Embed Size (px)
Citation preview

THE PAIN PATIENT:
NEGOTIATING THE TWIN TRAPS OF
OVERTREATMENT AND
THERAPEUTIC NIHILISM
Lize Weich

• I will apply, for the benefit of the sick, all measures that
are required, avoiding those twin traps of overtreatment
and therapeutic nihilism…”
• Hypocrites oath (Edelstein 1945)

Opioids are…
• Essential medications-
one of the most
effective drugs for
relief of pain and
suffering
• Yet feared because of
potential for misuse,
addiction and diversion

WHAT IS PAIN…

Pain
• “An unpleasant sensory and emotional
experience associated with actual or potential
tissue damage, or described in terms of such
damage” International association for the study of pain

Pain
• Integral part of life
• The body’s defence- aimed to deal with threats and ensure survival
• Signals a need to act, therefore often associated with strong feelings • Anxiety/fear
• Anger/rage
• Subjective, perceived different by different people
• Both sensory and affective dimensions
• Affects physical, psychological and social wellbeing of a person • Affects sleep, leads to depression and anxiety
• Impairs health, functionality and productivity and quality of life

Physiological basis
neuropathic or nociceptive
• Nociceptive pain
• At the site of insult
• Tends to resolve
spontaneously, but may
persist if tissue damage
persist
• May be intermittent
Savage et al; Add Sci&Clin Pract 2008

Neuropathic pain
• Result of aberrant
functioning along the
neural pathways that
normally conduct
nociceptive pain
• Peripheral nerve

Neuropathic pain 2
• Disruption of normal
relationship of
peripheral neurons and
secondary neurons in
spinal cord- central
sensitization -
translates non-painful
stimuli into pain

Neuropathic pain 3
• Central or regional e.g.
thalamus, dorsal horn
• Aberrant central
processing of non-
pain stimuli – via abN
NT’s
• Sometimes mixed
aetiologies

Neuropathic vs. nociceptive pain
nociceptive
• Physiological
• Tissue damage
• Acute, abrupt, short
• Understandable, obvious
causes
• Protective
• Biomedical model
• Illness with cure as goal
• Treatment though traditional
pain medication
neuropathic
• Pathological
• Nerve damage, poorly localized, parasthesia, numbing, burning
• Chronic, gradual onset, longer than expected
• Medically difficult to explain
• Not protective
• Bio-psycho-social model
• Treatment though mastery/control

Acute or chronic
• Acute
• abrupt onset
• Due to physical condition
• Etiology usually identifiable
• Often self-limiting
• Often nociceptive
• Sympathetic response
• Chronic
• No longer serves a survival function/beneficial purpose
• May be due to ongoing pathology, neuropathic cause or
combination

Unique experience of pain
• Same pain generator may be very different
for different individuals
• Depends on • Biogenetic make-up
• Sociocultural experience
• Gender
• Co-occurring medical and psychiatric conditions

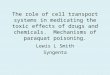
Bio-psycho social context

From S Passik: “Aberrant behaviors in chronic pain patients”

TERMINOLOGY RELATED
TO OPIOID USE

Medication abuse/misuse
• Taking a medication in a manner other than how if was
prescribed or for an indication different to what it was
prescribed for
• Intentionally used outside the normal standards of its use, e.g. use
for a non-medical purpose, like altering your state of consciousness
or getting high

Physical dependence
• State of physiological adaptation
• Tolerance
• withdrawal
• Common with repeated opioid use for pain
• Does not in itself indicate misuse or addiction
• Therapeutic dose withdrawal
• Tapering of dose during discontinuation required

DSM 5 Substance use disorder:
• Problematic substance use, leading to significant distress
or impairment
• At least 2 symptoms from a list of 11 during a 12-month
period.

1. Taking the substance longer or in larger amounts than planned
2. Desire or efforts to cut down substance use that are not successful
3. Large amount of time is spent to obtain or use the substance and to
recover from its effects.
4. Cravings
5. Role failure in work, school or home as a result of substance use
6. Relationship difficulties or social problems due to/or made worse by
the substance
7. Important activities are neglected or given up due to substance
use, including at work, social or recreational activities
8. Substance use is physically hazardous situations
9. Ongoing substance use even when the individual is aware that it is
responsible for, or aggravating medical or psychological problems
10. Tolerance
11. Withdrawal

• “Addiction is not about taking medication for pain relief,
but taking a drug and acting like a drug addict”.

ALL OPIOIDS ARE NOT
EQUAL…

Some more rewarding than others…
• Rate of increase • Rate of rise in blood levels: the faster the influx the better the high
• IV > IM/s/c > po
• Peak blood level attained • The higher the level relevant to the tolerance, the more rewarding
• IV > po
• Stable effect less rewarding than intermittent rise and fall • Continuous/controlled release < boluses
• Long acting < short acting
• Receptor effects • Mu > kappa
• Mu sub receptor variations: different individuals experience varying reward

THE CHRONIC PAIN PATIENT:
TO USE OPIOIDS OR NOT TO
USE …

On the one hand…
• The Tragedy of Needless Pain
• By Ronald Melzack
• Contrary to popular belief, the author says, morphine
taken solely to control pain is not addictive. Yet patients
worldwide continue to be undertreated and to suffer
unnecessary agony…

CAVEAT VENDITOR

Epidemiology
• No studies have investigated prospectively
• Most studies exclude patients with histories of SUD
• Rates then are low
• However in pain medication addiction cohorts, most took
their first pain medication for valid pain
• Misuse (rather than addiction) range from 1-38%
• Interplay of
• Drugs rewarding effects
• Genetic make-up
• Modulatory effects like pain, stress and psychosocial context of use

From S Passik: “Aberrant behaviors in chronic pain patients”

Prescribers in a difficult position
• Many prescribers do not have a problem with medicating
acute pain, cancer pain or end of life pain
• With chronic non-cancer pain, many prescribers shy away
from opioids
• Recognize opioids are effective, but concerned they may
contribute to abuse and diversion

PRACTICAL APPROACH TO
CHRONIC NON-CANCER PAIN

“Diabolical” chronic pain • Chronic, non-functional pain:
• Vague and disproportionate
• Described in emotional terminology
• Constant
• Focus on opioid pain medication, resistance to other treatments
• Patient: • Sx of MH problems, e.g. anxious, depressed, angry, helpless,
somatic conviction, H/o abuse
• Hx of SUD
• FH of pain/SUD
• May have borderline, dependent, avoidant traits
• Socially often have stressors
• Disability and compensation

Detailed assessment
• Assessment of pain • Intensity, quality, location, radiation, factors that increase or
decrease, interventions tried etc.
• Impact of pain on mood, sleep, stress, functioning at work, relationships, recreational activities
• (Brief pain inventory)
• Also assess • Psychiatric history and MSE: assess for significant anxiety or
depression
• Including personal and family h/o substance use disorder
• h/o legal problems
• heavy tobacco use
• Childhood abuse and trauma (risk for pain syndromes and addictions)

Assessment c/t
• Family style
• Fostering disability
• Justify medication overuse
• Assessment of SU history require MI skills
• Empathy predicts extent of disclosure
• Before and during treatment – urine toxicology
• Also consider in diff Dx
• Undetermined medical d/o
• Somatic symptom d/o: pain disorder may be a mental disorder
when psychological factors are NB to onset, severity, exacerbation,
perpetuation
• Malingering/ Factitious

Tools for pre-screening
patients for opioid misuse risk
• Screener and opioid assessment for patients with pain (SOAPP) • Akbik et al 2006
• Self report
• 14 item, 5 points/item
• Cutoff of 8 or more
• Opioid risk tool (ORT) • Webste r& Webster 1995
• 5 yes/no self report items
• 0-3 low risk; 4-7 moderate risk; 8+ high risk
• Face value issue issue: susceptible to deception

When using chronic opioids for non-
cancer pain
• Negative outcomes more common when
• High levels of psychological distress
• Negative beliefs and expectations re pain
• Pain-related fear and avoidance
• Attitude of anger, hostility, alienation
• Maladaptive coping and cognitive distortions or catastrophic
thinking

Opioids for chronic non-malignant pain
• Risk-benefit ratio
• Opioids can foster incapacity and greater risk for injury and
accidents
• Chronic pain has no discernable end point
• Lifestyle modifications appropriate – like weight loss or exercise
and opioids may hinder this
• Patients may become reliant on opioids to cope with negative
emotional states
• Genetic polymorphisms associated with opioid addictions
• ? future possibly screen for at risk individuals

When using chronic opioids for non-
cancer pain • Risk assessment
• Stratify risk:
• Risk larger if <50 y
• Pre treatment h/o SUD or mental illness
• sedative hypnotic use
• larger number of days’ medication supplied at once
• larger daily dose with higher potency opioids
(Edlund et al)

Before starting… • Disclose risks
• Informed written consent
• Written treatment plan with expectations
• Need to accommodate risk into treatment plan
• Consider specialist care
• Selection of treatment: abuse deterrent formulations
• Controls on amounts dispensed (number of units/frequency of dispensing)
• Supervision and monitoring (regular visits, urine screening, pill counts etc.)
• recovery activities
• Exit strategy before initiating treatment • Trial periods with clear goals
• Discontinue if no longer meets goals of improved pain, stable/improved functioning, enhanced quality of life; safety issues, diversion, resolved pain

Monitoring
• Consider 4 domains during follow-up
• Analgesia
• Activities of daily living
• Adverse effects
• Aberrant drug-taking behavior

Suggestive of aberrant medication use
behavior • Multiple unsanctioned dose increases
• Repeated prescription losses
• Repeated requests for early refills
• Concurrent abuse of related illicit drugs
• Obtaining from multiple unsanctioned/ non-medical
sources
• Stealing prescriptions pads/forging prescriptions
• Borrowing/stealing medication from another patient
• Injecting oral formulation
• Selling medication

Aberrant medication use behavior
• Misunderstanding instructions (written instructions)
• Elective use for reward/euphoria – abuse
• Addiction
• Misuse due to mental health difficulty (personality d/o; chemical coping, depression, anxiety, sleep etc.)
• Pseudo-addiction – undertreated pain
• Criminal intent – diversion for profit
• Patient may have both pain and addiction!

In or out of the box?
Passik, Kirch Ex Clin Psychopharm 2008, 16(5): 400-404

Managing chronic pain: beyond opioids
• Acknowledge- affirm reality of experience
• Prevent/manage SUD
• ID physical, psychological and social Fx
• Negotiate appropriate goals
• Increased QoL, less reliant on analgesia
• CBT+/- other Rx
• Shifting emphasis from controlling pain to coping, living
despite pain

Other pharmacological/non-
pharmacological options for pain:
From: Savage et al; Add Sci&Clin Pract 2008

THE ADDICTED PAIN
PATIENT…

Many myths around pain and the addict…
• Addicts • Don’t suffer pain
• Don’t need pain relief
• Pain medication don’t work for them
• Its illegal to use opioids in these patients
• It will lead to relapse
• Don’t deserve
• Reality • Have higher pain scores
• Develop tolerance and hyperalgesia
• Respond well to analgesia
• On OST: Need baseline opioids
• Require higher doses

Often intertwined disorders…

Addicted pain patients…
• Tend to believe that substances help them cope and
function better, while the reality is the opposite
• Rarely use in a manner that creates a state of
physiological homeostasis – fluctuate between
intoxication and withdrawal – “on-off” phenomena
that increase pain
• Difficulties complying with pain regime
recommendations
• Perceive their substance use as transient, as the
believe it is justified in view of their pain and required
for coping

Some thoughts on prevention
• Careful selection of patients – identify and treat
comorbidity
• Unethical to withhold pain relief in acute pain
• Close monitoring- focus on functional improvement rather
than a pain free utopia
• Modulating reward though drug selection and dosing
• Longer acting drugs
• Tamper proof formulations

Some thoughts on management
• Joint management
• Manage psychiatric comorbidity
• Expect lots of resistance - MI
• Address the addiction via evidence based approaches,
e.g. CBT, MI, 12 steps
• Involve families

Role of the addiction care practitioner
• Joint management with pain specialists with good
communication routes
• May do CBT for both pain and addiction
• Partake in the development of a care plan
• Provide treatment for the addiction
• Support and monitor during recovery

QUESTIONS?