Embed Size (px)
DESCRIPTION
Neck Lymphadenitis Due to Silicone Granuloma After Mammary
Citation preview

Acta Otorrinolaringol Esp. 2013;64(3):217---222
www.elsevier.es/otorrino
ORIGINAL ARTICLE
Neck Lymphadenitis Due to Silicone Granuloma After MammaryImplants�
Francisco Javier García Callejo,a,∗ Jordi Calvo González,a
Jaime Agustí Martínez,b Carmen Bécares Martínez,a Rafael Monzó Gandía,c
Jaime Marco Algarraa
a Servicio de Otorrinolaringología, Hospital Clínico Universitario, Valencia, Spainb Departamento de Anatomía Patológica, Hospital Clínico Universitario, Valencia, Spainc Servicio de Otorrinolaringología, Hospital de Requena, Requena, Valencia, Spain
Received 15 September 2012; accepted 19 December 2012
KEYWORDSSilicone;Granulomatouslymphadenitis;Cervical node;Silicone
AbstractIntroduction: A foreign body reaction due to silicone where it is infiltrated or at the placesto which it can migrate is known as siliconoma. The use of silicone in breast augmentationprocedures can provoke this reaction at the neck level in cases of leakage from mammaryimplants.Methods: We reviewed the cases of patients with increased size neck lymph nodes who hadpreviously undergone plastic surgery of the breast with highly cohesive silicone gel implants.Results: In a 10-year period, we identified 12 cases with silicone-infiltrated neck lym-phadenopathies, histologically confirmed by fine needle aspiration. They represented 3.5% ofpatients attended for neck lymph node study. We removed those detected by physical examina-tion and CT in 5 cases, due to pathological characteristics of the node or a previous malignanthistory. In 2 of these nodes recurred, and node size also increased in 2 of the other 7 non-operated cases. After implant removal, silicone leakage was observed in only 7 cases.Conclusions: Cohesive gel silicone used for mammary implants can generate increased necklymphadenopathies as a secondary effect due to systemic reactions against the silicone whenit migrates in cases of implant failure. Surgical options for involved nodes usually do not offergood long-term results.© 2012 Elsevier España, S.L. All rights reserved.
PALABRAS CLAVE
Siliconoma;Adenitisgranulomatosa;Linfadenitis cervical debida a granuloma de silicona tras implantes mamarios
ResumenIntroducción: La reacción a cuerpo extrano producida por silicona donde se infiltra o en losterritorios donde migra se conoce como siliconoma. Su empleo en las técnicas de aumento depecho puede generar esta reacción en niveles cervicales si la cápsula del implante se rompe.
� Please cite this article as: García Callejo FJ, et al. Linfadenitis cervical debida a granuloma de silicona tras implantes mamarios. ActaOtorrinolaringol Esp. 2013;64:217---22.
∗ Corresponding author.E-mail address: [email protected] (F.J. García Callejo).
2173-5735/$ – see front matter © 2012 Elsevier España, S.L. All rights reserved.

218 F.J. García Callejo et al.
Nódulo cervical;Silicona
Métodos: Se han revisado los casos que consultaron por adenopatías cervicales de tamano ele-vado en pacientes previamente sometidos a cirugía plástica de mama con geles cohesivos desilicona.Resultados: En 10 anos han sido constatados 12 casos con adenopatías cervicales infiltradas porsilicona, confirmados mediante punción-aspiración con aguja fina. Suponen el 3,5% de todos lospacientes atendidos para estudio de adenopatías cervicales. Fueron retiradas aquellas detec-tadas por exploración física y TC en 5 casos, bien por presentar características patológicas opor historial previo de malignidad. En dos casos intervenidos los ganglios reaparecieron, mien-tras que en dos de los 7 pacientes donde se decidió no actuar, el volumen de las adenopatíastambién aumentó. Tras retirar los implantes, sólo se observaron fugas en 7 casos.Conclusiones: La silicona empleada en geles cohesivos para implantes mamarios es susceptiblede generar como efecto secundario aumento del volumen de los ganglios linfáticos del cuellodebido a reacciones sistémicas frente a la misma cuando migra. Las alternativas quirúrgicas delas adenopatías afectas no suelen ofrecer buenos resultados a largo plazo.© 2012 Elsevier España, S.L. Todos los derechos reservados.
I
Aaesfgiit
cot
isrrtcaorta
cbInNdirt
bao
clTltmr
rilio
P
TwcA2
gnaea(
obbl
ntroduction
t present, numerous medical and surgical proceduresimed at enhancing the body are as common as untested orven banned due to their secondary effects. In this regard,ilicone is a commonly used filling agent, as are autologousat or non-biocompatible substrates --- hyaluronic acid, colla-en or hydroxyapatite. The points in favour of the former arets thermostability, sterilisation capacity, viscoelastic stabil-ty against chemical compounds and minimal adherence toissues.
However, the risk of treatment lies in the possibility ofausing rejection and migration, which are very commonccurrences with liquid silicone. In the case of implants,hey occur due to breakage of the implant capsule.
The infiltration of liquid or scarcely cohesive gelled sil-cone favours local infections in the form of cellulitis andubepidermal abscesses, and in deep tissues generates aedistribution of subcutaneous fat, with disorganisation andemodelling of the adipose panniculus.1 This lipid restruc-uring often promotes contact between the infiltratedompound and cells containing antigens, thus activating
wide range of defence mechanisms, from productionf foreign body granulomas to delayed hypersensitivityeactions,2 through aetiopathogenic pathways similar tohose of sarcoidosis. This offers a potentially therapeuticpplication.3
Foreign body granulomatous reactions caused by sili-one in tissues with a significant fibrosis component haveeen well-documented and are known as siliconomas.1,2,4
n the absence of anatomical barriers, their movement toeighbouring tissues resulting in deformities is not unusual.either is migration to other parts of the body, usuallyetected by regional lymphatic chains in the axilla, abdom-nal wall or limbs. Intranodal lesions may extend to severalegions in the organism before foci are observed in the infil-ration area or signs of implant infection are identified.4,5
The rate of rupture of breast implants is not over 1%,ut an increase reaching up to 10%---12% in the first 3 yearsfter implantation has been reported in relation to the usef cohesive gels by a French firm in the past 2 decades.
R
Tp
The damage to health is not due to the toxicity of the gelontents, but rather to the capacity of silicone to induceocal defensive reactions and to move within the organism.he latter was the cause of the prohibition of treatment with
iquid silicone in increase and enhancement surgeries, andhe reason for the suspension of the use of breast implantsarketed by the investigated brand, given the possibility of
eleasing the substance into the body.Although the lymph node chains initially involved in a
eaction to silicone are those closest to the implant, nodalnvolvement is first detected due to extension at the cervicalevel. Otolaryngologists should be aware of this possibil-ty. We have carried out a review according to the findingsbserved in patients using these implants.
atients and Methods
hrough a longitudinal, descriptive and retrospective study,e collected patient data from the computer records of ourentre, labelled as diagnoses of cervical lymphadenopathy.
total of 342 subjects were thus identified between January002 and January 2012.
The only criteria for inclusion in the series were: under-oing a complete physical examination of the neck andodal regions accessible to the physician --- head, axillae,bdomen, groin ---, a cervical ultrasonography imaging study,co-Doppler ultrasound or computed tomography (CT) scan,nd histopathological confirmation by fine needle aspirationFNA).
Thus, we established a much more specific diagnosisf granulomatous adenitis or siliconoma due to foreignody reaction against silicone. We recorded the chrono-iological and anatomical peculiarities of the relevantymphadenopathies.
esults
able 1 shows the clinical and topographic data of all lym-hadenopathies detected.

Neck
Lymphadenitis
Due
to Silicone
Granulom
a After
Mam
mary
Implants
219
Table 1 Clinical, Topographic and Epidemiological Characteristics of the Lymphadenopathies Detected, Along With Attitude Adopted and Evolution.
Age, years Mammoplastytechnique
Time betweenmammoplastyand diagnosis,months
Level Cervicalchain
Number ofcervicaladenopathies
Maximumdiameter,mm
Other chains Attitude Evolution
38 Increase 12 iv Transversecervical
3 16 Axillary Expectant Stabilisation
33 Increase 18 iv Transversecervical
2 22 Mediastinal Cervicotomy Reappearance
44 Increase 10 v Spinal 1 14 AxillaryinternalMammarymediastinal
Expectant Increase
30 Reconstruction 8 iv Transversecervical
1 18 No Cervicotomy Disappearance
48 Increase 14 vi Anteriorjugular
1 20 No Expectant Stabilisation
38 Increase 24 iv---vi Internalandanteriorjugular
2 15 AxillaryMammaryinternal
Expectant Increase
50 Increase 40 v Spinal 3 24 Axillary Cervicotomy Disappearance33 Increase 60 v Transverse
cervical1 13 No Expectant Disappearance
46 Increase 22 iv Transversecervical
>3 19 AxillaryinternalMammarymediastinalparaaortic
Cervicotomy Disappearance
54 Reconstruction 36 iii---iv Internaljugular
2 17 No Cervicotomy Reappearance(reintervention)
33 Increase 70 iv Transversecervical
1 23 Axillary Expectant Stabilisation
29 Increase 20 iv Transversecervical
1 15 Axillarymediastinal
Expectant Disappearance

220 F.J. García Callejo et al.
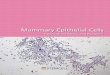
Figure 1 Fine needle aspiration (FNA) of an infiltratedlymphadenopathy with giant multinucleated cellularity phago-c(
piwp(tcdaa
cgmm
pIbpi3fvap
vwot
oipn
lt
Fl
p1p
1Rowm
D
Lpof bacterial growth and stable viscosity. However, its use wasbanned in the United States in 1965, due to the continuedoccurrence of side effects including foreign body granu-loma, cellulitis, ulcers, skin necrosis and even hepatitis and
ytising foreign material compatible with prosthetic materialPapanicolaou stain, 400×).
A total of 12 cases with significant cervical lym-hadenopathies secondary to silicone infiltration weredentified in the studied time period --- 3.5% of all patientsith a primary diagnosis of ‘‘studied adenopathy’’. The 12atients were all females aged between 29 and 54 yearsmean: 39.9±8.4 years) who had previously undergone plas-ic surgery for implantation of breast augmentation --- forosmetic purposes, or reconstruction --- after mastectomyue to malignancy, with a time interval ranging between 8nd 70 months (mean: 40.6±8.1 months) between surgerynd the onset of lymphadenopathy.
The report of the FNA conducted showed haematologi-al and lymphoid extension with abundant, optically empty,loboid material, compatible with prosthetic material andultinucleated giant cellularity phagocytising said foreignaterial by intracellular vacuolisation (Fig. 1).In all cases, the location of the affected lym-
hadenopathies was in caudal cervical segments, at levelsV---VI, with a maximum adenopathy diameter varyingetween 13 and 24 mm. In 50% of cases, cervical lym-hadenopathies detected by physical examination andmaging techniques were unique, whilst in 25% of cases,
or more were observed in the same patient. The mostrequently involved cervical lymph node chain was the trans-erse cervical, with 7 cases (Fig. 2). In addition, CT studieslso detected a significant increase of non-cervical lym-hadenopathies in 8 patients, mainly axillary.
The attitude adopted in these adenomegalies was conser-ative in 7 cases, whilst in the remaining 5 cases the decisionas to carry out excision by cervicotomy and obtain intra-perative biopsies, depending on the pathological volume ofhe nodules observed or the prior neoplastic history.
The histopathological image in the lymphadenopathiesbtained surgically was repetitive: large silicone vesiclesnterposed between activated lymphocytes, interfollicularlasma cells and multinucleated giant cells (Fig. 3). Malig-
ancy was ruled out in all cases.Regarding the attitude adopted, stabilisation of theesion or disappearance thereof upon physical examina-ion was observed in 9 patients. Of the 3 cases in which
Fwi
igure 2 Axial CT section showing lymphadenopathies in theeft, transverse cervical chain, up to 15 mm in size.
ersistence of lymphadenopathic growth was observed, only case underwent a new nodal excision surgery due to therior neoplastic history of the patient.
Removal of breast implants was conducted in all2 patients studied by the Department of Plastic andeconstructive Surgery. An MRI study detected only 1 casef prosthesis breakage, whilst microscopic silicone leaksere identified in another 6 cases after their postoperativeanipulation.
iscussion
iquid silicone was used for years in cosmetic medicine as aermanent, non-carcinogenic, filler substance, without risk
igure 3 Histopathological image of a lymphadenopathyhere the silicone is identified by an absence of staining of
ntercellular vacuoles (May---Grünwald---Giemsa stain, 100×).

ary I
rascncad
ocIcvtbtic5paai
hsctraa
csslataCtrifs
chdsa
C
T
Neck Lymphadenitis Due to Silicone Granuloma After Mamm
pneumonitis, especially in immunocompromised patients. InSpain, an exaggerated abnormal medical practice and igno-rance by patients have allowed the continuation of thesetechniques.
However, silicone or polydimethylsiloxane (PDMS) --- a syn-thetic polymer based on silicon, oxygen and methane --- isalso used for medical applications, as a solid in prosthesesand as a cohesive gel, especially for breast implants.
In the latter case, the European company mentioned ear-lier was reported in 2010 in relation to the occurrence ofpost-implantation breast cancer. Additionally, the potentialto detect subjects at risk of systemic silicone migration hasincreased.
Cervical lymphadenopathies infiltrated by silicone areoften undervalued by physicians and patients, as they donot offer signs of other growths.5,6 Omakobia et al.7 haverecently pointed to breast implants as a causal factor in theneck region. The high number of procedures for the enlarge-ment of breasts with implants, which carry an unaffordableincidence of breakage, promote this collateral effect.8
The first lymphadenopathies involved in this defencereaction against foreign substrates cause adenomegalies,which are often subclinical, in axillary and internal mam-mary chains.9---12 However, based on the classical cervicaltopography, there are 2 fundamental nodal groups com-prised by the anterior and lateral cervical chains of the neck.The latter is, undoubtedly, the most significant due to thenumber of constituent nodes and because it represents theprincipal cephalic lymphatic efferent, as well as retrogradefrom the thorax. The deep lateral nodes are systematisedin the triangle of Rouvière in the internal jugular, spinaland transverse cervical chains.13 This explains the poten-tial for head and neck neoplasms to generate intrathoracicmetastases, as well as the possibility that an axillary, nodal,granulomatous reaction by mammary inflammation directlycauses supraclavicular adenopathies. Consistent with this,Aktouf et al. reported an incidence of 8% distant exten-sion to the breast and axilla in a series of women who hadbeen implanted with PIP model prostheses.14 This wouldultimately justify why, in our review, the most commonlydetected nodules after breast implantation were the lowerlevels of the internal jugular and transverse cervical chains.
Cervical adenitis should be studied by FNA cytology. Thistest is harmless and effective, as the presence of multinu-cleated giant cells and especially the visualisation of siliconevacuoles in intranodular histiocytes are a highly reliable signof the condition.
The imaging technique of choice is CT, as it can identifythe number, shape, size and location of lymphadenopathiesin the chest and abdomen, which, according to the docu-mented criteria for radiological nodal malignancy, help toguide and complement diagnostic suspicion.15 Cervical ultra-sound imaging shows a characteristic, albeit not definitive,‘‘snowstorm’’ image, with diffuse hyperechogenicity andposterior reverberation caused by the difference in speed ofultrasounds through the infiltrated tissue.16,17 The Dopplertest does not provide valid additional information. How-ever, imaging tests are inconclusive and can generate a
false suspicion --- together with a physical examination --- ofcervical metastases or lymphoproliferative syndrome.18 Fur-thermore, silicone masses can capture fluorodeoxyglucoseintensely in PET-CT studies.19 In the case of patients withR
mplants 221
econstructive mammoplasties due to previous neoplasms,s in 2 of our cases, these circumstances require a prudenturgical resection attitude. Although the association of sili-one leakage with recurrence of tumour in the breast hasot been demonstrated, it does not rule out a potentialoncomitant recurrence of the disease. A cervicotomy withdenectomy provides abundant material and sufficient for aefinitive diagnosis.
From the standpoint of therapeutic efficacy, excisionf the siliconoma is not usually definitive unless signifi-ant segments of adjacent healthy tissue are also removed.n addition, the number of infiltrated lymphadenopathiesannot be predicted. Thus, the attitude to follow is contro-ersial. As lymphatic circulation has no anatomical barriers,he identification of a cervical lymphadenopathy infiltratedy silicone requires its neighbours to be considered poten-ially affected. Our results show that in 5 of the 7 casesn which we chose not to act, the lymphadenopathic pro-ess stabilised or disappeared spontaneously, whilst for the
cases where exploratory cervicotomy was performed, lym-hadenopathy recurred in 2 patients. Cawrse and Pickfordlso warned of the recurrence of adenomegaly symptomsfter excision of adenitis infiltrated by gel derived from PIPmplants.20
Except for cases with suspicion of malignancy, given theigh number of cases where excision is not satisfactory, theurgical attitude in cases of cervical lymph node growth withonfirmed infiltration by silicone should be discussed withhe patient. In our opinion, surgical approaches should beestricted to those patients with marked aesthetic alter-tions, and always after providing adequate informationbout a potential recurrence of the lesions.
Other documented options, including minocycline,yclosporine and isotretinoin, have shown partial and tran-ient clinical responses, as well as a considerable array ofide effects.21,22 Etanercept has provided valid results in skinesions in direct contact with silicone.23,24 Imiquimod, annti-TNF agent used successfully in sarcoidosis which inhibitshe expression of the GLI-1 oncogene, has also shown ther-peutic efficacy in cases of systemic nodal progression.3,22
O2 laser can vaporise the granuloma by overcoming thehermal stability of polysiloxane, although not without theisk of devitalising adjacent tissue. Thus, it is more safelyndicated for silicone globules in the facial or thoracic sur-aces, and can also remove multiple scattered lesions in theame surgical procedure.25
In short, we are faced with a new cervical entity. Physi-ians should be aware of the location, as well as the medicalistory of each individual. When adequately filiated, theefinitive therapeutic option is still a matter for discus-ion, in terms of the experience of side effects which breastugmentation surgical procedures can cause.
onflict of Interests
he authors have no conflict of interests to declare.
eferences
1. Yanagihara M, Fuji T, Wakamatu N, Ishizaki H, TakeharaT, Nawate K. Silicone granuloma on the entry points of

2
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
22
acupuncture, venepuncture and surgical needles. J CutanPathol. 2000;27:301---5.
2. Narins RS, Beer K. Liquid injectable silicone: a review of its his-tory, immunology, technical considerations, complications andpotential. Plast Reconstr Surg. 2006;118:77---84.
3. Macaron NC, Cohen C, Chen SC, Arbiser JL. Gli-1 oncogeneis highly expressed in granuloma skin disorders, includingsarcoidosis, granuloma annulare and necrobiosis lipoidica dia-beticorum. Arch Dermatol. 2005;141:259---62.
4. Lai CS, Lin TM, Lee SS, Yang CC, Lin SD. Surgical treatment offacial siliconoma involving the temporal area. Plast ReconstrSurg. 2005;115:553---8.
5. Lahiri A, Waters R. Locoregional silicone spread after high cohe-sive gel silicone implant rupture. J Plast Reconstr Aesthet Surg.2006;59:885---6.
6. Vaamonde R, Cabrera JM, Vaamonde-Martín RJ, Jimena I, Mar-cos Martín J. Silicone granulomatous lymphadenopathy andsiliconomas of the breast. Histol Histopathol. 1997;12:1003---11.
7. Omakobia E, Oorter G, Armstrong S, Denton K. Silicone lym-phadenopathy: an unexpected cause of neck lumps. J LaryngolOtol. 2012;126:970---3.
8. Khan UD. Left unilateral breast autoinflation and intraprostheticcollection of sterile pus: an unusual operative finding of sili-cone gel bleed with silicone lymphadenitis. Aesthetic Plast Surg.2008;32:684---7.
9. Dragu A, Theegarten D, Bach AD, Polykandriotis E, Arkudas A,Kneser U, et al. intrapulmonary and cutaneous siliconomas aftersilent silicone breast implant failure. Breast J. 2009;15:496---9.
0. Falk S, Neudert H, Radeljic A. Axilläre silicon-lymphadenopathie nach mammaaugmentation. GeburtshilfeFrauenheilkd. 1996;56:55---7.
1. Ganau S, Tortajada L, Rodríguez X, González G, Sentís M. Sili-cone lymphadenopathy: an inusual cause of internal mammarylymph node enlargement. Breast J. 2008;14:502---3.
2. Kaufman GJ, Sakr RA, Inguenault C, Sarfati I, Nos C, Clough KB.Silicone migration to the contralateral axillary lymph nodes and
breast after highly cohesive silicone gel implant failure: a casereport. Cases J. 2009;2:6420.3. Medina JE. Linfadenectomías cervicales. In: Suárez C, GilCarcedo LM, Marco J, Medina JE, Ortega P, Trinidad J, editors.
2
F.J. García Callejo et al.
Tratado de Otorrinolaringología y Cirugía de Cabeza y Cuello.2nd ed. Madrid: Panamericana; 2007. p. 3938---63. Tomo IV.
4. Aktouf A, Auquit-Auckbur I, Coquerel-Beghin D, Delpierre V,Milliez PY. Augmentation mammaire par prothèses en gel desilicone de la marque Poly Implant Prothèses (PIP): étude rétro-specive de 99 patientes. Analyse des ruptures et prise encharge. Ann Chir Plat Esther. 2012;57:558---66.
5. García Callejo FJ, Dualde Beltrán D, Benlloch Ramos E, MontoroElena MJ, Hernandorena González M, Marco Algarra J. Empleode patrones de imagen en la identificación de metástasis cervi-cal mediante tomografía computarizada en tumores de cabezay cuello. Acta Otorrinolaringol Esp. 2008;59:257---62.
6. Román Soler A, Sánchez Torres L. Imagen Diagn. Siliconoma.2011;2:75---6.
7. Lorenz R, Stark GB, Hedde JP. The value of sonography for thediscovery of complications after the implantation of siliconegel prostheses for breast augmentation or reconstruction. Rofo.1997;166:233---7.
8. Péoc’h M, Duprez D, Grice G, Fabre-Bocquentin B, Gressin R,Pasquier B. Silicone lymphadenopathy mimicking a lymphomain a patient with a metatarsophalangeal joint prosthesis. J ClinPathol. 2000;53:549---51.
9. Grubstein A, Cohen M, Steinmetz A, Cohen D. Siliconomas mim-icking cancer. Clin Imaging. 2011;35:228---31.
0. Cawrse NH, Pickford MA. Cutaneous manifestation of siliconedissemination from a PIP implant --- a case for prophylacticexplantation. J Plast Reconstr Aesthet Surg. 2011;64:208---9.
1. Arin M, Bate J, Krieg T, Hunzelmann N. Silicone granulomaof the face treated with minocycline. J Am Acad Dermatol.2005;52:53---6.
2. Baumann LS, Halem ML. Lip silicone granulomatous foreign bodyreaction treated with aldara (imiquimod 5%). Dermatol Surg.2003;29:429---32.
3. Pastermack FR, Fox LP, Enger DE. Silicone granuloma treatedwith etanercept. Arch Dermatol. 2005;141:13---5.
4. Desai AM, Browning J, Rosen T. Etanercept therapy for silicone
granuloma. J Drugs Dermatol. 2006;5:894---6.5. Chui CH, Fong PH. Carbon dioxide laser vaporization of facialsiliconomas: flash in the pan or way of the future. Ann PlastSurg. 2008;60:272---5.