Embed Size (px)
Citation preview

12/9/2014
1
New England Practice & Policy
Webinar #2
December9,20141:00‐2:30PM(Eastern)
“MeetingtheNeedsofFamiliesintheChildWelfareSystem AffectedbySubstanceUseDisorders"
Screening and Assessment for Family Engagement
and Retention
NancyK.Young,PhDExecutiveDirector
NationalCenteronSubstanceAbuseandChildWelfare
SaraJ.Becker,PhDNewEnglandAddiction
TechnologyTransferCenterBrownUniversity
Welcome & Opening Remarks
• Establishedin2002• Anationalresourcecenter
providinginformation,expertconsultation,trainingandtechnicalassistancetochildwelfare,dependencycourtandsubstanceabusetreatmentprofessionalstoimprovethesafety,permanency,well‐beingandrecoveryoutcomesforchildren,parentsandfamilies
National Center on Substance Abuse and Child Welfare
NE ATTC Mission
• Establishedin1993bySAMHSA• Nationalnetworkcomprisedof10regionalcenters,4nationalfocusareacenters,andacoordinatingoffice.
• Networkmissionisto:raiseawarenessandskillsoftheworkforcethatservesindividualsaffectedbysubstanceusedisorders;acceleratetheadoptionandimplementationofevidence‐basedpractices;andfosterregionalandnationalalliances amongdiverseclinicians,researchers,policymakers,fundersandtherecoverycommunity.

12/9/2014
2
In your region, what are the top three general areas of greatest training need? Please select three responses. (N=63)
Collaboration across systems(e.g. CWS, AOD,
Courts) Evidence-based interventions for families affected
by SUDs
Retention and engagement of
families in treatment
67.2%65.6% 63.9%
Budgeting for and sustaining new initiatives
32.8% (20)
Substance use screening and assessment
32.8% (20)
Tracking and measuring family outcomes
26.3% (15)
Other 3.3% (2)(N=41)
(N=40)
(N=39) Assessing impact of parental substance abuse on children, especially infants and those under 5 throughout involvement. Budgeting for sufficient staff and services to respond to increased need. Cross training of DCF and providers.
All of those, truly!
• A National Perspective Screening and Assessment for Family Engagement and Retention
• A Case Example: Connecticut’s Recovery Specialist Voluntary Program Collaborative Model
• National Resources and Tools• The next webinar in the series• Discussion
Today’s Webinar Agenda
LindaCarpenter,MEdProgramDirector
NationalCenteronSubstanceAbuseandChildWelfare
A National Perspective
Screening and Assessment for Family
Engagement and Retention
Improvingtheoutcomesofchildrenandfamiliesaffectedbyparentalsubstanceuse requiresacoordinatedresponsewhichdrawfromthetalentsandresourcesofatleastthreesystems:• ChildWelfare• SubstanceAbuse
Treatment• Courts
Better together
No Single Agency Can Do This Alone

12/9/2014
3
Mission and Underlying Values
Howdoesyourmissionimpactscreening,assessment,engagementandretention?
• Whomdoyouserve?• Differenceinperceptionoftheprimaryclient:theparent,the
child,thefamily.• Differenceinperceptionofthetargetpopulation• Differenceinperceptionofaddiction,recoveryandparenting• Differenceinunderstandingandperceptionofterms(e.g.
screening,assessment,successfulcompletion,etc)
9
EarlyScreeningandIdentificationofparentalsubstanceuseinchildwelfarecasesiscritical.
• 61%— thepercentageofconfirmeddrugoralcoholdependenceamongsubstantiatedabuseorneglectcasesmissedbyfrontlineCWSsocialworkers(Gibbons,Barth,Martin,2005)
• Anecdotalreportsfromchildwelfarestaffclaimparentalsubstanceabuseasafactorintheircasestobeashighas85%.
Current Screening Practices
• Currentlynostatehasauniversalscreeningforallchildwelfarecases
• Somescreenatinvestigativestage• Someonlywithsubstantiatedcases• Somethroughoutthelifeofthecase
• Somestatesandlocalitiesreportmuchhigherratesofsubstanceabusewhenthereis
• Workertraining—togainabetterunderstandingofaddictionandrecovery,engagementandtrauma
• Agreementonwho,how,whatandwhyofscreening• Interagencyagreementsonwhatwillhappenasaresultofapositivescreen
11
Questions to Consider with a Screening Protocol?
• Whoisyourtargetpopulation?• UniversalorSpecificSegment• ScreeningInvs.ScreeningOut
• Doesyourprogramaddressotherissuesthatfamiliesareexperiencing?• Whathappenswithpositivescreen?• Howarereferralsmadeforfurtherassessment?• Howisinformationcommunicatedwithparents?Withtreatmentproviders?Areappropriateconsentsinplaceandconsistentlysigned?• Doprovidersacceptthescreeningresults?• Whatfollow‐upexistswithparents?Withtreatmentproviders?• Doyouscreenonlywhenchildsafetyisanissue?• Aresome“substances”agreaterconcernthanothers?• Whattrainingandsupportdostaffwhoareconductingthescreeningneedtofeelcomfortable/confidentaskingthesequestions?
12

12/9/2014
4
Timely engagement and access to assessment and
treatment matters.
Questions to Consider with an Assessment Protocol?
• Howistheindividualreferredforassessment?• Onanaveragehowlongdoesittaketogofromreferraltoassessment?• Whoconductstheassessmentandwhattoolsareused?• Whatadditionalinformationfromchildwelfareandotherpartnerswouldbehelpfulinunderstandingtheneedsoftheparent,childandfamily?
• Howisinformationcommunicatedtotheparent?Tothechildwelfarestaff?Tothecourts?Aretheappropriateconsentsinplaceandconsistentlysigned?
• Whathappensiftheparentdoesn’tshowforassessment?• Whatarethenextstepsiftreatmentisindicated?Iftreatmentisnotindicated?• Ifthepersons/systems/agenciesconductingtheassessmentsarenotthesameastheonesprovidingtreatment,isthereawarmhand‐off?
14
Assessment is an On-Going Process
Assessmenthappensalongacontinuumtodetermine:PresenceandImmediacy
• Isthereanissuepresent?
• Whatistheimmediacyoftheissue?
NatureandExtent• Whatisthenatureoftheissue?
• Whatistheextentoftheissue?
Developing&MonitoringChange,TransitionsandOutcomesofTreatmentandCasePlans
Whatistheresponsetotheissue?
Aretheredemonstrablechangesintheissue?
Isthefamilyreadyfortransition?
DidtheInterventionswork?
Rethinking Engagement
Will they come?
16
12/9/2014
5
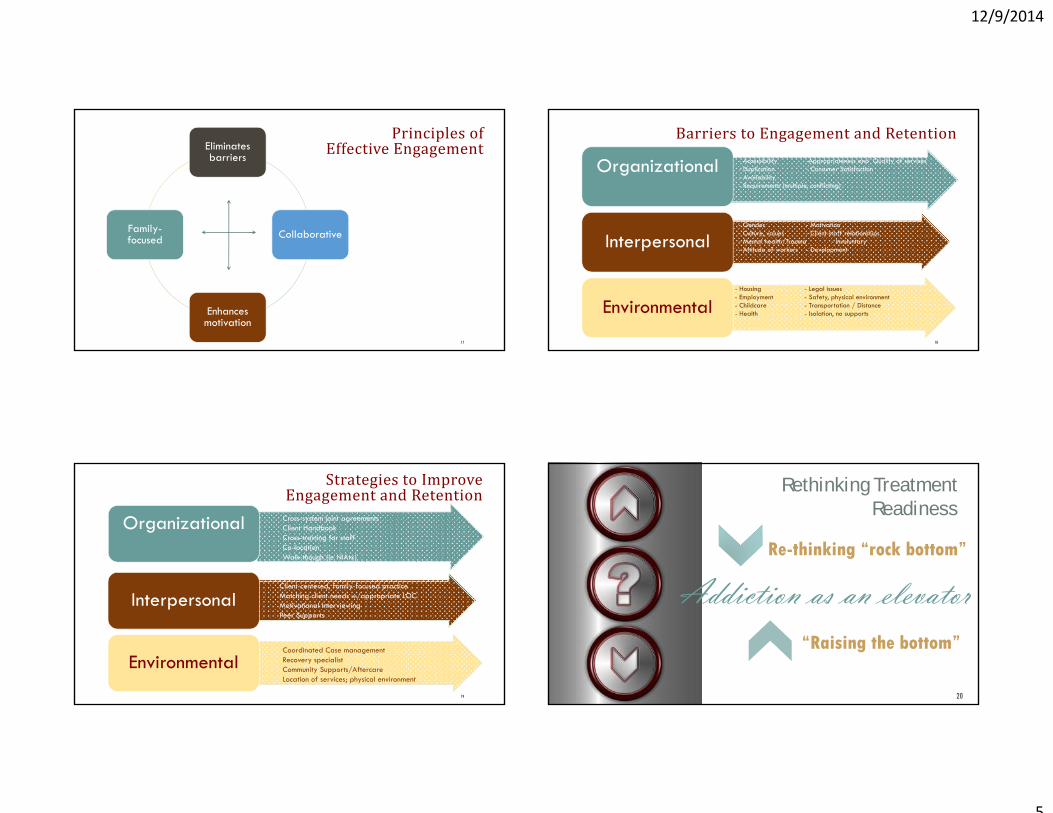
PrinciplesofEffectiveEngagement
17
Eliminates barriers
Collaborative
Enhances motivation
Family-focused
BarrierstoEngagementandRetention
18
• - Accessibility -Appropriateness and Quality of services• - Duplication - Consumer Satisfaction• - Availability • - Requirements (multiple, conflicting)
Organizational
• - Gender - Motivation• - Culture, values - Client-staff relationships• - Mental health/Trauma - Involuntary• - Attitude of workers - Development
Interpersonal
• - Housing - Legal issues• - Employment - Safety, physical environment• - Childcare - Transportation / Distance• - Health - Isolation, no supportsEnvironmental
StrategiestoImproveEngagementandRetention
19
Organizational
Interpersonal
EnvironmentalCoordinated Case managementRecovery specialistCommunity Supports/Aftercare Location of services; physical environment
Client-centered, family-focused practiceMatching client needs w/appropriate LOCMotivational InterviewingPeer SupportsRecovery Specialist
Cross-system joint agreementsClient HandbookCross-training for staffCo-locationWalk-though (ie NIAtx)
Rethinking Treatment Readiness
Addiction as an elevatorRe-thinking “rock bottom”
“Raising the bottom”
20

12/9/2014
6
Rethinking Treatment Readiness
Re-thinking “Rock Bottom”
“Raising the bottom”
• “Tough love” - in the hopes that they will hit rock bottom and wanting to change their life.
• Collective knowledge in the community is to “cut them off, kick them out, or stop talking to them.”
• Addiction as a disease of isolation
• Getting off on an earlier floor• Has realistic expectations and
understands both the neuro-chemical effects on people with substance related and addiction disorders and difficulties and challenges of early recovery
• Readiness • Recovery occurring in the context of
relationships
21
Drop‐offAnalysis221 cases referred for SA assessment
(assuming all caregivers receive an assessment)
169 received SA assessment (144 assessed, 25 in treatment but no assessment date)
(24% drop off = 52)
Number referred to SA treatment = 166
Number made it to SA treatment = 162
(2% drop off)
85 successfully completed SA tx*
Payoff22
*This#mayincreaseslightlyassomeclientsarestillenrolledintreatmentandmaysuccessfullycompleteinthefuture
• PairedCounselorandChildWelfareWorker• CounselorOut‐StationedatChildWelfare• OfficeorCourt• ParentMentorsandRecoverySpecialists• SubstanceAbuseSpecialists• MultidisciplinaryJointCasePlanningTeams• FamilyTreatmentDrugCourt
Effective Models of Collaborative Practice Connecticut: A Case Example
Listen for the key premises and principles

12/9/2014
7
Taming the Many Headed Dragon:Recovery Specialist Voluntary
ProgramCollaborative Model
Marilou Giovannucci, Manager, (CIP Director) Judicial Branch Christine Lau, Regional Administrator, Department of Children and Families (DCF)
Janet Storey, Behavioral Health Program Manager, Department of Mental Health and Addiction Services (DHMAS)
Jane Ungemack, Assistant Professor, University of Connecticut School of Medicine (UCHC)
Recovery Specialist Voluntary Program(RSVP)
Both a policy and a practice model Voluntary program offered to parent/caregiver whose child or children are removed by court order as a result of alleged abuse or neglect and substance abuse is a factor in the removal RSVP introduced to parent/caregiver by court staff (Court Services Officer) at the first court hearing on the Order of Temporary Custody (OTC) Removal Parent signs an agreement to participate that includes adherence to a court standing order
RSVP is a collaborative program of: Department of Children and Families (DCF) Department of Mental Health and Addiction Services (DMHAS) Judicial Branch ‐ Court Operations
Along with: Advanced Behavioral Health, Inc. (ABH), an administrative services organizationOffice of the Chief Public Defender, Juvenile Delinquency and Child Protection UnitOffice of the Attorney General
Began as an IDTA project with the NCSACW27
Funding, Data Sharing and Communication
• Financing the initiatives: • Re‐purposed existing Project Safe recovery case management dollars;• Developed braided funding among partners, including CIP dollars for training and evaluation;• Re‐deployed savings (hair test reductions) to expand the program;• Leverage competitive federal grant dollars to test new models
• Began organically• Survived administration and staffing changes and expanded
• Communication and Confidentiality on the client level:• Developed an MOA and Standing Order governing communication/confidentiality and data sharing;
• Data Sharing to Inform Practice and to Evaluate Outcomes:• Developed a Data Use/Sharing Agreement
12/9/2014
8
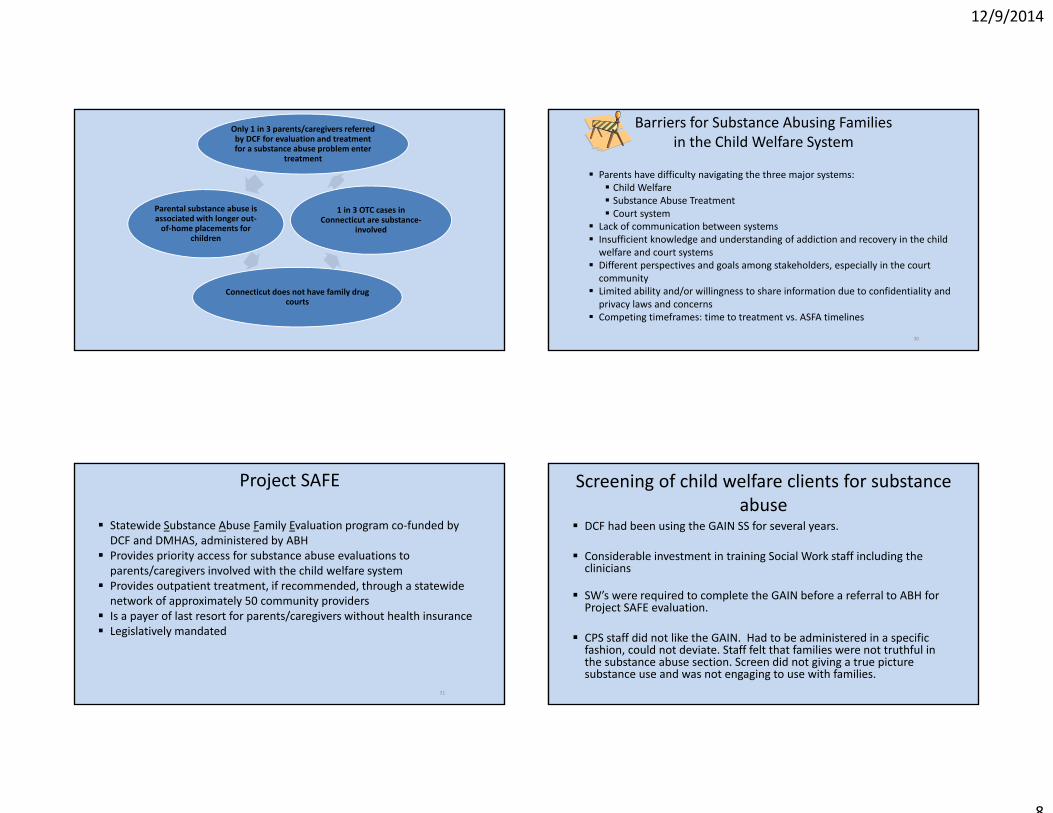
Connecticut does not have family drug courts
1 in 3 OTC cases in Connecticut are substance‐
involved
Only 1 in 3 parents/caregivers referred by DCF for evaluation and treatment for a substance abuse problem enter
treatment
Parental substance abuse is associated with longer out‐of‐home placements for
children
Barriers for Substance Abusing Families in the Child Welfare System
Parents have difficulty navigating the three major systems: Child Welfare Substance Abuse Treatment Court system
Lack of communication between systems Insufficient knowledge and understanding of addiction and recovery in the child welfare and court systems
Different perspectives and goals among stakeholders, especially in the court community
Limited ability and/or willingness to share information due to confidentiality and privacy laws and concerns
Competing timeframes: time to treatment vs. ASFA timelines
30
Project SAFE
Statewide Substance Abuse Family Evaluation program co‐funded by DCF and DMHAS, administered by ABH
Provides priority access for substance abuse evaluations to parents/caregivers involved with the child welfare system
Provides outpatient treatment, if recommended, through a statewide network of approximately 50 community providers
Is a payer of last resort for parents/caregivers without health insurance Legislatively mandated
31
Screening of child welfare clients for substance abuse
DCF had been using the GAIN SS for several years.
Considerable investment in training Social Work staff including the clinicians
SW’s were required to complete the GAIN before a referral to ABH for Project SAFE evaluation.
CPS staff did not like the GAIN. Had to be administered in a specific fashion, could not deviate. Staff felt that families were not truthful in the substance abuse section. Screen did not giving a true picture substance use and was not engaging to use with families.

12/9/2014
9
Screening of child welfare clients for substance abuse
In 2011, DCF began work to implement a new Practice Model with a strong emphasis on family engagement;
Implementation of Differential Response System (DRS) in 2012.
With the implementation of DRS, the GAIN was dropped as an expectation for Family Assessment Response (FAR) staff.
GAIN was believed to not be useful and a barrier in family engagement given the nature of the tool.
Investigation staff felt they should not use it either and was later dropped as an expectation for them.
Instead FAR and Investigation staff use a set of guiding questions to assess factors and indicators that would point to substance abuse and a referral to ABH for Project SAFE evaluation
DCF Assessment Process
History of using the GAIN Short Screen to assess parental substance problems Reduce reliance on screening tools to assess families strengths and needs; Partner with the family at every step of the child welfare case; Use motivational interviewing to engage families; Examine behaviors and supports systems to inform child welfare decision‐making.
Goals of RSVP
Help parents navigate the DCF, Court and substance abuse treatment systems Establish a shared definition of substance abuse treatment and recovery Help the systems talk to each other Do it fast!
Shared Mission
Improve child well‐being, safety and permanency when parental substance abuse has been identified as a significant issue resulting in children being removed from their homes.
36

12/9/2014
10
Goals of RSVP Collaboration
Increase system capacity to better serve families impacted by substance use disorders: Implement a recovery‐oriented integrated system of care for families Improve access to evaluation and treatment services and collateral recovery supports
Facilitate collaborative problem resolution for concerns and issues raised by the parties involved
Bridge multi‐system policies, procedures and practices Improve communication and information exchange among state agencies, practitioners, communities, consumers and families
Engage and educate the court community including judges, agency and parent/child attorneys and court staff
Structure and Processes of RSVP
Operates under a Memorandum of Understanding/Data Use Agreement Oversight by Agency Commissioners and Chief Administrative Judge Shared decision‐making and leadership by DCF, DMHAS, and Judicial through the Core Management Team Substance Abuse Managed Service System (SAMSS) meeting in each area office Solicits stakeholder input Develop and jointly provide multidisciplinary training that promotes cross‐agency understanding of: Addiction and recovery Evidence‐based interventions Children’s mental health Child development and well‐being Impact of substance abuse/dependency on parenting Culturally and gender‐appropriate service delivery
RSVP Program Components
Three phases lasting approximately 3 months each at different levels of intensity and frequency of meetings with the Recovery Specialist and random alcohol/drug tests Engagement in substance abuse treatment Attendance at self‐help support groups Participation in case conferences
RSVP Recovery Specialist
ABH staff, Supervised by ABH Program Manager Trained to use motivational interviewing with clients Identify needs and Assist parent/caregiver in accessing and engaging in
substance abuse treatment and other support services Advocates for parent/caregiver Conducts reliable random drug screens Tool to support recovery, Not punitive
Provides regular compliance monitoring to DCF, courts, and attorneys Supports parent/caregiver in increasing building recovery capital and self
advocacy skills through recovery coaching

12/9/2014
11
Substance Abuse Managed Service System(SAMSS) Meetings
Unique feature not found in drug court models Developed organically on the local level, expanded and supported by leadership Solution‐focused Facilitated by DCF Held weekly or biweekly Case overview presented by DCF Social Worker Active participation from DMHAS, ABH and local treatment providers
SAMSS Supports Recovery Capital
SAMSS is viewed as an systems intervention: Review evaluation findings and recommendations for individual parent/caregiver Develop a plan of action through collaborative problem solving and resource identification to eliminate barriers to recovery Close collaboration and communication among providers, DCF and clients provides opportunities for engagement and treatment to take place Discussions highlight system issues that create barriers to treatment Having decision makers participate assists in addressing systems issues in a timely manner
Court Case Status Conferences
Facilitated by Court Services Officer; The purpose is to discuss compliance with RSVP, engage and encouragethe parent in her/his recovery efforts,
Reinforce the impact of recovery on their court case; Allow the parent to share any barriers or challenges that s/he is experiencing; and
Engage in collective case problem‐solving.
Data for the Evaluation
DCF Child-centered Numbers and characteristics of OTC cases Family reunification, child permanency and re-entry Family strengths/needs and safety assessments
DMHAS Adult client-centered Number and characteristics of substance abuse treatment clients
Judicial Child-centered Time to disposition and disposition status
ABHNumber and characteristics of clients served by RSVPTimeliness of treatment entryMonthly functional assessmentsProgram participation and discharge status

12/9/2014
12
Co-occurring Problems among RSVP Clients: 2009 – 2012
(n=208)
Ever arrested 72%
Current criminal justice involvement 51%
History of domestic violence 42%
History of trauma 24%
History of mental health problems 51%
Unemployed 79%
Never married or divorced/separated/widowed 74%
Problem Substances among RSVP Clients in Treatment: 2009 – 2012
24%
16%
29%
8%
15%
42% 44%
34%
18%
39%
ALCOHOL COCAINE/CRACK HEROIN OTHER OPIATES MARIJUANAPrimary Problem Any Problem
Substance Abuse Treatment Outcomes for RSVP Clients
97% of OTC enrollees referred to RSVP were evaluated to need treatment84% of RSVP clients enrolled in substance abuse treatment68% within 30 days
61% had a prior history of substance abuse treatmentLevel of care: 6% Detoxification only15% Methadone maintenance30% Outpatient28% Intensive outpatient/partial hospitalization21% Residential
Median length of stay was 88 days75% of RSVP clients had a successful discharge from their RSVP-related treatment
admission compared to 43% of substance abuse clients statewide
Percent of Child Exits Reaching Permanent Placement within 12 Months: RSVP vs. Statewide*
0
20
40
60
80
RSVP Statewide
74%
49%
* 76% of RSVP children were reunified with their parent/caregiver

12/9/2014
13
Summary of Findings
Substance‐abusing parents in need of treatment are being identified and enrolled Participants who comply with RSVP are more likely to be successfully reunited with their
children and in a more timely manner RSVP clients present with multiple and complex problems that require intensive
intervention and coordination across service systems Some challenges remain: 1‐in‐4 eligible OTCs are not referred to RSVP Statewide expansion Obtaining access to other needed services Housing Mental health services Trauma services Employment/vocational training
Sustaining the Efforts
• Sustaining your efforts:• Report utilization and outcomes monthly, quarterly and annually to leadership and stakeholders;
• Examining economic impact;• Celebrate success with program participants.• Exploring creative funding sources for expansion. (Pay for Success, Social Impact Bonds)
Parting Words
“Together we embrace safety, permanency and well‐being, and substance abuse recovery. Our ultimate goal is to achieve positive
results for a family that will last a lifetime.”
NCSACWWrap-up,Resources and
Tools

12/9/2014
14
Guiding Principles
• Improvingtheoutcomesofchildrenandfamiliesaffectedbyparentalsubstanceusedemandsurgentattentionandthehighestpossiblestandardsofpracticefromeveryoneworkinginsystemschargedwithpromotingchildsafetyandfamilywell‐being.
• Since 85% of all children with substantiated abuse and neglect cases stay home or return home to their parents, child and family well‐being requires services for both children and families.
• Successispossibleandfeasible.Staffinchildwelfare,substanceabuse,andcourtsystemshavethedesireandpotentialtochangeindividuallivesandcreateeffectivepracticesandresponsiblepublicpolicies.
Guiding Principles
• Thefamilyisthefocusofconcern• Theteamisthetool,andpeople,nottools,makedecisions
• Problemsdon’tcomeindiscretepackages;theyarejumbledtogether
• Ongoingassessmentisasharedresponsibility• Developingandsustainingeffectivecollaborationsishard—butessentialwork
• Sharedmissionandvision‐ agreementandunderstandingoftargetpopulationandexpectedoutcomes
• Clearandconsistentreferralprocess—preferablywarmhand‐off
• Coordinatedcaseplanning,informationsharing,• timelyandongoingcommunicationandfollow‐up• Understandingofandattentiontocompeting“clocks”—timeframes–recognizingthattimeisoftheessence!
Essential Elements Cross-System Collaboration Includescollaborativepracticesandtoolsforlinkingsubstanceabuse,childwelfare,andfamilycourts.
• CollaborativePracticeModel• MatrixofProgress• CollaborativeValuesInventory
• CollaborativeCapacityInstrument
Pleasevisitourresourcepage:https://www.ncsacw.samhsa.gov/collaboration/default.aspx

12/9/2014
15
Collaborative Practice
• SAFERR• CollaborativePracticeModel
• Cross‐SystemsCollaborationPrimer
• Cross‐SystemsDataPrimer
Pleasevisitourresourcepage:http://www.ncsacw.samhsa.gov/resources
58
1. Understanding Substance Abuse and Facilitating Recovery: A Guide for Child Welfare Workers
2. Understanding Child Welfare and the Dependency Court: A Guide for Substance Abuse Treatment Professionals
3. Understanding Substance Use Disorders, Treatment and Family Recovery: A Guide for Legal Professionals
National Center on Substance Abuse and Child WelfareOnline Tutorials
Please visit: www.ncsacw.samhsa.gov
Client Screening,
Assessment, Engagement &
Retention
Pleasevisitourresourcepage:https://www.ncsacw.samhsa.gov/resources/daily‐practice‐client.aspx
Resource: Substance Abuse Specialist in Child Welfare Agencies
and Dependency Courts
6 State Case Studies
Todownloadacopy,pleasevisit:http://www.ncsacw.samhsa.gov/files/SubstanceAbuseSpecialists.pdf

12/9/2014
16
Resource: Drug Testing in Child Welfare: Practice and
Policy Considerations
http://www.ncsacw.samhsa.gov/files/DrugTestinginChildWelfare.pdf
Todownloadacopy,pleasevisit:http://www.ncsacw.samhsa.gov/files/SAFERR.pdf
Resource: Screening and Assessment for Family Engagement, and Recovery
(SAFERR)
Todownloadacopy,pleasevisit:
Just Released !
Todownloadacopy,visit:http://store.samhsa.gov/shin/content//SMA14‐4816/SMA14‐4816.pdf
• Assistsbehavioralhealthprofessionalsinunderstandingtheimpactandconsequencesforthosewhoexperiencetrauma
• Discussespatientassessment,treatmentplanningstrategiesthatsupportrecovery,andbuildingatrauma‐informedcareworkforce
NationalCollaborativeonWorkforceandDisabilityPolicyBrief‐ http://www.ncwd‐youth.info/policy‐brief‐02
SAMHSATIPs:TIP31ScreeningandAssessingAdolescentsforSubstanceUseDisordersandTIP32TreatmentofAdolescentsWithSubstanceUseDisordershttp://store.samhsa.gov/shin/content/SMA01‐3596/SMA01‐3596.pdf
The ATTC and the National Institute on Drug Abuse jointly created a suite of blending products: http://www.attcnetwork.org/explore/priorityareas/science/blendinginitiative/
NewEnglandResources:RhodeIsland‐ AdolescentHealthCareTransitionProgram‐ OfficeofSpecialHealthcareNeedsattheDept.ofHealth:http://www.health.ri.gov/programs/adolescenthealthcaretransition/
Massachusetts ‐ DepartmentofMentalHealthTransitionAgeYouth(TAY)Initiativehttp://www.mass.gov/eohhs/gov/departments/dmh/transitional‐age‐youth‐initiative.html
Connecticut ‐ Dept.ofMentalHealth&AddictionsServices‐ YoungAdultServicesDivisionhttp://www.ct.gov/dmhas/cwp/view.asp?q=334784
Vermont‐ VermontFamilyNetwork‐ resourceguidefortransitionageyouthwithmentalhealthorsubstanceuseissues: http://www.vermontfamilynetwork.org/wp‐content/uploads/2012/12/Resource‐Guide‐for‐Parents‐of‐Transition.pdf
Maine ‐ MaineYouthTransitionCollaborativewebsite‐ http://maine‐ytc.org/
NewHampshire‐ Dept.ofHealthandHumanServices‐ YoungAdultResourceGuide:http://www.dhhs.state.nh.us/dcyf/documents/youngadult.pdf
Resources - Youth

12/9/2014
17
Next in theWebinar Series…
In your region, what are the top three special topic areas of greatest training need? Please select three responses. (N=63)
Trauma-informed approaches to
careOpioid abuse and
medication-assisted
treatmentTransition-age
youth; aging out of the system70.5%
59.0%52.5%
Substance-exposed newborns 37.7% (23)
Prescription drug abuse 26.2% (16)
Minority and underserved populations
17.5% (10)
Parental custody rights 13.1% (8)
Medicaid/ACA implementation 9.8% (6)
Other 8.2% (5)(N=43)
(N=36)
(N=32)
How to assess child safety related to substance abuse/reunification
Training and support for foster parents who are asked to care for children impacted by parental substance abuse.
CBT skills training for providers
Diagnosis
Screening and treatment for adolescents
The Webinar SeriesSeptember 30, 2014Kick‐OffWebinar
December 9, 2014ScreeningandAssessmentforFamilyEngagementand
Retention
March 2015ConductingTrauma‐InformedSystems
AssessmentQ&AandDiscussion

12/9/2014
18
Contact InformationNancyK.Young,PhDExecutiveDirectorNationalCenteron
(714)505‐3525
SaraJ.Becker,PhDNewEnglandAddiction
TechnologyTransferCenterBrownUniversity
[email protected](401)863‐6604