.Regulacor,v echanism
heme biosvnthesis n liver are drstinct from those in che bmarrow and appear !o account lor activation of hepaticph,vriasduring aduLt li ie rather than childhood. Homozyforms of che hepatic porph,vrias may manifest clinically priopubertl and asymptomatic heteroz-vgouschildren rnay preu'ith nonspecilic and unrelated symptoms. Parents often reqadvice about Long-term rognosisand intormation abou! m
ll4andibularypoplasia - +
,{heDsderc5i5 + +
osteopeoia/o(mporcsis + +
L!rySedtopi'yiShwa) + +
Ilymi( rcphy + -
D lbrdbleItpogonadhm + +Grcersur(ep'btt) + -
MlM,MendelianderitancnMro+,pnltinj-,absnli,lodiftedtDir1egekA:'rwirqleinenpng€iiy oms on r 001J62r416*417
LAB0RAT0RY INDINGS.hriable degreesof insulin resistance
ioccasionallv,nsulin dependenr iabetesmellirus),abnormalines
ar e no demonstrable bnormaliries f chyroid,parathyroid,pitu-
itar-v, r adrcnal tunccron.
M0IECULABPAIH0GEi{ES|S. he nuclear lamrna, a procein-
containing layer arcached o the inner nuclear membtane, is com-
by alternative spl ing of rhe LMNA gene transcript. SeParale
genes ncode ami Bl and 82. Lamin A is normally svnthesized
as a precursormo cuJe prelaminA). Alternativesplicingwichrn
exon l0 givesrise to tu'o different mRNAs that code for prelamin
A and lamin C. PrelaminA, rvith 564 amino acids,ha s 98 uniqLre
carboxy-termrnal mino acids.Lamin C has six uniquecarboxv
termrnaLamino cids.Because relamin A containsa CAAX (cvs-
teine-alipharic lipharic-anv amino acid) box ar its carboxyl
terminus, r is modilied by farnesylation,whereas amin C is noc.
After farnesylation, cleavage of the last three amino acids, and
methvlahon of che C-terminus,an internal proteolytic cleavage
occurs, removing the last 15 coding amino acids, to Senerate
mature lamrn A with 646 amino acids. The most common HGPSmutation is a G608G (GGC > GGT) muration in exon 11. This
mutalion results n an activation of a crvptic splice site within
exon 11, result ing n production of a rranscript hat deletes50
amino acids near the C-terminus.The HGPS G508G mucation
and consequent abnormal splicing produces a prelamin A
that relains the C,{AX box but is missing he site for endopro-
teolytic cleavage.This HGPS mLrtation acts as a dominant nega-
tlve mutatron.A grorving li sc of other diseases s associated with differenr
mutations in IMNA, which have come !o be knoE n as
laminoparhies. These nclude Emery Dreifuss muscular d,vstrophy
tvpe 2, familial dilated cardiomyopatbyand conduction s,vstem
defects, Dunnigan t,vpe amilial partial lipodysrrophy; limb girdle

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 147/177
638 PABTX MetabolicDiseases
agementoi thesedisordersand drugs rhat can be taken safely o
lrcat other common conditions.
The D\A sequences nd chromosomal locatxrns arc escablished for the hrLman genesof rhe enzvmes n this pathwan and:nult iple diseasc clated mutations have been iound fol eachporph,vna.Al l bu t 3 oi the inheritedporphyrias displav autosonraL dominant jnheritance.Although iniriaL diagnosis of por-ph,rria by biochemicalmerhods emainsesscntial, r is especrallyirrportanr in chilclrcnco conlirm the dragnosis ,vdemonsrracing
a speciEcgene lnu tation(s).
THE EME IOSYNTHETICATHWAY
Heme is required for a variery of hemoprotcins such as hemo-globin, m,voglobin, respiraror,v c_vtochromes, and c,vrochrome
P450 enzyrnes (CiYPs). k rs believed rhat the ll enzyrnes in thepathway for heme bursynthesis re acrive n all r issues.Hemo-globin s,r'nrhesisn erythroid precursor cells accounts for =85-nzo
r f . l ; i l y hcm r un rhc . r ' r rhuman. .Hepa to . r t c .a . co r r r r o r rnu r t
of the resr.primarily ior s,vnrhesisf CYls, u.hich are especially
abrndant in the liver endoplasmic criculLLrnER), and turn overnrore rapidly than many other hemoproteins,such as the mito-
chondnal respiratory cltochromes. As shorl,l in Figure 9l l,
pnth\.ay inrcrmediates re the porphvrin precursors i-aminole-
vulinic acid (l\Lr\, alsoknorvn as l-aminoler.uLiniccid)an d po rphobilinogen (l' ]BG),and porphyrins (mostly in rheir reduced
forras, knou'Lr as porphvnnogens).Ar least in humans, these
intermediates o not accumulale n signif icanramounts under
normal condit ions or have rnportant physiologic r.rnccions.
A deficierrcy oi each enzyme in rhe pathrvay, *'irh rhe excep-
tion of che1st, s associated -itha differentporphvria lTable 91 -
1). The 1sr enzyme,AI-A synthase AIAS), occurs n 2 fonns.
Al erythroid specilic form, f ermed ALAS2, is deficienr in X
linked sideroblastic nemia,due fo mutationsof rhe AI-A52 gene
ol chromosorneXp1l.2. The ubiquitorLs brm of rhis enzyme,
rermedALASI, is found in all r issuesnclnding iver,and ils gene
is locatcd on chromosomc3p21.1. Discasc elatedmutations of
AI,AS L have rot been described.
Regulation of heme svnthesisdiffers rn the 2 m:rlor heme-
tbrming t issucs I-ivcr henc biosynthesiss primary conrrolledbyALASl . S,vnchcsisf ALASl in liver s reg acedby a "free" heme
pool {seeFig. 91-li, rvhich can be augmenrcdb, vner;r' ly vnsized heme or bv exis ring hcme released rom hernoproreins destrned or brcakdown to biliverdjn by heme oxygenase.
In the cryrhron, no\el regulatory nrechanisrns allorv fbrproduction of drc ver,v argeamountsof hemeneedeclor heglobin synrhesis. he response o stimuli for hemoglobinsynsi soccursdLrring el ldifferenriation, eading o an increasel number- Also, unlikc th e liver, heme has a shmulatory rolehemoglobin ormation, and the stimularion of hemc s,vntheerythroid cells s accompaniedby incrcases ot onl,v ll ALA
but also b,v sequenrial induction of other hcme biosynthenzymes. Separate ertthroid specilic and noner;-throid
"housekeeping" ran\cripts are known ior the 1sc4 enzvmethe pathu'ay, The separarc iorms of ALAS are encoded by ge
on differentchrooosomcs, bur for eachof the othcr 3, erythrald nooervthroid trdnscrpt s are rranscribedb, valtcrnativep
moters n the samegene.Heme also regulates he rate of its srhesis n erythroid cellsbv controll ing thc transporr of iron iretrculocyles.
Intermediares of the heme biostntheric pathway are efficienconverced o hene irnd, Lrormally,otly small amounrs of inrermediates are excreted. Some may undergo chemical modcations bcfore excretion.Whereas he porphyril precursors
and I 'BG are colorless, nonfluorescenr,and largeL-v rcreunchanged n urine, PB(i ma1'degrade o colored producrs s
as rhe L)rolv11ishigrnent calLedporphobilit or spontaneopolymerize o ur<>porpb,vrLls.orphvrins are red in color a
displavbright red f luorescence hen cxposed o long wavelen
ulrravioler ight. l 'orphlnnogens, rvhich arc colorlessand tr
fluorescent, are the reducecl orrr of porpbyrins, and lr'hen t
accumulatc,ar c readily aucoxidized o the correspondingp
phyrins outside the cell. OnLl' the c1'pe II isomers of uropphynnogenand coproporphvrinogenare cor'rvertedo herneF ig .91 1 ) .
ALA and IrB(] are excreted n urinc- Excrcrion of porphvr
an d porphvrinogens n urinc or bile s determinedby the num
of carboxll groups. those rvirh many carboxvl groups. such
uroporphvrin (ocrac;rrboxllporphyrin) and heptacarboxylp
phyrin), are rvater soLuhle nd readiJ,v xcrctcd n urinc. Thrvith ferver carl.oxll grorrps. such as protoporphvrin (dicarbo
porphvrio), are not warcr solr.rble nd are excreted n bile afeces. Coproporph,vrin (terracarboxyl porphyrin) is excre
0t5EA5rABSfiEVrAflo
ij Am olevuliniidderyiraraie
ro.ph/ ADPI
AtuL.ntermrtteftr0[lri (AlP]
lomozyqowAlP(onqenitari'lhropoielirorphyrai:EP) Utapophynaqenll ynth,ta
iURtr'Porpi l r i .utaneidd ara )rt i re
Pl : iqpe:r
P(l ype
Hpprtocrythropor:porpilr (lraF)
Heft taryop,cporphl'rf1:P)
flo oryqo,r5][r
liri4dreorFhyriiVP)|]oloztqorsVo
Erythmpfti( rotcporpf!rir:PPl
|npuph[Lncq deatbatybte
iI]PCD)
aapnpatphwiaaet r)datc(lY))
l tq,attf tnnv Drtdlr (PPi)\
ferlthdons?ff[t1)
fiUIATloilSf IHls ZYmt PnEEilIATl0ll
Nomozygoue flosrlyostubary
fleteroryqour Po$pubertyllomo?ygous 0ildhood|]omo?yqoLrs lnuteroi nfan(y
None Adrllls
fleterozygoui AdiltsNooe Adrlr5flomoz|1tous [hildhoodfletemzygous PgtpubenyNcmo4llous (hiidhood
Hrleuyqoirs PoitpubeftyHomozygous th dhaodHopmlylousheteroalelkith th dhmd
ow xpresrionomalleh)ff n0rnoryg0ur
EITZYMIABBREVIATION)
dehjd tnte ALAD)
Pu hah ney n deo i nateP860
J(
XX
xx
I
I
xX
x
XXX
X
Xx x "XI XXX X
X
.AtP&d r1tPircoftdend r lai lFoar. rlphynas,bltbtait al:Il(frFs i dilho.itezi( prolopoahr5u9Fn nnihopoklromFrmnttp| : i5dUet0nhb(0noihepi | tUf00AUls0m; |donmdlmha| i imeolapar Iade[ ( iency0lU800isaplEdl

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 148/177
,frFr|lr T PotIMos
=
'tr
R
_!
E
I
*6

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 149/177
64ll PABTX ilerabolic iseases
partly in urine and pardy in bile. Because oproporphyrin ismore eadily€xcretedn bile than s coproporphyrrn II, impairedhepatobiliary unction may increaseotal coproporphyrinexcre-tion and the ratio of these somers.
CTASSIFICATION1'ID IAGNOSISFPOBPHYRIAS
Two classification chemes eflect either the underlyingpatho-physiologyor clinical eatures, nd both are useful or diagnosisand reatment see able91-1). n hepaticand erythropoietic or-phyrias, he sourceof excess roductionof porphyrin precursorsand porphynns s the iver and bonemarrow, respectively. cuteporphyriascauseneurologicsymptoms hat are associated ithincreasesf 1 or both of theporphyrin precursors LA and PBG.In the cutaneous orphyrias,photosensitivity esults rom trans-port of porphyrins n blood rorn he iver or bonemarrow to theskin. Dua[ porphyria refers o the very rare occurrence f defi-ciencies f 2 differenrhemepathway enzymes,
It is notable hat acute ntermittentporphyria (AIP),porphyriacutanea arda (PCT), and erythropoieticprotoporphyria (EPP),the 3 mostcommonporphyrias,are very different n clinicalpre-se[tation, precipitating actors,methodsof diagnosis, nd effec-tive therapy (Table91-2). EPP s probably rhe porphyria rhatmost commonlybecomesmanifesc eforepubercy. wo of the 4acuteporphyrias, hereditarycoproporphyria (HCP) and varie-gateporphyria(VP),can alsocauseesionsndistinguishableromPCT (see able91-1).Congenital rythropoietic orphyria (CEP)causesmore severe listering esions, ften with secondarynfec-tion andmutilation. EPP s distinct rom the other cutaneous or-
phvrias n causingnonblirrering hotosensiti\ 'rtyha t occursacutetyatter sunexposure.
FISSI-I-INEAB0BAT0SYDlAGilO$lC TESTING. few sensitiveand soecific irstline laboratorv esn should be reled on when-ever symptomsor signssuggest he diagnosis f porphyna. f afrrst-lineor screeningest is significantlyabnormal, more com-prehensive estingshould follovv to establish he type of porphyria, Overuseof laboratory tests for screening an lead tounnecessaryxpense nd evendelay n diagnosis.n patientswhopresentwith a past diagnosisof porphyria, laboratory reportsthat were the basis or the original diagnosismust be reviewed,and if thesewere nadequate,urther testingconsidered.
Acute porphyria should be suspectedn patientswith neuro-visceralsymptomssuch as abdominalpain after puberty,wheninitial clinical evalualiondoes not suggestanother cause,anduritaty porphytix ptec&rcors ALA and PBG.)should be mea-sured, Urinary PBG is virtually always rncreased uring acuteartacksof AIP, HCP, and VP, and is not substantially ncreasedin any other medicalconditions.Therefore, his measurementsboth sensrtive nd specilic.A method or rapid, in-housecestingfor urinary PBG,suchas he TracePBGkit (TraceAmerica/TraceDragnoscics,ouisville,CO), should be available n houseat allmalor medical facilities. Results rom spot (singlevoid) urinespecimensare highly informative because very substantialincreases re expected uring acuteattacksof porphvria.A 24 hrcolleccion an unnecessarilyelaydiagnosis, he samespot urinespecimen hould besaved or quantirative etermination f ALAand PBG, n order coconfirm hequalitativePBG esult,and also
detect patientswith ALA dehydratase orphyria. Urinary pophyrins may remain ncreasedonger han porphvrin preculsin HCP and VP. Therefore, t is useful o measureotal urinaporphyrins n thesame ample, eeping n mind rhat urinarypophyrin increases re often nonspecific,Measurement f urinaporphyrinsalone should be avoided or screening, ecauseheareoften ncreasedn many disorders ther han porphyrias, uaschronic iver disease, nd misdiagnosesf porphyriacan resfrom minimal increasesn urinaryporphyrins hat haveno dianostlcslgnlncance.
PBG is a colorlesspyrrole rhat forms a violet pigment wiEhrlich reagent (p-dimethylamrnobenzaldehyde).ther sustances, rincipally urobilinogen, also react with Ehrlich aldhyde, The Vacson Schwartzand Hoesch ests,which involvrnitial addition of Ehrlich reagent o urine, are considered bslere. A reliable quantitative method for both ALA and PBwhich uses mall amon and cationexchange olumns o separinterfering substances efore adding Ehrlich reagent,has beavailable or manyyears.ALA ls reacted o form ap1'rrole,whris thenalsomeasured sing Ehrlich reagent.The TracePBG kis based n this method.
Measurement of erythrocyte porphobilinogen deamina(PBGD) s not usefulasa firstline test n rhe acutesettingbecauir does not differentiate atent from acriveAIR Moreover, henzymeactivity is not decreasedn all AIP patientsand is nev
deficient n other acuteporphyrias.BlisteringCutsneous orphyrias, listeringskin lesionsdue
porphyna are virtually alwavsaccompanied y increasesn totplasmapotphyrins. A fluorometricmethod s preferred,becauthe porphyrins n plasma n VP are mostly covalendy inked plasma proreins and may be less readily derectedby higpressure iquid chromatography HPLC),The normal range oplasmaporphyrins s somewhat ncreasedn Fatientswith enstase enaldisease,
lionhlistering utaneousorphyria.hhough a total plasmapophyrin determinacion ill usuallydetectEPI an erythrocyte rtoporphyrin determination is more sensirive. ncreaseserythrocyte protoporphyrin occur in many other conditionTherefore, he diagnosis f EPPmust be conflrmedby showingpredominant ncrease n free protoporphyrin rarher than zin
protoporphyrin. nterpretationof laboratory repons can be d6cult, becausehe term "freeerlthrocyteprotoporphyrin" somtimes actually epresents inc protoporphyrin.
SEC0ND-I|I{E ESTlilG,More extensive esting is v .ell justifiwhen a firstline test rs positive.A substantial ncreasen PBmay be due to AIB HCP, or VP. Theseacuteporphyriascan bdistinguishedby measuring erythrocyte PBGD, urinary pophyrins using he same pot urine sample), ecalporphyrins,anplasmaporphyrins,The variousporphyrias hat causeblisteriskin lesionsare differentiated y measuring orphyrins n urinfeces,and plasma.Confirmationat the DNA level s importaonce he dragnosiss established y biochemical esring.Furthdetails are provided n the follou'ing sectionson each type porphyfia.
TESTINGOB UBCLlillGAt0flPHYBIA.t r sofien diffrcult o dianose or "rule out" porphyria in patients who had sugges

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 150/177
to euid rhe choiceof tests or rhe family members.The index
casi or nother arnilymemberwith conlirmedporphyriashould
be retestedf necessary.dentilicationof a disease-causinguta-
tion rn an index casegreatly facilitatesdetecrionof additional
Sene arrlers.
6-AMINOTEVUTINICCIDDEHYOBATASEPOBPHYRIAADPI
This s the most ecendydescribed umanporphyriaand s some-
times ermedDossporphylio aket th,envestigator ho described
the 1st 2 cases.fhe
tern pluttboporpDyriaemphasizeshe sim-
ilarity of this conditionto leadpoisoning,but rncorrectlymplies
that it is dr-reo lead exposure.
PATH0t0GY NDPATH0GENESIS.LAD catalyzeshe condensa-
tion of two molecules f ALA to form the pyrrole PBG(seeFig.
91-1).The enzymes subject o rnhibitionby a numberof exoge-
nous and endogenous hemicals.ALAD is rhe pnncipal lead-
binding protein m erl/throcytes, nd lead can displace he zinc
atomsof the enzyme.ErythrocyteALAD acrivity s alsoa sensi-
rive ndex of lead exposure,A1lADP casesnheriteda differentALAD mutatron rom each
parent.ElevenALAD mutations,mostl point mutations,hav€
beeo dentified,someexpressing arrial ctivirv,such hat heme
synthesiss partially preserved. he amount of residualenzyme
activity may predict the phenorypic severicyof this disease.Immunochemical tudies n 3 cases emonstracedonfunctional
enzymeprorein that cross reactedwith anti-ALAD antibodies.
Late-onset asesassociatedwith a myeloproliferativedrsolder
may be heterozygous r have a somaticmutatron, with expan
sion of an affected lone of erythroidcellsADP is often classified sa hepaticporphyria,although he sice
of overproductionof ALA is not established. patient with
severe, early-onset diseaseunderwent liver transplantation,
rvirhout significantclinical or biochemical mprovement,whrch
might suggesthat the excessnrermediates id not originate n
the liver Excess rinary coproporphyrin II in ADP might origi-
nate ro mmetabolismfALA to porphyrinr.:gensn a tissue ther
rhan the site of ALA overproduction Adminisrration of large
doses f ALA to normalsubjecrslso eadso substantialopro-
porphyrinuria.ncreasedryrhrocyteroloporphyrinma), as ni ll orherhomozygousorphyrias, eexplained y accumularion
of earlierpathway ntermediatesn bonemarrow erythroidcells
duringhemoglobin ynrhesis,ollowed by their transformation oprotoporphyrin after hemoglobinsynthests s complete.As in
other acuteporphyrias, hepathogenesisf the neurologicsymp-
toms s poorly understood see eccion n AIP).
CtlNlCAt MANIFESTATI0NS.n most cases, ymptoms esemble
otheracuteporphyrias, ncludingacuteartacks f abdominalpain
and neuropathy. Precipitating facrors, such as exposure to
harmful drugs,havenot beenevident n most cases. our of the
6 reportedcaseswere adolescentmales.A Swedish nfant had
more severe isease, rth neurologic mpairment and fai lure ro
Chtptergl ThaPo4lryrias 6
rhrive. A 63 yr old man in Belgiumdevelopedan acute motpolyneuropathy oncurrenrlywith a myeloproliferative rsord
tAB0BAT0RY INDINGS. rinary ALA, coproporphyrin lI, aer],throcyte zinc procoporphyrin are substantially increas
Urinary PBG s normal or slighrly rncreased. rythrocyteALAactivity is markedly reduced, and both parents should haapproximatelyhalf-normal activity of this enzymeand norm
urinary ALA.
DIAGN0SISNDDIFFEREI{TIAL|AGN0SlS.he 3 otheracute ophyrias are characterized y substantialncreasesn both ALand PBG. n contrast,ALA but Dot PBG s substanciallyncreain ADP A marked deficiencyof erythrocyteALAD and hanormal activity n the parents uppor! he diagnosis.Other cauof ALAD deficiencnsuch as ead poisoning,must be excludSuccinylacetoneccumulatesn hereditaryyrosinemia ype1 ais structurally similar to ALA, inhibits ALAD, and car cauincreased rinary excretionof ALA and clinical manifestatithat resemble cuteporphyria, Idiopathic acquiredALAD deciency has beenreported. Unlike lead poisoning, he deliciALAD activity is nor restored by the in vitro addition sulfhydryl eagents uchas dithiothreitol. Even f no other cauof ALAD deficiencys found, it is essential o confrm the dianosis
ofADP by molecularstudies.
TREATMENTreatment experiences Lnited but is similarother acuteporphyrias.Glucose eems ot veryeffeclivebut mbe ried for mild symptoms,Hemin therapywas apparentlyefftive for acuteattacks n adolescenrmale cases, nd weekly nsions orevenced ctacks n I of these cases.Hemin wa neffectiveeither biochemicallyor clinically in the Swedrsh hwith severe rsease,nd produceda biochemical esponse utclinical mprovement n the Belgianman wirh a late-onsetorwho had a peripheralneuropathybut no acuteacracks. emrnalsoeffective n treatingporphyrialrke symptoms ssociatedvhereditary yrosinemia, nd can significanrly educeurinary ALand coproporphyrin n leadpoisoning.Avoidanceof drugs hare harmful n otheracuce orphyriass advisable,jver ra
plantationwas not effectrven the child with severe isease.
PROGN0SIS.he outlook is generally good ir typical casalthough recurrentattacksmay occur The coutsewas unlavable n cheSwedish hild with more severe isease, nd rs unctain in adultswith late-onset isease ssociated ith myelopIiferative isorders.
PREVENTI0NN0 GENETIC0UNSEtING.eterozygousareshould be aware that subsequent hildren are at risk for tdisease, s n any autosomal ecessiveisorder.Diagnosisn uris possible, ut has not been eported,
ACUTENTERMITTENTORPHYRIAAIP}
This disorder has also been tennedpyrroloporphyria, Suteporphyia, and ifltefttlittent acute porphyria and is the mcommon ypeof acutc orphyria n mostcuuntrie..
ETl0t0GY- IP resuhs rom the deficientactrvrty of the houkeeping orm of PBG deaminasePBGD).This erzyme s aknown as hydroxymethylbilaneHMB) synthase;he prior teuroporphyrinogen synthase s obsolete.PBGD catalyzesdeaminationand head-to-tarl ondensation f 4 PBG molecto form the linear errapyrrole,HMB (alsoknown aspreuropphyrinogen;eeFig. 91 1). A uniquedipyrromethaneofabinds the pyrrole intermedrates r rhe catalytic sice r.rntpyrroles (including rhe dipyrrole cofactor) are assembledn

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 151/177
642 PARTX Mebbolic oiseases
Iinear fashron, after rvhich rhe tetrap,vrrole H\.{B is reLeascd. heepo deamjnase enerateshe dipyrrole cofactor o fornr fhe holodearninase. nd fhi s occurs more readrl,v rom HMB thar iroml'BG. lnclecd,high concentrarions f PB G mal inhibir formarionof rhe holodeamilase. The product HMB can c1'clizc onenzymalicall,v o form nonphysiologicaluroporphylinogen I, but rnth e plesence f the nexc enzyme n the pachrvav s more rapidlvclclized to iorm uroporphvrinogen ll .
Eryrhroid and housekeeping orms ol the enzvrne re cncodedby a singlc geneor hurnan clrromosome l I I1t124.1->qZ4.2),
r,r 'hich ontains 15 exors. fhe 2 isoenzlmesare both lnonomericproteins and diifer or-rly hghdv in molccurlrr weighr (=40 an d42 kd, respectrvelv), nd rcsult rorn alternative plicingof exons1 and 2. The crvthroid specif ic soenzyme, hcrcfore, s encodedb, vexons 2 through 15, and rhe eryfhrordpromoter. vhich un cti(xrs onlv in erychroid cells, is locarcd immediateLy pstreamlron exon 2. Thc housekeepingsoz_ynles cncodccl l exons 1ancl3 rhrough f-i, and rs promoter s nrnediateh upstream ionrexor I (l is lcring sequences ind thc erlrhroid specif icD\A-
bindrng factorsNF E1 and NI,-1,i2,eading ro c\pressi(D of rhe
cr,vthroidpromoter.The housekeepirgpronloter f l lncoons in al lcell types, rcl uding erylhroid cclls.
The pattern oi inhcritanceof AIP it autosornaLlominanr, vithr.ery are homozygous ases hat present r childhood. .{ore rhan200 l:BCD rnutati()ns, nclLrdingmissense, onscnse, nd splic
iog rnutations and insertionsan d dclctions have been rdenril iedin i\ lP, ald in manv populatron groups, lclucling l>lecks. \ ' lostmlrtarions are lound in only 1 or a fcu families. But due rofounder eifecrs,somc ar c rrore commoLr n cerrain geographic
nrcas such ns northern Su.eden V'19llX), Holland iR116\fl,Argentina ((il l6R), Nova Scotia (l(17iW), anrl Srviczeriald(If283X). De novo mutations may hc fbr.rnclu =37u of cases.
Ohester porphyna was initiallJ' describcd as a variant forrn of
acutc porphyria in a large Lnglish famill-, brrr \ras iound ft) be
ciuc ro a PBGD rnutation.' lhe naturc of rhc PBCD mutation
does not account ior the severity of che clinical presentation,
n'hich varics markedll r, ithin lamilies.
\. lost murations ead ro approximatelyhalf-norrnalactivity of
the housekeeping ard eryrhroid isozymes an d half norrnalamounls of rheir respectivc nzymeproteins D alL issues f het-
eroz,vgotes.n =5!16of unrelatedAI P parlents, hc housekeepingisoz,vmes deficicnt.but the erythroid specrfic sozymes norrnal.
\4utarions caLrsinghis variant are usuallv found rvjthin cxon 1
or irs -i ' splice clonor sire or iniriation of rranslation codon.Lnrnunochemical methods can distinguish mLrfations hat are
CRlN4-posirrve r.e., havJng cxcesscross reactive mnunoi()gic
material CRl,\.11elative t) he mutanI cnz! me activit,v)!whereas
CRI\{ negative mutafions either do rot synfhesizca mutanl
enzlme protein. or the proteiD s not staL)le Ll dn()t immunolog
icall,v detectable using ann-PBC;D intibodres. A chiid rl, ith
homoz-vgousAIP was founcl to have inheritcd a diftcrcnt CRIN'I
p()sitrve utarion from eachparent.
PATII0L0GY N0 PATH0GENESIS.nducrion of rhe rateJimiting
heparic nz,vneAl-AS1 s thought to underlieacureexacerbations
of rhrs and rhe other acure porph,vrias.AIP remarns arent (o ras)'mptomatic) n the great mxjority o{ rhosc rvho are heterozv
[jous carriersof PBGD mutatiots, and rhis s aimosf a]rlays the
casebeforepuberty. n rhose vith no hisrorv of acutesymproms,
porphvrin precursorexcrccion s usuall,v ormal, suggesling hat
half nornal hepatic PBCD acrivity is sui6cienc and hepatic
ALAS1 accivity s not rncreased.Many nongenetic acrors chat
lead to clinical expressiono[ AII ' , including cerrain drugs an d
steroidhormonesJ ave he capaclty o inducchepaticAI AS1 and
CYPs. tJnder condit ions n r.hich heme synchcsiss increasedn
the liver, hrif normal PBGD actrvity ma-v become limirrng and
ALA, PBG, and othe. heme parhway intennediates malv accu
muLate. n addit ion, heme synthesrs ecomesmpaired and heme
mediatcd rcprcssionoi hepatic Al,ASl is lesseffecrive.
Ir is not proven,horvc\jer-ha t hepaticPBGD renains conar =50-! ' .oi normal dcriviry during exacerbarions nd remof AIP, as in er_vthroc-vrcs.n earl,v cport suggested haenzvmcactivit l. s consrderaLrlyess han half-nornlal n rheduring an acuteatrack. lepatic PBGD activity night be rediurther once,{ll ' becorncsactivared f, as rccenrly suggexcess BC, nterfcres,vlthassembl,vf ch edipyrromerhanetor for dris cnzymc. t also seems ikely chatcurrentlv unkngeneti. f ircors play a contriburing role in, for examplc! pau.ho cortinue to hat,e artacks even rvhen l<rtou'n prccipitant
avoided,The fau thar,{lP is :rlmostalwa,vs atenr bcfore puberry
gesfs h:rt cndocrine actors,adult Icr,els f sreroidhormoneimporrant ior clinical exprcssion.Symptoms arc more comin u'omcn, which sr.rggesrsrole for fcr rale hormones.Prcstrual attacks are probrbll due to endogenousprogesteAcutc porphvrias ar e sometirncs exacerbared bv cxoge' te ro rJ . . r r r . r r . l r n l I ' r . co r r t rac ! , p l r rn rc ld i l i o ' r ( \ r 'D lJprogesfins.Surprlsingll-, regnancy s usuallyu'ell tolcratedgc:cing rLrat beueficial rnetabolic changesma,v arncliorat
cffuctsof high Jevels i progesterone.
l)rugs rhat are unsafc in acute porphvrias (Table 91 3) incthose har.ing rhe capacit,v o induce hepatic ALAS1. r.vhcloscl,v ssociated ,vith nducrion oi (lYPs. Griseofulvin exanple oi a .hcrnical thrt can iDcrease eme turnover by
m.rting the destruction of specihc (lYPs co form an inhibitoferrochelaraseFE(il{. th c linal enzvme n rhe pathwa,v), uN-rncthyl pror6p6rphyrrr. Sulfonarnideandbiotics are harLrutapparett l l not inducersoi hepaticheme svnthesis.Ethand orhcr alcoholserc inclLrcersf ALr\ synthasc nclsomeC
Nutrit ional factors,principalll-. educed ntake of caloric
carbohvclrates. s nlay occur $.ith il lncss or attempfs to
UI{5AfE
Bartituctes*tllfonamideaniol15'Mepr0bamaie*
,rh0mebutariate,*
butamate*)[arisoprcdo]"6lutethmLdr*Meihyprylontth(horvynoL'MepnenyloinPhenytlrin*5ucof rde![abimazepne*IonazepamPnnidone*Vaiprciccd'Pyftolone5min0pyrine,nllpyrine)6ri5eofLjn*
EqolsMetodopEmde*RibnFn*
PyGzhamide*Di(loftnac*PngeneonendynlhetpmEen5*Danazo'AkohlrlA[E h]bors6pecalynapril)Gkiurnh,rnnelblo(keIerpKialyedipineJKet0c0nazl)leRifumpn
SlFt
tarcctcrdl!P5
A5prfn
Arelirinophen
fnenct lzfe5Pel inalli dl1fi!at
nfepto:nyci; Ji:riar-io5
BDmCe!
n 5 u t 1
Aircp e(rmetdrne
llanitiirne
Aietin mhm(frira
Afctazclariie
A opurf !
lm or e
Bethdnidre
Bumetanide
ainei re
lcumirnr:luoxerre
iaD;pPftn
aent imnir(ra1.":hid?
CtuMlpr.iFLn..cl
5u( y honi
Tetirqliins
Ihr pifiil nnq cr not dudealauilibhfdnadonbodruqlelyr drulerphlrlallh€'ourc:hronlulteior ruq5otblEl] e{e
'PoqhIzirIned,r5i cirrEindicr0n.w?mqpit(d!t n,,r dvefi?llerln U.5 bel]nqo ttu edrugrrl|c,ko ted rhaflnfrlpo0hym,r h p&€nnrplraH! hirmful&uLe 0]r!fts iody $d ony rerfew henog€nrqterLrcmbndio$ h errrsFntn exrr€ftarel {rere5 c:e vidrnftrrEarc
'Po0hlm5 BEd apRrarimnU abtllnqu firdtuq ow$Elirisdilgra.!2rd€i5qley tlfi50!

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 152/177
\,r'eight, an increase orphyrin precursorexcretionand tnduce
anail. of porphlrra. ncreasedarbohvdfatentakemavamelio-
.n re" r t r . i r .
Recen tind ing ' nd icarehar hepat ic LASI is
regulatedby the peroxisomeProliferator-activatedeceptory
co"activatoru (PG'C-1cr),hichmay represencn mporrant ink
betweennurritional statusand acureporphyrias.
rologic manrfestations.
EP|DEM|0L0GYIP occursn all races nd rs he mosl common
controls,Populationscreening y erythrocyrePBGD activiryor
DNA analysis evealeda prevalence f =200 hecerozygoteser
100,000n FinLand,nd1 in abour ,675 60/100,000)in rance.
nosnc crlterla,
CLlNlCAt MANIFESTATIONS.eurovisceral manifestations of
acure porphvrias may appear any time after pubeny; but rarel,v
before. Verv .are casesof bomozygous AIP develop severeneu-
rologic manifestations early in chrldhood, and acu!e attacks do
not occur.
In affected heterozygotes, acute attacks are characterized by a
constellation of nonspecrfics,vmptoms,which may become severe
and life-threarening. Abdominal pain occurs in 85-957o of cases,
rs usually severe, steadn and poorly localzed, but somenmes
cramping, and accompanied by srgns of ileus, including abdom-
ChaFergl r ThePoiphyrias
inal distention and decreasedbowel sounds. Nausea, vomiti
carecholamines, Ocher common manifestations include me
\!mptomsi pain in the extremities.head, neck. or chesti mu
weakness: and sensorv loss. Becauseall these manifestations
neurologic rather than rnflammacory there is little or no abdinal tenderness, ever, or leukocytosis.
Porphyric neuropathy is primarily motor and appears to le
from axonal degeneration rather than demyelinization. Sen
involvement is indicated by parn in lhe extremities, which m
be descnbed as muscle or bone pain, and by numbness, pa
thesias, nd dysesthesias.aresisma y occur early in an att
bur is more often a late manifestation in an attack that is not
ognrzed and adequately treared, Rarely, sevete neuropalhy
velops when there is lrtrle or no abdominal pain. Motor weak
most commonly begins rn the proximal muscles of the up
exlremities and then progresses o the lower exrremities and
periphery. It is usually symmetric, but occasionally asvmmetri
focal. lnitrall,v, tefldon reflexes may be little affected or hype
tive and become decreasedor absent. Cranial nerves, most c
rnonly the 10th and 7th, may be affected, and blindness finvolvement of the optic nerves or occiprtal lobes has b
reporced. More common central nervous system manifestat
include seizr.rres, nxiecy, insomnia, depression, disorientat
hallucinations, and paranoia. Seizuresma1'result from hypo
tremia, porphyria itself, or an unrelated cause. Chronic dep
sion and other mental symptoms occur in some pacients,
attriburion to porphyria is often diffrcult.
Hyponatremia is common duflng acute attacks. Inappropr
antidiuretic hormone (ADH) secretion is ofren the mosc li
mechanism, but ir is diffrcuk to document and other mechan
musf be considered in rndrvidual cases.Salt depletion from ex
renal sodium loss, gastroinrestinal loss, and poor intake h
been suggested as causes of hypooatremia in AIP In s
pa[ients, unexplained reductions in total blood and red blood
volumes were found and increasedADH secretion might thean appropriate physiologic response- Other electrolyte ab
malities may include hypomagnesemraand hypercalcemia.
The atcack usually resolves qurte rapidly, unless trearme
delayed. Abdomrnal pain may resolve within a few hours
paresis wichin a few days, Even severe motor neuroparhy
rmprove over months or several years, buc may leave some
srdual weakness. Progressron of neuropathy to respiratory
bulbar paralysis and death is uncommon with approprjate t
menr and removal of harmful drugs. Sudden death may r
from cardiac arrhythmia.
tAB0RAT0BYFINDINGS. evels of ALA and PBG are substant
increased during acute aftacks and these may decrease afte
attack but usually remain increased unless the disease becoas,vmptomatic or a prolonged period. A populatton based s
in Sweden indicated that symptoms suggestiveof porphyria
occur in heterozygotes during childhood, in contrast to ad
even when urinary porphyria pt€cursors are nor elevated.
study lacked, however, a comparison with the frequency of
nonspecrfic symptoms in a control group of children.
Porphvrins are also markedly increased, whrch account
reddish r.rrine n AIP These are predominantly uroporph;r
which can form noneozymatically from PBG. But becaus
increased urinary porphyrins in AIP are predorninantlv rsome
rheir formation is likely to be largely enzymatic, whrch m
occur if excessALA produced in liver enters cells in other tls
and is tben converted to porphyrins via the heme biosynt

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 153/177
644 PABTX Motdbolic iseasos
pathway. Porphobilin, a degradation product of PBG, anddipyrrylmethenes ppear o account or brownishurinary discol-oration, Total fecal porphyrins and plasma porphyrins arenormal or slightly ncreasedn AIP Eryrhroclte protoporphyrinmay be somewhatncreasedn patientswith manrfestAIP
Erythroc;te PBGD activiry is approximarelyhalf-normal inmos! patients 7U8O%) with AIP, The norrnal range s wide,however,and overlapswith the range or AIP heterozygotes. snoted, somePBGDgenemutationscause he enzyme o be defi-cient only in nonerythroid issues.Also, PBGD s highly depen-
dent on e rychrocyte ge,and an ncreasen erythropoiesis r-reoconcurrent llness n an AIP patientmay raise heactivity nto theIrormal ange.
porphyrias see able91-2),MeasuringPBG n serum spreferredwhenthere s coexistent evere enaldisease, uc s lesssensitivewhen renal function is normal, Measuremenr f urinary ALA isless ensitivehan PBGand also essspecific, ut will detectADP,the ourth type of acuteporphyria.ErythrocyrePBGDactivity sdecreasedn most AIP patients,and helpsconfirm the diagnosisin a patrefltwith high PBG. A normal enzymeacdvity in ery-throcytesdoes not excludeAIP, however, or reasonsdiscussedearlier.MeasuringerythrocyrePBGD s quite useful or screeningfamily members f a patientwirh AIP known ro have ow enzymeactiviry n erythrocytes.However,5-1570 of indiv idualscan bemisclassified srng the eflzymatic assay.This is not useful ininfants <4 mo of age, when rhe enzymecan be physiologicallyincreased n erythrocyles.Erythrocyte PBGD activity may befalsely ow if processing, torage,or transport of the sample scompromised. Simultaneousmeasurementof multiple hemebiosyntheticpalhway enzymes, s offered by some commerciallaborarories,s less eliable han assayshat urilizespecilicsub-srrates. report of low activitres f both erythrocyreALAD andPBGD suggests n unreliable esult,
Knowledgeof the PBGD mutation n a family enables eliableidentificationof other gene arriers,PBGD deficiency anbe doc-umentedn a ferus y measuringheenzyme ctivity n amnioricfluid cells,or more reliably by frndinga PBGD mutadon n thes€cel ls.
C0MPtlCAT|0NS.IP and other acuteporphyriasare commonlyassociated ith mild abnormaliriesn liver function.The risk ofmore advancediver disease nd hepatocellular arcinoma s alsoincreased uring adult ife, perhaps 0- o 7O-fold, ven n asymp-tomatic ndividualswho have ncreased orphyrinsor porphyrinprecursors.Few patients who developed his neoplasm hadincreasesn serumo,-fetoprotein, herefore,cufrent recommen-dationsare hat patientswith acr-rceorphyrias,especially 50 yrold, be screened t leastyearly by ultrasoundor an alternativeimaging method.
The risk of chronic hypenensionand impairedrenal funcrionappears o be increased n AIP Hypertension or a possible
nephrotoxiceffectof ALA may explain mpaired enal funcrionin AIP, which may progress o severe enal failure and requirerenal ransplantation.
Increasedserum thyroxin levels due to increased hyroxin-binding globulin occur in some AIP parients. Hypercholes-terolemiaand elevatedow-density ipoproteincholesterol ppearco be esscommon n this disorder han previously hought.
TREATMET'lTHemin. ntravenoushemin, combined with symptomaticand
supportivemeasures,s the treatmentof choice or most acuteattacksof porphl,ria.There s a favorablebiochemical nd clin-ical response o early reatmentwith hemin, and less esponseftreatmeflt s delayed. t is no longer recommendedhat therapy
with hemin for a severe ttack be srartedonlv after an uncessfulrialof inrravenousiucoseor several ayr.MiJdatrawithout severemanifestations uchasparesis nd hyponatremay be treared nitially with intravenousglucose.After invenousadministration,hemin binds o hemopexinand albuin plasma nd s rakenup primarily n heparocyte..emin entersand augments he regulatoryheme pool in hepatocrepresses he synthesisof hepatic ALAS1, and dramaticreduces orphyrin precursoroverproduction.
Hemin+ is available for intravenousadminisrration n
United Stares sa lyophilizedhematinpreparation PanhernOvation). Degradationproducts begin o form as soon aslyophilizedproduct s reconsrituted ith srerilewater, and thare responsibleor phlebitisat che iteof infusronand a transancicoagulant ffect. Loss of venous accessdue to phleis common after repeated administrarion. StabrlizatroIyophilizedhematinby reconstiturionwith 307o human albucarrprevent hese dverse ffects, nd s recommended,specif a peripheralvein is used for the infusion. Uncommon seffectsof hemin include ever,aching,malaise,hemolysis,aphylaxis,and circulatorycollapse.Hemearginate,a more stahenin preparation, s available n Europeand SouthAfrica.
Hemin reatment should be nstitutedonlv aftera diagnosacute orphyrra as ee nnirially onErmed'bymarked"incin urinary PBG determinedmost rapidly r.rsiog kit, asdesct
earlier),When prior documentation f the diagnosiss availfor review, t is not essentialo confrrman increasen PBG wevery recurrent artack, if other causesof the symptomsexcludedlinically. he standardegimen f hemin oi rrearmof acuteporphyric attacks s 3-4 mg,4<gaily for 4 days. Lodoses ave esseffecron porphyrinprecursorexcretionaod prably less clinical benefit. An investigationalapproach iscombineheme herapy with an inhibitor of heme breakdosuchas in proroporphyrinor tin mesoporphyrin,o prolongefficacyof the administered eme.
Genetal nd SupportiveMeasures.Drugs that may exacerporphyrias (seeTable 9l-3) should be discontinuedwhenepossible,and other precipitaring actors dentified.Hospitaltion iswarranted,except or mild attacks, or treatmentof sepain, nausea,and vomiting; for administrationof hemin a
fluids; and for monitoring vitaLcapaciry, utritional status,nrologic unction,and electrolytes. ainusually equires narcanalgesic;here s low risk for addictionafter recovery romacuteattack. A phenothiazine uch as chlorpromazines neefor nausea, omiting, anxietn and restlessness.hloral hydror low dosesof short-acringbenzodiazepinesan be givenrestlessnessr nsomnia. p-Adrenergicblocking agentsmayusefulduring acu!eattacks o control tachycardra nd hypersion, but may be hazardous in patients with hypovoleand incipient cardiac failure. becausencreased atecholamsecrerio;may in this srtuation e an imporrant ompensmecnanlsm,
Carbohydrate-oading. he effectsof carbohydrares n repting hepaticALAS1 and reducingporphyrin precursorexcreare weak compared o those of hemin. Therefore,only m
attacks nild pain, no paresis r hyponatremia) re trearedwcarbohydrate oading.Glucosepolymersolucions y mouthsomerimes olerated. At least 300g of intravenous glucousually given as a 1Oo/" olution, has been recommendedadults hospitalizedwith attacksof porphyria. Amounts up500 g daily may bemore effective,but largevolumesmay fadevelopment f hyponatremia.
*Hemin is rhe gen€ncname for alt heme prepararionsused or inEa"en
administradon- Henin is also a chemical term thac refers to the oxidr(ferric) form of beme /iron proroporphrrin IX), and is usualty isolate
hernrnchloride. In alkalin€ solution, the €hloride s replac€dby $e hydro
ion, forming hydroxyhen].e, r bendtin.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 154/177
before this can be.ecommended. Cimeridine' a well-known
Dro l t ransp lan ta t ion .'s Padentl often do well with avoidance
o[ drugs known or strongly suspected,o t the acute porphynas are listed in
Table 91-6. Updaredand more xtensive istingsare availableon
an i eractive website of th European Porphyria Initiative
probably be avoided rn patients with acute porphyria. Danazol
can be carried out safely inspecrallY iI barbiturates are
ommended as an inhalation
agenr and propofol and midazolam as intravenous induction
a contraindicaced dmg sometimes used to treat hyperemesis
gravldarum.
Diabetes mellirus and other endocrine condirions are not
known to precrpitace attacks of porphyria ln fact, the onset of
diabetes mellitus and resulting high circulating glucose evels may
decrease he frequency of attacks and lower porphyrin Precursorlevels in AIP
PBOGN0SIS.The outlook for patients with acute porphyrias has
improved markedly in the past several decades. n Finland, for
exanple,74lo of pacients with AIP or VP reported that they led
normal lives, and less han % had recurrent attacks during several
years of follow-up. In those presentrng with acute symptoms,
recurrent aftacks were mosr Lkely within the nexr 1-3 yr More-
over, only 57o of gene carriers who had never had atracks devel-
oped symptoms. The improved outlook may resuh from earlier
detectlon, belter treatment of acute attacks, and replacement of
harmful drugs such as barbiturates and sulfonamides with safer
drugs. A smaller number of patients, however, continue to har,e
Chaptelgl ThcPorPhYlias
recurrentatlacks,chronic parn, and orher symptomsevena
avoidrng nownexacerbatingactor:.
high n carbohydrace 60-7Oy'of total calories) nd sufficiemaintain weisht is recommended. here is little evidence
additional dietary carbohydrarehelps further in prevenattacks,and t may ead coweightgain.Patientswho wish to excesswerght should do so graduallyand rvhen cheyare ccally stable. ron del iciency, hich can bedetected y a ow seferritin, should be corrected.
GnRH analogs,which reversiblysuppress vulation, can
dramaticallyeffective or prevenlrng requentlv ecurring uphaseattacks,but baselineand continuinggynecologic vtron and bone densirymeasurements re lmportan!, and t dermal estrogenor a biphosphonatemav be added o pre
bone oss.Hemrn adrninisrerednceor cwiceweeklycan prefrequent,noncyclicattacksof porphyria n somepahents.
GEI{ETIC OUNSEL|i{G.hildren with a family history ofphyria are often seenby pediatncians or evaluacion nd co
seling, nforrnation and laborarory' results rom a relativewproven porphyriamust be reviewed n order to guide estinrhe child, which is di fferentdepending n the type of acutephvna. A muration denti lied n the index case an be sougthe child. If the child is found to have nherited he mutacounselingco avoid porentially harmful drugs is approprCounseling houldalsoemphasizehat thegreatmajority of thwho rnherit a PBGD mutationneverdevelopsymptoms, ndprognosrsof those who do is favorable. Therefore,a norhealrhy ife is expected,especiallywith avoidanceof hardrugsand other factorsand prompt recognition nd treatmesymploms should they occur Given the favorable outlookmosr mutation carriers,evenduring pregnancnhavrngchilis not precluded,and prenatal diagnosisof acuteporphyriless mportant han it i s for manyother rnherited iseases.n
rtanceof a PBGD muratronshould be resardedas confideinlormacion nd not inlerlerewirh emplovmenr r insueligibiliry.
CONGET{IIAIRYTHBOPOIET|COBPHYRIACEP}
Also termed Gtinther disease,his rare disease suallyprewith photosensirjviry hortly after birth, or io urero as nomunenyorops.
ETI0L0GY EP s an autosomal ecessive isease ue o a madeficiency of uroporphyrinogen II synthase(UROS). MUROSmutatrons avebeendentifiedamoneCEP amilies.L
onset iseasen adulrs s likely o be a'sociared irh myelliferativedisorders nd expansion f a cloneof erlthroblastscarry a UROS mutation.
PATH0t0cY NDPATH0cENESIS.ROS,which is markedlycrent n CEP,caralyzesnversionof pyrrole ring D of HMBpyrrole ring shownon the righr end of the molecule n Frgur1) and raprd cychzationof the linear tetrapyrrole o form porphyrinogenIL This enzymes also rermeduroporphyrincosynrhase. he humanenzyme s a monomei The gene oenzymes foundon chromosome0q25.3->q25.3,nd con10 exons.Eryrhroid and housekeepinganscripts aregenebv alternative romoters ut encode hesame nzvme. he hokeeping ransciiptcontains xon 1 (untranslated)pliced o e

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 155/177
645 PARTX MetabolicDiseases
28 through 10, while the erythroid rranscript contains exor 2A(untranslated) also spiiced to exons 28 through 10. The house-keeping promoter is upstream of exon 1, whereas the eryrhroid-specrficproximal promoter is upstream of exon 2A and containserychrord transcription factor binding sires ncluding GATA1 andNF-E2. Thus, there is erythroid-specifc regularion, but theenzyrne product is the same in all tissues.
In CEq large amounts of HMB accumulate in erythroid cellsduring hemoglobin synthesis and cychze nonenzymatically toform uroporphyrinogen I, which is auro-oxidized ro uropor-
phyrin L Some of rhe uropurphyrinogen I rhar accrmuLresis merabolized to coproporphvrinogen I, wbich accumularesbecause it is not a substrate for coproporphyrinogen oxidase.Thus, both uroporphyrin I and coproporph,vrin I accumulate intbe bone marrow and are then found in circulating erythrocytes,plasma,urine, aod feces.
A variery of UROS mutatrons have been rdenrified in CEP,including missenseand nonse[se mutations, large and small deletions and insertions, splicing defects, and nfionic branch poinrmutarions. At least 4 mutations have been identified in rheerythroid-specific promoter. Many pacienrs inherited a differentmutatron from each parent, and most mutations have beendetected in o y 1 or a few families. An exception is a commonmutation, C73R, whrch is at a mutatronal hotspor aod was foundin =3 3% of alleles.
Genotvpe phenotype correla ons have been based on rhe invitro expression of var ious CEP mutanons and the severity ofassociatedphenorypic mamfesrations. The C73R allele, which isassociated v'icha severephenotype in homozygotes or rn patientsheceroallelic for C73R and another mu[arion expressing littleresidual actrvitg resulted in < 17o of normal enzyme activity.Patients wirh the C73R al lele and heteroallelic for other muta-tions expressing more residual activrty have mrlder drsease.
Hemolysis is a common feature of CEP Excessporphyrins incirculating erythrocytes cause cell damage, perhaps bv a photo-toxic mechanism, leading to both intravascular hemolysis andincreased splenic clearance of ert/lhrocvtes. Also important isineffective erythropoiesis, wich intramedullarydesrruction of por-phyrinJaden erythroid cells and breakdou,'n of heme. Expansionof the bone marrow due to ervthroid hyperplasia mav contribute
to bone loss. Nutrrent de6ciencies sometimes cause ervthroidhypoplasia. Despite the marked deficiency of UROS, heme pro
dr-rction n the bone marrow is increased,due to hemolysis and acompensatory increase in hemoglobin production. This occurs,however, at the expense of marked accumulation of HMB, whichis converted to porphyrinogens and porphyrins.
CtlNlCAt MANIFES l0NS. In severe cases,CEP can cause fetalloss, or be recognized in utero as intrauterine hemolytic anemiaand nonimmune hydrops fetalis. CEP may be associated withneonacal hyperbilirubinemia, and phototherapy may uninten-tionally induce severephorosensitivity.
The most characteristic presentation is reddish urrne or pinkstainrng of diapers by urine or meconium shordy aFter birth (Fig.
91 2). Wifi sun exposure, severe blistering les ions appear on
exposed areas of skin on the face and hands, and have beentermed ltydroa aestiualebecause hey are more severewrth greater
sunlighr exposure during summer (Fig. 91 3). Vesiclesand bullae,as well as flabrlry, hypertrichosis, scarring, thickenirg, and areasof hvpo- and hvperpigmentation are very similar to those seen nPCT, but usually much more severe. nfeclion aod scar.ing som€-rimes cause loss of facial feacuresand fingers and damage ro thecornea, ears, and narls. Porphylns are deposrted in dentine andbone in utero- Reddish-brown teeth in normal light, an ap-pearance termed erythrodontia, displa;,'' reddish fluorescenceunder long wave ultraviolet liglt {Fig, 91 4), Hemolysis andsplenomegalv are features of many cases.Bone marrow compen-sation may be adequate, especially in milder cases.Pacientswithsevere phenotypes, however, are often transfusion-dependent.
ligure 91-2. Congenital r_]'thropoieticorphyria. he diaperoI an affba 1. emonstrareshe edco1o. { urine.}'ron PaUef S,MaciniAJ:H,]rClinicalPedidttic etnarologl .lrd ed.Philadelphia,lsevier aunderc,
Splenomegaly may contribure ro the anemia and cause eukonia and thrombocytopenia, which may be complicated by sigicant bleeding. Neuropathic sl.mproms are absenc, and therno sensitivi ry to drr :gs, hormones, and carbohydrate restrictiThe liver may be damaged by iron overload or hepatitis acquifrom blood lransfusions.
Milder casesof CEP with onset of svmocoms in adult life awirhour eryrhrodontiama v more rlosell mimic PCT. These aonser casesare likely to be associatedwith m-veloproliferativeo rde r . .andexpans ion fa c lone rce l l s a r r y ing UROSsommutation.
tAB0BAT0RY FINDINGS,Urinary porphyrin excrelion and cirlating porphyrin levels n CEP are much higher than in almost
other porphyrias. Urinary porphyrin excretion can be as high50-100 mg dail-v, and consisrs mosdy of uroporphyrin I coproporphyrin I. ALA and PBG are normal. Fecal porphyn
are ma_rkedly increased, with a predominance of coprop
Pnyrln r.
Marked rncreases n eryrhrocyte porphvrins rn CEP conmostly of uroporphyrin I and coproporphyrin L These pphyrins are also increased n bone marrow, spleen, plasma, ato a lesser excent) iver . The porph;rrin partern in erythrocytesinfluenced by racesof erythropoiesis and erythroid maturation.pledominance of procoporphyrin has been noted rn some C
Figurc 9l l. Congenitaleryrhropoieticporphyria. Vesicles, ullae, and cr
on sun exposedareas (From PaLlerAS, Macni Al: Hureitz Clinical Pedia
Dermatologl,3rd ed. PhiJadelphia,lsevier Saunders, 006, p 517,)

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 156/177
Figurc 91-4. Congeniralerlthropoieric porphyria. Brownish teeth that fluo-
p s17. )
patients, nd n 1 suchpatient!uroporphyrinandcoproporphyrin
increased hen erythropoiesis as srimulated y blood removal
DIAGN0SISNDDlfFEltl{Tl,AtDIAGI{OSIS.he diagnosrs f CEP
shouldbe documented y full characterization f porphyrinpar-
ternsand denrification f the underlyingmutations ln later onset
cases,an underlying myeloprohferative isorder and a UROS
somaticmutation shouldbe suspected nd studied n detail'
red-brown discolorationand increased orPhyrins n amnioric
Iluid, measuring orphyrins n fetal erythrocytes nd plasmaand
UROS acuvitv in culrured amnioric fluid cells, or identiffing
UROSgenemutations n chorionicvtlli or culturedamnioriccells
sunlightexposure,minimizing skinn! of anY cutaneousnfectionsareg CE P(see able91-4) Sunscreensometimes eneficial. ransfusions
to achievea level of hemoglobrn ufficienc o suppless lythro-
poiesis ignrficantly an bequrte effective n reducingporphyrinievelsand photosensitiviryConcurtenrdefetoxamrne o reduce
iron overload, and hydroxyurea to suppresservthropoiesis
further may provide addidonal benefit. Splenectomyeduces
hemolysisand transfusion equirementsn somepatients.Oral
charcoalmay increase ecal loss of porphyrins, bur may con
cribute ittle irr more severe ases. nrravenoushemin may be
somewhateffeccive, ut has not been exlensivelystudied and
seems nlikely to provide ong-termbenefit.Chloroquinehasnot
beenbeneficial.Bonemarrow or stemcell ransplantation, hrchhasmarkedly
reduced orphyrin evelsandphotosensltiviry nd ncreasedong-
rermsurvival,shouldbe consrdered,speciallyor severe rsease
Gene herapymay be accomplishedn the future.To date,human
Ghaptei r ThePorpftYria
UROS cDNA has been subcloned into retrovital vectors, w
hare been used o lransduceFbroblast*an d lrmphobla'rs
padents u'ith CEI resulrrng n significant levels of enzvme ex
iion. Transducuon of hematopoietic progenitor cells arrd
erythroid cells was also achieved.
PB0G 0SlS. The outlook is favorable in milder cases an
patienm wlth more severe disease reated by transfusions
ii"nt to .upp.... erlthropoiesis and bone rnarrow porph
production at least partiallv. Successfulbone marrow or stem
transplantation has proven effective.
PBEVtilTlo$ tlDGENETICoUltlSEtlNG.enetic ounseimoorcant or affected amilies,becauseCEP can be recog
before birch and a severephenotype can often be predicte
idenrifying he nature of the UROS mutation\.
PORPHYRIAUTAIIIEAABDAPCTI
Thrs s rhe mosrcommonan d readily reated umanporp(see able 91-2). t occurs n mid or late adult ife, and s ra
children, Prevrous erms include symptorfiaticporphlri',
symptomatica, nd diosyncrrlti.porpDyrr,r. he underlyingis a iiver-specific,cquireddeficiencv f uroporphyrinogen
boxylase UROD) with contributionsby severalypes of gfactors, UROD mutations are found in famihal PCT
homozygous orm of familial PCT is HEB which has a
severe resentation, sually n childhooO.
ET|OI0GY. CT is due to a marked deficiency f hepaticURThis enzyme efrciency us t be substantial'20'lo of n
activity or less) or PCT to becomemanifest,and ts develois atribured to generation f a UROD inhibrtor specilicallyliver This inhrbiror,which has noc beencharacterized,s defrom a hemepathway intermediatesuchas uroporphyrinand CYPs suchas CYP1A2, as well as iron, are involvedformation (Fig.91-5J.Evenwith substantialnhrbition of hUROD activity, the amoun! of enzvme protein meaimmunochemicallyemainsat its genetically etermined e
UROD catalyzes he decarboxylation f the 4 acetrcacichainsof uroporphyrinogen anoctacarboxylporphyrinogform coproporphyrtnogena tefi acarboxylporphyrinoge
Glycine+ SuccinylCoAI
ALASII
6-Aminolevulinicci d
II
I CYPIA2
CoproporPhyrinogen
IIl- E^2+I -
Heme
t'igurc 91-5. Formation of a specinc nhibrror of uroporphvrinogen
boxylase n rhe iver in porphtria cutanea arda. AL.\S, &aminolevuti
synthase; CYPlA2, c-vtochrome P450 1A2r UROD, uroporphy

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 157/177
648 I PARTX MetabolicDiseas€s
Fig. 91 1). The enzyme reaction occurs rn a sequertjal, clockwisel:ashion,wirh lhe i nrermediare ormarion oi hepra-. hexa-. an d
strate. Human UROD is a dimer with rhe 2 acrive sire cleftsjuxtaposed. The UROD gene is on chromosome 1p-j4 and con-ta ins 0exons . ' " r ' i r hon lvp rum o le r . l he re fo re . h i gene s r ranscribed as a sinele mRNA in all trssucs.
Th e majoritv of PCT parrenrs =80%) have no UROD mura-rions and are said to have sporadrc (rype 1) disease.Some are het-
erozygous for UROD mutarrols and are said to have farnilial
cause PCT unless a UROD inhibitor is also generated. Becausepenetrance of the genetic ait rs loq many parienrs with familial PCT have no famrlv hi orv of the disease.
lnduction of hepaticALAS1 rs nor a promin t feature nPCT,although alcohol may increase this enzyme ightLy.. ron andestrogens are also not potent inducers of ALAS1 and drugs thatar epotelt inducers f ALASl and CYPs ar e much less ommonlyrmplicated n PCT rhan in acurepurphyrias.
Blistering skin lesions resulc from porphyrins tlar are releasedfrom the liver Sunlight exposure leads to generation of reactiveoxy_genspecies n the skin, complement activation, and lysoso-mar oamage.
E es probably relate to geo-g ctors suchas hepatit jsC ande he United K insdom was esti-mared r 2 -51 1 ,000.000. nd hep fe ra lencen cheUn i red ra lesand Czechoslovakia .i 'asestimaled ac =1/25,000 and 1/5.000.respectivel). The disease *.as reported to be prevalent in theBanrusof South Africa in associationwirh iron overload.PCT ismore common in males, possible due to greater alcohol intake,and m wornen it is commonly associated with estrogen use.
A massive outbreak of PCT occurred in easrernTurkev in thelq50 \ . !Vhea r nrended or p lan r ing and r re . r redw i th hexa-
chlorohenzene as a fungicide was consumed bv man,v at a timeof {ood shortage. Cases and small outbreaks of PCT after expo,sure to other chemicals including dr- and rrichlorophenols and2,3,7,8-cetrachlorodibenzo-p-dioxin (TCDD, dioxin) have beenreported. The manlfestatlons rmproved in most cases when lheexposure rvas stopped. There are, however, reported cases ofdelayedonsecmany yearsafter chemicalexposure.
PATH0[0GY ND PATH0GENESIS.CT is currentlv classif ied ntot c l i n i ca l l y im r la r 1pe r ,Gene ra t ion f a UROD inh rb i ro r n rheliver plays an important role rn all 3 qvpes.The -80% of parientsrvrth type I (sporadic) PCT have no UROD mutationsr andUROD activity is normal in nonhepatic issues.n familial (type
2) PCT, a UROD mutation is associated wirh a partial (=50%)deficrency i UROD in nonhepatic i* 'ue.. fh e genericalllderer.mined level of rhe enzl.me is also 50% in rhe lir.er, bur rs muchlower when a UROD inhrbiror is generated and the diseasebecumes linrcallr acrive.Type t is rare. and deocrrbe, C f rvrrhnormal erytbrocyte UROD activity occurring in more than 1family member UROD muradons or another seneric basis haveno r been denril ied n rype 1. an d tamilial occurrence 5 the ont]feature that distinguishes it from tvpe 1.
CYPs, especially CYPY1A2, can catalyze the oxidation of uro-porphyrinogen to uroporphyrin. This uroporphyrinogen oxidase(URO-OX) activit]' is enhanced by iron, and leads ro formahonof a UROD inhibitor (seeFig. 91-5). CYP1A2 seems ssentralordevelopmenr of uroporphyria in rodents, because experimental
n ropo rphy r rad , ' cs no ' 6 .u " ,op in CYPIA2 knoek lu r m iS tud iesw i rh CYP2El Inockuurr rugge ' r ha t h i \ enTvmemalso contriblrte. Mrce wrth disruption of one UROD allele aeither 1 or 2 disrupred HFE alleles provide an important modfor PCT wichouc adminrsrration of halogenated cliemicals.
patlelrt.
lron. A normal or increasedamounr of iron in the liver is ess
major cause of hemochromatosis i *.hire people, is increasedboth tvpe 1 and cype2 PCI and 10% of pacienrs re C282homozygotes. In sourhern Europe, where rhe C282Y is lessprevlent, rhe H63D mutatjoo is mote commonly associated.PCT moccur with secondary iron overload.
Hepatitis C. This viral infecdon is highly prevalent in PCTmost geographic locations; in the United States, for example,rs present in 56-747o of cases,which is simrlar to tbe (ate cir
oxjd ve stress Jn hepaticis C may favor rron mediated genetion reactive oxygen speciesand a UROD inhibitor
HIV Many reporcs suggest HIV rnfection can contribute to thdevelopmenc of PC! hoLrgh ess commonl,v than does hepatis C. The mechanism no t known.
Ethanol.The long-recognized assocjation between alcohol anPCT may be expJained y chegeneracion f acriveoxygenspec
increased production of endotoxm, and activation of Kupflecells.
Smoking and CytochromeP450Enzymes.Smoking has not be
CYPs and oxidative srress, Hepatic CYPs are thought to
CYP1A2 and 1A1 have been imphcated rn human PCT. The frquency of an inducible genotype was more common rn PCpalenls rhan in controls rn 2 studies
Antioxidant Status.Ascorbic acid de6cienc,vhas been rmphcarein conrriburing to uroporphyla rn laborarorv models and humaPCT. In 1 series, plasma ascorbate levels were substanciareduced in 847" of patients \\,rth PCT. Lorl'' levels of serucarotenoids were also described, furcher suggesting hac oxidaostress rl heparocytes s importanr in PCT.
Esttogens.Use of escrogencontaining oral contraceptives opostmenopausal strogen eplacemen!s very commonlv assoated wich PCT (type 1 or 2) in women. PCT sometimes occuduring pregnancy, afthough it is noc clear whether the nsk
lncreased.
CU'CAI. MAI{IFESTATIONSCutafleousManitestations. PCT is read ,v recognized by blisre
ing and crusted skin lesions on rhe backs oI rhe hands, rvhich arhe most sun-exposedareas of the body',and somewhat less commonly on rhe forearms, face, ears, neck, legs, and feet. The fluidfilled vesiclescommonlv rupture and become crusced or denudeareas, heal slowln and are subject to infecion. The skin on rhbacks of the hands is characteristically friable, and minor traummay cause blisters or denudation of skin. Small white plaque
tetmed tui\fu, ma1' precede or follow vesicle formation. Facihypertnchosis and hyperpigmentation are also common. Seve
scarring and rhickeningof sun-exposed kjn mav resemble cl

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 158/177
chanses reno l soecilicor PCT.Th esame indings ccur n VP
an d FCP,an d reiemblehose f ( tl and HE P bu t are usually
lessserrere, nsetof the drseasen childhood s rare' and is more
tAB0RAT0RYlN0lNGS. orphyrinaccumulatesn the ivermostly
and II.
Chaptelgl r ThePorDhyrias 6
DIAGN0SIS NDDIFFERENTIAIlAGN0SlSPLasma orph,vrins
aLways ncreased in clinically manifest PCI and a total plasm
porplvrin determination rs most useful for screening. A norm
value rules out PCT and other porphvrias rhat produce bltste
ing skin lesions. If increased, t is useful to determine the plasm
fluorescen.. emission maxrmum at neutral pH, because
maximum near 519 nm is characteristic of PCT (as well as CE
and HCP) and, most important, excludes VP, which has
distinctlv different fluorescence maximum lncreased urina
normal,
PC! but with an additional marked tncrease n erythrocyte z
stage renal disease.
C0MPLICATI0NS, utaneous blisters may ruptute and beco
infecred, sometimes eading to cellulitis. In more severedrseas
patients with end-scage enal disease, epeated infections can
mutilating, as in CEP, Pseudoscleroderma, with scarring, co
tracrion, and calcification of skin and subcutaneous trssue, i
rare complication. Other complications, such as advanced liv
diseaseand hepatocellular carcinoma, were alreadv discussed
TFEATMENI Management of PCT includes choice of 2 spec
aod effective forms of treatment, phlebotomv or low-do
hydroxvchloroquine, and removal of susceptibility factors wh
possible. The diagnosis of PCT mLrst be 6rmly established, aiondirions thar produce identical cutaneous esions exclud
because hese do not respond to treatments used in PCT. Tre
and tested for hepatitrs C, HIV, and HFE mutations. Some s
ceprrbility factors influence the choice of treatment.
Phlebotomy is considered standard therapn and is effec
both in children and adults with PCT because t reduceshepa
rron contenr. Treatment is guided bv plasma (or serum) ferri
and porphyrin levels,Hemoglobin or hematocrit levels shoul
follou.ed to prevent symptomattc anemia. For adults, a un
blood 1=456-1; is temoved at =2 wk intervals urtil a larserum ferritin near the lower lmit of normal (=15 ndml-)
achieved. A rotal of 6 to 8 phlebotomies is often sufficienr. Af
this, plasma porphynn concentrations continue to fall from p
treatment levels (g€nerally 10-25 pgldl-) to below the upper li
of normal \=1pg/dL), usually after severalmore weeks.Thi
followed by gradual clearing of skin lesions, sometimes nclud
pseudoscleroderrna. Lrver function abnormalities may impro
and hepanc siderosrs,needleJike inclusions, and red fluoresce
of liver tissue will drsappear Although remission usually pels
even rf ferritin levels later return to normal, it is advlsable
follow porphyrin levels and reinstitute phleboromies if th
begin to rise. lnfusions of deferoxamine, an tron chelator, may
used when phlebotomy is contraindicated.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 159/177
650 PABTX MetabolicDiseases
An alternarive *'hen phlebotomy is concraindicared or poorlytolerared is a low-dose regimen of chloroquine or hvdroxy-chloroquine. Normal doses of these 4-aminoquinoline anti-malarials increase plasma and urinarv porphvrin levels andincrease photosensitivicf in PCI reflecring an outpouring of por-phvrrns from the liver This is accompanied by acure hepatocel-lular damage, with fever. malaise, nausea, and increased serumtraflsaminases, but is followed by complete remission of the por-phyria. These adverse consequencesof normal doses are largelyavoided by a low-dose regimen (chloroquine 125 mg or hvdroxy-
chloroquine 100 mg, Y. of a normal tablet, twice weekly), whichcan be continued undl plasma or urine porpbyrins are normalized. There is ar least some risk of rerrnopathy, which may belower with hydroxychloroquine. Prospective treatment trialscomparing chis reacmentwith phlebotomy are lacking. Low-dosechloroqurne ma)' not be effective in patrents homozygous for theC282Y mutation in the HFE gene,Therefore, the degreeof excessheparic iron may influence response o chis creatment. The mech-anism of action of 4-aminoquinolines in PCT is not known, butis quice specific, since these drugs are not useful in otherporphyrias.
In patients with PCT afld hepatitis C, PCT should be treared1st because this condition rs more svmgtomatic and can berreatedmore quicLly an d eflectrvell. reatmenc of PCT hr phle-
botorny may not be possible once rnterferon-ribavirin treatment
is complicared by anemia. Moreover, treatment of hepatiris Cmay be more effecrive after iron reduction. Resrstanceof hepati-tis C to treatment with rnterferon-d or pegylated interferon andribavirin has been eporred in patiencspreviousl,v reated for PC!
but prospective studies are lacking (seeChapter 355).PCT rn patients with end-stage renal disease is often more
sel'ere and difficult to rreaf. Although phlebotom,v is ofren con-
traindicated initiall,v, er1'thropoietrn admrnistratron can correct
anemia, mobilize iron, and support phlebotomy in manv cases.
Response may also occur after renal transplantacion, due in part
ro resumption of endogenous erythropoieric production.
Liver imaging and a serum o-fetoprorein determination may be
advisable in all PCT patients, perhaps at 6-12 mo intervals for
early detection of hepatocellular carcinoma. Finding low er,v-throcyte UROD activity or a UROD mutation identi fies those
with an underll,ing genetic predrsposition, whrch does not altertreatment but is useful for genetic counseling (see ater).
PR0GN0SIS.PCT is the most readily treated form of porphyria,
and complete renissron rsexpectedwlth treacment either by phle-
bocomy or low dose hydroxychloroquine. There is iittle infor
mation on rates of recur rence and long-term ourlook. Risk for
hepatocellular carcinoma is increased, and some suscepribilitv
factors such as hepatitis C can lead to complications even afcer
PCT rs n remission,
PREVEI'|T|0NllDGENETIC0UNSEtlNG.atients ith PCTmayhave concerns about risk ro other family members, A hericable
L,'ROD nutauon can usually be detected or excluded by mea-
suring erythrocvte IIROD acrivity, although DNA studies aremore sensitive. Relarives of Datientswith UROD mucations have
an rncreased isk for developingPC! and may'have increased
motivation ro avoid adverse behaviors such as ethanol and
tobacco use and exposures to hepatitis C and HI\'. Such coun-
seling would be given to an,vone,however. The linding of HFE
muratrons, and especially C282Y, should prompt screening of rel
ativesr some of r.r.hommay be C282Y homozygotes and &'arrant
I i i e longm un i ro r rng f re rum e r r t t t n .
HEPATOERYTHROPOIETICORPHYRIA
Hepatoervthropoietic orph,vriaHEP), vhich s the homoz),gousform of famrlial (type 2) PCT, resembles EP clinically.Excess
porphyrins originate mostl ,v from liver, wlth a paltern cons!.i'ith severeUROD deficiency. This rare disorder has no palar racial predominance.
ETl0L0GY HEP is an aucosomal recessivedisorder, altbough patients have inherited a diflerent mutacion liom unreparenrs. n contrast !o most mutalions in familial (tvpe 2) most causing HEP are associated with expressiot of some rual enzyme activiry. At least 1 genotype is associated withpredominanr excretion of pentacarboxyl porphyrin.
PATH0L0GY ND PATH0GENESIS.xcessporphyrins originatemarily from the liver io HEP, although che substanrial increaeryrhrocyte zinc procoporphyrin indicares rhat the heme biotheuc pathway is also impaired rn bone marrorv erythroid Apparently, porph,vrinogens accumulate in the marrow whemoglobin svnthesis s mosc active, and are merabolized roroporphvrin alter hemoglobin synthesis rs complece. The neous lesions are due to photoacti vation of porphy rins in as n other cutaneousporphyrias.
CUNICALMANIFESTATI0NS. ike CEP. rhis disease usuallvsenrswirh blisrering ,kin esions. l perrrichosis.carrrng.anurine in infancy or childhood. Sclerodermoid skin change
sometimes orominent. Unusuallv mild caseshave been descrConcurreni condrtions rhat affect liver funcrion can alter diseverity. For example, hepatirs A caused the disease ro becmanifest in a 2 year old child, and then improved with recoof liver function.
LASORATORYlt{DlNGS. Brochemical frndings resemble thoPCT with accumularion and excretjon of uroporphyln,
tacarboxyl porphyrin and isocoproporphvrin. But in addi
erythroclte zinc procoporphyrin rs substantially increased.
DIAGN0SISAND DIFFERENTIALIACN0S|S. HEP is drstineui
lrom CE P hv Incr ea5.s n borh uroporphyrin and hepra.irhporphyln, and rsocoproporphyrins. In CEP the exc€ss erytcyce porphyrins are predormnantly uroporphyrin and copro
phyrin racher than proroporphl'rin, Blistering skin lesionsunusual in EPI the excess erlthroc,vte protoporphyrin indisease s free and_noc complexed with zinc, and urinarypnylrns are normal.
IREATMEI'IT ND PR0GN0SIS.Avording sunJight exposure is m
important in managing chis disease,as rn CEP.Oral charcoalhelpful in a severecase associacedwith dyserythropoiesis. P
botomy has sholr'n litcle or no beneft. The outlook depend
the severity of the enzvme deliciency and may be favorable rf
light can be avoided, Retrovirus-mediaced gene transfer correporphyria in transduced lvmphoblastoid cells from HEP patie
suggescing hat gene therapv may eventually be developed.
PnEVENTI0NND GENETIC 0UNSEUNG, s part of geneticcseling in affecred families, it is feasible to diagnose HEP in u
either by analys is of porphyrins in amntottc fluid or DNA stu
HEREDITARYOPROPORPHYRIAHCP}
This autosomal omrnanthepaticporphvria s due o a deficof coproporph,vrinogenxidaseCPO). hediseaseresenracuteatlacks, as in AIP Cutaneous hotosensitivitymay obut much less commonly than in VP Rare homozvgouspresentn childhood.
ETI0LOGY partial (=50%) defrciencyn CPO activitv hasfound rn all cellssrudied rom patients {'ith HCP A much m

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 160/177
ture release f harderoporphyrinogen.
EPIDEMI0LOGYCP is lesscommon than AIP and VP, but its
PATHOTOGYNDPATH0GENESIS.ncreased LA and PBGdunng
rn HCP
GtlNtCAtMAI{|FESTATI0NSymptomsare identical o those of
AIP except that attacks are generally milder, and c.utaneous
lesions hit resemble hose n PCT developoccasionallySevere
acute orphyrias.Th cLnical featuresof homozygousHCP, whrch begin in
early childhood, may include ,aundice, hemolytic anemia,
hepatosplenomegalv,nd skin photosensitivity. hesesymptoms
ari getre.ally r-:ite istrnct rom thoseseen n heterozygotes
S Theporphyrin recursor\ LA and PBGculeattacks, ul ma ydecreaseore apidltncreasesn coproporphyrin II in urine and
Chaptelg'l ThrPorphYrias
coproporphyrrn.Plasmaporphyrins are usuallynormal or o
slightly ncreased.
DIAGNOSISNDDlttERCNT|ALIAG[{0SlS.he diagnosrsf H
mostlycoproporphyrin isomer II) in HCP,whereasn VP,co
porphyrin lll and protoporphytin are often rncleased PP
marely equally.Plasmaporphyrins are usuallynormal in H
and increasedn \?.
family members.
TREATMENTt{D PR0GNOSIS.cute attacksof HCP are tre
erally berter han in AIP
PREVENTI0NNDGENETIC0UNSEI-lNG.heseare he same
other acuteporPhYrias.
VARIEGATEORPHYRIAVP}
This hepatic porphyria is due ro a deficiencyof proto
phyrinogenoxidase PPO),which is inherited as an autos
dominant trait. The disorder s terrneduariegate ecauset
presentwirh neurologicor cutaneousmamfestions.Other tehave iocluded porPhyria eariegata,proto.opropotphJtw,South Aftican geneticporphyria. Rare cases f homozygouare symptomatrcn childhood.
EflOIOGYPPO s approximacely alf normal in all cellsstu
in patientswith VP The enzyme s more markedly deficie
rare cases f homozygousVP, with approxrmately alf-no
enzymeactivity in arents.Human PPO s homodimer hat containsFAD and is l
ized to the cytosohcside of the inner mitochondrialmemb
Membrane-brnding omainsmay be dockedonto hurnanFEthe next enzymen the pathway,whrch s embeddedn the o
srte side oI the memb.ane.PPO catalyzeshe oxidation ot
and by certainherbicideshat causeprocoporphyrin o acclate and inducephototoxicity in plants. nhibrtion bv bihmay account or decreased POactivity rn Gilbert disease
The hr-rman POgeneon chromosome q22-q23 consistnoncodingand 12 coding exons,A singlePPO ranscript s
duced n a varieryof tissues, ut putative tansclrptionalele
binding sequences a allow for erythroid specificexPreMany PPO mutadons ave been eported n VP farnilies A
sensemulation, R59W, is prevalent n South Africa. No

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 161/177
652 PABTX Metabolic iseoses
vincing genotype-phenotypeorrelationshave been rdentified.Mutations in homozygous ases f VP are more ikely to encodeenzymeproteinswith residualactivity.
EP|DEM|0L0GY.P is lesscommon than AIP in most countries.The R59\V mutation s highly prevalent n SouthAfrican whites(=3/1,000).This exampleof geneticdrift or "founder effect" hasbeen raced o a mafl or his wife who emierared rom Hollandro Sourh Airica in 1o88. In linland. rhe orevalences' L /100 ,000 nd sabour scommon sAIP
PATH0LOGYNO PATHOGENESIS.cute attacks develop in aminority (=25%) of hererozygotesor PPO deficiencnand areoften aftributable o drugs,steroids, nd nutritional factors harplay a role in other acute porphyrias.Protoporphylnogen IXaccumulates nd undergoesauto-oxidation to protoporphyrinIX. CoproporphyrinogenII may accumulate ue o a close unc-tronal association etweenPPO n the nner mitochondrialmem-brane and CPO in the intermembrane pace.Liver porphyrincontenr is nor ilcreased. The increasedporphyrin contenr inplasmaconsrsts f porphyrin-peptide onjugates,which may beformed from protoporphyrinogen. ncreasedALA and PBGduring acuteattacksmay be explained,as n HCP, by inductionof ALASl by exacerbatingactors,and by the normallyrelativelylorv activityof PBGD n liver Furthermore,PBGD s nhibitedbyproroporphyrinogen,he substrate or PPO.
CUNICALMANIFESTATI0NS.ymptoms develop in some het,erozygotes ter puberty.Neurovisceral ymptomsoccurringasacuteatracksare idenrical o AII but are generallymilder andlessoften fatal. Drugs,steroids,and nutritional alterations uchas fasting,which are harmful in AII can also nduceattacksofVP.Attacksoccur equally n malesand females, t least n SouthAJrica.Cutaneous ragility, vesicles, ullae, hyperpigmentation,and hypertrichosis f sun-exposedreas remuchmore commonthan in HCP They are likely to occur aparr from and be moreIong lasting than rhe neurovisceral ymptoms.Oral contracep-tivescanDreciDitateutaneousmanrfestatiols. cuteaftackshavebecome ess ommon, and skin manifestationsare more fre-quently rhe nihal presentation; his may be due co earlier
diag-nosis and counsel ing.The risk of hepatocellularcarcinoma sincreasedn Vl as n other acuteporphyrias.
Symptoms f homozygousVP begin n infancy or childhood.Thesechildrengenerally avesevere hotosensitivitS eurologicsymptoms, onvulsions, evelopmental isturbances, nd some-timesgrowth rerardation,but do not haveacuteattacks.
IAB0RATOSY|N0|NGS. rinary ALA, PBG, and uroporphyrinare ncreased urilg acuteartacksbut often lessso than irl AIP,and thesemay benormal or only slightly ncreased ttlng rernis-sion, Plasmaporphyrins, urinary and fecal coproporphyrin II,and fecalcoproporphyrin II and protoporphyrin are more per-sistently ncreased etweenattacks.Erythrocytezinc protopor-phvrin evelsare markedly ncreasedn homozygous l and may
be modestly ncreasedn heterozygousases.
DIAGN0SISNDDIFFERENTIALIAGN0SIS.P is readilydistin-guished rom AIP and HCI which alsopresentwith acuteactacksand increasesn PBG. Plasmaporphyrin analysis s especiallyuseful, becausehe plasmaporphyrins n VP are tightly proternbound, resulting n a characteris tic luorescence missionspec-ffum at neutral pH. Fecalporphyrins are increased,wirh ap-proximately equal amounts of coproporpbyrin III andprotoporphyrin.Fluorometricdetectionof plasmaporphyrins smore sensitivehan stoolporphyrin analysisn asymptomatic PPPO assays sing cells that contain mitochondria,such as lym-phocytes,are sensitiveor identifying asymptomatic arriersbutar enot widelyavailable.
TREATMENI cuteatracksare treatedas n AIP.Hemin is beficial for acuteattacks but not for cutaneous ymptoms,Liprotection s mportant n padentswith in manifestations,slong-sleevedlothing,gloves,a broad- mrred hat, and opasunscreen reparations.Exposure o shorr-wavelengrh ltralet light,whrch doesnot exci!eporphyrins,may ncrease kin pmentation and provide some protection. Phlebotomychloroquineare not effective.Surprisingll., ral activatedchcoal.was eported o increase orphyrin levelsand worsen smanrlestallons.
PROGN0SISND PREVENTION.he outlook of padenrswith has mproved,which may be attributed o improved teatmearlier diagnosis,and detection of lat€nt cases.Cyclic acattacks n womencan be preventedwith a GnRH analog,aAIP. A diagnosis f VP or any other acuteporphyria shouldlead to difficulry obtaining insurance, ecausehe prognosusr.rally ood once he diagnosiss established.
GENETICOUNSEIING.heseare the sameas n other acuteophyrias.
EBYTHROPOIETICBOTOPORPHYRIAEPP}
In this autosomal dominanr disorder, protoporphyrin accumlates due co a partial deficiency of FECH, the last enzyme in heme biosynthetic patbway. EPP is sometimes @tmed protopphyria ot etythrohepdtic protoporphyria, although the liver dnot concribute sr.rbstantially o production of excess protopphyrin in uncomplicated cases.
ETl0t0GY. FECH, the enzyme that is defcienr rn EPP, catalythe final step in heme synthesis, which is lnsertion of ferrous ir(Fe'?*)nt o protoporphyrin IX (seeFig.91-1), Th e enzyme s atermed heme sykthetase or protohetue fettolyase. The humenzyme is a dimer, and each homodimer contains a [2Fe-cluster, whrch nay have a role in bridging homodimers. FECHfound in the mitochondrial inner membrane where its active faces the mirochondrial matrix. It mav be associated w
complex I of the mitochondrial electron transporr chain, andferrous iron substrate may be produced upon nicotinamidadenine dinucleotide (NADH) oxidarion. FECH is specilic for reduced form of iron, but can utilize other metals such as Zand Co'* and other dicarboxyl porphyrins. Accumulation of fprotoporphyrin rather than zinc protoporphyrin in EPP ndica
that formation of the latter is dependent on FECH activrty
Th e human FECH gene s locaredon chromosome 18q21has a single promoter sequence, and contains 11 exons. TmRNAs of =1.5 an d =2.5kb were described,which mayexplained by the use of 2 alternarive polyadenylation signals. Tlarger cranscripc s more abundant in murine er;.throid cells, sgesringerythroid-specilic regulation of FECH. A vanety of FECmutarions have been reported in EPP, ncluding missense, no
sense,and splicing murations, small and large deletions, and rnsertio[.
The inheritance of 2 alleles associated with reduced FEC
activity is required for diseaseexpression. This is consistent w
FECH activities as low as 15-25% of normal in EPP patrents
most patients, a disabling mutation on one FECH allele is cobined with a common polymorphism affecting the other alle
whrch produces less than normal amounts of enzyme. T
intronic single nucleotide polymorphism, [VS3-4ST/C, results
the expression of an aberrantly spliced mRNA that is degrad
by a nonsense-mediatedRNA decay rnechanism, which decreathe steady-srate evel of FECH mRNA. Inheritance of EPP n m
affecred families i s correctly rermed autosomal dominant beca
the IVS3-48Ti C polymorphism by irself does not cause disea

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 162/177
with normal subunits would have enzyme activlty'
ln rianc casesof EPP,FECH activrty is normal, and both free
EPIDEMI0[0GY.EPP rs the 3rd most comrnon porphyria' although
irs orevalence s no r precisel' known (seeTable 9l-2l lt is
describedmostly in whrte people. hut occurs in other race' a'
well, including blacks. ihe IVS3'48T/C polv-morphism is
common in rvhlicesand East Asians buc rare in Africans, thtch
would be predictive of a lower diseaseprevalence n populations
of African origin.
FECH is deficient in these cissues
blasts has been noted in the bone malrow of some patients'
however, suggesring har FECH deficiency sometimes mPairs ery-
rhroid heme synthesrs.Liver damage that develops in a small proportion of EPP
D.rt ienrss atrriburedro excess rotoporphvrtn. which rs insolu-
61 . ,n *ut.. and is excreredonly by hepari( uptake an d biliary
excretion, Some mav be reabsorbed by the intestine and undergo
enteroheDatic circulation. Excess protoporphyrin can decrease
hepadc 6ile formation and flow, form crystalline structures in
hepatocvtes, and impair mitochondrial function.
CtlNlCAt MAiIIFESTATIONS- ymptoms of cutaneous photosensi-
tivitv beein in childhood, and consist of Pain, redness,and itching
occurrin-g within minutes of sr-:nlight exposure. Swelhng may
resemblJ angioneurottc edema, These are referred to as solar
urticaria and are usually worse in the spring and summer
Chaptcr l . ThePorphyrias
triglyceridemra nd somewhat ower levelsol erlthrucYte pfo
poiphyrin an d increasedsunhght rolerancedr-rringpreBna
have beendescribed.
porphyrins and porphyrin precursols are normal in uncom
cated EP P
DIAGNOSISND DIFFERENTIALIAGNOSIS. diagnosisof EP
conlirmed primarilv by 6nding a substantially elevated conc
tralron of eryth.ocyre protoporphyrin, which is predominan
must be interpreted with care
The increase n plasma total porphyrin concenrratjon ln EP
often less than in ocher cutaneous porphvrias. Great care mbe taken to avoid light exposure during sample process
becauseplasma porphyrins in EPP are partrcularly subiect ro Prodegradation. Other findings rnclude normal levels of urin
porphyrrn precursors and porphyrrns.
Measurement of FECH activity requires cells containing m
chondria and is not widely available. Demonstration of nol
FECH activity and a greater than expected proportjon of
protopoporphyrin in erythrocytes is importalt in idenrify
variant EPP Dr..r..A tudies are increasingly important {or c
firming the mode of inheritance and for genetic counseling.
The development of life-thr€atening hepatic complications
EPP is accompanied by abnormal liver function tests, ncrea
erythrocyte and plasma protoporphyrrn levels, and incre
photosensicivity, Increases in urinary porphyrins, espec
coproporphyrin, are attributable to hver dysfunction.
COMPtlGATl0NS. Biliary stones conraining protoporphyrin
sometimes symptomatic and require cholecysrectomy. L
diseaseoccurs i; 1-2% of EPP patienrs, including children,
viral hepaticis, alcohol rntake, iron deficrency' asting, or oral
traceptive steroids, may contribute. Liver histology sh
markid deposirion of protoporphyrio in liver cells and
canaliculi. Pattents with procoporphyric liver failure, which

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 163/177
654 r PART . MetEbolicDiseases
resentsa severephenotype, most often have "null mutations" andthe IVS3-48T/C polymorphism in the nonmutant allele, bur somenay have 2 mutant alleles and autosomal recessive nheritance.The bone marror;r. is probably the major source of protopor-phyrin, even in EPP patients wrrh heparrc failure.
TBEATMENT. xposure ro sunlight should be avoided wheneverpossibLe,which is aided by wearing closely woven cloching, Oralbeta-carotene eads !o clinical improvement and greater toleranceto light in some patients, usually 1 to 3 mo after srarling treat-ment. In mosr adulrs,dosesof 120-180 mg daily will maintainserum carotene levels in the recommended ranee of 600-800 mg/dl . bur do.e, up ro J00 mg daily mav he nieded. Mildskin discoloracion due to carorenemia is expeced. The recom-mended producc is Solatene (Tishcon), lvhich u,.asdeveloped as adrug specrficallvor treating rhis direase, arher rhan nuirit ionalproducts that are less standardized. Beta-carotene may quenchsinglet oxvgen or {ree radicals, but does not substantially alcercirculating porphyrin levels. Be er rolerance of sunlight nayresult in tanning, which provides ddirional protection. Oral cys-teine may also quench excited oxygen species and was foundmole recently to increase rolerance to sunlight in EPP
Other measuresro darken lhe skrn may also be helpful. Thisma 1 be accomplishedby n.rrrow band UV-B photorherapr orwrth topical products such as dihydroxyacetone and lawsone{ndph thoqu inone ) . a lo r i c res r r i c r ion nd d rugs or hormonepreparadons that imparr hepatic excretory fr-rncdon shor.rld beavoided, and iron deficrencv should be corrected rf present.
Treatment of protoporphlric lir.er disease must be individual
coal may rnterrupt the enterohepatic circulation of protopor-phyrin, promote its fecal excretion, and reduce liverprotoporph;'rin conlent. Spleflectomy may be benelicial whenEPP s complicated by hemolysis and splenomegaly.Spontaneousresolution may occur, especially f another reversiblecause of liverdysfunction, such as viral hepatitis or alcohol abuse, is contributing. Otheru,ise! exchange transfusioo, plasma exchange,and intravenous hemin to suppresserythroid and hepatic proto-porphyrin production may be beneficral.
Motor neuropathy resembling rhat seen in acute porphyrias
sometimes develops n EPP patients with livet diseaseafter trans-fusion or liver transplantation and is sometrmes reversible. A rti-ficial lighcs, such as operating room lights during livertransplantation or other surgery, may cause severe photosensi-tivily, w.irh extensive burns of the skin and petironeum andphotodamage of circulating erlthrocytes in parients withprotoporphvric liver drsease.
NVirhcontinued progression of liver disease, iver ransplantation ma) be considered. But because ivel dlssar. may recur inthe transplanted liyer due to continued bone marrow produccion
of excessprotoporphyrin, bone marrow transplantation (BMT)
should also be considered f a suitabledonor is available.BMTdid ameliorate hver disease n a murine model of protoporphyria,
and led to remissionof protoporphyria in a patient who under-
wenr BMT for acute myelogenous leukemia. Gene therapy srrate-gies are und€r study in murne models. For example, a dual genetherapy approach allowed selection of hemaropoietic srem cellswith erythroid-speci6c expression of the cherapeutic FECH gene,leading to a progressive ncrease of normal erythrocyres and cor-rection of photosensirivity,
PR0GN0SIS-Typlcal EPP patients have lifelong photosensitivity,b can othenvise expect rormal longeviry Protoporphyric liverd ase is often life-threatenrng; however, the incidence is low.
PBEVENTI0I{.Symptoms can be prevented by avording sunlight.Avoiding agents that may cause liver damage may help preventliver complicahons.
GENETIC 0UNSEIING. NA studies are i reasingly mpofor genetic counseling, especialll'rn famili in which a chiadult has developed protoporphyric hepatopachy. Thisusually identify a disabling FECH mrrtarion and the IVS3-48polymorphism. In some EPP families, however, 2 disassociated mulations are foLrnd, with a pattern of aucosrecessrve nhericance. EPP may in-rproveduring pregnancy.
DUAtPORPHYRIA
Dual pctrpbyria relers ro patients \.ith porphyria who havecrenciesof more than 1 enzymeof the heme biosynthetic pathMolecular documentation is Lmportant in such cases
UROD mutarrons. An infant with severepotphyria was fobased on enzyme measurements, o have rnherited CPO deficfrom 1 parent and UROS deficiency from borh parencs.Cotence of UROS and UROD deficiencies *'ere described
pa ent wilh an erythropoietic porphyla. A iamily u.ith delicies of both PBGD and CPO has also been descnbed.
PORPHYRIAUE OTUMORS
carefully. Hepatocellular carcinomas complicaring PCT and ahepatrc porphyrias usuallv are nor described as containingamounts of porphyrins. Eryrhropoietic porphyrias can devlace n life due ro clonal expansion of erythroid cells contaia specrfic enzyme deliciency in parients who have develmyelodysplastic or myeloproliferative syndromes.
General
AndersonKE, SassaS, Bishop DF, Desnick RI: Discrders of heme biosysis: X linked sideroblastic anerniasand the porphyrias. In ScriveBeaudetAL, Sly \i/S, et at leds): The Metabah. and Molealat BaInherited Disease,vol II, 8rh ed. \es York, Mc(]ra\'! Hill, 20{l2991-3062.
Hjft RJ, MejssnerPN, An analvsis of 112 acure porphyric arracks DTown, Sourh Africa. rvednne 2005;8+48-60.
Kauppinen Rl Potphyllas. La ..et 2005;365:241-252.
Congenital Erythropoietic Porphyria
l)upuis-cirod S, Akkan V, Ged C, et al: Successfulmatch-unrelareddbone maro.* transplantation for congenital ervthropoicric porp
(Gunth€r diseasel.E,rr / Pedidtr 2005;164:101-107.Pjomelli S, Poh-FLapatlick N{B, SeamanC, er al: Complete suppression
symptoms of congenrtal erychropoietic porphyria by long term trea
with highlcvel ranstusion s. Erg 1. l M? d 1985;314:1029-r031.
Soljs C, Aizencans CI,.{strin KH, et al: Uroporphyrinogen III synrhasthroid promoter mutarioRs n adjacenrGAIA1 and CP2elements ausgeniral eryrhropoieticpo.phyti^. J Clin Inuest 2001;107:753-762.
VerstraetenL, Van R€gemorterN, Pardou A, et at: BiochenicaLdiagnoa faral case of Gunrher's disease n a newborn with hydropsJeralis Cl in ChemClin Biochem1993;31:121-128.
Acutc lnrermittent Porphyria
Andant C, Puy H, Bogard C, et al: Hepatoceltularcarcinoma n parients
acure hepacic porphyria: Frequencyof occurrence and related facto
H etatol 2000;32.9 3 3 9 39.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 164/177
t
2005;142:439-450
Ve1.erUA, Schuur-"ns MNl, Lindbers RLI': Acute porPhvrias: Patho8enesis
oi newological rianlfest..dons semin Liuet Dis 1998;18:43 52
SolisC, N{ariinez-Bermejo \, Naidich TB cr aL:Acute ntermirrent porPhvria:
Srudies fthe severe omozygousdomtnant diseasc rovide nsigh$ inro rhe
izat ionof a myth l 'enpe.t B/olMe d 1990i13:598-611'
Hereditary Coproporphyria and Variegare Porphyria
Hifr RJ, Meissne. PN, An analysx of 112 ac e po'ph,vric attacks iD Cape
Tor,n, South AfDca: Evtdence hat acute rnr mittcnt porphvia and varre
gare iorphv.ia djfie. in suscepribilir) and rerio Medi'ine (Babimofe)
Porphyria Cumnea Tarda
EggerNG, Coeger DE, PayneDA, et aL:Porphvria cutanea arda: N{ulriplic-
ity ofrisk facion lncluding HFE mutations, heparitisC. and inherked uro-
oorohvr inosen r.arborrla'e def i rrenevDrs DA 5,r 2002'4-:4le4Z6'
l l t ter ' r, i l , Porphrr i : cutrne.r arJa :n d re lareddr'orden ln Krdr'h K\ l
Snirh K, Guilard R (eds):Porphyrin Hanclbook, pa't II! vol l4 San Drego,
AcademicP.css,2003, PP 67-92
Erythropoietic ProtoPorphyria
Cox TNL Protoporphyria ln KadishKV, SmithK' Guilard R (eds)'Porpbviz
Halldbook, pa-tll, vol14. SanDicgo, AcademicPress'2003, pp 121 149
Goodivin RG, Kell V{, Laidler B et al, Photosensirivitv nd acute iver iniDrv
in myeloproliferative disorder secondarv to late onset Protoporphjrra
ca"r.i trv d.t.tion o{ a ferrrxhelatascgene rn hematopoietic cells Blood
11:1i90-1596.
ChaPtelg2 HyPoglycemia
cipitously o levels bar impair brain funccion,an elaborate
ulatory systemhas evolved.
The defense against hypoglycemia is integrared by the au
DEFIt{lTl0trl
There is evrdence rhat hypoxemra and ischemia may Poten
concentralion of <50 mg/dl (10-15% higher fot serum
plasma) represents ,vpogll 'cemia.
SIGI{IFICAI{CE1{O EOUELAE
Merabolism bv the adult brain accounts or chemajortry of
and chrldren can retard brain development and function. T
sient solatedhypoglycemiaof short duration doesnot appe
be associatedwrth rhese severesequelae. n the rapidly gror
brain, glucose may also be a source of membrane liprdstogether \^'ith protein synrhesis, t can provide structural plo
an d myelinatronchatar e mportant for normal brain matura
Under conditions of severe and sustained hypoglvcemra,
cerebral strucrural subslrates ma,v become degraded to en
usable ntermediates uch as acta!e,pytuvale, amino acids
ketoacids,which can support brain metabolismat the expen
brarn growch. The capaci!)' of rhe newborn brain to take uP
oxidizl ketone bodies is abour livefold greater than thar o
Glucoseha s a central role in fuel economy an d rs a source of

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 165/177
656. PART r MetabolicDiseasos
m€tabolize ketones, rhese alternate fuels cannor completelyreplace glucose as an essentialcentral nervous syscem CNS) fuel.The deprrvation of the brain's major energy source during hypo-glycemia and the limiced availability of alternare fuel sourcesdr-rring hyperinsulinemia have predicrable advetse corseqLrenceson brain metabolism and growth: decreased brain oxygeri con-sumption and increased breakdown of endogenous strucru.alcomponenrs with destruction of functional membrane integrit,v.Hypoglycemia may thus lead ro permanenr impairment of braingrowch and funcrion. The potenriating effects of hypoxia may
exacerbare brain darnage or indeed be responsible for rr whenblood glucose values are not in the classic hypoglycemic range,
The major long-term sequelae of severe, prolonged hypo-glvcemia are mental rerardation, recurrent seizure activlty, orboth. Subtle effects on personalrty are also possible but have notbeen clearll' defined. Permanent neurologic sequelaeare presentin 25-50% of patients with severe recurrent sympromatic hypo-gl1'cemiawho are younger than 6 mo of age. These sequelaemaybe reflecred n pathologic changescharacterized by atrophic gyri,reduced myelination in cerebral whrte matter, and atrophy in thecerebral cortex. Infarcrs are absent if hvooxia-ischemia drd notconrrrbure o cerehralmanifeslarions; he-cerebellums spared fhypoglvcemra s rhe sole insulr. These srquelaeJre more I ikelywhen alternative fuel sources are limited. as occurs with hvoer-insulinemia.when Lh eepisodes f hypoglycemiaare reperirive r
prolonged, or when rhey are compounded b1' hypoxia, There isno precise knowledge relaring the duration or severrry of hypo-glycemra to subsequent neurologic development of children in apredictable manner Although less common, hypoglycemia inolder chrldren may also produce long-term ner-rrologic defecrsthrough neuronal death medrated, in part, by cerebral excitotox-ins releasedduring hypoglycemia.
SUBSTRATE,]'IZYME,NDHORMONATI'{TEGRATIONFGTUCOSEOMEOSTASIS
lN THE NEWB0BN ISEECHAPIER107). Uoder nonstressed condi-tions, fetal glucose is derived enrirely from che mother t hroughplacental transfer. Therefore, fetal glucose concentration usually
reflects but i s slJghtly lower than marernal glucose levels. Cate-cholamine release,which occurs wirh fetal stresssuch as hypoxia,mobilizes fetal glucose and free fatty acids (FFAs) through p-
adrenergic mechanisms, reflecting p-adrenergic activity in {etalliver and adipose tissue. Catecholamines mal also inhibit fetalinsulin and srimulate glucagon release.
The acute incerruption of macernal glucose transfer ro lhe fetusat delivery imposes an immediare need to mobilize endogenousglucose. Three related events facilitate this transition: changes nhormones, changes n their receptors, and changes n key' enzyme
activitl'. There is a three- to fivefold abrupt increase n glucagon
concenuation within minutes to hours of binh. The level ofrnsulin usuallv falls initially and remains in the basal range forseveral days without demonstrating rhe usual bri sk response tophysiologic stimuli such as glucose, A dramatic surge in sponta-
neous catecholamrne secretion rs also characteristic. Eoineohrinecan also rugment growth hormone secrerion bv o-idrenergicmechanisms; grouth hormone levelsare elevated at brrth. Acting
in unison, these hormonal changes at birth mobrlze glucose viaglycogenolysis and gluconeogenesrs, activate Lpolysis, andpromote kerogenesis, As a result of these processes, plasmaglucose concentradon stabilizes after a transient decrease mme-diatel;' after birth, liver glycogen stores become rapidly deptetedwirhin hours of binh, and gluconeogenesrs rom alanine, a majorgluconeogenic amino acid, can account lot =10ok of glucose
tumover ln the human newborn infant by several hours of age.FFA concentrations also increase sharply in concert with thesurges n glucagon and epinephrine and are followed by rises inketone bodies. Glucose is thus partially spared for brarn utiliza-
non while FFAs and ketones provide alternative fuel sourcemuscle as well as essential gluconeogenic factors such as acoenzyme A (CoA) and the reduced forn of nicotinamide-adedinucleocide (NADH) from hepatic fattv acrd oxidation, whicrequired to drive gluconeogenesis.
In the early postnatal period, responsesof the endocrinecreas avor glucagonsecrerion o thar blood glucoseconcetion can be maincained. These adaptrve changes in hormsecretion are paralleled b1' similarly striking adaptive changhormone receptors. Key enzl'mes nvolved in glucose produc
also change dramatically in the perinatal period. Thus, thererapid fall in glycogeo synthase actrvitv and a sharp rise in pphorylase after delivery. Similarly, the amounr of rate limienzyme for gluconeogenesis, phosphoenolpyruvate carboxnase, rrses dramatically after birth, activaced n part by the sin glucagon and the fall in insulin. This framework can expseveral auses l neonaralhypoglvcemiaba'ed on inappropchanges In hormone secrerion and unavailability of adeqreservesof subs[rates in the form of hepatic glycogen, musca source of amino acids for gluconeogenesis,and lipid storethe releaseof fatty acids. n addition, appropriate activities ofenzymes governirrg glucose homeostasis are required (see
87-1) .
Ittl 0IDEB INFANTSAND CHlLDfiEN.Hypoglycemia in older inf
and children is analogous to that of adults, in whom gluhomeostasis is maintarned by glycogenolysis n the jmmed
postfeedin8 penod and by gluconeogenesrsser.eral hours ameals. The Lver of a 10 kg child contarns =20-25 g o{ gllrcowhich is suffcient to meet normal glucose requirements o6 mg&g/min for only 6-12 hr. Beyond this period, heparic coneogenesismust be activated. Both glycogenolysis and gluneogenesis depend on rhe metabolic pachway' summanzedFigure 87-1. Delects in glycogenolysis or gluconeogenesisnot be manifested in infanrs until the frequent feeding ac 3-4intervals ceasesand infants sleep through the night, a situausually present by 3-6 mo of age. The source of gluconeogprecursors is derived primarilv from muscle protein, The mubulk of infants and small children is substantially smaller relato body mass chan thac of adults, whereas glucose reqr
menrs/unit of body mass are greater in chrldren, so the abilitycompeflsate for glucose deprir.ation by gluconeogenesis s mlimited in infants and young chiLdren, as is the abiliry ro wstand fasting for prolonged periods. The ability of muscle ro gerate alanrne, the principal gluconeogenic amino acrd, maybe kmited, Thr-rs, n normal yotrng children, the blood gluclevel falls afrer 24 hr of fasrrng, nsulin concentrations fall apppriately to levels of <5-10 pU/mL, Iipolysis and kecogenesiactivated, and ketones may appear in the urine,
The switch from glycogen synthesis dunng and immedia
after meals to glycogen breakdown and later gluconeogenesgoverned by hormones, of which insulin is of central rmportanPlasma insulin concenlrations increase to peak levels of100 pU/mL after meals, which serve to lower rhe blood gluc
concentration through the activation of glycogen synthe
enhancement of peripheral glucose uptake, and inhibition glucose production. In addition, lipogenesis is stimulawhereas lipolysis and ketogenesrs are curtailed. During fastplasma insulin concentratlons fall to <5-10 pU/mL, and togewirh other hormonal changes, his fall results in acrivation ofconeogenic paihways (seeFrg, 87-1). Fas ting glucose concertions are mainrained through the activation of glycogenolysisgluconeogenesis, nhrbitioo of glycogen synthesrs,and activad
of Lpolysis and ketogenesis. It should be emphasrzed thaplasma insulin concentration of >5 pU/mL, in association wir
blood glucose concentratron of <40 mg/dl (2.2 mM), is abnmal, indicating a hyperinsulinemic state and failure of the neanisms that normally result il suppressioo of insulin secreduring fasting or hypogl;rcemia.

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 166/177
Chaptergz Hypoglycemia
in infancv an d childhood rtilect rnapproPnatc a(lapt' f()n to
iastlng.
CtINICAtMANIFESTATIONSSEE HAPIER07)
RITEASE*
PeApiralion'PaipLtaln ra(hy.ard)h o rTremuusmss
luryerNauSeaEm6Anqi(withormdloronaryneri6)
FTATURTSSSO(ITTDITHEREBMT1U(OP[IIIAHeadarhe'Mentalonfuscn'Vi5ualdurbancesJ aruy,diplop)
0rqani(eBonallyahange5lnJbit[10 onrentrateU)5art|lru5hringPale51he5,r5Dizine5i
Ahxia,in(oordinauonsomnolence,lelhaqySeizues[omaStrcke,emidq, phasDecerubmte]r ecortateo5ture
5ome0f tele e,nu|6 i I beatsMFd 'f epat$i I tie Yn9EadRmBi.b o3:ngaqenl5
G1\,1S4500
10%(12t126)
5%
\2/40)
10%
,;e' ,iii;^,
67./.10/1
I t r r l26 30 34 38 42 46
Gestationwk )
i1,/rnlft-.1971i47:8I1-88 l
.rremissed.Occasrolallv.hvpogl,vceniamaY be asymptomat
the mmedlacc ewborn period.Nervbornswirh h,vperinsulir
LncLuclcitterinessor tremors, apachl, episodes f c,van()sis
rulsions. intermirrentapnercspelJs r tachypnca, ,r ' 'eakr h
sugar o rormal Jcvcls; f rhe,"do not. orher dtagnoscs nu
considered.
3500
2504
50 0
ttaTuRtgSSoqATEDnHfTlvAllollFAuloiloMl(tRlro,sYSTEMt{oPltltPHnlNt

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 167/177
658 PARTX Metabolic iseases
CTASSIFICATIONFHYPOGTYCEMIAN INTANTSANDCHITDREN
NEONAIAT, RANSIENISMATLFORGESTATIONAI-GE,AND PRE.MATUBTNFANTSSE E HAPTEB07). hc csrirlatednciclencefsymptornaricypoglycernian neu,bornss I j/1.(l0tlhv ebirths.'lhis
incidences ncreasedevcralfbldn certain igh-risk eona-t.LL roufs (see ablc 92 2 and Fig. 91.1j. Thc prenarurcan dsrnrll for gcsrlrionalag c (SGA) nfantsar e vulneraLrlet> rhedevcloprrenr f h,vpogl,vcernia.he factors csponsiblcor rhehigh rcqoenc,vf hvpogllcerrian thisgroll. l, s well as n othergroLrpslrt| led lrrTablc 2 1, are claretl ) he nddequatel(]fesof livergl!cogen,musclc rotein,nd bod,vat rceded o susfil inthe subsrrirresequircd o rreetcnerg)DeeLls.hesenfaursar e
snrallbr ' r ' rrtueof prernaturirl or rrrrpairecl lacental rans
In confritst ro dcficiencvoa substratcsor etrzvntes! hc
signif icantns e in glucose.During rhe nirial 24 hr of lrf i: , plcoLrcenrratronsf acetorcefate nd Jl hVdroxybutyrate rrc li rr SGA niarrcs han n frdl temr rhncs, implving dinLnishcdscores, Lminishedat.v acid mobilization, mpaired ketogeor a combination of drese ondiri< >ns.imilishcd lipiclstorcmosr ikely bccause at itr ighceride) tcccling<>f ovbons rc
Asrociaredith nadequateubstnleafifiature ntymeln(lionnotherwiseonralneonatet
+enrturitl5rr llfore5tdt]nalaE,
Tranrienteonatalype rulinhmho rcsentn:lnkntofdabetirotfersna orqenathnaq€ll crdantwnB halchyxifdf ]f oxem:motlr,or
i]EONATAt,NIANTILE,R II.DI{OO|)TRSISTENTYPOGTYGMIAS
HornonaldirodeBH,rperr,n5m
llereiseK{rrh?'rneltaailGrhanneDaflinantKrpcnannelNDanrnanrqu(okne5el
|minarl htafiialethydroger5r liD,pelin5ulism/hyperamnnem5I1dftrme)A(qJredetadelornaBe|k$rti,(eceranrtndrome
n5.tlndlr iiratrl]n[lunl:']aLrfnyndror,rey nrry)oral ulton/rriatuqt{ongeIit,]lol15ofqlycojybrn
(ounterrcgulatoryormoneef lnryPrnftpcpltJ:fis,nhc redironhmrnoneei(i?niyAd€nocoftrdrcFtomcree hxr!Lld cf d 5ea5e
Ep ephr.neeni:enq
Glycogenolysi!nd9lu(oneogenelirisorde6
!aucc5ephoiphataieefuienryGSDal(iLrco5e'5-phospfrte ar'oca5el]fri,.n(rG5Db)
Arnyl0,5 lur05ida5edebranrflnqnzyme)eli(ierryGSD)
Lir'efh0rph0lla!eehden(yCSD6)Pfo5phory5e rase eii encyGii 9l
Gy.oqentnihetai?ef(enq G5D])
Fru.to5€,6 ihospiat;ieefide1(y
Ffuvatilarboxyie efrenq
6alattose
flaeditrryrurnle toehne
Lipolysisiioderu
FattyaddxidaondirnrdeB
Gl| t ne'ransporGrencqq !inrarycirnitinee6arrc,
[an t]nealm o!tranlleD!eCefriienij/[amitrr:eeri cie denflenr/
[a.nitce a rtcyrrandeTdseden(e].cy
ClD,qroqcirifate ealer|],yFinrrlnrni,r,la,e9(rccGJ5mhdre
lerondaryrnitne efraieni5very nq04 .nreiiumrhofl hain.y cAdehydrc_oene
oTHIR TtotoclEsSubrtrate-limihd(€totrhypo!ty(ginii
Poisoninl rlgj5arqare5
Ord ypocy(em(aqe n6
tn5ut1
Prlrprunolol
P r a n d n e
lisopfamiCe
A.keetri nrpe)-hypcg){ n/aor ratepolslrn)Trmeih0prmulhmetl.omzoh!r /h cnal;iluE)
Liv€rditaase
leve yrdomeflepitr
I rhos5
fleFtonr
Amino ddandorga0i(addisorderslVapsyrLrprn.. 5ta5ePnpon(acdFmid
[lathyharffaridemia
1'rosinc55Glutirr(ddurnI'ilydrcry melh/lohrl,: cidLrrid
lyttemic isodeE5P!5s(a( nnmaAarcfi'asecieiing-'-rniulniieErofltnrior
)Hearl fai lue
MalnLrlon
lVabiorptonAni nsu etepton[bodiesirr in5LrJnl $dies
Neondayperuisoiily
Rerrala ,'re
DErrhea
Burn5
Shork
Fcneur!cal
F5e,Jdahipo!em hrrcrytoli5,otqthenraiL(e55r€n5uinhezpyf n!u ncependentdbeiesne t,.
taitt:oLifl55enundo0{at,oFdL ping lrCome)fu parum dl,.ia

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 168/177
should be treatedwith diazoxide.
l]{fAl{TSEOBI{T0 DIABEfIC oTHERSSEf CHAFIEI1o}. of the
transient hyperinsulinemic states, infants born to diabetic
mothersare tfuemostcommon.Gestadonal iabetes ffects ome
ins themto hvposlvcemia."trloth..r
t"hosJiiabeteshas beenwell controlledduring preg-
listed n Table 92-2.Infants born with crytbroblastosisfetalis may also have hyper-
insulinemiaand sharemanyphysical eatures, uchas argebody
size, with infants born to diabetic mothers.The causeof the
hypirinsulinemia n in{antswith erythroblastosiss not clear'
PERSISTEilTRRECURRET{TYPOGTYCEMIAilll{fANTS ttlDCHItDREt{
HYPERISUUiIISI|, Most children with hyperinsulinism hat
causes ypoglycemiapres€nt rl the neonatalperiod or later in
ChaPlolg2 Hypoglycenia
allv it is 1st evident n older children. nsulin concentration
inaooropriarelv levatedat the time of documenred y
elviimii; *ith non-hyperinsulinernichyroglycemia. pla
insulinconcentrationshouldbe <5 puiml and no higher
administrationof insulinas a {orm of child abuse Muncha
by prory syndrome), SeeChapter 36'2.] Provocative ests
rolbutamideor leucine r€not necessaryn infants;hypoglyc
92.7) .The measurement f serum GFBP-1concentrationmay
diagnosehyperinsulinemia. he secretionof IGFBP-I is acinhibited by insulin; IGFBP-1 concentrationsare low du
hyperinsulinism-inducedypoglycernia.n patientswith spneousor fasting-induced ypoglycemiawith a low insulin (ketotichypoglycemia, ormal fastilg), IGFBP-1coflc€ntra
are significantly higherThe differential diagnosis of endogenoushyperinsul
includes di{fuse p-cell hyperptasiaor focal p-cell microadenThe distinction between hese wo major eotities s imPo
becausehe former, f unresponsiveo medical herapy, eq

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 169/177
66 0 PABT I Metabolic iseases
TYPE
tpcrad(
IflPOGTY(ETIIA/
MA(flIXOMIA IIYPERITISUIINITIIA
P,esrntb h ltrlodecelewrcn 5tCa)5oweeb i e
ASS0OATIDtllllftL, ntJm $I0 R[(0t1tr,ltttDtDFAMILY 8t0(Hti{Gt,0R t rDtcfl. SuRGt(AtHIsTORYMOLT(UIARtfI(TS MOITOTAIIATURTsMI}IAGTMEI.ITPfNOA(H
Ne_oatve ItURl/KN6)
MLrtalions0talwaysiCentiReddifu5ehyperpla5ia
Los5Fraero4go5itynmicrc,rdenom,Iouj
l !5Ue
6enerallypooI
niy resp0nd
benero
man0
0ldZoXrCe
l:rld pai(reiteatl]rJl
l -a3l t rodc9 rr5rn i
nlde miirljdderomi
iulr.rtd !t%
5uLto:3anarealedo.l))'
!urqery5Lrlinot eqIed
hrtd pan(rei redcn!ni l f
nreotG anrllmeE 5)uqe
luju3 lol e(jLco
Nolrerommend,.d
Pn(XNo
[rrelenr
Gu3ded;db
nel i tu5derelcp
ofFatie
nvpo!1apeAh[npanrral
riTmftne
shohsq
nui i in- d rus
n/perptlil]irded
[xrrlent
L{celleri
Fr(eentlol
fyp0qr/r
ai50iat€
enbr)o'a
tumo15!!1hepitob
tun
retes5e
domrnart
Autc5omil
Be.l( h
wecemann
5ln0i0tne
[onqerild
d sdrderslgyrolEnon
Presen,lbrrth sel/eren 5tdaysor'rcekiflitu
LlnurLl2 [lcdera(enletsuallyprtnan0tage
'Jnu5Lral ll0dpr,ttcnietsualypcll m0 laqe
Pre5eillbirt[ Mcderate,sNmaneousrcJoivrsosi6mo Fage
Nol 5ua l\,loderare/onseto5iI moofage
tUlJKa6) (o[sa uinityeaturen Poortome puiat0n5
6fu(0kdie cvariig) None Verymd 0\omea5e5qene ex(elent
Gluiamale ModesiypeBfitrnoftmiiVeq 0rd0'lehydrcgena'e e)((elent
(activalnq)
Dupiratinll/mpdntnqva(mgloi5a,onphalorele,oodn hromo5ome hemlhypeffiophyl l c l5 l
Po5live
Po5:1ve
Neqalve
NeQate 6ood htTtann0!esuppernenr
Phosphomanro5e Hepatomeliltvomitng,i50meE5eefr:enc! intractableanhed
l lear totrrl pilncreelectom\i dcspite which hypoglycellra tnavpcrsistor rLabetesmcllitusmav ensueat somc irtcf frme.Bv corri r r r t . t . r . : l , t . l r r r , ' r n r . d iaqno 'eJ p r r , , l ' . r r r r re l r ' ' i n r r , r , l ' e r . r
nvch pcnnif loc:rlrzed urarivc esectionwith subscqLrentormdlghLcosc rctaLroLisrn.Lrour 509/oof rhe au<rsomal recessi\r )r
spordclic orms of neonatal/ inlhlt i le h1'perinsulinisnrre dre roiocal n-icroaclenonas, rhich ma,v be t l ist ingLrishedrorn rh cclif fuse orn by thr lirttcrn of insulin responsc o sclectivensulin
secretirgoguesLniusctl nto irn arrery suppl,ving fhc pirncreas '!.ithsrmpling viu rhe heparic vein. Positror enission tomographv(Pt-l scannnlf l) sinq 18 f luoro L <1opa an disringLrishhe diffuseform (ulifornr lluorrscence hroughorLt hc pl crcas) ion fhc
5U85TMTIS6lurosPireeiacytirdrl(eloft5L3ataltu l ca (
HoRMollt5lnrutntortl5ol.lrohftromoneihl.crine,hyrod-stimutingFrmoner3F3P
'6 urdgdr,l rqlkq rhm mumf I mq V r M'M!:r!rc0fte0n
! bebreoi|1erq(iqondmiii{,m0n iem9l!(seol>40mg/d: lifl gu{dgongMndther'me
rf hy".0911{em,rnqy 5uqq6tia hypernlulmrir tre wt zdeqeareepdtk ['(o,;enores ndnh(rglirdEe.o,t s4mei I dnm0nlis eel'alrd 100-100,M, i3'der rrivarg mlbrm ot gidamal€
6igP , n5!ln l€oroMh'?r1rndinqorerr
locrl fomr (iocal uprakc <rf 8lluoro I- clopaand localizcdrescence)Scc rig. :,123.].
ILrsulil-sccrcfng macroailenomls are rare in chilclhooc
rnay be diaenoscdprcoperafii 'elyvi a CT or MRL The pialcr'cis o1 insulin alrrc, holvever,cannoc disringuish he lfomenti(ncd cntit ics.Th e diffuse or nricroaclelomarousorlttislet cell hypcfplasia ep resert a vnrietv of eeleric defects essible or abnorrralit ics n the erdocrine pancreas haracterizaLronomous ls l in secrctiol fhat is nor appropnarelv rcclu'hen blood glucose decliles sponfarreousl] ' r in resporsprovocafi\.emaneuvers lrch as fasfins (scc abies 92,r- a||d8). Cllinical, riochcmical, nd moleculergeneticapplo:rchespermit classilic.rt ionoI congeniral h,vpcrinsulinisnr. ornterrnednesidioblasrosis,nt o disrincrcnrit ies. 'ersisrcnr vpesulincmic hypoglycemiaoI infancy (PHHI) nray lre nherircdsporadic, s sclcre, ancl s causedby lrrutirf ions Lr hc rcgulaof rhe porassium hannel ntimately nvolved r Lrsulin sccrcby chepancrearicB ccll (Fig. 92 2). Nororally, glucose ntrv
th ep
cell s enahledb-v hc non insulin-rcsponsive lucose rporter GLL-l' l-2.On enfry, glucose s phosphorylateclo li luc5 phosph.ate by rhr cnz,-rne glucr>kinase, enabling gluc
I ilypedn!u[[emiapasmansu,n2 lJ/mL]r2 |]ypofaftyacidemiapaifidree tlya(ids 15 flmo,/l)I HypoketonempldgmaFlrydrcxybutyrdte:<2] mmo/i)
4 lnappropflaielly{emrie5p0n5poqlucagon,:! iV decqucoie40m_q,/dll*Cependron en5i!iryfnrdn5s?lfmn5hnlqLd lomron 5.ilE0d DN,ral: ypqtFrma. nfdn15rid Le0niIEl5refiq ]VA d 0,):
ladwn\hrytd ed,P\it)ehn,\\8aunder.?002p l5 l59

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 170/177
A(UT[SYMPTott'lSRESIIIT
su5pe{tyFllniulinemiar alty dd xidande{KLfpre*nt,uspetfetothcnnone
hotm|]neeasLlreremsnTabk2-5
piruilaryi5ed5e,rboth.dm ohospal or omonaest g nd elloimaEng
pignentdtnhdrenaailuE);5hlurend eurcqlc 1alu5il0itrrysea5e)
when cLrleymplorxsrcsent
b Pituitary-adrenauntton slngrqrn,nein5ulintmu,ltone5t nd akd
syn0lome,e(
Pancreatic Ce
Gl!cose
Chaplergz HyPoglycemia
rLlarions.nofabl,v Arabic and Ashkenazi Jervish communi
u,here r nay reachan incidence rI bout 1/2,500,comparedu
the sporadic ates n rhe generalpopulation of =1/-50,000. h
auroiomal recelsive forms of PHHI t,vpicaliv Presenf in
/Glulamale
//
+GDH
a-Ketoglutarate
oo
srMuLArEp_./
-r$:
"rf\{'l'N\
BESTING
gL'=:a

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 171/177
062 PABT t MetabolicDiseases
(0 DfloN
N0[naHypern!rnerniaK:tolir'yprgre|r
futly (d.rd;. lisol:rl l lrD0pilurdr5mddrcna5Jfliren.ytzimeetcenti
ilur:D5eiorpiataleebi herrroiploryla$
hucos?,6 rphc5pl'alajeGl aaicfn J
Fludolr ntoeran(e
IIYPOGTYGMIA
0Reautrc4l5ewTe
severe{hm[5ed ea
5everc,ith
miJsedeal,4oderdteithmi55ec eals
te\,e,ethm$edmea
Severeon5lanl
Modetule! lh astng
[lildmoderire
!everewith5inq
Aiier lkormkpadurt5
Aftertuctose
URINARYI(ETO5OR TDUONGUGARs
00rcrcnuraH
iemnularci0nura-^elonuna(erorLrda+(,oto,ruda+[etonJla+0 Ketones;ii)+0 K."tonei;ir)+
HEPATOMEGALY
0ll
c
0 o+Abnornawr ufr:oltct-H
Deta50|ei . (0ndl00ardid$!ednI iete(c 'abq:e] idJndf te5F5tn! t } 'ma]h( f0df f6e;1
irnrnediete neu-Lrorn eriocl irs nracros()rlic reu,horns r,r ' irh aweighr >,1.0 g and scvere ecLrrreltf )r persisreLrtvpoglycernia
manifesting,n lhcinit iLrl
ours or days of l if i.(, lucosc
infusionsas hJgh rs 1.5-20 /k/min and frerluent cec[ngs ail ro rnain
rail cuglvccmra.Diazoxide, vhich:rcrsbv opening, r '" channels(see ig. 92-2). fajls o concrolhy|.Tog)vcerniaclequarelv. omato
stlrrirr. \,hich nlso opels K111 nd inhibrts c;rlciunr 1ux,mav bepa r t ia l l y i i cc f i vc n =50 i ' , o f L ra f ien t sseeFrg .92 -2 ) . -a lc iL rn r
channcl hLocLin.e gents have had rncorsistcnr cticcts. \\ iheLrallecrerlparicnrsarc Lrnrcsporrsiveo thesemelsures.pancrcatcc
tonry is st ronglv rec()rnrrendedt) avoid thc long rcr r neurolt>gic
secluclac i hr poglvccrria. i surgerl is Llnderfaken. rcopcrarire(i l or N{RI f irclv rcvcalsat isoiafedaden()[r.r,\,LrLchvould rhcnpcrmit locrl fcsccrior).lrttaoperativeuLtrasonogrphv mav rden
tif,va small irrpllplble acienona,pernirung local rcscction.Ad e
lomls ofren present in lare inlancv or earlr chilclhood.
Disringuishrng Lrcnvccn ocal and diffusc cascs oi persistent
hvperinsulinismha s bccn artcnrprcd n sevcrai vars. Preopera-rivcll. , ranshcpirt ic (rrtnlvcin cathctcri?irt ion nd selecrirepan-
crearicveDousSaLIplir lg () neasure ilsulin rnav localizc a focal
lcsion rom th e stcp up in insulin colcelfration rt a speciiic ite.
Selective athcrerizariol of arterial branchessupplying the pan
creas, ollo\cd br infusion of a sccrct:rgoglrcLrch s crlciunr an dporral veill srrrrplrrrg or insulrn concenlriloon ertenal srimuLa
fi()n-venous arnplrlgl rna,vocalizca lcsion.Both eppfoaches r 'e
highlr- invasr"e. restricted o speclalized enfers. rnd not Lrri-
iorrrly sr.rccessfuln clist inguishing he loca fronr the diffrLsc
iorms. l8F llbc)cd I clopa cornbined wirh Pt.T scuniLrg is :r
pornisirg, rncani t() disrin[juish hc iocal frorn rhc c]if fuse esions()f hrferinsulinrsrnLrnresponsivco mcdicdlmlrnaecrrcnt Fig.92
.1). I-hc'gold
sranciard" cmarns rltraopcr.t iyc histologicchar
ilcrcri7.lcio11.iffusc h,rperilsulinisll is chdrrcferireclbv lrr14e
cclls \.\, ithrbrrornally
large rtuclei,whereas ocrl ddenomat()Lls
l cs ions l sp l r r y m i l l i r nd nonn. l B ce l l nL rc lc i - l r hoL rgh URI
nrutilf l()ns.rc prcscLrfn both 11pes, hc focal lcsio s alisc bv arnrrcll) irrr)sr rI rrrit terrally lnprinredgrou'rh inhrbrtorygelre ll
nrtefnal chronlos()rne 1p il associ:rf iorlwith pafcrlrxl rr:rlrs
orission f a nruritcd .S{-iR or K|16- 2 prrcrnrl chr'onr' :rsomeI pr.
ThLrs hc rrrcrl iofm representsa cloLrble rt ()ss oi nrarenlal
rcpress()r nd trrnsrlrission f a pitcrnel nrrrrrrt ion.-ocalercision
of focal . ldenonraftrusslercelL yperpl:rsiir csulfsLr 11cr.Lrcvirh
lrrt lc or no rccurrc rrcc- or rhe clif iuse ofnr, rrcrr tofrl resection
oi 8.5-90'11,i thc p.rrcrc.s s rcconrrncrrrled.hc rcer rotal pan-
crcilfccrorrr\ reqrrired k)r rhe diffuse hi'perplasric lcsions is ,
hor,r 'ever,ifel rss()ciatcd "vithpcrsistcnfhvpoglr'ccrrirr virh rh e
later dcr.clopmcnrof hypelglvcenril or frank. irsLrLiu cquirurg
diabctcs ncllitus.
Further resecrion i thc rcm:riningpancrcirsnril)_ ccisionbe necessar,vi hypogli.ccmil recurs alld cannot be cortt()l le
medrcaimcaslrrcs, uch rs the Llsroi somdtostafinor diazoxLxpcricnccdpcdiatric sLrrgeorsn rnedical cntersequippeprovide dre ncccssnrvl)rL1)pcrafivend posropcrlt ire care, drrosticev.rlLrafxxr! ncl rnanagernent hoLrlcl crform srrgersonrepaticnrswh o hlve beeu managcd rcdically,hyperil lsrmi a and ht po.qLvcemLaegrcssover nonths. This is siurilarvhat oc.Lrrs n childlcn wirh rhe h,vperlnsulincrnicyL.og[1
sccn n Beckuith-Wiedenann syndronc.It hvpoglrccrrria sr rrrrrrifests ern'ccn3 ancl 5 rn o oI ag
later a rherapeutic rlal rLsing redicelapproaches virh dieic1e.onatosratin, lnd freqnent ccdings au be rtteDfted fo
to 2-4 wk. l 'arlurc to marntain clll l l lcerriit with()ut undcsir
side effecrs rom the drugs miy pronrpt the leecL irr surg
Sone successn suppressrngnsulirr clcase lld c()rrecnngh,
gJlcernia n pirt ients ii ith PHHI has been reporrcd vi th thc
ol rhc long-rcting som:lt(rstafirr nalog octreofLde.Most casneolaral PHHI ,rrcsporaciic; amllial fornts pennit !,cncti ' : oselingon rhe L.asis f anncrpared utosonral ecessivenherita
,\ 2nd iorm oi farril i l l PHHI suggests utosomal domininhcritancc, Lrechnical eatures enrl () bc lcssscr,efe, nc looi hypog,lvceLlJas nosr likcJ1',brrr rrot exclusLvell-,r> obcvond thc rnrrnediatc crvborn period errclusuall]. bclondper' iod ) i \t 'eanilrgat aLraveragcaec rr onset of dbouf I rrbirth, rnlcnrsornia s rlr 'clv obsen'ed. urd responsc o cli ir?ois alnrosr Lnifbnn.Thc lrrit ial presenretionLral be dclal'cd
rarely occLrr s ldte as l0,vr, ulrlcssprovokecl bi 1:rstinggeneoc bisjs ior rhis .rurosornaldonrinant f ' :rrrnha s ror b
cleli learedrt is nor alu,rlr l inked ro Kl16-2l-lt iR1. Howcver
activrt ing nutati(r1 in ,5lucokrrrases transrnitcedrt ln eut
r n , r l J , , r ' r 'r l r ' r n . r r r . , r J n r r l \ r i r r u r \ \ l r e \ ( r ) t . F e n r r ' ('
sellng or-a j0'] l rceurrence arccan bc
given oriuture
of|spr
A .lrcl iornr of per-srstenrllHI i\ .rssociared it h mild
asymptonaric hypcrammonemia, usualLr as a sporadic oc
rcnce. althotlgh dominarrr inhcrirancc occurs, Itresentafrrrrorc likc rhe i lLrtosonrirl onrinant for-nr han the aut()s
recessi\.eofrn Dier ancl Ji:rzoxidecorlrrol symptonls. )Lrtp
crcatcctonrl nrrlv be ncccssir\r n sor'ne ases. hc associarrhl.perrnsuLiLrLsrrnd lrvperammolemia s calLscd y err rnhc
or dc novo girirrof funcfion f iLrfation rrl the enz)ine gLuta
dehvdrrrgellasc.he result ing ncrcrsc ll glutarrrirte)xid:lf i(
the p,rncrcntic ccll rrrses he ATP conccntrrrior ancl,hcnce
rario of ATP:,{Dl \\ 'hichclosesK.r-rr,elcling o membranede
la r i za t ion , a l c i rLn rn f lux . nd nsu l in cc rc r ionscc ig - 92 2
rhc livcr, hc cxccssrvc xidation oi it lutarndfc o [] kcroglt it i
nriry gcnerare lnrnronir alrd divelt glLrtnmdte Ionr lr

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 172/177
Chapter92| Hypoglycemi
ttFtCT f 2+36HfiFlsT ll PLasMA
GIYCXT(fitsm 5E 06UKr60ll
FASTED
JT
J
JJ0-rJ0-.rJ0 .l,J0,tJ0-+J0 !J.
T1,|,|
,|T0,t0-t11t
LAOATE
No0ralNomalNormrl
KNONES ALAIIINE
T IJ., Nllrmdl
11 lJ
1I JJT1 JJlt 111T JI1T JJ11 tl, I J, I J
GLUOSTI
I
INsULIN
11Jftntraindoted
JJJJTJt
ALANINEUPID5
Nofma
Norqa rt
liorma
Abao|nalNofmal
NoTmal't1
Noflrl
Noinral
ftNomi
N0[]ti
URKKID
NomalNorm,rlNonnal
1N0ma
N0ma'f'l
Noma
NOIA'ttlornal
NomalN0nna
TTN0nailornalT1NOIMA
N0ma
' f 1'f 'f
J JT TT 1
proc
cJrL)
w r h
d iso rde rs i t hc K11p he t r t r c
occurs il ntluv oi thcsc infirnrs- )if fuse rslcr ccll hvp.cr-plasia
occLrrs!l ini.rrltswirh hvpoglrcenli,r ' lhe dr.tgrrosrrcnd dlcrr-
I
\Yilnrs t luuor, heplrobirrstonre. rclrrnrI carcir]olri l, gonadttrL)nre. :rndrhebdonl,voslrcotrit . Ihis o"'crgro*'rh synclror
tufc5 rrd paltcrnsof transmrisir)rr. vpogllcemia ma,v eso
\!ccl\ to mollths of meclical heraP\- )ancreatic escction
rlso bc neecleJ.
L)irorilersof proccin .e,lvc()svletionsLril l lv rcscnr with ne
\
o l f r r ( n I \ \ r f h d r f i u s c n r r m r r i e o r r g c n i r . r lr r p c r i n s u l nn r ' l ) r f t u s c r P
rorrr r . r l . r: : t rr. rr,c :suc or , rrt l rrmrn.r Ir (1, l i i fus, : f lnlc of l ! l l )o
' t .1t r(nr.H. le. rd i prncr(: r\ i . r . r i lo i f . rr. Lrs l l l .D. ls lFoL.rl l r 3l
, , t n . r c . r s r Jl S I l l f O l . \ u 1 - ' t . r l cr s r , . r l i : i Jn d r t h c r r l o i d r . p L r r t $
ro,rrr l p. rrcri . rt i t is{ t l r l r r r r ' r . L: \ \ \l (^\ Jl , ndmrl pl rnrt tet i . ns
n . r r o r o a l l S l : l ) O P . \ u r r i l c n : t l ) r l r r r e r c . r t i c h c . r . l r ' t h c o t r s t r r r r r i
r c s lo f l ) r l ) l g r I l , r r d \ . l h r l d r c r l ' \] ( , s p , r r l r ' h i . t t l c l p h . r l

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 173/177
664 PABT r ilelabolicDisoases
and hypoglycemia seeChapter87,5).Thesedisordersare oftenunderdiagnosed,One entity associatedwith hyperinsuLnemichypoglycemia s caused by phosphomannosesomerasedefi-ciency,and clinical improvement ollowed supplemental reat-mentwrth oral mannose t a doseof 0.17g/kg six timesper day.
After the 1s t 12 mo of life,hyperinsulinemic tates re uncom-mon unril isletcell adenomaseappear sa cause fter hepatientis several earsof age.Hyperinsulinemia ue o isletcell adenomashould be consideredn any child 5 yr or older presenringwithhlpoglycemia.The diagnosticapproach s outlined n Tables92-
7 alnd92-8. Fasting or tp to 24-36 hr usuallyprovokeshypo-glycemia; coexisting hyperinsulinemiaconErms the diagnosis,provided hat factitiousadminislrationof insuhnby the parenrs,a form of Munchausen yndromeby proxy, is excluded.Occa-sionally,provocaciveestsmay be requrred.Exogenously dmin-istered nsulin can be distinguished rom endogenousnsulin bysimultaneousmeasurement f C-peptide concentration. f C-peptide levels are elevated,endogenous nsulin secretion sresponsibleor the hypoglycemia;f C peptide evelsare ow butinsulinvaluesarehigh,exogenousnsulinhas beenadministered,perhapsas a form of child abuse. slet cell adenomas r this ageare treatedby surgicalexcision; amrl ial multiple endocnneade-nomatosrsype iVermer syndrome) houldbe considered. nti-bodies o rnsulin or the insulinreceptor insulinmrmeticacrion)are also rarely associatedwith hypoglycemia,Some tumors
produce rnsulinJike growth facors, therebyprovoking hypo-glycemiaby interactingwith the nsulinreceptorThe asrute lin-ician must alsoconsider he possibilrry f deliberate r accidentalingestionof drugs such as a sulfonylureaor relaced ompoundthat stimulalesnsulinsecretion.n suchcases,nsulinand C-peDtide oncentratio[s n blood will beelevated.nadvertenr ub-iriiution of an insulin secretagoguey a drspensrngrror shouldbe consideredn those aking medicationswho suddenlydevelopdocumented ypoglycemia.
A rare form of hyperinsulinemichypoglycemia has beenreported after exercrse. 0hereas glucose and insulin remainunchanged n most people after moderate,short-termexercise,rare patientsmanifesrseverehvpoglycemrawith hyperinsuline-mia 15-50 min after rhe samestandardized xercise. his {ormof exercise-inducedyperinsuhnism ay be caused y an abnor-
mal responsivenessf p-cell nsulin releasen responseo pvru-vategenerated uring exercise.
Nesidioblascosisas also rarely beenreported after bariatricsurgery or obesiry
END0CRINEEFICIENGYypoglycemia ssociated i!h endocrinedeficiency s usually causedby adrenal insufficiencywith orwirhour assocratedrowth hormonedeficiency seeChapters 58and 576). In panhypopituitarism, solatedadrenocorticorropichormone (ACTH) or growth hormonede6cienc,.',r combinedACTH deliciency lus growth hormonedeficiency,he incidenceof hypoglycemias as high as20%. In the newbornperiod,hypo-glycemiamay be the presenting eatureof hypopituitarism; nmales,a rnicrophallusmav provide a clue to a coexistentdefi-crencyof gonadotropin,Newborns with hypoprtuirarismoften
havea form of "hepaticis"and the syndromeof septo-optic ys-plasia.When adrenaldiseases severe, s in congenitaladrenalhyperplasia ausedby cortisol syntheticenzymedefects, drenalhemorrhage, r congenitalabsence f the adrenalglands,distur-bances n serum electrolyteswith hyponatremiaand hyper-kalemiaor ambiguous enitalsmay provide diagnostic lues seeChapter577). n older children, ai lure of growth should suggesrgrowth hormonedeficiencv. yperprgmentationmay provide heclue to Addlson diseasewith increased CTH levelsor adrenalLrnresponsivenesso ACTH owing to a defect n the adrenalreceptor or ACTH. The frequentassociation f Addison diseasein childhood wich hypoparathyroidrsmhypocalcernia),hronicmucocutaneous andidiasis, nd other endocrinopathies houldbe considered. drenoleukodystrophy hould also be considered
in the differential diagnosis of primary Addison disease n ochildren (seeChapter 86.2).
Hypoglycemia in cortisol-growth hormone deficiency maycaused by decreasedgluconeogenic enzymes with conisol dciency, rncreasedglucose utilzation due to a lack of the antanistic effects of growth hormone on insulin action, or failurestrpply endogenousgluconeogenic substrate In the form of alanand lactate with cornpensatory breakdown of fat and generaof ketones. Deficiency of these hormones results in reduced coneogenic subsrrate, which resernbles he syndrorne of ket
hypoglycemia. Investigaron of a child with hypoglycemia, thfore, requires exclusion of ACTH-cortisol or growrh hormdeficiency and, if diagnosed, its appropriate replacement wcortisol or growth hormone.
Epinephrine deficiency could theoretically be responsiblehypoglycemia. Urinary exctetron of epinephrine has been dimished n some patients with spontaneous or insulin-induced hyglycemia in whom absence of pallor and tachycardia was anoted, suggesting that f ailure of catecholamine release,duea defect anywhere along the hvpothalamic-autonom
adrenomedullary axis, might be responsible for the hyglycemia. This possibrlrty has been challenged, owing to the raof hypoglycemia m patients with bilaceral adrenalectomy, pvided that they recei.'e adequate glucocorricoid replacernent,because drminished epinephrine excretion is found in norm
pa ents witb repeated insulin-rnduced hypogll'cemia. Manythe patients described as having hypoglycemia with failure of nephrine excretion fit the criteria for ketoric hypoglycemia.
Glucagon deficiency in infants or children may rarely be aciated with hypoglycemra.
SUBSTfiATE IMITED
Ketotic Hypoglycemia.This is the most commor form of ch
hood hypoglycemia, This conditron usually presents betweenages of 18 mo and 5 yr and remits spontaneously by the age8-9 yr Hypoglycemic episodes typically occur during periodsintercurrent illness when food intake is limited. The clahisrory is of a child who eats poorly or completely avoids evening meal, is diflicult to arouse from sleep the followmorning, and may have a seizuaeor be cornatose by midmo
ing. Another common presentatio[ occurs when parents sleepand the affected chrld is Lrnable o eat breakfast, thus prolong
the overnieht fasr.
At the time of documenred hypoglycemra, rhere is associa
ketonuria and keronemia; plasma insulin concentrations
appropriately low, <5-10 pU/mL, thus excluding hyperinsulimia. A ketogenic provocative diet, formerly used as a diagno
!est, is not essential to establish the dragnosis because ast
alone provokes a hypoglycemic episode with ketonemia
ketonuria within 12-18 hr in susceptible individuals. Normchrldren of similar age can withstand fasting wirhout hvglycemia developing during the same period, although e
normal children may acquire these features by 35 hr of fascinChildren with ketotic hypoglycemra have plasma alanine c
cenffatiols that are markedly reduced in the basal state after
overrught fast and dechne even further with prolonged fastAlanine, produced in muscle, is a major gluconeogenlc precur
Alaoine is the only amino acid that is significantly lower in thchildren, and infusions of alanine (250 mg/kg) produce a ra
rise in plasma glucose wrthout causing significanr changes
blood lactate or pyruvate levels, ndicating that the entire glu
neogenic pathway from the level of pyruvace is intact, but tthere is a deficiency of substrate. Glycogenolytic pathways
also intact becauseglucagon induces a normal gly'cemic espo
in affected children in the fed state, The levels of hormones tcounter hypoglycemia are appropriately elevated, and insulin
appropriately low.The etiology of kerotic hvpoglycemia may be a defect in a
of the complex steps involved in protein catabolism, oxidat

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 174/177
deaminatron of amino acids, transamination, alanine synrhesis,
or alanine efflux from muscle. Children with ketotic hypo-
hypoglycemJa-
GLYCOGENTOBAGE ISEASE. eeChapter 87.1.
Affected untreated children manifest growth {ailure' mental
continuous gastric feeding. The dayome feedings are given eve
34 hr: 60-70L of the calories as carbohydrate low in fructo
an d qalactose, 2-15% of rh e caloriesas protein, an d 15-25%
of th*e alories as fat. At night, a small nasogastric cube s passed
1.87o as safflower oll, and 9 2o/" as crystalline amino acids
(\rivonex,Novartis Nutrit ion, St. Lours Park MN 55416). Noc-
Chapter 2 I HYPoglycomia
turnal cornsrarch therapy is also beneficial. Transtenr noctur
hypoglvcemia is not completely prevented, and renal glomeru
dysfuncrion plus formation of hepatic adenoma lemain seli
complications, Liver transplantacion offers promrse of long-te
cufe,
defects have been described. Hepatomegaly, excessivedepositof gLycogen n liver, growth retardation, and occasional svmp
maiic hypoglycemia occur A dret hrgh in Prot€in and reduce
cholamines, are appropnately elevated or normal, and ins
levels are appropriarely low. The liver is nor enlarged. Prot
rich feedings at frequent rntervals result in dramatic cltn
improvement, rncluding growth velociry This condition mim
the syndrome of ketotic hvpoglvcemia aod should be considein the differential diagnosis of that syndrome
DISOBOEBSFGTUCONEOGENESIS
provokedbv inhibrt ion ol glycogenolysis. lrco8enol)cr s em
inracr,an d glucagonelrerts normal glycemic e\ponse n the
but not rn rhe fasted, state. Accordingly, affected individuals h
Clinical features simulare those of rype I glycogen sco
disease.Hepatomegaly n individuals with fructose-1,5-di
phatase deficiency is due to hpid storage talhet than glyco
storage. Lactic acidosis, ketosis, hyperliprdemra, and hy
uricemia occur; their pathogenesis s related to the severiq'
durarion of hypoglycemia and lhe resultant lorv levels of ins
and high levels of counter-regulatory hormones. Therapy
these infants, consistrng of a diet high in carbohydtates 15excluding fructose, which cannot be utilzed), lorv in pro
(12%), an d normal in far composrtion (32%), ha s perm
normal growth and developmenr- Continuous nocturnal pr
sion of calories rhrough rhe intragastric infusion svstem descr
earlier for tvpe I glycogen storage disease s also applicabl
children with fructose 1,6-diphosphatase de6cienc,v. Duintercurrent illnesseswith vomiting, intravenous glucose inlu
is necessaryo preventsevere ypoglycemia.
Oelects n Fatty Acid Oxidalion (See Chapter861.The impor
role of fattl acid oxidation in maintaining gluconeogene
underscored by examples oI congeniral or drug-induced de
rn fatry acid metabolism that may be assocratedwith fa
hypoglycemia-
Various congenitaI enzymadc deficrencies ausrng defective
nitine or fatty acid merabolism occur. A severe and relar
common form of fasting hvpoglycemia with heparomegall',
diomyopathv, and hvpotonia occurs with long and med
chain faty acid coenzyme-A dehydrogenase deficrency (LC
and IvICAD). Plasma carnitine leveLsare low, ketones ate

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 175/177
666 r PARTX Melabolicoise8ses
present in urine, but dicarboxylic aciduria is present. Clinically,pacients rvith acyl CoA dehydrogenase deficiency present with aReye-like syndrome (see Chapcer 358), recurrent episodes ofsevere fasting hypoglycemic coma, and cardiorespiratory arrest(sudden nfant death syndrome-like events).Severehypoglvcemiaand metabolic acrdosiswithout ketosis also occur in oatients withmulriplea.rl ( oA dehydrogenase isorder' . HypuroniaJ eizures,and acrid odor are other chnical clues, Survival depends onwhether rhe deiect, are 'evere or mildi diagnosrs s eirablishedfrom scudies of enzvme activlty ln liver biopsy tissue or rn cul-
tured fibroblasts from affected patients. Tandem mass spectrom-etry can be employed for blood samples , eyen those on frlterpaper, tor screening of congenital inborn errors. The frequencyof this disorder s ar leasr1/10,000*15,000birrhs. Avoidanceoffasting and supplementation with carnitine mav be lifesaving inthese patients lvho generally present in infancl'.
Interference with {artv acrd metabolism also underlies thefasting hypoglycemia associated with Jamaican vomiting sick-ness,with atractyloside, and with rhe drug valproate. ln Jamaicanvomiting sickness, he unripe ackee fruit contains a water-solubletoxin, hypoglycin, which produces vomiting, CNS depression,and severe hypoglycernia. The hvpoglvcemic acciviry of h1'po-glycin denves from its inhibition of gluconeogenesissecondary toits interference vvith the acyl CoA and carnitine mecabolism essen-tial for rhe oxidarion of long-chain fatty acids, The disease rs
almosc torally confined to Jamaica, where ackee forms a stapleof the diet for the poor. The ripe ackee fruit no longer containsthis toxin. Atldctlloside rs a reagent that inhibits oxidative phos-
phorylation in mitochondria by preventing the rranslocation ofadenine nucleotides, such as ATP, across he mitochondrral mem-brane. Atractyloside is a perhvdrophenanthrenic glycoside
derrved from Atractyls gummrfera. This plant rs found in rhe
Medicerranean basin; ingesrron of this "thistle" is associatedwith
hvpoglycemia and a syndrome similar to Jamaican vomiting sick-
ness, The anticonvulsalt drug valproate is associated with sideeffecrs, predominantly in young infants, which include a Rer.e-like syndrome, low serum carnitlne levels, and the porential forfasting hypoglycemia. In all these conditions, hypoglvcemra is zol
associated uith ketonu/u,Acute Alcohol Intoxication. The liver metabolizes alcohol as a
preferred fuel, and generalion of reducrng equivalents during theoxidation of ethanol alters the NADH:NAD ratio, which is essen-
tial for cerrajn gluconeogenic steps. As a result, gluconeogenesis
is impaired and hypoglycemia ma,v ensue if glycogen stores are
depleted by starvation or by pre-existing abnormalities in gl1'co-
gen metabolism. In toddlers who have been unfed for some cime,
even the consumptioo of small quantities of alcohol can precipi-
late rhese events. The hypoglycemia promptly responds !o intravenous glucose, which should ahr.ays be considered in a childrvho presencs nitiaLly rvith coma or seizure, after taking a blood
sample to determine glucose concentration. The possrbilit,vof the
child's ingesting alcoholic drinks must also be considered if there
was a preceding adulr evening parq'. A careful history allows the
diagnosis to be made and may avoid needlessand expensive hos-
pitalizacionaod investigation.
Salicylate Intoxication (SeeChapter5Sl.Both hypergh'cemia andhypoglycemia occur rn children with salicylare intoxication.
Accelerared urrlizarion of glucose, resulting from augmentarion
of insulin secretion by salicylares,and possible interference with
gluconeogenesis may contribute ro hypoglycemia. Infants are
more susceprible chan are older children. Momtoring of bloodglucose levels with appropriate glucose infusion in the event ofhypoglycemia should form part of the therapeutic approach co
salicylate inroxrcatron ln chlldhood. Ketosrs may occur.
Phosphoenol Pyruvate Caftorykinase Deliciency. Deficiency ofthis rateJimicing gluconeogenic enzyme is associated vr.rthseverefascing h1'poglycemia and variable onset after birth. Hypo-glvcemia may' occur within 24 hr aher birth. and defecrive glu-
coneogenesis from alanine calt be documenled rn vrvo. Liver,
kidnel and myocardium demonsrrate atqv infiltration,atrophy of th optic nerveand vrsual cortex may occur.Hyglycemiamay eprofound.Lacrateand pvruvareevelsn plahavebeennormal, but a mild metaboli acidosrsmay be preThe fatty rnfiltrationof variousorgans caused ,v ncreasemation ol acetylCoA, u.hichbecomes vailableor fattv acidthesis.Diagnosisof this rare enrity can be made,"l.rth erronlr through appropriare nzymaric erermrnarionrn biopsymaterial.Avoidance f periodsof fasring hrough reqfeedingsich in carbohydrare houldbe helpful because lyc
synthesis nd breakdownare ntact.PyruvateCalboxylase eficiencySeeGhapter 7). This is
dominanclya drsease f the CNS characterized y a subanecrotizing ncephalomvelopathynd high evelsof blood acand pyruvate.Hypoglycemia s not a prominent eatureof syndrome,presumably ecause luconeogenesisrom precuother than alanine emains ntact, and theseprecursorsbythe p)'ruvatecarboxylase tep.The utilization of alamneasas lactate hrough pyruvatecannot proceed,however,so tsubstrates ccumulate n blood, and modesthypoglycemiaresultduring fastrng.AffectedpatieotsLrsually ie of progreCNS disease.
OTHER ]IIZYMEEfECTSGalactosenia Galactose-1-Phosphateridyl TransferaseD
ciencyl. eeChapter 7.Fructosentolerancetructose-l-PhosphateldolaseDeficie
[SeeChapter 71, cute h,vpoglycemias due to the inhibiciofructose-1-phosphate f glycogenolysis ia the phosphorsyscem nd of gluconeogenesist rhe evelof fructose-1,5-diphatealdolase.Affected ndivrdualsusually earn spontaneto eliminate ructose rom their diet.
DEFECTSN GTUCOSERAI{SPOBTERSGLIJT-IDeficiencv. wo infancswith a seizuredisorderw
found to have ow cerebrospinalluid (CSF)glucose oncetions despilenormal plasma glucose.LactateconcentratioCSF were also lolri suggesting ecreased lycolvsis ather tbacterial infection, whjch causes ow CSF glucosewith h
lactare.The erythroq/te glucoseuanspofter was defective,gescing simrlardefect n the brain glucose ransporter espble for the clinical eatures.A ketogenicdiet reduced he sevof seizures y supplying an allernatesourceof brain fuel bypassedhe defect n glucoseransport.
GLUT-2 eficiency. hildren vichheparomegal,v,alactosenerance, nd renal ubular dysfuncrion Fanconi-Bickel yndrohave been shown to have a deficienc,v f the GLUT-2 glucransponer f plasmamembranes,n addition o Lver and kidtubules, GLUT2 is also expressedn pancreaticp cells.Hethe chnical manifesradonseflect mpairedglucose elease liver and defective ubular reabsorptionof glucoseplus ppharuria nd aminoaciduria.
SYSTEMIC ISOBDERS.everal ystemic isordersare assoc
wirh hypoglycemia n inlants and children.Neonaral sepsoften associated ith hypoglycemia, ossiblyas a resultof dimished caloric intake wi rh rmpaired gluconeogenesis. imnechanismsmay apply to the hypoglvcemia ound in sevmalnourishednfantsor thosewichseveremalabsorption,Hyviscositywith a central hematocritol >65"/o s associatedhvpoglycemian at least10-157" of affecred nfancs. alcipamalaria has been associatedwirh hyperinsulinemia nd hyglycemia.Hean and renal ailure havealsobeenassociatedhypoglycemia, ut the mechanism s obscure. nfants and cdren with Nisseo undoplicat ion,a relativelycommonproceused to ameliorate gastroesophagealeflux, frequently han associated dumping" syndrome .ith hypoglvcemia,Cacteristic features nclude srgnificanthyperglycemraof up

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 176/177
500 mg/dl 30 minutes postprandiallv and severe hypoglvcemia
(aleraie 32 me./d in oni .eriesl 1.5-3-0hr larer. hc earlvhvper-
elycem"ia ha.e r\ associaredwirh brisk an d excessivr nsulin
i. i.rr" ,hl cau\e\ rhe rebound hypogllcemia 6lucagon
responseshave been inappropriatel]- low ir some. Although the
oh is io loe jcmechan j \ms re no r l lways c lea r l yapparent , nd
anemore"drearmenrs or alwavselfective'acarbose, n inhibtlor
of glucose absorption, has been reported ro be successflrl n one
small series.
DIAGiIOSISNDDIFFEREI'ITIALIAGNOSIS
Table92 8 lists he pertinentclinical and iochemical indings n
rhe commonchildhooddisordersassocia d with hypoglycemia
5exes.
suggescsyperinsulinemia r a defect n fatry acid oxidarion' In
moit othet caos.tof hypoglycemia, rth the exceptionof galac-
tosemiaand fructose ntolerance, etonemiaand kelonuria are
Dresen tt rhe rme, ' i as t ing ypog lycemia .t the imeof rhe
irvpog.lvcemia.erumshouldbe obrained or determinarioni
h,rrm"onesnJ \ubslrares,ollowedby repeatedmeasurement
afteran intramuscularr intravenousnjecnon f glucaSon, s
rapidlv by the histo lnadvertentor deliberatedrug ingestion
and ertors n dispen g medrcineshouldalsobe considered.
When the history is suggestive, ut acuresymptoms re not
present,a 24-36 hr supervisedast can usuallyprovok hypo-
Chapterg r Hypoglycemia
e l l cem iaand reso l \ e he ques t ion f hype r rn ' l i nema or o
iondicion* L5ee able q2 8) . Such a fasr is conrraindicated
fatty acid oxidatron defect is suspected;ocher approaches suc
mass randem spectrometry or molecular diagnosis, or b
shor:ld be considered. Becauseadrenal insuffrciency may mi
necessary,
ln the presence of hepacomegaly and hvpoglycemia, a
sumptil'e diagnosis o[ the enzyme defect can otten be m
through the clinical manifestations, Presenceof hyperlipidem
acidoJis, hyperuricemia) resPonse to glucagon in the fed
expertise available only in cerrain rnstirutions,
TREATMENT
somatostalln alogs.
Treatment acute symptomatic neonatal ot infant h
gl,vcemia inc des intravenous administtatron of 2 mUkg
D1n w, follo ed by a conrinuous rnfuslon of glucose a
8 mg/kg/min, djusting rhe rate to mainrain blood glucose l
In the normal range. If hvpoglycemic seizuresare presenl' s
recommend a 4 mUkg bolus of D16 !(/.
The managemenr of persistent neonatal or infanrile h
glycemia rncludes rncreasing he rare of intrarcnolrs glucose
sion to 10-15 mg/kg/min or more, if needed. This may requ
central venous or umbilical venous catheter to adminis
h-vperromc 15-25% glucose solution. If hyperinsulinemi
present, it should be medically managed itiall,v with diazo
and lhen somatostarin analogs or calciu channel blocke
hvpoglvcemra is unresponsive to intravenous glucose plus
zoxide (maximal doses up to 25 mg/kg/day) and somastos
analogs, surgery via partial or near-total pancreatectom; sh
be considered.
Oral diazoxrde, 10-25 mg,&gi24hr given in divided d
every 5 hr, may reverse hyperrnsulinemtc hypoglycemra but
alsoproducehirsutism,edema,nausea, yperuricemia, lect
disrurbances, advanced bone age, IgG deliciencl', and, ra
tive in controlling hyperinsuhnemrc hvpoglycemia in pat
v' ith islet cell disordersno t causedby genecicmutations in
channel and rslet cell adenoma. Octreotrde is adrninistered
cutaneously very 6-12ht in dosesof 20-50 pg in neonate
young infanrs. Potencial bur unusual cornphcations include
growth due ro inhibition of growth hormone release,pain a
injection site, vomrtrng, drarrhea, and hepatic dysfun
(hepatit is,cholelithiasis).Octreocide s usually employed
temporizing agent for various periods before subtotal pancre

5/9/2018 Nelson 2007 Parte 9 y 10 Gen Metab - slidepdf.com
http://slidepdf.com/reader/full/nelson-2007-parte-9-y-10-gen-metab 177/177
668 PABTX Metabolic iseases
tomy for KArpchannel disorders. ft mav be parricularly useful forthe rreatment of refracrory hvpoglycemia despite subtotal pan-createctomy. Tcrtalpancreacectomy s not oprimal therapy, owingto the risks of surgery,permanent diabetes mellitus, and exocrinepancreatic insufliciencl'. Conrinued prolonged medical therapywjrhour pancreatic resection if hypoglycemia rs controllable isworthu'hile becausesome children have a soontaneous resolution, , i t he hype r rnsu l rnemiclpog l ' cem ia .Th is ' hou ld be ba lancedagainst the risk of hypoglycemia-induced CNS rnjury and rhe toxlcll,vor orugs,
PROGNOSIS
The prognosis is good in aslmptomatic neonaces with hypo-glycemia of shorr duration. Hypoglycemia recurs rn 10-15o% ofinfants afcer adeoLraLereatment. Recurrence is more common iflntravenous fluids are extravasared or discontinued too raoidlv
beforeoral teedine.are well t .r lerated.Children in whom keL.rrichypoglvcemia latir develops have an rncreased rncidence ofneonatal hypoglvcemia.
The prognosis for normal inrellectual function must be guarded
because prolonged, recurrent, and severe symptomatic hypogl_v-cemias associaled u'rrh neuroLogic sequelae. Sympcomatic
infants wrrh hvpoglycemra, particularl). low-birthweighc infants,those with persistent hyperinsulinemic hvpoglycemia, and infants
of draberic mothers, have a poorer prognosis for subsequent
normal intellectual development than asympromatic infants do.
Ahmad A, Kahle rSC, KishnaniPS .et al : Treatmenr f pyruvare arboxyJase
deficiency uith high doses oI ci[ate and aspartate An I Med Geftet1 9 9 9 ; 8 7 : 3 3 13 8 .
Bachrach BE. Weinstein DA, Orbo-MeLander M, et al: Glvcogen synthase
dcficiency gl1(ogenstoragedisease ype 0t presentingurrh hypergtycemia
and gtucosuria: Rcporr of three new mulatrons. I L'ediatr 2002\\40:
781-i83.
Dacou-Vouterakis C, Psrchou I Maniatr-Chrisridrs Mr Persrstent yperinsu
linemic hl.pogJ-vcemiaf infancy: l,ong term rcs:ults. Pedidtr Endoctinol
Metub 1998;1| :137-L4l .Dalgic N, lirgenekon E, Soysal S, et al: Transienr neonatal hypoglycemir-
l-ong term eflects on neurodevelopmenralo:utcome. Pediatr Lndacriftol
Metab 2002;l5 319-324.
DeBaun MR, King AA. White N: H-vpoglycemjan Belkwtrh-wiedemann syn-
drome. Se-iri Pelinutol 2000\2+1t44-l /-1
de Lonlar P, BenelhC, Fouque4 et al: Hyperinsulinism and hIp€rammon€-
mja svndrome: Report of 12 unrelared parJena. Pediatu Res
2001i50:-]51 57.
de Lonlay ( (lDer Nl, Vuillaumier-Barrot S, ef al, Hyperinsulinenic hypo
glycemiaas a presenringsign in phosphomannosesomerasedeiciency: A
nelv rnanifesrarionof carbohydracedeficientglvcoprorein syndrome rrear
able $'irh mannose J Pedidtr 1999;1351379-383.
de Lonley R ciurgea l, Touari G, et al: Neonatal h-vposlycaemia, etiolosies.
Semi Neonatol 2004\9'49 58
dc Lonla,v-Debency Poggi-Traven 4 Fournet J-C, er at: Clinical fearures
of 52 neonares g.ith hyperinsulinism. N Engl I Med 1999340:1169-
1 175
l)evivLr DC, IrifiLciti RR, Jacobson RI, er al: Defective glucosetransport
across dre bLood-brain barrier as a causeof persisrenthypoBlycorrhachia,
seLzures, nd deveLopmcntal elay.N ,Engl/ Med 1991;325:703 709.
Dunne N{J, Kane C. ShepherdRM, et al, Familial perststenr vperlnsulinenic
hypoglycemiaof inlancy and mutarions n rhe suifonylurea receptor.N Ettgl
J Med L997:336 703-706.
Fr€ckmann Ml-, Thorburn llR, Kirby DM, et at: Mirochondrial eteccron
transporr charn defecr presendng as hyposlycemia. I Pedidtr 1997\1301.+31-436.
Giurge. I,I-aborde K, Touati G, e t al: Acute insuln responses a calciun and
colbutanrdedc not differentiate ocal fron difluse congenrrathyperinsuLin-
i\n CIin Lndo.nnol Metdb 2004;89:925-929.
Hardy OT, H€rnandez'PampaloniM, SafferJR, er al, Diagnosisand locanon of Iocal congenital h;,perinsullnism by l8f-fluorodopa PET sc
Pedid t 2007 150:'140-1 5.Huopio H, Reimann F, Ashfeld R, er al: Domjnanrlv inhcrrted hyperins
ism causedbv a muration in chesulfonylureareceprot ypc 7. J Clin lf
2000;106,897-906.
Katz LE, Ferry RJ Jr , StanleyCA, et al: Suppressn,n f insulin over secr
by subcutaneous ecombinant human insLrlin ike growth iacror 1 jn
dren v'nh congeniml hyperinsulinxm due ro defecrivebera-ccJl ulfcnyrccepror Cln Endo.rinol Metab t999\84:3117 3124.
Kelly A, Ng D, Ferrv RJJr ,
ei al: Acure insulin responses o leucine n
dren with the hyperinsulinism/hvperammonemiasvndrome. /Endod inol Metab 2001 86:3724 3728.
Kinnala A, Rikalainen H, LapinLeimuH, et al: Cerebral magnedc reson
imaging and ultrasonography indings after neonataLhypogtycemia.P
dtrics 1999 ,101:724:29 .
Lucas A, Morley R, Cole TJ: AdverseneDrodevelopmenrel utcome of m
erate neonaraL ypoglyceml^. b Med J 1988;297:1304 1308.
Magge SN, Shvng SL, MacMullen C, et al: Fanrlial leucinesensitivehglvcemia of infancy due to a dominanr muradon of the beta cell sulfrurea recepror / Clik Endo.tinol Metab 2004;89:4450-4456.
Mayefskv JH, Sarnaik AP, PosrellonDC: FactLtious rcoglycemla Pedlr
1982j69:804-805.
NleissnerT, Wesdet U, Burgard P, et al: Long rerm tbLlow-up of I14 pat
with consenital hype.insulinism.Eur J Erutoomol 2003l.'149.43-51
Melis D, Parenri G, Della CR, er al: Brain damage n glycogensrofasedis
qpeI. J Pediatu2004\144:637642.
Menni F, delonlay P, Sevin C, ec at: Neurologic outcomesof 90 neonateinfancs w'irh persistenr hyperinsulinemic hypogll'cemia. Pedr
2001.,107:47479
Molven A, Rishaung U, Nlarre CE, er at: Hundng for a hlpo$ycer a g
Severe eonaralhypoglycemia n a consanguneous familv.Am I Med G
2002;113:4046 .Ng DD, Feny RJ Jr, Kellv A, et al: Acarbose rearmenrof posrprandialh
glycemia in children after Nissen tuDdoplicarion J Pediatr 2001;
877-879.Njuguna P, Newton C: Managementof severe alcjparum malaria. ?osr
Med 2004;50:4550 .
Osier FH, BerkleyJA, RossA, et al: Abnormal blood gLucose oncentra
on adnissron to a rural Kenyan dist.ict hospital: Prevalence nd oucc
Arch Dis Child 2003;88i2r-625 .
Otonkoskr T, Nanro-SalonenK, SeppanenM, et a1:NoniDvasivediagros
{ocal hyperinsulinrsm of infancy u.ith Ir8F]-DOPA posirron emis
tomographl. D abetes2006;55 13-1 8.
Otonkoski I Kaminen N, Usnnov J, et al: Physical exercisenduced hyinsulinemic h,vpoglycemia s an autosonafdominant uait characte
by abnormal pyruvate induced insulin release Dlabetes 2003.52.
204.
Rrizen DM, Brooks Kayal ,\, Sreinkauss L, er a| CentraLnervous sy
hyperexcitabitity associatedwirh gluramatedeh-vdrogenascain of func
mut^ti,ons. Pediatr 2005i146:388-394.
tubeiro MJ, de Lonlay P, DeLzescaux et al: Characterizationof hyp
suLinismn infancy assessed irh PET and 18F-Flucrro-L-DOPA. NazlM
200i i46:550-.r66.
SparJA, Lewine.fD, Orrison vW Jr: Neonatal hypoglycenra: CT and
lindings.,a,u/ Nerrolrdiol L994;15 1477 147 8.
Sperling MA, Menon RK: Differenrial diagnosis and managernentof ne
tal hypoglycemia.Psdia* Cli11North Am 2004t5L:703 723.
StanleyCAr Advances n diagnosisand treannentof hwerinsulinrsm in inf
and children. / Clin Etulo.tlnol Metab 2002;87,4857-4859.
StanleyCA, Thornron PS.Gangulv A, et al: Preoperativeevaluation oi inr
wirh local or diffuse congenitalhyperlnsulinismb-v ntrav€nousacure nsr€sponse estsand selecriveFancreaticafterial calciuln stirnulation.
F,ndocrinolMeab 2004;89:288-29 6,
SteinkraussL, Lrpman TH, Hendell CD, er al: Eflecrs of h,vpoglycem
de"eLopmentaloDtcome in children wirh congenital hvperinsuli*m
Pediatr N /s 2005\2U109 118.
Sun I-, Eklund EA, Chung \vK, et ai: Congenrraldisorder of glycosvlati
presentins vith hypcrinsulinemichypoglycemia and isLet ell hyperpla
Clin Endocnnol Metab 2005r90:4371 437J.
Taylor SI, Barbetri F, Accili D, er al: Sl.ndromesof autoimrnuniw and h
glvcemia: Auroantibodies directed against jnsuLin and Lts rccc
Endo.rinol Metab Chn Noth Am r989;r8:123-143
Thornton PS, Satin-Snith li'ts, Herold K, er al: Famjlial h,vperinsulinism